bronchiolitis obliterans after allo-sct: clinical criteria and treatment options
TRANSCRIPT

REVIEW
Bronchiolitis obliterans after allo-SCT: clinical criteria and treatment options
HH Uhlving1,2, F Buchvald1,3, CJ Heilmann1, KG Nielsen1,3, M Gormsen4 and KG Muller1,2
1Paediatric Clinic, National University Hospital Rigshospitalet, Copenhagen, Denmark; 2Department of Rheumatology, Institute ofInflammation Research, National University Hospital Rigshospitalet, Copenhagen, Denmark; 3Paediatric Pulmonary Service,National University Hospital Rigshospitalet, Copenhagen, Denmark and 4Department of Radiology, National University HospitalRigshospitalet, Copenhagen, Denmark
Bronchiolitis obliterans (BO) following allogeneic haemato-poietic SCT (HSCT) is a serious complication affecting1.7–26% of the patients, with a reported mortality rate of21–100%. It is considered a manifestation of chronic graft-versus-host disease, but our knowledge of aetiology andpathogenesis is still limited. Diagnostic criteria are beingdeveloped, and will allow more uniform and comparableresearch activities between centres. At present, no rando-mised controlled trials have been completed that coulddemonstrate an effective treatment. Steroids in combinationwith other immunosuppressive drugs still constitute thebackbone of the treatment strategy, and results from our andother centres suggest that monthly infusions of high-dosepulse i.v. methylprednisolone (HDPM) might stabilise thedisease and hinder progression. This article provides anoverview of the current evidence regarding treatment optionsfor BO and presents the treatment results with HDPM in apaediatric national HSCT-cohort.Bone Marrow Transplantation (2012) 47, 1020–1029;doi:10.1038/bmt.2011.161; published online 29 August 2011Keywords: bronchiolitis obliterans; allogeneic haemato-poietic SCT; chronic graft-versus-host disease; treatmentoutcome; methylprednisolone
Introduction
Bronchiolitis obliterans (BO) is an obstructive lung diseaseseen after allogeneic haematopoietic SCT (HSCT).1 Re-spiratory symptoms include cough, dyspnoea and wheeze,but patients may remain relatively asymptomatic despitemoderate-to-severe obstruction. The pronounced variabil-ity in reported incidences (1.7–26%) and mortality rates(21–100%)2–11 of BO may be because of the lack ofconsistent definitions.11–16 No validated treatment protocolhas been established.
This article reviews our current knowledge of thepathogenesis of BO and outlines the current practice inthe treatment of this serious complication. Finally, wepresent our experience of high-dose i.v. pulse methylpred-nisolone treatment (HDPM) in children with BO afterallogeneic HSCT.
Pathogenesis
Because BO resembles allograft-rejection in lung-transplantrecipients (BO syndrome (BOS)) at a pathological, im-munological and physiological level,17 studies of BO inHSCT patients are discussed along with studies of BOS inlung transplant patients in the following.
Increasing evidence suggests that T-cell-mediated recog-nition of alloantigens expressed in the lung tissue consti-tutes a central event in the pathogenesis of BO. Thus, inlung transplanted patients HLA mismatch confers anincreased risk,18 and signs of BO after HSCT is oftenaccompanied by alloreactivity in other organs (for example,skin, liver and eyes).1,3–8,19–22 The essential role of T-cell-mediated allorecognition was further indicated by a studyshowing reduced frequency of BO in HSCT patientsreceiving a T-cell-depleted graft.23 Other reported riskfactors are BU-based conditioning regimens,9,24–26 theintensity of conditioning,27 time from leukaemia diagnosisto HSCT, peripheral blood-derived stem cell source, gradeII–IV acute GvHD (aGvHD),9 pre-transplant airflowobstruction and viral respiratory tract infection within thefirst 100 days after HSCT.10 The findings are however, notconsistent between studies.
Histopathologically, the BO process begins with lym-phocyte infiltration around the small vessels and beneaththe respiratory epithelial lining in the small airways,followed by epithelial cell necrosis and denudation ofmucosa.28 A secondary cascade of non-specific inflamma-tory mediators attracts other cells, including neutrophils,and leads to migration of fibroblasts, proliferation ofsmooth muscle cells, and eventually collagen depositionand fibrous obliteration of the lumen.29,30
Interestingly, studies of BOS in lung transplant recipientshave suggested a central role of T-cell-mediated reactivitytowards collagen. Thus, infiltrating monocytes as well ascollagen type V (col(V))-specific Th17 cells are seen in the
Received 4 February 2011; revised 4 July 2011; accepted 6 July 2011;published online 29 August 2011
All authors have approved the final version.
Correspondence: Dr HH Uhlving, Paediatric Clinic 4072, NationalUniversity Hospital Rigshospitalet, Blegdamsvej 9, 2100 CopenhagenOe, Denmark.E-mail: [email protected]
Bone Marrow Transplantation (2012) 47, 1020–1029
& 2012 Macmillan Publishers Limited All rights reserved 0268-3369/12
www.nature.com/bmt

inflammatory focus.31 Col(V), which is essential for lung-tissue elasticity and compliance, is in healthy individualsnot exposed to immune cells. It is conceivable, although notyet shown, that T-cell-mediated recognition of col(V) mayalso play a pathogenetic role in BO after HSCT, wherecol(V) may be exposed as a result of epithelial damage bychemotherapy and/or irradiation.
T-cell activation is initiated by APCs—usually DCs anddifferentiation of T-cells into T helper 1 (Th1), Th2, Th17and/or regulatory T-cells (Treg) is determined by thecytokine profiles in the microenvironment during T-celldifferentiation.32 Animal studies have suggested a mutuallyexclusive differentiation of CD4þ cells into either Th17 orTreg, depending on the presence (Th17) or absence (Treg) ofIL-6.33 The Th17 subset is important in the development ofinflammation and autoimmunity, while Tregs may down-regulate inflammatory activity in autoimmune diseases andinhibit graft rejection in organ transplantation.32 Lungtransplant patients affected with BOS have a lower level ofcirculating CD4þCD25þTreg than patients in a stableclinical condition.34 In line with this, an animal model ofBOS has shown increased local IL-17 production, withdecreased peripheral blood levels of Tregs.
35 IL-17 has beenshown to induce IL-8 secretion,36,37 which in turn is relatedto airway neutrophilia.38,39 This may be of potential clinicalinterest because the number of neutrophils in the airwayshas been associated with clinically defined BOS phenotypesfollowing lung transplantation.40
Increasing interest is rewarded the role of B cells inchronic GvHD.41 Elevated blood levels of B-cell activatingfactor, essential for survival and differentiation of B cells,have been demonstrated in cGvHD-42,43 and BO-patients.44
A study in lung transplant recipients has suggested atemporal relationship between development of anti-HLAantibodies and BOS.45 Murine studies have demonstratedthat specific antibodies towards HLA class I activateparenchymal cells in a tracheal allograft, resulting inproliferation, growth factor production and apoptosis.This process leads to the activation of fibroblasts, tissueremodelling and proliferation of fibrous tissue observedduring BOS development.46
Taken together, these data suggest a model in whichrespiratory insults and extensive inflammation during thetransplantation constitute a ‘primary hit’ that results inupregulation of MHC molecules and exposure of ‘neoanti-gens’ including col(V). This leads to Th17-biased differ-entiation of T-cells, and subsequently IL-8-drivenneutrophilia. B-cell activation, Ag presentation and pro-duction of anti-HLA Abs may result in aggravation andmaintenance of the inflammatory response and ultimatelyepithelial destruction and pulmonary fibrosis.
Efforts to prevent and treat BO have been directedtowards various steps of this cascade, but the limitedclinical success underlines that our knowledge of thiscondition is still sparse.
Diagnosis
Early diagnosis of BO is difficult, because patients are oftenasymptomatic in the early stages of the disease7 and
inconsistency in applied diagnostic criteria have made itdifficult to compare research results with respect toaetiology, treatment and outcome. The National Instituteof Health (NIH) Consensus Development Project pub-lished in 2006 the first comprehensive attempt to defineclinical criteria for the diagnosis.12 Accordingly, thediagnosis of BO requires fulfillment of all of the followingcriteria:
(1) Absence of active infection.(2) Forced expiratory volume in 1 second (FEV1) o75%
of predicted normal and FEV1/forced vital capacity �
ratio o0.7.(3) Evidence of air trapping or small airway thickening or
bronchiectasis on high-resolution computed tomogra-phy, residual volume 4120% of predicted or patholo-gical confirmation of constrictive bronchiolitis
Chronic GvHD may be diagnosed when BO is proven bylung biopsy. BO diagnosed via clinical criteria requires atleast one manifestation in a separate organ system toestablish the diagnosis of cGvHD.12
The term idiopatic pneumonia syndrome is by theAmerican Thoracic Society defined as widespread alveloarinjury evidenced by radiology, signs and symptoms ofpneumonia and either an increased alveolar to arterialoxygen gradient or a restrictive pulmonary function test notattributed to infection, cardiac dysfunction, renal failure oriatrogenic fluid overload.47 Although BO primarily isdefined as an obstructive lung disease, cases of BO willoften also fit the idiopatic pneumonia syndrome definition.Most cases of idiopatic pneumonia syndrome, however,occurs in the first 3 months after SCT.47–50
The need for further development of these criteria is,however, a matter of ongoing discussion. In a retrospectivestudy by Williams et al.,11 only 18% of previouslydiagnosed BO patients with a FEV1 of o55%, met theNIH consensus criteria. As forced vital capacity and totallung capacity in HSCT patients can be falsely low becauseof restriction from scleroderma or myositis, these authorssuggested a definition of obstruction confirmed by eitherFEV1/slow vital capacity or air trapping on high-resolutioncomputed tomography with residual volume or residualvolume/total lung capacity4120%.11
Treatment
Although a number of first- or second-line treatmentstrategies have been described in the literature, norandomised controlled trials have described a long lastingeffect of any treatment modality for BO.51–53 A Medlinesearch on English literature, including prospective andretrospective studies, randomised or not randomised, withmore than three participants published since 2000, revealed18 studies54–72 and 10 treatment modalities (Table 1). Usingthe NIH grading system, no treatment modality reached anevidence level above III (evidence from opinions ofrespected authorities based on clinical experience, descrip-tive studies or reports from expert committees). Thestrength of recommendation was C (insufficient evidenceto support recommendation or outweigh adverse effects or
Bronchiolitis obliterans in clinical practice
HH Uhlving et al
1021
Bone Marrow Transplantation

Table 1 Clinical studies on treatment strategies for BO and chronic lung GvHD after HSCT
Treatment
regimens
SoR-EL Author Dosage Type of publication cGVHD and BO definitions No. and age of patients enrolled Results
HDPM C-III Ratjen54 i.v. Methylprednisolone
10mg/kg for 3 consecutive
days every 4–6 weeks.
Median 4 treatment cycles
(range 1–6)
Retrospective
paediatric study, no
randomisation or
control group
4/5 of criteria fulfilled: (1) airway
obstruction without reversibility; (2) no
pulmonary infiltrates; (3) no signs of
infection in blood or BAL; (4) reduced
FEV1 without airway restriction; (5)
bronchial dilatation and mosaic pattern
on HRCT
Nine patients, of whom five
were able to perform
spirometry. Median age 8
years (range 1–17)
Significant improvement in FEV1 at 2
months (Po0.02). 7/9 remained clinically
stable. One died from respiratory
failure. Mean follow-up 42±20 months
(range 19–67)
Inhaled
steroids
C-III Bergeron55 Budenosid/formoterol 400/
12 mg� 2/daily
Retrospective study,
no randomisation or
control group
FEV1/VCo5th percentile of normal
value without reversibility OR HRCT
with air-trapping score 45 (maximum
score 18,73). No extrathoracic signs of
cGVHD
13 patients. Median age 44
years (range 16–57)
410% increase in FEV1 in 13/13 patients.
Mean increase in FEV1 36±27%
(P¼ 0.018). Decreased dyspnea in 11/13 pt.
Median follow-up 12.8 months (range 5–
29)
Montelukast C-III Or56 10mg � 1. Median
treatment period 16 months
(range 2–29)
Prospective cohort
study, no
randomisation or
control group
Severe cGVHD with BO according to
the NIH Consensus Criteria12Five patients with BO/19 with
cGVHD. Median age 33 years
(range 17–54)
430% increase in FEV1 in 3/5 patients. 2/5
patients died of end-stage BO. Follow-up
time not reported
Azithromycin C-III Khalid57 500mg � 1 for 3 days,
followed by 250mg three
times/week for 3 months
Observational study,
no randomisation or
control group
Decline in FEV1 of 420%, and evidence
of air trapping on HRCT
Eight patients. Mean age 36
years (range 18–63)
412% improvement in FEV1 in 7/8
patients. Mean increase in FEV1 20.58%
(Po0.0067) and FVC 21.57% (Po0.0052).
Follow-up 12 weeks
Lam58 250mg � 1 for 12 weeks Randomised double-
blinded placebo-
controlled study
FEV1o75%, FEV1/FVC ratioo0.7 and
reduction of FEV1 by 410% compared
with baseline values
12 patients in treatment group,
mean age 44.5 years (range 31–
56), 10 patients control group
mean age 43 years (24–57)
No significant changes in respiratory scores
and FEV1 in the treatment and control
groups
TNF-a
inhibitor
C-III Busca59 Etanercept subcutaneously
25mg twice weekly for 4
weeks, followed by once
weekly for 4 weeks
Retrospective study,
no randomisation or
control group
Steroid-refractory cGVHD with BO
according to the NIH Consensus
Criteria12
Five patients with BO/8 with
cGVHD. Median age all
patients 52 years (range 26–70)
Partial response in 3/5 (450% response in
one evaluable organ without deterioration
of other). Progressive disease in 2/5. 1/5
died of GVHD and septic shock. Median
follow-up 13.5 months (range 10.1–22.5)
Chiang60 Etanercept 25mg (0.4mg/kg
for children) twice weekly for
4 weeks, followed by once
weekly for 4 weeks
Prospective cohort
study, no
randomisation or
control group
Steroid dependent cGVHD involving
lungs (not specified further)
Five patients with lung
involvement/10 with cGVHD.
Median age all patients 38
years (range 3–48)
Partial response in 2/5 (450%
improvement in symptoms, reduction in
steroid dose or immunosuppressive agents).
One died of TTP. Median follow-up all
patients 7 months (range 3–18)
Extracorporal
photopheresis
C-III Flowers61 Three cycles/week for 1 week
followed by twice weekly on
consecutive days during
weeks 2–12
Randomised, single-
blinded multicentre
study
Extensive cGVHD with lung
involvement, as defined by Lee et al.:13
FEV1o80% and a decrease in FEV1/
FVC by 10% in o1 year not explained
by infection, asthma or aspiration.
Stable corticosteroid dose for at least 2
weeks before inclusion
Nine patients with lung
involvement/48 with cGVHD
in ECP group. 7/47 in control
group. Median age ECP group
41 years (range 16–67),
controls 43 years (range 13–67)
Improvement defined as investigators
assessment of complete resolution or
objective improvement: ECP group 11%,
control group 29%; NS. Follow-up
12 weeks
Couriel62 Two to four treatments/week
until partial response,
subsequently tapered by 1/
week. Maintenance regimen
two treatments/2 weeks.
Retrospective,
non-randomised,
single-centre study
cGVHD with symptomatic BO and (1)
decrease in FEV1 420% in 1 year, (2)
air trapping or small-airway thickening
or bronchiectasis on HRCT or
pathologic confirmation of BO and (3)
11 patients with lung
involvement/71 with cGVHD.
Median age all patients 39
years (range 5–70)
Complete response in 1/11. Partial response
in 5/11 (sustained improvement in FEV1
and/or the ability to taper corticosteroids
by 50% without deterioration of
pulmonary function). Follow-up 6 months
Bronchiolitis
obliteransin
clinicalpractice
HH
Uhlving
etal
1022
BoneMarro
wTransplantatio
n
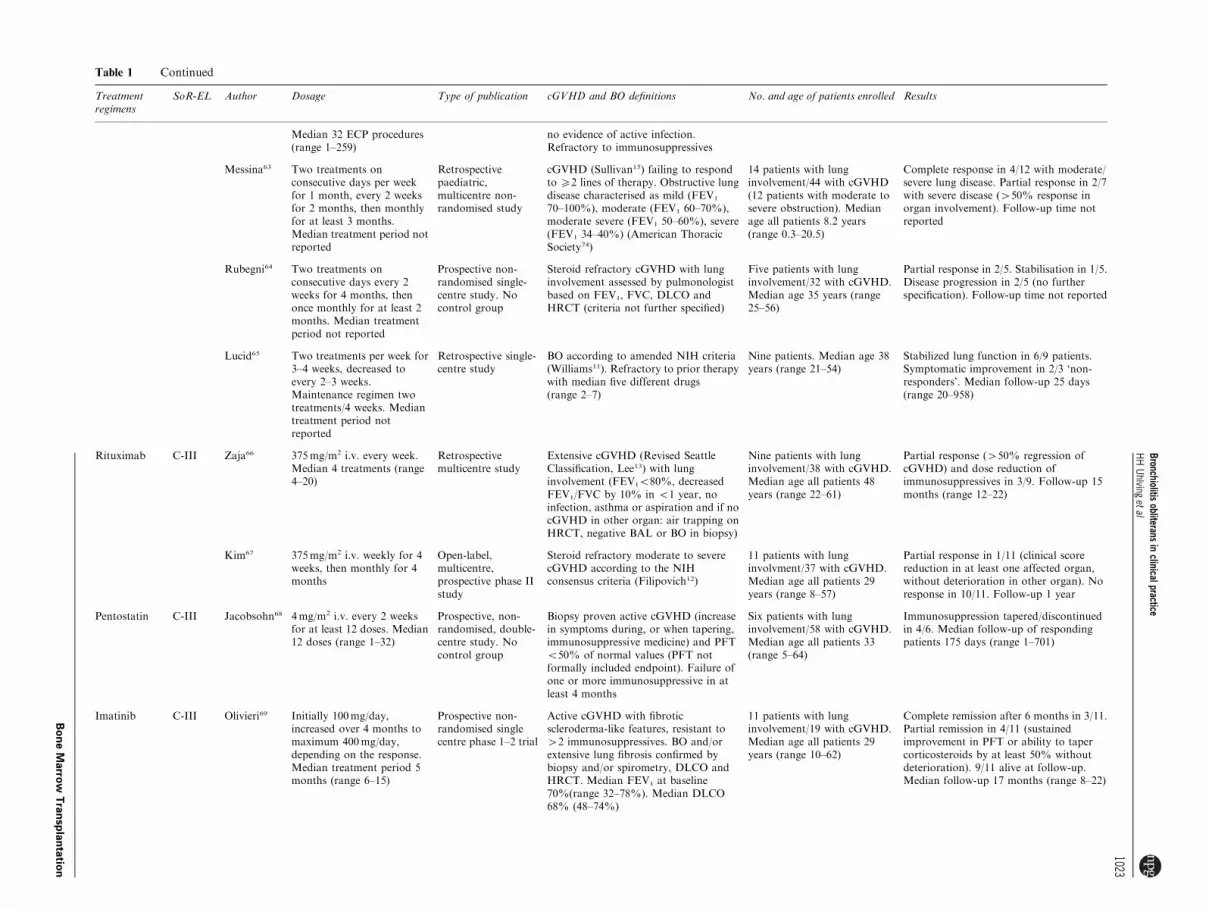
Table 1 Continued
Treatment
regimens
SoR-EL Author Dosage Type of publication cGVHD and BO definitions No. and age of patients enrolled Results
Median 32 ECP procedures
(range 1–259)
no evidence of active infection.
Refractory to immunosuppressives
Messina63 Two treatments on
consecutive days per week
for 1 month, every 2 weeks
for 2 months, then monthly
for at least 3 months.
Median treatment period not
reported
Retrospective
paediatric,
multicentre non-
randomised study
cGVHD (Sullivan15) failing to respond
to X2 lines of therapy. Obstructive lung
disease characterised as mild (FEV1
70–100%), moderate (FEV1 60–70%),
moderate severe (FEV1 50–60%), severe
(FEV1 34–40%) (American Thoracic
Society74)
14 patients with lung
involvement/44 with cGVHD
(12 patients with moderate to
severe obstruction). Median
age all patients 8.2 years
(range 0.3–20.5)
Complete response in 4/12 with moderate/
severe lung disease. Partial response in 2/7
with severe disease (450% response in
organ involvement). Follow-up time not
reported
Rubegni64 Two treatments on
consecutive days every 2
weeks for 4 months, then
once monthly for at least 2
months. Median treatment
period not reported
Prospective non-
randomised single-
centre study. No
control group
Steroid refractory cGVHD with lung
involvement assessed by pulmonologist
based on FEV1, FVC, DLCO and
HRCT (criteria not further specified)
Five patients with lung
involvement/32 with cGVHD.
Median age 35 years (range
25–56)
Partial response in 2/5. Stabilisation in 1/5.
Disease progression in 2/5 (no further
specification). Follow-up time not reported
Lucid65 Two treatments per week for
3–4 weeks, decreased to
every 2–3 weeks.
Maintenance regimen two
treatments/4 weeks. Median
treatment period not
reported
Retrospective single-
centre study
BO according to amended NIH criteria
(Williams11). Refractory to prior therapy
with median five different drugs
(range 2–7)
Nine patients. Median age 38
years (range 21–54)
Stabilized lung function in 6/9 patients.
Symptomatic improvement in 2/3 ‘non-
responders’. Median follow-up 25 days
(range 20–958)
Rituximab C-III Zaja66 375mg/m2 i.v. every week.
Median 4 treatments (range
4–20)
Retrospective
multicentre study
Extensive cGVHD (Revised Seattle
Classification, Lee13) with lung
involvement (FEV1o80%, decreased
FEV1/FVC by 10% in o1 year, no
infection, asthma or aspiration and if no
cGVHD in other organ: air trapping on
HRCT, negative BAL or BO in biopsy)
Nine patients with lung
involvement/38 with cGVHD.
Median age all patients 48
years (range 22–61)
Partial response (450% regression of
cGVHD) and dose reduction of
immunosuppressives in 3/9. Follow-up 15
months (range 12–22)
Kim67 375mg/m2 i.v. weekly for 4
weeks, then monthly for 4
months
Open-label,
multicentre,
prospective phase II
study
Steroid refractory moderate to severe
cGVHD according to the NIH
consensus criteria (Filipovich12)
11 patients with lung
involvment/37 with cGVHD.
Median age all patients 29
years (range 8–57)
Partial response in 1/11 (clinical score
reduction in at least one affected organ,
without deterioration in other organ). No
response in 10/11. Follow-up 1 year
Pentostatin C-III Jacobsohn68 4mg/m2 i.v. every 2 weeks
for at least 12 doses. Median
12 doses (range 1–32)
Prospective, non-
randomised, double-
centre study. No
control group
Biopsy proven active cGVHD (increase
in symptoms during, or when tapering,
immunosuppressive medicine) and PFT
o50% of normal values (PFT not
formally included endpoint). Failure of
one or more immunosuppressive in at
least 4 months
Six patients with lung
involvement/58 with cGVHD.
Median age all patients 33
(range 5–64)
Immunosuppression tapered/discontinued
in 4/6. Median follow-up of responding
patients 175 days (range 1–701)
Imatinib C-III Olivieri69 Initially 100mg/day,
increased over 4 months to
maximum 400mg/day,
depending on the response.
Median treatment period 5
months (range 6–15)
Prospective non-
randomised single
centre phase 1–2 trial
Active cGVHD with fibrotic
scleroderma-like features, resistant to
42 immunosuppressives. BO and/or
extensive lung fibrosis confirmed by
biopsy and/or spirometry, DLCO and
HRCT. Median FEV1 at baseline
70%(range 32–78%). Median DLCO
68% (48–74%)
11 patients with lung
involvement/19 with cGVHD.
Median age all patients 29
years (range 10–62)
Complete remission after 6 months in 3/11.
Partial remission in 4/11 (sustained
improvement in PFT or ability to taper
corticosteroids by at least 50% without
deterioration). 9/11 alive at follow-up.
Median follow-up 17 months (range 8–22)
Bronchiolitis
obliteransin
clinicalpractice
HH
Uhlving
etal
1023
BoneMarro
wTransplantatio
n

costs of the approach) for all treatment modalities apartfrom treatment with corticosteroids (A-III), which isdiscussed in the following.
CorticosteroidsIn 2005, Ratjen et al.54 reported their experience withHDPM treatment in a small cohort of nine children. To ourknowledge, no other published study has described thistreatment regimen for BO after HSCT. HDPM treatment isrecommended in other inflammatory lung diseases inchildren.75,76 Reported side effects include transient flush-ing, headache, mood changes77 and sinus bradycardia,78
but no serious long-term events have been described inchildren. HDPM has been the standard treatment of BOsince 1999 at our centre, and we here summarise the results.
HDPM treatment in the Danish paediatric BO cohort. Withinthe recent 12 years BO has been diagnosed in 13 childrenfollowing HSCT (median age 9.3 years, range 0.6–13.4) at thenational paediatric HSCT centre in Denmark. This corre-sponds to 7.3% of Danish SCT patients below 16 years of agein this period. Nine of the patients were able to perform areliable spirometry and had significantly reduced levels offunction (Table 2). In five cases BO was confirmed by openlung biopsy. The final diagnosis of BO was based on acombination of decreased lung function parameters, high-resolution computed tomography findings, lung biopsy and/orclinical symptoms, but none of the nine patients fully met theNIH clinical criteria for BO.
Our patient cohort was treated with a combination ofconventional immunosuppressive agents (Table 3) and i.v.HDPM 15mg/kg for 2–3 consecutive days every 4–6 weeks.Median time from HSCT to first BO symptoms was 141days (range 53–254) and from symptoms to first course ofHDPM 35 days (3–244). Spirometry was performed beforeHSCT, before initiating HDPM therapy, and thenmonthly. Patients with FEV1 o35% and patients whowere unable to taper oral prednisolone within 6 months ofHDPM initiation were given additional treatment withmonthly infusions of infliximab.
One patient (no. 8) died of respiratory insufficiencybecause of CMV-pneumonia 1 month after initiation oftherapy, whereas one patient (no. 6) died of leukaemicrelapse. In the patients tested, a significant increase in FEV1
was seen 3 months (P¼ 0.010) and 1 year (P¼ 0.011) afterinitiation of HDPM (the Wilcoxon rank sum test), withmedian increase in FEV1 from 48.1% at treatmentinitiation to 71.4% and 83.0%, respectively (Figure 1).During further follow-up lung function generally stabilisedat a moderately reduced level.
This small population-based study of a rather hetero-geneous group of patients has obvious limitations, sharedby the majority of the previous studies presented in Table 1,and does not allow firm conclusions. Our data suggests thatstabilisation of lung function in BO patients may beachieved by early commencement on high-dose pulsecorticosteroids in combination with other immunosuppres-sive treatment. The effect of HDPM on relapse rate andinfectious complications cannot be properly assessed in astudy of this size. Further studies, preferebly a multicenterT
able
1Continued
Treatm
ent
regim
ens
SoR-EL
Author
Dosage
Typeofpublication
cGVHD
andBO
definitions
No.andageofpatientsenrolled
Results
Stadler7
0100–400mg/day.Median
treatm
entperiod4months
(range1–17)
Prospective,
single
centre,
open-label
non-randomised
study
Severepulm
onary
cGVHD,resistantto
extensiveim
munosuppressivetherapy.
MedianFEV
129%
(range18–41)
Ninepatients.Medianage45
years
(range24–50)
Recoveryoflungfunction(from
severeto
moderate
reduction)in
1/9.Abilityto
taper
steroidsin
2/9.Nochangein
5/9.2/9
died
ofBO
and/orrelapse.Follow-uptimenot
reported
Thalidomide
C-III
Kulkarni71
Initially50–100mg�3,
increasedgradually
dependingontolerance
and
clinicalresponse
Median
dailydose
400mg(range
50–1200).Mediantreatm
ent
period61days(range
1–1210)
Retrospective,
non-
randomised
study
ExtensivecG
VHD
(presentin
41
organ)withlunginvolvem
ent
(Sullivan,14Akpek
16).No,or
insufficient,response
toprednisolone
andcyclosporineand/orazathioprine
14patients
withlung
involvem
ent/59withcG
VHD.
Medianageallpatients
31.5
years
(range2–52)
Complete
response
3/14.Partialresponse
in
2/14(improved
perform
ance
status,450%
resolutionofsignsandsymptoms).Median
follow-up53months(range5–159)
Abbreviations:BAL¼bronchoalveolarlavage;BO¼bronchiolitisobliterans;cG
VHD¼chronicGVHD;DLCO¼carbonmonoxidediffusingcapacity;EL¼evidence
level;ECP¼extracorporealphotopheresis;
FEV
1¼forced
expiratory
volumein
1second;FVC¼forced
vitalcapacity;HDPM
¼high-dose
pulsei.v.methylprednisolone;
HRCT¼high-resolutioncomputedtomography;HSCT¼haem
atopoieticSCT;
NS¼nonsignificant;NIH
¼NationalInstitute
ofHealth;PFT¼pulm
onary
functiontest;SoR¼strength
ofrecommendation;TTP¼thromboticthrombocytopenic
purpura.
Bronchiolitis obliterans in clinical practice
HH Uhlving et al
1024
Bone Marrow Transplantation

randomised study would be needed to properly adress bothtreatment response and possible adverse effects of HDPMtherapy.
Corticosteroids have been the backbone of cGvHDtherapy, since Sullivan et al.14 in 1981 demonstratedimproved outcome in cGvHD patients receiving corticos-teroids in combination with other immunosuppressors.14
The role of prednisolone was further established in tworandomised studies,79,80 where the addition of azathiopr-ine79 and cyclosporine80 did not seem to further improveoutcome in standard risk cGvHD patients. However, theeffect of orally administrated prednisolone on lunginvolvement was not reported in those studies. First-linetreatment of cGVHD mainly consists of prednisolone witha starting dose of 1mg/kg/day orally.52
Inhaled corticosteroids in combination with long-actingbronchodilators are now being tested in BO patients in a
Table 2 The Danish paediatric BO cohort accordance with NIH clinical criteria at time of diagnosis
BO on
biopsy
FEV1% FEV1/
FVC%
HRCT RV% Infection RV/TLC% cGVHD in
other organ
1 Yes 42.8 106.8 Bronchiectasis, air trapping Unknown No Unknown Skin
2 Yes 39 89.4 Air trapping Unknown No Unknown No3 No 53.5 77.4 Bronchiectasis, bronchial thickening, small nodular opacities 111.40 No 137.70 No4 No 29.3 91.0 Air trapping, bronchiectasis, bronchial thickening Unknown No Unknown No5 No 62.0 95 Bronchiectasis, bronchial thickening, air trapping 127 No 142 No6 No 61 85 — 131 No 132 Skin7 Yes 53.5 65.8 Centrilobular opacities and reduced transparency Unknown No Unknown No
8 Yes 40.4 109.3 Air trapping, bronchiectasis, bronchial thickening, groundglass opacities, consolidation of peripheral lung segments
Unknown No Unknown No
9 No 39.8 69.3 Normal Unknown No Unknown No
Abbreviations: BO¼bronchiolitis obliterans; cGVHD¼ chronic GVHD; FEV1¼ forced expiratory volume in 1 second; FVC¼ forced vital capacity;
HRCT¼ high-resolution computed tomography; NIH¼National Institute of Health; RV¼ residual volume; TLC¼ total lung capacity.
Table 3 Patient characteristics
Diagnosis Age at
HSCT
SCT
conditioning
GVHDprophylaxis
Days between
SCT and onset
Days from
symptoms
to HDPM
BO treatment Outcome
1 JMML 11 Bu, Cy,Me, ATG
MTX,Cic/MPA
159 16 HDPM, Po,In, Ra/Ta
Stable for 3 y. Deterioration afterwidened HDPM-intervals. Dead fromend-stage BO 5 years after BO-diagnosis.
2 SAA 4 Bu, Cy, ATG MTX, Cic 57 244 HDPM,Cic/Ta, In
Alive, stable
3 MDS secondary toALL
10 Bu, Cy,Me, ATG
MTX,Cic/MPA
254 35 HDPM, Po Alive, stable
4 Pre-B-ALL 7 Bu, Cy,Et, ATG
MTX, Cic 212 111 HDPM, In Lost to follow-up after 6 months
5 HLH 13 Bu, Cy, ATG MTX, Cic 231 16 HDPM, Po Paraplegia after car-accident6 Pre-B ALL 13 Cy, ATG,
TBIMTX,Cic/MPA
72 21 HDPM, Po Relapse 8 months after BO diagnosis.Dead
7 MLD 9 Bu, Cy, ATG MTX,Cic/MPA
141 86 HDPM, Po Alive, stable
8 T-ALL 10 Cy, ATG,TBI
MTX, Cic 99 3 HDPM, Po Dead from respiratory insufficiency(CMV pneumonia) 1 month afterHDPM initiation.
9 SAA 11 Bu, Cy, ATG MTX,
Cic/MPA
53 106 HDPM, Po,
In, Ra
Alive, stable
Abbreviations: ATG¼ anti-thymocyte globulin; BO¼ bronchiolitis obliterans; Bu¼ busulfex; Cic¼ ciclosporine; Et¼ etophos; HDPM¼ high-dose pulse
i.v. methylprednisolone; HLH¼ haemophagocytic lymphohistiocytosis; HSCT¼haematopoietic SCT; In¼ infliximab; JMML¼ juvenile myelomonocytic
leukaemia; Me¼melphalan; MDS¼myelodysplastic syndrome; MLD¼metachromatic leucodystrophy; MPA¼mycophenolate mofetil; Po¼ oral
prednisolone; Ra¼ rapamune; SAA¼ severe aplastic anemia; Ta¼ tacrolimus.
120
*P =0.010
*P =0.011
Patient 1
Patient 2
Patient 5
Patient 6
Patient 7
Patient 3
Patient 4
11010090
7080
6050
FE
V1%
pre
d
40
2030
100
Bef
ore S
CT
BO d
iagnosi
s
+1 m
onth
+3 m
onths
+6 m
onths
>12
month
s
Figure 1 A significant increase in FEV1 is seen from time of BO diagnosis
and initiation of HDPM compared with 3 months and 1 year after
initiation of therapy.
Bronchiolitis obliterans in clinical practice
HH Uhlving et al
1025
Bone Marrow Transplantation

prospective multicentre, randomised double-blinded trial.81
A pilot study of 13 patients with respiratory symptoms, butno extrapulmonary signs of cGvHD, showed some effecton lung function parameters55 (Table 1).
TNF-a inhibitorsInsights into the role of proinflammatory cytokines indisease pathogenesis, has led to the use of TNF-a inhibitorsas second-line BO treatment. The three patients in theDanish cohort, who received infliximab due to a decrease inlung function during the standard HDPM regimen,experienced stabilisation after commencement of inflixi-mab. A case study from Texas described completeresolution of symptoms in a patient with steroid refractoryBO on etanercept treatment.82 The two studies on the effectof infliximab described in Table 1(refs 59,60) suggests someimprovement. An ongoing study of etanercept therapy atthe Ann Arbor Cancer Center (NCT00141726) mayprovide further insights.
AzithromycinThe ability of azithromycin to inhibit airway neutrophiliaand IL-8 production39,40 may explain the improvementafter treatment in a subgroup of lung transplant recipientswith BOS.83,84 Similar positive results have been reported ina preliminary study on 8 patients with BO after HSCT57
(Table 1). However, a randomised placebo-controlledclinical trial from Hong Kong58 failed to prove superiorityof azithromycin to placebo when initiated (mean) 4.3 and5.8 years, respectively, after BO diagnosis. A recentlypublished case-series indicates a steroid sparing effect ofazithromycin in combination with inhaled corticosteroidsand montelukast in patients with newly diagnosed BO.85
Further studies are needed to establish an eventual effect ofazythromycin on incipient BO.
Extracorporeal photopheresisSelective downregulation of T-cell-mediated immunity isthought to explain the effect of extracorporeal photopher-esis in the treatment of GvHD.86 Though several studieshave been performed in patients with BO after HSCT61–
65,87–91 and lung transplantation,92–94 the studies are difficultto interpret because of the heterogeneity in the treatmentschedules, diagnostic criteria and response assessmentcriteria (Table 1). A prospective randomised study ofextracorporeal photopheresis treatment performed byFlowers et al.61 revealed a significant improvement ofcGVHD in the skin, and indicated a steroid sparing effecton cGvHD in general. No effect on lung functionparameters was noted.
RituximabAn attempt to attack the B-cell response suspected to be apart of cGvHD aetiology has led to the application of themonoclonal CD20-Ab Rituximab. Although several studieshave suggested an effect on cGvHD in the skin,66,95–98 noconvincing effect on BO has been established.66,67
Conclusion
Solid evidence regarding the efficacy of the variousavailable treatment modalities in BO is still sparse. Ongoingclinical trials together with new insights into the pathogen-esis will hopefully contribute to fill this gap. Thoughestablished clinical criteria are important as a research tool,the experience with the NIH Consensus Criteria mayindicate a need for further development of clinical criteriaand simplification of these. Our experience emphasises theneed for improved diagnostic criteria, in particular for theyoung children who are unable to perform spirometry.
The preliminary experiences with HDPM treatment fromour and other centres suggest that the efficacy of thistreatment regimen, including the long-term effects deservesfurther validation in clinical trials. Though alternativetreatment options may seem promising, corticosteroids arestill likely to remain a mainstay in GvHD treatment in thecoming years. However, with improved insights into thepathogenesis of BO new treatment modalities, includingcytokine antagonists and cellular therapy, may changetreatment strategies fundamentally.
Conflict of interest
The authors declare no conflict of interest.
Acknowledgements
This work was supported by grants from the Danish Children’sCancer Association and the Research Council at the NationalUniversity Hospital Rigshospitalet.
References
1 Chien JW, Duncan S, Williams KM, Pavletic SZ. Bronchiolitis
obliterans syndrome after allogeneic hematopoietic stem cell
transplantation-an increasingly recognized manifestation of
chronic graft-versus-host disease. Biol Blood Marrow Trans-
plant 2010; 16(Suppl 1): S106–S114.
2 Dudek AZ, Mahaseth H, DeFor TE, Weisdorf DJ. Bronch-
iolitis obliterans in chronic graft-versus-host disease: analysis
of risk factors and treatment outcomes. Biol Blood Marrow
Transplant 2003; 9: 657–666.
3 Nakaseko C, Ozawa S, Sakaida E, Sakai M, Kanda Y, Oshima
K et al. Incidence, risk factors and outcomes of bronchiolitis
obliterans after allogeneic stem cell transplantation. Int J
Hematol 2011; 93: 375–382.
4 Nishio N, Yagasaki H, Takahashi Y, Muramatsu H, Hama A,
Tanaka M et al. Late-onset non-infectious pulmonary
complications following allogeneic hematopoietic stem cell
transplantation in children. Bone Marrow Transplant 2009; 44:
303–308.
5 Sakaida E, Nakaseko C, Harima A, Yokota A, Cho R, Saito Y
et al. Late-onset noninfectious pulmonary complications after
allogeneic stem cell transplantation are significantly associated
with chronic graft-versus-host disease and with the graft-
versus-leukemia effect. Blood 2003; 102: 4236–4242.
6 Holland HK, Wingard JR, Beschorner WE, Saral R, Santos
GW. Bronchiolitis obliterans in bone marrow transplantation
Bronchiolitis obliterans in clinical practice
HH Uhlving et al
1026
Bone Marrow Transplantation

and its relationship to chronic graft-v-host disease and low
serum IgG. Blood 1988; 72: 621–627.
7 Clark JG, Crawford SW, Madtes DK, Sullivan KM.
Obstructive lung disease after allogeneic marrow transplanta-
tion. Clinical presentation and course. Ann Intern Med 1989;
111: 368–376.
8 Schultz KR, Green GJ, Wensley D, Sargent MA, Magee JF,
Spinelli JJ et al. Obstructive lung disease in children
after allogeneic bone marrow transplantation. Blood 1994;
84: 3212–3220.
9 Santo Tomas LH, Loberiza Jr FR, Klein JP, Layde PM,
Lipchik RJ, Rizzo JD et al. Risk factors for bronchiolitis
obliterans in allogeneic hematopoietic stem-cell transplanta-
tion for leukemia. Chest 2005; 128: 153–161.
10 Chien JW, Martin PJ, Gooley TA, Flowers ME, Heckbert SR,
Nichols WG et al. Airflow obstruction after myeloablative
allogeneic hematopoietic stem cell transplantation. Am J
Respir Crit Care Med 2003; 168: 208–214.
11 Williams KM, Chien JW, Gladwin MT, Pavletic SZ. Bronch-
iolitis obliterans after allogeneic hematopoietic stem cell
transplantation. JAMA 2009; 302: 306–314.
12 Filipovich AH, Weisdorf D, Pavletic S, Socie G, Wingard JR,
Lee SJ et al.National Institutes of Health consensus development
project on criteria for clinical trials in chronic graft-versus-host
disease: I. Diagnosis and staging working group report. Biol
Blood Marrow Transplant 2005; 11: 945–956.
13 Lee SJ, Vogelsang G, Flowers ME. Chronic graft-versus-host
disease. Biol Blood Marrow Transplant 2003; 9: 215–233.
14 Sullivan KM, Shulman HM, Storb R, Weiden PL, With-
erspoon RP, McDonald GB et al. Chronic graft-versus-host
disease in 52 patients: adverse natural course and successful
treatment with combination immunosuppression. Blood 1981;
57: 267–276.
15 Sullivan KM, Agura E, Anasetti C, Appelbaum F, Badger C,
Bearman S et al. Chronic graft-versus-host disease and other
late complications of bone marrow transplantation. Semin
Hematol 1991; 28: 250–259.
16 Akpek G, Zahurak ML, Piantadosi S, Margolis J, Doherty J,
Davidson R et al. Development of a prognostic model for
grading chronic graft-versus-host disease. Blood 2001; 97:
1219–1226.
17 Philit F, Wiesendanger T, Archimbaud E, Mornex JF, Brune J,
Cordier JF. Post-transplant obstructive lung disease (‘bronch-
iolitis obliterans’): a clinical comparative study of bone
marrow and lung transplant patients. Eur Respir J 1995; 8:
551–558.
18 Schulman LL, Weinberg AD, McGregor CC, Suciu-Foca NM,
Itescu S. Influence of donor and recipient HLA locus
mismatching on development of obliterative bronchiolitis after
lung transplantation. Am J Respir Crit Care Med 2001; 163:
437–442.
19 Schwarer AP, Hughes JM, Trotman-Dickenson B, Krausz T,
Goldman JM. A chronic pulmonary syndrome associated with
graft-versus-host disease after allogeneic marrow transplanta-
tion. Transplantation 1992; 54: 1002–1008.
20 Clark JG, Schwartz DA, Flournoy N, Sullivan KM, Crawford
SW, Thomas ED. Risk factors for airflow obstruction in
recipients of bone marrow transplants. Ann Intern Med 1987;
107: 648–656.
21 Palmas A, Tefferi A, Myers JL, Scott JP, Swensen SJ, Chen
MG et al. Late-onset noninfectious pulmonary complications
after allogeneic bone marrow transplantation. Br J Haematol
1998; 100: 680–687.
22 Duncan CN, Buonanno MR, Barry EV, Myers K, Peritz D,
Lehmann L. Bronchiolitis obliterans following pediatric
allogeneic hematopoietic stem cell transplantation. Bone
Marrow Transplant 2008; 41: 971–975.
23 Ditschkowski M, Elmaagacli AH, Trenschel R, Peceny R,
Koldehoff M, Schulte C et al. T-cell depletion prevents from
bronchiolitis obliterans and bronchiolitis obliterans with
organizing pneumonia after allogeneic hematopoietic stem cell
transplantation with related donors. Haematologica 2007; 92:
558–561.
24 Ringden O, Remberger M, Ruutu T, Nikoskelainen J, Volin L,
Vindelov L et al. Increased risk of chronic graft-versus-host
disease, obstructive bronchiolitis, and alopecia with busulfan
versus total body irradiation: long-term results of a rando-
mized trial in allogeneic marrow recipients with leukemia.
Nordic Bone Marrow Transplantation Group. Blood 1999; 93:
2196–2201.
25 Bruno B, Souillet G, Bertrand Y, Werck-Gallois MC, So SA,
Bellon G. Effects of allogeneic bone marrow transplantation
on pulmonary function in 80 children in a single paediatric
centre. Bone Marrow Transplant 2004; 34: 143–147.
26 Marras TK, Chan CK, Lipton JH, Messner HA, Szalai JP,
Laupacis A. Long-term pulmonary function abnormalities and
survival after allogeneic marrow transplantation. Bone Marrow
Transplant 2004; 33: 509–517.
27 Yoshihara S, Tateishi U, Ando T, Kunitoh H, Suyama H,
Onishi Y et al. Lower incidence of bronchiolitis obliterans in
allogeneic hematopoietic stem cell transplantation with re-
duced-intensity conditioning compared with myeloablative
conditioning. Bone Marrow Transplant 2005; 35: 1195–1200.
28 Yousem SA. The histological spectrum of pulmonary graft-
versus-host disease in bone marrow transplant recipients. Hum
Pathol 1995; 26: 668–675.
29 Shulman HM, Kleiner D, Lee SJ, Morton T, Pavletic SZ,
Farmer E et al. Histopathologic diagnosis of chronic graft-
versus-host disease: National Institutes of Health Consensus
Development Project on Criteria for Clinical Trials in Chronic
Graft-versus-Host Disease: II. Pathology Working Group
Report. Biol Blood Marrow Transplant 2006; 12: 31–47.
30 Estenne M, Maurer JR, Boehler A, Egan JJ, Frost A, Hertz M
et al. Bronchiolitis obliterans syndrome 2001: an update
of the diagnostic criteria. J Heart Lung Transplant 2002; 21:
297–310.
31 BurlinghamWJ, Love RB, Jankowska-Gan E, Haynes LD, Xu
Q, Bobadilla JL et al. IL-17-dependent cellular immunity to
collagen type V predisposes to obliterative bronchiolitis in
human lung transplants. J Clin Invest 2007; 117: 3498–3506.
32 Afzali B, Lombardi G, Lechler RI, Lord GM. The role of T
helper 17 (Th17) and regulatory T cells (Treg) in human organ
transplantation and autoimmune disease. Clin Exp Immunol
2007; 148: 32–46.
33 Bettelli E, Carrier Y, Gao W, Korn T, Strom TB, Oukka M
et al. Reciprocal developmental pathways for the generation of
pathogenic effector TH17 and regulatory T cells. Nature 2006;
441: 235–238.
34 Meloni F, Vitulo P, Bianco AM, Paschetto E, Morosini M,
Cascina A et al. Regulatory CD4+CD25+ T cells in the
peripheral blood of lung transplant recipients: correlation with
transplant outcome. Transplantation 2004; 77: 762–766.
35 Nakagiri T, Inoue M, Morii E, Minami M, Sawabata N,
Utsumi T et al. Local IL-17 production and a decrease in
peripheral blood regulatory T cells in an animal model of
bronchiolitis obliterans. Transplantation 2010; 89: 1312–1319.
36 Laan M, Linden. IL-17 as a potential target for modulating
airway neutrophilia. Curr Pharm Des 2002; 8: 1855–1861.
37 Vanaudenaerde BM, Wuyts WA, Dupont LJ, Van Raemdonck
DE, Demedts MM, Verleden GM. Interleukin-17 stimulates
release of interleukin-8 by human airway smooth muscle cells
in vitro: a potential role for interleukin-17 and airway smooth
muscle cells in bronchiolitis obliterans syndrome. J Heart Lung
Transplant 2003; 22: 1280–1283.
Bronchiolitis obliterans in clinical practice
HH Uhlving et al
1027
Bone Marrow Transplantation

38 Zheng L, Whitford HM, Orsida B, Levvey BJ, Bailey M,
Walters EH et al. The dynamics and associations of airway
neutrophilia post lung transplantation. Am J Transplant 2006;
6: 599–608.
39 Verleden GM, Vanaudenaerde BM, Dupont LJ, Van Raem-
donck DE. Azithromycin reduces airway neutrophilia and
interleukin-8 in patients with bronchiolitis obliterans syn-
drome. Am J Respir Crit Care Med 2006; 174: 566–570.
40 Verleden GM, Vos R, De Vleeschauwer SI, Willems-Widyas-
tuti A, Verleden SE, Dupont LJ et al. Obliterative bronchiolitis
following lung transplantation: from old to new concepts?
Transpl Int 2009; 22: 771–779.
41 Alousi AM, Uberti J, Ratanatharathorn V. The role of B cell
depleting therapy in graft versus host disease after allogeneic
hematopoietic cell transplant. Leuk Lymphoma 2010; 51:
376–389.
42 Sarantopoulos S, Stevenson KE, Kim HT, Cutler CS, Bhuiya
NS, Schowalter M et al. Altered B-cell homeostasis and excess
BAFF in human chronic graft-versus-host disease. Blood 2009;
113: 3865–3874.
43 Sarantopoulos S, Stevenson KE, Kim HT, Bhuiya NS, Cutler
CS, Soiffer RJ et al. High levels of B-cell activating factor in
patients with active chronic graft-versus-host disease. Clin
Cancer Res 2007; 13: 6107–6114.
44 Kuzmina Z, Weigl R, Krenn K, Petkov V, Koermoeczi U,
Rottal A et al. Excess of BAFF and distortion of B-cell
homeostasis in patients with newly diagnosed bronchiolitis
obliterans syndrome associated with chronic graft-versus-host
disease. Bone Marrow Transplantation 2011; 46(Suppl 1): S7.
Ref Type: Abstract.
45 Jaramillo A, Smith MA, Phelan D, Sundaresan S, Trulock E,
Lynch J et al. Temporal relationship between the development
of anti-HLA antibodies and the development of bronchiolitis
obliterans syndrome after lung transplantation. Transplant
Proc 1999; 31: 185–186.
46 Maruyama T, Jaramillo A, Narayanan K, Higuchi T,
Mohanakumar T. Induction of obliterative airway disease by
anti-HLA class I antibodies. Am J Transplant 2005; 5: 2126–
2134.
47 Panoskaltsis-Mortari A, Griese M, Madtes DK, Belperio JA,
Haddad IY, Folz RJ et al. An official American thoracic
society research statement: noninfectious lung injury after
hematopoietic stem cell transplantation: idiopathic pneumonia
syndrome. Am J Respir Crit Care Med 2011; 183: 1262–1279.
48 Zhu KE, Hu JY, Zhang T, Chen J, Zhong J, Lu YH.
Incidence, risks, and outcome of idiopathic pneumonia
syndrome early after allogeneic hematopoietic stem cell
transplantation. Eur J Haematol 2008; 81: 461–466.
49 Gower WA, Collaco JM, Mogayzel Jr PJ. Lung function and
late pulmonary complications among survivors of hemato-
poietic stem cell transplantation during childhood. Paediatr
Respir Rev 2010; 11: 115–122.
50 Fukuda T, Hackman RC, Guthrie KA, Sandmaier BM,
Boeckh M, Maris MB et al. Risks and outcomes of idiopathic
pneumonia syndrome after nonmyeloablative and conven-
tional conditioning regimens for allogeneic hematopoietic stem
cell transplantation. Blood 2003; 102: 2777–2785.
51 Hildebrandt GC, Fazekas T, Lawitschka A, Bertz H, Greinix
H, Halter J et al. Diagnosis and treatment of pulmonary
chronic GVHD: report from the consensus conference on
clinical practice in chronic GVHD. Bone Marrow Transplant
2011; 46: 1283–1295.
52 Wolff D, Gerbitz A, Ayuk F, Kiani A, Hildebrandt GC,
Vogelsang GB et al. Consensus conference on clinical practice
in chronic graft-versus-host disease (GVHD): first-line and
topical treatment of chronic GVHD. Biol Blood Marrow
Transplant 2010; 16: 1611–1628.
53 Wolff D, Schleuning M, von HS, Bacher U, Gerbitz A, Stadler
M et al. Consensus conference on clinical practice in chronic
GVHD: second-line treatment of chronic graft-versus-host
disease. Biol Blood Marrow Transplant 2011; 17: 1–17.
54 Ratjen F, Rjabko O, Kremens B. High-dose corticosteroid
therapy for bronchiolitis obliterans after bone marrow
transplantation in children. Bone Marrow Transplant 2005;
36: 135–138.
55 Bergeron A, Belle A, Chevret S, Ribaud P, Devergie A,
Esperou H et al. Combined inhaled steroids and bronchodi-
latators in obstructive airway disease after allogeneic stem cell
transplantation. Bone Marrow Transplant 2007; 39: 547–553.
56 Or R, Gesundheit B, Resnick I, Bitan M, Avraham A, Avgil M
et al. Sparing effect by montelukast treatment for chronic graft
versus host disease: a pilot study. Transplantation 2007; 83:
577–581.
57 Khalid M, Al SA, Saleemi S, Al DS, Zeitouni M, Al MA et al.
Azithromycin in bronchiolitis obliterans complicating bone
marrow transplantation: a preliminary study. Eur Respir J
2005; 25: 490–493.
58 Lam DCL, Lam B, Wong MKY, Lu C, Au WY, Tse EWC
et al. Effects of Azithromycin in bronchiolitis obliterans
syndrome after hematopoietic SCT—a randomized double-
blinded placebo-controlled study. Bone Marrow Transplant
2011; 46: 1551–1556.
59 Busca A, Locatelli F, Marmont F, Ceretto C, Falda M.
Recombinant human soluble tumor necrosis factor receptor
fusion protein as treatment for steroid refractory graft-versus-
host disease following allogeneic hematopoietic stem cell
transplantation. Am J Hematol 2007; 82: 45–52.
60 Chiang KY, Abhyankar S, Bridges K, Godder K, Henslee-
Downey JP. Recombinant human tumor necrosis factor
receptor fusion protein as complementary treatment for
chronic graft-versus-host disease. Transplantation 2002; 73:
665–667.
61 Flowers ME, Apperley JF, van BK, Elmaagacli A, Grigg A,
Reddy V et al. A multicenter prospective phase 2 randomized
study of extracorporeal photopheresis for treatment of chronic
graft-versus-host disease. Blood 2008; 112: 2667–2674.
62 Couriel DR, Hosing C, Saliba R, Shpall EJ, Anderlini P,
Rhodes B et al. Extracorporeal photochemotherapy for the
treatment of steroid-resistant chronic GVHD. Blood 2006; 107:
3074–3080.
63 Messina C, Locatelli F, Lanino E, Uderzo C, Zacchello G,
Cesaro S et al. Extracorporeal photochemotherapy for
paediatric patients with graft-versus-host disease after haema-
topoietic stem cell transplantation. Br J Haematol 2003; 122:
118–127.
64 Rubegni P, Cuccia A, Sbano P, Cevenini G, Carcagni MR,
D’Ascenzo G et al. Role of extracorporeal photochemotherapy
in patients with refractory chronic graft-versus-host disease. Br
J Haematol 2005; 130: 271–275.
65 Lucid CE, Savani BN, Engelhardt BG, Shah P, Clifton C,
Greenhut SL et al. Extracorporeal photopheresis in patients
with refractory bronchiolitis obliterans developing after allo-
SCT. Bone Marrow Transplant 2011; 46: 426–429.
66 Zaja F, Bacigalupo A, Patriarca F, Stanzani M, Van Lint MT,
Fili C et al. Treatment of refractory chronic GVHD with
rituximab: a GITMO study. Bone Marrow Transplant 2007; 40:
273–277.
67 Kim SJ, Lee JW, Jung CW, Min CK, Cho B, Shin HJ et al.
Weekly rituximab followed by monthly rituximab treatment
for steroid-refractory chronic graft-versus-host disease: results
from a prospective, multicenter, phase II study. Haematologica
2010; 95: 1935–1942.
68 Jacobsohn DA, Chen AR, Zahurak M, Piantadosi S, Anders
V, Bolanos-Meade J et al. Phase II study of pentostatin in
Bronchiolitis obliterans in clinical practice
HH Uhlving et al
1028
Bone Marrow Transplantation

patients with corticosteroid-refractory chronic graft-versus-
host disease. J Clin Oncol 2007; 25: 4255–4261.
69 Olivieri A, Locatelli F, Zecca M, Sanna A, Cimminiello M,
Raimondi R et al. Imatinib for refractory chronic graft-versus-
host disease with fibrotic features. Blood 2009; 114: 709–718.
70 Stadler M, Ahlborn R, Kamal H, Diedrich H, Buchholz S,
Eder M et al. Limited efficacy of imatinib in severe pulmonary
chronic graft-versus-host disease. Blood 2009; 114: 3718–3719.
71 Kulkarni S, Powles R, Sirohi B, Treleaven J, Saso R, Horton C
et al. Thalidomide after allogeneic haematopoietic stem cell
transplantation: activity in chronic but not in acute graft-versus-
host disease. Bone Marrow Transplant 2003; 32: 165–170.
72 Couriel D, Carpenter PA, Cutler C, Bolanos-Meade J, Treister
NS, Gea-Banacloche J et al. Ancillary therapy and supportive
care of chronic graft-versus-host disease: national institutes of
health consensus development project on criteria for clinical
trials in chronic Graft-versus-host disease: V. Ancillary
Therapy and Supportive Care Working Group Report. Biol
Blood Marrow Transplant 2006; 12: 375–396.
73 De Jong PA, Dodd JD, Coxson HO, Storness-Bliss C, Pare
PD, Mayo JR et al. Bronchiolitis obliterans following lung
transplantation: early detection using computed tomographic
scanning. Thorax 2006; 61: 799–804.
74 American Thoracic Society. Lung function testing: selection of
reference values and interpretative strategies. Am Rev Respir
Dis 1992; 146(5 Part 1): 1368–1369.
75 Clement A. Task force on chronic interstitial lung disease in
immunocompetent children. Eur Respir J 2004; 24: 686–697.
76 Desmarquest P, Tamalet A, Fauroux B, Boule M, Boccon-
Gibod L, Tournier G et al. Chronic interstitial lung disease in
children: response to high-dose intravenous methylpredniso-
lone pulses. Pediatr Pulmonol 1998; 26: 332–338.
77 Buchvald F, Petersen BL, Damgaard K, Deterding R,
Langston C, Fan LL et al. Frequency, treatment, and
functional outcome in children with hypersensitivity pneumo-
nitis. Pediatr Pulmonol (e-pub ahead of print 26 May 2011).
78 Akikusa JD, Feldman BM, Gross GJ, Silverman ED,
Schneider R. Sinus bradycardia after intravenous pulse
methylprednisolone. Pediatrics 2007; 119: e778–e782.
79 Sullivan KM, Witherspoon RP, Storb R, Weiden P, Flournoy
N, Dahlberg S et al. Prednisone and azathioprine compared
with prednisone and placebo for treatment of chronic graft-v-
host disease: prognostic influence of prolonged thrombocyto-
penia after allogeneic marrow transplantation. Blood 1988; 72:
546–554.
80 Koc S, Leisenring W, Flowers ME, Anasetti C, Deeg HJ, Nash
RA et al. Therapy for chronic graft-versus-host disease: a
randomized trial comparing cyclosporine plus prednisone
versus prednisone alone. Blood 2002; 100: 48–51.
81 Bergeron A, Chagnon K, Feuillet S, Chevret S, Tazi A.
Prospective evaluation of the efficacy of the combination of
budesonide/formoterol in obstructive airway disease after
allogeneic hematopoietic stem cell transplantation]. Rev Mal
Respir 2009; 26: 794–800.
82 Fullmer JJ, Fan LL, Dishop MK, Rodgers C, Krance R.
Successful treatment of bronchiolitis obliterans in a bone
marrow transplant patient with tumor necrosis factor-alpha
blockade. Pediatrics 2005; 116: 767–770.
83 Gottlieb J, Szangolies J, Koehnlein T, Golpon H, Simon A,
Welte T. Long-term azithromycin for bronchiolitis obliterans
syndrome after lung transplantation. Transplantation 2008; 85:
36–41.
84 Vanaudenaerde BM, Meyts I, Vos R, Geudens N, De WW,
Verbeken EK et al. A dichotomy in bronchiolitis obliterans
syndrome after lung transplantation revealed by azithromycin
therapy. Eur Respir J 2008; 32: 832–843.
85 Norman BC, Jacobsohn DA, Williams KM, Au BKC,
Au MA, Lee SJ et al. Fluticasone, azithromycin and
montelukast therapy in reducing corticosteroid exposure in
bronchiolitis obliterans syndrome after allogeneic hematopoie-
tic SCT: a case series of eight patients. Bone Marrow
Transplant 2011; 46: 1369–1373.
86 Kanold J, Merlin E, Halle P, Paillard C, Marabelle A, Rapatel
C et al. Photopheresis in pediatric graft-versus-host disease
after allogeneic marrow transplantation: clinical practice
guidelines based on field experience and review of the
literature. Transfusion 2007; 47: 2276–2289.
87 Ilhan O, Arat M, Arslan O, Ayyildiz E, Sanli H, Beksac M
et al. Extracorporeal photoimmunotherapy for the treatment
of steroid refractory progressive chronic graft-versus-host
disease. Transfus Apher Sci 2004; 30: 185–187.
88 Garban F, Drillat P, Makowski C, Jacob MC, Richard MJ,
Favrot M et al. Extracorporeal chemophototherapy for the
treatment of graft-versus-host disease: hematologic conse-
quences of short-term, intensive courses. Haematologica
2005; 90: 1096–1101.
89 Foss FM, DiVenuti GM, Chin K, Sprague K, Grodman H,
Klein A et al. Prospective study of extracorporeal photopher-
esis in steroid-refractory or steroid-resistant extensive chronic
graft-versus-host disease: analysis of response and survival
incorporating prognostic factors. Bone Marrow Transplant
2005; 35: 1187–1193.
90 Berger M, Pessolano R, Albiani R, Asaftei S, Barat V,
Carraro F et al. Extracorporeal photopheresis for steroid
resistant graft versus host disease in pediatric patients: a pilot
single institution report. J Pediatr Hematol Oncol 2007; 29:
678–687.
91 Bisaccia E, Palangio M, Gonzalez J, Adler KR, Scarborough
R, Goldberg SL et al. Treatment of extensive chronic graft-
versus-host disease with extracorporeal photochemotherapy.
J Clin Apher 2006; 21: 181–187.
92 O’Hagan AR, Stillwell PC, Arroliga A, Koo A. Photopheresis
in the treatment of refractory bronchiolitis obliterans compli-
cating lung transplantation. Chest 1999; 115: 1459–1462.
93 Benden C, Speich R, Hofbauer GF, Irani S, Eich-Wanger C,
Russi EW et al. Extracorporeal photopheresis after lung
transplantation: a 10-year single-center experience. Transplan-
tation 2008; 86: 1625–1627.
94 Morrell MR, Despotis GJ, Lublin DM, Patterson GA,
Trulock EP, Hachem RR. The efficacy of photopheresis for
bronchiolitis obliterans syndrome after lung transplantation. J
Heart Lung Transplant 2010; 29: 424–431.
95 Kharfan-Dabaja MA, Mhaskar AR, Djulbegovic B, Cutler C,
Mohty M, Kumar A. Efficacy of rituximab in the setting of
steroid-refractory chronic graft-versus-host disease: a systema-
tic review and meta-analysis. Biol Blood Marrow Transplant
2009; 15: 1005–1013.
96 Teshima T, Nagafuji K, Henzan H, Miyamura K, Takase K,
Hidaka M et al. Rituximab for the treatment of corticosteroid-
refractory chronic graft-versus-host disease. Int J Hematol
2009; 90: 253–260.
97 Cutler C, Miklos D, Kim HT, Treister N, Woo SB, Bienfang D
et al. Rituximab for steroid-refractory chronic graft-versus-
host disease. Blood 2006; 108: 756–762.
98 von BM, Oelschlagel U, Radke J, Stewart M, Ehninger G,
Bornhauser M et al. Treatment of chronic steroid-refractory
graft-versus-host disease with low-dose rituximab. Transplan-
tation 2008; 86: 875–879.
Bronchiolitis obliterans in clinical practice
HH Uhlving et al
1029
Bone Marrow Transplantation