follicular bronchiolitis in association with connective tissue diseases
TRANSCRIPT

Lung 11985) 163:305-314
Follicular Bronchiolitis in Association with Connective Tissue Diseases
Teresa I. Fortoul,* Fernando Cano-Valle, Elena Oliva and Roberto Barrios
Electron Microscopy Unit, Facultad de Medicina, UNAM, Pulmonary Medicine Ward "Dr. Alejandro Celis," General Hospital and the Department of Pathology. National Institute of Cardiology "lgnacio Chavez," Mexico City, Mexico
Abstract. Eleven patients with connective tissue diseases were found to have bronchiolar lesions associated with minimal or no alveolar septal thick- ening. Seven of these patients had rheumatoid arthritis, 3 had Sj6gren's syndrome, and I had ankylosing spondylitis.
Radiographic studies showed an interstitial pattern in all patients. The patients were nonsmokers and received no treatment prior to biopsy. All lung biopsy specimens showed inflammatory bronchiolar lesions which con- sisted of bronchiolar and peribronchiolar lymphocytic infiltrates (follicular bronchiolitis). The bronchiolar lesion has been reported previously in pa- tients with connective tissue diseases treated with D-penicillamine; whether it represents a component of the systemic disease or a lack of effect of the therapeutic agent had not been established. The present study shows that several connective tissue diseases can be associated with inflammatory bronchiolar lesions.
Key words: Bronchiolitis--lnterstitial lung diseases--Connective tissue dis- eases--SjOgren's syndrome--Rheumatoid lung.
Introduction
It has been known for years, largely on the basis of postmortem observations, that pleural and pulmonary lesions often accompany connective tissue disease such as rheumatoid arthritis and systemic lupus erythematosus. It has also been accepted that such lesions may be an integral part of the diseases and not due to secondary infections [1, 2, 6, 7, 16, 17, t9-21, 23, 25]. Although bron-
* To whom offprint requests should be addressed at Unidad de Microscopia Electronica, Fa- cultad de Medicina, UNAM, Mexico, D.F.C.P. 04510, Mexico.

306 T.I. Fortoul et al.
chial o b s t r u c t i o n has been reported in associa t ion with connec t ive t i ssue dis- eases , this has been at t r ibuted to smoking [3, 11, 24, 26]. Epler et al. have desc r ibed an associa t ion be tween bronchiol i t i s and admin i s t r a t ion of D-penic i l - l amine in 2 pa t ien ts with rheumatoid arthri t is and eosinophi l ic fasciit is. These au thors desc r ibed the histologic changes as " fo l l icular b ronch io l i t i s " [8]. We s tudied a series of 11 pat ients with several connec t ive t issue diseases in w h o m the ma in p u l m o n a r y lesions were found at the level of the terminal b ronch io les .
The pa t i en t s were nonsmoker s and had no history of previous p u l m o n a r y infec- t ion; it seems to us that the bronchio la r les ions are part of the sys temic mani fes - ta t ions of the connec t ive tissue diseases ana lyzed in this report.
Methods
Patients Studied
The study group consisted of II patients, 10 women and 1 man, with a mean age of 44 years and a range of 16-56 years. None of the subjects was a smoker. All patients underwent an open lung biopsy after analysis of the clinical history, radiographic studies, and pulmonary function tests to rule out other types of interstitial lung diseases. Biopsy site was selected according to areas that had evidence of disease roentgenographically and grossly at the time of surgery.
Light Microscopy
Paraffin sections from formalin-fixed tissue were prepared and stained by the following methods: hematoxylin and eosin, Masson trichrome, periodic acid-Schiff (PAS). and Weigert's elastic fiber stain.
Immunofluorescence Studies
Direct immunofluorescence was performed. Fluorescein-labeled antisera to lgG, lgA, IgM, IgD, IgE, C3, Clq, C4, fibrin, fibrinogen, and albumin were obtained from Hoechst Laboratories. Lung tissue from each biopsy specimen was frozen as soon as it was received from the surgeon and sections were cut on a cryostat and fixed with cold acetone. The sections were stained with an antisera dilution 1:6 in PBS for 30 minutes, washed with PBS pH 7.4, and read on a Zeiss microscope with halogen light source. The antisera were tested with known positive controls.
Results
Clinical and Laboratory. Studies
The du ra t i on of symptoms ranged f rom 1 to 252 months (mean, 110 mon ths ) . In 9 pa t i en t s there was an increase in the a lveo la r - a r t e r i a l pO2 d i f fe rence (A- apO2); in 6 pa t ients there was h y p o x e m i a and resp i ra tory alkalosis. T w o pa- t ients had func t iona l ev idence of a i rway obs t ruc t ion . Eight pat ients had high
Follicular Bronchiolit is
Table 1. Clinical data
307
Patient Sex Age Clinical Months Previous Symptoms Rheumato id (years) diagnosis from onset to t reatment factor
biopsy
1 F 56 RA 36 ASA dyspnea 1:640 2 F 43 RA 228 ASA dyspnea 1:160 3 F 30 RA 60 ASA dyspnea negat ive 4 F 47 RA 12 ASA dyspnea 1:640 5 F 49 RA 192 ASA dyspnea 1:1280 6 F 45 RA 120 ASA dyspnea 1:1280 7 F 55 RA 252 ASA dyspnea 1:80 8 F 42 SS 36 ASA dyspnea negat ive 9 F 56 SS 36 ASA dyspnea 1:640
10 F 55 SS 240 ASA dyspnea 1:2560 11 M 16 AS 1 none dyspnea negative
ASA, acetylsalicylic acid; RA. rheumatoid arthritis; SS, Sjogren 's syndrome; AS, ankylosing spondylit is
Table 2. Pulmonary function tests (% predicted)
Patient FVC FEVI MEV(L/sec) MVV Po:(mmHg) Pco: (mmHg) pH A-aPo , (mmHg)
1 58 94 2.6 81 45 22 7.37 312 2 65 83 2.6 72 61 28 7.50 198 3 86 87 - - 82 61 20 7.40 153 4 31 85 - - 70 48 20 7.51 234 5 30 90 - - 60 45 20 7.43 284 6 51 70 - - 100 47 34 7.50 234 7 . . . . . . . .
8 102 90 - - 82 57 31 7.43 234 9 66 70 - - 71 68 30 7.42 193
10 77 80 2 65 56 32 7.36 225 11 a . . . . . . .
a Test not done FVC, forced vital capacity; FEVI , forced expiratory volume in 1 sec; MEV, midexpira tory volume (normal 3_1 -+ 1.9 L/sec); MVV. maximal voluntary ventilation: A-aPoz. difference in pressure of oxygen between alveolar air and arterial blood breathing 100% oxygen (normal < 160 mmHg)
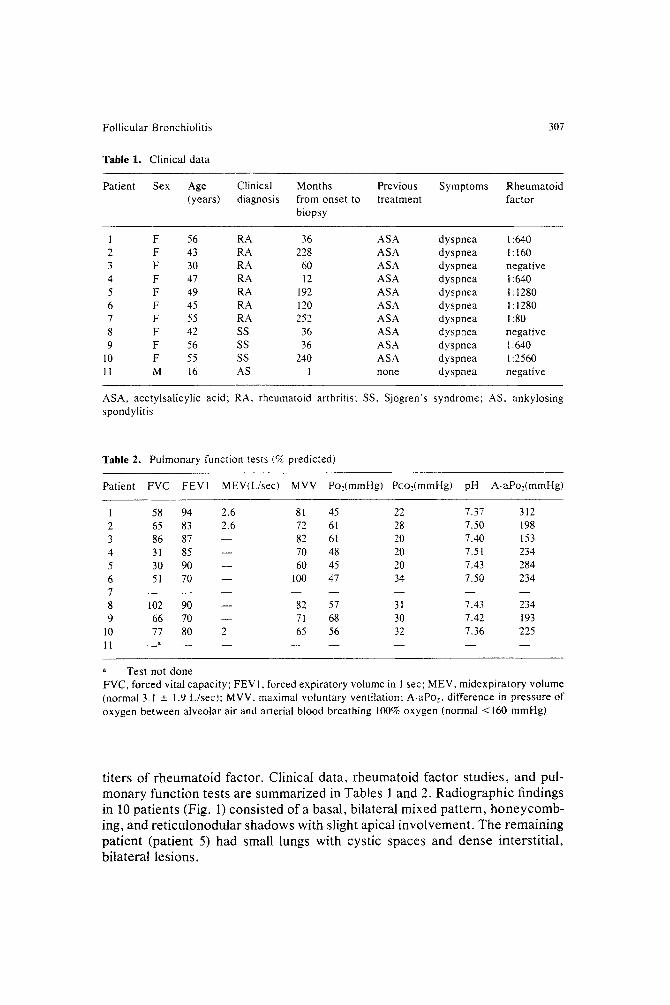
titers of rheumatoid factor. Clinical data, rheumatoid factor studies, and pul- monary function tests are summarized in Tables 1 and 2. Radiographic findings in 10 patients (Fig. I) consisted of a basal, bilateral mixed pattern, honeycomb- ing, and reticulonodular shadows with slight apical involvement. The remaining patient (patient 5) had small lungs with cystic spaces and dense interstitial, bilateral lesions.
308 T. I. Fortoul et al.
Fig. 1. Chest roentgenogram of patient 3. There is a bilateral reticulonodular pattern and signs of pulmonary hypertension; a healed rib fracture is also seen
Light Microscopic Observations
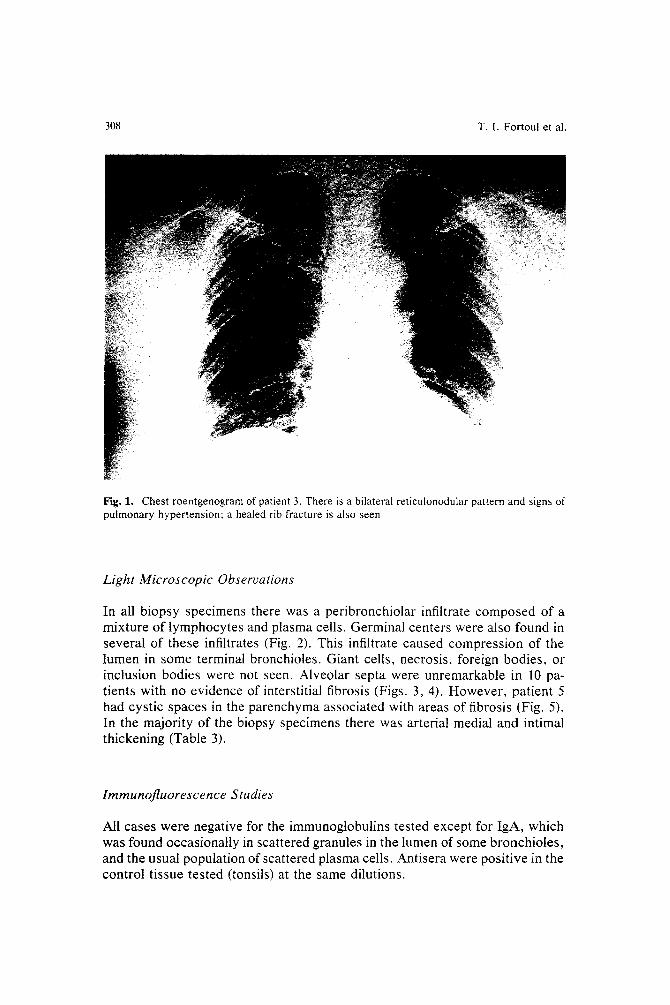
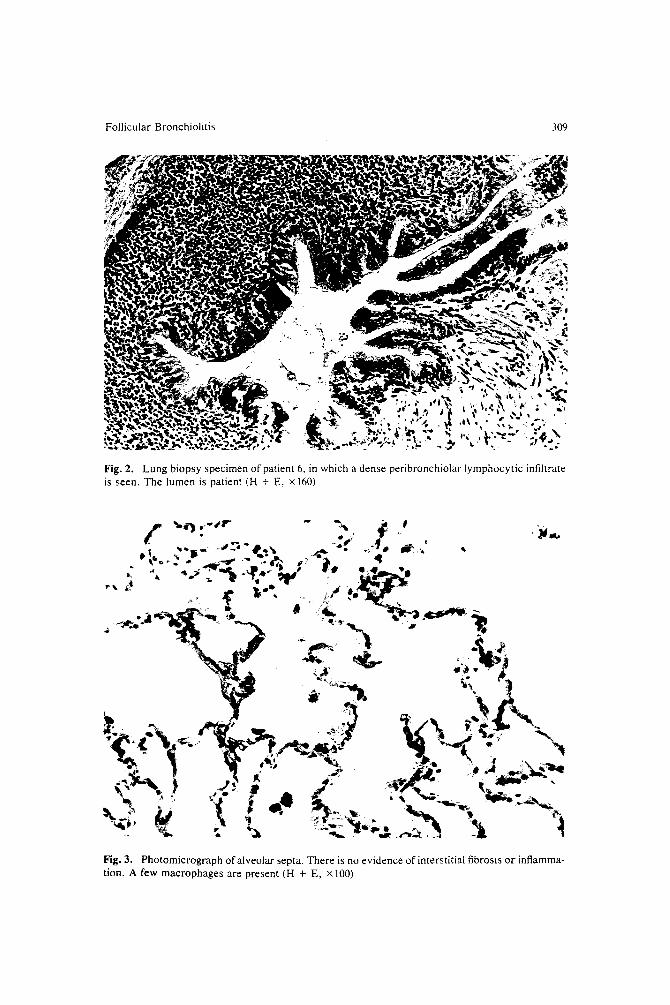
In all biopsy specimens there was a peribronchiolar infiltrate composed of a mixture of lymphocytes and plasma cells. Germinal centers were also found in several of these infiltrates (Fig. 2). This infiltrate caused compression of the lumen in some terminal bronchioles. Giant cells, necrosis, foreign bodies, or inclusion bodies were not seen. Alveolar septa were unremarkable in 10 pa- tients with no evidence of interstitial fibrosis (Figs. 3, 4). However , patient 5 had cystic spaces in the parenchyma associated with areas of fibrosis (Fig. 5). In the majority of the biopsy specimens there was arterial medial and intimal thickening (Table 3).
Immunofluorescence Studies
All cases were negative for the immunoglobulins tested except for IgA, which was found occasionally in scattered granules in the lumen of some bronchioles, and the usual population of scattered plasma cells. Antisera were positive in the control tissue tested (tonsils) at the same dilutions.
Follicular Bronchiolitis 309
. ~ . ,..9~r.,~ _ m .7"P F IrtP" Q .,is ~,~.
Q,
:J. "X
Fig. 2. Lung biopsy specimen of patient 6, in which a dense peribronchiolav lymphocytic infiltrate is seen. The lumen is patient (H + E, z 160)
Fig. 3. Photomicrograph of alveolar septa. There is no evidence of interstitial fibrosis or inflamma- tion. A few macrophages are present (H + E, x 100)
310
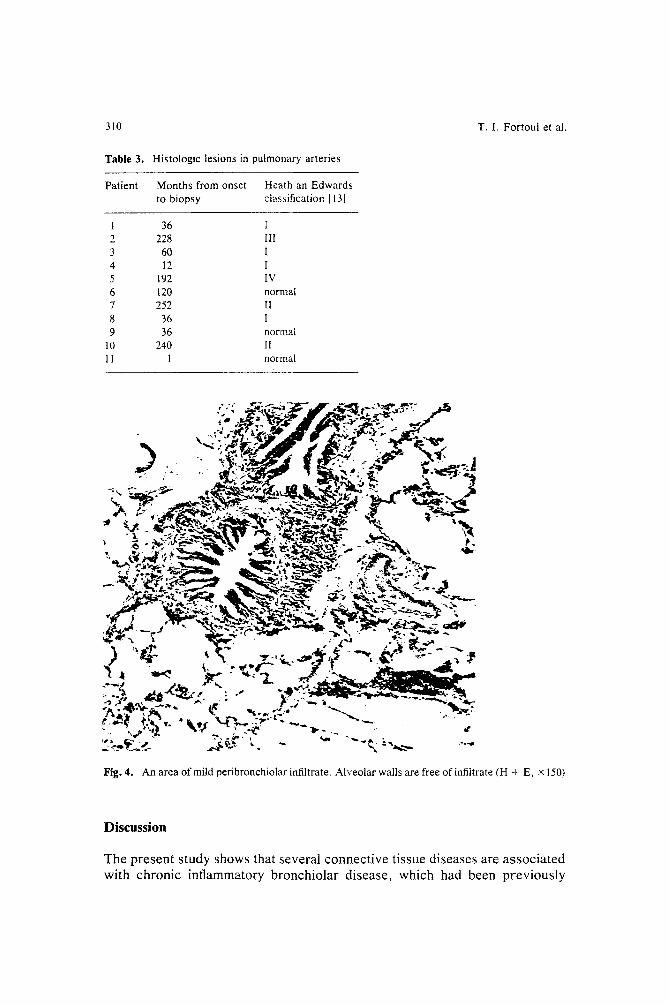
Table 3. Histologic lesions in pulmonary arteries
Patient Months from onset Heath an Edwards to biopsy classification [131
1 36 I 2 228 [II 3 60 I 4 12 I 5 192 IV 6 120 normal 7 252 [I 8 36 ! 9 36 normal
10 240 II 11 1 normal
T. I. Fortoul et al.
..-.-., .£.i:~7 i :_iT~-',~F r_ ; ~ . r r ? ~ , , ~ v . , ~
" " "" ~ ~,;~h': ~ , ~ " " " ~ ~ '~ . . . . ~. •
.~" ? ,~ '~ ' - < ~ L ~ . ~ L ~ ~,':~'~2~ ~ ~ -~ i~ , , ' . i .~ - , . : _
Fig. 4. An area o f mild peribronchiolar infiltrate. Alveolar walls are free of infiltrate (H + E, x 150)
D i s c u s s i o n
T h e p r e s e n t s t u d y s h o w s t h a t s e v e r a l c o n n e c t i v e t i s s u e d i s e a s e s a r e a s s o c i a t e d
w i t h c h r o n i c i n f l a m m a t o r y b r o n c h i o l a r d i s e a s e , w h i c h h a d b e e n p r e v i o u s l y
Follicular Bronchiolitis 311
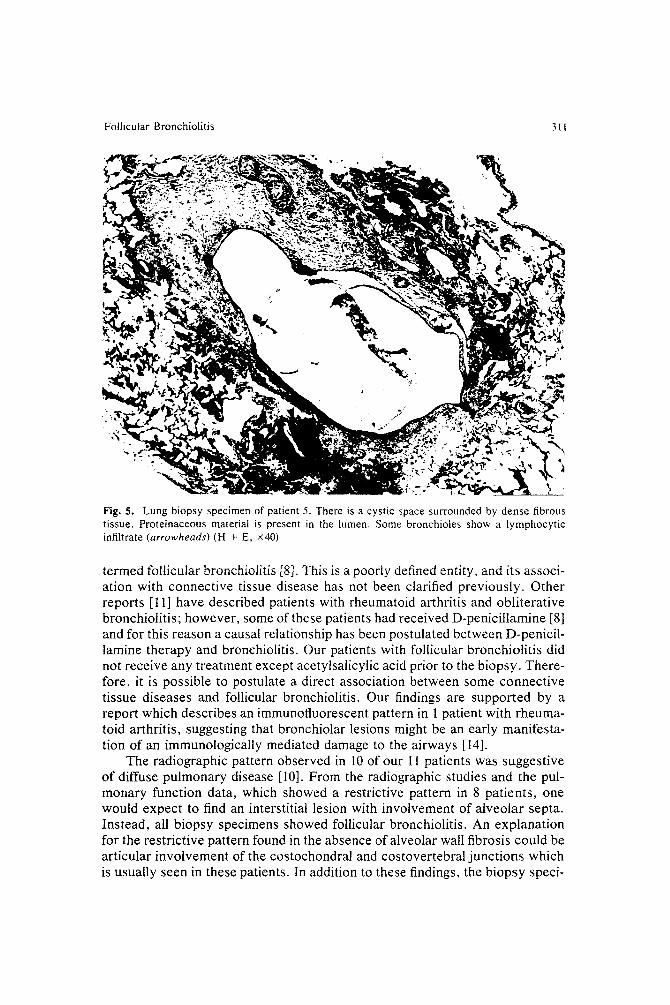
Fig. 5. Lung biopsy specimen of patient 5. There is a cystic space surrounded by dense fibrous tissue. Proteinaceous material is present in the lumen. Some bronchioles show a lymphocytic infiltrate (arrowheads) (H + E, x40)
termed follicular bronchiolitis [8]. This is a poorly defined entity, and its associ- ation with connective tissue disease has not been clarified previously. Other reports [11] have described patients with rheumatoid arthritis and obliterative bronchiolitis; however, some of these patients had received D-penicillamine [8] and for this reason a causal relationship has been postulated between D-penicil- lamine therapy and bronchiolitis. Our patients with follicular bronchiolitis did not receive any treatment except acetylsalicylic acid prior to the biopsy. There- fore, it is possible to postulate a direct association between some connective tissue diseases and follicular bronchiolitis. Our findings are supported by a report which describes an immunofluorescent pattern in 1 patient with rheuma- toid arthritis, suggesting that bronchiolar lesions might be an early manifesta- tion of an immunologically mediated damage to the airways [14].
The radiographic pattern observed in 10 of our I I patients was suggestive of diffuse pulmonary disease [I0]. From the radiographic studies and the pul- monary function data, which showed a restrictive pattern in 8 patients, one would expect to find an interstitial lesion with involvement of alveolar septa. Instead, all biopsy specimens showed follicular bronchiolitis. An explanation for the restrictive pattern found in the absence of alveolar wall fibrosis could be articular involvement of the costochondral and costovertebral junctions which is usually seen in these patients. In addition to these findings, the biopsy speci-
312 T . I . Fortoul et al.
men from patient 5 showed microcystic spaces surrounded by dense fibrous connective tissue (Fig. 5). The latter findings are those of advanced <'rheuma- toid lung" [4, 20]. Thus, the histologic changes shown in patient 5, who had rheumatoid arthritis, may be considered end-stage lesions [4]. The biopsy spec- imens from the other I0 patients showed no evidence of cystic lesions or thickening of alveolar septa. Therefore, the radiographic findings in these pa- tients must be attributed to follicular bronchiolitis and associated bronchiolar thickening.
The radiologic distinction between follicular bronchiolitis and bronchiolitis obliterans can be difficult, particularly when the radiographic findings are atypi- cal and similar to those seen in other pulmonary disease [12].
Follicular bronchiolitis and bronchiolitis obliterans appear to be two mor- phologically distinct types of reactions. Bronchiolitis obliterans consists of polypoid masses of granulation tissue which occlude the lumen of the airways, whereas follicular bronchiolitis is characterized by conglomerates of lymphoid cells around terminal and respiratory bronchioles resulting in extrinsic com- pression rather than direct occlusion of the lumen. In addition to bronchiolitis obliterans, the microscopic differential diagnosis of follicular bronchiolitis must include pseudolymphoma, necrotizing bronchiolitis, and extrinsic allergic al- veolitis.
Lymphoid interstitial pneumonia is frequently seen in patients with SjO- gren's syndrome [9, 22]. It is possible that interstitial lymphoid pneumonia begins as a peribronchiolar lymphocytic infiltrate and subsequently involves alveolar septa. If this hypothesis is correct, follicular bronchiolitis could repre- sent an early stage of interstitial lymphoid pneumonia or pseudolymphoma.
It is also possible that follicular bronchiolitis progresses to bronchiolar fibrosis. This is suggested by a report of a patient in whom Sj6gren's syndrome was associated with bronchiolar fibrosis and slight bronchiolar inflammation [18]. On the other hand, some reports suggested that early bronchiolar lesions could develop into chronic obstructive pulmonary disease, as in cases of viral bronchiolitis in childhood [27].
We are unaware of reports of an association between bronchiolitis and ankylosing spondylitis. Patient 11 in the present study showed this association.
Positive immunofluorescence studies (IgG and complement) have been re- ported in lung biopsy specimens from patients with rheumatoid arthritis [5, 14]. Our negative findings do not rule out a humoral immunologic mechanism, since immune complexes could have been cleared from the tissue early in the course of the disease. IgA in the lumen of the airways can be considered a normal finding, since IgA is a secretory immunoglobulin [15].
Although severe lesions might be expected in patients with a long history of connective tissue disease, the correlation between the duration of symptoms and the severity of the morphologic lesions was poor. Seven patients had elevated titers of rheumatoid factor; however, these titers did not show a direct correlation with the severity of the lesions. A possible explanation for this phenomenon would be that rheumatoid factor titers reflect systemic activity, while bronchiolar lesions could be explained on the basis of local mechanisms.
Follicular Bronchiolitis 313
Acknowledgment. The authors thank Dr. Victor Ferrans of the National Heart, Lung and Blood Institute, and Dr. Benjamin Felson of the Department of Radiology, University of Cincinnati, for their helpful advice and critical review of the manuscript, and Miss Sitvia Resendiz for secretarial assistance.
References
1. Benisch B, Peison B (1979) The association of lymphocytic interstitial pneumonia and sys- temic lupus erythematosus. Mr. Sinai J Med 46:398-401
2. Brannan H, Good CA, Divertie MB, Bagenstoss HA (1964) Pulmonary diseases associated with rheumatoid arthritis. JAMA 189:914-918
3. Collins RL, Turner RA, Johnson AM, et al (1976) Obstructive pulmonary disease in rheuma- toid arthritis. Arthritis Rheum 19:623-628
4. Cruickshank B (1959) Interstitial pneumonia and its consequences in rheumatoid diseases. Br J Dis Chest 53:226-236
5. DeHoratius RJ, Abruzzo JL, Witliams RC Jr (1972) Immunofluorescent and immunologic studies of rheumatoid lung. Arch Intern Med 129:441-446
6. Doctor L, Snider GL (1962) Diffuse interstitial fibrosis associated with arthritis. Am Rev Respir Dis 85:413-422
7. Eisenberg H, Dubois EL. Russel P, Balchum OJ (1973) Diffuse interstitial lung diseases in systemic lupus erythematosus. Ann Intern Med 79:37-45
8. Epler GR, Snider GL, Gensler AE, et al (1979) Bronchiolitis and bronchitis in connective tissue disease. A possible relationship to the use of penicillamine. JAMA 242:528-532
9. Feing DS, Siegelman SS, Theros EC. King FM (1977) Lymphoid disorders of the chest. Am J Roentgenol 129:22t-228
10. Felson B (1979) A new look at pattern recognition of diffuse pulmonary disease. A JR 133:183- 189
11. Geddes DM, Brewerton DA. Davies RJ. Turner-Warwick M (1977) Progressive airway obliter- ation in adults and its association with rheumatoid arthritis. Q J Med 46:427-444
12. Gosik BB, Friedman PJ, Liebow AA (1973) Bronchiolitis obliterans: roentgenologic-patho- logic correlation. ARJ 177:816-832
13. Heath D, Edwards JE (1958) The pathology of hypertensive pulmonary vascular disease. A description of six grades of structural changes in the pulmonary arteries with special reference to congenital cardiac septal defects. Circulation 18:553-547
14. Herzog CA, Miller RR. Hoidal JR (1981) Bronchiolitis and rheumatoid arthritis. Am Rev Respir Dis 124:636-639
15. Kaltreider HB (1976) Expression of immune mechanisms in the lung. Am Rev Respir is 113:347-379
16. Kallenbach J, Prinsloo I. Zwi S (1977) Progressive systemic sclerosis complicated by diffuse pulmonary haemorrhage Thorax 32:767-70
17. Matthay RA, Schwartz MI, Petty TL, et al (1974) Pulmonary manifestations of systemic lupus erythematosus Review of twelve cases of acute lupus erythematosus pneumonitis. Medicine 54:397-409
18. Newboll HH, Brahim AS (1977) Chronic obstructive airways disease in patients with Sj6gren's syndrome Am Rev Respir Dis 115:295-304
19. Park S, Nyan WL (1975) Fatal pulmonary involvement in dermatomyositis. Am J Dis Child 129:723-726
20. Rubin HE (1979) The lung in systemic diseases. Charles C Thomas, Springfield, 111, p 83 2l. Schwartz MI, Matthay RA, Sahn SA, et al (1976) Interstitial lung disease in polymyositis and
dermatomyositis: analysis of six cases and review of the literature. Medicine 55:99-103 22. Strilman CV, Rosenow EC liI, Weiland LH, Brown LR, (1978) Lymphocytic interstitial
pneumonitis. Review of 13 cases. Ann Intern Med 88:616-621 23. Talbott JA, Calkins E (1964) Pulmonary involvement in arthritis, JAMA 189:911-913

314
24.
25. 26.
27.
T. I. Fortoul et al.
Turner-Warwick M, Courtenay RE (1977) Pulmonary manifestations of rheumatoid arthritis. Clin Rheum Dis 3:549-564 Walker WC, Wright V (1968) Pulmonary and rheumatoid arthritis. Medicine 47:501-520 Whorwell PJ, Wojtulewski JA. Lacey BW (1975) Respiratory function in rheumatoid arthritis. Br Med J 2:175 Wobl MEB, Chernick V (1978) Bronchiolitis. Am Rev Respir Dis 118:759-781
Accepted for publication: March 13. 1985