fractures of the proximal humerus in children
TRANSCRIPT

Abstract Ninety-one children who had been treated forfractures of the proximal humerus (59 metaphyseal frac-tures; 32 epiphyseal fractures) from 1980 to 1992 at anaverage age of 10.7 years (range 3 to 14 years) werereviewed. In 82 cases a nonsurgical treatment (Desaultbandage in 11 cases, hanging cast in nine cases, closedreduction and shoulder spica cast in 62 cases) was per-formed. At a mean time of 7.2 months (range 1 to156 months), 96% of patients showed good/excellentclinical results. In 15 cases, radiographs were reviewed ata mean follow-up of 8 years (range 1 to 23.5 years): justa slight metaphyseal or meta-diaphyseal varus deformitywas found in three cases. In nine cases surgery wasrequired. Patients were reviewed by clinical examinationat a mean time of 34.8 months (1–150 months), and in sixcases radiographs were reviewed at a mean time of5 years and 5 months (range 1 to 12.5 years) after surgery.In one case, a septic process occurred, that caused asevere deformity of the epiphysis and a noticeable func-tional deficit. Good/excellent clinical and radiographicresults were achieved in the other patients.Conservative treatment of fractures of the proximalhumerus in children is recommended. Surgery should bereserved for specific cases.
Keywords Proximal humerus · Epiphyseal fracture ·Children · Conservative treatment
Introduction
Fractures of the proximal humerus represent approxi-mately 0.45% of all pediatric fractures [1], and 4%–7%of all epiphyseal fractures [2, 3]. The proximal physis ofthe humerus accounts for 80% of the growth in length ofthis bone. As a consequence, its remodeling potential isconsiderable, and is related to the age of the patient: theolder the child the lower the potential [4].
Excellent results are generally reported in the litera-ture after conservative treatment. Surgery is very rarelyindicated and may lead to several complications.
The purpose of this work was to review our experi-ence in the treatment of these fractures.
Materials and methods
Ninety-one consecutive cases (52 boys, 39 girls) of frac-tures of the proximal humerus (metaphyseal and epiphy-seal fractures) that came to our observation between1980 and 1992 were included in the study.
The mean age at the time of fracture was 10.7 years(range 3 to 14 years). In 66 cases, presentation wasimmediately after the trauma; the other children present-ed after a mean time of 4.6 days (range 1 to 26 days).Seven patients had multiple injuries (Fig. 1).
The Salter-Harris [5] and Neer-Horwitz [3] classifica-tions were used for radiographic assessment.
As concerns the type of fracture, 59 cases were meta-physeal fractures, 32 children showed epiphyseal frac-tures: among these cases, two were graded type 1 and 30type 2 according to the Salter-Harris [5] classification.
The amount of displacement was assessed accordingto the Neer-Horwitz classification [3] (grade I: less than5 mm; grade II: up to one third of the diameter of the
Chir Organi Mov (2008) 92:89–95DOI 10.1007/s12306-008-0050-7
O R I G I N A L A R T I C L E
Fractures of the proximal humerus in children
Giovanni Luigi Di Gennaro • Mauro Spina • Manuele Lampasi •Rolando Libri • Onofrio Donzelli
Received: 5 March 2008 / Accepted: 5 May 2008 / Published online: 24 June 2008© Springer-Verlag 2008
G.L. Di Gennaro (�) · M. Spina · M. Lampasi · R. Libri · O. DonzelliDepartment of Paediatric Orthopaedics and TraumatologyIstituto Ortopedico RizzoliVia Pupilli 1, 40136 Bologna, Italye-mail: [email protected]
metaphysis; grade III: between one third and two thirdsof the diameter of the metaphysis; grade IV: greater thantwo thirds). Displacement of the fragments is almostalways associated with angulation, particularly in gradesIII and IV: the distal fragment is generally displacedanteriorly and laterally due to the muscular forces, and insome cases it may lacerate the periosteum, penetrate thedeltoid, and protrude under the skin.
Based on this classification, 20% of fractures in ourseries showed severe displacements (grades III and IV).In two cases the dislocation of the humeral epiphysis wasassociated.
All the cases were reviewed to determine type oftreatment performed, complications, and treatment out-come. Evaluation of the outcome at follow-up was madeby including data from clinical and radiographic records.For clinical evaluation, motility on all the planes (abduc-tion, internal and external rotation, elevation) wasrecorded as a percentage of the motility of the contralat-eral shoulder. The lowest percentage was used, and fourgrades were given (excellent: residual motility:90%–100% of the contralateral shoulder; good:65%–89%, fair: 40%–64%, poor: less than 39%).
Results
Eighty-two children underwent conservative treatment;in nine cases surgical treatment was performed.
As regards conservative treatment, in 11 cases aDesault bandage and in nine cases a hanging cast wereapplied; in 62 cases a closed reduction followed byshoulder spica cast was performed (Figs. 2, 3). Theshoulder spica cast was applied under general anesthesiain 40 patients (in 26 cases after a period of skeletal trac-tion at the olecranon). Reduction was performed immedi-ately after the trauma in 65% of the cases and after1–16 days in the other cases.
Patients were reviewed by clinical examination at amean follow-up of 7.2 months (range 1 to 156 months).In 79 patients (96.3% of cases) functional results wereexcellent/good (in 73 patients the motility was complete;residual range of movement was 80% in two patients and65% in other two patients; two patients showed completemotility, but complained of pain in extreme degrees ofinternal and external rotation). In three patients clinicalresults were poor (residual motility: 35%).
Neurological complications occurred in 10 cases,including nine nerve palsies (five ulnar, three radial andone median nerve) and one patient with paresthesia bothin the radial and ulnar areas. All resolved within4 months. No vascular complication was recorded.
Radiographs were performed at a mean follow-up of1 year and 7 months (range 1 month to 23.5 years).However, if we consider only cases where follow-up waslonger than 1 year, 15 cases were reviewed at a meantime of 8 years (range 1 to 23.5 years) after trauma.Among these cases, in three patients a slight (10°–20°)metaphyseal or metadiaphyseal varus deformity was evi-dent, but all of them had still open physes, so that furtherremodeling may be expected.
Surgical treatment was performed after failure ofclosed reduction: in two cases the interposition of thelong head of biceps tendon was described, in one casesoft tissues retraction, and in another case the persistenceof the proximal epiphysis dislocation. The time fromtrauma to surgery ranged from 1 to 15 days.Osteosynthesis was performed by plate and screws inthree cases (all with metaphyseal fractures next to skele-tal maturity) and by 1–3 Kirschner wires in six cases(Figs. 4, 5). In the postoperative period, six patients wereimmobilized in shoulder spica cast, one patient in aDesault bandage, and one in a hanging cast; in a 14-year-old polytraumatized patient, where a stable fixation ofthe fracture was achieved by plate and screws, no immo-bilization was applied.
90 Chir Organi Mov (2008) 92:89–95
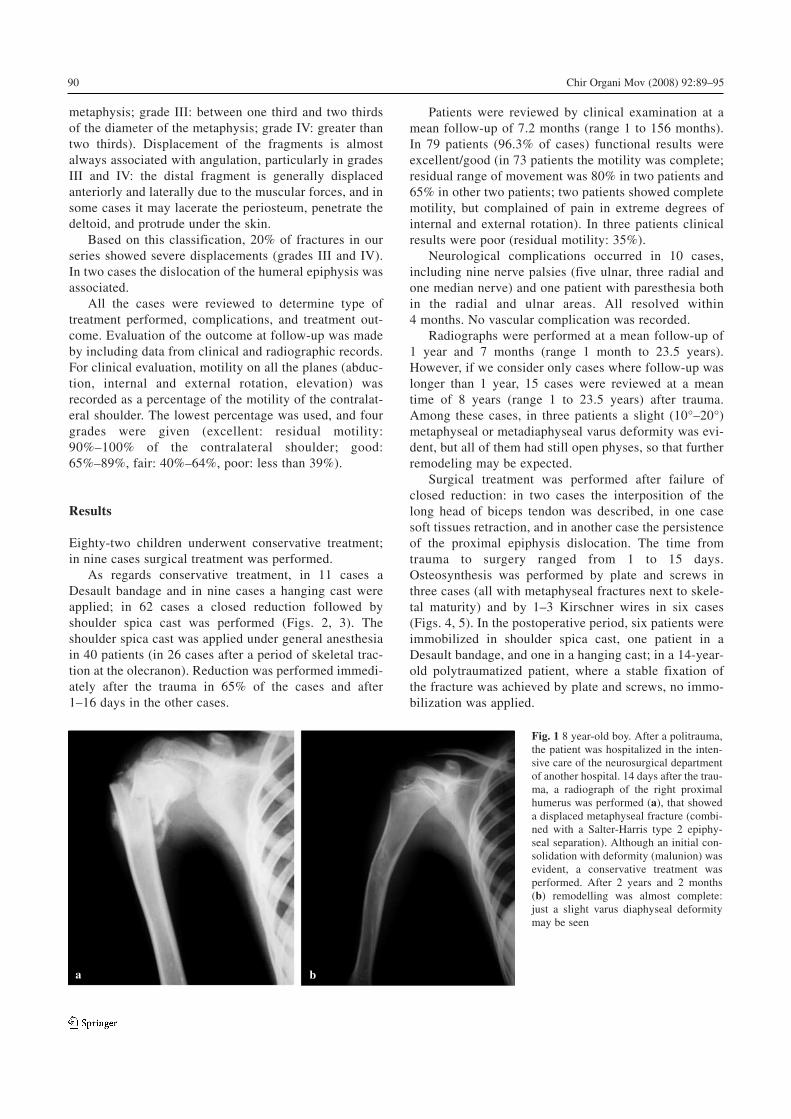
Fig. 1 8 year-old boy. After a politrauma,the patient was hospitalized in the inten-sive care of the neurosurgical departmentof another hospital. 14 days after the trau-ma, a radiograph of the right proximalhumerus was performed (a), that showeda displaced metaphyseal fracture (combi-ned with a Salter-Harris type 2 epiphy-seal separation). Although an initial con-solidation with deformity (malunion) wasevident, a conservative treatment wasperformed. After 2 years and 2 months(b) remodelling was almost complete:just a slight varus diaphyseal deformitymay be seen
a b
91Chir Organi Mov (2008) 92:89–95
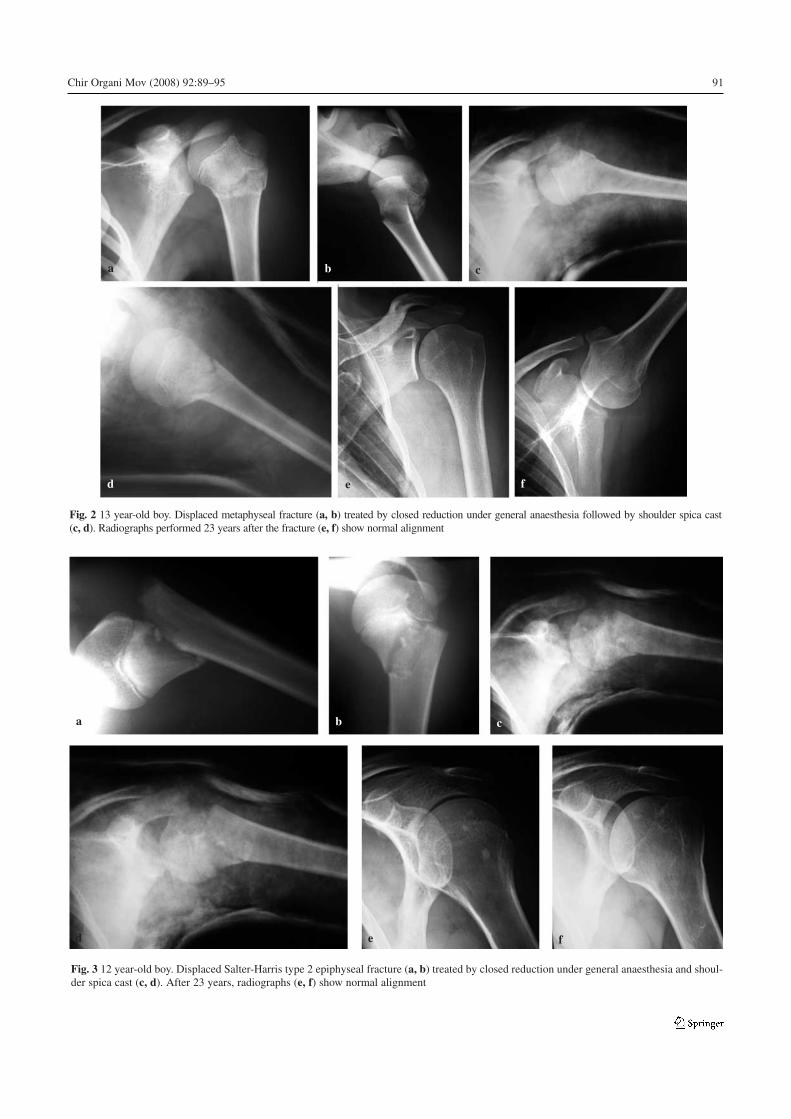
Fig. 2 13 year-old boy. Displaced metaphyseal fracture (a, b) treated by closed reduction under general anaesthesia followed by shoulder spica cast(c, d). Radiographs performed 23 years after the fracture (e, f) show normal alignment
a cb
d fe
Fig. 3 12 year-old boy. Displaced Salter-Harris type 2 epiphyseal fracture (a, b) treated by closed reduction under general anaesthesia and shoul-der spica cast (c, d). After 23 years, radiographs (e, f) show normal alignment
a cb
d fe
Patients were reviewed by clinical examinations at amean time after surgery of 34.8 months (1–150 months).No neurological or vascular complication was recorded.Good/excellent results were found in eight cases (sevenpatients showed complete motility, in one case residualrange of movement was 65%). In one case, where a sec-ond operation was required a few days after the firstoperation, due to a mistake made in the osteosynthesis
(which led to a secondary displacement of the fracture),a septic process occurred, that caused a severe deformityof the epiphysis and a noticeable reduction of the rangeof movement: residual abduction was 50% and externalrotation was 35% (poor clinical result).
Radiographs were performed at a mean follow-up of3 years and 8 months. Yet, radiographs with a follow-uplonger than 1 year were available in only six patients, at
92 Chir Organi Mov (2008) 92:89–95
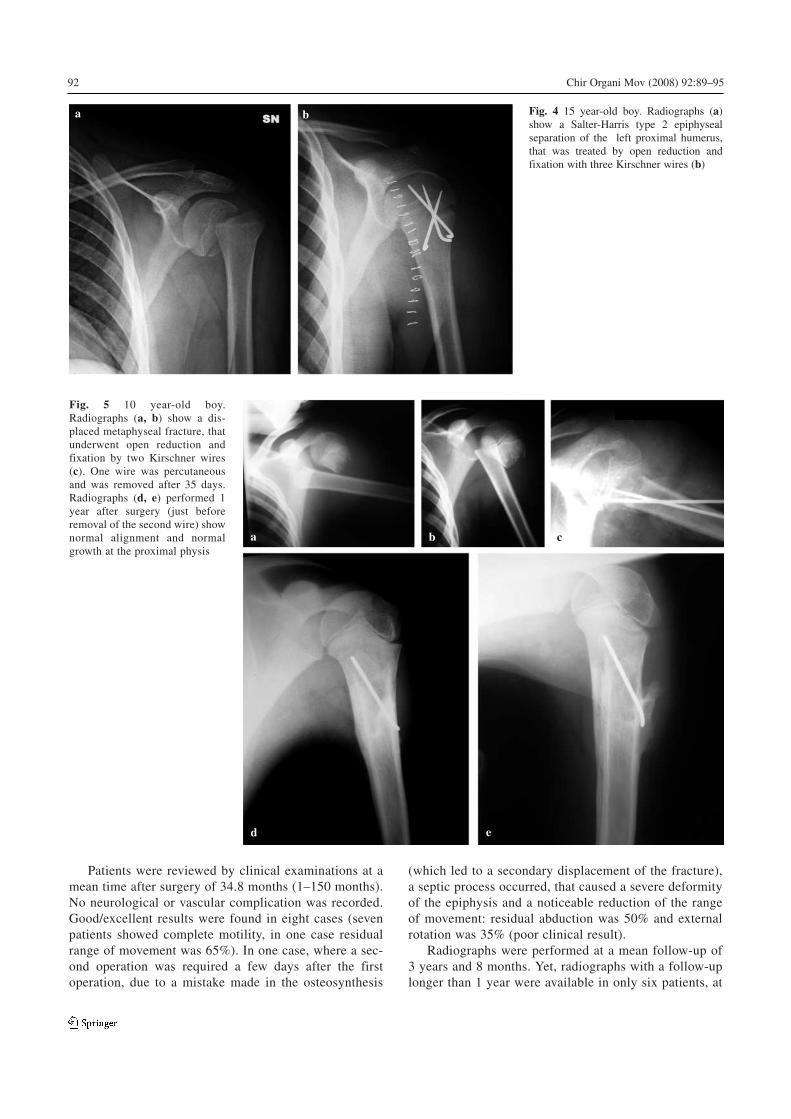
a b Fig. 4 15 year-old boy. Radiographs (a)show a Salter-Harris type 2 epiphysealseparation of the left proximal humerus,that was treated by open reduction andfixation with three Kirschner wires (b)
Fig. 5 10 year-old boy.Radiographs (a, b) show a dis-placed metaphyseal fracture, thatunderwent open reduction andfixation by two Kirschner wires(c). One wire was percutaneousand was removed after 35 days.Radiographs (d, e) performed 1year after surgery (just beforeremoval of the second wire) shownormal alignment and normalgrowth at the proximal physis
a cb
d e

a mean time of 5 years and 5 months (range 1 to12.5 years) after surgery. Apart from the above-men-tioned case with deformity of the epiphysis, no otherpatient showed residual deformity.
Discussion
The proximal epiphysis of the humerus is completelycartilaginous at birth. The primary ossification centerappears at about 4–6 months of age, and only successive-ly do the greater tuberosity (3 years) and the lessertuberosity (5 years) ossification centers make theirappearance. Fusion into a single nucleus occurs at about7 years of age. In the newborn and child up to 4–5 yearsof age, the growth plate is shaped like a hockey puck;successively it looks like a thin, wide cone with its tipslightly displaced medially and posteriorly. Capsularinsertion extends medially onto the metaphysis. Due tothese anatomic features, Salter-Harris type II epiphysealseparations with a medial and posterior metaphyseal tri-angle attached to the epiphysis are more frequent afterthe age of 5 years.
The proximal growth plate of the humerus is the mostactive physis of the whole skeleton, accounting for 80%of the growth in length of this bone. As a consequence,the potential for self-correction is considerable, whichinfluences the limits for residual deformities that may betolerated after reduction.
The forces responsible for a proximal humerus injurymay act with a mechanism of compression, inclination,flexion, shear, and torsion. Torsion forces generally pro-duce metaphyseal fractures below the tuberosities, where-as shear forces usually cause epiphyseal separations.
Fractures of the proximal metaphysis occur moreoften in younger children; physeal fractures of the prox-imal humerus may occur in children of any age, but occurmore commonly in adolescents [6].
The type 1 Salter-Harris fracture (pure epiphysealseparation) is a fracture through the physis, which caus-es separation between the epiphysis and metaphysis: thisis facilitated by the disk shape of the physis until4–5 years of age. The obstetrical epiphyseal fracture-sep-aration is a typical example of this type of injury. In thiscase, the cartilaginous epiphysis is not entirely visible onstandard x-rays: some useful information may beachieved only if comparative A-P views with limbsadducted and abducted respectively are performed.Ultrasonography may be very useful. Anyway, anamnesis(dystocic delivery) and clinical examination (swelling,pseudoparalysis) are essential for a correct diagnosis, andthe old Camera’s aphorism (“clinical signs of fracture +radiographic signs of dislocation = epiphyseal separa-tion”) should be kept in mind. In these cases, reductionby delicate maneuvers (traction, abduction, flexion and
slight external rotation) and bandage should be per-formed. Surgical reduction with suture of the periostealsheath, as suggested by some authors [7] in the case offailure of conservative treatment, should be avoided inour opinion.
The Salter-Harris type 2 epiphyseal separations aremore frequent than type 1 fractures (ratio 4:1); the frac-ture is through the lateral part of the physis and thenextends into the metaphysis, detaching a posterior-medi-al triangular fragment. The Salter-Harris type 3/4 frac-tures and the epiphyseal fractures associated with epi-physeal dislocation are very rare [8].
Conservative treatment is the treatment of choice forepiphyseal and metaphyseal fractures of the proximalhumerus in children [6], and includes different therapeu-tic options. Since our review included 91 consecutivecases seen and treated in our department, the type oftreatment was also influenced by the preference andexperience of each orthopedist. Yet, some general rulesmay be assumed: at presentation, a Desault bandage or ahanging cast were applied and a radiographic evaluationwas undertaken after the immobilization; in cases ofsevere displacement or when reduction after immobiliza-tion was inadequate, a closed reduction (usually undergeneral anesthesia) followed by shoulder spica cast wasperformed.
Since the muscular forces produce abduction, flexion,and slight external rotation of the epiphysis, reductivemaneuvers should include corresponding actions on thedistal fracture fragment. Reduction may be difficult,since the epiphysis is small, mobile, and hard to grasp;therefore, it should be held between the thumb and indexfinger while the distal fragment is reduced. Reductivemaneuvers under general anesthesia are not always effec-tive. Baxter and Wiley [9] reported improvement of thedegree of initial displacement only in 11 cases out of 33.Skeletal traction at the olecranon may facilitate the pro-cedure.
Tachdjian suggests fixing the epiphysis by a percuta-neous Kirschner wire that crosses the acromion: yet, sev-eral risks should be considered, as in the case of percuta-neous insertion of ascending wires under an image inten-sifier [10].
Indications for surgery reported in the literature arelimited: (1) irreducible fractures (due to interposition ofthe periosteum or of the long head of the biceps tendon);(2) insufficient reduction in patients near skeletal maturi-ty; (3) displaced or unstable fractures in patients who donot tolerate any immobilization (polytraumatized, myo-pathic, spastic, etc.): in these cases stable fixation will berequired, like in adult patients; (4) open fractures or frac-tures associated with vascular or nervous lesions.
The approach is typically through a delto-pectoralapproach, which, however, produces unaesthetic scars.The axillary approach has been proposed by some
93Chir Organi Mov (2008) 92:89–95

Authors, but it is difficult and provides only a limitedvision of the fracture. In very young patients, the perios-teum should not be surgically detached near the physis dueto the risk of iatrogenic epiphysiodesis. In some cases evensurgical reduction may be difficult and may not provideanatomical reduction of the fracture fragments [9].
Bone fixation may be realized by Kirschner wires (per-cutaneous or bent subcutaneously) in younger patients, andby plates in older patients. The suture of the laceratedperiosteum increases stability of the fracture.
The prognosis of epiphyseal separations of the proxi-mal humerus is generally favorable, since type 3/4 fracturesare extremely rare and since in type 1/2 separations thefracture occurs through the hypertrophic layer of the physis(the basal and proliferative layers are not involved).
Angular deviations due to asymmetrical growth platearrest are very rare and limb discrepancies do not exceed3–4 cm, even in the most severe cases.
Conversely, malunions due to poor initial reduction arequite frequent (25% according to Clement et al. [11]). Inthe case of residual translation of the fracture fragments,remodeling occurs after about 6 months, due to periostealactivity. Residual angulations are corrected only if remain-ing potential of growth is sufficient: tolerable values varywith age, gender, and according to the different authors.
Most authors agree that, under the age of 13 years forgirls and 15 years for boys, angulations up to 20° and trans-lations up to 50% may be tolerated. According to Beaty[12], angulations up to 70° and complete translations of thefragments are acceptable under 5 years of age, 40°–70° ofangulation are acceptable between 5 and 12 years of age,and up to 40° of angulation and 50% of apposition may betolerated for children over 12 years of age. Dameron andRockwood [13, 14] suggest the following tolerability val-ues: 70° of angulation from 1 to 5 years of age and 40°–45°from 5 to 12 years, with 50% of translation.
Nilson and Svartholm [15] reported no severe function-al deficit in 43 cases out of 44 children with considerabledisplacement. Dameron and Reibel [13] reported the sameconclusions in a long-term review of 46 patients. Beringeret al. [16] reported the long-term results of 48 patients whohad severely displaced proximal humeral fractures. Ninechildren underwent surgery, and one had complications.They described the functional results of patients who hadacceptable displacement and of patients with a radiograph-ic malunion: neither group had functional problems.
As regards the risk of posttraumatic disturbances affect-ing the growth in length of the humerus, no radiographicexamination was performed in the present work, to evalu-ate this feature. Neer and Horwiz [3], in a review of 89patients, reported a shortening of the humerus (1–3 cm) in9% of grade I-II displacements and in 33% of grade IV dis-placements. Shortening was never found in cases of frac-tures in children under the age of 11 years. After this age,slight shortening and axial deviations were described, butfunctional and cosmetic results were always satisfactory.
The authors concluded that remodeling potential of theupper epiphysis of the humerus is so great that risks of sur-gical reduction are rarely justified.
Weber [17] in a review of 53 cases reported varus-procurvatum diaphyseal deformity in five cases, valgusdeformity (5°–10°) in two, and some complaint duringsports activity in three.
Even if the evolution of these fractures is generallyfavorable, it seems advisable in cases of children over11 years of age to tell the parents that remodeling might notbe complete and that a slight shortening or axial deviationmight derive.
Conclusions
When evaluating children with fractures of the proximalhumerus, the age of the patient and the features of thefracture (axis, displacement, and stability) should be con-sidered.
As a general rule, conservative treatment is the treat-ment of choice. We suggest being satisfied with the reduc-tion achieved, if there is enough residual growth potential.
In the case of severely displaced fractures in adoles-cents with limited remodeling potential, our treatment pro-tocol includes an attempt at closed reduction (stabilizationby percutaneous Kirschner wires is performed, if needed);in cases of failure, open reduction and internal fixation areperformed. Yet, it should be considered that even severecomplications are possible after surgical treatment, as weexperienced in the patient who developed a septicprocess.
References
1. Rose SH, Melton LJ 3rd, Morrey BF et al (1982) Epidemiologicfeatures of humeral fractures. Clin Orthop Relat Res 168:24–30
2. Peterson CA, Peterson HA (1972) Analysis of incidence of inju-ries to the epiphyseal growth plate. J Trauma 12:275–281
3. Neer CS 2nd, Horwitz BS (1965) Fractures of the proximalhumeral epiphysial plate. Clin Orthop Relat Res 41:24–31
4. Dobbs MB, Luhmann SL, Gordon JE (2003) Severely displacedproximal humeral epiphyseal fractures. J Pediatr Orthop23:208–215
5. Salter RB, Harris WR (1963) Injuries involving the epiphysealplate. J Bone Joint Surg Am 45:587–622
6. Shrader MW (2007) Proximal humerus and humeral shaft fractu-res in children. Hand Clin 23:431–435
7. Blount WP (1954) Fractures in children. Schweiz MedWochenschr 84:986–988
8. Nicastro JF, Adair DM (1982) Fracture-dislocation of the shoul-der in a 32-month-old child. J Pediatr Orthop 2:427–429
9. Baxter MP, Wiley JJ (1986). Fractures of the proximal humeralepiphysis. Their influence on humeral growth. J Bone Joint SurgBr 68:570–573
10. Tachdjian MO (1990) Fractures involving the proximal humeralphysis: fracture-separations of upper epiphysis of humerus. In:Pediatric orthopaedics, vol 4, 2nd Edn. Saunders, Philadelphia,pp 3046–3052
94 Chir Organi Mov (2008) 92:89–95

11. Clement JL, Cahuzac JP, Gaubert J et al (1988) Epiphyseal frac-tures and separation of the upper part of the humerus. Apropos ofa series of 148 cases. Rev Chir Orthop Reparatrice Appar Mot74[Suppl2]:139–144
12. Beaty JH (1992) Fractures of the proximal humerus and shaft inchildren. In: Eibert RE (ed) AAOS instructional course lectures.American Academy of Orthopaedic Surgeons, Chicago,pp 369–372
13. Dameron TB Jr, Reibel DB (1969) Fractures involving the proxi-mal humeral epiphyseal plate. J Bone Joint Surg Am 51:289–297
14. Rockwood CA, Wilkins KE, King RE (1991) Fractures in chil-dren. Lippincott, Philadelphia
15. Nilsson S, Svartholm F (1965) Fracture of the upper end of thehumerus in children. A follow-up of 44 cases. Acta Chir Scand130:433–439
16. Beringer DC, Weiner DS, Noble JS, Bell RH (1998) Severely dis-placed proximal humeral epiphyseal fractures: a follow-up study.J Pediatr Orthop 18:31–37
17. Weber BG (1966) The prevention of axial malpositioning in thetreatment of pediatric fractures. Z Unfallmed Berufskr 59:80–95
95Chir Organi Mov (2008) 92:89–95