fertility and sterility
TRANSCRIPT

COVERA model of disease for endometriosis based ondata from both animal and human studies (seepage 1196).
EDITOR’S CORNER1001 What is happening to the price of eggs?
S. N. Covington and W. E. GibbonsSociety for Assisted Reproductive TechnologyIn an anonymous survey of SART clinics, the standardcompensation for ovum donors averaged $4,200.
MODERN TRENDS1005 Pathologic findings and outcomes of a minimally
invasive approach to ovarian remnant syndromeR. M. Kho, J. F. Magrina, and P. M. MagtibayScottsdale, ArizonaA primarily minimally invasive approach (conven-tional laparoscopy and robot-assisted laparoscopy)for surgical management of patients with ovarianremnant syndrome can be safe and effective.
IN VITRO FERTILIZATION1010 Use of phenazopyridine for reducing discomfort
during embryo transferGary N. Frishman, Jenifer E. Allsworth,Jennifer B. Gannon, and Kristen P. WrightProvidence, Rhode IslandPhenazopyridine, a bladder analgesic, was found tobe no better than placebo in decreasing the painassociated with the full bladder required for transab-dominal ultrasound use during embryo transfer.
1015 The presence of pinopodes in the humanendometrium does not delineate the implantationwindowC. Quinn, E. Ryan, E. A. Claessens, E. Greenblatt,P. Hawrylyshyn, B. Cruickshank, T. Hannam,C. Dunk, and R. F. CasperToronto, Ontario, CanadaPinopode formation in the human endometrium wasassessed using scanning electron microscopy. Pi-nopodes were seen from luteinizing hormone day 0through week 11 of pregnancy with no demarcationof an implantation window.
1022 Fertilization, embryo development, and clinicaloutcome of immature oocytes from stimulatedintracytoplasmic sperm injection cyclesY. Shu, J. Gebhardt, J. Watt, J. Lyon, D. Dasig, andB. BehrStanford, CaliforniaAlthough immature oocytes from stimulated cyclescan be normally fertilized, developmental compe-tence of embryos derived from immature oocyteswas significantly reduced.
1028 Risk of monozygotic twinning with blastocysttransfer decreases over time: an 8-yearexperienceS. E. Moayeri, B. Behr, R. B. Lathi, L. M. Westphal,and A. A. MilkiStanford, CaliforniaThe risk of monozygotic twinning from blastocysttransfer diminishes over time and is comparable tothat observed with day 3 embryo transfer.
MAY 2007
VOLUME 87
NUMBER 5
Copyright ©2007 American Society for Reproductive Medicine

1033 Oocyte karyotyping by comparative genomichybrydization provides a highly reliable methodfor selecting “competent” embryos, markedlyimproving in vitro fertilization outcome: amultiphase studyG. Sher, L. Keskintepe, M. Keskintepe, M. Ginsburg,G. Maassarani, T. Yakut, V. Baltaci, D. Kotze, andE. UnsalBursa and Ankara, TurkeyOocyte karyotype (by comparative genomic hy-bridization performed on polar body-1, DNA) is themajor determinant of subsequent embryo compe-tence. Transfer of �2 (1.3 � 0.7) euploid embryosyielded an implantation and ongoing pregnancyrate of 82% and 74%, respectively.
1041 Late stages of embryo progression are a much betterpredictor of clinical pregnancy than early cleavage inintracytoplasmic sperm injection and in vitrofertilization cycles with blastocyst-stage transferK. S. Rehman, O. Bukulmez, M. Langley, B. R. Carr,A. C. Nackley, K. M. Doody, and K. J. DoodyBedford and Dallas, TexasNovel metrics of embryo progression and morphol-ogy during extended embryo culture show that blas-tulation stages of embryo development better predictclinical pregnancy than does measuring early cleav-age in blastocyst-stage transfer cycles.
1053 High incidence of complex chromosomeabnormality in cleavage embryos from patientswith repeated implantation failureL. Voullaire, V. Collins, T. Callaghan, J. McBain,R. Williamson, and L. WiltonParkville and East Melbourne, AustraliaPreimplantation screening using comparativegenomic hybridization shows that the frequency ofaneuploidy for one to two chromosomes increaseswith maternal age, whereas that of complex abnor-mality is independent of maternal age but related toin vitro fertilization history.
MALE FACTOR1059 Stimulation of the nitric oxide/cyclic guanosine
monophosphate signaling pathway elicits humansperm chemotaxis in vitroE. Miraglia, M. L. Rullo, A. Bosia, M. Massobrio,A. Revelli, and D. Ghigo,Torino, ItalyThis study demonstrates that nitric oxide may attracthuman spermatozoa via activation of the solubleguanylate cyclase/cyclic guanosine monophosphate(cGMP) pathway and the subsequent activation ofcGMP-dependent protein kinases.
1064 Sildenafil citrate improves sperm motility butcauses a premature acrosome reaction in vitroD. R. J. Glenn, C. M. McVicar, N. McClure, andS. E. M. LewisBelfast, United KingdomRecreational concentrations of sildenafil citrate en-hance sperm motility and induce acrosome reactionsin vitro.
1071 Tissue perfusion-controlled guided biopsies areessential for the outcome of testicular spermextractionR. Herwig, K. Tosun, A. Schuster, P. Rehder,B. Glodny, L. Wildt, K. Illmensee, andG.-M. PinggeraVienna, Innsbruck, and Feldkirch, AustriaThis is the first demonstration, using a new perfusion-based testicular sperm extraction technique, to showthat sperm quality and quantity depend on tissueperfusion within the testicle.
1077 Frequency of human sperm carrying structuralaberrations of chromosome 1 increases withadvancing ageE. D. Sloter, F. Marchetti, B. Eskenazi,R. H. Weldon, J. Nath, D. Cabreros, andA. J. WyrobekLivermore and Berkeley, California; andMorgantown, West VirginiaAdvancing male age is associated with a gradual andsignificant increase in the frequency of sperm carry-ing breaks and segmental duplications and deletionsof chromosome 1.
1087 Prevalence of sexually transmissible pathogens insemen from asymptomatic male infertility patientswith and without leukocytospermiaG. Bezold, J. A. Politch, N. B. Kiviat, J. M. Kuypers,H. Wolff, and D. J. AndersonBoston, Massachusetts; Seattle, Washington; andMunich, GermanySexually transmissible pathogens were detected in19% of semen samples from infertility patients seek-ing routine semen analyses. Their presence was notassociated with leukocytospermia, but was associ-ated with reduced semen quality.

OVULATION INDUCTION1098 Early pregnancy loss in women stimulated with
gonadotropin-releasing hormone antagonistprotocols according to oral contraceptive pillpretreatmentJ. Bellver, C. Albert, E. Labarta, and A. PellicerValencia, SpainCurrent evidence suggests that oral contraceptivepill pretreatment in gonadotropin-releasing hormoneantagonist cycles should not be considered as a riskfactor for miscarriage.
1102 Ovulatory status and follicular response predictsuccess of clomiphene citrate-intrauterineinseminationS. J. Park, J. R. Alvarez, G. Weiss, S. Von Hagen,D. Smith, and P. G. McGovernNewark, New JerseyClomiphene citrate-intrauterine insemination therapyis a more effective treatment in anovulatory womenthan in ovulatory women. In both groups, pregnancyrates increase with multiple follicular development.
POLYCYSTIC OVARY SYNDROME1108 Polycystic ovary syndrome and risk of uterine
leiomyomataL. A. Wise, J. R. Palmer, E. A. Stewart, andL. RosenbergBoston, MassachusettsIn a prospective cohort study of premenopausal Af-rican-American women, a positive association wasfound between physician-diagnosed polycysticovary syndrome and the risk of uterine leiomyomata.
REPRODUCTIVE ENDOCRINOLOGY1116 The progesterone receptor gene polymorphism,
PROGINS, may be a factor related to thedevelopment of uterine fibroidsM. T. V. Gomes, R. de A. Castro, F. E. Villanova,I. D. C. G. da Silva, E. C. Baracat, G. R. de Lima,and M. J. B. C. GirãoSão Paulo, BrazilWe demonstrated in a case-control study that thePROGINS polymorphism is a proctetive factor for thedevelopment of uterine leiomyomas in Brazilian non-White women.
1122 Ovarian response to the human chorionicgonadotrophin stimulation test in normalovulatory women: the impact of regressing corpusluteumI. Y. Jarvela, M. Niinimaki, H. Martikainen,A. Ruokonen, and J. S. TapanainenOulu, FinlandOvarian stimulation using a human chorionic gona-dotrophin stimulation test reactivates regressing cor-pus luteum from the past menstrual cycle in regularlyovulating women, a finding that should be taken intoaccount when comparing ovulatory and anovulatorywomen.
1131 Ovarian suppression with a gonadotropin-releasing hormone agonist does not alter insulin-stimulated glucose disposalB. C. Cooper, C. K. Sites, P. R. Casson, andM. J. TothBurlington, VermontOvarian hormone suppression with leuprolide ace-tate does not alter insulin-stimulated glucose dis-posal.
REPRODUCTIVE SURGERY1139 Hyaluronic acid fluid agents for the prevention of
adhesions after fertility-preserving gynecologicalsurgery: a meta-analysis of randomized controlledtrialsM. Metwally, D. Gorvy, A. Watson, and T. C. LiJessop Wing, Sheffield, Cheshire, and Lancashire,United KingdomHyaluronic acid has been used in several agents foradhesion prevention. This meta-analysis shows thathyaluronic acid may indeed have the potential to helpdecrease adhesion formation.
REPRODUCTIVE BIOLOGY1147 Effect of atosiban on rabbit embryo development
and human sperm motilityP. Pierzynski, B. Gajda, Z. Smorag,A. D. Rasmussen, and W. Kuczynski,Bialystok and Balice/Krakow, Poland; andCopenhagen, DenmarkAtosiban is compatible with preimplantation rabbitembryo development and human sperm motility inthe range up to 15-fold therapeutic concentrationclinically occurring in human beings.

1153 Apoptosis and ultrastructural assessment aftercryopreservation of whole human ovaries withtheir vascular pedicleB. Martinez-Madrid, A. Camboni, M.-M. Dolmans,A. Van. Langendonckt, and J. DonnezBrussels, Belgium; and Rome, Italy
We studied cryopreservation of intact human ovarieswith their vascular pedicle. After thawing, there wasno sign of induction of apoptosis, and a normal ul-trastructure was observed in primordial and primaryfollicles, and in stromal and vascular cells.
1166 Novel method to characterize primary cultures ofleiomyoma and myometrium with the use ofconfirmatory biomarker gene arraysM. Malik and W. H. CatherinoBethesda, Maryland
We describe a rapid method to confirm that leiomy-oma and myometrium primary cultures maintain themolecular phenotype of the progenitor tissues,based on the biomarker gene array.
1173 Effect of endometrioma cyst fluid exposure onperitoneal adhesion formation in a rabbit modelL. P. Smith, C. D. Williams, J. O. Doyle,W. B. Closshey, W. K. Brix, and L. M. PastoreCharlottesville, VirginiaIn a prospective, randomized, blinded rabbit model,instillation of human endometrioma fluid in the peri-toneal cavity was strongly associated with adhesionformation if followed by copious saline irrigation.
1180 Molecular profiling of experimental endometriosisidentified gene expression patterns in commonwith human diseaseI. Flores, E. Rivera, L. A. Ruiz, O. I. Santiago,M. W. Vernon, and C. B. AppleyardPonce, Puerto Rico; and Morgantown, West VirginiaDeoxyribonucleic acid microarray analysis of exper-imental endometriosis tissues identified gene ex-pression profiles in common with human disease,which support the value of this animal model as atool for testing new therapeutic avenues for endome-triosis.
TECHNIQUES AND INSTRUMENTATION1200 Use of trypan blue staining to assess the quality
of ovarian cryopreservationP. Fauque, A. Ben Amor, C. Joanne, G. Agnani,J. L. Bresson, and C. RouxBesancon, FranceThe viability of follicles in cryopreserved ovarian tis-sue can be verified by a quick test and used routinelyas quality control in ovarian cryopreservationprocedures.
IMAGES IN REPRODUCTIVE MEDICINE1208 Lithopedion: laparoscopic diagnosis and removal
N. Z. Burger, Y. E. Hung, A. N. Kalof, and P. R.CassonBurlington, Vermont; and Manhasset, New YorkA lithopedion is a rare obstetric phenomenon thatcan be successfully diagnosed and treatedlaparoscopically.
1210 In utero incrustation of intrauterine systems—consequent complications and monitoringK. Patai, D. Kiss, L. Devenyi, and R. ZelkoBudapest, HungaryAs a result of physical aging of intrauterine therapeu-tic systems, in utero incrustments form on the intra-uterine system membrane.
CASE REPORT SUMMARIES1212 Successful pregnancy outcome with the use of
in vitro fertilization after Essure® hysteroscopicsterilizationJ. F. Kerin and S. CattanachAdelaide, South Australia, and South Brisbane,Queensland, Australiathe utero-tubal presence of the Essure® microinsertused for hysteroscopic sterilization appears to becompatible with implantation and successful preg-nancy outcomes after in vitro fertilization procedures.
1212 Serum total testosterone levels in a patient withlate onset 21-hydroxylase deficiency and a twingestationL. M. Mains, R. B. Lathi, R. O. Burney, andM. H. DahanNew Orleans, Louisiana; and Stanford, CaliforniaSevere hyperandrogenism may occur in a pregnantwoman with nonclassic 21-hydroxylase deficiencyand twins.

1212 Repeated pregnancies and live births after in vitromaturation treatmentM. Al-Sunaidi, T. Tulandi, H. Holzer, C. Sylvestre,Ri-C. Chian, S. L. TanQuebec, CanadaIn vitro maturation (IVM) treatment can result in re-peated pregnancies and births. In vitro maturation isan effective treatment for some women, especiallythose with a high AFC. It can lead to repetitive suc-cess and may be effective in some women who havefailed IVF treatment. We report 10 singleton and 2twin live births, and 1 ongoing pregnancy as a resultof IVM treatment in six women with polycystic ovarysyndrome.
1212 A new approach to preserve fertility by using acoated nitinol stent in a patient with recurrentcervical stenosisD. Grund, C. Kohler, H. Krauel, and A. SchneiderBerlin and Weissenfels, GermanyA 33-year-old patient with recurrent cervical stenosisand hematometra was treated with a coated nitinolstent. Eight months after insertion, the patient wasstill free of symptoms and had normal menstruation.
1213 Supernumerary minute ring chromosome 14 in aman with primary infertility and left varicoceleB. C. Stahl, S. R. Patil, C. H. Syrop, A. E. T. Sparks,and M. WaldIowa City, IowaWe present a case of a supernumerary minute ringchromosome 14 found in a man during evaluation forprimary infertility and oligospermia. Varicocele repairresulted in improved sperm concentration and motility.
CORRESPONDENCE1214 Heat-shock proteins modulate the incidence of
apoptosis and oxidative stress in preimplantationmouse embryosN. Esfandiari, T. Falcone, J. M. Goldberg,A. Agarwal, and R. K. SharmaCleveland, OhioSupplementation of culture media with antibodies toheat-shock proteins 60 and 70 has a detrimentaleffect on mouse embryo development and increasesthe incidence of apoptosis in blastocysts.
1218 Prolonged duration of transfer does not affectoutcome in cycles with good embryo qualityH. N. Ciray, S. Tosun, O. Hacifazlioglu, A. Mesut,and M. BahceciIstanbul, TurkeyProlonged duration of transfer does not affect out-come in cycles with good embryo quality.
1222 Ureteral suspension facilitates surgery for deeppelvic endometriosisF. Alessandri, D. Lijoi, E. Mistrangelo, S. Ferrero,N. Ragni, and V. RemorgidaGenoa, ItalySuspension of the ureter facilitates its identification,thus preventing injuries during laparoscopic excisionof deep endometriosis.
1225 Simple vaginal mold for use in the postoperativecare of patients with a transverse vaginal septumJ. Lacy, G. R. Correll, D. K. Walmer, and T. M. PriceDurham, North CarolinaWe describe a simple vaginal mold made by an occu-pational therapist for use after resection of a transversevaginal septum. The mold may be individualized forpatients, and is inexpensive and easy to make.
1227 Serum and ovarian Mullerian inhibitingsubstance, and their decline in reproductive agingJ. Yeh, B. Kim, J. Peresie, Y. J. Liang, and A. ArroyoBuffalo, New YorkWith increasing reproductive age in the rat, serumlevels of Mullerian inhibiting substance decline. Thereis evidence to suggest that this reflects a decline inthe number of small ovarian follicles that expressMullerian inhibiting substance.
1231 The levonorgestrel-releasing intrauterine systemand endometriosis stagingM. K. O. Gomes, R. A. Ferriani, J. C. Rosa e Silva,A. C. Japur de Sa Rosa e Silva, C. S. Vieira, andF. J. Cândido dos ReisRibeirão Preto, BrazilTwenty-two patients with laparoscopy-confirmed en-dometriosis were treated for 6 months with a GnRHagonist or with the levonorgestrel-releasing intrauterinesystem. Posttreatment laparoscopies showed thatboth treatments reduced endometriosis severity.

1235 The influence of abdominal ultrasound-guidedembryo transfer on pregnancy rate: a preliminaryreportSu-Chee Chen, Tsung-Hsuan Lai, and Fa-Kung LeeTaipei and Hsin Chu, TaiwanAbdominal ultrasound guidance during fresh embryotransfer does not improve the clinical pregnancy ratebut does enhance physician and patient confidenceand satisfaction.
BOOK REVIEW
1238 Review of Genetic Counselling: A PsychologicalApproach, edited by Christine EvansReviewed by Joann Paley Galst
LETTERS TO THE EDITOR
1240 Metformin and fetal malformationsL. Shahine, R. B. Lathi, and M. H. DahanStanford, California–Reply: G. Koren
1241 Trying to avoid the transmission of humanimmunodeficiency virus particles in spermejaculatesL. Bujan, N. Moinard, M. Daudin, andC. PasquierToulouse, France–Reply: N. Garrido and M. Meseguer
CME Notice to readers: We have recently implementedmore stringent requirements concerning thedisclosure of authors’ potential conflicts of interest.Continuing Medical Education tests will besuspended temporarily while we make thetransition.
CLASSIFIED ANNOUNCEMENTSi Classified Announcements
: Continuing Medical Education Article
: Complete article available online
Visit www.fertstert.org for e-only ande-extra materials
Complete instructions for authors may befound in the June and December issues of thejournal and at the journal’s website,http://www.fertstert.org

OFFICIAL JOURNAL OF THE AMERICAN SOCIETY FORREPRODUCTIVE MEDICINE, Society for Reproductive Endo-crinology and Infertility, Society of Reproductive Surgeons,Society for Assisted Reproductive Technology, Society forMale Reproduction and Urology, and the Pacific Coast Re-productive Society.
Editor-in-ChiefAlan H. DeCherney, M.D.Bethesda, Maryland
Deputy EditorsGautam Chaudhuri, M.D., Ph.D.Los Angeles, CaliforniaRichard J. Paulson, M.D.Los Angeles, California
Associate EditorsPaul G. McDonough, M.D.Augusta, Georgia(Letters-to-the-Editor)Edward E. Wallach, M.D.Lutherville, Maryland(Modern Trends)
Managing EditorEric SteinmehlBirmingham, Alabama
Editorial BoardKurt Barnhart, M.D., M.S.C.E.Philadelphia, Pennsylvania(Society for Reproductive Endocrinology andInfertility)Susan H. Benoff, Ph.D.Manhasset, New YorkRobert G. Brzyski, M.D., Ph.D.San Antonio, TexasJohn E. Buster, M.D.Houston, Texas (Book Review Editor)Charles C. Coddington, M.D.Denver, Colorado
Bryan D. Cowan, M.D.Jackson, Mississippi
Owen K. Davis, M.D.New York, New York(Society for Assisted ReproductiveTechnology)Christopher DeJonge, Ph.D., H.C.L.D.Minneapolis, Minnesota
Esther Eisenberg, M.D.Nashville, Tennessee
Tommaso Falcone, M.D.Cleveland, Ohio
William E. Gibbons, M.D.Baton Rouge, Louisiana
William W. Hurd, M.D.Dayton, Ohio
Keith Isaacson, M.D.Newton, Massachusetts(Society of Reproductive Surgeons)
William H. Kutteh, M.D., Ph.D.Memphis, Tennessee
Stanley P. Leibo, Ph.D.New Orleans, Louisiana
William R. Meyer, M.D.Chapel Hill, North Carolina
Camran Nezhat, M.D.Stanford, California
Steven J. Ory, M.D.Margate, Florida
Nanette Santoro, M.D.Bronx, New York
William D. Schlaff, M.D.Aurora, Colorado
Mark Sigman, M.D.Providence, Rhode Island(Society for Male Reproduction andUrology)
Ronald C. Strickler, M.D.Detroit, Michigan (CME Editor)
Eric S. Surrey, M.D.Englewood, Colorado
Hugh Taylor, M.D.New Haven, Connecticut
International Editorial BoardPaul Devroey, M.D., Ph.D.Brussels, Belgium
David Healy, M.D., Ph.D.Melbourne, Victoria, Australia
Neri Laufer, M.D.Jerusalem, Israel
Guillermo Marconi, M.D.Buenos Aires, Argentina
Francois Olivennes, M.D., Ph.D.Paris, France
Antonio Pellicer, M.D.Valencia, Spain
Basil C. Tarlatzis, M.D., Ph.D.Thessaloniki, Greece
Togas Tulandi, M.D.Montreal, Quebec, Canada
Editorial Advisory BoardChristos Coutifaris, M.D.Philadelphia, Pennsylvania
Marian Damewood, M.D.York, Pennsylvania
Anil Dubey, Ph.D.Washington, D.C.
David Frankfurter, M.D.Washington, D.C.
Suheil Muasher, M.D.Fairfax, Virginia
James Segars, M.D.Bethesda, Maryland
Richard Sherins, M.D.Fairfax, Virginia
Robert Stillman, M.D.Rockville, Maryland
Former EditorsPendleton Tompkins, M.D.Editor 1950–1952
M. Edward Davis, M.D.Editor 1953–1969
Luigi Mastroianni, Jr., M.D.Editor 1970–1975
Roger D. Kempers, M.D.Editor 1976–1997
Fertility and Sterility� (ISSN 0015-0282) is a registered trademark of the American Society of Reproductive Medicine and is published monthly in two indexed volumes by Elsevier Inc., 360 ParkAvenue South, New York, NY 10010-1710. Business Office: 1600 John F. Kennedy Blvd., Philadelphia, PA 19103. Editorial Office: 360 Park Avenue South, New York, NY 10010-1710. Accountingand Circulation Offices: 6277 Sea Harbor Drive, Orlando, FL 32887-4800. Periodicals postage paid at New York, NY and at additional mailing offices. Membership dues to the American Societyfor Reproductive Medicine include $50.00 for Fertility and Sterility�. Subscriptions: Institutional rates: USA $436.00; all other countries US$574.00. Personal rates: USA $256.00; all other countriesUS$367.00. Students: All countries US$118.00. Prices include postage and are subject to change without notice. Any enquiry relating to subscriptions should be sent to: The Americas: ElsevierPeriodicals Customer Service, 6277 Sea Harbor Drive, Orlando, FL 32887-4800. Tel: (800) 654-2452 (U.S. and Canada); (407) 345-4000 (outside U.S. and Canada). Fax: (800) 225-4030 (U.S.and Canada); (407) 363-9661 (outside U.S. and Canada). E-mail: [email protected]. Japan: Elsevier Inc., Customer Support Department, 9-15 Higashi-Azabu 1-chome, Minato-ku, Tokyo106-0044, Japan (Tel: (�81) 3 5561-5033. FAX: (�81) 3 5561-5047. e-mail: [email protected]). Asia Pacific (excluding Japan ): Elsevier Inc. (Singapore) Pte Ltd. No. 1 Temasek Avenue, 17-01Millenia Tower, Singapore 039192. (Tel: (�65) 434-3727. FAX: (�65) 337-2230. e-mail: [email protected]). Latin America: Elsevier Inc., Rua Sete de Setembro 111/16 Andar, 20050-002Centro, Rio de Janeiro - RJ, Brazil. (Tel: (�55) (21) 3970 9300; FAX: (�55) (21) 2507 1991; e-mail: [email protected]). [Note (South America): for orders, claims and help deskinformation, please contact the Regional Sales Office in Florida as listed above]. Rest of World: Elsevier Inc. Customer Service Department, P.O. Box 211, 1001 AE Amsterdam, the Netherlands.(Tel: (�31) 20-485-3757. FAX: (�31) 20-485-3432. e-mail: [email protected]).POSTMASTER: Send address changes to Fertility and Sterility�, Elsevier Periodicals Customer Service, 6277 Sea Harbor Drive, Orlando, FL 32887-4800.

EDITOR’S CORNER
What is happening to the price of eggs?Sharon N. Covington, M.S.W.,a and William E. Gibbons, M.D.,b for the Society for AssistedReproductive Technologya Shady Grove Fertility Reproductive Science Center, Rockville, Maryland; and b Woman’s Center for Reproductive Medicine,
Baton Rouge, Louisiana
Objective: To survey reproductive medical programs that are members of the Society for Assisted ReproductiveTechnology (SART) to ascertain their ovum donor compensation rates.Design: Survey.Setting: Society of Assisted Reproductive Technology member programs.Patient(s): None applicable.Intervention(s): One-page anonymous e-mail survey returned by FAX within 1 week.Main Outcome Measure(s): Clinics were asked if they have a donor oocyte program, and, if yes, their standardcompensation rate. In addition, clinics were asked if there are other variables that increase compensation rates,and, if yes, the maximum compensation. Data were analyzed according to U.S. geographic regions.Result(s): Over half SART clinics (53%, 207 out of 394) responded to the survey, with 191 (92%, 191 out of 207)having a donor oocyte program. The national average for standard donor compensation was $4,217, with a maxi-mum payment average of $4,576. Geographic location affected compensation rates, with highest reported standardmean compensation in the East/Northeast ($5,018) and West regions ($4,890), and lowest in the Northwest($2,900).Conclusion(s): The national average for compensating oocyte donors in reporting SART programs is approxi-mately $4,200. (Fertil Steril� 2007;87:1001–4. �2007 by American Society for Reproductive Medicine.)
Key Words: Donor compensation, oocyte donors, egg donors, Society for Assisted Reproductive Technology,SART
Hardly a week goes by without a newspaper headline or tele-vision story about egg donation and the compensation paid toovum donors: ‘‘Golden Eggs’’ (1), ‘‘Egg Donor BusinessBooms on Campuses’’ (2), or advertisements offering$25,000 to $50,000 to elite donors seem to scream out tothe public about an industry gone awry. The issue of compen-sating donors is clouded further by a worldview whereby pay-ment of gamete donors is prohibited by law in many countriesor is considered culturally/religiously unacceptable in others.The interest and debate extend to Sterility and Fertility, witheditorials on what is ‘‘reasonable compensation’’ (3–7) andresearch on the effect of increasing compensation on ovumdonor recruitment (8). On the Internet, a quick consultationof a search engine for ‘‘egg donation’’ brings up over350,000 hits, with over 100 related to ‘‘egg donor compensa-tion.’’ The majority of these links lead to agencies and pro-grams recruiting donors.
In 2000, the Ethics Committee of American Society of Re-productive Medicine (ASRM) addressed the issue of donorcompensation in the position paper ‘‘Financial Incentives in
Received August 9, 2006; revised and accepted December 13, 2006.
Reprint requests: Sharon N. Covington, M.S.W., Shady Grove Fertility
Reproductive Science Center, 15001 Shady Grove Road, Suite 220,
Rockville, Maryland 20850 (FAX: 301-545-1245; E-mail: sharon.
0015-0282/07/$32.00doi:10.1016/j.fertnstert.2006.12.037 Copyright ª2007 American
Recruitment of Oocyte Donors’’ (9). The Committee stated,‘‘Payments to women providing oocytes should be fair and[yet] not so substantial that they become undue inducementsthat will lead a donor to discount risks’’ (p. 218). They wenton to say, ‘‘Although there is no consensus on the precise pay-ment that oocyte donors should receive, at this time sums of$5,000 or more require justification and sums above $10,000go beyond what is appropriate. Programs recruiting oocytedonors and those assisting couples who have recruited theirown donors should establish a level of compensation thatminimizes the possibility of undue inducement of donorsand the suggestions that payment is for the oocytes them-selves’’ (p. 219). Additionally, the Committee stated that, toavoid commodifying human gametes, compensation shouldnot be based on a donor’s ethnic or personal characteristics.The ASRM Ethics Committee recommendation serves ascompensation guidelines for the Society for Assisted Repro-ductive Technology’s (SART) clinical practices.
In May 2005, the SART Executive Council, with the sup-port of consumer organizations RESOLVE and the AmericanFertility Association (AFA), sent a letter to all independentagencies providing oocyte donation matching services statingthat all outside agencies using SART member clinics are ex-pected to abide by ASRM compensation guidelines for all do-nors they recruit. The agencies were asked to sign voluntarily
Fertility and Sterility� Vol. 87, No. 5, May 2007 1001Society for Reproductive Medicine, Published by Elsevier Inc.

an abidance agreement, notify the SART clinics they workwith, and, in return, have their names posted on the SARTWeb site as following compensation guidelines. (Recently,a revised list of donor agencies agreeing to compensationlimits was posted on the ASRM Web site home page.) Inaddition, this information was forwarded to RESOLVE andAFA to provide information to patient-consumers interestedin locating agencies compliant with the guidelines. In Febru-ary 2006, a follow-up letter was sent to donor agencies statingthat failure to adhere to SART/ASRM guidelines would resultin removal of the agency from the list of approved programs.
The concern regarding overcompensation of donors goesbeyond the general public and the fertility industry becauseit most significantly impacts the most vulnerable popula-tion—infertile patients. The cost of donor payment is un-avoidably passed on to ovum recipients, adding to theiroverall stress: psychosocial, medical, ethical, and financial.Despite the media perception that donor compensation is sky-rocketing, no research exists on what compensation is actu-ally paid to ovum donors. To gain objective data on thisissue, the SART Executive Committee decided to conductan anonymous survey of member clinics to determine thestandard compensation range of ovum donors and the factorsthat may influence compensation amounts.
MATERIALS AND METHODS
A one-page, nonidentifying information questionnaire wase-mailed to all SART clinics in April 2006. The SART Re-search Committee approved the survey, and no patient dataor health information was requested or given. Responseswere check boxes or fill-in-the-blank, with no open-endedquestions.
Clinics were asked if they have a donor recruitment pro-gram; how many yearly donor cycles are performed; wheredonors are recruited from; financial compensation factors(i.e., if all donors are paid the same and if factors such as priordonation, fertility history, or ethnicity effected compensationamount); and the geographic region where the clinic was sit-uated. The clinic’s location was requested to determinewhether compensation was greater in larger, urban areas orEast versus West coast. Locations were divided into six re-gions: East/Northeast, South/Southeast, Midwest, Southwest,Northwest, and West.
The clinics were told that the survey would take less than 5minutes to complete, was confidential, and was conducted toidentify average compensation among member clinics toappropriately respond to media attention on the issue. The sur-vey was e-mailed only once, and clinics were asked to returnit via FAX within 1 week to the SARTadministrator at ASRM.It is interesting that many clinics noted in their responsesthat they were most anxious to hear the results of the survey.
RESULTS
The survey was filled out by 207 of the 394 SART clinic pro-grams, a response rate of 53%. Sixteen responding programs
1002 Covington and Gibbons Donor compensation
(8%; 16 out of 207) said that they did not have an ovum donorprogram; compensation results were tabulated on the remain-ing 191 clinics (92%; 191 out of 207). Separated into regions,the number of clinics replying were East/Northeast, 70clinics; South/Southeast, 19 clinics; Midwest, 56 clinics;Southwest, 25 clinics; Northwest, 6 clinics; and West, 31clinics. Each region had one to two clinics without donor pro-grams, with the exception of the Midwest, which had 10clinics without a program.
Clinics with a donor program were asked about the clinic’srecruitment strategies. Most clinics reported multiple strate-gies, that is, patient families, use of donor agencies, and/ortheir own recruitment programs. Over 94% of the programs(179 out of 191) recruited donors via their patients (i.e., fam-ily members or friends); 75% had a paid anonymous clinicdonor recruitment program (144 out of 191); and 71% useddonors from donor recruitment agencies (136 out of 191).
The SART clinics were asked about their financial com-pensation of donors and their ‘‘standard’’ payment as wellas the ‘‘maximum’’ compensation that may occur under cer-tain circumstances. Over 86% (125 out of 146) stated thatcompensation was the same for all paid donors. In addition,clinics were asked if variables would affect the compensationamount, and they were given the examples of donating a num-ber of times before, prior fertility history, and ethnicity. Themajority of clinics (80%, 117 out of 146) reported that theypay one standard fee to all donors in all situations and donot compensate for other factors.
Concerning the standard compensation of donors, the na-tional average for SART programs was $4,216. Regionally,standard mean payment of donors was highest in the East/Northeast and West, averaging around $5,000, and lowestin the Northwest at $2,900 (Fig. 1). For programs reportinga maximum payment, the national average was $4,576. Thehighest reported maximum payment was $15,000 by oneclinic in the West, and $10,000 for two programs in theEast/Northeast. The lowest payment was $1,500 by one pro-gram each in the East/Northeast and Midwest (Table 1).
FIGURE 1
Mean compensation in dollars for each U.S. region.
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
National East/NE South/SE Midwest SW NW West
Standard Maximum
Covington. Donor compensation. Fertil Steril 2007.
Vol. 87, No. 5, May 2007

TAB
LE1
Co
mp
ari
so
no
fo
oc
yte
do
no
rc
om
pe
nsa
tio
nra
ng
e.
Na
tio
na
lE
ast/
NE
So
uth
/SE
Mid
we
st
So
uth
we
st
No
rth
we
st
We
st
Std
Ma
xS
tdM
ax
Std
Ma
xS
tdM
ax
Std
Ma
xS
tdM
ax
Std
Ma
x
Mean
$4,2
17
$4,5
76
$5,0
18
$5,2
17
$3,6
07
$3,8
21
$3,3
97
$3,6
36
$3,1
56
$3,5
67
$2,9
00
$3,2
00
$4,8
90
$6,0
27
SD
$1,7
18
$2,0
78
$2,0
65
$2,1
83
$1,2
89
$1,3
10
$894
$1,1
94
$926
$1,1
63
$741
$837
$884
$2,7
14
Min
$1,5
00
$8,0
00
$1,5
00
$1,5
00
$2,0
00
$2,0
00
$1,5
00
$1,5
00
$2,0
00
$2,0
00
$2,0
00
$2,0
00
$3,0
00
$3,0
00
Max
$1,5
00
$15,0
00
$8,0
00
$10,0
00
$6,0
00
$6,0
00
$5,0
00
$7,0
00
$5,0
00
$5,5
00
$4,0
00
$4,0
00
$6,0
00
$15,0
00
Covi
ngto
n.
Don
orco
mpe
nsati
on.
Fer
til
Ster
il200
7.
Fertility and Sterility�
DISCUSSION
The SART survey is a beginning step in understanding com-pensation rates for ovum donors. The national standardcompensation rate for donors in over half of SART programswas found to be approximately $4,200, well within ASRM/SART guidelines. Geographic location influenced donorcompensation; payment of donors was highest in the East/Northeast and West, averaging around $5,000.
The vast majority of SART programs have one compensa-tion payment for all donors. However, one in five programsreported that they consider fertility history, prior donation,or ethnicity in the compensation amount. While the EthicsCommittee stated that compensation should not be basedon a donor’s ethnic or personal characteristics, our survey ex-amples grouped ethnicity along with prior donation and fer-tility history, which are not mentioned in the report. Thus,we are not able to determine whether these programs are out-side stated guidelines.
We are aware that there are limitations to the survey. Wedid not include donor egg agencies. As previously stated,we had written donor agencies ‘‘reminding’’ them of theguidelines and ‘‘warning’’ them that we would be eliminatingguideline offenders from the SART list of approved agencies.Because it was felt that this warning letter could adversely af-fect survey responses, we decided that contacting SART pro-grams directly to ask about compensation from all sourceswas more appropriate. While not all SART programs partic-ipated, a response rate of 53% for this type of study is consid-ered reasonable and valid.
This survey provides a better understanding of what clinicsare actually paying oocyte donors. Competition betweenclinics located in the same area (3, 4), costs associated withrecruiting a limited number of potential donors (10), and in-creasing demand for ovum donors (11) all contribute to thecontinuing debate on appropriate, ethical, and reasonablecompensation of oocytes donors. A significant factor in thedebate is the burgeoning, consumer-driven industry of donoregg agencies. Although 66 agencies agreed to abide by SARTcompensation limits (and have a vested interest in doing so bybeing listed on the SART and ASRM Web sites), it is unclearwhether they are in fact doing so. A recent study reviewingfees listed on the Web sites of donor agencies registeredwith SART found similar (but somewhat higher) results asour survey (12). The national average compensation ratesfor ovum donors was approximately $5,200, with only oneagency listing compensation greater than $10,000; paymentwas, as in our survey, highest in the West and lowest in theMidwest.
Currently, there are no standardized mechanisms in placeto assess the appropriate level of compensation for egg dona-tion. In looking at other cost-of-living variables, the regionaldifferences in compensation observed in our survey seem un-derstandable. Many investigators have made justifiable argu-ments for compensation that should be fair, but not excessive,with payments ‘‘reflect[ing] the time, inconvenience, and
1003

physical and emotional demands associated with the pro-cess’’ (9, p. 219). The ASRM Ethics Committee statement re-fers to a 1993 analysis estimating that donors spend 56 hoursin a medical setting during an oocyte donation cycle (13).Comparing this with the average payment to sperm donorsof $60 to $75 in the year 2000, this produced a ‘‘justifiable’’payment of $3,360 to 4,200 at the time the Ethics Committeedocument was published in August 2000. Because there areno current mechanisms to set compensation limits in an objec-tive manner, it may be that this formula is an appropriate stan-dard and could be used periodically to update compensation.
So where do the reports of high dollar payments for donoreggs come from? As in most aspects of American life, objectsperceived as valuable are market driven. One Western agencyreplied to SART’s compliance letter indicating that it couldnot operate within the guidelines and remain competitive inthe marketplace. Still, it is reassuring that in the largest sur-vey regarding donor compensation of clinics in the UnitedStates, involving over half of SART’s membership, the vastmajority of clinics are following ASRM/SART guidelinesand recommendations.
The data from this survey will be evaluated by the SARTQuality Assurance and Practice Committees, which are chargedwith setting and maintaining the standards to which SARTclinics are held. It is hoped that a part of their response overtime will include an ongoing process to assess the parametersthat need to be considered in determining fair compensationfor oocyte donors. In addition to SART and ASRM members,this process also should include the input of all of the share-holders, including donors, patients, clinics, and even donoragencies. Patients (and caregivers) could use the informationfrom this survey to become better consumers as they navigate
1004 Covington and Gibbons Donor compensation
the complicated process of gamete donation, and focus on usingassisted reproduction programs and donor egg agencies thatdemonstrate equitable treatment of both patients and donors.
Acknowledgments: The authors thank Joyce Zeitz, executive administrator of
SART, for her assistance in collecting data for this survey.
REFERENCES1. Hempel C. Golden eggs. Boston Globe, June 25, 2006. Available at: http://
www.boston.com/news/globe/magazine/articles/2006/06/25/golden_eggs/.
Accessed December 2006.
2. Hopkins J. Egg-donor business booms on campuses. USA Today, March
15, 2006. Available at: http://www.usatoday.com/money/industries/
health/2006-03-15-egg-donors-usat_x.htm. Accessed December 2006.
3. Sauer M. Indecent proposal: $5,000 is not ‘‘reasonable compensation’’
for oocyte donors. Fertil Steril 1999;71:7–8.
4. Bergh P. Indecent proposal: $5,000 is not ‘‘reasonable compensation’’ for
oocyte donors—a reply. Fertil Steril 1999;71:9–10.
5. Friedman S. The Debate Continues: Indecent proposal [letter]. Fertil
Steril 1999;72:182.
6. Sauer M. The Debate Continues: Indecent proposal [letter]. Fertil Steril
1999;72:182–3.
7. Bergh P. The Debate Continues: Indecent proposal [letter]. Fertil Steril
1999;72:183.
8. German EK, Mukherjee T, Osborne D, Copperman AB. Does increasing
ovum donor compensation lead to differences in donor characteristics?
Fertil Steril 2001;76:75–9.
9. American Society of Reproductive Medicine Ethics Committee. Finan-
cial incentives in recruitment of oocyte donors. Fertil Steril 2000;74:
216–20.
10. Gorrill MJ, Johnson LK, Patton PE, Burry KA. Oocyte donor screening:
the selection process and cost analysis. Fertil Steril 2001;75:400–4.
11. Barlyn S. Compensating egg donors. Is the money worth it? N J Med
1999;96:33–5.
12. Luk J, Petrozza J. Evaluation of compliance and range of fees by ASRM
listed egg donor and surrogacy agencies. Fertil Steril 2006;86:S190.
13. Seibel MM, Kiessling A. Compensating egg donors: equal pay for equal
time? N Engl J Med 1993;328:737.
Vol. 87, No. 5, May 2007

MODERN TRENDSEdward E. Wallach, M.D.Associate Editor
Pathologic findings and outcomes of a minimallyinvasive approach to ovarian remnant syndromeRosanne M. Kho, M.D., Javier F. Magrina, M.D., and Paul M. Magtibay, M.D.
Department of Obstetrics and Gynecology, Mayo Clinic, Scottsdale, Arizona
Objective: To review outcomes and pathologic findings of a primarily minimally invasive approach to ovarianremnant syndrome.Design: Data were abstracted from medical records documenting bilateral salpingo-oophorectomy and subsequenttreatment between 1996 and 2006 for pathologically confirmed ovarian remnant tissue. Follow-up was by mailedquestionnaires and telephone interviews.Setting: Tertiary care academic medical institution.Patient(s): Twenty patients (mean age, 48 years) receiving treatment for ovarian remnant tissue after prior bilateralsalpingo-oophorectomy.Intervention(s): Primarily minimally invasive approach (conventional laparoscopy and robot-assisted laparos-copy) for removal of ovarian remnant tissue.Main Outcome Measure(s): Postoperative complications and recurrence.Result(s): The 20 patients had a mean follow-up of 30 months. Indications were endometriosis in 8 and ovarianneoplasm in 6. Eighteen patients presented with pain, and 2 presented with a pelvic mass. Nineteen had laparos-copy (14 conventional; 5 robotic), and 1 had laparotomy. Remnant ovarian tissue was associated with endometri-osis in 5 and corpus luteum in 3. Two patients had malignancy in remnant ovarian tissue. Postoperativecomplications included pneumonia (1 case). Follow-up identified no recurrence.Conclusion(s): Ovarian remnant syndrome can be managed safely and successfully with minimally invasive sur-gery. Risk of carcinoma mandates surgical resection. (Fertil Steril� 2007;87:1005–9. �2007 by American Societyfor Reproductive Medicine.)
Key Words: Laparoscopy, malignancy, minimally invasive surgery, ovarian remnant syndrome, surgery, robot-assisted surgery
Ovarian remnant syndrome is defined as the finding of histo-logically confirmed ovarian cortical tissue during surgical ex-ploration in a woman who presents with pain or a pelvic massand who has had a previous bilateral salpingo-oophorectomy.The largest case series published recently involved 186 pa-tients who were all approached by laparotomy (1). Althoughmanagement of ovarian remnant syndrome with laparoscopyhas been described (2, 3), debate about the optimal surgicalroute remains. The dense adhesions usually encounteredwith ovarian remnant syndrome have led to the belief thatlaparotomy is the ideal way to minimize operative complica-tions, dissect the retroperitoneum, and completely exciseovarian remnant tissue (4).
Received July 18, 2006; revised December 11, 2006; accepted December
13, 2006.
Presented as a poster at the annual meeting of the Society of Gynecologic
Surgeons, Tucson, Arizona, April 2006.
Correspondence to: Rosanne M. Kho, M.D., Department of Obstetrics and
Gynecology, Mayo Clinic, 13400 E. Shea Blvd., Scottsdale, AZ 85259
(E-mail: [email protected]).
0015-0282/07/$32.00doi:10.1016/j.fertnstert.2006.12.075 Copyright ª2007 American
Our objective was to review surgical outcomes, includingpathologic findings, of patients with ovarian remnant syn-drome whose condition was managed principally with a min-imally invasive approach.
MATERIALS AND METHODS
A computer-generated search of the institutional medicalrecords database identified all patients who had surgical man-agement for ovarian remnant syndrome between January 1996and January 2006 in the gynecology department of MayoClinic, Scottsdale, Arizona. After approval from the MayoClinic Institutional Review Board, patient records were re-viewed and a follow-up letter was mailed; a follow-up tele-phone call was made, when necessary. Inclusion criteriaincluded a documented history of prior bilateral salpingo-oophorectomy in the course of one or more gynecologic proce-dures and pathologic confirmation of residual ovarian tissueduring surgical exploration and excision at Mayo Clinic.
The surgical approach followed in this series of patientswas initially described by Webb (5) and more recently by
Fertility and Sterility� Vol. 87, No. 5, May 2007 1005Society for Reproductive Medicine, Published by Elsevier Inc.

one of the authors of this study (1). Regardless of the surgicalroute, the same basic surgical principles were followed: [1]high religation and resection of the gonadal vessels, [2] bilat-eral stripping and excision of the pelvic sidewall peritoneum,and [3] wide excision of the tissue surrounding the remnantovary (Figs. 1–3). Since the addition of the da Vinci SurgicalSystem (Intuitive Surgical, Inc., Sunnyvale, CA) to our facil-ity in March 2004, some cases of ovarian remnant syndromehave been approached robotically. Advanced laparoscopicskills were required to accomplish the procedure with con-ventional laparoscopy or the robotic surgical system. The op-erative technique began by careful adhesiolysis of remnanttissue often involving the bowel, omentum, bladder, and ure-ters that was commonly encountered in these patients. Theperitoneum was incised at the pelvic brim to identify the ure-ter, which was mobilized and lateralized through its entirecourse in the pelvis. The gonadal vessels were then religatedat the level of the aortic bifurcation with a vessel-sealing de-vice. The pelvic sidewall peritoneum was stripped and ex-cised to include the tissue surrounding the ovarian remnant.
Follow-up information was obtained from reviewing pa-tient records and responses to questionnaires that were com-pleted and returned. When data were incomplete, the patientwas contacted by telephone or letter to try to obtain the miss-ing information. Postoperative complications were defined asany untoward side effects that occurred within 6 weeks afterthe surgical procedure.
RESULTS
Twenty patients were identified as having ovarian remnantsyndrome (Table 1). The mean age for this cohort was 48years (range, 25–78 years). Of the 20 patients, 11 (55%) un-derwent prior bilateral salpingo-oophorectomy by laparo-
FIGURE 1
Ovarian remnant tissue (arrow) densely adherent topelvic sidewall.
Kho. Ovarian remnant syndrome. Fertil Steril 2007.
1006 Kho et al. Ovarian remnant syndrome
tomy, 7 (35%) by laparoscopy, and 2 (10%) by thetransvaginal approach. The indication for bilateral sal-pingo-oophorectomy was not available in 4 of 20 patients.In the other 16 patients, the most common indication was en-dometriosis (8 patients; 50%) or ovarian neoplasm (6 pa-tients; 38%). Other indications included uterine neoplasm(1 patient) and pelvic inflammatory disease (1 patient). Themean number of previous laparotomies and laparoscopieswas 2.7 (range, 0–11) and 1.4 (range, 0–4), respectively.
FIGURE 2
The peritoneum is opened widely at the pelvic brimto allow high religation and resection of the gonadalvessels (arrow).
Kho. Ovarian remnant syndrome. Fertil Steril 2007.
FIGURE 3
The ureter (arrow) is completely mobilized to allowstripping of the sidewall peritoneum and wideresection of the tissue surrounding the ovarianremnant.
Kho. Ovarian remnant syndrome. Fertil Steril 2007.
Vol. 87, No. 5, May 2007

OR time(min)
LOS(d)
Postoperativepain
185 5 Improved210 4 Resolved225 2 Improved201 2 Resolved
a60 1 Resolved
137 0 Resolved70 0 Resolved75 3 Resolved
127 0 Resolved88 3 NA
150 0 Resolved188 0 NA155 0 Resolved164 0 Improved
260 0 Improved
110 0 Improved137 1 No improvement76 0 Resolved
216 0 Resolved
litis101 4 Resolved
y; NA ¼ not available; OR ¼ operating room;
Fertilityand
Sterility
1007
TABLE 1Characteristics of 20 patients with ovarian remnant syndrome.
BSO
PatientAge(y)
Route(y)
Indication(pathology)
Presentingsymptoms
ORSsurgery
Pathologicfindings
1 47 LPTY (1997) Ov neoplasm Pain LSC Endometriosis2 43 LSC (1995) Ov neoplasm Pain LSC Corpus luteum3 31 LPTY (1993) Ov neoplasm Pain LSC Corpus luteum4 38 LPTY (1999) Ov neoplasm Pain LSC Corpus luteum5 76 VAG (2000) Ov neoplasm,
benign mucinouscystadenoma
Pain LSC Grade 2 ov mucinouscystadenocarcinom
6 45 LSC (2001) NA Pain LSC Ov tissue7 47 LPTY (1996) Ov neoplasm Pain LSC Ov tissue8 65 VAG (1984) NA Pain LSC Ov tissue9 26 LSC (2000) Endometriosis Pain LSC Ov tissue
10 78 LPTY (1952) NA Pelvic mass(19 cm)
LPTY Grade 1 endometrioidadenocarcinoma
11 25 LSC (1995) Endometriosis Pain LSC Ov tissue12 57 LPTY (1982) Endometriosis Pelvic mass Robot Ov tissue13 34 LPTY (1996) PID Pain LSC Endometriosis14 43 LPTY (2003) Endometriosis Pain, ureteral
obstructionLSC Ov tissue
15 68 LSC (1979) Endometriosis Pain, ureteralobstruction
LSC Endometriosis
16 45 LSC (2000) Endometriosis Pain LSC Endometriosis17 29 LSC (2003) Endometriosis Pain Robot Endometriosis18 74 LPTY (1968) NA Pain Robot Ov tissue19 42 LPTY (1996) Endometriosis Pain Robot Ov tissue20 49 LPTY (1994) Uterine neoplasm Pain Robot Ov tissue,
perforated diverticu
Note: BSO ¼ bilateral salpingo-oophorectomy; LOS ¼ length of hospital stay; LPTY ¼ laparotomy; LSC ¼ laparoscopORS ¼ ovarian remnant syndrome; Ov ¼ ovarian; PID ¼ pelvic inflammatory disease; VAG ¼ vaginal.
Kho. Ovarian remnant syndrome. Fertil Steril 2007.
�

No patient in this series had undergone a previous surgicalattempt at resection in ovarian remnant syndrome. One pa-tient was given a GnRH agonist after diagnosis of ovarianremnant syndrome before being seen by us. After presenta-tion, no medical therapy or radiotherapy was attempted. Infour patients, stimulation with clomiphene citrate (100 mgdaily for 10 days) was conducted before imaging and resec-tion. This diagnostic tool was found to help facilitate identi-fication of ovarian remnant syndrome tissue in three of thefour patients.
The most common presenting symptom of ovarian rem-nant syndrome in this cohort of patients was pain (18 patients;90%). In 2 patients, the presenting sign was a pelvic mass.One patient was seen with a large (19 cm) pelvic mass, andanother had a pelvic mass found incidentally during magneticresonance imaging after a hip injury. Only 4 patients under-went preoperative hormonal evaluation. In 3 of these patients,premenopausal levels of FSH (<30 IU/dL) and E2 (>35pg/mL) were recorded.
Ten patients had ultrasonograms that revealed a pelvicmass; computed tomograms in seven patients identifieda mass in six. Magnetic resonance imaging in three patientsidentified a mass in all three. The mean size of the pelvicmass identified by imaging was 3.6 cm (range, 0–19 cm).In the sole patient who presented with complete unilateralureteral obstruction and a 5-cm pelvic mass, a cystoscopyand ureteral stent placement were performed before surgery.No other preoperative procedure (e.g., intravenous pyelo-gram or barium enema) was performed in the other patients.
The patients in this series predominantly had managementby a minimally invasive route: 19 (95%) patients underwentlaparoscopy (14 had conventional laparoscopy and 5 hadrobot-assisted laparoscopy using the robotic surgical system).Only 1 patient who presented with a large 19-cm complexpelvic mass underwent laparotomy.
The mean operating time was 147 minutes (range, 69–260minutes). The mean estimated blood loss was 106 mL (range,20–300 mL). There were no intraoperative complicationsin this cohort of 20 patients. All laparoscopic procedureswere accomplished without conversion. No patient requireda blood transfusion. Postoperative complications consistedof pneumonia in 1 patient, who required hospital readmis-sion. The mean length of hospital stay was 1.25 days (range,0–5 days).
Histologically, ovarian remnant tissue was associated withendometriosis in five patients (25%), one of whom was 68years old, and with a corpus luteum in three patients (15%).Two cases of malignancy were identified. One was a grade2 mucinous cystadenocarcinoma in a 74-year-old womanwho presented with pain and a 4-cm cystic mass identifiedon a computed tomogram. A frozen section resulted in a diag-nosis of an encapsulated borderline mucinous tumor. Twoyears earlier during a bilateral salpingo-oophorectomy, thispatient was found to have a benign mucinous cystadenoma.The other case of malignancy was found in a 78-year-old
1008 Kho et al. Ovarian remnant syndrome
woman with a large 19-cm serous cyst with foci of grade 1endometrioid cystadenocarcinoma. A frozen section revealeda benign serous cyst with no evidence of malignancy. This pa-tient’s original bilateral salpingo-oophorectomy had beenperformed 52 years earlier for an unknown indication. Inboth cases, fluid cytologic test results were found to be neg-ative for malignant cells. Both patients, clinically staged withstage IA disease, received no adjuvant chemotherapy. Bothpatients were alive and had no evidence of disease at 35and 14 months, respectively.
Mean follow-up time was 30 months (range, 1–111months). Follow-up of more than 12 months was recordedfor 11 patients (55%). Follow-up data from clinical recordsand completed questionnaires were available for all patients.All patients reported resolution of pain except for 1 patient,who reported no improvement in pelvic pain a year after heroperation despite negative findings by imaging and examina-tion. This series had no recurrence of ovarian remnantsyndrome.
DISCUSSION
Ovarian remnant syndrome usually results from uninten-tional incomplete dissection and removal of an ovary or ova-ries during a difficult oophorectomy in patients who haveendometriosis or dense pelvic adhesions after multiple previ-ous surgeries. Surgical removal of an ovarian remnant there-fore can be challenging and has a modest intraoperative riskof injury to the bowel, bladder, or ureters (1). In the largestrecent case series of ovarian remnant syndrome, Magtibayet al. (1) reported that all patients whose cases were managedby laparotomy had a minimal (<1%) recurrence rate andclinically significant improvement (>90% resolution) inpain.
The laparoscopy approach to ovarian remnant syndromehas been described as having a good outcome in 13 patients(2). To ensure complete resection of ovarian remnant tissue,we followed the surgical principles originally described byWebb (5) in 1989 and achieved a 95% laparoscopy rate inour series of 20 patients. No inadvertent injuries to the blad-der, bowel, or ureters occurred in this series. At a mean fol-low-up of 30 months, no recurrence of ovarian remnantsyndrome was found and 95% of patients reported improve-ment in or resolution of pain. Because of the high suspicion ofmalignancy (which was confirmed), the open approach wasselected for 1 patient who presented with a large 19- �15-cm complex pelvic mass. Compared with laparotomy,laparoscopy offers the skilled surgeon the advantage of bettervisualization with greater magnification of the retroperito-neal structures. With the recent availability of the robotic sur-gical system, we have found that precise dissection of denselyadherent tissue is facilitated by the articulated tips of the sur-gical instruments and the three-dimensional view of the oper-ative field. More important, a minimally invasive route offersthe patient a shorter stay in the hospital, a faster recovery, anda faster return to normal activity. The mean length of hospitalstay in this cohort was 1.25 days.
Vol. 87, No. 5, May 2007

The use of conservative medical treatment and radiother-apy without histologic diagnosis has been suggested as analternative management approach to minimize operativecomplications often encountered in ovarian remnant syn-drome (4, 6). However, malignancy may be found withinthe ovarian remnant tissue, as was the case in 2 of our 20 pa-tients. In addition to the case of endometrioid adenocarci-noma described in the original report by Shemwell andWeed (6), other reports of malignancies discovered in ovarianremnant tissue have been published in the international med-ical literature (7–11). A case report by Dereska et al. (7) de-scribed 1 patient from our series. Our study supports surgicalexcision with pathologic confirmation as the preferred ap-proach to management of ovarian remnant syndrome. It is im-portant to recognize that unexplored pelvic masses mayrepresent malignant neoplasms, thus forbidding conservativemedical management.
Diagnosis by frozen section has become the standard ap-proach in many surgical practices. Although infrequent, a dis-crepancy between frozen section and permanent pathologicfindings may occur. Frozen-section diagnosis of ovarian tu-mors has an accuracy of about 95%, with better sensitivityand specificity in frankly malignant or benign tumors com-pared with borderline tumors (12, 13). Frozen and permanentpathologic findings have been reported to be consistent forborderline ovarian tumors 60% of the time, with a positivepredictive value of 89% (14).
Tumors other than serous tumors are more likely to beunderdiagnosed. In our series, one patient had a borderlinemucinous tumor on frozen section, and later diagnosis wasmade of a grade 2 mucinous cystadenocarcinoma. A sec-ond patient initially found to have a large benign serouscyst on frozen section was later found to have a lesionwith grade 1 endometrioid cancer. Cognizant of the possi-ble discrepancy between frozen and permanent pathologicfindings, we routinely perform a careful gross survey ofthe entire abdomen and pelvis and collect fluid for cyto-logic examination as part of the surgical management ofpatients with pelvic masses. Subsequent treatment strate-gies (including observation, need for further surgical stag-ing, or adjuvant chemotherapy) may be affected byintraoperative findings.
Although ovarian remnant syndrome is a rare conditionwith a difficult-to-determine incidence, it can occur aftera previous bilateral salpingo-oophorectomy. The cases of
Fertility and Sterility�
most patients with ovarian remnant syndrome are managedby laparotomy, but our experience with a predominantly min-imally invasive approach used the same radicality known toproduce an excellent outcome. Our findings indicate thata minimally invasive approach can be safe and effective aslong as the same surgical principles are applied. Because ofthe small risk of malignancy in ovarian remnant tissue, surgi-cal excision is the preferred approach. The advent of robotictechnology in laparoscopy may further facilitate the preciseand thorough dissection that is required in patients with ovar-ian remnant syndrome.
Acknowledgment: Editing, proofreading, and reference verification were pro-
vided by the Section of Scientific Publications, Mayo Clinic.
REFERENCES1. Magtibay PM, Nyholm JL, Hernandez JL, Podratz KC. Ovarian remnant
syndrome. Am J Obstet Gynecol 2005;193:2062–6.
2. Nezhat F, Nezhat C. Operative laparoscopy for the treatment of ovarian
remnant syndrome. Fertil Steril 1992;57:1003–7.
3. Kamprath S, Possover M, Schneider A. Description of a laparoscopic
technique for treating patients with ovarian remnant syndrome. Fertil
Steril 1997;68:663–7.
4. Lafferty HW, Angioli R, Rudolph J, Penalver MA. Ovarian remnant syn-
drome: experience at Jackson Memorial Hospital, University of Miami,
1985 through 1993. Am J Obstet Gynecol 1996;174:641–5.
5. Webb MJ. Ovarian remnant syndrome. Aust N Z J Obstet Gynaecol
1989;29:433–5.
6. Shemwell RE, Weed JC. Ovarian remnant syndrome. Obstet Gynecol
1970;36:299–303.
7. Dereska NH, Cornella J, Hibner M, Magrina JF. Mucinous adenocarci-
noma in an ovarian remnant. Int J Gynecol Cancer 2004;14:683–6.
8. Fueyo J, Garces JM, Soriano JC, Coll J, Rubies-Prat J. Adenocarcinoma
of the ovary in the ovarian remnant syndrome [Spanish]. Rev Clin Esp
1990;186:415–6.
9. Bruhwiler H, Luscher KP. Ovarian cancer in ovarian remnant syndrome
[German]. Geburtshilfe Frauenheilkd 1991;51:70–1.
10. Elkins TE, Stocker RJ, Key D, McGuire EJ, Roberts JA. Surgery for
ovarian remnant syndrome: lessons learned from difficult cases. J Reprod
Med 1994;39:446–8.
11. Narayansingh G, Cumming G, Parkin D, Miller I. Ovarian cancer devel-
oping in the ovarian remnant syndrome: a case report and literature re-
view. Aust N Z J Obstet Gynaecol 2000;40:221–3.
12. Yeo EL, Yu KM, Poddar NC, Hui PK, Tang LC. The accuracy of intra-
operative frozen section in the diagnosis of ovarian tumors. J Obstet Gy-
naecol Res 1998;24:189–95.
13. Obiakor I, Maiman M, Mittal K, Awobuluyi M, DiMaio T,
Demopoulos R. The accuracy of frozen section in the diagnosis of ovar-
ian neoplasms. Gynecol Oncol 1991;43:61–3.
14. Houck K, Nikrui N, Duska L, Chang Y, Fuller AF, Bell D, et al. Border-
line tumors of the ovary: correlation of frozen and permanent histopath-
ologic diagnosis. Obstet Gynecol 2000;95:839–43.
1009

Ihaa
iu
RP
C
FP
P
P
R
IN VITRO FERTILIZATION
Use of phenazopyridine for reducing discomfort duringembryo transferGary N. Frishman, M.D., Jenifer E. Allsworth, Ph.D., Jennifer B. Gannon, M.D., andKristen P. Wright, M.D.
Department of Obstetrics and Gynecology, Women & Infants’ Hospital, Brown Medical School, Providence, Rhode Island
Objective: The embryo transfer is a critical part of in vitro fertilization. When performed under abdominalultrasound guidance, the embryo transfer procedure requires a full bladder. Patients often state that the discomfortof the distended bladder causes more pain than the actual transfer procedure. Phenazopyridine HCl is a bladderanalgesic. The objective of this study was to determine if a single dose of phenazopyridine prior to embryotransfer reduces patient discomfort during that procedure.Design: Prospective randomized double-blinded clinical trial.Setting: University-based Reproductive Medicine practice.Patient(s): Eighty-five reproductive age infertile women undergoing in vitro fertilization.Intervention(s): Phenazopyridine (200 mg) or placebo taken 1 hour prior to embryo transfer utilizing transab-dominal sonography.Main Outcome Measure(s): Pain as assessed by visual analogue pain scale and physician and nurse assessmentof patient discomfort.Result(s): Study groups were similar in their demographic background. Mean pain score as assessed by a visualanalogue pain scale during the procedure was 2.95 � 2.4 in the placebo group, and 3.03 � 2.6 in the activemedication group (NS). There were also no significant differences in the observations of pain assessments.Conclusion(s): Phenazopyridine used in a single dose prior to embryo transfer does not alleviate patientdiscomfort (Fertil Steril� 2007;87:1010–4. ©2007 by American Society for Reproductive Medicine.)
Key Words: Ultrasound, embryo transfer, pain, phenazopyridine
w(htntchfqnc
bhsstpbps
n vitro fertilization (IVF) is an established technology forelping couples conceive. In 2003, 48,000 babies were borns a result of assisted reproduction technology treatmentsccounting for �1% of all US deliveries (1).
An atraumatic, precisely placed embryo transfer is a crit-cal step in the IVF process. The use of transabdominalltrasound assistance to improve embryo transfer for IVF
eceived April 6, 2006; revised and accepted August 12, 2006.resented at the New England Fertility Society Annual Meeting, Newport,Rhode Island, 2006, and the Pacific Coast Reproductive Society, In-dian Wells, California 2006.ommercial product mentioned in title: Phenazopyridine HCl (Pyridium;Parke Davis, Morris Plains, New Jersey).
inancial support: Noneresent address of Jenifer E. Allsworth: Department of Obstetrics andGynecology, Washington University School of Medicine, St. Louis,Missouri.
resent address of Jennifer B. Gannon: Mount Kisco Medical Group,Northern Westchester Hospital, Mount Kisco, New York.
resent address of Kristen P. Wright: Department of Obstetrics andGynecology, University of Vermont, Burlington, Vermont.
eprint requests: Gary Frishman, M.D., Department of Obstetrics andGynecology, Women & Infants’ Hospital, Brown Medical School, 101Dudley Street, Providence, Rhode Island 02905 (FAX: 401-453-7599,
tE-mail: [email protected]).
1010 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
as first described by Strickler et al. (2) in 1985 and Leong3) in 1986. Its use has been shown in two meta-analysis toelp improve pregnancy rates when compared to the clinicalouch method (4, 5). Independent of any impact on preg-ancy rates, ultrasound’s ability to permit visualization ofhe transfer catheter provides reassurance to both the clini-ian and patient (2, 6, 7). Ultrasound may also be useful toelp map out the position of the uterus, which may changerom the time of the mock transfer (8), decrease the fre-uency of difficult transfers (9), as well as improve preg-ancy rates by facilitating the correct positioning of theatheter within the uterine fundus (10).
The use of the transabdominal ultrasound requires a fullladder to aid visualization. The distended bladder may alsoelp ease the passage of the transfer catheter via its effect ontraightening an anteverted uterus. However, discomfort as-ociated with the ultrasound has been reported in the litera-ure (11), and we find that approximately one third of ouratients complain of significant discomfort from their fullladder, especially with the ultrasound transducer beingressed down on the abdomen. Over half of these womentate that the pain associated with the full bladder is worse
hat any discomfort associated with the embryo transfer0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.097

iwgctha
Ptmehcie
pttwo
wdt
MTaItpkpappprmata
F
tself. Independent of the improved ability to view the uterusith a full bladder noted clinically, consideration could beiven to not filling the bladder. However, a randomized trialomparing a full to an empty bladder in women utilizingransabdominal guidance during embryo transfer revealed aigher likelihood of needing to use a tenaculum, obturator,nd/or sound if the bladder was not filled (11).
Phenazopyridine HCl (Pyridium; Parke Davis, Morrislains, NJ) exerts a topical analgesic effect on the mucosa of
he urinary tract, with its precise mechanism of action re-aining unknown. It is a category B medication, and is
mployed frequently in pregnancy. In addition to its longistory of use for urinary tract infections and interstitialystitis, phenazopyridine is indicated to relieve pain, burn-ng, urgency, or frequency caused by trauma, surgery, andxamination procedures (12–14).
In both speaking to the manufacturer (Park Davis) ofhenazopyridine as well as performing a literature, Web, andextbook search, we were not able to find any data addressinghe use of phenazopyridine during embryo transfer or to helpith the discomfort of a full bladder associated with the usef an abdominal probe ultrasound. The purpose of this study
TABLE 1Patient characteristics by treatment group.
Age (mean � SD) (N � 41, 38)Race/ethnicity (N � 42, 41)
WhiteBlackHispanicAsian/Pacific IslanderNot known/other
BMI (mean � SD) (N � 36, 37)Ever pregnant (N � 41, 38)Any children (N � 41, 37)Painful periods (N�41, 38)Chronic pelvic pain (N � 41, 38)Interstitial cystitis (N � 41, 38)Frequent UTI (N � 41, 38)Usual time between voids (N � 41, 38)
�1 hour1–2 hours2–3 hours3–4 hours�4 hours
Voided after taking study medication (N � 37, 34)Has taken phenazopyridine in the past (N � 41, 38)Believes took phenazopyridine (n � 21, 21)a P value from Fisher’s exact test.
Frishman. Phenazopyridine during embryo transfer. Fertil Steril 2007.
ertility and Sterility�
as to investigate whether administration of phenazopyri-ine prior to ultrasound-guided embryo transfer reduces pa-ient discomfort during that procedure.
ATERIALS AND METHODShis prospective randomized double-blind clinical trial waspproved by the Institutional Review Board at Women &nfants’ Hospital. Exclusion criteria included an unwillingnesso participate in the study, a history of an allergy to phenazo-yridine, a history of G6PD deficiency, or a history of liver oridney disease. A power analysis was performed based on 80%ower and a type I error of .05. For the power calculation, pains assessed by the visual analogue pain scales (VAS) of 10atients undergoing embryo transfer was used. The averageain score, on a scale of 0 to 10, was 3. To reduce this level ofain by 20%, a clinically significant amount, 175 patients wereequired in each arm. The primary study outcome was pain aseasured by the VAS. Secondary outcomes included pain as
ssessed by physician and nurse observers, ease of embryoransfer, bladder volume (measured by amount of urine voided),nd clinical pregnancy rates.
PlaceboN � 42
PhenazopyridineN � 41
Pvalue
34.8 (4.9) 34.5 (5.5) .81
34 (81) 34 (83) .45a
1 (2) 00 1 (2)
4 (10) 1 (2)3 (7) 5 (12)
26.5 (6.5) 26.7 (6.1) .9019 (46) 22 (58) .309 (20) 12 (32) .19
26 (63) 21 (55) .463 (7) 4 (11) .71a
0 1 (2) .48a
1 (2) 0 1.00
1 (2) 4 (11) .17a
9 (22) 12 (32)12 (29) 13 (34)11 (27) 7 (18)8 (20) 2 (5)3 (8) 3 (9) 1.00a
11 (27) 2 (5) .01a
12 (57) 13 (62) .75
1011

RIpsdnapi
obaosafai
imttoabDowetw
otitapc
aaedata
ta
REaagfTbhvpn
Patients undergoing embryo transfer at the Division ofeproductive Endocrinology and Infertility at Women &
nfants’ Hospital, Brown Medical School were invited toarticipate. Entry into the study was prior to the start oftimulation medications with a baseline VAS obtained on theay of the baseline ultrasound monitoring visit. A question-aire was administered to obtain demographic informationnd also included questions about any history of pelvic pain,rior phenazopyridine use, history of frequent urinary tractnfections, and diagnosis of interstitial cystitis.
Patients were randomized to receive either a 200-mg dosef phenazopyridine or placebo. All medication was preparedy the pharmacy at Women & Infants’ Hospital, with bothctive and placebo drugs placed in a common capsule with-ut identifying markings. The capsules were packaged andealed in identical envelopes with the study number. Thectual packet was given to the patient prior to dischargeollowing her egg retrieval. The randomization schedule waschieved through a computer-generated block design utiliz-ng sealed opaque envelopes.
On the day of embryo transfer, participating patients werenstructed to empty their bladder prior to taking the studyedication and to attempt to not void again until after the
ransfer. This was designed to prevent patients from seeinghe color of their urine, as phenazopyridine causes a classicrange color that may alert the patient that she was on thective medication. In performing a literature, Web, and text-ook search, as well as speaking to the manufacturer (Parkeavis), there is no available data concerning the speed ofnset of action of phenazopyridine and peak effectiveness. Itas felt that 1 hour was a reasonable time frame to achieve
fficacy and, as such, the patients were instructed to takeheir medication 1 hour prior to the embryo transfer, whichas scheduled in mid to late morning.
Patients were asked to fill out a VAS prior to the initiationf stimulation medications and on the day of the embryoransfer, both prior to and after the transfer procedure. Dur-ng the assessment recorded after the embryo transfer, pa-ients were asked to rate both their pain after the procedures well as the maximum pain they felt during the transferrocedure. In addition, an assessment of the patient’s dis-
TABLE 2Patient pain scores.
Baseline (mean � SD) (N � 41, 37)Before procedure (mean � SD) (N � 36, 35)During procedure (mean � SD) (N � 37, 34)After procedure (mean � SD) (N � 37, 34)Frishman. Phenazopyridine during embryo transfer. Fertil Steril 2007.
omfort including variables of body movement, moaning,
1012 Frishman et al. Phenazopyridine during embryo transfe
nd table grabbing was independently made by the physiciannd nurse involved in the transfer. Data concerning thembryo transfer such as the ease and duration of the proce-ure, adequate bladder volume for ultrasound visualizationnd speculum size was also collected. Following the embryoransfer, patients were asked to void into a collection devicend the volume of urine was recorded.
For statistical analysis, t tests, chi-square, Fisher exactests, and a general linear regression model were used asppropriate.
ESULTSighty-five patients were recruited. A preliminary datanalysis by an analyst blinded to the study was performedfter 80 patients were recruited. No patients reportedlucose-6-phosphate dehydrogenase deficiency, kidneyailure, active liver disease, or allergy to phenazopyridine.able 1 demonstrates similar demographics including age,ody mass index, ethnicity, parity, history of voidingabits, and pain between patients who took the placeboersus the active medication. There was a difference inrevious exposure to phenazopyridine with an increasedumber of patients in the treatment arm reporting prior
lacebo PhenazopyridineP
value
.41 (0.1) 0.30 (0.2) .56
.61 (2.2) 2.09 (2.6) .41
.95 (2.4) 3.03 (2.6) .89
.73 (2.1) 1.97 (2.2) .64
TABLE 3Physician assessment of patient pain.
Placebo PhenazopyridineP
value
MovementNone 31 27 .48Mild/mod 6 8
MoaningNone 35 30 .25Mild /mod 2 5
Table grabbingNone 35 31 .42Mild/mod 2 4
P
0121
Frishman. Phenazopyridine during embryo transfer. Fertil Steril 2007.
r Vol. 87, No. 5, May 2007

etmbTv(
t(stcadmtwtc
wtfinw1p
c
DTpww
dprisgtseqed
cnepnperpaodpt
ussakabwutawapr
At
R
F
xposure. However, patients were asked on their ques-ionnaire whether they thought they were taking the activeedication, and equal numbers of patients in each group
elieved that they had received the active medication.here was no difference between women who needed tooid prior to their embryo transfer by treatment groupP�1.0).
There was no difference in the self-report by the pa-ients for a history of pelvic pain between treatment armsP�.71). There was no difference in the baseline paincores and pain scores before, during, or after the embryoransfer procedure between women taking either the pla-ebo or active medication (Table 2). This was still truefter adjusting for baseline pain and duration of proce-ure. In addition, both the physician and nursing assess-ent of patient discomfort revealed no differences be-
ween the placebo and active arms (Tables 3 and 4). Thereere no differences in the volume of urine in women
aking the placebo compared to the active medication (448c � 206 cc vs. 448 cc � 221 cc, P�.99).
There was no difference in the physician’s impression ofhether the bladder was adequately full to facilitate the
ransfer procedure (P�.79) or in the level of technical dif-culty (P�.80) between the two treatment groups. Of theine women who voided a volume of 750 cc or more, twoere in the treatment arm. The one woman who voided,000 cc reported her VAS prior, during, and after therocedure as 0; she was in the treatment arm.
There was no difference in intrauterine pregnancy out-ome (33% placebo vs. 39% active medication, P�NS).
ISCUSSIONhis study was designed and powered to evaluate whetherhenazopyridine reduces self-reported pain associatedith embryo transfer. Based on our initial power analysis,
TABLE 4Nursing assessment of patient pain.
Placebo PhenazopyridineP
value
MovementNone 31 27 .48Mild/mod 6 8
MoaningNone 32 29 .67Mild/mod 5 6
Table grabbingNone 33 29 .44Mild/mod 4 6
Frishman. Phenazopyridine during embryo transfer. Fertil Steril 2007.
e computed a conditional power after the first interim
ertility and Sterility�
ata analysis evaluating 42 treatment and 43 placeboatients. From this computation we found that, given theesults for these 85 women, if we continued the trial to ournitially calculated endpoint, we were unlikely to find atatistically significant difference in pain between the tworoups (P�.01). Based on these results, and the trendoward increasing pain in the active medication group, thetudy was terminated. Because this study was terminatedarly, it is possible that our results are because of inade-uate sample size. Fortunately, there is no evidence fromxamination of the randomization that bias was intro-uced through noneffective randomization.
There was a nonstatistically significant trend toward in-reased baseline pain in the placebo group. However, giveno difference in procedure related pain, this further strength-ns our conclusion that phenazopyridine is nonefficacious inreventing pain during embryo transfer. There was also aonstatistically significant trend toward increased priorhenazopyridine exposure in the treatment group. However,qual numbers of patient in each group believed they hadeceived the active medication, demonstrating that both thelacebo and active groups were unaware of their treatmentrm. Thus, it is unlikely that either of these trends influencedur results. With any study assessing pain, it is difficult toifferentiate a possible psychologic component, as well as ahysical one, to a patient’s discomfort, and this may affecthe findings.
Patient discomfort with the use of an abdominal probeltrasound with a full bladder is a real phenomenon forome women (11). This, compounded with the apprehen-ion that may accompany an embryo transfer, can make anlready challenging procedure even more difficult. To ournowledge, there are no reports in the world literaturessessing ways to reduce the pain associated with the fullladder required to perform a transabdominal ultrasoundhen used for any purpose. Given the positive impact ofltrasound guidance on pregnancy rates when comparedo the clinical touch technique (4, 5), discomfort associ-ted with a full bladder will be an ongoing issue for someomen. Our data shows that phenazopyridine does not
lleviate this discomfort. Other interventions such as acu-uncture, biofeedback, or a trial of a different analgesicemain to be studied.
cknowledgements: We gratefully acknowledge the support and participa-ion of the physicians and nurses in the Division of Reproductive Medicine.
EFERENCES1. CDC: http://www.cdc.gov/reproductivehealth/DRH/activites/ART.htm2. Strickler RC, Christianson C, Crane JP, Curato A, Knight AB, Yang V.
Ultrasound guidance for human embryo transfer. Fertil Steril 1985;43:54–61.
3. Leong M, Leung C, Tucker M, Wong C, Chan H. Ultrasound assistedembryo transfer. J In Vitro Fert Embryo Transf 1986;3:383–5.
4. Buckett WM. A meta-analysis of ultrasound-guided versus clinical
touch embryo transfer. Fertil Steril 2003;80:1037–41.1013

1
1
11
5. Sallam HN, Sadek SS. Ultrasound-guided embryo transfer: a meta-analysis of randomized controlled trials. Fertil Steril 2003;80:1042– 6.
6. Hurley VA, Osborn JC, Leoni MA, Leeton J. Ultrasound-guided em-bryo transfer: a controlled trial. Fertil Steril 1991;55:559–62.
7. Al-Shawaf T, Dave R, Harper J, Linehan D, Riley P, Craft I. Transferof embryos into the uterus: how much do technical factors affectpregnancy rates? J Assist Reprod Genet 1993;10:31–6.
8. Henne MB, Milki AA. Uterine position at real embryo transfer com-pared with mock embryo transfer. Hum Reprod 2004;3:570–2.
9. Matorras R, Urquijo E, Mendoza R, Corcóstegui B, Expósito A, Ro-
driguez-Escudero FJ. Ultrasound-guided embryo transfer improves 11014 Frishman et al. Phenazopyridine during embryo transfe
pregnancy rates and increases the frequency of easy transfers. HumReprod 2002;17,1762–6.
0. Frankfurter D, Trimarchi JB, Silva CP, Keefe DL. Middle to lower uterinesegment embryo transfer improves implantation and pregnancy rates com-pared with fundal embryo transfer. Fertil Steril 2004;81:1273–7.
1. Lorusso F, Depalo R, Bettocchi S, Vacca M, Vimercati A, Selvaggi L.Outcome of in vitro fertilization after transabdominal ultrasound-as-sisted embryo transfer with a full or empty bladder. Fertil Steril 2005;84:1046–8.
2. http://www.rxlist.com/cgi/generic3/phenazopyridine_ids.htm3. http://www.nlm.nih.gov/medlineplus/druginfo/medmaster/a682231.html
4. http://www.phenazopyridine.comr Vol. 87, No. 5, May 2007

Bnotrbff
temw(awc
sl
RTR
0d
The presence of pinopodes in the human endometriumdoes not delineate the implantation windowClaire Quinn, M.Sc.,a Edward Ryan, M.D.,b E. Anne Claessens, M.D.,b Ellen Greenblatt, M.D.,c
Peter Hawrylyshyn, M.D.,d Barbara Cruickshank, M.D.,c Thomas Hannam, M.D.,d
Caroline Dunk, Ph.D.,a and Robert F Casper, M.D.a,b
a Division of Reproductive Sciences, Samuel Lunenfeld Research Institute, and the Fran and Lawrence Bloomberg Departmentof Obstetrics and Gynecology, Mount Sinai Hospital, Institute of Medical Sciences, University of Toronto; b Toronto Center forAdvanced Reproductive Medicine (TCART); c Mount Sinai Hospital Fertility Center; and d LifeQuest Center for ReproductiveMedicine, Toronto, Ontario, Canada
Objective: To assess pinopode formation in human endometrium during the luteal phase of the menstrual cycleand in the first trimester of pregnancy.Design: Prospective clinical study.Setting: Outpatient infertility clinics and outpatient family planning clinic.Patient(s): Thirty-two regularly cycling infertile women, 15 regularly cycling fertile women, 9 women receivingelective termination of pregnancy, and 1 woman receiving GnRH agonist and hormone therapy addback.Intervention(s): Endometrial tissue was collected by suction pipelle and examined by scanning electron micros-copy for pinopode formation.Main Outcome Measure(s): Endometrial tissue was scored (0, 1, 2, 3, or 4) depending on the percentage of thesurface covered in pinopodes (from 0% to �20% of 100 fields).Result(s): Pinopodes were present throughout the luteal phase of the menstrual cycle, up to the 11th week ofpregnancy, and in the endometrium of the woman on GnRH agonist and hormone therapy.Conclusion(s): Pinopodes can be detected in the progesterone-exposed endometrium for an extended per-iod of time, in contradistinction to the perception that they are markers for the implantation window inthe human endometrium. (Fertil Steril� 2007;87:1015–21. ©2007 by American Society for ReproductiveMedicine.)
Key Words: Endometrium, pinopode, pregnancy, human, implantation window, scanning electron microscopy
�etraddottma
tfwetffieda
oth the embryo and endometrium must reach a synchro-ized stage of maturation for successful implantation toccur (1). Endometrial maturation is maternally regulated byhe ovarian steroids estradiol (E2) and progesterone (P4), andenders the uterus transiently receptive to implanting em-ryos (2, 3). A marker of uterine receptivity would, there-ore, be of great clinical value to determine the ideal datesor frozen and donor embryo transfers.
Endometrial morphology (histology and scanning elec-ron microscopy [SEM]) is often used to date and assessndometrial maturation (4, 5). One specific morphologicarker that has been proposed to be associated with theindow of implantation is the appearance of pinopodes
3, 6 –12). Pinopodes can be detected by SEM in rodentsnd humans around the time that embryo implantationould be expected to occur, and appear as smooth bulging
ells on the apical surface of the endometrium (Fig. 1).
Previous studies suggested that mature pinopodes areeen only during a brief window following the midcycleuteinizing hormone (LH) surge (�48 hours between LH
eceived April 8, 2006; revised and accepted August 9, 2006.his work was supported by the CIHR grant #HGG-62292.eprint requests: R.F. Casper, 150 Bloor St W, Suite 210, Toronto,
eOntario, Canada (FAX: 416-972-0036; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.08.101 Copyright ©2007 American Soc
6 and LH � 8) and are indicative of a receptivendometrium (5, 8, 13, 14). Based on data from endome-rial biopsies during a previous cycle, Nikas et al. (13, 14)ecommended that frozen embryo transfer dates can bedjusted (forward or backward a day or 2) to accommo-ate for each women’s specific day of receptivity asetermined by SEM detection of pinopodes. In contrast,ther groups have shown that pinopode formation lastshroughout the luteal phase with no obvious “window” ofime when they are preferentially expressed (15, 16),aking the clinical value of pinopode formation question-
ble (17–21).
To determine if SEM could be used in a clinical settingo detect endometrial receptivity in a diverse group ofertile and infertile women, we conducted a study inhich subjects were asked to have from one to three
ndometrial biopsies performed during the luteal phase ofhe menstrual cycle. Biopsies were assessed for pinopodeormation by SEM. In view of the contradictory findingsound by Acosta et al. (15) and Usadi et al. (16) suggest-ng the absence of a pinopode window, we also obtainedndometrial and decidual tissue from a woman receivingepot GnRH agonist and chronic addback hormonal ther-py (HT), and from nine women undergoing first trimester
lective termination of pregnancy.1015Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

MPEppwivnostccCItS
tnlaafo0
CPbu
pc
SSptcsSm
PEae3icctacbb
SSre
ATERIALS AND METHODSarticipantsndometrial biopsies were collected throughout the lutealhase of the menstrual cycle from 47 normally cyclingatients between 26 and 42 years old. Thirty-two patientsere attending an outpatient infertility clinic with a min-
mum 2-year history of infertility, and 15 were healthyolunteers with a history of at least one clinical preg-ancy. Physicians were asked to collect endometrial bi-psies between LH day 0 and LH day 13 to determine ifignificant changes in pinopode scores occur across thisime span. One patient was on depot GnRH agonist andhronic addback HT. All endometrial biopsies wereollected using a suction pipelle (Milex Product Inc.,hicago, IL) followed by fixation in gluteraldehyde.
nformed consent was obtained from all patients. (Insti-utional review board approval was obtained from Mountinai Hospital: MSH REB #04-0151-E.)
In addition, decidua parietalis was dissected out fromotal tissue extracted during elective first trimester termi-ation of pregnancy from nine patients. Tissue was col-ected into ice-cold phosphate-buffered saline prior tossessment of apical epithelial integrity followed by fix-tion in gluteraldehyde. Informed consent was obtainedrom all patients. (Institutional review board approval wasbtained from Mount Sinai Hospital: MSH REB #04-018-U.)
ycle Monitoringatients were monitored daily starting on day 10 of the cycley either daily morning blood sampling or daily morning
FIGURE 1
SEM picture of the apical surface of the human endoindividual cells. (A) Absence of pinopodes. Microvilliof individual cells. (B) Three pinopodes with smooth(B) � 5 �m.
Quinn. Pinopodes in the human endometrium. Fertil Steril 2007.
rine analysis (Clearblue fertility monitor) depending on (
1016 Quinn et al. Pinopodes in the human endometrium
atient and physician preference. Day of the LH surge wasonsidered LH day 0.
canning Electron Microscopyamples were fixed in 2% glutaraldehyde in 0.1 M phos-hate buffer, rinsed in buffer, postfixed in 1% osmiumetroxide in buffer, dehydrated in a graded ethanol series,ritical point dried, and sputter coated with gold. Theamples were then examined using a FEI XL30 (FEIystems Canada Inc., Toronto, Canada) scanning electronicroscope.
inopode Scoringndometrial tissue was examined under the SEM andssigned a score. One hundred randomly selected fields ofndometrial epithelium were examined per sample at,500� magnification. Scores ranged from 0 to 4 depend-ng on the percentage of the endometrial surface that wasovered in pinopodes: score 0 (0% of the apical surfaceovered in pinopodes), score 1 (1% to �5%), score 2 (5%o �10%), score 3 (10% to 20%), score 4 (�20%). Theverage score from all 100 fields was rounded to thelosest whole number to assign a final score to eachiopsy. The same observer scored all biopsies and waslinded to the day of the cycle.
tatistical Analysiscores in fertile and infertile patients were analyzed usingegression modeling with day of the menstrual cycle mod-led as a fixed effect. SAS statistical software version 9.1
rium. Borders (valleys) can be seen aroundcilia can be seen extending from the surfaceces can be seen. Scale bars: (A) � 5 �m,
metandsurfa
Statistical Analysis Systems Institute Inc., Cary, NC, 1999)
Vol. 87, No. 5, May 2007

wed(
RPMPsfo(sis
PiPsfb(�dp(d�sp(
F
as used for data analysis and P values �.05 were consid-red statistically significant. Scores were not significantlyifferent between patients on different days in both fertileP�.1067) and infertile (P�.8553) patients.
ESULTSresence of Pinopodes During the Luteal Phase of theenstrual Cycle in Infertile Patientsinopodes were present from LH � 4 to LH � 13 withcores ranging from 0 to 4. Of the 42 biopsies (collectedrom 32 patients), scores were as follows; score � 0 (9 bi-psies [21.4%]), score � 1 (6 biopsies [14.3%]), score � 217 biopsies [40.5%]), score � 3 (6 biopsies [14.3%]),core � 4 (4 biopsies [9.5%]). Pinopode scores, and selectedmages of pinopodes, on various days of the luteal phase arehown in Figure 2.
FIGURE 2
Day of the menstrual cycle (LH days seen in boxes u(A) Each green bar in the graph represents a patientrepresent patients that gave �2 biopsies during onethem (three bars/three different patients) represent pasubsequent cycle. (B) SEM pictures of pinopodes froScale bars, upper row � 20 �m, lower row � 5 �m.
Quinn. Pinopodes in the human endometrium. Fertil Steril 2007.
ertility and Sterility�
resence of Pinopodes During the Luteal Phasen Fertile Patientsinopodes were present from LH day 0 to LH � 13 withcores ranging from 0 to 4. Of the 17 biopsies (collectedrom 15 patients), scores were as follows; score � 0 (6iopsies [5.3%]) score � 1 (2 biopsies [11.7%]), score � 23 biopsies [17.8%]), score � 3 (2 biopsies [11.7%]), score
4 (4 biopsies [23.5%]) (Fig. 3A). One biopsy taken on LHay 0 (as determined by blood tests and pathology) wasositive for pinopodes. The patient was a 26-year-oldG1P1) (patient #46), and results of blood tests done on theay of the biopsy showed LH � 44 IU/L, E2 � 797 pmol/L, P4
2 nmol/L. A portion of the biopsy sent for histologic datinghowed “mid proliferative, no luteal development yet.” Pino-ode score was 3, and full fields of pinopodes could be seenFig. 3B). Patient #48 scored zero on all three biopsies taken in
r graph) verses pinopode score in infertile patients.gave only one biopsy. Other colored bars
le (one color/patient). Bars with a square abovets who went on to become pregnant in aatients on LH � 4, LH � 8, LH � 11, and LH � 12.
ndethatcyctien
m p
1017

op
PAOpmpCiMcma
PTEl
fw
DIotd�f(2(b(a�a
ne cycle (LH � 4, LH � 7, and LH � 11) and becameregnant the subsequent cycle. Her pregnancy is ongoing.
resence of Pinopodes in a Patient on Depot GnRHgonist Plus HT Addbackne patient (separate from the infertile, fertile, and pregnantatients) agreed to endometrial biopsy while receiving treat-ent for endometriosis. GnRH agonist (Lupron depot [leu-
rolide acetate] 3.75 mg, Abbott Pharmaceutical, Montreal,anada) monthly, was administered together with micron-
zed 17�-estradiol 1 mg (Estrace, Roberts Pharmaceutical,ississauga, Canada) and norethinedrone 0.35 mg (Mi-
ronor, Janssen-Ortho, Toronto, Canada) add back. Endo-etrial biopsy was performed after 24 days of continuous
ddback treatment. Pinopode score was 2 (Fig. 4).
resence of Pinopodes in Endometrial Tissue from Firstrimester Elective Termination of Pregnancyndometrial tissue was dissected out from total tissue col-
FIGURE 3
Day of the menstrual cycle verses pinopode score ingraph indicate specific patients. (B) Pinopodes in anpatient (patient #46). Scale bars (i) � 20 �m, (ii) � 10
Quinn. Pinopodes in the human endometrium. Fertil Steril 2007.
ected following elective termination of pregnancy per- i
1018 Quinn et al. Pinopodes in the human endometrium
ormed between weeks 5 and 11 of gestation. Pinopodesere present up to week 11 of gestation (Fig. 5).
ISCUSSIONn support of our data, other groups have found the presencef well-formed pinopodes from day 20 through to day 28 ofhe menstrual cycle with no apparent rise in their appearanceuring the predicted window of receptivity (�LH � 6 to LH
8) (15, 16). Some investigators have shown that smallorming pinopodes appear as early as day 15 of the cycle�LH � 1), with well-formed pinopodes developing on day0 (�LH � 6) and remaining through to day 28 (�LH � 14)15). In fact, for some patients the presence of pinopodes cane seen in two separate biopsies taken a full 7 days apart15). In addition, Usadi et al. (16) looked at fertile womennd found that pinopodes were consistently present from LH
5 through to LH � 14 with no apparent rise in scoresround the expected window of receptivity.
Our results showed that pinopodes in both fertile and
ularly cycling fertile patients. (A) Numbers in barometrial sample taken on LH day 0 from a fertile.
regend�m
nfertile patients covered between 1% and 50% of the sur-
Vol. 87, No. 5, May 2007

fmsradeic
eescmciu�ash
tfemron3d(cqc
fwboaitmTu
pnibgam
aagdpfos
b(dp
F
ace area viewed. Never was the entire surface of the endo-etrium covered in pinopodes with most of the samples
howing between 5% and 20% coverage. Novotny et al. (22)eported that endometrial biopsies taken between �LH � 2nd LH � 7 were between 2% and 17% covered in pinopo-es, which is in agreement with our findings. This means thatven when the endometrium was assigned a high score (i.e., 3)n the present study, up to �85% of the endometrium was notovered in pinopodes.
Other groups have scored pinopodes as: few (�20% of thendometrial surface covered), moderate (20%–50% cov-red), and abundant (�50% covered) (8). With further clas-ification as developing (bulging cells still covered in mi-rovilli), developed (bulging cells no longer covered inicrovilli), or regressing (bulging cells covered in mi-
rovilli) (13), we found designating pinopodes as “develop-ng” or “regressing” difficult, as the surface of each individ-al biopsy was highly diverse, often with a mix of small (�2m pinopode like structures), medium (�2 �m to 12 �m),nd large (�12 �m) pinopodes that were in varying states ofmooth, wrinkled, fuzzy, or covered in microvilli, making itard to decide which fields to score and how.
Another interesting finding by Ordi et al. (19) showedhat there is a great deal of variability in pinopode scorerom cycle to cycle in the same patient. For this studyach patient gave one biopsy a month for 3 consecutiveonths between postovulatory days 6 and 8. Patients
eceived a score of 0, 1, 2, or 3, depending on the numberf pinopodes present. One patient in particular (patientumber 5) scored zero, one, and three for cycles 1, 2, and, respectively, with all three biopsies being dated asay 7 after ovulation by both histology and ultrasound19). They concluded that pinopode scores from oneycle cannot be reliably used to predict scores in a subse-uent cycle because of poor within-subject between-cycle
FIGURE 4
Pinopodes detected in a patient administered depotestradiol and norethindrone addback. Scale bars: (A)
Quinn. Pinopodes in the human endometrium. Fertil Steril 2007.
onsistency. (
ertility and Sterility�
Contradictions in scoring and the percentage of the sur-ace area covered in pinopodes as well as comparisons ofithin-subject between-cycle score discrepancies may beecause of many problems. First, we found that the surfacef the endometrium is highly diverse, making it hard tossign an appropriate overall score. Most biopsy procedures,ncluding ours, are performed blind using suction pipelle andhe piece or pieces of endometrium examined under theicroscope are often between 1 mm and 3 mm in diameter.hus, the surface area is small and its origin within the uterusnknown.
Another noteworthy finding in the current study was theresence of pinopodes during the first trimester of preg-ancy. Many studies have suggested that pinopode formations progesterone dependent (7, 23–25). It is, therefore, possi-le that pinopodes are a reflection of raised maternal pro-esterone levels and persist as long as progesterone levelsre elevated (i.e., until the end of the luteal phase of theenstrual cycle or into pregnancy).
The presence of pinopodes following depot leuprolidecetate treatment and after 24 days of micronized estradiolnd norethindrone addback may also be a reflection of pro-esterone exposure. To account for the expression of pinopo-es throughout the luteal phase and into the first trimester ofregnancy, it may be possible that they form in wavesollowing exposure to progesterone. In this way, one groupf pinopodes may be regressing while a neighboring group istarting to develop.
Also of interest is the finding that most of the womeneing treated for infertility scored positive for pinopodes6, 19, 20, 26). In one study, 15 women with a meanuration of 4.6 years of infertility scored positive for theresence of pinopodes in at least one of three biopsies
rolide acetate followed by 24 days of micronized0 �m, (B) � 5 �m.
leup� 1
one biopsy per month for 3 months between postovula-
1019

ti
tsis
ohhacmpa
tpc
pm
Aaw
R
ory days 6 and 8) (19), and 9 were positive for pinopodesn all three cycles.
Although many groups have studied pinopodes, their ac-ual function in the endometrium is unknown. It has beenuggested that blastocysts attach to pinopodes during thenitial processes of implantation, but this has never beenhown in vivo.
Preliminary studies, done in vitro, revealed that three outf three blastocysts attached to pinopode presenting areas ofuman endometrial cells in culture (27). Subsequent studiesave been less convincing where 11 blastocysts were visu-lized following attachment to human endometrial cells inulture. SEM pictures were taken of 10 out of the 11 attach-ent sites and showed that only 1 of the 10 sites had
ronounced pinopode formation (�50%) and 2 of the 10ttachment sites had no pinopode formation at all (25).
In summary, our data demonstrate that pinopodes are seenhroughout the luteal phase and at least up to week 11 ofregnancy. In addition, four patients in our study that be-
FIGURE 5
Pinopodes detected in endometrial tissue dissectedperformed between weeks 5 and 11 of gestation. (A)endometrial tissue collected from week 7 of gestation
Quinn. Pinopodes in the human endometrium. Fertil Steril 2007.
ame pregnant all scored 0 for pinopode formation in a
1020 Quinn et al. Pinopodes in the human endometrium
revious cycle. We conclude that using pinopodes as aethod of scoring endometrial “receptivity” is not useful.
cknowledgments: The authors thank Doug Holmyard for his technicalssistance with scanning electron microscopy and Brian Knight for helpith statistical analysis.
EFERENCES1. Psychoyos A. Hormonal control of ovoimplantation. Vitam Horm
1973;31:201–56.2. Psychoyos A. Hormonal control of uterine receptivity for nidation.
J Reprod Fertil Suppl 1976:17–28.3. Sharkey AM, Smith SK. The endometrium as a cause of implantation
failure. Best Pract Res Clin Obstet Gynaecol 2003;17:289–307.4. Noyes RW, Hertig AT, Rock J. Dating the endometrial biopsy. Am J
Obstet Gynecol 1975;122:262–3.5. Nikas G. Endometrial receptivity: changes in cell-surface morphology.
Semin Reprod Med 2000;18:229–35.6. Cortinez A, De Carvalho I, Vantman D, Gabler F, Iniguez G, Vega M.
Hormonal profile and endometrial morphology in letrozole-controlledovarian hyperstimulation in ovulatory infertile patients. Fertil Steril2005;83:110–5.
7. Nikas G, Drakakis P, Loutradis D, Mara-Skoufari C, Koumantakis E,
following elective termination of pregnancygraph of pinopode scores. (B) SEM pictures of
cale bars: (i) � 20 �m, (ii) � 10 �m.
outBar. S
Michalas S, et al. Uterine pinopodes as markers of the “nidation
Vol. 87, No. 5, May 2007

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
F
window” in cycling women receiving exogenous oestradiol andprogesterone. Hum Reprod 1995;10:1208–13.
8. Nikas G, Develioglu OH, Toner JP, Jones HW Jr. Endometrial pinopo-des indicate a shift in the window of receptivity in IVF cycles. HumReprod 1999;14:787–92.
9. Nikas G. Pinopodes as markers of endometrial receptivity in clinicalpractice. Hum Reprod 1999;14(Suppl 2):99–106.
0. Develioglu OH, Hsiu JG, Nikas G, Toner JP, Oehninger S, Jones HWJr. Endometrial estrogen and progesterone receptor and pinopode ex-pression in stimulated cycles of oocyte donors. Fertil Steril 1999;71:1040–7.
1. Martel D, Frydman R, Glissant M, Maggioni C, Roche D, Psychoyos A.Scanning electron microscopy of postovulatory human endometrium inspontaneous cycles and cycles stimulated by hormone treatment.J Endocrinol 1987;114:319–24.
2. Pantos K, Nikas G, Makrakis E, Stavrou D, Karantzis P, Grammatis M.Clinical value of endometrial pinopodes detection in artificial donationcycles. Reprod Biomed Online 2004;9:86–90.
3. Nikas G, Makrigiannakis A, Hovatta O, Jones HW Jr. Surface mor-phology of the human endometrium. Basic and clinical aspects. Ann NY Acad Sci 2000;900:316–24.
4. Aghajanova L, Stavreus-Evers A, Nikas Y, Hovatta O, Landgren BM.Coexpression of pinopodes and leukemia inhibitory factor, as well as itsreceptor, in human endometrium. Fertil Steril 2003;79 Suppl 1:808–814.
5. Acosta AA, Elberger L, Borghi M, Calamera JC, Chemes H, DoncelGF, et al. Endometrial dating and determination of the window ofimplantation in healthy fertile women. Fertil Steril 2000;73:788–98.
6. Usadi RS, Murray MJ, Bagnell RC, Fritz MA, Kowalik AI, Meyer WR,et al. Temporal and morphologic characteristics of pinopod expressionacross the secretory phase of the endometrial cycle in normally cyclingwomen with proven fertility. Fertil Steril 2003;79:970–4.
7. Oborna I, Novotny R, Brezinova J, Petrova P, Lichnovsky V, FingerovaH. Changes in the development of uterine pinopodes in steroid hormone
supplemented cycles. Physiol Res 2004;53:423–9.ertility and Sterility�
8. Creus M, Ordi J, Fabregues F, Casamitjana R, Carmona F, Cardesa A,et al. The effect of different hormone therapies on integrin expressionand pinopode formation in the human endometrium: a controlled study.Hum Reprod 2003;18:683–93.
9. Ordi J, Creus M, Quinto L, Casamitjana R, Cardesa A, Balasch J.Within-subject between-cycle variability of histological dating, alpha vbeta 3 integrin expression, and pinopod formation in the human endo-metrium. J Clin Endocrinol Metab 2003;88:2119–25.
0. Ordi J, Creus M, Casamitjana R, Cardesa A, Vanrell JA, Balasch J.Endometrial pinopode and alphavbeta3 integrin expression is not im-paired in infertile patients with endometriosis. J Assist Reprod Genet2003;20:465–73.
1. Creus M, Ordi J, Fabregues F, Casamitjana R, Ferrer B, Coll E, et al.alphavbeta3 integrin expression and pinopod formation in normal andout-of-phase endometria of fertile and infertile women. Hum Reprod2002;17:2279–86.
2. Novotny R, Malinsky J, Oborna I, Dostal J. Ultrastructure of endome-trial surface relief in normal menstrual cycle and after hormonal stim-ulation. Acta Univ Palacki Olomuc Fac Med 1999;142:47–55.
3. Stavreus-Evers A, Nikas G, Sahlin L, Eriksson H, Landgren BM.Formation of pinopodes in human endometrium is associated with theconcentrations of progesterone and progesterone receptors. Fertil Steril2001;76:782–91.
4. Martel D, Monier MN, Roche D, Psychoyos A. Hormonal dependenceof pinopode formation at the uterine luminal surface. Hum Reprod1991;6:597–603.
5. Petersen A, Bentin-Ley U, Ravn V, Qvortrup K, Sorensen S, Islin H, et al.The antiprogesterone Org 31710 inhibits human blastocyst-endometrialinteractions in vitro. Fertil Steril 2005;83(Suppl 1):1255–63.
6. Garcia-Velasco JA, Nikas G, Remohi J, Pellicer A, Simon C. Endo-metrial receptivity in terms of pinopode expression is not impaired inwomen with endometriosis in artificially prepared cycles. Fertil Steril2001;75:1231–3.
7. Bentin-Ley U, Sjogren A, Nilsson L, Hamberger L, Larsen JF, Horn T.Presence of uterine pinopodes at the embryo–endometrial interface
during human implantation in vitro. Hum Reprod 1999;14:515–20.1021

A(rwsctsebc
RP
R
Fertilization, embryo development, and clinicaloutcome of immature oocytes from stimulatedintracytoplasmic sperm injection cyclesYimin Shu, M.D., Ph.D., Janice Gebhardt, B.S., Jill Watt, Ph.D., Jennifer Lyon, M.S.,Danny Dasig, M.S., and Barry Behr, Ph.D.
In Vitro Fertilization Program, Division of Reproductive Endocrinology and Infertility, Department of Obstetrics andGynecology, Stanford University Medical Center, Stanford, California
Objective: To evaluate the fertilization and developmental potential of immature oocytes obtained from controlledovarian hyperstimulated cycles of patients undergoing intracytoplasmic sperm injection (ICSI).Design: Retrospective study.Setting: Academic assisted reproductive technology program.Patient(s): Two hundred patients with at least one mature oocyte and one immature oocyte (study 1), and 44patients with no mature oocytes (study 2) at time of oocyte denudation.Intervention(s): Oocyte denudation was performed immediately after retrieval. Oocytes were cultured in vitro for4–6 hours before ICSI and then categorized into four groups: group I, metaphase II (MII) oocytes at denudation;group II, in vitro matured MII oocytes; group III, metaphase I (MI) oocytes that did not progress to MII; andgroup 4, germinal-vesicle (GV) oocytes that converted to MI.Main Outcome Measure(s): Fertilization and embryo development were compared among groups in study 1.Pregnancy and implantation rates were evaluated in study 2.Result(s): Although the fertilization rate in group III was significantly lower than in groups I and II, no significantdifference was found between groups I and II. Day 3 embryos in group I had the highest mean number ofblastomeres, proportions of good embryos, and blastocyst formation rate when compared with groups II and III.Two clinical pregnancies were achieved from 26 transfer cycles in study 2, resulting in pregnancy andimplantation rates of 7.7% and 4% per transfer cycle, respectively.Conclusion(s): Although our results show that immature oocytes from stimulated cycles can be normally fertilizedand used to increase the number of embryos available for transfer, the increase in number of embryos derivedfrom immature oocytes cannot be efficiently translated into pregnancies and live births. The clinical significanceof using immature oocytes in stimulated cycles needs further investigation. (Fertil Steril� 2007;87:1022–7. ©2007 by American Society for Reproductive Medicine.)
Key Words: In vitro maturation, oocytes, stimulated cycles, oocyte denudation, fertilization, embryo development,clinical outcome
otmpovb
ctreA2atrc
n important aspect of the intracytoplasmic sperm injectionICSI) procedure involves the removal of cumulus and co-ona cells immediately or a few hours after oocyte retrieval,hich allows a precise determination of nuclear maturation
tatus and oocyte morphology. About 20% of retrieved oo-ytes from controlled ovarian stimulation cycles are imma-ure, either at metaphase I (MI) or germinal-vesicle (GV)tage, in human IVF (1,2). Some of these oocytes mayxtrude the first polar body during in vitro culture, and maye used as a source of oocytes for sperm injection in ICSIycles. It was shown that immature oocytes released from
eceived May 1, 2006; revised and accepted August 15, 2006.resented in part at the 60th Annual Meeting of the American Society forReproductive Medicine, Philadelphia, Pennsylvania, October 17–19,2004.
eprint requests: Barry Behr, Ph.D., In Vitro Fertilization Program, Divi-sion of Reproductive Endocrinology and Infertility, Department of Ob-stetrics and Gynecology, Stanford University, 900 Welch Road, Suite350, Palo Alto, California 94304 (FAX: 650-736-7036, E-mail: behr@
ostanford.edu).
1022 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
varian follicles have the potential for spontaneous matura-ion in vitro and subsequent development in different mam-alian species, including humans (3). Although sporadic
regnancies from immature oocytes obtained from super-vulated cycles were reported (4–7), there is still contro-ersy regarding the rate of fertilization and subsequent em-ryonic development of these immature oocytes.
Oocyte maturation in vitro is a relatively fast event thatan occur shortly after oocyte retrieval (8). Close observa-ion of 468 oocytes matured in vitro within 3 hours afteretrieval, as performed by Balakier et al. (8), provided directvidence about the timing of oocyte maturation in vitro.mong these oocytes, 90 (19%), 182 (39%), 168 (36%), and8 (6%) oocytes underwent maturation during 30 minutes,nd 1, 2, and 3 hours of in vitro culture, respectively. Givenhat oocyte denudation is performed a few hours after oocyteetrieval, the maturational profile might be misleading, be-ause some MI oocytes become mature and some GV-stage
ocytes move on to metaphase I before oocyte denudation. It0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.110

iod
ccaepic
opmpbvecan
MPTRToarftiymtctrciaivd
STipcca
dMaohaMGdMss
e(s391caw
3pgsfsooGacctbwbv
pfmm�(fofftc
F
s therefore necessary to take into account the timing ofocyte denudation when fertilization and ensuing embryoevelopment are evaluated.
Embryos derived from immature or in vitro matured oo-ytes are usually deprioritized for transfer. Occasionally,ombined transfers of embryos derived from both in vitrond in vivo matured oocytes are performed if there are notnough embryos from in vivo matured oocytes for an appro-riate ET. It is difficult to tell whether embryos derived frommmature or in vitro matured oocytes contribute to pregnan-ies or live births (6,9).
In this study, we investigated the fate of immature oocytesbtained from stimulated cycles. Oocyte denudation waserformed immediately after retrieval to obtain an accurateaturational profile. Oocytes at different stages of meiotic
rogression were then cultured separately for 4–6 hoursefore ICSI. Metaphase II oocytes, matured in vivo and initro, were injected along with MI oocytes. Fertilization andarly embryo development were compared. In addition, ICSIycles with no mature oocytes at oocyte denudation werelso included, to evaluate the implantation rates and preg-ancy outcomes of immature oocytes.
ATERIALS AND METHODSatients and Stimulation Protocolhis retrospective study was approved by the Institutionaleview Board of Stanford University, Stanford, California.he controlled ovarian hyperstimulation protocol consistedf GnRH agonist down-regulation, followed by FSH/hMGnd hCG, microdose flare, or antagonist protocols. Oocyteetrieval was performed by transvaginal ultrasound-guidedollicle aspiration 34–36 hours after 10,000-IU hCG injec-ion. This study consisted of two parts. In study 1, wencluded a total of 200 patients (mean age � SD, 37.1 � 4.9ears) undergoing 214 ICSI cycles containing at least oneature oocyte and one immature oocyte at oocyte denuda-
ion between October 2003–November 2004. The ICSI cy-les with completely mature oocytes were excluded fromhis study. Fertilization and early embryo development wereecorded and compared between immature and mature oo-ytes. To investigate the further developmental potential ofmmature oocytes from stimulated cycles, we retrospectivelynalyzed 46 ICSI cycles (from 44 patients) containing onlymmature oocytes at retrieval between January 2001–No-ember 2004 in study 2. The fertilization rate, early embryoevelopment, and implantation rate were recorded.
tudy Protocolhe removal of cumulus cells from oocytes was performed
mmediately after retrieval. Oocyte-corona-cumulus com-lexes were briefly exposed to hyaluronidase at a final con-entration of 80 IU/mL (Sigma, St. Louis, MO), and me-hanically cleaned from their surrounding cumulus cells by
spiration with the use of stepwise denuding pipettes with wertility and Sterility�
iameters of 275 and 135 �m (MidAtlantic Diagnostic, Inc.,arlton, NJ). The oocyte maturational profile was checked,
nd denuded oocytes were classified into four groups, basedn their maturation status at oocyte denudation and then 4–6ours later, prior to ICSI. Group I consisted of MII oocytest time of removal of cumulus cells. Group II consisted ofI oocytes at time of cumulus removal that matured in vitro.roup III consisted of MI oocytes at oocyte denudation thatid not progress to MII prior to ICSI. Group IV consisted ofI oocytes converted from GVs. A standard procedure of
perm injection was performed, based on the protocol de-cribed by Palermo et al. (10).
The injected oocytes were cultured in groups under min-ral oil in 100–150-�L droplets of Sage Cleavage MediumCooper Surgical, Inc., Trumbull, CT) with 10% syntheticerum substitute (SSS; Irvine Scientific, Santa Ana, CA) at7°C with a humidified atmosphere of 5% O2, 5% CO2, and0% N2 in desiccators. A fertilization check was performed6–18 hours after ICSI. The zygotes with two clear pronu-lei (PN) were cultured for another 48 hours in Sage Cleav-ge Medium with 10% SSS. Oocytes with 1PN or �3PNere considered abnormally fertilized.
Embryo development was assessed on the morning of day, including blastomere number, size, and regularity, and theresence and percentage of fragmentation. All embryos wereraded on a scale of 1–5. Grade 1 embryos consisted ofymmetrical blastomeres of equal size and no cytoplasmicragmentation. Grade 2 embryos had blastomeres of equalize and minor cytoplasmic fragmentation covering �10%f the embryo surface. Grade 3 embryos had blastomeresf distinctly unequal sizes and variable fragmentation.rade 4 embryos had blastomeres of equal or unequal size
nd moderate-to-significant cytoplasmic fragmentationovering �10% of the embryo surface. Grade 5 embryosontained few blastomeres of any size and severe fragmen-ation covering �50% of the volume of the embryos. Em-ryos with equal-sized 6–8 cells and �10% fragmentationere defined as good embryos. Those embryos with �4lastomeres were defined as arrested embryos, regardless ofolume of fragmentation.
Embryo transfer was performed on day 3 or day 5, de-ending on day 3 embryo development. If there were at leastour eight-cell-stage embryos at grade 1 or grade 2 on theorning of day 3, day 5 blastocyst transfer was recom-ended. After day 3 transfer, any remaining embryos with5 blastomeres were cultured in Sage Blastocyst Medium
Cooper Surgical, Inc.) with 10% SSS for another 2 or 3 daysor possible cryopreservation. Embryos generated from MIIocytes in group I were given priority in selection for trans-er. Embryos derived from groups II or III were consideredor transfer only if they were of much better quality, or ifhere were not enough embryos derived from group I oo-ytes. Any expanding, expanded, and hatching blastocysts
ith good ICM and trophectoderm epithelium were frozen1023

op
TIctd
SRFtc
RIi(t(aodmft(A
iwzg
Pb�owirepidcb1(eb
oaanm(
n day 5 or day 6. The blastocyst freezing and thawingrotocols we used were described elsewhere (11).
Ultrasound-guided ET was performed with the use of aefcat or Echotip Softpass catheter (Cook Ob/Gyn, Spencer,
N), with a transfer volume of 20–30 �L. Clinical pregnan-ies were defined by the presence of an intrauterine gesta-ional sac with a heartbeat as seen on ultrasound, or by theiagnosis of an ectopic pregnancy.
tatistical Analysisesults were expressed as means � SD. The chi-square test,isher’s exact test, one-way analysis of variance, and Student’s
-test were used to compare groups as appropriate. P�.05 wasonsidered statistically significant.
ESULTSn total, 2,401 oocytes were collected from 214 ICSI cyclesn study 1. Among them, 1,740 (73%) were mature, 48320%) were MI oocytes, and 178 (7%) were GV oocytes athe time of cumulus removal. Of those MI oocytes, 25954%) matured to MII, and 221 (46%) remained at MI aftern in vitro culture of 4–6 hours. Thirty-five (20%) GVocytes progressed to MI after in vitro culture. Table 1escribes the fertilization and embryo development of im-ature oocytes and in vivo matured sibling oocytes. The
ertilization rate in group III (25%) was significantly lowerhan in groups I and II (69.5% and 62.2%, respectively)P�.001). No normal fertilization was observed in group IV.lthough the fertilization rate of oocytes from group I was
TABLE 1Comparison of fertilization and embryo developm
Variables Grou
No. of oocytes injected 1,74Fertilization
2PN 1,210 (61PN 40 (23PN 46 (2
CleavageCleaved embryos 1,203 (9Cell number on day 3 (mean � SD) 7.0 � 1No. of 8-cell embryos 675 (5No. of �6-cell embryos 902 (7
Note: Data are presented as n or n (%) unless otherwise sdenudation; group II, in vitro matured oocytes from MI; gto MII prior to ICSI; group IV, MI oocytes converted fro
a P�.001.b P�.001.c P�.01.d P�.05.
Shu. Developmental competency of immature oocytes. Fertil Steril 2007.
1024 Shu et al. Developmental competency of immature ooc
ncreased compared to those from group II, the differenceas not statistically significant (P�.182). Abnormal fertili-
ation (1PN � 3PN) did not differ significantly amongroups (P�.05).
Cleavage rates were similar among the three groups (all�.05). Embryos in group I had the highest number oflastomeres (7.0 � 1.9) when compared with group II (6.1
1.9) and group III (5.7 � 1.9) (P�.001). The proportionsf 8-cell and �6-cell embryos in group I were much higherhen compared with groups II and III (Table 1). No signif-
cant differences were found between groups II and III withespect to cell number of day 3 embryos, proportions ofight-cell embryos, and proportions of �6-cell embryos. Theercentages of good embryos and arrested embryos on day 3n the three groups are shown in Figure 1. Further embryoevelopment was observed in 39-day, 5 blastocyst transferycles. Blastocyst formation rates of day 3 embryos with �5lastomeres in groups I and II were 52.0% (173/333) and6.7% (4/24), respectively. Their difference was significantP�.05). Only one blastocyst was obtained out of 10 day 3mbryos in group III, which was significantly lower thanlastocyst formation rate of group I (P�.05).
Day 3 ET was performed in 167 cycles. The proportionsf cleaved embryos selected for day 3 ET were comparablemong group I (469/784; 59.8%), group II (56/112; 50%),nd group III (22/43; 51.2%) (P�.05). However, the cellumber of transferred embryos in group I (7.2 � 1.6) wasarkedly higher than in group II (6.2 � 1.6) and group III
6.2 � 1.5) (P�.01). No clinical pregnancy was obtained
t among groups.
Group II Group III Group IV
259 224 35
a 161 (62.2)b 56 (25)a,b 05 (1.9) 1 (0.4) 18 (3.1) 13 (5.8) 0
159 (98.8) 55 (98.2) NAb 6.1 � 1.9a 5.7 � 1.9b NAa,b 55 (34.6)a 12 (21.8)b NAc,d 89 (56.0)c 27 (49.1)d NAfied. NA � not applicable. Group I, MII oocytes at oocyteIII, MI oocytes at oocyte denudation that did not progress
V.
en
p I
0
9.5).3).6)
9.4).9a,
6.1)5.0)peciroupm G
ytes Vol. 87, No. 5, May 2007

fr
oI2rApvSc(bCccwdnaroot
wa
DItvsstwbuciI
ptrsvr(hod(bmr
F
rom three cycles with transferred embryos exclusively de-ived from oocytes in groups II or III.
In study 2, 46 ICSI cycles from 44 patients with no matureocytes at oocyte denudation were recruited out of 1,249CSI cycles performed between January 2001–November004. Among them, 28, 15, and 3 cycles fell within theanges of 1–3, 4–8, �8 oocytes retrieved, respectively.fter 4–6 hours of culture prior to ICSI, 84 MI oocytesrogressed to MII; the maturation rate was 65.1%. Germinal-esicle breakdown occurred in 18 (37.5%) GV oocytes.ixty-five oocytes (44.2%) were fertilized with 2PN, andleaved in 26 cycles. No ET was performed in 20 cycles43.5%). Of those, ICSI was not performed in two cyclesecause all oocytes remained at GV stage at time of ICSI.omplete fertilization failure occurred in the other 18ycles. The rates of oocyte maturation, fertilization, andleavage for study 2 are shown in Table 2. Fifty embryosere transferred in 26 cycles, including 49 embryos onay 3, and one blastocyst on day 5. Two clinical preg-ancies were achieved, leading to pregnancy rates (PRs)nd implantation rates of 7.7% and 4% per transfer cycle,espectively. However, both pregnancies were spontane-usly aborted (early abortion). Six blastocysts were frozenn day 5 from two cycles. Two frozen blastocysts were
FIGURE 1
Percentages of good embryos (blue bars) andarrested embryos (red bars) developed from groupI (MII oocytes), group II (MI–MII oocytes), andgroup III (arrested MI oocytes). Differences inpercentage of good embryos between groups Iand II, and groups I and III, are statisticallysignificant. Groups I and II, P�.01. Groups Iand III, P�.01. Groups II and III had higherpercentages of arrested embryos than group I(P�.001 and P�.001, respectively). No significantdifferences were found between groups II and III inthe percentages of good embryos and arrestedembryos (P�.05).
68.2
49.7
38.2
14.7
30.8 32.7
0
10
20
30
40
50
60
70
80
Group I (N=1203) Group II (N=159) Group III (N=55)
Source of embryos
Perc
enta
ges
of g
ood
and
arre
sted
em
bryo
s
Shu. Developmental competency of immature oocytes. Fertil Steril 2007.
ransferred back to the uterus after thawing; no pregnancy
ertility and Sterility�
as obtained. The other four blastocysts remain in storaget this time.
ISCUSSIONn the past 15 years, there have been a number of publica-ions on the pregnancies obtained from patients having initro maturation (IVM) as infertility treatment (12–14). Ithould be noted that the immature oocytes collected in thistudy were from stimulated cycles of patients seeking IVFreatment. These oocytes were already under stimulationith high doses of gonadotropins, and were exposed to hCGefore retrieval. The nuclear maturation, cytoplasmic mat-ration, and ensuing developmental capacity of these oo-ytes may very well be different in comparison withmmature oocytes collected from small antral follicles ofVM cycles (15).
The maturation rates of immature oocytes from previouslyublished reports vary from 16.4%–88.3%, depending onhe period of in vitro culture (16). Generally, the maturationate increases with a prolonged in vitro culture period. In thistudy, the maturation rates of MI oocytes after 4–6 hours initro culture in studies 1 and 2 were 54.0% and 65.1%,espectively, which is close to the results of Balakier et al.8), who performed oocyte denudation shortly (within 1our) after retrieval. However, a maturation rate of 43% wasbtained by Vanhoutte et al. (17), who performed oocyteenudation 1–2 hours after retrieval. Similarly, De Vos et al.6) showed that 26.7% of MI oocytes extruded the first polarody after 4 hours of in vitro culture. A decreased rate ofaturation of 16.4% was reported by Chen et al. (16), who
emoved the cumulus cells from oocytes 6 hours after re-
TABLE 2Outcome of ICSI cycles with no matureoocytes at oocyte denudation.
No. of retrieval cycles 46No. of oocyte retrieved 177Maturation status at cumulus
removalMI 129 (72.9)GV 48 (27.1)
No. of MII oocytes convertedfrom MI
84 (65.1)
Total MI and MII oocytes injected 147No. of 2PN oocytes 65 (44.2)No. of cleaved 2PN zygotes 65 (100)No. of embryos transferred 50No. of transfer cycles 26Clinical pregnancy 2 (7.7)Implantation 2 (4.0)Note: Data are presented as n or n (%).
Shu. Developmental competency of immature oocytes. Fertil Steril 2007.
1025

t(rb
sscoitigmbip4Aoaf
oHitfiwrdptbmcsooymegptm
himeoped
dsdfbmo
dbaviom(sdcc
oeifn2bdcmrcodama
pococsttm
wobdt
rieval. Based on our results and other published reports9,16,17), there is an obvious trend to the effect that reportedates of maturation decrease with an increased time intervaletween retrieval and oocyte denudation.
The between-study differences in maturation rates mighttem from different timings of oocyte denudation. The de-ign of the present study on timing of removal of cumulusells enabled us to obtain an accurate maturational profile ofocytes at the time of retrieval. In other studies wheremmediate oocyte denudation was not performed, oocyteshat matured in vitro prior to denudation were not counted asn vitro matured oocytes, but fell into an in vivo maturedroup. The maturation rate was then underestimated, and theaturational profile was therefore inaccurate, and might not
e representative of the immature oocyte population. Tonvestigate the fate of immature oocytes from stimulatedatients, we also cultured GV oocytes in vitro. Obviously,–6 hours are not enough for GV oocytes to move to MII.lthough a successful pregnancy was established from GVocytes derived from stimulated cycles (7), overnight culturend sperm injection for vitro matured oocytes are not per-ormed in our ICSI program.
Decreased rates of fertilization from in vitro maturedocytes were reported in several previous studies (6,8,9).owever, we failed to find a significant difference in fertil-
zation rate between in vitro and in vivo matured oocytes inhis study. The discrepancy in fertilization rate between ourndings and other investigations can be explained in twoays. First, as already discussed, the variation in reported
ates of fertilization is dependent on the timing of oocyteenudation. In those reports where delayed denudation waserformed, the reported rate of fertilization came only fromhose late matured oocytes. Second, the IVM time intervaletween the first polar body extrusion and sperm injectionay also contribute to this difference. Although the prein-
ubation of mature oocytes prior to ICSI is still controver-ial, it has proven to have a positive effect on immatureocytes (1,18). Given the same incubation period betweenocyte retrieval and sperm injection, early matured oocytesielded higher fertilization rates and better embryo develop-ent than their later matured counterparts. (8). Plausibly,
arly matured oocytes that fell into the in vivo maturedroup were those with better fertilization and developmentalotential, resulting in a reported lower rate of fertilizationhan the in vitro matured oocytes that contained only lateatured oocytes.
With regard to embryo development, our results showed aigher rate of cleavage arrest beyond the 4–8-cell stage forn vitro matured and arrested MI oocytes. This is in agree-ent with most reported data (6,12,19). However, similar
mbryo development between in vivo and in vitro maturedocytes was reported by Strassburger et al. (9). When inter-reting this discrepancy, it must be mentioned that day 2mbryo development was observed in their study. Because
ay 2 embryo development was shown to be a poorer pre- p1026 Shu et al. Developmental competency of immature ooc
ictor of continued development than day 3 or blastocysttage, their results seem relatively inconclusive (20). Fewata are presently available regarding blastocyst formationrom in vitro matured oocytes. As shown in our results, thelastocyst formation rate of embryos derived from in vitroatured oocytes is lower than those from in vivo matured
ocytes.
Oocyte quality is defined as the potential of that oocyte toevelop into a viable offspring (21). In this study, no liveirth was obtained from 29 transfers (3 transfers in study 1,nd 26 transfers in study 2) with only embryos derived fromitro matured or immature oocytes. Although normal fertil-zation can be obtained from immature and in vitro maturedocytes, their further developmental competence is compro-ised, as shown in our results and other published reports
22,23). To our knowledge, this study contains the largestample size of transfer cycles with embryos exclusivelyerived from immature oocytes obtained from stimulatedycles. The limited number of available reports and transferycles makes it difficult to draw solid conclusions.
Several factors may contribute to the incompetent devel-pment of immature and in vitro matured oocytes. Onexplanation involves incomplete oocyte maturation, includ-ng nuclear or cytoplasmic maturation or both. Successfulertilization and embryo development depend not only onuclear maturity, but also on cytoplasmic maturation (24–6). For in vitro matured oocytes, nuclear maturation occursefore the ooplasm has reached full maturity. The lack orefect of some cytoplasmic remodeling events involvingytoskeletal organization from in vitro matured oocytesight influence the morphogenesis of the meiotic spindle,
esulting in embryos with nuclear disorganization or withhromosomal abnormalities (27,28). Emery et al. (29) dem-nstrated that in vitro oocyte maturation and subsequentelayed fertilization are associated with increased embryoneuploidy. Incomplete nuclear maturation and cytoplasmicaturation can at least partly explain the poor fertilization
nd embryo development of arrested MI oocytes.
Cumulus-oocyte communication via the gap junctionlays a critical role in oocyte maturation and embryo devel-pment. It was shown that the retention of attached cumulusells can help achieve higher rates of cytoplasmic maturationf human oocytes (30). However, immature oocytes wereompletely denuded of surrounding cumulus cells in thistudy, to visualize their maturation status prior to ICSI. Theransfer of low molecular substrates such as ions, nucleo-ides, and amino acids, which are essential for completion ofaturation, could then be interrupted (31).
In conclusion, although comparable fertilization ratesere obtained between in vitro and in vivo matured oocytes,ur data show that the developmental competence of em-ryos derived from immature oocytes was significantly re-uced, compared with sibling in vivo matured oocytes. Pa-ients should be informed of the poor developmental
otential of immature oocytes if there are no mature oocytesytes Vol. 87, No. 5, May 2007

asish
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
F
vailable at the time of oocyte denudation. The results of thistudy raise questions about the cost effectiveness of spermnjection for immature oocytes after superovulation. Furthertudies are needed to define the optimal IVM conditions foruman immature oocytes from stimulated cycles.
EFERENCES1. Rienzi L, Ubaldi F, Anniballo R, Cerulo G, Greco E. Preincubation of
human oocytes may improve fertilization and embryo quality afterintracytoplasmic sperm injection. Hum Reprod 1998;13:1014–9.
2. Huang FJ, Chang SY, Tsai MY, Lin YC, Kung FT, Wu JF, et al.Relationship of the human cumulus-free oocyte maturational profilewith in vitro outcome parameters after intracytoplasmic sperm injec-tion. J Assist Reprod Genet 1999;16:483–7.
3. Edwards RG. Maturation in vitro of mouse, sheep, cow, pig, rhesusmonkey, and human varian oocytes. Nature 1965;208:349–51.
4. Coetzee K, Windt ML. Fertilization and pregnancy using metaphase Ioocytes in an intracytoplasmic sperm injection program. J Assist Re-prod Genet 1996;13:768–71.
5. Tucker MJ, Wright G, Morton PC, Massey JB. Birth after cryopreser-vation of immature oocytes with subsequent in vitro maturation. FertilSteril 1998;70:578–9.
6. De Vos A, Van de Velde H, Joris H, Van Steirteghem A. In-vitromatured metaphase-I oocytes have a lower fertilization rate butsimilar embryo quality as mature MII oocytes after intracytoplasmicsperm injection. Hum Reprod 1999;14:1859 – 63.
7. Kim BK, Lee SC, Kim KJ, Han CH, Kim JH. In vitro maturation,fertilization, and development of human germinal vesicle oocytes col-lected from stimulated cycles. Fertil Steril 2000;74:1153–8.
8. Balakier H, Sojecki A, Motamedi G, Librach C. Time-dependent ca-pability of human oocytes for activation and pronuclear formationduring metaphase II arrest. Hum Reprod 2004;19:982–7.
9. Strassburger D, Friedler S, Raziel A, Kasterstein E, Schachter M,Ron-El R. The outcome of ICSI of immature MI oocytes and rescued invitro matured MII oocytes. Hum Reprod 2004;19:1587–90.
0. Palermo G, Joris H, Devroey P, Van Steirteghem AC. Pregnancies afterintracytoplasmic injection of single spermatozoon into an oocyte. Lan-cet 1992;340:17–8.
1. Behr B, Gebhardt J, Lyon J, Milki AA. Factors relating to a successfulcryopreserved blastocyst transfer program. Fertil Steril 2002;77:697–9.
2. Trounson A, Anderiesz C, Jones G. Maturation of human oocytes invitro and their developmental competence. Reproduction 2001;121:51–75.
3. Son WY, Yoon SH, Lee SW, Ko Y, Yoon HG, Lim JH. Blastocystdevelopment and pregnancies after IVF of mature oocytes retrievedfrom unstimulated patients with PCOS after in-vivo HCG priming.Hum Reprod 2002;17:134–6.
4. Rao GD, Tan SL. In vitro maturation of oocytes. Semin Reprod Med2005;23:242–7.
5. Sun QY, Lai L, Bonk A, Prather RS, Schatten H. Cytoplasmic changes
in relation to nuclear maturation and early embryo developmentalertility and Sterility�
potential of porcine oocytes: effects of gonadotropins, cumulus cells,follicular size, and protein synthesis inhibition. Mol Reprod Dev2001;59:192–8.
6. Chen SU, Chen HF, Lien YR, Ho HN, Chang HC, Yang YS. Scheduleto inject in vitro matured oocytes may increase pregnancy after intra-cytoplasmic sperm injection. Arch Androl 2000;44:197–205.
7. Vanhoutte L, De Sutter P, Van der Elst J, Dhont M. Clinical benefit ofmetaphase I oocytes. Reprod Biol Endocrinol 2005;3:71–6.
8. Ho JY, Chen MJ, Yi YC, Guu HF, Ho ES. The effect of preincubationperiod of oocytes on nuclear maturity, fertilization rate, embryo quality,and pregnancy outcome in IVF and ICSI. J Assist Reprod Genet2003;20:358–64.
9. Moor RM, Dai Y, Lee C, Fulka J Jr. Oocyte maturation and embryonicfailure. Hum Reprod Update 1998;4:223–36.
0. Laverge H, De Sutter P, Van der Elst J, Dhont M. A prospective,randomized study comparing day 2 and day 3 embryo transfer in humanIVF. Hum Reprod 2001;16:476–80.
1. Hunter MG. Oocyte maturation and ovum quality in pigs. Rev Reprod2000;5:122–30.
2. Liu H, Krey LC, Zhang J, Grifo JA. Ooplasmic influence on nuclearfunction during the metaphase II-interphase transition in mouse oo-cytes. Biol Reprod 2001;65:1794–9.
3. Combelles CMH, Cekleniak NA, Racowsky C, Albertini DF. Assess-ment of nuclear and cytoplasmic maturation in in-vitro matured humanoocytes. Hum Reprod 2002;17:1006–16.
4. McConnell JM, Campbell L, Vincent C. Capacity of mouse oocytes tobecome activated depends on completion of cytoplasmic but not nu-clear meiotic maturation. Zygote 1995;3:45–55.
5. Eppig JJ. Coordination of nuclear and cytoplasmic oocyte maturation ineutherian mammals. Reprod Fertil Dev 1996;8:485–9.
6. Schoevers EJ, Bevers MM, Roelen BA, Colenbrander B. Nuclear andcytoplasmic maturation of sow oocytes are not synchronized by specificmeiotic inhibition with roscovitine during in vitro maturation. Theriog-enology 2005;63:1111–30.
7. Nogueira D, Staessen C, Van de Velde H, Van Steirteghem A. Nuclearstatus and cytogenetics of embryos derived from in-vitro maturedoocytes. Fertil Steril 2000;74:295–8.
8. Sanfins A, Plancha CE, Overstrom EW, Albertini DF. Meiotic spindlemorphogenesis in in vivo and in vitro matured mouse oocytes: insightsinto the relationship between nuclear and cytoplasmic quality. HumReprod 2004;19:2889–99.
9. Emery BR, Wilcox AL, Aoki VW, Peterson CM, Carrell DT. In vitrooocyte maturation and subsequent delayed fertilization is associatedwith increased embryo aneuploidy. Fertil Steril 2005;84:1027–9.
0. Goud PT, Goud AP, Qian C, Laverge H, Van der Elst J, De Sutter P,Dhont M. In-vitro maturation of human germinal vesicle stage oocytes:role of cumulus cells and epidermal growth factor in the culturemedium. Hum Reprod 1998;13:1638–44.
1. Dekel N, Beers WH. Development of rat oocytes in vitro: inhibition andinduction of maturation in the presence or absence of cumulus-oophorus.
Dev Biol 1980;75:247–54.1027

Maadar(ppg
batiH(Tt
oce
RR
Risk of monozygotic twinning with blastocyst transferdecreases over time: an 8-year experienceSharon E. Moayeri, M.D., M.P.H., Barry Behr, Ph.D., Ruth B. Lathi, M.D.,Lynn M. Westphal, M.D., and Amin A. Milki, M.D.
Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology and Infertility, Stanford UniversityMedical Center, Stanford, California
Objective: The purpose of our study is to compare the occurrence of monozygotic twinning (MZT) fromblastocyst transfer (BT) in our program between an earlier and more recent time period.Design: Retrospective.Setting: Academic IVF practice.Patient(s): All pregnancies conceived between March 2002 and December 2005 (N � 932) in our program werecompared to pregnancies conceived before March 2002 (N � 554), which were the subject of a previous study.Intervention(s): None.Main Outcome Measure(s): The incidence of MZT with day 3 embryo transfer and BT were compared betweenthe study and control groups.Result(s): During the study period, the rate of MZT was not significantly different for BT at 2.3% (9/385)compared to day 3 embryo transfer at 1.8% (10/547). This rate of 2.3% for BT was significantly lower than therate of 5.6% (11/197) reported at our institution for BT before March 2002.Conclusion(s): Our study suggests that the risk of MZT with BT is significantly lower in the more recent timeperiod and is in the range of what is seen with cleavage stage transfer. It is likely that improvements in culturesystems as experience is gained with BT played a role. (Fertil Steril� 2007;87:1028–32. ©2007 by AmericanSociety for Reproductive Medicine.)
Key Words: IVF, monozygotic twinning, blastocyst transfer, culture system
Jwosc
rtipmdm
MIcMrFdprtr
onozygotic (MZ) twinning is rare in nature, occurring inpproximately 0.4% of all births (1). These pregnancies aressociated with more perinatal complications as compared toizygotic twins (2). Ovarian stimulation, with or withoutssisted reproductive technology (ART), may increase theisk for identical twinning in addition to fraternal twinning3–9). Several explanations for this phenomenon have beenroposed including the superovulation itself (10, 11), zonaellucida (ZP) manipulation (5, 12, 13), high order multipleestations (8), and stage of embryo transfer (14–17).
Recent data suggest that the use of extended culture to thelastocyst stage in women with many good quality embryost the cleavage stage may facilitate embryo selection,hereby supporting the transfer of fewer embryos and reduc-ng the risk of a multiple gestation pregnancy (18–22).owever, several reports have linked blastocyst transfer
BT) to a higher incidence of MZ twinning (14–17, 23–25).his may reduce the potential benefit of the extended culture
reatment modality.
Mechanisms suggested in the literature to explain thebserved increased MZ twin rate include: extended time inulture (16, 24), culture media composition (26, 27), andmbryology laboratory experience (14). In this last study by
eceived May 13, 2006; revised and accepted September 1, 2006.eprint requests: Amin A. Milki, M.D., 900 Welch Road, Suite 350, Palo
fAlto, CA 94304 (FAX: 650-498-6175; E-mail: [email protected]).
1028 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
ain et al. (14) there were 38 pregnancies from 75 BT ofhich 5 resulted in MZ twinning. Three of the five MZ twinsccurred in the first seven pregnancies. The numbers aremall, but suggest a possible “learning curve” for blastocystulture and transfer methods.
We previously reported on the incidence of MZ twinsesulting from BT in our IVF program from January 1, 1998o February 28, 2002 (17). The purpose of the current studys to compare the occurrence of MZ twinning with BT in ourrogram between our initial experience (first 4 years) and aore recent time period to assess whether this potential
rawback of extended culture has diminished as we gainore expertise.
ATERIALS AND METHODSn the present study, we analyzed all viable pregnanciesonceived in our program from IVF cycles initiated betweenarch 1, 2002 and December 31, 2005 and compared the
ate of MZ twinning to our initial study that ended onebruary 28, 2002 (17). The incidence of MZ twins wasetermined among pregnancies resulting from BT as com-ared to day 3 embryo transfer during this time period. Theesults from this recent period (study group) were comparedo data obtained before March 2002 (control group), whicheflected our initial experience with extended culture (17).
Controlled ovarian hyperstimulation (COH) was per-
ormed using FSH/hMG stimulation protocols combined0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.09.013

wOauthus
ssC1et(CsC
dmpaZJr
ee((tG
n
ag
atgspnum
uPr
ROptii
Befia1(
5((ttmbgctg
F
ith GnRH agonist (long or microdose flare) or antagonist.ocytes were aspirated under transvaginal ultrasound guid-
nce approximately 35 hours after SC injection of eitherrinary or recombinant hCG. Insemination occurred conven-ionally or by intracytoplasmic sperm injection (ICSI) 3–4ours after egg retrieval. For ICSI, oocytes were denudedsing a hyaluronidase solution combined with mechanicaltripping.
Oocytes were then rinsed and those at the metaphase IItage were injected in modified human tubal fluid with 10%erum substitute supplement (Irvine Scientific, Sana Ana,A). Embryos were cultured in groups under mineral oil in50-�L droplets of P1/cleavage stage medium (Irvine Sci-ntific) with 10% serum substitute supplement for the con-rol group and in Quinn’s Advantage cleavage stage mediumSage, Assisted Reproduction Products, A CooperSurgicalompany, Trumbull, CT) for the study group. All cleavage
taged embryos were cultured under 37°C in a 5% O2, 5%O2, and 90% N2 environment for 72 hours.
In selected cases, assisted hatching was performed beforeay 3 embryo transfer. Embryos for hatching were placed inodified human tubal fluid with 10% serum substitute sup-
lement. A small opening (�20 �m) was made using eithercidified Tyrode’s solution (pH 2.3) or laser in an area of theP that was between blastomeres. Laser was used starting inune 2003 of the study period. Embryos were then rinsed andeturned to culture until embryo transfer.
In cases where there were more than three embryos at theight-cell stage, extended culture was recommended. Thembryos were moved on day 3 into Blastocyst MediumIrvine Scientific) or Quinn’s Advantage Blastocyst MediumSage). They were cultured for an additional 48 hours. Allransfers were performed with either a Tefcat (Cook Ob/yn, Spencer, IN) or Cook Echotip catheter (Cook Ob/Gyn).
We excluded patients who underwent preimplantation ge-etic diagnosis from our study (N � 15).
A viable pregnancy was defined as the presence of cardiacctivity confirmed by transvaginal ultrasound at 6–7 weeks’estation. The number of fetuses and gestational sacs was
TABLE 1Control group and study group details.
Control group (N
Day 3 ET
No. of pregnancies 357MZ twins 7 (1.96%)a 1Multiple gestationb 84 (23.5%) 4a �, P � .02 within the control group between day 3 embb �, P�.001 between control and study groups.
Moayeri. Monozygotic twinning in blastocyst transfer. Fertil Steril 2007.
ertility and Sterility�
ssessed. Monozygotic twinning was diagnosed when morehan one fetus with cardiac activity was seen in the sameestational sac. There was no incidence of more gestationalacs than the number of embryos transferred. Also, theresence or absence of a dividing amnionic membrane wasoted. The findings were reconfirmed with both a repeatltrasound examination 2 weeks later and follow-up infor-ation for the rest of the pregnancy and delivery.
Statistical analysis was performed on contingency tablessing �2 statistics. Statistical significance was determined at�.05. Institutional review board approval was obtained for
eview of patient charts.
ESULTSverall, the MZ twin rate was 2.5% (37 of 1,486 viableregnancies) across the time period and embryo stage atransfer. Among BT, there were 9 of 385 (2.3%) MZ twinsn our study period compared to 11 of 197 (5.6%) observedn our control period (P�.03).
Within the study period the rate of MZ twinning amongT (2.3%) was comparable to the rate observed from day 3mbryo transfer at 1.8% (10 in 547) (P�.59). In contrast,ndings of our previous report (control group) demonstratedsignificantly higher rate of MZ twins among BT (5.6%,
1/197 pregnancies) as compared with day 3 embryo transfer2%, 7/357 pregnancies; P�.02) (Table 1).
The multiple gestation rate increased from 22.9% (127 of54 pregnancies) in the control group time period to 32.4%302 of 932 pregnancies) in the more recent study groupP�.001). Within the study group there was no difference inhe rate of multiple gestations based on day of embryoransfer. Specifically, there were 184 instances (33.6%) ofultiple gestation pregnancies from the cleavage stage em-
ryo transfer group as compared to 118 (30.7%) in the BTroup (P�.392). The control group also showed no signifi-ant difference in the overall multiple gestation rate betweenhe day 3 embryo transfer group (84 of 357; 24%) and BTroup (43 of 197, 22%; P�.50).
54) Study group (N � 932)
T Day 3 ET BT
97 547 385.6%)a 10 (1.8%) 9 (2.3%)1.8%) 184 (33.6%) 118 (30.7%)ransfer (ET) and blastocyst transfer (BT).
� 5
B
11 (53 (2
ryo t
1029

DTcomhfm
dliitoaoo
Apdptep2bt
imsmfbp
z(aTZda
1(mfedtM
atmqtSbI
ocmtlihbssofitttg
oosebwf
ptcpi
compfld
awtc(
ISCUSSIONhe rate of MZ twinning in our BT group declined from ourontrol to study period from 5.6% to 2.3%, whereas the ratef MZ twinning in our day 3 embryo transfer group re-ained stable (2%–1.8%). The main advantage of BT is its
igh implantation rate, which encourages the transfer ofewer embryos and may facilitate the reduction of fraternalultiple births.
This benefit is potentially offset by the increased inci-ence of MZ twinning described by several reports in theiterature (15, 23, 24, 28). However, only a few studiesnclude a cleavage stage embryo transfer group for compar-son (14, 16, 17, 25, 29). A review of these reports showshat some of them note a disproportionately higher incidencef MZ twinning in the early stages of BT implementation forparticular program. This may inflate the reported incidencef MZ twins over the entire study period, especially in viewf the small sample size in these reports.
The largest study examined the 1999 and 2000 Society ofssisted Reproductive Technology (SART) data with 7,921regnancies from day 5 embryo transfer and 29,144 fromay 3 embryo transfer (25). Among the resulting 226 MZregnancies there was a fourfold increased likelihood of MZwinning with day 5 embryo transfer compared to day 3mbryo transfer after controlling for multiple treatment andatient factors. The time frame of Wright’s analysis (1999–000) coincides with our control period (1998–2002) andoth studies demonstrate a similar magnitude of effect be-ween day 3 and day 5 embryo transfer MZ twinning.
Several explanations have been proposed to explain thencreased risk of MZ twinning with ART. The MZ splittingay be higher in pregnancies when two or more gestational
acs are present (4, 11, 17, 30). We observed a higher rate ofultiple gestation pregnancies in our study group. There-
ore, the decrease in MZ twinning in the study period cannote accounted for by the occurrence of multiple gestationregnancies.
In addition, in vitro culture conditions may harden theona making an embryo more susceptible to MZ twinning13, 16). Procedures using assisted hatching or ICSI may bessociated with increased MZ twinning (5, 6, 12, 31, 32).hese techniques leave small openings or thin areas in theP that may cause herniation of the embryo through theseefects and the inner cell mass (ICM) may get pinched offnd divide forming identical twins (5, 16).
However, recent studies do not support these theories (8,0, 17, 25, 30, 33). Although a large study by Schieve et al.12) of U.S. data in 1996 suggested that assisted hatching (AH)ay pose a risk for MZ twinning, a larger more recent study
ailed to confirm such an association (25). Furthermore, a studyxamining the rate of MZ pregnancies in zona-free embryosemonstrated an increased rate of MZ twinning at 1.2%,hereby casting doubt as to the influence of the ZP in leading to
Z twinning (34). g
1030 Moayeri et al. Monozygotic twinning in blastocyst trans
Explanations for the increased rate of MZ pregnanciesmong BT include aspects of in vitro conditions, as well ashe extended time in culture. Animal studies suggest thatice blastocysts duplicate their ICM in vitro more fre-
uently than in vivo (35, 36). A case report has suggestedhat this mechanism may exist in humans (37). A report byteinman (38) proposed that the long exposure time oflastocysts to lower calcium levels in culture predisposesCM division as intercellular bonds are destabilized.
Alternatively, Menezo and Sakkas (26) found no instancesf MZ pregnancies in more than 800 births resulting fromo-cultured blastocyts. They postulate that sequential cultureedia (in contrast to co-culture) have higher glucose con-
ent, which produces more free radicals that induce apoptosiseading to disruption of the ICM and presumably splittingnto identical twins. Cassuto et al. (27) found a 10 timesigher rate of MZ twinning in pregnancies conceived fromlastocysts cultured in relatively glucose rich media, but noignificant increase among day 2/3 embryo transfers. Theyuggest that those embryos initially cultured in such “sub-ptimal” conditions, with high glucose and absent or insuf-cient level of sulfa amino acids, have a lower threshold for
olerating subsequent extended culture conditions. However,he concept of free radicals may not accurately account forhe increase in MZ twins as many sequential cultures includelutathione or taurine, which are free radical scavengers.
Perhaps the suboptimal conditions are precipitated byther components of the culture media, such as the absencef growth factors or cytokines, which may mediate apopto-is. During short incubations, embryos may be able to tol-rate such circumstances, but with prolonged culture thelastocyst may experience excess metabolic stress, therebyeakening cellular adhesions and increasing the propensity
or identical twinning (17).
Studies that examine the influence of culture media inromoting MZ twinning have primarily examined the blas-ocyst culture component. Alternatively, it is possible thatonditions at various stages of a culture system could inter-lay and sequentially expose susceptible embryos to anncreased risk of MZ twinning.
During the study period we made several changes in ourulture system. First, we moved the location of our embry-logy laboratory to a significantly larger facility that accom-odated a larger number of incubators. This allowed for the
rovision of more homeostatic culture conditions whereuctuations were minimized and potential embryonic stressecreased.
Second, we switched the culture media for both cleavagend blastocyst stage embryos. Before 2002, all embryosere cultured in P1/cleavage stage medium (Irvine Scien-
ific) until day 3. During the study period embryos wereultured in Quinn’s Advantage cleavage stage mediumSage) until day 3. In contrast with P1 medium, which is
lucose free and contains only taurine, Quinn’s Advantagefer Vol. 87, No. 5, May 2007

cs
mWeoQtcpbbdc
wI(ecg“(tgo3gs
npvecrca
mabb
pMide
gcr
elp
R
1
1
1
1
1
1
1
1
1
1
2
2
F
leavage stage medium has some glucose (0.1 mM) andeveral amino acids including taurine.
In addition to using a different cleavage stage cultureedium, we transitioned to an alternate blastocyst medium.hereas all embryos from the control period that underwent
xtended culture were placed in Irvine’s Blastocyst mediumn day 3, during the study period our laboratory began usinguinn’s Advantage Blastocyst medium (Sage). Therefore, in
he study period some patients had all of their blastocystsultured in Blastocyst Medium (Irvine Scientific) and someatients had their embryos split between “Irvine” and “Sage”lastocyst medium until eventually all embryos eligible forlastocyst culture were grown using “Sage” medium fromay 3 onward. “Irvine” has more than double the glucoseoncentration (6 mM) as compared to “Sage” (2.78 mM).
Specifically, among those subjects in the study grouphose blastocysts were split in culture between Sage and
rvine (N � 28), two instances of MZ twinning were noted7.1%). Because it is impossible to know which transferredmbryo resulted in a pregnancy, we cannot draw any con-lusions regarding the split group. Looking at the other tworoups, where patients had their embryos cultured in eitherSage” (N � 171) or “Irvine” (N � 54), we noted three1.8%) and two (3.7%) instances of MZ twinning, respec-ively. It is difficult to draw conclusions from these smallerroups as to whether culture in Irvine Blastocyst medium, aspposed to Quinn’s Advantage Blastocyst medium, from dayto day 5 increases the risk of MZ splitting of embryos
rown for the first 3 days in Quinn’s Advantage cleavagetage medium.
It is possible that the blastocyst culture media alone areot as important as the effects of the culture in sequence. Ourrevious culture system had embryos in a glucose free en-ironment that were transferred on day 3 to a glucose richnvironment. The magnitude of difference in glucose con-entration between various cultures may promote a stresseaction resulting in embryo or ICM splitting. Our currentulture system, thus, may support embryos in a more favor-ble milieu.
Finally, it is likely that as the embryology team gainedore experience with blastocyst culture, their ability to
ssess optimal blastocyst morphology has matured. It coulde that blastocysts with good morphology reflect healthierehavior in culture and a decreased propensity for splitting.
The benefit of BT compared to cleavage stage transfer isotentially offset by the purported increased incidence ofZ pregnancies (14–17, 24, 25, 28). However, reports may
nflate the true incidence of MZ twinning over time, as theirenominators are small or they are reporting their earliestxperience with BT (14).
Comparing time periods, our more recent experience sug-ests that the risk of MZ twinning among BT has signifi-antly declined. The explanation for this is unclear, but may
ely on improvements in our culture system. Further studiesertility and Sterility�
xamining the rate of MZ pregnancies resulting from BT inarger series that reflect more than the initial experience of arogram are needed to confirm our findings.
EFERENCES1. Bulmer MG. The biology of twinning in man. Oxford: Oxford Univer-
sity Press, 1970.2. Malone FD. Monochorionic pregnancy—where have we been? Where
are we going? Am J Obstet Gynecol 2003;189:1308–9.3. Edwards RG, Mettler L, Walters DE. Identical twins and in vitro
fertilization. J In Vitro Fert Embryo Transf 1986;3:114–7.4. Wenstrom KD, Syrop CH, Hammitt DG, Van Voorhis BJ. Increased
risk of monochorionic twinning associated with assisted reproduction.Fertil Steril 1993;60:510–4.
5. Alikani M, Noyes N, Cohen J, Rosenwaks Z. Monozygotic twinning inthe human is associated with the zona pellucida architecture. HumReprod 1994;9:1318–21.
6. Hershlag A, Paine T, Cooper GW, Scholl GM, Rawlinson K, Kvapil G.Monozygotic twinning associated with mechanical assisted hatching.Fertil Steril 1999;71:144–6.
7. Abusheikha N, Salha O, Sharma V, Brinsden P. Monozygotic twinningand IVF/ICSI treatment: a report of 11 cases and review of literature.Hum Reprod Update 2000;6:396–403.
8. Sills ES, Tucker MJ, Palermo GD. Assisted reproductive technologiesand monozygous twins: implications for future study and clinical prac-tice. Twin Res 2000;3:217–23.
9. Blickstein I, Jones C, Keith LG. Zygotic-splitting rates after single-embryo transfers in in vitro fertilization. N Engl J Med 2003;348:2366–7.
0. Schachter M, Raziel A, Friedler S, Strassburger D, Bern O, Ron-El R.Monozygotic twinning after assisted reproductive techniques: a phe-nomenon independent of micromanipulation. Hum Reprod 2001;16:1264–9.
1. Derom C, Vlietinck R, Derom R, Van den Berghe H, Thiery M.Increased monozygotic twinning rate after ovulation induction. Lancet1987;1:1236–8.
2. Schieve LA, Meikle SF, Peterson HB, Jeng G, Burnett NM, Wilcox LS.Does assisted hatching pose a risk for monozygotic twinning in preg-nancies conceived through in vitro fertilization? Fertil Steril 2000;74:288–94.
3. Alikani M, Cekleniak NA, Walters E, Cohen J. Monozygotic twinningfollowing assisted conception: an analysis of 81 consecutive cases.Hum Reprod 2003;18:1937–43.
4. Jain JK, Boostanfar R, Slater CC, Francis MM, Paulson RJ. Monozy-gotic twins and triplets in association with blastocyst transfer. J AssistReprod Genet 2004;21:103–7.
5. Behr B, Fisch JD, Racowsky C, Miller K, Pool TB, Milki AA. Blastocyst-ET and monozygotic twinning. J Assist Reprod Genet 2000;17:349–51.
6. da Costa AA, Abdelmassih S, de Oliveira FG, Abdelmassih V, Abdel-massih R, Nagy ZP, et al. Monozygotic twins and transfer at theblastocyst stage after ICSI. Hum Reprod 2001;16:333–6.
7. Milki AA, Jun SH, Hinckley MD, Behr B, Giudice LC, Westphal LM.Incidence of monozygotic twinning with blastocyst transfer comparedto cleavage-stage transfer. Fertil Steril 2003;79:503–6.
8. Gardner DK, Schoolcraft WB, Wagley L, Schlenker T, Stevens J, HeslaJ. A prospective randomized trial of blastocyst culture and transfer inin-vitro fertilization. Hum Reprod 1998;13:3434–40.
9. Milki AA, Fisch JD, Behr B. Two-blastocyst transfer has similarpregnancy rates and a decreased multiple gestation rate compared withthree-blastocyst transfer. Fertil Steril 1999;72:225–8.
0. Racowsky C, Jackson KV, Cekleniak NA, Fox JH, Hornstein MD,Ginsburg ES. The number of eight-cell embryos is a key determinantfor selecting day 3 or day 5 transfer. Fertil Steril 2000;73:558–64.
1. Toledo AA, Wright G, Jones AE, Smith SS, Johnson-Ward J, Brock-man WW, et al. Blastocyst transfer: a useful tool for reduction ofhigh-order multiple gestations in a human assisted reproduction pro-
gram. Am J Obstet Gynecol 2000;183:377–82.1031

2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
2. Karaki RZ, Samarraie SS, Younis NA, Lahloub TM, Ibrahim MH.Blastocyst culture and transfer: a step toward improved in vitro fertil-ization outcome. Fertil Steril 2002;77:114–8.
3. Peramo B, Ricciarelli E, Cuadros-Fernandez JM, Huguet E, HernandezER. Blastocyst transfer and monozygotic twinning. Fertil Steril 1999;72:1116–7.
4. Sheiner E, Har-Vardi I, Potashnik G. The potential association betweenblastocyst transfer and monozygotic twinning. Fertil Steril 2001;75:217–8.
5. Wright V, Schieve LA, Vahratian A, Reynolds MA. Monozygotictwinning associated with day 5 embryo transfer in pregnancies con-ceived after IVF. Hum Reprod 2004;19:1831–6.
6. Menezo YJ, Sakkas D. Monozygotic twinning: is it related to apoptosisin the embryo? Hum Reprod 2002;17:247–8.
7. Cassuto G, Chavrier M, Menezo Y. Culture conditions and not pro-longed culture time are responsible for monozygotic twinning in humanin vitro fertilization. Fertil Steril 2003;80:462–3.
8. Sheiner E, Kivilevitch Z, Levitas E, Sonin Y, Albotiano S, Har-VardiI. Monozygotic twins following blastocyst transfer: a report of twocases. Eur J Obstet Gynecol Reprod Biol 2001;98:135–8.
9. Rijnders PM vOH, Jansen CA. Increased incidence of monozygotictwinning in following the transfer of blastocysts in human IVF/ICSI.Fertil Steril 1998;70:15–6.
0. Elizur SE, Levron J, Shrim A, Sivan E, Dor J, Shulman A. Monozy-
gotic twinning is not associated with zona pellucida micromanipulation1032 Moayeri et al. Monozygotic twinning in blastocyst trans
procedures but increases with high-order multiple pregnancies. FertilSteril 2004;82:500–1.
1. Slotnick RN, Ortega JE. Monoamniotic twinning and zona manipula-tion: a survey of U.S. IVF centers correlating zona manipulation pro-cedures and high-risk twinning frequency. J Assist Reprod Genet 1996;13:381–5.
2. Saito H, Tsutsumi O, Noda Y, Ibuki Y, Hiroi M. Do assisted repro-ductive technologies have effects on the demography of monozygotictwinning? Fertil Steril 2000;74:178–9.
3. Blickstein I, Verhoeven HC, Keith LG. Zygotic splitting after assistedreproduction. N Engl J Med 1999;340:738–9.
4. Frankfurter D, Trimarchi J, Hackett R, Meng L, Keefe D. Monozygoticpregnancies from transfers of zona-free blastocysts. Fertil Steril 2004;82:483–5.
5. Hsu YC, Gonda MA. Monozygotic twin formation in mouse embryosin vitro. Science 1980;209:605–6.
6. Chida S. Monozygous double inner cell masses in mouse blastocystsfollowing fertilization in vitro and in vivo. J In Vitro Fert EmbryoTransf 1990;7:177–9.
7. Meintjes M, Guerami AR, Rodriquez JA, Crider-Prikle SS, Madden JD.Prospective identification of an in vitro-assisted monozygotic preg-nancy based on a double-inner-cell-mass blastocyst. Fertil Steril 2001;76:172S–3S.
8. Steinman G. Mechanisms of twinning. IV. Sex pregerence and lacta-
tion. J Reprod Med 2001;46:1003–7.fer Vol. 87, No. 5, May 2007

T1adtgowic
ch
RR
0d
Oocyte karyotyping by comparative genomichybrydization provides a highly reliable method forselecting “competent” embryos, markedly improvingin vitro fertilization outcome: a multiphase studyGeoffrey Sher, M.D.,a,b Levent Keskintepe, Ph.D.,a Meral Keskintepe, Ph.D.,c
Mike Ginsburg, M.S.,c Ghanima Maassarani, Dr. Med.,a Tahsin Yakut, M.D.,d
Volkan Baltaci, M.D.,e Dirk Kotze, M.S.,a and Evrim Unsal, B.S.e
a Sher Institute for Reproductive Medicine, Las Vegas; b Department of Obstetrics and Gynecology, University of NevadaSchool of Medicine, Reno; c ReproCure Reproductive Genetics, Las Vegas, Nevada; d School of Medicine, University ofUludag, Bursa; and e Gen-ART, Ankara, Turkey
Objective: To assess the karyotypic relationship between prefertilized/postfertilized oocytes and embryos usingcomparative genomic hybridization (CGH) on polar body-1 (PB-1), PB2, and blastomere biopsies and to evaluateIVF outcomes after transfer of blastocysts derived from euploid oocytes.Design: Prospective cohort.Setting: Medical center.Patient(s): Phase1: Fourteen oocyte donors (23–29 years). Phase 2: Forty-one healthy embryo recipients aged29–43 years free of endometrial implantation dysfunction. In 30 cases own eggs were used. Eleven women useddonated oocytes.Intervention(s): Phase 1: PB-1 biopsies followed intracytoplasmic sperm injection (ICSI), PB-2, and day 3blastomere biopsies. Phase 2: PB-1 biopsy followed by ICSI using normal sperm and the subsequent embryotransfer of �2 blastocysts derived from euploid oocytes. Comparative genomic hybridization on all DNA derivedfrom phase 1 and 2 biopsies.Main Outcome Measure(s): Pregnancy and implantation rate.Result(s): Phase 1: 39% of oocytes and 88% of zygotes were euploid; �95% progressed to blastocysts.Mosaicism as evidenced by euploid oocytes developing into aneuploid zygotes or embryos occurred in 13% ofconcepti. Phase 2: Six of 30 women using own eggs, who failed to produce euploid oocytes, were cancelled.Thirty-five women underwent embryo transfers with �2 (mean, 1.3 � 0.7) blastocysts derived from euploidoocytes. The ongoing pregnancy/implantation rates per embryo transfer were 74% and 82%, respectively.Conclusion(s): Transferring euploid embryos markedly improved IVF outcome. These findings, if corroborated,could initiate a paradigm shift in assisted reproductive technology (ART). (Fertil Steril� 2007;87:1033–40. ©2007 by American Society for Reproductive Medicine.)
Key Words: Comparative genomic hybridization, karyotype, embryo transfer, pregnancy, implantation
(cf
npss(m
wcno
he earliest attempts at karyotyping human oocytes in the early970s yielded limited data due to the inadequacy of materialnd the limitations of available technology (1). In the ensuingecade the introduction and development of IVF techniques, forhe first time, made human oocytes readily available for cyto-enetic analysis, thereby precipitating a resurgence of interest inocyte karyotyping (2, 3). The numerous studies that followedere severely hampered by limited knowledge and technical
nability to optimize chromosome preparations or achieve ac-urate chromosome identification.
However, since the mid-90s, the application of sophisti-ated molecular cytogenetic techniques to human oocytesas developed significantly. The development of polar body
eceived June 16, 2006; revised and accepted August 18, 2006.eprint requests: Geoffrey Sher, M.D., Sher Institute for ReproductiveMedicine, Las Vegas, 3121 S. Maryland Parkway, Suite 300, Las Vegas,
eNV 89109 (FAX: 702-892-9666; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.08.108 Copyright ©2007 American Soc
PB) biopsy techniques using sequential, multicolor fluores-ent in situ hybridization (FISH) labeling was a giant steporward (4–6).
Unfortunately, FISH has serious limitations in that it doesot permit access to full karyotyping of all 23 chromosomeairs. The recent introduction of more advanced techniques,uch as comparative genomic hybridization (CGH) (7–9),pectral karyotyping (10), primed in situ labeling (PRINS)11), and peptide nucleic acid (PNA) (12) techniques, haveade karyotyping of all 23 chromosome pairs possible.
These new methodologies proved to be rather intensiveith respect to time, technology, and cost. Due to this, their
linical application has been severely circumscribed, butevertheless, a large body of data has accumulated as a resultf academic studies performed using these techniques.
Although it has long been assumed the karyotype of an
mbryo is in large part a function of the karyotype of its1033Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

oi“ocdi(tcoh
avpmpdmaoeclep
hnnccrcUmpovn
atPtoo
MNpa
PPacfhshbpsbafb6p1sb
P(TedbtoaahtofpsOPfTcw4aemtmnwow
Ag
ocyte of origin, and that an embryo’s karyotype determinests potential to propagate a viable, normal pregnancy (i.e., itscompetence”), the exact propagation of karyotype fromocyte to embryo has until now remained a subject ofontention (12, 13). Most authorities believe that embryoserived from aneuploid oocytes (meiotic aneuploidy) willnevitably lead to embryo aneuploidy and “incompetence”14, 15). However, the role of mosaicism (i.e., postfertiliza-ion, mitotic aneuploidy) in the propagation of embryo in-ompetence and the extent to which an advanced embryo canvercome the ill effects of mosaicism, remains a subject ofot debate (16–18).
Needless to say, both the incidence and origin of embryoneuploidy (meiotic vs. mitotic) and the potential of a de-eloping embryo to overcome the effects of mitotic aneu-loidy (mosaicism) are highly relevant to the ultimate deter-ination of embryo competence. If embryo aneuploidy is
rimarily a function of meiotic aneuploidy, and it can beemonstrated conclusively that an oocyte’s karyotype is, inost cases, linearly perpetuated in its postfertilized zygote
nd embryo, then evidence gained through full karyotypingf the PB-1 would provide a high level of confidence that thembryo in question is most likely to be euploid and thusompetent. Such knowledge could herald a time where se-ectively transferring only one embryo to a receptive uterinenvironment would consistently result in a single viableregnancy.
Such ability could transform many accepted techniques inuman reproduction. It would rapidly reverse currently stag-ant IVF success rates, eliminate the risk of multiple preg-ancies, and minimize the occurrence of first trimester mis-arriages (mostly due to aneuploidy), as well as manyhromosomal birth defects. Improvement in IVF successates might also lead to a reduction in the cost per IVF baby,urrently estimated to be between $70,000 to $100,000 in thenited States. All of these factors may serve as a strongotivating influence on health insurance providers to im-
rove coverage for IVF services. In total, this new technol-gy could make assisted reproductive technology (ART) aiable option to a host of women who currently could/wouldot consider it.
A two-phase study was completed. In Phase 1 we evalu-ted whether a linear karyotypic correlation exists betweenhe prefertilized and postfertilized oocyte and embryo and, inhase 2, we assessed how and to what extent the selective
ransfer of no more than two blastocysts derived from euploidocytes, would affect IVF implantation potential and viablengoing pregnancy rates (beyond the first trimester).
ETHODS AND MATERIALSo IRB approval was obtained for this research, but allarticipants were fully informed and signed a consent form,
nd all met the requirements of the 1975 Helsinki guidelines. t1034 Sher et al. Karyotyping pre- and postfertilized oocytes
atientshase 1 Fourteen normally ovulating healthy oocyte donorsged 23–29 years (mean age 27.5 � 5.7 years) were re-ruited from a licensed agency, screened, counseled, andully informed. All women undergoing controlled ovarianyperstimulation (COH) were pretreated as previously de-cribed (19). A total of 132 mature (MII) oocytes werearvested. All oocytes underwent first polar body (PB-1)iopsy. Thereupon each MII oocyte underwent intracyto-lasmic sperm injection (ICSI) using sperm derived fromeven normospermic donors recruited from a licensed spermank. Oocyte injection and embryo culture were performeds described elsewhere (20). The PB-2 biopsy was per-ormed approximately 16 hours after ICSI. All cleaved em-ryos were subjected to single cell blastomere biopsy at4–72 hours after ICSI, and then incubated for an additionaleriod of 48–72 hours. Embryos that progressed to the grade–2 blastocysts stage were cryopreserved for future dispen-ation. The DNA specimens derived from PB-1, PB-2, andlastomeres were fully karyotyped using CGH.
hase 2 Forty-one women ranging in age from 29–43 yearsmean age 37.5 � 5.5 years) were included in this study.hirty patients used their own eggs. In eleven cases, thembryos resulted from fertilization of oocytes derived fromonors. All recipients [1] had normal, regular uterine cavitiesased on hysterosonography or hysteroscopy performed inhe preceding 12 months, [2] tested negative for alloimmuner autoimmune immunologic implantation dysfunction (i.e.,ntiphospholipid antibodies, natural killer cell activation,nd/or shared HLA similarities with their partners), and [3]ad endometrial linings that measured �9.0 mm in sagittalhickness before embryo transfer. In 30 cases the patients’wn oocytes were used. COH was performed as describedor patients in Phase 1. After egg retrieval (ER), all meta-hase II (MII) oocytes underwent PB-1 biopsy and the DNApecimens so derived were fully karyotyped using CGH.ocyte injection and embryo culture were performed as inhase 1 (20). Only fresh blastocysts (�2 per embryo trans-er) derived from euploid oocytes of origin were transferred.he remaining (abnormal) blastocysts were discarded. Inases of oocyte donation, the recipients’ endometrial liningsere prepared with E2 valerate administered at a dosage of–8 mg IM every 3 days. The exact dosage was adjusted tochieve a plasma E2 concentration of 500–1,000 pg/mL and anndometrial lining measuring �9 mm. Intramuscular P (100g/d IM) was administered starting 6 days before embryo
ransfer and continued with twice weekly IM Delestrogen ad-inistrations until the 10th week of pregnancy or until preg-
ancy was discounted. Daily, oral dexamethasone (0.75 mg)as given throughout the cycle until a negative pregnancy testr the completion of the 10th week of pregnancy, whereupon itas tailed off over a period of 1 week and discontinued.
An informed consent form for embryo transfer based onmerican Society For Reproductive Medicine (ASRM)uidelines was signed. Up to two competent blastocysts were
ransferred per woman (mean 1.3 � 0.7 per embryo trans-with CGH Vol. 87, No. 5, May 2007

fbwt(Stdtg
CEDfo2(a5
GmaLeebt9aN
NfiN
PGTpe(DqtcCp
IT4pom
uCmoosD
uR(ofismn
SDtu
RPTa8eegmdetwNgse
Iea
9abo
cid
F
er). The cervical canal was cleansed and gently flushedefore transfer using warmed culture media. All embryosere transferred atraumatically on day 5 of culture under
ransvaginal ultrasound guidance using a flexible catheterWallace, Smith Medical, Kent, UK) in �20 �L of media.erum hCG levels were measured 7 and 9 days after blas-
ocyst embryo transfer. Two values above 5.0 IU (doublinguring 48 hours) were considered positive. Ongoing gesta-ion was defined by fetal heart activity and appropriaterowth at 12 weeks of gestation.
omparative Genomic Hybridizationxtraction and amplification of genomic DNA GenomicNA was obtained by laser dissection and needle aspiration
rom three sources: oocyte PB-1, oocyte PB-2, and embry-nic blastomeres. The cellular material was aspirated into a00-�L thin-walled polymerase chain reaction (PCR) tubecatalog #82006-602; VWR, West Chester, PA) for analysisnd amplification using the Qiagen Repli-g kit (catalog9045) as described in the manufacturers’ manual.
enomic DNA confirmation and quantification For confir-ation of whole genomic amplification products, 5-�L re-
ction aliquots were mixed with 1 �L 6X Blue-Orangeoading Dye (Promega G1881, Mountain View, CA) andlectrophoresed through a 1.0% agarose gel containing 0.1%thidium bromide in TBE buffer (90 mM Tris-HCl, 90 mMoric acid, and 2 mM EDTA, pH 8.0). For quantification ofhe genomic DNA, 5-�L reaction aliquots were diluted with5 �L of molecular biology-grade, nuclease-free water andnalyzed with an Eppendorf BioPhotometer (Westbury,Y).
ick translation of genomic DNA The whole genomic ampli-cation products were fluorescently labeled using the Vysisick Translation Kit (catalog 32-801024; Des Plaines, IL).
robe Preparation and Comparativeenomic Hybridizationhe Spectrum Green-labeled probes were purified by ethanolrecipitation. Briefly, 10 �L/200 ng nick-translated refer-nce DNA, 1 �L/100 ng SprectrumRed reference DNAVysis 32-80423 or 32-804024), and 10 �L/10 �g Cot-1NA (Vysis 32-800028) used to suppress repetitive se-uences and prevent nonspecific hybridization, were addedo a 1.5-�L microcentrifuge tube, and hybridization wasarried out as instructed in the manufacturers’ manual. TheGH normal metaphase slides (Vysis 30-806010) were pre-ared following the manufacturer’s protocol.
mage Capture and Analysishe slides were mounted in DAPI II (Vysis) containing=,6-diamidino-2-phenylindole and antifade. Metaphasereparations were examined using an Olympus BX 61 flu-rescence microscope (San Jose, CA). An average of 10
etaphases per hybridization were captured and analyzed fertility and Sterility�
sing Cytovision v3.7 software (Applied Imaging, San Jose,A). The average red:green fluorescence ratio for each chro-osome was determined by the CGH software. Deviations
f the ratio �0.8 (where the test DNA is under-represented)r �1.2 (where the test DNA is over-represented) werecored as loss or gain of material in the test or referenceNA, respectively.
The following optical filters visualized the fluorochromessed in the hybridization: a filter set specific for DAPI, Texased (catalog 30-150491) and FITC (fluorescein isothiocyanate)
catalog 30-150291) to view the counterstain; Spectrum-Redr Spectrum-Green DNA, respectively, a triple bandpasslter set designed to simultaneously excite and emit lightpecific for DAPI. Telomeric, centromeric, and heterochro-atic regions were excluded from the analysis for being
oninformative.
tatistical Analysisifferences between groups were evaluated using Student’s
-tests. Differences in rates and proportions were evaluatedsing the �2 test. Significance was set at P�.05.
ESULTShase 1able 1 demonstrates that 65% (60/92) of the MII oocytes wereneuploid, whereas 35% (32/92) were euploid. Approximately8% (28/32) of the postfertilized euploid oocytes were likewiseuploid and 96% (27/28) of these developed into euploidmbryos. Ninety-three percent (25/27) of the latter pro-ressed to grade 1–2, day 5–6 blastocysts. Thus, approxi-ately 89% (25/28) of postfertilized euploid MII oocytes
eveloped into grade 1–2 blastocysts, all of which were alsouploid. In comparison, the postfertilized aneuploid oocyte-o-blastocyst conversion rate was 20% (11/54), all of whichere aneuploid (P�.05, confidence interval [CI] � 1–4).inety-three percent (25/27) of euploid embryos progressed torade 1–2 blastocysts as compared to 21% (11/52) for conver-ion of aneuploid embryos (P�.05, CI � 1–4). The overallmbryo-to-blastocyst conversion rate was 46% (36/79).
Approximately 13% (4/32) of euploid MII oocytes, afterCSI, developed into one or more aneuploid zygotes ormbryos. This would suggest that the incidence of mitoticneuploidy (mosaicism) was about 13% in this study.
Forty-three embryos failed to progress to blastocyst. In5% of these cases (41/43) the embryos of origin wereneuploid. In contrast, only 3% (2/43) of cases where em-ryos failed to reach blastocysts, involved cases where theriginal embryos were euploid.
Table 2 illustrates that the common aneuploidies involvedhromosomes 2, 4, 5, 9, 10, 12, 16, and 22, with abnormal-ties in chromosomes 4, 5, 16, and 22 the most prevalent. Ourata further illustrate that in general trisomies were more
requently encountered than monosomies (57% vs. 43%) and1035

t(
PTpeT(eisoTpp(wwk
DNcc
luetmcabp2mmt
ca6sfYnmbmf
hat of 72 oocytes examined, 48% had complex aneuploidies�1 chromosome affected).
hase 2able 3 presents the demographic characteristics of the 41atients treated in Phase 2. Six women who used their ownggs did not have euploid embryos available for transfer.hirty-five women each had �2 blastocysts transferred
mean 1.3 � 0.7 per embryo transfer). The mean age of thegg providers was 37.5 � 5.5 years. The indications for IVFn the 35 women who underwent embryo transfers are pre-ented in Table 3. There were 30 cases where the patients’wn eggs were fertilized and 11 cases of ovum donation.wenty-eight (80%) ultrasound-confirmed pregnancies com-rised 19 (68%) singletons and 9 (32%) twins. The ongoingregnancy rate (PR) beyond the first trimester was 74%26/35) and the implantation rate per blastocyst transferredas 82% (37/45). There were 2 miscarriages; one of whichas associated with monosomy X and the other had a normalaryotype.
ISCUSSIONumerical chromosome irregularities (aneuploidies) are
ommon in early human embryos and contribute signifi-
TABLE 1Correlation between the karyotype of embryos aorigin: study involving serial comparative genom
% of MII oocytes successfully karyotyped% MII oocytes that were aneuploid% MII oocytes that were euploid% euploid MII oocytes propagated euploid zygotes% MII aneuploid oocytes propagated aneuploid zyg% euploid oocytes propagated aneuploid zygotes% aneuploid oocytes propagated euploid zygotes% zygotes successfully analyzed% zygotes that were euploid% zygotes that were aneuploid% euploid zygotes propagated euploid embryos% euploid zygotes propagated aneuploid embryos% aneuploid zygotes propagated aneuploid embryo% embryo biopsies successfully karyotyped% embryos that were euploid% embryos that were aneuploid% embryos that propagated G1-2 blastocysts% euploid embryos that propagated grade1–2 blast% aneuploid embryos that propagated grade 1–2 bSher. Karyotyping pre- and postfertilized oocytes with CGH. Fertil Steril 2007.
antly to implantation failure as well as to early pregnancy w
1036 Sher et al. Karyotyping pre- and postfertilized oocytes
oss (13, 21). Although the spermatozoon certainly contrib-tes, it is primarily the oocyte that is the driving force in thestablishment of embryo competence (6, 7, 9). The karyo-ype of the mature (MII) oocyte has emerged as being theost important single determinant of oocyte developmental
ompetence with aneuploid oocytes rendered unfertilizable,rresting at various stages after fertilization, producing em-ryos that fail to implant, resulting in early miscarriages, orroducing a variety of chromosomal birth defects (12, 13,2). Assessment of embryo morphology with phase-contrasticroscopy, although helpful, fails to provide reliable infor-ation by which to define the developmental competence of
he embryo (23).
Traditional karyotyping of metaphase chromosomes usingommercially available FISH is too inefficient and unreliablet the single cell level to be of practical use in fresh IVF (5,, 8, 24). Although widely used to identify embryo chromo-ome irregularities, FISH is of limited value because only aew chromosomes can be identified in each cell (usually X,, 13, 15, 16, 18, 21, and 22). An attempt to increase theumber of chromosomes analyzed by simultaneously addingore FISH probes, reduces the accuracy of differentiating
etween various chromosomal elements and can lead toisdiagnosis (25). The matter is further complicated by the
act that the chromosome probes used in commercial FISH
he prefertilized and postfertilized oocytes ofybridization on PB-1, PB-2, and blastomeres.
%
PB-1 PB-2 Blastomere
91 (92/102)65 (60/92)35 (32/92)88 (28/32)95 (57/60)9 (3/32)0 (0/60)
96 (82/85)34 (28/82)62 (54/82)96 (27/28)4 (1/28)
100 (54/54)96 (79/82)34 (27/79)66 (52/79)46 (36/79)
sts 93 (25/27)cysts 21 (11/52)
nd tic h
otes
s
ocylasto
ere designed to detect aneuploidies involved in spontane-
with CGH Vol. 87, No. 5, May 2007

osa
kecabC
eluczittabp
ic
adbfofa(nsayrp
(z(
F
us miscarriages, not necessarily the often lethal chromo-omal aneuploidies that lead to dysfunctional embryogenesisnd failed implantation.
Newer technologies such as CGH, facilitate single cellaryotyping (7, 9). Comparative genomic hybridization, bothnumerates and provides a comprehensive assessment of eachhromosome, thereby identifying breakages and even partialneuploidies. There have been reports of healthy IVF babiesorn after preimplantation genetic diagnosis (PGD) using fullGH karyotyping (26).
An often cited limitation of CGH is that it cannot differ-ntiate between certain ploidy errors, such as haploidy, trip-oidy, and tetraploidy. However, this would not preclude itsse in IVF, where such defects are readily identified bylosely observing the number of pronuclei present in theygote. The main problems associated with the use of CGHn determining the ploidy of blastomeres are: [1] it is veryime consuming, taking at least 5–6 days to complete, suchhat the embryos so tested would have to be cryopreservednd stored until CGH results were available and thereupone thawed for subsequent transfer to the uterus, [2] the
TABLE 2Spectrum of oocyte karyotypic abnormalities deton DNA derived from PB-1, PB-2, and blastomer
Autosomalchromosomes
Monosomy
PB-1 PB-2
A 1 7 42 123 34 7 155 767 88 39
10 121112 1213 7 81415 816 1017 7 818 719 2 820 821 8 422 15 12
Sher. Karyotyping pre- and postfertilized oocytes with CGH. Fertil Steril 2007.
rocess itself is expensive, and [3] it is very technology e
ertility and Sterility�
ntensive (27, 28). These factors have all but precludedlinical use of CGH for blastomere PGD in clinical IVF.
In 2004, Gutiérrez-Mateo et al. (29) reported an oocyteneuploidy incidence of 48% after CGH performed on DNAerived from 25 oocytes’ first PBs. In a separate study usingoth CGH and FISH performed on 54 oocytes (30) derivedrom 36 women, the same researchers found the incidence ofocyte aneuploidy to be 57% and the chromosomes morerequently involved in aneuploidy to be chromosomes 1, 4,nd 22, followed by chromosome 16. Twenty-five percent25%) of the aneuploid doublets would have been misdiag-osed as normal using FISH with probes for nine chromo-omes. Our findings indicate that the incidence of oocyteneuploidy, even in young women (mean age 27.0 � 2.5ears), is considerably higher (i.e., 65%). Our study furtherevealed aneuploidies of chromosomes 4, 5, 16, and 22, andredominantly in the form of trisomies.
Table 1 depicts that aneuploid oocytes fertilized by ICSIusing normal sperm), consistently propagated aneuploidygotes (57/57) as well as embryos (57/57), and that in 87%27/31) of cases, euploid oocytes developed into euploid
ed by comparative genomic hybridization (CGH)opsies of human oocytes.
Trisomy (%)
stomere PB-1 PB-2 Blastomere
7 92 27 94 11 13
4 9 13 189 2
9 7 44 4 2
13 77 47 24 9 47 7 49 74 2 2
29 7 44 9 2 24 44 4 9 24 2 2 98 2
29 2 2 7
ecte bi
(%)
Bla
mbryos. These findings establish that embryo ploidy is
1037

lctia2
tlbaitwow
aosadei(ita
rs
hwodaot1la
Prassttninat
Paphcs
inearly propagated after fertilization, suggesting that itould be possible, by selecting embryos derived from karyo-ypically normal oocytes to improve IVF outcome. It alsollustrates that euploid embryos are far more likely to prop-gate blastocysts than were aneuploid embryos (93% vs.1%).
In our Phase study, 95% of embryos that failed to progresso blastocysts were aneuploid. This latter observation chal-enges the widely held belief that embryos are better offeing transferred earlier, in the cleaved state (i.e., 2–3 daysfter fertilization) rather than later, as blastocysts. This is anmportant observation because, if confirmed by other inves-igators, it could establish a rational basis for routinelyaiting for embryos to attain the blastocyst stage of devel-pment before embryo transfer as many aneuploid embryosould be culled out in the process.
Aneuploidy, which arises during meiosis I, will inevitablyffect all of the cells of the embryo. The rank and the numberf chromosomes so affected would likely impact embryourvival, the incidence of miscarriage, as well as the risk ofbirth defect (31). Conversely, embryo aneuploidy arising
uring mitosis (i.e., mosaicism), depending on the stage ofmbryonic development at which it occurs, is often compat-ble with the subsequent propagation of a viable offspring32). Chromosome studies in blastocysts indicate that mosa-cism is in fact quite a common finding in concepti and thathe preponderance of aneuploid cells might decrease withdvancing development (33).
The high incidence of oocyte aneuploidy (65%) in theelatively young population group comprising our Phase 1
TABLE 3Demographics and characteristics in 29 patients
Number of women (n)Number of women who did not have ETNumber of women who underwent ETAge (y)Number of prior IVF failuresIndications for IVF with own eggs in women who un
o Tubal factoro Endometriosiso Age ( �39 y)o Unexplainedo Ovum donation
Number of blastocysts transferred per embryo transNumber of ongoing gestations per embryo transferNumber of singleton pregnanciesNumber of twin pregnanciesNumber of 1st trimester pregnancy lossesImplantation rate/blastocyst transferredSher. Karyotyping pre- and postfertilized oocytes with CGH. Fertil Steril 2007.
tudy helps to explain the relatively low fecundicity of e
1038 Sher et al. Karyotyping pre- and postfertilized oocytes
umans. Our findings also clearly indicate that in youngomen with fertile male partners, it is the karyotype of theocyte, rather than that of the spermatozoon that likelyetermines the embryo’s ploidy and competence. We havelso confirmed that oocyte karyotype is in the vast majorityf cases linearly conveyed to the zygote and embryo, andhat although mitotic aneuploidy (mosaicism) occurred in3% of cases, its disruptive impact on embryogenesis isikely to be much less significant than meiotic (oocyte)neuploidy.
The relatively low occurrence of mitotic aneuploidy in ourhase 1 study might, at least in part, be attributable to theelatively young age of the oocyte providers and the fact thatll oocytes were fertilized with sperm derived from normo-permic males. It is equally plausible to conclude that mo-aicism is a less common contributor to embryo aneuploidyhan hitherto believed. Moreover, the later in embryogenesishat the mitotic aneuploidy insult occurs, the fewer theumber of aneuploid cells, and the lower the likelihood thatt might compromise the offspring. We postulate that theumber and rank of chromosomes involved might also playsignificant role in determining the nature and severity of
he mitotic aneuploidy-related insult.
The single cell amplification technique employed in ourhase 1 and Phase 2 studies yielded inconclusive results inbout 15% of analyses performed. We have found that it isossible to reduce this incidence to �5% when repeatedybridization can be performed as needed. The fact thatomplete CGH analysis takes 5– 6 days to complete pre-ents a formidable barrier to the routine adaptation of such
ticipating in Phase 2.
416 (15%)
35 (86%)37.5 � 5.51.9 � 1.4
went Embryo transfer7567
101.3 � 0.7 (45/35)
26 (74%)19 (68%)9 (32%)
2/28 (7%)37/45 (82%)
par
der
fer
gg/embryo competency testing in the conventional, fresh
with CGH Vol. 87, No. 5, May 2007

IfmsltpbenpbVp
tbncmmvcK
dnIlaflwitetpt
rat
fcpo
Aapw
R
1
1
1
1
1
1
1
1
1
1
2
2
F
VF setting, where there is rarely more than 5 days availablerom performance of ER to fresh blastocyst transfer. Clearly,ore latitude in time is needed to allow for transportation of
pecimens from the IVF laboratory to a centralized CGHaboratory, as well as for repeated CGH testing in the eventhat initial analyses fail to yield conclusive results. Thisroblem could readily be overcome by temporarily cryo-anking blastocysts derived from euploid oocytes and/ormbryos in preparation for transfer during a subsequentatural or hormone replacement cycle. We predict that therocess of separating the cycle of ER/ICSI/PGD-CGH/andlastocyst vitrification from the ET cycle (i.e, Staggered-initro Fertilization [St-IVF]) will eventually find a permanentlace in the ART therapeutic armamentarium.
The recent introduction of ultra-rapid freezing (vitrifica-ion) (34) has markedly improved post-warming survival ofoth oocytes and embryos, as well as their subsequent preg-ancy-generating potential. As such it represents a signifi-ant improvement over hitherto conventional slow-freezingethods, which commonly resulted in intracellular ice for-ation and damage to the cytoskeleton of the cell. Thus,
itrification is ideally suited for use in St-IVF. Studies areurrently underway in both the United States and the Unitedingdom to evaluate ST-IVF.
The results of Phase 2 confirm that by selecting embryoserived from euploid eggs, it is possible to minimize theumber of embryos transferred and significantly improvingVF outcome. Since most early pregnancy loss, as well asate chromosomal fetal defects are attributable to embryoneuploidy, our approach to selecting competent embryosor transfer (or modifications thereof), if confirmed througharger studies, could establish PB-1 and/or blastomere biopsyith CGH as a valuable method by which to significantly
mprove IVF success rates, minimize the likelihood of mul-iple pregnancies, and bring us closer to the goal of onembryo, one baby. At the same time, it would likely reducehe incidence of early pregnancy loss and meiotic aneu-loidy-related chromosomal defects, regardless of the age ofhe egg provider.
These findings might also improve the current disappointingesults reported with oocyte cryopreservation, as it is possible,nd perhaps even likely, that euploid oocytes would betterolerate cryopreservation than would aneuploid oocytes.
Finally, an ability to identify euploid oocytes, which uponertilization would propagate euploid embryos and blasto-ysts, might also provide euploid inner cell mass cells, andresent a much needed “shot in the arm” for human embry-nic stem cell research (35).
cknowledgment: The authors wish to recognize and express our appreci-tion to Sharon Poon, M.D., who graciously and selflessly donated herrofessional time and services as an anesthesiologist, gratis and without
hom this study would not have been possible.ertility and Sterility�
EFERENCES1. Mikamo K. Anatomic and chromosomal anomalies in spontaneous
abortion. Possible correlation with over-ripeness of oocytes. Am JObstet Gynecol 1970;106:243–54.
2. Baranov VS, Dyban AP, Chebotar NA. Preimplantation development ofmouse embryos with monosomy of autosome No. 17. Ontogenez 1980;11:148–59.
3. Jagiello G, Fang JS. A pachytene map of the mouse oocyte. Chromo-soma 1980;77:113–21.
4. Clement-Sengewald A, Buchholz T, Schutze K. Laser microdissectionas a new approach to pre-fertilization genetic diagnosis. Pathobiology2000;68:232–6.
5. Martini E, Flaherty SP, Swann NJ, Matthews CD, Ramaekers FC,Geraedts JP. FISH analysis of six chromosomes in unfertilized humanoocytes after polar body removal. J Assist Reprod Genet 2000;17:276–83.
6. Gitlin SA, Gibbons WE, Gosden RG. Oocyte biology and geneticsrevelations from polar bodies. Reprod Biomed Online 2003;6:403–9.
7. Le Caignec C, Spits C, Sermon K, De Rycke M, Thienpont B, DebrockS, et al. Single-cell chromosomal imbalances detection by array CGH.Nucleic Acids Res 2006;34:e68.
8. Wilton L. Preimplantation genetic diagnosis and chromosome analysisof blastomeres using comparative genomic hybridization. Hum ReprodUpdate 2005;11:33–41.
9. Wells D, Levy B. Cytogenetics in reproductive medicine: the contri-bution of comparative genomic hybridization (CGH). Bioassays 2003;25:289–300.
0. Murthy SK, Demetrick DJ. New approaches to fluorescence in situhybridization. Methods Mol Biol 2006;319:237–59.
1. Chen CP, Lin SP, Lin CC, Li YC, Hsieh LJ, Huang JK, et al. Spectralkaryotyping and fluorescence in situ hybridization analysis of de novopartial trisomy 7p (7p21.2-�pter) and partial monosomy 12q(12q24.33-�qter). Genet Couns 2006;17:57–63.
2. Pellestor F, Andreo B, Anahory T, Hamamah S. The occurrence ofaneuploidy in human: lessons from the cytogenetic studies of humanoocytes. Eur J Med Genet 2006;49:103–16.
3. Pellestor F, Andreo B, Anahory T, Dechaud H, Hedon B, Hamamah S.The cytogenetics of human oocytes: 40 years of progress. GynecolObstet Fertil 2005;33:283–92.
4. Fragouli E, Wells D, Whalley KM, Mills JA, Faed MJ, Delhanty JD.Increased susceptibility to maternal aneuploidy demonstrated by com-parative genomic hybridization analysis of human MII oocytes and firstpolar bodies. Cytogenet Genome Res 2006;114:30–8.
5. Wang H, Hoog C. Structural damage to meiotic chromosomes impairsDNA recombination and checkpoint control in mammalian oocytes.J Cell Biol 2006;173:485–95.
6. Lightfoot DA, Kouznetsova A, Mahdy E, Wilbertz J, Hoog C. The fateof mosaic aneuploid embryos during mouse development. Dev Biol2006;289:384–94.
7. Delhanty JD. Mechanisms of aneuploidy induction in human oogenesisand early embryogenesis. Cytogenet Genome Res 2005;111:237–44.
8. Baart EB, Martini E, van den Berg I, Macklon NS, Galjaard RJ, FauserBC, et al. Preimplantation genetic screening reveals a high incidence ofaneuploidy and mosaicism in embryos from young women undergoingIVF. Hum Reprod 2006;21:223–33.
9. Sher G, Fisch JD. Effect of vaginal sildenafil on the outcome of in vitrofertilization (IVF) after multiple IVF failures attributed to poor endo-metrial development. Fertil Steril 2002;78:1073–6.
0. Sher G, Keskintepe L, Nouriani M, Roussev R, Batzofin J. Expressionof sHLA-G in supernatants of individually cultured 46-h embryos: apotentially valuable indicator of “embryo competency” and IVF out-come. Reprod Biomed Online 2004;9:74–8.
1. Selva J, Bergere M, Molina-Gomes D, Hammoud I, Lombroso R,Vialard F. Contribution of first polar body analysis to understandingof human aneuploidy mechanism. Bull Acad Natl Med 2005;189:
1761–72.1039

2
2
2
2
2
2
2
2
3
3
3
3
3
3
2. Montag M, Schimming T, van der Ven H. Spindle imaging in humanoocytes: the impact of the meiotic cell cycle. Reprod Biomed Online2006;12:442–6.
3. Ebner T, Moser M, Tews G. Is oocyte morphology prognostic ofembryo developmental potential after ICSI? Reprod Biomed Online2006;12:507–12.
4. Hewitson L, Simerly C, Schatten G. Cytoskeletal aspects of assistedfertilization. Semin Reprod Med 2000;182:151–9.
5. Murthy SK, Demetrick DJ. New approaches to fluorescence in situhybridization. Methods Mol Biol 2006;319:237–59.
6. Wilton L, Voullaire L, Sargeant P, Williamson R, McBain J. Preim-plantation aneuploidy screening using comparative genomic hybridiza-tion or fluorescence in situ hybridization of embryos from patients withrecurrent implantation failure. Fertil Steril 2003;80:860–8.
7. Wells D, Escudero T, Levy B, Hirschhorn K, Delhanty JD, Munne S.First clinical application of comparative genomic hybridization andpolar body testing for preimplantation genetic diagnosis of aneuploidy.Fertil Steril 2002;78:543–9.
8. Voullaire L, Wilton L, McBain J, Callaghan T, Williamson R. Chro-mosome abnormalities identified by comparative genomic hybridiza-tion in embryos from women with repeated implantation failure. Mol
Hum Reprod 2002;8:1035–41.1040 Sher et al. Karyotyping pre- and postfertilized oocytes
9. Gutiérrez-Mateo C, Benet J, Wells D, Colls P, Bermudez MG, Sanchez-Garcia JF, et al. Aneuploidy study of human oocytes first polar bodycomparative genomic hybridization and metaphase II fluorescence insitu hybridization analysis. Hum Reprod 2004;19:2859–68.
0. Gutiérrez-Mateo C, Benet J, Wells D, Colls P, Bermudez MG, Sanchez-Garcia JF, et al. Aneuploidy study of human oocytes first polar bodycomparative genomic hybridization and metaphase II fluorescence insitu hybridization analysis. Hum Reprod 2004;19:2859–68.
1. Warburton D, Kinney A. Chromosomal differences in susceptibility tomeiotic aneuploidy. Environ Mol Mutagen 1996;28:237–47.
2. Lamb NE, Sherman SL, Hassold TJ. Effect of meiotic recombination onthe production of aneuploid gametes in humans. Cytogenet GenomeRes 2005;111:250–5.
3. Munne S. Chromosome abnormalities and their relationship to mor-phology and development of human embryos. Reprod Biomed Online2006;12:234–53.
4. Takahashi K, Mukaida T, Goto T, Oka C. Perinatal outcome of blas-tocyst transfer with vitrification using cryoloop: a 4-year follow-upstudy. Fertil Steril 2005;84:88–92.
5. Hanson C, Caisander G. Human embryonic stem cells and chromosome
stability. APMIS 2005;113:751–5.with CGH Vol. 87, No. 5, May 2007

AooMdpds(mr
R
P
R
0d
Late stages of embryo progression are a much betterpredictor of clinical pregnancy than early cleavage inintracytoplasmic sperm injection and in vitrofertilization cycles with blastocyst-stage transferKhurram S. Rehman, M.D.,a,b Orhan Bukulmez, M.D.,a,b Martin Langley, B.Sc.,a
Bruce R. Carr, M.D.,b Anna C. Nackley, M.D.,a,b Kathleen M. Doody, M.D.,a,b
and Kevin J. Doody, M.D.a,b
a Center for Assisted Reproduction, Bedford; and b Division of Reproductive Endocrinology and Infertility, Department ofObstetrics and Gynecology, University of Texas Southwestern Medical Center, Dallas, Texas
Objective: To define and validate metrics of embryo progression and morphology during extended embryo cultureand to compare the effects of early cleavage (EC) vs. blastulation stages on clinical pregnancy.Design: Retrospective observational study.Setting: University-affiliated assisted reproduction center.Patient(s): One thousand two hundred ninety-two intracytoplasmic sperm injection and 842 IVF blastocyst-transfer cycles.Intervention(s): The embryo progression index (EPI) was calculated as the area under the curve of total cellnumber (TCN) over time, by using observed TCN for cleavage-stage embryos and estimated blastocyst TCNaccording to morphology. The EPI from days 1–3 measured early cleavage, and blastulation was assessedby EPI over extended embryo culture. Blastocyst morphology was converted into numerical blastocystquality scores (BQSs). Receiver operating characteristic curve analysis was used to evaluate predictors forclinical pregnancy.Main Outcome Measure(s): Clinical pregnancy.Result(s): Per-cycle mean EPI and mean BQS for all embryos developing into blastocysts, as well as mean BQSof the transferred embryos, were significant predictors of clinical pregnancy in intracytoplasmic sperm injectionand IVF cycles. Mean EPI for days 1–3 did not predict outcome.Conclusion(s): Early cleavage is a putative marker of embryo quality. Late-stage embryo development is moresensitive and specific in predicting clinical pregnancy than is early cleavage, supporting the use of extendedembryo culture for embryo selection. The embryo progression index and BQS may also be used for this purpose.(Fertil Steril� 2007;87:1041–52. ©2007 by American Society for Reproductive Medicine.)
Key Words: Blastocyst, morphology, embryo progression, early cleavage, in vitro fertilization, clinical pregnancy
agtc
Dsbtttdgapocn
ssessment of embryo morphology has been an integral partf the selection of embryos for transfer since the earliest daysf development of the assisted reproductive technologies.any detailed assessment and grading schemes have been
evised for each stage of embryo development, includingronuclear-stage zygotes and cleavage-stage embryos onays 2 and 3 after fertilization, and for blastocysts. As-essment of morphology in zygotes at the two-pronuclear2PN) stage includes measures such as pronuclear align-ent and morphology. Edwards and Beard (1, 2) have
eviewed the evidence that oocyte and pronuclear polarity
eceived January 14, 2006; revised November 1, 2006; accepted No-vember 7, 2006.
resented at the 61st Annual Meeting of the American Society for Repro-ductive Medicine, Montreal, Quebec, Canada, October 15–19, 2005.
eprint requests: Khurram S. Rehman, M.D., University to Texas South-western Medical Center at Dallas, Department of Obstetrics and Gy-necology, Division of Reproductive Endocrinology and Infertility, 5323Harry Hines Boulevard, #J6.114, Dallas, Texas 75390-9032 (FAX: 214-
r648-8066; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.11.014 Copyright ©2007 American Soc
re important. For cleavage-stage embryos, morphology-rading schemes usually include assessment of blas-omere number, blastomere fragmentation, and more re-ently, blastomere multinucleation (3– 6).
Grading of blastocyst morphology was first described byokras et al. (7), mainly considering the degree of expan-
ion; however, the morphology-grading scheme developedy Gardner and Schoolcraft (8) has gained the widest accep-ance. It incorporates assessment of degree of expansion ofhe blastocyst as well as visual estimation of cell numbers inhe inner cell mass (ICM) and the trophectoderm (TE), asescribed in more detail in Materials and Methods. Thisrading scheme has been applied for both research purposesnd clinically, in selection of embryos for transfer or cryo-reservation. Gardner and Schoolcraft blastocyst morphol-gy (8) has been shown to have predictive value for embryoompetence, as assessed by implantation and clinical-preg-ancy rates, with significantly higher clinical-pregnancy
ates with transfer of two top-scoring blastocysts on day 51041Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

tao
bdosacmvbotq(t
sessscmsasappdlpfdcsiwreeasfhd
decsb
ptdcbmet
MWmdAawsbRMr
tttett
tgtsTansu
CA(amaRbacncc
han when either only one top-scoring blastocyst was avail-ble or no top-scoring blastocysts were available for transfern day 5 (9).
Compared with assessment of embryo morphology, em-ryo progression is a less well-studied concept, reflectingynamic changes (growth and development) of the embryover time. Progression thus encompasses information fromerial embryo assessments over time, whereas morphology issnapshot of the embryo at one point in time, probably mostrucially on the day of embryo transfer. In contrast to theultiple morphology-grading schemes described in the pre-
ious two paragraphs for 2PN zygotes, cleavage-stage em-ryos, and blastocysts, fewer proposals exist for evaluationf embryo progression. One aspect of embryo progressionhat has been proposed as a putative early marker of embryouality and competence is the presence of early cleavageEC), referring to the timing of the first and second blas-omere divisions to reach the two- and four-cell stages.
The effects of EC on implantation rates were first de-cribed by Edwards et al. (10), who found that humanmbryos undergoing early first and second cleavage divi-ions had per-embryo implantation rate of 30%, which wasignificantly higher than those cleaving later. Since then,everal groups have defined scoring systems for selection ofleavage-stage embryos for transfer that incorporate ele-ents of both morphology assessment and assessment of EC
tages of embryo progression. This was described for 2PNnd two-cell stage transfers by Scott and Smith (11), whocored embryos on the basis of pronuclear and nucleolarlignment and morphology and the appearance of the cyto-lasm, with increased scores for embryos that had undergoneretransfer EC. They reported a 28% implantation and a 65%elivery rate with the highest mean embryo scores. Simi-arly, a strong predictive effect of EC on implantation andregnancy rates has been reported for single-embryo trans-ers (SETs) and double-embryo transfers (DETs) by usingay 2 cleavage-stage embryos (12, 13). For transfer of day 3leavage-stage embryos, a set of morphological and progres-ion characteristics of top-quality embryos has been defined,ncluding EC, with high implantation and pregnancy ratesith either SET or DET (14, 15). However, limited data exist
egarding the relevance of EC to embryo competency afterxtended embryo culture. Fenwick et al. (16) found thatmbryos undergoing early first cleavage within 25 hoursfter insemination had higher progression to the blastocysttage. Racowsky et al. (17) found that blastocysts developingrom embryos with seven or eight blastomeres on day 3 hadigher implantation and clinical-pregnancy potential thanid those developing from other cleavage stages.
The present study has three aims. First, we set out toefine novel quantitative metrics of embryo progression andmbryo morphology that are relevant to extended embryoulture with transfer of blastocyst or compacted morula-tage embryos. Second, we aimed to validate these measures
y investigating whether indices of embryo morphology or (1042 Rehman et al. Blastulation vs. early cleavage
rogression during extended embryo culture had any predic-ive value in determining clinical pregnancy in fresh, non-onor oocyte intracytoplasmic sperm injection (ICSI) or IVFycles. Last, we wished to compare the assessment of em-ryo progression during the EC stages of embryo develop-ent with that during the last stages of embryo progression,
ncompassing morula formation and blastulation, in regardo predicting clinical pregnancy.
ATERIALS AND METHODSe undertook a retrospective analysis of serial embryoorphology observations and clinical pregnancy outcome
uring ICSI and IVF cycles performed at the Center forssisted Reproduction, a university-affiliated private
ssisted-reproduction program. Extended embryo cultureith use of sequential culture media has been used univer-
ally since January 1999. All analyzed cycles took placeetween April 1998 and November 2004. The Institutionaleview Board of the University of Texas Southwesternedical Center determined that this study was exempt from
eview.
A total of 1,292 ICSI and 842 IVF cycles were included inhe study. The demographics and clinical characteristics ofhese cycles are summarized in Table 1. The inclusion cri-eria were fresh cycles, resulting in transfer of at least onembryo on day 5 or day 6 after fertilization. The majority ofransfers occurred on postfertilization day 5, with observa-ion of embryos up to days 6 to 7 after fertilization.
Exclusion criteria comprised cycles using frozen embryoransfer, use of donor oocytes or donor embryos, or use ofestational carrier surrogacy. Serial daily embryo observa-ions were recorded in the Electronic Medical Record (EMR)oftware, DOC version 5 (Digital MD Systems, Bedford,X). Pregnancy outcomes were recorded in the EMR andlso were recorded in an outcomes database. Clinical preg-ancy was defined as the presence of at least one gestationalac with positive fetal heart activity, detected by transvaginalltrasound performed 30–34 days after oocyte retrieval.
ontrolled Ovarian Hyperstimulationll of the patients were treated with oral contraceptive pills
Desogen; Organon, West Orange, NJ) on cycle days 2 to 4nd discontinued this treatment after 14 to 28 days of ad-inistration. All patients received a recombinant FSH prep-
ration (either Follistim [Organon] or Gonal-F [Serono,ockland, MA]). Pituitary suppression was achieved eithery a conventional GnRH agonist protocol (long or flare) orGnRH antagonist protocol. The GnRH antagonist protocol
onsisted of precycle suppression and microdose recombi-ant hCG treatment during FSH stimulation. We have re-ently described both GnRH agonist and antagonist proto-ols in detail (18).
Upon confirmation of at least three dominant follicles
mean diameter, 18 mm), recombinant hCG (Ovidrel, Se-Vol. 87, No. 5, May 2007

rt
EAtd(4anh
tmSwS
1beSbsw
Irttn
ua
GBcgdevi3elath
taAfbf
BWgamhf
F
ono; 250 �g SC) or urinary hCG (5,000 IU) was adminis-ered, with oocyte retrieval occurring 36–38 hours later.
mbryo Culture and Transferfter retrieval (day 0), oocytes were placed in human
ubal fluid (HTF; Irvine Scientific, Santa Ana, CA) me-ium plus 12% (by volume) synthetic serum substituteSSS; Irvine Scientific) and were cultured for approximatelyhours. After IVF or ICSI, embryo culture was performed inhumidified incubator with 6% CO2, 5% O2, and 89%
itrogen at 37°C (18). Fertilization was evaluated 16–18ours after insemination or sperm injection (day 1).
From April 1998 to February 1999, embryos were cul-ured for 48 hours in S1 (IVF Science, Vero Beach, FL)edium, followed by 48 to 72 hours culture in S2 (IVFcience) to day 5 or day 6. In February 1999, a media changeas made, and G1.2 (IVF Science) and G2.2 or CCM (IVFcience) replaced S1 and S2, respectively.
Fertilized oocytes were cultured in Petri dishes containing00-�L microdrops of S1/G1.2 medium under oil, two em-ryos per drop, for 48 hours. On day 3, cleavage-stagembryos were transferred to fresh 100-�L microdrops of2/G2.2 or CCM medium under oil and cultured, two em-ryos per drop, for an additional 48 to 72 hours. Blastocyst-tage embryos with a well-defined ICM and expanding TEere used for transfer on day 5.
All patients received luteal phase support with 50 mg ofM P in oil daily, which was initiated on the day after oocyteetrieval. An abdominal ultrasound (5 MHz) was used for allransfers to assist intrauterine placement of the embryo-ransfer catheter (Edwards-Wallace catheter; Marlow Tech-
TABLE 1Demographics and cycle characteristics for ICSI
Parameter
No. of cyclesFemale age (y)BMI (kg/m2)Cycle no.Day 2/3 FSH (mIU/mL)FSH used (IU)Peak E2 (pg/mL)Oocyte no.Metaphase II/ mature oocyte rate (%)Fertilization rate (%)No. of embryos transferredClinical-pregnancy rate, % (n)Note: Data are expressed as mean � SEM, unless otherw
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.
ologies, Willoughby, OH). Patients were advised to transfer o
ertility and Sterility�
p to two to four blastocysts, depending on patient agend/or embryo quality.
ardner and Schoolcraft Blastocyst Morphology Gradinglastocysts were graded according to the morphologyriteria of Gardner and Schoolcraft (8). Blastocysts wereiven a numerical score from 1 to 6 on the basis of theiregree of expansion and hatching status, as follows: 1, anarly blastocyst with a blastocoel that is less than half of theolume of the embryo; 2, a blastocyst with a blastocoel thats half of or greater than half of the volume of the embryo;, a full blastocyst with a blastocoel completely filling thembryo; 4, an expanded blastocyst with a blastocoel volumearger than that of the early embryo, with a thinning zona; 5,hatching blastocyst with the TE starting to herniate though
he zona; and 6, a hatched blastocyst, in which the blastocystas completely escaped from the zona.
The development of the ICM was graded as follows: A,ightly packed, many cells; B, loosely grouped, several cells;nd C, very few cells. Last, the TE was assessed as follows:, many cells forming a cohesive epithelium; B, few cells
orming a loose epithelium; or C, very few large cells. Thelastocyst illustrated in Figure 1 is a 4AA embryo, that is,ully expanded with good ICM and TE morphology.
lastocyst Quality Scoringe sought to define a numerical blastocyst morphology-
rading system based on the criteria established by Gardnernd Schoolcraft (8). Of the three components of theirorphology-grading scheme, degree of expansion and
atching status was already numerically coded by an integerrom 1 to 6, whereas ICM and TE grades are represented by
IVF cycles.
ICSI IVF
1,292 84234.0 � 0.1 34.1 � 0.125.9 � 0.2 25.6 � 0.21.42 � 0.02 1.3 � 0.025.36 � 0.12 5.31 � 0.13
3,136.9 � 43.4 3,011.0 � 45.72,276.4 � 36.6 2,289.2 � 45.2
13.4 � 0.2 13.8 � 0.279.6 � 0.7 89.8 � 0.674.3 � 0.5 61.2 � 0.72.04 � 0.02 2.06 � 0.02
34.1 (440/1,292) 42.9 (361/842)indicated. BMI � body mass index.
and
ise
ne letter each, with A representing the highest grade. We
1043

cpcwo
(
wwcgqdasm
baI3fBcio
EAssesmsnvzbd
l
oded these letter grades into numeric form in the simplestossible manner, using A � 3, B � 2, and C � 1. Toombine these three values to yield a single summary score,e evaluated both additive and multiplicative combinationsf the three component numbers.
For a 4AA embryo, the additive blastocyst quality scoreBQS-A) was equal to 4 � 3 � 3, giving a BQS-A of 10,
FIGURE 1
The method of conversion of blastocystmorphology grading into the numerical BQS.Blastocyst quality score is the product of degreeof expansion (numbered 1 to 6) and ICM and TEgrades, where grade A � 3, grade B � 2, andgrade C � 1. The embryo illustrated represents anexpanded blastocyst with excellent morphology,with a BQS of 36.
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.
TABLE 2Gardner and Schoolcraft blastocyst morphology
Morphology BQS Morphology
1AA 9 3AA1AB/1BA 6 3AB/3BA1BB 4 3BB1AC/1CA 3 3AC/3CA1BC/1CB 2 3BC/3CB1CC 1 3CC2AA 18 4AA2AB/2BA 12 4AB/4BA2BB 8 4BB2AC/2CA 6 4AC/4CA2BC/2CB 4 4BC/4CB2CC 2 4CC
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.1044 Rehman et al. Blastulation vs. early cleavage
hereas the multiplicative blastocyst quality score (BQS-M)as equal to 4 � 3 � 3, giving a BQS-M score of 36. We
hose the BQS-M measure over BQS-A because it gave areater spread of values between lower-quality and higher-uality blastocysts. This was reflected in slightly better pre-ictive value for clinical-pregnancy outcome for both IVFnd ICSI cycles when using BQS-M over BQS-A (data nothown). In the remainder of this study, BQS refers to theultiplicative version, BQS-M.
To restate, BQS is a metric of blastocyst quality that isased on established morphologic criteria, and it is defineds the product of degree of expansion and hatching status andCM and TE grades, where letter grade A is given the value, grade B � 2, and grade C � 1. A sample BQS calculationor a 4AA-grade embryo is illustrated in Figure 1, with aQS of 36. Table 2 shows examples of Gardner and School-raft (8) morphology grades with their corresponding numer-cal conversions into BQS. Of note, different combinationsf morphological criteria can yield identical BQS values.
mbryo Progression Indexlthough blastocyst morphology scoring is relatively
traightforward and relies on an existing blastocyst gradingcheme, to measure embryo progression during extendedmbryo culture, we needed to create a novel measurementcheme. Figure 2 shows the calculation of our proposedeasure. The embryo progression curve illustrated repre-
ents the observed or estimated total cell number (TCN; seeext section) from serial daily observations of a single de-eloping embryo, plotted against time in days after fertili-ation, in this example for an embryo reaching an earlylastocyst stage (Gardner and Schoolcraft grade 1AA) onay 5 of culture.
The embryo progression index, or EPI for short, is calcu-ated as the area under this curve (AUC), by using trapezoi-
des, with corresponding BQS.
BQS Morphology BQS
27 5AA 4518 5AB/5BA 3012 5BB 209 5AC/5CA 156 5BC/5CB 103 5CC 5
36 6AA 5424 6AB/6BA 3616 6BB 2412 6AC/6CA 188 6BC/6CB 124 6CC 6
gra
Vol. 87, No. 5, May 2007

dtslf
TTnmencsit4sT
tnlccacc
t
cicefTfb
mcegtefib
cwkhm1Tc
dTobdwc
F
al integration. For the sample progression curve shown forhe embryo cultured to day 5, the EPI is the sum of the fourhaded trapezoidal areas: a, b, c, and d (Fig. 2). The calcu-ation of observed or estimated TCN is described in theollowing section.
otal Cell Number Observation and Estimationotal cell number represents the overall blastomere cellumber in the embryo. For cleavage-stage embryos andorulae, TCN is simply the cell count of blastomeres in the
mbryo. In the blastocyst, TCN represents the sum of theumber of cells in the ICM and the number of TE cells. Totalell number is easily assessed noninvasively for cleavage-tage embryos by counting the blastomeres using standardnverted light microscopy. Cleavage of the zygote to yieldwo-cell, four-cell, and eight-cell stages typically results in–12 blastomeres by day 3 after fertilization. For cleavage-tage embryos, we can thus directly use the cell count as theCN, with some straightforward examples shown in Table 3.
However, for compacting morulae and blastocysts, blas-omere boundaries become less well defined, and it often isot possible to accurately count individual blastomeres in theiving embryo using standard light microscopy. This pre-ludes rapid visual assessment of TCN. Reliable blastomereounting involves mechanically disrupting the embryo, usu-lly fresh or thawed supernumerary embryos from IVF-ICSIycles; spreading out the cells; fixing and staining; and thenounting the nuclei.
Since the original article measuring TCN in human blas-
FIGURE 2
Calculation of EPI. The embryo progression curveshown represents an early blastocyst reaching anestimated TCN of 48 cells on day 5 afterfertilization. Embryo progression index is the AUCof observed or estimated TCN plotted against timein days after fertilization; EPI for days 1–5 is thesum of the areas of the four shaded trapezoids:a, b, c, and d.
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.
ocysts by Hardy et al. (19), which found a mean TCN of 58
ertility and Sterility�
ells on day 5, there have been a number of published studiesn which human blastocysts were fixed and TCN wasounted after nuclear staining. The first study by Dumoulint al. (20) used spare IVF and ICSI embryos that were notrozen and found a mean day 5 blastocyst TCN of 43–47.he second study from the same group used spare embryos
rom ICSI only and found a mean day 5 and 6 TCN ofetween 43 and 53 cells (21).
Devreker et al. (22) found that TCN varied between aean of 62 to 100 on day 6, depending on the amino acid
omposition of the sequential culture media used. Archert al. (23) used frozen cleavage-stage embryos that wererown to blastocysts in sequential media after thawing, andhey found a mean day 6 TCN of 57–58 cells. They used twoxample day 6 blastocysts with corresponding stained andxed TCN preparations, with a TCN of 42 for an earlylastocyst and 106 for an expanded blastocyst.
The study by Fong and Bongso (24) represents an outlier,omparing blastocysts grown in sequential media with andithout co-culture with Vero cells (African green monkeyidney epithelial cells). Those investigators reported muchigher cell numbers than the other studies on day 6, withean day 6 TCN in good-morphology blastocysts of 64 to
68 cells. In summary, these studies found mean blastocystCN of approximately 40–60 cells on day 5 and 50 to �100ells on day 6.
In the present study, the above data were used to guide theevelopment of a mathematical model to allow estimation ofCN from noninvasive morphology observations conductedn human blastocysts. Using a model to estimate TCN forlastocysts is useful for clinical IVF programs in whichestroying the embryo is obviously not an option, and inhich safe nonlethal nuclear staining of blastomeres is not
urrently possible.
TABLE 3Examples of TCN values for cleavage-stageembryos and compacting morulae.
Stage TCN
Zygote (2PN, etc.) 12 cell 24 cell 45 cell 56 cell 67 cell 78 cell 8
10 cell 1012 cell 12Morula 24a
a Estimated TCN.
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.
1045
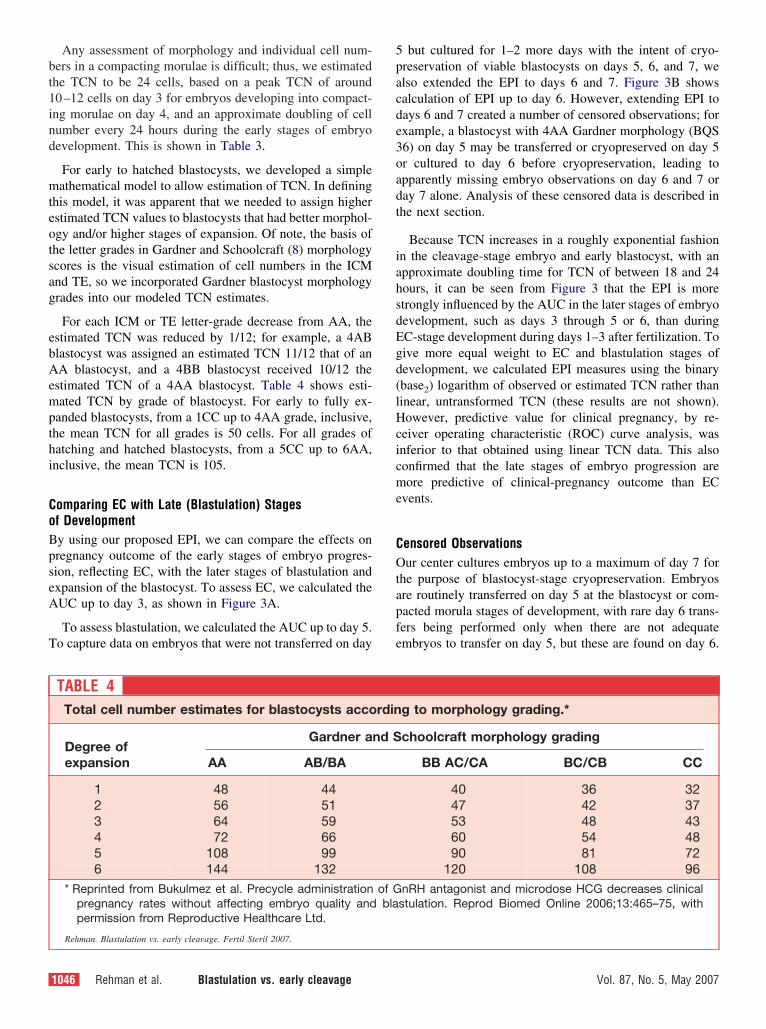
bt1ind
mteotsag
ebAempthi
CoBpseA
T
5pacde3oadt
iahsdEgd(lHcicme
COtapfe
Any assessment of morphology and individual cell num-ers in a compacting morulae is difficult; thus, we estimatedhe TCN to be 24 cells, based on a peak TCN of around0–12 cells on day 3 for embryos developing into compact-ng morulae on day 4, and an approximate doubling of cellumber every 24 hours during the early stages of embryoevelopment. This is shown in Table 3.
For early to hatched blastocysts, we developed a simpleathematical model to allow estimation of TCN. In defining
his model, it was apparent that we needed to assign higherstimated TCN values to blastocysts that had better morphol-gy and/or higher stages of expansion. Of note, the basis ofhe letter grades in Gardner and Schoolcraft (8) morphologycores is the visual estimation of cell numbers in the ICMnd TE, so we incorporated Gardner blastocyst morphologyrades into our modeled TCN estimates.
For each ICM or TE letter-grade decrease from AA, thestimated TCN was reduced by 1/12; for example, a 4ABlastocyst was assigned an estimated TCN 11/12 that of anA blastocyst, and a 4BB blastocyst received 10/12 the
stimated TCN of a 4AA blastocyst. Table 4 shows esti-ated TCN by grade of blastocyst. For early to fully ex-
anded blastocysts, from a 1CC up to 4AA grade, inclusive,he mean TCN for all grades is 50 cells. For all grades ofatching and hatched blastocysts, from a 5CC up to 6AA,nclusive, the mean TCN is 105.
omparing EC with Late (Blastulation) Stagesf Developmenty using our proposed EPI, we can compare the effects onregnancy outcome of the early stages of embryo progres-ion, reflecting EC, with the later stages of blastulation andxpansion of the blastocyst. To assess EC, we calculated theUC up to day 3, as shown in Figure 3A.
To assess blastulation, we calculated the AUC up to day 5.o capture data on embryos that were not transferred on day
TABLE 4Total cell number estimates for blastocysts acco
Degree ofexpansion
Gardner a
AA AB/BA
1 48 442 56 513 64 594 72 665 108 996 144 132
* Reprinted from Bukulmez et al. Precycle administrationpregnancy rates without affecting embryo quality andpermission from Reproductive Healthcare Ltd.
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.
1046 Rehman et al. Blastulation vs. early cleavage
but cultured for 1–2 more days with the intent of cryo-reservation of viable blastocysts on days 5, 6, and 7, welso extended the EPI to days 6 and 7. Figure 3B showsalculation of EPI up to day 6. However, extending EPI toays 6 and 7 created a number of censored observations; forxample, a blastocyst with 4AA Gardner morphology (BQS6) on day 5 may be transferred or cryopreserved on day 5r cultured to day 6 before cryopreservation, leading topparently missing embryo observations on day 6 and 7 oray 7 alone. Analysis of these censored data is described inhe next section.
Because TCN increases in a roughly exponential fashionn the cleavage-stage embryo and early blastocyst, with anpproximate doubling time for TCN of between 18 and 24ours, it can be seen from Figure 3 that the EPI is moretrongly influenced by the AUC in the later stages of embryoevelopment, such as days 3 through 5 or 6, than duringC-stage development during days 1–3 after fertilization. Toive more equal weight to EC and blastulation stages ofevelopment, we calculated EPI measures using the binarybase2) logarithm of observed or estimated TCN rather thaninear, untransformed TCN (these results are not shown).owever, predictive value for clinical pregnancy, by re-
eiver operating characteristic (ROC) curve analysis, wasnferior to that obtained using linear TCN data. This alsoonfirmed that the late stages of embryo progression areore predictive of clinical-pregnancy outcome than EC
vents.
ensored Observationsur center cultures embryos up to a maximum of day 7 for
he purpose of blastocyst-stage cryopreservation. Embryosre routinely transferred on day 5 at the blastocyst or com-acted morula stages of development, with rare day 6 trans-ers being performed only when there are not adequatembryos to transfer on day 5, but these are found on day 6.
g to morphology grading.*
choolcraft morphology grading
BB AC/CA BC/CB CC
40 36 3247 42 3753 48 4360 54 4890 81 72
120 108 96nRH antagonist and microdose HCG decreases clinicalstulation. Reprod Biomed Online 2006;13:465–75, with
rdin
nd S
of Gbla
Vol. 87, No. 5, May 2007

tcsfEihtamcd
SIlCcmscfatRsc
RBbbC4ade
vrad
ettAA
dpnnt0
F
For embryos that were transferred on day 5, we assignedhe same TCN observed on day 5 to day 6 and day 7 whenalculating EPI. Similarly, embryos transferred or cryopre-erved on day 6 were assigned the last observed TCN scorerom day 6 on day 7. This allowed for simple computation ofPI involving censored data, without recourse to extrapolat-
ng or estimating the degree of further progression that mayave occurred in culture, had the embryo not been eitherransferred or cryopreserved. However, an embryo reaching
high-quality blastocyst stage on day 5 would still have auch higher EPI, reflecting the AUC of the estimated TCN
urve, than another embryo reaching the same stage ofevelopment on day 6 or day 7.
tatistical Analysisntracytoplasmic sperm injection and IVF cycles were ana-yzed separately by using SPSS, version 12 (SPSS Inc.;hicago, IL); thus, the means of each parameter are notompared between ICSI and IVF. For each treatment cycle,eans of BQS and EPI were calculated and entered as
eparate variables. Then, ROC curve analysis was used toompare the predictive ability of mean BQS of the trans-erred blastocysts, mean BQS of the entire blastocyst cohort,nd mean EPI during both the cleavage stage only andhroughout extended embryo culture, using the AUC of theOC curves to quantitatively compare the sensitivity and
pecificity of the measures of interest. The categorical out-
FIGURE 3
Use of the EPI to quantify early cleavage vs. blastulaprogression curves shown represent TCN plotted onthe left, EPI from days 1 to 3 is shown as the shadeddays 1 to 6 is shown as the shaded AUC, measuring
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.
ome variable was clinical pregnancy. F
ertility and Sterility�
ESULTSlastocyst quality score was calculated for both transferredlastocysts and for the entire cohort of embryos reaching thelastocyst stage for all 1,292 ICSI and 842 IVF cycles.omplete daily embryo-progression data were available for62 ICSI and 315 IVF cycles resulting in blastocyst transfer,nd these data were used to calculate EPI on days 1–3 andays 1–7, day 7 being the latest possible day of extendedmbryo culture before cryopreservation or discarding.
Figure 4A shows an ROC curve analysis of the predictivealue of mean BQS and mean EPI on clinical-pregnancyates in ICSI cycles. The reference line, equivalent to tossingcoin to determine pregnancy outcome, is the heavy black
iagonal.
For ICSI cycles alone, mean BQS for the transferredmbryos had an area under the ROC curve of 0.645. Blas-ocyst quality score for all embryos developing to the blas-ocyst stage was the strongest outcome predictor, with anUC of 0.652, and the mean EPI for all blastocysts had anUC of 0.62.
Figure 4B shows an ROC curve analysis of the EPI forays 1 to 3 and female age in the prediction of clinicalregnancy in ICSI cycles. The EPI for days 1 to 3 waseither a sensitive nor a specific predictor of clinical preg-ancy in ICSI cycles. This ROC curve can be seen to crosshe reference line, and the area under the ROC curve is.461, compared with an AUC of 0.5 for the reference line.
stages of embryo development. The embryoear scale against time in days after fertilization. OnC, measuring early cleavage. On the right, EPI fromstulation.
tiona linAUbla
or comparison, using female age to predict clinical preg-
1047

nippeb
fcsc
dt
acscAln
ancy resulted in an ROC curve with an AUC of 0.568. Thisndicated some predictive ability of female age for clinicalregnancy; however, age alone was less predictive of clinicalregnancy than was either mean BQS for the transferredmbryos or mean BQS for all embryos developing to thelastocyst stage, or the mean EPI for all blastocysts.
Figure 4C shows an ROC curve analysis of BQS and EPIor prediction of clinical pregnancy in IVF cycles. For IVFycles alone, mean BQS for the transferred embryos was thetrongest outcome predictor, with an area under the ROC
FIGURE 4
Receiver operating characteristic curves of mean BQ(A) Receiver operating characteristic curves for BQScycles. The embryo progression index reflects all avaoperating characteristic curves for EPI on days 1–3 aICSI cycles. (C) Receiver operating characteristic curin IVF cycles. Embryo progression index reflects all a(D) Receiver operating characteristic curves for EPI opregnancy in IVF cycles.
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.
urve of 0.680. Blastocyst quality scores for all embryos c
1048 Rehman et al. Blastulation vs. early cleavage
eveloping to the blastocyst stage had an AUC of 0.645, andhe mean EPI for all blastocysts had an AUC of 0.648.
Figure 4D shows the ROC curves of EPI for days 1 to 3nd female age for prediction of clinical pregnancy in IVFycles. As found for ICSI, EPI for days 1 to 3 was neither aensitive nor a specific predictor of clinical pregnancy in IVFycles. This ROC curve crosses the reference line, and theUC of the ROC curve is 0.488, again below the reference
ine AUC of 0.5. Using female age to predict clinical preg-ancy resulted in an ROC curve AUC of 0.642. This indi-
d mean EPI in the prediction of clinical pregnancy.EPI as predictors of clinical pregnancy in ICSI
le embryo morphology data (days 1–7). (B) Receiveremale age as predictors of clinical pregnancy infor BQS and EPI as predictors of clinical pregnancyble embryo morphology data (days 1–7).ys 1–3 and female age as predictors of clinical
S anandilabnd fvesvailan da
ated much better predictive value of female age for clinical
Vol. 87, No. 5, May 2007

pHtaE
fiaafB�eFpBwtBm
necsst(st
wtws
�tPt1d
os4f(i
DFbrmcmtamjabc
ama(tee
psteTpmotpiqf
m
F
regnancy in IVF cycles than we had found for ICSI cycles.owever, age alone was less predictive of clinical pregnancy
han was either mean BQS for the transferred embryos or forll embryos developing to the blastocyst stage, or the meanPI for all blastocysts.
Clinical-pregnancy rates for ICSI and IVF cycles, strati-ed according to the mean BQS of the transferred embryos,re provided in Figure 5. All rates are expressed as percent-ges. For ICSI cycles, mean clinical-pregnancy rate declinedrom 48.8% � 4.5% in the group with the highest meanQS, equivalent to a 4AA or higher morphology, to 25.6%2.6% in the group with the lowest mean BQS transferred,
quivalent to embryos averaging below 1AA morphology.or IVF, higher pregnancy rates were noted overall com-ared with ICSI, except in the group with the lowest meanQS. Again, a sharp decline in mean clinical-pregnancy rateas observed as the mean BQS of the transferred embryos in
he group fell, between 60.2% � 5.1% in the highest meanQS group to 25.0% � 3.4% in the group with the lowestean BQS transferred.
From the ROC curve analysis predicting clinical preg-ancy, the best cutoff values for EPI for days 1–7 of allmbryos and mean BQS of the transferred embryos werealculated. For ICSI cycles, EPI �144.4 (sensitivity, 67.3%;pecificity, 64.4%) and BQS of �10.3 (sensitivity, 58.9%;pecificity, 67.3%) were the best threshold values in predic-ion of clinical pregnancy. In IVF cycles, EPI of �146.7sensitivity, 66.7%; specificity, 59.3%) and BQS �8.3 (sen-itivity, 66.9%; specificity, 57.7%) were the calculatedhresholds.
The cycles were then analyzed in two groups in regards tohether EPI or BQS either were greater than or were equal
o or below the calculated cutoff values. Implantation ratesere calculated for each group as total number of gestational
FIGURE 5
Clinical-pregnancy rates for ICSI and IVFcycles, stratified according to mean BQS of thetransferred embryos. Pregnancy rates (%)are expressed as mean � SEM.
Rehman. Blastulation vs. early cleavage. Fertil Steril 2007.
acs per total number of embryos transferred. r
ertility and Sterility�
For ICSI cycles, implantation rates for EPI of �144.4 and144.4 were 34.8% (168/482) and 17.1% (73/427), respec-
ively (odds ratio: 2.59, 95% confidence interval: 1.9–3.6,�.001). Implantation rates for the groups with mean BQS
ransferred of �10.3 and �10.3 were 41.3% (151/365) and6.3% (84/514), respectively (odds ratio: 3.61; 95% confi-ence interval: 2.6–5.0; P�.001).
For IVF cycles, implantation rates for EPI of �146.7 andf �146.7 were 47.3% (151/319) and 23.2% (71/306), re-pectively (odds ratio: 2.97; 95% confidence interval: 2.08–.26; P�.001). Implantation rates when mean BQS trans-erred was �8.3 and �8.3 were 47.4% (150/316) and 23.1%70/292), respectively (odds ratio: 2.87; 95% confidencenterval: 1.99–4.12; P�.001).
ISCUSSIONor extended embryo culture with the ultimate aim oflastocyst-stage embryo transfer, to date there have beenelatively limited data regarding the effects of blastocystorphology on clinical pregnancy. Where progression is
oncerned, there are no published studies regarding measure-ent of embryo progression over the entire course of ex-
ended embryo culture before transfer. The present studyddresses the question of which is more important, theorphology of the embryo on the day of transfer, or the
ourney that the embryo took to progress to that stage. Inddition, the relevance of EC to embryo competency haseen less well defined for extended culture programs than forleavage-stage transfers.
The abilities of mean BQS of the transferred blastocysts,nd mean BQS and EPI days 1–7 of all blastocysts wereore powerful for predicting clinical pregnancy than those
chieved by mean EPI days 1–3, in both ICSI and IVF cyclesFig. 4.). This finding suggests that assessment of fertiliza-ion on day 1, changing to sequential medium on day 3, andmbryo observation and scoring starting on day 5 may bequivalent in value to daily serial embryo observations.
Although Gardner and Schoolcraft (8) blastocyst mor-hology grading is a clinically useful scheme and has beenhown to predict implantation rates, there are several limi-ations associated with the use of an alphanumeric label forach combination of degree of expansion, ICM grade, andE grade. Some of these limitations, as compared with ourroposed numeric BQS, include the inability to calculate theean blastocyst grade of the transferred embryos where two
r more embryos are transferred; the inability to determinehe mean grade of the whole embryo cohort at any givenoint in time, such as on day 5; and the increased difficultyn grouping or stratifying embryos into a number of defineduality levels, for example representing excellent-, good-,air-, or poor-quality blastocysts.
Our data showing clinical-pregnancy rates according toean BQS of the transferred embryos, almost exclusively
epresenting DETs, are a good example of the greater ana-
1049

let
ebooseef
lcfptaeEat
ott(c(d
mmresrgipolad
iticdgte
gahbw
cpptobotsmoca
pbebabdtmndtpt
dpntcspm
tt(trpbTr
ytical power that is afforded to assessment of outcome inxtended embryo-culture cycles by simply converting blas-ocyst morphology grades into BQS.
Similarly, although EPI is a relatively crude measure ofmbryo progression during extended embryo culture, it cane calculated by using simple algorithms and easily gatheredbservations of embryo cell number and blastocyst morphol-gy. Again, having a numeric summary measure facilitatesemiquantitative analysis of embryo progression both atarly stages of development and later stages of development,ncompassing compaction and morula formation, blastocystormation, and blastocoel expansion.
We are thus able to compare the predictive value of EC vs.ate-stage embryo development for the first time. Earlyleavage has been incorporated into many proposed schemesor selection of cleavage-stage embryos for transfer as autative marker of embryo quality. In this study, we showhat late-stage embryo development is a much more sensitivend specific predictor of pregnancy outcome in extendedmbryo culture cycles with day 5 transfer. In addition, bothPI over the course of extended embryo culture (days 1–7)nd BQS of transferred embryos may also predict implanta-ion rates, as demonstrated.
Early-cleavage events are likely to be a reflection ofocyte competence rather than embryo competence, becausehey occur before embryonic genome activation at the four-o eight-cell stage, approximately 2–3 days after fertilization25). Several studies have indicated that there is a paternalomponent to embryo progression to the blastocyst stage26–28). It is likely that these paternal effects manifesturing the post-EC phase.
The importance of the late stages of embryo develop-ent on days 4 and 5 of extended embryo culture reflectsany important events in human embryogenesis occur-
ing after activation of the embryonic genome. Thesevents include polarization of the blastomeres that can beeen with light microscopy and blastomere differentiation,esulting in formation of the ICM and TE. The changes inene expression occur before visible evidence of polar-zation. These events, which require both maternal andaternal genetic contribution, may well be more reflectivef embryo competency (implantation potential) than ear-ier events, such as blastomere cleavage on days 2 and 3nd blastomere fragmentation during early embryoevelopment.
Our findings are consistent with those of a previous reportndicating that progression of supernumerary embryos cul-ured to the blastocyst stage had a strong predictive effect formplantation and pregnancy outcome in ICSI cycles withleavage-stage transfer (29). The potential exists for moreetailed assessment of events that occur after embryonicenome activation, including assessment of blastomere me-abolism, production of soluble or cell-surface markers of
mbryo competency, and ultimately assessment of blastocyst d1050 Rehman et al. Blastulation vs. early cleavage
ene expression. Such research strategies may well lead todvances in our ability to select the blastocysts with theighest intrinsic potential from a cohort of developing em-ryos. Thus, the aim will be to optimize pregnancy outcome,ith the trend toward transfer of fewer embryos.
Our data clearly support the use of extended embryoulture for embryo selection. We have shown a significantredictive ability of blastocyst morphology on clinical-regnancy rates, a much closer surrogate for live-birth rateshan assessment of implantation rates alone. In this study,ur ability to predict clinical-pregnancy outcome forlastocyst-stage transfer cycles on the basis of assessmentf either blastocyst morphology or embryo progression tohe blastocyst stage compares favorably with reportedtudies on the predictive ability of morphology assess-ents of cleavage-stage embryos with clinical-pregnancy
utcome of cleavage-stage transfer cycles. Our data alsoompare well with studies using detailed morphologicalssessment of the pronuclear-stage zygote.
Our results for mostly DET, showing that high clinical-regnancy rates can be achieved with low numbers of em-ryos transferred, supports the concept of using extendedmbryo culture and blastocyst transfer for selection of em-ryos for elective SET. However, further studies, ideally ofprospective nature, need to be performed for elective SET,oth to confirm these findings for SET and to provide moreetailed outcome information for clinicians and patients con-emplating elective SET as a means to address the highultiple-pregnancy rates of many assisted reproductive tech-
ology programs. We expect that SET cycles will provideetailed per-embryo outcome data, potentially allowing fur-her refinement of the assessment of both blastocyst mor-hology and blastocyst implantation and pregnancy poten-ial.
The major criticism of the EPI as described here is that itoes not incorporate observations of either the zygote or ofroperties of cleavage-stage embryos other than blastomereumber, which have been shown to affect embryo compe-ence and implantation rates, particularly in programs withleavage-stage transfer that do not practice universal orelective extended embryo culture. These parameters includeronuclear and polar-body morphology, blastomere frag-entation, and multinucleation.
High fragmentation in day 3 embryos has been reportedo result in lower blastulation rates during extended cul-ure, compared with embryos with �20% fragmentation30). There is also some evidence suggesting that blas-omere fragmentation during the cleavage stages may beeflected later in reduced cell numbers in the TE, andossibly in the ICM (31). This would obviously impactoth blastocyst morphology grading and our estimatedCN numbers, which would thus lower BQS and EPI,
espectively.
Other parameters of importance in the cleavage stages of
evelopment, such as multinucleation, are not presently in-Vol. 87, No. 5, May 2007

cvbfaqsniwsmwp
tpisssesiossor
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
F
orporated into the proposed BQS and EPI measures. Ko-acic et al. (32) have reported that detailed assessment oflastocyst morphology incorporating multinucleation andragmentation has very high correlation with implantationnd clinical-pregnancy rates. In addition, more detaileduantitative morphologic assessment of the ICM has beenhown to be more predictive than assessment of TE cellumber (33). These studies highlight the need for furthernvestigation to optimize our ability to select the embryosith the highest developmental competency for blastocyst-
tage transfer. Our current state of knowledge of blastocystorphology will likely be extended and refined as world-ide experience with extended embryo culture continues torogress.
Nevertheless, we have described practical, semiquantita-ive numeric summary measures (metrics) of blastocyst mor-hology and embryo progression, which are of particularnterest to extended embryo culture programs. These mea-ures, EPI and BQS, may be applied in a variety of clinicalituations and in comparisons of different embryo cultureystems. Possible applications range from comparing theffects of use of different culture system components such asequential culture media, protein sources, or different phys-cal culture conditions on embryo progression and morphol-gy, to clinical comparisons such as prospective or retro-pective studies of the effects of different down-regulation ortimulation protocols on embryo progression and morphol-gy. Further clinical evaluation of these measures is war-anted, ideally in a prospective fashion.
EFERENCES1. Edwards RG, Beard HK. Oocyte polarity and cell determination in
early mammalian embryos. Mol Hum Reprod 1997;3:863–905.2. Edwards RG, Beard HK. Is the success of human IVF more a matter of
genetics and evolution than growing blastocysts? Hum Reprod 1999;14:1–4.
3. Puissant F, Van Rysselberge M, Barlow P, Deweze J, Leroy F. Embryoscoring as a prognostic tool in IVF treatment. Hum Reprod 1987;2:705–8.
4. Bolton VN, Hawes SM, Taylor CT, Parsons JH. Development of sparehuman preimplantation embryos in vitro: an analysis of the correlationsamong gross morphology, cleavage rates, and development to theblastocyst. J In Vitro Fert Embryo Transf 1989;6:30–5.
5. Steer CV, Mills CL, Tan SL, Campbell S, Edwards RG. The cumulativeembryo score: a predictive embryo scoring technique to select theoptimal number of embryos to transfer in an in-vitro fertilization andembryo transfer programme. Hum Reprod 1992;7:117–9.
6. Pickering SJ, Taylor A, Johnson MH, Braude PR. An analysis ofmultinucleated blastomere formation in human embryos. Hum Reprod1995;10:1912–22.
7. Dokras A, Sargent IL, Barlow DH. Human blastocyst grading: anindicator of developmental potential? Hum Reprod 1993;8:2119–27.
8. Gardner DK, Schoolcraft WB. In vitro culture of human blastocysts. In:Jansen R, Mortimer D, ed. Towards reproductive certainty: fertility andgenetics beyond 1999: the plenary proceedings of the 11th WorldCongress on In Vitro Fertilization & Human Reproductive Genetics.Pearl River, NY: Parthenon, 1999:378–88.
9. Gardner DK, Lane M, Stevens J, Schlenker T, Schoolcraft WB. Blas-tocyst score affects implantation and pregnancy outcome: towards a
single blastocyst transfer. Fertil Steril 2000;73:1155–8.ertility and Sterility�
0. Edwards RG, Fishel SB, Cohen J, Fehilly CB, Purdy JM, Slater JM, etal. Factors influencing the success of in vitro fertilization for alleviatinghuman infertility. J In Vitro Fert Embryo Transfer 1984;1:3–23.
1. Scott LA, Smith S. The successful use of pronuclear embryo transfersthe day following oocyte retrieval. Hum Reprod 1998;13:1003–13.
2. Salumets A, Hyden-Granskog C, Makinen S, Suikkari AM, Tiitinen A,Tuuri T. Early cleavage predicts the viability of human embryos inelective single embryo transfer procedures. Hum Reprod 2003;18:821–5.
3. Van Montfoort AP, Dumoulin JC, Kester AD, Evers JL. Early cleavageis a valuable addition to existing embryo selection parameters: a studyusing single embryo transfers. Hum Reprod 2004;19:2103–8.
4. Gerris J, De Neubourg D, Mangelschots K, Van Royen E, Van deMeerssche M, Valkenburg M. Prevention of twin pregnancy afterin-vitro fertilization or intracytoplasmic sperm injection based on strictembryo criteria: a prospective randomized clinical trial. Hum Reprod1999;14:2581–7.
5. Van Royen E, Mangelschots K, De Neubourg D, Valkenburg M, Vande Meerssche M, Ryckaert G, et al. Characterization of a top qualityembryo, a step towards single-embryo transfer. Hum Reprod 1999;14:2345–9.
6. Fenwick J, Platteau P, Murdoch AP, Herbert M. Time from insemina-tion to first cleavage predicts developmental competence of humanpreimplantation embryos in vitro. Hum Reprod 2002;17:407–12.
7. Racowsky C, Combelles CM, Nureddin A, Pan Y, Finn A, Miles L, etal. Day 3 and day 5 morphological predictors of embryo viability.Reprod Biomed Online 2003;6:323–31.
8. Bukulmez O, Rehman KS, Langley M, Carr BR, Nackley AC, DoodyKM, et al. Precycle administration of GnRH antagonist and microdoseHCG decreases clinical pregnancy rates without affecting embryo qual-ity and blastulation. Reprod Biomed Online 2006;13:465–75.
9. Hardy K, Handyside AH, Winston RM. The human blastocyst: cellnumber, death and allocation during late preimplantation developmentin vitro. Development 1989;107:597–604.
0. Dumoulin JC, Coonen E, Bras M, van Wissen LC, Ignoul-VanvuchelenR, Bergers-Jansen JM, et al. Comparison of in-vitro development ofembryos originating from either conventional in-vitro fertilization orintracytoplasmic sperm injection. Hum Reprod 2000;15:402–9.
1. Dumoulin JM, Coonen E, Bras M, Bergers-Janssen JM,Ignoul-Vanvuchelen RC, van Wissen LC, et al. Embryo developmentand chromosomal anomalies after ICSI: effect of the injection proce-dure. Hum Reprod 2001;16:306–12.
2. Devreker F, Hardy K, Van den Bergh M, Vannin AS, Emiliani S,Englert Y. Amino acids promote human blastocyst development invitro. Hum Reprod 2001;16:749–56.
3. Archer J, Gook DA, Edgar DH. Blastocyst formation and cell numbersin human frozen-thawed embryos following extended culture. HumReprod 2003;18:1669–73.
4. Fong CY, Bongso A. Comparison of human blastulation rates and totalcell number in sequential culture media with and without co-culture.Hum Reprod 1999;14:774–81.
5. Braude P, Bolton V, Moore S. Human gene expression first occursbetween the four- and eight-cell stages of preimplantation development.Nature 1988;332:459–61.
6. Janny L, Menezo YJ. Evidence for a strong paternal effect on humanpreimplantation embryo development and blastocyst formation. MolReprod Dev 1994;38:36–42.
7. Shoukir Y, Chardonnens D, Campana A, Sakkas D. Blastocyst devel-opment from supernumerary embryos after intracytoplasmic sperminjection: a paternal influence? Hum Reprod 1998;13:1632–7.
8. Seli E, Gardner DK, Schoolcraft WB, Moffatt O, Sakkas D. Extent ofnuclear DNA damage in ejaculated spermatozoa impacts on blastocystdevelopment after in vitro fertilization. Fertil Steril 2004;82:378–83.
9. Balaban B, Urman B, Sertac A, Alatas C, Aksoy S, Nuhoglu A.Progression of excess embryos to the blastocyst stage predicts preg-nancy and implantation rates after intracytoplasmic sperm injection.
Hum Reprod 1998;13:2564–7.1051

3
3
3
3
0. Rijnders PM, Jansen CA. The predictive value of day 3 embryo mor-phology regarding blastocyst formation, pregnancy and implantationrate after day 5 transfer following in-vitro fertilization or intracytoplas-mic sperm injection. Hum Reprod 1998;13:2869–73.
1. Hardy K, Stark J, Winston RM. Maintenance of the inner cell mass in
human blastocysts from fragmented embryos. Biol Reprod 2003;68:1165–9.1052 Rehman et al. Blastulation vs. early cleavage
2. Kovacic B, Vlaisavljevic V, Reljic M, Cizek-Sajko M. Developmentalcapacity of different morphological types of day 5 human morulae andblastocysts. Reprod Biomed Online 2004;8:687–94.
3. Richter KS, Harris DC, Daneshmand ST, Shapiro BS. Quantitativegrading of a human blastocyst: optimal inner cell mass size and shape.
Fertil Steril 2001;76:1157–67.Vol. 87, No. 5, May 2007

Aectamgst
(tsppaem
RR
0d
High incidence of complex chromosome abnormalityin cleavage embryos from patients with repeatedimplantation failureLucille Voullaire, M.Sc.,a Veronica Collins, Ph.D.,a Tracey Callaghan, B.Sc.,b
John McBain, M.B., B.S.,b Robert Williamson, Ph.D.,a and Leeanda Wilton, Ph.D.b
a The Murdoch Childrens Research Institute, University of Melbourne Department of Paediatrics, Royal Children’s Hospital,Parkville, Australia, and b Melbourne IVF, East Melbourne, Australia
Objective: To analyze the chromosome abnormalities observed in the course of preimplantation aneuploidyscreening using comparative genomic hybridization (CGH) on single blastomeres in relation to maternal age andprevious IVF history.Design: Retrospective analytical study.Setting: A large IVF unit and the research laboratory of an associated clinical genetics unit.Patient(s): Twenty-eight women referred for aneuploidy screening of cleavage embryos.Intervention(s): Blastomere biopsy.Main Outcome Measure(s): The incidence of aneuploidy and complex abnormality in human cleavage embryos.Result(s): The incidence in embryos of aneuploidy for one to two chromosomes was significantly increased withadvanced maternal age, but was independent of any history of recurrent implantation failure. In comparison, theincidence of complex chromosome abnormality (which involves three or more chromosomes) was independentof maternal age but significantly increased in embryos from patients with a history of recurrent implantationfailure.Conclusion(s): The incidence of complex abnormality in healthy cleavage embryos is independent of maternalage but is increased in patients with a history of recurrent implantation failure. These results suggest that thepathology underlying complex abnormality is different from that resulting in aneuploidy of one to twochromosomes but particularly relevant to women with recurrent implantation failure. (Fertil Steril� 2007;87:1053–8. ©2007 by American Society for Reproductive Medicine.)
Key Words: Preimplantation genetic diagnosis, aneuploidy screening, complex abnormality, comparative genomichybridization, recurrent implantation failure
crp
mpaccfaqfXdfoc(
at
high level of chromosome abnormality occurs in humanmbryos. Evidence showing this was first obtained fromhromosome studies on spontaneously aborted fetuses. Morehan 60% of spontaneously aborted fetuses �12 weeks ofge have either aneuploidy involving autosomal trisomy oronosomy for the X chromosome (1). The findings sug-
ested that other abnormalities, such as autosomal mono-omy, which would have a lower viability, occur at concep-ion but result in early fetal death.
The development of fluorescent in situ hybridizationFISH) allowed the use of chromosome-specific probes forhe detection of aneuploidy in embryos from IVF. Chromo-ome abnormality was shown to occur in more than 50% ofreimplantation embryos after IVF, including aneuploidy,olyploidy, and haploidy (2, 3). Because most chromosomebnormalities detected are unlikely to be compatible withmbryo development, this high level of chromosome abnor-ality could explain why less than half of all human con-
eceived January 6, 2006; revised and accepted January 6, 2006.eprint requests: Lucille Voullaire, The Murdoch Childrens ResearchInstitute, University of Melbourne Department of Paediatrics, RoyalChildren’s Hospital, Parkville, VIC 3052, Australia (FAX: 61-03-8341-
h6366; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.11.043 Copyright ©2007 American Soc
eptions result in a live birth (4, 5). It also explains theelatively low implantation rate after IVF even when mor-hologically good-quality embryos are transferred (6, 7).
Preimplantation screening of cleavage embryos for chro-osome abnormality has become an accepted practice for
atients undergoing IVF who have a poor prognosis ofchieving a successful pregnancy (6, 7). Generally this isarried out using FISH with probes of five to nine differenthromosomes on a single blastomere biopsied on day 3 afterertilization (8). The probes generally selected for FISHnalysis detect the chromosomes known to be most fre-uently involved in chromosome aneuploidy seen in abortedetuses and liveborn individuals, including 13, 21, 16, 18, 22,
and Y, and more rarely 14 and 15. Embryos that areiagnosed as normal on the biopsied blastomere are selectedor transfer. The FISH studies have shown that the incidencef aneuploidy for chromosomes 13, 16, 18, and 21 is in-reased in embryos from patients of advanced maternal age9, 10).
Patients regarded as having a poor prognosis of achievingsuccessful pregnancy after IVF may be of advanced ma-
ernal age (AMA), have had recurrent abortion (RA), have a
istory of recurrent implantation failure (RIF) after IVF, or,1053Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

looAiawcctf1fgmA
cc(cw(tsi
“inmaineodosatodwucdieb
uaR
tR
MPTsrlatoephwsIwtpi
atoHaatgeg3dagos
CSfbmemr
CBsa
ess frequently, have had a previous trisomic conception orne in which there is a male meiotic abnormality. Detectionf aneuploidy using FISH on embryos from women withMA or with a history of RA has resulted in increased
mplantation rates (6, 11) and ongoing pregnancy rates (12)s well as a significant reduction in spontaneous abortion inomen �35 years old with a history of RA (13). This
onfirms that this limited analysis of the karyotype is suffi-ient to detect a significant cause of pregnancy failure inhese groups of patients. Results have been more equivocalrom patients with recurrent implantation failure (6, 11, 12,4–16). This may be because RIF can be caused by variousactors, or because the chromosomes that are being investi-ated in the test are less specific for the chromosome abnor-ality associated with RIF than for that associated withMA and RA.
Comparative genomic hybridization (CGH) is a molecularytogenetic technique that allows a total genome scan forhromosome abnormality to be conducted on a single cell17, 18). The test is labor intensive and takes 5 days toomplete. This necessitates cryopreservation of the embryo,hich reduces implantation potential by approximately 30%
19). This has been a limitation of the general application ofhe technique. Previously reported studies using CGHhowed that any chromosome can be involved in abnormal-ty in human blastomeres (17, 18).
Early FISH investigations of cleavage embryos identifiedchaotic embryos” in which the chromosome complement ofndividual blastomeres varies markedly (20). The CGH tech-ique has identified complex chromosome abnormality as aain feature of chaotic embryos (17, 18), in which complex
bnormality is defined as whole chromosome imbalancenvolving more than two chromosomes (17). Complex ab-ormality generally occurs during mitotic division in thembryo (17, 18, 21–23), and may be present in any numberf the cells of the embryo, with individual cells havingifferent karyotypic abnormalities (17, 18). Furthermore,bservations from CGH studies have shown that chromo-ome involvement in complex abnormality is random (24),nd this recently has been confirmed by an initial investiga-ion using CGH arrays (24). In our earlier report of databtained using CGH to carry out preimplantation geneticiagnosis (PGD) aneuploidy screening on embryos fromomen referred for RIF, we confirmed (23) extensive studiessing FISH that have shown that the level of aneuploidy inleavage embryos is higher in women of AMA (9, 10). Theata also suggested that the incidence of complex abnormal-ty was higher in the diagnostic study group than that seen inarlier studies of disaggregated embryos in which the em-ryos were surplus to the needs of the patients (17, 18).
Here we present data from PGD aneuploidy screeningsing CGH on 176 embryos from 28 women referred forneuploidy screening. Twenty-two women had a history of
IF, and six did not. The data permit a direct comparison of d1054 Voullaire et al. Complex abnormality in PGD AS
he PGD findings in women with and without a history ofIF.
ATERIALS AND METHODSatient Selection and IVF Procedurewenty-two women were referred for PGD aneuploidycreening because of a history of RIF, and six women wereeferred for other reasons but with no history of RIF. In theatter group, three were of AMA, two had a history of RA,nd one had insisted on the test after television coverage ofhe work. Women were classified as having RIF irrespectivef maternal age when at least 10 (mean 16.5) or morembryos had been transferred previously without achieving aregnancy. Women who were classified as not having aistory of RIF had had 0 (4 women), 4 (1 woman), or 8 (1oman) embryos transferred. All couples underwent coun-
eling, which is mandatory in the State of Victoria, beforeVF. Women considering PGD attend an additional sessionith a genetic counselor before deciding whether to consent
o embryo biopsy and preimplantation screening for aneu-loidy by CGH. The procedures have been approved by ournstitutional review board.
Multiple ovarian follicular development was achieved bydministration of exogenous gonadotrophins. After collec-ion, oocytes were inseminated by intracytoplasmic injectionf a single sperm (ICSI), and embryos were cultured inuman Tubal Fluid (HTF, Irvine Scientific, CA). On day 2
fter insemination, the morphology of the embryos wasssessed and graded on the basis of cytoplasmic fragmenta-ion (grade 1 embryos have �5 cytoplasmic fragments,rade 2 embryos have up to 10% fragmentation, and grade 3mbryos have 10% to 30% fragmentation). Poorer-qualityrade 4 or 5 embryos did not proceed to PGD. Early on dayof development the number of blastomeres per embryo wasetermined. Embryos were biopsied 2 to 5 hours later, whensingle blastomere was biopsied from embryos that were
rade 1 to 3 and contained at least six cells. The full detailsf the clinical IVF procedures and embryo biopsy are de-cribed elsewhere (25, 26).
ryopreservation and Thawing of Biopsied Embryosingle-cell CGH takes 5 days to complete, necessitating thereezing of the embryos for transfer at a later cycle. Initiallyiopsied embryos were cryopreserved and thawed usingethods found to be successful for intact cleavage-stage
mbryos (19). Modifications to the method were imple-ented during this study that have improved the survival
ate of biopsied embryos (27).
omparative Genomic Hybridizationlastomeres were analyzed using CGH as previously de-
cribed by us (28, 29). Individual blastomeres underwentlkaline lysis followed by whole-genome amplification using
egenerative oligonucleotide primed polymerase chain reac-Vol. 87, No. 5, May 2007

tlIpaITnisCpngcws
AIcvwvivbtw
DTepgaw
twwobeSTg
RPitwSwoacissyo(ci2
frhbfimi
F
ion (DOP-PCR). The DOP-PCR product (test DNA) wasabeled with Spectrum Green (Vysis Inc, Downers Grove,L) by nick translation. Genomic DNA extracted from lym-hocytes from a normal man was amplified using DOP-PCR,nd the PCR product was labeled with Spectrum Red (Vysisnc) by nick translation to provide a normal reference DNA.est and reference DNA were simultaneously hybridized toormal male metaphase template slides, and the fluorescentmages were captured and analyzed using Cytovision CGHoftware (Version 3.52, 1997; Applied Imaging, Santa Clara,A) to determine the average green:red fluorescence ratiorofile for each chromosome. When the relative DNA copyumber in the test and reference DNA is the same, thereen:red fluorescence ratio is 1.0. When the relative DNAopy number is less in the test DNA, the ratio is �1.0, andhen it is in excess, the ratio is �1.0. Thresholds for
ignificant deviation were set at 0.75 and 1.25.
neuploidy and Complex Abnormalityn the context of analysis using CGH, we have definedomplex abnormality as whole-chromosome imbalance in-olving three or more chromosomes. In the majority of cellsith complex abnormality the abnormality is extensive, in-olving more than 4 chromosomes. When there is extensivembalance in the karyotype, the precise chromosomal in-olvement cannot be reliably defined from the CGH profilesecause each chromosomal profile is determined relative tohe cell mean fluorescence (17, 30). We define aneuploidy ashole-chromosome imbalance of one or two chromosomes.
ata Analysishe proportion of embryos with aneuploidy vs. all othermbryos (including those with a normal karyotype and com-lex abnormalities) were compared between maternal ageroups (�37 years and �37 years) and between women withnd without a history of RIF. The proportion of embryosith complex abnormalities was compared similarly be-
TABLE 1Cytogenetic results obtained from preimplantatioblastomere from embryos from 28 patients: the ntwo chromosomes or complex abnormality withi
No. embryos a
Aneuploidy 1–2chromosomes
Maternal age �37 y 23 (18.9%)Maternal age �37 y 23 (42.6%)Combined 46 (26.1%)Note: Maternal age vs. aneuploidy, OR � 3.3 (95% CI � 1
� 1.0 (95% CI � .5 to 2.2), P�.99.
Voullaire. Complex abnormality in PGD AS. Fertil Steril 2007.
ertility and Sterility�
ween the maternal age groups and between women with andithout a history of RIF. Odds ratios (ORs) were calculatedith 95% confidence intervals (CIs), and P values werebtained from �2 tests. To account for possible correlationetween embryos from the same woman (31), generalizedstimating equations (GEE) were calculated using xtgee inTATA (version 9, 2005, StataCorp, College Station, TX).he ORs, 95% CIs, and P values from these models areiven in the tables.
ESULTSreimplantation diagnosis for chromosome abnormality us-
ng CGH was successfully carried out on individual blas-omeres biopsied from 176 embryos from 28 women, ofhom 22 had a history of RIF and 6 had no history of RIF.eventy-six (45%) embryos showed a normal karyotype andere suitable for transfer, 46 (27%) showed aneuploidy forne or two chromosomes, 7 (4%) showed partial aneuploidy,nd 49 (29%) had complex abnormality. Of the cells withomplex abnormality, 45 of 49 had chromosomal imbalancenvolving more than four chromosomes. Analysis of the datahows that the level of aneuploidy for one to two chromo-omes is significantly higher for embryos from women 37ears of age or older (taken as the age at which fertilizationccurred) than for embryos from women �37 years of ageOR � 3.3, 95% CI � 18 to 6.0, P�.001) (Table 1). Inontrast, the risk of complex abnormality was found to bendependent of maternal age (OR � 1.0, 95% CI � 0.5 to.2, P�.99) (Table 1).
The majority of the women (22 of 28) had been referredor aneuploidy screening because of a history of RIF. Theemainder of the women, with the exception of one woman,ad been referred because of AMA or with a history of RA,ut none had a history of RIF. Analysis of the chromosomendings on the basis of whether the women, irrespective ofaternal age, had a history of RIF or not showed that the
ncidence of embryos with aneuploidy for one to two chro-
neuploidy screening (CGH) of a singleber (%) of embryos with aneuploidy for one toaternal age groups.
zed
Complexabnormal All other
Totalembryos
34 (27.9%) 65 (53.2%) 12215 (27.8%) 16 (29.6%) 5449 (27.8%) 81 (46.0%) 1766.0), P�.001. Maternal age vs. complex abnormality, OR
n aum
n m
naly
.8 to
1055

m�taw3cwwaWsi
DOeaahdbdpmi
ac3cgpirc
aipcd
ati(fWodsaaatpia
Rbshtc�sapip
osomes was independent of the referral indication (OR0.7, 95% CI � 0.3 to 1.7, P�.358) (Table 2). In comparison,
he level of complex abnormality was significantly increasedmong embryos from women who had had RIF comparedith those from women who had no history of RIF (OR �.5, 95% CI � 1.1 to 10.9, P�.035) (Table 2). The OR foromplex abnormality is significant in the RIF group evenhen clustering is accounted for. The number of patientsith no history of RIF was too small to permit independent
nalysis of two other referral categories (AMA and RA).ithin the recurrent implantation failure group there was no
ignificant difference in the incidence of complex abnormal-ty in the two maternal age groups.
ISCUSSIONbservation of chromosome abnormality in human cleavage
mbryos using the molecular cytogenetic techniques of FISHnd CGH has identified single and multiple chromosomeneuploidy, partial aneuploidy after chromosome breakage,aploidy, polyploidy, and complex abnormality. Studies ofisaggregated embryos have shown that the abnormality cane either meiotically or mitotically (i.e., postzygotically)erived. There is evidence showing that meiotic abnormalityreferentially involves specific chromosomes, whereas initotic chromosome abnormality there is a more random
nvolvement of the chromosomes (23).
In the investigation of chromosome abnormality in cleav-ge embryos, the presence of aneuploidy for three or morehromosomes has been defined as complex abnormality (17,2). Because complex abnormality has a relatively low in-idence in oocytes (21, 22), and as complex abnormality isenerally mosaic, it can be assumed to be generally ofostzygotic occurrence. The complex abnormality observedn blastomeres, which often involves total karyotypic disar-ay, is specific to early embryonic development. Tumor cells
TABLE 2Cytogenetic results obtained from preimplantatioblastomere from embryos from 28 patients: the ntwo chromosomes, or complex abnormality, fromfailure (RIF) are compared with those without a h
No. embryos an
Aneuploidy 1–2chromosomes
History of RIF 35 (24.6%)No history of RIF 11 (32%)Combined 46 (26.1%)Note: RIF vs. aneuploidy, OR � 0.7 (95% CI � 0.3 to 1.7), P
to 10.9), P�.035.
Voullaire. Complex abnormality in PGD AS. Fertil Steril 2007.
an frequently have similar karyotypic disarray, but gener- �
1056 Voullaire et al. Complex abnormality in PGD AS
lly the chromosome number remains high. In comparison,n some dividing blastomeres only a few chromosomes areresent (17), probably reflecting the lack of dependency ofell division on the cellular (fetal) genome at this stage inevelopment.
Previous analysis of results obtained from preimplantationneuploidy screening using CGH carried out on single blas-omeres from the embryos of women referred with recurrentmplantation failure (23) confirmed data from FISH studies9, 10), showing that the level of chromosome aneuploidyor one to two chromosomes is increased in women of AMA.
e further confirm these findings with this enlarged groupf patients by showing that the risk of having an embryoiagnosed with an aneuploidy involving one or two chromo-omes increases with maternal age (Table 1). Studies havelso shown that mitotic abnormality is generally not associ-ted with maternal age (9, 10), except where the mitoticbnormality is caused by nondisjunction (32). We show herehat complex abnormality detected at PGD by CGH is inde-endent of maternal age (Table 1), confirming the generalndependence of mitotic abnormalities in relation to maternalge.
The majority of women studied (22 of 28) had a history ofIF, whereas six women were referred for other indicationsut did not have a history of RIF. Analysis of the chromo-ome findings on the basis of whether the women had aistory of RIF or not (irrespective of maternal age) showedhat the incidence of embryos with aneuploidy for one to twohromosomes is independent of a past history of RIF (OR
0.7, 95% CI � 0.3 to 1.7, P�.358) (Table 2). These resultsuggest that aneuploidy for one to two chromosomes is notsignificant cause of recurrent implantation failure. In com-arison, the level of complex abnormality is significantlyncreased among embryos from women who had RIF com-ared with embryos from women with no history of RIF (OR
neuploidy screening (CGH) of a singleber (%) of embryos with aneuploidy for one totients with a history of recurrent implantationry of RIF.
ed
Complexabnormal
All otherembryos
Totalembryos
45 (31.6%) 62 (43.7%) 1424 (11.8%) 19 (55.9%) 34
49 (27.8%) 81 (46%) 17658. RIF vs. complex abnormality, OR � 3.5 (95% CI � 1.1
n aumpa
isto
alyz
�.3
3.5, 95% CI � 1.1 to 10.9, P�.020) (Table 2).
Vol. 87, No. 5, May 2007

cfse(taehbwlarr
j(epwdpfinaa
Ctmrccntiee(maspowru
ipnp
emcbrmkfmdaaarllpfo
R
1
1
1
1
F
In a previous report (23), we suggested that the level ofomplex abnormality in our PGD study group of embryosrom 20 women referred with recurrent implantation failureeemed to be higher than in our study of 12 disaggregatedmbryos that had been classified as surplus to patient needs17). We had two reservations about this comparison. First,he studies were conducted differently, and second, the di-gnostic group had had ICSI, whereas the disaggregatedmbryos had been normally fertilized. The data presentedere of chromosome abnormality detected at PGD in em-ryos allow a direct comparison between embryos fromomen with and without a history of RIF, and show that the
evel of complex abnormality is not dependent on maternalge but is increased in women with RIF. Furthermore, theesults suggest that ICSI is not associated with an increasedisk for complex abnormality.
A study using FISH and 13 probes showed that the ma-ority of abnormalities detected are observed using 5 probes82%), with a further 15% of abnormalities detected using anxtra 4 probes, whereas with the addition of a further 4robes a further 3% of abnormalities is detected (33). Itould be anticipated that a complete genome study wouldetect further abnormalities than those detected with the 13robes, albeit at a low rate. This concurs with the resultsrom our previous CGH study of embryos screened at PGD,n which we showed that 38% of abnormal embryos wouldot be diagnosed as abnormal if a five-probe set were used,nd 25% of abnormal embryos would still be undiagnosed iffurther 4 probes were included.
Complex abnormality is more accurately identified usingGH than with FISH because of the ability of this technique
o provide a whole-genome analysis. Chromosome involve-ent in complex abnormality seems to be random, and as a
esult FISH will miss complex abnormality if none of thehromosomes included in the FISH set are involved in theomplex abnormality (13, 24). Alternatively, complex ab-ormality will be misinterpreted as aneuploidy if only one orwo of the chromosomes involved in the complex abnormal-ty are included in the FISH set. In the study of disaggregatedmbryos using FISH, the same problem arises, in which thembryo might be described as chaotic. Chaotic embryosembryos with different abnormalities in different cells)ight arise after chaotic division associated with complex
bnormality or through mitotic loss and/or gain of one oreveral chromosomes. The inability of FISH to detect com-lex abnormality in all cases might be a factor in the equiv-cal results obtained from PGD testing of RIF patients, asell as an explanation for the slightly higher implantation
ate obtained when PGD using CGH is compared with PGDsing FISH (25).
Aneuploidy for one to two chromosomes in early embryoss generally meiotically derived, but also may occur at aostzygotic division. It seems to occur after chromosomeondisjunction, chromosome lag, or chromosome endoredu-
lication. Complex abnormality can be assumed to be gen-ertility and Sterility�
rally mitotically derived because the chromosome abnor-ality is only observed at a low incidence in oocytes (21, 22)
ompared with blastomeres, in studies of disaggregated em-ryos it is often only present in some cells, and also it variesandomly between different cells in the embryo (17, 18). Theechanism leading to the formation of the abnormality is not
nown, but it is considered to be dependent on the lack ofunctioning cell cycle checkpoints at that stage of develop-ent (20). Further support for postulating an underlying
ifference in the mechanism between complex abnormalitynd aneuploidy is obtained from the difference in effect ofdvancing maternal age on the incidence of the two types ofbnormality. Therefore it is likely that complex abnormalityesults from a different type of underlying cellular or mo-ecular pathology than that associated with mitotic or meioticoss or gain of one or two chromosomes. We have previouslyostulated that this might be caused by heritable maternalactors. The data presented here suggest that some women,r couples, might be prone to this type of abnormality.
EFERENCES1. Boué A, Boué J, Gropp A. Cytogenetics of pregnancy wastage. Adv
Hum Genet 1995;14:1–57.2. Harper JC, Coonen E, Handyside AH, Winston RML, Hopman AHN,
Delhanty JDA. Mosaicism of autosomes and sex chromosomes inmorphologically normal, monospermic pre-implantation human em-bryos. Prenat Diagn 1995;15:41–9.
3. Munné S, Grifo J, Cohen J, Weier H-UG. Chromosome abnormalitiesin human arrested preimplantation embryos: a multi-probe FISH study.Am J Hum Genet 1994;55:150–9.
4. Short RV. When a conception fails to become a pregnancy. In: WhelanJ, ed. Maternal recognition of pregnancy. Amsterdam: Excerpta Med-ica, 1979:377–87.
5. Edmonds DK, Lindsay KS, Miller JF, Williamson E, Wood PJ. Earlyembryonic mortality in women. Fertil Steril 1982;38:447–53.
6. Gianaroli L, Magli MC, Ferraretti AP, Munné S. Preimplanatationdiagnosis for aneuploidies in patients undergoing in vitro fertilisationwith a poor prognosis: identification of the categories for which itshould be proposed. Fertil Steril 1999;72:837–44.
7. Kahraman S, Bahçe M, Samli H, Imirzalioglu N, Yakisn K, Cengiz G,et al. Healthy births and ongoing pregnancies obtained by preimplan-tation genetic diagnosis in patients with advanced maternal age andrecurrent implantation failure. Hum Reprod 2000;15:2003–7.
8. Munné S, Magli C, Bahçe M, Fung J, Legator M, Morrison L, et al.Preimplantation diagnosis of the aneuploidies most commonly found inspontaneous abortions and live births: XY, 13, 14, 15, 16, 18, 21, 22.Prenat Diagn 1998;18:1459–66.
9. Munné S, Alikani M, Tomkin G, Grifo J, Cohen J. Embryo morphol-ogy, developmental rates, and maternal age are correlated with chro-mosome abnormalities. Fertil Steril 1995;64:382–91.
0. Márquez C, Sandalinas M, Bahçe M, Alikani M, Munné S. Chromo-some abnormalities in 1255 cleavage-stage human embryos. ReprodBiomed Online 2000;1:17–26.
1. Munné S, Sandalinas M, Escudero T, Velilla E, Walmsley R, SadowyS, et al. Improved implantation after preimplantation genetic diagnosisof aneuploidy. Reprod Biomed Online 2003;7:91–7.
2. Munné S, Magli C, Cohen J, Morton P, Sadowy S, Gianaroli J, et al.Positive outcome after preimplantation diagnosis of aneuploidy in hu-man embryos. Hum Reprod 1999;14:2191–9.
3. Munné S, Chen S, Fischer J, Colls P, Zheng X, Stevens J, et al.Preimplantation genetic diagnosis reduces pregnancy loss in womenaged 35 years and older with a history of recurrent miscarriages. Fertil
Steril 2005;84:331–5.1057

1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
4. ESHRE Preimplantation Genetic Diagnosis Consortium: data collectionIII (May 2001). Hum Reprod 2002;17:233–46.
5. Sermon K, Moutou C, Harper J, Geraedts J, Scriven P, Wilton L, et al.ESHRE PGD Consortium data collection IV: May–December 2001.Hum Reprod 2005;20:19–34.
6. Harper JC, Boelaert K, Geraedts J, Harton G, Kearns WG, Moutou C,et al. ESHRE PGD Consortium data collection V: cycles from Januaryto December 2002 with pregnancy follow-up to October 2003. HumReprod 2006;21:3–21.
7. Voullaire L, Slater H, Williamson R, Wilton L Chromosome analysis ofblastomeres from human embryos using comparative genomic hybrid-ization. Hum Genet 2000;106:210–7.
8. Wells D, Delhanty JDA. Comprehensive chromosomal analysis ofhuman preimplantation embryos using whole genome amplification andsingle cell comparative genomic hybridization. Mol Hum Reprod 2000;6:1055–62.
9. Edgar DH, Bourne H, Speirs AL, McBain JC. A quantitative analysis ofthe impact of cryopreservation on the implantation potential of humanearly cleavage stage embryos. Hum Reprod 2000;15:175–9.
0. Delhanty JDA, Harper JC, Ao A, Handyside AH, Winston RML.Multicolour FISH detects frequent chromosomal mosaicism and cha-otic division in normal preimplantation embryos from fertile patients.Hum Genet 1997;99:755–60.
1. Gutierrez-Mateo C, Wells D, Benet J, Sanchez-Garcia JF, BermudezMG, Belil I, et al. Reliability of comparative genomic hybridization todetect chromosome abnormalities in first polar bodies and metaphase IIoocytes. Hum Reprod 2004;19:2118–25.
2. Gutierrez-Mateo C, Benet J, Wells D, Colls P, Bermudez MG, Sanchez-Garcia J F, Egozcue J, et al. Aneuploidy study of human oocytes firstpolar body comparative genomic hybridization and metaphase II fluo-rescence in situ hybridization analysis. Hum Reprod 2004;19:2859–68.
3. Voullaire L, Wilton L, McBain J, Callaghan T, Williamson R. Chro-
mosome abnormalities identified by comparative genomic hybridiza-1058 Voullaire et al. Complex abnormality in PGD AS
tion in embryos from women with repeated implantation failure. MolHum Reprod 2002;8:1035–41.
4. Le Caignec C, Spits C, Sermon K, DeRycke M, Thienpont B, DebrockS, et al. Single-cell chromosomal imbalances detection by array CGH.Nucl Acids Res 2006;34:e68.
5. Wilton L, Voullaire L, Williamson R, McBain J. Preimplantationscreening using comparative genomic hybridization or fluorescent insitu hybridization of embryos from patients with recurrent implantationfailure. Fertil Steril 2003;80:860–8.
6. Wilton L, Williamson R, McBain J, Edgar D, Voullaire L. Birth of ahealthy infant after preimplantaation confirmation of euploidy by com-parative genomic hybridization. N Engl J Med 2001;345:1537–41.
7. Jericho H, Wilton L, Gook D, Edgar D. A modified cryopreservationmethod increases the survival of human biopsied cleavage stage em-bryos. Hum Reprod 2003;18:568–71.
8. Voullaire L, Wilton L, Slater H, Williamson R. Detection of aneuploidyin single cells using comparative genomic hybridization. Prenat Diagn1999;19:846–51.
9. Wilton L, Voullaire L. Preimplantation genetic diagnosis using com-parative genomic hybridization in a clinical IVF laboratory setting. In:Martin D, ed. Methods in molecular medicine. Nashville: Parthenon,2004:329–39.
0. Piper J, Rutovitz D, Sudar D, Kallioniemi A, Kallioniemi OP, WaldmanFM, et al. Cytometry 1995;19:10–26.
1. Hogan JW, Blazar AS. Hierarchical logistic regression models forclustered binary outcomes in studies of IVF-ET. Fertil Steril 2000;73:575–81.
2. Munné S. l Chromosome mosaicism in cleavage stage human em-bryos: evidence of a maternal age effect. Reprod Biomed Online2002;4:223–32.
3. Abdelhadi I, Colls P, Sandalinas M, Escudero T, Munné S. Preimplan-tation genetic diagnosis of numerical abnormalities for 13 chromo-
somes. Reprod Biomed Online 2003;6:226–31.Vol. 87, No. 5, May 2007

Amintbi
rslcfl
RS
R
MALE FACTOR
0d
Stimulation of the nitric oxide/cyclic guanosinemonophosphate signaling pathway elicits humansperm chemotaxis in vitroErica Miraglia, B.Sc.,a Maria Luisa Rullo, B.Sc.,b Amalia Bosia, M.D.,a Marco Massobrio, M.D.,b
Alberto Revelli, M.D.,b and Dario Ghigo, M.D.a
a Department of Genetics, Biology and Biochemistry, University of Torino, 10126 Torino, Italy; and b Reproductive Medicine andIVF Unit, Department of Obstetrical and Gynecological Sciences, University of Torino, S. Anna Hospital, 10126 Torino, Italy
Objective: To investigate whether nitric oxide (NO) may attract human spermatozoa via activation of the solubleguanylate cyclase (sGC)/cyclic guanosine monophosphate (cGMP) pathway.Design: Prospective study.Setting: Academic research institution.Patient(s): Seven normozoospermic patients belonging to couples presenting for infertility evaluation.Intervention(s): Sperm samples were processed by the swim-up technique.Main Outcome Measure(s): Sperm chemotaxis detected by a choice device (specially designed three-wellplexiglass chamber), intracellular level of cGMP (by radioimmunoassay), and sperm motility parameters (bycomputer-assisted sperm analysis).Result(s): After a 20-minute incubation, the NO donor S-nitrosoglutathione (GSNO) increased the synthesis ofcGMP and exerted a significant chemoattraction on human spermatozoa. The GSNO-induced migration of spermwas inhibited by PTIO (a NO scavenger), ODQ (an sGC inhibitor), and Rp-8-Br-cGMPS (an inhibitor ofcGMP-dependent protein kinases). The cell-permeating cGMP analog 8-Br-cGMP acted as a potent chemoat-tractant per se: this effect was inhibited by Rp-8-Br-cGMPS.Conclusion(s): These data suggest that NO may exert a chemoattractant effect on human spermatozoa and that thesignal transduction involves the activation of sGC, the synthesis of cGMP, and the activation of cGMP-dependentprotein kinases. (Fertil Steril� 2007;87:1059–63. ©2007 by American Society for Reproductive Medicine.)
Key Words: Cyclic GMP (cGMP), soluble guanylate cyclase (sGC), nitric oxide (NO), sperm chemotaxis, spermmotility, cGMP-dependent protein kinases (PKGs)
mTr
ccAhaTtso
whdn
ttraction between gametes of the opposite sexes by che-otaxis (the modulation of the movement direction accord-
ng to the gradient of a chemoattractant) is a common phe-omenon in marine species with external fertilization (1). Inhe last decade, such a chemical guidance mechanism haseen described also in sperm of species with internal fertil-zation, such as mammals, including humans (2).
Chemotactic egg-derived peptides, such as resact and spe-act, have been identified in echinoderms: their binding topecific sperm receptors belonging to the membrane guany-ate cyclase (mGC) family causes an increase of intracellularyclic guanosine monophosphate (cGMP) and mediates ionuxes across the sperm membrane; in turn, this affects flagellar
eceived April 3, 2006; revised and accepted July 24, 2006.upported by grants (PRIN, ex-60%) from Ministero dell’Università edella Ricerca, Rome, Italy.
eprint requests: Dario Ghigo, M.D., Dipartimento di Genetica, Biologia eBiochimica—Sezione di Biochimica, Via Santena, 5/bis, 10126 Torino,
sItaly (FAX: �39-011-6705845; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.07.1540 Copyright ©2007 American Soc
otion and finally determines the direction of movement (3).hus, cGMP is considered to play a pivotal role in the motility
esponse of sea urchin sperm to chemoattractants.
On the other hand, the molecular mechanisms of spermhemotaxis in mammals are largely unknown, and the role ofGMP in human sperm functions still needs to be clarified.trial natriuretic peptide (ANP), another ligand for mGC,as been observed to attract human spermatozoa in vitro (4)nd has been proposed as a chemotactic signal in mammals.his hypothesis is still waiting confirmation. In the mean-
ime, signaling pathways not involving cGMP have beenuggested, such as the release of progesterone (5) or ligandsf G protein–associated odorant receptors (6).
In most cells, a soluble guanylate cyclase (sGC) coexistsith mGC. One of its main activators is nitric oxide (NO), aighly reactive free radical gas which participates as a me-iator in several biologic processes, such as vasodilatation,eurotransmission, immune response, and apoptosis, and is
ynthesized from L-arginine by NADPH-dependent NO syn-1059Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

ttbsstrthaaca1phia
MRSl[afc3wSaAp(w
SSdttsaaeatmlu
nTst
srwtcpsw
CTfWtoctotiwcwwMp
MTdim�faswp3Enn1s
MActaptww
hases (NOS) (7). The sGC isoform has been recently iden-ified in human sperm by immunoblotting (8), and NO haseen shown to increase the intracellular levels of cGMP inpermatozoa: the NO donors sodium nitroprusside andpermine-NONOate have been reported to increase the in-racellular cGMP levels in human and murine spermatozoa,espectively (9, 10). It has been reported that low concen-rations of NO enhance the motility of mouse, hamster, anduman spermatozoa, the acrosomal reactivity of mouse, bull,nd human spermatozoa, and the zona pellucida–bindingbility of human spermatozoa (9, 10). However, higher NOoncentrations exert detrimental effects on the motility, vi-bility, and metabolism of human spermatozoa in vitro (10,1). Until now, no experimental evidence exists about aossible involvement of the NO/cGMP signaling pathway inuman sperm chemotaxis. The aim of this work has been tonvestigate whether NO may attract human spermatozoa viactivation of the sGC/cGMP pathway.
ATERIALS AND METHODSeagents-Nitrosoglutathione (GSNO), 2-phenyl-4,4,5,5-tetramethy-
imidazoline-1-oxyl-3-oxide (PTIO), 1H-[1,2,4]oxadiazolo-4,3-a]quinoxalin-1-one (ODQ), 8-bromo-cGMP (8-Br-cGMP),nd 3-isobutyl-1-methylxanthine (IBMX) were purchasedrom Sigma Chemical Co. (St. Louis, MO). The inhibitor ofGMP-dependent protein kinases (PKGs) 8-bromoguanosine-=,5=-monophosphorothioate Rp-isomer (Rp-8-Br-cGMPS)as from Biolog Life Science Institute (Bremen, Germany).perm-washing medium (SWM) was from Celbio (Milan, It-ly). The [3H]cGMP radioimmunoassay kit was supplied bymersham International (Buckinghamshire, UK). Electro-horesis reagents were obtained from Bio-Rad LaboratoriesHercules, CA). The protein content of cell lysates was assessedith the bicinchoninic acid kit from Pierce (Rockford, IL).
perm Samplesperm samples were obtained by masturbation after 3–5ays of sexual abstinence from seven normozoospermic pa-ients belonging to couples presenting for infertility evalua-ion. Each donor gave informed consent about the use of hisemen for our experiments. The Institutional Review Boardpproval was obtained by the internal ethical committee thatuthorized the use of semen samples submitted to semenxamination for experimental purposes. All samples werellowed to liquefy for at least 30 minutes at 37°C, and thenhey were evaluated for sperm concentration, motility, andorphology according to World Health Organization guide-
ines (12). Only specimens with normal parameters weresed in the experiments.
Motile spermatozoa were harvested by the swim-up tech-ique (37°C for 2 hours in a 5% CO2 atmosphere) using SWM.he presence of round cells was initially below 1 � 106 in allperm samples and was minimal if not absent after the swim-up
echnique in the final suspension. After swim-up, the motile l1060 Miraglia et al. NO/cGMP signaling and sperm chemotax
perm–rich fraction was centrifuged at 600g for 10 minutes atoom temperature, the supernatant was removed, and the pelletas resuspended in SWM. Then, concentration and motility of
he spermatozoa suspension were assessed in a Makler countinghamber (Sefi Medical Instruments, Haifa, Israel) under ahase-contrast microscope (magnification 20�). Only suspen-ions containing �40 � 106 spermatozoa/mL (seven samples)ere used in the experiments.
hoice Assayhe separation of spermatozoa by chemotaxis was per-
ormed in a three-well plexiglass chamber (provided byeizmann Institute of Science, Israel) (13, 14) containing
hree wells connected by capillaries. Capillaries were previ-usly filled with 65 �L SWM and closed. Subsequently, theentral well was filled with 150 �L sperm suspension andhe lateral wells were filled with an equal volume of SWMnly (control well) or SWM containing the substance(s) toest (sample well). The separation chamber was put into anncubator (5% CO2 atmosphere, 37°C), and the capillariesere opened to allow spermatozoa to migrate from the
entral to the lateral wells. After 20 minutes, the capillariesere closed; 150 �L suspension was collected from eachell, and spermatozoa concentration was assessed using aakler counting chamber. Each experimental condition was
erformed in duplicate for each sperm sample.
easurement of Intracellular cGMPhe level of intracellular cGMP was measured as previouslyescribed (15). Briefly, aliquots (500 �L) of sperm suspensionsn SWM, containing 15 � 106 cells, were pretreated for 20inutes with the phosphodiesterase inhibitor IBMX (200mol/L) to inhibit cGMP hydrolysis and then were coincubated
or 20 minutes with the same substances used in the choicessay (GSNO, ODQ, PTIO, and 8-Br-cGMP). Subsequently,amples were centrifuged at 13,000g for 1 minute. Supernatantsere discarded, and 50 �L absolute ethanol was added to theellets; ethanol was evaporated by vacuum centrifugation, and50 �L Tris/EDTA buffer (50 mmol/L Tris-HCl, 4 mmol/LDTA, pH 7.5) was added. After 10 minutes, 100 �L super-atant was tested for the cGMP level with a [3H]cGMP immu-oassay system. Cyclic GMP content was expressed as pmol/06 cells. Cross-reactivity of the [3H]cGMP immunoassayystem with cAMP was less than 0.001%.
easurement of Kinetic Parametersliquots of sperm suspensions (200 �L) in SWM, each
ontaining 40 � 106 cells, were incubated for 20 minutes inhe absence or presence of the substances used in the choicessay. Sperm motility parameters were measured by com-uter-assisted sperm analysis (CGA-WLJY-9000; CGA Dis-ribution, Florence, Italy). The following kinetic parametersere measured: percentage of spermatozoa exhibiting a for-ard progressive motility (A�B WHO classes); straight
inear velocity (VSL, expressed as �m/s); curvilinear veloc-
is Vol. 87, No. 5, May 2007

i�dc
SAaTP
RIctfNdc(ccGRmo
swcd8th
oivanUes
DIpmcstamsaza
Nsdmcw
F
ty (VCL, expressed as �m/s); linearity [LIN � (VSL/VCL)100]; and straightness (STR, the percentage of correspon-
ence of the cell’s pathway to a straight line, with 100%orresponding to the maximal extent of straightness) (16).
tatistical Analysisll data are provided as mean � SEM. The results were
nalyzed by a one-way analysis of variance (ANOVA) andukey test (SPSS 11.0 for Windows; SPSS, Chicago, IL). Avalue of �.05 was considered to be significant.
FIGURE 1
Human sperm chemotactic response to nitricoxide (NO)/cyclic guanosine monophosphate(cGMP) pathway–modulating substances. Columnsindicate the percentage of human spermatozoamigrated in the test wells containing differentsubstances versus the percentage of spermatozoamigrated in the respective control well, which wasassumed as 100%. Test wells contained, alone ordifferently combined, the following substances:S-nitrosoglutathione (GSNO, 100 nmol/L), 2-phenyl-4,4,5,5-tetramethylimidazoline-1-oxyl-3-oxide (PTIO, 100 �mol/L), 1H-[1,2,4]oxadiazolo-[4,3-a]quinoxalin-1-one (ODQ, 50 �mol/L), 8-bromo-cGMP (8-Br-cGMP, 1 mmol/L), and 8-bromoguanosine-3=,5=-monophosphorothioate Rp-isomer (Rp-8-Br-cGMPS, 10 �mol/L). All data arepresented as mean � SEM (n � 7). The meanvalue of spermatozoa in the control wells was 8� 2. Significance vs. control: *P�.02; **P�.002;***P�.001; vs. GSNO: °P�.01; °°P�.005;°°°P�.001; vs. ODQ: #P�.001; vs. GSNO � ODQ:§P�.001; vs. 8-Br-cGMP: ^P�.01.
tMiraglia. NO/cGMP signaling and sperm chemotaxis. Fertil Steril 2007.
ertility and Sterility�
ESULTSn the choice assays, after a 20-minute incubation the per-entage of spermatozoa that migrated in the well containinghe NO donor GSNO was significantly higher than the oneound in the control well (Fig. 1). The presence of either theO scavenger PTIO or the sGC inhibitor ODQ (which bothid not exhibit any significant effect when added alone)ompletely inhibited the chemoattraction exerted by GSNOFig. 1). On the other hand, 8-Br-cGMP, a cell-permeatingGMP analog, acted as a potent chemoattractant per se, andompletely reverted the inhibitory effect of ODQ on theSNO-elicited migration (Fig. 1). Finally, the PKG inhibitorp-8-Br-cGMPS alone did not significantly affect the che-otactic movement of spermatozoa but abolished the effects
f GSNO and 8-Br-cGMP on sperm migration (Fig. 1).
Under the same concentration and incubation time, GSNOignificantly increased the synthesis of cGMP (Fig. 2),hereas PTIO and ODQ reduced the intracellular level of
GMP and completely abolished the increase of cGMP in-uced by GSNO (Fig. 2). As expected, after incubation with-Br-cGMP, alone or together with PTIO or ODQ, the in-racellular content of the cyclic nucleotide was significantlyigher than the control (Fig. 2).
Finally, to evaluate whether NO could exert an effect alson sperm motility, progressive motility was measured afterncubation under the same experimental conditions of pre-ious experiments. The results reported in Table 1 show that20-minute incubation with these compounds did not sig-
ificantly alter the progressive motility of human sperm.nder the same experimental conditions, the kinetic param-
ters investigated (VCL, VSL, STR, and LIN) were notignificantly modified (data not shown).
ISCUSSIONncreasing evidence supports a role for the NO/cGMP-signalingathway in modulating several biologic functions of the mam-alian reproductive tract (17). As far as male gametes are
oncerned, NO released by sodium nitroprusside has beenhown to play an important role in mouse sperm hyperactiva-ion and in the maintenance of post-thaw human sperm motilitynd viability, whereas the NOS inhibitor NG-nitro-L-arginineethyl ester and the NO scavenger methylene blue inhibited
perm motility (9, 10). Moreover, spermatozoa themselves areble to produce NO, and the basal release of NO by spermato-oa has been observed to be higher in normozoospermic than insthenospermic sperm samples (18).
In the present study, the experimental data suggest that theO/cGMP-signaling pathway could be involved in human
perm chemotaxis. In a choice assay that was previouslyemonstrated to be appropriate to assess human sperm che-otaxis (13, 14), the NO donor GSNO exerted a significant
hemoattractant effect on human spermatozoa. This effectas mediated by NO, because it was completely reverted by
he NO scavenger PTIO. This is in accordance with previous
1061

rseboGsa
acGwOt
pcoecowim
apsstrctPdnicb
wtdaesldcdcba
sTocadgucbtsnN
esults reporting that sodium nitroprusside is able to exert aignificant chemotactic effect on murine sperm (19): suchffect on mouse spermatozoa was detectable at a 50 nmol/Lut not at a 100–200 nmol/L concentration, whereas webtained a significant chemotactic effect using 100 nmol/LSNO. This difference may be attributable to the different
pecies examined, the longer time of incubation (3–5 hours),nd the different kind of NO donor (19).
The effect of NO released from GSNO is likely to be medi-ted by cGMP, because ODQ, an inhibitor of sGC, reverted thehemoattractant action exerted by GSNO. The incubation withSNO increased the intracellular level of cGMP, an effect thatas completely prevented with the presence of either PTIO orDQ. Furthermore, the cGMP analog 8-Br-cGMP, whose in-
FIGURE 2
Intracellular cGMP in human spermatozoaincubated with NO- and cGMP-modulating agents.Sperm samples were pretreated with 200 �mol/L3-isobutyl-1-methylxanthine (IBMX) for 20 min andsubsequently incubated in the absence (CTRL) orpresence of the following substances, alone ordifferently combined: 100 nmol/L GSNO, 100�mol/L PTIO, 50 �mol/L ODQ, and 1 mmol/L 8-Br-cGMP (abbreviations as in Fig. 1). After 20 min,intracellular cGMP concentration was determinedas described in the Materials and Methodssection. Data are presented as mean � SEM(n � 4). Significance vs. control: *P�.02; **P�.005;***P�.001; vs. GSNO: °P�.002; °°P�.001; vs.GSNO � ODQ: #P�.02; vs. GSNO � PTIO:^P�.02.
Miraglia. NO/cGMP signaling and sperm chemotaxis. Fertil Steril 2007.
racellular content increased 3.5-fold after incubation, was able c
1062 Miraglia et al. NO/cGMP signaling and sperm chemotax
er se to elicit a threefold increase of sperm attraction whenompared with controls. As expected, the effect of 8-Br-cGMPn sperm migration was not significantly modified by the pres-nce of ODQ and GSNO, confirming that ODQ inhibitedhemotaxis by impairing cGMP synthesis. Finally, no changef progressive motility under the same experimental conditionsas observed, suggesting that the chemotactic effects observed
n the choice assay are not related to an increase of spermotility.
Taken together, these data suggest that NO may behave aschemoattractant for human spermatozoa, and its signaling
athway might involve the activation of sGC and the sub-equent increase of intracellular cGMP levels. Cyclic GMPeems to play a role in human sperm chemotaxis via activa-ion of a PKG, because the PKG inhibitor Rp-8-Br-cGMPSeverted the chemoattractant effect of both GSNO and 8-Br-GMP. The PKGs are a family of serine/threonine kinaseshat are expressed in mammals under two different isoforms,KG I and PKG II (20). In a recent study, no PKG I wasetectable by immunoblotting in human sperm (8); this doesot rule out the possibility that the PKG II isoform might benvolved in human sperm chemotaxis. Indeed, Rp-8-Br-GMPS is a nonspecific PKG inhibitor, and is able to blockoth isoforms (21).
The role of cGMP in invertebrate sperm chemotaxis isidely acknowledged; as far as mammalian sperm chemo-
axis is concerned, fewer data are available. More than aecade ago, Zamir et al. (4) observed that ANP, a knownctivator of mGC, induces attraction and swimming speednhancement on human spermatozoa in vitro; the authorsuggested that either an ANP-like substance is the physio-ogic attractant for human spermatozoa or, more likely, ANPirectly affects guanylate cyclase in a manner similar to thataused by the physiologic, still unknown, attractant (4). Ourata are in line with this report, providing evidence thatGMP plays a role in mammalian sperm chemotaxis inducedy NO; furthermore, we show that cGMP-induced spermttraction involves the activation of PKGs.
It has been recently observed that human oocytes andurrounding cumulus cells secrete sperm chemoattractants.his suggests that sperm chemoattractants are secreted notnly before ovulation within the follicle, but also after oo-yte maturation outside the follicle (14). Nitric oxide islready known to be synthesized in the ovarian cells ofifferent mammalian species (17). Its features make NO aood candidate as a chemotactic factor. Indeed it is relativelynreactive to be a free radical, so that it can diffuse from theell in which it is produced to the neighbor cells withouteing destroyed before reaching its target (22). Furthermore,he distance to which NO may diffuse in a very short time isurprisingly long (150–300 �m in few seconds) (23). Fi-ally, the ability of human sperm to synthesize and releaseO allows one to hypothesize that during chemotaxis a
omplex interplay may occur, not only between spermatozoa
is Vol. 87, No. 5, May 2007

aa
tbNb(
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
F
nd oocytes and other cells of the reproductive tract, but alsomong spermatozoa themselves.
In conclusion, the present results suggest the possibilityhat human sperm function and fertilization potential mighte pharmacologically modulated by altering the synthesis ofO and/or cGMP. Furthermore, they show that PKGs maye implicated not only in the NO-induced acrosome reaction15) but also in human sperm chemotaxis.
EFERENCES1. Eisenbach M. Sperm chemotaxis. Rev Reprod 1999;4:56–66.2. Eisenbach M, Tur-Kaspa I. Do human eggs attract spermatozoa? Bioes-
says 1999;21:203–10.3. Neill AT, Vacquier VD. Ligands and receptors mediating signal trans-
duction in sea urchin spermatozoa. Reproduction 2004;127:141–9.4. Zamir N, Riven-Kreitman R, Manor M, Makler A, Blumberg S, Ralt D,
Eisenbach M. Atrial natriuretic peptide attracts human spermatozoa invitro. Biochem Biophys Res Commun 1993;197:116–22.
5. Jaiswal BJ, Tur-Kaspa I, Dor J, Mashiach S, Eisenbach M. Humansperm chemotaxis: is progesterone a chemoattractant? Biol Reprod1999;60:1314–9.
6. Spehr M, Gisselmann G, Poplawski A, Riffell JA, Wetzel CH, ZimmerRK, Hatt H. Identification of a testicular odorant receptor mediatinghuman sperm chemotaxis. Science 2003;299:2054–8.
7. Wink DA, Mitchell JB. Chemical biology of nitric oxide: insights intoregulatory, cytotoxic, and cytoprotective mechanisms of nitric oxide.Free Radic Biol Med 1998;25:434–56.
8. Willipinski-Stapelfeldt B, Lubberstedt J, Stelter S, Vogt K, MukhopadhyayAK, Muller D. Comparative analysis between cyclic GMP and cyclic AMPsignalling in human sperm. Mol Hum Reprod 2004;10:543–52.
9. Herrero MB, Gagnon C. Nitric oxide: a novel mediator of spermfunction. J Androl 2001;22:349–56.
0. Revelli A, Ghigo D, Moffa F, Massobrio M, Tur-Kaspa I. Guanylate
TABLE 1Effects of NO and cGMP modulation on human s
ControlGSNO (100 nmol/L)ODQ (50 �mol/L)GSNO (100 nM) � ODQ (50 �mol/L)PTIO (100 �mol/L)GSNO (100 nM) � PTIO (100 �mol/L)8-Br-cGMP (1 mmol/L)ODQ (50 �M) � 8-Br-cGMP (1 mmol/L)PTIO (100 �M) � 8-Br-cGMP (1 mmol/L)Rp-8-Br-cGMPS (10 �mol/L)GSNO (100 nM) � Rp-8-Br-cGMPS (10 �mol/L)8-Br-cGMP (1 mM) � Rp-8-Br-cGMPS (10 �mol/L)Note: Data presented as mean � SEM, n � 4. Abbreviatia Progressive motility was assessed by computer-assiste
(control) or presence of the indicated substances, alone
Miraglia. NO/cGMP signaling and sperm chemotaxis. Fertil Steril 2007.
cyclase activity and sperm function. Endocr Rev 2002;23:484–94.
ertility and Sterility�
1. Rosselli M, Dubey RK, Imithurn B, Macas E, Keller PJ. Effects of nitricoxide on human spermatozoa: evidence that nitric oxide decreases spermmotility and induces sperm toxicity. Hum Reprod 1995;10:1786–90.
2. World Health Organization. Laboratory manual for the examination ofhuman semen and sperm–cervical mucus interaction. Cambridge: Cam-bridge University Press, 1999.
3. Sun F, Giojalas LC, Rovasio RA, Tur-Kaspa I, Sanchez R, EisembachM. Lack of species-specificity in mammalian sperm chemotaxis. DevBiol 2003;15:423–7.
4. Sun F, Bahat A, Gakamsky A, Girsh E, Katz N, Giojalas LC, Tur-KaspaI. Human sperm chemotaxis: both the oocyte and the surrounding cumuluscells secrete sperm chemoattractants. Hum Reprod 2005;20:761–7.
5. Revelli A, Costamagna C, Moffa F, Aldieri E, Ochetti S, Bosia A, et al.Signaling pathway of nitric oxide–induced acrosome reaction in humanspermatozoa. Biol Reprod 2001;64:1708–12.
6. Mortimer ST. A critical review of the physiological importance andanalysis of sperm movement in mammals. Hum Reprod Update 1997;3:403–39.
7. Rosselli M, Keller PJ, Dubey RK. Role of nitric oxide in the biology,physiology and pathophysiology of reproduction. Hum Reprod Update1998;4:3–24.
8. Lewis SEM, Donnelly ET, Sterling ESL, Kennedy MS, Thompson W,Chakravarthy U. Nitric oxide synthase and nitrite production in humanspermatozoa: evidence that endogenous is beneficial to sperm motility.Mol Hum Reprod 1996;2:873–8.
9. Sliwa L, Stochmal E. Effect of sodium nitroprusside on mouse spermmigration in vitro. Arch Androl 2000;45:29–33.
0. Hofmann F. The biology of cyclic GMP–dependent protein kinases.J Biol Chem 2005;280:1–4.
1. Kawada T, Toyosato A, Islam MO, Yoshida Y, Imai S. cGMP-kinasemediates cGMP- and cAMP-induced Ca2� desensitization of skinnedrat artery. Eur J Pharmacol 1997;323:75–82.
2. Denninger JW, Marletta MA. Guanylate cyclase and the NO/cGMPsignaling pathway. Biochim Biophys Acta 1999;1411:334–50.
3. Kröncke KD, Fehsel K, Kolb-Bachofen V. Nitric oxide: cytotoxicityversus cytoprotection—how, why, when, and where? Nitric Oxide
m progressive motility.
Progressive motility(A � B),a %
67.3 � 4.968.3 � 4.865.9 � 4.664.9 � 4.066.3 � 4.763.6 � 3.665.0 � 3.162.1 � 1.962.0 � 3.464.4 � 2.663.9 � 3.066.3 � 4.5
as in Figure 1.perm analysis after a 20-min incubation in the absencedifferently combined.
per
onsd sor
1997;1:107–20.
1063

Wwiwp
eamarthrmdbtenk
RP
R
Sildenafil citrate improves sperm motility but causesa premature acrosome reaction in vitroDavid R. J. Glenn, M.R.C.O.G., Carmel M. McVicar, Ph.D., Neil McClure, F.R.C.O.G.,and Sheena E. M. Lewis, Ph.D.
School of Medicine, Obstetrics and Gynaecology, Queen’s University Belfast, Institute of Clinical Science, Belfast,United Kingdom
Objective: To determine whether sildenafil citrate, a cyclic monophosphate-specific type 5 phosphodiesteraseinhibitor, influences sperm motility or the acrosome reaction.Design: Laboratory analysis of sperm motility after exposure to sildenafil citrate using computer-assisted semenanalysis and acrosome reaction by fluorescein isothiocyanate-labeled peanut agglutinin staining.Setting: An assisted reproductive technology (ART) unit.Patient(s): Fifty-seven male patients.Intervention(s): Sperm were divided into 90% (those with the best fertilizing potential used in assistedconception) and 45% (the poorer population) fractions by density centrifugation and incubated with sildenafilcitrate (0.67 �M) at 37°C for up to 180 minutes.Main Outcome Measure(s): Both the number and velocity of progressively motile sperm were significantlyincreased by sildenafil citrate between 15 and 135 minutes. Furthermore, samples revealed that these effects wereconsistent in the 90% and 45% populations of sperm. In both populations, sildenafil also caused a significantincrease in the proportion of acrosome-reacted sperm—22.1% compared with 11.8% in the control group of thegood quality fraction and 16.6% compared with 9.4% in the control group of the poorer quality fraction.Conclusion(s): The use of sildenafil citrate may adversely affect male fertility. (Fertil Steril� 2007;87:1064–70.©2007 by American Society for Reproductive Medicine.)
Key Words: Sildenafil citrate, sperm motility, acrosome reaction
tt
redomd
cIEisst
soisnmd
ithin 14 days of its introduction in 1998, doctors wereriting more than 110,000 sildenafil scripts a week. To date
t has been prescribed to more than 23 million men world-ide and more than 1 billion doses of sildenafil have beenrescribed (1).
As a result of this huge success, marketing strategies havextended to include younger men; therefore phosphodiester-se (PDE) inhibitors, like sildenafil, are used increasingly byen of reproductive age (2, 3). These drugs are widely
vailable on the internet, which facilitates their use as rec-eational drugs (2, 3) and there is now robust evidence (3)hat their use in recreation has gained credence in young,ealthy men as sexual enhancers as well for older men,equiring them for erectile dysfunction problems. Further-ore, the reproductive age range for men has extended
ramatically during the past decades with older parentingecoming more popular and second families with older fa-hers constituting an increasing proportion of Western soci-ty. Moreover, PDE inhibitors are reportedly sold illegally inightclubs to use along with illicit “club drugs” such asetamine and amyl nitrite. They are offered inappropriately
eceived November 1, 2005; revised and accepted November 3, 2006.resented at Spring meeting, British Fertility Society, Cheltenham,England, April 2004.
eprint requests: Sheena E. M. Lewis, Ph.D., Obstetrics & Gynaecology,Institute of Clinical Science, Grosvenor Road, Belfast BT12 6BJ, United
gKingdom (FAX: 44-2890328247; E-mail: [email protected]).
1064 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
hrough e-mail attachments, offering prospective purchasershe opportunity to obtain them without visiting their doctors.
A further niche market for PDE inhibitors is to target theapidly increasing population of young men who suffer fromrectile dysfunction related to medical conditions such asiabetes and spinal cord injuries to use them in the treatmentf their erectile dysfunction (4). Because the partners ofany of these men are hoping to conceive, it is vital to
etermine the effects of sildenafil on sperm function.
Probably of more concern, however, is the extensive ac-eptance of this drug by assisted conception units in the U.K.n a questionnaire audit of all the Human Fertilization andmbryology Authority’s licensed assisted conception units
n the U.K., we demonstrated that 42% would prescribeildenafil to patients finding it difficult to produce semenamples on demand and particularly in timed cycles ofreatment.
This widespread use of sildenafil is of concern as it is aelective type 5 PDE inhibitor (PDE5), one of a large familyf different types of PDE inhibitors. There are 11 PDEnhibitors and 21 subfamilies, most with high levels ofpecificity. They act by modulating the activity of cyclicucleotides, the second messengers and controllers of nu-erous cell functions, thus regulating their degradation. Sil-
enafil acts by increasing intracellular levels of cyclic
uanosine monophosphate (cGMP) and cyclic adenosine0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.11.017

mtieerwdwlrrgetmee
sal
MSSmrihcnpNwtms
cau
PPanp(Egr2a
TvdTlpfs
m�wntongpo
its
SrysBtl0Tsml(1V
PDTivooawiAh(
F
onophosphate (cAMP) (5). Previously, other phosphodies-erase inhibitors, such as pentoxifylline, a type 4 PDE inhib-tor, have been shown to affect sperm function (6). Spermxposed to pentoxifylline underwent motility alterations andarly acrosome reactions. If sperm are prematurely acrosomeeacted, they are rendered incapable of fertilization. Theseere in vitro experiments and the effects persisted after therug was washed from the semen, suggesting that the effectsere irreversible. Another common property of pentoxifyl-
ine and sildenafil is their ability to inhibit formation ofeactive oxygen species (ROS). Koupparis et al. (7) haveeported the inhibition of superoxide and expression ofp47(phox) NAD [P]H oxidase by sildenafil in corpus cav-rnosal smooth muscle cells. Similarly, our group has shownhe protective effects of pentoxifylline against ROS in hu-an sperm (8). Since ROS (at low concentrations) are nec-
ssary for normal sperm function, it is important that theffects of sildenafil on human sperm are fully elucidated.
The aim of this study was to investigate the effects ofildenafil on sperm motility using computer-assisted semennalysis and acrosome reaction by fluorescein isothiocyanate-abeled peanut agglutinin (FITC-PNA) staining with time.
ATERIALS AND METHODSubjectsemen samples (n � 57) were obtained from unselecteden, aged 26 – 42 years, attending the Andrology Labo-
atory, Royal Maternity Hospital, Belfast, for infertilitynvestigations. Their semen analyses indicated that theyad asthenozoospermic profiles (volume, 3.5 � 0.47 mL;oncentration, 82 � 11.3 � 106/mL; motility, 40.0% � 2.3%;ormal morphology 12.0% � 0.7%) as is the most commonrofile of patients attending for infertility investigations inorthern Ireland. Informed written consent for participationas obtained from each recruit. The project was approved by
he Queen’s University Belfast Research and Ethics Com-ittee and was in accordance with the Declaration of Hel-
inki, as revised in 1983.
Samples were obtained by masturbation, into a sterileontainer, after a minimum of 2 and a maximum of 5 daysbstinence. Subjects were only excluded if they were alreadysing sildenafil or other recreational drugs.
reparation of Semen Using Density Centrifugationreparation of samples After liquefaction, routine semennalyses were performed according to World Health Orga-ization (WHO) recommendations (9) and then samples wererepared using a two-step discontinuous Percoll gradient90%–45%; Pharmacia Biotech AB, Uppsala, Sweden).ach aliquot of liquefied semen was layered on top of theradient and centrifuged at 450 � g for 12 minutes. Theesulting sperm pellet was concentrated by centrifugation at00 � g for 6 minutes and the low-density sperm removed
nd concentrated by centrifugation at 200 � g for 6 minutes. certility and Sterility�
he final sperm preparations were suspended in a suitableolume of Biggers, Whitten, and Whittingham (BWW) me-ium (10) supplemented with 600 mg of albutein (Alphaherapeutic UK Ltd., Norfolk, England). Hence, two popu-
ations of sperm were prepared: that with the best fertilizingotential as used in assisted conception treatments (90%raction), and that with the poorer population (45% fraction)imilar to the sperm profile of men with male infertility (11).
Soluble sildenafil citrate was prepared by dissolving 10g of pure sildenafil citrate (Pfizer, Sandwich, U.K.) in 100L of 99% ethanol. The final concentration of ethanol tohich sperm were exposed was 0.0095%, which was shownot to have any toxic effects on sperm function. This washen diluted in BWW medium to give a final concentrationf 900 ng/mL Viagra. When mixed with an equal volume ofeat semen, the concentration was reduced to 450 ng/mL toive a final concentration of 0.67 �M, equivalent to thelasma concentration, 1 hour after oral ingestion, of 100 mgf sildenafil—the maximum recommended dose.
Semen and prepared sperm (90% and 45%) were dividednto aliquots and incubated in the presence or absence (con-rol; by adding the same volume of BWW medium) ofildenafil.
perm motility assessment Quantitative sperm motility pa-ameters were assessed using computer-assisted semen anal-sis (Hamilton Thorne Integrated Visual Optical Systemperm analyzer; version 10.7; Hamilton-Thorne Research,everly, CA). The settings used for analysis were acquisi-
ion rate, 30 Hz; minimum contrast, 7; minimum size, 6;ow-size gate, 0.4; high-size gate, 1.6; low-intensity gate,.4; high intensity gate, 1.6; HTM magnification factor, 2.04.en microliters from each sample were placed on preheatedlides (37°C) and inserted into the machine. Percentageotility, percentage progressive motility, average path ve-
ocity (VAP), progressive velocity, and curvilinear velocityVCL) were determined at intervals of 0, 15, 30, 45, 75, and35 minutes. Cells were counted as progressively motile ifAP was �25 �msec�1.
reparation of Sperm for Acrosome Reactionetermination by FITC-PNA Stainingwo hours after ejaculation, prepared sperm was divided
nto aliquots and incubated in the presence of an equalolume of sildenafil in solution (to give a final concentrationf 0.67 �M) or absence (control) by adding the same volumef BWW medium) of sildenafil. After incubation of the testnd control samples for 1 h at 37°C, sperm acrosome statusas assessed by FITC-PNA (Sigma, Dorset, UK) (12) stain-
ng and epifluorescence microscopy. Peanut agglutinin, fromrachis hypogea, is specific for �-D-galactose residues and,ence, binds to, and labels, the outer acrosomal membrane13).
Briefly, 20 �L of sperm suspension were spread over a
lean microscope slide and allowed to air-dry. The smear1065

wa(itbpd1t
I
STtwsttprdb
woa
REApa(sT(mileaWncs
E4SelmiDg
as then fixed in 95% ethanol for 5 minutes and againllowed to air-dry. Fixed slides were stained in FITC-PNA600-�L aliquot of FITC-PNA in 15.4 mL of reagent watern a foil-covered Coplin jar) for 15 minutes, at ambientemperature. Slides were rinsed by dipping in phosphate-uffered saline (PBS) twice before fixing for 15 minutes inaraformaldehyde at ambient temperature. Slides were air-ried, mounted, and stored in the dark until scoring. Between00 and 250 sperm were counted per slide and scored intohree classes for PNA labeling (12).
I: acrosome intact—whole acrosome labeling, denotes anintact outer acrosomal membrane;
II: partially acrosome reacted—patchy acrosome labeling,suggestive of a transition stage where the outer acroso-mal membrane is fenestrating;
II: acrosome reacted—equatorial segment only labeling,denoting a normally acrosome-reacted spermatozoa thathas lost the outer acrosomal membrane over the anteriorcap of the acrosome but has retained the equatorialsegment of the acrosome intact.
tatistical Analysiso determine changes in sperm motility parameters with
ime after exposure to sildenafil, we calculated the time-eighted values of percentage progressive motility and
traight-line velocity (VSL). This is equivalent to calculatinghe area under the curve using the trapezium rule. Theseime-weighted values were then compared using Student’saired t-test to avoid multiple comparisons and give a moreobust single statistic on which to determine the effects of therug. Student’s t-tests were also used to measure differences
FIGURE 1
The effects of sildenafil on progressive motility ofhuman sperm‘control sperm ° sperm incubatedin the presence of 0.67 �M sildenafil citrate Valuesare means for 22 samples; P�.001.
Glenn. Sildenafil citrate accelerates sperm function. Fertil Steril 2007.
etween prepared populations of sperm. A value of P�.05
1066 Glenn et al. Sildenafil citrate accelerates sperm functio
as considered significant. Comparisons of the proportionsf sperm with intact, partially reacted, and fully reactedcrosomes were made using �2 analysis.
ESULTSffects of Sildenafil Citrate on Total Sperm Motilityfter incubation with the test substance for 15 minutes, theercentage of progressively motile sperm in the sildenafilliquots had increased markedly compared with controlsFig. 1). This effect was observed at each time point mea-ured. By 120 minutes there was a 52% increase (P�.001).he drug also enhanced VSL of the sperm after 15 minutes�11%). Again, this effect was sustained through to 120inutes (�14%; Fig. 2). Curvilinear velocity showed similar
ncreases at each time point (data not shown), therefore theinearity of movement was unchanged. No significant differ-nces were noted in amplitude of lateral head movementsnd beat frequency between the groups (data not shown).ithin this patient group, 50% of the semen samples were
ormozoospermic and the rest, asthenozoospermic. The per-entage increase in progressive motility was similar in eachample whether it was normal or asthenozoospermia.
ffects of Sildenafil Citrate on Motility in 90% and5% Percoll Fractionsildenafil citrate had similar effects on the motility param-ters of good (90% Percoll layer) and poor (45% Percollayer) quality populations of sperm. In the 90% layer, by 120inutes, the percentage of highly progressive motile sperm
n the sildenafil group was substantially (�28%) increased.espite a very small proportion of sperm in the controlroup of the poor quality (45%) fraction exhibiting progres-
FIGURE 2
The effect of sildenafil citrate on the velocity ofhuman sperm‘control sperm ° sperm incubatedin the presence of 0.67 �M sildenafil citrate Valuesare means for 22 samples; P�.001.
Glenn. Sildenafil citrate accelerates sperm function. Fertil Steril 2007.
n Vol. 87, No. 5, May 2007
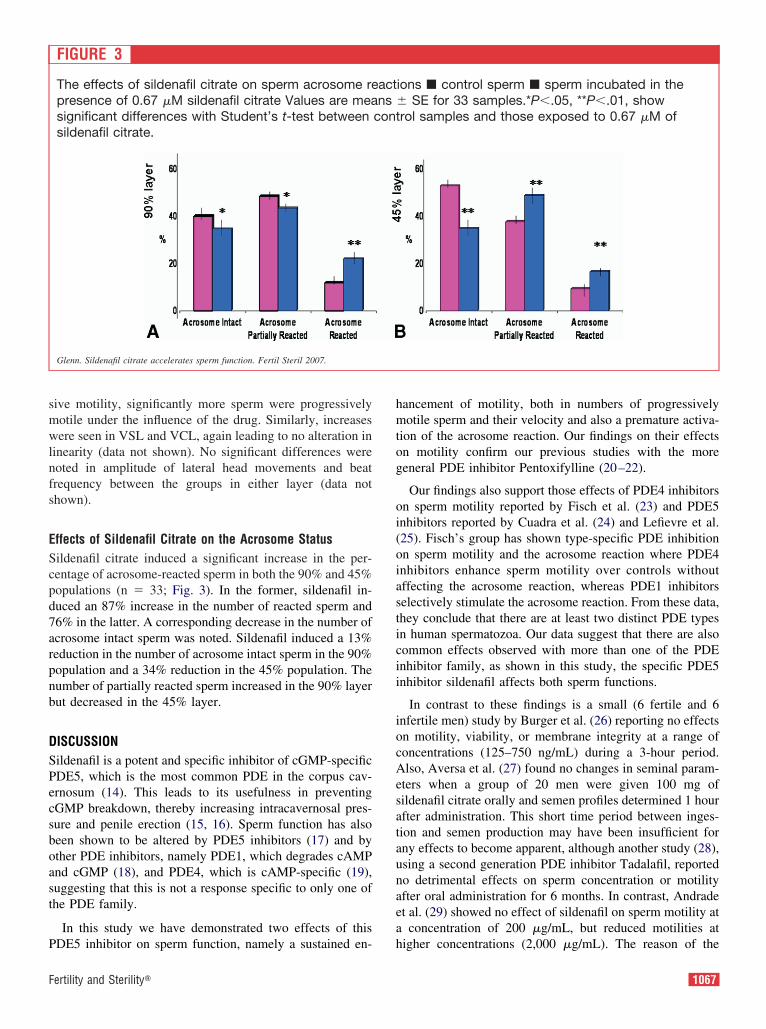
smwlnfs
EScpd7arpnb
DSPecsboast
P
hmtog
oi(oiasticii
iocAesataunaea
F
ive motility, significantly more sperm were progressivelyotile under the influence of the drug. Similarly, increasesere seen in VSL and VCL, again leading to no alteration in
inearity (data not shown). No significant differences wereoted in amplitude of lateral head movements and beatrequency between the groups in either layer (data nothown).
ffects of Sildenafil Citrate on the Acrosome Statusildenafil citrate induced a significant increase in the per-entage of acrosome-reacted sperm in both the 90% and 45%opulations (n � 33; Fig. 3). In the former, sildenafil in-uced an 87% increase in the number of reacted sperm and6% in the latter. A corresponding decrease in the number ofcrosome intact sperm was noted. Sildenafil induced a 13%eduction in the number of acrosome intact sperm in the 90%opulation and a 34% reduction in the 45% population. Theumber of partially reacted sperm increased in the 90% layerut decreased in the 45% layer.
ISCUSSIONildenafil is a potent and specific inhibitor of cGMP-specificDE5, which is the most common PDE in the corpus cav-rnosum (14). This leads to its usefulness in preventingGMP breakdown, thereby increasing intracavernosal pres-ure and penile erection (15, 16). Sperm function has alsoeen shown to be altered by PDE5 inhibitors (17) and byther PDE inhibitors, namely PDE1, which degrades cAMPnd cGMP (18), and PDE4, which is cAMP-specific (19),uggesting that this is not a response specific to only one ofhe PDE family.
In this study we have demonstrated two effects of this
FIGURE 3
The effects of sildenafil citrate on sperm acrosome represence of 0.67 �M sildenafil citrate Values are measignificant differences with Student’s t-test betweensildenafil citrate.
Glenn. Sildenafil citrate accelerates sperm function. Fertil Steril 2007.
DE5 inhibitor on sperm function, namely a sustained en- h
ertility and Sterility�
ancement of motility, both in numbers of progressivelyotile sperm and their velocity and also a premature activa-
ion of the acrosome reaction. Our findings on their effectsn motility confirm our previous studies with the moreeneral PDE inhibitor Pentoxifylline (20–22).
Our findings also support those effects of PDE4 inhibitorsn sperm motility reported by Fisch et al. (23) and PDE5nhibitors reported by Cuadra et al. (24) and Lefievre et al.25). Fisch’s group has shown type-specific PDE inhibitionn sperm motility and the acrosome reaction where PDE4nhibitors enhance sperm motility over controls withoutffecting the acrosome reaction, whereas PDE1 inhibitorselectively stimulate the acrosome reaction. From these data,hey conclude that there are at least two distinct PDE typesn human spermatozoa. Our data suggest that there are alsoommon effects observed with more than one of the PDEnhibitor family, as shown in this study, the specific PDE5nhibitor sildenafil affects both sperm functions.
In contrast to these findings is a small (6 fertile and 6nfertile men) study by Burger et al. (26) reporting no effectsn motility, viability, or membrane integrity at a range ofoncentrations (125–750 ng/mL) during a 3-hour period.lso, Aversa et al. (27) found no changes in seminal param-
ters when a group of 20 men were given 100 mg ofildenafil citrate orally and semen profiles determined 1 hourfter administration. This short time period between inges-ion and semen production may have been insufficient forny effects to become apparent, although another study (28),sing a second generation PDE inhibitor Tadalafil, reportedo detrimental effects on sperm concentration or motilityfter oral administration for 6 months. In contrast, Andradet al. (29) showed no effect of sildenafil on sperm motility at
concentration of 200 �g/mL, but reduced motilities at
ions � control sperm � sperm incubated in the� SE for 33 samples.*P�.05, **P�.01, showrol samples and those exposed to 0.67 �M of
actns
cont
igher concentrations (2,000 �g/mL). The reason of the
1067

r2rcm3mase
cpapcppfip(isbsaseofl
sitttNtetogdTioefasd
atb
(ep
t(tiPCTspeplYcw
ahapifpgostiTsPP
me(sclebr
fk(srtt
eduction may be due to toxic effects at higher dosage, as,000 �g/mL is considerably higher than physiological se-um concentration. In contrast with this study, we chose aoncentration of sildenafil that is equivalent to the meanaximum total plasma concentration (440 ng/mL) present
0 minutes after a single oral dose of 100 mg. Although theanufacturers’ information sheet (30) shows negligible
mounts (0.0002% of 100-mg oral dose) of sildenafil inemen, the concentration of sildenafil to which sperm arexposed in the epididymis is unknown.
The rates at which drugs pass from blood (or plasma) andoncentrate in the biological fluids are regulated by theirhysicochemical characteristics (31), with the concentrationnd lipid solubility of the undissociated drug being thehysical properties most important in determining the disso-iation constant (32). These specific characteristics are notublished for sildenafil but given its hydrophobic nature, it isrobable that it crosses the blood–testis barrier without dif-culty. We know that sperm are very vulnerable during therolonged period when they pass through the epididymis33). The manufacturer states that the final quantity of drugn semen averages only 188 ng (30). This concentration isubstantially less than that to which sperm are exposedefore ejaculation. At that point semen is 5% sperm and 95%eminal plasma, composed of contributions from the prostatend seminal vesicles. Thus, it is difficult to determine theildenafil concentrations to which immature testicular andpididymal sperm are exposed in the interval from ingestionf the drug until the sperm are mixed with the ejaculatoryuids as part of the ejaculatory process.
The effects of sildenafil on sperm function reported in thistudy were all performed in vitro. Thus extrapolations to then vivo situation must be considered with care. Althoughhese concentrations are similar to physiological concentra-ions in the male reproductive tract, the presence of poten-ially modulating factors in the body may alter its effects.onetheless, an additional characteristic of PDE inhibitors
hat causes concern is the persistence of their effects. Theseffects have been observed for at least 3 hours after at-empted removal by repeated washings (6). In a case reportf Viagra use for human-assisted reproduction the investi-ators noted that there was no fertilization of the oocytesespite the intracytoplasmic injection of the sperm (34).hey attributed the failed fertilization to the delay in obtain-
ng the semen sample and the resultant advanced age of theocytes. However, it is possible that Viagra had a deleteriousffect on sperm function and it was the reason for theertilization failure. When Viagra is given to patients by oraldministration there is no opportunity to remove either theperm or the embryos from its potentially persistent andamaging effects.
In this study we have also shown an early activation of thecrosome reaction with this PDE5 inhibitor. This has impor-ant clinical implications because sperm that acrosome- react
efore contact with the oocyte are incapable of fertilization f1068 Glenn et al. Sildenafil citrate accelerates sperm functio
35, 36). Given that the majority of sperm acrosome react onxposure to sildenafil, the drug may cause significant im-airment to their fertilizing potential.
Again the literature regarding the effects of PDE inhibi-ors on sperm acrosome reactions is conflicting. Fisch et al.23) have shown that PDE1 inhibitors selectively stimulatehe acrosome reaction, whereas, in their hands, PDE4 inhib-tors have no effect. Furthermore, Lefievre et al. (37) and dulessis et al. (38) found no effect with PDE5, whereasuadra et al. (24) found a marked early acrosome reaction.he latter are in agreement with the well-documented acro-ome activation effects of general PDE inhibitors such asentoxifylline (39, 40) and caffeine (41). Indeed, Tasdemirt al. (42) showed the direct benefits of PDE in an IVFrogram where Pentoxifylline-enhanced acrosome reactioned to an improved fertilization rate and because of that factovich (43) recommended the addition of pentoxifylline in
ases of assisted reproduction where the acrosome reactionas suboptimal.
Most recently, an in vivo study (44) has reported thatnother PDE, PDE11, the most recently discovered family ofuman PDEs, is highly expressed in testis, prostate gland,nd developing sperm. This suggests that PDEs have ahysiological role in the male reproductive tract, although its as yet unproven. In support of this, Wayman et al. (45)ound that ejaculated sperm from PDE11 (�/�) mice dis-layed reduced sperm concentration, rate of forward pro-ression, and percentage sperm viability. This group alsobserved a marked premature spontaneous capacitance ofperm from PDE11 knockout mice. This adds to concernshat drugs that inhibit PDEs may disrupt the delicate phys-ological balance and “lead to reduced fertilizing ability.”hese researchers suggest that the role of PDE inhibitors onperm fertilizing capacity requires clarification. The role ofDE11 in human testicular function and its interaction withDE inhibitors remains controversial (44).
The mechanism by which PDE inhibitors exert their phar-acological effects is by inhibiting phosphodiesterase, an
nzyme responsible for the degradation of cGMP to GMP46). This creates an environment with increased energyubstrates. These raised levels of cGMP affect many intra-ellular functions including calcium transport (47). Alteredevels of calcium are known to affect sperm motion and annergy-dependent influx of calcium into the sperm cell iselieved to be responsible for initiation of the acrosomeeaction (48).
An additional function of cGMP is as a second messengeror nitric oxide (NO) and PDE inhibitors, which are alsonown to augment NO production (49). We have shown50, 51) that NO assumes a key role in the maintenance ofperm motility, but is only beneficial within a very carefullyegulated concentration range. Nitric oxide is a potent reac-ive oxygen species that will interact with superoxide anionso form hydroxyperoxyl radicals or peroxynitrite, which will
orm the hydroxyl radical; all of which are detrimental ton Vol. 87, No. 5, May 2007

sftb
tmepoeaoaimascu
homh
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
33
3
3
3
3
3
3
F
perm (51). Thus, sildenafil has the potential to alter spermunction by in vivo effects on the NO concentration range, ashe beneficial effects of NO at nanomolar concentrationsecome highly detrimental at millimolar concentrations.
The PDE inhibitors are known to impair both preimplan-ation (52, 53) and postimplantation (44) embryo develop-ent. Cell numbers of blastocysts and development of the
arly embryo are both significantly reduced after exposure toentoxifylline (54). Lacham-Kaplan and Trounson (52) alsobserved embryonic arrest and retarded development afterxposure to pentoxifylline. Elevated levels of cAMP havelso been shown to inhibit germinal vesicle breakdown andocyte maturation (55). Morales et al. (56) have reported thatlthough sildenafil is a selective inhibitor of type 5, it hasnhibitory effects similar to types 1 and 6 PDE. In agree-ent, we have shown no differences between general PDE
nd specific PDE5 inhibitors in sperm function. If they actimilarly in embryo development, we have further cause foroncern. Studies on their effects on embryo development arergently needed before their use in the clinic is advocated.
There are also considerable implications in terms of publicealth education and the need to inform recreational usersf its potential side effects. These concerns make it all theore crucial to elucidate fully any effects sildenafil has on
uman reproduction.
EFERENCES1. Pfizer Ltd. www.viagra.com/whyViagra/provenSafety.asp, 2005.2. Aldridge J, Measham F. Sildenafil (Viagra) is used as a recreational
drug in England. BMJ 1999;318:669.3. Smith KM, Romanelli F. Recreational use and misuse of phosphodiet-
erase 5 inhibitors. J Am Pharm Assoc (Was DC) 2005;45:63–5.4. Monga M, Bernie J, Rajasekaran M. Male infertility and erectile dys-
function in spinal cord injury: a review. Arch Phys Med Rehabil1999;80:1331–9.
5. Glossmann H, Petrischor G, Bartsch G. Molecular mechanisms of theeffects of SC (VIAGRA). Exp Gerontol 1999;34:305–18.
6. McKinney KA, Lewis SE, Thompson W. Persistent effects of pentoxi-fylline on human sperm motility, after drug removal, in normozoosper-mic and asthenozoospermic individuals. Andrologia 1994;26:235–40.
7. Koupparis AJ, Jeremy JY, Mazaffar S, Persad R, Shukla N. Sildenafilinhibits the formation of superoxide and the expression of gp47(phox)NAD[P]H oxidase induced by the thromboxane A2 mimetic,U46619, in corpus cavernosal smooth muscle cells. B J Urol 2005;96:423–7.
8. McKinney KA, Lewis SEM, Thompson W. The effects of pentoxifyl-line on the generation of reactive oxygen species and lipid peroxidationin human spermatozoa. Andrologia 1996;28:15–20.
9. World Health Organization. WHO laboratory manual for the examina-tion of human semen and sperm–cervical mucus interaction. Cam-bridge: Cambridge University Press, 1999.
0. Biggers JD, Whitten WK, Whittingham DG. The culture of mouseembryos in vitro. In: Daniel JC, ed. Methods in mammalian embryol-ogy. San Francisco: Freeman, 1971:86–116.
1. O’Connell M, McClure N, Powell LA, Steele EK, Lewis SE. Differ-ences in mitochondrial and nuclear DNA status of high-density andlow-density sperm fractions after density centrifugation preparation.Fertil Steril 2003;79(Suppl 1):754–62.
2. Mortimer D. Sperm fertilizing ability testing. In: Mortimer D, ed.Practical laboratory andrology. Oxford: Oxford University Press, 1994:
199–240.ertility and Sterility�
3. Mortimer D, Curtis EF, Miller RG. Specific labelling by peanut agglu-tinin of the outer acrosomal membrane of the human spermatozoon.J Reprod Fertil 1987;81:127–35.
4. Morales A, Gingell C, Collins M, Wicker PA, Osterloh IH. Clinicalsafety of oral sildenafil citrate (VIAGRA [TM]) in the treatment oferectile dysfunction. Int J Impotence Res 1998;2:69–73.
5. Fabbri A, Aversa A, Isidori A. Sildenafil and erectile dysfunction.J Endo Inv 1999;6:486–91.
6. Goldstein I, Rosen RC, Steers ED. Sildenafil in the treatment of erectiledysfunction (Reply). N Engl J Med 1999;339:701–2.
7. Fisch JD, Behr B, Conti M. Enhancement of motility and acrosomereaction in human spermatozoa: differential activation by type-specificphosphodiesterase inhibitors. Hum Reprod 1998;13:1248–54.
8. Beavo JA. Cyclic-nucleotide phosphodiesterases—functional implica-tions of multiple isoforms. Phys Rev 1995;75:725–48.
9. Conti M, Nemoz G, Sette C, Vicini E. Recent progress in under-standing the hormonal-regulation of phosphodiesterases. Endo Rev1995;16:370 – 89.
0. Lewis SE, Moohan JM, Thompson WI. Effects of pentoxifylline onhuman sperm motility in normospermic individuals using computerassisted analysis. Fertil Steril 1993;59:418–23.
1. McKinney KA, Lewis SEM, Thompson W. The effect of pentoxifyllineon human sperm motility and its persistence after drug removal innormozoospermic and asthenozoospermic individuals. Andrologia 1994;26:235–40.
2. Lewis SEM, McKinney K, Thompson. The influence of pentoxifyllineon human sperm motility in asthenozoospermic individuals using com-puter assisted analysis. Arch Androl 1994;32:175–83.
3. Fisch JD, Behr B, Conti M. Enhancement of motility and acrosomereaction in human spermatozoa: differential activation by type-specificphosphodiesterase inhibitors. Hum Reprod 1998;13:1248–54.
4. Cuadra DL, Chan PJ, Patton WC, Stewart SC, King A. Type 5 phos-phodiesterase regulation of human sperm motility. Am J Obstet Gy-necol 2000;182:1013–5.
5. Lefievre L, De Lamirande E, Gagnon C. The cyclic GMP-specificphosphodiesterase inhibitor, SC, stimulates human sperm motility andcapacitation but not acrosome reaction. J Androl 2000;21:929–37.
6. Burger M, Sikka SC, Bivalacqua TJ, Lamb DJ, Hellstrom WJ. Theeffect of SC on human sperm motion and function from normal andinfertile men. Int J Impot Res 2000;12:229–34.
7. Aversa A, Mazzilli F, Rossi T, Delfino M, Isidori AM, Fabbri A.Effects of SC (Viagra) administration on seminal parameters and post-ejaculatory refractory time in normal males. Hum Reprod 2000;15:131–4.
8. Hellstrom WJG, Overstreet JW, Yu A, Saikal K, Shen W, Beasley CM,et al. Tadalafil has no detrimental effect on human spermatogenesis orreproductive hormones. J Urol 2003;170:887–91.
9. Andrade JR, Traboulsi A, Hussain A, Dubin NH. In vitro effects of SCand phentolamine, drugs used for erectile dysfunction, on human spermmotility. Am J Obstet Gynecol 2000;182:1093–5.
0. Pfizer Ltd. www.emc.medicines.org.uk, 2002.1. Winningham DG, Nemoy NJ, Stamey TA. Diffusion of antibiotics from
plasma into prostatic fluid. Nature 1968;219:139–43.2. Pichini S, Zuccaro P, Pacifici R. Drugs in semen. Clin Pharmacokinet
1994;26:356–73.3. Jones R. Sperm survival versus degradation in the mammalian epidid-
ymis: a hypothesis. Biol Reprod 2004;72:1405–11.4. Tur-Kaspa I, Segal S, Moffa F, Massobrio M, Meltzer S. Viagra for
temporary erectile dysfunction during treatments with assisted repro-ductive technologies. Hum Reprod 1999;14:1783–4.
5. Tesarik J, Mendoza C, Carreras A. Effects of phosphodiesterase inhib-itors caffeine and pentoxifylline on spontaneous and stimulus-inducedacrosome reactions in human sperm. Fertil Steril 1992;58:1185–90.
6. Lanzafame F, Chapman MG, Guglielmino A, Gearon CM, Forman RG.Pharmacological stimulation of sperm motility. Hum Reprod 1994;9:192–9.
7. Lefievre L, De Lamirande E, Gagnon C. The cyclic GMP-specific
phosphodiesterase inhibitor, sildenafil, stimulates human sperm mo-1069

3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
tility and capacitation but not acrosome reaction. J Androl2000;21:929 –37.
8. du Plessis SS, de Jongh PS, Franken DR. Effect of acute in vivosildenafil citrate and in vitro 8-bromo-cGMP treatments on semenparameters and sperm function. Fertil Steril 2004;81:1026–33.
9. Esteves SC, Spaine DM, Cedenho AP, Srougi M. Cryopreservation ofsperm from oligo-asthenozoospermic men with pentoxifylline improvesthe post-thaw agonist-induced acrosome reaction rate. J Urology 2002;167(Suppl S):318.
0. Ain R, Uma Devi KU, Shivaji S, Seshagiri PB. Pentoxifylline-stimulated capacitation and acrosome reaction in hamster spermatozoa:involvement of intracellular signalling molecules. Mol Hum Reprod1999;5:618–26.
1. Tesarik J, Mendoza C, Carreras A. Effects of phosphodiesterase inhib-itors caffeine and pentoxifylline on spontaneous and stimulus-inducedacrosome reactions in human sperm. Fertil Steril 1992;58:1185–90.
2. Tasdemir M, Tasdemir I, Kodama H, Tanaka T. Pentoxifylline-enhanced acrosome reaction correlates with fertilization in vitro. HumReprod 1993;8:2102–7.
3. Yovich JL. Pentosifylline: actions and applications in assisted repro-duction. Hum Reprod 1993;8:1986–91.
4. Francis SH. Phosphodiesterase 11 (PDE11): is it a player in humantesticular function? Int J of Imp Res 2005;17:467–8.
5. Wayman C, Phillips S, Lunny C, Webb T, Fawcett L, Baxendale R,Burges G. Phosphodiesterase 11 (PDE11) regulation of spermatozoaphysiology. Int J Impot Res 2005;17:216–23.
6. Omote M. Pharmacological profiles of SC (VIAGRA) in the treatmentof erectile dysfunction: efficacy and drug interaction with nitrate. Nip-pon Yakurigaku Zasshi 1999;114:213–8.
7. Middendorff R, Davidoff MS, Behrends S, Mewe M, Miethens A,Muller D. Multiple roles of the messenger molecule cGMP in testicular
function. Andrologia 2000;32:55–9.1070 Glenn et al. Sildenafil citrate accelerates sperm functio
8. Rossato M, Di Virgilio F, Rizzuto R, Galeazzi C, Foresta C. Intracel-lular calcium store depletion and acrosome reaction in human sperma-tozoa: role of calcium and plasma membrance potential. Mol HumReprod 2001;7:119–28.
9. Kim NY, Pae HO, Kim YC, Choi CK, Rim JS, Lee HS, et al. Pentoxi-fylline potentiates nitric oxide production in interleukin-1beta-stimulated vascular smooth muscle cells through cyclic AMP-dependentprotein kinase A pathway. Gen Pharmacol 2000;35:205–11.
0. Lewis SE, Donnelly ET, Sterling ES, Kennedy MS, Thomson W,Chakravarthy U. Nitric oxide synthase and nitrite production in humanspermatozoa: evidence that endogenous nitric oxide is beneficial tosperm motility. Mol Hum Reprod 1996;2:873–8.
1. Donnelly ET, Lewis SE, Thompson W, Chakravarthy U. Sperm nitricoxide and motility: the effects of nitric oxide synthase stimulation andinhibition. Mol Hum Reprod 1997;3:755–62.
2. Lacham-Kaplan O, Trounson AO. Embryo development capacity ofoocytes fertilized by immature sperm and sperm treated with motilitystimulants. Reprod Fertil Dev 1994;6:113–6.
3. Scott L, Smith S. Human sperm motility-enhancing agents have detri-mental effects on mouse oocytes and embryos. Fertil Steril 1995;63:166–75.
4. Tournaye H, Van der Linden M, Van den Abbeel E, Devroey P, VanSteirteghem A. Effect of pentoxifylline on implantation and post-implantation development of mouse embryos in vitro. Hum Reprod1993;8:1948–54.
5. Siracusa G, De Felici M, Salustri A. Meiotic maturation of the mam-malian oocyte. In: Asch RH, Balmaceda JP, Johnston I, eds. Gametephysiology. Norwell, MA: Serono Symposia USA, 1990:129–44.
6. Morales A, Gingell C, Collins M, Wicker PA, Osterloh IH. Clinicalsafety of oral sildenafil citrate (VIAGRA (TM)) in the treatment of
erectile dysfunction. Int J Impo Res 1998;10:69–73.n Vol. 87, No. 5, May 2007

Ubmstcsiwt
R
T
P
R
0d
Tissue perfusion-controlled guided biopsiesare essential for the outcome of testicularsperm extractionRalf Herwig, M.D.,a Kadir Tosun, M.D.,b Antonius Schuster, M.D.,c Peter Rehder, M.D.,b
Bernhard Glodny, M.D.,d Ludwig Wildt, M.D.,e Karl Illmensee, Ph.D.,e
and Germar-Michael Pinggera, M.D.b
a Department of Urology, Medical University of Vienna, Vienna; b Department of Urology, Medical University of Innsbruck,Innsbruck; c Department of Radiology, LKH General Hospital Feldkirch, Feldkirch; and d Department of Radiology I, ande Department of Gynecological Endocrinology and Reproductive Medicine, Medical University of Innsbruck, Innsbruck,Austria
Objective: To determine if there are areas of major and minor perfusion in a single testicle, and if the quality andquantity of sperm are correlated with the level of perfusion, we collected testicular tissue from areas with differentlevels of perfusion.Design: Controlled clinical study.Setting: Consecutive patients with azoospermia.Patient(s): Patients with azoospermia undergoing testicular sperm extraction (TESE) biopsy for the retrieval ofsperm to be used in an assisted reproduction program.Intervention(s): Perfusion mapping was performed with the use of color Doppler ultrasound. Areas with differentlevels of perfusion were marked with needles. After incision with radiofrequency cutting, the exposed tissue wasexamined with a laser Doppler flowmeter, and biopsies were taken for TESE and histology. Sperm were analyzedusing World Health Organization criteria, and prepared for intracytoplasmic sperm injection (ICSI).Main Outcome Measure(s): Correlation of sperm quality and quantity in testicular-tissue biopsies, with tissue-perfusion units (TPU) measured by laser Doppler flowmeter.Result(s): From 40 biopsies taken from 20 testicles of 12 patients, tissue was analyzed for sperm quality andquantity. Sperm quality was highest in areas of high tissue perfusion. In areas of 70 TPU, 72.3% progressivesperm were detected, whereas in areas of 10 TPU, only 13.3% progressive sperm and elevated numbers ofprecursor cells could be observed. The number of motile sperm isolated from tissue samples correlated well withthe intensity of tissue perfusion.Conclusion(s): We have shown for the first time that in patients suffering from azoospermia, sperm quality andquantity depend on tissue perfusion within the testicle. (Fertil Steril� 2007;87:1071–6. ©2007 by AmericanSociety for Reproductive Medicine.)
Key Words: Laser Doppler flowmetry, perfusion-controlled testicular biopsy testicular sperm extraction (TESE),color Doppler ultrasound, intracytoplasmic sperm injection (ICSI), assisted reproductive technology (ART)
atphrsoc
cttmlow
ntil recently, various surgical interventions on testiculariopsies were carried out randomly, and focal areas of sper-atogenesis were determined (1). Although the outcome of
urgical intervention is unpredictable, testicular sperm ex-raction (TESE) has proved to be a quite reliable and suc-essful sperm-recovery technique for use in intracytoplasmicperm injection (ICSI) when helping male factor-dependentnfertile couples (2–4). However, the difficulty of predictinghich patient with azoospermia may have sperm involves
he evaluation of hormonal levels and/or testicular histology
eceived March 6, 2005; revised October 2, 2006; accepted October 11,2006.
his work was done at the Department of Urology, Medical University ofInnsbruck, Innsbruck, Austria.
resented at the 100th Annual Meeting of the American Urologic Asso-ciation, San Antonio, Texas, May 21–26, 2005.
eprint requests: Ralf Herwig, M.D., Department of Urology, MedicalUniversity of Vienna, Waehringer Guertel 18–20, A-1190 Vienna, Aus-
itria (FAX: �43 1 40400 2601; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.10.010 Copyright ©2007 American Soc
s variable parameters for surgical sperm retrieval (5). Fur-hermore, biopsies with focal spermatogenesis may require arolonged search for viable sperm, sometimes lasting severalours. In some cases, bilateral or multiple biopsies takenandomly are required for sperm retrieval. To improve theuccess rates of TESE, it would be useful to have a methodf determining testicular areas with a high probability ofontaining normal sperm.
Recently we described a novel approach to improving thehances of sperm retrieval from testicular biopsies, based onesticular tissue perfusion (6,7). Areas of good perfusion in aesticle are identified by external color Doppler ultrasound,arked by precisely placed needles and verified by local
aser Doppler flowmetry for measuring perfusion within thepened testicle. The aim of this study was to examinehether there is a correlation between the level of perfusion
n testicular areas and the quantity and quality of sperm
1071Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

ra
MPIpoap(attt
efsratbb
PPasDi
5q
tbmfycs
sqsrmDlmda
arw(sf
bmr
ecovered from these areas, after TESE in patients withzoospermia.
ATERIALS AND METHODSatientsn a total of 12 patients, perfusion-guided TESE surgery waserformed (20 testicles: 10 right side, and 10 left side). Fourf the 12 patients had only one testicle because of testicleblation for treatment of testicular tumors. In 2 patients, arevious biopsy of both testicles revealed a Sertoli-cell-onlySCO) syndrome (Table 1). All patients underwent preoper-tive staging, including sperm count, hormone analysis, andesticular ultrasound, as well as normal staging for testicularumors. This study was approved by the Ethics Committee ofhe Medical University of Innsbruck, Innsbruck, Austria.
Patients with testicular tumors had no sperm in theirjaculate. In the other patients, no sperm had been retrievedrom previous TESE biopsies. Chromosomal analysis andearch for the azoosperm factor deletion in all 12 patientsevealed no cytogenetic abnormalities. The patients’ meange was 36.7 years (age range, 25–47 years). Mean hospi-alization was for 1 day. Routinely, testicles from whichiopsy samples were obtained were scanned by ultrasoundefore patients were discharged from the hospital.
erfusion-Controlled Testicular Biopsyatients underwent TESE for assisted reproduction (ICSI),s previously described (6,7). Preoperative testicular perfu-ion mapping using contrast-enhanced, high-resolution coloroppler ultrasound was performed (Fig. 1) and repeated
ntraoperatively using a �12 MHz probe of Acuson Sequoia
FIGURE 1
Contrast-enhanced color Doppler ultrasound of lefttesticle of patient 5. Arrows indicate areas ofmajor and minor perfusion.
Herwig. Testicle perfusion predicts sperm quality and quantity. Fertil Steril
d2007.
1072 Herwig et al. Testicle perfusion predicts sperm quality
12 (Acuson, Mountainview, CA), fitted with a high-fre-uency linear ultrasound probe (15LW40).
The reason for using an invasive method in combina-ion with our novel technology is that noninvasive needleiopsy does not permit precise localization of high sper-atogenic areas, and therefore leads to a random search
or sperm retrieval. Furthermore, tissue perfusion cannotet be measured via noninvasive needle biopsy. Thisonsideration is of greater importance in patients with nonob-tructive azoospermia.
A 22-gauge needle was placed in the area of best perfu-ion. Afterwards, a small incision was made with radiofre-uency cutting (Fig. 2). The exposed tissue was additionallycreened with a 3-mm laser Doppler probe, and perfusionates were determined using a BLF21 laser Doppler flow-eter (Transonic Systems, Inc., Ithaca, NY). The laseroppler flowmeter converts the “Doppler shift” of a laser
ight beam, which is frequency-shifted and reflected by aoving column of blood. Tissue perfusion units (TPU) were
efined arbitrarily, and were based on mean cell velocity andverage concentration of moving blood (mL/min/100 g).
Tissue biopsies were obtained for TESE from the leftnd/or right testicle, respectively (Fig. 3). Additionally, aandom biopsy was taken from the same testicle, and TPUere measured as previously described (6,8). Four biopsies
two perfusion-controlled, and two taken randomly) corre-pond to the average of four biopsies routinely taken blindlyrom patients with nonobstructive azoospermia (9).
Measurement of tissue perfusion levels was performedefore TESE. Radiofrequency cutting was used, because thisethod provides the best intact surface in deeper testicular
egions.
Testicular biopsy-score counts (Johnsen score) (10) were
FIGURE 2
Needle placement before radiofrequency cuttingand opening of the testicle.
Herwig. Testicle perfusion predicts sperm quality and quantity. Fertil Steril2007.
etermined from random biopsies. The size of testicular
and quantity Vol. 87, No. 5, May 2007
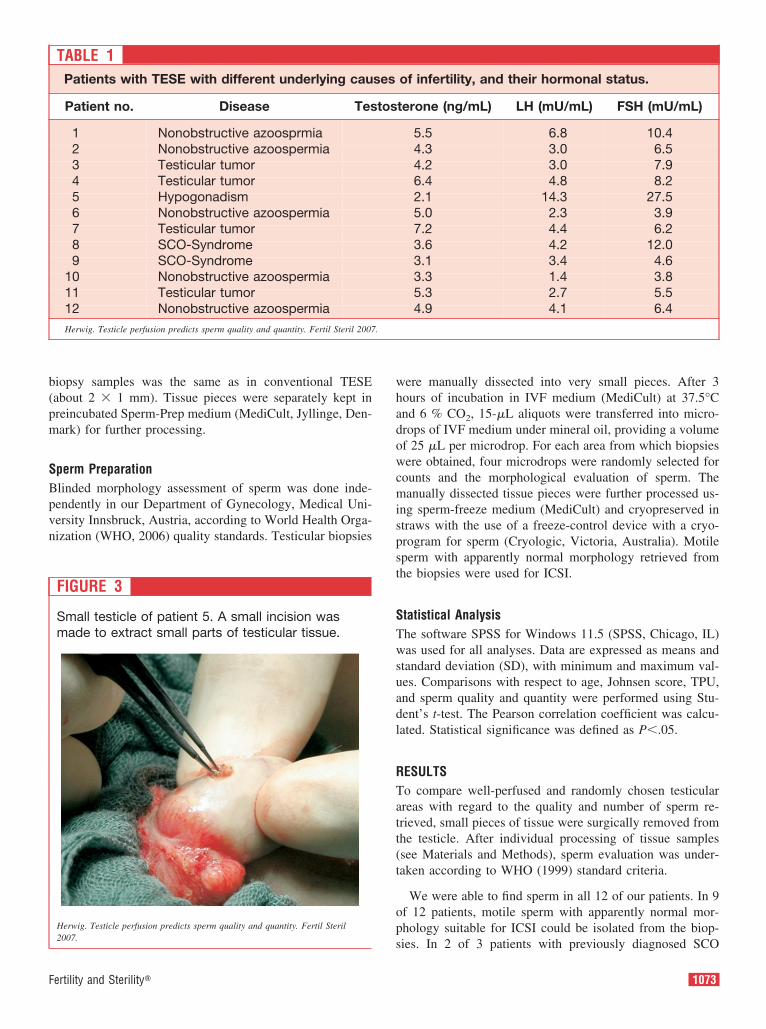
b(pm
SBpvn
whadowcmispst
STwsuadl
RTatt(t
op
.
F
iopsy samples was the same as in conventional TESEabout 2 � 1 mm). Tissue pieces were separately kept inreincubated Sperm-Prep medium (MediCult, Jyllinge, Den-ark) for further processing.
perm Preparationlinded morphology assessment of sperm was done inde-endently in our Department of Gynecology, Medical Uni-ersity Innsbruck, Austria, according to World Health Orga-ization (WHO, 2006) quality standards. Testicular biopsies
FIGURE 3
Small testicle of patient 5. A small incision wasmade to extract small parts of testicular tissue.
Herwig. Testicle perfusion predicts sperm quality and quantity. Fertil Steril
TABLE 1Patients with TESE with different underlying cau
Patient no. Disease Tes
1 Nonobstructive azoosprmia2 Nonobstructive azoospermia3 Testicular tumor4 Testicular tumor5 Hypogonadism6 Nonobstructive azoospermia7 Testicular tumor8 SCO-Syndrome9 SCO-Syndrome
10 Nonobstructive azoospermia11 Testicular tumor12 Nonobstructive azoospermiaHerwig. Testicle perfusion predicts sperm quality and quantity. Fertil Steril 2007
s2007.
ertility and Sterility�
ere manually dissected into very small pieces. After 3ours of incubation in IVF medium (MediCult) at 37.5°Cnd 6 % CO2, 15-�L aliquots were transferred into micro-rops of IVF medium under mineral oil, providing a volumef 25 �L per microdrop. For each area from which biopsiesere obtained, four microdrops were randomly selected for
ounts and the morphological evaluation of sperm. Theanually dissected tissue pieces were further processed us-
ng sperm-freeze medium (MediCult) and cryopreserved intraws with the use of a freeze-control device with a cryo-rogram for sperm (Cryologic, Victoria, Australia). Motileperm with apparently normal morphology retrieved fromhe biopsies were used for ICSI.
tatistical Analysishe software SPSS for Windows 11.5 (SPSS, Chicago, IL)as used for all analyses. Data are expressed as means and
tandard deviation (SD), with minimum and maximum val-es. Comparisons with respect to age, Johnsen score, TPU,nd sperm quality and quantity were performed using Stu-ent’s t-test. The Pearson correlation coefficient was calcu-ated. Statistical significance was defined as P�.05.
ESULTSo compare well-perfused and randomly chosen testicularreas with regard to the quality and number of sperm re-rieved, small pieces of tissue were surgically removed fromhe testicle. After individual processing of tissue samplessee Materials and Methods), sperm evaluation was under-aken according to WHO (1999) standard criteria.
We were able to find sperm in all 12 of our patients. In 9f 12 patients, motile sperm with apparently normal mor-hology suitable for ICSI could be isolated from the biop-
of infertility, and their hormonal status.
terone (ng/mL) LH (mU/mL) FSH (mU/mL)
5.5 6.8 10.44.3 3.0 6.54.2 3.0 7.96.4 4.8 8.22.1 14.3 27.55.0 2.3 3.97.2 4.4 6.23.6 4.2 12.03.1 3.4 4.63.3 1.4 3.85.3 2.7 5.54.9 4.1 6.4
ses
tos
ies. In 2 of 3 patients with previously diagnosed SCO
1073
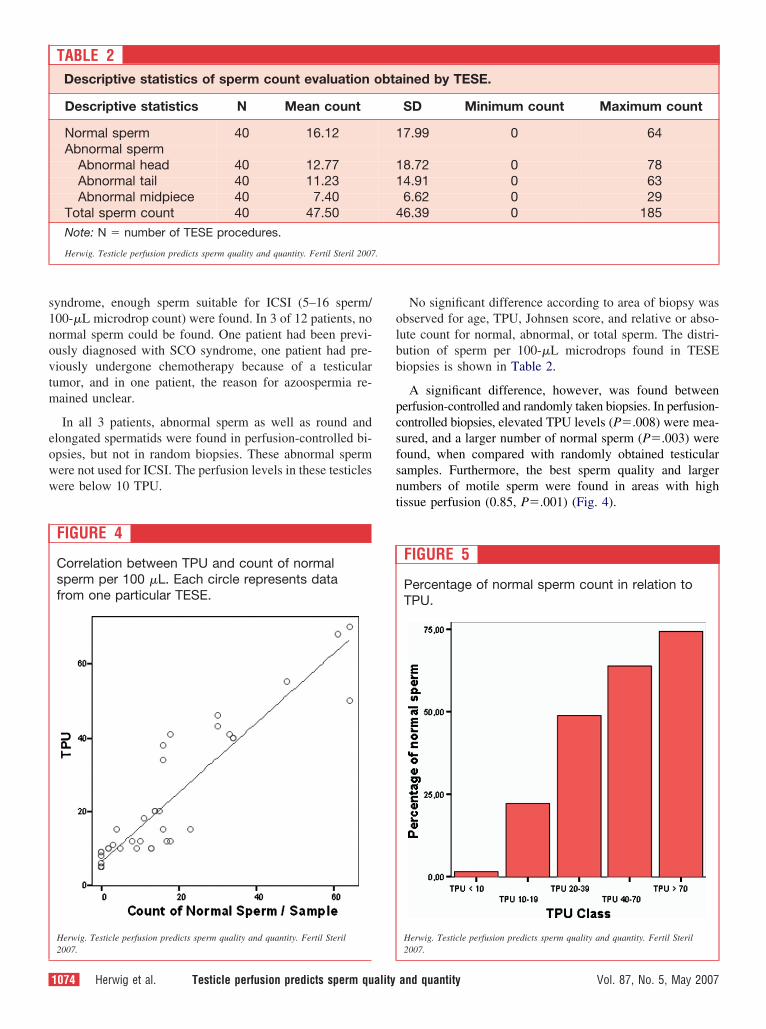
s1novtm
eoww
olbb
pcsfsnt
.
yndrome, enough sperm suitable for ICSI (5–16 sperm/00-�L microdrop count) were found. In 3 of 12 patients, noormal sperm could be found. One patient had been previ-usly diagnosed with SCO syndrome, one patient had pre-iously undergone chemotherapy because of a testicularumor, and in one patient, the reason for azoospermia re-ained unclear.
In all 3 patients, abnormal sperm as well as round andlongated spermatids were found in perfusion-controlled bi-psies, but not in random biopsies. These abnormal spermere not used for ICSI. The perfusion levels in these testiclesere below 10 TPU.
FIGURE 4
Correlation between TPU and count of normalsperm per 100 �L. Each circle represents datafrom one particular TESE.
TABLE 2Descriptive statistics of sperm count evaluation
Descriptive statistics N Mean count
Normal sperm 40 16.12Abnormal sperm
Abnormal head 40 12.77Abnormal tail 40 11.23Abnormal midpiece 40 7.40
Total sperm count 40 47.50Note: N � number of TESE procedures.
Herwig. Testicle perfusion predicts sperm quality and quantity. Fertil Steril 2007
2007.
1074 Herwig et al. Testicle perfusion predicts sperm quality
No significant difference according to area of biopsy wasbserved for age, TPU, Johnsen score, and relative or abso-ute count for normal, abnormal, or total sperm. The distri-ution of sperm per 100-�L microdrops found in TESEiopsies is shown in Table 2.
A significant difference, however, was found betweenerfusion-controlled and randomly taken biopsies. In perfusion-ontrolled biopsies, elevated TPU levels (P�.008) were mea-ured, and a larger number of normal sperm (P�.003) wereound, when compared with randomly obtained testicularamples. Furthermore, the best sperm quality and largerumbers of motile sperm were found in areas with highissue perfusion (0.85, P�.001) (Fig. 4).
FIGURE 5
Percentage of normal sperm count in relation toTPU.
ined by TESE.
SD Minimum count Maximum count
7.99 0 64
8.72 0 784.91 0 636.62 0 296.39 0 185
Herwig. Testicle perfusion predicts sperm quality and quantity. Fertil Steril
Herwig. Testicle perfusion predicts sperm quality and quantity. Fertil Sterilobta
1
11
4
2007.
and quantity Vol. 87, No. 5, May 2007

q4wsfsabs(apmmssd
wwts
hoi
DAotdthp(aslsic
pesmtoosmh
nrds
waolptIpfaA“tc
tsJI2dT
tsdcsifwprtrawh
trTt
aarps
F
In tissue areas with �70 TPU, 74.42% progressive A-uality sperm (Fig. 5) were found. In tissue areas with about0 TPU, 65.94% � 4.93% motile sperm were found, alongith nonmotile sperm and elongated spermatids as well as
perm with various kinds of abnormal morphology. Tissuerom areas with 20–40 TPU contained a lower number ofperm (48.84% � 6.02%) that were suitable for ICSI. Inddition, many abnormal sperm (double head, pinhead, dou-le and short tail, and defective midpiece) and elongatedpermatids were detected. Only very few normal sperm2.75% � 4.7%) were isolated from samples obtained fromreas of about 10 TPU; the rest were abnormal sperm andrecursor cells. Using motile sperm with apparently normalorphology for ICSI, the fertilization rate (2 pronuclei for-ation) ranged between 76%–89%. We did not observe a
ignificant difference in fertilization rate with the use ofperm from areas with different TPU levels, although theseata must be considered preliminary.
Because we found a highly significant correlation of TPUith the pathologically determined Johnsen score (P�.001),e were able to find sperm in all of our patients, even in
hose with a Johnsen score far below 8. The mean Johnsencore found in our patients was 7.21 (range, 2.1–9.5).
In routine postbiopsy control of the testicles, a smallematoma was observed in 8 of 40 testicles biopsied. Nother complications occurred after the described TESEntervention.
ISCUSSIONzoospermia is rather common in infertile men, and mayccur in 10%–20% of patients with abnormal semen (11). Inhe past, azoospermic men could fulfill their desire for chil-ren only via donor insemination in IVF programs. Theechnique of ICSI (12) in combination with TESE (13,14)as enabled motile sperm to be selected from azoospermicatients and utilized in assisted reproductive technologyART). A variety of different techniques of sperm retrievalnd biopsy, selected on the basis of patients’ infertilityyndromes, have enabled appreciable success rates for ICSI,eading to pregnancies and deliveries (15–20). Men whouffer from azoospermia now have the opportunity to fertil-ze their partners’ oocytes with their own sperm, and to havehildren with their own genetic profile.
An increase in the rate of miscarriages was recently re-orted for patients using TESE sperm in ART, and this wasxplained as most likely caused by genetically defectiveperm (21). In another report, no increased incidence ofiscarriages was found when comparing surgically retrieved
esticular sperm with freshly ejaculated sperm (3). More-ver, no difference in pregnancy loss or delivery rates wasbserved between freshly used and frozen-thawed testicularperm. On the other hand, parameters such as the maturity,orphology, and motility of testicular sperm were shown to
ave a major influence on fertilization outcomes and preg- c
ertility and Sterility�
ancy rate. Furthermore, maternal age and ovarian function,esponsible for oocyte quality and quantity, can significantlyetermine the outcome of ICSI with the use of testicularperm (22,23).
Previously, mostly randomly localized testicle biopsiesere carried out on azoospermic patients, and were predict-
bly associated with hormonal evaluation and classic histol-gy (24,25). Multiple biopsies were proposed to increase theikelihood of sperm retrieval (26). However, in azoospermicatients, random biopsy for TESE is associated with uncer-ainty of sperm recovery (27), resulting in cancellations ofVF cycles and discouragement in couples enrolled in ARTrograms. Fine-needle aspiration (FNA) has been employedor more precise testicle sampling, to gain local informationbout spermatogenesis and to identify sperm suitable forRT (28,29). It was also suggested that visually identified
fat” tubules containing sperm in patients with nonobstruc-ive azoospermia may be found, during micro-TESE, to belose to the vascular supply (30).
The testicular biopsy score count first described and in-roduced by Johnsen in 1970 is a method for registration ofpermatogenesis in human testes (10). Normally, a minimumohnsen score of 8 is required to find sperm suitable for ICSI.n our group of patients, a mean Johnsen score of 7.2 (range,.1–9.5) in random biopsies was registered. Therefore, weo not consider random biopsy to be an efficient method forESE.
Constant improvements in focally localizing presumptiveesticular areas for sperm retrieval were reported in the pasteveral years. Nevertheless, striking differences in spermetection and retrieval rates were observed among variouslinics, including our hospital, most likely due to differenturgical techniques and etiological variations in patients’nfertility syndromes. Therefore, we initiated and success-ully applied a novel technology by measuring perfusionithin the testis to determine whether the level of tissueerfusion correlates with the quality and quantity of spermetrieved from TESE. We documented for the first time thathe level of tissue perfusion matches well with the level ofecovered sperm in both quality and quantity. Less perfusedreas contain only few sperm of lower quality, whereasell-perfused areas contain a higher number of sperm ofigher quality, according to WHO (1999) criteria.
We did not observe a correlation between TPU levels andhe patients’ underlying diseases, which might be due to theelatively small number of patients analyzed. Whether or notPU levels correlate with a patient’s particular disease needs
o be investigated in future studies.
Our novel technique of perfusion-controlled testicular biopsyllows for predictable TESE, and better sperm samples for ICSInd cryopreservation in assisted reproduction. We thereforeecommend this new method of sperm retrieval in azoospermicatients. Because the outcome of ICSI is strongly dependent onperm quality, random TESE should be replaced by perfusion-
ontrolled biopsy of testicle tissue.1075

Abt
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
cknowledgments: The authors thank Ulrike Massie and Eva Maria Lem-erger for excellent technical assistance, and Rajam Csordas-Iyer for edi-orial and linguistic assistance.
EFERENCES1. Gordon UD. Assisted conception in the azoospermic male. Hum Fertil
(Camb) 2002;5(Suppl):S9–14.2. Kahraman S, Ozgur S, Alatas C, Aksoy S, Tasdemir M, Nuhoglu A, et
al. Fertility with testicular sperm extraction and intracytoplasmic sperminjection in non-obstructive azoospermic men. Hum Reprod 1996;11:756–60.
3. Palermo GD, Schlegel PN, Hariprashad JJ, Ergun B, Mielnik A, Zani-novic N, et al. Fertilization and pregnancy outcome with intracytoplas-mic sperm injection for azoospermic men. Hum Reprod 1999;14:741–8.
4. Sukcharoen N, Promviengchai S, Boonkasemsanti W, Sithipravej T,Chinpilas V. The outcome of sperm retrieval and intracytoplasmicsperm injection for obstructive azoospermia. J Med Assoc Thai 2001;84:1569–75.
5. Wood S, Lewis-Jones I, Troup S, Desmond A, Kingsland C. Surgicalsperm retrieval: a review of current practice. Hum Fertil (Camb) 2002;5:17–22.
6. Herwig R, Tosun K, Pinggera GM, Soelder E, Moeller KT, Pallwein L,et al. Tissue perfusion essential for spermatogenesis and outcome oftesticular sperm extraction (TESE) for assisted reproduction. J AssistReprod Genet 2004;21:175–80.
7. Herwig R, Tosun K, Pinggera GM, Leonhartsberger N, Gozzi C,Illmensee K, et al. Tissue perfusion essential for spermatogenesis andoutcome of testicular sperm extraction (TESE) for assisted reproduc-tion. Hum Reprod 2004;19:56.
8. Schuster A, Frauscher F, Strasser H, Recheis W, Pallwein L, Herwig R,et al. Power Doppler ultrasound imaging for quantification of urinarybladder neck blood flow changes. Ultrasound Med Biol 2004;30:1379 – 84.
9. Vernaeve V, Krikilion A, Verheyen G, Van Steirteghem A, Devroey P,Tournaye H. Outcome of testicular sperm recovery and ICSI in patientswith non-obstructive azoospermia with a history of orchidopexy. HumReprod 2004;19:2307–12.
0. Johnsen SG. Testicular biopsy score count—a method for registrationof spermatogenesis in human testes: normal values and results in 335hypogonadal males. Hormones 1970;1:2–25.
1. Ezeh UI. Beyond the clinical classification of azoospermia: opinion.Hum Reprod 2000;15:2356–9.
2. Palermo G, Joris H, Devroey P, Van Steirteghem AC. Pregnancies afterintracytoplasmic injection of single spermatozoon into an oocyte. Lan-cet 1992;340:17–8.
3. Jow WW, Steckel J, Schlegel PN, Magid MS, Goldstein M. Motilesperm in human testis biopsy specimens. J Androl 1993;14:194–8.
4. Schoysman R, Segal L, Van der Zwalmen P, Nijs M, Bertin G, CittadiniE, et al. Fertilization of oocytes by testicular spermatozoa and preg-nancy in the human. Acta Eur Fertil 1993;24:103–5.
5. Silber SJ, Van Steirteghem AC, Liu J, Nagy Z, Tournaye H, DevroeyP. High fertilization and pregnancy rate after intracytoplasmic sperminjection with spermatozoa obtained from testicle biopsy. Hum Reprod
1995;10:148–52.1076 Herwig et al. Testicle perfusion predicts sperm quality
6. Silber SJ, Devroey P, Tournaye H, Van Steirteghem AC. Fertilizingcapacity of epididymal and testicular sperm using intracytoplasmicsperm injection (ICSI). Reprod Fertil Dev 1995;7:281–92.
7. Ubaldi F, Nagy ZP, Rienzi L, Tesarik J, Anniballo R, Franco G, et al.Reproductive capacity of spermatozoa from men with testicular failure.Hum Reprod 1999;14:2796–800.
8. Madgar I, Hourvitz A, Levron J, Seidmann DS, Shulman A, Raviv GG,et al. Outcome of in vitro fertilization and intracytoplasmic injection ofepididymal and testicular sperm extracted from patients with obstruc-tive and nonobstructive azoospermia. Fertil Steril 1998;69:1080–4.
9. De Croo I, Van der Elst J, Everaert K, De Sutter P, Dhont M. Fertili-zation, pregnancy and embryo implantation rates after ICSI in cases ofobstructive and non-obstructive azoospermia. Hum Reprod 2000;15:1383–8.
0. Lin YM, Hsu CC, Kuo TC, Lin JS, Wang ST, Huang KE. Percutaneousepididymal sperm aspiration versus microsurgical epididymal spermaspiration for irreparable obstructive azoospermia—experience with100 cases. Taiwan I Hsueh Hui Tsa Chih (J Formos Med Assoc)2000;99:459–65.
1. Borges E, Rossi-Ferragut LM, Pasqualotto FF, dos Santos DR, RochaCC, Iaconelli A. Testicular sperm results in elevated miscarriage ratescompared to epididymal sperm in azoospermic patients. Sao Paulo MedJ 2002;120:122–6.
2. Silber SJ, Nagy Z, Devroey P, Camus M, Van Steirteghem AC. Theeffect of female age and ovarian reserve on pregnancy rate in maleinfertility: treatment of azoospermia with sperm retrieval and intracy-toplasmic sperm injection. Hum Reprod 1997;12:2693–700.
3. Altay B, Kefi A, Tavmergen E, Cikili N, Semerci B, Tavmergen GokerE. The effects of female age on the outcome of testicular spermextraction and intracytoplasmic sperm injection in infertile patientswith azoospermia. Int Urol Nephrol 2002;33:95–9.
4. Nagy ZP, Joris H, Verheyen G, Tournaye H, Devroey P, Van Steirteg-hem AC. Correlation between motility of testicular spermatozoa, tes-ticular histology and the outcome of intracytoplasmic sperm injection.Hum Reprod 1998;13:890–5.
5. Meng MV, Cha I, Ljung BM, Turek PJ. Relationship between classichistological pattern and sperm findings on fine needle aspiration map ininfertile men. Hum Reprod 2000;15:1973–7.
6. Schlegel PN, Palermo GD, Goldstein M, Menendez S, Zaninovic N,Veeck LL, et al. Testicular sperm extraction with intracytoplasmicsperm injection for nonobstructive azoospermia. Urology 1997;49:435– 40.
7. Tournaye H, Verheyen G, Nagy P, Ubaldi F, Goossens A, Silber S, etal. Are there any predictive factors for successful testicular spermrecovery in azoospermic patients? Hum Reprod 1997;12:80–6.
8. Turek PJ, Cha I, Ljung BM. Systematic fine-needle aspiration of thetestis: correlation to biopsy and results of organ “mapping” for maturesperm in azoospermic men. Urology 1997;49:743–8.
9. Mulhall JP, Burgess CM, Cunningham D, Carson R, Harris D, OatesRD. Presence of mature sperm in testicular parenchyma of men withnonobstructive azoospermia: prevalence and predictive factors. Urol-ogy 1997;49:91–5.
0. Schlegel PN, Li PS. Microdissection TESE: sperm retrieval in non-
obstructive azoospermia. Hum Reprod Update 1998;4:439.and quantity Vol. 87, No. 5, May 2007

Obtamd
RS
T
T
T
R
0d
Frequency of human sperm carrying structuralaberrations of chromosome 1 increaseswith advancing ageEddie D. Sloter, Ph.D.,a,b,c Francesco Marchetti, Ph.D.,a Brenda Eskenazi, Ph.D.,c
Rosana H. Weldon, M.P.H.,c Joginder Nath, Ph.D.,b Debby Cabreros, B.S.,a
and Andrew J. Wyrobek, Ph.D.a
a Biosciences Directorate, Lawrence Livermore National Laboratory, Livermore, California; b Genetics and DevelopmentalBiology Program, West Virginia University, Morgantown, West Virginia; and c Department of Epidemiology, School of PublicHealth, University of California, Berkeley, California
Objective: To investigate the association between male age and the frequency of sperm with de novo structuralchromosomal abnormalities.Design: Semen specimens collected from two groups of 10 healthy, nonsmoking men, aged 22–28 and 65–80years, were analyzed with the use of a multicolor fluorescence in situ hybridization assay for detecting breaks,segmental duplications and deletions, and aneuploidy and diploidy involving chromosome 1.Setting: Healthy volunteer workers and retirees from a government research environment.Main Outcome Measure: Sperm carrying numerical and structural chromosomal abnormalities.Result(s): We detected significant increases in the frequency of sperm carrying breaks and segmental duplicationsand deletions of chromosome 1 among older men compared with younger men. Older men carried twice thefrequency of sperm with segmental duplications and deletions of chromosome 1. The frequency of sperm carryingbreaks within the 1q12 fragile-site region nearly doubled in older men. In contrast to female gametes, there wasno effect of age on the frequency of sperm with numerical chromosomal abnormalities.Conclusion: Our findings suggest that advancing male age is associated with a gradual and significant increasein the risk of fathering children with various chromosomal defects such as segmental aneusomy syndromes.(Fertil Steril� 2007;87:1077–86. ©2007 by American Society for Reproductive Medicine.)
Key Words: Male age, human sperm, structural aberrations, chromosome 1, sperm FISH
amed(dIpinrlvaflc8
sssp
n average, about two million pregnancies per year are lostefore week 20 of gestation in the United States. Of thosehat survive to birth, about 7% have low birth weight, andbout 5% are born with a birth defect (1). The social andedical costs of abnormal reproductive outcomes are formi-
able, yet their causes are not well-understood.
eceived April 11, 2006; revised and accepted August 14, 2006.upported by the University of California, Berkeley, California (LawrenceLivermore National Laboratory contract W-7405-ENG-48), under theauspices of the U.S. Department of Energy, Washington, D.C., and bya grant from the Superfund (5P42ES0470511) of the National Instituteof Environmental Health Sciences, Research Triangle Park, North Caro-lina, and with tuition and travel support provided by West VirginiaUniversity, Morgantown, West Virginia (E.D.S.).
his work was done at the Biosciences Directorate, Lawrence LivermoreNational Laboratory, Livermore, California, and the Department of Ep-idemiology, School of Public Health, University of California, Berkeley,California.
he present address of Eddie D. Sloter, Ph.D., is the Department ofDevelopmental and Reproductive Toxicology, WIL Research Labora-tories, L.L.C., Ashland, Ohio.
he present address of Francesco Marchetti, Ph.D., is the Life SciencesDivision, Lawrence Berkeley National Laboratory, Berkeley, California.
eprint requests and present address: Andrew J. Wyrobek, Ph.D., LifeSciences Division, Lawrence Berkeley National Laboratory, 1 CyclotronRoad, 74R0157, Berkeley, California 94720 (FAX: 510 486-6746;
iE-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.08.112 Copyright ©2007 American Soc
A major proportion of abnormal reproductive outcomesre known to be associated with paternally transmitted nu-erical and structural chromosomal abnormalities (2). It was
stimated that 80% of structural chromosomal aberrationsetected during development or at birth are paternal in origin3–6), and de novo gene mutations for several autosomaliseases are also predominantly of paternal origin (7–10).ncreased life expectancies, changes in family-planningractices, and advances in assisted reproductive techniquesn industrialized countries are resulting in an increasingumber of births to couples aged 34–54 years (11). Thisaises substantial health concerns regarding the possibleong-term consequences of increasing paternal ages on theiability and genetic health of offspring because of theccumulation of damage in male germ cells. In contrast toemale fertility, which declines significantly by a woman’sate 30s, spermatogenesis continues well into male senes-ence (12), with only a gradual decline in fertility up to age0 years (13–15).
Advanced maternal age is known to increase the risk ofeveral abnormal pregnancy outcomes, including aneuploidyyndromes such as Down syndrome (16–21). Offspringtudies showed that older fathers are also at higher risk forroducing certain abnormal reproductive outcomes, includ-
ng pregnancy loss (22, 23), developmental and morpholog-1077Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

ivHosstiisgc
isb(nwgimuicyafsfdtactrAfccm
iowcpMg[1cgans
mfdlsd
MDTd6t(iadmllttuca
SSelisTplddAGItp
c(adiwphshqs
cal birth defects (24–26), neurological disorders (27), andarious clinical syndromes and genetic diseases (7, 28, 29).owever, determining the effect of male age from epidemi-logical studies of human offspring has been limiting foreveral reasons: [1] there are few affected offspring for eachyndrome available for study; [2] there is potential bias dueo indeterminate loss of chromosomally abnormal embryosn utero; and [3] there are established difficulties in separat-ng maternal and paternal effects (e.g., couples’ ages aretrongly correlated, as are lifestyles). Assays that detectenetic damage directly in male germ cells have helpedircumvent these issues.
Concern that certain types of chromosomal damage mayncrease with age in male germ cells derives, in part, fromtudies of somatic cells. Chromosomal damage, as measuredy frequencies of translocations (30, 31), acentric fragments31, 32), telomere shortening and loss (33–35), and micro-ucleus formation (36), was shown to increase progressivelyith age among actively dividing somatic cells. In maleerm cells, human and rodent data showed age-relatedncreases in the number of sperm with chromosomal frag-ents, which suggests that postmeiotic cell types are partic-
larly vulnerable to the effects of aging (37). A labor-ntensive method for analyzing human sperm metaphasehromosomes with the use of zona-free hamster eggs (38)ielded ambiguous data concerning age effects on breaksnd fragments (39–41), and was too inefficient to measurerequencies of rearrangements, duplications, and deletions inperm. New DNA hybridization strategies were developedor the detection of chromosomal aberrations (duplications,eletions, and breaks) in human and mouse sperm by mul-icolor fluorescence in situ hybridization (FISH) (42–44),nd are beginning to generate data on the effects of age onhromosomal aberrations in sperm. An age-related effect onhe frequency of centromeric deletions of chromosome 1 waseported in a cohort of 18 men aged 20–58 years (45).nother study found a significant age-related increase in the
requency of sperm with duplications and deletions for theentromeric and subtelomeric regions of chromosome 9, andhromosome 9 disomy as well as diploidy in a cohort of 18en aged 24–74 years (43).
In the present study, FISH was used to target three repet-tive sequence regions along chromosome 1 for the detectionf specific de novo breaks and rearrangements directlyithin human sperm nuclei. This multicolor FISH method,
alled the ACM sperm FISH assay because it utilizes DNArobes specific for the Alpha (1cen), Classical (1q12), andidi (1p36.3) satellite regions of chromosome 1 (42), inte-
rates four concepts of prior work into a single procedure:1] the detection of duplication and deletion products for thep36.3 chromosomal region (46); [2] the detection of dupli-ation and deletion products for the 1cen chromosomal re-ion (46); [3] the measurement of chromosomal breakslong the 1q12 fragile-site region (47); and [4] analyses ofumerical abnormalities (48). We applied the ACM assay to
perm samples from two groups of 10 healthy, nonsmoking r1078 Sloter et al. Age and chromosome aberrations in sperm
en, aged 22–28 and 65–80 years, to determine whetherrequencies of sperm carrying specific structural (breaks,uplications, and deletions) or numerical (disomy, and dip-oidy) abnormalities of chromosome 1 are higher in theperm of older men, and if so, whether the age responsesiffer across types of defects.
ATERIALS AND METHODSonor Recruitmenthe study population consisted of the youngest 10 spermonors (aged 22–28 years) and 10 oldest sperm donors (aged5–80 years) selected from among 97 healthy male volun-eers recruited for the Age and Genetic Effects on SpermAGES) Study (13). The AGES Study was approved by thenstitutional review board of each participating institution,nd all volunteers gave written consent to participate. Theonors were employees or retirees of the Lawrence Liver-ore National Laboratory (LLNL), Livermore, California, a
arge multidisciplinary government research laboratory. Pre-iminary screenings excluded [1] men who had current fer-ility or reproductive problems; [2] had smoked cigarettes inhe previous 6 months; [3] had a vasectomy or a history of anndescended testicle or prostate cancer; [4] had receivedhemotherapy or radiation treatments for cancer; or [5] hadprevious semen analysis with zero sperm count.
perm Analysesemen samples were collected by masturbation and deliv-red within two hours of collection to the semen-analysisaboratory at LLNL. Technicians were blinded to the age anddentity of each man. Semen smears were prepared on glasslides and stored at �20°C in nitrogen gas with desiccant.he sperm decondensation and ACM FISH hybridizationrocedures were as previously described (42), with the fol-owing modification. The 1cen alpha satellite probe waserived from a purified plasmid clone, pSD21-1 (49), andirectly labeled with tetramethylrhodamine-6-dUTP (Rochepplied Science, Indianapolis, IN) with the use of theIBCO BRL Nick Translation System (Life Technologies,
nc., Gaithersburg, MD). All DNA probes were hybridizedo human lymphocyte metaphase chromosomes, to verifyrobe specificity.
The ACM FISH method had high hybridization efficien-ies in sperm (�99.99%), and high probe sensitivities�99.94% for 1p36.3, and �99.99% for 1cen and 1q12,ssuming the extreme case that all missing domains wereue to technical reasons). For each donor, two slides werendependently hybridized and scored by two blinded scorersith the use of slides that were coded for analysis by a thirderson. Each scorer analyzed �5,000 sperm from the topalf of each slide. The slides were then recoded, and aecond set of 5,000 sperm were analyzed from the bottomalf of each slide for a total of �10,000 sperm per slide. Foruality control, the first and second scoring analyses of eachlide for each scorer were compared with the use of Coch-
an’s equal-proportions test (50).Vol. 87, No. 5, May 2007

BdoobIdsm1pwrw1rpflcc
tir
STanofm01
Stcgci
F
Strict microscope scoring criteria were utilized (42).riefly, sperm carrying an abnormal number of same-coloromains were scored as abnormal only if the domains weref similar size and intensity, and were clearly separated byne full domain width. Each fluorescence domain had toe located within the boundary of an intact sperm nucleus.n this article, “dup” or “del” refers to duplication oreletion, respectively, of an unknown amount of chromo-omal material that extends beyond the chromosomal seg-ent hybridized by the DNA probe. Breaks involving the
q12 region were assigned to 10 groups based on location, asreviously described (42). Briefly, group 1 included spermith breaks occurring directly between the 1cen and 1q12
egions (Fig. 1F). Groups 2–10 included sperm with breaksithin the 1q12 region (Fig. 1E). The relative size of the twoq12 signals produced by a break was used to estimate theelative breakpoint location within 1q12 (Fig. 2). Overlap-ing sperm nuclei were not scored. Only cells that had aagellum (or tail attachment site) under phase-contrast mi-roscopy were scored. Because DNA probes may not effi-iently penetrate condensed sperm chromatin, sperm smaller
FIGURE 1
Detection of chromosomally abnormal human spermlabeling strategy for the fluorescent DNA probes spePacific Blue), and Midi (1p36.3, FITC) satellite regionssperm nuclei taken under �1,000 magnification withprobes, and with phase-contrast imaging to visualizeshowing one red (1cen), one blue (1q12), and one grregions are contiguous on chromosome 1, and theirnormal sperm. (C) Sperm carrying a duplication of 1pSperm with a duplication of the 1cen–1q12 region (1one green terminal 1p36.3 domain. (E) Break within 1(red) domain, and one 1p36.3 (green) domain. (F) Abn(blue) chromosomal regions, consistent with a breakcarrying two copies of each of the three probes on cdiploidy.
Sloter. Age and chromosome aberrations in sperm. Fertil Steril 2007.
ertility and Sterility�
han the normal size limits for decondensed sperm (5–10 �mn length, as determined by using a microscope eyepieceeticle) were excluded from analysis.
tatistical Analyseshis study was designed to have 80% power to detect at least50% difference in the frequencies of chromosomally ab-
ormal sperm between the youngest and oldest groups, basedn the mean and variance of preexisting ACM FISH datarom nine healthy donors (unpublished data). Power esti-ates were based on an alpha of 0.05 (one-tailed), a beta of
.8, 10,000 sperm scored per semen specimen, and a Poisson
.4-fold variance inflation.
All statistical analyses were performed with the use oftata 8.0 (StataCorp LP, College Station, TX). Age was
reated as a dichotomous variable with the “young” group,ontaining individuals aged 22–28 years, and the “old”roup, containing individuals aged 65–80 years. Each out-ome measured by the ACM assay contained two values perndividual because of the two independent scorings. One
the use of the ACM sperm FISH method. (A) Dye-for the Alpha (1cen, rhodamine), Classical (1q12,-G) Photomicrographs of normal and abnormaluse of fluorescence microscopy to visualize thesperm head and tail. (B) Normal haploid sperm
(1p36.3) fluorescence domain. The 1cen and 1q12escent domains are adjacent to each other in
(1p36.3 dup, Table 1) with two green domains. (D)dup, Table 1), with two centromeric domains but, indicated by two 1q12 (blue) domains, one 1cenal separation between the 1cen (red) and 1q12een these two regions. (G) Larger sperm nucleusosome 1, indicating either disomy 1 or sperm
withcific. (Bthethe
eenfluor36.3
cenq12orm
betwhrom
1079

mopsgbi
aastomw
lswmeaef
s4bitSpTtitowc
RAhcmfsmed2batmcw
t1dadttntfm
an from the 22–28-year age group was excluded as anutlier from statistical analyses, because both scorers re-orted unusually high frequencies of sperm with chromo-omal abnormalities compared to the mean of the two ageroups (2.1-fold, 5.7-fold, and 8.1-fold differences forreaks, duplications and deletions, and numerical abnormal-ties, respectively).
Generalized estimating equations (GEE) were used toccount for correlations between scorers (51), and the neg-tive binomial family was chosen to adjust for overdisper-ion in the data. Although an exchangeable correlation struc-ure between an individual’s counts was assumed, the robustption was used to obtain estimates of the SE. Separateodels were fit for each ACM measurement, and each model
FIGURE 2
Breakpoint distribution patterns were not normallydistributed along 1q12. In total, 558 breaksdetected by ACM FISH were classified into 10different breakpoint groups, using strict scoringcriteria (42). The diagram of chromosome 1indicates the general regions where breakage wasobserved along 1q12. A separation of signals byone full domain width was the strict criterion usedfor all breaks at each location. As shown in theidiogram, breakpoint 1 represents breaks locateddirectly between the 1cen (red) and 1q12 (blue)regions, and breakpoint 10 represents breakslocated in the most distal region of 1q12. Mostbreaks were observed at locations 1 and 6. Datapoints represent the average frequency of breaks(per 10,000 � SE) at each specified location within1q12 among the men in each age group. Menaged 65–80 years (�) and 22–28 (�) years.
Sloter. Age and chromosome aberrations in sperm. Fertil Steril 2007.
as offset by the total number of sperm scored. Due to the s
1080 Sloter et al. Age and chromosome aberrations in sperm
imited sample size, the GEE models were only adjusted bycorer. The interaction of age and scorer on the outcomesas investigated by adding an interaction term to the GEEodels. All regression-model assumptions were checked by
valuating standardized residuals for mean values close to 0nd SDs close to 1. Regression-model coefficients werexponentiated to obtain incident rate ratios (IRRs) and trans-ormed 95% confidence intervals for each outcome.
To obtain further insights into the shape of the age re-ponse, data from four healthy, nonsmoking men in their0s, previously analyzed with the use of the ACM assay (42)y one of the scorers of the current study, were integratednto the present data set. These four men were recruitedhrough an institutional review board-approved Anonymousemen Donor Program, and were from the same underlyingopulation as the current study, i.e., employees of LLNL.he GEE models were used to examine whether the rela-
ionships between continuous age and structural and numer-cal abnormalities were generally linear, particularly be-ween the ages of 30–65 years. Figure 4 was generated byverlaying the predicted fit of the data from the GEE modelsith scatterplots of the frequency of anomalies per 10,000
ells scored (averaged by participant) and age in years.
ESULTSs shown in Table 1, older men compared to younger menad a significantly higher frequency of sperm with structuralhromosomal abnormalities, including chromosome 1 seg-ental duplications and deletions and breaks within the 1q12
ragile site (P�.001). Stratified analyses showed that bothcorers found that all classes of sperm with structural chro-osomal abnormalities detected by the ACM assay were
levated in older men with respect to younger men, but withifferent significance levels between the two scorers (Table). Given that the direction of the effect was the same foroth scorers (i.e., higher frequencies of sperm with structuralberrations in older men), both sets of data were included inhe analyses. In addition, the scores were not averaged beforeodeling, and the correlations between scorers were ac-
ounted for by the GEE model (see Materials and Methods),hich provided more valid estimates of the SE.
There was a 2.3-fold increase in the number of sperm witherminal (1p36.3) duplications and deletions (P�.001), and a.7-fold increase in centromeric (1cen) duplications andeletions (P�.07), in the older group. In total, there werebout 2–3-fold more sperm with segmental duplications andeletions involving the subtelomere (1p36.3) than the cen-romere (1cen), regardless of the age group (Table 1). Al-hough the frequency of sperm containing duplications wasot statistically different from the frequency of sperm con-aining deletions, there was a slight trend toward higherrequencies of sperm with segmental duplications in eachan, regardless of chromosomal region or age.
Older men had a 1.6-fold increase in the frequency of
perm with breaks in the 1q12 fragile site (P�.001). TheseVol. 87, No. 5, May 2007

cpgnmtdbFHm(bddS
Stoabotd
cdmo
F
hromosomal breaks were classified according to the ap-roximate location of their breakpoint within the 1q12 re-ion. As shown in Figure 2, the breakpoint locations wereot randomly distributed within 1q12; rather, they occurredost frequently in two regions regardless of age: adjacent to
he alpha centromeric satellite sequences, and near the mid-le of the region. This distribution pattern was consistentetween the two scorers. Except for breakpoint location 4 inigure 2, all other breakpoint locations increased with age.owever, only breakpoint location 2 near the alpha centro-eric satellite sequences reached statistical significance
P�.02). In both age groups, the frequencies of sperm withreaks in 1q12 and the frequencies of sperm with segmentaluplications and deletions (1p36.3 dup, 1p36.3 del, 1cenup, 1cen del) were strongly correlated (P�.001, r � 0.59,
TABLE 1Frequencies of sperm with structural and numergroups of healthy men, as determined by ACM s
Age
22–28 ye(24.9)
Number of menTotal sperm analyzedc 186,53Segmental duplications and deletionsd
1cen dupd 1.0 � 01cen deld 0.5 � 0
1cen total 1.5 � 01p36.3 dup 2.2 � 01p36.3 del 1.6 � 0
1p36.3 total 3.8 � 0Total duplications and deletionse 5.3 � 0Breaks within 1q12 10.9 � 0Total structural 16.2 � 1Numerical
Disomy 1 and diploidyf 12.9 � 2Nullisomy 1g 0.3 � 0
Total numerical 13.1 � 2Total anomaliesh 29.4 � 2Note: Frequency per 10,000 sperm (�SE).a Incident rate ratio, using generalized estimating equatiob 95% confidence interval of IRR.c For each donor, two scorers each analyzed 10,000 sperd Abbreviations “dup” and “del” indicate duplications and d
material encompassing the probe.e Sum of 1cen total and 1p36.3 total.f The ACM assay cannot distinguish disomy 1 from spe
pattern in this assay.g Sperm with no hybridization domains may represent nuh Includes total sperm with structural and numerical abnorm
10,000 sperm in young and old groups, respectively). “Ocarrying 1p36.3 dup as well as a break within 1q12.
Sloter. Age and chromosome aberrations in sperm. Fertil Steril 2007.
pearman’s correlation, Fig. 3). c
ertility and Sterility�
When data from the two age groups of men of the AGEStudy were integrated with data from the from four donors in
heir 40s previously analyzed using the ACM assay (42) byne of the scorers of the present study, the age response forll three classes of structural abnormalities (dup, del, andreaks) was generally linear, with no indication of a thresh-ld (Fig. 4). Overall, there was an estimated 13% increase inhe frequencies of sperm with structural aberrations for everyecade of life, beginning in a man’s 20s (Table 3).
In contrast to the significant effects of age on the frequen-ies of sperm with structural aberrations, no age effects wereetected for the frequency of sperm with numerical abnor-alities of chromosome 1 (P�.9, Fig. 4A). The frequencies
f sperm with an extra copy of chromosome 1 (i.e., sperm
chromosomal abnormalities among two ageFISH.
up (mean)
65–80 years(70.1) IRRa 95% CIb P-value
10201,152
2.1 � 0.50.9 � 0.23.0 � 0.5 1.69 0.94–2.28 .075.3 � 0.63.6 � 0.68.8 � 1.0 2.26 1.69–3.03 �.001
11.9 � 1.0 2.25 1.64–3.08 �.00117.6 � 2.0 1.61 1.23–2.10 �.00129.5 � 2.6 1.77 1.41–2.24 �.001
14.2 � 2.40.8 � 0.2
15.1 � 2.4 1.01 0.70–1.47 .9545.4 � 4.1 1.42 1.18–1.72 �.001
dels (see Materials and Methods).
n independently hybridized slides.ions, respectively, of an unknown stretch of chromosomal
iploidy, which has the same fluorescence hybridization
y 1.ies plus those sperm classified as “other” (0.2 and 0.8 per” includes sperm with multiple abnormalities, e.g., sperm
icalperm
gro
ars
95
.3
.2
.3
.4
.3
.3
.6
.9
.3
.1
.2
.1
.4
n mo
m oelet
rm d
llisomalit
ther
ontaining six probe signals) were �10 times higher than
1081

spoasanonir
DWessamcisctapbs
emrfc11tba1ctscs
otta
perm missing chromosome 1 (i.e., sperm with no detectablerobe signals). However, because sperm with an extra copyf chromosome 1 may also represent diploid sperm, a sep-rate aneuploidy assay was applied to these men in a separatetudy with the use of FISH probes for chromosomes X, Y,nd 21. We found that nearly all of these numerically ab-ormal sperm were indeed diploid (data not shown). Finally,nly 22 sperm out of �390,000 (i.e., 0.5 per 10,000) showedo hybridization signals. Sperm that lack all three hybrid-zation domains may represent true nullisomy 1, or they mayepresent technical artifacts.
TABLE 2Incident rate ratios, 95% confidence intervals, an
Sc
IRR 95%
Total breaks 2.06 1.45–Total duplications and deletions 2.82 2.03–Total structural aberrations 2.29 1.73–Total numerical abnormalities 0.96 0.64–Total anomalies 1.63 1.29–Note: IRR � incident rate ratio; 95% CI � 95% confidenc
Sloter. Age and chromosome aberrations in sperm. Fertil Steril 2007.
FIGURE 3
Association between frequencies of sperm withsegmental duplications and deletions of thecentromeric and telomeric regions of chromosome1 and frequencies of sperm with breaks in 1q12.Each data point represents the frequency ofabnormal sperm (per 10,000 sperm) in eachdonor’s semen sample (r � 0.59, P�.001).
aSloter. Age and chromosome aberrations in sperm. Fertil Steril 2007.
1082 Sloter et al. Age and chromosome aberrations in sperm
ISCUSSIONe employed the ACM sperm FISH assay to examine the
ffects of male age on the frequency of sperm carryingpecific structural and numerical defects involving chromo-ome 1. Significant associations with age were observedcross several categories of structural chromosomal abnor-alities, including the 1p36 deletion site, which was asso-
iated with severe developmental and morphological defectsn human offspring (52–54). Frequencies of sperm carryingegmental duplications and deletions of chromosome 1 in-reased at about the same rate per decade of male age ashose with breaks in the 1q12 fragile site. Although we foundge-associated changes in sperm chromosomal breaks, du-lications, and deletions, no evidence for an associationetween age and numerical chromosomal abnormalities inperm was observed.
Our findings identify paternal age as a risk factor in thetiology of 1p36 deletion syndrome. Monosomy 1p36 (ter-inal deletion of chromosome 1) is associated with mental
etardation, developmental delay, and major congenital mal-ormations in children, and is considered one of the mostommon terminal deletion syndromes, affecting as many as–2 children per 10,000 (53, 55). Although the incidence ofp36 duplications among children is considerably rarer thanhat of 1p36 deletions (56), perhaps due to an ascertainmentias related to a milder phenotype, our data also predict anssociation of male age in the frequency of conceptuses withp36 duplications. The relationship of age and 1p36 dupli-ations and deletions appears to be comparable in magnitudeo the observed exposure-related associations in humanperm chromosomes after various environmental exposures:hemotherapy (a 1.4–4-fold increase versus controls) (48),moking (�2-fold) (57, 58), and diazepam (1.5–2.5-fold) (59).
The frequencies of sperm carrying segmental duplicationsr deletions of the same chromosomal region were not sta-istically different from each other (Table 1), which suggestswo possible etiologies underlying their increase with malege. Duplications and deletions in sperm could arise from an
values for ACM outcomes by scorer.
1 Scorer 2
P value IRR 95% CI P value
�.0001 1.26 0.88–1.79 .21�.0001 1.70 0.96–3.00 .07�.0001 1.36 0.96–1.93 .08
.85 1.05 0.68–1.61 .83�.0001 1.25 0.94–1.66 .13
terval.
d P
orer
CI
2.923.933.021.452.05e in
ge-related increase in the frequency of spermatogonia car-
Vol. 87, No. 5, May 2007

r(pecvrsccifssc
gsmpsmrdsnci
q1hit6
Sloter. Age and chromosome aberrations in sperm. Fertil Steril 2007.
Fertility and Sterility�
ying a reciprocal translocation or inversion involving 1p4% of the human genome). Indeed, phenotypically normalarents are often identified as reciprocal translocation carri-rs after the birth of offspring carrying de novo partialhromosomal duplications or deletions. Our laboratory pre-iously analyzed semen from a t(1;10)(p22.1;q22.3) recip-ocal translocation carrier, and found similar frequencies ofperm containing duplications and deletions of the probedhromosomal segment (60). Spermatogonia carrying a peri-entric inversion with subsequent recombination within thenversion loop during meiosis could also produce such de-ective sperm. Alternatively, misalignment of chromosomalegments during meiotic recombination (61), especially inubtelomeric regions (62), could produce sperm with dupli-ated or deleted chromosomal regions.
Frequencies of sperm with segmental duplications wereenerally slightly higher than frequencies of sperm withegmental deletions of the same chromosomal region in eachan regardless of age, suggesting that there may not be a
erfectly symmetrical relationship in the formation or per-istence of these presumably reciprocal events during sper-atogenesis. Further research is needed to determine the
elative contributions of these mechanisms for producingefective sperm that lead to offspring with segmental aneu-omy syndromes (63). Further sperm technology is alsoeeded to determine whether sperm associated with otherhromosomal terminal deletions show similar age-relatedncreases and sensitivities.
We found a significant age-related increase in the fre-uency of sperm with breaks within the 1q12 region (Table). The large block of heterochromatin located at 1q12 isighly polymorphic, and was identified as a 5-azacytidine-nduced fragile site (64). Band 1q12 was found to be sensi-ive to breakage in mutagen-exposed lymphocytes (47, 65–7), buccal mucosal cells (68), cells in amniotic fluid (69),
TABLE 3Incidence rate ratios with their 95%confidence intervals for the change in ACMoutcomes per decade increase in age.
IRR 95% CI P value
Total breaks 1.11 1.05–1.17 �.0001Total duplications
and deletions1.18 1.11–1.26 �.0001
Total structuralaberrations
1.13 1.08–1.19 �.001
Total numericalabnormalities
1.02 0.93–1.13 .62
Total anomalies 1.09 1.04–1.15 .001Note: IRR � incident rate ratio; 95% CI � 95% confi-
dence interval.
FIGURE 4
Age response for categories of chromosomaldefects detected by ACM sperm FISH. Negativebinomial models are shown of the counts of spermanomalies versus age with the overlaid fittednegative binomial model adjusted by scorer. (A)Total structural and total numerical abnormalities.(B) Total duplications and deletions. (C) The 1p36terminal duplications and deletions, and 1cenduplications and deletions. (D) Total breaks withinthe 1q12 fragile site. Data from the four men intheir 40s are from Sloter et al. (42).
Sloter. Age and chromosome aberrations in sperm. Fertil Steril 2007.
1083

abp[mstgqoui
miosssnsadeao
aasaRf(tacbmtce
eaiaaioascl2
qt�mdsdvralaFai
foptmswsdca1auwOwtir
AwatbSdSmWS
R
nd cancer cells (70, 71). The age-related increase in 1q12reaks in sperm observed in the current study may be: [1] theroduct of rearrangements affecting 1q12 in spermatogonia,2] the products of unequal crossing over in primary sper-atocytes, or [3] the result of breaks occurring during early
permiogenesis. We observed good agreement (P�.5) be-ween the overall frequency of breaks within 1q12 across ageroups (�15 breaks per 104 sperm) and the calculated fre-uency of 18 breaks per 104 sperm karyotypes (9/5,055)bserved in the same chromosomal region by laboratoriessing the human-sperm and hamster-egg cytogenetic methodn a total of 56 healthy donors (40, 72–75).
Our results suggest that breaks within 1q12 in sperm areost likely the consequence of increasing chromosomal
nstability in the DNA-repair-deficient postmeiotic stagesf spermatogenesis with age, leading to unrejoined chromo-omal breaks within this region in mature sperm. Indeed, atudy using the human-sperm and hamster-egg techniquehowed that acentric fragments were the most common ab-ormality in the sperm of older men (41). Fertilization byperm carrying such breaks would be expected to producecentric fragments that would be lost during early embryonicevelopment, or to provide the opportunity for chromosomalxchanges in the zygote, resulting in early pregnancy loss orchromosomal rearrangement in the chromosomes of the
ffspring (76).
Our study is the first to use a sperm FISH assay that, inddition to detecting segmental duplications and deletionsnd numerical changes, allows for the detection of chromo-omal breaks in sperm. Moreover, this assay demonstratedn increased association of chromosomal breaks with age.ecent studies also reported age-related increases in the
requencies of sperm with partial duplications or deletions43, 45). Taken together, these results show that as men age,heir frequencies of sperm that carry chromosomal structuralberrations increase, and the results suggest that the spermhromatin of older men may be more prone to chromosomalreaks than that of younger men. Age-related associationsay be due to physiological alterations in the aging testis,
he decreased efficiency of DNA repair systems, or an ac-umulation of DNA damage from environmental and endog-nous sources (14, 15, 37).
In contrast to our finding of increased chromosomal ab-rrations in the sperm of older men, our study did not find ange-related increase in the frequencies of sperm with numer-cal abnormalities. This is in agreement with the results ofnother study of the same population that used a sperm FISHssay specific for numerical chromosomal abnormalities,.e., aneuploidy and diploidy (77). Previous results fromther FISH studies provided ambiguous evidence for anssociation of men’s age and autosomal aneuploidies inperm (37, 77–81). For example, an increase in the frequen-ies of sperm with chromosome 9 disomy, as well as dip-oidy, was reported in a cohort of 18 healthy men aged
4–74 years (43).1084 Sloter et al. Age and chromosome aberrations in sperm
Bosch et al. (43) also reported significantly higher fre-uencies of duplications and deletions for chromosome 9han those we reported for chromosome 1 (�7-fold and
3-fold higher for duplications and deletions of the centro-eric and telomeric regions, respectively). The observed
iscrepancy in the magnitude of an age effect for chromo-omes 1 and 9 may be explained by as yet unknown cohortifferences in chromosome-specific baseline or age-relatedariations. However, differences in technique, especially inegard to sperm pretreatments, hybridization efficiencies,nd scoring criteria, are known to account for large inter-aboratory variations in the frequencies of chromosomallybnormal sperm, even when the same probe is used (82).inally, microscope scoring criteria remain subjective, ands shown in the present study, even intralaboratory variations difficult to eliminate completely.
Overall, our findings suggest that the increasing trend ofathering children at older ages predicts a greater incidencef abnormal reproductive outcomes and genetic diseases ofaternal origin resulting from chromosomal breaks, duplica-ions, and deletions, assuming that sperm with these abnor-alities are as likely to fertilize as normal sperm. A broad
pectrum of abnormal reproductive outcomes was associatedith the types of chromosomal defects that we detected in
perm, such as spontaneous abortions, neonatal death, birthefects, developmental delay, and mental retardation. Spe-ifically, our data predict that advancing paternal age may bessociated with an increased risk for offspring carrying thep36 deletion syndrome. Aging men are also predicted to bet increased risk for transmitting the 1p36 duplication prod-ct to offspring, although the health consequences associatedith duplications are less understood than those of deletions.ur observed association of age with the frequency of spermith a 1q12 breakage may have significant clinical implica-
ions, given the general concurrence between genomic frag-le sites and de novo breakpoint locations of chromosomalearrangements in spontaneous abortions and newborns (83).
cknowledgments: The authors thank Sharon Kidd, M.P.H., for assistanceith donor recruitment and initial data management, Xiu Lowe, M.D., for
ssistance with the initial study design, Dan Moore, Ph.D., for helping withhe preliminary statistical analyses, Nicholas Jewell, Ph.D., and Alan Hub-ard, Ph.D., for consultation on the GEE models, and Lee Moore, Ph.D.,uzanne Young, M.H.P., and Elana Wallenstein, M.P.H., for managingonor questionnaire data. We acknowledge Dan Pinkel, Ph.D., and Rickegrave, Ph.D., for generously providing the pUC1.77 and pSD21-1 plas-id clones. This paper was published with the approval of the director of theest Virginia Agriculture, Forestry, and Consumer Sciences Experiment
tation as paper no. 2972.
EFERENCES1. Statistical abstract of the United States, U.S. Bureau of the Census.
112th ed. Washington, DC, 1992.2. Shelby MD, Bishop JB, Mason JM, Tindall KR. Fertility, reproduction,
and genetic disease: studies on the mutagenic effects of environmentalagents on mammalian germ cells. Environ Health Perspect 1993;100:283–91.
3. Olson SB, Magenis RE. Preferential paternal origin of de novo struc-
tural chromosome rearrangements. In: Daniel A, ed. The cytogeneticsVol. 87, No. 5, May 2007

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
F
of mammalian autosomal rearrangements. New York: Alan R. Liss,1988:583–99.
4. Cody JD, Pierce JF, Brkanac Z, Plaetke R, Ghidoni PD, Kaye C, et al.Preferential loss of the paternal alleles in the 18q� syndrome. Am JMed Genet 1997;69:280–6.
5. Dallapiccola B, Mandich P, Bellone E, Selicorni A, Mokin V, Ajmar F,et al. Parental origin of chromosome 4p deletion in Wolf-Hirschhornsyndrome. Am J Med Genet 1993;47:921–4.
6. Overhauser J, McMahon J, Oberlender S, Carlin ME, Niebuhr E,Wasmuth JJ, et al. Parental origin of chromosome 5 deletions in thecri-du-chat syndrome. Am J Med Genet 1990;37:83–6.
7. Crow JF. The origins, patterns and implication of human spontaneousmutations. Nat Rev Genet 2001;1:40–7.
8. Tiemann-Boege I, Navidi W, Grewal R, Cohn D, Eskenazi B, WyrobekAJ, et al. The observed human sperm mutation frequency cannotexplain the achondroplasia paternal age effect. Proc Natl Acad Sci USA2002;99:14952–7.
9. Glaser RL, Broman KW, Schulman RL, Eskenazi B, Wyrobek AJ, JabsEW. The paternal-age effect in Apert syndrome is due, in part, to theincreased frequency of mutations in sperm. Am J Hum Genet 2003;73:939–47.
0. Goriely A, McVean GA, Rojmyr M, Ingemarsson B, Wilkie AO.Evidence for selective advantage of pathogenic FGFR2 mutations in themale germ line. Science 2003;301:643–6.
1. Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, MunsonML. Births: final data for 2002. Natl Vital Stat Rep 2003;52:1–113.
2. Kidd SA, Eskenazi B, Wyrobek AJ. Effects of male age on semenquality and fertility: a review of the literature. Fertil Steril 2001;75:237–48.
3. Eskenazi B, Wyrobek AJ, Sloter E, Kidd SA, Moore L, Young S, et al.The association of age and semen quality in healthy men. Hum Reprod2003;18:447–54.
4. Kuhnert B, Nieschlag E. Reproductive functions of the ageing male.Hum Reprod Update 2004;10:327–39.
5. Rolf C, Nieschlag E. Reproductive functions, fertility and genetic risksof ageing men. Exp Clin Endocrinol Diabetes 2001;109:68–74.
6. Hook EB, Schreinemachers DM, Willey AM, Cross PK. Rates ofmutant structural chromosome rearrangements in human fetuses: datafrom prenatal cytogenetic studies and associations with maternal ageand parental mutagen exposure. Am J Hum Genet 1983;35:96–109.
7. Hecht F, Hecht BK. Aneuploidy in humans: dimensions, demography,and dangers of abnormal numbers of chromosomes. In: Vig BK, Sand-berg AA, eds. Aneuploidy part II: incidence and etiology. New York:Alan R. Liss, 1987:9–49.
8. Hassold T, Hunt PA, Sherman S. Trisomy in humans: incidence, originand etiology. Curr Opin Genet Dev 1993;3:398–403.
9. Wyrobek AJ, Aardema M, Eichenlaub-Ritter U, Ferguson L, Mar-chetti F. Mechanisms and targets involved in maternal and paternalage effects on numerical aneuploidy. Environ Mol Mutagen 1996;28:254 – 64.
0. Hassold T, Hunt P. To err (meiotically) is human: the genesis of humananeuploidy. Nat Rev Genet 2001;2:280–91.
1. Nicolaidis P, Petersen MB. Origin and mechanisms of non-disjunctionin human autosomal trisomies. Hum Reprod 1998;13:313–9.
2. de la Rochebrochard E, Thonneau P. Paternal age and maternal age arerisk factors for miscarriage: results of a multicentre European study.Hum Reprod 2002;17:1649–56.
3. Selvin S, Garfinkel J. Paternal age, maternal age and birth order and therisk of a fetal loss. Hum Biol 1976;48:223–30.
4. Lian ZH, Zack MM, Erickson JD. Paternal age and the occurrence ofbirth defects. Am J Hum Genet 1986;39:648–60.
5. Olshan AF. Lessons learned from epidemiologic studies of environ-mental exposure and genetic disease. Environ Mol Mutagen 1995;25(Suppl 26):74–80.
6. Tellier AL, Cormier-Daire V, Abadie V, Amiel J, Sigaudy S, Bonnet D,et al. CHARGE syndrome: report of 47 cases and review. Am J Med
Genet 1998;76:402–9.ertility and Sterility�
7. Bertram L, Busch R, Spiegl M, Lautenschlager NT, Muller U, Kurz A.Paternal age is a risk factor for Alzheimer disease in the absence of amajor gene. Neurogenetics 1998;1:277–80.
8. Risch N, Reich EW, Wishnick MM, McCarthy JG. Spontaneous mu-tation and parental age in humans. Am J Hum Genet 1987;41:218–48.
9. Zhang Y, Kreger BE, Dorgan JF, Cupples LA, Myers RH, SplanskyGL, et al. Parental age at child’s birth and son’s risk of prostate cancer.The Framingham Study. Am J Epidemiol 1999;150:1208–12.
0. Lucas JN, Deng W, Moore D, Hill F, Wade M, Lewis A, et al.Background ionizing radiation plays a minor role in the production ofchromosome translocations in a control population. Int J Radiat Biol1999;75:819–27.
1. Ramsey MJ, Moore DH Jr, Briner JF, Lee DA, Olsen L, Senft JR, et al.The effects of age and lifestyle factors on the accumulation of cytoge-netic damage as measured by chromosome painting. Mutat Res 1995;338:95–106.
2. Bolognesi C, Abbondandolo A, Barale R, Casalone R, Dalpra L, DeFerrari M, et al. Age-related increase of baseline frequencies ofsister chromatid exchanges, chromosome aberrations, and micronu-clei in human lymphocytes. Cancer Epidemiol Biomarkers Prev1997;6:249 –56.
3. Frenck RW Jr, Blackburn EH, Shannon KM. The rate of telomeresequence loss in human leukocytes varies with age. Proc Natl Acad SciUSA 1998;95:5607–10.
4. Lindsey J, McGill NI, Lindsey LA, Green DK, Cooke HJ. In vivo lossof telomeric repeats with age in humans. Mutat Res 1991;256:45–8.
5. Vaziri H, Dragowska W, Allsopp RC, Thomas TE, Harley CB, Lans-dorp PM. Evidence for a mitotic clock in human hematopoietic stemcells: loss of telomeric DNA with age. Proc Natl Acad Sci USA1994;91:9857–60.
6. Catalan J, Autio K, Kuosma E, Norppa H. Age-dependent inclusion ofsex chromosomes in lymphocyte micronuclei of man. Am J Hum Genet1998;63:1464–72.
7. Sloter E, Nath J, Eskenazi B, Wyrobek AJ. Effects of male age on thefrequencies of germinal and heritable chromosomal abnormalities inhumans and rodents. Fertil Steril 2004;81:925–43.
8. Rudak E, Jacobs PA, Yanagimachi R. Direct analysis of the chromo-some constitution of human spermatozoa. Nature 1978;274:911–3.
9. Brandriff BF, Gordon LA, Moore DI, Carrano AV. An analysis ofstructural aberrations in human sperm chromosomes. Cytogenet CellGenet 1988;47:29–36.
0. Martin RH, Rademaker AW. The effect of age on the frequency ofsperm chromosomal abnormalities in normal men. Am J Hum Genet1987;41:484–92.
1. Sartorelli EM, Mazzucatto LF, de Pina-Neto JM. Effect of paternal ageon human sperm chromosomes. Fertil Steril 2001;76:1119–23.
2. Sloter E, Lowe X, Moore DI, Nath J, Wyrobek AJ. Multicolor FISHanalysis of chromosomal breaks, duplications, deletions, and numericalabnormalities in the sperm of healthy men. Am J Hum Genet 2000;67:862–72.
3. Bosch M, Rajmil O, Egozcue J, Templado C. Linear increase ofstructural and numerical chromosome 9 abnormalities in human spermregarding age. Eur J Hum Genet 2003;11:754–9.
4. Marchetti F, Pearson FS, Bishop JB, Wyrobek AJ. Etoposide induceschromosomal abnormalities in mouse spermatocytes and stem cellspermatogonia. Hum Reprod 2006;21:888–95.
5. McInnes B, Rademaker A, Martin R. Donor age and the frequency ofdisomy for chromosomes 1, 13, 21 and structural abnormalities inhuman spermatozoa using multicolour fluorescence in-situ hybridiza-tion. Hum Reprod 1998;13:2489–94.
6. Van Hummelen P, Lowe XR, Wyrobek AJ. Simultaneous detection ofstructural and numerical chromosome abnormalities in sperm of healthymen by multicolor fluorescence in situ hybridization. Hum Genet 1996;98:608–15.
7. Eastmond DA, Rupa DS, Hasegawa LS. Detection of hyperdiploidy andchromosome breakage in interphase human lymphocytes following
exposure to the benzene metabolite hydroquinone using multicolor1085

4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
8
8
8
8
fluorescence in situ hybridization with DNA probes. Mutat Res1994;322:9–20.
8. Robbins WA, Meistrich ML, Moore D, Hagemeister FB, Weier HU,Cassel MJ, et al. Chemotherapy induces transient sex chromosomal andautosomal aneuploidy in human sperm. Nat Genet 1997;16:74–8.
9. Waye JS, Durfy SJ, Pinkel D, Kenwrick S, Patterson M, Davies KE, etal. Chromosome-specific alpha satellite DNA from human chromosome1: hierarchical structure and genomic organization of a polymorphicdomain spanning several hundred kilobase pairs of centromeric DNA.Genomics 1987;1:43–51.
0. Snedecor GW, Cochran WG. Statistical methods. 6th ed. Ames, IA:Iowa State University Press, 1967.
1. Diggle P, Heagerty P, Liang KY, Zeger S. Analysis of longitudinaldata. 2nd ed. New York: Oxford University Press, 2002.
2. Slavotinek A, Shaffer LG, Shapira SK. Monosomy 1p36. J Med Genet1999;36:657–63.
3. Shaffer LG, Heilstedt HA. Terminal deletion of 1p36. Lancet 2001;358(Suppl):S9.
4. Riegel M, Castellan C, Balmer D, Brecevic L, Schinzel A. Terminaldeletion, del(1)(p36.3), detected through screening for terminal dele-tions in patients with unclassified malformation syndromes. Am J MedGenet 1999;82:249–53.
5. Zenker M, Rittinger O, Grosse KP, Speicher MR, Kraus J, Rauch A, etal. Monosomy 1p36—a recently delineated, clinically recognizablesyndrome. Clin Dysmorphol 2002;11:43–8.
6. Heilstedt HA, Shapira SK, Gregg AR, Shaffer LG. Molecular andclinical characterization of a patient with duplication of 1p36.3 andmetopic synostosis. Clin Genet 1999;56:123–8.
7. Shi Q, Ko E, Barclay L, Hoang T, Rademaker A, Martin R. Cigarettesmoking and aneuploidy in human sperm. Mol Reprod Dev 2001;59:417–21.
8. Robbins WA, Vine MF, Truong KY, Everson RB. Use of fluorescencein situ hybridization (FISH) to assess effects of smoking, caffeine, andalcohol on aneuploidy load in sperm of healthy men. Environ MolMutagen 1997;30:175–83.
9. Baumgartner A, Schmid TE, Schuetz CG, Adler ID. Detection ofaneuploidy in rodent and human sperm by multicolor FISH afterchronic exposure to diazepam. Mutat Res 2001;490:11–9.
0. Van Hummelen P, Manchester D, Lowe X, Wyrobek AJ. Meioticsegregation, recombination, and gamete aneuploidy assessed in a t(1;10)(p22.1;q22.3) reciprocal translocation carrier by three- and four-probe multicolor FISH in sperm. Am J Hum Genet 1997;61:651–9.
1. Potocki L, Chen KS, Park SS, Osterholm DE, Withers MA, Kimonis V,et al. Molecular mechanism for duplication 17p11.2—the homologousrecombination reciprocal of the Smith-Magenis microdeletion. NatGenet 2000;24:84–7.
2. Mefford HC, Trask BJ. The complex structure and dynamic evolutionof human subtelomeres. Nat Rev Genet 2002;3:91–102.
3. Emanuel BS, Shaikh TH. Segmental duplications: an “expanding” rolein genomic instability and disease. Nat Rev Genet 2001;2:791–800.
4. Sutherland GR. Chromosomal fragile sites. Genet Anal Tech Appl1991;8:161–6.
5. Rupa DS, Hasegawa L, Eastomand DA. Detection of chromosomalbreakage in the 1 cen–1q12 region of interphase human lymphocytesusing multicolor fluorescence in situ hybridization with tandem DNAprobes. Cancer Res 1995;55:640–5.
6. Rupa DS, Hasegawa LS, Eastmond DA. Detection of chromosomalalterations affecting the 1cen–1q12 region in irradiated granulocytesand lymphocytes by multicolour FISH with tandem DNA probes.
Mutagenesis 1997;12:195–200.1086 Sloter et al. Age and chromosome aberrations in sperm
7. Rupa DS, Schuler M, Eastmond DA. Detection of hyperdiploidy andbreakage affecting the 1cen–1q12 region of cultured interphase humanlymphocytes treated with various genotoxic agents. Environ Mol Mu-tagen 1997;29:161–7.
8. Rupa DS, Eastmond DA. Chromosomal alterations affecting the 1cen–1q12 region in buccal mucosal cells of betel quid chewers detectedusing multicolor fluorescence in situ hybridization. Carcinogenesis1997;18:2347–51.
9. Dopp E, Schuler M, Schiffmann D, Eastmond DA. Induction of mi-cronuclei, hyperdiploidy and chromosomal breakage affecting the cen-tric/pericentric regions of chromosomes 1 and 9 in human amnioticfluid cells after treatment with asbestos and ceramic fibers. Mutat Res1997;377:77–87.
0. Parada LA, Limon J, Iliszko M, Czauderna P, Gisselsson D, HoglundM, et al. Cytogenetics of hepatoblastoma: further characterization of 1qrearrangements by fluorescence in situ hybridization: an internationalcollaborative study. Med Pediatr Oncol 2000;34:165–70.
1. Dopp E, Papp T, Schiffmann D. Detection of hyperdiploidy and chro-mosome breakage affecting the 1 (1cen–q12) region in lentigo malig-nant melanoma (LMM), superficial spreading melanoma (SSM) andcongenital nevus (CN) cells in vitro by the multicolor FISH technique.Cancer Lett 1997;120:157–63.
2. Brandriff B, Gordon L, Ashworth L, Watchmaker G, Carrano A,Wyrobek A. Chromosomal abnormalities in human sperm: comparisonsamong four healthy men. Hum Genet 1984;66:193–201.
3. Brandriff B, Gordon L, Ashworth L, Watchmaker G, Moore D, Wy-robek AJ, et al. Chromosomes of human sperm: variability amongnormal individuals. Hum Genet 1985;70:18–24.
4. Estop AM, Cieply K, Vankirk V, Munn S, Carver K. Cytogeneticstudies in human sperm. Hum Genet 1991;87:447–51.
5. Jenderny J, Jacobi M, Ruger A, Rohrborn G. Chromosome aberrationsin 450 sperm complements from eight controls and lack of increaseafter chemotherapy in two patients. Hum Genet 1992;90:151–4.
6. Marchetti F, Wyrobek AJ. Mechanisms and consequences of paternally-transmitted chromosomal abnormalities. Birth Defects Res C EmbryoToday 2005;75:112–29.
7. Wyrobek AJ, Eskenazi B, Young S, Arnheim N, Tiemann-Boege I, JabsEW, et al. Advancing age has differential effects on DNA damage,chromatin integrity, gene mutations, and aneuploidies in sperm. ProcNatl Acad Sci USA 2006;103:9601–6.
8. Buwe A, Guttenbach M, Schmid M. Effect of paternal age on thefrequency of cytogenetic abnormalities in human spermatozoa. Cyto-genet Genome Res 2005;111:213–28.
9. Shi Q, Martin RH. Aneuploidy in human sperm: a review of thefrequency and distribution of aneuploidy, effects of donor age andlifestyle factors. Cytogenet Cell Genet 2000;90:219–26.
0. Guttenbach M, Kohn FM, Engel W, Schmid M. Meiotic nondisjunctionof chromosomes 1, 17, 18, X, and Y in men more than 80 years of age.Biol Reprod 2000;63:1727–9.
1. Luetjens CM, Rolf C, Gassner P, Werny JE, Nieschlag E. Spermaneuploidy rates in younger and older men. Hum Reprod 2002;17:1826–32.
2. Wyrobek AJ, Marchetti F, Sloter E, Bishop J. Chromosomally defectivesperm and their developmental consequences. In: Anderson D, Kara-kaya AE, Sram RJ, eds. Human monitoring after environmental andoccupational exposure to chemical and physical agents. NATO scienceseries, series A, life sciences. Amsterdam: IOS Press, 2000:134–50.
3. Hecht F, Hecht B. Fragile sites and chromosome breakpoints in con-stitutional rearrangements II. Spontaneous abortions, stillbirths and
newborns. Clin Genet 1984;26:174–7.Vol. 87, No. 5, May 2007

Stmftgng
RS
T
R
0d
Prevalence of sexually transmissible pathogens insemen from asymptomatic male infertility patientswith and without leukocytospermiaGuntram Bezold, M.D.,a Joseph A. Politch, Ph.D.,a,b Nancy B. Kiviat, M.D.,c
Jane M. Kuypers, Ph.D.,c Hans Wolff, M.D.,d and Deborah J. Anderson, Ph.D.a,b
a Fearing Research Laboratory, Department of Obstetrics, Gynecology and Reproductive Biology, Brigham and Women’sHospital, Harvard Medical School, and b Department of Obstetrics and Gynecology, Boston University School of Medicine,Boston, Massachusetts; c Department of Pathology, University of Washington, Seattle, Washington; and d Department ofDermatology, Ludwig-Maximilians University of Munich, Munich, Germany
Objective: To determine the prevalence of pathogens that cause sexually transmitted infections (STIs) in semenfrom asymptomatic male infertility patients with and without leukocytospermia (LCS), and associations betweenSTIs, inflammatory markers, and other semen variables.Design: Retrospective, controlled study.Setting: Academic Medical Center.Patient(s): Two hundred and forty-one male infertility patients undergoing routine semen analysis: 132 with LCS,and 109 without LCS.Intervention(s): None.Main Outcome Measure(s): The DNA from STI pathogens (human papillomavirus [HPV], cytomegalovirus[CMV], herpes simplex virus [HSV], human herpesvirus type 6 [HHV-6], Epstein-Barr virus [EBV], hepatitis Bvirus [HBV], and Chlamydia trachomatis [CT]), routine semen parameters, and markers of accessory gland andepididymal function and inflammation.Result(s): The DNA from STI pathogens was detected in 45/241 (18.7%) of the samples (CMV, 8.7%; HPV,4.5%; HHV-6, 3.7%; HSV, 3.7%; CT, 2.5%; EBV, 0.4%; and HBV, 0%), with no difference in prevalencebetween the LCS and non-LCS groups. The DNA of STI pathogens in semen was associated with a decrease insperm concentration, motile sperm concentration, total sperm count, and neutral �-glucosidase concentration,whereas LCS was associated with a decrease in total sperm count, percent normal forms, and fructoseconcentration.Conclusion(s): The DNA of STI pathogens was detected in semen from a high percentage of asymptomatic maleinfertility patients, and was associated with poor semen quality. Efforts to diagnose and treat subclinicalgenital-tract infections should be intensified. (Fertil Steril� 2007;87:1087–97. ©2007 by American Society forReproductive Medicine.)
Key Words: Infection, virus, Chlamydia trachomatis, PCR, infertility, semen, leukocytospermia, cytokines
i(((1tt
pmstp2cr
exually transmitted infections (STIs) are of major concerno clinicians and researchers in the field of reproductiveedicine. Many STI pathogens cause incurable and often
atal diseases, and have been transmitted through insemina-ion procedures (1–3). Furthermore, several of these patho-ens can be transmitted from infected mothers to the fetus orewborn (2–5). Men can harbor subclinical infections in theenital tract over extended periods of time. Several viruses,
eceived April 27, 2006; revised and accepted August 8, 2006.upported by grants (R01AI35564 and P01AI46518) from the NationalInstitutes of Health, Bethesda, Maryland, and by a research fellowshipfrom the Deutsche Forschungsgemeinschaft, Bonn, Germany (to G.B.).
his work was performed at the Fearing Research Laboratory, Depart-ment of Obstetrics, Gynecology and Reproductive Biology, Brighamand Women’s Hospital, Harvard Medical School, Boston, Massa-chusetts.
eprint requests: Deborah J. Anderson, Ph.D., Department of Obstetricsand Gynecology, Boston University School of Medicine, 670 AlbanyStreet, Suite 516, Boston, Massachusetts 02118 (FAX: 617-414-8481;
gE-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.08.109 Copyright ©2007 American Soc
ncluding cytomegalovirus (CMV), Epstein-Barr virusEBV), human papillomavirus (HPV), hepatitis B virusHBV), hepatitis C virus (HCV), herpes simplex virus type 2HSV-2), human herpesvirus type 6 (HHV-6), and HIV type(HIV-1), as well as the intracellular bacterium Chlamydia
rachomatis (CT), have been detected in semen from asymp-omatic men (5–8).
Leukocytospermia (LCS), also known as leukospermia,yospermia, or pyosemia, is a term used to designate abnor-ally high concentrations of white blood cells (WBCs) in
emen (9), and was defined by the World Health Organiza-ion (WHO) as �106 WBCs per milliliter of semen (10). Therevalence of LCS in male infertility patients varies from%–40% in published reports (9, 11–13), and elevated con-entrations of WBCs in semen have been associated witheduced sperm function and quality (9, 13–23).
Although it is widely assumed that LCS is an indicator of
enital-tract infection, bacteria have been detected in only a1087Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

mtrsgpbcmsL
yaHMCawmo
loaawoaq
MPTosua(bwLwt
SScwaCmtu
Ssmenw–ae
DDpuz�cGgenrwiowact0r2awncpaaawcmt2
Dt(EBovkwb
inority of LCS samples (11, 24, 25). In addition, antibioticherapy for the treatment of LCS has produced conflictingesults (26–30). Thus, there has been little evidence for atrong relationship between bacterial infection in the maleenital tract and LCS (11). However, CT, an intracellulararasite which is the most prevalent sexually transmittedacterial pathogen in industrialized nations (31), was asso-iated with LCS. A recent study using nested plasmid poly-erase chain reaction (PCR) found both significantly higher
eminal WBC concentrations and a greater prevalence ofCS in men who were positive for DNA of CT (32).
Although viral STIs are also common and can persist forears, often without symptoms, they have not been system-tically studied as an etiologic factor in LCS. ElevatedIV-1 levels in semen were associated with LCS (33, 34).ore recently, Krause et al. (12) compared the prevalence ofMV, EBV, and HSV antibodies in the serum of men withnd without LCS. Herpes simplex virus IgM seropositivityas associated with LCS, but an additional smaller experi-ent by the investigators that used PCR to detect the DNA
f HSV in semen failed to identify any positive samples (12).
The purpose of our study was to use powerful new mo-ecular techniques to determine the prevalence and quantityf DNA from several common sexually transmitted virusesnd CT in semen from asymptomatic infertility patients withnd without LCS. In addition, we sought to determinehether the detection of pathogen DNA is associated withther measures of genital-tract inflammation, impairedccessory-gland or epididymal function, or reduced semenuality.
ATERIALS AND METHODSatientshis study was approved by the Institutional Review Boardf the Brigham and Women’s Hospital, Boston, Massachu-etts. Male infertility patients from couples undergoing eval-ation for infertility at the Center for Reproductive Medicinet Brigham and Women’s Hospital were screened for LCS�106 polymorphonuclear neutrophils [PMNs]/mL semen)y the Endtz assay (35). One hundred and thirty-two menith LCS and 109 patients with �106 PMNs/mL (“non-CS” group) were included in the study. None of the menas symptomatic for genital-tract infections or inflamma-
ion. Subjects ranged in age from 22–55 years.
emen Collection and Analysisemen samples were obtained by masturbation into sterileontainers after sexual abstinence of 48–72 hours. Samplesere subjected to semen analysis within 1 hour of collection,
nd processed for freezing within 2 hours of collection.oncentrations of sperm and sperm motility were deter-ined using a Hamilton-Thorne Motility Analyzer (Hamil-
on Thorne Biosciences, Inc., Beverly, MA). All settings
sed in this semen analysis were described previously (28). c1088 Bezold et al. Pathogens in semen from infertility patien
perm with a velocity of �10 �m per second were con-idered motile. Sperm morphology was assessed onethanol-fixed smears of fresh ejaculate stained with
osin and thiazine under a light microscope. Polymorpho-uclear neutrophils were counted after peroxidase stainingith Endtz reagent (35). Whole semen was stored frozen at70°C until used for DNA extraction and measurement ofccessory organ markers, interleukin (IL)-1�, and PMN-lastase.
etection of Pathogen DNA in SemenNA extraction All preparation work for the PCR assay waserformed in a “clean room” (no post-PCR DNA products)nder a laminar flow hood to minimize contamination. Fro-en semen samples were thawed and centrifuged at 2,000
g for 5 minutes. The seminal plasma was removed, and theell pellet was resuspended in 1 mL of Trizol (GIBCO BRL,aithersburg, MD). This extraction system is based on aciduanidinium isothiocyanate-phenol-chloroform (36), whichxtracts DNA from somatic “round” cells and pathogens, butot from the condensed nuclei of sperm (37). If the totalound-cell number in the pellet was �107, 1 mL of Trizolas used for any additional 107 round cells. Tubes were
ncubated at room temperature for 5 minutes. Then, 0.2 mLf chloroform per milliliter of Trizol was added. The tubesere mixed, incubated at room temperature for 3 minutes,
nd centrifuged at 4°C and 12,000 � g for 15 minutes. Afterentrifugation, the interphase layer containing the DNA, andhe lower phenol phase containing protein, were mixed with.3 mL of pure ethanol. After incubating for 3 minutes atoom temperature, the tubes were centrifuged at 4°C and,000 � g for 5 minutes. The supernatant containing phenolnd protein was removed, and the pellet was washed twiceith 1 mL of 100 mM sodium citrate containing 10% etha-ol, incubated at room temperature for 30 minutes, andentrifuged at 4°C and 2,000 � g for 5 minutes. Then theellet was washed once with 1 mL of 75% ethanol, incubatedt room temperature for 20 minutes, and centrifuged at 4°Cnd 2,000 � g for 5 minutes. The supernatant was removed,nd the pellet was air-dried and dissolved in sterile, distilledater. To remove all insoluble material, the solution was
entrifuged at room temperature and 12,000 � g for 10inutes. The supernatant was saved, and the DNA concen-
ration was determined by optical density (OD) reading at60 nm.
NA standards Cytomegalovirus DNA of known concentra-ion was obtained from the National Institutes of HealthBethesda, MD), and DNA of HSV-1, HSV-2, HHV-6, andBV of known concentration was obtained from Advancediotechnologies (Columbia, MD). Hepatitis B virus wasbtained from the American Type Culture Collection (Rock-ille, MD). As the HBV concentration in this sample was notnown, PCR of the HBV was performed, and the productas separated on a 2% agarose gel containing ethidiumromide and made visible under ultraviolet light. The spe-
ific HBV band was cut out, and the DNA was extractedts Vol. 87, No. 5, May 2007

umtfmpMT
SsCoHGsoq
wcct
dv
hdTa11cdsaTtaDPt
mat61s9ss
F
sing the Quiagen Gel Extraction Kit, a silicate-basedethod (Quiagen, Chatsworth, CA). The fragment concen-
ration was determined by OD reading at 260 nm. Theragment was used as the HBV standard. Chlamydia tracho-atis elementary bodies with known concentration wereurchased from Advanced Biotechnologies (Columbia,D). The DNA of the CT elementary bodies was
rizol-extracted.
emiquantitative PCR The PCR was performed as de-cribed by Saiki et al. (38). Oligonucleotide sequences forMV, HHV-6, HSV-1 and -2 (together), and EBV werebtained from the literature (39–43). The sequences forBV were obtained from Boehringer Mannheim (Penzberg,ermany). The oligonucleotides were synthesized by Geno-
ys (Woodlands, TX). Primers and a probe for �-actin werebtained from Genemed (South San Francisco, CA). Se-uences are given in Table 1.
Quantitation of the pre-PCR copy number was performedith the use of an external standard curve and internal
ontrols of similar size (mimics). Internal controls wereonstructed using the PCR-MIMIC-Construction Kit (Clon-ech, Palo Alto, CA).
During PCR, the synthesized fragments were labeled withigoxigenin (dig) with the use of dig-labeled nucleotides pro-ided in the PCR ELISA Dig Labeling Kit (Boehringer Mann-
TABLE 1Oligonucleotide sequences.
Name
Chlamydia, upstream CCTGTGChlamydia, downstream GTCGAAChlamydia, probe AAACCTTCMV, upstream CCGCAACMV, downstream CGTTTGGCMV, probe TTCTTCTHSV, upstream CATCACCHSV, downstream GGGCCAHSV, probe CTTTGTCHHV-6, upstream GTATCCCHHV-6, downstream TTAAACAHHV-6- probe GAGATTCEBV, upstream CCAGAGEBV, downstream GACCGGEBV, probe TTCTGCTActin, upstream ATGGATGActin, downstream CTAGAAGActin, probe GGCTGGMimic, probe CAATCAGNote: All probes were 5=-biotinylated. The oligonucleotide
(Mannheim, Germany).
Bezold. Pathogens in semen from infertility patients. Fertil Steril 2007.
ertility and Sterility�
eim, Indianapolis, IN), in which 5% of dTTP are labeled withig as dig-dUTP. The final PCR mixture contained 12.5 mMRIS, pH 8.3, 62.5 mM KCL, 200 �M each of dATP, dCTP,nd dGTP, 190 �M dTTP, 10 �M dig-dUTP, 2.5 mM MgCl2,�M of both primers, 200 DNA copies of internal controls, and.0 unit of Taq polymerase in a total of 40 �L. For a negativeontrol reference group, we used semen from 12 commercialonors who had tested negative for antibodies against CT inemen, for antibodies against HSV-1, HSV-2, CMV, HIV-1,nd HIV-2 in blood, and for HBV surface antigen in blood.hese specimens, provided as frozen aliquots, were a gift from
he New England Cryogenic Center (Boston, MA). Other neg-tive controls for the PCR assay were 0.4 �g of herring spermNA and sterile distilled water (reagent control). The �-actinCR was performed as a positive control to assure DNA quan-
ity and quality.
The PCR consisted of a first heating step (95°C for 5inutes), 37 amplification cycles, and a final extension step
t 72°C for 7.5 minutes. One amplification cycle consisted ofhese parameters: for CMV and CT, 95°C for 15 seconds and0°C for 60 seconds; for HSV-1 and -2 and HHV-6, 95°C for5 seconds and 55°C for 60 seconds; for EBV, 95°C for 15econds, 47°C for 30 seconds, and 72°C for 30 sec; for HBV,5°C for 15 seconds, 52°C for 30 seconds, and 72°C for 30econds; and for �-actin, 95°C for 15 seconds, 55°C for 30econds, and 72°C for 90 seconds.
Sequence (5=–3=)
A ATCCTGCTGA AA AAGTCWCCRT AGTAC AYAGAATTCC GTCGATCATA AGGCTTGGG GTGCCCATGGT GCGCAGCGGG
ACGCCAACGA CATCTACCGC ATCTTCGCCGC CCGGAGAGGG ACCG CTTGTTGGTG TA
ACCGCCGAAC TGAGCAGACA CCCGCGCGCGC GGCAGAGGTTC GTTGTCAGGGG AATCGAGCACA GTGGACTTC TTCTTAGGCCCAAC
G ATATCGCCGC GT TTGCGGTGGA CGATGGAGGG GCCG TTGAAGGTCT CAAACATGAT
C ACGAAACTTGences for HBV were obtained from Boehringer Mannheim
GGGAACCC
CCTGT
GGGGA
GGCTCGAGCTG
GTATGCAAGATCA
GGTCT
sequ
1089

totnhstrte4
PDu�mpsmw�waeaTcl
faotPT�hpwm
Coepmtttsthnse
Smtccu
Dcdpwwpnpc
Dpsp
DIpbCmtCTordpwn
Pems(p
F(wMe
Cdmi(
To decrease nonspecific amplification occurring duringhe first PCR cycle, a hot-start technique was used. A piecef wax (Ampliwax; Perkin-Elmer, Norwalk, CT) was addedo 13 �L of the initial PCR mix containing MgCl2, primers,ucleotides, and part of the buffer, and this solution waseated to melt the wax. After the wax had solidified, aecond mix (7 �L) containing Taq polymerase (Boehringer),he same amount of internal controls per tube, and theemaining amount of buffer was added, and finally 20 �L ofemplate DNA (standard). An external standard curve wasstablished from the DNA standards, ranging from–40,000 copies of the specific DNA per PCR tube.
olymerase chain reaction ELISA The PCR ELISA Digetection Kit (Boehringer) was used to quantify PCR prod-cts. Aliquots of the PCR products were denatured with 20L denaturation solution in a microcentrifuge tube. After 10inutes, 200 �L of the hybridization solution containing 7.5
mol of biotinylated probe per milliliter were added. Of thisolution, 200 �L were added to one well of an avidin-coatedicroplate and incubated at 55°C for 3 hours. Then the wellas washed five times with 375 �L washing buffer, and 200L of a 1:100-diluted, peroxidase-labeled, anti-dig-antibodyere added. The plate was incubated at 37°C for 30 minutes
nd washed five times, and 200 �L of 2,2=-azino-bis-(3-thylbenzothiazoline-6-sulfonic acid) (ABTS) solution weredded and incubated at room temperature for 10 minutes.he reaction was stopped by adding 100 �L of 1 M hydro-hloric acid. The OD was measured immediately, at a wave-ength of 405 nm.
For every external DNA standard and sample, three dif-erent aliquots were processed. For CMV, CT, EBV, HSV-1nd -2, and HBV, aliquots 1 and 2 contained 0.25 and 10 �Lf PCR product, respectively, and were hybridized with theemplate-specific probe. Aliquot 3, containing 1.0 �L ofCR product, was hybridized with the mimic-specific probe.he corresponding volumes for HHV-6 were 1, 20, and 10L. For detection of �-actin, 15 �L of PCR product wereybridized with the �-actin-specific probe. To increase theipetting accuracy of these small volumes, the PCR productas diluted appropriately with distilled water, so that ainimum volume of 5 �L was pipetted.
alculation Net ODs were calculated by subtracting the ODf the negative control DNA from the measured ODs of thexternal template standards, and from template and mimicroducts of experimental samples. Next, a template-OD:imic-OD ratio was obtained by dividing the net OD from
he well with aliquot 1 (low volume, hybridized with theemplate-specific probe) by the net OD from the well withhe corresponding aliquot 3 (hybridized with the mimic-pecific probe). An additional ratio was obtained by dividinghe net OD from the well with aliquot 2 (high volume,ybridized with the template-specific probe) by the mimicet OD; this second value was utilized to improve theensitivity of the PCR method and quantification in the lower
nd of the range. a1090 Bezold et al. Pathogens in semen from infertility patien
tandard curve and quantification of samples The template:imic ratios of the standards were plotted against the log of
he known template copy number. The number of pre-PCRopies in experimental samples could be determined byalculating the template:mimic ratio, and comparing to val-es on the standard curve.
efinition of negative and positive samples As the coeffi-ient of variation of 10 negative controls was 10%, and hugeifferences were observed between negative and low-ositive samples, a signal was considered positive if the ODas at least twice the OD of the negative control. A sampleas considered negative when the OD signal for the tem-late was below the threshold, and there were positive sig-als for the mimics and �-actin. A sample was consideredositive if it had a positive template signal (with the negativeontrol being negative).
etection of HPV Human papillomavirus was detected by arimer screening method (filter paper blot), followed byubtype analysis by restriction fragment length polymor-hism (RFLP), as previously described (44).
etermination of IL-1� and Biochemical Markersnterleukin-1� Interleukin-1�, a proinflammatory cytokinerimarily secreted by macrophages and epithelial cells, haseen associated with LCS, accessory-gland inflammation,T infection, and decreased sperm parameters (45–49). Weeasured concentrations of IL-1� in seminal plasma with
he use of a commercially available ELISA kit (Genzyme,ambridge, MA), following the manufacturer’s protocol.en microliters of seminal plasma were diluted with 90 �Lf the provided sample diluent. Two standard curves wereun: [1] the usual IL-1� standards diluted in provided sampleiluent, and [2] the same IL-1� standards diluted in seminallasma from a healthy non-LCS man. The standard curvesere always the same, indicating that seminal plasma doesot interfere with IL-1� detection in this assay system.
MN-elastase Polymorphonuclear neutrophil-elastase, annzyme secreted by activated PMNs (50) and a marker forale genital tract inflammation (51, 52), was measured in
eminal plasma with the use of a commercial ELISA kitPMN-Elastase ELISA; Merck, Darmstadt, Germany), asreviously described (49).
ructose Fructose, a marker for seminal-vesicle function10), was determined according to the WHO manual (10),ith the use of a modified hexokinase method (Boehringerannheim, Indianapolis, IN). Fructose levels �13 �mol per
jaculate (2.34 mg/ejaculate) are considered normal (10).
itrate Citrate, a marker for prostatic function (53), wasetermined according to the ultraviolet method recom-ended by WHO (53) using a commercial test kit (Boehr-
nger Mannheim, Indianapolis, IN). According to WHO53), citrate levels �52 �mol per ejaculate (9 mg/ejaculate)
re considered normal.ts Vol. 87, No. 5, May 2007

NempppssKs32mtstdsbu
SFu
pbScctKoapssFuaaMw
RAsgs
F
eutral �-glucosidase Neutral �-glucosidase, a marker forpididymal function (10, 54), was determined according to theethod of Chapdelaine et al. (55), using the principle of a
rotocol developed by Cooper et al. (54). To facilitate therocessing of a large number of samples, the whole assay waserformed in uncoated microtiter plates. Eight microliters ofeminal plasma and 100 �L p-nitrophenyl-glucopyranosideolution (5 mg/mL in potassium phosphate buffer [KH2PO4/
2HPO4], 100 mM, pH 6.8, containing 1% sodium dodecylulfate) were incubated in the wells of a microtiter plate at7°C for 1 hour as triplicates. The reaction was stopped by00 �L sodium carbonate solution (0.5 M), and ODs wereeasured in a microtiter plate reader at 405 nm. The OD of
he blank (8 �L of a seminal plasma pool, 4 �L castano-permine 10 mM, and 100 �L substrate solution) was sub-racted. Glucosidase activity (mU/mL) was calculated byividing the sample OD by the slope of a p-nitrophenoltandard curve (expressed as OD per �M) and multiplyingy 0.6417. Neutral �-glucosidase levels �20 mU per ejac-late are considered normal (10).
tatistical Analysisor continuous data, nonparametric statistical tests weretilized, or data were logarithmically transformed prior to
TABLE 2Pathogen prevalence and amount in semen sam
Pathogen LCS
Any pathogenPrevalence 25/132 (18.9)
HPVPrevalence 3/70 (4.3)
C. trachomatisPrevalence 3/132 (2.3)Range 10,000–460,000
CMVPrevalence 14/132 (10.6)Range 110–580,000
HSV-1 and HSV-2Prevalence 4/132 (3.0)Range 510–15,000
HHV-6Prevalence 5/132 (3.8)Range 250–81,000,000
EBVPrevalence 1/132 (0.8)Range 210
HBVPrevalence 0/132 (0)
Note: LCS � leukocytospermic (�106 PMN/mL); Non-LCparenthesized values � number of positive samples/tocopy number per ejaculate.
Bezold. Pathogens in semen from infertility patients. Fertil Steril 2007.
ertility and Sterility�
arametric analysis when the assumptions of normal distri-ution and/or homogeneity of variance were not fulfilled.pecifically, the Mann-Whitney U test was used for theomparison of two groups, and Spearman’s rank correlationoefficient was used to determine the correlation betweenwo variables. One-factor analysis of variance (ANOVA) orruskal-Wallis one-way ANOVA was used for comparisonsf �2 groups. Two-factor ANOVA was performed to ex-mine the two independent variables, LCS (�/�) and STIathogen DNA detection (�/�). Fisher’s protected leastignificant difference (PLSD) or Dunn’s multiple-compari-on tests were utilized for post hoc pairwise comparisons.isher’s exact test and the Fisher-Freeman-Halton test weretilized for analysis of categorical variables. Data were an-lyzed by StatView (version 5.0.1; SAS Institute, Cary, NC)nd StatXact (version 6; Cytel Software Corp., Cambridge,A) statistical software. In all cases, statistical significanceas assumed when P�.05.
ESULTSs shown in Table 2, the overall prevalence of STI DNA in
emen of infertility patients was 18.7%. LCS and non-LCSroups had similar STI DNA detection rates (18.9% for LCSamples and 18.3% for non-LCS samples, P�.10, Fisher’s
.
Non-LCS Total
20/109 (18.3) 45/241 (18.7)
5/109 (4.6) 8/179 (4.5)
3/108 (2.8) 6/240 (2.5)8,300–590,000 8,300–590,000
7/109 (6.4) 21/241 (8.7)3,200–12,000,000 110–12,000,000
5/109 (4.6) 9/241 (3.7)300–22,000 300–22,000
4/109 (3.7) 9/241 (3.7)4,400–1,500,000 250–81,000,000
0/108 (0) 1/240 (0.4)210
0/109 (0) 0/241 (0)nonleukocytospermic. Values with virgules followed by
umber (percentage) of analyzed samples. Range � DNA
ples
S �tal n
1091

egHwtsstspgOfwff
aCHfpepsl
evps�Spitnv(cLaMc
paH[[wgnWi
[gMtc[gMcs[gTww(vP
d[[P�aUH[1msr
mav
mttPPt(c
mPPP�i
xact test). Cytomegalovirus was the most prevalent patho-en detected (8.7%), followed by HPV (4.5%), HSV (3.7%),HV-6 (3.7%), and CT (2.5%). Epstein-Barr virus DNAas detected in only one sample; HBV DNA was not de-
ected in any semen sample. Human papillomavirus wasubtyped with an RFLP panel that differentiated 18 HPVubtypes: three HPV-positive samples were HPV-16, a sub-ype associated with cervical cancer; the remaining fiveamples were indeterminate. Eight of the 45 pathogen-ositive samples contained DNA from more than one patho-en (four in the LCS group, and four in the non-LCS group).ne of these samples, from the LCS group, was positive
or three pathogens; the other seven coinfected samplesere positive for two pathogens. Five of the eight coin-
ected samples were positive for HPV, four were positiveor CMV, and four contained CT.
The copy numbers of pathogen DNA per ejaculate showedlarge range (Table 2). Overall, DNA copy numbers of
MV ranged from 110–12,000,000 copies per ejaculate; ofSV, from 300–22,000 copies per ejaculate; and of HHV-6,
rom 250–81,000,000 copies per ejaculate. The only EBV-ositive sample contained 210 copies. None of the 12 refer-nce semen samples from seronegative sperm donors wereositive for STI pathogens with the exception of one, aample from a CMV-seronegative donor, which contained aow amount (950 copies) of CMV DNA.
Table 3 shows the results of two-factor ANOVAs thatxamined both LCS and STI pathogen DNA as independentariables. Samples with detectable DNA for any of the STIathogens (n � 45) had a significantly decreased motileperm concentration, total motile sperm count, and neutral-glucosidase concentration (P�.05 for all variables).perm concentration was also reduced in STI pathogen-ositive samples, but this effect was not statistically signif-cant (P�.10). Leukocytospermia was associated with a sta-istically significant decrease in total sperm count, percentormal forms, and fructose concentration (P�.05 for allariables). As expected, the three inflammation variablesPMN concentration, PMN elastase concentration, and IL-�oncentration) in semen were significantly elevated in theCS groups (P�.0001 for all variables). A significant inter-ction between LCS and STI was revealed for motility.otility in the LCS�/STI� group was significantly de-
reased in comparison to the other groups (P�.05).
When individual STI pathogens were analyzed, most of theathogens were associated with reduced sperm concentration,lthough this decrease was only statistically significant for theSV� group (HSV� group � 34.0 [7.0–109.0], median
range] � 106/mL, versus the no-pathogen group � 77.00–379.0], P�0.05, Mann-Whitney U test). Sperm motilityas also significantly reduced in the HSV� group (HSV�roup � 39.0 [7.0–73.0], median [range] percent, versus theo-pathogen group � 58.0 [2.0 –97.0], P�.05, Mann-hitney U test). Paradoxically, motility was significantly
ncreased in the HHV6� group (HHV6� group � 79.0 v
1092 Bezold et al. Pathogens in semen from infertility patien
50.0–97.0], median [range] percent, versus the no-pathogenroup � 58.0 [2.0–97.0], P�.01, Mann-Whitney U test).ost of the pathogens were also associated with reduced
otal sperm counts, although this decrease was only statisti-ally significant for the HPV� group (HPV� group � 139.313.0–214.5], median (range) � 106, versus the no-pathogenroup � 171.8 [0–1,340.0], P�.05, Mann-Whitney U test).ost pathogens were associated with reduced motile sperm
oncentrations, although this decrease was only statisticallyignificant for the HSV� group (HSV� group � 22.20.6–43.7], median [range] � 106/mL, versus the no-pathogenroup � 47.3 [0.2–306.2], P�.05, Mann-Whitney U test).otal motile sperm count was also reduced in samplesith DNA for most of the pathogens, although this decreaseas only statistically significant for the HSV� group
HSV� group � 29.8 [0.9–153.1], median [range] � 106,ersus the no-pathogen group � 108.0 [0.6–1,165.8],�.05, Mann-Whitney U test).
Neutral �-glucosidase concentration was significantly re-uced in CT� and HSV� samples (CT� group � 9.21.7–28.5], median (range) mU/mL, HSV� group � 7.21.7–44.9], versus the no-pathogen group � 16.7 [1.2–86.6],�.05, Mann-Whitney U test). Similar reductions in neutral-glucosidase concentration for CMV� and HPV� samplespproached statistical significance (P�.10, Mann-Whitney
test). Citrate concentration was significantly reduced inSV� samples (HSV� group � 2.8 [1.4–5.3], median
range] mg/mL, versus the no-pathogen group � 3.8 [0.8–5.3], P�.05, Mann-Whitney U test). Mean values for theale sex accessory-gland and epididymal markers in semen
amples without any detectable pathogens exceeded theirespective WHO reference values (10, 53).
Coinfection with STIs (samples containing DNA fromore than one pathogen) and STI copy number were not
ssociated with a further alteration in any of the semenariables (all P�.10, one-factor ANOVA).
Concentrations of accessory-gland and epididymal functionarkers that were significantly correlated with semen parame-
ers by Spearman’s rank correlation coefficients included: neu-ral �-glucosidase with sperm concentration (rho � �0.53,�.0001), motile sperm concentration (rho � �0.46,�.0001), total motile sperm (rho � �0.34, P�.0001), and
otal sperm count (rho � �0.35, P�.0001). Also, citratemg/ejaculate) was significantly correlated with total spermount (rho � �0.29, P�.0001).
By Spearman’s rank correlation coefficients, all three inflam-ation variables were significantly correlated with one another:MN-elastase and PMN concentration (rho � �0.78,�.0001), IL-1� and PMN concentration (rho � �0.71,�.0001), and IL-1� and PMN-elastase concentration (rho�0.73, P�.0001). Detection of STI DNA and markers of
nflammation were not associated with differences in semen
olume or patient age.ts Vol. 87, No. 5, May 2007

TABLE 3Semen parameters in infertility patients with LCS and/or STI pathogens in semen.
Semen variableLCS�/STI�
(N � 89)LCS�/STI�
(N � 20)LCS�/STI�(N � 107)
LCS�/STI�(N � 25) Significance
Sperm/mL � 106 107.0 (1.0–363.0) 73.5 (3.0–314.0) 64.0 (0–379.0) 34 (1.0–261.0) STI2a
Motility (%) 59.0 (8.0–90.0) 39.5 (5.0–88.0) 54.0 (2.0–97.0) 53.0 (16.0–97.0) STI � LCSb
Total sperm � 106 236.0 (2.5–1,340.0) 253.5 (9.8–519.2) 162.0 (0–1,124.5) 85.0 (4.0–965.7) LCS2b
Motile sperm/mL � 106 66.9 (0.8–300.6) 36.0 (0.2–276.3) 40.3 (0.2–306.2) 20.0 (0.5–240.1) STI2b
Total motile sperm � 106 135.4 (2.1–1,165.8) 96.8 (0.6–442.1) 88.9 (0.6–787.2) 43.3 (1.8–888.4) STI2b
Percent normal forms 52.0 (7.0–90.0) 53.5 (22.0–96.0) 48.0 (3.0–76.0) 48.0 (10.0–74.0) LCS2b
PMN/mL � 106 0 (0–0.8) 0 (0–0.8) 2.0 (1.0–19.0) 1.6 (1.0–8.8) LCS1c
PMN-elastase (ng/mL) 195.0 (0–15,126.0) 175.5 (0–5,885.0) 3,515.0 (0–38,802.0) 3,246.0 (482.0–18,396.0) LCS1c
IL-1� (pg/mL) 30.0 (0–310.0) 40.0 (0–230.0) 203.0 (0–9,650.0) 130.0 (0–1,130.0) LCS1c
Neutral �-glucosidase (mU/mL) 16.4 (1.6–49.6) 10.9 (5.9–49.1) 16.8 (1.2–86.6) 12.5 (1.7–44.9) STI2b
Citrate (mg/mL) 4.3 (1.3–15.3) 3.6 (2.0–8.8) 3.5 (0.8–12.1) 3.5 (1.4–8.7) NSFructose (mg/mL) 2.2 (0.3–5.5) 2.3 (0.8–5.8) 2.1 (0.1–4.48) 1.9 (0.1–4.7) LCS2b
Note: LCS � leukocytospermic (�106 PMN/mL). STI � sexually transmissible pathogen detected in semen. NS � not significant. Values are median (range).Significance refers to F-test significance for main effects and interactions. Arrows in the significance column indicate whether an increase or decrease in theparticular semen variable is associated with STI detection or LCS.
a P�.10 (NS).b P�.05.c P�.0001.
Bezold. Pathogens in semen from infertility patients. Fertil Steril 2007.
1093Fertility
andSterility�

DTl(pgrflwbouHaot
awmwCsrCctotcCpdt
aiwdm(uastdc�wo(ismfq
npi
vt1cptidtHpaaspraim
aiCcrCitchiSdeii
cBs8sptoPis
o
ISCUSSIONhe importance of genital-tract microorganisms as an etio-
ogic factor in male infertility is still a controversial topic5, 11, 31). The purpose of this study was to determine therevalence of several common sexually transmitted patho-ens in healthy, male infertility patients, and study theirelationship to LCS and other markers of genital-tract in-ammation, and to semen-quality parameters. For this study,e chose six common STI viruses and one intracellularacterium that can chronically infect the male genital tract,ften without causing symptoms. Two other common, sex-ally transmitted pathogens were not included in the study:IV-1 was not studied because it is a retrovirus and requiresdifferent processing and assay system; and Neiserria gon-rrhea was not studied because its infection is usually symp-omatic in men.
Cytomegalovirus is a member of the herpesvirus family,nd can cause a variety of teratogenic effects in newborns, asell as a clinical illness in adults resembling infectiousononucleosis (56). Its presence and persistence in semenere reported previously (57–60). In the current study,MV was the most frequently detected pathogen in the
emen of infertility patients (8.7%), with copy numbersanging from 110–12,000,000. Detection of a low level ofMV DNA in semen from one of the CMV-seronegativeommercial sperm donors could reflect a recent infection inhis individual. We did not observe a significant associationf CMV DNA with semen parameters in this study, althoughhere was a trend for lower motile sperm and �-glucosidaseoncentrations in the CMV-infected group, indicating thatMV infection could have a modest effect on semen quality,erhaps by affecting epididymal function. Previous studiesid not show an association of CMV infection with a reduc-ion in semen parameters (7, 59).
Herpes simplex virus mainly affects epithelial surfaces,nd is a major cause of genital ulcers. Whereas primarynfection usually occurs through direct or indirect contactith herpetic lesions (61, 62), HSV-1 and HSV-2 wereetected in semen (7, 60, 63) and on sperm (64), and trans-ission of HSV-2 has occurred through donor insemination
2). The detection rate of HSV-1 and HSV-2 DNA in ejac-lates from infertility patients in the current study was rel-tively low (3.7%). However, HSV was associated with thetrongest effect of any of the pathogens on semen parame-ers. The HSV DNA-positive samples had significantly re-uced sperm concentration, sperm motility, motile spermoncentration, total motile sperm count, and neutral-glucosidase and citrate concentrations. This is consistentith earlier studies that found associations between HSV-1r HSV-2 in semen and low sperm count and poor motility7, 64), as well as infertility (65). Antiviral treatment of malenfertility patients positive for HSV in semen resulted inuccessful pregnancies (64, 65). Thus, HSV infection of theale genital tract could explain some cases of male in-
ertility, because of its association with decreased semen
uality. Our study showed decreased concentrations of c1094 Bezold et al. Pathogens in semen from infertility patien
eutral �-glucosidase and citrate in HSV-positive sam-les, suggesting that the effect on fertility may be due tompaired epididymal and prostate function.
Human papillomaviruses represent a group of small DNAiruses that induce epithelial-cell proliferation. More than 35ypes of HPV infect the genital tract. The DNA from HPVs6, 18, 31, and 45 were associated with invasive squamous-ell cancers of the genital tract and anus (66, 67). Humanapillomavirus is primarily transmitted through direct epi-helial contact (62), but high-risk HPV types were detectedn both semen and spermatozoa (68–71), as well as in the vaseferens (72). In the current report, 3 out of the 8 cases thatested positive for DNA of generic HPV were subtyped asPV-16 (the other five cases were indeterminate). Humanapillomavirus DNA was not associated with LCS, but wasssociated with a significant decrease in total sperm count,nd a statistically nonsignificant trend for lower total motileperm count and neutral �-glucosidase concentrations. Arevious study reported an association between HPV andeduced sperm motility (70), while another study did not findny affects on sperm quality (71). Thus, additional researchs needed to determine whether HPV infection contributes toale infertility.
Chlamydia trachomatis infects the genital tract and eye,nd was associated with conjunctivitis and pneumonia innfants infected via the birth canal (73, 74). Our study foundT DNA in semen from 2.5% of infertility patients, withopy numbers ranging from 8,300–590,000. This prevalenceate is consistent with that in earlier publications (32, 75, 76).hlamydia trachomatis DNA was associated with a signif-
cant decrease in neutral �-glucosidase concentration (and arend toward lower total sperm and total motile spermounts). Other studies showed that men with CT in semenave reduced sperm concentration, motility, velocity, viabil-ty, morphology, acrosome reaction, and citrate (77–80).permatozoa incubated with elementary bodies of CT hadecreased motility and increased cytotoxicity (81). Theseffects were attributed to lipopolysaccharide (82). Thus, CTnfection of the male genital tract may contribute to malenfertility.
Epstein-Barr virus, a member of the herpesvirus family,auses infectious mononucleosis, and was associated withurkitt’s lymphoma (83). Epstein-Barr virus is found in
emen (7, 60), and is thought to be sexually transmitted (84,5). In the current study, EBV was detected in only oneample. The low detection rate probably reflects the lowrevalence of EBV infection in this country, and the fact thathe virus’ primary host cell, the B-lymphocyte, representsnly a small minority of all WBCs in semen (11, 86).revious studies reported a higher prevalence of EBV in
nfertility patients in Europe, although no association ofeminal EBV with reduced semen quality was found (7, 60).
Hepatitis B virus is the cause of hepatitis B, an infectionf the liver that often progresses to a chronic inflammatory
ondition associated with liver-cell carcinoma (87). Hepatitists Vol. 87, No. 5, May 2007

BaaNeuHfciipi
paeEydhpHhds
snasm�pcscctS4
l1rl(lariom
b
atfamagtttgoe
tttmspichs
AMmiSpM
R
F
virus is transmitted through infected bodily fluids suchs blood and semen (87, 88), and was transmitted byrtificial insemination (3). Because HBV is not endemic inorth America, and infertility patients as a group do not
ngage in high-risk behaviors such as intravenous drugse, a low prevalence of HBV was expected. Indeed, theBV DNA was not detected in any of the semen samples
rom our study. These data suggest that HBV does notontribute substantially to male infertility in North Amer-ca, except perhaps in high-risk groups. However, HBVnfection is endemic in other areas of the world, and itsotential contribution to male infertility should be studiedn these regions.
Human herpesvirus type 6, another member of the her-esvirus family, was detected in semen (60), and is causallyssociated with exanthema subitum (89), acute febrile dis-ases, and seizures in young children (90, 91), and withBV-negative and CMV-negative cases of mononucleosis inoung adults (92, 93). In this study, HHV-6 DNA wasetected in 3.8% of semen samples, and often occurred inigh copy numbers (up to 81,000,000). None of the semenarameters measured in our study was adversely affected byHV-6 infection; in fact, sperm motility was paradoxicallyigher in HHV-6-positive samples. Therefore, our data in-icate that genital-tract HHV-6 infection does not contributeignificantly to male infertility.
Overall, STI DNA was detected in 45/241 (18.7%) of theamples, with no difference in prevalence between LCS andon-LCS groups. STI DNA and LCS were independentlyssociated with poor semen parameters. STI DNA was as-ociated with a significant decrease in sperm concentration,otile sperm concentration, total sperm count, and neutral-glucosidase concentration. Eight of the STI-positive sam-les contained DNA from more than one pathogen, but STIoinfection was not associated with a further reduction inemen quality. Leukocytospermia was associated with de-reased sperm count, percent normal forms, and fructoseoncentration, a measure of seminal-vesicle function. Thus,he present study confirms and extends earlier reports thatTIs and LCS are associated with poor semen quality (7, 13,5, 48, 49, 51, 64, 65, 70, 77–82).
Leukocytospermia was strongly associated with elevatedevels of the inflammatory markers, PMN-elastase and IL-�, a proinflammatory cytokine produced by activated mac-ophages, epithelial cells, and other cell types (94). Simi-arly, concentrations of all three markers of inflammationPMNs, PMN-elastase, and IL-1�) were significantly corre-ated with one another, which was expected, as both PMNsnd macrophages are important participants in inflammatoryesponses, and because numbers of PMNs and macrophagesn semen are highly correlated (9, 45, 48, 49, 86). The DNAf STIs was not associated with elevations in any of thesearkers of inflammation .
The present study also revealed significant correlations
etween semen parameters and levels of accessory-glandertility and Sterility�
nd epididymal function markers, which highlights the rela-ionship between semen quality and normal genital-tractunction (10, 53, 95). Leukocytospermia was associated with
reduction in fructose concentration, suggesting that LCSay affect seminal-vesicle function. Pathogen DNA was
ssociated with reduced levels of neutral �-glucosidase, sug-esting that subclinical infections affect epididymal func-ion. In the case of one pathogen, HSV, citrate concentra-ions were also significantly reduced, suggesting an effect ofhis pathogenic virus on prostate function. Of all the patho-ens studied, HSV was associated with the strongest effectsn both semen quality and levels of accessory-gland andpididymal function markers.
In conclusion, using sensitive molecular assays, we de-ected an unexpectedly high prevalence of sexually transmit-ed pathogens in semen from asymptomatic infertility pa-ients. Pathogen DNA was not associated with LCS or otherarkers of inflammation, but was associated with decreased
emen parameters and signs of reduced epididymal androstate function. These findings indicate that asymptomaticnfections of the male genital tract are common and mayontribute to male infertility. Because they also threaten theealth of partners and offspring, efforts to diagnose and treatubclinical genital-tract infections should be intensified.
cknowledgments: The authors thank Florina Haimovici, M.D., Chong Xu,.D., and Samuel Mok, Ph.D., for helpful advice and critical reading of theanuscript, Greg McGuinness, B.S., for technical counseling in establish-
ng the semiquantitative PCR assay, George Mutter, M.D., and Beverlyedensky, M.H.P, M.T.(A.S.C.P.) for providing the study materials, and theharmaceutical companies Merck (Darmstadt, Germany) and Boehringerannheim (Mannheim, Germany) for reagent support.
EFERENCES1. Wortley PM, Hammett TA, Fleming PL. Donor insemination and
human immunodeficiency virus transmission. Obstet Gynecol 1998;91:515–8.
2. Moore DE, Ashley RL, Zarutskie PW, Coombs RW, Soules MR, CoreyL. Transmission of genital herpes by donor insemination. J Am MedAssoc 1989;261:3441–3.
3. Berry WR, Gottesfeld RL, Alter HJ, Vierling JM. Transmission ofhepatitis B virus by artificial insemination. J Am Med Assoc 1987;257:1079–81.
4. Politch J, Anderson DJ. Use of assisted reproduction technology toprevent the transmission of HIV-1 in HIV-discordant couples desiringchildren. In: Arici A, ed. Immunology and allergy clinics of NorthAmerica, volume 22. Philadelphia: W.B. Saunders, 2002:663–79.
5. Dejucq N, Jegou B. Viruses in the mammalian male genital tract andtheir effects on the reproductive system. Microbiol Mol Biol Rev2001;65:208–31.
6. Pekler VA, Robbins WA, Nyamathi A, Yashina TL, Leak B, RobinsTA. Use of versant TMA and bDNA 3.0 assays to detect and quantifyhepatitis C virus in semen. J Clin Lab Anal 2003;17:264–70.
7. Kapranos N, Petrakou E, Anastasiadou C, Kotronias D. Detection ofherpes simplex virus, cytomegalovirus, and Epstein-Barr virus in thesemen of men attending an infertility clinic. Fertil Steril 2003;79(Suppl 3):1566–70.
8. Hamdad-Daoudi F, Petit J, Eb F. Assessment of Chlamydia trachomatisinfection in asymptomatic male partners of infertile couples. J MedMicrobiol 2004;53:985–90.
9. Anderson DJ, Politch JA. White blood cells in semen and their impact
on fertility. In: Centola GM, Ginsburg KA, eds. Evaluation and treat-1095

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
ment of the infertile male. Cambridge: Cambridge University Press,1996:263–76.
0. World Health Organization. WHO laboratory manual for the examina-tion of human semen and sperm-cervical interaction. 4th ed. Cam-bridge: Cambridge University Press, 1999.
1. Wolff H. The biologic significance of white blood cells in semen. FertilSteril 1995;63:1143–57.
2. Krause W, Herbstreit F, Slenzka W. Are viral infections the cause ofleukocytospermia? Andrologia 2002;34:87–90.
3. Wolff H, Politch JA, Martinez A, Haimovici F, Hill JA, Anderson DJ.Leukocytospermia is associated with poor semen quality. Fertil Steril1990;53:528–36.
4. Berger RE, Karp LE, Williamson RA, Koehler J, Moore DE, HolmesKK. The relationship of pyospermia and seminal fluid bacteriology tosperm function as reflected in the sperm penetration assay. Fertil Steril1982;37:557–64.
5. Chan PJ, Su BC, Tredway DR, Whitney EA, Pang SC, Corselli J, et al.White blood cells in semen affect hyperactivation but not sperm mem-brane integrity in the head and tail regions. Fertil Steril 1994;61:986–9.
6. Maruyama DK Jr, Hale RW, Rogers BJ. Effects of white blood cells onthe in vitro penetration of zona-free hamster eggs by human sperma-tozoa. J Androl 1985;6:127–35.
7. Cohen J, Edwards R, Fehilly C, Fishel S, Hewitt J, Purdy J, et al. Invitro fertilization: a treatment for male infertility. Fertil Steril 1985;43:422–32.
8. Talbert LM, Hammond MG, Halme J, O’Rand M, Fryer JG, EkstromRD. Semen parameters and fertilization of human oocytes in vitro: amultivariable analysis. Fertil Steril 1987;48:270–7.
9. Eggert-Kruse W, Bellmann A, Rohr G, Tilgen W, Runnebaum B. Differ-entiation of round cells in semen by means of monoclonal antibodies andrelationship with male fertility. Fertil Steril 1992;58:1046–55.
0. Gonzales GF, Kortebani G, Mazzolli AB. Leukocytospermia and func-tion of the seminal vesicles on seminal quality. Fertil Steril 1992;57:1058–65.
1. Omu AE, Al-Qattan F, Al-Abdul-Hadi FM, Fatinikun MT, FernandesS. Seminal immune response in infertile men with leukocytospermia:effect on antioxidant activity. Eur J Obstet Gynecol Reprod Biol 1999;86:195–202.
2. Vicino M, Loverro G, Simonetti S, Mei L, Selvaggi L. The correlationbetween idiopathic leukocytospermia, embryo quality and outcome inthe FIVET and ICSI procedures [in Italian]. Minerva Ginecol 1999;51:413–20.
3. Thomas J, Fishel SB, Hall JA, Green S, Newton TA, Thornton SJ.Increased polymorphonuclear granulocytes in seminal plasma in rela-tion to sperm morphology. Hum Reprod 1997;12:2418–21.
4. Cottell E, Harrison RF, McCaffrey M, Walsh T, Mallon E, Barry-Kinsella C. Are seminal fluid microorganisms of significance or merelycontaminants? Fertil Steril 2000;74:465–70.
5. Trum JW, Mol BW, Pannekoek Y, Spanjaard L, Wertheim P, BlekerOP, et al. Value of detecting leukocytospermia in the diagnosis ofgenital tract infection in subfertile men. Fertil Steril 1998;70:315–9.
6. Erel CT, Senturk LM, Demir F, Irez T, Ertungealp E. Antibiotic therapy inmen with leukocytospermia. Int J Fertil Womens Med 1997;42:206–10.
7. Branigan EF, Spadoni LR, Muller CH. Identification and treatment ofleukocytospermia in couples with unexplained infertility. J Reprod Med1995;40:625–9.
8. Yanushpolsky EH, Politch JA, Hill JA, Anderson DJ. Antibiotic ther-apy and leukocytospermia: a prospective, randomized, controlled study.Fertil Steril 1995;63:142–7.
9. Zorn B, Virant-Klun I, Meden-Vrtovec H. Semen granulocyte elastase:its relevance for the diagnosis and prognosis of silent genital tractinflammation. Hum Reprod 2000;15:1978–84.
0. Branigan EF, Muller CH. Efficacy of treatment and recurrence rate ofleukocytospermia in infertile men with prostatitis. Fertil Steril 1994;62:580–4.
1. Keck C, Gerber-Schafer C, Clad A, Wilhelm C, Breckwoldt M. Sem-inal tract infections: impact on male fertility and treatment options.
Hum Reprod Update 1998;4:891–903.1096 Bezold et al. Pathogens in semen from infertility patien
2. Hosseinzadeh S, Eley A, Pacey AA. Semen quality of men withasymptomatic chlamydial infection. J Androl 2004;25:104–9.
3. Anderson DJ, O’Brien TR, Politch JA, Martinez A, Seage GR III,Padian N, et al. Effects of disease stage and zidovudine therapy on thedetection of human immunodeficiency virus type 1 in semen. J Am MedAssoc 1992;267:2769–74.
4. Xu C, Politch JA, Tucker L, Mayer KH, Seage GR III, Anderson DJ.Factors associated with increased levels of human immunodeficiencyvirus type 1 DNA in semen. J Infect Dis 1997;176:941–7.
5. Politch JA, Wolff H, Hill JA, Anderson DJ. Comparison of methods toenumerate white blood cells in semen. Fertil Steril 1993;60:372–5.
6. Chomczynski P. A reagent for the single-step simultaneous isolation ofRNA, DNA and proteins from cell and tissue samples. Biotechniques1993;15:532–534, 536–7.
7. Giusti A, Baird M, Pasquale S, Balazs I, Glassberg J. Application ofdeoxyribonucleic acid (DNA) polymorphisms to the analysis of DNArecovered from sperm. J Forensic Sci 1986;31:409–17.
8. Saiki RK, Gelfand DH, Stoffel S, Scharf SJ, Higuchi R, Horn GT, et al.Primer-directed enzymatic amplification of DNA with a thermostableDNA polymerase. Science 1988;239:487–91.
9. Holland SM, Gaydos CA, Quinn TC. Detection and differentiation ofChlamydia trachomatis, Chlamydia psittaci, and Chlamydia pneu-moniae by DNA amplification. J Infect Dis 1990;162:984–7.
0. Saito I, Servenius B, Compton T, Fox RI. Detection of Epstein-Barrvirus DNA by polymerase chain reaction in blood and tissue biopsiesfrom patients with Sjogren’s syndrome. J Exp Med 1989;169:2191–8.
1. Shibata D, Martin WJ, Appleman MD, Causey DM, Leedom JM,Arnheim N. Detection of cytomegalovirus DNA in peripheral blood ofpatients infected with human immunodeficiency virus. J Infect Dis1988;158:1185–92.
2. Cao M, Xiao X, Egbert B, Darragh TM, Yen TS. Rapid detection ofcutaneous herpes simplex virus infection with the polymerase chainreaction. J Invest Dermatol 1989;92:391–2.
3. Cone RW, Huang ML, Ashley R, Corey L. Human herpesvirus 6 DNAin peripheral blood cells and saliva from immunocompetent individuals.J Clin Microbiol 1993;31:1262–7.
4. Kuypers JM, Critchlow CW, Gravitt PE, Vernon DA, Sayer JB, ManosMM, et al. Comparison of dot filter hybridization, Southern transferhybridization, and polymerase chain reaction amplification for diagno-sis of anal human papillomavirus infection. J Clin Microbiol 1993;31:1003–6.
5. Comhaire F, Bosmans E, Ombelet W, Punjabi U, Schoonjans F. Cyto-kines in semen of normal men and of patients with andrologicaldiseases. Am J Reprod Immunol 1994;31:99–103.
6. Dousset B, Hussenet F, Daudin M, Bujan L, Foliguet B, Nabet P.Seminal cytokine concentrations (IL-1beta, IL-2, IL-6, sR IL-2, sRIL-6), semen parameters and blood hormonal status in male infertility.Hum Reprod 1997;12:1476–9.
7. Gruschwitz MS, Brezinschek R, Brezinschek HP. Cytokine levels in theseminal plasma of infertile males. J Androl 1996;17:158–63.
8. Sanocka D, Jedrzejczak P, Szumala-Kaekol A, Fraczek M, Kurpisz M.Male genital tract inflammation: the role of selected interleukins inregulation of pro-oxidant and antioxidant enzymatic substances in sem-inal plasma. J Androl 2003;24:448–55.
9. Sanocka D, Fraczek M, Jedrzejczak P, Szumala-Kakol A, Kurpisz M.Male genital tract infection: an influence of leukocytes and bacteria onsemen. J Reprod Immunol 2004;62:111–24.
0. Fritz H, Jochum M, Duswald K-H, Dittmer H, Kortmann H, NeumannS. Granulocyte proteinases as mediators of unspecific proteolysis ininflammation: a review. In: Goldberg DM, Werner MM, eds. Selectedtopics in clinical enzymology. New York: deGruyter-Verlag, 1984:305–28.
1. Wolff H, Anderson DJ. Evaluation of granulocyte elastase as a seminalplasma marker for leukocytospermia. Fertil Steril 1988;50:129–32.
2. Jochum M, Pabst W, Schill WB. Granulocyte elastase as a sensitivediagnostic parameter of silent male genital tract inflammation. Andro-
logia 1986;18:413–9.ts Vol. 87, No. 5, May 2007
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
8
8
8
8
8
8
8
8
8
8
9
9
9
9
9
9
F
3. World Health Organization. Laboratory manual for the examination ofhuman semen and sperm-cervical mucus interaction. 3rd ed. New York:Cambridge University Press, 1992.
4. Cooper TG, Weidner W, Nieschlag E. The influence of inflammation ofthe human male genital tract on secretion of the seminal markersalpha-glucosidase, glycerophosphocholine, carnitine, fructose and citricacid. Int J Androl 1990;13:329–36.
5. Chapdelaine P, Tremblay RR, Dube JY. P-nitrophenol-alpha-D-glucopyranoside as substrate for measurement of maltase activity inhuman semen. Clin Chem 1978;24:208–11.
6. Drew WL, Bates MP. Cytomegalovirus infection. In: Holmes KK,Mardh P-A, Sparling PF, Lemon SM, Stamm WE, Piot P, et al., eds.Sexually transmitted diseases, 3rd ed. New York: McGraw-Hill, 1999:313–26.
7. Aynaud O, Poveda JD, Huynh B, Guillemotonia A, Barrasso R. Fre-quency of herpes simplex virus, cytomegalovirus and human papillo-mavirus DNA in semen. Int J STD AIDS 2002;13:547–50.
8. Lang DJ, Kummer JF, Hartley DP. Cytomegalovirus in semen. Persis-tence and demonstration in extracellular fluids. N Engl J Med 1974;291:121–3.
9. Yang YS, Ho HN, Chen HF, Chen SU, Shen CY, Chang SF, et al.Cytomegalovirus infection and viral shedding in the genital tract ofinfertile couples. J Med Virol 1995;45:179–82.
0. Bezold G, Schuster-Grusser A, Lange M, Gall H, Wolff H, Peter RU.Prevalence of human herpesvirus types 1–8 in the semen of infertilitypatients and correlation with semen parameters. Fertil Steril 2001;76:416–8.
1. Corey L, Wald A. Genital herpes. In: Holmes KK, Mardh P-A, SparlingPF, Lemon SM, Stamm WE, Piot P, et al., eds. Sexually transmitteddiseases, 3rd ed. New York: McGraw-Hill, 1999:285–312.
2. Elder K, Baker DJ, Ribes JA. Infections, infertility, and assisted repro-duction. Cambridge: Cambridge University Press, 2005.
3. el Borai N, Inoue M, Lefevre C, Naumova EN, Sato B, Yamamura M.Detection of herpes simplex DNA in semen and menstrual blood ofindividuals attending an infertility clinic. J Obstet Gynaecol Res 1997;23:17–24.
4. Kotronias D, Kapranos N. Detection of herpes simplex virus DNA inhuman spermatozoa by in situ hybridization technique. In Vivo 1998;12:391–4.
5. El Borai N, LeFevre C, Inoue M, Naumova EN, Sato K, Suzuki S, et al.Presence of HSV-1 DNA in semen and menstrual blood. J ReprodImmunol 1998;41:137–47.
6. Galloway DA. Biology of genital human papillomaviruses. In: HolmesKK, Mardh P-A, Sparling PF, Lemon SM, Stamm WE, Piot P, et al.,eds. Sexually transmitted diseases, 3rd ed. New York: McGraw-Hill,1999:335–46.
7. Koutsky LA, Kiviat NB. Genital human papillomavirus. In: HolmesKK, Mardh P-A, Sparling PF, Lemon SM, Stamm WE, Piot P, et al.,eds. Sexually transmitted diseases, 3rd ed. New York: McGraw-Hill,1999:347–59.
8. Kyo S, Inoue M, Koyama M, Fujita M, Tanizawa O, Hakura A.Detection of high-risk human papillomavirus in the cervix and semen ofsex partners. J Infect Dis 1994;170:682–5.
9. Lai YM, Yang FP, Pao CC. Human papillomavirus deoxyribonucleicacid and ribonucleic acid in seminal plasma and sperm cells. FertilSteril 1996;65:1026–30.
0. Lai YM, Lee JF, Huang HY, Soong YK, Yang FP, Pao CC. The effectof human papillomavirus infection on sperm cell motility. Fertil Steril1997;67:1152–5.
1. Rintala MA, Grenman SE, Pollanen PP, Suominen JJ, Syrjanen SM.Detection of high-risk HPV DNA in semen and its association with thequality of semen. Int J STD AIDS 2004;15:740–3.
2. Rintala MA, Pollanen PP, Nikkanen VP, Grenman SE, Syrjanen SM.Human papillomavirus DNA is found in the vas deferens. J Infect Dis2002;185:1664–7.
3. Stamm WE. Chlamydia trachomatis infections of the adult. In: Holmes
KK, Mardh P-A, Sparling PF, Lemon SM, Stamm WE, Piot P, et al.,ertility and Sterility�
eds. Sexually transmitted diseases, 3rd ed. New York: McGraw-Hill,1999:407–22.
4. Schacher J. Biology of Chlamydia trachomatis. In: Holmes KK, MardhP-A, Sparling PF, Lemon SM, Stamm WE, Piot P, et al., eds. Sexuallytransmitted diseases, 3rd ed. New York: McGraw-Hill, 1999:391–405.
5. Eggert-Kruse W, Rohr G, Kunt B, Meyer A, Wondra J, Strowitzki T, etal. Prevalence of Chlamydia trachomatis in subfertile couples. FertilSteril 2003;80:660–3.
6. Wolff H, Neubert U, Volkenandt M, Zochling N, Schlupen EM, Bezold G,et al. Detection of Chlamydia trachomatis in semen by antibody-enzymeimmunoassay compared with polymerase chain reaction, antigen-enzymeimmunoassay, and urethral cell culture. Fertil Steril 1994;62:1250–4.
7. Jungwirth A, Straberger A, Esterbauer B, Fink K, Schmeller N. Acro-some reaction in Chlamydia-positive and negative patients. Andrologia2003;35:314–6.
8. Veznik Z, Pospisil L, Svecova D, Zajicova A, Unzeitig V. Chlamydiaein the ejaculate: their influence on the quality and morphology of sperm.Acta Obstet Gynecol Scand 2004;83:656–660.
9. Cengiz T, Aydoganli L, Baykam M, Mungan NA, Tuncbilek E, et al.Chlamydial infections and male infertility. Int Urol Nephrol 1997;29:687–93.
0. Wolff H, Neubert U, Zebhauser M, Bezold G, Korting HC, Meurer M.Chlamydia trachomatis induces an inflammatory response in the malegenital tract and is associated with altered semen quality. Fertil Steril1991;55:1017–9.
1. Hosseinzadeh S, Brewis IA, Eley A, Pacey AA. Co-incubation ofhuman spermatozoa with Chlamydia trachomatis serovar E causespremature sperm death. Hum Reprod 2001;16:293–9.
2. Hosseinzadeh S, Pacey AA, Eley A. Chlamydia trachomatis-induceddeath of human spermatozoa is caused primarily by lipopolysaccharide.J Med Microbiol 2003;52:193–200.
3. Slobod KS, Sixbey JW. Epstein-Barr virus infection. In: Holmes KK,Mardh P-A, Sparling PF, Lemon SM, Stamm WE, Piot P, et al., eds.Sexually transmitted diseases, 3rd ed. New York: McGraw-Hill, 1999:327–33.
4. van Baarle D, Hovenkamp E, Dukers NH, Renwick N, Kersten MJ,Goudsmit J, et al. High prevalence of Epstein-Barr virus type 2 amonghomosexual men is caused by sexual transmission. J Infect Dis 2000;181:2045–9.
5. Crawford DH, Swerdlow AJ, Higgins C, McAulay K, Harrison N,Williams H, et al. Sexual history and Epstein-Barr virus infection.J Infect Dis 2002;186:731–6.
6. Wolff H, Anderson DJ. Immunohistologic characterization and quan-titation of leukocyte subpopulations in human semen. Fertil Steril1988;49:497–504.
7. Lemon SM, Alter MJ. Viral hepatitis. In: Holmes KK, Mardh P-A,Sparling PF, Lemon SM, Stamm WE, Piot P, et al., eds. Sexuallytransmitted diseases, 3rd ed. New York: McGraw-Hill, 1999:361–84.
8. Jenison SA, Lemon SM, Baker LN, Newbold JE. Quantitative analysisof hepatitis B virus DNA in saliva and semen of chronically infectedhomosexual men. J Infect Dis 1987;156:299–307.
9. Yamanishi K, Okuno T, Shiraki K, Takahashi M, Kondo T, Asano Y,et al. Identification of human herpesvirus-6 as a causal agent forexanthem subitum. Lancet 1988;1:1065–7.
0. Asano Y, Yoshikawa T. Human herpesvirus-6 and parvovirus B19infections in children. Curr Opin Pediatr 1993;5:14–20.
1. Hall CB, Long CE, Schnabel KC, Caserta MT, McIntyre KM, CostanzoMA, et al. Human herpesvirus-6 infection in children. A prospective studyof complications and reactivation. N Engl J Med 1994;331:432–8.
2. Krueger GR, Klueppelberg U, Hoffmann A, Ablashi DV. Clinical corre-lates of infection with human herpesvirus-6. In Vivo 1994;8:457–85.
3. Pellett PE, Black JB, Yamamoto M. Human herpesvirus 6: the virus andthe search for its role as a human pathogen. Adv Virus Res 1992;41:1–52.
4. Thomson AW, Lotze MT. The cytokine handbook. Boston: AcademicPress, 2003.
5. Grudzinskas JG, Yovich J. Gametes: the spermatozoon. New York:
Cambridge University Press, 1995.1097

Oitedroroait(
spu
RR
OVULATION INDUCTION
Early pregnancy loss in women stimulated withgonadotropin-releasing hormone antagonist protocolsaccording to oral contraceptive pill pretreatmentJosé Bellver, M.D., Carmen Albert, Ph.D., Elena Labarta, M.D., and Antonio Pellicer, M.D.
Instituto Valenciano de Infertilidad, Universidad de Valencia, Valencia, Spain
Objective: To evaluate and compare the risk of early pregnancy loss in patients stimulated with GnRH antagonistprotocols according to oral contraceptive pill (OCP) pretreatment.Design: Retrospective case–control study.Setting: Instituto Valenciano de Infertilidad. University of Valencia. Spain.Patient(s): One thousand five hundred thirty-nine patients, aged �36, stimulated with GnRH antagonists for IVFbetween January 1, 2000 and November 1, 2005.Intervention(s): Reproductive outcome was compared based on the application (or not) of OCP pretreatment: 944women were included in the OCP group and 595 in the non-OCP group. The Student’s t test was used forstatistics.Main Outcome Measure(s): Pregnancy, biochemical pregnancy, ectopic pregnancy, early clinical pregnancy loss,early pregnancy loss, and ongoing pregnancy rates.Result(s): No significant differences were observed in any of the outcome parameters. Early pregnancy loss rateswere similar: 23% in the OCP pretreatment group versus 19.2% in the non-OCP pretreatment group. However,longer periods of ovarian stimulation and higher doses of gonadotropins needed to be employed in the OCPgroup.Conclusion(s): There is not sufficient evidence to confirm OCP pretreatment as a risk factor for miscarriage inpatients stimulated with GnRH antagonist protocols. (Fertil Steril� 2007;87:1098–101. ©2007 by AmericanSociety for Reproductive Medicine.)
Key Words: GnRH antagonist, oral contraceptive pill, early pregnancy loss, ongoing pregnancy
ahonrIppci
of
MPTa(w
ral contraceptive pill (OCP) pretreatment is widely appliedn women undergoing ovarian stimulation with GnRH an-agonists for cycle scheduling purposes. OCP pretreatmentnables the clinician to initiate ovarian stimulation indepen-ently on the occurrence of spontaneous menstruation. Untilecently, this protocol was not thought to have any deleteri-us effect on pregnancy outcome (1–3). However, a recentandomized study of the effects of OCP pretreatment onngoing pregnancy rates in patients stimulated with GnRHntagonists and recombinant FSH for IVF showed a signif-cantly higher incidence of early pregnancy loss (36.4%) inhe pretreated group (n � 214) than in nonpretreated group21.6%, n � 211) (4).
Two previous randomized trials using OCP for cycleheduling in GnRH antagonist protocols had not shown aoorer reproductive outcome (1, 2). However, they did notse the same definition of early pregnancy loss as Kolibi-
eceived April 6, 2006; revised and accepted August 4, 2006.eprint requests: José Bellver, M.D., Instituto Valenciano de Infertilidad,Plaza de la Policía Local, 3, 46015, Valencia, Spain. (FAX: 34-96-
J3050999; E-mail: [email protected]).
1098 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
nakis et al. (4): proportion of patients with initially positiveCG in whom pregnancy failed to develop before 12 weeksf gestation. This definition also included biochemical preg-ancies. We have performed a retrospective study of theeproductive outcome of our GnRH antagonist cycles forVF in young women, both receiving and not receiving OCPretreatment. We have applied the same definition for earlyregnancy loss as Kolibianakis et al. (4), and we haveonsidered only young women to compare to previous stud-es (1, 2, 4).
The aim of the present study was to help to clarify whetherr not OCP pretreatment should be considered as a riskactor for miscarriage in GnRH antagonist protocols for IVF.
ATERIALS AND METHODSatientshis study was a retrospective analysis of all the GnRHntagonist cycles performed in our center in young women�35 years of age) undergoing IVF treatment (both with andithout intracytoplasmic sperm injection [ICSI]) between
anuary 1, 2000 and November 1, 2005. Most of our patients
0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.098

wsgawcianaR
PPeiIdosh
dapStpcotevGtSw�atl
omLSfr
sUswt
tpo
OBpgppssc1gtstiipti
SSaCada
RDocw
gud(
ohph
o(nr
F
ho go through a GnRH antagonist protocol for ovariantimulation receive OCP pretreatment to facilitate cycle pro-ramming. However, we use this protocol more frequently inged or low responder women. For the purpose of this study,e limited the collection of data to that of young patients, to
ompare results with those published in previous random-zed trials (1, 2, 4), in which the mean age of the subjects waslways under 35 years old. One thousand five hundred thirty-ine patients were included: 944 receiving OCP pretreatmentnd 595 not receiving OCP pretreatment. The Institutionaleview Board approval was obtained.
rotocolatients were pretreated with an OCP (0.25 mg of levonorg-strel plus 0.05 mg of ethinylestradiol; Neogynona, Scher-ng, Madrid, Spain) during the cycle prior to the scheduledVF/ICSI procedure. Ovarian stimulation was initiated 5ays after discontinuation of the pill in the OCP group andn cycle day 2 in the non-OCP group. All the patients weretimulated with recombinant FSH, both with or withoutMG/recombinant LH.
Recombinant FSH (Gonal-F, Serono Laboratories, Ma-rid, Spain; or Puregon, Organon, Barcelona, Spain) wasdministered with or without highly purified hMG (Meno-ur, Ferring, Madrid, Spain) or recombinant LH (Luveris,erono Laboratories). On days 1 and 2 of ovarian stimula-
ion, doses varied from 150 to 300 U/d depending on theatient’s age, body mass index, ovarian pattern, menstrualycles, basal hormones, and response to previous controlledvarian stimulations (if performed). From day 3 of stimula-ion, gonadotropin doses were adjusted according to serumstradiol levels and ovarian response, which was assessed byaginal ultrasound, every 2 days. A daily dose of 0.25 mg ofnRH antagonist (Cetrotide, Serono Laboratories) adminis-
ration was initiated on day 6 of stimulation. hCG (Ovitrelle,erono Laboratories) was administered subcutaneouslyhen at least two leading follicles reached a mean diameter18 mm. Daily administration of gonadotropins and GnRH
ntagonist was discontinued on the day of hCG administra-ion. Transvaginal oocyte retrieval was scheduled 36 hoursater.
Embryo transfer was performed 2, 3, 5, or 6 days afterocyte retrieval via the vaginal route. In our program, 400g/d of micronized intravaginal progesterone (Progeffik,aboratories Effik S.A., Madrid, Spain; or Utrogestan, SEID.A., Barcelona, Spain) were administered from the dayollowing oocyte pick up, and continued at least until theesult of the pregnancy test was obtained.
Fourteen to 16 days after oocyte retrieval a quantitativeerum value of �hCG was obtained, with a result of �10I/L being considered positive. When �hCG was positive, a
econd �hCG test and a primary transvaginal ultrasoundere performed 1 week later (21–23 days after oocyte re-
rieval). Scans were repeated weekly until the detection of n
ertility and Sterility�
he embryo’s heartbeat, and monthly thereafter. Micronizedrogesterone was continued at the same dosage until day 80f pregnancy.
utcome Measuresiochemical pregnancy was diagnosed when a previouslyositive pregnancy test became negative prior to ultrasono-raphic detection of an embryonic sac in the fifth week ofregnancy or later. Ectopic pregnancy was defined as aregnancy sited out of the endometrium, detected by ultra-ound or laparoscopy, or strongly suspected because ofymptoms and/or the �hCG serum curve of the patient. Earlylinical pregnancy loss was defined as a miscarriage up to2th week of gestation after ultrasonographic detection ofestational sac(s). Our definition of early pregnancy loss washat of Kolibianakis et al. (4): pregnancies diagnosed witherum-positive �HCG, failing to reach 12 weeks of gesta-ion. In this way, early pregnancy losses included biochem-cal pregnancies and early clinical pregnancy losses. Ongo-ng pregnancy rate per initiated cycle was defined as theercentage of pregnancies surpassing the 12th week of ges-ation in relation to the number of GnRH antagonist cyclesnitiated.
tatistical Analysistatistical analysis was performed using the Statistical Pack-ge for Social Science version 11.0 (SPSS Inc., Chicago, IL).ategoric data were expressed as number and percentage,nd numeric data as mean and standard deviation. The Stu-ent’s t test was used for statistics. Significance was assumedt P�.05.
ESULTSuring the study period, 1539 patients younger than 36 yearsld who had undergone an antagonist protocol were in-luded. Nine hundred forty-four of them were pretreatedith OCP (61.3%) and 595 (38.7%) were not.
There were no significant differences between the tworoups with respect to mean age at the initiation of stim-lation, number of patients achieving embryo transfer,ay of embryo transfer, or number of transferred embryosTable 1).
Women undergoing OCP pretreatment presented longervarian stimulations and needed higher doses of rFSH andMG (Table 1). One thousand two hundred eighty-fouratients (83.4%) were stimulated with rFSH plus rLH orMG.
No significant differences were observed in any of theutcome parameters. Early pregnancy loss rates were similar23.0% in the OCP pretreatment group vs. 19.2% in theon-OCP pretreatment group), even when they were sepa-ated into biochemical pregnancies and early clinical preg-
ancy losses. Similarly, no differences were detected in1099

pr
DGfwdGmib
tdmsnblppt
w
ptdhwoti(wOaOr
apt30sc1�
regnancy, ectopic pregnancy rates, or ongoing pregnancyate per initiated cycle (Table 1).
ISCUSSIONnRH antagonists are used in controlled ovarian stimulation
or the prevention of LH surge. Unlike GnRH agonists,hich supress gonadotropin secretion through receptorown-regulation and desensitization of the gonadotroph,nRH antagonists directly compete against the endogenousolecule for receptor binding (3). This allows for an almost
mmediate suppression of gonadotropin secretion, which cane quickly reversed (5).
Cycle programming has become more complicated withhe use of GnRH antagonists, as initiation of stimulation isependent on menstruation taking place (4). OCP pretreat-ent has been employed in these protocols for cycle
cheduling purposes, making easier the inititation of go-adotropins 3 to 5 days after pill discontinutation. Possi-le drawbacks of this procedure could be the need foronger ovarian stimulations and higher doses of gonadotro-ins, because of the contraceptive pill’s suppression of theituitary–ovarian axis, and its implications for the reproduc-ive outcome.
A recent randomized study by Kolibianakis et al. (4),
TABLE 1Reproductive outcome of patients <36 years oldgonadotropins for in vitro fertilization according
OCP g
Patient age 3ET n (%) 9Day of ET n (%)
Day 2 1Day 3 5Day 5/6 2
Transferred embryosDuration of stimulation (days) 1Dose of rFSH 236Dose of hMG 133Dose of rLH 85Pregnancy n (%) 4Biochemical pregnancy n (%)Ectopic pregnancy n (%)Early clinical pregnancy loss n (%)Early pregnancy loss n (%) 1Ongoing pregnancy rate per cycle started 3Note: Unless otherwise indicated, values are means � SDNS � not significant. ET � embryo transfer; early clinical p
ultrasonographic detection of gestational sac; Early prpregnancy losses.
Bellver. Oral contraceptive pill and miscarriage. Fertil Steril 2007.
hich assessed the effect of OCP pretreatment on ongoing r
1100 Bellver et al. Oral contraceptive pill and miscarriage
regnancy rates in IVF patients stimulated with GnRH an-agonists and rFSH, highlighted the two aforementionedownsides. On one hand, longer ovarian stimulations andigher doses of rFSH were necessary in the OCP group,hile a lower number of follicles of any size were recordedn day 6 of stimulation (slower follicular recruitment). Onhe other hand, early pregnancy loss was significantly highern the OCP group (36.4%) than in the non-OCP subjects21.6%). We also found that ovarian stimulation periodsere longer and doses of rFSH and hMG were higher in theCP group (Table 1). These results confirm those of Kolibi-
nakis et al. (4), and underline the shortcomings of the use ofCP pretreatment for cycle programming, especially in low
esponders.
However, the second finding of Kolibianakis et al. (4)bout the increase of early pregnancy losses in womenretreated with OCP is perplexing, and even more soaking into account that the mean age of their subjects was1 years of age (31.2 � 0.3 in the OCP group and 31.5 �.3 in the non-OCP group). Two previous randomizedtudies, in which OCP was used for GnRH antagonistycle scheduling (1, 2), detected lower miscarriage rates:3.3% (4 of 30) with rFSH and 14.7% (5 of 34) with rFSH
rLH in the first report (1); and 12.5% (2 of 16) with
ulated with GnRH antagonists andral contraceptive pill (OCP) pretreatment.
(n � 944) Non-OCP group (n � 595) P
0.1 31.7 � 0.1 NS95.9) 575 (96.6) NS
13.0) 72 (12.6) NS64.6) 386 (67.1) NS22.4) 117 (20.3) NS
0.0 1.9 � 0.0 NS0.1 9.8 � 0.1 �.00135.3 1866.0 � 36.6 �.00141.3 1049.4 � 41.9 �.0218.0 804.2 � 27.0 NS
51.4) 291 (50.6) NS15.1) 34 (11.7) NS4.3) 7 (2.4) NS8.0) 22 (7.6) NS23.0) 56 (19.2) NS35.8) 228 (38.3) NS
ancy loss: miscarriage up to 12 weeks of pregnancy afterncy loss � biochemical pregnancies plus early clinical
stimto o
roup
2.1 �05 (
17 (85 (03 (
1.8 �0.9 �1.5 �1.5 �1.2 �65 (70 (20 (37 (07 (38 (.
regnegna
FSH in the second (2).
Vol. 87, No. 5, May 2007

sec2rptbtn
tosatcfsLl
smrp(Lacj
crafiLsoacidw
oipDr
pfddrsectm
R
1
1
F
The study of Cedrin-Durnerin et al. (1) established theame cutoff point for miscarriage (12 weeks) as Kolibianakist al. (4). One of the said studies used a single dose ofetrorelix 3 mg (1) and the other, a daily dose of Ganirelix50 �g (2). In addition, like Kolibianakis et al. (4), botheports evaluated young women. However, biochemicalregnancies were probably not considered. Our study usedhe same criteria as Kolibianakis et al. (4) and includediochemical pregnancies, but we found no differences inerms of early pregnancy loss between the OCP and theon-OCP pretreatment groups (Table 1).
Both multiple-dose and single-dose protocols have provedo be effective in IVF/ICSI cycles (6). A “minimum thresh-ld” of LH secretion has to be maintained to ensure adequateteroidogenesis and folliculogenesis. Antagonists are usuallydministered when follicles become increasingly responsiveo LH because of acquisition of LH receptors on granulosaells and when LH may operate with FSH to achieve fullollicular maturity and oocyte competence (1, 7). As a con-equence, it may be assumed that the dramatic decrease inH secretion induced by GnRH antagonist administration is
ikely to be detrimental for the follicle–oocyte complex.
As the inhibitory effect of GnRH antagonists upon LHecretion has been shown to be dose dependent (8) and theeasurement of serum LH values is not valid for assesing
esidual LH bioactivity (9) or for defining a subgroup ofatients that may benefit from exogenous LH administration10), supplementation with exogenous LH (recombinant orH bioactivity as hMG) has been suggested as an alterativepproach to balance the possible LH depletion. In fact, in ourenter, rLH or hMG is associated to rFSH in the vast ma-ority of cycles (83.4% of cases in the present study).
Westergaard et al. (11) showed that low serum LH con-entrations in cycles with mid-luteal GnRH agonist down-egulation and ovarian stimulation with rFSH were related tofivefold higher rate of early pregnancy loss. Based on thisnding, Kolibianakis et al. (4) hypothesized that the lowerH levels observed in the OCP group during the ovariantimulation could have been responsible for the higher ratef early pregnancy loss found in their study. However, nossociation between LH and ongoing pregnancy rate perycle started was found in the OCP group. In addition, thenvestigators affirmed that their study was underpowered toetect a difference in the ongoing pregnancy rate of 5%,hich was considered to be clinically significant.
LH (or LH activity) administration (hMG/rLH) in most ofur ovarian stimulations could have reversed any negativempact of low LH levels on miscarriage rates in our OCPretreatment group. Nevertheless, in the reports of Cedrin-urnerin et al. (1) and Barmat et al. (2), low miscarriage
ates were also found when only rFSH was administered.
ertility and Sterility�
Based on the current evidence, we consider that OCPretreatment in GnRH antagonist protocols remains an ef-ective option for cycle programming. The only possiblerawback we would highlight is the higher doses of gona-otrophins and the longer duration of ovarian stimulationsequired, which could have a negative impact in low re-ponders and aged patients. Further studies are needed forxploring reproductive outcome in these patients. However,urrently, we believe that OCP pretreatment in GnRH an-agonist cycles should not be considered as a risk factor foriscarriage.
EFERENCES1. Cedrin-Durnerin I, Grange-Dujardin D, Laffy A, Parneix I, Massin
N, Galey J, et al. Recombinant human LH supplementation inIVF/ICSI cycles: a prospective randomized study. Hum Reprod2004;19:1979 – 84.
2. Barmat LI, Chantilis SJ, Hurst BS, Dickey RP. A randomized prospec-tive trial comparing gonadotropin-releasing hormone (GnRH) antago-nist/recombinant follicle-stimulating hormone (rFSH) versus GnRHagonist/rFSH in women pretreated with oral contraceptives before invitro fertilization. Fertil Steril 2005;83:321–30.
3. Shapiro DB, Mitchell-Leef D, Carter M, Nagy ZP. Ganirelix acetate usein normal- and poor-prognosis patients and the impact of estradiolpatterns. Fertil Steril 2005;83:666–70.
4. Kolibianakis EM, Papanikolau EG, Camus M, Tournaye H, Van Steir-teghem AC, Devroey P. Effect of oral contraceptive pill pretreatmenton ongoing pregnancy rates in patients stimulated with GnRH antago-nists and recombinant FSH for IVF. A randomized controlled trial.Hum Reprod 2006;21:352–7.
5. Al-Inany H, Aboulghar M. GnRH antagonist in assisted reproduction:a Cochrane review. Hum Reprod 2002;17:874–85.
6. Olivennes F, Cunha-Filho JS, Fanchin R, Bouchard P, Frydman R. Theuse of GnRh antagonists in ovarian stimulation. Hum Reprod Update2002;8:279–90.
7. Hillier SG. Gonadotropic control of ovarian follicular growth anddevelopment. Mol Cell Endocrinol 2001;179:39–46.
8. Ganirelix Dose-finding Study Group. A double-blind, randomized,dose-finding study to assess the efficacy of the gonadotrophin-releasinghormone antagonist Ganirelix (Org 37462) to prevent premature lutein-izing hormone surges in women ungergoing ovarian stimulation withrecombinant follicle stimulating hormone (Puregon). Hum Reprod1998;13:3023–31.
9. Jaakkola T, Ding Y, Valavaara R, Matikainen H, Tapanainen J, Ron-nberg L, et al. The ratios of serum bioactive/immunoreactive luteinin-zing hormone and follicle-stimulating hormone in various clinicalconditions with increased and decreases gonadotrophin secretion: re-evaluation by a highly sensitive immunoassay. J Clin Endocrinol Metab1990;70:1496–505.
0. Peñarrubia J, Fábregues F, Creus M, Manau D, Casamitjana R, Qui-mera M, et al. LH serum levels during ovarina stimulation as predictorsof ovarian response and asssited reproductive outcome in down regu-lated women stimulated with recombinant FSH. Hum Reprod 2003;18:2689–97.
1. Westergaard LG, Laureen SB, Andersen CY. Increased risk for earlypregnancy loss by profound supression of luteinizing hormone duringovarian stimulation in normogonadotrophic women undergoing assisted
reproduction. Hum Reprod 2000;15:1003–8.1101

Tltc[tiitrO(rsrw
RP
R
Ovulatory status and follicular response predict successof clomiphene citrate-intrauterine inseminationSusanna J. Park, M.D.,a Jesus R. Alvarez, M.D.,a Gerson Weiss, M.D.,a
Stanley Von Hagen, Ph.D.,b Dayna Smith, M.D.,a and Peter G. McGovern, M.D.a
a Department of Obstetrics, Gynecology, and Women’s Health, and b Biostatistics Division, Department of Preventive Medicineand Community Health, University of Medicine and Dentistry of New Jersey (UMDNJ)—New Jersey Medical School, Newark,New Jersey
Objective: To test the hypothesis that anovulatory women would have good pregnancy rates (PRs), regardless ofsingle or multiple follicular development, in response to clomiphene citrate (CC), whereas ovulatory womenwould have good PRs only when achieving multifollicular responses to CC.Design: Retrospective chart review.Setting: University-based infertility center.Patient(s): Two hundred and fifty-four women underwent 585 CC-IUI treatment cycles over a 3-year period.Intervention: Treatment with CC-IUI.Main Outcome Measure(s): Various factors were examined as predictors of clinical pregnancy rate (CPR) andlive-birth rate (LBR) per cycle with the use of logistic regression.Result(s): Overall, the CPR was 11.1%, and the LBR was 8.7%. Of 65 clinical pregnancies, 81.5% resulted inlive births (singletons, 67.7%; twins, 13.8%). There were no higher-order deliveries. In anovulatory women, theCPR and LBR were 15.7% and 13.6%, respectively. In ovulatory women, the CPR and LBR were 8.8% and 6.3%,respectively. As the number of large follicles increased from one to two, the LBR increased from 6.8% to 10.5%.Regarding the interaction of follicles with ovulatory status, anovulatory women had nearly double the CPR andLBR compared to those in ovulatory women, irrespective of the number of large follicles.Conclusion(s): Treatment with CC-IUI is more successful in anovulatory women than in ovulatory women. Themultiple follicular response in both ovulatory and anovulatory women increases PRs. (Fertil Steril� 2007;87:1102–7. ©2007 by American Society for Reproductive Medicine.)
Key Words: CC, follicles, intrauterine insemination, predictive factors, pregnancy rate
lwfmfnoer
cetotWowctbea
reatment of infertility with clomiphene citrate (CC) fol-owed by IUI is a useful infertility treatment when offered tohe appropriate candidates. Clomiphene citrate-IUI may in-rease fecundity via a number of proposed mechanisms:1] increasing the number of oocytes available for fertiliza-ion, [2] overcoming subtle ovulatory dysfunction, [3] allow-ng for more precise timing of insemination, and [4] increas-ng the number of sperm in the upper female reproductiveract. Published overall pregnancy rates (PRs) per cycleange from 3%–12% (1–10); one study reported 26.1% (11).verall live-birth rates per cycle were reported to be 5%–8%
4, 12). A major advantage of this treatment is a decreasedisk of complications (injection problems, ovarian hyper-timulation syndrome, and multiple births) compared to theisks associated with the use of gonadotropins (hMG,hether in conjunction with IUI or IVF).
eceived September 20, 2006; revised and accepted November 9, 2006.resented as a poster at the Society for Gynecologic Investigation, Hous-ton, Texas, March 2004.
eprint requests: Susanna J. Park, M.D., Department of Obstetrics, Gy-necology, and Women’s Health, University of Medicine and Dentistry ofNew Jersey (UMDNJ)—New Jersey Medical School, 185 South OrangeAvenue, MSB E-506, Newark, New Jersey 07103 (FAX: 973-972-9045;
aE-mail: [email protected]).
1102 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
For anovulatory women, production of even a single fol-icle should greatly improve the chances for pregnancy,hereas the ovulatory woman might be expected to benefit
rom use of CC only when she responds to the drug withultiple follicles. (We must mention that despite a mono-
ollicular response to CC therapy, some ovulatory womenonetheless benefit from CC therapy, because CC influencesther factors, in addition to oocyte production.) We thereforevaluated the significance of ovulatory status and follicularesponse in the PRs of CC-IUI treatment cycles.
Most previous studies that looked at infertility diagnosesategorized couples by their most significant problem. Forxample, if the man has very poor sperm, the couple isypically categorized as having male factor infertility. Thevulatory status of women in whom other significant infer-ility diagnoses exist is usually not studied in these articles.
e therefore reviewed each patient chart, to determine thevulatory status of every woman in the study, regardless ofhether or not other infertility factors were present. To
ategorize a woman as ovulatory, we required that at leastwo of the following be documented in the patient chartefore initiation of CC-IUI therapy: regular menstrual cyclesvery 25–35 days, a biphasic basal body temperature chart,secretory-phase endometrial biopsy, serum P �3 ng/mL, or
positive color change visualized on a home urine LH kit.0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.11.037

spuawwa
MD2wwd
PAeTelticwrpn
tchoignmu
SAcmKfg
IAtce
sdrtattf(OIhof
PI�p1nydpdc
SWdaTldfpbofdsmtdcPmmrcr
RAA
F
This study aimed to assess the importance of ovulatorytatus and follicular response in pregnancy success (clinicalregnancy and live births), with the use of CC-IUI at ourniversity-based infertility center. We hypothesized thatnovulatory women would have a good PR regardless ofhether they responded with single or multiple follicles,hereas ovulatory women would have a good PR only when
chieving a multifollicular response to CC.
ATERIALS AND METHODSuring the 3-year period between January 1, 1998–December 31,000, 585 CC-IUI treatment cycles were performed on 254omen at our university-based infertility center. No cyclesere excluded. Institutional review board approval to con-uct this study was obtained.
atient Evaluationll women underwent a complete history and physical
xamination. Endocrine examinations typically includedSH, PRL, menstrual cycle day 3 FSH, and E2. Anatomicvaluations consisted of a hysterosalpingogram (HSG) oraparoscopy. Confirmation of at least one patent fallopianube was required for inclusion in this study. Abnormal-ties of the endometrial cavity were reassessed hysteroscopi-ally, and surgically corrected if necessary. Ovulatory statusas confirmed by the presence of �2 of the following:
egular cycles every 25–35 days, biphasic basal body tem-erature, secretory-phase endometrial biopsy, serum P at �3g/mL, and color change visualized on an ovulation kit.
Infertility diagnoses were categorized in accordance withhe Society for Assisted Reproductive Technology (SART)lassification as follows: tubal factor (peritubal adhesions orydrosalpinx at laparoscopy or laparotomy, or hydrosalpinxr distal tubal occlusion on HSG); endometriosis (visiblemplants at surgery, or confirmatory pathology sample); oli-oanovulation, subdivided into hypogonadotropic, normogo-adotropic, and hypergonadotropic etiology; uterine (abnor-al cavity on HSG or saline ultrasound); male factor; and
nexplained.
emen Evaluationll male partners had semen analysis performed at an endo-
rinology laboratory. Semen analysis was defined as abnor-al based on a count �20 � 106/mL, motility �50%, orruger morphology �4%. Semen specimens were prepared
or IUI by either the swim-up technique or the density-radient technique, as determined by the andrology staff.
nduction of Ovulationfter either a spontaneous or induced menstrual cycle, pa-
ients were treated with CC 50mg from cycle days 3–7 orycle days 5–9 (according to the attending physician’s pref-
rence). Doses of CC were increased in 50-mg increments in certility and Sterility�
ubsequent cycles (CC 100mg for 5 days, CC 150mg for 5ays, and CC 200mg for 5 days) if there was an insufficientesponse, defined as monofollicular development in ovula-ory women or no dominant follicular development innovulatory women. On cycle days 10–11, transvaginal ul-rasounds were performed to measure mean endometrialhickness and mean follicular diameters. When the leadollicle measured �18 mm in mean diameter, 5,000 IU hCGProfasi; Serono, Brussels, Belgium, or Pregnyl; Organon,ss, the Netherlands) was administered IM that evening.
ntrauterine inseminations were performed approximately 36ours after hCG administration. Six days after the first dosef hCG, a second dose of 2,500 IU hCG was administeredor luteal support.
regnancy Outcomesf menses had not occurred 14 days after IUI, serum levels of-hCG were measured. Positive �-hCG values were re-eated in 2 days. Transvaginal ultrasounds were performed4 days after the second positive �-hCG. A clinical preg-ancy was defined as an intrauterine gestational sac with aolk sac and fetal pole. Clinical pregnancy rate (CPR) wasefined as the number of patients with clinical pregnancieser number of treatment cycles. Live-birth rate (LBR) wasefined as the number of live births per number of treatmentycles.
tatistical Analysise studied all cycles together, and then reevaluated the
ata, using only the first treatment cycle per patient tovoid bias due to multiple cycles in unsuccessful subjects.he statistical approach was that of proposing various
ogistic regression models, and (via stepwise elimination)etermining a final model which incorporated only thoseactors which were deemed to be important contributors inredicting the outcome (either clinical pregnancy or liveirth). The first full model included the following factors:vulatory status, number of follicles achieved after CC,emale age, years of infertility, parity, day 3 FSH, SARTiagnosis, history of prior infertility treatments, day oftarting CC, daily dose of CC, number of follicles �16m, endometrial thickness, cycle day of hCG administra-
ion, total number of motile sperm inseminated, use ofonor versus husband sperm, and number of treatmentycles. For preliminary models, only those factors with�.20 were left incorporated in the models. Subsequentodels were then reevaluated until only those factorseeting the more stringent requirement of P�.05 were
etained in the model. Significance was determined by thehi-square statistic (i.e., 2*-LogLiklihood) for the logisticegression models.
ESULTSll CC-IUI Cycles
total of 254 women underwent 585 CC-IUI treatment
ycles. One hundred and sixty-one women (63.4%) were1103

oaToyh(hpImfccc1cC
(1ocpo
p
wniapelth
s((a1a1d
�AtL(pab
vulatory; 93 women (36.4%) were anovulatory. The meange was 32.7 years (SD, �4.2), with a range of 18–48 years.he mean day 3 FSH was 6.8 IU/L (SD, �2.0), with a rangef 2.5–15.4 IU/L. The mean duration of infertility was 2.9ears (SD, �4.5 years), with a range of 1–21 years. Almostalf (48.4%) of the patients were nulligravid. Most womenn � 148) had received some prior infertility care: 48.4%ad undergone previous CC-IUI cycles, 5.9% had undergonerevious hMG-IUI cycles, and 3.9% had undergone previousVF cycles. There was marked attrition throughout treat-ent: 254 first cycles, 169 second cycles, 88 third cycles, 44
ourth cycles, and only 30 fifth or greater cycles were re-orded in our database. In the first cycle, 13.4% of womenonceived; 7.1% conceived in the second cycle; 2.8% con-eived in the third cycle; 0.4% conceived in the fourth cycle;.1% conceived in the fifth or greater cycle; and 75.2% neveronceived. Table 1 shows some characteristics of the 585C-IUI treatment cycles.
The overall CPR was 11.1% (65/585), of which 84.6%55/65) were single sacs, 13.8% (9/65) were double sacs, and.5% (1/65) was triple sacs. No clinical pregnancy consistedf �4 gestational sacs. First-trimester pregnancy losses oc-urred in 18.5% (12/65) of the clinical pregnancies. Tworegnancies (3.1%) resulted in ectopic pregnancies, of whichnly one required surgical intervention.
Overall LBR was 8.7% (51/585). Forty-four of 65 clinicalregnancies (67.7%) resulted in singleton deliveries, of
TABLE 1Characteristics of 585 CC-IUI treatment cycles.
Characteristics
CC start day (n � 585)Day 3Day 5Not specified
Daily dose of CC (n � 585)Missing25 mg50 mg100 mg150 mg200 mg
Number of follicles �16 mm (n � 584)Maximum endometrial thickness (mm) (n � 577)Day of hCG administrationMillions of motile sperm inseminated (n � 584)Source of sperm (n � 585)
NondonorDonor
Number of treatment cyclesPrior CC-IUI treatment cycles (n � 148)
Park. Success in CC-IUI. Fertil Steril 2007.1104 Park et al. Success in CC-IUI
hich 41 delivered at term (four were initially twin preg-ancies which spontaneously reduced to single pregnanciesn the first trimester), and three delivered preterm at 34, 36,nd 36 weeks of gestational age. Nine of 65 (13.8%) clinicalregnancies resulted in twin deliveries, of which two deliv-red preterm at 35 and 32 weeks of gestational age. Theatter was a spontaneous reduction from triplet to twin ges-ation during the first trimester. There were no triplet origher deliveries.
Logistic regression revealed that only two factors wereignificant predictors of treatment success: ovulatory statusCPR, P�.008; LBR, P�.002) and number of large folliclesCPR, P�.002; LBR, P�.015). The CPR in ovulatory versusnovulatory women was 8.8% (35/394) versus 15.7% (30/91), respectively (Fig. 1). The LBR in ovulatory versusnovulatory women was 6.3% (25/394) versus 13.6% (26/91), respectively. All other factors examined failed to pre-ict treatment success with any significance.
In one treatment cycle in our study, the number of follicles16 mm was not recorded, and thus we assessed 584 cycles.s the number of large follicles increased from one to two,
here was a significant increase in LBR, i.e., one follicle,BR � 6.8% (22/322); and two follicles, LBR � 10.5%
20/190). More than two follicles did not significantly im-rove the success rate: three follicles, LBR � 12% (6/50);nd �4 follicles, LBR � 13.6% (3/22). The rate of multipleirths was higher with more follicles. With one follicle there
Total (%) Mean (�SD) (range)
159 (27.2)282 (48.2)144 (24.6)
86 (14.7)4 (0.7)
288 (49.2)138 (23.6)65 (11.1)4 (0.7)
1.62 (�0.85) (1–7)7.75 (�2.3) (2–17)
14.83 (�3.06) (8–27)64.59 (�93.97) (0.1–918.6)
514 (87.9)71 (12.1)
2.07 (�1.34) (1–10)72 (48.6)
Vol. 87, No. 5, May 2007

wfbtfa
FA2rf(sode
IRBwrtidwlo
DPCTcispttpapdo
wCtcswetiaCt
F
ere 3/22 twin births (13.6%), versus 7/29 (24.1%) with �2ollicles. There was no apparent difference in twin birthsetween women with two follicles (5/20 or 25%) versushose with �3 follicles (2/9 or 22%), although there were tooew live births among women with �3 follicles to evaluateccurately the risks of multiple birth.
irst CC-IUI Cycle Onlynalyzing only the first treatment cycle per patient (n �54), we discovered nonsignificant trends toward similaresults, but we had insufficient power to conclude that anyactors were positively associated with treatment successCPR or LBR). For example, we had 41% power to detect aignificant difference at an alpha of 0.05 in CPRs betweenvulatory and anovulatory women. To achieve 80% power toetect this difference, we would have needed 324 women inach arm (total n � 628 women).
nteraction Between Ovulatory Status and Follicularesponseecause ovulatory status strikingly affected CPR and LBR,e further analyzed the number of follicles �16 mm in
elation to ovulatory status (Table 2). As expected, whenhere was more than one follicle �16 mm, there was anncrease in CPR and LBR. Anovulatory women had nearlyouble the CPR and LBR compared to those in ovulatoryomen, irrespective of the number of large follicles. Anovu-
atory women did not seem to have an increased risk of twin
FIGURE 1
Clinical pregnancy rates (CPRs) and live birth rates(LBRs) in relation to ovulatory status in 585 CC-IUIcycles.
Park. Success in CC-IUI. Fertil Steril 2007.
r greater deliveries when there were �2 large follicles.
ertility and Sterility�
ISCUSSIONrevious studies that evaluated factors that affect success inC-IUI treatment cycles are at variance with one another.hese disparities in the literature are due to varying patientharacteristics (age, duration of infertility, parity, etiology ofnfertility, and dissimilar infertility evaluations), dissimilartimulation protocols (dose of CC, day of CC administration,resence or absence of hCG administration, and timing be-ween ovulation and insemination), different sperm prepara-ions and insemination techniques, low number of studyarticipants and/or treatment cycles, and differences in thenalysis and presentation of study results (PRs or live birthser cycle, cumulative PRs, and life-table analysis). Thus, it isifficult to extrapolate which specific factors are prognosticf success with CC-IUI treatment.
In our study, the most significant predictors of successere anovulatory status and the number of large follicles.omparison of ovulatory and anovulatory women revealed
hat the CPR and LBR were double in anovulatory womenompared to those in ovulatory women (Fig. 1). This was noturprising, because it was shown that 85.3% of anovulatoryomen ovulate with CC (13). Thus, CC-IUI is a more
ffective treatment in anovulatory women. It must be men-ioned that we only evaluated couples in whom CC was usedn conjunction with IUI. The typical first-line therapy fornovulation at our center during this treatment period wasC-intercourse, so couples would only have been enrolled in
his study if their attending physician had deemed that IUI
TABLE 2CPRa and LBRb in follicles ≥16 mm inrelation to ovulatory status in 584 CC-IUIc
cycles.
Ovulatorystatus
# Follicles ≥16 mm
1 ≥2
Ovulatory n � 201 n � 192CPR 11 (5.5%) 24 (12.5%)LBR 8 (4%) 17 (8.9%)Singleton 8 (100%) 13 (76.5%)Twins 0 4 (23.5%)Triplets 0 0
Anovulatory n � 121 n � 70CPR 16 (13.2%) 14 (20%)LBR 14 (11.5%) 12 (17%)Singleton 13 (92.9%) 11 (91.7%)Twins 1 (7.1%) 1 (8.3%)Triplets 0 0
aCPR � clinical pregnancy rate per cycle
bLBR � live birth rate per cycle
cCC-IUI � CC-intrauterine insemination
Park. Success in CC-IUI. Fertil Steril 2007.
1105

wp
ldfTstciT�hwCo3�(pw
cwtqmbcr1
ppptdtd
sm(Hv1
nTctte
fTsl
distwt
dIraiisaTatT�sw�ocTnlaTm�ibnst
cpP
R
as necessary, for instance because of male factor, or a poorostcoital test with CC.
Does increasing the number of follicles �16 mm in anovu-atory women increase the risk of multiple deliveries? Weemonstrated that as the number of follicles �16 mm increasedrom one to �2 follicles, there was a parallel increase in LBR.his relationship was also apparent in relation to ovulatorytatus. When �2 follicles �16 mm were induced in anovula-ory women, there was a significant increase in CPR and LBRompared to those in ovulatory women, without an attendantncreased risk in the number of multiple deliveries (Table 2).here were insufficient numbers of women with �3 follicles16 mm to draw reliable conclusions about an increased risk of
igher-order deliveries. However, the risk of multiple gestationsith CC-IUI treatment must not be disregarded. Of 1,713C-IUI cycles conducted by Dickey et al., 1.7% were higher-rder (triplet or greater) multiple gestations, which tripled to.8% (without an increase in PR) in women �35 years old with6 follicles measuring �12 mm at time of hCG administration
14). We did not have any higher-order deliveries in our study,ossibly because we usually recommend cycle cancellation if aoman develops �5 large follicles after taking CC.
Does there exist a threshold number of CC-IUI treatmentycles after which the treatment is no longer effective? Thereere insufficient women in our study who underwent mul-
iple CC-IUI treatment cycles to address this matter ade-uately. However, analysis of the literature shows that treat-ent with CC-IUI should be limited to four treatment cycles,
ecause cumulative PRs do not rise significantly after fourycles in all age groups (15). In contrast, other studiesevealed constant fecundity through seven (4), 10 (16), and4 (6) cycles of CC-IUI treatment.
In our study, the following factors were not significantrognostic factors of CPR and LBR with CC-IUI treatments:atient-specific factors (female age, duration of infertility,arity, basal FSH, diagnosis, and history of prior infertilityreatments) and cycle-specific factors (day of starting CC,ose of CC, endometrial thickness, day of hCG administra-ion, total number of motile sperm count [TMSC], use ofonor sperm, and number of treatment cycles).
Female age was not found to be a prognostic factor in thistudy. This may be because our center typically recommendsore aggressive treatment for women �40 years of age
there were only 12 women aged �40 years in our study).owever, the exact age at which the PR is adversely affectedaries by study, and ranges from age 35 to �43 years (4, 15,7, 18).
A diagnosis of infertility (other than ovulatory status) wasot influential in treatment success with CC-IUI in our study.his is in agreement with several other studies (5, 18). Inontrast, other studies demonstrated that CC-IUI is an effec-ive treatment for women diagnosed with unexplained infer-ility or surgically corrected endometriosis (10, 11). How-
ver, the presence of uncorrected endometriosis or tubal1106 Park et al. Success in CC-IUI
actor negatively impacts PRs by nearly 50% (4, 16, 17).his disparity may be explained by the inclusion and exclu-ion criteria of the studies. In our study, confirmation of ateast one patent fallopian tube was required for inclusion.
Endometrial thickness was not a significant factor in pre-icting CC-IUI treatment success in our study. Similar find-ngs were demonstrated elsewhere (19). In contrast, othertudies showed that endometrial thickness is prognostic ofreatment success (20). In one study, there was no pregnancyhen endometrial thickness on the day of hCG administra-
ion was �6 mm (21).
In our study, the quality of the sperm being inseminatedid not significantly influence treatment success with CC-UI. An analysis of published studies provides conflictingesults because of a lack of standard criteria for semennalysis, variations in the method of semen preparation fornsemination, and nonuniform reporting of semen character-stics. Some studies provided results based on unprocessedemen specimens. Dickey et al. concluded that CC-IUI wasn effective treatment if unprocessed semen specimen had aMSC �5 � 106/mL (22). Van Voorhis et al. recommendedTMSC �10 � 106 in the unprocessed ejaculate as a
hreshold value for IUI based on an LBR/cycle of 2.5% ifMSC �10 � 106, versus an LBR/cycle of 7.1% if TMSC10 � 106, in CC-IUI treatment cycles (18). Arici et al.
howed that CC-IUI was an ineffective treatment in menith semen analysis yielding �20 � 106/mL, motility50%, or normal morphology �50% (11). On the contrary,
ther studies provided semen-quality results based on pro-essed specimens. Berg et al. concluded that a thresholdMSC value of 0.8 � 106 after the swim-up technique wasecessary for conception with CC-IUI treatment (6). Ombe-et et al. (23) demonstrated an average PR/cycle of 14.6%nd LBR/cycle of 9.7% after three CC-IUI cycles if theMSC was �1 � 106 after the swim-up technique. A spermorphology of �4% was essential only if the TMSC was1 � 106 (23). A meta-analysis was performed to determine
f a specific cutoff value of TMSC of processed semen coulde used to predict IUI success (24). Such a criterion couldot be established. It was concluded that the cutoff valuehould be dependent on each center’s sperm preparationechnique and patient characteristics.
In conclusion, anovulatory women had a much betterhance of pregnancy with the use of CC-IUI therapy, com-ared to their ovulatory counterparts. In both groups, a betterR was obtained when multiple follicles were achieved.
EFERENCES1. Plosker SM, Jacobson W, Amato P. Predicting and optimizing
success in an intra-uterine insemination program. Hum Reprod1994;9:2014 –21.
2. Hannoun A, Abu-Musa A, Kaspar H, Khalil A. Intrauterine insemina-tion IUI: the effect of ovarian stimulation and infertility diagnosis onpregnancy outcome. Clin Exp Obstet Gynecol 1998;25:144–6.
3. Kemmann E, Bohrer M, Shelden R, Fiasconaro G, Beardsley L. Active
ovulation management increases the monthly probability of pregnancyVol. 87, No. 5, May 2007

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
F
occurrence in ovulatory women who receive intrauterine insemination.Fertil Steril 1987;48:916–20.
4. Dickey RP, Olar TT, Taylor SN, Durole DN, Rye PH. Relationship offollicle number and other factors to fecundability and multiple preg-nancy in CC-induced intrauterine insemination cycles. Fertil Steril1992;57:613–9.
5. Van Der Westerlaken LA, Naaktgeboren N, Helmerhorst FM. Evalua-tion of pregnancy rates after intrauterine insemination according toindication, age, and sperm parameters. J Assist Reprod Genet 1998;15:359–64.
6. Berg UB, Brucker CB, Berg FD. Effect of motile sperm count afterswim-up on outcome of intrauterine insemination. Fertil Steril 1997;67:747–50.
7. Martinez AR, Bernardus RE, Voorhorst FJ, Vermeiden JPW, Schoe-maker J. Intrauterine insemination does and CC does not improvefecundity in couples with infertility due to male or idiopathic fac-tors: a prospective, randomized, controlled study. Fertil Steril 1990;53:847–53.
8. Melis GB, Paoletti AM, Strigini F, Fabris FM, Canale D, Fioretti P.Pharmacologic induction of multiple follicular development improvesthe success rate of artificial insemination with husband’s semen incouples with male-related or unexplained infertility. Fertil Steril 1987;47:441–5.
9. Stone BA, Vargyas JM, Ringler GE, Stein AL, Marrs RP. Determinantsof the outcome of intrauterine insemination: analysis of outcomes of9963 consecutive cycles. Am J Obstet Gynecol 1999;180:1522–34.
0. Deaton JL, Gibson M, Blackmer KM, Nakajima ST, Badger GJ, Brum-sted JR. A randomized, controlled trial of CC and intrauterine insem-ination in couples with unexplained infertility or surgically correctedendometriosis. Fertil Steril 1990;54:1083–8.
1. Arici A, Byrd W, Bradshaw K, Kutteh SH, Marshburn P, Carr BR.Evaluation of CC and human chorionic hMG treatment: a prospective,randomized, crossover study during intrauterine insemination cycles.Fertil Steril 1994;61:314–8.
2. Hendin BN, Falcone T, Hallak J, Godlberg J, Thomas AJ, Nelson DR,et al. Effect of clinical and semen characteristics on efficacy of ovula-tory stimulation in patients undergoing intrauterine insemination.J Assist Reprod Genet 2000;17:189–93.
3. Gysler M, March CM, Mishell DR Jr, Bailey EJ. A decade’s experiencewith an individualized clomiphene treatment regimen including its
effect on the postcoital test. Fertil Steril 1982;37:161–7.ertility and Sterility�
4. Dickey RP, Taylor SN, Lu PY, Sartor BM, Rye PH, Pyrzak R.Relationship of follicle numbers and estradiol levels to multipleimplantation in 3,608 intrauterine insemination cycles. Fertil Steril2001;75:69 –78.
5. Agarwal SK, Buyalos RP. CC with intrauterine insemination: is iteffective therapy in women above the age of 35 years? Fertil Steril1996;65:759–63.
6. Hammond MG, Halme JK, Talbert LM. Factors affecting the pregnancyrate in CC induction of ovulation. Obstet Gynecol 1983;62:196–202.
7. Dickey RP, Taylor SN, Lu PY, Sartor BM, Rye PH, Pyrzak R. Effectof diagnosis, age, sperm quality, and number of pre-ovulatory follicleson the outcome of multiple cycles of CC-intrauterine insemination.Fertil Steril 2002;78:1088–95.
8. Van Voorhis BJ, Barnett M, Sparks AE, Syrop CH, Rosenthal G,Dawson J. Effect of total motile sperm count on the efficacy andcost-effectiveness of intrauterine insemination and in vitro fertilization.Fertil Steril 2001;75:661–8.
9. Kolibianakis EM, Zikopoulos KA, Fatemi HM, Osmanagaoglu K,Evenpoel J, Van Steirteghem A, et al. Endometrial thickness cannotpredict ongoing pregnancy achievement in cycles stimulated with CCfor intrauterine insemination. Reprod Biomed Online 2004;8:115–8.
0. Wolman I, Sagi J, Pauzner D, Yovel I, Seidman DS, David MP.Transabdominal ultrasonographic evaluation of endometrial thicknessin CC-stimulated cycles in relation to conception. J Clin Ultrasound1994;22:109–12.
1. Dickey RP, Olar TT, Taylor SN, Curole DN, Matulich EM. Relation-ship of endometrial thickness and pattern to fecundity in ovulationinduction cycles: effect of CC alone and with human menopausal hMG.Fertil Steril 1993;59:756–60.
2. Dickey RP, Pyrzak R, Lu PY, Taylor SN, Rye PH. Comparison of thesperm quality necessary for successful intrauterine insemination withWorld Health Organization threshold values for normal sperm. FertilSteril 1999;71:684–9.
3. Ombelet W, Vandeput H, Van de Putte G, Cox A, Janssen M, Jacobs P,et al. Intrauterine insemination after ovarian stimulation with CC:predictive potential of inseminating motile count and sperm morphol-ogy. Hum Reprod 1997;12:1458–63.
4. Van Weert JM, Repping S, Van Voorhis BJ, Van Der Veen F, BossuytPM, Mol BWJ. Performance of the postwash total motile sperm countas a predictor of pregnancy at the time of intrauterine insemination: a
meta-analysis. Fertil Steril 2004;82:612–20.1107

PitdHitbod2ro
R
S
R
POLYCYSTIC OVARY SYNDROME
Polycystic ovary syndrome and risk of uterineleiomyomataLauren A. Wise, Sc.D.,a Julie R. Palmer, Sc.D.,a Elizabeth A. Stewart, M.D.,b
and Lynn Rosenberg, Sc.D.a
a Slone Epidemiology Center, Boston University, and b Center for Uterine Fibroids, Department of Obstetrics, Gynecology,and Reproductive Biology, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts
Objective: To examine the association between polycystic ovary syndrome (PCOS) and the risk of uterineleiomyomata (UL).Design: Prospective cohort study.Setting: Participants from the Black Women’s Health Study, an ongoing prospective cohort study of African-American women aged 21–69 years in 1995 residing in the United States. Participants completed mailedquestionnaires about their health status every 2 years.Patient(s): Premenopausal women with no history of UL at the start of follow-up (N � 23,571).Intervention(s): No interventions were administered.Main Outcome Measure: Incidence of UL among those with and without self-reported, physician-diagnosedPCOS over a 6-year period of follow-up (1997–2003). Medical-record validation in a random subset of UL casesconfirmed 96% of diagnoses.Result(s): During 114,373 person-years of follow-up, 3,631 new cases of UL confirmed by ultrasound (N �2,926) or hysterectomy (N � 705) were reported. After adjustment for potential confounders, the incidence of ULwas 65% higher among women with PCOS than women without PCOS (incidence rate ratio, 1.65; 95%confidence interval, 1.21–2.24). The incidence rate ratios remained constant with increasing time after thediagnosis of PCOS. Results were similar when analyses were confined to women reporting a recent Papanicolaousmear, a proxy for a pelvic examination.Conclusion(s): The present study suggests a positive association between PCOS and UL in African-Americanwomen. (Fertil Steril� 2007;87:1108–15. ©2007 by American Society for Reproductive Medicine.)
Key Words: Stein-Leventhal syndrome, polycystic ovaries, uterine neoplasms, leiomyoma, African-Americans,premenopausal, females
itNrf
acidcteoolbs
olycystic ovary syndrome (PCOS) is a disease character-zed by menstrual irregularity and androgen excess not at-ributable to another cause (1,2). A more comprehensiveefinition of PCOS arose at a 1990 National Institutes ofealth (NIH) conference on the disorder (3), and was revised
n 2003 (4). The 1990 NIH diagnostic criteria required thathe patient have both chronic anovulation and clinical and/oriochemical signs of hyperandrogenism, and no evidence ofther related disorders, such as hyperprolactenemia, thyroidisorders, or nonclassic adrenal hyperplasia (3). The revised003 criteria added ultrasound evidence of polycystic ova-ies as a third criterion, and required that patients manifest 2f the 3 criteria. While estimates of the prevalence of PCOS
eceived June 19, 2006; revised September 19, 2006; accepted October21, 2006.
upported by grant no. CA58420 from the National Cancer Institute(Bethesda, MD).
eprint requests: Lauren A. Wise, Sc.D., Slone Epidemiology Center,Boston University, 1010 Commonwealth Avenue, Boston, Massachu-
Esetts 02215 (FAX: 617-738-5119; E-mail: [email protected]).
1108 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
n the general population range from 2%–20%, depending onhe definition used, a recent prospective study using the 1990IH criteria estimated the prevalence to be 3%–6% of
eproductive-aged women (5,6). The prevalence did not dif-er markedly between black and white women (6).
Women with PCOS often have elevated LH levels (2), andre at higher risk for developing infertility, endometrialarcinoma, and a number of metabolic disorders, includingnsulin resistance, diabetes, hypertension, and cardiovascularisease (7–10). Whether PCOS is associated with an in-reased risk of uterine leiomyomata (UL) is unknown. Al-hough UL are thought to be influenced primarily by endog-nous levels of estrogens (Es) and P, there is a growing bodyf literature to suggest that elevated LH levels, independentf ovarian function (11–14), and dysregulation of the insu-in-growth factor and growth hormone (IGF-GH) axis, maye important in the etiology of UL (15–19). The cross-ectional Uterine Fibroid Study of the National Institute of
nvironmental Health Sciences (NIEHS) found a positive0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.11.012

apsw(F(Ptru
SAs
MSTwAtssrmhsceocrM(
omqwpqnmwisrr9cmcdw
t2switaf
AO“diascrpPdtt
mawtp“siaplvBsacnt
3ftcmdaci
F
ssociation between urinary LH levels and risk of UL,articularly for large tumors (12). Other epidemiologictudies found the risk of UL to be positively associatedith medication-treated diabetes (20) and hypertension
20,21), conditions that are associated with PCOS (9).inally, PCOS was associated with a high ratio of E2 to P22), which may be an important mechanism by whichCOS affects the risk of UL. Thus, PCOS may influence
he development of UL via elevation of LH levels, dys-egulation of the IGF-GH axis, and/or increased levels ofnopposed estrogens.
With the use of data from the Black Women’s Healthtudy (BWHS), a large prospective cohort study of African-merican women, we evaluated the association between
elf-reported PCOS and UL.
ATERIALS AND METHODStudy Populationhe BWHS is an ongoing, prospective cohort study thatas established in 1995. Approximately 59,000 African-merican women aged 21– 69 years were enrolled
hrough self-administered questionnaires mailed to sub-cribers of Essence magazine, members of black profes-ional organizations, and friends and relatives of earlyespondents (23). The baseline questionnaire elicited infor-ation on demographic and behavioral characteristics,
ealthcare utilization, and medical conditions. Women whoelf-identified as “black” on their 1997 questionnaire wereonsidered eligible for inclusion. The cohort is followedvery 2 years by postal questionnaire, and �80% of theriginal cohort completed a questionnaire in each follow-upycle. The study protocol was approved by the institutionaleview boards of Boston University Medical Center (Boston,
assachusetts) and Howard University Cancer CenterWashington, D.C.).
Follow-up for the incidence of UL began in 1997, the startf the second questionnaire cycle, because self-reportedethod of confirmation for UL was first elicited on the 1999
uestionnaire. We restricted the sample to premenopausalomen with intact uteri because UL are rare after meno-ause (24). Of the 53,176 women who completed the 1997uestionnaire, we therefore excluded women who reportedatural menopause (N � 5,193), hysterectomy without re-oval of both ovaries (N � 6,685), bilateral oophorectomyith or without hysterectomy (N � 4,259), medication-
nduced menopause (N � 42), or unknown menopausaltatus (N � 418) at the start of follow-up. Women whoeported a diagnosis of UL before 1997 (N � 10,502), whoeported UL without information on year of diagnosis (N �4) or method of confirmation (N � 182), who did notomplete a follow-up questionnaire (N � 1,610), or who hadissing data on key covariates (N � 586) were also ex-
luded. Finally, the 34 incident UL cases who reported aiagnosis of PCOS in the same year as their diagnosis of UL
ere excluded from the analysis because we could not de- certility and Sterility�
ermine which diagnosis occurred first. The remaining3,571 women were followed for incidence of UL in theubsequent 6-year period. The small proportion of womenho did not complete a follow-up questionnaire or who had
ncomplete data on covariates had a lower educational at-ainment than respondents, but were similar with respect toge, parity, age at menarche, and other established riskactors for UL.
ssessment of Exposure and Other Covariatesn the 1995 and 1997 questionnaires, women reported
polycystic ovary syndrome” or “Stein-Leventhal syn-rome” under an open-ended question about “other seriousllness” along with year of first diagnosis. On the 1999nd 2001 follow-up questionnaires, women were askedpecifically whether they had been diagnosed with “poly-ystic ovarian syndrome” by a physician and, if so, toeport the calendar year of first diagnosis. To ensure arospective analysis, we required that the reported year ofCOS diagnosis precede that of the UL diagnosis. Theate of diagnosis for PCOS does not necessarily refer tohe actual onset of PCOS, which typically occurs aroundhe time of adolescence (1,2).
On the baseline survey, data were obtained on age atenarche, oral contraceptive (OC) use, number of live births
nd stillbirths (parity), age at each birth, height, currenteight, weight at age 18 years, physician-diagnosed diabe-
es, alcohol intake, cigarette smoking, education, and occu-ation. We also asked about history of infertility (defined astrying to become pregnant for at least 1 year withoutuccess”), the age at which infertility first occurred, and itsnvestigated causes. On the 2003 questionnaire, we askedbout household income and number of individuals sup-orted by this income. Body mass index (BMI) was calcu-ated as weight (kg) divided by height squared (m2). Aalidation study of anthropometric measures among 115WHS participants from the Washington, D.C. area
howed high correlation (r � 0.97) between self-reportednd technician-measured weight (25). Covariates thathanged over time were updated on follow-up question-aires (e.g., age, parity, and BMI), and were treated asime-dependent variables in the analysis.
An open-ended question about “medications used at leastdays a week” was included on the baseline (1995) and
ollow-up questionnaires. We considered women with PCOSo be taking appropriate medications if they reported use ofombined OCs or any of the following: biguanides (e.g.,etformin), thiazolidinediones (e.g., pioglitazone), antian-
rogens (e.g., cyproterone acetate, spironolactone, or flut-mide), antiestrogens (e.g., clomiphene citrate), glucocorti-oids (e.g., prednisone), ornithine decarboxylasenhibitors (e.g., eflornithine hydrochloride), and 5-�-redu-
atase inhibitors (e.g., finasteride) (26).1109

AOwwyd“ti“Ah“ec
dseretfebbtp
sscfmp1psm(nbtd1it
tr[spm
rg
DIfihwr1fci2(mPcwN
tfcom[h(b�mnipoodi�lspgRsl
awime
ssessment of Outcomen the 1999, 2001, and 2003 follow-up questionnaires,omen were asked about whether they had been diagnosedith “fibroids” in the previous 2-year interval, the calendarear in which they were first diagnosed, and whether theiriagnosis was confirmed by “pelvic examination” and/or byultrasound and hysterectomy.” In 2003, we changed “hys-erectomy” to “surgery” because myomectomy was becom-ng more common as a treatment option, and dividedultrasound” and “surgery” into two separate questions.mong cases reporting confirmation by “ultrasound andysterectomy” or “surgery,” a diagnosis was consideredhysterectomy-confirmed” if the woman reported hyster-ctomy on the same questionnaire, and “ultrasound-onfirmed” otherwise.
Ultrasound has been the standard method to confirm ULiagnoses in clinical practice (24). Ultrasound has high sen-itivity (99%) and specificity (91%) relative to histologicvidence (27,28). Because histologically confirmed casesepresent only 10%–30% of cases for which ultrasoundvidence is available, and because studies restricted to his-ologically confirmed cases may spuriously identify riskactors associated with disease severity or treatment prefer-nce (29), our outcome definition included cases confirmedy ultrasound or hysterectomy. Cases reporting confirmationy pelvic examination only were not considered as part ofhe case group, because such diagnoses may represent otherathologies (30).
We assessed the accuracy of self-report in a randomample of 248 cases. These cases were mailed supplementalurveys regarding their initial date of diagnosis, method ofonfirmation, symptoms, and treatment, and they were askedor permission to review their medical records. We obtainededical records from 127 of the 128 women who gave us
ermission, and verified the self-report by medical record in22 cases (96%). Among the 188 (76%) cases who com-leted the supplemental survey, 71% reported UL-relatedymptoms prior to being diagnosed with the condition. Theost commonly reported symptoms were menorrhagia
53%) and pelvic pain (46%). When asked how their diag-osis had come to clinical attention, 55% of cases reportedeing diagnosed while seeking care for UL-related symp-oms, and an additional 32% reported having UL clinicallyetected at the time of pelvic examination. The remaining3% reported having UL detected incidentally while receiv-ng care for another condition (�85% cited “pregnancy” ashe other condition).
There were no statistically significant differences be-ween cases who did and did not release their medicalecords with respect to [1] established risk factors for UL;2] self-reported method of confirmation; [3] the report ofymptoms prior to the initial diagnosis; [4] the type ofresenting symptoms; or [5] how the initial diagnosis was
ade (31). Therefore, the cases who released their medical e1110 Wise et al. PCOS and risk of uterine leiomyomata
ecords were likely to be representative of the larger caseroup.
ata Analysisncident cases were defined as women who self-reported arst diagnosis of UL, which was confirmed by ultrasound orysterectomy. Cases confirmed by pelvic examination onlyere analyzed as part of the noncase group. Person-years at
isk were calculated from the start of follow-up (March997) until the diagnosis of UL, menopause, death, loss toollow-up, or the end of follow-up (March 2003), whicheverame first. Cox regression models, stratified by age (1-yearntervals) and time period (1997–1999, 1999–2001, and001–2003), were used to estimate incidence rate ratiosIRRs) and 95% confidence intervals (CIs) for UL, and theseodels compared women with and without self-reportedCOS. A 95% CI that excluded 1.0 was considered statisti-ally significant (i.e., P�.05). All analyses were carried outith the use of SAS statistical software (SAS, Inc., Cary,C) (32).
A covariate was included in the multivariable analyses ifhe literature supported its role as an independent risk factoror UL, or if adding it to a model containing all otherovariates changed the exposure IRR by �10% (33). Basedn these criteria, we constructed three sets of multivariableodels: [1] a model that controlled for age and time period;
2] a model that additionally controlled for reproductive andormonal risk factors for UL, including age at menarcheyears), parity (0, 1, 2, 3, or �4 births), infertility, age at firstirth (years), years since last birth (�5, 5–9, 10–14, or15), and use of OCs (current, former, or never); and [3] aodel that additionally controlled for lifestyle and socioeco-
omic risk factors for UL that may be related to PCOS,ncluding BMI (�20, 20–24, 25–29, 30–34, or �35),hysician-diagnosed diabetes (no, yes without medication,r yes with medication), cigarette smoking (current, former,r never), current alcohol consumption (�1, 1–6, or �7rinks per week), education (�12, 13–15, 16, or �17 years),ncome (�$25,000, $25,001–$50,000, $50,001–$100,000,
$100,000, or missing income), marital status (married oriving with partner; divorced, separated, or widowed; oringle), occupation (white collar, nonwhite collar, not em-loyed or other employment, or missing occupation), andeographic region (Northeast, South, Midwest, and West).esults were stratified by “recency of Papanicolaou (Pap)
mear,” which we used as a proxy for gynecologic surveil-ance among participants.
Age was the strongest confounder of the PCOS and ULssociation, increasing the PCOS effect estimate by 13%hen included in the Cox model. When we assessed the
ndividual contribution of each covariate to the age-adjustedodel, those with the largest influence on the PCOS effect
stimate were parity and years since last birth (change in IRR
stimate, 6% and 7%, respectively).Vol. 87, No. 5, May 2007
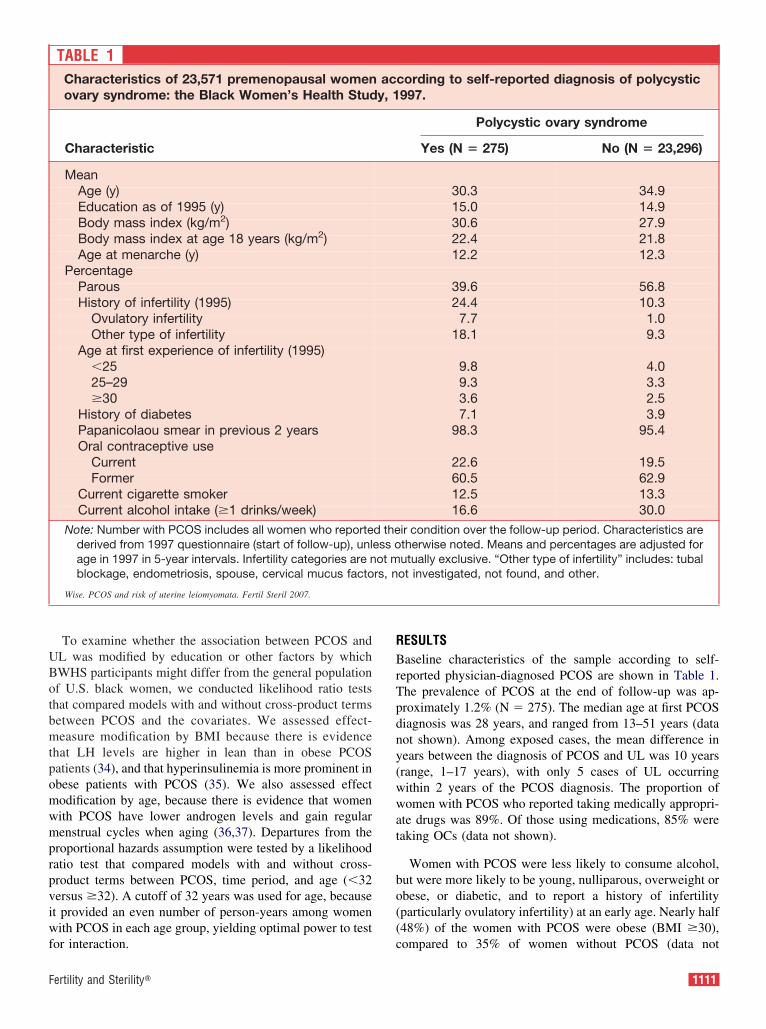
UBotbmtpomwmprpviwf
RBrTpdny(wwat
bo((
F
To examine whether the association between PCOS andL was modified by education or other factors by whichWHS participants might differ from the general populationf U.S. black women, we conducted likelihood ratio testshat compared models with and without cross-product termsetween PCOS and the covariates. We assessed effect-easure modification by BMI because there is evidence
hat LH levels are higher in lean than in obese PCOSatients (34), and that hyperinsulinemia is more prominent inbese patients with PCOS (35). We also assessed effectodification by age, because there is evidence that womenith PCOS have lower androgen levels and gain regularenstrual cycles when aging (36,37). Departures from the
roportional hazards assumption were tested by a likelihoodatio test that compared models with and without cross-roduct terms between PCOS, time period, and age (�32ersus �32). A cutoff of 32 years was used for age, becauset provided an even number of person-years among womenith PCOS in each age group, yielding optimal power to test
TABLE 1Characteristics of 23,571 premenopausal womenovary syndrome: the Black Women’s Health Stud
Characteristic
MeanAge (y)Education as of 1995 (y)Body mass index (kg/m2)Body mass index at age 18 years (kg/m2)Age at menarche (y)
PercentageParousHistory of infertility (1995)
Ovulatory infertilityOther type of infertility
Age at first experience of infertility (1995)�2525–29�30
History of diabetesPapanicolaou smear in previous 2 yearsOral contraceptive use
CurrentFormer
Current cigarette smokerCurrent alcohol intake (�1 drinks/week)
Note: Number with PCOS includes all women who reportederived from 1997 questionnaire (start of follow-up), unlage in 1997 in 5-year intervals. Infertility categories are nblockage, endometriosis, spouse, cervical mucus facto
Wise. PCOS and risk of uterine leiomyomata. Fertil Steril 2007.
or interaction. c
ertility and Sterility�
ESULTSaseline characteristics of the sample according to self-
eported physician-diagnosed PCOS are shown in Table 1.he prevalence of PCOS at the end of follow-up was ap-roximately 1.2% (N � 275). The median age at first PCOSiagnosis was 28 years, and ranged from 13–51 years (dataot shown). Among exposed cases, the mean difference inears between the diagnosis of PCOS and UL was 10 yearsrange, 1–17 years), with only 5 cases of UL occurringithin 2 years of the PCOS diagnosis. The proportion ofomen with PCOS who reported taking medically appropri-
te drugs was 89%. Of those using medications, 85% wereaking OCs (data not shown).
Women with PCOS were less likely to consume alcohol,ut were more likely to be young, nulliparous, overweight orbese, or diabetic, and to report a history of infertilityparticularly ovulatory infertility) at an early age. Nearly half48%) of the women with PCOS were obese (BMI �30),
cording to self-reported diagnosis of polycystic997.
Polycystic ovary syndrome
Yes (N � 275) No (N � 23,296)
30.3 34.915.0 14.930.6 27.922.4 21.812.2 12.3
39.6 56.824.4 10.37.7 1.0
18.1 9.3
9.8 4.09.3 3.33.6 2.57.1 3.9
98.3 95.4
22.6 19.560.5 62.912.5 13.316.6 30.0
ir condition over the follow-up period. Characteristics aretherwise noted. Means and percentages are adjusted forutually exclusive. “Other type of infertility” includes: tubalot investigated, not found, and other.
acy, 1
d theess oot mrs, n
ompared to 35% of women without PCOS (data not
1111

sgospp
dhiP1wtnwIwctoa6i
foU(
oP
vwowHeblIe1(
92atmpvwr0ra
hown). Women with and without PCOS had high levels ofynecologic surveillance (�95%), as indicated by the reportf a Pap smear in the previous 2 years. They were alsoimilar with respect to various indicators of socioeconomicosition, including education (Table 1), marital status, occu-ation, and income (data not shown).
During 114,373 person-years of follow-up, 3,631 inci-ent cases of UL, confirmed by ultrasound (N � 2,926) orysterectomy (N � 705), were reported (Table 2). Thencidence of UL was 65% higher among women withCOS than women without PCOS (fully adjusted IRR,.65; 95% CI, 1.21–2.24). The IRRs remained elevatedith increasing time after diagnosis of PCOS (test for
rend, P�.80), even among women �6 years after diag-osis. When we confined the exposed group to womenho were taking appropriate medications for PCOS, the
RR was 1.51 (95% CI, 1.08 –2.12). Results were similarhen analyses were restricted to women reporting a re-
ent PAP smear, a proxy for a pelvic examination. Amonghis subgroup, the IRR comparing women with and with-ut PCOS was 1.64 (95% CI, 1.20 –2.24). Results werelso similar when we included as part of the case group97 women who reported UL confirmed by pelvic exam-nation only (IRR, 1.57; 95% CI, 1.16 –2.12).
Because there is evidence that disease characteristicsor PCOS differ for lean and obese women, we stratifiedur analyses by BMI. The association between PCOS andL was stronger among lean women than obese women
TABLE 2Polycystic ovary syndrome and risk of uterine le1997–2003.
Cases co
CasesPerson-
yearsCru
IR
Overall 3,631 114,373 31PCOS
No 3,589 113,528 31Yes 42 845 49
Years after PCOS diagnosis�2 5 101 492–3 9 261 344–5 13 200 65�6 15 283 52
Test for ordinal trendNote: IR � incidence rate per 1,000 person-years, IRR �
adjusted for age and time period. Model 2 is additionallsince last birth, OC use, and infertility. Model 3 is additiosmoking, education, marital status, occupation, income
Wise. PCOS and risk of uterine leiomyomata. Fertil Steril 2007.
Table 3), but there was no statistical evidence of heter- P
1112 Wise et al. PCOS and risk of uterine leiomyomata
geneity across BMI categories (test for interaction,�.28).
The association between PCOS and UL appeared toary with age (data not shown), such that the associationas stronger among women who were 32 years of age orlder (IRR, 1.89; 95% CI, 1.31–2.72) compared withomen �32 years of age (IRR, 1.22; 95% CI, 0.69 –2.18).owever, the IRRs were not statistically different from
ach other (test for interaction, P�.24). The associationetween PCOS and UL was relatively uniform acrossevels of educational attainment (data not shown). TheRRs among women with �12, 13–15, and �16 years ofducation were 1.80 (95% CI, 0.65–5.00), 1.71 (95% CI,.00 –2.91), and 1.62 (95% CI, 1.07–2.43), respectivelytest for interaction, P�.88).
Associations were similar among women with (IRR, 1.72;5% CI, 0.83–3.55) and without (IRR, 1.68; 95% CI, 1.19–.36) a history of infertility, a condition that is positivelyssociated with both PCOS and UL. Because insulin resis-ance and hyperinsulinemia are mechanisms by which PCOSay increase the risk of UL, we evaluated the association of
hysician-diagnosed diabetes with UL. Diabetes was in-ersely associated with risk of UL. Compared with womenho never reported diabetes, fully adjusted IRRs for women
eporting diabetes with and without use of medication were.77 (95% CI, 0.60–0.98) and 0.91 (95% CI, 0.64–1.28),espectively. Adjustment for diabetes in the main multivari-ble models made little difference in the effect estimate for
omata in the Black Women’s Health Study,
med by ultrasound or hysterectomy
Model 1,IRR (95%CI)
Model 2,IRR (95%CI)
Model 3,IRR (95%CI)
1.00 (reference) 1.00 (reference) 1.00 (reference)1.82 (1.34–2.47) 1.64 (1.21–2.23) 1.65 (1.21–2.24)
1.83 (0.76–4.41) 1.66 (0.69–4.01) 1.67 (0.70–4.03)1.32 (0.69–2.55) 1.20 (0.62–2.31) 1.19 (0.62–2.29)2.47 (1.43–4.27) 2.18 (1.26–3.76) 2.20 (1.27–3.80)1.81 (1.093.00) 1.65 (0.99–2.75) 1.66 (1.00–2.76)
P�.80ence rate ratio, and CI � confidence interval. Model 1 isusted for age at menarche, parity, age at first birth, yearsadjusted for BMI, diabetes, current alcohol consumption,
d geographic region.
iomy
nfir
de
.7
.6
.7
.4
.5
.0
.9
incidy adjnally, an
COS.
Vol. 87, No. 5, May 2007

DIanrfTltt
tsgLsendatteef
b
obtpia
tlsccPtheewLvoweP
M
F
ISCUSSIONn the present study of African-American women, PCOS wasssociated with a 65% increase in the risk of UL. There waso evidence that time after diagnosis of PCOS influenced theisk of UL, suggesting that the association was not accountedor by detection of UL shortly after a diagnosis of PCOS.he association between PCOS and UL was stronger among
eaner women than obese women, and among older womenhan younger women, but these differences were not statis-ically significant.
Women with PCOS have several interrelated characteris-ics that may predispose them to UL, including insulin re-istance, increased serum IGF-I levels (38), hyperandro-enism, and altered gonadotropin dynamics (e.g., elevatedH levels) (2). If chronic hyperinsulinemia and insulin re-istance increase the risk of UL (15–17,19,20), one wouldxpect to find an association of diabetes with UL. We foundo such association; nor did we find any evidence thatiabetes modifies the association between PCOS and UL. Inddition, infertility, which may be influenced by PCOS (par-icularly ovulatory infertility), was not associated with UL inhe BWHS (39). The association between PCOS and UL wasvident after adjustment for infertility in multivariable mod-ls, and within subgroups of infertility, suggesting that in-ertility did not confound or modify the observed relation.
Prolonged anovulation represents one possible mechanism
TABLE 3Polycystic ovary syndrome and risk of uterine leHealth Study, 1997–2003.
Cases confir
CasesPerson-
yearsCrude
IR
BMI �25 (kg/m2)PCOS
No 1,302 42,424 30.7Yes 10 197 50.7
BMI 25–29 (kg/m2)PCOS
No 1,098 33,809 32.5Yes 17 253 67.1
BMI �30 (kg/m2)PCOS
No 1,189 37,295 31.9Yes 15 395 38.0
Note: IR � incidence rate per 1,000 person-years, IRRadjusted for age and time period. Model 2 is additionallsince last birth, OC use, and infertility. Model 3 is additioalcohol consumption, smoking, education, marital statu
Wise. PCOS and risk of uterine leiomyomata. Fertil Steril 2007.
y which PCOS may influence the risk of UL, because it is d
ertility and Sterility�
ften accompanied by continued secretion of E unopposedy P. Such an endogenous hormonal milieu may enhancehe development and growth of UL, and others haveostulated this to be the mechanism by which PCOSnfluences risk of endometrial cancer (2,40), which is also
hormone-dependent disease of the uterus.
Another plausible mechanism by which PCOS increaseshe risk of UL relates to hypersecretion of LH. Absoluteevels of circulating LH and their ratio to FSH levels areignificantly elevated in women with PCOS compared withontrols (34,41). Elevated LH concentrations (�95th per-entile of normal) are observed in �60% of women withCOS (42,43), and the LH:FSH ratio may be elevated in up
o 95% of nonovulating women with PCOS (34). LH mayave a direct effect on the uterus, independent of its influ-nce on the ovary (11,13,14). In addition, there is nowvidence in humans that high levels of LH are associatedith an increased risk of UL (12), and that suppression ofH and FSH with GnRH agonists can result in a reduction inolume of UL and significant uterine shrinkage (44,45). Ourbservation that the effect of PCOS is stronger among leanomen than obese women lends support to the LH hypoth-
sis, as levels of LH are highest among lean women withCOS (34).
A limitation of our study is that PCOS was self-reported.oreover, the definition of the disease itself continues to be
omata, according to BMI: the Black Women’s
by ultrasound or hysterectomy
Model 1,R (95% CI)a
Model 2,IRR (95% CI)b
Model 3,IRR (95% CI)c
0 (reference) 1.00 (reference) 1.00 (reference)9 (1.07–3.72) 1.95 (1.04–3.65) 1.97 (1.05–3.69)
0 (reference) 1.00 (reference) 1.00 (reference)0 (1.41–3.73) 2.04 (1.26–3.32) 2.07 (1.27–3.37)
0 (reference) 1.00 (reference) 1.00 (reference)8 (0.83–2.31) 1.29 (0.77–2.15) 1.29 (0.77–2.16)
cidence rate ratio, CI � confidence interval. Model 1 isusted for age at menarche, parity, age at first birth, yearsadjusted for BMI (continuous variable), diabetes, current
ccupation, income, and geographic region.
iomy
med
IR
1.01.9
1.02.3
1.01.3
� iny adjnallys, o
ebated among endocrinologists. The diagnosis of PCOS
1113

masp(dmnpbn
owncwresniiaFPrerpw
sWfdmm
frbtaMrc
wpastep
tttwpab
AAp
R
1
1
1
1
1
1
1
ay depend on the astuteness of the physician and thewareness of the patient herself. The lower prevalence ofelf-reported PCOS in our cohort (1.7%) compared with aopulation-based sample of reproductive-aged black women3.4%), who were screened using a widely accepted NIHefinition of PCOS (3), suggests that some underreportingay have occurred (5). Because UL had not yet been diag-
osed at the time of a woman’s PCOS diagnosis, underre-orting of PCOS in the present study would most likely haveeen random, and would have resulted in bias toward theull.
Women with PCOS typically seek medical care becausef menstrual dysfunction, hirsutism, and/or infertility. Ifomen with PCOS are more likely to undergo regular gy-ecologic screening relative to women without PCOS, thisould explain the increased incidence of UL among womenith PCOS. We attempted to minimize detection bias by
estricting our analyses to women who reported similar lev-ls of gynecologic surveillance, using “recency of Papmear” as a proxy for a pelvic examination. The results didot change appreciably. We also controlled for a variety ofndicators of socioeconomic position that may serve as prox-es for access to medical care, including education, income,nd occupation, but the results were not materially affected.inally, when we examined the number of years betweenCOS and UL diagnoses, we found no dramatic increase inisk for UL soon after the PCOS diagnosis, as would bexpected if increased surveillance completely explained theesults. Therefore, it is unlikely that our findings are ex-lained by increased incidental detection of UL amongomen with PCOS.
We validated the self-report of UL through a detailedupplementary questionnaire and review of medical records.
e were able to verify the diagnosis in �96% of the casesrom whom we obtained medical records. There was littleifference between those who did and did not release theiredical records with respect to reported symptomatology,ethod of diagnosis, or important risk factors for UL.
Women in the BWHS were not systematically screenedor UL. It is likely that data from the BWHS more accuratelyepresent the number of women with symptomatic tumors,ecause most cases in the validation survey reported symp-oms prior to the initial diagnosis of the disease, and because
low percentage of cases (13%) was detected incidentally.oreover, rates of UL diagnoses in the BWHS are similar to
ates reported in other U.S. studies based on prospectiveohort and hospital discharge data (31).
Although the BWHS is a convenience sample of womenith a higher level of education than the general population,revalence estimates of suspected risk factors for UL, i.e.,ge at menarche (46), parity (46), and body weight (47), areimilar to those found in nationally representative studies. Ashe association between PCOS and UL did not vary byducation, the present findings might extend to the general
opulation of U.S. black women.1114 Wise et al. PCOS and risk of uterine leiomyomata
Approximately 3,000,000 reproductive-aged women inhe United States have PCOS (5,6), and its association withhe development of several chronic diseases, such as diabe-es, cardiovascular disease, and endometrial cancer, has beenell-documented (2). Before UL can be added to the list ofossible health consequences of PCOS, the positive associ-tion observed in the present study will require confirmationy future studies.
cknowledgments: The authors acknowledge the feedback of Shafikabrahams-Gessel, M.S., and the ongoing contributions of the BWHSarticipants and staff.
EFERENCES1. Guzick D. Polycystic ovary syndrome: symptomatology, pathophys-
iology, and epidemiology. Am J Obstet Gynecol 1998;179(Suppl):S89 –93.
2. Guzick DS. Polycystic ovary syndrome. Obstet Gynecol 2004;103:181–93.
3. Zawadzki JK, Dunaif A. Diagnostic criteria for polycystic ovary syn-drome: towards a rational approach. In: Dunaif A, Givens JR, HaseltineFP, Merriam GR, eds. Polycystic ovary syndrome. Boston: Blackwell,1992:377–84.
4. The Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Work-shop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). HumReprod 2004;19:41–7.
5. Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR,Azziz R. Prevalence of the polycystic ovary syndrome in unselectedblack and white women of the southeastern United States: a prospectivestudy. J Clin Endocrinol Metab 1998;83:3078–82.
6. Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO.The prevalence and features of the polycystic ovary syndrome in anunselected population. J Clin Endocrinol Metab 2004;89:2745–9.
7. Rebuffe-Scrive M, Cullberg G, Lundberg PA, Lindstedt G, Bjorntorp P.Anthropometric variables and metabolism in polycystic ovarian dis-ease. Horm Metab Res 1989;21:391–7.
8. Dahlgren E, Friberg LG, Johansson S, Lindstrom B, Oden A, SamsioeG, et al. Endometrial carcinoma; ovarian dysfunction—a risk factor inyoung women. Eur J Obstet Gynecol Reprod Biol 1991;41:143–50.
9. Dahlgren E, Janson PO. Polycystic ovary syndrome: long-term effects.Ann Med 1993;25:307–8.
0. Dahlgren E, Janson PO, Johansson S, Lapidus L, Oden A. Polycysticovary syndrome and risk for myocardial infarction. Evaluated from arisk factor model based on a prospective population study of women.Acta Obstet Gynecol Scand 1992;71:599–604.
1. Shemesh M. Actions of gonadotrophins on the uterus. Reproduction2001;121:835–42.
2. Baird DD, Kesner JS, Dunson DB. Luteinizing hormone in premeno-pausal women may stimulate uterine leiomyomata development. J SocGynecol Invest 2006;13:130–5.
3. Tesarik J, Hazout A, Mendoza C. Luteinizing hormone affects uterinereceptivity independently of ovarian function. Reprod Biomed Online2003;7:59–64.
4. Stewart EA. Gonadotropins and the uterus: is there a gonad-independentpathway? J Soc Gynecol Invest 2001;8:319.
5. Burroughs KD, Howe SR, Okubo Y, Fuchs-Young R, LeRoith D,Walker CL. Dysregulation of IGF-I signaling in uterine leiomyoma.J Endocrinol 2002;172:83–93.
6. Giudice LC, Irwin JC, Dsupin BA, Pannier EM, Jin IH, Vu TH, et al.Insulin-like growth factor (IGF), IGF binding protein (IGFBP), and IGFreceptor gene expression and IGFBP synthesis in human uterine
leiomyomata. Hum Reprod 1993;8:1796–806.Vol. 87, No. 5, May 2007

1
1
1
2
2
2
2
22
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
F
7. Wolanska M, Bankowski E. An accumulation of insulin-like growthfactor I (IGF-I) in human myometrium and uterine leiomyomas invarious stages of tumour growth. Eur Cytokine Netw 2004;15:359–63.
8. Gloudemans T, Prinsen I, Van Unnik JA, Lips CJ, Den Otter W,Sussenbach JS. Insulin-like growth factor gene expression in humansmooth muscle tumors. Cancer Res 1990;50:6689–95.
9. Poretsky L, Kalin MF. The gonadotropic function of insulin. EndocrRev 1987;8:132–41.
0. Faerstein E, Szklo M, Rosenshein NB. Risk factors for uterine leiomy-oma: a practice-based case-control study. II. Atherogenic risk factorsand potential sources of uterine irritation. Am J Epidemiol 2001;153:11–9.
1. Boynton-Jarrett R, Rich-Edwards J, Malspeis S, Missmer SA, WrightR. A prospective study of hypertension and risk of uterine leiomyo-mata. Am J Epidemiol 2005;161:628–38.
2. Doi SAR, Al-Zaid M, Towers PA, Scott CJ, Al-Shoumer KAS. Irreg-ular cycles and steroid hormones in polycystic ovary syndrome. HumReprod 2005;20:2402–8.
3. Rosenberg L, Adams-Campbell LL, Palmer JR. The Black Women’sHealth Study: a follow-up study for causes and preventions of illness.J Am Med Wom Assoc 1995;50:56–8.
4. Stewart EA. Uterine fibroids. Lancet 2001;357:293–8.5. Wise LA, Palmer JR, Spiegelman D, Harlow BL, Stewart EA, Adams-
Campbell LL, et al. Influence of body size and body fat distribution onrisk of uterine leiomyomata in U.S. black women. Epidemiology 2005;16:346–54.
6. Ehrmann DA. Polycystic ovary syndrome. N Engl J Med 2005;352:1223–36.
7. Loutradis D, Antsaklis A, Creatsas G, Hatzakis A, Kanakas N, Go-ugoulakis A, et al. The validity of gynecological ultrasonography.Gynecol Obstet Invest 1990;29:47–50.
8. Dueholm M, Lundorf E, Hansen ES, Ledertoug S, Olesen F. Accuracyof magnetic resonance imaging and transvaginal ultrasonography in thediagnosis, mapping, and measurement of uterine myomas. Am J ObstetGynecol 2002;186:409–15.
9. Schwartz SM, Marshall LM. Uterine leiomyomata. In: Goldman MB,Hatch MC, eds. Women and health. San Diego, CA: Academic Press,2000:240–52.
0. Robboy SJ, Andersen MC, Russell P. Pathology of the female repro-ductive tract. London: Churchill Livingstone, 2002.
1. Wise LA, Palmer JR, Stewart EA, Rosenberg L. Age-specific incidencerates for self-reported uterine leiomyomata in the Black Women’sHealth Study. Obstet Gynecol 2005;105:563–8.
2. SAS Institute, Inc. SAS/STAT user’s guide, version 8.02. Cary, NC:SAS Institute, 2002.
3. Greenland S. Modeling and variable selection in epidemiologic analy-sis. Am J Public Health 1989;79:340–9.
4. Taylor AE, McCourt B, Martin KA, Anderson EJ, Adams JM, Schoen-
feld D, et al. Determinants of abnormal gonadotropin secretion inertility and Sterility�
clinically defined women with polycystic ovary syndrome. J ClinEndocrinol Metab 1997;82:2248–56.
5. Pasquali R, Casimirri F, Venturoli S, Antonio M, Morselli L, Reho S,et al. Body fat distribution has weight-independent effects on clinical,hormonal, and metabolic features of women with polycystic ovarysyndrome. Metabolism 1994;43:706–13.
6. Elting MW, Korsen TJ, Rekers-Mombarg LT, Schoemaker J. Womenwith polycystic ovary syndrome gain regular menstrual cycles whenageing. Hum Reprod 2000;15:24–8.
7. Bili H, Laven J, Imani B, Eijkemans MJ, Fauser BC. Age-related differ-ences in features associated with polycystic ovary syndrome in normogo-nadotrophic oligo-amenorrhoeic infertile women of reproductive years.Eur J Endocrinol 2001;145:749–55.
8. Berker B, Emral R, Demirel C, Corapcioglu D, Unlu C, Kose K.Increased insulin-like growth factor-I levels in women with polycysticovary syndrome, and beneficial effects of metformin therapy. GynecolEndocrinol 2004;19:125–33.
9. Wise LA, Palmer JR, Harlow BL, Spiegelman D, Stewart EA, Adams-Campbell LL, et al. Reproductive factors, hormonal contraception andrisk of uterine leiomyomata in African-American women: a prospectivestudy. Am J Epidemiol 2004;159:113–23.
0. Gadducci A, Gargini A, Palla E, Fanucchi A, Genazzani AR. Polycysticovary syndrome and gynecological cancers: is there a link? GynecolEndocrinol 2005;20:200–8.
1. Fauser BC, Pache TD, Lamberts SW, Hop WC, de Jong FH, Dahl KD.Serum bioactive and immunoreactive luteinizing hormone and follicle-stimulating hormone levels in women with cycle abnormalities, with orwithout polycystic ovarian disease. J Clin Endocrinol Metab 1991;73:811–7.
2. van Santbrink EJ, Hop WC, Fauser BC. Classification of normogona-dotropic infertility: polycystic ovaries diagnosed by ultrasound versusendocrine characteristics of polycystic ovary syndrome. Fertil Steril1997;67:452–8.
3. Laven JS, Imani B, Eijkemans MJ, Fauser BC. New approach topolycystic ovary syndrome and other forms of anovulatory infertility.Obstet Gynecol Surv 2002;57:755–67.
4. Nakamura Y, Yoshimura Y, Yamada H, Ubukata Y, Ando M, SuzukiM. Treatment of uterine leiomyomata with a luteinizing hormone-releasing hormone agonist: the possibility of nonsurgical managementin selected perimenopausal women. Fertil Steril 1991;55:900–5.
5. Stewart EA, Friedman AJ. Steroidal treatment of myomas: preoperativeand long-term medical therapy. Semin Reprod Endocrinol 1992;10:344–57.
6. Abma JC, Chandra A, Mosher WD, Peterson LS, Piccinino LJ. Fertil-ity, family planning, and women’s health: new data from the 1995National Survey of Family Growth [Series 23, No. 9]. Vital Health Stat1997;23:19.
7. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trendsin obesity among US adults, 1999–2000. J Am Med Assoc 2002;288:
1723–7.1115

Ufapfim
RT
T
R
REPRODUCTIVE ENDOCRINOLOGY
The progesterone receptor gene polymorphism,PROGINS, may be a factor related to the developmentof uterine fibroidsMariano Tamura Vieira Gomes, Ph.D., Rodrigo de Aquino Castro, Ph.D.,Fabiola Elizabeth Villanova, M.S., Ismael Dale Cotrim Guerreiro da Silva, Ph.D.,Edmund Chada Baracat, Ph.D., Geraldo Rodrigues de Lima, Ph.D., andManoel João Batista Castello Girão, Ph.D.
Department of Gynecology, Universidade Federal de São Paulo, São Paulo, Brazil
Objective: To assess the possible association between the polymorphic allele of the progesterone receptor gene,named PROGINS, and uterine leiomyomas.Design: Case–control study.Setting: Department of Gynecology. Teaching hospital.Patient(s): One hundred twenty-two premenopausal women with fibroids and 125 postmenopausal controls notpresenting the disease.Intervention(s): The subjects were classified as White or non-White (Black and Mulatto) and the progesteronereceptor genotyping was performed, with DNA extracted from uterus in cases and from peripheric blood incontrols and submitted to polymerase chain reaction (PCR) and agarose gel electrophoresis.Main Outcome Measure(s): The presence of the PROGINS allele was recorded, and its frequency as well as thegenotypic distribution among cases and controls were compared according to race.Result(s): PROGINS-positive genotypes (heterozygous or mutant homozygous) were found in 19% of White and11% of non-White women, and allelic frequency of PROGINS in the groups was 10.4% and 6.2%, respectively.Comparing patients and controls, we observed a significant difference among non-White women, both regardingpresence of PROGINS-positive genotypes (4.9% vs. 25%, respectively), and PROGINS allele frequency (3.3%vs. 12.5%, respectively). There was no significant difference in PROGINS-positive genotypes among White casesand controls (16.4% vs. 20.6%, respectively), and in their allelic frequency (8.2% vs. 11.9%, respectively). Theodds ratio showed reduced risk of fibroids related to PROGINS-positive genotypes in non-White women (oddsratio � 0.16, 95% confidence interval: 0.04–0.66), but not among White subjects (odds ratio � 0.76, 95%confidence interval: 0.33–1.74).Conclusion(s): The PROGINS polymorphism revealed to be protective in terms of uterine fibroids in Braziliannon-White women. (Fertil Steril� 2007;87:1116–21. ©2007 by American Society for Reproductive Medicine.)
Key Words: Uterine fibroids, uterine leiomyoma, risk factors, sexual steroids receptors, progesterone receptor,polymorphism, PROGINS
tbpmil(p
lii
terine fibroid is the most frequent benign neoplasm of theemale reproductive system in the premenopause, and affectst least 30% of those aged over 30 years (1). It has a higherrevalence in Black individuals, and is more frequent amongrst-degree relatives in families with two or more affectedembers (2, 3). Although estrogen is considered a major
eceived April 11, 2006; revised and accepted August 21, 2006.his article was funded by Fundação de Amparo à Pesquisa do Estado deSão Paulo (FAPESP) Grant 03/04533-1.
here are not any financial or other interests regarding the submittedmanuscript that might be construed as a conflict of interest.
eprint requests: Mariano Tamura Vieira Gomes, Ph.D., Avenida Ibi-rapuera, 2907, conjunto 406, São Paulo/SP 04029-200, Brazil (FAX:55-11-50424848; E-mail: [email protected]; marianotamura@
eterra.com.br).
1116 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
umor promoter, there is evidence indicating the role playedy progesterone, through interaction with its cell receptors,ositively modulating the mitotic activity, propagating so-atic mutations, and stimulating tumor growth (4, 5). There
s a single progesterone receptor (PR) gene in humans,ocated in the long arm of chromosome 11, in bands 22–2311q22–23), and it is responsible for translation of tworotein isoforms, PR-A and PR-B (6).
Recently, some genotypic variations were described, high-ighting the PROGINS polymorphism, which is a mutationdentified in the PR gene consisting of a 306 base pairs (bp)nsertion of PV/HS-1 Alu subfamily in intron G, between
xons 7 and 8—codifying region of hormone binding0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.099

dawac(cvtPeGu
MPWtd[c
wfimBy4phgTcuwBAzct(
MIrsppbvbTm(eo
IpaDsbgs(tfv
pPATD0m2TPll5f5rsh
aoH(tiim
STtaBthtHsev
F
omain—a silent mutation in exon 5 (C¡T) and a singlemino acid change from exon 4 (Val¡Leu). Such insertionould lead to anomalous transcription and codification of an
lternative exon 8, with consequent loss of hormone bindingapacity and receptor activity in response to progesterone7–9). The presence of this polymorphism was previouslyompared among 21 different populations, and its prevalencearied from zero in two African groups (!Kung and Nguni)o 22% in the Greek Cypriot group, with an averageROGINS allele frequency of 11% and an average het-rozigosity of 18.8% (10). Hence, the presence of the PRO-INS allele as a possible risk or protection factor regardingterine leiomyomas was evaluated in Brazilian women.
ATERIALS AND METHODSatientse carried out a case-control study, which was approved by
he Institutional Review Board of the Universidade Federale São Paulo/Escola Paulista de Medicina (UNIFESP/EPM)Medical School]. All the participants signed an informedonsent form.
The case group was composed of 122 premenopausalomen with diagnosis of symptomatic uterine fibroid (con-rmed by histopathology) and indication of surgical treat-ent, seen at a teaching hospital in the City of São Paulo/razil, from 2002 to 2004. The mean age was 43.9 � 7.3ears, and the mean uterine volume on ultrasonography was29.8 � 293.4 cm3. For the control group, 125 postmeno-ausal volunteers seen during the same period at the sameospital were recruited. All were clinically and ultrasono-raphically evaluated, ruling out the presence of fibroids.he mean age was 56.9 � 7.4 years, with menopause oc-urring at 48.1 � 5.1 years, and the mean uterine volume onltrasound was 38.1 � 21.7 cm3. As to race, the subjectsere classified as white or non-White—a group comprisinglacks and Mulattos. The term non-White refers to thefrican inheritance present in the composition of the Bra-
ilian population and to the intense racial miscegenationharacteristic of our country that hinders a precise differen-iation among ethnic groups based on their physical features11).
ethodsn the case group, a 1 cm3 fragment of the uterine tissue wasemoved during hysterectomy or myomectomy, and pre-erved at �80°C up to DNA extraction. To this end, aortion of the extracted tissue was placed in 100 �L ofroteinase K digestion buffer, and this material was incu-ated at 50°C, for 12 hours. Later, proteinase K was inacti-ated for 15 minutes at 70°C and 500 �L of GFX kit lysisuffer (Amersham Biosciences Piscataway, NJ) was added.he lysate obtained was centrifuged at 5.4 g/4°C (Eppendorfodel 5804 R) for 1 minute in a chromatographic column
silica). After two washing and centrifugation stages withthanol-containing buffers, the DNA was diluted in 100 �L
f milli-Q water, preheated at 70°C. wertility and Sterility�
The purified DNA was stored at �80°C up for further use.n the control group, 5 mL of blood were withdrawn byeripheral venous puncture, using a vacutainer with antico-gulant solution (EDTA). Immediately after, the genomicNA was extracted using the GFX kit (Amersham Bio-
ciences) by adding 500 �L of lysis buffer to 100 �L oflood. The same procedures described above for the caseroup were later performed. The amount of DNA was mea-ured by purified DNA aliquot spectrophotometry (260 nm)Spectronic, model Genesys 5). The polymerase chain reac-ion (PCR) was carried out using oligonucleotides (primers)or �-globin, which was considered as positive control toerify quality of DNA and efficacy of amplification (12).
The following primers were used in the PCR of therogesterone receptor gene for amplification and detection ofROGINS—sense: 5= GGC AGA AAG CAA AAT AAAAG A 3= and antisense: 5= AAA GTA TTT TCT TGCAA ATG TC 3= (8, 13). Two microliters (100 ng) of totalNA were used in a final 25 �L reaction volume containing.4 pmol/�L of each primer and 22 �L of mix Promega (20M of Tris–HCl pH 8.4, 50 mM of KCL, 5 mM of MgCl2,
00 �M of dNTPs, and 1.25 U of Taq DNA polymerase).he reactions were incubated in a thermocycler (GeneAmpCR System 9700, Perkin Elmer, Norwalk, CT) in the fol-
owing conditions: denaturation at 94°C for 5 minutes, fol-owed by 40 cycles at 94°C for 1 minute (denaturation),5°C for 1 minute (oligonucleotid hybridization), and 72°Cor 1 minute (polymerization), finally incubated at 72°C for
minutes. The amplification products were applied in aga-ose gel 2%, stained with ethidium bromide (1 �g/mL), andubmitted to electrophoresis for 20 minutes at 100 volts, in aorizontal cube containing TBE buffer 1�.
Detection was made by visualization of PCR products ingarose gel in an ultraviolet light transiluminator. They could bef two different sizes, depending on the presence of Alu PV/S-1 insertion of 306 bp into intron G, between exons 7 and 8
PROGINS). If the progesterone receptor gene did not presenthe insertion, a 149-bp fragment would be obtained, represent-ng the wild-type allele (T1); however, if the gene had thensertion, the fragment would have 455 bp, corresponding to theutant or polymorphic allele (T2) (8, 14).
tatisticshe PROGINS allele frequency and its genotypic distribu-
ion were compared among White and non-White womennd between the case and control groups according to race.ecause there were few mutant homozygous in our series,
he PROGINS-positive genotypes (heterozygous and mutantomozygous) were analyzed together in the comparison withhe PROGINS-negative genotype (wild homozygous).ence, the chi-square frequency test was applied, with a
ignificance level of 5% (P�.05). The risk to the disease wasstimated by odds ratio (OR), using the software SPSS,ersion 11.0, and the confidence interval (CI) established
as 95% (95% CI). Finally, based on the found PROGINS1117

atttrTtba
RTecgPmWrpoo
ivf2P(p(bWaP
DPfec1eat
llele frequency, we compared the real genotypic distribu-ion with the expected rates in all subgroups. This distribu-ion, if in Hardy-Weinberg equilibrium, should be close tohe following: wild homozygous rate � T12/heterozygousate � 2 � T1 � T2/mutant homozygous rate � T22 (15).he purpose of the Hardy-Weinberg calculation is to certify
hat the results obtained do not carry any sample or specimenias, because a representative population, studied by theppropriate means, usually respects the equilibrium.
ESULTShe genotypic distribution remained in Hardy-Weinbergquilibrium in the whole series, and in the case-White,ase-non-White, control-White and control-non-White sub-roups (data not shown). Considering all subjects,ROGINS-positive genotypes (heterozygous or mutant ho-ozygous) were found in 19% of White and 11% of non-hite, with PROGINS allele frequency of 10.4% and 6.2%,
espectively (P�.11) (Table 1). Among controls, PROGINS-ositive genotypes were present in 20.6% of White and 25%f non-White (P�0.62). Comparing patients to controls, webserved a significant difference in the non-White subgroup,
TABLE 1Genotypic distribution and allelic frequency per r
Variable Category White n �
Genotypes T1/T1 128 (8T1/T2 27 (1T2/T2 3 (1
Genotypes T1/T1 128 (8T1/T2 and T2/T2 30 (1
Alleles T1 283 (8T2 33 (1
Gomes. PROGINS protects against fibroids. Fertil Steril 2007.
TABLE 2Genotypic distribution and allelic frequency for n
Variable Category Case n
Genotypes T1/T1 58T1/T2 2T2/T2 1
Genotypes T1/T1 58T1/T2 and T2/T2 3
Alleles T1 118T2 4
Gomes. PROGINS protects against fibroids. Fertil Steril 2007.
1118 Gomes et al. PROGINS protects against fibroids
n terms of presence of PROGINS-positive genotypes (4.9%s. 25%, respectively) (P�.01), and of polymorphic allelerequency (3.3% vs. 12.5%, respectively) (P�.038) (Table). For White women, there was no significant difference inROGINS-positive genotypes between cases and controls16.4% vs. 20.6%, respectively) (P�.51), as well as inolymorphic allele frequency (8.2% vs. 11.9%, respectively)P�.30) (Table 3). The OR indicated risk reduction of fi-roid related to PROGINS-positive genotypes among non-hite (OR � 0.16, 95% CI: 0.04–0.66, P�.01), but not
mong White females (OR � 0.76, 95% CI: 0.33–1.74,�.51) (Table 4).
ISCUSSIONROGINS polymorphism has been considered a risk factoror some benign and malignant gynecologic diseases, such asndometriosis (9), hyperprolactinemia (16), and ovarian can-er (8, 13, 14), and a protective factor to breast cancer (13,7). Apparently, this variant leads to encoding an alternativexon 8 in PR gene, and consequently, to expression of anberrant form of progesterone receptor, with impaired pro-ein interaction and hormone regulation properties, as well as
, for all subjects.
Race
P value8 (%) Non-White n � 89 (%)
) 79 (88.8) .323) 9 (10.1)
1 (1.1)) 79 (88.8) .112) 10 (11.2)) 167 (93.8) .110) 11 (6.2)
White cases and controls.
Group
P value1 (%) Control n � 28 (%)
.1) 21 (75.0) .004) 7 (25.0)) 0 (0.0).1) 21 (75.0) .010) 7 (25.0).7) 49 (87.5) .038) 7 (12.5)
ace
15
1.07.1.9)1.09.09.60.4
on-
� 6
(95(3.3(1.6(95(4.9(96(3.3
Vol. 87, No. 5, May 2007

lravspPpatswa
atatmKi4cga(
tWtwaa(mrfiptebcopwnit
amn
F
oss of binding capacity and transcriptional activation inesponse to progesterone (14). Because sexual steroids play
role in controlling the myometrial metabolism, geneticariations related to these hormones raise interest in thetudy of uterine fibroids. It is known that progesterone androgestins act in cells through their receptors (PR-A andR-B), which originate from the PR gene (18). It has beenut forward that PR-B homodimers would mediate hormonection, whereas the truncated variant PR-A would inhibitranscription (19–21). Therefore, Fabjani et al. (17), in 2002,uggested that the PR-A, when associated with PROGINS,ould have higher stability and inhibit more intensely the
ction mediated by PR-B in target genes.
Polymorphisms are inherited genetic variations present inll cells (germinative or somatic, healthy or impaired), andheir prevalence varies in different populations. Thus, anymplified cell lineage would be representative for studyinghe body. However, chromosome alterations and geneticutations may occur in somatic cells, particularly in tumors.nown deletions, translocations and rearrangements involv-
ng chromosomes 3, 6, 7, 10, 12, and 14 are found in up to0% of fibroids (22, 23). This fact does not interfere in ourhoice of uterine tissue as biologic material in the caseroup, because these alterations, when present, do not affectll cells of a certain nodule (24), and spare chromosome 11site of the PR gene).
TABLE 3Genotypic distribution and allelic frequency for W
Variable Category Case n
Genotypes T1/T1 51T1/T2 10T2/T2 0
Genotypes T1/T1 51T1/T2 and T2/T2 10
Alleles T1 112T2 10
Gomes. PROGINS protects against fibroids. Fertil Steril 2007.
TABLE 4Risk of uterine fibroids in relation to different PR
Race Genotypes
White T1/T1T1/T2 � T2/T2
Non-White T1/T1T1/T2 � T2/T2
Note: CI � confidence interval, OR � odds ratio.
Gomes. PROGINS protects against fibroids. Fertil Steril 2007.
ertility and Sterility�
Even so, if there were any somatic alterations involvinghe PR gene locus (11q22–23), a deviation in the Hardy-
einberg equilibrium testing would be expected in geno-ypic distribution, with reduction of heterozygous genotypeshen eliminating one of the alleles (which was not found in
ny group or subgroup), or no visualization of the bands aftergarose gel electrophoresis when eliminating two alleleswhich did not occur in any subject). Moreover, it is worthentioning that the product of PCR amplification in cases
epresents the DNA of all present cells, such as leucocytes,broblasts, and normal myometrium, besides some neo-lastic cells. If there were a somatic mutation in thisissue—with insertion of 306 bp of the Alu family, gen-rating the polymorphic allele PROGINS—there woulde a higher prevalence of this variant in the case groupompared to controls, and not a lower prevalence, asbserved. Previous comparisons of the presence of otherolymorphisms in blood, myometrium, or leyomiomaere conducted by several investigators (25–27), who didot find differences in these tissues, thus corroborating thedea that the DNA we obtained provides reliable resultshat represent the body cells.
Having postmenopausal and asymptomatic women with neg-tive ultrasound screening as controls provides better approxi-ation of a group truly not affected by uterine fibroids and with
o risk of developing the condition in the future. Although the
e cases and controls.
Group
P value1 (%) Control n � 97 (%)
.6) 77 (79.4) .472
.4) 17 (17.5)) 3 (3.1).6) 77 (79.4) .510.4) 20 (20.6).8) 171 (88.1) .300) 23 (11.9)
notypes per race.
OR (95% CI) P value
1.0 .510.76 (0.33–1.74)
1.0 .010.16 (0.04–0.66)
hit
� 6
(83(16(0.0(83(16(91(8.2
ge
1119

coswlpt
PBDtcfisBhwpfiwambj
MIdIotpw(er
fitafiaalaaPipmp
R
1
1
1
1
1
1
1
1
1
1
2
2
linical and ultrasonographic exams could not completely ruleut the existence of a neoplasm because there might be micro-copic lesions, it should be noted that the accidental presence ofomen with fibroids in the control group would reduce the
ikelihood of finding an association (positive or negative) ofolymorphism and the condition. This makes the results ob-ained even more relevant.
We observed in our series a different prevalence ofROGINS among Brazilian White and non-White (Mulatto andlack) women, which is in agreement with a study presented byonaldson et al. (10), in 2002, but this difference is not statis-
ically significant. Nevertheless, when we consider only theontrols—excluding the uterine fibroid factor—the non-Whiteemales presented an allelic frequency of PROGINS very sim-lar to White women (12.5% vs. 11.9%, respectively). Thus, weuppose that the less frequent presence of this polymorphism inlacks, as previously registered (10), could be associated to theigher prevalence of fibroids in this racial group. In our series,hen assessing only non-White subjects, we observed markedrotection of PROGINS in terms of occurrence of uterinebroids. The same results were not found for White women,ho did not present any association between polymorphism
nd presence of the disease. The sample size studied, theultifactorial nature of this illness, as well as its biologic
ehavior plurality, especially in distinct ethnic groups, mayustify these findings.
The presence of PROGINS was previously analyzed byassart et al. (28) and by Hsieh et al. (16), among White
talian and Chinese women, respectively. Both investigatorsid not find differences among fibroid patients and controls.t should be emphasized, as mentioned by the investigatorsf the Italian study, that their results may not be extrapolatedo other ethnic groups, excluding the possibility of thisolymorphism be a risk or protection marker in populationsith other characteristics (28). In the study by Hsieh et al.
16), the population chosen as control was still in the prem-nopause, at risk of developing the disease in the future, thuseducing accuracy of results presented.
We consider PROGINS allele as a protection marker forbroids among Brazilian non-White females, and suggest
his polymorphism may protect women by means of smallerction of progesterone in target genes. However, this is therst investigation to point out the existence of this relationnd further studies with different populations are essential,s well as investigations that definitely determine the bio-ogic role of PROGINS, because the association of certainlleles or genotypes with a disease does not necessarily meann etiologic relation. Because we suppose the presence of theROGINS allele would be really protective, it would be
nteresting to carry out studies with sufficiently large sam-les, so that we could separately analyze the role of theutant homozygous genotype (less prevalent) and check if it
rovides greater protection than the heterozygous genotype.
1120 Gomes et al. PROGINS protects against fibroids
EFERENCES1. Marshall LM, Spiegelman D, Barbieri RL, Goldman MB, Manson JE,
Colditz GA, et al. Variation in the incidence of uterine leiomyomaamong premenopausal women by age and race. Obstet Gynecol 1997;90:967–73.
2. Kjerulff KH, Guzinski GM, Langenberg PW. Hysterectomy and race.Obstet Gynecol 1993;82:757–64.
3. Vikhlyaeva EM, Khodzhaeva ZS, Fantschenko ND. Familial predispo-sition to uterine leiomyomas. Int J Gynecol Obstet 1995;51:127–31.
4. Rein MS, Barbieri RL, Friedman AJ. Progesterone: a critical role in thepathogenesis of uterine myomas. Am J Obstet Gynecol 1995;172:14–8.
5. Rein MS. Advances in uterine leiomyoma research: the progesteronehypothesis. Environ Health Perspect 2000;108(Suppl 5):791–3.
6. Rousseau-Merk MF, Mirashi M, Loosfelt H, Milgrom E, Berger R.Localization of the human progesterone receptor gene to chromosome11q22–23. Hum Genet 1987;77:280–2.
7. Vegeto E, Allan GF, Schrader WT, Tsai M-J, McDonnell DP, O’MalleyBW. The mechanism of RU 486 antagonism is dependent upon theconformation of the carboxy-terminal tail of the human progesteronereceptor. Cell 1992;69:703–13.
8. McKenna NJ, Kieback DG, Carney DN, Fanning M, McLinden J,Headon DR. A germline TaqI restriction fragment length polymor-phism in the progesterone receptor gene in ovarian carcinoma. Br JCancer 1995;71:451–5.
9. Wieser F, Scheneeberger C, Tong D, Tempfer C, Huber JC, Wenzi R.PROGINS receptor gene polymorphism is associated with endometri-osis. Fertil Steril 2002;77:309–12.
0. Donaldson CJ, Crapanzano JP, Watson JC, Levine EA, Batzer MA.PROGINS Alu insertion and human genomic diversity. Mutat Res2002;501:137–41.
1. Parra FC, Amado RC, Lambertucci JR, Rocha J, Antunes CM, PenaSDJ. Color and genomic ancestry in Brazilians. Proc Natl Acad SciUSA 2003;100:177–82.
2. Gattas GJF, Soares-Vieira JA. Cytochrome P450-2E1 and glutathione Stransferase polymorphisms among caucasians mulattoes from Brazil.Occup Med 2000;50:508–11.
3. Lancaster JM, Berchuck A, Carney ME, Wiseman R, Taylor JA.Progesterone receptor gene polymorphism and risk for breast andovarian cancer. Br J Cancer 1995;71:341–5.
4. Rowe SM, Coughlan SJ, McKenna NJ, Garret E, Kieback DG, CarneyDN, et al. Ovarian carcinoma-associated TaqI restriction fragmentlength polymorphism in intron G of the progesterone receptor gene isdue to an Alu sequence insertion. Cancer Res 1995;55:2743–5.
5. Nussbaum RL, McInnes RR, Willard HF. Thompson & Thompsongenetics in medicine. 6th rev. ed. Philadelphia: WB Saunders, 2001:83–95.
6. Hsieh YY, Chan IP, Wang HI, Chang CC, Huang CW, Lin CS.PROGINS Alu sequence insertion is associated with hyperprolactinae-mia but not leiomyoma susceptibility. Clin Endocrinol 2005;62:492–7.
7. Fabjani G, Tong D, Czerwenka K, Schuster E, Speiser P, Leodolter S,et al. Human progesterone receptor gene polymorphism PROGINS andrisk for breast cancer in Austrian women. Breast Cancer Res Treat2002;72:131–7.
8. Kastner P, Krust A, Turcotte B. Two distinct estrogen-regulated promotersgenerate transcripts encoding the two functionally different human proges-terone receptor forms A and B. EMBO J 1990;9:1603–14.
9. Vegeto E, Shahbaz MM, Wen DX. Human progesterone receptor Aform is a cell- and promoter-specific repressor of human progesteronereceptor B function. Mol Endocrinol 1993;7:1244–55.
0. Attia GR, Zeitoun K, Edwards D, Johns A, Carr BR, Bulun SE.Progesterone receptor form A but not B is expressed in endometriosis.J Clin Endocrinol Metab 2000;85:2897–902.
1. Mulac-Jericevic B, Mullinax RA, DeMayo FJ, Lydon JP, Coneely OM.Subgroup of reproductive functions of progesterone mediated by pro-
gesterone receptor-B isoform. Science 2000;289:1751–4.Vol. 87, No. 5, May 2007

2
2
2
2
2
2
2
F
2. Rein MS, Friedman AJ, Barbieri RL, Pavelka K, Fletcher JA, MortonCC. Cytogenetic abnormalities in uterine leiomyomata. Obstet Gynecol1991;77:923–6.
3. Mantovani MS, Neto JB, Philbert PM, Casartelli C. Multiple uterineleiomyomas: cytogenetics analysis. Gynecol Oncol 1999;72:71–5.
4. Marshal RD, Fejzo MLS, Friedman AJ, Mitchner N, Nowak RA,Rein MS, et al. Analysis of androgen receptor DNA reveals theindependent clonal origin of uterine leiomyoma and secondary na-ture of cytogenetic aberrations in the development of leiomyomata.Gen Chrom Cancer 1994;11:1– 6.
5. Gloudemans T, Pospiech I, Van Der Ven LTM, Lips CJM, Den Otter
W, Sussenbach JS. An AvaII restriction fragment length polymorphismertility and Sterility�
in the insulin-like growth factor II gene and the occurrence of smoothmuscle tumors. Cancer Res 1993;53:5754–8.
6. Patrikis MI, Bryan EJ, Thomas NA, Rice GE, Quinn MA, Baker MS,et al. Mutation analysis of the CDP, TP53, and KRAS in uterineleiomyomas. Mol Carciong 2003;37:61–4.
7. Al-Hendy A, Salama AS. Catechol-O-Methyltransferase polymorphismis associated with increased uterine leiomyoma risk in defferent ethnicgroups. J Soc Gynecol Investig 2006;13:136–44.
8. Massart F, Becherini L, Marini F, Noci I, Piciocchi L, Del Monte F, etal. Analysis of estrogen receptor (ER� and ER�) and progesteronereceptor (PR) polymorphisms in uterine leiomyomas. Med Sci Monit
2003;9:BR25–30.1121

Hdiwwca(t
cohdtnow
RSR
Ovarian response to the human chorionicgonadotrophin stimulation test in normal ovulatorywomen: the impact of regressing corpus luteumIlkka Y. Järvelä, M.D.,a Maarit Niinimäki, M.D.,a Hannu Martikainen, M.D.,a
Aimo Ruokonen, M.D.,b and Juha S. Tapanainen, M.D.a
a Departments of Obstetrics and Gynecology and b Clinical Chemistry, Oulu University Hospital, Oulu, Finland
Objective: To evaluate the impact of the regressing corpus luteum on the hormone secretion during hCGstimulation. The hCG stimulation test in the early follicular phase has been used to assess the capacity of theovarian theca cells to secrete steroids.Design: A prospective observational study.Setting: University hospital.Patient(s): The study group consisted of 11 women with confirmed ovulation in the past cycle (corpus luteumpositive [CL�]) and the control group of 11 women using oral contraceptive pills (OC; no CL).Intervention(s): An hCG test (5,000 IU IM) was performed 2 to 4 days after menstrual bleeding, and the ovarianresponse was measured at 0, 48, and 96 hours after injection.Main Outcome Measure(s): Changes in serum concentrations of P, 17-hydroxyprogesterone (17-OHP), andro-stenedione (A), T, E2, and vascular endothelial growth factor (VEGF), and in ovarian vasculature and volume(three-dimensional power Doppler ultrasonography) were measured.Result(s): Secretion of P and 17-OHP increased after hCG injection in the CL group, whereas no change wasobserved in women on OCs (P � .001). Concomitant increases were observed in volume and vasculature of theovary with a CL (P�.05), but not in the contralateral ovary or in women on OCs. The changes in volume andvasculature correlated with levels of P and 17-OHP (P�.05).Conclusion(s): The regressing corpus luteum from the past menstrual cycle reactivates and secretes steroids inresponse to hCG stimulation performed during the early follicular phase, which should be taken into accountwhen comparing hormone profiles of ovulatory and anovulatory women. (Fertil Steril� 2007;87:1122–30. ©2007by American Society for Reproductive Medicine.)
Key Words: 17-OHP, progesterone, three-dimensional power Doppler, vasculature, VEGF
pb
ahamprpi9s
bibnttc
yperandrogenism associated with polycystic ovary syn-rome (PCOS) results from an intrinsic abnormality in ovar-an theca cell steroidogenesis (1, 2). Cultured theca cells,hich have been isolated from antral follicles in patientsith PCOS, show markedly increased steroidogenesis in
omparison with theca cells from normal ovaries (1, 2). Inddition to cell cultures, both hCG (3–10) and GnRH agonist5, 11–13) stimulation tests have been used in vivo to assesshe hyperandrogenism in PCOS.
In women with PCOS, hCG stimulation induces an in-rease in 17-hydroxyprogesterone (17-OHP), androstenedi-ne (A), T, and E2 secretion (5–7, 9). Particularly, 17-OHPyperresponsiveness to hCG has been interpreted as an in-ication of cytochrome P450c17� overactivity and charac-eristic for PCOS (4–7, 9). The 17-OHP hyperresponsive-ess in PCOS seems to be related to the increased numberf antral follicles, because in addition to anovulatoryomen with PCOS, regularly menstruating women with
eceived April 27, 2006; revised and accepted August 7, 2006.upported by a grant from The Finnish Medical Foundation (I.Y.J.).eprint requests: Ilkka Y. Järvelä, M.D., Department of Obstetrics andGynecology, Oulu University Hospital, P.O. Box 5000, FIN-90014 Oulu,
pFinland (FAX: 35-84-08-20-8478; E-mail: [email protected]).
1122 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
olycystic-appearing ovaries respond to hCG stimulationy extended 17-OHP secretion (4).
Regularly ovulating and menstruating women have usu-lly acted as a control group for PCOS women (3–10). TheCG stimulation test has been performed either immediatelyfter the start of menstrual bleeding (3, 5, 6, 8–10) or in theidfollicular phase (4, 7) to stimulate only the antral follicle
ool but not the dominant follicle nor the corpus luteum. Inegularly menstruating women hCG also stimulates steroidroduction, but the response is much lower (5–7, 10). Thencrease in the 17-OHP level takes place more slowly (3–7,, 10); nevertheless, it eventually seems to exceed that ob-erved in women with PCOS (6, 9, 10).
When regularly menstruating women have been stimulatedoth after an ovulatory cycle and after a GnRH agonist–nduced anovulatory cycle, the steroidogenic response haseen different (4, 8). The increase in 17-OHP secretionearly disappears during hCG stimulation after the anovula-ory cycle (4, 8). The most obvious ovarian difference be-ween these stimulation cycles is the lack of regressingorpus luteum after an anovulatory cycle. Therefore it is
ossible that when the response to hCG stimulation is as-0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.114

swsn
rwowo
MPT1wcmopctoCtq
aU
HAdlscEca
ASaBNflRCObVae
w5fTw
F
essed in the early follicular phase in regularly ovulatingomen, the corpus luteum from the previous cycle starts
ecreting hormones and the steroidogenic profile observed isot entirely produced by the antral follicles only.
The main goal here was to assess the steroidogenicesponse to hCG stimulation in two groups of normalomen, the first one consisting of women with confirmedvulation in the past menstrual cycle and the other one ofomen with past anovulatory cycle caused by the use ofral contraceptives.
ATERIALS AND METHODSatientswo groups of women were recruited. Group 1 consisted of1 women with regular menstrual cycles (28 to 35 days)ithout any kind of hormonal medication. In this group,
orpus luteum (CL) formation was confirmed first by deter-ining the side of the dominant follicle (larger than any
ther follicle, diameter �10 mm in ultrasonography) in therevious menstrual cycle (day 10 to 12). Thereafter, serumoncentrations of P were measured during the luteal phase 6o 9 days before the next expected menstrual bleed. A levelf P � 20 nmol/L was considered as confirmation of normalL function. Group 2 consisted of 11 women who were
aking combined oral contraceptive pills and who subse-uently had regular menstrual cycles without ovulation.
Informed written consent was obtained from each subject,nd the study was approved by the ethics committee of Ouluniversity Hospital, Oulu, Finland.
FIGURE 1
Three-dimensional power Doppler ultrasonographic imcontralateral ovary (left) 96 hours after hCG injection.network (white arrow). The volume of the left ovary wmL. On the right side, the measurements were 17.0 m
Järvelä. hCG test and regressing corpus luteum. Fertil Steril 2007.
ertility and Sterility�
CG Testsll subjects (both groups) were stimulated with a single IMose of hCG (5,000 IU, Pregnyl; Organon, Oss, the Nether-ands) 2 to 4 days after menstrual bleeding. In group 1,timulation was performed after the confirmed ovulatoryycle. Blood samples for assays of FSH, P, 17-OHP, A, T,
2, and vascular endothelial growth factor (VEGF) wereollected before injection of hCG and at 48 and 96 hoursfterward.
ssayserum concentrations of T and P were analyzed using anutomated chemiluminescence system (Advia Centaur;ayer Healthcare LCC, Diagnostic Division, Tarrytown,Y). Serum concentrations of FSH were analyzed byuoroimmunoassay (Wallac, Ltd., Turku, Finland), andIAs were used for 17-OHP, A (Diagnostic Productsorp., Los Angeles, CA), and E2 (Orion Diagnostica,ulunsalo, Finland), following the instructions providedy the manufacturers. Total VEGF (VEGFtot) and freeEGF (VEGFfree) were determined by enzyme immuno-
ssay (EIA) using commercial reagents (Cytimmune Sci-nces Inc., College Park, MD).
The intraassay and interassay coefficients of variationere 3.8% and 4.3%, respectively, for FSH, 5.0% and.4% for 17-OHP, 5.0% and 8.6% for A, 4.0% and 5.6%or T, 5.7% and 6.4% for E2, and 3.7% and 5.4% for P.he intraassay and interassay coefficients of variationere 8.9% and 11.1% for VEGFtot and 7.3% and 10.5%
es of an ovary with a rescued CL (right) and theCL is surrounded by an extensive vascular
.0 mL, and the volume of the vasculature was 0.3nd 2.8 mL, respectively.
agTheas 6L a
1123

fwac
O
TdKTiwiuolsmml
wacaa311tviiwwpov
u
or VEGFfree. External quality control of the hormone assaysas organized by national (Labquality Ltd., Helsinki, Finland)
nd international (Bio-Rad Laboratories EQAS, Irvine, CA)ompanies.
varian Volume and Vascularization Measurements
he ovaries were examined at each visit using three-imensional (3D) ultrasonography (Voluson Expert 730;
retz, Zipf, Austria) equipped with a transvaginal probe.his technique enabled the determination of ovarian volume,
ncluding possible changes in the intraovarian vascular net-ork. Volume acquisition and storage have been described
n detail elsewhere (14). Identical preinstalled settings weresed to acquire the power Doppler information from thevaries. The setting conditions for this study were as fol-ows: frequency, mid; dynamic set, 2; balance, G�170;mooth, 5/5; ensemble, 16; line density, 7; power Dopplerap, 5; and the setting conditions for the subpower Dopplerode were: gain, �5.6; quality, normal; wall motion filter,
ow 1; velocity range, 0.9 kHz.
TABLE 1Serum basal hormone levels and AUC at 96 hour(5,000 IU) in women with and without a CL.
CL�
Age 30.8 �Body mass index 23.2 �Basal hormone levels
P (nmol/L) 3.1 �17-OHP (nmol/L) 4.6 �Androstenedione (nmol/L) 8.7 �T (nmol/L) 1.4 �E2 (nmol/L) 0.11 �FSH (U/L) 7.3 �VEGFtot (ng/mL) 6.2 �VEGFfree (pg/mL) 66.8 �
AUC (0–96 h)P 18.4 �17-OHP 13.0 �Androstenedione 21.1 �T 3.2 �E2 0.43 �FSH 12.5 �VEGFtot 9.7 �VEGFfree 120.0 �
Ratio of AUCs (0–96 h)P/17-OHP 2.6 �17-OHP/Androstenedione 1.24 �Androstenedione/T 13.6 �T/E2 18.8 �
Note: Data are shown as mean � SE. Statistical significa
Järvelä. hCG test and regressing corpus luteum. Fertil Steril 2007.
1124 Järvelä et al. hCG test and regressing corpus luteum
Determination of ovarian volume and vascularizationas performed using the built-in virtual organ computer-
ided analysis Imaging Program (VOCAL, GE Health-are, Zipf, Austria) for 3D power Doppler histogramnalysis. The manual mode of the virtual organ computer-ided analysis Contour Editor was used to cover the wholeD volume of the ovary, with 15° rotation steps. Hence,2 contour planes were analyzed for each ovary to cover80°. After obtaining the total ovarian volume (Fig. 1),he program calculated the ratio of color voxels to alloxels; this ratio (%) was expressed as the vascularizationndex (VI). Raine-Fenning et al. (15) observed in ann-vitro flow phantom study that VI increased linearlyith an increase in flow rate, suggesting that VI measuredith standardized settings is closely related with the blooderfusion in the organ. Vascularized volume (mL) in thevary was calculated by multiplying the total ovarianolume by the VI.
The reproducibility of volume and VI measurementssing transvaginal 3D power Doppler ultrasonography has
flecting responses to a single dose of hCG
CL� P
28.1 � 1.1 NS25.4 � 1.5 NS
2.1 � 0.4 NS3.7 � 0.9 NS9.0 � 1.3 NS1.6 � 0.2 NS
0.07 � 0.02 NS3.7 � 0.7 .0285.2 � 2.6 NS
140.4 � 35.2 NS
4.1 � 0.6 �.0017.4 � 1.4 .001
20.0 � 2.7 NS3.3 � 0.3 NS
0.24 � 0.04 .02811.2 � 1.2 NS12.1 � 5.6 NS
272.3 � 65.3 NS
1.2 � 0.1 .0180.78 � 0.12 .00612.0 � 0.8 NS44.2 � 6.9 .001
P�.05. NS � not significant.
s re
1.11.0
0.30.70.90.20.021.32.319.4
5.10.91.60.30.051.53.035.1
0.50.070.62.4nce,
Vol. 87, No. 5, May 2007

bcw
STtmtm
lhbintPrmw
F
een assessed earlier (16). The intraobserver correlationoefficient for volume measurements was 1.0, and for VIas 0.89 (16).
tatisticshe general linear model for repeated measures was used
o measure significance within a group and also to deter-ine whether the stimulation patterns differed between
he groups. Areas under the curve (AUCs) for the hor-one, vascularization, and volume responses were calcu-
FIGURE 2
Responses of serum P (A), 17-OHP (B), A (C), T (D),in women with and without a CL. *Statistical significa
Järvelä. hCG test and regressing corpus luteum. Fertil Steril 2007.
ertility and Sterility�
ated using the trapezoidal method. To compare serumormone levels and ovarian responses to hCG (AUCs)etween different age groups at each time point, thendependent samples t test was used as a post hoc test forormally distributed variables, and the Mann-Whitney Uest was used for variables with skewed distribution. Theearson correlation coefficient (r) was calculated to cor-elate ovarian volume and vascularization with the hor-one levels measured. The limit of statistical significanceas set at P�.05.
), and FSH (F) to a single dose of hCG (5,000 IU)between the groups at each time point, P�.05.
E2 (Ence
1125

RHBe5psarPPai
gob1b
OTbCacw
ivt
Fcic4i(wo(
vvc
RVTuAr
DAsdcioat
ESULTSormone Responses to hCGasal hormone levels did not differ between the groups,xcept for FSH (Table 1). The range for basal P was 0.9 to.0 nmol/L. The hormone response patterns to hCG areresented in Figure 2. Analysis of repeated measurementshowed changes in the concentrations of P, 17-OHP, A, T,nd E2, but not in those of FSH, VEGFtot, or VEGFfree. Theesponse patterns were different in the two groups regarding, 17-OHP, E2, and FSH. No change was observed in serumor 17-OHP levels in the control group. Mean P, 17-OHP,
nd E2 levels were higher 48 and 96 hours after hCGnjection in women with a CL.
The AUCs of P, 17-OHP, and E2 at 96 hours werereater in women with a CL, whereas no difference wasbserved in the AUCs of A, T, FSH, VEGFtot, or VEGFfree
etween the groups (Table 1). The AUCs of P/17-OHP,7-OHP/A, and T/E2 ratios showed statistical differencesetween the groups.
varian Volume and Vascularization Responses to hCGhe ultrasonographic data provided three different groups toe compared in statistical analysis: the ovary containing theL (CL�), the contralateral ovary from the same woman,nd the control group (CL�), in which no CL existed. In theontrol group the mean values of the right and left ovaryere used for statistical analysis.
At baseline, the CL� ovaries were larger than the ovariesn the control group regarding total, vascularized, and non-ascularized volume, but they did not differ from the con-ralateral ovaries (Table 2).
TABLE 2Ovarian basal total, vascularized, and nonvasculvolume responses to a single dose of hCG (5,000
CL�
CL� ovaryCon
C
Basal valuesOvarian volume (mL) 7.41 � 0.80 6Vascularized volume (mL) 0.46 � 0.09 0Nonvascularized volume (mL) 6.95 � 0.73 5
AUC (0–96 h)Ovarian volume 17.3 � 1.7 1Vascularized volume 2.2 � 0.5Nonvascularized volume 15.2 � 1.2 1
Note: In the CL� group, the ovary containing the CL (CL�are presented separately. In the control group (no CL), thas mean � SE. Statistical significance, P�.05. NS � n
Järvelä. hCG test and regressing corpus luteum. Fertil Steril 2007.
1126 Järvelä et al. hCG test and regressing corpus luteum
The volume response patterns to hCG are presented inigure 3. Analysis of repeated measurements showed in-reases in total, vascularized, and nonvascularized volumesn the CL� ovaries but no change in the contralateral orontrol ovaries. The means of all three volumes were higher8 and 96 hours after hCG injection in the CL� ovaries thann the contralateral or control ovaries. At 96 hours, the VImean � SE) in the CL-containing ovaries (13.3% � 2.4%)as significantly higher (P�.005) than in the contralateralvaries (3.7% � 1.4%) or in the ovaries of the control group2.6% � 0.8%).
The AUCs of total, vascularized, and nonvascularizedolumes at 96 hours are presented in Table 2. All of theolumes were greater in CL� ovaries than in contralateral orontrol ovaries, which did not differ from each other.
elationship Between Hormone Secretion and Ovarianolume and Vascularizationhe AUCs of P and ovarian total and vascularized vol-mes at 96 hours correlated in CL� women (Fig. 4). TheUCs of 17-OHP and ovarian vascularized volume cor-
elated significantly in the same group.
ISCUSSIONccording to our results, the hormonal profile after the hCG
timulation test performed in the early follicular phase wasifferent after an ovulatory and an anovulatory menstrualycle. It seems that hCG stimulation reactivated the regress-ng CL in the ovulatory women. This reactivation was notnly reflected by increasing serum hormone levels, but waslso seen as a concomitant increase in CL-containing ovarianotal and vascularized volume.
d volumes and AUC at 96 hours reflecting the).
P, CL�ovary vs.
contralateral
CL� P, CL�ovary vs.control(no CL)
ateral toovary
Control(no CL)
� 0.80 NS 4.91 � 0.60 .021� 0.09 NS 0.11 � 0.02 .001� 0.74 NS 4.81 � 0.57 .001
� 1.5 .009 9.8 � 1.0 .001� 0.2 .004 0.2 � 0.1 .005� 1.4 .019 9.6 � 1.0 .002ry) and the contralateral one (contralateral to CL� ovary)lues represent the means of both ovaries. Data are shownnificant.
arizeIU
tralL�
.07
.27
.80
1.40.50.9ova
e vaot sig
Vol. 87, No. 5, May 2007
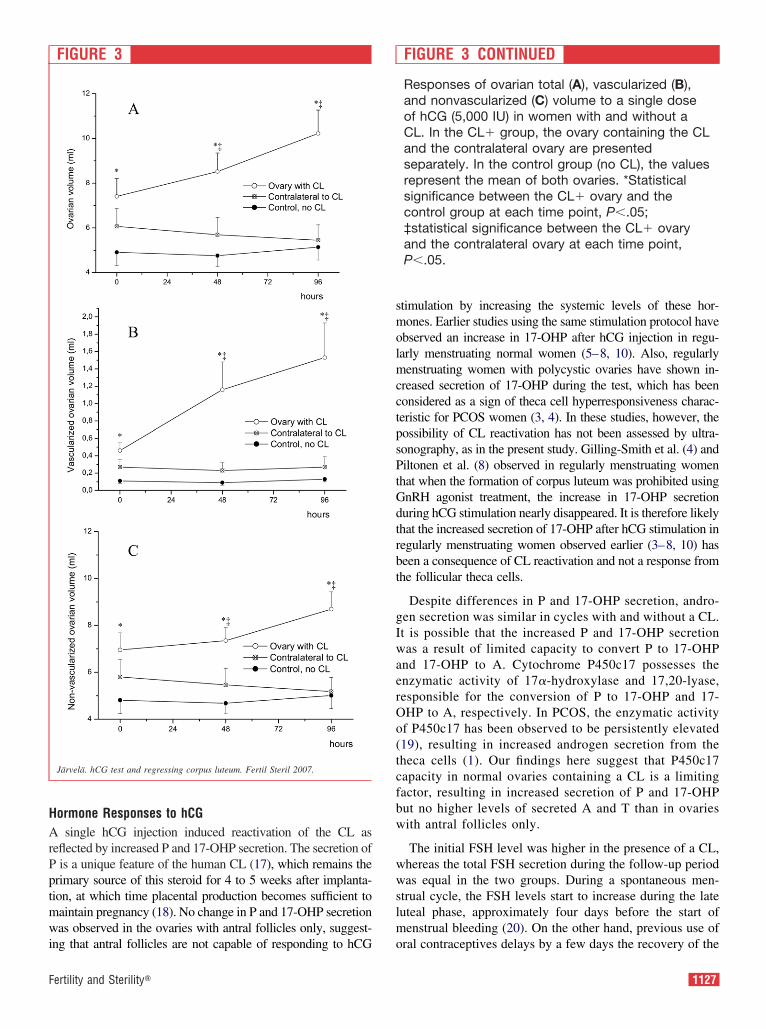
HArPptmwi
smolmcctpsPtGdtrbt
gIwaerOo(tcfbw
wwslm
F
ormone Responses to hCGsingle hCG injection induced reactivation of the CL as
eflected by increased P and 17-OHP secretion. The secretion ofis a unique feature of the human CL (17), which remains the
rimary source of this steroid for 4 to 5 weeks after implanta-ion, at which time placental production becomes sufficient toaintain pregnancy (18). No change in P and 17-OHP secretionas observed in the ovaries with antral follicles only, suggest-
FIGURE 3
Järvelä. hCG test and regressing corpus luteum. Fertil Steril 2007.
ng that antral follicles are not capable of responding to hCG o
ertility and Sterility�
timulation by increasing the systemic levels of these hor-ones. Earlier studies using the same stimulation protocol have
bserved an increase in 17-OHP after hCG injection in regu-arly menstruating normal women (5–8, 10). Also, regularlyenstruating women with polycystic ovaries have shown in-
reased secretion of 17-OHP during the test, which has beenonsidered as a sign of theca cell hyperresponsiveness charac-eristic for PCOS women (3, 4). In these studies, however, theossibility of CL reactivation has not been assessed by ultra-onography, as in the present study. Gilling-Smith et al. (4) andiltonen et al. (8) observed in regularly menstruating women
hat when the formation of corpus luteum was prohibited usingnRH agonist treatment, the increase in 17-OHP secretionuring hCG stimulation nearly disappeared. It is therefore likelyhat the increased secretion of 17-OHP after hCG stimulation inegularly menstruating women observed earlier (3–8, 10) haseen a consequence of CL reactivation and not a response fromhe follicular theca cells.
Despite differences in P and 17-OHP secretion, andro-en secretion was similar in cycles with and without a CL.t is possible that the increased P and 17-OHP secretionas a result of limited capacity to convert P to 17-OHP
nd 17-OHP to A. Cytochrome P450c17 possesses thenzymatic activity of 17�-hydroxylase and 17,20-lyase,esponsible for the conversion of P to 17-OHP and 17-HP to A, respectively. In PCOS, the enzymatic activityf P450c17 has been observed to be persistently elevated19), resulting in increased androgen secretion from theheca cells (1). Our findings here suggest that P450c17apacity in normal ovaries containing a CL is a limitingactor, resulting in increased secretion of P and 17-OHPut no higher levels of secreted A and T than in ovariesith antral follicles only.
The initial FSH level was higher in the presence of a CL,hereas the total FSH secretion during the follow-up periodas equal in the two groups. During a spontaneous men-
trual cycle, the FSH levels start to increase during the lateuteal phase, approximately four days before the start ofenstrual bleeding (20). On the other hand, previous use of
FIGURE 3 CONTINUED
Responses of ovarian total (A), vascularized (B),and nonvascularized (C) volume to a single doseof hCG (5,000 IU) in women with and without aCL. In the CL� group, the ovary containing the CLand the contralateral ovary are presentedseparately. In the control group (no CL), the valuesrepresent the mean of both ovaries. *Statisticalsignificance between the CL� ovary and thecontrol group at each time point, P�.05;‡statistical significance between the CL� ovaryand the contralateral ovary at each time point,P�.05.
ral contraceptives delays by a few days the recovery of the
1127

pp(l
fs
ituitary gland and prolongs especially the early follicularhase during the following spontaneous menstrual cycle21). These facts explain the difference in the initial FSH
FIGURE 4
Correlations of AUCs between P, 17-OHP, and ovarivolume and vascularization concern only the CL-convolume and vascularization are means of both ovarie
Järvelä. hCG test and regressing corpus luteum. Fertil Steril 2007.
evels between the groups in the present study. m
1128 Järvelä et al. hCG test and regressing corpus luteum
Stimulation with hCG resulted in elevated E2 secretionrom the ovaries with reactivated corpora lutea. The FSHtimulates the conversion of T to E2 by activating the aro-
olume and vascularization. In the CL� group,ng ovary. In the CL� group (no CL, control group),
an vtainis.
atizing capacity of cytochrome P450arom. In the present
Vol. 87, No. 5, May 2007

sqlp(awsT
i(sTaaVglaoesacr
OStctt
sptitiorh
astsDaTtCm
eMtppcw
iadtt
CIpfrnrpo1CAbtc
R
F
tudy, the increased E2 production may have been a conse-uence of the higher basal FSH level at the start of stimu-ation because there was no difference in T levels at anyoint. A similar finding has been reported by Piltonen et al.10). They compared normally menstruating women overnd under 30 years of age and observed that in older women,ho initially had higher FSH levels, hCG stimulation re-
ulted in more marked increase in E2 secretion despite lowersecretion.
During luteal development, extensive neovascularizations a prerequisite for normal growth and function of the CL22). This angiogenesis seems to be controlled by localecretion of growth factors (23), especially VEGF (24–27).he expression and synthesis of VEGF is regulated by LHnd hCG (28), and therefore VEGF levels were measuredlso in the present study. No differences in total or freeEGF levels were observed within or between the tworoups. Molskness et al. (29) measured free and total circu-ating VEGF levels in natural cycles in rhesus monkeys andlso observed no changes. On the other hand, in controlledvarian stimulation cycles, when several active corpora luteaxisted in both ovaries, the levels of circulating VEGFhowed significant changes (29). It may be that in the case ofsingle CL, the systemic levels of VEGF do not reflect localoncentrations of VEGF, angiogenesis, or vasculature accu-ately enough.
varian Volume and Vascularization Responses to hCGtimulation with hCG resulted in significant increases in
otal, vascularized, and nonvascularized volumes in the CL-ontaining ovaries, whereas none of these effects were de-ected in either the contralateral ovaries or the ovaries con-aining only antral follicles.
During the normal menstrual cycle, theca lutein cells aremall and do not undergo a change in size during the lutealhase, whereas granulosa lutein cells enlarge from the earlyo the mid-luteal phase (26). After hCG stimulation simulat-ng early pregnancy, granulosa lutein cells become largerhan at any stage of the cycle (26). It is possible that thencrease in total size and nonvascularized volume in thevary containing the CL, observed in the present study,eflects this change in the size of luteal cells in response toCG stimulation.
In addition, CL rescue with hCG has been observed to bessociated with a second wave of angiogenesis and vasculartabilization (26), which probably explains the increase inhe vascularized volume of the CL-containing ovary ob-erved here by means of 3D ultrasonography. According toharmarajan et al. (30), capillary lumina in pregnant rats
ccount for 22% of the total volume of the corpus luteum.he vasculature in our study accounted for up to 13% of the
otal ovarian volume. If the proportion had been related toL volume only, it probably would have been considerably
ore.ertility and Sterility�
We found relationships between the hormonal parameters,specially P secretion and CL vascularization and volume.iyazaki et al. (31) have investigated the relationship be-
ween P level and corpus luteal blood flow during lutealhase using two-dimensional power Doppler ultrasonogra-hy. They observed that P concentration was positivelyorrelated with the corpus luteal vascularization volume,hich supports our results.
Despite the fact that P secreted by the corpus luteum maynhibit the folliculogenesis in the contralateral ovary (32)nd subsequently affect the ovarian volume, we did notiscover any differences in the volumes between the con-ralateral ovaries in the ovulatory group and the ovaries inhe anovulatory group.
onclusionsf an hCG stimulation test is performed in the early follicularhase in regularly menstruating women, the regressing CLrom the past cycle reactivates and responds to hCG. Theesponse to the hCG test may thus be considered a combi-ation of the capacity of both follicular theca cells and theeactivated CL to synthesize and secrete steroids. It also isossible that a GnRH-agonist stimulation test in normalvulatory women with and without polycystic ovaries (5,1–13) is associated with a similar reactivation of regressingL, if the test is performed during the early follicular phase.s a conclusion, ovulation in the past menstrual cycle shoulde taken into account when performing ovarian stimulationests in regularly menstruating women, and especially whenomparing ovulatory and anovulatory women.
EFERENCES1. Gilling-Smith C, Willis DS, Beard RW, Franks S. Hypersecretion of
androstenedione by isolated thecal cells from polycystic ovaries. J ClinEndocrinol Metab 1994;79:1158–65.
2. Nelson VL, Legro RS, Strauss JF 3rd, McAllister JM. Augmentedandrogen production is a stable steroidogenic phenotype of propagatedtheca cells from polycystic ovaries. Mol Endocrinol 1999;13:946–57.
3. Adams JM, Taylor AE, Crowley WF Jr, Hall JE. Polycystic ovarianmorphology with regular ovulatory cycles: insights into the pathophys-iology of polycystic ovarian syndrome. J Clin Endocrinol Metab 2004;89:4343–50.
4. Gilling-Smith C, Story H, Rogers V, Franks S. Evidence for a primaryabnormality of thecal cell steroidogenesis in the polycystic ovary syn-drome. Clin Endocrinol (Oxf) 1997;47:93–9.
5. Ibanez L, Hall JE, Potau N, Carrascosa A, Prat N, Taylor AE. Ovarian17-hydroxyprogesterone hyperresponsiveness to gonadotropin-releasinghormone (GnRH) agonist challenge in women with polycystic ovarysyndrome is not mediated by luteinizing hormone hypersecretion: ev-idence from GnRH agonist and human chorionic gonadotropin stimu-lation testing. J Clin Endocrinol Metab 1996;81:4103–7.
6. Koivunen RM, Morin-Papunen LC, Ruokonen A, Tapanainen JS, Mar-tikainen HK. Ovarian steroidogenic response to human chorionic go-nadotrophin in obese women with polycystic ovary syndrome: effect ofmetformin. Hum Reprod 2001;16:2546–51.
7. Levrant SG, Barnes RB, Rosenfield RL. A pilot study of the humanchorionic gonadotrophin test for ovarian hyperandrogenism. Hum Re-
prod 1997;12:1416–20.1129

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
8. Piltonen T, Koivunen R, Morin-Papunen L, Ruokonen A, HuhtaniemiIT, Tapanainen JS. Ovarian and adrenal steroid production: regulatoryrole of LH/HCG. Hum Reprod 2002;17:620–4.
9. Piltonen T, Koivunen R, Perheentupa A, Morin-Papunen L, RuokonenA, Tapanainen JS. Ovarian age-related responsiveness to human cho-rionic gonadotropin in women with polycystic ovary syndrome. J ClinEndocrinol Metab 2004;89:3769–75.
0. Piltonen T, Koivunen R, Ruokonen A, Tapanainen JS. Ovarian age-related responsiveness to human chorionic gonadotropin. J Clin Endo-crinol Metab 2003;88:3327–32.
1. Carmina E, Lobo RA. Polycystic ovaries in hirsute women with normalmenses. Am J Med 2001;111:602–6.
2. Chang PL, Lindheim SR, Lowre C, Ferin M, Gonzalez F, Berglund L,et al. Normal ovulatory women with polycystic ovaries have hyperan-drogenic pituitary-ovarian responses to gonadotropin-releasinghormone-agonist testing. J Clin Endocrinol Metab 2000;85:995–1000.
3. Rosenfield RL, Barnes RB, Ehrmann DA. Studies of the nature of17-hydroxyprogesterone hyperresonsiveness to gonadotropin-releasinghormone agonist challenge in functional ovarian hyperandrogenism.J Clin Endocrinol Metab 1994;79:1686–92.
4. Järvelä IY, Sladkevicius P, Kelly S, Ojha K, Campbell S, Nargund G.Effect of pituitary down-regulation on the ovary before in vitro fertil-ization as measured using three-dimensional power Doppler ultrasound.Fertil Steril 2003;79:1129–35.
5. Raine-Fenning NJ, Ramnarine KV, Nordin NM, Campbell BK. Quan-tification of blood perfusion using 3D power Doppler: an in-vitro flowphantom study. Journal of Physics: Conference Series 2004;1:181.
6. Järvelä IY, Sladkevicius P, Tekay AH, Campbell S, Nargund G. In-traobserver and interobserver variability of ovarian volume, gray-scaleand color flow indices obtained using transvaginal three-dimensionalpower Doppler ultrasonography. Ultrasound Obstet Gynecol 2003;21:277–82.
7. Retamales I, Carrasco I, Troncoso JL, Las Heras J, Devoto L, Vega M.Morpho-functional study of human luteal cell subpopulations. HumReprod 1994;9:591–6.
8. Csapo AI, Pulkkinen M. Indispensability of the human corpus luteum inthe maintenance of early pregnancy. Luteectomy evidence. ObstetGynecol Surv 1978;33:69–81.
9. Wickenheisser JK, Quinn PG, Nelson VL, Legro RS, Strauss JF 3rd,McAllister JM. Differential activity of the cytochrome P450 17alpha-hydroxylase and steroidogenic acute regulatory protein gene promotersin normal and polycystic ovary syndrome theca cells. J Clin EndocrinolMetab 2000;85:2304–11.
0. Miro F, Aspinall LJ. The onset of the initial rise in follicle-stimulatinghormone during the human menstrual cycle. Hum Reprod 2005;20:96–
100.1130 Järvelä et al. hCG test and regressing corpus luteum
1. Klein TA, Mishell DR. Gonadotropin, prolactin, and steroid hormonelevels after discontinuation of oral contraceptives. Am J Obstet Gynecol1977;127:585–9.
2. Fraser HM, Dickson SE, Lunn SF, Wulff C, Morris KD, Carroll VA,et al. Suppression of luteal angiogenesis in the primate after neutral-ization of vascular endothelial growth factor. Endocrinology 2000;141:995–1000.
3. Hazzard TM, Stouffer RL. Angiogenesis in ovarian follicular and lutealdevelopment. Baillieres Res Clin Obstet Gynaecol 2000;14:883–900.
4. Sugino N, Kashida S, Takiguchi S, Karube A, Kato H. Expression ofvascular endothelial growth factor and its receptors in the human corpusluteum during the menstrual cycle and in early pregnancy. J ClinEndocrinol Metab 2000;85:3919–24.
5. Wulff C, Wilson H, Rudge JS, Wiegand SJ, Lunn SF, Fraser HM.Luteal angiogenesis: prevention and intervention by treatment withvascular endothelial growth factor trap(A40). J Clin Endocrinol Metab2001;86:3377–86.
6. Wulff C, Dickson SE, Duncan WC, Fraser HM. Angiogenesis in thehuman corpus luteum: simulated early pregnancy by HCG treatment isassociated with both angiogenesis and vessel stabilization. Hum Reprod2001;16:2515–24.
7. Fraser HM, Wilson H, Morris KD, Swanston I, Wiegand SJ. Vascularendothelial growth factor trap suppresses ovarian function at all stagesof the luteal phase in the macaque. J Clin Endocrinol Metab 2005;90:5811–8. Epub 2005 Jul 26.
8. Fraser HM, Bell J, Wilson H, Taylor PD, Morgan K, Anderson RA,et al. Localization and quantification of cyclic changes in the ex-pression of endocrine gland vascular endothelial growth factor in thehuman corpus luteum. J Clin Endocrinol Metab 2005;90:427–34.Epub 2004 Oct 13.
9. Molskness TA, Stouffer RL, Burry KA, Gorrill MJ, Lee DM, PattonPE. Circulating levels of free and total vascular endothelial growthfactor (VEGF)-A, soluble VEGF receptors-1 and -2, and angiogeninduring ovarian stimulation in non-human primates and women. HumReprod 2004;19:822–30. Epub 2004 Feb 12.
0. Dharmarajan AM, Bruce NW, Meyer GT. Quantitative ultrastructuralcharacteristics relating to transport between luteal cell cytoplasm andblood in the corpus luteum of the pregnant rat. Am J Anat 1985;172:87–99.
1. Miyazaki T, Tanaka M, Miyakoshi K, Minegishi K, Kasai K, YoshimuraY. Power and colour Doppler ultrasonography for the evaluation of thevasculature of the human corpus luteum. Hum Reprod 1998;13:2836–41.
2. Goodman AL, Hodgen GD. Antifolliculogenic action of progesteronedespite hypersecretion of FSH in monkeys. Am J Physiol 1982;243:
E387–97.Vol. 87, No. 5, May 2007

Atmhhlc
occpdoem
RSR
0d
Ovarian suppression with a gonadotropin-releasinghormone agonist does not alter insulin-stimulatedglucose disposalBrian C. Cooper, M.D.,a Cynthia K. Sites, M.D.,a Peter R. Casson, M.D.,a
and Michael J. Toth, Ph.D.b
a Departments of Obstetrics and Gynecology and b Medicine, University of Vermont, Burlington, Vermont
Objective: Aging is associated with reduced tissue sensitivity to insulin. In women, these age-related changes maybe accelerated by menopause. The effect of ovarian hormone deficiency on tissue insulin sensitivity in humans,however, has not been defined clearly. Thus, the goal of this study was to evaluate the effect of suppression ofendogenous ovarian hormone production on insulin-stimulated glucose disposal.Design: Randomized, single-blind, placebo-controlled trial.Setting: General clinical research center.Patients: Thirteen healthy, nonobese premenopausal women.Intervention(s): Insulin-stimulated glucose disposal was determined by hyperinsulinemic (40 mU/m2/min) clampduring the early to midfollicular and midluteal phase of the menstrual cycle. Volunteers then received 2 monthsof treatment with the GnRH agonist (GnRHa) leuprolide acetate (n � 6) or placebo (n � 7) and were retested.Main Outcome Measure(s): Total, oxidative, and nonoxidative insulin-stimulated glucose disposal.Result(s): Because no effect of cycle phase was found on total, oxidative, or nonoxidative glucose disposal,pretreatment follicular and luteal phase values were averaged. Treatment with GnRHa had no effect on totalglucose disposal (GnRHa: 10.6 � 0.9 to 10.8 � 0.9 vs. placebo: 10.2 � 0.7 to 10.4 � 1.0 mg/kg fat-freemass/min, P � .99). Similarly, there was no effect of GnRHa administration on oxidative (GnRHa: 2.77 � 0.58to 3.89 � 0.58 vs. placebo: 2.74 � 0.42 to 3.33 � 0.62 mg/kg fat-free mass/min, P � .52; n � 6 and 6,respectively) or nonoxidative (GnRHa: 7.82 � 0.68 to 6.91 � 0.66 vs. placebo: 7.94 � 0.72 to 7.79 � 0.99 mg/kgfat-free mass/min, P � .59; n � 6 and 6, respectively) components of glucose disposal.Conclusion(s): Our results suggest that endogenous ovarian hormones do not regulate tissue responsiveness toinsulin or intracellular pathways of glucose disposal. (Fertil Steril� 2007;87:1131–8. ©2007 by American Societyfor Reproductive Medicine.)
Key Words: Ovarian hormones, estrogen, insulin sensitivity, GnRH agonist
sifisccas
iswcwpwipv
ging is characterized by a decline in tissue insulin sensi-ivity (1, 2). In women, this decline may be accelerated after
enopause (3). Some have hypothesized that ovarianormone deficiency contributes to disturbances in glucoseomeostasis (4). The role of ovarian hormones in regu-ating tissue insulin sensitivity, however, has not beenlearly defined.
Studies in rodent models have consistently shown thatvarian hormone deficiency impairs insulin-stimulated glu-ose disposal and that replacement of ovarian hormonesorrects insulin resistance (5–8). Whether ovarian hormoneslay a similar role in regulating insulin-stimulated glucoseisposal in humans is less clear. Cross-sectional comparisonsf premenopausal and postmenopausal women have shownither no difference (9) or increased insulin action in post-enopausal women (10).
eceived February 27, 2006; revised and accepted November 8, 2006.upported by NIH AG-021602 and NIH RR-00109.eprint requests: Michael J. Toth, Ph.D., Health Science Research Facil-ity 126 B, 149 Beaumont Avenue, University of Vermont, Burlington,
pVermont 05405 (FAX: 802-656-0747; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.11.045 Copyright ©2007 American Soc
In further contrast, work in postmenopausal women hashown that resistance to the effects of insulin develops withncreasing menopausal age (11). Studies examining the ef-ect of hormone replacement therapy on glucose metabolismn postmenopausal women are equally divergent, with resultshowing increased (12, 13), unchanged (14–18), and de-reased insulin sensitivity (19, 20). From these studies, it islear that no conclusions can be drawn regarding the role, ifny, that ovarian hormones play in the regulation of insulin-timulated glucose disposal in women.
Our goal in the present study was to determine the phys-ological role of endogenous ovarian hormones on insulin-timulated glucose disposal. To accomplish this objective,e measured glucose disposal under hyperinsulinemic
lamp conditions in healthy, nonobese, premenopausalomen during the early to midfollicular and midlutealhases of the menstrual cycle and after 2 months of treatmentith either GnRH agonist (GnRHa) or placebo. This exper-
mental model permits us to compare the effects of an acuteeriod of ovarian hormone deficiency (i.e., GnRHa group)s. the effects of normal cycling levels of the hormones (i.e.,
lacebo group) on glucose disposal. Because animal studies1131Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

stweowsn
MST(nkbpgonfhtrmbspsrt2egd
EEwigtnlcsntsdQd
m8
amlmiwggPtimtDwdp
pCoscoias(b[pmlcbmPtmtu
aiatnmpsp
AP
uggest that ovarian hormones regulate glucose disposalhrough alterations in components of the nonoxidative path-ay (7, 8, 21), we further sought to define the effects of
ndogenous ovarian hormones on intracellular pathways ofxidative and nonoxidative glucose disposal. Our hypothesisas that ovarian hormone deficiency would reduce insulin-
timulated glucose disposal by decreasing flux through theonoxidative pathway.
ATERIALS AND METHODSubjectshirteen healthy women ranging in age from 21 to 35 years
mean � SE, 27 � 1 year) were recruited. Women wereonobese (body mass index [BMI] �28 kg/m2, 22 � 1g/m2); had a stable body weight (� 2 kg) for 6 monthsefore the study; were healthy based on medical history,hysical examination, and routine blood test results; werelucose tolerant (glucose �7.77 mmol/L 2 hours after 75 gral glucose load); had no history of tobacco use; and wereot on any medication that could affect ovarian/reproductiveunction or insulin sensitivity. All women were nulliparous,ad not been exposed to any form of hormone-based con-raceptive therapy for at least 6 months before the study, andeported having at least two spontaneous cycles in the 3onths before recruitment. The nature, purpose, and possi-
le risks of the study were explained to each subject beforehe gave written consent to participate. The experimentalrotocol was approved by the Committee on Human Re-earch at the University of Vermont. Data from this cohortegarding the effects of GnRHa administration on proteinurnover and blood flow have been published elsewhere (22,3). The primary goal of these studies was to assess theffect of GnRHa on protein metabolism, with the secondaryoal of examining the effects of insulin-stimulated glucoseisposal.
xperimental Protocolach volunteer underwent an outpatient screening visit, athich time medical history, physical examination, biochem-
cal laboratory tests, an exercise stress test, and an orallucose tolerance test were performed. Volunteers who methe eligibility criteria were randomized by the study coordi-ator using a stratified block approach to receive the GnRHaeuprolide acetate (n � 6, Lurpon Depot [Tap Pharmaceuti-als, Lake Forest, IL], 3.75 mg IM) or placebo (n � 7, 0.9%aline). Groups were stratified for age and BMI. All person-el performing metabolic testing on volunteers were blindedo treatment status. Before the study, each volunteer’s men-trual cycle was monitored using a combination of menstrualiaries and ovulation prediction kits (Ovu-Quick One-Step;uidel Co., San Diego, CA), and midluteal phase bloodraws were used to discern cycle and phase length.
Each woman was tested on two occasions before treat-ent: during the early to midfollicular phase (cycle day 3 to
) and the midluteal phase (cycle day 19 to 25, assuming an b
1132 Cooper et al. Ovarian hormones and glucose disposal
verage cycle length of 28 days). The order of pretreatmentetabolic testing with respect to cycle phase (follicular–
uteal vs. luteal–follicular) was randomized. After pretreat-ent testing, GnRHa or placebo was administered by IM
njection during the midluteal phase. The second injectionas given 30 days after the first injection in the GnRHaroup and 25 to 32 days after the first injection in the placeboroup, depending on the volunteer’s menstrual cycle length.osttreatment metabolic testing was performed 60 days after
he first injection in the GnRHa group. Posttreatment testingn the placebo group was performed in the phase of theenstrual cycle that was tested second during pretreatment
esting approximately 50 to 64 days after the first injection.irectly preceding each bout of metabolic testing, volunteersere provided 3 days of a weight-maintenance, standardizediet (20% protein, 25% fat, and 55% carbohydrate). The dietrovided at least 200 g of carbohydrate per day.
Insulin-stimulated glucose disposal measurements wereerformed the morning after an overnight visit to the Generallinical Research Center. Volunteers were fasted after 19:00n the evening of admission. At approximately 06:00, theubject was awakened and catheters were placed in an ante-ubital vein for infusion and retrograde in a dorsal hand veinf the contralateral arm and were kept patent with salinenfusion. The hand was placed in a warming box to obtainrterialized venous blood (24). Baseline blood and breathamples were taken, and a primed (4.5 �mol/kg), continuous4.5 �mol/kg/h) infusion of [1-13C]leucine was started. Theicarbonate pool was primed (1.6 �mol/kg) with sodium13C]bicarbonate. Leucine kinetic data were used to measurerotein oxidation. At 210 minutes, insulin was started (40U/m2/min) with the goal of achieving circulating insulin
evels that approximate postprandial levels. In addition, aonstant-rate (1.5 ml/kg/h) infusion of 10% Aminosyn (Ab-ott Laboratories; Chicago, IL) was started. Glycemia wasaintained by a variable-rate infusion of 20% dextrose.lasma glucose levels were monitored every 5 minutes, and
he dextrose infusion rate was adjusted to maintain euglyce-ia. All infusions were stopped at 330 minutes except for
he 20% dextrose infusion, which was continued and taperedntil no longer required to maintain normal glycemia.
Blood and breath samples were drawn at 285, 300, 315,nd 330 minutes for measurement of leucine oxidation dur-ng the clamp. Plasma was isolated and stored at �70°C untilnalysis. Oxygen consumption and carbon dioxide produc-ion rates were determined using the ventilated hood tech-ique (DeltaTrac, Yorba Linda, CA). Indirect calorimetryeasurements were not performed on one volunteer in the
lacebo group because of technical problems. Body compo-ition measurements were performed directly after the clamprocedure.
nalytical Methodslasma �-ketoisocaproate (KIC) enrichment was measured
y electron impact ionization gas chromatography massVol. 87, No. 5, May 2007

semPa
CIamlrcihpgv(
dam[taE(tab
ssts1
�p1
ffattfwiswtwc(
dc
BBIeaL
LswtawTvtttncsAbpL
SNWctuBdptv�pma1
ROoasOrw
F
pectrometry (GCMS) as described previously (25). Thenrichment of expired CO2 was measured by isotope ratioass spectrometry (VG Sira II, Middlewich, Cheshire, UK).lasma glucose concentrations were measured by a glucosenalyzer (Yellow Springs Instruments, Yellow Springs, OH).
alculationsnsulin-stimulated glucose disposal was calculated as theverage glucose infusion rate (mg/min) during the last 30inutes of the clamp. Based on prior studies from our
aboratory showing that the degree of hyperinsulinemiaeached with this rate of insulin infusion results in near-omplete suppression of endogenous glucose productionn women (26), and the fact that variation in ovarianormones have minimal effects on endogenous glucoseroduction (20, 27, 28), we assumed that endogenouslucose production was completely suppressed in theseolunteers and was not affected by menstrual cycle phase27) or GnRHa treatment (28).
To partition glucose disposal into oxidative and nonoxi-ative pathways, we measured carbohydrate (i.e., glucose)nd fat oxidation using a combination of indirect calorimetryeasurements and estimates of protein oxidation from
13C]leucine, as described previously (26). Leucine oxida-ion is derived from the rate of 13CO2 excretion into expiredir (F13C, �mol/kg · h�1), which is calculated as: FCO2 ·
CO2 · 10/0.81, where FCO2 is the CO2 production rate�mol/kg · h�1), ECO2 is the enrichment of expired 13CO2,he constant 10 accounts for unit changes, and the factor 0.81ccounts for the recovery of 13CO2 released from the bicar-onate pool (29).
During the clamp, the use of endogenous energy sub-trates will be decreased in favor of the use of exogenousubstrates (30). This will alter 13CO2 excretion because ofhe different 13C abundances of endogenous and exogenousubstrates (31). To account for this change, we measured3CO2 excretion in a separate group of six young women (30
1 years; 22 � 1 kg/m2) undergoing an identical clamprotocol as described above, but without administration of3C isotope tracers. Average 13CO2 enrichments derivedrom theses studies were used to correct 13CO2 enrichmentsor contribution from exogenously administered glucose andmino acids, as described previously (25). Dividing F13C byhe rate of 13C infusion (i13C) gives the fraction of the tracerhat is oxidized to CO2 (fox). To calculate leucine oxidation,
ox was then multiplied by leucine appearance rate, whichas calculated from standard equations (25) that were mod-
fied to account for the input of isotope tracer from twoources, as described previously (26). Leucine oxidation dataere used to estimate protein oxidation, with the assumption
hat 8% of body protein is leucine. Protein oxidation dataere used together with VO2 and VCO2 data to calculate
arbohydrate and fat oxidation using standard equations
32). Nonoxidative glucose disposal was calculated as the pertility and Sterility�
ifference between insulin-stimulated glucose disposal andarbohydrate oxidation.
ody Compositionody mass was measured on a metabolic scale (Scale-Tronix,
nc.; Wheaton, IL). Fat mass, fat-free mass, and bone min-ral mass were measured by dual-energy roentgenogrambsorptiometry using a GE Lunar Prodigy densitometer (GEunar Co., Madison, WI). Bone mass data are not reported.
Abdominal adiposity was measured between the L1 and4 vertebral bodies using the Region of Interest option of theoftware after the general approach of Glickman et al. (33),ith minor modifications. The inferior boundary was set at
he top of the iliac crest, and the superior boundary was sett the T12–L1 intervertebral space. The lateral boundariesere drawn to include all soft tissue in the abdominal region.o standardize the cut point placements within the sameolunteer, the aforementioned transverse sections were de-ermined on the scan that provided the best visualization ofhe T12–L1 intervertebral space, and the distance betweenhe superior and inferior cut points was measured to theearest millimeter. Using the transverse section on the iliacrest as a starting point, this distance was then used to set theuperior cut point for the analysis of all subsequent scans.ll scans were analyzed by the same technician, who waslinded to the volunteer’s treatment status. Analysis waserformed using the Prodigy version 5.60.003 software (GEunar Co., Madison, WI) for body composition analysis.
tatisticsormality was confirmed for all variables using the Shapiro-ilk test before analysis. Unpaired t tests were used to
ompare baseline characteristics between groups. Pairedtests were used to compare data between pretreatment follic-lar and luteal phase measurements in the entire cohort.ecause no effect of cycle phase was found on glucoseisposal measures, follicular and luteal phase measurementserformed before treatment were averaged and are referredo as pretreatment values. A repeated measures analysis ofariance (RMANOVA) model was then used to detect group
time interaction effects, with treatment group (GnRHa vs.lacebo) as the between-subjects factor and time (pretreat-ent vs. posttreatment) as the within-subjects factor. All
nalyses were conducted with SPSS software (SPSS version2.0; SPSS, Inc., Chicago, IL).
ESULTSvarian suppression (E2�50 pg/mL) was confirmed in fivef six volunteers randomized to GnRHa treatment 10 daysfter the initial injection. In one volunteer, ovarian suppres-ion was confirmed at 16 days after the initial injection.varian suppression was again confirmed in all women
andomized to GnRHa treatment at the posttreatment study,ith circulating estrogen levels�50 pg/mL (range 14 to 38
g/mL).1133

Tbsobe
teTae
dt�1mpP
rp
oFgpPn2�r�fc
chsl�
Body composition measurements are shown in Table 1.here was no significant effect of menstrual cycle phase onody composition (n � 13). Thus, data were pooled for allubsequent analyses. There were no differences in body sizer composition between the GnRHa and placebo groups ataseline. Moreover, there were no group � time interactionffects observed for any body composition variable.
Indirect calorimetry and substrate oxidation data duringhe clamp are shown in Table 2. There was no significantffect of menstrual cycle phase on any variable (n � 12).here were no differences in baseline values, nor were thereny group � time interaction effects for any of the measures,xcept protein oxidation (P � .02).
Figure 1 shows total, oxidative, and nonoxidative glucoseisposal measurements in the follicular and luteal phases ofhe menstrual cycle. There were no differences in total (10.7
0.6 vs. 10.0 � 0.7 mg/kg fat-free mass/min, P � .45; n �3), oxidative (2.85 � 0.45 vs. 2.61 � 0.38 mg/kg fat-freeass/min, P � .66; n � 12), or nonoxidative glucose dis-
osal (8.11 � 0.63 vs. 7.67 � 0.75 mg/kg fat-free mass/min,� .66; n � 12) between the follicular and luteal phases,
TABLE 1Body composition.
Follicular
GnRHa Placebo
Weight (kg) 62.9 � 2.6 59.7 � 3.0Fat mass (kg) 20.6 � 2.1 16.2 � 1.5Fat-free mass (kg) 40.7 � 1.0 41.8 � 2.3Percent fat 33.3 � 2.3 27.9 � 2.0Intra-abdominal fat (kg) 1.58 � 0.21 1.34 � 0.20Note: Data are mean � SEM.
Cooper. Ovarian hormones and glucose disposal. Fertil Steril 2007.
TABLE 2Indirect calorimetry data under euglycemic–hype
Pre
GnRHa
VO2 (mL/min) 236 � 5VCO2 (mL/min) 197 � 6Protein oxidation (mg/min) 34 � 5Carbohydrate oxidation (mg/min) 114 � 24Fat oxidation (mg/min) 54 � 11Note: Data are mean � SEM. VO2 � oxygen consumption* P � .02 for group � time interaction.
Cooper. Ovarian hormones and glucose disposal. Fertil Steril 2007.
1134 Cooper et al. Ovarian hormones and glucose disposal
espectively. Because of the absence of menstrual cyclehase effects, pretreatment data were pooled.
The effect of ovarian suppression with GnRHa on total,xidative, and nonoxidative glucose disposal is shown inigure 2. Treatment with GnRHa had no effect on totallucose disposal (GnRHa: 10.6 � 0.9 to 10.8 � 0.9 vs.lacebo: 10.2 � 0.7 to 10.4 � 1.0 mg/kg fat-free mass/min,� .99; n � 6 and n � 7, respectively). Similarly, there was
o effect of GnRHa administration on oxidative (GnRHa:.77 � 0.58 to 3.89 � 0.58 vs. placebo: 2.74 � 0.42 to 3.33
0.62 mg/kg fat-free mass/min, P � .52; n � 6 and n � 6,espectively) or nonoxidative (GnRHa: 7.82 � 0.68 to 6.91
0.66 vs. placebo: 7.94 � 0.72 to 7.79 � 0.99 mg/kgat-free mass/min, P � .59; n � 6 and n � 6, respectively)omponents of glucose disposal.
Group mean and individual values for circulating glu-ose and insulin levels under fasting and euglycemic–yperinsulinemic conditions are shown in Figure 3. Ovarianuppression with GnRHa had no effect on fasting glucoseevels (GnRHa: 75.0 � 1.3 to 73.7 � 0.9 vs. placebo: 73.8
1.0 to 72.4 � 0.8 mg/dL, P � .99) or glucose levels
Luteal Posttreatment
GnRHa Placebo GnRHa Placebo
.7 � 2.5 59.9 � 3.2 62.2 � 2.4 59.3 � 2.9
.6 � 2.3 16.1 � 1.7 20.7 � 2.1 15.9 � 1.1
.3 � 1.0 41.8 � 2.5 40.0 � 1.4 41.7 � 2.5
.5 � 2.7 27.6 � 2.5 33.8 � 2.5 27.8 � 1.71 � 0.25 1.36 � 0.22 1.64 � 0.23 1.36 � 0.15
ulinemic conditions.
atment Posttreatment
Placebo GnRHa Placebo
231 � 9 230 � 7 230 � 3195 � 9 203 � 8 201 � 833 � 3 34 � 6 46 � 4*
119 � 18 155 � 24 142 � 2549 � 6 34 � 9 33 � 9
O2 � carbon dioxide production.
622040331.6
rins
tre
, VC
Vol. 87, No. 5, May 2007

d8�e�oc1f
DTnsomttsGai
nrsigasca
socwaefi
F
uring the euglycemic–hyperinsulinemic clamp (GnRHa:2.1 � 1.1 to 80.8 � 0.9 vs. placebo: 83.7 � 0.9 to 84.6
1.4 mg/dL, P � .07). Treatment with GnRHa also had noffect on fasting insulin levels (GnRHa: 12.5 � 1.0 to 12.2
1.1 vs. placebo: 11.3 � 0.5 to 13.5 � 1.1 �IU/mL, P � .17)r insulin levels during the euglycemic–hyperinsulinemiclamp (GnRHa: 134 � 6 to 122 � 7 vs. placebo: 128 � 5 to24 � 6 �IU/mL, P � .38; n � 6 and n � 6, respectively,or posttreatment).
ISCUSSIONhe present study examined the hypothesis that endoge-ous ovarian steroid hormones regulate whole-body insulin-timulated glucose uptake through their effects on non-xidative pathways. To address this hypothesis, weeasured glucose disposal under hyperinsulinemic condi-
ions in healthy, nonobese, premenopausal women duringhe early to midfollicular and midluteal phases of the men-trual cycle and after 2 months of treatment with eithernRHa or placebo. Our results indicate that total, oxidative,
nd nonoxidative glucose disposal are not affected by ovar-an hormone suppression with GnRHa.
Our study shows that a short-term deficiency of endoge-ous ovarian hormones does not influence tissue insulinesponsiveness in nonobese adult women. The present re-ults agree with data from Dumesic et al. (28), who exam-ned the effect of 3 months of leuprolide acetate therapy onlucose disposal in hyperandrogenic, anovulatory womennd healthy controls. An important caveat to this earliertudy, however, was that both hyperandrogenic women andontrols were obese (mean BMI � 35 kg/m2). Because total
FIGURE 1
Effect of menstrual cycle phase on total (n � 13),oxidative (Ox; n � 12), and nonoxidative (NonOx;n � 12) insulin-stimulated glucose disposal.Glucose disposal data are expressed per kilogramof fat-free mass (FFM). Values are mean � SEM.
Cooper. Ovarian hormones and glucose disposal. Fertil Steril 2007.
nd abdominal obesity are important modulators of insulin
ertility and Sterility�
ensitivity (34, 35), it is possible that the absence of an effectf ovarian hormone deficiency on glucose disposal wasaused by the confounding effect of adiposity. In otherords, ovarian hormone deficiency may not affect insulin
ction in obese populations above and beyond the inhibitoryffect of adiposity (i.e., floor effect). Our results extend thesendings to show that in the absence of the confounding
FIGURE 2
Effect of GnRHa or placebo administration on total(A), oxidative (B), and nonoxidative (C) insulin-stimulated glucose disposal. For oxidative andnonoxidative disposal, n � 6 for the placebogroup. Pretreatment values are filled bars, andposttreatment values are open bars. Pretreatmentvalues are the average of follicular and lutealphase measurements. Glucose disposal data areexpressed per kilogram of fat-free mass (FFM).Values are mean � SEM.
Cooper. Ovarian hormones and glucose disposal. Fertil Steril 2007.
1135

ec
mcnrfdgwtcd
(mesai
atgtisctwesa
pwaaomet
ffect of obesity, GnRHa-induced ovarian hormone defi-iency has no effect on insulin-stimulated glucose disposal.
The effect of ovarian hormones on glucose metabolismay not be apparent when only total glucose disposal is
onsidered. For instance, there may be reciprocal changes inonoxidative and oxidative glucose disposal that effectivelyesult in no net change in total glucose disposal. To accountor this possibility, we also measured oxidative and nonoxi-ative components of glucose disposal. In accord with totallucose disposal, neither oxidative nor nonoxidative path-ays of glucose disposal were altered by GnRHa adminis-
ration. Thus, our data suggest that ovarian hormone defi-iency does not alter intracellular pathways of glucoseisposal.
Our results, together with the findings of Dumesic et al.28) and studies performed during different phases of theenstrual cycle (27, 36, 37), argue against a role for endog-
nous ovarian hormones in the regulation of tissue insulinensitivity in adult women. This conclusion is at odds withnimal studies showing that ovariectomy promotes tissue
FIGURE 3
Group mean and individual values for circulating glucduring the hyperinsulinemic clamp (B and D) in womplacebo (n � 7; open squares). Pre � pretreatment;placebo group in B have pretreatment and posttreatmn � 6 for placebo for D.
Cooper. Ovarian hormones and glucose disposal. Fertil Steril 2007.
nsulin resistance (5–8). Differences between human and p
1136 Cooper et al. Ovarian hormones and glucose disposal
nimal studies may be explained by species differences inhe effect of sex steroids on tissue insulin action and/orlucose metabolism. In addition, an important caveat tohese animal studies is that ovariectomy stimulates foodntake and body fat accumulation (38–39), which has beenhown to reduce insulin-stimulated glucose disposal by de-reasing flux through nonoxidative pathways (40). In con-rast, we did not observe changes in total or central adiposityith GnRHa administration (Table 1). Thus, species differ-
nces in the effect of ovarian hormones on energy homeosta-is may account for divergent findings with respect to insulinction.
The short-term nature of our study influences the inter-retation of our findings. Our model of ovarian suppressionith GnRHa is not representative of the hormonal changes that
ccompany the normal menopause. In this respect, our findingsre limited to the physiological effects of a short-term period ofvarian hormone deficiency on insulin-stimulated glucoseetabolism. However, we specifically chose to study the
ffect of GnRHa over a short period of time (i.e., 2 months)o minimize the effects of ovarian suppression on other
and insulin levels under fasting (A and C) andndomized to GnRHa (n � 6; blue squares) or� posttreatment. Note: three volunteers in the
t values of 84 and 86 mg/dL, respectively, and
oseen raPost
en
hysiological systems that could influence glucose disposal
Vol. 87, No. 5, May 2007

mffipteosihmohr4sapboagat
ePrrtrdacAswatcgcdgiotiatow
htt
wtip
At
R
1
1
1
1
1
1
1
1
1
F
easurements. In this respect, our study design permits aocused examination of the effects of ovarian hormone de-ciency, per se, on insulin-stimulated glucose disposal. Im-ortantly, this period of study should be more than sufficiento allow for any alterations in gene transcription and proteinxpression of insulin signaling pathways and glucose metab-lism machinery in target tissues. On the other hand, thetudy period may not be sufficient to observe changes innsulin sensitivity related to the secondary effects of ovarianormones on other physiological systems, such as whatight occur during the normal menopause. For example,
varian hormone deficiency associated with the menopauseas been hypothesized to cause accumulation of body fat andedistribution of fat toward the abdominal compartment (41,2). With prolonged periods of ovarian hormone deficiency,uch changes in body fat levels and distribution may developnd could promote insulin resistance. Indeed, a significantroportion of the age-related decline in insulin sensitivity iselieved to be caused by changes in the size and distributionf adipose tissue (43–45). In this context, our conclusionsre limited to the short-term effect of ovarian suppression onlucose metabolism. Nevertheless, our results do not supportdirect effect of ovarian hormones on tissue insulin sensi-
ivity or intracellular pathways of glucose metabolism.
We should acknowledge that our results could be influ-nced by the inclusion of amino acids during the clamp.revious studies have shown that infusion of amino acidseduces whole-body and skeletal muscle glucose uptake inesponse to insulin (46, 47), although it is important to notehat this finding is not unanimous (48, 49). For severaleasons, we believe that any effect of amino acids on glucoseisposal in our study was minimal. First, the effect of aminocids to inhibit glucose disposal (46) is similar mechanisti-ally to the effects of fatty acids on glucose disposal (50).lthough substrate-induced insulin resistance has been
hown in men, recent studies suggest that it does not occur inomen (51). Nonetheless, one could argue that if women are
fforded protection against substrate-induced insulin resis-ance by ovarian hormones (51), women treated with GnRHaould become susceptible to an effect of amino acids onlucose disposal. This possibility is unlikely, however, be-ause there were no changes in insulin-stimulated glucoseisposal in either group with treatment. Second, rates oflucose disposal reported in the present study are very sim-lar to those reported in healthy premenopausal women byur laboratory (9) and others (51, 52). In comparison withhese studies, we find no evidence for a profound reductionn insulin-stimulated glucose disposal reported with aminocid administration reported by others (46). Thus, we favorhe interpretation that any effect of the amino acid infusionn insulin-stimulated glucose disposal in the present studyas minimal.
In conclusion, our study showed that endogenous ovarianormone suppression brought about by GnRHa administra-ion in healthy, nonobese women does not alter total, oxida-
ive, or nonoxidative glucose disposal. These findings, alongertility and Sterility�
ith prior studies (27, 28, 36, 37), support the hypothesishat endogenous ovarian hormones do not regulate tissuensulin sensitivity or intracellular pathways of glucose dis-osal in adult women.
cknowledgments: The authors thank all of the participants who volun-eered their time for this study.
EFERENCES1. Rowe JR, Minaker KD, Pallotta JA, Flier JS. Characterization of the
insulin resistance of aging. J Clin Invest 1983;71:1581–7.2. Defronzo RA. Glucose intolerance and aging. Evidence for tissue
insensitivity to insulin. Diabetes 1979;28:1095–101.3. Wu SI, Chou P, Tsai ST. The impact of years since menopause on the
development of impaired glucose tolerance. J Clin Epidemiol 2001;54:117–20.
4. Godsland IF. Influence of female sex steroids on glucose metabolismand insulin action: human studies. J Intern Med 1996;240:25–49.
5. Puah JA, Bailey CJ. Effect of ovarian hormones on glucose metabolismin mouse soleus muscle. Endocrinol 1985;117:1336–40.
6. Ahmed-Sorour H, Bailey CJ. Role of ovarian hormones in the long-term control of glucose homeostasis. Hormone Res 1980;13:396–403.
7. Kumagai S, Holmang A, Björntorp P. The effects of oestrogen andprogesterone on insulin sensitivity in female rats. Acta Physiol Scand1993;149:91–7.
8. Rincon J, Holmang A, Wahlstrom EO, Lonnroth P, Björntorp P, ZierathJR, et al. Mechanisms behind insulin resistance in rat skeletal muscleafter oophorectomy and additional testosterone treatment. Diabetes1996;45:615–21.
9. Toth MJ, Sites CK, Eltabbakh GH, Poehlman ET. Effect of menopausalstatus on insulin-stimulated glucose disposal: comparison of middle-aged premenopausal and early postmenopausal women. Diabetes Care2000;23:801–6.
0. Walton C, Godsland IF, Proudler AJ, Wynn V, Stevenson JC. Theeffects of the menopause on insulin sensitivity, secretion and elimina-tion in non-obese, healthy women. Eur J Clin Invest 1993;23:466–73.
1. Proudler AJ, Felton CV, Stevenson JC. Ageing and the response ofplasma insulin, glucose and C-peptide concentrations to intravenousglucose in postmenopausal women. Clin Sci 1992;83:489–94.
2. O’Sullivan AJ, Ho KKY. A comparison of the effects of oral andtransdermal estrogen replacement on insulin sensitivity in postmeno-pausal women. J Clin Endocrinol Metab 1995;80:1783–8.
3. Cagnacci A, Soldani R, Carriero PL, Paoletti AM, Fioretti P, Melis GB.Effects of low doses of transdermal 17�-estradiol on carbohydratemetabolism in postmenopausal women. J Clin Endocrinol Metab 1992;74:1396–40.
4. Lasco A, Alvaro S, Frisina N, Di Benedetto A, Denuzzo G, CucinottaD. Long-term transdermal estrogen therapy improves lipid profile butnot insulin resistance in healthy postmenopausal women. Diabetes Care2000;23:422–4.
5. Duncan AC, Lyall H, Roberts RN, Petrie JR, Perera MJ, Monaghan S,et al. The effect of estradiol and a combined estradiol/progestagenpreparation on insulin sensitivity in healthy postmenopausal women.J Clin Endocrinol Metab 1999;84:2402–7.
6. Cucinelli F, Paparella P, Soranna L, Barini A, Cinque B, Mancuso S, etal. Differential effect of transdermal estrogen plus progestagen replace-ment therapy on insulin metabolism in postmenopausal women: rela-tion to their insulinemic secretion. Eur J Endocrinol 1999;140:215–23.
7. Mattiasson I, Rendell M, Tornquist C, Jeppsson S, Hulthen UL. Effectsof estrogen replacement therapy on abdominal fat compartments asrelated to glucose and lipid metabolism in early postmenopausalwomen. Horm Metab Res 2002;34:583–8.
8. Walker RJ, Lewis-Barned NJ, Sutherland WH, Goulding A, EdwardsEA, deJong SA, et al. The effects of sequential combined oral 17�-
estradiol and norethisterone acetate on insulin sensitivity and body1137

1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
composition in healthy postmenopausal women: a randomized singleblind placebo-controlled study. Menopause 2001;8:27–32.
9. Kimmerle R, Heinemann L, Heise T, Bender R, Weyer C, HirshbergerS, et al. Influence of continuous combined estradiol-norethisteroneacetate preparations on insulin sensitivity in postmenopausal nondia-betic women. Menopause 1999;6:36–42.
0. Sites CK, L’Hommedieu GD, Toth MJ, Brochu M, Cooper BC,Fairhurst PA. The effect of hormone replacement therapy on bodycomposition, body fat distribution, and insulin sensitivity in meno-pausal women: a randomized, double-blind, placebo-controlled trial.J Clin Endocrinol Metab 2005;90:2701–7.
1. Beckett T, Tchernof A, Toth MJ. Effect of ovariectomy and estradiolreplacement on skeletal muscle enzyme activity in female rats. Metab-olism 2002;51:1397–401.
2. Toth MJ, Sites CK, Matthews DE, Casson PR. Ovarian suppressionwith gonadotropin-releasing hormone agonist reduces whole body pro-tein turnover in women. Am J Physiol 2006;291:E483–90.
3. Cooper BC, Sites CK, Fairhurst PA, Toth MJ. Evidence against a rolefor ovarian hormones in the regulation of blood flow. Fertil Steril2006;86:440–7.
4. Abumrad NN, Rabin D, Diamond MP, Lacy WW. Use of a heatedsuperficial hand vein as an alternative site for the measurement ofamino acid concentrations and for the study of glucose and alaninekinetics in man. Metab Clin Exp 1981;20:936–40.
5. Toth MJ, Tchernof A, Rosen CJ, Matthews DE, Poehlman ET. Regu-lation of protein metabolism in middle-aged, premenopausal women:roles of adiposity and estradiol. J Clin Endocrinol Metab 2000;85:1382–7.
6. Toth MJ, Sites CK, Cefalu WT, Matthews DE, Poehlman ET. Deter-minants of insulin-stimulated glucose disposal in middle-aged, pre-menopausal women. Am J Physiol Endocrinol Metab 2001;281:E113–21.
7. Diamond MP, Jacob R, Connolly-Diamond M, DeFronzo RA. Glucosemetabolism during the menstrual cycle. Assessment with the euglyce-mic, hyperinsulinemic clamp. J Reprod Med 1993;38:417–21.
8. Dumesic DA, Nielsen MF, Abbott DH, Eisner JR, Nair KS, Rizza RA.Insulin action during variable hyperglycemic-hyperinsulinemic infu-sions in hyperandrogenic anovulatory patients and healthy women.Fertil Steril 1999;72:458–66.
9. Allsop JR, Wolfe RR, Burke JF. Tracer priming the bicarbonate pool.J Appl Physiol 1978;45:137–9.
0. Wolfe RR, Shaw JHF, Nadel ER, Wolfe MH. Effect of substrate intakeand physiological state on background 13CO2 enrichment. J ApplPhysiol 1984;56:230–4.
1. Schoeller DA, Klein PD, Watkins JB, Heim T, MacLean WC. 13Cabundances of nutrients and the effect of variations in 13C isotopicabundances of test meals formulated for 13CO2 breath tests. Am J ClinNutr 1980;33:2375–85.
2. Simonson DC, DeFronzo RA. Indirect calorimetry: methodological andinterpretative problems. Am J Physiol Endocrinol Metab 1990;258:E399–412.
3. Glickman SG, Marn CS, Supiano MA, Dengel DR. Validity and reli-ability of dual-energy x-ray absorptiometry for the assessment of ab-dominal adiposity. J Appl Physiol 2004;97:509–14.
4. Ross R, Freeman J, Hudson R, Janssen I. Abdominal obesity, musclecomposition, and insulin resistance in premenopausal women. J Clin
Endocrinol Metab 2002;87:5044–51.1138 Cooper et al. Ovarian hormones and glucose disposal
5. Abate N, Haffner SM, Garg A, Peshock RM, Grundy SM. Sex steroidhormones, upper body obesity, and insulin resistance. J Clin EndocrinolMetab 2002;87:4522–7.
6. Toth EL, Suthijumroon A, Crockford PM, Ryan EA. Insulin action doesnot change during the menstrual cycle in normal women. J Clin Endo-crinol Metab 1987;64:74–80.
7. Yki-Jarvinen H. Insulin sensitivity during the menstrual cycle. J ClinEndocrinol Metab 1984;59:350–3.
8. Richard D. Effect of ovarian hormones on energy balance and brownadipose tissue thermogenesis. Am J Physiol Renal Physiol 1986;250:R245–9.
9. Chen Y, Heiman ML. Increased weight gain after ovariectomy is not aconsequence of leptin resistance. Am J Physiol Endocrinol Metab2001;280:E315–22.
0. Banerjee S, Saenger P, Hu M, Chen W, Barzilai N. Fat accretion andthe regulation of insulin-mediated glycogen synthesis after puberty inrats. Am J Physiol Renal Physiol 1997;273:R1534–9.
1. Toth MJ, Tchernof A, Sites CK, Poehlman ET. Effect of menopausalstatus on body composition and abdominal fat distribution. Int J Obes2000;24:226–31.
2. Tchernof A, Desmeules A, Richard C, LaBerge P, Daris M, Mailloux J,et al. Ovarian hormone status and abdominal visceral adipose tissuemetabolism. J Clin Endocrinol Metab 2004;89:3425–30.
3. Ferrannini E, Vichi S, Beck-Nielsen H, Laasku M, Paolisso G, Smith U,European Group for the Study of Insulin Resistance (EGIR). Insulinaction and age. Diabetes 1996;45:947–53.
4. Kohrt WM, Kirwan JP, Staten MA, Bourey RE, King DS, Holloszy JO.Insulin resistance in aging is related to abdominal obesity. Diabetes1993;42:273–81.
5. Basu R, Breda E, Oberg AL, Powell CC, Man CD, Basu A, et al.Mechanisms of the age-associated deterioration in glucose tolerance.Contribution of alterations in insulin secretion, action and clearance.Diabetes 2003;52:1738–48.
6. Krebs M, Krssak M, Bernroider E, Anderwald C, Brehm A, MeyerspeerM, et al. Mechanism of amino acid-induced skeletal muscle insulinresistance in humans. Diabetes 2002;51:599–605.
7. Pisters PWT, Restifo NP, Cersosimo E, Brennan MF. The effects ofeuglycemic hyperinsulinemia and amino acid infusion on regional andwhole body glucose disposal in man. Metab Clin Exp 1991;40:59–65.
8. Buckspan R, Hoxworth B, Cersosimo E, Devlin JT, Horton E, AbumradN. alpha-Ketoisocaproate is superior to leucine in sparing glucoseutilization in humans. Am J Physiol Endocrinol Metab 1986;251:E648 –53.
9. Boden G, Tappy L. Effects of amino acids on glucose disposal. Dia-betes 1990;39:1079–84.
0. Roden M, Price TB, Perseghin G, Petersen KF, Rothman DL, ClineGW, et al. Mechanism of free fatty acid-induced insulin resistance inhumans. J Clin Invest 1997;97:2859–65.
1. Frias JP, Macaraeg GB, Ofrecio J, Yu JG, Olefsky JM, Kruszynska YT.Decreased susceptibility to fatty acid-induced peripheral tissue insulinresistance in women. Diabetes 2001;50:1344–50.
2. Perseghin G, Scifo P, Pagliato E, Battezzati A, Benedini S, Soldini L,et al. Gender factors affect fatty acids-induced insulin resistance innon-obese humans: effects of oral steroidal contraception. J Clin En-
docrinol Metab 2001;86:3188–96.Vol. 87, No. 5, May 2007

REPRODUCTIVE SURGERY
Hyaluronic acid fluid agents for the prevention ofadhesions after fertility-preserving gynecologicalsurgery: a meta-analysis of randomizedcontrolled trialsMostafa Metwally, M.R.C.O.G.,a Dylan Gorvy, Ph.D.,b Andrew Watson, M.R.C.O.G.,c
and Tin Chiu Li, Ph.D.a
a The Academic Unit of Reproductive and Developmental Medicine, The University of Sheffield and Sheffield Teaching
Hospitals, Jessop Wing, Sheffield; b University of Liverpool, Philip Leverhulme Equine Hospital, Cheshire; and c Department
of Obstetrics and Gynecology, Tameside General Hospital, Lancashire, United Kingdom
Objective: To investigate the role of hyaluronic acid–based fluid agents in the prevention of adhesions after fer-tility-preserving gynecological surgery.Design: Meta-analysis.Setting: The authors searched the Cochrane Menstrual Disorders and Subfertility Group Specialized Register ofControlled Trials, The Cochrane Central Register of Controlled Trials, MEDLINE, and EMBASE for randomizedcontrolled trials of hyaluronic acid fluid agents compared with no treatment or placebo.Patient(s): Women undergoing fertility-preserving gynecological surgery.Intervention(s): Hyaluronic acid fluid agents.Main Outcome Measure(s): [1] Prevalence and change in adhesion severity at second-look laparoscopy and [2]live birth rate.Result(s): Four studies were included in the meta-analysis. The use of hyaluronic acid agents was associated witha decrease in the prevalence of adhesions at second-look laparoscopy (odds ratio, 0.31; 95% confidence interval,0.19 to 0.51) and a lesser chance of deterioration of preexisting adhesions (odds ratio, 0.28; 95% confidence in-terval, 0.12 to 0.66). There was, however, no evidence for improvement in the adhesion score (odds ratio, 1.55;95% confidence interval, 0.82 to 2.92).Conclusion(s): There is evidence that hyaluronic acid agents may decrease the prevalence of adhesions and pre-vent the deterioration of preexisting adhesions. However, because of the limited number of studies available, thisevidence should still be interpreted with caution. (Fertil Steril� 2007;87:1139–46. �2007 by American Society forReproductive Medicine.)
Key Words: Meta-analysis, adhesions, hyaluronic acid
Intraperitoneal adhesions are an important cause of postoper-ative intestinal obstruction, abdominal discomfort, and infer-tility (1). Despite careful attention to minimize tissue traumaand ensure hemostasis, pelvic surgery is associated with bothde novo adhesion formation and reformation. Adhesionsoccur after approximately 80% of gynecological surgicalprocedures, and reformation after surgical lysis occurs post-operatively in 85% of patients (2, 3).
Despite improvement in the success of IVF, reproductivesurgery remains an important component of assisted repro-
Received April 13, 2006; revised and accepted September 14, 2006.
A.W. received lecture fees from Gynecare (Edinburgh, Germany) for a
lecture on Intergel in 1998.
Reprint requests: Mostafa Metwally, M.R.C.O.G., Academic Unit of Re-
productive and Developmental Medicine, University of Sheffield, Jes-
sop Wing, Tree Root Walk, S10 4ED, Sheffield, United Kingdom (FAX:
44-114-2261074; E-mail: [email protected]).
0015-0282/07/$32.00doi:10.1016/j.fertnstert.2006.09.018 Copyright ª2007 American
ductive technologies (ART) for many couples. In addition,many pelvic operations are performed on women of repro-ductive age for indications unrelated to fertility. Adhesionformation after these procedures may compromise futurefertility of the patient.
A study investigating the effect of tubal and ovarian adhe-siolysis on subsequent fertility found that the cumulativepregnancy rate in the group that underwent salpingo-ovariol-ysis was three times higher than that in the nontreated group(4, 5); hence, adhesion preventive measures are important.Numerous substances have been used experimentally in ani-mal models, including many that have been advocated for useduring surgery in human beings (6).
Hyaluronic acid–containing solutions or fluid-like agents,including ferric hyaluronate (Intergel; Gynecare Worldwide,Ethicon Inc., Somerville, NJ), autocross-linked hyaluronic
Fertility and Sterility� Vol. 87, No. 5, May 2007 1139Society for Reproductive Medicine, Published by Elsevier Inc.

acid gel (Hyalobarrier gel; Baxter, Pisa, Italy), and Sepracoat(Genzyme Corporation, Cambridge, MA), are among thoseinvestigated.
This meta-analysis forms part of a Cochrane review (7)on fluid and pharmacological agents that are used for theprevention of adhesions after fertility-preserving gyneco-logical surgery. The aim is to evaluate the impact of hyalur-onic acid–containing fluid agents that are used as adjuvantsduring pelvic surgery on the prevalence and/or severity ofpostoperative adhesion formation after fertility-preservinggynecological surgery.
MATERIALS AND METHODS
Criteria for Study Inclusion
Randomized controlled trials of hyaluronic acid–containingfluid agents compared with either no treatment or placebo.
Participants
Participants included women in their reproductive period whowere undergoing fertility-preserving pelvic surgery (laparos-copy or laparotomy). Patients in whom fertility was not con-served, such as in the case of hysterectomy, were not included.
Search Strategy
The review drew on the search strategy that was developed forthe Menstrual Disorders and Subfertility Group. We searchedthe Cochrane Menstrual Disorders and Subfertility Group Spe-cialized Register of Controlled Trials (last searched November2005), The Cochrane Central Register of Controlled Trials(last searched November 2005), MEDLINE (1966 to week 2of November 2005), and EMBASE (1980 to week 47 of 2005).
Data Extraction
Only randomized controlled trials were included (Fig. 1). Fur-ther information was sought from investigators whose articles
FIGURE 1
Flow chart for data extraction and analysis.RCT ¼ randomized controlled trial.
5 Potentially relevant RCTs identified
No RCTs excluded
5 RCTs retrieved for moredetailed
One RCT excluded from meta-analysis. Data were presented in agraphical form. (n=1)
4 RCTs included in meta-analysis
Metwally. Hyaluronic acid for adhesion prevention. Fertil Steril 2007.
1140 Metwally et al. Hyaluronic acid for adhesion preven
contained insufficient information to make a decision regard-ing eligibility. Surgery performed included both open andlaparoscopic procedures. For each trial, information was col-lected regarding the location of the study, methodology, theparticipants (age and eligibility criteria), the nature of the in-terventions, and data related to the specified outcomes.
Where continuous data were presented graphically and ex-act figures could not be obtained, the data were not includedin the meta-analysis (8).
Quality Assessment
Two of the reviewers (M.M. and A.W.) independently as-sessed the quality of all studies that were deemed eligiblefor the review, on the basis of the method of randomization,quality of allocation concealment, use of blinding, inten-tion-to-treat analysis, and power calculation. Quality assess-ment of the included studies is seen in Table 1.
Outcome Measures
These included the following: prevalence of adhesions at sec-ond-look laparoscopy, improvement or deterioration of adhe-sion score at second-look laparoscopy, change in meanadhesion score or extent (cm2), and live birth rate.
Quantitative Data Analysis
Statistical analysis was performed in accordance with theguidelines developed by the Cochrane Collaboration (9). Het-erogeneity between studies was determined by examining theresults of the c2 and I2 statistics. A c2 statistic that was largerthan its degree of freedom or an I2 statistic with a value of>50% provided evidence of heterogeneity of treatment effects.Where appropriate, the outcomes were pooled statistically.
Dichotomous data extracted from the individual studieswere expressed as an odds ratio with 95% confidence inter-vals (CIs) and were combined for meta-analysis by usingthe RevMan software (Review Manager, Version 4.2 for Win-dows; Cochrane Collaboration, Nordic Cochrane Centre,Copenhagen, Denmark).
Because of the use of different scoring systems to describethe severity and extent of adhesions, we used the standardizedmean difference to compare continuous data. The standard-ized mean difference was calculated by using the mean andSD. Where the SEM was given, it was converted to SDs bymultiplying SEM by the square root of the number of patients.
RESULTS
Study Details
All studies investigating hyaluronic acid–containing fluidswere combined. Statistical analysis of the data was possibleonly from four of five studies identified.
In the studies measuring the prevalence and change in ad-hesion severity, there was no evidence of significant
tion Vol. 87, No. 5, May 2007

TABLE 1Quality assessment of included studies.
Study Pellicano et al. (12) Lundorff et al. (11) Johns et al. (10) Diamond (13)
Allocationconcealment clear
Yes No No Yes
Randomization True True True TrueBlinding Yes Yes Yes YesIntention-to-treat
analysisYes No No No
Power calculation No No No No
Metwally. Hyaluronic acid for adhesion prevention. Fertil Steril 2007.
heterogeneity detected between the studies, as determined bythe overlapping of the CIs and by the I2 and c2 statistics(Figs. 2 and 3). Three studies investigated the role of 0.5%ferric hyaluronate gel (Intergel; 365 total patients in all threestudies) (8, 10, 11), with lactated Ringer’s solution used asthe control.
One study with 36 women investigated autocross-linkedhyaluronic acid gel (Hyalobarrier) and used no treatmentfor the control group (12). The final study by Diamond (13)investigated the role of dilute hyaluronic acid solution (Se-pracoat) and included 245 women with phosphate-bufferedsaline as the placebo control. Only the study by Pellicanoet al. (12) stated infertility as an inclusion criterion, andnone of the five studies evaluated pregnancy as an outcome.
Only one study (14) performed laparoscopy as the primaryprocedure (laparoscopic myomectomy); the remaining stud-
Fertility and Sterility�
ies involved a laparotomy and peritoneal surgery for a varietyof conditions (Table 2).
Prevalence of Adhesions
Four studies commented on the prevalence of adhesions at sec-ond-look laparoscopy (10–13) (Fig. 2) and showed evidencefor a decreased prevalence of adhesions in patients whowere treated with hyaluronic acid, compared with those givenplacebo or no treatment (odds ratio, 0.31; 95% CI, 0.19–0.51).
Change in Adhesion Score
Lundorff et al. (11) and Johns et al. (10) recorded the changein the adhesion score at second-look laparoscopy. Both stud-ies used the American Fertility Society score. In the meta-analysis, change in adhesion scores was treated as a binaryoutcome with two levels; deterioration, defined as a higher
FIGURE 2
Prevalence of adhesions at second-look laparoscopy. There is a significant decrease in the prevalence ofadhesions at second look. OR ¼ odds ratio.
Metwally. Hyaluronic acid for adhesion prevention. Fertil Steril 2007.
1141
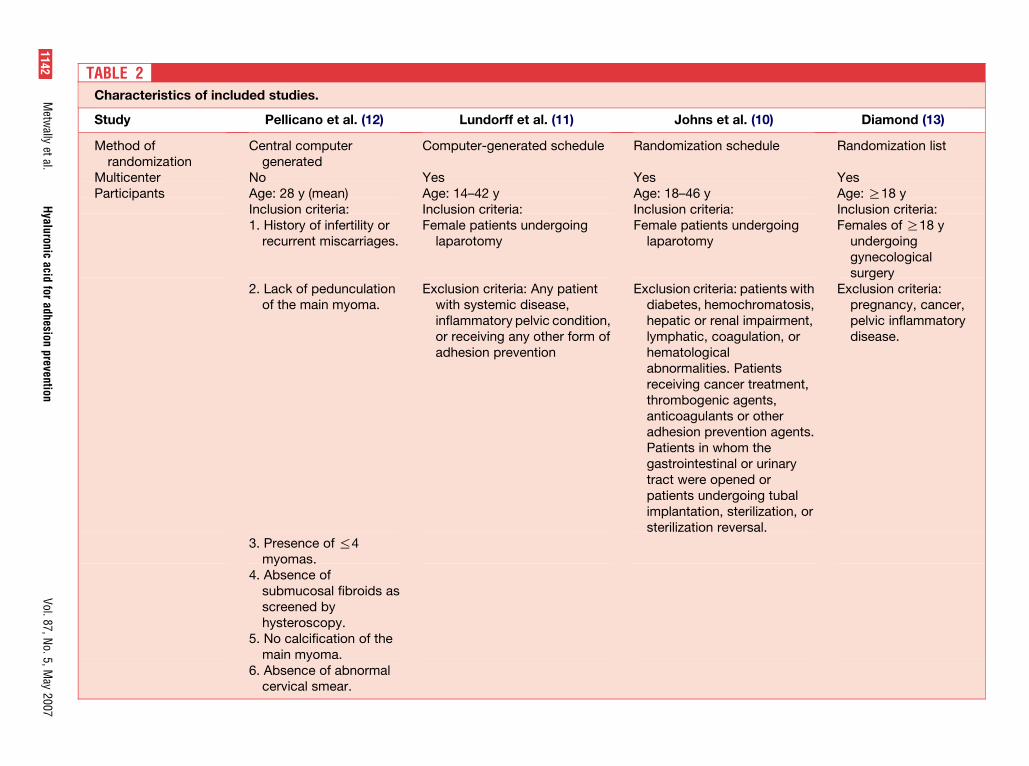
al. (10) Diamond (13)
chedule Randomization list
YesAge: R18 yInclusion criteria:
undergoing Females of R18 yundergoinggynecologicalsurgery
: patients withchromatosis,l impairment,gulation, or
Patientser treatment,agents,or otherntion agents.m thel or urinaryned orgoing tubalterilization, orersal.
Exclusion criteria:pregnancy, cancer,pelvic inflammatorydisease.
TABLE 2Characteristics of included studies.
Study Pellicano et al. (12) Lundorff et al. (11) Johns et
Method ofrandomization
Central computergenerated
Computer-generated schedule Randomization s
Multicenter No Yes YesParticipants Age: 28 y (mean) Age: 14–42 y Age: 18–46 y
Inclusion criteria: Inclusion criteria: Inclusion criteria:1. History of infertility or
recurrent miscarriages.Female patients undergoing
laparotomyFemale patients
laparotomy
2. Lack of pedunculationof the main myoma.
Exclusion criteria: Any patientwith systemic disease,inflammatory pelvic condition,or receiving any other form ofadhesion prevention
Exclusion criteriadiabetes, hemohepatic or renalymphatic, coahematologicalabnormalities.receiving cancthrombogenicanticoagulantsadhesion prevePatients in whogastrointestinatract were opepatients underimplantation, ssterilization rev
3. Presence of %4myomas.
4. Absence ofsubmucosal fibroids asscreened byhysteroscopy.
5. No calcification of themain myoma.
6. Absence of abnormalcervical smear.
1142M
etwally
etal.
Hyaluronic
acidfor
adhesionprevention
Vol.
87,N
o.5,
May
2007

al. (10) Diamond (13)
Laparotomy
ted Ringer’s Sepracoat vs. placebo
sent atparoscopy.
[1] Adhesions presentat second-looklaparoscopy
of adhesion [2] Mean adhesionscore
of adhesion [3] Mean extent ofadhesion score
ed AFS.
[4] Mean incidence ofde novo adhesionsat second-looklaparoscopy
duction inscore
[5] Mean extent ofadhesion score atsecond-looklaparoscopy.
xtent of
27740 d (average)
TABLE 2Continued.
Study Pellicano et al. (12) Lundorff et al. (11) Johns et
7. Negative urinepregnancy test.
Exclusion criteria:Patients who did not fulfill
the inclusion criteria.Surgery Laparoscopic
myomectomyLaparotomy Laparotomy
Intervention Autocross-linkedhyaluronic acid gel vs.no treatment
Intergel vs. lactated Ringer’s Intergel vs. lacta
Outcomes [1] Presence of adhesionsat second-looklaparoscopy.
[1] Presence of adhesions atsecond look.
[1] Adhesions presecond-look la
[2] Incidence ofadhesions with regardsto the site of theprimary myoma
[2] Improvement or deteriorationof adhesion. scores at secondlook.
[2] Improvementscore
[3] Change in mean adhesionscore.
[3] Deteriorationscore
[4] Severity and extent ofadhesions.
[4] Shift in modifiadhesion score
[5] Modified AFS scorecategorized by surgicalprocedure.
[5] Percentage remodified AFS
[6] Severity and eadhesions
Sample size 36 77 281Follow-up (time at
which second-looklaparoscopy wasperformed)
60–90 d 6–12 wk 6–12 wk
Note: AFS ¼ American Fertility Society.
Metwally. Hyaluronic acid for adhesion prevention. Fertil Steril 2007.
Fertilityand
Sterility
�1143

FIGURE 3
Deterioration of adhesion score at second-look laparoscopy. Patients in the control group hadsignificantly worse adhesion scores on second-look laparoscopy, compared with those who receivedhyaluronic acid. OR ¼ odds ratio.
Metwally. Hyaluronic acid for adhesion prevention. Fertil Steril 2007.
adhesion score, or improvement, defined as a lower adhesionscore. Although there was no evidence for improved adhesionscores in the treatment group (odds ratio, 1.55; 95% CI, 0.82–2.92), there was a significant deterioration in the adhesionscore in the control group (odds ratio, 0.28; 95% CI, 0.12–0.66; Fig. 3).
Mean Adhesion Score
The mean adhesion score was calculated from two studies(11, 13); the result showed no significant difference betweentreatment and control groups (standardized mean difference,39.76; 95% CI, �114.6–35)
DISCUSSION
Hyaluronic acid is a linear polysaccharide with repeating di-saccharide units that are composed of sodium D-glucuronateand N-acetyl-D-glucosamine. It is a major component ofmany body tissues and fluids, in which it provides mechani-cally protective and physically supportive roles (10).
Hyaluronic acid solutions have been shown in both labora-tory animals (15) and clinical trials (13) to prevent adhesionformation after abdominopelvic surgery. Intergel, Sepracoat,and Hyalobarrier are all solutions that contain hyaluronicacid as the active component, and accordingly, this studyhas combined all these agents in one meta-analysis. We be-lieved it appropriate to combine the effect of different agents,all sharing the common basic component, hyaluronic acid,because of the absence of heterogeneity when the studieswere combined; that is, a similar effect for all hyaluronicacid agents was observed.
1144 Metwally et al. Hyaluronic acid for adhesion preven
Hyalobarrier is a crosslinked derivative of hyaluronic acidthat is characterized by its high viscosity (14). Intergel (0.5%hyaluronic acid) is a sterile, nonpyrogenic gel of highly puri-fied sodium hyaluronate that is ionically crosslinked with fer-ric ion and adjusted to isotonicity with sodium chloride (11).Crosslinking between carboxylate groups on the hyaluronicacid molecule with ferric ions results in a marked increasein viscosity (11).
Intergel was approved for use in the United States on No-vember 16, 2001 and was intended to be used in open, conser-vative gynecological surgery as an adjunct to good surgicaltechnique. After off-license use in laparoscopic surgery,side effects were reported, namely pelvic pain and allergic re-actions. Accordingly, Intergel was removed from the marketin 2003, pending further investigation.
Finally, Sepracoat (0.4% solution of sodium hyaluronate)failed to gain Food and Drug Administration approval in1998 as a result of a lack of significant evidence from studiesin human beings. Despite the fact that some of the productsmentioned in this article have been withdrawn from the mar-ket, they all draw on a common chemical structure and aretherefore worthy of investigation.
Four of five studies were included in the meta-analysis; allfour of these studies evaluated the prevalence of adhesions atsecond-look laparoscopy and showed a significant reductionin the prevalence of adhesions. When one evaluates the otheroutcomes, it is important to note that the number of studiesincluded in the meta-analysis was limited (Figs. 3–5). The ev-idence therefore is less robust regarding the change in adhe-sion scores. This only serves to highlight the need for more
tion Vol. 87, No. 5, May 2007

FIGURE 4
Improvement of adhesion score at second-look laparoscopy. There is no evidence for a significantimprovement in adhesion scores with the use of hyaluronic agents. OR ¼ odds ratio.
Metwally. Hyaluronic acid for adhesion prevention. Fertil Steril 2007.
studies. Nevertheless, the available data suggest a decreasedchance of deterioration of the adhesion score when hyalur-onic acid agents were used.
Data were represented graphically in the study byThornton et al. (8) and were excluded from the meta-analysisbecause exact numerical data could not be obtained. Theresults of this study nevertheless agreed with the result of
Fertility and Sterility�
the meta-analysis, showing a lower prevalence of adhesionsat second-look laparoscopy in patients who were treatedwith hyaluronic acid; when adhesions did occur, they weresignificantly less extensive and severe.
Three of the four studies (10, 11, 13) included patientsundergoing laparotomy, whereas the remaining study byPellicano et al. (12) included patients undergoing
FIGURE 5
Mean adhesion score. There is no evidence of a significant difference in the mean adhesion scorebetween the two groups.
Metwally. Hyaluronic acid for adhesion prevention. Fertil Steril 2007.
1145

laparoscopy. Even though the method of surgery was not con-sistent, the same effect for hyaluronic acid was observedacross the studies.
None of the studies reported pregnancy rates. Because anattempt to decrease adhesions after fertility-preserving pelvicsurgery aims mainly at preserving fertility, future studiesshould focus on live birth rate as a primary outcome.
In conclusion, hyaluronic acid has been used in severalagents for adhesion prevention. This meta-analysis showsthat hyaluronic acid may have the potential to help decreaseadhesion formation. However, as a result of the limitednumber of studies available, this evidence should be inter-preted with caution. Ideally, severity of adhesions shouldnot be used as a surrogate marker for future fertility poten-tial, and therefore, future studies should include live birthrate as a primary outcome measure and have adequatefollow-up periods.
REFERENCES1. Nehez L, Vodros D, Axelsson J, Tingstedt B, Lindman B, Andersson R.
Prevention of postoperative peritoneal adhesions: effects of lysozyme,
polylysine and polyglutamate versus hyaluronic acid. Scand J Gastroen-
terol 2005;40:1118–23.
2. Diamond MP, Freeman L, eds. Incidence of postsurgical adhesions. New
York: Springer-Verlag, 2000.
3. Verco SJ, Peers EM, Brown CB, Rodgers KE, Roda N, diZerega G. De-
velopment of a novel glucose polymer solution (icodextrin) for adhesion
prevention: pre-clinical studies. Hum Reprod 2000;15:1764–72.
4. Lok F, Ledger WL, Li TC. Surgical intervention in infertility manage-
ment. Hum Fertil 2003;6.
1146 Metwally et al. Hyaluronic acid for adhesion prevent
5. Tulandi T, Collins JA, Burrows E, Jarrell JF, McInnes RA, Wrixon W, et al.
Treatment-dependent and treatment-independent pregnancy among
women with periadnexal adhesions. Am J Obstet Gynecol 1990;162:354–7.
6. diZerega G. Contemporary adhesion prevention. Fertil Steril
1994;61:219–35.
7. Metwally M, Watson A, Lilford R, Vandekerckhove P. Fluid and pharma-
cological agents for adhesion prevention after gynaecological surgery.
Cochrane Database Syst Rev 2006;3:CD001298.
8. Thornton MH, Johns DB, Campeau JD, Hoehler F, DiZerega GS. Clini-
cal evaluation of 0.5% ferric hyaluronate adhesion prevention gel for the
reduction of adhesions following peritoneal cavity surgery: open-label
pilot study. Hum Reprod 1998;13:1480–5.
9. Higgins JPT, Green S. Cochrane handbook for systematic reviews of in-
terventions 4.2.5. Chichester, United Kingdom: Wiley and Sons, 2005.
10. Johns BD, Keyport GM, Hoehler F, diZerega G. Reduction of postsurgi-
cal adhesions with Intergel adhesion prevention solution: a multicenter
study of safety and efficacy after conservative gynecologic surgery. Fertil
Steril 2001;76:595–604.
11. Lundorff P, Geldorp H, Tronstad SE, Lalos O, Larsson B, Johns DB, et al.
Reduction of postsurgical adhesions with ferric hyaluronate gel: a Euro-
pean study. Hum Reprod 2001;16:1982–8.
12. Pellicano M, Bramante S, Cirillo D, Palomba S, Bifulco G, Zullo F, et al.
Effectiveness of autocrosslinked hyaluronic acid gel after laparoscopic
myomectomy in infertile patients: a prospective, randomized, controlled
study. Fertil Steril 2003;80:441–4.
13. Diamond MP. Reduction of de novo postsurgical adhesions by intraoper-
ative precoating with Sepracoat (HAL-C) solution: a prospective, ran-
domized, blinded, placebo-controlled multicenter study. The Sepracoat
Adhesion Study Group. Fertil Steril 1998;69:1067–74.
14. Acunzo G, Guida M, Pellicano M, Tommaselli GA, Di Spiezio Sardo A,
Bifulco G, et al. Effectiveness of auto-cross-linked hyaluronic acid gel in
the prevention of intrauterine adhesions after hysteroscopic adhesiolysis:
a prospective, randomized, controlled study. Hum Reprod 2003;18:
1918–21.
15. Kramer K, Senninger N, Herbst H, Probst W. Effective prevention of
adhesions with hyaluronate. Arch Surg 2002;137:278–82.
ion Vol. 87, No. 5, May 2007

ACpthneut
iEufsu
RR
REPRODUCTIVE BIOLOGY
0d
Effect of atosiban on rabbit embryo development andhuman sperm motilityPiotr Pierzynski, M.D., Ph.D.,a Barbara Gajda, M.Sc., Ph.D.,b Zdzislaw Smorag, M.Sc., Ph.D.,b
Allan Dahl Rasmussen, Ph.D.,c and Waldemar Kuczynski, M.D., Ph.D.a
a Center for Reproductive Medicine KRIOBANK, Bialystok, Poland; b National Research Institute of Animal Production,Department of Animal Reproduction Biotechnology, Balice/Krakow, Poland; and c Ferring Pharmaceuticals A/S, InternationalPharmaScience Center, Department of Non-Clinical Development, Copenhagen, Denmark
Objective: To investigate embryotoxic potential and effects on human sperm motility of the mixed vasopressinV1a/oxytocin receptor antagonist atosiban considered for novel indication of improvement of uterine receptivityin embryo-transfer recipients.Design: One-cell rabbit embryo bioassay and human sperm motility bioassay were performed in control mediaor in media containing atosiban.Setting: Private center of reproductive medicine and academic research institute of reproduction biotechnology.Animal(s): Rabbit females (New Zealand and California, N � 15) aged 4.5–6.5 months.Intervention(s): In vitro exposure of one-cell rabbit embryos and human sperm to atosiban in the range oftherapeutic concentrations clinically occurring in human beings.Main Outcome Measure(s): Embryo development and sperm motility.Result(s): Preimplantation development of one-cell rabbit embryos was not affected by atosiban in the concen-trations �15,000 nM, which was 50-fold higher than the mean plasma concentration reached during regulartherapy (300 nM). Atosiban did not affect human sperm motility in concentrations of �3,000 nM, in other words,10 times the human mean plasma concentration.Conclusion(s): Clinical application of atosiban in the proposed indication may be safe for embryos because it iscompatible with preimplantation rabbit embryo development and human sperm motility. (Fertil Steril� 2007;87:1147–52. ©2007 by American Society for Reproductive Medicine.)
Key Words: Embryotoxicity, rabbit embryo bioassay, human sperm motility, atosiban, oxytocin antagonists,embryo transfer, IVF
Ehi
rpfa
o1wbpmf
p
tosiban (TRACTOCILE; Ferring Pharmaceuticals A/S,openhagen, Denmark) is a uterine-specific, mixed vaso-ressin V1a and oxytocin-receptor antagonist that is regis-ered for tocolysis in imminent premature birth (1). It alsoas been demonstrated to inhibit uterine contractility inonpregnant women (2). For the novel clinical application ofmbryo transfer (ET), atosiban is suggested to decreaseterine contractions and promote uterine receptivity in pa-ients undergoing ET (3).
Pregnancy rates after IVF-ET decrease in a stepwise fash-on with increasing frequency of uterine contractions (4). InT recipients, in addition to spontaneous contractions, theterus is also exposed to strong contractile stimuli arisingrom transcervical passage of the transfer catheter and, inome cases, from using a tenaculum (5, 6). Exaggeratedterine contractile activity may last as long as 1 hour after
eceived April 5, 2006; revised and accepted August 22, 2006.eprint requests: Piotr Pierzynski, M.D., Ph.D., Center for ReproductiveMedicine KRIOBANK, Stoleczna 11, 15-889 Bialystok, Poland (FAX:
o48857441378; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.08.089 Copyright ©2007 American Soc
T and cause expulsion of embryos from the uterus (6). Itas been shown that up to 50% of embryos could be foundn the uterine cavity after ET (7).
Application of oxytocin antagonists like atosiban or ba-usiban (8) during ET may decrease uterine contractions andrevent embryo expulsion. Prolonged application may alsoacilitate embryo implantation that takes place 48–72 hoursfter the ET (9, 10).
A good safety profile of atosiban already has been dem-nstrated in human studies preceding its registration (11,2), although these were conducted after the 24th gestationaleek (the time of completion of fetal organogenesis). Atosi-an showed no postimplantation fetal toxicity in studieserformed in rats and rabbits (13, 14). Also, maternal treat-ent with atosiban caused no fetotoxicity in a rat cross-
ostering study (15).
However, these studies did not cover the preimplantationhase of the embryonic development. Because the possibility
f contact between early embryos and maternal blood cannot1147Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

bbpqcEoss
MRTfb1a1BBaaiaccm
gi(ocneemm4i
tmMbsPtc
favb
bsS
HAfssbose(mftnt
wtaSLptsaaCnfw
svomvaw
(motAsvtyTc
e excluded during ET (16), clinical application of atosibanefore and during ET should be preceded with evaluation ofotential risks for patients and transferred embryos. To ac-uire embryotoxic data that could support such a novellinical application, an embryotoxicity study was performed.mbryotoxic potential of atosiban was assessed in rabbitne-cell embryos (see Rabbit Embryo Bioassay) and humanperm (see Human Sperm Motility Bioassay). This is the firsttudy on the early embryotoxicity of atosiban.
ATERIALS AND METHODSabbit Embryo Bioassayhe experiments were carried out after receiving consent
rom the local ethics committee in 262 one-cell rabbit em-ryos. Rabbit females (New Zealand and California, N �5) 4.5–6.5 months of age and weighing 3–4 kg were useds donors. Females were superovulated by IM injection of00 IU of postmenopausal gonadotropin (Serogonadotropin;iowet, Poland), followed by 100 IU of hCG (Biogonadyl,iomed, Poland), injected IV 72 hours later. Immediatelyfter hCG injection, donors were inseminated. The embryost the one-cell stage were collected at 18 to 20 hours afternsemination. The embryos were recovered at room temper-ture by flushing the Fallopian tubes with 10 mL of Dulbec-o’s solution (PBS, Sigma) supplemented with 20% fetalalf serum (Sigma). The recovered embryos were examinedorphologically under a stereomicroscope.
Morphologically normal embryos were divided into sixroups: one control and five experimental groups. Exper-mental embryos were cultured in vitro in B2 mediumINRA, Ménézo, bioMerieux, France) (17) with additionf atosiban (Ferring Pharmaceuticals A/S, Denmark) atoncentrations of 300 nM, 1,000 nM, 3,000 nM, 6,000M, and 15,000 nM (groups I–V, respectively). Controlmbryos (group VI) were cultured in B2 medium. Thembryos were washed in a B2 medium and cultured in 1.0L of the medium in four-well multidishes (Nunc, Den-ark) in a CO2 incubator (5% CO2 in air at 38°C) for 3 ordays. The cultured embryos were evaluated at 24-hour
ntervals (18).
The viability of embryos was determined by estimatinghe percentage of expanded or hatched blastocysts. Assess-ents were carried out under a stereomicroscope (Nikon).oreover, a sample of the embryos that developed to the
lastocyst stage were assessed for cell number. They weretained with 2 �g/mL of bisbenzimide (Hoechst 33342) inBS for 15 minutes and put on a glass slide with a drop of
he dye solution (19, 20). Counts were taken with a fluores-ence microscope (Nikon).
Analysis of repeated marginal probabilities was usedor the assessment of influence of atosiban concentrationnd exposure time on the development of embryos. Aariance analysis test was used for comparison of num-
ers of cells in blastocysts. Test assumptions were verified a1148 Pierzynski et al. Study on embryotoxicity of atosiban
y using the Kolmogorov-Smirnov and Bartlett tests. Alltatistical procedures were undertaken with the SASTAT 8 package.
uman Sperm Motility Bioassayssessments of human sperm motility were performed on
resh samples taken from 15 healthy donors with perfecteminal parameters. Initial evaluation of parameters ofperm motility and velocity showed no significant differenceetween consecutive donors. Swim-up ascending migrationn human sperm preparation medium (21) was applied toelect alive and motile spermatozoa. After such a selection,ach semen sample was divided into eight equal aliquotsabout 200 �L each, volume adjusted to maintain the sper-atozoa concentration at 10 million/�L) that were trans-
erred to sterile Eppendorf tubes. In addition to two controlubes, six tubes had atosiban added at concentrations of 300M, 1,000 nM, and 3,000 nM (two aliquots per concentra-ion).
Throughout the time of the experiment (24 hours), tubesere incubated in a 5% CO2 environment, with constant
emperature and humidity conditions. Sperm motility wasssessed in a computer-assisted sperm analyzer (Hobsonperm Tracker, Model 7V1B; Hobson Tracking Systemstd., Sheffield, United Kingdom) connected to a contrasthase microscope (Olympus BX-40; Olympus Corp, Japan)hat was equipped with a heating table. Computer-aidedperm assessments were performed at a �400 magnificationfter 1, 8, and 24 hours of exposure to atosiban. For eachssessment, 4 �L of each aliquot was added to a warmedell Vue Glass Semen Analysis Chamber (Fertility Tech-ologies Inc). The sperm remained in the calibrated frameor �3 seconds (minimum track time) before their tracksere accepted in the system.
Microscopy was performed at �400 magnification in aearch radius of 12.50 �m, at a framing rate of 25 Hz (PALideo). Computer-aided sperm assessment was performedver a fixed time interval of 120 seconds. All the assess-ents were performed by the same technician. The kappa
alue of intraobserver variability was equal to 0.8; accuracynd reproducibility of the Hobson Sperm Tracker Systemas 97%.
In total, 120 samples were assessed by 375 measurements3 measurements at 1, 8, and 24 h per sample � 15 controleasurements at zero timepoint). In the analysis, parameters
f sperm motility, that is, total percentages of motile, ac-ively motile, and hyperactivated spermatozoa (Motile%,ctive% and Hyper%, respectively) as well as parameters of
perm velocity, that is, curvilinear (total) and straight-lineelocity (VCL and VSL, respectively), were included. Sta-istical analysis involved two-factor repeated measures anal-sis of variance. When data did not satisfy the assumption ofype H covariance (test for sphericity) (22), the P value wasalculated for the adjusted test (23). P values of �.05 were
ccepted as statistically significant.Vol. 87, No. 5, May 2007

RRDamhaemtcbtecT
onbn6im�6n
HIfwgcta
ctcoaa
obtisa(dMbF
DTaainhsermboIao
F
ESULTSabbit Embryo Bioassayevelopment of embryos after 24 hours of culture was not
nalyzed statistically because all cells developed nor-ally. In the analysis of embryo viability after 48 and 72
ours of exposure to atosiban, it was shown that percent-ge of developing embryos was unaffected by atosibanxposure (influence of concentration on embryo develop-ent, P�.77). In addition, there was no interaction be-
ween time and concentration of atosiban (no influence ofoncentration on atosiban/time interaction, P�.49). Via-ility of rabbit embryos was significantly affected by theime length of the culture (significant influence of time onmbryo development, P�.0011), which is a natural out-ome of culture in vitro. Detailed results are presented inable 1.
In the analysis of the influence of atosiban on the numberf blastomeres in blastocysts, reflecting their development,o significant differences between controls and exposed em-ryos were found (analysis of variance, P�.79). The meanumber of blastomeres in the control group (n � 8) reached8.5 � 14.48 (mean � SD), and in consecutive groups ofncreasing atosiban concentrations, it reached respectiveean (� SD) values of 70.14 � 13.48 (300 nM; n � 7), 74.416.1 (1,000 nM; n � 5), 71.6 � 8.385 (3,000 nM; n � 7),
6 � 11.89 (6,000 nM; n � 7), and 65 � 6.86 (15,000 nM;� 7).
uman Sperm Motility Bioassayn the human sperm motility bioassay assessments, no ef-ects of atosiban on human sperm motility were detectedhen compared to controls. Generally, there was a notableradual decrease of activity and velocity of spermatozoaonnected to the duration of the experiment. These parame-ers did not differ between the control and groups exposed to
TABLE 1One-cell rabbit embryo bioassay: percentages ofexposure to atosiban.
Atosiban (nM)No of cultured
embryos/replications 24 h
Control 46/4300a 43/31,000b 43/33,000 43/36,000 43/315,000 44/3a Corresponding to the mean human plasma concentratiob Corresponding to the maximum human plasma concent
Pierzynski. Atosiban lacks embryotoxic potential. Fertil Steril 2007.
tosiban. No significant interactions between time and con- e
ertility and Sterility�
entration were found for all analyzed values, so the effect ofime did not differ significantly in the four groups of con-entrations (0, 300, 1,000, and 3,000). The effect of atosibann sperm motility and velocity was not significant for allnalyzed parameters, with P values reaching .58, .06, .94,nd .45 for Motile%, Active%, VCL, and VSL, respectively.
The statistically significant (P�.0038) effect of atosibann hyperactivity of the spermatozoa is considered incidentalecause no clear dose relationships were present at any of theime points (1, 8, and 24 hours). Duration of culture speciallynfluenced parameters of sperm velocity. Time effect wastatistically significant for both VCL and VSL (P�.0001); inddition, for VSL values, there was a significant linear trendP�.0001). For values describing sperm motility, analysisid not reveal statistical significance (P�.32 and P�.11 forotile% and Active%). Data for the human sperm motility
ioassay study are presented in Table 2 and are visualized inigures 1 and 2.
ISCUSSIONhis report is the first assessment of early embryotoxicity oftosiban, a mixed vasopressin V1a and oxytocin receptorntagonist that is considered for the novel indication ofmproving the uterine receptivity in ET recipients. Tech-iques used in the study, the rabbit embryo bioassay and theuman sperm motility bioassay, are considered reliable andensitive in terms of the determination of the influence ofxtrinsic factors on human embryos (24). Because it iseliable and inexpensive, human sperm motility bioassayay be applied in practices of reproductive medicine of even
asic laboratory infrastructure. It may be used for assessmentf methods of culture or new laboratory equipment (25, 26).n addition, it has been shown to be of equivalent value tonimal embryo tests (24). In planning the clinical applicationf atosiban, we decided to perform additional tests on rabbit
veloping embryos after 24, 48, and 72 hours of
n (%) that developed embryos after
16 cells) 48 h (morula) 72 h (blastocyst)
100) 45 (97.8) 43 (94.5)100) 41 (95.3) 40 (93.0)100) 43 (100) 43 (100)100) 42 (97.7) 39 (90.7)100) 43 (100) 38 (88.4)100) 42 (95.4) 38 (86.4)
n.
de
(8–
46 (43 (43 (43 (43 (44 (n.ratio
mbryos, which could provide complimentary data. Single-
1149

TABLE 2Human sperm motility bioassay: effect of atosiban on parameters of sperm motility and velocity.
Atosiban level (nM)
Time (h) by spermparameters 0 (control) 300 1,000 3,000 P values
MotilityMotility%
1 93 � 8.8 93 � 7.6 94.9 � 7.9 92.1 � 11.4 .32a
8 91 � 6.4 90 � 10.0 87.1 � 14.4 92.2 � 7.4 .58b
24 97.3 � 7.1 95.6 � 6.7 92.4 � 8.9 94.3 � 7.1 .73c
Active%1 66.7 � 13.0 60.9 � 14.7 61.3 � 12.5 66.3 � 11.9 .11a
8 69.0 � 5.9 71.4 � 12.0 61.1 � 12.3 62.8 � 10.2 .06b
24 56.9 � 14.2 56.4 � 16.3 53.8 � 18.7 56.7 � 16.6 .52c
Hyper%1 19.7 � 6.6 22.0 � 11.4 18.6 � 10.8 22.4 � 11.1 .0001ad
8 30.2 � 9.4 24.8 � 8.8 20.0 � 8.6 21.9 � 6.0 .0038bd
24 21.6 � 14.3 19.4 � 15.5 15.4 � 10.9 19.0 � 16.6 .23c
Sperm velocity(�m/s)
VCL1 142.4 � 15.6 143.0 � 18.8 143.0 � 15.8 143.4 � 13.0 .0001ad
8 148.0 � 13.6 147.7 � 10.7 146.7 � 15.8 143.2 � 14.1 .94b
24 123.1 � 22.0 116.2 � 17.7 116.8 � 18.2 120.1 � 20.6 .62c
VSL1 103.3 � 13.1 103.7 � 15.1 105.1 � 15.0 104.1 � 13.0 .0001ad
8 101.8 � 12.5 103.8 � 10.1 106.8 � 19.2 103.1 � 15.2 .45b
24 79.6 � 16.2 77.0 � 13.1 78.5 � 18.2 81.0 � 16.2 .67c
a For testing the hypothesis of no time effect.b For testing the hypothesis of no concentration effect.c For testing the hypothesis of no interaction between time and concentration effect.d Statistically significant at P�.05.
Pierzynski. Atosiban lacks embryotoxic potential. Fertil Steril 2007.
FIGURE 1
Human sperm motility bioassay: analysis of parameters of sperm motility after 1, 8, and 24 hours ofexposure to atosiban. Motility% � percentage of motile spermatozoa; Active% � percentage of activelymotile spermatozoa; Hyper% � percentage of hyperactively motile spermatozoa.
Pierzynski. Atosiban lacks embryotoxic potential. Fertil Steril 2007.
1150 Pierzynski et al. Study on embryotoxicity of atosiban Vol. 87, No. 5, May 2007

cw
dhabtbod
hpanbta1r
tr(ta(toihpp
p
rnwaw1
otcnIg
AKvah
R
1
1
1
1
1
F
ell rabbit embryos, because they are closer to human (27),ere chosen for a model.
The effect of atosiban on viability of rabbit embryos wasetermined by assessment of percentage of expanded oratched blastocysts 48 hours after the start of exposure. Inddition, we applied assessment of numbers of cells inlastocysts as an independent measure, providing verifica-ion of results. Concentrations of atosiban applied rangedetween 10- and 50-fold of the mean plasma concentrationsf pregnant women. No embryotoxic effect of atosiban wasetected by using both techniques.
Atosiban was also shown to have no adverse effect onuman sperm in the measured range of concentrations. Inregnant women treated for imminent premature birth, meannd maximal plasma concentrations of atosiban reach 300M and 1,000 nM, respectively (28). In the human spermioassay study, we assessed the effect of atosiban concen-rations of 300 nM, 1,000 nM, and 3,000 nM, that is, 1-, 3.3-,nd 10-fold the human mean plasma concentration or 0.3-,-, and 3-fold the maximum human plasma concentration,espectively.
The receptor profile of atosiban indicates a higher affinityoward vasopressin V1a receptors as compared with oxytocineceptors, reflecting their density in the nonpregnant uterus29). Atosiban may effectively decrease the contractile ac-ivity of the nonpregnant uterus, and in addition, oxytocinntagonism has been shown to decrease PGF2a formation30) and increase uterine perfusion (31). Such a multidirec-ional mode of action may be of benefit in comparison tother tocolytic agents such as piroxicam (cyclooxygenasenhibitor) or ritodrine (beta-2 adrenoreceptor agonist). Bothave been tested in ET recipients, showing some benefit forregnancy rates, but have not been introduced into clinicalractice, probably as a result of safety concerns (32, 33).
Results of this embryotoxicity study encouraged us to
FIGURE 2
Human sperm motility bioassay: analysis ofparameters of sperm velocity after 1, 8, and 24hours of exposure to atosiban. Both VCL and VSLare in �m/s.
Pierzynski. Atosiban lacks embryotoxic potential. Fertil Steril 2007.
roceed with a clinical application of atosiban in an ET
ertility and Sterility�
ecipient: a 42-year-old woman with a history of sevenegative IVF-ET attempts. In this experimental treatment,e demonstrated a significant reduction in uterine contractile
ctivity associated with a clinical success: a normal twin,ith diamniotic pregnancy confirmed sonographically at the2th gestational week (3).
In conclusion, atosiban has been demonstrated to be freef embryotoxic effects in vitro in the range of concentrationshat are reached during clinical administration and also atoncentrations of �50-fold of achieved human values. Theovel application of oxytocin antagonists in the treatment ofVF patients and ET recipients should be further investi-ated.
cknowledgment: The authors would like to acknowledge Malgorzataretowska, Ph.D., from the Institute of Computer Science, Technical Uni-ersity of Bialystok (Bialystok, Poland), for performing statistic analysis,nd Peter A. McAnulty, Ph.D., from Ferring Pharmaceuticals A/S (Copen-agen, Denmark), for critically reviewing the manuscript.
EFERENCES1. European Medicines Agency (EMEA). European public assessment report:
Tractocile. European Medicines Agency, 2005. Available at: http://www.emea.eu.int/humandocs/PDFs/EPAR/Tractocile/025399en6.pdf.
2. Akerlund M. Involvement of oxytocin and vasopressin in the patho-physiology of preterm labor and primary dysmenorrhea. Prog Brain Res2002;139:359–65.
3. Pierzynski P, Reinheimer T, Kuczynski W. Oxytocin antagonists mayimprove infertility treatment. Fertil Steril. In press.
4. Fanchin R, Righini C, Olivennes F, Taylor S, de Ziegler D, Frydman R.Uterine contractions at the time of embryo transfer alter pregnancy ratesafter in-vitro fertilization. Hum Reprod 1998;13:1968–74.
5. Lesny P, Killick S, Robinson J, Raven G, Maguiness S. Junctional zonecontractions and embryo transfer: is it safe to use tenanculum? HumReprod 1999;14:2367–70.
6. Lesny P, Killick S, Tetlow R, Robinson J, Maguiness S. Embryotransfer—can we learn anything new from the observation of junctionalzone contractions? Hum Reprod 1998;13:1540–6.
7. Menezo L, Anker D, Salat-Baroux J. Conception and realization ofartificial dried embryo for training in in vitro fertilization and embryotransfer (IVF and ET). Acta Eur Fertil 1985;16:55–8.
8. Pierzynski P, Lemancewicz A, Reinheimer T, Akerlund M, LaudanskiT. Inhibitory effect of barusiban and atosiban on oxytocin-inducedcontractions of myometrium from preterm and term pregnant women. JSoc Gynecol Investig 2004;11:339–41.
9. Bergh PA, Navot D. The impact of embryonic development and endo-metrial maturity on the timing of implantation. Fertil Steril 1992;58:537–42.
0. Damario MA, Lesnick TG, Lessey BA, Kowalik A, Mandelin E,Seppala M, et al. Endometrial markers of uterine receptivity utilizingthe donor oocyte model. Hum Reprod 2001;16:1893–9.
1. Coomarasamy A, Knox E, Gee H, Khan K. Oxytocin antagonists fortocolysis in preterm labour—a systematic review. Med Sci Monit2002;8:268–73.
2. The Worldwide Atosiban versus Beta-agonist Study Group. Effective-ness and safety of the oxytocin antagonist atosiban versus beta-adren-ergic agonists in the treatment of preterm labour. Br J Obstet Gynaecol2001;108:133–42.
3. Zellers JE, Davis CC, Oldham JW, Mackey MJ, Szot RJ. Subcutaneousdevelopmental toxicity study of RWJ-22164-021 (atosiban) in femaleCrl:CD B.R., VAF/Plus rats. Raritan (NJ): RW Johnson PharmaceuticalResearch Institute; 1996. Internal Report No. 382520:1-DS-94307.
4. Zellers JE, Krayer JH, Takacs AR, Mackey MJ, Oldham JW. Subcu-
taneous developmental toxicity study of RWJ-22164-021 (atosiban) in1151

1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
female New Zealand White rabbits. Raritan (NJ): RW JohnsonPharmaceutical Research Institute; 1996. Internal Report No.404286:1-DS-94314.
5. McAnulty PA, Burns LM. Evaluation of the maternal and neonataleffects of the oxytocin antagonist, atosiban, in a cross-fostering study inrats. Reprod Toxicol 2004;19:65–70.
6. Lessey BA. Endometrial receptivity and the window of implantation.Baillieres Best Pract Res Clin Obstet Gynaecol 2000;14:775–88.
7. Menezo Y. Synthetic medium for gamete survival and maturation andfor culture of fertilized eggs. C R Acad Sci Hebd Seances Acad Sci D1976;282:1967–70.
8. Smorag Z, Gajda B. Vitrification of non-cultured and cultured rabbitembryos. Anim Reprod Sci 1991;26:151–8.
9. Gajda B, Smorag Z. Cells number in pig blastocyst cultured in differentmedia. Ann Anim Sci 2004;4:315–20.
0. Pursel V, Wall R, Rexroad C, Hammer R, Brinster R. A rapid whole-mount staining procedure for nuclei of mammalian embryos. Theriog-enology 1985;24:687–91.
1. Henkel RR, Schill WB. Sperm preparation for ART. Reprod BiolEndocrinol 2003;1:108.
2. Anderson T. An introduction to multivariate statistical analysis. NewYork: John Wiley and Sons, Inc, 1958.
3. Huynh H, Feldt L. Estimation of the box correction for degrees offreedom from sample data in the randomized clock and split plotdesigns. J Educ Stat 1976;1:69–82.
4. Miller J, Morgan K, McAlister A, Johnson T, Rong N, Freeman M. Acomparison between the human sperm bioassay and the mouse embryobioassay. Fertil Steril 2001;76:S104.
5. Claassens O, Wehr J, Harrison K. Optimizing sensitivity of the humansperm motility assay for embryo toxicity testing. Hum Reprod 2000;
15:1586–91.1152 Pierzynski et al. Study on embryotoxicity of atosiban
6. Scott L, Smith S. Mouse in vitro fertilization, embryo development andviability, and human sperm motility in substances used for human spermpreparation for assisted reproduction. Fertil Steril 1997;67:377–81.
7. Al-Hasani S, Hepnar C, Diedrich K, van der Ven H, Krebs D. Cryo-preservation of rabbit zygotes. Hum Reprod 1992;7:81–3.
8. Goodwin TM, Millar L, North L, Abrams LS, Weglein RC, HollandML. The pharmacokinetics of the oxytocin antagonist atosiban inpregnant women with preterm uterine contractions. Am J Obstet Gy-necol 1995;173:913–7.
9. Akerlund M, Bossmar T, Brouard R, Kostrzewska A, Laudanski T, Le-mancewicz A, et al. Receptor binding of oxytocin and vasopressin antag-onists and inhibitory effects on isolated myometrium from preterm andterm pregnant women. Br J Obstet Gynaecol 1999;106:1047–53.
0. Serradeil-Le Gal C, Valette G, Foulon L, Germain G, Advenier C,Naline E, et al. SSR126768A (4-chloro-3-[(3R)-(�)-5-chloro-1-(2,4-dimethoxybenzyl)-3-methyl-2-oxo-2,3-dihydro-1H-indol-3-yl]-N-ethyl-N-(3-pyridylmethyl)-benzamide, hydrochloride): a new selective andorally active oxytocin receptor antagonist for the prevention of pretermlabor. J Pharmacol Exp Ther 2004;309:414–24.
1. Vedernikov Y, Betancourt A, Shi S, Shi L, Reinheimer T, Garfield R.Oxytocin antagonistic effect of barusiban and atosiban in isolateduterine artery from late pregnant rats. Presented at the SGI AnnualMeeting, Toronto, Canada; 2006.
2. Moon H, Park S, Lee J, Kim K, Joo B. Treatment with piroxicam beforeembryo transfer increases the pregnancy rate after in vitro fertilizationand embryo transfer. Fertil Steril 2004;82:816–20.
3. Tsirigotis M, Pelekanos M, Gilhespie S, Gregorakis S, Pistofidis G.Ritodrine use during the peri-implantation period reduces uterinecontractility and improves implantation and pregnancy rates post-implantation. Presented at the 16th Annual Meeting of the EuropeanSociety of Human Reproduction and Embryology, Bologna, ltaly;
2000:O-024.Vol. 87, No. 5, May 2007

Sotaaft
S
B
R
R
0d
Apoptosis and ultrastructural assessment aftercryopreservation of whole human ovaries with theirvascular pedicleBelen Martinez-Madrid, V.M.D., Ph.D.,a Alessandra Camboni, M.D.,a,b
Marie-Madeleine Dolmans, M.D., Ph.D.,a Stefania Nottola, M.D., Ph.D.,b
Anne Van Langendonckt, Ph.D.,a and Jacques Donnez, M.D., Ph.D.a
a Department of Gynecology, Cliniques Universitaires Saint Luc, Université Catholique de Louvain, Brussels, Belgium; andb Department of Anatomy, University of Rome “La Sapienza,” Rome, Italy
Objective: To investigate possible damage caused by freeze-thawing whole human ovaries.Design: Prospective experimental study.Setting: Academic gynecology research unit in a university hospital.Patient(s): Ovaries were obtained from three women (aged 29–36 years).Intervention(s): Ovaries were perfused and bathed in cryoprotective solution, and slow freezing was performed.Rapid thawing was achieved by perfusion and bathing with a decreased sucrose gradient.Main Outcome Measure(s): Apoptosis was assessed by the terminal deoxynucleotidyl transferase-mediatedbiotinylated deoxyuridine triphosphates nick end-labeling (TUNEL) method and by immunohistochemistry foractive caspase-3 in fresh ovaries, after cryoprotectant exposure, and after thawing. Morphometric analysis ofTUNEL-positive surface area was performed. Ultrastructure was assessed by transmission electron microscopy(TEM) in the thawed tissue.Result(s): No primordial or primary follicles were found to be positive for either TUNEL or active caspase-3. Nostatistically significant difference in mean TUNEL-positive surface area values was found between the threegroups: fresh, 0.05% � 0.03%, with 134 high-power fields (HPFs); cryoperfused, 0.02% � 0.01%, with 130HPFs; and thawed, 0.09% � 0.03%, with 622 HPFs. By means of TEM, follicles and vessels showed awell-preserved ultrastructure, with 96.7% (29/30) healthy-looking primordial and primary follicles, and 96.3%(180/187) healthy-looking endothelial cells.Conclusion(s): Cryopreservation of intact human ovary with its vascular pedicle, according to the freeze-thawingprotocol described here, is not associated with any signs of apoptosis or ultrastructural alterations in any celltypes. Whole-organ vascular transplantation may thus be a viable option in the future. (Fertil Steril� 2007;87:1153–65. ©2007 by American Society for Reproductive Medicine.)
Key Words: Cryopreservation, human, whole ovary, apoptosis, TUNEL, caspase-3, TEM
stc2foh
epdoacvand
urvival rates of cancer patients are on the increase becausef constant improvements in the diagnosis and treatment ofhe disease. However, patients requiring chemotherapynd/or radiotherapy for cancer or other benign pathologiesre likely to experience premature ovarian failure and loss ofertility as a consequence of these potentially gonadotoxicreatments. Several options are currently available to pre-
upported by the Fonds National de Recherche Scientifique (grant3.4.599.02.F); Televie (grant 7.4519.04); the Fondation St. Luc, theBelgian Federation Against Cancer; Baron Albert Frère; the Comte deSpoelberch; the Italian Ministry of Education, Universities, and Re-search (grant C26A049412); and the Italian Ministry of Foreign Affairs(VII Executive Program of Scientific Collaboration between Italy and theFrench-Speaking Community of Belgium 2005–2006).
elen Martinez-Madrid, V.M.D., Ph.D., and Alessandra Camboni, M.D.,contributed equally to this article.
eceived February 28, 2006; revised August 23, 2006; accepted Novem-ber 1, 2006.
eprint requests: Jacques Donnez, M.D., Ph.D., Department of Gynecol-ogy, Cliniques Universitaires Saint Luc, Université Catholique de Lou-vain, Avenue Hippocrate 10, 1200 Brussels, Belgium (FAX: 32-2-764-
C95-07; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.11.019 Copyright ©2007 American Soc
erve fertility in these patients, giving them the opportunityo become mothers when they have overcome their disease:ryopreservation of embryos, oocytes, or ovarian tissue (1,). The choice of the most suitable strategy for preservingertility depends on different parameters: the type and timingf chemotherapy, the type of cancer, the patient’s age, ander partner status.
The only established method of fertility preservation ismbryo cryopreservation (3), but this option requires theatient to be of pubertal age and to have a partner or useonor sperm, and to be in a position to undergo a cycle ofvarian stimulation, which is not possible when chemother-py must be started immediately or when stimulation isontraindicated according to the type of cancer. Cryopreser-ation of oocytes can be performed in single women who areble to undergo a stimulation cycle, although the effective-ess of this technique is very low, with pregnancy andelivery rates ranging from 1%–5% per frozen oocyte (4).
ryopreservation of ovarian tissue is the only option for1153Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

pc
wiohfabTciat
attcoef((f(r
sticvmlTtddt
tosotothpac
MCTILttrfafc
hoc(mhmwswVa�t
TFLibrtma
AApimfiawsfnDf
repubertal girls and women who cannot delay the start ofhemotherapy.
Ovarian tissue can be frozen and grafted in three differentays: as fragments of ovarian cortex, as an entire ovary with
ts vascular pedicle, or as isolated follicles (5). So far,varian cryopreservation and transplantation proceduresave been almost exclusively limited to avascular corticalragments in both experimental and clinical studies (6–8)nd, for now, this is the only procedure that has yielded liveirths in humans after autologous transplantation (9, 10).he main drawback of this method is that the graft isompletely dependent on the establishment of neovascular-zation and, as a result, a significant proportion of folliclesre lost due to ischemic damage by the time neovasculariza-ion is achieved (6, 11–15).
Reducing the ischemic interval between transplantationnd revascularization is therefore essential to maintaininghe follicular reserve and extending the life span and func-ion of the graft. Transplantation of intact ovaries with vas-ular anastomosis would allow immediate revascularizationf the transplant, and would avoid problems related to isch-mic injury. Ovarian vascular transplantation was success-ully performed with the use of intact fresh ovaries in rats16, 17), rabbits (18), sheep (19, 20), dogs (21), monkeys22), and humans (23–25). In the last few years, attempts atreezing and grafting whole ovaries in rats (16, 17), rabbits26), sheep (27–30), and pigs (31) also yielded encouragingesults.
It appears that, in large mammals and humans, anastomo-is of the ovarian pedicle is technically feasible. However, inhese species, cryopreserving such a large-sized intact ovarys problematic due to the difficulty of adequate diffusion ofryoprotective agents into large tissue masses and the risk ofascular injury caused by intravascular ice formation. Theain challenge of ovarian vascular transplantation therefore
ies in successfully cryopreserving whole human ovaries.his procedure needs to avoid cryoinjury due to the freeze-
hawing procedure itself, as well as ischemic and toxic injuryuring cryoprotectant perfusion, while allowing adequateiffusion of cryoprotective agents into the deepest parts ofhe ovary.
We previously described a cryopreservation protocol forhe intact human ovary with its vascular pedicle, and dem-nstrated high survival rates of follicles (75.1%), small ves-els, and stroma, and a normal histological structure in allvarian components after thawing (32). Despite these posi-ive results, it is essential to conduct a thorough examinationf the effects of this protocol on ovarian tissue before at-empting vascular autotransplantation of whole ovaries inumans. The aim of the present study is to further investigateossible injury caused by this freeze-thawing protocol, bynalyzing apoptosis and ultrastructural damage to all ovarian
ell types. d1154 Martinez-Madrid et al. Freezing whole human ovaries
ATERIALS AND METHODSryopreservation of the Intact Ovaryhe use of human tissue for this study was approved by the
nstitutional Review Board of the Université Catholique deouvain, Brussels, Belgium. Ovaries were obtained from
hree women (29, 31, and 36 years of age) after oophorec-omy during a Wertheim-Meigs procedure prior to pelvicadiotherapy. All three ovaries showed normal macroscopiceatures at the time of oophorectomy, i.e., size, vasculature,nd surface appearance, with the presence of some antralollicles and corpora lutea on the cortex. The ovaries wereryopreserved as previously described (32).
Briefly, the ovary was perfused via the ovarian artery witheparinized physiologic solution and transported to the lab-ratory, where it was perfused and immersed in a bathontaining a cryoprotective solution of Leibovitz-15 mediumGIBCO, Paisley, Scotland), supplemented with 10% di-ethyl sulfoxide (DMSO) (Sigma, St. Louis, MO) and 0.4%
uman serum albumin (Red Cross, Brussels, Belgium) for 5inutes at 4°C. The ovary was placed in a cryovial where itas preequilibrated at 4°C in a bath with the cryoprotective
olution for 10 minutes. The cryovial containing the ovaryas placed in a 5100 Cryo 1°C Freezing Container (Nalgene,WR, Leuven, Belgium) precooled at 4°C, and deposited in�80°C freezer. This confers a theoretical cooling rate of1°C/minute. After 24 hours at �80°C, the cryovial con-
aining the ovary was transferred to liquid nitrogen (LN2).
hawing of the Intact Ovaryor thawing, the cryovial was directly transferred from theN2 to a water bath at 60°C, where it was immersed until the
ce melted. To remove the cryoprotectant, the ovary wasathed and perfused in three steps, for 10 minutes each atoom temperature (RT), with a reversed sucrose concentra-ion gradient (0.25 M, 0.1 M, and 0 M sucrose) in L-15edium, to avoid osmotic injuries. Perfusion was performed
t the same flow rate as already described.
ssessment of Apoptosist three different times (with freshly removed ovary, afterreequilibration with cryoprotective solution before freez-ng, and after thawing), samples were taken for assess-ent of apoptosis. Cortical and medullar tissues werexed in 4% formalin in phosphate-buffered saline (PBS),nd embedded in paraffin. Five-micron-thick sectionsere cut from the blocks and air-dried on slides. Apopto-
is was analyzed by a terminal deoxynucleotidyl trans-erase-mediated biotinylated deoxyuridine triphosphatesick end-labeling (TUNEL) technology method to detectNA fragmentation, and by immunohistochemistry (IHC)
or active caspase-3 to detect cells programmed to un-
ergo apoptosis.Vol. 87, No. 5, May 2007

ASwrwn1htCRwmtrcPD5(ites(flbappgsp
aVrtnbnp
wtpscatwtiat
bs
ITabeiantemeBndcfchabkpLKmSwdea
UAmwrtidpdtwemwngbt
F
nalysis of DNA Strand Breaks by TUNELections were dewaxed with histosafe (NV Yvsolab, Ant-erp, Belgium), rehydrated with isopropanol, and washed in
unning deionized water. The slides were then pretreatedith 20 �g/mL of proteinase K working solution (catalogueo. 745723; Roche Applied Science, Penzberg, Germany) in0 mM Tris-HCl, pH 7.5, for 30 minutes at 37°C in aumidified chamber. Strand breaks of DNA occurring duringhe apoptotic process were detected by means of the In Situell Death Detection Kit, TMR Red (catalogue no. 2156792;oche Applied Science), a TUNEL assay. After washingith PBS, slides were incubated with a TUNEL reactionixture: 50 �L enzyme solution (terminal deoxynucleotidyl
ransferase) and 450 �L label solution (nucleotide mixture ineaction buffer) for 60 minutes at 37°C in a humidifiedhamber protected from light, followed by rinsing with PBS.ositive control sections were treated with 1,500 U/mLNase I (catalogue no. 104132; Roche Applied Science) in0 mM Tris-HCl, pH 7.5, 1 mg/mL bovine serum albuminBSA), for 10 minutes at RT in a humidified chamber, beforencubation with the TUNEL reaction mixture. Negative con-rol sections were incubated with label solution withoutnzyme solution. Finally, slides were covered with Vecta-hield Mounting Medium with 4=,6-diamino-2-phenylindoleDAPI) (Vector Laboratories, Burlingame, CA). This specialormulation is intended to preserve fluorescence during pro-onged storage and, at the same time, to counterstain DNAy means of DAPI. Slides were coverslipped and sealedround the perimeter with nail polish, stored at 4°C, androtected from light until examination. Seven replicates wereerformed, each including one slide from the three differentroups (freshly removed ovary, after cryoprotectant expo-ure, and after thawing) from all three patients, as well asositive and negative controls.
TUNEL-stained and DAPI-counterstained slides were ex-mined under an inverted fluorescence microscope (Leica;an Hopplynus Instruments, Brussels, Belgium). Red fluo-
escence could be visualized in TUNEL-positive cells withhe use of an excitation wavelength in the range of 520–560m, and by observing the emitted light at a wavelengthetween 570–620 nm. DAPI reached excitation at about 360m, and emitted at about 460 nm when bound to DNA,roducing a blue fluorescence in all nuclei.
Morphometric analysis of TUNEL-positive surface areaas performed to quantify apoptosis. For this purpose, sec-
ions were examined at �200 magnification, and all high-ower fields (HPFs) were digitalized, either for TUNELtaining or DAPI counterstaining, using a Leica DFC320amera and IM50 program (Leica). ImageJ, a freely avail-ble image-processing and analysis program developed athe National Institutes of Health (http://rsb.info.nih.gov/ij/),as used to delimit all TUNEL-positive cells and to measure
heir surface area, as well as to determine total surface arean each section (by measuring DAPI-counterstained surfacerea). Antral follicles and corpora lutea were excluded from
he morphometric analysis of TUNEL-positive surface areas sertility and Sterility�
ecause the physiological occurrence of apoptosis in thesetructures, as well as their large size, could distort the results.
mmunohistochemical Detection of Active Caspase-3he active caspase-3 technique is an immunohistochemicalssay for the detection of the enzyme caspase-3, which cane activated during the apoptotic process and which, in turn,ventually activates endonucleases that cause the character-stic morphology of apoptotic cells. After deparaffinationnd rehydratation of slides as already described, an immu-operoxidase method was performed. Briefly, slides werereated with 0.3% H2O2 for 30 minutes at RT to inactivatendogenous peroxidase activity, heated in a solution of 10M sodium citrate at 95°C for 75 minutes to retrieve
pitopes, and incubated with 10% normal goat serum and 1%SA in Tris-buffered solution for 30 minutes at RT to blockonspecific staining. The slides were incubated in a 1:100ilution of the primary antibody, an anti-human rabbit poly-lonal antibody directed against a peptide from the p18ragment of human caspase-3 (Anti-Active® Caspase-3 pAb,atalogue no. G7481; Promega Corp., Madison, WI) for 16ours at RT. They were then incubated with a secondaryntibody conjugated to peroxidase, EnVision�® System La-elled Polymer-HRP Anti-Rabbit (catalogue no. K4003; Da-oCytomation, Carpenteria, CA), for 2 hours at RT. Theresence of peroxidase was revealed by incubating withiquid DAB� Substrate Chromogen System (catalogue no.3468; DakoCytomation) for 15 minutes at RT. Humanenstrual endometrium was used as a positive control.lides were counterstained with hematoxylin. Four replicatesere performed, each including one slide from the threeifferent groups (freshly removed ovary, after cryoprotectantxposure, and after thawing) from all three patients, as wells positive and negative controls.
ltrastructural Assessmentfter thawing whole ovaries, samples of the cortex andedulla were taken for ultrastructural evaluation. The tissueas fixed in 2.5% glutaraldehyde for 2–5 days at 4°C. After
insing in PBS, samples were postfixed with 1% osmiumetroxide (Agar Scientific, Stansted, Essex, United Kingdom)n PBS, and rinsed again in PBS. The samples were thenehydrated through ascending series of ethanol, immersed inropylene oxide overnight for solvent substitution, embed-ed in Epon 812, and sectioned with a Reichert-Jung Ul-racut E ultramicrotome. Semithin sections (1–7 �m thick)ere stained with toluidine blue (Sigma, St. Louis, MO),
xamined by light microscopy (LM) with a Zeiss Axioskopicroscope (Zeiss, Munich, Germany), and photographedith a Leica camera (DFC230). Ultrathin sections (60–80m) were cut with a diamond knife, mounted on copperrids, and contrasted with saturated uranyl acetate followedy lead citrate. They were examined and photographed withhe use of Zeiss EM109 and Zeiss EM 10 electron micro-
copes at 80 kV. Criteria established by Motta et al. (33)1155

wtsoc
amtao
STsosu
RAADgfitsa
AFfaT(s
so1inw
wWeTo0t
�n
IEcpaapc
tiao�cfosp
gTaseftffotrtr
UOtt
FTptlflpem
ere used to define the developmental stage of small prean-ral follicles: primordial (diplotene oocyte, surrounded by aingle layer of flattened follicular cells) or primary (growingocyte, surrounded by a single layer of cuboid follicularells).
The following elements were evaluated for qualitativessessment of ultrastructural preservation: nuclear content,embrane integrity, density of the cytoplasm and intrami-
ochondrial matrix, cytoplasmic organelles (quality, type,nd microtopography), and intercellular contacts (betweenocytes and follicular cells, and between endothelial cells).
tatistical Analysishe significance of differences observed in TUNEL-positiveurface area between groups was tested by one-way analysisf variance. Probability values of at least P�.05 were con-idered statistically significant. Analyses were carried outsing SPSS 11.5 (SPSS Inc., Chicago, IL).
ESULTSssessment of Apoptosispoptosis was assessed in freshly removed ovaries, afterMSO exposure before freezing, and after thawing. In eachroup, apoptosis was quantified in primordial and primaryollicles and evaluated in the rest of the ovarian components,.e., antral follicles, corpora lutea, stromal cells, and cellypes composing vessels (endothelial cells, pericytes, andmooth muscle cells). The percentage of apoptotic surfacerea was also analyzed by morphometry.
nalysis of DNA Strand Breaks by TUNELifty-six primordial and primary follicles were analyzed inresh ovarian tissue, 131 after DMSO exposure, and 199fter thawing (Fig. 1A). All were negative for TUNEL. TheUNEL-positive cells were mainly found in antral follicles
Fig. 1B) and corpora lutea. Occasionally, a few isolatedtromal cells stained positive for TUNEL.
In all three groups, endothelial cells, pericytes, andmooth muscle cells of medullar and cortical blood vesselsf different types (from capillaries to arteries and veins; Fig.C,D) were found to be negative for TUNEL. Only a fewsolated endothelial cells were TUNEL-positive. None of theegative controls showed any TUNEL-positive signals,hile TUNEL staining was observed in all positive controls.
Morphometric analysis of TUNEL-positive surface areaas carried out, excluding antral follicles and corpora lutea.e analyzed 134 HPFs in fresh ovary, 130 after DMSO
xposure, and 622 after thawing. The mean values ofUNEL-positive surface area were 0.05% � 0.03% in freshvary, 0.02% � 0.01% after DMSO exposure, and.09% � 0.03% after thawing (Table 1). The results revealed
hat the total surface area of cells with cleaved DNA was t1156 Martinez-Madrid et al. Freezing whole human ovaries
0.1% in all three groups, which was not statistically sig-ificant.
mmunohistochemical Detection of Active Caspase-3arly apoptosis was detected by means of immunohisto-hemical analysis of active caspase-3. We analyzed 121rimordial and primary follicles in fresh ovarian tissue, 182fter cryoprotectant exposure, and 244 after thawing, andll were negative for active caspase-3. Active caspase-3-ositive cells were found in antral follicles (Fig. 2D) andorpora lutea (Fig. 2C).
Smooth muscle cells, pericytes, and the majority of endo-helial cells were found to be active caspase-3-negative,rrespective of the size of the vessels (from capillaries torteries and veins) (Fig. 2A,B). Some endothelial cells wereccasionally slightly stained. Nevertheless, after counting2,000 endothelial cells per group, the percentage of active
aspase-3-positive endothelial cells was �1% in all groups:resh tissue, after DMSO exposure, and after thawing. Nonef the negative controls showed any active caspase-3 expres-ion, while positive signals were consistently observed inositive controls.
The difference in the number of follicles analyzed perroup (fresh, DMSO-exposed, and frozen-thawed), both forUNEL analysis (56, 131, and 199 follicles, respectively)nd for caspase detection (121, 182, and 244 follicles, re-pectively), was partly due to the variable density and un-ven distribution of follicle clusters in adult women, bothrom patient to patient and between different fragments ofhe same ovary (34). Furthermore, ovarian samples from theresh and DMSO-exposed groups were smaller than thoserom the frozen-thawed group, because the former consistedf biopsies of ovarian tissue taken from whole ovaries duringhe cryopreservation procedure, while the latter were theemaining whole ovaries. This also explains the difference inhe number of HPFs assessed per group (134, 130, and 622,espectively) in the morphometric analysis.
ltrastructural Assessmentvarian follicles and vessels were analyzed by LM and
ransmission electron microscopy (TEM) in frozen-thawedissue.
ollicular Compartmenthirty follicles (10 per patient) with the characteristics ofrimordial and primary follicles were investigated in frozen-hawed tissue by LM and TEM. By LM, these folliclesooked like regularly rounded structures, varying in diameterrom 40–80 �m. The oocytes were surrounded by a singleayer of follicular cells, flattened or cuboidal in shape, inrimordial and primary follicles, respectively. At the periph-ry, all the follicles were observed along a continuous basalembrane. By TEM, 29 (96.7%) of these follicles appeared
otally healthy-looking, presenting all the ultrastructural fea-
Vol. 87, No. 5, May 2007

F
FIGURE 1
Assessment of apoptosis. Analysis of DNA strand breaks by TUNEL in frozen-thawed whole ovary. (A)Primary follicle and stromal cells: (A1) DAPI counterstaining, and (A2) TUNEL staining. (B) Antral follicle: (B1)DAPI counterstaining, and (B2) TUNEL staining. (C and D) Blood vessels of different sizes: (C1 and D1)DAPI counterstaining, and (C2 and D2) TUNEL staining. Bars � 100 �m (A, C, and D), and 50 �m (B).
Martinez-Madrid. Freezing whole human ovaries. Fertil Steril 2007.
1157ertility and Sterility�

tmcm(f
uapovfffMartinez-Madrid. Freezing whole human ovaries. Fertil Steril 2007.
Martinez-Madrid. Freezing whole human ovaries. Fertil Steril 2007.
1158 Martinez-Madrid et al. Freezing whole human ovaries
ures of normal follicles (Fig. 3): intact nuclear and cellularembranes, normally arranged chromatin, well-preserved
ytoplasmic organelles, and a continuous normal thick basalembrane, according to criteria established by Motta et al.
33). In just one follicle out of 30 analyzed, some alteredeatures were detected (Fig. 4).
Healthy-looking follicles showed oocytes with a large vesic-lar nucleus, in which the chromatin appeared finely granularnd dispersed. One or more nucleoli were seen in the nucleo-lasm (Fig. 3A). In the oocyte cytoplasm, the majority ofrganelles were close to the nucleus, forming Balbiani’sitelline body. Rounded mitochondria with a pale matrix and aew peripheral cristae, membranes of endoplasmic reticulum,ree ribosomes, and, occasionally, multivesicular bodies wereound in the cytoplasm of oocytes (Fig. 3A,B).
n of active caspase-3 in frozen-thawed whole. (B) Vein negative for active caspase-3 staining. (C)e-3 staining. (D) Antral follicle with GCs positive for
50 �m (C and D).
TABLE 1Morphometric analysis of apoptosis by theTUNEL method before freezing, after DMSOexposure, and after thawing.
HPFsanalyzed
MeanTUNEL-positive
surface area
Before freezing 134 0.05 � 0.03a
After DMSOexposure
130 0.02 � 0.01a
After thawing 622 0.09 � 0.03a
a P�.05 (nonsignificant).
FIGURE 2
Assessment of apoptosis. Immunohistochemical detectioovary. (A) Arteriole negative for active caspase-3 stainingCorpus luteum with luteal cells positive for active caspasactive caspase-3 staining. Bars � 100 �m (A and B), and
Vol. 87, No. 5, May 2007

ttn
das
F
At the oocyte-follicular cell interface, close interdigita-ions between oocyte microvilli and follicular cell projec-ions were seen (Fig. 3C). Follicular cells showed a volumi-
FIGURE 3
Primary follicle with well-preserved features in frozen-thsingle layer of cuboidal follicular cells (Fc) on a continuoclustered in clouds in the oocyte cytoplasm, and the nustromal cells are visible close to the basal membrane. (and peripheral cristae in the oocyte cytoplasm. (C) Deta(Fc) projections and oocyte (O) microvilli. Note a desmofollicular cells, showing indented nuclei with peripheralmitochondria (m) in the cytoplasm. bm � continuous basand 0.62 �m (D).
Martinez-Madrid. Freezing whole human ovaries. Fertil Steril 2007.
ous, indented nucleus, in which the chromatin was d
ertility and Sterility�
istributed in isolated peripheral patches (Fig. 3A,D). This istypical feature of follicular cells, and does not represent a
ign of apoptosis. Rod-shaped mitochondria were observed
d whole ovary. (A) The oocyte (O) is surrounded by aasal membrane (bm). Note the mitochondria (m)lus (nu) visible in the oocyte nucleus (N). *Twoetail of a rounded mitochondrion with a pale matrixclose interdigitations observed between follicular celle connecting two follicular cells (arrow). (D) Detail ofhes of heterochromatin and numerous rod-shapedembrane. Bars � 1 �m (A), 0.25 �m (B), 0.43 �m (C),
aweus bcleo
B) Dil ofsom
patcal m
ispersed in the follicular cell cytoplasm (Fig. 3D). Numer-
1159

otA�
amcscbtdui
VSr
sTwb(tp(e
ttvn
itod
fTmtoc
DCsttittpfm
tmpEWvrvpbm
t
us junctions (gap junctions, desmosomes, and tight junc-ions) connected the follicular cells to each other (Fig. 3C).
continuous basal membrane of normal thickness (0.5–1.0m) divided all the follicles from the stroma (Fig. 3A,D).
Only one primordial follicle showed some morphologicallterations. These included rupture of the oocyte nuclearembrane, condensation of chromatin, and oocyte mito-
hondria with swollen and disrupted cristae (Fig. 4), whichuggested necrosis. The altered oocyte was surrounded by aontinuous layer of flattened follicular cells, among whichoth normal and apoptotic cells were found (Fig. 4). Despitehe alterations found in this follicle, normal-featured inter-igitations were detected between the oocyte and the follic-lar cells, as well as a continuous basal membrane surround-ng the follicle.
ascular Compartmentixty blood vessels (20 per patient) of different types (arte-
FIGURE 4
Primordial follicle with altered features in frozen-thawed whole ovary (in total, 3.3% of primordialand primary follicles showed ultrastructuralalterations). In the oocyte (O), note rupture of thenuclear membrane and condensation of chromatin(arrow), and among the follicular cells (Fc), onealtered follicular cell with condensation ofchromatin (arrowhead). N � oocyte nucleus.Bar � 2.27 �m.
Martinez-Madrid. Freezing whole human ovaries. Fertil Steril 2007.
ioles, capillaries, and venules), ranging from 5–100 �m in (
1160 Martinez-Madrid et al. Freezing whole human ovaries
ize, were analyzed in frozen-thawed tissue by LM andEM. The majority of vessels were totally healthy-looking,ith all vascular compartments (endothelial cells, basal mem-rane, smooth muscle cells, and pericytes) well preservedFig. 5A). They had a continuous endothelium and intact junc-ions between the endothelial cells, which showed a well-reserved nucleus containing normally arranged chromatinFig. 5B). No vessels showing any loss of endothelial cells orxposed connective tissue were observed.
Arterioles showed thick endothelial cells protruding intohe lumen, with abundant cytoplasmic processes toward ei-her the lumen or the basal membrane (Fig. 5B), whileenules contained flat endothelial cells with an elongateducleus and a thin muscular layer (Fig. 5A).
In total, 187 endothelial cells of all vessel types werenvestigated, 180 (96.3%) of which were healthy-looking. Inhese endothelial cells, cytoplasm organelles, such as numer-us abluminal and basal pinocytotic vesicles and mitochon-ria, appeared well preserved (Fig. 5B,C).
A small number of endothelial cells (7/187) with alteredeatures were encountered in a few arterioles and venules.hese included endothelial cells with nuclear and cytoplas-ic condensation (Fig. 6A), with a swollen and electron-
ranslucent cytoplasm typical of edematous cells (Fig. 6B),r with separations of intercellular contacts (Fig. 6A). Noapillaries showed an altered ultrastructure.
ISCUSSIONryopreservation of human ovarian cortex with the use of
tandard slow freezing and rapid thawing protocols appearso maintain the viability, morphology, and function of suchissue after thawing (35). However, follicular loss due toschemia after transplantation significantly shortens the func-ional life span of a graft. Ovarian cortical strip transplanta-ion may reverse the menopause and restore fertility inatients, but only for relatively short periods of time until theollicular reserve is depleted, with a subsequent return toenopausal levels (5, 36).
Vascular transplantation of intact ovaries would reducehe period of posttransplantation ischemia to just a fewinutes, allowing more follicles to survive and extending the
eriod of time that ovarian grafts remain functional (32).ncouraging results were recently documented in animals.ang et al. (16) and Yin et al. (17) described successful
ascular transplantation of frozen-thawed rat ovaries andeproductive tract in 4 out of 7 (57%) transplants that sur-ived for �60 days, were ovulatory, and resulted in oneregnancy. Chen et al. (26) showed that frozen-thawed rab-it ovaries remained functional for at least 7 months aftericrovascular transplantation in 13 of 15 (86.7%) animals.
Three recent studies achieved good results after freeze-hawing whole ovaries in large mammal species, i.e., pigs
31) and sheep (29, 30), with the birth of a live lamb (30).Vol. 87, No. 5, May 2007

F
FIGURE 5Blood vessels showing normal ultrastructure in frozen-thawed whole ovary. (A) Venule with flattened endothelialcells. (B) Arteriole containing thickened endothelial cells protruding into the lumen, with abundant cytoplasmicprocesses toward either the lumen or the basal membrane. The cytoplasm is filled with organelles and intactconnections between endothelial cells. (C) Detail of mitochondria (m) with intact membranes from an endothelialcell. N � endothelial cell nucleus. L � vascular lumen. Bars � 1.56 �m (A), 1 �m (B), and 0.3 �m (C).
Martinez-Madrid. Freezing whole human ovaries. Fertil Steril 2007.
1161ertility and Sterility�

Hod
mwata
ttDsdapiIcoiag
smfdfa(pgwto
tvisajccoap
dic(v
b
owever, since sheep ovaries are about one tenth of the sizef human ovaries, problems related to heat and mass transferFIGURE 6
Arterioles with a few altered endothelial cells infrozen-thawed whole ovary (in total, 3.7% ofendothelial cells showed ultrastructural alterations).(A) Separation of intercellular connections. *Anendothelial cell with nuclear and cytoplasmiccondensation (arrow) in an arteriole. (B) Swollenendothelial cell with electron-translucentcytoplasm in an arteriole. L � vascular lumen.Bars � 2.2 �m (A) and 0.75 �m (B).
Martinez-Madrid. Freezing whole human ovaries. Fertil Steril 2007.
uring freezing and thawing are presumed to be more p
1162 Martinez-Madrid et al. Freezing whole human ovaries
arked in humans. The aim of this study was to investigatehether the present cryopreservation protocol would induce
poptosis in any human ovarian cells, either after cryopro-ectant perfusion or after freeze-thawing, and to further an-lyze any ultrastructural alterations in the thawed ovary.
The hallmark of apoptosis is the presence of typical in-ranucleosomal DNA fragmentation, which is identifiable byhe DNA end-labeling method (TUNEL). Fragmentation ofNA is triggered by the activation of specific endonucleases,
uch as caspases. In particular, caspase-3 is the principalownstream effector enzyme of cell death, and it triggers thectivation of endogenous endonucleases. Therefore, theresence of caspase-3 identifies the early stage of apoptosisn those cells that are due to undergo programmed cell death.t is well known that apoptosis, the mechanism by whichells are eliminated through programmed cell death, alsoccurs in the ovary (37–39), where the process of remodel-ng is continuous. Physiologically, apoptosis is seen in lutealnd thecal cells of healthy corpora lutea, as well as inranulosa cells (GCs) of antral follicles.
Despite this physiologic removal of cells through apopto-is, assessment of apoptosis recently proved to be a goodethod to evaluate and compare the outcome of different
reeze-thawing protocols for human ovarian tissue (40). In-eed, some cryopreservation protocols induce apoptosis inrozen-thawed cells, which was detected by TUNEL (40)nd by immunohistochemical expression of active caspase-341). Although the mechanism of cell death during cryo-reservation is not fully understood, Tirelli et al. (42) sug-ested that increased apoptosis in GCs after cryopreservationas probably caused by physical alterations due to low
emperature, high salt concentrations, and an impaired anti-xidant metabolism.
Moreover, it was shown that cold preservation (43) andhe ischemic process (44) may induce apoptosis. Cryopreser-ation of a whole ovary requires a relatively long period ofschemia and cold preservation during cryoprotectant perfu-ion, which might induce apoptosis. It was proved thatpoptosis plays a crucial role after ischemia-reperfusion in-ury in organ transplantation, and specific inhibition ofaspase-3 decreases the number of apoptotic endothelialells in rat liver transplantation (45), improving the survivalf grafts. Thus, it is likely that the absence of apoptosisctivation in endothelial cells would be a good marker toredict the outcome of vascular transplantation.
In the present study, TUNEL and immunohistochemicaletection of active caspase-3 were applied to investigatenduction of apoptosis in whole human ovaries as a result ofold storage and ischemia during perfusion before freezingDMSO-exposed group), and as a result of the cryopreser-ation procedure itself (frozen-thawed group).
We did not find any signs of induction of apoptosis, eithery the TUNEL method or active caspase-3 expression, in
rimordial or primary follicles, either after DMSO exposureVol. 87, No. 5, May 2007

acato(rdo
(mcvtccdprb
paffpt�
qisibclj
ocaiafi
aaTmatl
aaoccam
vpIsanwpc
ttacalio
tattnttov
AtcUce
R
F
nd perfusion or after thawing. Our results in humans areompletely in line with those obtained by Dermici et al. (46)nd Bedaiwy et al. (27) in animals. Indeed, using TUNEL,hey did not observe any induction of apoptosis in primordialr primary follicles after thawing of sheep ovarian cortex46) or whole sheep ovaries (27). Rimon et al. (40), however,eported TUNEL-detected induction of apoptosis in primor-ial and primary follicles after cryopreservation of humanvarian cortical pieces.
We did not detect any induction of apoptosis in vesselsendothelial cells, smooth muscle cells, or pericytes) or stro-al cells in any group, either by TUNEL or IHC for active
aspase-3 detection. The absence of induction of apoptosis inascular cells, especially endothelial cells, is of great impor-ance because they are in the front line of exposure duringryoprotectant perfusion. Once again, our results in humansonfirm those observed in sheep. Arav et al. (29) found noifference in vascular or follicular survival or tissue mor-hology before and after freeze-thawing whole sheep ova-ies. Recovery of vascular function after thawing was provedy the production of factor VIII by endothelial cells.
In our study, TUNEL-positive cells or active caspase-3-ositive cells were mainly found in GCs of antral folliclesnd in luteal cells of corpora lutea, which is a physiologicaleature. Excluding these antral follicles and corpora lutearom the assessment, our morphometric analysis of TUNEL-ositive surface area revealed no significant differences inhe total surface area of cells with cleaved DNA, which was
0.1% in all three groups.
Transmission electron microscopy analysis was subse-uently applied to complete our apoptosis evaluation bynvestigating possible ultrastructural damage to ovarian tis-ue after thawing. TEM is a well-known method for detect-ng any subcellular alterations (such as fine damage to mem-ranes and organelles) that may occur in tissue afterryopreservation procedures. Indeed, TEM analysis of fol-icular integrity in human ovarian cortical fragments sub-ected to cryopreservation has already been used (11,47–50).
We analyzed, by TEM, three cryopreserved whole humanvaries, paying particular attention to the follicular and vas-ular compartments. No discernible ultrastructural alter-tions were encountered in frozen-thawed ovaries, confirm-ng our previous histology and viability findings (32), as wells the results of the present study of apoptosis. All theollicles but one (96.7%) were healthy-looking, and exhib-ted normal ultrastructural features.
Our results with thawed whole human ovaries are in totalgreement with those of Nisolle et al. (11), Eyden et al. (50),nd Hreinsson et al. (49) with human ovarian cortical pieces.hey reported similarities in the ultrastructural quality of pri-ordial and primary follicles before and after freeze-thawing
vascular human ovarian cortical fragments. Nevertheless, inhese studies, a few altered follicles containing either vacuo-
ated oocytes (11, 49) or follicular cells with pyknotic nuclei orertility and Sterility�
swollen cytoplasm (49, 50) were occasionally detected. Innimals, only one study has so far used TEM to evaluatevarian tissue after cryopreservation of whole ovaries, in thisase porcine (31). It demonstrated the feasibility of intact ovaryryopreservation in this model, showing good viability (84.4%)nd a well-preserved ultrastructure of the follicular compart-ent after cryostorage.
In our opinion, proving the ultrastructural integrity of theascular compartment is of crucial importance in any cryo-reservation protocol for whole organ vascular transplantation.ndeed, endothelial cell loss and apoptosis were also demon-trated by TEM in the iliac artery (51) and liver vessels (43)fter cryopreservation procedures. However, to our knowledge,o ultrastructural study has been performed on cryopreservedhole ovaries in any species to evaluate their vascular com-artment, even though cryoinjury to the vascular compartmentould result in organ failure after transplantation.
Therefore, in the present study, blood vessels of differentypes and sizes were scrupulously analyzed. All were foundo be well preserved, with no discernible ultrastructurallterations in the endothelial cells, basal membrane, peri-ytes, or smooth muscle cells. Indeed, we did not observeny subcellular alterations, cell-cell contact detachment, oross of endothelial cells, features which were described inschemia-reperfusion-injured or cryoinjured vessels in otherrgans (43, 51, 52).
In conclusion, the present study shows that cryopreserva-ion of an intact human ovary with its vascular pedicle is notssociated with induction of apoptosis or ultrastructural al-erations in any of the ovarian components. These data,ogether with our previous findings of high survival rates andormal histological structure in all ovarian elements afterhawing (32), lead us to conclude that the present freeze-hawing protocol does not cause significant injury to humanvaries, and may be a suitable technique for the cryopreser-ation of whole ovaries before transplantation.
cknowledgments: The authors thank Mira Hryniuk, B.A., for reviewinghe manuscript, and G.. Macchiarelli, M.D., for fruitful discussions andritical review. The authors also thank the Department of Anatomopathology,niversité Catholique de Louvain, Brussels, Belgium, for advice in the setup of
aspase-3 IHC, for help with TEM procedures, and for specimen-mbedding and hematoxylin-eosin staining.
EFERENCES1. Donnez J, Bassil S. Indications for cryopreservation of ovarian tissue.
Hum Reprod Update 1998;4:248–59.2. Donnez J, Godin PA, Qu J, Nisolle M. Gonadal cryopreservation in the
young patient with gynaecological malignancy. Curr Opin Obstet Gy-necol 2000;12:1–9.
3. The Ethics Committee of the American Society for Reproductive Med-icine. Fertility preservation and reproduction in cancer patients. FertilSteril 2005;83:1622–8.
4. Stachecki JJ, Cohen J. An overview of oocyte cryopreservation. ReprodBiomed Online 2004;9:152–63.
5. Donnez J, Dolmans MM, Martinez-Madrid B, Demylle D, Van Lan-gendonckt A. The role of cryopreservation for women prior to treatment
of malignancy. Curr Opin Obstet Gynecol 2005;17:333–8.1163

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
6. Baird DT, Webb R, Campbell BK, Harkness LM, Gosden RG. Long-term ovarian function in sheep after ovariectomy and transplantation ofautografts stored at �196°C. Endocrinology 1999;140:462–71.
7. Oktay K, Buyuk E, Veeck L, Zaninovic N, Xu K, Takeuchi T, et al.Embryo development after heterotopic transplantation of cryopreservedovarian tissue. Lancet 2004;363:837–40.
8. Silber SJ, Lenahan KM, Levine DJ, Pineda JA, Gorman KS, Friez MJ,et al. Ovarian transplantation between monozygotic twins discordantfor premature ovarian failure. N Engl J Med 2005;353:58–63.
9. Donnez J, Dolmans MM, Demylle D, Jadoul P, Pirard C, Squifflet J, etal. Livebirth after orthotopic transplantation of cryopreserved ovariantissue. Lancet 2004;364:1405–10.
0. Meirow D, Levron J, Eldar-Geva T, Hardan I, Fridman E, Zalel Y, etal. Pregnancy after transplantation of cryopreserved ovarian tissue in apatient with ovarian failure after chemotherapy. N Engl J Med 2005;353:318–21.
1. Nisolle M, Casanas-Roux F, Qu J, Motta P, Donnez J. Histologic andultrastructural evaluation of fresh and frozen-thawed human ovarianxenografts in nude mice. Fertil Steril 2000;74:122–9.
2. Liu J, Van der Elst J, Van den Broecke R, Dhont M. Early massivefollicle loss and apoptosis in heterotopically grafted newborn mouseovaries. Hum Reprod 2002;17:605–11.
3. Newton H, Aubard Y, Rutherford A, Sharma V, Gosden R. Lowtemperature storage and grafting of human ovarian tissue. Hum Reprod1996;11:1487–91.
4. Candy CJ, Wood MJ, Whittingham DG. Effect of cryoprotectants onthe survival of follicles in frozen mouse ovaries. J Reprod Fertil1997;110:11–9.
5. Gunasena KT, Villines PM, Critser ES, Critser JK. Live births afterautologous transplant of cryopreserved mouse ovaries. Hum Reprod1997;12:101–6.
6. Wang X, Chen H, Yin H, Kim SS, Tan SL, Gosden RG. Fertility afterintact ovary transplantation. Nature 2002;415:385.
7. Yin H, Wang X, Kim SS, Chen H, Tan SL, Gosden RG. Transplanta-tion of intact rat gonads using vascular anastomosis: effects of cryo-preservation, ischemia and genotype. Hum Reprod 2003;18:1165–72.
8. Winston RM, Browne JC. Pregnancy following autograft transplanta-tion of fallopian tube and ovary in the rabbit. Lancet 1974;2:494–5.
9. Jeremias E, Bedaiwy MA, Gurunluoglu R, Biscotti CV, Siemionow M,Falcone T. Heterotopic autotransplantation of the ovary with microvas-cular anastomosis: a novel surgical technique. Fertil Steril 2002;77:1278–82.
0. Goding JR, McCracken JA, Baird DT. The study of ovarian function inthe ewe by means of a vascular autotransplantation technique. J Endo-crinol 1967;39:37–52.
1. Paldi E, Gal D, Barzilai A, Hampel N, Malberger E. Genital organs.Auto and homotransplantation in forty dogs. Int J Fertil 1975;20:5–12.
2. Scott JR, Keye WR, Poulson AM, Reynolds WA. Microsurgical ovar-ian transplantation in the primate. Fertil Steril 1981;36:512–5.
3. Leporrier M, Von Theobald P, Roffe JL, Muller G. A new technique toprotect ovarian function before pelvic irradiation. Cancer 1987;60:2201–4.
4. Hilders CG, Baranski AG, Peters L, Ramkhelawan A, Trimbos JB.Succesful human ovarian autotransplantation to the upper arm. Cancer2004;101:2771–8.
5. Mhatre P, Mhatre J, Magotra R. Ovarian transplant: a new frontier.Transplant Proc 2005;37:1396–8.
6. Chen C, Chen S, Chang F, Wu G, Liu J, Yu C. Autologous heterotopictransplantation of intact rabbit ovary after cryopreservation. Hum Re-prod 2005;20(Suppl 1):i149–50.
7. Bedaiwy A, Jeremias E, Gurunluoglu R, Hussein MR, Siemianow M,Biscotti C, et al. Restoration of ovarian function after autotransplanta-tion of intact frozen-thawed sheep ovaries with microvascular anasto-mosis. Fertil Steril 2003;79:594–602.
8. Revel A, Elami A, Bor A, Yavin S, Natan Y, Arav A. Whole sheepovary cryopreservation and transplantation. Fertil Steril 2004;82:
1714 –5.1164 Martinez-Madrid et al. Freezing whole human ovaries
9. Arav A, Revel A, Nathan Y, Bor A, Gacitua H, Yavin S, et al. Oocyterecovery, embryo development and ovarian function after cryopreser-vation and transplantation of whole sheep ovary. Hum Reprod 2005;20:3554–9.
0. Imhof M, Bergmeister H, Lipovac M, Rudas M, Hofstetter G, HuberJ. Orthotopic microvascular re-anastomosis of whole cryopreservedovine ovaries resulting in pregnancy and live birth. Fertil Steril 2006;85:1208–15.
1. Imhof M, Hofstetter G, Bergmeister H, Rudas M, Kain R, Lipovac M,et al. Cryopreservation of a whole ovary as a strategy for restoringovarian function. J Assist Reprod Genet 2004;21:459–65.
2. Martinez-Madrid B, Dolmans MM, Van Langendonckt A, Defrere S,Donnez J. Freeze-thawing intact human ovary with its vascular pediclewith a passive cooling device. Fertil Steril 2004;82:1390–4.
3. Motta PM, Nottola SA, Familiari G, Makabe S, Stallone T, Macchiarelli G.Morphodynamics of the follicular-luteal complex during early ovariandevelopment and reproductive life. Int Rev Cytol 2003;223:177–288.
4. Schmidt KLT, Byskov AG, Nyboe Andersen A, Muller J, YdingAndersen C. Density and distribution of primordial follicles in singlepieces of cortex from 21 patients and in individual pieces of cortex fromthree entire human ovaries. Hum Reprod 2003;18:1158–64.
5. Hovatta O. Methods for cryopresevation of human ovarian tissue. RBMOnline 2005;6:72934.
6. Donnez J, Dolmans MM, Demylle D, Jadoul P, Pirard C, Squifflet J, etal. Restoration of ovarian function after orthotopic (intraovarian andperiovarian) transplantation of cryopreserved ovarian tissue in a womantreated by bone marrow transplantation for sickle cell anaemia: casereport. Hum Reprod 2006;21:183–8.
7. Tilly JL. Apoptosis and the ovary: a fashionable trend or food forthought? Fertil Steril 1997;67:226–8.
8. Johnson AL, Bridgham JT. Caspase-mediated apotosis in the vertebrateovary. Reproduction 2002;124:19–27.
9. Depalo R, Nappi L, Loverro G, Bettocchi S, Caruso ML, Valentini AM,et al. Evidence of apoptosis in human primordial and primary follicles.Hum Reprod 2003;18:2678–82.
0. Rimon E, Cohen T, Dantes A, Hirsh L, Amit A, Lessing JB, et al.Apoptosis in cryopreserved human ovarian tissue obtained from cancerpatients: a tool for evaluating cryopreservation utility. Int J Oncol2005;27:345–53.
1. Yagi T, Hardin JA, Valenzuela YM, Miyoshi H, Gores GJ, Nyberg SL.Caspase inhibition reduces apoptosis death of cryopreserved porcinehepatocytes. Hepatology 2001;33:1432–40.
2. Tirelli M, Basini G, Grasselli F, Bianco F, Tamanini C. Cryopreserva-tion of pig granulosa cells: effect of FSH addition to freezing medium.Domest Anim Endocrinol 2005;28:17–33.
3. Moriga T, Arii S, Takeda Y, Furuyama H, Mizumoto M, Mori A, et al.Protection by vascular endothelial growth factor against sinusoidalendothelial damage and apoptosis induced by cold preservation. Trans-plantation 2000;69:141–7.
4. Kim SS, Yang HW, Kang HG, Lee HH, Lee HC, Ko DS, et al.Quantitative assessment of ischemic tissue damage in ovarian corticaltissue with or without antioxidant (ascorbic acid) treatment. Fertil Steril2004;82:679–85.
5. Mueller TH, Kienle K, Beham A, Geissler EK, Jauch KW, Rentsch M.Caspase 3 inhibition improves survival and reduces early graft injuryafter ischemia and reperfusion in rat liver transplantation. Transplanta-tion 2004;15:1267–73.
6. Dermici B, Salle B, Frappart L, Franck M, Guerin JF, Lornage J.Morphological alterations and DNA fragmentation in oocytes fromprimordial and primary follicles after freezing-thawing of ovarian cor-tex in sheep. Fertil Steril 2002;77:595–600.
7. Gook DA, Edgar DH, Stern C. Effect of cooling rate and dehydrationregimen on the histological appearance of human ovarian cortex followingcryopreservation in 1,2-propanediol. Hum Reprod 1999;14:2061–8.
8. Gook DA, Edgar DH, Stern C. The effects of cryopreservation regi-mens on the morphology of human ovarian tissue. Mol Cell Endocrinol
2000;169:99–103.Vol. 87, No. 5, May 2007

4
5
5
5
F
9. Hreinsson J, Zhang P, Swahn ML, Hultenby K, Hovatta O. Cryopreser-vation of follicles in human ovarian cortical tissue. Comparison ofserum and human serum albumin in the cryoprotectant solutions. HumReprod 2003;18:2420–8.
0. Eyden B, Radford J, Shalet SM, Thomas N, Brison DR, Lieberman BA.Ultrastructural preservation of ovarian cortical tissue cryopreserved indimethylsulfoxide for subsequent transplantation into young female
cancer patients. Ultrastruct Pathol 2004;28:239–45.ertility and Sterility�
1. Pascual G, Rodriguez M, Corrales C, Turegano F, Garcia-HonduvillaN, Bellon JM, et al. New approach to improving endothelial preser-vation in cryopreserved arterial substitutes. Cryobiology 2004;48:62–71.
2. Chiavarelli R, Macchiarelli G, Familiari G, Chiavarelli M, MacchiarelliP, Del Basso P, et al. Ultrastructural changes of coronary artery endo-thelium induced by cardioplegic solutions. Thorac Cardiovasc Surg
1989;37:151–7.1165

Ubaifi5e
RP
T
S
R
Novel method to characterize primary cultures ofleiomyoma and myometrium with the use ofconfirmatory biomarker gene arraysMinnie Malik, Ph.D.,a and William H. Catherino, M.D., Ph.D.a,b
a Department of Obstetrics and Gynecology, Uniformed Services University of the Health Sciences, Bethesda, Maryland; andb Reproductive Biology and Medicine Branch, National Institute of Child Health and Human Development, National Institutesof Health, Bethesda, Maryland
Objective: To develop a rapid biomarker method for confirming that leiomyoma and myometrium primarycultures maintain the molecular phenotype of the progenitor tissues.Design: Confirmation of primary cultures from leiomyoma and myometrium tissues.Setting: University hospital.Patient(s): Women undergoing hysterectomy for symptomatic leiomyomas.Intervention(s): Primary cell cultures, reverse-transcriptase polymerase chain reaction (RT-PCR), microarray,real time RT-PCR, and immunofluorescence.Main Outcome Measure: Relative messenger RNA and protein expression in leiomyoma and myometrial cellcultures.Result(s): We developed primary cell cultures from human leiomyoma and patient-matched myometriumobtained from hysterectomy specimens. In the primary cultures, we confirmed the presence of smoothmuscle-specific �-actin as well as filamentous actin. Based on microarray analysis, we expected andconfirmed, in the progenitor tissue and derived primary cultures, an overexpression of versican (8.31 fold� 2.2 SEM and 4.3 fold � 1.01 SEM, respectively), transforming growth factor beta-3 (5.66 fold � 0.82SEM and 4.92 fold � 0.58 SEM, respectively), and cytochrome P450-26A1 (6.76 fold � 0.80 SEM and 6.17fold � 2.02 SEM, respectively), and an underexpression of dermatopontin (�5.6 fold � 1.82 SEM and�3.41 � 1.20 SEM, respectively).Conclusion(s): Primary cell cultures offer a reliable in vitro model system for leiomyoma disease, if confirmed.Analysis of a gene array that distinguishes between myometrium and leiomyoma molecular phenotypes offers arapid and reliable confirmation method, and provides confidence that in vitro findings resemble in vivo disease.(Fertil Steril� 2007;87:1166–72. ©2007 by American Society for Reproductive Medicine.)
Key Words: Leiomyoma, myometrium, primary cultures, microarray, RT-PCR, Western blot, �-actin, biomarkers
hlwe
oymhmTdmi
etmFg
terine smooth muscle leiomyomas are the most commonenign pelvic tumor, affecting about 40% of reproductive-ged women, and increasing to a 70%– 80% cumulativencidence by age 50 years (1). Leiomyomas were identi-ed in �70% of hysterectomy specimens (2), with 20%–0% of these tumors causing symptoms significantnough to warrant intervention (3). In addition, 27% of
eceived January 17, 2006; revised and accepted August 14, 2006.resented in part at the 61st Annual Meeting of the American Society forReproductive Medicine, Montreal, Quebec, Canada, October 15–19,2005.
he opinions or assertions contained herein are the private views of theauthors and are not to be construed as official or as reflecting the viewsof the Department of Health and Human Services, the Department ofthe Army, or the Department of Defense of the United States.
upported by an intramural research grant (CC085CC) from the UniformedServices University of the Health Sciences, Bethesda, Maryland, and bythe Intramural Research Program of the Reproductive Biology and Med-icine Branch, National Institute of Child Health and Human Development,National Institutes of Health, Bethesda, Maryland.
eprint requests: William H. Catherino, M.D., Ph.D., Department of Ob-stetrics and Gynecology, Uniformed Services University of the HealthSciences, 4301 Jones Bridge Road, Bethesda, Maryland 20814 (FAX:
m301-295-6774; E-mail: [email protected]).
1166 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
ysterectomies were performed to treat symptomaticeiomyomas (3,4), and it was estimated that 10%–15% ofomen between ages 25– 64 years will require a hyster-
ctomy for these tumors (2).
Despite the significant morbidity associated with leiomy-mata, these growths are incompletely understood. In recentears, molecular characterization of human uterine leiomyo-as with the use of technologies such as microarray analysis
as led to some understanding of the different pathways thatay be involved in the development of these tumors (5–9).he strength of such studies is their direct relation to humanisease, but they are limited by their high expense andinimal capability to evaluate the long-term impact of var-
ous treatments or therapies with the use of human samples.
To address such limitations, laboratory model systems aressential. In vivo animal models were developed to studyhis disease, and include the Eker rat (10), the guinea pigodel (11,12), and the transgenic mouse model (13,14).emale Eker rats (with a defect in the Tsc2 tumor-suppressorene) and rat tumor cell lines are the most common in vivo
odels and in vitro cell lines in use (10). These models may0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.111
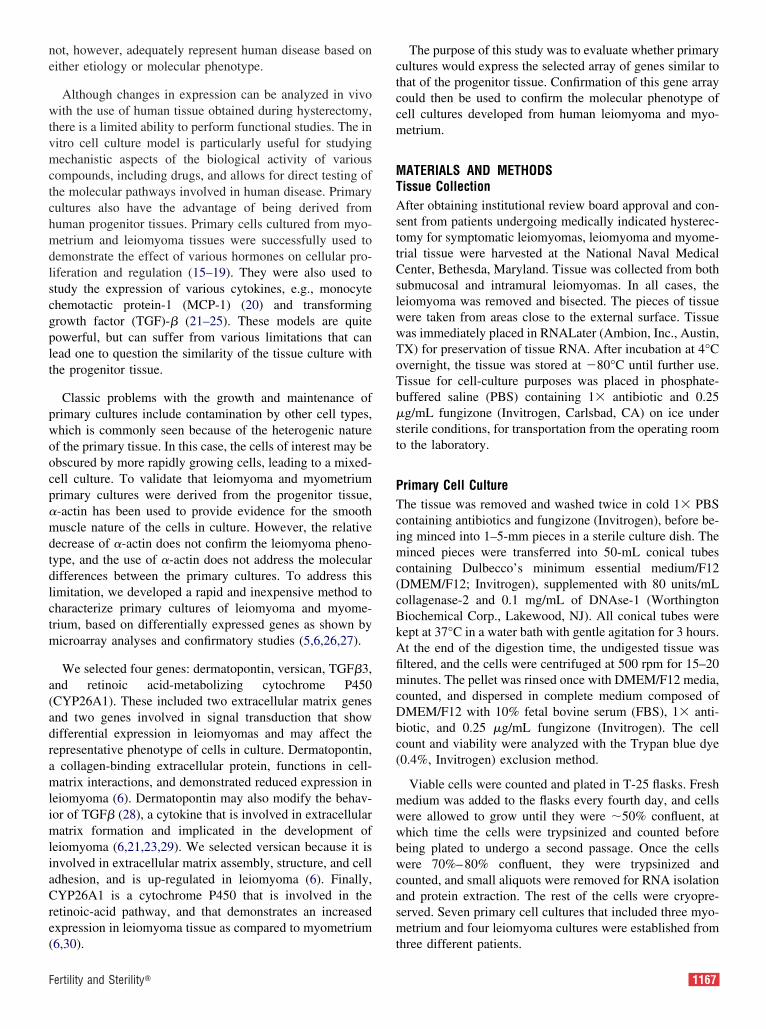
ne
wtvmctchmdlscgplt
pwoocp�mdtdlctm
a(adramlimliaCre(
ctccm
MTAsttCslwwToTb�st
PTcimc(cBkAfimcDbc(
mwwbwcasm
F
ot, however, adequately represent human disease based onither etiology or molecular phenotype.
Although changes in expression can be analyzed in vivoith the use of human tissue obtained during hysterectomy,
here is a limited ability to perform functional studies. The initro cell culture model is particularly useful for studyingechanistic aspects of the biological activity of various
ompounds, including drugs, and allows for direct testing ofhe molecular pathways involved in human disease. Primaryultures also have the advantage of being derived fromuman progenitor tissues. Primary cells cultured from myo-etrium and leiomyoma tissues were successfully used to
emonstrate the effect of various hormones on cellular pro-iferation and regulation (15–19). They were also used totudy the expression of various cytokines, e.g., monocytehemotactic protein-1 (MCP-1) (20) and transformingrowth factor (TGF)-� (21–25). These models are quiteowerful, but can suffer from various limitations that canead one to question the similarity of the tissue culture withhe progenitor tissue.
Classic problems with the growth and maintenance ofrimary cultures include contamination by other cell types,hich is commonly seen because of the heterogenic naturef the primary tissue. In this case, the cells of interest may bebscured by more rapidly growing cells, leading to a mixed-ell culture. To validate that leiomyoma and myometriumrimary cultures were derived from the progenitor tissue,-actin has been used to provide evidence for the smoothuscle nature of the cells in culture. However, the relative
ecrease of �-actin does not confirm the leiomyoma pheno-ype, and the use of �-actin does not address the molecularifferences between the primary cultures. To address thisimitation, we developed a rapid and inexpensive method toharacterize primary cultures of leiomyoma and myome-rium, based on differentially expressed genes as shown byicroarray analyses and confirmatory studies (5,6,26,27).
We selected four genes: dermatopontin, versican, TGF�3,nd retinoic acid-metabolizing cytochrome P450CYP26A1). These included two extracellular matrix genesnd two genes involved in signal transduction that showifferential expression in leiomyomas and may affect theepresentative phenotype of cells in culture. Dermatopontin,
collagen-binding extracellular protein, functions in cell-atrix interactions, and demonstrated reduced expression in
eiomyoma (6). Dermatopontin may also modify the behav-or of TGF� (28), a cytokine that is involved in extracellularatrix formation and implicated in the development of
eiomyoma (6,21,23,29). We selected versican because it isnvolved in extracellular matrix assembly, structure, and celldhesion, and is up-regulated in leiomyoma (6). Finally,YP26A1 is a cytochrome P450 that is involved in the
etinoic-acid pathway, and that demonstrates an increasedxpression in leiomyoma tissue as compared to myometrium
6,30). tertility and Sterility�
The purpose of this study was to evaluate whether primaryultures would express the selected array of genes similar tohat of the progenitor tissue. Confirmation of this gene arrayould then be used to confirm the molecular phenotype ofell cultures developed from human leiomyoma and myo-etrium.
ATERIALS AND METHODSissue Collectionfter obtaining institutional review board approval and con-
ent from patients undergoing medically indicated hysterec-omy for symptomatic leiomyomas, leiomyoma and myome-rial tissue were harvested at the National Naval Medicalenter, Bethesda, Maryland. Tissue was collected from both
ubmucosal and intramural leiomyomas. In all cases, theeiomyoma was removed and bisected. The pieces of tissueere taken from areas close to the external surface. Tissueas immediately placed in RNALater (Ambion, Inc., Austin,X) for preservation of tissue RNA. After incubation at 4°Cvernight, the tissue was stored at �80°C until further use.issue for cell-culture purposes was placed in phosphate-uffered saline (PBS) containing 1� antibiotic and 0.25g/mL fungizone (Invitrogen, Carlsbad, CA) on ice under
terile conditions, for transportation from the operating roomo the laboratory.
rimary Cell Culturehe tissue was removed and washed twice in cold 1� PBSontaining antibiotics and fungizone (Invitrogen), before be-ng minced into 1–5-mm pieces in a sterile culture dish. Theinced pieces were transferred into 50-mL conical tubes
ontaining Dulbecco’s minimum essential medium/F12DMEM/F12; Invitrogen), supplemented with 80 units/mLollagenase-2 and 0.1 mg/mL of DNAse-1 (Worthingtoniochemical Corp., Lakewood, NJ). All conical tubes wereept at 37°C in a water bath with gentle agitation for 3 hours.t the end of the digestion time, the undigested tissue wasltered, and the cells were centrifuged at 500 rpm for 15–20inutes. The pellet was rinsed once with DMEM/F12 media,
ounted, and dispersed in complete medium composed ofMEM/F12 with 10% fetal bovine serum (FBS), 1� anti-iotic, and 0.25 �g/mL fungizone (Invitrogen). The cellount and viability were analyzed with the Trypan blue dye0.4%, Invitrogen) exclusion method.
Viable cells were counted and plated in T-25 flasks. Freshedium was added to the flasks every fourth day, and cellsere allowed to grow until they were �50% confluent, athich time the cells were trypsinized and counted beforeeing plated to undergo a second passage. Once the cellsere 70%–80% confluent, they were trypsinized and
ounted, and small aliquots were removed for RNA isolationnd protein extraction. The rest of the cells were cryopre-erved. Seven primary cell cultures that included three myo-etrium and four leiomyoma cultures were established from
hree different patients.
1167

RTlgttItwF(p
GW(oitTLipT
ipt
CFccst0nnmsos6awca(
NA Extractionotal cellular RNA was extracted from myometrium and
eiomyoma tissue with the use of TRIzol Reagent (Invitro-en), as described previously (5). For primary cultures, cellshat underwent a second passage were used for RNA isola-ion with the use of the RNAqueous Mini-Prep (Ambion,nc.), according to the manufacturer’s instructions. To ensurehat no contaminating DNA was present, all RNA samplesere treated with DNAse-I enzyme by means of the DNA-ree kit, in accordance with the manufacturer’s protocolAmbion, Inc.). The RNA was quantified at A260 spectro-hometrically before storage at �80°C.
ene Expression Analysise used the reverse transcriptase-polymerase chain reaction
RT-PCR) as well as real-time RT-PCR, as described previ-usly (5,6), to evaluate genes that were differentially expressedn leiomyomas (Table 1). These genes were selected based onhe microarray analyses performed by our laboratory (5,6,26).he primer sequence and PCR conditions are listed in Table 2.eiomyoma and myometrium samples were run side-by-side at
dentical concentrations of template. Glyceraldehyde-3-phos-hate dehydrogenase (GAPDH) was used as an internal control.he figures presenting gel electrophoresis results represent an
TABLE 1Expression of selected genes, as demonstrated
Genes of interestPathway
represented
Dermatopontin Extracellular matrixVersican Extracellular matrixTGF�3 TGF�/SMAD pathwayCYP26A1 Retinoic-acid pathwayMalik. Biomarkers to confirm leiomyoma cultures. Fertil Steril 2007.
TABLE 2Primer sequence and PCR conditions for genes
Genes Primer sequence (5=
Dermatopontin F: CCACAGAGCCTCGGGGR: GATTCCAGAGCCGCTAC
Versican F: GAAAAGTCAGCCTACCTR: GATGCGGAGAAATTCAC
TGF�3 F: TGCAGACACAACCCACAR: ACATTTACAAGACTTCAC
CYP26A1 F: AACATTCGCGCCAAGATR: AGGTAAGTGATCAGAGA
Note: F � forward; R � reverse.
Malik. Biomarkers to confirm leiomyoma cultures. Fertil Steril 2007.
1168 Malik and Catherino Biomarkers to confirm leiomyoma
ndependent experiment. For real-time RT-PCR, the data com-rise the average of seven cell lines derived from separateissues from different patients.
ytoimmunofluorescenceor immunofluorescence microscopy to study smooth mus-le specific �-actin, myometrium and leiomyoma primaryultures were grown to 70% confluence on glass chamberlides (Nalge Nunc International, Rochester, NY). The cul-ures were fixed with cold methanol and permeabilized with.2% Triton X-100 (Sigma-Aldrich, St. Louis, MO). Theonspecific sites were blocked using 1% BSA and 10%ormal goat serum, and the cells were incubated with smoothuscle-specific (SMC) �-actin (NeoMarkers AP-1; Lab Vi-
ion Corporation, Fremont, CA) antibody at 1:50 dilutionvernight at 4°C. Alexa-594 (Invitrogen) was used as theecondary dye at a 1-�g/mL concentration. Nuclear dye-diamino-2-phenylindole (DAPI; Sigma-Aldrich) wasdded at 0.1 �g/mL in PBS before the cells were examinedith an Axiovert 405M epifluorescence inverted light mi-
roscope (Carl Zeiss, Oberkochen, Germany). Images werecquired with a charge-coupled device (CCD) cameraHamamatsu Orca, Shizuoka, Japan).
icroarray analysis.
pression in leiomyomasicroarray analysis) (5) Fold (F:M) Change
Down-regulated �9.41Up-regulated 5.79Up-regulated 3.0Up-regulated 15.0
terest.
Productsize (bp)
Annealingtemperature (°C)
C 123 58.0GAGTC 80 54.8
175 58.0CCAT
200 57.0GG
by m
Ex(m
of in
–3=)
AACTTC
TGTTGGGCCA
CTGTGT
cultures Vol. 87, No. 5, May 2007

cchctbcc
0f
SAPi
F
To study filamentous actin (F-actin) expression, the primaryultures were grown to 70% confluence on Permanox Lab-Tekhamber slides (Nalge Nunc Int.) and fixed with 4% formalde-yde. Phalloidin-FITC (Sigma-Aldrich) antibody was used ac-ording to the manufacturer’s instructions. Briefly, after fixa-ion, the cells were permeabilized with 0.1% Triton X-100, andlocked with the use of 0.5% BSA for 30 minutes before theells were incubated with phalloidin-FITC antibody at a 5 mg/L
FIGURE 1
Expression of �-actin in primary cultures of myometrimmunofluorescence. Cells were grown in four-well cwas localized using smooth muscle-specific �-actin a(see Materials and Methods). The nuclei were stained�-actin was identified in cells derived from both myo
Malik. Biomarkers to confirm leiomyoma cultures. Fertil Steril 2007.
oncentration (1:200 dilution) for 30 minutes. We used DAPI at a
ertility and Sterility�
.1 �g/mL PBS as the nuclear dye. Observations were per-ormed as already described.
tatistical Analysisll experiments were done in triplicate. For real-time RT-CR data, the results are reported as means � SEM, includ-
ng the range value of the data set. For each culture, the
and leiomyoma, as detected byber slides. The cells were fixed, and the �-actinody and Alexa-594-labeled secondary antibodynucleic acid-specific DAPI antibody. Staining for
rium and leiomyoma. Magnification � �63.
iumhamntibby
met
verage expression of three replicates was calculated before
1169

rtwWt
RAmaagCicpma
budccbPfRttc
iUomslpPt
elative quantification with the use of normalization againsthe housekeeping gene was performed. Relative expressionas calculated, based on the method of Pfaffl (31). Theilcoxon signed rank test was used for nonparametric sta-
istical evaluation.
ESULTSs shown in Figure 1, expression of �-actin was observed byeans of immunofluorescence in cultures of myometrium
nd leiomyoma. The presence of smooth muscle-specificctin indicated that cell cultures derived from the two pro-enitor tissues retained their smooth muscle characteristics.ontrol experiments with no primary antibody showed min-
mal background staining. The myometrial and fibroidalultures also demonstrated the presence of F-actin (Fig. 2), aolymer form of actin that plays a fundamental role inaintaining cyoskeletal structure and cellular functions such
s cell adhesion.
Decreased dermatopontin expression was demonstrated toe a consistent characteristic of leiomyomas (6). With these of RT-PCR, we demonstrated a decreased expression ofermatopontin gene in leiomyoma tissue and in the primaryulture, compared to the normal myometrium tissue andulture (Fig. 3A). Decreased expression of dermatopontin inoth primary cultures (�3.41 � 1.2-fold; range, 2.2–4.6;�.01) and leiomyoma progenitor tissue (�5.6 � 1.82-
old,; range, 4.3–6.6; P�.01) was observed by real timeT-PCR (Fig. 3C). These findings were representative of
hree primary cultures derived from tissues of different pa-ients. The difference between the progenitor tissue and the
FIGURE 2
Expression of F-actin in primary cultures ofmyometrium and leiomyoma, as detected byimmunofluorescence. Cells were fixed and thenstained with phalloidin-FITC. The nuclei werestained by nucleic acid-specific DAPI antibody(see Materials and Methods). Magnification ��10.
Malik. Biomarkers to confirm leiomyoma cultures. Fertil Steril 2007.
ell lines was not significant.
1170 Malik and Catherino Biomarkers to confirm leiomyoma
Versican, a chondroitin sulfate proteoglycan, is involvedn matrix assembly, matrix structure, and cell adhesion.p-regulation (sixfold) of versican was reported in leiomy-ma tissue (8) by microarray analysis relative to the myo-etrium. As shown in Figure 3B,C, expression of the ver-
ican gene was up-regulated in the primary cell cultures ofeiomyoma (4.3 � 1.01-fold; range, 3.4–5.1; P�.01) and itsrogenitor tissue (8.31 � 2.2-fold; range, 6.5–10.3;-fold;�.01). The difference between the progenitor tissue and
he cell lines was not significant.
FIGURE 3
Expression of extracellular matrix genes in primarycultures of myometrium (Mc) and leiomyoma (Lc),and corresponding parent tissues (M and L). Lane1 in all gels represents the molecular size marker.(A) Expression of dermatopontin gene was down-regulated in leiomyoma tissue (L versus M) andcultures derived from it (Lc versus Mc).(B) Versican expression was up-regulated in boththe leiomyoma tissue (L) and the derived primaryculture (Lc). (C) Real-time RT-PCR data, showingfold difference in expression of dermatopontin andversican in progenitor tissue (L:M, yellow bar) andcell cultures (Lc:Mc, orange bar). The data are themean of seven cell lines derived from threeseparate patients. The difference betweenprogenitor tissue and cell lines was not significant(P�.05, Wilcoxon signed rank test).
Malik. Biomarkers to confirm leiomyoma cultures. Fertil Steril 2007.
cultures Vol. 87, No. 5, May 2007

dl4tbr(
eR0sc55
oomdFt
DWCtmafiHtammtegtsta
uopCismos�ott
ltkrsmrwmc
m
F
The cytochrome CYP26A1 is responsible for the break-own of retinoic acid in the cell, and was overexpressed ineiomyomas as compared to the myometrium (Table 1, Fig.A). A similar overexpression was observed in the tissue andhe primary culture derived from the parent tissues, as showny RT-PCR and gel electrophoresis (Fig. 4A). An up-egulation of TGF�3 was observed by means of RT-PCRFig. 4B) in primary cultures of leiomyoma.
Figure 4C demonstrates a quantitative difference in thexpression of CYP26A1 and TGF�3 as shown by real timeT-PCR in progenitor tissue and cell cultures. A 4.92 �.58-fold (range, 4.4–5.4; P�.05) difference in the expres-ion of TGF�3 was observed in leiomyoma-cell culture asompared to myometrium-cell culture, while there was a.66 � 0.82-fold difference in progenitor tissue (range,
FIGURE 4
Expression of CYP26A1, a retinoic acid-metabolizing cytochrome P450, and TGF�3.(A and B) The RT-PCR data, as analyzed by gelelectrophoresis. The up-regulation of both genesis clearly demonstrated in leiomyoma tissue (Lversus M) as well as in the derived primary cultureof leiomyoma (Lc versus Mc). (C) Histogramrepresenting fold difference in expression ofTGF�3 and CYP26A1 in progenitor tissue (L:M,yellow bar) and cell cultures (Lc:Mc, orange bar),as analyzed by real time RT-PCR. The differencebetween progenitor tissue and cell lines was notsignificant (P�.05, Wilcoxon signed rank test).
Malik. Biomarkers to confirm leiomyoma cultures. Fertil Steril 2007.
.1–6.2; P�.05). The expression of CYP26A1 in leiomy- l
ertility and Sterility�
ma cultures demonstrated an average increased expressionf 6.17 � 2.02-fold (range, 5.9–6.4; P�.01) as compared toyometrium cultures, and compared to a 6.76� 0.80-fold
ifference in the progenitor tissue (range, 6.5–7.1; P�.01;ig. 4C). The difference between the progenitor tissue and
he cell lines was not significant.
ISCUSSIONe demonstrated that dermatopontin, versican, TGF�3, and
YP26A1 mRNA were differentially expressed biomarkershat may be used for validation of primary cultures of myo-etrium and leiomyoma. The presence of �-actin and F-
ctin in the cells, as shown by immunofluorescence, con-rmed the smooth muscle nature of the two cultures.owever, the presence of �-actin and F-actin confirms only
he smooth muscle nature of the cultures, and not the char-cteristics that differentiate the leiomyoma from the normalyometrium. We further validated leiomyoma cultures fromyometrium cultures, based on the molecular characteristics
hat distinguish tumor from normal tissue. In our study,xtracellular matrix genes, dermatopontin, and versicanenes demonstrated a similar expression in the primary cul-ures and the parent leiomyoma tissue. Similarly, expres-ions of TGF�3 and CYP26A1, involved in signal transduc-ion pathways, were also differentially expressed in culturess in the parent tissue.
Much of the in vitro research on the biology of humanterine leiomyomas has proceeded from the use of explantsr primary monolayer cultures established from tissue sam-les taken after hysterectomy or myomectomy (21,32,33).haracterization of cell cultures derived from primary tissue
s a very important factor in the development of a modelystem. Most laboratories that use cell cultures as theirodel system tend to distinguish the smooth muscle nature
f the cultures based on the expression of smooth muscle-pecific cytoskeletal proteins such as myosin, desmin, and-actin. While such studies demonstrate the smooth musclerigin of the cultured cells, they may not necessarily identifyhe tissues derived from leiomyomata compared with thosehat were derived from myometrium.
The use of molecular biomarkers in myometrium andeiomyoma cultures supports the supposition that the cul-ures are derived from the progenitor tissue. These “biomar-er” genes can be quickly and inexpensively used in labo-atories to confirm the nature of the tissues used. Primerequences are provided in Table 2. To establish a reliableodel system for in vitro studies, the cultures should closely
epresent the nature of the parent tissue from which theyere derived. In this study, we demonstrated that, based onolecular characteristics, primary cultures can retain in vivo
haracteristics.
In conclusion, we have developed an in vitro cell cultureodel system that is based on differential gene expression in
eiomyomas and corresponding myometrium. After confir-
1171

mlmnosl
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
ation with the use of the described biomarkers, in vitroeiomyoma model systems may be used to perturb promisingolecular pathways that may determine the leiomyoma phe-
otype, and for the initial testing of novel therapies. Thispportunity to test novel therapies would provide a criticaltep in the advancement of effective treatments for uterineeiomyomas.
EFERENCES1. Baird DD. Invited commentary: uterine leiomyomata—we know so
little but could learn so much. Am J Epidemiol 2004;159:124–6.2. Cramer SF, Patel D. The frequency of uterine leiomyomas. Am J Clin
Pathol 1990;94:435–8.3. Buttram VC, Reiter RC. Uterine leiomyomata: etiology, symptomatol-
ogy, and management. Fertil Steril 1981;36:433–45.4. Pokras R, Hufnagel VG. Hysterectomy in the United States, 1965–
1984. Am J Public Health 1988;78:852–54.5. Catherino WH, Prupas C, Tsibris JC, Leppart PC, Payson M, Nieman
LK, et al. Strategy for elucidating differentially expressed genes inleiomyomata identified by microarray technology. Fertil Steril 2003;80:282–90.
6. Catherino WH, Leppert PC, Stenmark MH, Payson M, Potlog-NahariC, Nieman LK, et al. Reduced dermatopontin expression is a molecularlink between uterine leiomyomas and keloids. Genes ChromosomesCancer 2004;40:204–17.
7. Leitao MM, Soslow RA, Nonaka D, Olshen AB, Aghajanian C, Sab-batini P, et al. Tissue microarray immunohistochemical expression ofestrogen, progesterone, and androgen receptors in uterine leiomyomataand leiomyosarcoma. Cancer 2004;101:1455–62.
8. Luo X, Ding L, Xu J, Chegini N. Gene expression profiling of leiomy-oma and myometrial smooth muscle cells in response to transforminggrowth factor-beta. Endocrinology 2005;146:1097–118.
9. Lee EJ, Kong G, Lee SH, Rho SB, Park CS, Kim BG, et al. Profilingof differentially expressed genes in human uterine leiomyomas. Int JGynecol Cancer 2005;15:146–54.
0. Walker CL, Hunter D, Everitt J. Uterine leiomyoma in the Eker rat: aunique model of important diseases of women. Genes ChromosomesCancer 2003;38:349–56.
1. Dallenbach FD, Thomas JA. Experimentally induced myofibroblasticneoplasia in guinea pigs. Indian J Med Res 1982;76:272–80.
2. Porter KB, Tsibris JC, Nicosia SV, Murphy JM, O’Brien WF, Rao PS,et al. Estrogen-induced guinea pig model for uterine leiomyomas: dothe ovaries protect? Biol Reprod 1995;52:824–32.
3. Romangnolo B, Molina T, Leroy G, Blin C, Porteux A, Thomasset M,et al. Estradiol-dependent uterine leiomyomas in transgenic mice. J ClinInvest 1996;98:777–84.
4. Webster MA, Martin-Soudant N, Nepveu A, Cardiff RD, Muller WJ.The induction of uterine leiomyomas and mammary tumors in trans-genic mice expressing polyomavirus (PyV) large T (LT) antigen isassociated with the ability of PyV LT antigen to form specific com-plexes with retinoblastoma and CUTLI family members. Oncogene1998;16:1963–72.
5. Nowak RA, Rein MS, Heffner LJ, Friedman AJ, Tashjian AH. Produc-tion of prolactin by smooth muscle cells cultured from human uterinefibroid tumors. J Clin Endocrinol Metab 1992;76:1308–13.
6. Bulun SE, Simpson ER, Word RA. Expression of the CYP19 gene andits product aromatase cytochrome P450 in human uterine leiomyoma
tissues and cells in culture. J Clin Endocrinol Metab 1993;78:736–43.1172 Malik and Catherino Biomarkers to confirm leiomyoma
7. Kobayashi Y, Zhai YL, Iinuma M, Horiuchi A, Nikaido T, Fujii S.Effects of a GnRH analogue on human smooth muscle cells culturedfrom normal myometrial and from uterine leiomyomal tissues. MolHum Reprod 1997;3:91–9.
8. Horiuchi A, Nikaido T, Yoshizawa T, Itoh K, Kobayashi Y, Toki T, etal. HCG promotes proliferation of uterine leiomyomal cells morestrongly than that of myometrial smooth muscle cells in vitro. Mol HumReprod 2000;6:523–8.
9. Sumitani H, Shozu M, Segawa T, Murakami K, Yang H-J, Shimada K,et al. In situ estrogen synthesized by aromatase P450 in uterine leiomy-oma cells promotes cell growth probably via an autocrine/intracrinemechanism. Endocrinology 2000;141:3852–61.
0. Sozen I, Olive DL, Arici A. Expression and hormonal regulation ofmonocyte chemotactic protein-1 in myometrium and leiomyomata.Fertil Steril 1998;69:1095–102.
1. Lee BS, Nowak RA. Human leiomyoma smooth muscle cells showincreased expression of transforming growth factor-beta 3 (TGFbeta3)and altered responses to the antiproliferative effects of TGF beta. J ClinEndocrinol Metab 2001;86:913–20.
2. Chegini N, Tang X-M, Chunfeng MA. Regulation of transforminggrowth factor-�1 expression by granulocyte macrophage-colony-stimulating factor in leiomyoma and myometrial smooth musclecells. J Clin Endocrinol Metab 1999;84:4138 – 43.
3. Arici A, Sozen I. Transforming growth factor-�3 is expressed at highlevels in leiomyoma where it stimulates fibronectin expression and cellproliferation. Fertil Steril 2000;73:1006–11.
4. Arici A, Sozen I. Expression, menstrual cycle-dependent activation,and bimodal mitogenic effect of transforming growth factor-�1 inhuman myometrium and leiomyoma. Am J Obstet Gynecol 2003;188:76–83.
5. Luo X, Ding L, Xu J, Chegini N. Gene expression profiling of leiomy-oma and myometrial smooth muscle cells in response to transforminggrowth factor-�. Endocrinology 2004;146:1097–118.
6. Catherino WH, Salama A, Potlog-Nahari C, Leppert P, Tsibris J, SegarsJ. Gene expression studies in leiomyomata: new directions for research.Semin Reprod Med 2003;22:83–90.
7. Catherino WH, Segars JH. Microarray analysis in leiomyomas: whichgene list is the correct list? Fertil Steril 2003;80:293–4.
8. Okamoto O, Fujiwara S, Abe M, Sato Y. Dermatopontin interacts withtransforming growth factor beta and enhances its biological activity.Biochem J 1999;337:537–41.
9. Tsibris JCM, Segars JH, Coppola D, Mane S, Wilbanks GD, O’BrienWF, et al. Insights from gene arrays on the development and growthregulation of uterine leiomyomas. Fertil Steril 2002;78:114–21.
0. Malik M, Mayers C, Leppert PC, Segars J, Catherino WH. Molecularalterations in retinoic pathway of uterine leiomyomas. Presented atAdvances in Leiomyoma Research: 2nd NIH International Congress.National Institutes of Health, Bethesda, MD, February 24–25, 2005.
1. Pfaffl MW. A new mathematical model for relative quantification inreal-time RT-PCR. Nucleic Acids Res 2001;29:e45.
2. Tsibris JC, Porter KB, Jazayeri A, Tzimas G, Nau H, Huang H, et al.Human uterine leiomyomata express higher levels of peroxisome pro-liferator-activated receptor gamma, retinoid X receptor alpha, and all-trans retinoic acid than myometrium. Cancer Res 1999;59:5737–44.
3. Loy CJ, Evelyn S, Lim FK, Liu MH, Yong EL. Growth dynamics ofhuman leiomyoma cells and inhibitory effects of the peroxisomeproliferator-activated receptor-gamma ligand, pioglitazone. Mol
Hum Reprod 2005;11:561– 6.cultures Vol. 87, No. 5, May 2007

Esw3ltl
mtpiemu
RP
R
0d
Effect of endometrioma cyst fluid exposure onperitoneal adhesion formation in a rabbit modelLaura Proud Smith, M.D.,a Christopher D. Williams, M.D.,b Joseph O’Brien Doyle, M.D.,a
Wendy B. Closshey, M.D.,a William K. Brix, M.D.,c and Lisa M. Pastore, Ph.D.a
Departments of a Obstetrics and Gynecology, b Obstetrics and Gynecology, Division of Reproductive Endocrinology andInfertility, and c Pathology, University of Virginia Health System, Charlottesville, Virginia
Objective: To determine whether copious lavage and suction of human endometrioma fluid placed in theperitoneal cavity of rabbits reduces adhesion formation compared to no lavage.Design: Prospective, randomized, blinded study.Setting: Academic research environment.Animal(s): Twenty-four female New Zealand white rabbits.Intervention(s): Rabbits randomized into three groups: [1] laparoscopy with instillation of human endometriomamaterial, no lavage; [2] laparoscopy with instillation of human endometrioma material, followed by clearance ofall visible endometrioma fluid by saline lavage and suction; [3] laparoscopy alone.Main Outcome Measure(s): Six weeks after laparoscopy, adhesions scored by laparotomy using standard visualassessment scoring system and histologic microscopic evaluation. Data evaluated using Kruskal-Wallis andmedian nonparametric tests.Result(s): For groups 1, 2, and 3, respectively, mean total clinical adhesion scores were 0.67 (95% confidenceinterval [CI] �0.87, 2.2), 3.67 (95% CI 1.27, 6.07), and 0 (95% CI 0, 0). Group 2 had statistically significantlyhigher mean adhesion scores compared to group 1. Histologic adhesion scores followed the trend of clinicaladhesion scores.Conclusion(s): In this rabbit model, human endometrioma fluid exposure in the peritoneal cavity is not associatedwith adhesion formation. Instillation of endometrioma fluid followed by copious saline lavage is stronglyassociated with adhesion formation. (Fertil Steril� 2007;87:1173–9. ©2007 by American Society for Reproduc-tive Medicine.)
Key Words: Adhesion, endometrioma, rabbit model, lavage
m(pscrrd
pttpsfeded
MSA
ndometriosis, a disease involving ectopic endometrial tis-ue, is widely prevalent, affecting 4%–44% of asymptomaticomen, 40%–60% of women with dysmenorrhea, and 20%–0% of subfertile women (1–3). Endometriomas, cystic col-ections of endometriosis of the ovary, occur in 17%–44% ofhose with endometriosis (1, 3). These cysts can becomearge and painful, requiring surgical management.
Multiple surgical techniques are used to treat endometrio-as. A common element to these approaches involves inten-
ional cyst rupture, spillage of the contents of the cyst into theelvic cavity, removal of the cyst wall, followed by aggressiverrigation and suction (4, 5). Laparoscopic cystectomy is anffective and widely used surgical technique for treating endo-etriomas, with 92% of patients with endometriomas who
ndergo the procedure showing no evidence of ovarian endo-
eceived November 16, 2005; revised and accepted August 11, 2006.resent addresses: Dr. Joseph O’Brien Doyle, Brigham and Women’sHospital, Department of Obstetrics and Gynecology, Boston, Massa-chusetts; and Dr. Wendy B. Closshey, University of San Francisco,Department of Obstetrics and Gynecology, Division of ReproductiveEndocrinology and Infertility, San Francisco, California.
eprint requests: Christopher D. Williams, M.D., Reproductive Medicineand Surgery Center of Virginia, Martha Jefferson Outpatient Care Cen-ter, 595 Peter Jefferson Parkway, Suite 390, Charlottesville, VA 22911
a(FAX: 434-982-8521; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.08.104 Copyright ©2007 American Soc
etrioma on second-look laparoscopy within 3–6 months1, 6). Although no statistically significant difference in com-lications or recurrence rate is evident, cystectomy has beenhown to have superior outcomes relative to drainage andoagulation for pain relief, cumulative postoperative pregnancyates (PR), and the disease-free interval (7). The recurrence rate,egardless of surgical technique, appears to correlate with theuration of follow-up (8).
Rupture of the cyst with spillage of the contents into theelvic cavity is contrary to the management of some otherypes of ovarian cysts. For instance, avoidance of cyst rup-ure during resection of mature teratomas is considered im-ortant (9). The perception is that copious irrigation anduction of released endometrioma contents reduces adhesionormation; however, there is a paucity of clinical literature tovaluate this assumption. The goal of this study was toetermine whether copious lavage and suction of humanndometrioma fluid in the peritoneal cavity of rabbits re-uces adhesion formation compared to no lavage.
ATERIALS AND METHODSubjects and Study Designpproval for the study was obtained from the Animal Care
nd Use Committee and the Institutional Review Board
1173Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

(foIamw(
glt[eesoherssgtF
bte2cstdt
wHBadarshaisosTtias
(wesahfltcla6sumassocwrpr0
sluramnsWtscFab
HAmufldhicrot
IRB) at the University of Virginia Health System. Twenty-our sexually mature female New Zealand white rabbits werebtained from a commercial source (Burleson Enterprises,nc., Unionville, VA) and were observed for 8 days tossess general health status before experimentation. Ani-al weights ranged from 3,500 to 5,500 g. The animalsere maintained on Teklad Global High Fiber Rabbit Diet
Harlan, Madison, WI) and water ad libitum.
The rabbits were randomized into three experimentalroups. The three experimental groups underwent the fol-owing procedures: [1] laparoscopy with pelvic instilla-ion of 2 mL of human endometrioma material, no lavage;2] laparoscopy with pelvic instillation of 2 mL of humanndometrioma material, followed by clearance of all visiblendometrioma fluid with copious normal saline lavage anduction; [3] laparoscopy without instillation of endometri-ma material or lavage (surgical control). For our results toave 90% confidence and 80% power in detecting differ-nces by treatment group, we determined the need for nineabbits in group 1, nine in group 2, and six in group 3. Thisample size was based on the assumption of an adhesioncore of 1.0 for group 2 and an adhesion score of 3.6 forroup 1 on a subscale that ranged up to 4.0. These assump-ions were based on the adhesion results demonstrated byiedler et al. (10) and our a priori judgment.
An ear tag bearing a unique four-digit identification num-er was placed on each animal by the supplier. These iden-ification numbers were used throughout the study to identifyach animal. The initial surgery was performed during a-day period. On the day of the surgery, the animal careoordinator, who was not involved in the surgery or adhesioncoring, randomly selected rabbits to be assigned to the threereatment arms. Each animal’s ear tag was covered beforeelivery of the animal to the surgeons, effectively blindinghem to the animal’s identity during surgery.
Laparoscopies were performed under sterile conditionsith 2 mL of ketamine (100 mg/mL; Fort Dodge Animalealth, Fort Dodge, IA) and 1 mL of xylazine (20 mg/mL;urns Veterinary Supply, Inc., Westbury, NY) anesthesiadministered IM. Rabbits were masked with 100% oxygenuring the procedure to avoid hypoxia and hypercapnia, andnesthesia was maintained with isofluorane to effect. Eachabbit received 1 mL of enrofloxacin (Bayer, Shawnee Mis-ion, KS) as antibiotic prophylaxis before the surgery. Theair over the abdomen was shaved and the skin prepared forn aseptic procedure by three alternating scrubs of providoneodine and 70% alcohol. Either a 10-mm or 5-mm laparo-cope with an attached videoscopic camera setup was usedn an alternating basis from one rabbit to the next to expediteurgical turn-around time while equipment was sterilized.he laparoscope was introduced into the upper abdomen
hrough an open technique. Manual elevation of the abdom-nal wall allowed adequate visual inspection of the entirebdominal cavity to confirm normal anatomy and the ab-
ence of adhesions. a1174 Smith et al. Endometrioma cyst fluid and adhesions
A 60-mL container of refrigerated endometrioma materialsee section on Human Endometrioma Cyst Fluid) wasarmed to room temperature. In groups 1 and 2, 2 mL of
ndometrial material were instilled using a 6-mL syringe,uch that the rabbits were exposed to a weight-adjustedmount of endometrial tissue grossly equivalent to potentialuman exposure. The capped container of endometriomauid was mixed before aspiration into the syringe to ensure
hat all aliquots injected would be expected to have identicalontents. The syringe was introduced through the suprapubicaparoscopic port and directed toward the pelvis. For thenimals that received normal saline irrigation (group 2), a0-mL syringe was introduced through the same laparo-copic port to perform repeated lavage using normal salinentil there was no visual evidence of residual endometriomaaterial on laparoscopy. Each animal in group 2 underwenttotal of 10 rounds of normal saline lavage. The force of
uction lavage used on each animal was kept constant by aingle surgeon doing the lavage on every animal and the timef evacuation of each 60-mL syringe was likewise keptonstant. After the procedure, the peritoneum and fasciaere reapproximated with 3-0 polyglactin 910 sutures in a
unning full-thickness stitch. The skin was closed with 4-0olyglactin 910 sutures (Ethicon Inc., Cornelia, GA) in aunning subcuticular stitch with a buried knot. Bupivicaine.25% was injected locally for postoperative analgesia.
After the animals were maintained for 6.5 weeks undertandard husbandry conditions, each animal underwent aaparotomy for adhesion scoring. The order of the rabbitsndergoing surgery was randomly selected, and surgeonsemained blinded to the treatment group. Animals werenesthetized with 1.5 mL of ketamine (100 mg/mL) and 1.5L of xylazine (100 mg/mL) administered IM and eutha-
ized by lethal intracardiac injection with 2 mL of Euthana-ia Solution (5 g/mL, 1 mL/10 lbs; Virbac AH Inc., Fort
orth, TX), per standard rabbit euthanasia protocol. Duringhe laparotomy, the clinical appearance of the pelvis wascored by three investigators (L.P.S., C.D.W., J.O.D.) ac-ording to the standard visual assessment scoring system ofiedler et al. (10). Biopsies were taken from representativereas on the ovary, uterine horn, peritoneal sidewall, andladder of each animal and preserved in formalin.
uman Endometrioma Cyst Fluidpproval was obtained from the Human Investigation Com-ittee at the University of Virginia Health System for the
se of human endometrioma cyst fluid. Endometrioma cystuid was collected in the operating room under sterile con-itions from a single large endometrioma from an intactuman pathological specimen. A single human female gavenformed consent and served as the source of all pathologi-ally confirmed endometrioma cyst fluid. At the time of aoutine laparoscopy for the excision of a large endometri-ma, endometrioma cyst fluid was aspirated directly fromhe cyst cavity. The contents of the cyst were drained into
sterile container approved by the Institutional BiosafetyVol. 87, No. 5, May 2007

Cist
AAeisteTt
HAsia(twtpifi
afipnflfism�fmsgwa
STswwrlwI
F
ommittee. The container of endometrioma cyst fluid wasmmediately stored at minus 80°C until surgery. Strictterile technique was maintained during the handling ofhe material.
dhesion Scoringn abdominal laparotomy was carried out on each animal to
valuate and score adhesion formation according to the scor-ng system in Table 1, as used by Fiedler et al. (10). Theame three surgeons performed the laparotomy and dissec-ion on each animal and the surgeons remained blinded toach animal’s assigned group (L.P.S., C.D.W., J.O.D.).hese three investigators jointly scored the adhesions. Pho-
ographs were taken of the peritoneal cavity of each rabbit.
istologic Evaluation of Rabbit Biopsiesfter laparotomy and clinical assessment of adhesion
cores, representative biopsies were taken from each an-mal, fixed in 10% buffered formalin, embedded in par-ffin, cut at 4 �m, and stained with hematoxylin and eosinH & E). Biopsies were taken from representative areas onhe ovary, uterine horn, fallopian tubes, abdominal side-all, and bladder. The slides were reviewed by two pa-
hologists (K.A. and W.B.) who were blinded to therocedure. All cases were assessed for acute and chronicnflammation, abscess formation, granulation tissue, and
TABLE 1Criteria for clinical scoring of adhesions.
Category
Extent No intraabdominal adh�25% of abdomen inv�50% of abdomen inv�75% of abdomen inv�75% of abdomen inv
Type No adhesionsFilmy, transparent, avaOpaque, translucent, aOpaque, capillaries prOpaque, larger vessels
Tenacity No adhesionsAdhesions essentiallyAdhesions lysed withAdhesions require sha
Inflammation NoneMild erythema, localizeModerate erythema anSevere erythema andSevere erythema and
Maximum total scoreSmith. Endometrioma cyst fluid and adhesions. Fertil Steril 2007.
brosis. The histologic scoring system used by Fiedler et a
ertility and Sterility�
l. (10) was used. Acute inflammation was graded on aour-point scale: 0 � inflammation absent; 1 � focal–mildnflammation with scattered, fewer than 10 neutrophils�er �400 field; 2 � moderate inflammation with 10 –100eutrophils per �400 field; 3 � widespread–severe in-ammation with greater than 100 neutrophils per �400eld. Chronic inflammation was graded on a four-pointcale: 0 � inflammation absent; 1 � focal mild inflam-ation with scattered lymphocyte and plasma cells per400 field; 2 � moderate inflammation with less than 5
ollicles per �400 field; 3 � widespread–severe inflam-ation with greater than 5 follicles per �400 field. Ab-
cess formation, granulation tissue, and fibrosis wereraded as present or absent. The scores in each categoryere added for each animal and a final histologic score
ssigned to each rabbit.
tatistical Analysishe mean, 95% confidence interval around the mean,tandard error, and median total adhesion scores by groupere calculated. The groups were then further analyzedith the Kruskal-Wallis one-way analysis of variance by
anks, the median test, and �2 analysis with P values ofess than .05 showing statistical significance. All analysesere done using SPSS version 11 (SPSS, Inc., Chicago,
L). These nonparametric tests were selected as appropri-
escription Score
ns 0d 1d 2d 3d 4
0lar 1cular 2t 3sent 4
0part 1ion 2issection 3
0urface involvement 1dema, localized surface involvement 2
a, localized surface involvement 3a, widespread surface involvement 4
15
D
esioolveolveolveolve
scuvas
esenpre
fall atractrp d
d sd e
edemedem
te because of the small sample size.
1175

RActsfntI
Tsm
(iwscdic
shT(awmmis
DTotibsathuod
itp
ESULTSll 24 animals survived the surgery. There were no surgical
omplications, significant postoperative morbidity or mor-ality before euthanasia. One rabbit experienced two epi-odes of diarrhea 2 days postoperatively and stool was sentor bacterial culture and parasites, both of which returnedegative. This rabbit received 5 days of empiric sulfame-hoxazole and trimethoprim (15 mg/kg; Alpharma USPDnc., Baltimore, MD), and the diarrhea resolved.
The mean and median clinical adhesion scores are shown inable 2 as well as in Figure 1. The mean adhesion scores wereignificantly higher in group 2 than group 1 (P�.027). Theean adhesion scores were lower in group 3 than group 1
TABLE 2Comparison of group means for clinical adhesio
Group 1 (n � 9)a
Mean (95% CI) 0.67 (�0.87, 2.2)Median 0Standard error 0.667P valued .027 (1 vs. 2)a Laparoscopy and endometrioma fluid instillation.b Laparoscopy, endometrioma fluid, and lavage.c Laparoscopy alone.d Data evaluated with Kruskal-Wallis one-way analysis of
Smith. Endometrioma cyst fluid and adhesions. Fertil Steril 2007.
FIGURE 1
Total clinical adhesion scores. Quantitativeanalysis of adhesions using system shown inTable 1. Results are given for each animal withanimals divided by group: group 1: laparoscopyand endometrioma fluid instillation; group 2:laparoscopy, endometrioma fluid instillation, andsaline lavage; group 3: laparoscopy alone.
oSmith. Endometrioma cyst fluid and adhesions. Fertil Steril 2007.
1176 Smith et al. Endometrioma cyst fluid and adhesions
P�.414). The mean adhesion scores were significantly lowern group 3 than group 2 (P�.017). The animals in group 3ere found to have no visible adhesions. The clinical adhe-
ion score of rabbit 2 in group 2 was statistically signifi-antly higher than that of any other animal in the groupespite rigid consistency in amount of endometrioma fluidnstilled and no difference in the content of endometriomayst fluid between animals.
Histologic scores are shown in Table 3. The total histologiccores were higher in group 2 than group 1 (P�.19). The totalistologic scores were lower in group 3 than group 1 (P�.11).he total histologic scores were lower in group 3 than group 2
P�.61). The fallopian tubes, ovaries, and tissues of thebdominal sidewall (skeletal muscle and the associated fat)ere the sites most commonly affected by the procedure. Theost common finding was a mild-to-moderate chronic inflam-ation. The histologic results follow the trend demonstrated
n the clinical scoring of adhesions, but are not of statisticalignificance.
ISCUSSIONhe most common surgical technique for treating endometri-mas involves intentional rupture and spillage of the con-ents of the cyst into the pelvic cavity followed by extensiverrigation and suction (7, 11). In humans, the perception haseen that copious irrigation and suction of the pelvis afterpillage of endometrioma contents intraperitoneally reducesdhesion formation. However, there is a lack of evidence inhe medical literature to support this assumption. No studyas used an animal or human model to prospectively eval-ate whether avoiding intraperitoneal spillage of endometri-ma fluid or thorough lavage of endometrioma spillage re-uces postoperative adhesion formation.
A human study comparing adhesions and peritonealmplants of endometriosis before and after laparoscopicreatment of endometriomas showed that most new im-lants on second-look were on the pelvic floor as a result
ores.
Group 2 (n � 9)b Group 3 (n � 6)c
3.67 (1.27, 6.07) 0 (0, 0)4 01.041 0
.017 (3 vs. 2) .414 (3 vs. 1)
nce.
n sc
varia
f “chocolate-like material that could not be aspirated.”
Vol. 87, No. 5, May 2007

Amc
ablbbhsidasseti
oadtsiaitsdcc
sr
cfleflsgflTbmsh
phsh
ssttsatndcadaasdc
F
dhesions were more frequent and extensive in the endo-etrioma excision group on second-look compared to the
ontrol group (5).
In our study, rabbits were chosen as the study animal tovoid repeating baseline experimentation. One group of rab-its was used to control for inflammatory consequences ofaparoscopy alone. A normal saline lavage control was notelieved to be necessary because normal saline lavage haseen demonstrated not to be associated with either clinical oristologic adhesion formation in a rabbit model (10). Thistudy attempts to replicate the method of saline lavage donen the study by Fiedler et al. (10), but there were someifferences in the techniques. In the Fiedler study, the lavagelone group was exposed to 10 rounds of 100 mL of normalaline lavage for a total of 1 L of irrigation through a Corsonuction irrigator. The present study used a 60-mL syringe toxpose animals to 10 rounds of normal saline irrigation for aotal of 600 mL of lavage and we did not use a formal suctionrrigator due to equipment malfunction.
This difference is important because the smaller volumef irrigant used in the present study could potentially havellowed for residual endometrioma fluid. However, no en-ometrioma fluid was visible laparoscopically at the end ofhe procedure, the same standard that is currently used in theurgical treatment of endometriomas in humans. The type ofrrigator may also have affected the formation of adhesionsnd it may be that the commercial laparoscopic suctionrrigator used by Fiedler et al. created more force and morehoroughly rinsed endometrioma fluid than the hand-heldyringe technique used in the present study. We proceededespite the differences in suction irrigation technique be-ause normal saline lavage had not been shown to be asso-iated with adhesions in the Fiedler animal model.
The results of the study were unexpected. The currenturgical management of endometriomas in humans involves
TABLE 3Comparison of group means for histologic adhes
Histologic category Group 1 (n � 9)a
Acute inflammation 0.07 � 0.07Chronic inflammation 0.36 � 0.13Abscess 0Granulation 0Fibrosis 0.21 � 0.16Total histologic score 1.00 � 0.37P valued .19 (1 vs. 2)a Laparoscopy and endometrioma fluid instillation.b Laparoscopy, endometrioma fluid instillation, and lavagec Laparoscopy alone.d Data evaluated with Kruskal-Wallis one-way analysis of
Smith. Endometrioma cyst fluid and adhesions. Fertil Steril 2007.
upture with spillage of endometrioma fluid, followed by n
ertility and Sterility�
opious saline irrigation and aspiration to remove all visibleuid. In line with current practice, we hypothesized that thexperimental group without copious lavage of endometriomauid (group 1) would have the highest mean clinical adhe-ion scores. To the contrary, this study demonstrates that theroup with copious normal saline lavage of endometriomauid (group 2) had significantly more clinical adhesions.hese results were entirely unexpected as saline lavage haseen previously shown to decrease peritoneal adhesion for-ation in both animal and human studies evaluating adhe-
ion formation and histologic evidence of inflammation afteruman dermoid fluid spillage (10, 12–14).
The histologic adhesion scores follow a trend that sup-orts the clinical adhesion scores. The differences betweenistologic scores are not statistically significant, but thetudy was not powered to see differences by tissue or byistologic category.
A possible explanation for the higher mean clinical adhe-ion scores in the lavage group is that the saline lavage itselferved to spread the endometrioma fluid more effectively inhe abdominal cavity, thereby increasing the distribution ofissue contact and potential for adhesions compared to localpill. This does not reconcile why more extensive localizeddhesions were not present in group 1. Another possibility ishat the process of lavage mechanically irritates the perito-eal cavity and thereby causes adhesions by local tissueamage by the suction instrument. This seems unlikely be-ause data by Fiedler et al. (10) in a rabbit model evaluatingdhesion formation after peritoneal instillation of humanermoid material found no clinical or histologic evidence ofdhesion formation in their group evaluating saline lavagelone. Interestingly, Fiedler et al. (10) state that “sometatistical comparisons suggested that saline lavage afterermoid exposure resulted in higher adhesion scores thanontrol conditions,” although overall their data indicate that
scores.
Group 2 (n � 9)b Group 3 (n � 6)c
0.24 � 0.14 0.17 � 0.171.00 � 0.27 0
0 0.33 � 0.210.12 � 0.12 00.12 � 0.08 0.17 � 0.172.89 � 1.09 0.67 � 0.33.11 (3 vs. 2) .61 (3 vs. 1)
nce.
ion
.
varia
ormal saline lavage of dermoid cyst contents in the perito-
1177

nn
hharcoTiaBlmp(elcsmbtod
mhn(asrimTdwWitc
hnbslflohfwt
tipfmamaatav
imfortoaspceamcf
omorcrpoFaao
AeWSS
R
eal cavity reduces inflammation and adhesion formation toear control levels.
A separate concern is that although normal saline lavageas been shown to have no association with either clinical oristologic adhesion formation in a rabbit model, this baselinessumption may not be correct (10). Review of the literatureeveals few prospective studies with divergent results thatompare normal saline lavage to lactated Ringer’s solutionr other crystalloid, and associated adhesion formation.here is a body of literature asserting that normal saline
rrigation in rats does not cause peritoneal inflammation ordhesions compared with a variety of other irrigants (15–17).ut there is also evidence that peritoneal irrigation with
actated Ringer’s solution is superior to irrigation with nor-al saline and that lactated Ringer’s solution irrigation is
rotective against adhesions in both rat and rabbit models18, 19). Furthermore, van Westreenen et al. (20) foundnhanced peritoneal adhesion formation (P�.0001) in ratsavaged with all solutions tested, including normal saline,ompared to a surgical control. Close evaluation of theurgical methods described in many articles on the surgicalanagement of ovarian endometriomas in humans exposes
oth the inconsistency in irrigation solutions used as well ashe frequent complete absence of description of the mannerr degree of irrigation other than simply that lavage wasone (3–6, 11).
Other limitations include that the use of a rabbit modelay not offer data that extrapolates to humans. Given that
uman endometrioma fluid is foreign to the rabbit, the xe-ographic rejection phenomenon is a concern. Fiedler et al.10) addressed this concern in a rabbit model evaluatingdhesion formation after human dermoid tumor spillage by atudy arm instilling human follicular fluid (FF) into theabbit peritoneum as an antigenic control. The animals usedn that study demonstrated no histologic evidence of inflam-ation or adhesions in those exposed to the human FF.hose animals who received intraperitoneal instillation ofermoid material survived the instillation of this materialithout evidence of organ failure, fevers, or other morbidity.e anticipated that instillation of human endometrioma fluid
nto the rabbit peritoneum would have less antigenicity thanhat of the dermoid tumor, which contains many more humanell types.
In our study, none of the rabbits experienced adverseealth effects attributable to the endometrioma fluid andone demonstrated evidence of tissue rejection. It is possi-le, however, that rabbits do not mount an immune re-ponse against the cells in human endometrioma fluid. Aack of immune response would explain the lack of in-ammation and adhesions in the group with endometri-ma fluid without lavage. Similarly, the use of a singleuman source of the endometrioma fluid may have af-ected the antigenicity of the endometrioma fluid if thereere individual variability in the content of the cyst and
he amount of inflammatory factors. It may not be the case
1178 Smith et al. Endometrioma cyst fluid and adhesions
hat all human endometrioma fluid is equal in its ability toncite an inflammatory reaction in the rabbit. We were pur-oseful in our decision to use a single large endometriomarom a single human source for all endometrioma fluid toaintain constancy in this variable across the groups. It is
lso important to note that the capped container of endo-etrioma fluid was mixed before aspiration into the syringe
nd instillation into the animals studied to ensure that allliquots injected would be expected to have identical con-ents. Further investigation into the variability of cellularctivity in human endometrioma fluid would, however, bealuable.
Although this study is subject to limitations, it raises anmportant question: what if irrigation and suction of endo-etrioma cyst contents did prove to cause greater adhesion
ormation in humans? It is technically possible to minimizer avoid spillage of endometrioma contents during surgicalesection and thereby avoid the need for irrigation and suc-ion. Use of careful dissection, aspiration of the endometri-ma fluid before rupture, or a sterile bag collection device tovoid spillage of the endometrioma fluid are possible sub-titute techniques to the currently accepted surgical ap-roach. One must consider the surgical context when dis-ussing practice changes, and it is critical to recall thatndometriomas in humans are often associated with pelvicdhesions even before surgical therapy, therefore any animalodel must be followed by human investigation before
hanging surgical technique. In light of these possibilities,urther studies are important.
This study demonstrates that release of human endometri-ma fluid alone into the peritoneal cavity of rabbits causedinimal adhesion formation. Release of human endometri-
ma fluid followed by copious normal saline lavage withemoval of all visible endometrioma fluid caused signifi-antly higher mean adhesion scores. The reasons for theseesults are unclear. The study raises the concern thatresent surgical techniques in the treatment of endometri-mas causes increased peritoneal adhesion formation.urther investigation of the abdominal and peritonealdhesive effects of endometrioma fluid are needed tossure that the present surgical management of endometri-mas in humans is optimal.
cknowledgments: The authors are grateful to Patricia Foley for her vet-rinarian assistance and to Gina Wimer for her expertise with animal care.e thank Laurel Rice for the use of her laboratory facilities. We thank Tyler
hackelford for assistance with laparoscopic equipment. We thank Philipmith for editorial review.
EFERENCES1. Busacca M, Vignali M. Ovarian endometriosis: from pathogenesis to
surgical treatment. Curr Opin Obst Gynecol 2003;15:321–6.2. Rawson, JM. Prevalence of endometriosis in asymptomatic women.
J Repro Med 1991;37:513–5.3. Exacoustos C, Zupi E, Amadio A, Szabolcs B, De Vivo B, Marconi D,
et al. Laparoscopic removal of endometriomas: sonographic evaluationof residual functioning ovarian tissue. Am J Obstet Gynecol 2004;191:
68–72.Vol. 87, No. 5, May 2007

1
1
1
1
1
1
1
1
1
1
2
F
4. Donnez J, Smets M, Jadoul P, Pirard C, Squifflet J. Laparoscopicmanagement of peritoneal endometriosis, endometriotic cysts, and rec-tovaginal adenomyosis. Ann NY Acad Sci 2003;997:274–81.
5. Fayez JA, Vogel MF. Comparison of different treatment methods ofendometriomas by laparoscopy. Obstet Gynecol 1991;78:660–5.
6. Canis M, Mage G, Wattiez A, Chapron C, Pouly JL, Bassil S. Second-look laparoscopy after laparoscopic cystectomy of large ovarian endo-metriomas. Fertil Steril 1992;58:617–9.
7. Beretta P, Franchi M, Ghezzi F, Busacca M, Zupi E, Bolis P. Randomizedclinical trial of two laparoscopic treatments of endometriomas: cystectomyversus drainage and coagulation. Fertil Steril 1998;70:1176–80.
8. Busacca M, Marana R, Caruana P, Candiani M, Muzii L, Calia C, et al.Recurrence of ovarian endometrioma after laparoscopic excision. Am JObstet Gynecol 1999;180:519–23.
9. Pantoja E, Noy MA, Axtmayer RW, Colon FE, Pelegrina I. Ovariandermoids and their complications. Comprehensive historical review.Obstet Gynecol Surv 1975;30:1–20.
0. Fiedler EP, Guzick DS, Guido R, Kanbour-Shakir A, Krasnow JS.Adhesion formation from release of dermoid contents in the peritonealcavity and effect of copious lavage: a prospective, randomized, blinded,controlled study in a rabbit model. Fertil Steril 1996;65:852–9.
1. Chapron, C, Vercellini P, Barakat H, Vieira M, Dubuisson J-B. Man-agement of ovarian endometriomas. Hum Repro Update 2002;8:591–7.
2. Campo S, Garcea N. Laparoscopic conservative excision of ovariandermoid cysts with and without an endobag. J Am Assoc Gynecol
Laparosc 1998;5:165–70.ertility and Sterility�
3. Hessami SH, Kohanim B, Grazi RV. Laparoscopic excision of benigndermoid cysts with controlled intraoperative spillage. J Am AssocGynecol Laparosc 1995;2:479–81.
4. Milad MP, Olson E. Factors that increase the risk of leakage duringsurgical removal of benign cystic teratomas. Hum Repro 1999;14:2264–7.
5. Larsson B, Perbeck L. The possible advantage of keeping the uterineand intestinal serosa irrigated with saline to prevent intraabdominaladhesions in operations for fertility. An experimental study in rats. ActaChirurg Scand 1986:15–8.
6. Roberts LM, Sanfilippo JS, Raab S. Effects of laparoscopic lavageon adhesion formation and peritoneum in an animal model of pel-vic inflammatory disease. J Am Assoc Gynecol Laparosc 2002;9:503–7.
7. Al-Took S, Murray C, Tulandi T. Effects of pirfenidone and dermoidcyst fluid on adhesion formation. Fertil Steril 1998;69:341–3.
8. Sahakian V, Rogers RG, Halme J, Hulka J. Effects of carbon dioxide-saturated normal saline and Ringer’s lactate on postsurgical adhesionformation in the rabbit. Obstet Gynecol 1993;82:851–3.
9. Pagidas K, Tulandi T. Effects of Ringer’s lactate, Interceed (TC7) andGore-Tex Surgical Membrane on postsurgical adhesion formation. Fer-til Steril 1992;57:199–201.
0. van Westreenen M, van den Tol PM, Pronk A, Marquet RL, Jeekel J,Leguit P. Perioperative lavage promotes intraperitoneal adhesion in the
rat. Eur Surg Res 1999;31:196–201.1179

Esdaslaefsnsm
RS
P
R
Molecular profiling of experimental endometriosisidentified gene expression patterns in common withhuman diseaseIdhaliz Flores, Ph.D.,a Elizabeth Rivera, M.Ed.,a Lynnette A. Ruiz, B.S.,a Olga I. Santiago, B.S.,b
Michael W. Vernon, Ph.D.,c and Caroline B. Appleyard, Ph.D.b
a Department of Microbiology and b Department of Physiology and Pharmacology, Ponce School of Medicine, Ponce,Puerto Rico; and c Department of Obstetrics and Gynecology, Center for Reproductive Medicine, West VirginiaUniversity, Morgantown, West Virginia
Objective: To validate a rat model of endometriosis using complimentary DNA (cDNA) microarrays byidentifying common gene expression patterns between experimental and natural disease.Design: Autotransplantation rat model.Setting: Medical school department.Animals: Female Sprague-Dawley rats.Intervention(s): Endometriosis was surgically induced by suturing uterine horn implants next to the smallintestine’s mesentery. Control rats received sutures with no implants. After 60 days, endometriotic implants anduterine horn were obtained.Main Outcome Measure(s): Gene expression levels determined by cDNA microarrays and real-time quantitativepolymerase chain reaction (qPCR). The Cy5-labeled cDNA was synthesized from total RNA obtained fromendometriotic implants. The Cy3-labeled cDNA was synthesized using uterine RNA from a control rat. Geneexpression levels were analyzed after hybridizing experimental and control labeled cDNA to PIQOR (ParallelIdentification and Quantification of RNAs) Toxicology Rat Microarrays (Miltenyi Biotec, Cologne, Germany)containing 1,252 known genes. The Cy5/Cy3 ratios were determined, and genes with �2-fold higher or �0.5-foldlower expression levels were selected. Microarray results were validated by QRT-PCR.Result(s): We observed differential expression of genes previously shown to be up-regulated in patients,including growth factors, inflammatory cytokines/receptors, tumor invasion/metastasis factors, adhesion mole-cules, and antiapoptotic factors.Conclusion(s): This study presents evidence in support of using this rat model to study the natural history ofendometriosis and to test novel therapeutics for this incurable disease. (Fertil Steril� 2007;87:1180–99. ©2007by American Society for Reproductive Medicine.)
Key Words: Endometriosis, animal model, rat, validation, cDNA microarrays
mto
bmsmaCahmtmepwm
ndometriosis is a gynecological disease associated withevere pelvic pain and infertility, thus affecting the repro-uctive health and quality of life of millions of womenround the world (1). The pathogenesis of endometriosis istill unknown, and the mechanisms whereby endometrioticesions establish, progress, and migrate to extrapelvic sitesre not well understood (2). Human studies are limited bythical and practical considerations including: [1] the needor repeated surgical procedures to monitor disease progres-ion, [2] difficulties in controlling variables (individual ge-etic variation, environment, diet), and [3] difficulties intudying the early steps of disease development. Animalodels of this disease, such as the rat autotransplantation
eceived April 18, 2006; revised and accepted July 23, 2006.upported by S06-GM08239 from the National Institutes of Health, Be-thesda, Maryland (C.B.A. and I.F.).
resented at the Society for the Study of Reproduction Annual Meeting,Quebec, Canada, July 24–27, 2005.
eprint requests: Idhaliz Flores, Ph.D., Department of Microbiology,Ponce School of Medicine, P.O. Box 7004, Ponce, Puerto Rico 00732.
d(FAX: 787-290-0876; E-mail: [email protected]).
1180 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
odel developed by Vernon and Wilson in 1985 (3), wouldherefore offer an invaluable tool for studying the early stepsf disease pathogenesis and testing novel therapeutics.
Despite the clear advantages of using animal models iniomedical research, whether results obtained using experi-ental models of disease could be extrapolated to the human
cenario remains controversial (4–7). Therefore, animalodels need to be carefully evaluated to ensure that they
ccurately represent the disease they are meant to mimic.are must always be taken when making extrapolations fromrat model to the human, especially because the rat does notave spontaneously occurring endometriosis and does notenstruate. However, rats with surgically induced endome-
riosis show similar pathophysiological symptoms as hu-ans with spontaneous endometriosis. The rat ectopic and
utopic endometrium have the same differential secretoryattern of protein synthesis and are histologically similar tohat has been observed in human endometriosis. Further-ore, rats with surgically induced endometriosis show a
ecrease in their fecundity and natural killer cell activity that
0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.07.1550

prmnn
vltteiStrtameode
impmvfaGbcricscm
MTdCH
ASwSraati
fm1weacmgswfirs
booaaacptnfiTwei(a
TTmCcTtDatqe
TRlmeve
F
arallels the human disease (8–11). Moreover, we haveecently shown that, similar to the human disease, this ani-al model is characterized by a dysregulation of the tumor
ecrosis factor (TNF) system systemically and at the perito-eal level (12).
The goal of the present study was to further evaluate thealidity of this animal model by identifying functional bio-ogic categories in common with human disease. We proposehat gene expression profiling and functional characteriza-ion of transcripts that are differentially regulated in thexperimental condition could serve as the basis for validat-ng physiological mechanisms at play in natural disease.uch transcripts may, in turn, represent possible therapeutic
argets for this incurable condition. There have been someeports of gene expression and protein production patternshat are shared by experimental and human disease, but thesere mostly single gene/protein studies. Increasingly, compli-entary (cDNA) microarrays are being used to identify gene
xpression profiles associated with complex genetic diseasesf unknown etiology (13). This powerful technology showsisease-specific patterns in gene expression, thereby accel-rating the identification of candidate genes (14).
To expedite the identification of genes that may play a rolen the establishment, survival, and growth of ectopic endo-etrium, we applied cDNA microarray technology to com-
are gene expression patterns of ectopic and normal endo-etrium in a well-known rat model of endometriosis. To
alidate the cDNA microarray results, selected genes wereurther evaluated by qPCR and gene expression profiles werenalyzed using GoMiner (Genomics and Bioinformaticsroup, National Cancer Institute, Bethesda, MD), a systemsiology data mining tool (15). GoMiner identified signifi-antly enriched gene ontology (GO) categories, and theesults were compared with what has already been reportedn the literature for the human disease, including previousDNA microarray studies on endometriosis (16–22). In thistudy we report the identification of common pathway-spe-ific patterns of gene expression that support the use of thisodel for preclinical drug testing.
ATERIALS AND METHODShe experiments reported herein were performed in accor-ance with the principles described in the “Guide for theare and Use of Laboratory Animals,” National Institutes ofealth Publication No. 86-23.
nimal Model and Collection of Tissuestudies were performed with 15 female Sprague-Dawley ratseighing 275 to 300 g (Southern Veterinary Service, Poncechool of Medicine, PR). All animals were maintained inestricted-access rooms with a controlled temperature (23°C)nd a 12-hour light–dark cycle. Standard laboratory chownd drinking water were provided ad libitum. All experimen-al procedures involving animals were approved by the An-
mal Care and Use Committee at Ponce School of Medicine. certility and Sterility�
Intestinal endometriosis was induced surgically in matureemale rats under pentobarbital anesthesia, based on theethod by Vernon and Wilson (1985) (3). Briefly, the distalcm of the right uterine horn was removed and immersed inarm (37°C) sterile culture medium. The endometrium was
xposed by opening lengthwise with a pair of sterile scissors,nd four pieces of uterine horn measuring 2 � 2 mm wereut. Four implants of uterine tissue were sutured next to theesenteric vessels of the small intestine in the experimental
roup (n � 9). In the control group (n � 6), four silkutures were attached to the mesentery of the intestineithout implants, and the uterine horn was massaged withngertips for 2 minutes. All animals were allowed toecover for 60 days, and were killed with an overdose ofodium pentobarbital.
Vaginal cytologic smears were performed for all ratsefore and after surgical intervention, as well as at the timef death, to monitor their reproductive cyclicity. A laparot-my was performed, and the peritoneal cavity was openednd systematically examined for the presence of implantsnd the original sutures. Peritoneal fluid was asepticallyspirated using a sterile micropipette taking care not toontaminate with blood, a smear with Wright stain wasrepared for quantification of white blood cells (WBCs), andhe remainder was stored at �80°C for RNA analyses. Theumber of WBCs per high-power field was determined inve randomly selected fields as previously described (12).he classification of implants in terms of grades of growthas performed following the criteria described by Ingelmo
t al. (23). Tissue samples (e.g., uterine horn, endometrialmplants) were immediately immersed in RNAlater reagentAmbion, Austin, TX) and stored in tightly closed containerst �80°C.
otal RNA Extraction and Linear Amplificationotal RNA was isolated by standard methods using a com-ercially available RNA isolation kit (Qiagen, Valencia,A). The integrity of the extracted RNA was evaluated withapillary electrophoresis using a Bioanalyzer 2100 (Agilentechnologies, Palo Alto, CA). The RNA quantity was de-
ermined by spectrophotometry at OD260 in a GeneQuantNA/RNA calculator (Pharmacia, Piscataway, NJ). Linear
mplification of RNA was done following a modified pro-ocol of a previously described method (24). The quality anduantity of amplified RNA were determined by capillarylectrophoresis and spectrophotometry as described above.
he cDNA Microarraysat-specific PIQOR Toxicology arrays (Miltenyi Biotec, Co-
ogne, Germany) consisting of 1,252 selected cDNA frag-ents were used to generate gene expression profiles of
ctopic (array 1: a pooled sample of four endometrioticesicles from three rats, one to two vesicles from each) vs.utopic endometrium (array 2: uterine rat tissue from a
ontrol rat). Two micrograms of amplified RNA from eu-1181

trgmld5moMcg
p(2dpvSMSssspc
RTmlfcR(mGsfOAssC(
TcnsRkpf
itafs7dasdww
pHefmtDo
TTmlmdchlltsmiLb
RAAsrrar(vtnAe
opic and ectopic endometrium were reverse transcribed in aeaction containing 8 �l of 5� First Strand Buffer (Invitro-en, Carlsbad, CA), 2 �l Primer Mix (oligo dT and rando-eres, Miltenyi Biotech GmbH, Cologne, Germany), 2 �l
ow cytosine-deoxynucleotides (10 mM dATP, 10 mMGTP, 10 mM dTTP, 4 mM dCTP), 2 �l FluoroLink Cy3/-dCTP (Amersham Pharmacia Biotech, Freiburg, Ger-any), respectively, 4 �l 0.1 M 1,4-dithiothreitol, and 1 �l
f the ribonuclease inhibitor RNasin (20 to 40 U; Promega,adison, WI). Reverse transcription was conducted by in-
ubation with SuperScript II Reverse Transcriptase (Invitro-en, Carlsbad, CA) at 42°C for 30 minutes.
After RNAase H treatment, Cy3- and Cy5-labeled sam-les were combined and purified using Qiaquick columnsQiagen, Valencia, CA). Samples diluted 1:1 in prewarmed� hybridization solution were then subjected to a pre-efined PIQOR rat toxicology microarray. Hybridization andosthybridization washes were performed as described pre-iously (25). Slides were scanned by Miltenyi Biotec on acanArray 4000 Lite scanner (PerkinElmer, Wellesley,A). ImaGene software version 4.1 (BioDiscovery Inc., El
equndo, CA) was used for signal quantification and analy-is as described previously (26). Normalized ratios arehown as Cy5 signal intensity divided by Cy3 signal inten-ity of the respective gene. Microarray experiments wereerformed according to Minimum Information About a Mi-roarray Experiment guidelines (27).
eal-Time RT-PCR Validation of Microarray Datao validate the gene expression data obtained with cDNAicroarrays, real-time RT-PCR was performed on nine se-
ected genes, using total RNA from endometriotic vesiclesrom experimental rats (n � 6) and uterine horn tissues ofontrol animals (n � 5). The six experimental rats used forT-PCR did not overlap with those used for microarrays
n � 3). The five control rats used for the RT-PCR experi-ents did not include the control rat used for microarrays.enes were selected based on level of expression and plau-
ible role in disease etiology, and included PDGRB (2.1-old), LOXL1 (2.1-fold), IL2RG (3.2-fold), BCL2 (9.1-fold),PG (4.8-fold), MMP9 (24.3-fold), TGFB (2.4-fold),PRIL (3.1-fold), and PGH2 (2.2-fold). Primers were de-
igned based on published sequence data using Primer3oftware (Whitehead Institute for Biomedical Research,ambridge, MA) and synthesized by a commercial vendor
IDT DNA Technology, Inc., Coralville, IA).
In brief, total RNA was isolated from tissues using therizol LS reagent (Invitrogen, Carlsbad, CA). To removeontaminating DNA, samples were treated with deoxyribo-uclease I (DNA-free, Ambion, Austin, TX). Reverse tran-cription was performed on the PTC-200 thermalcycler (MJesearch, Waltham, MA) using the iScript cDNA synthesisit (Bio-Rad, Hercules, CA) following the manufacturer’srotocol. After cDNA synthesis, PCR reactions were per-
ormed in triplicate with specific oligo-primer pairs using the w1182 Flores et al. Molecular profiling of rat endometriosis
Q SYBR Green Super Mix kit according to the manufac-urer’s recommendations (Bio-Rad, Hercules, CA). The PCRmplification profile was as follows: 94°C for 4 minutesollowed by 50 cycles of denaturation at 94°C/30 s, gene-pecific annealing temperature/30 sec, and extension at2°C/40 s. Annealing temperatures per primer set wereetermined empirically. A melting curve was generatedfter each run to verify the specificity of the primers,hown by the presence of a single band and no primer-imer artifacts. Real-time analysis of PCR amplificationas performed with an iCycler iQ Optical System soft-are, version 3.0a (Bio-Rad, Hercules, CA).
Relative expression levels were calculated for each sam-le after normalization against the housekeeping genePRT, using the ��Ct method for comparing relative fold-
xpression differences (28). Statistical analysis was per-ormed using unpaired two-tailed t tests to compare relativeessenger RNA expression levels in experimental and con-
rol samples (GraphPad InStat 3; GraphPad software, Saniego, CA). Statistical significance was defined as a P valuef �.05.
he GO Category Analysis of Gene Expression Datao better understand the biologic meaning of the cDNAicroarray results obtained, gene expression data were ana-
yzed using GoMiner, a freely available computer-based dataining tool that automates the functional categorization of
ifferentially expressed genes according to their biologic,ellular, and molecular functions. GoMiner, which uses theierarchical structure of the Gene Ontology program, calcu-ates enrichment or depletion of functional categories (Bio-ogical Process, Cellular Component, and Molecular Func-ion). Potentially important categories are easily identified byorting quantitative and statistical results by either enrich-ent factor or P value. GoMiner allows for bioinformatic
ntegration by providing links to external databases such asocusLink, PubMed, GeneCards, NCBI’s Structure Data-ase, and pathway maps (BioCarta and KEGG).
ESULTSnimal Modelll rats were killed at the same time, exactly 60 days after
urgery. Vaginal cytologic smears were performed for allats before and after the surgical intervention to monitor theireproductive cyclicity. The estrous cycle stage (i.e., estrus,nestrus, proestrus, metestrus) at the time of killing was alsoecorded. Although rats are surgically induced when in estrusor proestrus in some cases), there was a spread among thearious cycle stages within both control and experimental rats athe time of killing; however, there was no statistically sig-ificant difference in the cycle stage between the groups.lso, there was no difference in the body weight between
xperimental and control rats at the time of death.
After the rats were killed, classification of the implants
as performed as described by Ingelmo (23). Briefly, vesi-Vol. 87, No. 5, May 2007

TABLE 1Genes differentially regulated in ectopic and eutopic endometrium of a rat model of endometriosis.
Gene symbol and aliases (byfold-expression) Gene name
Fold-expression % SDa
Previously shown tobe associated with
human endometriosis
MMP12 (HME) Macrophage metalloelastase precursor 70.13 7%MMP9 (CLG4B) 92 KDA type IV collagenase precursor 24.33 22% 46–50OPN (SPP1) Osteopontin (Bone sialoprotein 1) 24.14 3% 51MMP13 Collagenase 3 22.30 74%FABE (FABP5, MAL1, FABPE) Fatty acid–binding protein 14.55 7%CCL3 (SCYA3, MIP1A) Small inducible cytokine A3 (Macrophage
inflammatory protein 1-alpha)13.78 30%
ITGB2 (CD18) Integrin beta-2 (Cell surface adhesionglycoproteins beta-subunit)
13.67 11% 52
CCL9 (SCYA9, MIPG, MRP2) Small inducible cytokine A9 (Macrophageinflammatory protein 1-gamma)
12.35 20%
FABI (FABP2, I-FABP, FABPI) Fatty acid-binding protein, intestinal 10.26 57%LBP Lipopolysaccharide-binding protein 9.99 21%DMBT1 (CRPD, CRP) DMBT1 protein (CRP-Ductin) 9.36 5%BCL2A1 (BFL1) BCL2-related protein A1 (Bfl-1 protein) 9.14 16% 53–55S100A9 (MRP-14, CAGB) Calgranulin B (Migration inhibitory factor-related
protein 14)8.99 21% 56
C3 Complement C3 7.81 35% 18, 57ITGAM (CR3A, CD11B) Integrin alpha-M (Cell surface glycoprotein
MAC-1 alpha subunit)6.88 44%
CD36 (GP4, PAS-4) Platelet glycoprotein IV, CD36 antigen 6.70 14%CTGF (HCS24) Connective tissue growth factor (Hypertrophic
chondrocyte-specific protein 24)6.57 12% 58
ANPEP (PEPN, APN) Aminopeptidase N (Microsomal aminopeptidase) 6.48 5%DUSP1 (MKP1) Dual specificity protein phosphatase 1 (MAP
kinase phosphatase-1)6.38 9% 59
ATF3 Cyclic-AMP-dependent transcription factor(Activating transcription factor 3)
6.33 18%
FGR (SRC2) Proto-oncogene tyrosine-protein kinase 5.94 44%LIPL (LPL, LIPD) Lipoprotein lipase 5.94 6%TNC (HXB, TN) Tenascin (Cytotactin; Hexabrachion; Glioma-
associated extracellular matrix antigen)5.90 14% 60
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.1183Fertility
andSterility�

TABLE 1Continued.
Gene symbol and aliases (byfold-expression) Gene name
Fold-expression % SDa
Previously shown tobe associated with
human endometriosis
ITGB6 (INTEGRINB6) Integrin beta-6 5.61 22% 19, 61, 62CXCR4 C-X-C chemokine receptor type 4 (Stromal cell-
derived factor 1 receptor)5.48 5%
CXCL1 (CINC-1, SCYB1,GRO1)
Cytokine-induced neutrophil chemoattractant(Growth regulated protein; Platelet-derivedgrowth factor- inducuble protein)
5.43 38% 63
CXCL4 (SCYB4, PF4) Chemokine ligand 4 (Platelet factor 4;Oncostatin A)
4.92 8%
MUC1 (PEM, EMA) Mucin 1 (Polymorphic epithelial mucin; Tumor-associated mucin)
4.92 22% 64, 65
CD53 (MOX44, OX-44) Leukocyte surface antigen CD53 (Cell surfaceglycoprotein CD53; Leukocyte antigen MRCOX-44)
4.87 6%
MMP7 (MPSL1, PUMP1) Metalloproteinase-7 (Matrilysin; Uterinemetalloproteinase
4.85 12%
S100A8 (CAGA, MRP-8CFAG)
Calgranulin A (Migration inhibitory factor-relatedprotein 8; Cystic fibrosis antigen)
4.81 18% 56
TNFRSF11B (OPG) Tumor necrosis factor receptor superfamilymember 11B (Osteoprotegerin)
4.81 23% 66
CD3Z (T3Z, TCRZ) T-cell surface glycoprotein CD3 zeta chain (T-cell receptor T3 zeta chain)
4.74 —%
UPA (PLAU) Urokinase-type plasminogen activator 4.71 8% 67, 68CCL4 (SCYA4, MIP1B, ACT-2) Small inducible cytokine 4 (Macrophage
inflammatory protein 1-beta; T-cell activationprotein 2)
4.54 —%
MOA-TF (MITF, MI) Microphthalmia-associated transcription factor(Putative transcription factor mi)
4.42 40%
RAC2 RAS-related C3 (Botulinum toxin substrate 2) 4.31 7%LUMICAN (LUM) Lumican (Keratan sulfate proteoglycan) 4.27 19%CD72 (LY-32, LYB-2, CD72) B-cell differentiation antigen 4.23 —%IL18 (IL18, IGIF, IL-1,
GAMMA)Interleukin-18 (Interferon-gamma inducing factor;
Interleukin-1 gamma)4.15 20% 69
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
1184Flores
etal.M
olecularprofiling
ofratendometriosis
Vol.87,No.5,May
2007

TABLE 1Continued.
Gene symbol and aliases (byfold-expression) Gene name
Fold-expression % SDa
Previously shown tobe associated with
human endometriosis
IL1B Interleukin-1 beta (IL-1 beta; Catabolin) 3.96 20% 70SELPLG (PSGL-1) P-selectin glycoprotein ligand 1 3.93 31%THAS (TBXAS1, CYP5, TXS) Thromboxane-A synthase 3.91 20%THBS1 (TSP1) Thrombospondin 1 3.88 16% 71CYP7B1 Cytochrome p450 7B1 (Oxysterol 7-alpha-
hydroxylase)3.83 27%
LYL1 LYL-1 protein 3.73 63%TEF Thyrotroph embryonic factor 3.67 89%MMP11 (STMY3) Matrix metalloproteinase-11 (Stromelysin-3) 3.66 14%NDRG1 (DRG1) NDRG1 protein (Differentiation-related gene 1
protein)3.60 9%
CD74 (DHLAG) HLA class II histocompatibility antigen, gammachain (HLA-DR antigens associated invariantchain)
3.56 4% 16, 18
ALCAM Activated leukocyte-cell adhesion molecule(CD166 antigen)
3.50 5%
CD79A (IGA) B-cell antigen receptor complex associatedprotein alpha-chain
3.49 12%
JUNB Transcription factor JUN-B 3.48 4%ASC (TMS1, CARD5) Apoptosis-associated speck-like protein (Target
of methylation-induced silencing 1; Caspaserecruitment domain protein 5)
3.46 8%
VAV VAV proto-oncogene 3.46 15%ITGA4 (VLA-4) Integrin alpha-4 (VLA receptor alpha subunit) 3.43 13%FBLN2 Fibulin-2 3.31 13%COL11A1 Collagen alpha 1 (XI) chain 3.28 26% 19,72, 73IL2RG Cytokine receptor common gamma chain
(Interleukin-2 receptor gamma chain)3.18 14% 22
ZF9 (COPEB, BCD1) Core promoter element-binding protein (B-cellderived protein 1; Proto-oncogene BCD1)
3.16 7%
CCR5-CCR2 (CMKBR5) C-C Chemokine receptor type 5 (HIV-1 fusionco-receptor)
3.09 29%
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.1185Fertility
andSterility�

TABLE 1Continued.
Gene symbol and aliases (byfold-expression) Gene name
Fold-expression % SDa
Previously shown tobe associated with
human endometriosis
FIP2 (HYPL) Tumor necrosis factor alpha-inducible cellularprotein containing leucine zipper domains(Huntingtin interacting protein l)
3.09 17%
TNFSF13 (APRIL) Tumor necrosis factor ligand superfamilymember 13 (A Proliferation-Inducing Ligand)
3.08 12%
CXCL13 (BLC, BCA1) B lymphocyte chemoattractant (CXC chemokineBLC; B cell-attracting chemokine 1)
3.07 8% 63, 74
HMOX1 (HO1) Heme oxygenase 1 3.07 19%LCP2 (SLP76) Lymphocyte cytosolic protein 2 (SLP-76 tyrosine
phosphoprotein)3.03 24%
CD37 Leukocyte antigen CD37 3.01 10%FN1 (FN, CIG, MSF) Fibronectin (Cold-insoluble globulin; Migration
stimulating factor)2.93 7%
RBP2 (CRBP2) Retinol-binding protein II, cellular 2.93 43% 75SFA2 (BATF) ATF-like basic leucine zipper transcriptional
factor2.88 15%
GJA1 (CX43) Gap junction alpha-1 protein (Connexin 43) 2.87 11% 76GADD45 (DDIT1) Growth arrest and DNA-damage-inducible
protein (DNA-damage inducible transcript 1)2.79 3% 18
ALDH6 (RALDH3) Aldehyde dehydrogenase 6 (Retinaldehydedehydrogenase 3)
2.76 8%
SOD2 (SOD2, SOD-2) Superoxide dismutase [MN], mitochondrial 2.75 12% 77KAI1 (CD82, SAR2) CD82 antigen (Inducible membrane protein R2) 2.73 9%CCL2 (SCYA2, MCP1) Small inducible cytokine A2 (Monocyte
chemotactic protein 1)2.67 17% 78, 79
(LOX) Lysyloxidase (Protein-lysine 6-oxidase) 2.67 22%CD83 (HB15) CD83 antigen (Cell surfaceglycoprotein; B-cell
activation protein)2.63 7%
CP (CERP) Ceruloplasmin (Ferroxidase) 2.62 18%WNT2 Wnt-2 protein 2.57 11%TIMP1 Metalloproteinase inhibitor 1 (Tissue inhibitor of
metalloproteinases 1)2.55 4% 68, 80
WNT4 (WNT4, WNT-4) Wnt-4 protein 2.50 29%Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
1186Flores
etal.M
olecularprofiling
ofratendometriosis
Vol.87,No.5,May
2007

TABLE 1Continued.
Gene symbol and aliases (byfold-expression) Gene name
Fold-expression % SDa
Previously shown tobe associated with
human endometriosis
BST1 (LY65) ADP-ribosyl cyclase 2 (Cyclic ADP-ribosehydrolase 2)
2.48 10%
AHR (AHR) Aryl hydrocarbon receptor 2.45 17% 81CYP2D1-CYP2D5 Cytochrome p450 2D1 2.45 23%ICAM1 (ICAM1, ICAM-1) Intercellular adhesion molecule 1 2.44 15% 12, 82, 83TGFB1 (TGFB) Transforming growth factor beta 1 2.44 6% 16, 74, 84–86COL15A1 Collagen alpha 1 (XV) chain 2.42 7%TF (TF) Serotransferrin (Transferrin; Siderophilin) 2.40 8% 87, 88PAP3 (REG3G) Pancreatitis-associated protein 3 (REG III-
gamma)2.39 —%
THY1 (CD90) THY-1 membrane glycoprotein (CD90 antigen) 2.39 8%OSF (OSTF1, SH3D3) Osteoclast stimulating factor 1 (SH3 domain
protein 3)2.38 13%
CSF1R (CSFMR or FMS) Macrophage colony stimulating factor I receptor 2.36 12%BTK (ATK, AGMX1, BPK) Tyrosine-protein kinase BTK (Bruton’s tyrosine
kinase)2.35 29%
CDKN1A (CIP1, MDA6) Cyclin-dependent kinase inhibitor 1 (Melanomadifferentiation associated protein 6)
2.30 20%
PTAFR (PAFR) Platelet activating factor receptor 2.29 20%FN1 Fibronectin 2.28 11%BACH1 Basic leucine zipper transcription factor (BTB
and CNC homolog 1)2.26 29%
ERO1L ERO1-like protein alpha (Oxidoreductin 1-lalpha; Endoplasmic oxidoreductin 1-likeprotein)
2.25 17%
IL1R2 (IL1RB) Interleukin-1 receptor, type II 2.25 19% 74, 89CD2 (LFA-2) T-cell surface antigen CD2 precursor
(Lymphocyte function antigen 2)2.24 16%
DEC1 (BHLHB2, SHARP-2,STRA14)
Stimulated by retinoic acid 14 (Basic-helix-loop-helix protein)
2.23 15%
SOX9 Transcription factor Sox-9 2.22 50%TNFSF12 (APO3L, DR3LG,
TWEAK)Tumor necrosis factor ligand superfamily
member 12 (TNF-related weak inducer ofapoptosis)
2.19 225%
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
1187Fertility
andSterility�

TABLE 1Continued.
Gene symbol and aliases (byfold-expression) Gene name
Fold-expression % SDa
Previously shown tobe associated with
human endometriosis
PGH2 (PTGS2, COX2) Prostaglandin G/H synthase 2 (Cyclooxygenase-2)
2.18 26% 20, 21, 90
SOCS3 (CISH3) STAT-induced STAT inhibitor-3 (Cytokineinducible SH2-containing protein 3)
2.16 —%
ABME (APOBEC1, HEPR) Apolipoprotein B mRNA editing protein 2.15 16%INTEGRINB7 (ITGB7) Integrin beta-7 2.15 23%TLR4 (HTOLL) Toll-like receptor 4 2.15 19%SRC (SRC, SRC1) Proto-oncogene tyrosine-protein kinase src 2.12 13%LRP (MVP, LRP) Major vault protein (Lung resistance-related) 2.09 16%LAMB3 Laminin beta-3 chain (Kalinin B1 chain) 2.08 14%C1S Complement Cs component (C1 esterase) 2.07 4% 16, 18FMO5 Flavin-containing monooxygenase 5
(Dimethylaniline oxidase 5)2.06 42%
PDGFRB Beta platelet-derived growth factor receptor(CD140B antigen)
2.06 10% 20, 21
LAMP2 (LAMPB) Lysosome-associated membrane glycoprotein 2(Lysosomal membrane glycoprotein-type B)
2.05 10%
LOXL1 (LOX, RRG) Lysyl oxidase homolog (Lysyl oxidase-likeprotein; RAS excision protein
2.05 28% 22
POLD4 (POLDS) DNA polymerase delta subunit 4 (DNApolymerase delta subunit p12)
2.05 15%
ENO2 Gamma enolase (2-Phospho-D-Glycerate hydro-lyase)
2.04 3%
DCP1 (DCP, ACE) Angiotensin-converting enzyme, somatic isoform(Dipeptidyl carboxypeptidase I)
2.00 17% 91
GLUL (GLNS) Glutamine synthetase (Glutamate–ammonialigase)
2.00 10%
PRKCE (PKCE, NPKC-epsilon) Protein kinase c, epsilon type 2.00 19% 20, 21ERP5 (CABP1, PDIA6) Protein disulfide isomerase A6 (Protein disulfide
isomerase p5)0.50 6%
ILF (ILF1) Interleukin enhancer-binding factor 1 (Cellulartranscription factor ILF-1)
0.50 16%
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
1188Flores
etal.M
olecularprofiling
ofratendometriosis
Vol.87,No.5,May
2007

TABLE 1Continued.
Gene symbol and aliases (byfold-expression) Gene name
Fold-expression % SDa
Previously shown tobe associated with
human endometriosis
PLC (PLC-L) Phospholipase C 0.50 30%POD1 (TCF21) Mesoderm-specific basic-helix-loop-helix protein 0.50 13%SMAD5 (MADH5, SMAD5,
HSMAD5)Mothers against decapentaplegic homolog 5
(Mothers against dpp homolog 5)0.50 20% 92
IL12A (NKSF1) Interleukin-12 alpha chain (Cytotoxic lymphocytematuration factor 35 kda subunit; NK cellstimulatory factor chain 1)
0.49 13% 93
RFC5 (RFC36) Replication factor C, 36Kd subunit (Activator 136Kd subunit; RF-C 36 KDA subunit)
0.49 9%
CPT2 Carnitine o-palmitoyltransferase II, mitochondrial 0.48 12%HJ2 (HJ2, JAGGED2) Notch ligand jagged 2 0.48 —%MMP21-22-23 (MIFR) Matrix metalloproteinase mmp21/22a 23b
(Femalysin)0.48 9%
EBP2 (EBNA1BP2) Probable rRNA processing protein Ebp2 (Ebna1binding protein 2; nucleolar protein p40)
0.48 3%
TM4SF3 (TTSPAN8) Transmembrane 4 superfamily member(Tetraspanin 8; Tumor-associated antigen CO-29)
0.48 7%
ESR1 (ESR, NR3A1) Estrogen receptor (estradiol receptor) 0.47 1% 94, 95HSP40-3 (DNAJB5, HSC40) Dnaj homolog subfamily B member 5 (Heat
shock protein cognate 40)0.47 26% 96, 97
FKBP5 (FKBP54, FF1ANTIGEN)
54 kda Progesterone receptor-associatedimmunophilin (HSP90 binding immunophilin)
0.46 —%
LRRN3 Leucine-rich repeat protein 0.46 14%ACSL3 (ACS2, FACL3) Long-chain-fatty-acid-CoA ligase 3 (Long-chain
acyl-CoA synthetase 3)0.45 5%
IL4R (IL4RA) Interleukin-4 receptor alpha chain (IL-4R-alpha;CD124 antigen)
0.45 7%
TFRC (TFRC) Transferrin receptor protein (CD71 antigen) 0.45 26%THBD (THRM) Thrombomodulin (Fetomodulin) 0.45 11%VGR2 (VEGFR-2, KDR, FLK1) Vascular endothelial growth factor receptor 2
(Kinase insert domain receptor)0.45 —% 12
FMO1 Flavin-containing monooxygenase 1 0.44 13%POLD2 DNA polymerase delta small subunit 0.43 11%Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
1189Fertility
andSterility�

TABLE 1Continued.
Gene symbol and aliases (byfold-expression) Gene name
Fold-expression % SDa
Previously shown tobe associated with
human endometriosis
SULT1A1 (SULT1A1, PST-1) Aryl sulfotransferase (Phenol sulfotransferase;Sulfokinase)
0.43 3%
SYK Tyrosine-protein kinase SYK (Spleen tyrosinekinase)
0.43 8%
ID4 DNA-binding protein inhibitor 0.41 8%BCG1 (JCL-1, MAGED2) Breast cancer associated gene 1 (Melanoma-
associated antigen family D; JCL-1 protein)0.40 12%
IGF1 (IGF-IA, IBP1) Insulin-like growth factor I (Somatomedin) 0.40 4%FKBP14 (FKBP22, PPIase) FK506 binding protein 14, 22Kd (Peptidyl-prolyl
cis-trans isomerase; Rotamase)0.39 27%
FKBP11 (FKBP19, PPIase) FK506 binding protein 11, 19Kd (Peptidyl-prolylcis-trans isomerase; Rotamase)
0.37 8%
FKBP4 (FKBP59, HBI, HSP56) HSP binding immunophilin (Rotamase; FK506binding protein, 52Kd; p59 protein)
0.36 6%
MT1 Metallothionein-I 0.32 4%TRK-B (NTRK2) BDNF/NT-3 growth factors receptor (TRKB
tyrosine kinase)0.31 23% 20, 21, 98
UMAT (ABCB6, MTABC3,ABC7)
ABC-binding cassette (ABC transporter umat;Mitochondrial ABC transporter 3)
0.28 34%
WNT5A Wnt-5a protein 0.26 24% 59EGFR (ERBB1) Epidermal growth factor receptor (Receptor
protein-tyrosine kinase Erbb-1)0.24 38% 99, 100
MT2 Metallothionein-II 0.24 6%FKHL16 (FOXM1, HFH11,
WIN, MPP2)Forkhead protein M1 (Forkhead-related protein
Fkhl16; Hepatocyte nuclear factor 3 forkheadhomolog 11)
0.23 —%
GSTM1 (GST1, GTH4) Glutathione S-transferase Mu 1 (GST class mu;HB subunit 4)
0.23 7% 101
NGFR (TNFRSF16, p75NTR) Low-affinity nerve growth factor receptor (NGFreceptor; Low affinity neurotrophin receptor)
0.19 34%
FUT2 (SEC2) Fucosyltransferase 2 (GDP-l-fucose:beta-D-galactoside 2-alpha-l-fucosyltransferase 2)
0.15 8%
GLI1 Zinc finger protein (Glioma-associatedoncogene)
0.14 20%
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
1190Flores
etal.M
olecularprofiling
ofratendometriosis
Vol.87,No.5,May
2007

cgd4(strc�
AFfupgeshwse
RTRgcchloRcdGswttRafrlsTmeMicAB
LE1
Co
ntin
ued
.
Gen
esy
mb
ola
ndal
iase
s(b
yfo
ld-e
xpre
ssio
n)G
ene
nam
eFo
ld-
exp
ress
ion
%S
Da
Pre
vio
usly
sho
wn
tob
eas
soci
ated
wit
hhu
man
end
om
etri
osi
s
LEFT
Y1-
LEFT
Y2
(TG
F-B
ETA
,E
BA
F,TG
FB4)
Tran
sfor
min
ggr
owth
fact
orb
eta
4(E
ndom
etria
lb
leed
ing-
asso
ciat
edfa
ctor
)0.
1451
%10
2
HS
D11
B2
(HS
D11
K)
Cor
ticos
tero
id11
-bet
a-d
ehyd
roge
nase
,is
ozym
e2
0.05
10%
103
OR
M1
(AG
P1)
Alp
ha-1
-aci
dgl
ycop
rote
in1
(Oro
som
ucoi
d1)
0.03
23%
aP
erce
ntst
and
ard
dev
iatio
n(o
ther
wis
ekn
own
asth
ere
lativ
est
and
ard
dev
iatio
n,R
SD
)is
obta
ined
by
mul
tiply
ing
the
stan
dar
dd
evia
tion
by
100
and
div
idin
gth
isp
rod
uct
by
the
aver
age.
Flo
res.
Mol
ecul
arpr
ofili
ngof
rat
endo
met
rios
is.
Fer
til
Ster
il20
07.
Fertility
les at the suture sites (four sutures per rat) were classified inrades 1 to 4 (1 � no vesicle, 2 � vesicle is �2 mm iniameter, 3 � vesicle is �2 mm but �4.5 mm in diameter,� vesicle is �4.5 mm in diameter). The experimental
implanted) rats (n � 9) developed a vesicle in 67% of theirutures. None of the six control rats developed a vesicle athe site of the suture. The peritoneal fluid of experimentalats had a significantly higher WBC number (48.85 � 12.38ells per high-power field) compared with control rats (8.96
1.92; P�.05).
nalysis of cDNA Microarrayrom the 1,252 genes printed on the microarrays, 123 wereound to be more than twofold overexpressed and 45 werenderexpressed (�0.5-fold) in ectopic endometrium as com-ared with eutopic tissue (Table 1). From this gene list,enes that have been previously associated with humanndometriosis were identified by conducting a comprehen-ive search of the literature using PubMed. Novel genes thatave not been previously associated with human diseaseere also identified; further characterization of such tran-
cripts is expected to result in the generation of new hypoth-ses that would need to be tested.
eal-Time RT-PCR Validation of Microarray Datao validate the microarray data, we conducted real-timeT-PCR quantification of the expression of nine selectedenes in a second set of samples (not included in the mi-roarray experiments). The RNA was extracted from vesi-les obtained from six experimental rats and from uterineorn samples from five control animals. Because of theimited amount of RNA obtained from each vesicle, RNAbtained from two to three vesicles per animal was pooled.elative expression levels of the genes of interest wereompared with those of a reference gene. We tested fourifferent reference genes (HPRT, CYP, �-actin, andAPDH) and found no significant differences in the expres-
ion between groups, i.e., none of the tested reference genesere differentially regulated during the disease process, and
herefore all were valid to normalize the data (29). Arbi-rarily, we selected HPRT as our reference gene for analysis.elative expression levels were calculated for each samplefter normalization against HPRT, using the ��Ct methodor comparing relative fold-expression differences. All PCReactions had efficiencies of over 90%. From the nine se-ected genes, RT-PCR analysis validated the results foreven: PDGFA, LOXL1, IL2RG, BCL2, OPG, MMP9, andGFB. In Figure 1, scatter plots for each gene show theean and individual variation in gene expression levels in
xperimental vs. control rats. For LOXL1, IL2RG, BCL2,MP9, and TGFB, the differences in means between exper-
mental and control groups reached statistical significance. Aomparison between the cDNA microarray and RT-PCR
expression data is shown in Figure 2.
T
1191and Sterility�

FDtflneltlct(citd
DAnimimodisdaesm
unctional Categorization of Microarray Dataata mining using GoMiner identified 58 potentially impor-
ant functional categories based on both a high enrichmentactor and statistical significance (P�0.5). A total of 41 Bio-ogical Process categories (121 genes), eight Cellular Compo-ent categories (113 genes), and nine Molecular Function cat-gories (112 genes) were significantly enriched (Table 2). Theargest group of the functional categories was, as expected,hose related to immune modulation/inflammation. In particu-ar, interleukin 6 biosynthesis and action was one of theategories with the largest enrichment factor value (6.32),ogether with positive regulation of T cell proliferation6.32) and neutrophil chemotaxis (4.74). Other interestingategories that strongly relate to the human condition werentegrin binding (6.32), extracellular matrix (2.56), responseo wounding (2.25), angiogenesis (2.28), and metallopepti-
FIGURE 1
Scatter plots of gene expression levels in experimentUnpaired t tests were conducted to determine signifibetween the groups. Significance was set at P�.05;
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
ase activity (2.95) (Table 3). t
1192 Flores et al. Molecular profiling of rat endometriosis
ISCUSSIONt the present time, the cause of endometriosis and itsatural history are still unknown, treatment options are lim-ted, and there is no cure for this debilitating disease. Animalodels represent an invaluable tool for studying the initiat-
ng events leading to survival and establishment of endo-etriotic implants at ectopic sites, as well as for the devel-
pment of novel therapeutic strategies. Drug discovery andevelopment require that model organisms used in preclin-cal assays can accurately predict the clinical efficacy andafety of new drugs. One of the major obstacles to drugiscovery is the lack of—or inadequacy of—animal modelsvailable for conducting preclinical studies of safety andfficacy, target identification and validation, and drugcreening. Therefore, determining the validity of animalodels of disease has great implications for the pharmaceu-
� 6) and control (n � 5) rats analyzed by RT-PCR.differences in the mean level of gene expression
.05, **P�.01.
al (ncant*P�
ical and biotechnology fields.
Vol. 87, No. 5, May 2007

hsmbmhocssrs
tcehstera
PcocafBtmlfc
tiifhiafsugtfai
lGgdowrmsg(lroc
raft(poasgstrcfih
ldop
F
Animal model validation has been limited to pathological,istologic, and pharmacologic considerations. Single-genetudies have been conducted in an attempt to validate animalodels genetically, but this approach cannot provide a
roader picture (30). For instance, we have identified com-on gene expression phenomena between experimental and
uman disease, such as the significant decrease in expressionf the TNF receptor 2 (Tnfrsf1b) (12). However, for aomplex disease such as endometriosis, with no clear under-tanding of its etiology and progression, and for which nopecific biomarker has been identified despite decades ofesearch, there are very few obvious candidate genes totudy.
In this study we proposed that gene expression profiling ishe most appropriate tool for validating a much-needed ac-urate, inexpensive, and accessible preclinical model forndometriosis. Therefore, we applied a comprehensive,igh-throughput technology such as cDNA microarrays toolve the complex question at hand: is the autotransplanta-ion rat model of endometriosis a valid model of this dis-ase? To answer this question, we conducted cDNA microar-ay analysis to compare gene expression profiles of ectopicnd eutopic endometrium in this animal model.
To validate the cDNA microarray results, real-time RT-CR analysis of the level of expression of selected genes wasonducted. This technology constitutes an independent wayf validating the cDNA microarray results while providing aost-effective way of quantifying gene expression levels indditional sample sets. Of the nine genes initially selectedor microarray data validation (PDGFA, LOXL1, IL2RG,CL2, OPG, MMP9, TGFB, APRIL, PGH2), we confirmed
he results for the first seven (Fig. 2). Discrepancies betweenicroarray and real-time PCR results in both direction and
evel of expression have been reported before, providingurther support for the use of real-time RT-PCR to confirm
FIGURE 2
Comparison of fold-expression of candidate genesin ectopic vs. eutopic endometrium analyzed byeither microarrays or real-time QRT-PCR.
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
DNA microarray data (31, 32). o
ertility and Sterility�
A difficulty related to cDNA microarray studies relates tohe fact that large gene sets are identified in a single exper-ment, making these large-scale studies problematic for datanterpretation. Although gene annotations (National Centeror Biotechnology Information/Entrez/Online Mendelian In-eritance in Man Database, and others) are helpful, search-ng for patterns or for interesting gene functions that can bescribed to disease is labor intensive, subjective, and there-ore impractical. Data mining tools such as GoMiner makeelecting significant trends from such large data sets a moreser-friendly process. GoMiner compares the expression ofenes from an experiment against the distribution of all ofhe genes of the genome on the GO hierarchy of geneunctions. Those branches that are not enriched by chancelone are flagged, and the investigator easily can select thosenteresting categories for further experimentation (15).
The GO category analysis was conducted to provide bio-ogic meaning and functional coherence to the results. UsingoMiner, we analyzed the biologic classifications of the 168enes that were differentially expressed (123 upregulated, 45ownregulated) in ectopically growing endometrium. Webserved that, in particular, defense-related cellular path-ays were significantly enriched, including inflammatory
esponse (10 genes), immune response (23 genes), and che-otaxis (9 genes). In addition, angiogenesis (5 genes), re-
ponse to wounding (18 genes), programmed cell death (14enes), metallopeptidase function (8 genes), cell adhesion14), extracellular matrix (16 genes), and collagen metabo-ism (6 genes) were also significantly enriched. Of the down-egulated genes, only tube development (2 genes), regulationf ossification (3 genes), and G1/S transition of the mitoticell cycle (3 genes) reached statistical significance (Table 3).
It is now widely accepted that angiogenesis plays a majorole in the pathogenesis of endometriosis (33–35). In fact,ngiogenic inhibitors have been proposed as a novel therapyor this disease because it has been shown that they suppresshe growth of endometriotic lesions in an animal model36, 37). Likewise, both integrin and metalloproteinase ex-ression have been associated with the metastatic potentialf endometriosis lesions. The fact that the immune systemnd inflammatory mechanisms are activated in endometrio-is is also well known. This study also served to identify newene expression profiles that may characterize endometrio-is. Interesting novel functional categories that deserve fur-her exploration include metal ion binding and transport,egulation of bone ossification and remodeling, and cellycle arrest and response to reactive oxygen species. Thesendings are expected to promote the development of novelypotheses that likely will guide future research directions.
The present study has uncovered many interesting bio-ogic themes shared between the natural and experimentalisease. In agreement with observations made in patients, webserved gene-specific and pathway-specific patterns of ex-ression that may explain the observed survival and growth
f ectopic endometrium in rats. Endometriosis is most likely1193

TABLE 2Significantly enriched or depleted GO categories in ectopic vs. eutopic endometrium.
TermGoMiner
Enrichment factor Fisher P value
Biologic processOrganismal physiologic process 1.29 .05Regulation of organismal physiologic process 2.19 .01Positive regulation of organismal physiologic process 3.16 .01Angiogenesis 2.28 .05Histogenesis 1.99 .04Cartilage development 4.74 .01Tube development 5.44 .05Regulation of ossification 10.89 .01Negative regulation of bone remodeling 6.32 .02Cell adhesion 1.84 .01Cell cycle arrest 3.16 .05G1/s transition of mitotic cell cycle 5.44 .05Cell homeostasis 2.81 .04Ion homeostasis 2.6 .04Transition metal ion homeostasis 3.42 .03Response to wounding 2.25 .00Response to external stimulus 1.6 .01Response to abiotic stimulus 2 .01Response to chemical substance 2.71 .00Response to biotic stimulus 1.53 .01Response to external biotic stimulus 2.2 .00Response to pest, pathogen, or parasite 2.11 .00Defense response 1.69 .00Cellular defense response (sensu vertebrata) 2.81 .04Immune response 1.64 .01Regulation of immune response 2.33 .02Positive regulation of immune response 3.45 .00Positive regulation of lymphocyte proliferation 3.79 .03Positive regulation of T-cell proliferation 6.32 .02Inflammatory response 2.34 .01Chemotaxis 3.35 .00Immune cell chemotaxis 4.22 .01Immune cell migration 3.61 .01Neutrophil chemotaxis 4.74 .01Cytokine production 3.16 .01Cytokine biosynthesis 2.81 .04Positive regulation of cytokine biosynthesis 6.32 .02Interleukin-6 biosynthesis 6.32 .02Regulation of interleukin-6 biosynthesis 6.32 .02Collagen catabolism 3.95 .00Response to reactive oxygen species 6.32 .02
Cellular componentCell surface 2.81 .04Extracellular region 1.57 .00Extracellular matrix 2.56 .00Extracellular space 1.49 .00Plasma membrane 1.51 .03Intrinsic to membrane 1.33 .03
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
1194 Flores et al. Molecular profiling of rat endometriosis Vol. 87, No. 5, May 2007

tmigon
atc(tg
F
he result of the stepwise activation of a complex series ofolecular events that begin when endometrial cells present
n the menstrual fluid reach the peritoneal cavity by retro-rade menstruation (according to the Sampson theory). Ourbservations support the current knowledge from both theatural and experimental disease, which can be summarized
TABLE 2Continued.
Term
VacuoleLytic vacuole
Molecular functionIntegrin bindingIon bindingLipid bindingMetal ion bindingCation bindingMetallopeptidase activityMetalloendopeptidase activityTransition metal ion bindingTransition metal ion transport
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
TABLE 3Differentially expressed genes within relevant GO
GO category
Defense response SPP1, CD2, CD4, IL18,SYK, B2M, LBP, CCL2BST1, CCL4, CD74, S
Inflammatory response ITGAM, PTAFR, CCL4, SImmune cell migration
(neutrophils)IL1B, SPP1, ITGAM, CX
Angiogenesis ANPEP, HAND2, IL18, CBone remodelling PTGER4, OPG, SPP1, SResponse to reactive
oxygen speciesSOD2, GPX1
Cell adhesion CD2, ICAM1, SPP1, CTGTNC, CXCR4, ITGA4
Extracellular matrix SPP1, LAMA3, TNC, FNMMP9, MMP11, MMP
Programmed cell death OPN, HMOX1, NGFR, IGCDKN1A, CD2, AHR, T
Response to wounding THBD, C3, FN1, DMBT1CXCL1, IL18, CCL2, IT
Histogenesis SOX9, PTGER4, CTGF,Cell ion homeostasis MT1A, EDN1, TF, CPMetallopeptidase function MMP7, MMP9, MMP11,
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.ertility and Sterility�
s follows (Fig. 3): the initial attachment of cells that reachhe peritoneum to the extracellular matrix (adhesion mole-ule, integrin expression) is followed by tissue invasionmetalloprotease [MMPs] and tissue inhibitor of metallopro-ease activity), cell growth to form lesions (cell division,rowth factors, steroid hormones, k-ras mutations), survival
GoMinerEnrichment factor Fisher P value
2.6 .042.6 .04
6.32 .001.51 .054.22 .011.51 .051.58 .042.95 .002.71 .012.17 .016.32 .02
tegories.
Gene
R4, CDKN1A, CEBPB, IL1B, CD4, IL18, PTAFR,00A8, C3, TLR4, ITGAM, ICAM1, CXCL1, IL12A,, IL4R, IL2RG, FN1
1, CCL2, S100A8, C3, CXCL1, TLR4, IL1B, TGFB1
, ID15
ITGAM CD4, FN1, CD36, ALCAM, COL11A1, IL18,
TGF, HSPG2, COL11A1, OPG, TGFB1, MMP7,MMP13, MMP14, TIMP1, TIMP2GPX1, CEBPB, OPG, BCL2, FAIM, DDIT3, IL18,
B1R4, SOD2, CCL4, B2M, S100A8, TM4SF3, IL1B,
, SPP1, CD4, PTAFRD5, DMBT1, COL11A1, SPP1
P12, MMP13, MMP14, TIMP1, TIMP2
ca
CXC, S1
OD2PP
CL1
TGFMAD
F,
1, C12,F1,GF, TLGAMSMA
MM
1195

aitit(nvl
cmmmettdfleaaapad
mtta
couitoneaht
ArMo
R
t the ectopic site (angiogenesis, resistance to apoptosis,nduction of local immunosuppression), and finally activa-ion of wound healing mechanisms ensues, which may resultn the fibrosis, scarring, and adhesion formation that charac-erize severe endometriosis. Concomitantly, inflammatoryneutrophil chemotaxis, complement) and immune mecha-isms (T-cell activation, cytokines, chemokines) are acti-ated in response to the growth of cells at the abnormalocation, and these probably feed into the proposed pathway.
It should be noted that there are limitations to the use ofDNA microarrays for the study of endometriosis. Endo-etriotic tissue is heterologous, i.e., it is a mixture of endo-etrium, myometrium, serosa, connective tissue, and im-une cells. Therefore, there is no guarantee that the gene
xpression profiles that we have identified derive from tissuehat is significantly contributing to the pathophysiology ofhis disease. The recent application of laser capture micro-issection to molecular studies will undoubtedly facilitateollow-up studies of gene expression in the different cellineages that compose heterogeneous tissues such as thendometrial lesions (20). Also, because cDNA microarraysre assaying the message for protein synthesis but not thectual protein levels, it is important that follow-up studiesre conducted to determine the extent to which relevantroteins are produced. Similarly, functional studies in vitrond in vivo should ask whether differences in protein pro-uction are indeed related to disease.
In summary, although it is generally accepted that nonhu-an primate models of endometriosis most closely resemble
he disease (38), this study provides evidence in support ofhe autotransplantation rat model as a simple, inexpensive,
FIGURE 3
A model of disease for endometriosis based ondata from both animal and human studies.
Flores. Molecular profiling of rat endometriosis. Fertil Steril 2007.
nd useful alternative for studying certain aspects of this
1196 Flores et al. Molecular profiling of rat endometriosis
ondition. This model of endometriosis, originally devel-ped by Vernon and Wilson in 1985 (39), has already beensed for testing possible new drugs, including studies show-ng for the first time the potential of anti-TNF agents for thereatment of endometriosis (40–45). The common themesf gene expression between the experimental and theatural disease described herein should be consideredvidence in support of this surgically induced rat model asn appropriate and invaluable tool for studying the naturalistory of endometriosis and testing novel therapeutics forhis incurable disease. (33, 104)
cknowledgments: The authors thank Dr. Sükrü Tuzmen at TGen Corpo-ation, Tuczon, AZ, for data analysis support, and the Research Centers in
inority Institutions (RCMI) Publications Office and the Molecular Biol-gy Core, supported by RCMI Grant # 2G12 RR03050-18.
EFERENCES1. Mahmood TA, Templeton A. Prevalence and genesis of endometrio-
sis. Hum Reprod 1991;6:544–9.2. Witz CA, Allsup KT, Montoya-Rodríguez IA, Vaughan SL, Centonze
VE, Schenken RS. Pathogenesis of endometriosis—current research.Hum Fertil 2003;6:34–40.
3. Vernon MW, Wilson EA. Studies on the surgical induction of endo-metriosis in the rat. Fertil Steril 1985;44:684–94.
4. Story L, Kennedy S. Animal studies in endometriosis: a review. ILARJ 2004;45:132–8.
5. Sharpe-Timms KL. Using rats as a research model for the study ofendometriosis. Ann NY Acad Sci 2002;955:318–27.
6. Vernon MW. Experimental endometriosis in laboratory animals as aresearch model. Prog Clin Biol Res 1990;323:49–60.
7. D’Hooghe TM, Mwenda JM, Hill JA. A critical review of the useand application of the baboon as a model for research in women’sreproductive health. Gynecol Obstet Invest 2004;57:1– 60. Epub2003 Dec 29.
8. Sharpe KL, Vernon MW. Polypeptides synthesized and released by ratectopic uterine implants differ from those of the uterus in culture. BiolReprod 1993;48:1334–40.
9. Sharpe KL, Bertero MC, Vernon MW. Detection of a progesterone-induced secretory protein synthesized by the uteri but not the endo-metriotic implants of rats with induced endometriosis. Fertil Steril1991;55:403–10.
10. Uchiide I, Ihara T, Sugamata M. Pathological evaluation of the ratendometriosis model. Fertil Steril 2002;78:782–6.
11. Mizumoto Y, Hirata J, Tokuoka S, Furuya K, Kikuchi Y, Nagata I.Effect of culture supernatants of endometriotic lesions, uterine endo-metrium and peritoneum from rats with experimental endometriosison the natural killer activity of spleen cells. Gynecol Obstet Invest1996;41:122–7.
12. Rojas-Cartagena C, Appleyard CB, Santiago OI, Flores I. Experimen-tal intestinal endometriosis is characterized by increased levels ofsoluble TNFRSFa and downregulation of Tnfrsfa and Tnfrsfb geneexpression. Biol Reprod 2005;73:1211–8. Epub 2005 Aug 10.
13. Hughes TR, Shoemaker DD. cDNA microarrays for expression pro-filing. Curr Opin Chem Biol 2001;5:21–5.
14. Albertson DG, Pinkel D. Genomic microarrays in human geneticdisease and cancer. Hum Mol Genet 2003;12:R145–52.
15. Zeeberg BR, Feng W, Wang G, Wang MD, Fojo AT, Sunshine M, etal. GoMiner: a resource for biological interpretation of genomic andproteomic data. Genome Biol 2003;4:R28. Epub 2003 Mar 25.
16. Eyster KM, Boles AL, Brannian JD, Hansen KA. DNA microarrayanalysis of gene expression markers of endometriosis. Fertil Steril
2002;77:38–42.Vol. 87, No. 5, May 2007

F
17. Lebovic DI, Baldocchi RA, Mueller MD, Taylor RN. Altered expres-sion of a cell-cycle suppressor gene, Tob-1, in endometriotic cells bycDNA array analyses. Fertil Steril 2002;78:849–54.
18. Arimoto T, Katagiri T, Oda K, Tsunoda T, Yasugi T, Osuga Y, et al.Genome-wide cDNA microarray analysis of gene-expression profilesinvolved in ovarian endometriosis. Int J Oncol 2003;22:551–60.
19. Kao LC, Germeyer A, Tulac S, Lobo S, Yang JP, Taylor RN, et al.Expression profiling of endometrium from women with endometriosisreveals candidate genes for disease-based implantation failure andinfertility. Endocrinology 2003;144:2870–81.
20. Matsuzaki S, Canis M, Vaurs-Barriere C, Pouly JL, Boespflug-TanguyO, Penault Llorca F, et al. DNA microarray analysis of gene expres-sion profiles in deep endometriosis using laser capture microdissec-tion. Mol Hum Reprod 2004;10:719–28.
21. Matsuzaki S, Canis M, Vaurs-Barriere C, Boespflug-Tanguy O, Das-tugue B, Mage G. DNA microarray analysis of gene expression ineutopic endometrium from patients with deep endometriosis usinglaser capture microdissection. Fertil Steril 2005;84 Suppl 2:1180–90.
22. Flores I, Rivera E, Mousses S, Chen Y, Rozenblum E. Identificationof molecular markers for endometriosis in blood lymphocytes usingDNA microarrays. Fertil Steril 2006;85:1676–83.
23. Ingelmo MR, Quereda F, Acién P. Intraperitoneal and subcutaneustreatment of experimental endometriosis with recombinant humaninterferon-�-2b in a murine model. Fertil Steril 1999;71:907–11.
24. Eberwine J. Amplification of mRNA populations using aRNA gener-ated from immobilized oligo(dT)-T7 primed cDNA. Biotechniques1996;20:584–91.
25. Diegman J, Junker K, Gerstmayer B, Bosio A, Hindermann W, Rosen-hahn J, et al. Identification of CD70 as a diagnostic marker for clearcell renal cell carcinoma by gene expression profiling, real-time RT-PCR and immunohistochemistry. Eur J Cancer 2005;41:1794–801.
26. Hedenfalk I, Duggan D, Chen Y, Radmacher M, Bittner M, Simon R,et al. Gene-expression profiles in hereditary breast cancer. N EnglJ Med 2001;344:539–48.
27. Brazma A, Hingamp P, Quackenbush J, Sherlock G, Spellman P,Stoeckert C, et al. Minimum information about a microarray experi-ment (MIAME)—toward standards for microarray data. Nat Genet2001;29:365–71.
28. Livak KJ, Schmittgen TD. Analysis of relative gene expression datausing real-time quantitative PCR and the 2(-delta delta Ct) method.Methods 2001;25:402–8.
29. Radonic A, Thulke S, Mackay IM, Landt O, Siegert W, Nitsche A.Guideline to reference gene selection for quantitative real-time PCR.Biochem Biophys Res Commun 2004;313:856–62.
30. Fang Z, Yang S, Gurates B, Tamura M, Simpson E, Evans E, et al.Genetic or enzymatic disruption of aromatase inhibits the growth ofectopic uterine tissue. J Clin Endocrinol Metab 2002;87:3460–6.
31. Orr WE, Song BK, Geisert EE Jr. Comparing the use of Affymetrix tospotted oligonucleotide microarrays using two retinal pigment epithe-lium cell lines. Mol Vis 2003;9:482–96.
32. Jenson SD, Robetorye RS, Bohling SD, Schumacher JA, Morgan JW,Lim MS, et al. Validation of cDNA microarray gene expression dataobtained from linearly amplified RNA. Mol Pathol 2003;56:307–12.
33. McLaren J. Vascular endothelial growth factor and endometrioticangiogenesis. Hum Reprod Update 2000;6:45–55.
34. Groothuis PG, Nap AW, Winterhager E, Grummer R. Vascular de-velopment in endometriosis. Angiogenesis 2005;8:147–56. Epub 2005Oct 7.
35. Print C, Valtola R, Evans A, Lessan K, Malik S, Smith S. Solublefactors from human endometrium promote angiogenesis and regulatethe endothelial cell transcriptome. Hum Reprod 2004;19:2356–66.Epub 2004 Jul 8.
36. Becker CM, Sampson DA, Rupnick MA, Rohan RM, Efstathiou JA,Short SM, et al. Endostatin inhibits the growth of endometrioticlesions but does not affect fertility. Fertil Steril 2005;84 Suppl2:1144–55.
37. Laschke MW, Elitzsch A, Vollmar B, Vajkoczy P, Menger MD.
Combined inhibition of vascular endothelial growth factor (VEGF),ertility and Sterility�
fibroblast growth factor and platelet-derived growth factor, but notinhibition of VEGF alone, effectively suppresses angiogenesis andvessel maturation in endometriotic lesions. Hum Reprod2006;21:262–8.
38. D’Hooghe TM, Mwenda JM, Hill JA. A critical review of the useand application of the baboon as a model for research in women’sreproductive health. Gynecol Obstet Invest 2004;57:1– 60. Epub2003 Dec 29.
39. Vernon MW, Wilson EA. Studies on the surgical induction of endo-metriosis in the rat. Fertil Steril 1985;44:684–94.
40. Tjaden B, Galetto D, Woodruff JD, Rock JA. Time-related effects ofRU486 treatment in experimentally induced endometriosis in the rat.Fertil Steril 1993;59:437–40.
41. Keenan JA, Williams-Boyce PK, Massey PJ, Chen TT, Caudle MR,Bukovsky A. Regression of endometrial explants in a rat model ofendometriosis treated with the immune modulators loxoribine andlevamisole. Fertil Steril 1999;72:135–41.
42. Dogan E, Saygili U, Posaci C, Tuna B, Caliskan S, Altunyurt S, etal. Regression of endometrial explants in rats treated with thecyclooxygenase-2 inhibitor rofecoxib. Fertil Steril 2004;82 Suppl3:1115–20.
43. Lebovic DI, Kir M, Casey CL. Peroxisome proliferator-activatedreceptor-gamma induces regression of endometrial explants in a ratmodel of endometriosis. Fertil Steril 2004;82 Suppl 3:1008–13.
44. Matsuzaki S, Canis M, Darcha C, Dallel R, Okamura K, Mage G.Cyclooxygenase-2 selective inhibitor prevents implantation of eutopicendometrium to ectopic sites in rats. Fertil Steril 2004;82:1609–15.
45. D’Antonio M, Martelli F, Peano S, Papoian R, Borrelli F.Ability ofrecombinant human TNF binding protein-1 (r-hTBP-1) to inhibit thedevelopment of experimentally induced endometriosis in rats. J Re-prod Immunol 2000;48:81–98.
46. Mulayim N, Savlu A, Guzeloglu-Kayisli O, Kayisli UA, Arici A.Regulation of endometrial stromal cell matrix metalloproteinase ac-tivity and invasiveness by interleukin-8. Fertil Steril 2004;81 Suppl1:904–11.
47. Chung HW, Wen Y, Chun SH, Nezhat C, Woo BH, Lake-Polan M.Matrix metalloproteinase-9 and tissue inhibitor of metalloproteinase-3mRNA expression in ectopic and eutopic endometrium in women withendometriosis: a rationale for endometriotic invasiveness. Fertil Steril2001;75:152–9.
48. Ueda M, Yamashita Y, Takehara M, Terai Y, Kumagai K, Ueki K, etal. Gene expression of adhesion molecules and matrix metalloprotein-ases in endometriosis. Gynecol Endocrinol 2002;16:391–402.
49. Collette T, Bellehumeur C, Kats R, Maheux R, Mailloux J, VilleneuveM, et al. Evidence for an increased release of proteolytic activity bythe eutopic endometrial tissue in women with endometriosis and forinvolvement of matrix metalloproteinase-9. Hum Reprod 2004;19:1257–64. Epub 2004 Apr 22.
50. Bruner-Tran KL, Eisenberg E, Yeaman GR, Anderson TA, McBeanJ, Osteen KG. Steroid and cytokine regulation of matrix metallo-proteinase expression in endometriosis and the establishment ofexperimental endometriosis in nude mice. J Clin Endocrinol Metab2002;87:4782–91.
51. Lessey BA. Implantation defects in infertile women with endometri-osis. Ann N Y Acad Sci 2002;955:265–80. ; discussion 293–5, 396–406.
52. García-Velasco JA, Seli E, Arici A. Regulation of monocyte chemo-tactic protein-1 expression in human endometrial stromal cells byintegrin-dependent cell adhesion. Biol Reprod 1999;61:548–52.
53. Jones RK, Searle RF, Bulmer JN. Apoptosis and bcl-2 expression innormal human endometrium, endometriosis and adenomyosis. HumReprod Update 1998;4:702–9.
54. Cameron RI, Maxwell P, Jenkins D, McCluggage WG. Immunohis-tochemical staining with MIB1, bcl2 and p16 assists in the distinctionof cervical glandular intraepithelial neoplasia from tubo-endometrialmetaplasia, endometriosis and microglandular hyperplasia. Histopa-
thology 2002;41:313–21.1197

55. Nishida M, Nasu K, Ueda T, Fukuda J, Takai N, Miyakawa I.Endometriotic cells are resistant to interferon-gamma-induced cellgrowth inhibition and apoptosis: a possible mechanism involved in thepathogenesis of endometriosis. Mol Hum Reprod 2005;11:29–34.Epub 2004 Dec 3.
56. Hayrabedyan S, Kyurkchiev S, Kehayov I. FGF-1 and S100A13possibly contribute to angiogenesis in endometriosis. J Reprod Immu-nol 2005;67:87–101.
57. Tao XJ, Sayegh RA, Isaacson KB. Increased expression of comple-ment component 3 in human ectopic endometrium compared with thematched eutopic endometrium. Fertil Steril 1997;68:460–7.
58. Rageh MA, Moussad EE, Wilson AK, Brigstock DR. Steroidal regu-lation of connective tissue growth factor (CCN2; CTGF) synthesis inthe mouse uterus. Mol Pathol 2001;54:338–46.
59. Wu Y, Kajdacsy-Balla A, Strawn E, Basir Z, Halverson G, Jailwala P,et al. Transcriptional characterizations of differences between eutopicand ectopic endometrium. Endocrinology 2006;147:232–46. Epub2005 Sep 29.
60. Harrington DJ, Lessey BA, Rai V, Bergqvist A, Kennedy S, Manek S,et al. Tenascin is differentially expressed in endometrium and endo-metriosis. J Pathol 1999;187:242–8.
61. Lessey BA, Castelbaum AJ, Sawin SW, Buck CA, Schinnar R, BilkerW, et al. Aberrant integrin expression in the endometrium of womenwith endometriosis. J Clin Endocrinol Metab 1994;79:643–9.
62. Chrobak A, Gmyrek GB, Sozanski R, Sieradzka U, Paprocka M,Gabrys M, et al. The influence of extracellular matrix proteins onT-cell proliferation and apoptosis in women with endometriosis oruterine leiomyoma. Am J Reprod Immunol 2004;51:123–9.
63. Nishida M, Nasu K, Fukuda J, Kawano Y, Narahara H, Miyakawa I.Down-regulation of interleukin-1 receptor type 1 expression causesthe dysregulated expression of CXC chemokines in endometrioticstromal cells: a possible mechanism for the altered immunologicalfunctions in endometriosis. J Clin Endocrinol Metab 2004;89:5094–100.
64. Matalliotakis IM, Goumenou AG, Mulayim N, Karkavitsas N, Kou-mantakis EE. High concentrations of the CA-125, CA 19-9 and CA15-3 in the peritoneal fluid between patients with and without endo-metriosis. Arch Gynecol Obstet 2005;271:40–5. Epub 2004 Jul 9.
65. Hombach-Klonisch S, Kehlen A, Fowler PA, Huppertz B, Jugert JF,Bischoff G, et al. Regulation of functional steroid receptors andligand-induced responses in telomerase-immortalized human endome-trial epithelial cells. J Mol Endocrinol 2005;34:517–34.
66. Harada M, Osuga Y, Hirata T, Hirota Y, Koga K, Yoshino O, et al.Concentration of osteoprotegerin (OPG) in peritoneal fluid is in-creased in women with endometriosis. Hum Reprod 2004;19:2188–91. Epub 2004 Jul 8.
67. Bulletti C, Flamigni C, de Ziegler D. Implantation markers and en-dometriosis. Reprod Biomed Online 2005;11:464–8.
68. Ramon L, Gilabert-Estelles J, Castello R, Gilabert J, Espana F, RomeuA, et al. mRNA analysis of several components of the plasminogenactivator and matrix metalloproteinase systems in endometriosis usinga real-time quantitative RT-PCR assay. Hum Reprod 2005;20:272–8.Epub 2004 Dec 3.
69. Zhang X, Lin J, Qian Y, Deng L. Decreased levels of interleukin-18in peritoneal fluid but not in serum of patients with endometriosis.Fertil Steril 2004;81:1229–34.
70. Akoum A, Lemay A, Maheux R. Estradiol and interleukin-1beta exerta synergistic stimulatory effect on the expression of the chemokineregulated upon activation, normal T cell expressed, and secreted inendometriotic cells. J Clin Endocrinol Metab 2002;87:5785–92.
71. Tan XJ, Lang JH, Liu DY, Shen K, Leng JH, Zhu L. Expression ofvascular endothelial growth factor and thrombospondin-1 mRNA inpatients with endometriosis. Fertil Steril 2002;78:148–53.
72. Koks CA, Groothuis PG, Dunselman GA, de Goeij AF, Evers JL.Adhesion of menstrual endometrium to extracellular matrix: the pos-sible role of integrin alpha(6)beta(1) and laminin interaction. Mol
Hum Reprod 2000;6:170–7.1198 Flores et al. Molecular profiling of rat endometriosis
73. Matsuzaki S, Canis M, Darcha C, Dechelotte P, Pouly JL, Bruhat MA.Fibrogenesis in peritoneal endometriosis. A semi-quantitative analysisof type-I collagen. Gynecol Obstet Invest 1999;47:197–9.
74. Dimitriadis E, Stoikos C, Stafford-Bell M, Clark I, Paiva P, Kovacs G,et al. Cytokines, chemokines and growth factors in endometriumrelated to implantation. Hum Reprod Update 2006;69:53–64. Epub2005 Nov 28.
75. Orlandi A, Ferlosio A, Ciucci A, Sesti F, Lifschitz-Mercer B, Gabbi-ani G, et al. Cellular retinol-binding protein-1 expression in endome-trial stromal cells: physiopathological and diagnostic implications.Histopathology 2004;45:511–7.
76. Regidor PA, Regidor M, Schindler AE, Winterhager E. Aberrantexpression pattern of gap junction connexins in endometriotic tissues.Mol Hum Reprod 1997;3:375–81.
77. Ota H, Igarashi S, Hatazawa J, Tanaka T. Immunohistochemicalassessment of superoxide dismutase expression in the endometrium inendometriosis and adenomyosis. Fertil Steril 1999;72:129–34.
78. Gmyrek GB, Sozanski R, Jerzak M, Chrobak A, Wickiewicz D,Skupnik A, et al. Evaluation of monocyte chemotactic protein-1 levelsin peripheral blood of infertile women with endometriosis. Eur JObstet Gynecol Reprod Biol 2005;122:199–205.
79. Konno R, Yamada-Okabe H, Fujiwara H, Uchiide I, Shibahara H,Ohwada M, et al. Role of immunoreactions and mast cells in patho-genesis of human endometriosis—morphologic study and gene ex-pression analysis. Hum Cell 2003;16:141–9.
80. Chung HW, Lee JY, Moon HS, Hur SE, Park MH, Wen Y, et al.Matrix metalloproteinase-2, membranous type 1 matrix metallopro-teinase, and tissue inhibitor of metalloproteinase-2 expression in ec-topic and eutopic endometrium. Fertil Steril 2002;78:787–95.
81. Tsuchiya M, Katoh T, Motoyama H, Sasaki H, Tsugane S, Ikenoue T.Analysis of the AhR, ARNT, and AhRR gene polymorphisms: geneticcontribution to endometriosis susceptibility and severity. Fertil Steril2005;84:454–8.
82. Kusume T, Maeda N, Izumiya C, Yamamoto Y, Hayashi K, Oguri H,et al. Human leukocyte antigen expression by peritoneal macrophagesfrom women with pelvic endometriosis is depressed but coordinatedwith costimulatory molecule expression. Fertil Steril 2005;83 Suppl1:1232–40.
83. Wu MH, Yang BC, Lee YC, Wu PL, Hsu CC. The differentialexpression of intercellular adhesion molecule-1 (ICAM-1) and regu-lation by interferon-gamma during the pathogenesis of endometriosis.Am J Reprod Immunol 2004;51:373–80.
84. Johnson MC, Torres M, Alves A, Bacallao K, Fuentes A, Vega M, etal. Augmented cell survival in eutopic endometrium from women withendometriosis: expression of c-myc, TGF-beta1 and bax genes. Re-prod Biol Endocrinol 20058;3:45.
85. Hsieh YY, Chang CC, Tsai FJ, Peng CT, Yeh LS, Lin CC. Polymor-phism for transforming growth factor beta 1-509 (TGF-B1-509): as-sociation with endometriosis. Biochem Genet 2005;43:203–10.
86. Roberts M, Luo X, Chegini N. Differential regulation of interleukinsIL-13 and IL-15 by ovarian steroids, TNF-alpha and TGF-beta inhuman endometrial epithelial and stromal cells. Mol Hum Reprod2005;11:751–60. Epub 2005 Oct 27.
87. Lang GA, Yeaman GR. Autoantibodies in endometriosis sera recog-nize a Thomsen-Friedenreich-like carbohydrate antigen. J Autoimmun2001;16:151–61.
88. Mathur SP, Lee JH, Jiang H, Arnaud P, Rust PF. Levels of transferrinand alpha 2-HS glycoprotein in women with and without endometri-osis. Autoimmunity 1999;29:121–7.
89. Bellehumeur C, Collette T, Maheux R, Mailloux J, Villeneuve M,Akoum A. Increased soluble interleukin-1 receptor type II proteolysisin the endometrium of women with endometriosis. Hum Reprod2005;20:1177–84. Epub 2005 Feb 10.
90. Noble LS, Takayama K, Zeitoun KM, Putman JM, Johns DA, Hin-shelwood MM, et al. Prostaglandin E2 stimulates aromatase expres-sion in endometriosis-derived stromal cells. J Clin Endocrinol Metab
1997;82:600–6.Vol. 87, No. 5, May 2007

1
1
1
1
1
F
91. Hsieh YY, Chang CC, Tsai FJ, Hsu CM, Lin CC, Tsai CH. Angio-tensin I-converting enzyme ACE 2350*G and ACE-240*T-relatedgenotypes and alleles are associated with higher susceptibility toendometriosis. Mol Hum Reprod 2005;11:11–4. Epub 2004 Nov 5.
92. Luo X, Xu J, Chegini N. The expression of Smads in human endo-metrium and regulation and induction in endometrial epithelial andstromal cells by transforming growth factor-beta. J Clin EndocrinolMetab 2003;88:4967–76.
93. Gallinelli A, Chiossi G, Giannella L, Marsella T, Genazzani AD,Volpe A. Different concentrations of interleukins in the peritonealfluid of women with endometriosis: relationships with lymphocytesubsets. Gynecol Endocrinol 2004;18:144–51.
94. Harris HA, Bruner-Tran KL, Zhang X, Osteen KG, Lyttle CR. Aselective estrogen receptor-beta agonist causes lesion regression in anexperimentally induced model of endometriosis. Hum Reprod 2005;20:936–41. Epub 2004 Dec 23.
95. Matsuzaki S, Murakami T, Uehara S, Canis M, Sasano H, Okamura K.Expression of estrogen receptor alpha and beta in peritoneal andovarian endometriosis. Fertil Steril 2001;75:1198–205.
96. Nip MM, Miller D, Taylor PV, Gannon MJ, Hancock KW. Expressionof heat shock protein 70 kDa in human endometrium of normal andinfertile women. Hum Reprod 1994;9:1253–6.
97. Noda T, Murakami T, Terada Y, Yaegashi N, Okamura K. In-creased production of tumor necrosis factor-alpha by peritonealfluid mononuclear cells induced by 60-kDa heat shock protein inwomen with minimal to mild endometriosis. Am J Reprod Immu-
nol 2003;50:427–32.ertility and Sterility�
98. Kligman I, Grifo JA, Witkin SS. Expression of the 60 kDa heat shockprotein in peritoneal fluids from women with endometriosis: implica-tions for endometriosis-associated infertility. Hum Reprod 1996;11:2736–8.
99. Anaf V, Simon P, El Nakadi I, Fayt I, Simonart T, Buxant F, Noel JC.Hyperalgesia, nerve infiltration and nerve growth factor expression indeep adenomyotic nodules, peritoneal and ovarian endometriosis.Hum Reprod 2002;17:1895–900.
00. Hsieh YY, Chang CC, Tsai FJ, Lin CC, Tsai CH. T homozygote andallele of epidermal growth factor receptor 2073 gene polymorphismare associated with higher susceptibility to endometriosis andleiomyomas. Fertil Steril 2005;83:796–9.
01. Huang JC, Yeh J. Quantitative analysis of epidermal growth factorreceptor gene expression in endometriosis. J Clin Endocrinol Metab1994;79:1097–101.
02. Guo SW. Glutathione S-transferases M1/T1 gene polymorphisms andendometriosis: a meta-analysis of genetic association studies. MolHum Reprod 2005;11:729–43. Epub 2005 Nov 16.
03. Tabibzadeh S, Mason JM, Shea W, Cai Y, Murray MJ, Lessey B.Dysregulated expression of ebaf, a novel molecular defect in theendometria of patients with infertility. J Clin Endocrinol Metab 2000;85:2526–36.
04. Darnel AD, Archer TK, Yang K. Regulation of 11beta-hydroxysteroiddehydrogenase type 2 by steroid hormones and epidermal growthfactor in the Ishikawa human endometrial cell line. J Steroid Biochem
Mol Biol 1999;70:203–10.1199

Rlei
aoaaehi
RP
R
TECHNIQUES AND INSTRUMENTATION
Use of trypan blue staining to assess the qualityof ovarian cryopreservationPatricia Fauque, M.D.,a Anis Ben Amor, M.Sc.,a Christiane Joanne, Ph.D.,a
Germain Agnani, M.D.,b Jean Luc Bresson, M.D.,a and Christophe Roux, Ph.D., M.D.a
a Service de Génétique, Histologie, Biologie du Développement et de la Reproduction, Centres d’Etude et de Conservation desOeufs et du Sperme humain Franche-Comté Bourgogne, Hôpital Saint Jacques (Equipe Associée No. 3185: génétique etreproduction and Institut Fédératif de Recherche No. 133), University of Franche-Comté, and b Service de Gynécologie–Obstétrique, Hôpital Saint Jacques, Besançon, France
Objective: To check the efficiency of the cryopreservation procedure by using trypan blue staining of ovarian testfragments to assess the quality of frozen–thawed ovarian tissue.Design: Prospective study.Setting: University hospital.Patient(s): Patients with polycystic ovary syndrome undergoing laparoscopic ovarian drilling.Intervention(s): Ovarian cortical biopsies obtained from polycystic ovary syndrome patients were frozen using aslow freezing–rapid thawing protocol.Main Outcome Measure(s): Primordial and primary follicle viability was assessed with trypan blue staining.Unstained isolated follicles were studied by transmission electron microscopy. Histologic and immunohisto-chemical analysis of apoptosis was performed on tissue sections.Result(s): The percentage of unstained follicles considered live was lower (P�.015) after freezing/thawing(71.9%) than before cryopreservation (87.3%). Transmission electron microscopy on follicles considered liveconfirmed the lack of ultrastructural damage. After freezing/thawing, tissue morphology was preserved, butimmunohistochemical analysis shows a significant increase in the apoptosis process.Conclusion(s): Ovarian cortical test fragments combined with trypan blue staining on enzymatically isolatedfollicles is a useful and quick method of assessing the initial quality and viability of follicles in cryopreservedovarian tissue. This type of test should be used routinely as quality control in ovarian cryopreservationprocedures. (Fertil Steril� 2007;87:1200–7. ©2007 by American Society for Reproductive Medicine.)
Key Words: Apoptosis, cryopreservation, ovarian tissue, viability
caetw
nuhm
tracss
adiotherapy and chemotherapy have radically increased theong-term survival of young cancer patients, but major sideffects of these treatments are premature ovarian failure andnfertility in women of reproductive age (1).
Ionizing radiation has adverse effects on gonadal functiont all ages. The degree and persistence of the damage dependn the dose, irradiation field, and patient’s age. The ovariesre exposed to significant doses of radiation when radiother-py is used to treat pelvic and abdominal disease. Thestimated dose at which half of the follicles are lost inumans is 4 Gy (2). Thibaud et al. (3) showed that total bodyrradiation of �10 Gy given in a single dose before puberty
eceived May 2, 2006; revised and accepted August 7, 2006.resent address: Patricia Fauque, M.D., Laboratoire de Biologie de la Re-production, Université Paris V–Hôpital Cochin–Port-Royal, Paris France
eprint requests: Christophe Roux, Ph.D., M.D., Service de Génétique,Histologie, Biologie du Développement et de la Reproduction, CHUSaint Jacques, 25030 Besançon, France (FAX: 33-3-81-21-8806;
(E-mail: [email protected]).
1200 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
auses a high ovarian failure rate (55% to 80%), and after thege of 25 years total body irradiation is more toxic. How-ver, fractionated doses in total body irradiation are lessoxic to the ovaries, but ovarian failure is present in all casesith cumulative dose of �15 Gy.
Frequently, chemotherapeutic agents are used in combi-ation and the ovarian damage depends on the type of drugsed (alkylating agents, antimetabolites, vinca alkaloids in-ibitors, platinum agents), the dose, the duration of treat-ent, and the age of the patient (4, 5).
After cryopreservation of ovarian tissue but before initia-ion of the cytotoxic treatment, there is a possible option ofestoring fertility, either by autograft or in vitro maturation,fter remission. This technique is now performed by manylinical teams around the world (6–8). Animal studies havehown that frozen–thawed ovarian tissue can restore cyclicecretion of ovarian steroids after autograft (9) or allograft
10–12).0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.115

brrcecc
ctb�psbhsa
MOOl(2p
gdtimwa
ltv
FT(r(i[mm
paT
ttcmti
wwbtitm
IfTitm(weatItfuCHb(
CoAtlsp0pdnaeF
HFti
F
Pregnancies and births after frozen ovarian autograft haveeen reported in rats, mice, and ewes (13–19). Successfuleimplantation has been reported in humans (20–22), andecently reports of births after orthotopic transplantation ofryopreserved ovarian tissue were published (23, 24). Nev-rtheless it seems important to evaluate the quality of theryopreservation on the predominant types of ovarian folli-les, the primordial and primary follicles.
In this study, the efficiency of the cryopreservation pro-edure has been investigated in both fresh and frozen–hawed tissues by follicular viability assessment with trypanlue staining on small enzymatically isolated follicles (�60m). The evaluation of this staining procedure was com-leted first by transmission electron microscopy (TEM) ob-ervation of unstained frozen–thawed follicles with trypanlue staining and considered as live follicles, and second byistologic evaluation and an immunohistochemistry apopto-is assay on ovarian cortical tissue sections performed beforend after freezing.
ATERIALS AND METHODSvarian Tissuevarian biopsies were performed on 20 women undergoing
aparoscopic ovarian drilling for polycystic ovary syndromePCOS). The mean age of the women was 28.9 years (range4 to 35 years). The patients gave their consent, and therocedure was approved by the local ethical committee.
Ovarian cortical fragments were obtained using biopsyrasping forceps from an avascular portion of the ovaryevoid of visible follicles or luteal tissue, and before elec-rocoagulation of the puncture site. The specimens weremmediately transported to the laboratory in Leibovitz L-15edium (Eurobio, Les Ulis, France) at 4°C. Ovarian cortexas dissected and cut into small pieces (1 mm in thickness
nd 0.5 to 1 cm2 in area) on ice.
One piece per patient was immediately fixed in Bouiniquid for histologic and immunocytochemical examination,wo pieces were used before freezing to determine follicleiability, and the other specimens were frozen.
reezing and Thawing Procedurehe protocol used was previously described by Gosden et al.
14). Ovarian cortical fragments were transferred, afterinsing in Leibovitz L-15 medium, into 1.8 ml cryovialsCML, Nemours, France) each containing 1 ml of “freez-ng solution” (1.5 mol/L dimethyl sulfoxide (DMSO)Sigma-Aldrich, St. Quentin Fallavier, France] and 0.1ol/L sucrose [Sigma-Aldrich, France] in Leibovitz L-15edium supplemented with 10% patient serum).
The pieces were equilibrated for 30 minutes in the cryo-rotective solution at 4°C on a tilting table and frozen usingprogrammable freezer (Planer Kryo 360/3.3, Sunbury-on-
hames, England). The temperature was lowered from 4°C oertility and Sterility�
o �9°C at the rate of 2°C/min. After a manual seeding byouching the cryotubes with liquid nitrogen prechilled for-eps, the vials were cooled to �40°C at the rate of 0.3°C/in, then to �140°C at 10°C/min. After stabilization of
emperature for 10 minutes, the cryovials were transferrednto liquid nitrogen and stored until thawing.
Ovarian cortical fragments were quickly thawed: the vialsere air-warmed for 30 seconds and immersed in a 37°Cater bath (2 minutes). Tissue pieces were washed in Lei-ovitz L-15 medium two times for 5 minutes each at roomemperature (RT). For each patient, one fragment was fixedn Bouin liquid for histologic examination and immunohis-ochemical analysis. Two other pieces were used to deter-inate the follicle viability after thawing.
solation of Small Follicles and Trypan Blue Stainingor Viability Assessmenthis technique previously described in sheep (25) was mod-
fied as follows. Ovarian cortex fragments were thinly sec-ioned with a scalpel, in Leibovitz L-15 medium supple-ented with 1 mg/ml (200 IU/ml) type Ia collagenase
Sigma-Aldrich, St Quentin Fallavier, France). Specimensere incubated at 37°C for 2 hours and moved with a pipette
very 30 minutes. Collagenase activity was inhibited by theddition of 50% patient serum. The suspension was filteredhrough a 60-�m nylon filter (Bioblock Fisher Scientific,llkirch, France) and stained in a Petri dish with 0.4% finalrypan blue (Sigma-Aldrich) for 10 minutes at RT. Theollicular viability and the follicular stage were assessednder an inverted microscope (Nikon, Diaphot 300,hampigny-sur Marne, France) at �400 magnification withoffman illumination contrast. Dead follicles were stainedlue, and live ones were unstained. All of the small follicles�60 �m in diameter) obtained by filtration were checked.
haracterization by Transmission Electron Microscopyf Live Follicles
sample of small follicles recovered from frozen–thawedissue exposed to trypan blue and unstained, so considered asive, was examined by TEM. Suspension containing un-tained follicles was centrifuged at 400g for 5 minutes. Theellet was fixed for 2 hours at 4°C in 5% glutaraldehyde and.8% paraformaldehyde in 0.1 M phosphate-buffered saline,H 7.2. Samples were postfixed in 2% OsO4 for 30 minutes,ehydrated, and embedded in araldite. Ultrathin sections (60m) were laid on nickel grids and stained with uranyl acetatend lead citrate and observed with a JEOL 1230 transmissionlectron microscope (JEOL Europe, Croissy-sur-Seine,rance).
istologic Analysis and Immunohistochemical Analysisor each patient, one fragment of both fresh and frozen–
hawed ovarian cortex was fixed in Bouin liquid, embeddedn paraffin wax, and sliced (6 �m) perpendicularly to the
varian cortex surface.1201

sgcnogpwu�m
otocco
Tw3sRsAFttgrPtNws
p1rDstclaPf
cc(1
3r
w
sgm
SAstfwbs
RITittHeo1w
ita9(mpspi(
TIbsiosian
For histologic examination, every fifth serial section wastained with Masson staining (Haematoxylin-Fushin-Luzreen). The follicles were then observed and classified ac-ording to their morphological stage of development, theumber of granulosa cell layers, and the absence or presencef the antrum (26), modified from Gougeon (27). The cate-ories used were: primordial with oocyte partially or com-letely encapsulated by squamous follicular cells, primaryith follicle surrounded by a single layer of cuboidal follic-lar cells, preantral with enlarged oocyte encapsulated by1 granulosa cell layer without antrum, and antral withultiple granulosa cell layers and antrum formation.
Apoptosis was assayed by immunohistochemical analysisf three apoptotic markers: evaluation of DNA fragmenta-ion (by terminal deoxynucleotidyl transferase-mediated de-xyuridine triphosphate nick end-labeling [TUNEL]) on oo-yte and follicular cell nuclei and detection of twoytoplasmic proapoptotic proteins (caspase 3 labeling orverexpression of Bax).
The in situ detection of DNA fragmentation using theUNEL method is based on the addition of labeled nucleotidesith fluorescein by terminal deoxynucleotidyl transferase to the=-hydroxyl ends of DNA strand breaks. For TUNEL, tissueections were deparaffined, rehydrated, treated with a Targetetrieval solution (DAKO Corporation, Carpinteria, CA), and
tained (1 hour at 37°C) with the In Situ Cell Death DetectionP commercial kit (Roche Molecular Biochemicals, Meylan,rance) with controls, according to the manufacturer’s instruc-
ions. After end labeling, the incorporated fluorescein was de-ected by an antifluorescein antibody (Fab fragments) conju-ated with alkaline phosphatase (AP) for 35 minutes at 37°C,evealed by NBT/BCIP (Life Technologies–Invitrogen, Cergyontoise, France) after 20 minutes of incubation at RT. All of
he steps were performed in a dark and humidified chamber.uclear apoptotic bodies were stained brown. The treated slidesere mounted in phosphate-buffered saline glycerol and ob-
erved under a light microscope at 400� magnification.
The caspase 3 proapoptotic protein, in the oocyte cyto-lasm, was detected by a specific antibody labeling the7-kDa unit of the cleaved caspase 3. The antibody does notecognize the inactive form of this enzyme, procaspase 3.eparaffined and rehydrated sections, as previously de-
cribed, were incubated overnight at RT in the dark withhe antiprotein activated caspase 3 antibody (cleavedaspase 3 (Asp 175) antibody, Ozyme, St. Quentin Yve-ine, France) diluted 1:200, revealed by a goat fluorescentntibody (IgG) anti-rabbit (Alexa Fluor 488, Molecularrobes–Invitrogen, Cergy Pontoise, France) diluted 1:400or 1 hour at RT.
On the serried section, overexpression of Bax in oocyteytoplasm also was detected by the indirect immunofluores-ence technique; a monoclonal antibody anti-Bax protein556467, BD Bioscience, le Pont de Claix, France) diluted
:750 was revealed by a secondary fluorescent antibody (CyTM o1202 Fauque et al. Viability and human ovarian cryopreserva
-conjugated AffiniPure, Jackson ImmunoResearch Laborato-ies, Cambriddgeshire, UK) diluted 1:400 for 1 hour at RT.
For the detection of caspase 3 and Bax proteins, slicesithout primary antibodies were used as negative controls.
All of the slides were observed under a fluorescence micro-cope in epifluorescence configuration (Olympus DX50, Run-is, France) equipped with special block filters at 400�agnification.
tatistical Analysisfter trypan blue staining and immunohistochemical analy-
is, an independent �2 test was used to compare the result ofhe follicle group without freezing with those observed inreezing/thawing group. Data on the population of patientsere expressed as the range, mean, and SD, and the resultsetween populations of patients were compared using thetudent’s t-test.
ESULTSsolation of Small Follicles and Viability Assessmenthe total number of follicles analyzed was 765 before freez-
ng and 1,192 after thawing (Table 1). Microscope observa-ion of isolated follicles showed in both fresh and frozen–hawed follicles a similar morphological appearance. Underoffman modulation contrast, the Balbiani vitellin body was
asily identified in all of the oocytes (Fig. 1A). Follicles withnly uncolored structures were considered live follicles (Fig.B), and follicles with blue oocyte and/or follicular cellsere considered dead follicles (Fig. 1C).
For the 20 patients studied, the percentage of morpholog-cally normal follicles considered live follicles with therypan blue staining was significantly lower (P�.015)fter freezing and thawing 71.9% � 23.9% (range 12.5 to4.9) than before cryopreservation, 87.3% � 11.5%range 50 to 100). Moreover, for one patient, the follicularortality percent was very high (87.5%). This lowest
ercentage of live follicles after thawing (12.5%) corre-ponds to an attempt in which kinetics of the coolingrocedure were caused by a technical problem with annitial slope faster than normal and a missing seedingpatient 5, Table 1).
ransmission Electron Microscopysolated follicles of frozen–thawed tissue, exposed to trypanlue and unstained then examined by TEM, showed a pre-erved cytologic architecture of the oocyte and the surround-ng follicular cells (Fig. 2A). The zona pellucida was absentr developing. Oocyte and nuclear envelope were well pre-erved. Mitochondria with normal appearance were presentn the oocyte cytoplasm. Smooth endoplasmic reticulumnd lipid bodies were associated closely with an intactuclear membrane, and no vacuole was found in the
ocyte cytoplasm.tion Vol. 87, No. 5, May 2007

pa
HGf
F
Occasionally, follicular cells were destroyed with cyto-lasm occupied by vacuoles, (Fig. 2B) and membrane dam-ge in mitochondria was observed in oocytes (Fig. 2C).
TABLE 1Values and mean number (� SEM) of follicles aft
Subject
Before freezing
No. unstained No. blue Viable follicle
1 20 3 87.02 9 0 100.03 10 2 83.34 16 4 80.05 7 1 87.56 11 0 100.07 25 3 89.38 19 3 86.49 25 6 80.6
10 8 1 88.911 45 3 93.812 32 4 88.913 79 3 96.314 35 4 89.715 96 3 97.016 90 3 96.817 2 2 50.018 90 14 86.519 73 4 94.820 7 3 70.0Sum 699 66Mean 87.3 � 11* Differs significantly (P�.015).
Fauque. Viability and human ovarian cryopreservation. Fertil Steril 2007.
FIGURE 1
Isolated follicles after freezing and thawing. (A): Phasclearly defined (arrow). (B): Follicles considered as livblue oocyte and follicular cells considered as dead fo
Fauque. Viability and human ovarian cryopreservation. Fertil Steril 2007.
ertility and Sterility�
istologic Analysis and Immunohistochemical Analysisood stromal and follicle morphology was found in both
resh and frozen–thawed ovarian cortical tissue (Fig. 3A).
olation and trypan blue staining.
After freezing and thawing
) No. unstained No. blue Viable follicles (%)
3 5 37.54 5 44.4
21 4 84.030 2 93.81 7 12.5
11 6 64.76 9 40.0
14 17 45.211 6 64.79 1 90.0
23 3 88.520 3 87.028 2 93.3
402 45 89.9189 10 95.0108 12 90.032 14 69.666 12 84.631 4 88.612 4 75.0
1,021 17171.9 � 23.9*
ntrast observation of the Balbiani vitellin body isllicles after trypan blue staining. (C): Follicle withe.
er is
s (%
.5
e-coe follicl
1203
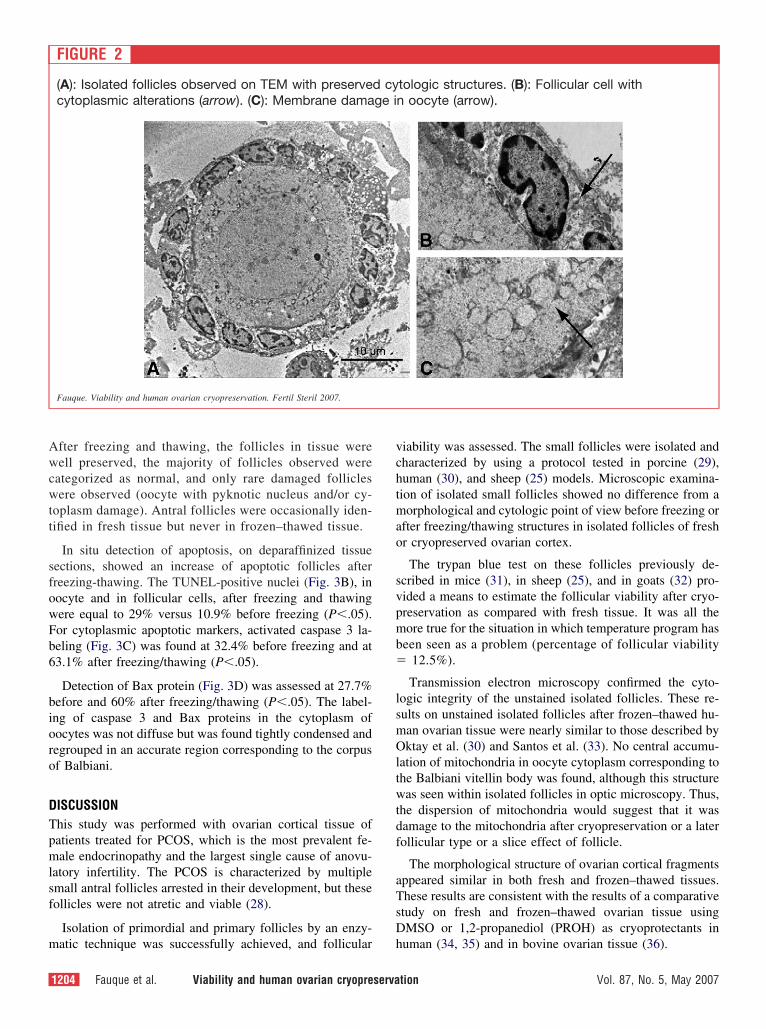
Awcwtt
sfowFb6
bioro
DTpmlsf
m
vchtmao
svpmb�
lsmOltwtdf
aTsD
fter freezing and thawing, the follicles in tissue wereell preserved, the majority of follicles observed were
ategorized as normal, and only rare damaged folliclesere observed (oocyte with pyknotic nucleus and/or cy-
oplasm damage). Antral follicles were occasionally iden-ified in fresh tissue but never in frozen–thawed tissue.
In situ detection of apoptosis, on deparaffinized tissueections, showed an increase of apoptotic follicles afterreezing-thawing. The TUNEL-positive nuclei (Fig. 3B), inocyte and in follicular cells, after freezing and thawingere equal to 29% versus 10.9% before freezing (P�.05).or cytoplasmic apoptotic markers, activated caspase 3 la-eling (Fig. 3C) was found at 32.4% before freezing and at3.1% after freezing/thawing (P�.05).
Detection of Bax protein (Fig. 3D) was assessed at 27.7%efore and 60% after freezing/thawing (P�.05). The label-ng of caspase 3 and Bax proteins in the cytoplasm ofocytes was not diffuse but was found tightly condensed andegrouped in an accurate region corresponding to the corpusf Balbiani.
ISCUSSIONhis study was performed with ovarian cortical tissue ofatients treated for PCOS, which is the most prevalent fe-ale endocrinopathy and the largest single cause of anovu-
atory infertility. The PCOS is characterized by multiplemall antral follicles arrested in their development, but theseollicles were not atretic and viable (28).
Isolation of primordial and primary follicles by an enzy-
FIGURE 2
(A): Isolated follicles observed on TEM with preservecytoplasmic alterations (arrow). (C): Membrane dama
Fauque. Viability and human ovarian cryopreservation. Fertil Steril 2007.
atic technique was successfully achieved, and follicular h
1204 Fauque et al. Viability and human ovarian cryopreserva
iability was assessed. The small follicles were isolated andharacterized by using a protocol tested in porcine (29),uman (30), and sheep (25) models. Microscopic examina-ion of isolated small follicles showed no difference from aorphological and cytologic point of view before freezing or
fter freezing/thawing structures in isolated follicles of freshr cryopreserved ovarian cortex.
The trypan blue test on these follicles previously de-cribed in mice (31), in sheep (25), and in goats (32) pro-ided a means to estimate the follicular viability after cryo-reservation as compared with fresh tissue. It was all theore true for the situation in which temperature program has
een seen as a problem (percentage of follicular viability12.5%).
Transmission electron microscopy confirmed the cyto-ogic integrity of the unstained isolated follicles. These re-ults on unstained isolated follicles after frozen–thawed hu-an ovarian tissue were nearly similar to those described byktay et al. (30) and Santos et al. (33). No central accumu-
ation of mitochondria in oocyte cytoplasm corresponding tohe Balbiani vitellin body was found, although this structureas seen within isolated follicles in optic microscopy. Thus,
he dispersion of mitochondria would suggest that it wasamage to the mitochondria after cryopreservation or a laterollicular type or a slice effect of follicle.
The morphological structure of ovarian cortical fragmentsppeared similar in both fresh and frozen–thawed tissues.hese results are consistent with the results of a comparativetudy on fresh and frozen–thawed ovarian tissue usingMSO or 1,2-propanediol (PROH) as cryoprotectants in
tologic structures. (B): Follicular cell withn oocyte (arrow).
d cyge i
uman (34, 35) and in bovine ovarian tissue (36).
tion Vol. 87, No. 5, May 2007

fdfitfra
pcteaolag
fcdssgc
cptehvop
F
The complementary results of the study show that thereezing combined with thawing induce an increase in theetection of apoptotic cells. The studies on the sheep did notnd more fragmentation of DNA after freezing (36, 37), but
he interpretation of results and the study model were dif-erent from ours. However, results of these investigatorsegarding the percentage and distribution of morphologicbnormalities showed tissue injury by cryopreservation.
In this study, we found that active caspase 3 and Baxrotein play a role in the apoptotic pathway induced byryopreservation. Caspase 3 is well-characterized proteasehat is involved in the effector phase of apoptosis (38). Itsxpression has been shown previously in ovarian somaticnd germ cells in the 24-hour cultures (39); however, a studyn a mouse ovary found that active caspase 3 was notocalized by immunohistochemistry to the granulosa cells ofny small follicles, but appeared in a later stage of follicle
FIGURE 3
Primordial follicles in frozen–thawed ovarian corticalmethod, positive nucleus in a follicular cell (arrow). (Ccondensed in the region corresponding to the corpus
Fauque. Viability and human ovarian cryopreservation. Fertil Steril 2007.
rowth (40). c
ertility and Sterility�
In a work on human cortical biopsies, the investogatorsailed to detect evidence of cleaved caspase 3, cleavedaspase 7, or DNA cleavage in nonatretic immature (primor-ial, primary) follicles (41). In antral follicles at the earliesttages of atresia (very few pyknotic granulosa cells perection), caspase 3 processing was the first sign of pendingranulosa cell death, with low or no staining of granulosaells by TUNEL.
Our results also show that the labeling of the activeaspase 3 is tightly localized in a region of oocyte cyto-lasm. This observation was also found for the Bax pro-ein, a proapoptotic member of the Bcl-2 gene familyxpressed in oocytes and granulosa cells (42, 43). Theypothesis for these labels was that they correspond to theitellin body of Balbiani. Indeed, the localized detectionf Bax protein would correspond to a movement of thisrotein at oocyte cytoplasm to membranes of one over-
e sections. (A): Masson staining. (B): TUNELaspase 3 labeling. (D): Bax detection, labelingBalbiani.
tissu): Cof
ellular compartment.
1205

iwmBpctib
dtt
tuctempq
thfatShe
AqHJ
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
This movement has been described by induction of apoptosisn murine thymocytes with dexamethasone or irradiation,hich shifts the subcellular locations of Bax from soluble toembrane-bound forms (44). Bax could be colocalized withcl-2 in the external membrane of the mitochondria, endo-lasmic reticulum, and nuclear envelope. This membraneompartment could correspond in follicles of human ovarianissue to the vitellin body of Balbiani. Therefore, furthernvestigation remains to be done to better define this mem-rane compartment.
In this work, we compared the results obtained from theifferent groups of follicles, but we were not able to comparehe sensitivity of patients with PCOS and normal patients tohe tissue dissociation and the cryopreservation.
The results of this study also suggest that human ovarianissue morphology and follicular viability were satisfactorysing cryopreservation in DMSO and sucrose, with the slowooling protocol well respected in this model. Ovarian cor-ical test fragments combined with trypan blue staining onnzymatically isolated follicles are a useful and quickethod for assessing the initial viability of follicles in cryo-
reserved ovarian tissue, and should be used routinely asuality control in ovarian cryopreservation procedures.
Further investigation, such as of the molecular explora-ions of ovarian tissue apoptosis, still remains to be done,owever, to explain the ultrastructural damage observed inrozen–thawed tissue. Therefore, more apoptosis could bettributable to ischemic injuries during the different times ofhe ovarian cortical tissue cryopreservation procedures (45).tudies report that cryopreservation techniques of an intactuman ovary with its vascular pedicle reduces these isch-mic injuries (46, 47).
cknowledgments: The authors thank Christophe Houdayer, Claude Jac-uemard, Daniel Fau, Ph.D., and Bernadette Griffon, Ph.D., Department ofistology, University of Besançon; for advice and technical assistance, and
oana Gaiffe for her help with the proofreading of the manuscript.
EFERENCES1. Wallace WH, Anderson RA, Irvine DS. Fertility preservation for young
patients with cancer: who is at risk and what can be offered? LancetOncol 2005;6:209–18.
2. Wallace WH, Shalet SM, Hendry JH, Morris-Jones PH, GattamaneniHR. Ovarian failure following abdominal irradiation in childhood: theradiosensitivity of the human oocyte. Br J Radiol 1989;62:995–8.
3. Thibaud E, Rodriguez-Macias K, Trivin C, Esperou H, Michon J,Brauner R. Ovarian function after bone marrow transplantation duringchildhood. Bone Marrow Transplant 1998;21:287–90.
4. Grundy R, Gosden RG, Hewitt M, Larcher V, Leiper A, Spoudeas HA,et al. Fertility preservation for children treated for cancer (1): scientificadvances and research dilemmas. Arch Dis Child 2001;84:355–9.
5. Meirow D, Nugent D. The effects of radiotherapy and chemotherapy onfemale reproduction. Hum Reprod Update 2001;7:535–43.
6. Poirot C, Vacher-Lavenu MC, Helardot P, Guibert J, Brugieres L,Jouannet P. Human ovarian tissue cryopreservation: indications andfeasibility. Hum Reprod 2002;17:1447–52.
7. Posada MN, Kolp L, Garcia JE. Fertility options for female cancer
patients: facts and fiction. Fertil Steril 2001;75:647–53.1206 Fauque et al. Viability and human ovarian cryopreserva
8. Schmidt KL, Andersen CY, Loft A, Byskov AG, Ernst E, AndersenAN. Follow-up of ovarian function post-chemotherapy followingovarian cryopreservation and transplantation. Hum Reprod 2005;20:3539 – 46.
9. Salle B, Lornage J, Demirci B, Vaudoyer F, Poirel MT, Franck M, et al.Restoration of ovarian steroid secretion and histologic assessment afterfreezing, thawing, and autograft of a hemi-ovary in sheep. Fertil Steril1999;72:366–70.
0. Candy CJ, Wood MJ, Whittingham DG. Follicular development incryopreserved marmoset ovarian tissue after transplantation. Hum Re-prod 1995;10:2334–8.
1. Newton H, Aubard Y, Rutherford A, Sharma V, Gosden R. Lowtemperature storage and grafting of human ovarian tissue. Hum Reprod1996;11:1487–91.
2. Baird DT, Webb R, Campbell BK, Harkness LM, Gosden RG. Long-term ovarian function in sheep after ovariectomy and transplantation ofautografts stored at �196 C. Endocrinology 1999;140:462–71.
3. Parrott DM. The fertility of mice with orthotopic ovarian grafts derivedfrom frozen tissue. J Reprod Fertil 1960;1:230–41.
4. Gosden RG, Baird DT, Wade JC, Webb R. Restoration of fertility tooophorectomized sheep by ovarian autografts stored at �196 degreesC. Hum Reprod 1994;9:597–603.
5. Cox SL, Shaw J, Jenkin G. Transplantation of cryopreserved fetalovarian tissue to adult recipients in mice. J Reprod Fertil 1996;107:315–22.
6. Gunasena KT, Villines PM, Critser ES, Critser JK. Live births afterautologous transplant of cryopreserved mouse ovaries. Hum Reprod1997;12:101–6.
7. Candy CJ, Wood MJ, Whittingham DG. Restoration of a normalreproductive lifespan after grafting of cryopreserved mouse ovaries.Hum Reprod 2000;15:1300–4.
8. Salle B, Demirci B, Franck M, Rudigoz RC, Guerin JF, Lornage J.Normal pregnancies and live births after autograft of frozen–thawedhemi-ovaries into ewes. Fertil Steril 2002;77:403–8.
9. Bordes A, Lornage J, Demirci B, Franck M, Courbiere B, Guerin JF, etal. Normal gestations and live births after orthotopic autograft ofvitrified-warmed hemi-ovaries into ewes. Hum Reprod 2005;20:2745–8.
0. Oktay K, Karlikaya G. Ovarian function after transplantation of frozen,banked autologous ovarian tissue. N Engl J Med 2000;342:1919.
1. Radford JA, Lieberman BA, Brison DR, Smith AR, Critchlow JD,Russell SA, et al. Orthotopic reimplantation of cryopreserved ovariancortical strips after high-dose chemotherapy for Hodgkin’s lymphoma.Lancet 2001;357:1172–5.
2. Oktay K, Buyuk E, Veeck L, Zaninovic N, Xu K, Takeuchi T, et al.Embryo development after heterotopic transplantation of cryopreservedovarian tissue. Lancet 2004;363:837–40.
3. Donnez J, Dolmans MM, Demylle D, Jadoul P, Pirard C, Squifflet J, etal. Livebirth after orthotopic transplantation of cryopreserved ovariantissue. Lancet 2004;364:1405–10.
4. Meirow D, Levron J, Eldar-Geva T, Hardan I, Fridman E, Zalel Y, etal. Pregnancy after transplantation of cryopreserved ovarian tissue in apatient with ovarian failure after chemotherapy. N Engl J Med 2005;353:318–21.
5. Demirci B, Lornage J, Salle B, Frappart L, Franck M, Guerin JF.Follicular viability and morphology of sheep ovaries after exposure tocryoprotectant and cryopreservation with different freezing protocols.Fertil Steril 2001;75:754–62.
6. Oktay K, Newton H, Mullan J, Gosden RG. Development of humanprimordial follicles to antral stages in SCID/hpg mice stimulated withfollicle stimulating hormone. Hum Reprod 1998;13:1133–8.
7. Gougeon A. Dynamics of follicular growth in the human: a model frompreliminary results. Hum Reprod 1986;1:81–7.
8. Homburg R, Amsterdam A. Polycystic ovary syndrome—loss of theapoptotic mechanism in the ovarian follicles? J Endocrinol Invest
1998;21:552–7.tion Vol. 87, No. 5, May 2007

2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
F
9. Roy SK, Greenwald GS. Methods of separation and in-vitro culture ofpre-antral follicles from mammalian ovaries. Hum Reprod Update1996;2:236–45.
0. Oktay K, Nugent D, Newton H, Salha O, Chatterjee P, Gosden RG.Isolation and characterization of primordial follicles from fresh andcryopreserved human ovarian tissue. Fertil Steril 1997;67:481–6.
1. Carroll J, Gosden RG. Transplantation of frozen–thawed mouse pri-mordial follicles. Hum Reprod 1993;8:1163–7.
2. Rodrigues APR, Amorim CA, Costa SHF, Santos RR, Lucci CM,Nunes JF, et al. Cryopreservation and short-term culture of isolatedcaprine primordial follicles. Small Ruminant Research 2005;56:103–111.
3. Santos RR, Rodrigues AP, Costa SH, Silva JR, Matos MH, Lucci CM,et al. Histological and ultrastructural analysis of cryopreserved sheeppreantral follicles. Anim Reprod Sci 2006;91:249–63.
4. Hovatta O, Silye R, Krausz T, Abir R, Margara R, Trew G, et al.Cryopreservation of human ovarian tissue using dimethylsulphoxideand propanediol-sucrose as cryoprotectants. Hum Reprod 1996;11:1268–72.
5. Hovatta O, Silye R, Abir R, Krausz T, Winston RM. Extracellularmatrix improves survival of both stored and fresh human primordialand primary ovarian follicles in long-term culture. Hum Reprod 1997;12:1032–6.
6. Lamaita RM, Bambirra EA, Camargos MG, Silva-Filho AL, Reis FM,Camargos AF. Histological evaluation of the effects of cryopreserva-tion in bovine ovarian tissue. J Assist Reprod Genet 2005;22:05–6.
7. Jeremias E, Bedaiwy MA, Nelson D, Biscotti CV, Falcone T. Assess-ment of tissue injury in cryopreserved ovarian tissue. Fertil Steril2003;79:651–3.
8. Cohen GM. Caspases: the executioners of apoptosis. Biochem J 1997;
326:1–16.ertility and Sterility�
9. Otala M, Erkkila K, Tuuri T, Sjoberg J, Suomalainen L, Suikkari AM,et al. Cell death and its suppression in human ovarian tissue culture.Mol Hum Reprod 2002;8:228–36.
0. Fenwick MA, Hurst PR. Immunohistochemical localization of activecaspase-3 in the mouse ovary: growth and atresia of small follicles.Reproduction 2002;124:659–65.
1. Matikainen T, Perez GI, Zheng TS, Kluzak TR, Rueda BR, Flavell RA,et al. Caspase-3 gene knockout defines cell lineage specificity forprogrammed cell death signaling in the ovary. Endocrinology 2001;142:2468–80.
2. Kugu K, Ratts VS, Piquette GN, Tilly KI, Tao XJ, Martimbeau S, et al.Analysis of apoptosis and expression of bcl-2 gene family members inthe human and baboon ovary. Cell Death Differ 1998;5:67–76.
3. Tilly JL, Tilly KI, Kenton ML, Johnson AL. Expression of members ofthe bcl-2 gene family in the immature rat ovary: equine chorionicgonadotropin-mediated inhibition of granulosa cell apoptosis is associ-ated with decreased bax and constitutive bcl-2 and bcl-xlong messengerribonucleic acid levels. Endocrinology 1995;136:232–41.
4. Hsu YT, Wolter KG, Youle RJ. Cytosol-to-membrane redistribution ofBax and Bcl-X(L) during apoptosis. Proc Natl Acad Sci USA 1997;94:3668–72.
5. Kim SS, Yang HW, Kang HG, Lee HH, Lee HC, Ko DS, et al.Quantitative assessment of ischemic tissue damage in ovarian corticaltissue with or without antioxidant (ascorbic acid) treatment. Fertil Steril2004;82:679–85.
6. Martinez-Madrid B, Dolmans MM, Van Langendonckt A, Defrere S,Donnez J. Freeze-thawing intact human ovary with its vascular pediclewith a passive cooling device. Fertil Steril 2004;82:1390–4.
7. Courbiere B, Massardier J, Salle B, Mazoyer C, Guerin JF, Lornage J.Follicular viability and histological assessment after cryopreservationof whole sheep ovaries with vascular pedicle by vitrification. Fertil
Steril 2005;84 Suppl 2:1065–71.1207

AsHfi(cse
e“
pi(At
cHrfauwi
RTR
IMAGES IN REPRODUCTIVE MEDICINEEdward E. Wallach, M.D.Associate Editor
Lithopedion: laparoscopic diagnosis and removalNatalie Z. Burger, M.D.,a Y. Elizabeth Hung, M.D., M.P.H.,b Alexandra N. Kalof, M.D.,c
and Peter R. Casson, M.D.a
a Division of Reproductive Endocrinology and Infertility, Department of Obstetrics and Gynecology, University of Vermont,Burlington, Vermont; b Department of Obstetrics and Gynecology, North Shore University Hospital, Manhasset, New York; andc Department of Pathology, University of Vermont, Burlington, Vermont
A lithopedion is an exceedingly rare obstetric phenomenon where the contents of an abdominal pregnancy calcifyand become preserved. We present the case of a young woman undergoing laparoscopy for infertility duringwhich a lithopedion was discovered. (Fertil Steril� 2007;87:1208–9. ©2007 by American Society for Repro-ductive Medicine.)
Key Words: Ectopic pregnancy, infertility, lithopedion
d
33-year-old, gravida 3, para 0, Ghanese emigrant pre-ented to us with a 5-year history of secondary infertility.er three previous pregnancies had occurred in Ghana, therst two of which were aborted by dilatation and curettageD&C), apparently without complications. In 1990, she be-ame pregnant for the third time. During early pregnancy,he experienced general feelings of illness, with multiplepisodes of syncope requiring hospitalization.
At approximately 12–14 weeks of pregnancy, she experi-nced heavy vaginal bleeding and received a D&C for amissed abortion.” No abnormal findings were noted.
Postoperatively, the patient continued to have abdominalain upon palpation as well as during long periods of stand-ng and lying in the prone position. A hysterosalpingogramHSG) performed in 1997 revealed “high-grade blockage.”
subsequent diagnostic laparoscopy confirmed bilateralubal blockage.
When the patient presented to us in 2002, she continued toomplain of episodes of the lower abdominal pain. A repeatSG again revealed bilateral proximal tubal blockage. In
etrospect, review of the HSG films revealed the outline of aetal calvarium (Fig. 1). Because of financial consider-tions, the patient and her husband opted for tubal eval-ation and possible repair rather than IVF. The patientas scheduled for a laparoscopy, hysteroscopy, and prox-
mal tubal cannulation.
eceived April 19, 2006; revised and accepted November 8, 2006.here are no potential conflicts of interest of a financial or other nature.eprint requests: Natalie Burger, M.D., University of Vermont, GivenC254, 89 Beaumont Avenue, Burlington, VT 05405 (FAX: 802-656-
b8771; E-mail: [email protected]).
1208 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
At the time of laparoscopy, significant pelvic adhesiveisease was noted, with the distal colon adherent to the
FIGURE 1
HSG indicating the outline of a fetal calvarium.
Burger. Lithopedion: diagnosis and removal. Fertil Steril 2007.
ladder and uterine fundus. Both fallopian tubes were
0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.11.065

twrBoo(
afr
DLsefiwt
lcpiimi
cpipntc
dfe
R1
2
3
4
5
F
ortuous, and the left tube was significantly dilated asell. Closer inspection revealed a foreign object near the
ight ovary and a firm region near the uterine fundus.lunt dissection demonstrated a small femur and multiplether pieces of bone. Dissection of the large, firm objectn the fundus demonstrated an almost intact calvariumFig. 2).
Laparoscopic chromopertubation confirmed tubal block-ge. Hysteroscopic attempts at cannulation were unsuccess-ul. The patient was informed of the findings at surgery and
FIGURE 2
Surgical specimens, including an intact calvariummeasuring 3 cm in diameter and multiple longbones.
Burger. Lithopedion: diagnosis and removal. Fertil Steril 2007.
ecovered from surgery without incident.
ertility and Sterility�
ISCUSSIONithopedion, literally “stone-child” in Greek, is a rare ob-tetric phenomenon in which the remains of an undiagnosedxtrauterine pregnancy calcify. The earliest report of such anding was in 1582. Autopsy of a 68-year-old Frenchoman revealed the remains of a calcified full-term fetus,
he pregnancy of which had been noted 28 years earlier (1).
Approximately 300 cases have been reported in the worlditerature. Modern presentation of lithopedions is rare be-ause of increased prenatal care and surveillance. However,atients presenting from areas lacking accurate diagnosticnstruments may still occasionally present with such a find-ng. Detection of a lithopedion can be difficult, and theajority are found incidentally during surgery, radiographic
maging, or at autopsy.
Reported complications from lithopedion formation in-lude: intestinal obstruction (2), pelvic abscess (3), cephalo-elvic disproportion with future pregnancy (4), and tubalnfertility (5). In our patient, we suspect that a previouselvic infection caused scarring, which led to the ectopic preg-ancy and lithopedion formation. However, it is also possiblehat an inflammatory reaction from the ectopic pregnancyaused the tubal damage secondarily.
Although an uncommon entity, the diagnosis of lithope-ion should be entertained in infertility patients presentingrom areas where modern diagnostic instruments are lacking,specially when an extrauterine mass is perceived on HSG.
EFERENCES. Bondeson J. The earliest known case of a lithopedion. J R Soc Med
1996;89:13–8.. Zaheer SA. Acute intestinal obstruction caused by lithopedion. Br J Surg
1971;58:401–2.. Jain T, Eckert LO. Abdominal pregnancy with lithopedion formation
presenting as a pelvic abscess. Obstet Gynecol 2000;96(5 Pt 2):808–10.. Leke RJ, Nasah BT, Shasha W, Monkam G. Cephalopelvic disproportion
at term involving a lithopedion: a case report. Int J Gynaecol Obstet1983;21:171–4.
. Shah-hosseini R, Evrard JR. Lithopedion: a case report. J Reprod Med
1987;32:131–3.1209

Sewp
rcmc(peppra
aIa
R
R
In utero incrustation of intrauterinesystems—consequent complications and monitoringKálmán Patai, Ph.D.,a Dorottya Kiss, M.D.,b László Dévényi, Ph.D.,c and Romána Zelkó, Ph.D.b
a Second Department of Obstetrics and Gynecology, b University Pharmacy Department of Pharmacy Administration, Sem-melweis University; and c Budapest University of Technology and Economics, Department of Materials Science and Engi-neering, Budapest, Hungary
As a result of physical aging of intrauterine therapeutic systems, in utero incrustments form on the rate-controllingmembrane of the IUSs. (Fertil Steril� 2007;87:1210–1. ©2007 by American Society for Reproductive Medicine.)
Apfcf
(t2cm
R1
2
3
4
5
even T-type intrauterine systems (IUSs) containing levonorg-strel (T-LNG-IUS, Mirena, Schering AG, Berlin, Germany)ere removed because of abdominal complaints and sus-ected inflammatory complications to the patients.
The photo- and electromicrographs of such systems (Fig. 1)evealed that the surface of the devices was covered withrystalline deposits, and microcracks were to be noted on theembrane surface controlling drug release. As a negative
ontrol, the image of an IUS prior to insertion is also shownFig. 2). The element analysis of the incrustment layer waserformed by means of energy dispersive roentgenogramxaminations, where the atoms excited by an electron beamroduce characteristic roentgenograms, forming typicaleaks in the spectrum for each element. According to theesults, the incrustment layer mainly consisted of calciumnd potassium salts (Fig. 3).
The background of the above phenomena is the physicalging of the siloxane-based polymeric membrane of theUSs. This aging process is manifested in volume relaxationnd consequent microcracks on the membrane surface (1).
eceived May 18, 2006; revised September 1, 2006; accepted November8, 2006.
eprint requests: Romána Zelkó, Ph.D., University Pharmacy, Institute ofPharmacy Administration, Semmelweis University, H �ogyes E. Street7-9, H-1092 Budapest, Hungary (FAX: 36-1-217 0927; E-mail:
1210 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
long these cracks, deposits of different compositions (de-ending on the biologic variability of the patients) can beormed, which then cause inflammatory complications be-ause of the hollow, uneven coating serving as a hiding placeor pathogens (2–4).
The deposits might also influence the drug release of IUSs5). As reported by the manufacturer, the hormone release ofhe devices decreases from 20 �g per 24 hours to 11 �g per4 hours over 5 years (6). This, besides the decrease of theoncentration gradient, might be attributed to the incrust-ent layer on the rate-controlling membrane surface.
EFERENCES. Süvegh K, Zelkó R. Physical ageing of polyvinylpyrrolidone under
different humidity conditions. Macromolecules 2002;35:795–800.. Sparks RA, Purrier B, Watt PJ, Elstein M. Bacteriological colonization
of uterine cavity: role of tailed intrauterine contraceptive device. BrMed J 1981;282:1189–91.
. Patai K, Berényi M, Sipos M, Noszál B. Characterization of calcifieddeposits on contraceptive intrauterine devices. Contraception 1998;58:305–8.
. Patai K, Dévényi L, Zelkó R. Comparison of surface morphology andcomposition of intrauterine devices in relation to the patient’s com-plaints. Contraception 2004;70:149–52.
. Zelkó R, Dévényi L, Patai K. Effect of physical ageing on the in uteroincrustation and subsequent changes in hormone release of intrauterinesystems. Eur J Pharm Sci 2005;25S1:S215–6.
. Mirena Product Monograph, Berlex Canada Inc. www.berlex.ca
0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.11.062
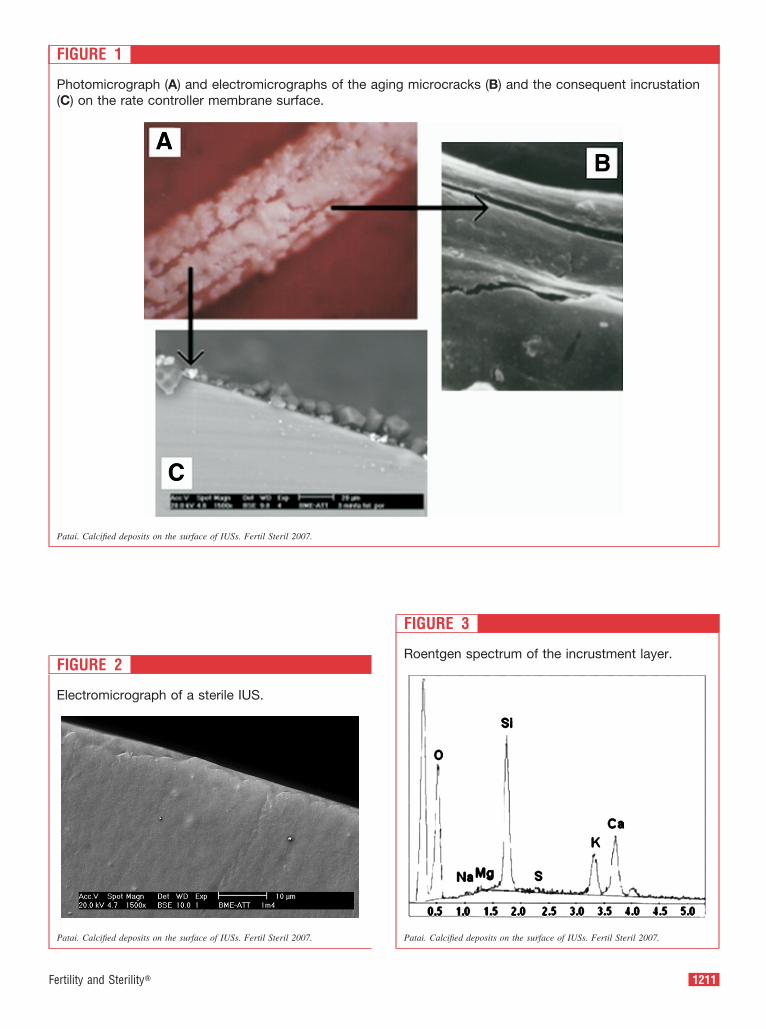
F
FIGURE 1
Photomicrograph (A) and electromicrographs of the aging microcracks (B) and the consequent incrustation(C) on the rate controller membrane surface.
Patai. Calcified deposits on the surface of IUSs. Fertil Steril 2007.
FIGURE 2
Electromicrograph of a sterile IUS.
Patai. Calcified deposits on the surface of IUSs. Fertil Steril 2007.
ertility and Sterility�
FIGURE 3
Roentgen spectrum of the incrustment layer.
Patai. Calcified deposits on the surface of IUSs. Fertil Steril 2007.
1211

HcaFpodWtI
wflapat
RC
R
CASE REPORT
0d
Successful pregnancy outcome with the use of in vitrofertilization after Essure® hysteroscopic sterilizationJohn F. Kerin, M.D., Ph.D.,a and Stephen Cattanach, M.D.b
a Flinders Reproductive Medicine Unit, Flinders University, Adelaide, South Australia, and b Mater Medical Centre, SouthBrisbane, Queensland, Australia
Objective: To assess the compatibility of pregnancy after IVF and ET procedures with the presence of the Essure®
microinsert.Design: Prospective, single-arm, clinical study (Canadian Task Force classification III).Setting: Clinical research center.Patient(s): Two women requesting IVF and ET procedures after Essure® microinsert sterilization.Intervention(s): Hysteroscopic sterilization, followed by IVF and ET procedures.Main Outcome Measure(s): Successful implantation and pregnancy outcomes after IVF procedures.Result(s): Both patients underwent a second-look hysteroscopy within 3 months of an IVF procedure. Deviceencapsulation by tissue ingrowth reduced the average number of coils trailing into the uterine cavity from fourto one, with no evidence of inflammation or any other abnormality. One woman conceived in her second IVFcycle after the transfer of two embryos, and the second woman conceived in her first cycle after the transfer of1 embryo. Ultrasound showed that the proximal echogenic segments of the microinserts remained �10 mmdistant from the pregnancy sac. Both women had spontaneous vaginal deliveries of healthy female infants.Postpartum ultrasound demonstrated that the microinserts maintained their prepregnancy utero-tubal locations.Conclusion(s): The Essure microinsert used for hysteroscopic sterilization may be compatible with implantationand successful pregnancy outcomes after IVF. (Fertil Steril� 2007;87:1212.e1–4. ©2007 by American Society forReproductive Medicine.)
Key Words: Essure®, hysteroscopic, sterilization, IVF, pregnancy
csumnm
MIdtatsbpqIttpd
ysteroscopic sterilization with the use of the Essure® mi-roinsert (Conceptus, Inc., Mountain View, CA) is the firstnd only transcervical method to receive approval by the USood and Drug Administration for clinical use. This ap-roval, granted in November 2002, followed the evaluationf phase II (1) and pivotal (2) multicenter clinical trials thatemonstrated acceptable safety and efficacy outcomes.omen undergoing this method of sterilization are informed
hat the procedure is irreversible, and that the alternatives ofVF and ET after the procedure remain untested.
The microinsert’s physical properties and dimensionsere described previously (3). Briefly, it consists of a soft,exible, outer, radially-expanding coil of nickel titaniumlloy (nitinol), designed to secure the microinsert in theroximal tube, and the microinsert extends from the ostium,long the intramural segment, across the utero-tubal junc-ion, and into the isthmic segment. An inner stainless-steel
eceived November 24, 2005; revised and accepted July 13, 2006.onflict of interest: The late Dr. John Kerin, M.D., Ph.D., was a consultantfor Conceptus, Inc., Mountain View, California.
eprint requests: Stephen Cattanach, M.D., Mater Medical Centre, 293Vulture Street, Suite 7, Level 6, South Brisbane, Queensland 4101,
pAustralia (FAX: 07-3844-4159; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.07.1549 Copyright ©2007 American Societ
oil houses polyethylene terephthalate fibers, which are de-igned to induce a benign, localized tissue ingrowth, andltimately complete occlusion of the tubal lumen (4). Theaterials comprising the microinsert are biocompatible, do
ot cause an inflammatory reaction, and are similar to theaterials used in cardiac and neurovascular stents (5).
ATERIALS AND METHODSn this case study, no institutional review board approval waseemed necessary, provided that informed consent was ob-ained prior to sterilization and IVF treatment. Two womenged 26 and 33 years, who had 2 and 4 children, respec-ively, underwent hysteroscopic sterilization using the Es-ure® system, one in March 2001, and the other in Septem-er 2001. Both women repartnered with men who had notreviously fathered children. Subsequently, both women in-uired about IVF procedures. Each couple was informed thatVF, ET, and pregnancy following this method of steriliza-ion had not been evaluated. Informed consents were ob-ained, and patients agreed to a second-look hysteroscopyrior to an IVF treatment cycle, as well as an ultrasound scanuring the first trimester of pregnancy and during the post-
artum period.1212.e1Fertility and Sterility� Vol. 87, No. 5, May 2007y for Reproductive Medicine, Published by Elsevier Inc.

sttacsmam
RTtwtct3if
The following information was obtained during theecond-look hysteroscopy: [1] photographic documenta-ion of the endometrial lining (particularly of the perios-ial area), [2] the number of exposed microinsert coils,nd [3] evidence of tissue ingrowth or encapsulation ofoils remaining in the uterine cavity. The spatial relation-hip of the echogenic microinserts to the pregnancy sacembranes was measured within the first trimester. The
ntenatal, intrapartum, and postnatal courses wereonitored.
FIGURE 1
View of microinserts in one patient at second-look hy(A) Hysteroscopic appearance of the trailing end of tcoils extend from the right ostium. (B) Second-look hdemonstrates complete tissue encapsulation of the in(C) Hysteroscopic view of left microinsert at completleft ostium. (D) Second-look hysteroscopy demonstracoil remaining visible on the left.
Kerin. IVF pregnancy after Essure® sterilization. Fertil Steril 2007.
1212.e2 Kerin and Cattanach IVF pregnancy after Essure® ster
ESULTShe interval between sterilization and the second-look hys-
eroscopy for the first woman was 41 months, and the secondoman, 28 months. The average number of trailing coils at
he time of microinsert placement was four (range, 3–5oils). At second-look hysteroscopy, the average number ofrailing coils was one (range, 0–2 coils). Ideally, between–8 coils are left trailing into the uterine cavity after micro-nsert placement. Each outer coil of the microinsert accountsor 1 mm of length, and therefore equates with an ideal
oscopy performed 28 months postprocedure.ght microinsert at completion of placement. Threeroscopy in the same woman 28 months laterterine portion of the right microinsert.f placement shows three coils extending from thetissue encapsulation, leaving only the tip of one
sterhe riystetrau
ion otes
ilization Vol. 87, No. 5, May 2007

tosbepdena
cngceematbltn
2am
wwain
ivTousre
DTsEtEwbtwb
F
railing length of 3–8 mm. The visual and photographicbservations of all trailing coils extending from the ostiahowed evidence of tissue ingrowth along the inner coil andetween the outer coils, which produced partial-to-completencapsulation (example provided in Fig. 1). Between bothatients, the average number of free trailing coils was re-uced from four to one because of a process of tissuencapsulation over an average time of 33 months. There waso evidence of abnormal vascular pattern, inflammation, orny other abnormality within the uterine cavities.
An ultrasound scan was performed 9 weeks after ET andonception. One patient’s ultrasound images of the preg-ancy sac, fetus, and chorion-decidual thickness in the re-ion of the echogenic microinserts in the upper uterineavity are shown in Figure 2. The microinserts extend lat-rally into the region of the intramural tube toward thexternal utero-tubal junction. The space between the proxi-al tip of the microinsert and the chorionic-sac membrane is
pproximately 10 mm, and is filled with chorion-decidualissue. An interrupted outline of the inner amniotic mem-rane can also be seen. Accompanying the ultrasound is aine drawing of the ultrasound, highlighting the spatial rela-ionships between the echogenic microinserts and the preg-ancy sacs.
At 8 weeks of gestation, one woman presented with a-day episode of light vaginal bleeding and minimal lower-bdominal pain. A diagnosis of threatened abortion was
FIGURE 2
Ultrasound scan following ET and conception. (A) Tragestation shows the gestational sac, which containstraverse the gravid uterus in the region of the intramumicroinserts and the pregnancy sac is approximatelydrawing highlights the spatial relationships between tThe arrows in (A) and (B) indicate the locations of the
Kerin. IVF pregnancy after Essure® sterilization. Fertil Steril 2007.
ade. The antenatal course proceeded normally until 31 o
ertility and Sterility�
eeks of gestation, when a diagnosis of “irritable uterus”as made. There was no cervical dilatation or shortening,
nd the symptoms resolved without need for tocolytic med-cation. The antenatal course of the other pregnancy wasormal.
Both women went into spontaneous labor. The first wentnto labor at 37 weeks of gestation, and had a spontaneousaginal delivery of a healthy female infant weighing 2.8 kg.he second had a spontaneous vaginal delivery, at 39 weeks,f a 3.1-kg healthy female infant. Both women had a pelvicltrasound assessment at 6 weeks postpartum that demon-trated that the echogenic microinserts maintained their cor-ect position in the area of the intramural tube, withoutvidence of distortion or movement.
ISCUSSIONo the best of our knowledge, this is the first report ofuccessful IVF pregnancy outcomes after performance of thessure procedure for the purpose of sterilization. The use of
his microinsert to seal off a hydrosalpinx, prior to IVF andT followed by the birth of twins to a previously infertileoman, was also described (6). As women and cliniciansecome aware that a less invasive option of female steriliza-ion is now available, its performance will become moreidespread. However, there will inevitably be a small num-er of women who will wish to have further children because
erse, transvaginal ultrasound image at 11 weeks ofble fetus. The left and right echogenic microinserts
tubes. The gap between the proximal ends of themm wide, and contains placental tissue. (B) A linechogenic microinserts and the pregnancy sacs.
croinserts.
nsva viaral10he emi
f unexpected life events.
1212.e3

cipsthpn
plwctpacssutflmhsbe
scnwatfi
cmwesqpbl
tnpttPtmf
R1
2
3
4
5
6
7
Careful presterilization counseling, thorough informedonsent, and an emphasis that this hysteroscopic method isrreversible will reduce the risk of regret, but will not com-letely eliminate it. Leading risk factors for strong regret andubsequent IVF request after female sterilization were iden-ified as age �30 years, having �2 children, and a desire toave a child with a new partner (7). One patient in theresent study was �30 years of age, and both patients hadew partners who had not previously fathered children.
Although this study contains observations on only tworegnancy outcomes, some useful information and guide-ines can be provided and used as a reference point fromhich further clinical experience can be evaluated. Clini-
ians commonly ask if the microinsert coils left trailing intohe uterine cavity following placement should be cut offrior to IVF and ET, with the use of a hysteroscopic graspernd scissors technique. This procedure is technically diffi-ult, and would leave a sharp edge which may traumatize theurrounding endometrium, and is best avoided. Furthermore,econd-look hysteroscopic observations showed that a grad-al tissue encapsulation of the trailing coils occurs (1), andhat the microinsert is biocompatible and induces a nonin-ammatory benign tissue response (4). In our opinion, theicroinsert is best left undisturbed. In the present report, a
ysteroscopy performed 3 months prior to IVF procedureshowed, on both occasions, that most of the trailing coils hadeen encapsulated, and that an average of one coil was leftxposed.
In the presence of these microinserts, ET followed byuccessful implantation occurred in 2 out of 3 IVF treatmentycles. Ultrasound evaluation in the first trimester of preg-ancy showed that the proximal segments of the microinsertsere a significant distance from the pregnancy membranes,
nd separated from them by �10 mm of chorion-decidualissue. The pregnancy outcomes in both cases were success-ul. The episode of threatened abortion and “irritable uterus”
n one of the women could have been coincidental or asso-1212.e4 Kerin and Cattanach IVF pregnancy after Essure® ster
iated with the microinsert. Since both conditions are com-on events during pregnancy, a large, case-controlled studyould be necessary to differentiate between such chance
vents and an association. Although these preliminary ob-ervations are reassuring, further case studies will be re-uired to determine if the presence of these microinsertsoses any risk of implantation failure, early pregnancyleeding, abortion, infection, premature labor, or other prob-ems during pregnancy.
Another positive observation resulting from this study ishe apparent preservation of microinsert location after preg-ancy. Despite the major uterine growth associated withregnancy, postpartum ultrasound assessments demonstratedhat the microinserts maintained their prepregnancy utero-ubal location without evidence of movement or distortion.reliminary evidence indicates that the uterine presence of
he Essure microinsert, used for transcervical sterilization,ay be compatible with successful pregnancy outcomes
ollowing IVF and ET procedures.
EFERENCES. Kerin JF, Cooper JM, Price T, Van Herendael B, Cayuela-Font E, Cher
D, et al. Hysteroscopic sterilization using a micro-insert device: resultsof a phase II study. Hum Reprod 2003;18:1223–30.
. Cooper JM, Carignan CS, Cher D, Kerin JF. Micro-insert non-incisionalhysteroscopic sterilization. Obstet Gynecol 2003;102:59–67.
. Kerin JF, Carignan CS, Cher D. The safety and effectiveness of a newhysteroscopic method for permanent birth control: results of the firstEssure PBC clinical study. Aust N Z J Obstet Gynaecol 2001;41:364–70.
. Valle RF, Carignan CS, Wright TC. Tissue response to the STOPmicrocoil transcervical permanent contraceptive device: results from apre-hysterectomy study. Fertil Steril 2001;76:974–80.
. Kerin JF. New methods for transcervical cannulation of the fallopiantube. Int J Gynaecol Obstet 1995;51(Suppl 1):29–39.
. Rosenfield RB, Stones RE, Coates A, Matteri RK, Helsa JS. Proximalocclusion of hydrosalpinx by hysteroscopic placement of microinsertbefore in vitro fertilization-embryo transfer. Fertil Steril 2005;83:1547–50.
. Kariminia A, Saunders DM, Chamberlain M. Risk factors for strongregret and subsequent IVF request after having tubal ligation. Aust N Z J
Obstet Gynaecol 2002;42:5:526–9.ilization Vol. 87, No. 5, May 2007

Cbadoscfip
rtCdp
ndr
RR
CASE REPORTS
0d
Serum total testosterone levels in a patient with lateonset 21-hydroxylase deficiency and a twin gestationLindsay M. Mains, M.D.,a Ruth B. Lathi, M.D.,b Richard O. Burney, M.D., M.Sc.,b
and Michael H. Dahan, M.D.b
a Department of Obstetrics and Gynecology, Ochsner Clinic Foundation, New Orleans, Louisiana and b Division ofReproductive Endocrinology, Stanford University School of Medicine, Stanford, California
Objective: To present serum androgen levels during pregnancy in a twin gestation complicated by maternal lateonset 21-hydroxylase deficiency.Design: Case report.Setting: University teaching hospital reproductive endocrinology and infertility practice.Patient(s): A 27-year-old with nonclassic 21-hydroxylase deficiency and infertility, twin female fetuses, andelevated androgens.Intervention(s): Steroid replacement.Main Outcome Measure(s): Serum T and 17-hydroxyprogesterone (17-OHP) levels.Result(s): Elevated androgen levels persisted throughout pregnancy in spite of aggressive steroid replacement.However, twin girls were born without any evidence of virilization.Conclusion(s): The changes associated with a twin gestation may result in excessive stimulation of androgens inmothers with nonclassic 21-hydroxylase deficiency. However, the increased placental aromatase providesprotection. (Fertil Steril� 2007;87:1212.e5–8. ©2007 by American Society for Reproductive Medicine.)
Key Words: Congenital adrenal hyperplasia, testosterone, twins, hyperandrogenism, pregnancy, 21-hydroxylasedeficiency
hwit
intnev0(
wmcP(He
p
ongenital adrenal hyperplasia (CAH) is an inherited meta-olic disorder caused by impaired cortisol synthesis in thedrenal cortex. Between 90% and 95% of CAH is caused by aeficiency of the enzyme 21-hydroxylase. This leads to a lackf negative glucocorticoid feedback on the hypothalamus, re-ulting in an increase in corticotropin, hyperplasia of adrenalortex, and androgen excess. Late onset 21-hydroxylase de-ciency has a prevalence of 1%–3%, and women typicallyresent with hirsutism and anovulation (1).
Although CAH is associated with subfertility, advancedeproductive technologies have facilitated pregnancies inhese patients. However, experience with pregnancy in theAH population is limited. Therefore, interpretation of an-rogen levels and monitoring of disease progression duringregnancy is currently a challenge (2, 3).
Elevated androgen levels in pregnancy can have pro-ounced adverse effects on female offspring. Excessive an-rogen exposure between 7 and 12 weeks of gestation canesult in ambiguous genitalia (4). After this period, labial
eceived April 17, 2006; revised and accepted July 17, 2006.eprint requests: Michael H. Dahan, M.D., Division of Reproductive En-docrinology and Infertility, Department of Obstetrics and Gynecology,300 Pasteur Dr. Stanford, CA 94305-5317 (FAX: 650-723-7737; E-mail:
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.07.1545 Copyright ©2007 American Societ
ypertrophy or clitoromegaly can result (4). The gestationalindow during which exposure to excess androgen can
mpact neurologic development is not known but may extendhroughout pregnancy (5).
Several studies have shown that maternal androgen levelsn a normal pregnancy are significantly higher than in theongravid state. Total T reaches values in the nonpregnantumor range during the second and third trimesters (�200g/dL and �400 ng/dL) (6–8). Free T is also markedlylevated by the third trimester with one study reportingalues of 3.04 � 0.24 ng/dL (normal nonpregnant levels.7–2.0 ng/dL) (6–8). Fetal levels of T and androstenedioneA) correlate with maternal serum levels (8).
In pregnancy the elevation in androgens is not associatedith maternal or fetal virilization due to several compensatoryechanisms. These mechanisms include the presence of pla-
ental aromatase (8), the competition for androgen receptors by(8), and the elevation in sex hormone-binding globulin
SHBG) resulting in a decrease in percentage of free T (7, 8).owever, these mechanisms may not be sufficient to always
xplain the lack of fetal symptomatology (8).
Management of CAH during pregnancy to prevent hy-erandrogenic effects on the female fetus has not been well
tudied. Worsening hyperandrogenism in obstetric patients1212.e5Fertility and Sterility� Vol. 87, No. 5, May 2007y for Reproductive Medicine, Published by Elsevier Inc.

wcap
gdlapa
CAhwhn
thwcdth
n6
(wowjltwn
anpoonand
(rh4
ith CAH, particularly during the first trimester, is cause foroncern and creates two main challenges for the clinician:dequate adrenal suppression and accurate counseling of theatient about the effect on the unborn female fetus.
We present a patient with late onset CAH and a twinestation who developed symptoms of worsening hyperan-rogenism in the first trimester of pregnancy. This is be-ieved to be the first reported case of androgenic changes in
late onset CAH patient with a twin gestation. Serum Teaked at 504 ng/dL and remained elevated in spite ofggressive treatment with exogenous steroids.
ASE REPORT27-year-old gravida zero, East Indian patient with a
istory of late onset CAH presented to her gynecologistith 2 years of infertility and amenorrhea. The subjectad a normal hysterosalpinogram, and her husband had aormal semen analysis.
The patient was homozygous for the 21-hydroxylase muta-ion, carrying one allele with an altered copy of intron 2 andaving a second allele with A/C replaced by a G. Her husbandas negative for CAH gene mutations. Her CAH had been
ontrolled since her diagnosis at age 16 years with 0.25 mg ofexamethasone taken nightly. Prepregnancy laboratory evalua-ion while treated with steroid replacement revealed a 17-ydroxyprogesterone (17-OHP) of 51 ng/dL (normal �285
FIGURE 1
Serum total testosterone as a function of gestational
Mains. Testosterone levels in a CAH pregnancy. Fertil Steril 2007.
1212.e6 Mains et al. Testosterone levels in a CAH pregnancy
g/dL), total T of 41 ng/dL (normal �100 ng/dL), and free T of.3 pg/mL (normal range 0.6–6.8 pg/mL).
The patient underwent three cycles of clomiphene citrateCC), days 3–7 of the menstrual cycle, at increasing dosesith each subsequent cycle (50 mg, 100 mg, 150 mg) andne cycle of letrozole, 5 mg daily, also taken cycle days 3–7,ithout ovulation. She was subsequently managed with in-
ections of recombinant gonadotropins, which induced fol-iculogenesis and intrauterine insemination (IUI). During thehird cycle of gonadotropins the patient became pregnantith dichorionic diamniotic twins. Dexamethasone 0.25 mgightly was continued with the pregnancy.
At 5 weeks gestation the subject complained of worseningcne and hirsutism. Steroid replacement was changed to pred-isone 5 mg daily. These symptoms persisted throughout herregnancy despite aggressive treatment with increasing dosesf steroids. Ovarian thecoma and adnexal mass were both ruledut by ultrasound. An adrenal mass was ruled out by mag-etic resonance imaging (MRI). The serum DHEAS levelt 5 weeks of pregnancy was 202 �g/dL (normal nonpreg-ant range 65–380 �g/dL). Serum total T values assayeduring the pregnancy can be seen in Figure 1.
At 6 weeks gestation total T (504 ng/dL) and 17-OHP2,150 ng/dL) peaked. Free T was 4 ng/dL (nonpregnantange 0.7–2.0 ng/dL). At 7–9 weeks of gestation the patient’sirsutism continued to worsen. Total T remained in the00–500 ng/dL range but 17-OHP decreased from 2,150 to
.
ageVol. 87, No. 5, May 2007

5w8ewmf
nSn1
atwvnnam
DTaw1pgcrh
ewpigsfapiwcutat�esln
ahag
apadovpnai
uoriowTstspcunmgo
ehmerFpplpifa
R1
2
F
60 ng/dL and free T was 2.9 ng/dL. The prednisone doseas increased at 7 weeks of gestation to 7.5 mg daily and atweeks of gestation, to 10 mg every morning and 5 mg
very evening. At 10 weeks of gestation her T declined,hen she was switched to hydrocortisone, 10 mg everyorning and 15 mg every evening. Amniocentesis diagnosed
emale twins.
At 27 weeks of pregnancy, despite serum total T being in theormal range for gestational age, her hirsutism again worsened.erum total T was 250 ng/dL, and serum 17-OHP was 1,370g/dL. At 29 weeks, her hydrocortisone dose was increased to5 mg every morning and 20 mg every evening.
At 36 weeks the patient presented in labor and underwentcesarean section for nonvertex presentation. She delivered
wo viable female infants weighing 2,545 g and 2,359 g, bothith apgars 8 and 9. Neither infant showed any evidence ofirilization. At 5 months postpartum total T (16 ng/dL,ormal �100 ng/dL) and 17-OHP (15 ng/dL, normal �285g/dL) normalized on the pregnancy dose of hydrocortisone,nd the patient was switched back to dexamethasone 0.25g daily without increase in her serum androgens.
ISCUSSIONhe gestational changes in steroid levels complicate thessessment of adrenal androgen excess in pregnant womenith CAH. The CAH control is normally monitored with7-OHP levels. Monitoring of disease progression duringregnancy is difficult as 17-OHP may not be reliable duringestation (7). Case series of patients with CAH who con-eive have revealed that virilization of female offspring isare, with a single case reported where the mother stoppeder steroid replacement during pregnancy (3, 4).
The patient presented here was found to have markedlylevated total and free T levels in the first trimester withorsening symptoms of hyperandrogenism despite goodrepregnancy control and compliance with the medical reg-men. The source of her elevated androgens is not clear. Theraphic representation of serum total T, depicted in Figure 1,eems to resemble early pregnancy corpus luteum (CL)unction with a peak at 8–10 weeks of gestation followed by
decline as placental function takes over, suggesting aossible ovarian origin. The elevated 17-OHP suggested thatnadequate glucocorticoid suppression of adrenal androgensas the etiology. However, the normal endocrinologic
hanges associated with pregnancy may have also contrib-ted to this elevation, specifically placental �-hCG stimula-ion of the LH receptor on the ovarian thecal cells and thedrenal gland resulting in an increase in androgenesis. Herwin gestation was likely associated with higher levels-hCG than a singleton pregnancy, thus resulting in anxaggerated elevation in androgens. Alternatively, ovariantimulation prepregnancy leads to multiple CL, which couldead to increased ovarian steroidogenesis during early preg-
ancy. Although infertility patients who conceive with theertility and Sterility�
ssistance of gonadotropins do not present with worseningirsutism and acne, evidence is lacking of early pregnancyndrogen levels in individuals with CAH who underwentonadotropin ovarian stimulation.
The subject was aggressively treated with steroids in anttempt to normalize serum T levels, which was not accom-lished until the third trimester. Despite exposure to elevatedndrogens between 7 and 12 weeks during external genitaliaevelopment, the twin girls were born without any evidencef virilization. The principal method of protection from fetalirilization in a normal pregnancy is thought to be thelacental aromatization of androgens to estrogens (8). It isot known at what T level the capacity of the placentalromatase system is exceeded, but that level may be highern a twin gestation due to increased placental volume.
The improved prognosis for fertility in women with CAHnderscores the need for further attention to the managementf pregnancy in these patients. Attention to glucocorticoidegulation of adrenal androgen excess during pregnancy ismportant, particularly when the fetus is female. The case ofne virilized female offspring delivered by a CAH patientho was not adequately suppressed emphasizes this point.he extent to which adrenal androgen production should beuppressed during pregnancy is not clear. The recommenda-ion according to Lo et al. is to aim for adrenal androgenuppression that approximates the high normal range ex-ected for each trimester of pregnancy (1, 2). Patients withongenital adrenal hyperplasia who conceive a pregnancysually obtain adequate adrenal replacement with prepreg-ancy steroid doses. However, it is possible that these dosesay need to be greatly increased in CAH patients with twin
estations due to the increased maternal-to-�-hCG levels,varian activity, and stress.
When counseling patients about the potential effects of thelevated androgens on the unborn female fetus and the likeli-ood of such effects, it should be taken into consideration thataternal levels of androgens are higher than fetal levels. It is
xpected to have maternal T levels in the nonpregnant tumorange once the pregnancy reaches the second trimester (6–8).urthermore, although T levels may be higher among CAHatients with twin gestations, the presence of two placentas mayrovide increased protection through aromatization. Neverthe-ess, CAH patients with excessively elevated androgens duringregnancy should be counseled about possible risks to the fetus,ncluding masculinization of the female brain, and should beollowed with ultrasonography to detect the development ofmbiguous genitalia.
EFERENCES. Stewart PM. The adrenal cortex. In: Larsen PR, Kronenberg HM,
Melmed S, Polonsky KS, eds. Williams textbook of endocrinology. 10thed. Philadelphia: WB Saunders, 2003:491–551.
. Lo JC, Schwitzgebel VM, Tyrrell JB, Fitzgerald PA, Kaplan SL, ConteFA, et al. Normal female infants born of mothers with classic congenitaladrenal hyperplasia due to 21-hydroxylase deficiency. J Clin Endocrinol
Metab 1999;84:930–6.1212.e7

3
4
5
6
7
8
. Kai H, Nose O, Iika Y, Ono J, Harada T, Yabuuchi H. Femalepseudohermaphroditism caused by maternal congenital adrenal hyper-plasia. J Pediatr 1979;95:418–20.
. Grumbach MM, Ducharme JR. The effects of androgens on fetal sexualdevelopment. Fertil Steril 1960:11:157–80.
. Cohen-Bendahan CC, van de Beek C, Berenbaum SA. Prenatal sexhormone effects on child and adult sex-typed behavior: methods and
findings. Neurosci Biobehav Rev 2005;29:353–84.1212.e8 Mains et al. Testosterone levels in a CAH pregnancy
. Bammann BL, Coulam CB, Jiang NS. Total and free testosterone duringpregnancy. Am J Obstet Gynecol 1980;137:293–8.
. O’Leary P, Boyne P, Flett P, Beilby J, James I. Longitudinal assessmentof changes in reproductive hormones during normal pregnancy. ClinChem 1991;37:667–72.
. Rivarola MA, Forest MG, Migeon CG. Testosterone, androstenedione anddehydroepiandrosterone in plasma during pregnancy and at delivery: con-
centration and protein binding. J Clin Endocrinol Metab 1968;28:34–40.Vol. 87, No. 5, May 2007

ItcTeottvc
i1o1aiIoHt
RR
CASE REPORT
0d
Repeated pregnancies and live births after in vitromaturation treatmentMohammed Al-Sunaidi, M.D., Togas Tulandi, M.D., M.H.C.M., Hananel Holzer, M.D.,Camille Sylvestre, M.D., Ri-Cheng Chian, Ph.D., Seang Lin Tan, M.D., M.B.A.
McGill Reproductive Center, Department of Obstetrics and Gynecology, McGill University, Montreal, Quebec, Canada
Objective: To discuss and describe the successful treatment of women with primary infertility using in vitro maturation(IVM) of immature human oocytes resulting in repeated pregnancies and live births in the same individuals.Design: Case report.Setting: McGill Reproductive Center, Royal Victoria Hospital, McGill University.Patient(s): Six patients who underwent IVM treatment.Intervention(s): In vitro maturation and fertilization of immature human oocytes.Main Outcome Measure(s): Clinical pregnancies and live births.Result(s): We report 11 singleton and 2 twin live births as a result of IVM treatment in six women with polycysticovary syndrome.Conclusion(s): In vitro maturation of human oocytes is a novel treatment in the management of infertility. It isan effective method of conception, especially in women who have polycyctic ovaries. (Fertil Steril� 2007;87:1212.e9–12. ©2007 by American Society for Reproductive Medicine.)
Key Words: In vitro fertilization, in vitro maturation, polycystic ovaries, infertility
o
MWcpIw
o66irwcmi
imsdd
n vitro maturation (IVM) of immature oocytes is a novelreatment for infertile women, particularly those with poly-ystic ovaries (PCO) or polycystic ovary syndrome (PCOS).hese women are extremely sensitive to stimulation withxogenous gonadotropins and are at increased risk of devel-ping ovarian hyperstimulation syndrome (OHSS). In IVMreatment, immature oocytes are collected without exposinghem to gonadotropin stimulation (1). Compared with initro fertilization (IVF), IVM is therefore simpler, lessostly, and, more importantly, avoids the risk of OHSS.
The first live birth as a result of IVM following transvag-nal ultrasound–guided oocyte collection was reported in994 (1). More pregnancies were subsequently reported byther centers (2–4), but pregnancy rates through much of the990s were relatively low. In 1999 our group reported thatdministration of a single injection of hCG 36 hours beforemmature oocyte retrieval significantly improved the rate ofVM of oocytes, the final number of metaphase II oocytesbtained, and the clinical pregnancy rate per cycle (5, 6).owever, repeated IVM pregnancies from individual pa-
ients have never been reported.
eceived February 4, 2006; revised and accepted July 18, 2006.eprint requests: Seang Lin Tan, M.D., M.B.A., Department of Obstetricsand Gynecology, McGill University, Women’s Pavilion, 687 Pine Ave-nue West, Montreal, H3A 1A1 Quebec, Canada (FAX: 514-843-1496;
dE-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.07.1542 Copyright ©2007 American Societ
We report 11 singletons and 2 twin live births as a resultf IVM treatment in six women with PCOS.
ATERIALS AND METHODSe have been recording data from IVM patients into a
omputerized database since 1998. For the purpose of theresent study, data from patients who had more than oneVM clinical pregnancy were retrieved. The IVM treatmentas conducted as we have previously described (7).
In short, a baseline scan is performed between days 2 and 5f induced or spontaneous menstrual cycle and repeated on dayto 8 of the cycle. When the endometrial thickness is more thanmm, a single injection of 10,000 IU hCG is administered, and
mmature oocyte collection is performed 36 hours later. Oocyteetrieval is performed transvaginally under ultrasound guidanceith a 19-gauge single-lumen aspiration needle. Immature oo-
ytes are incubated in a culture dish containing maturationedium for 24 to 48 hours. Mature oocytes are fertilized by
ntracytoplasmic sperm injection (ICSI).
To achieve optimal endometrial growth, estradiol valerates given starting on the day of oocyte retrieval. If the endo-etrial thickness is less than 6 mm, a daily dose of 12 mg is
tarted; if 6–8 mm, a daily dose of 10 mg; and if �8 mm, aaily dose of 6 mg. Luteal support is administered from theay of ICSI with IM injections of 50 mg progesterone-in-oil
aily or 200 mg micronized progesterone (Prometrium;1212.e9Fertility and Sterility� Vol. 87, No. 5, May 2007y for Reproductive Medicine, Published by Elsevier Inc.

Spt
CCTyrvcdtacti
CTictIsfb
CTmSprefiIi
CTircr
CTttIsfi
os
CTtPocTwdat
(mmp2t
DisaiOhdeTs
c(trch1
gpPIdmd(
n
chering, Montreal, Canada) three times daily. In the case ofregnancy, estradiol valerate and progesterone supplemen-ation are continued until 12 weeks of gestation.
ASE REPORTSase 1his patient was a 27-year-old woman with infertility of 3ears duration. The etiology of the infertility was PCOS-elated anovulation and oligospermia. Past history re-ealed four cycles of ovulation induction with clomipheneitrate and intrauterine insemination (IUI). After lengthyiscussion about alternative options, the couple consentedo IVM treatment. She conceived in the first IVM cyclend delivered a healthy male infant. The second IVMycle was unsuccessful, but the third and fourth IVMreatments resulted in a delivery of a singleton and twinnfants, respectively.
ase 2his patient was a 35-year-old woman with PCOS-related
nfertility of 6 years duration. Past history revealed fourycles of ovulation induction and intrauterine insemina-ion, as well as three cycles of unsuccessful IVF. The firstVM cycle resulted in a delivery of a healthy baby. Theecond and third IVM cycles were unsuccessful. Theourth IVM cycle resulted in a delivery of another healthyaby.
ase 3his 29-year-old patient had infertility due to PCOS andale factor infertility related to agenesis of the vas deferens.he previously underwent an IVF-ICSI cycle combined withercutaneous epididymal sperm aspiration (PESA), whichesulted in a first-trimester miscarriage. Subsequent frozenmbryo transfer was without success. She conceived in therst IVM cycle and delivered a healthy baby. The secondVM cycle was also successful, and she delivered twinnfants at term.
ase 4his patient was a 30-year-old woman with anovulatory
nfertility due to PCOS who had failed to respond to lapa-oscopic ovarian drilling and three IVF cycles. The first IVMycle was unsuccessful, whereas the second and third cyclesesulted in deliveries of healthy infants.
ase 5his patient was a 27-year-old woman with secondary infer-
ility of 5 years duration and who had failed to conceive afterhree cycles of superovulation with clomiphene citrate andUI. She refused to undergo gonadotropin treatment and wasubsequently treated with IVM. She did not conceive in the
rst cycle, but the second cycle was followed by a delivery i1212.e10 Al-Sunaidi et al. Repeated pregnancies and live birth
f a singleton baby. The third IVM treatment led to anotheringleton pregnancy and a delivery of a healthy baby.
ase 6his patient was a 27-year-old woman who had been trying
o conceive for 2 years. The cause of her infertility wasCOS-related anovulation and nonobstructive azoospermiaf her male partner. The couple was treated with IVMombined with testicular sperm extraction (TESE) and ICSI.he TESE failed to produce sperm, and subsequently ICSIith donor sperm was performed. The patient conceived andelivered a healthy baby. The couple subsequently returnednd was treated with another IVM cycle with donor spermhat resulted in a delivery of another healthy baby.
The dates of the IVM treatment, the antral follicle countAFC), number of germinal vesicle (GV) oocytes retrieved,atured, and fertilized, number of embryos transfered, cu-ulative embryo score, and the clinical outcome are de-
icted in Table 1. All infants were normal and healthy. Tabledemonstrates the newborns’ weight, gender, and gesta-
ional age at delivery.
ISCUSSIONn vitro maturation is a simple and successful treatment foruitable patients. This treatment avoids ovarian stimulationnd the risks and costs associated with it. Most importantly,t is not associated with a risk of OHSS. The incidence ofHSS, especially in young women with PCO, could be asigh as 6% (8, 9). Although many strategies have beeneveloped to predict and prevent this potentially life-threat-ning complication, none has been unequivocally successful.he only reliable method to prevent OHSS is to avoidtimulation with FSH (10).
Since the first reported pregnancy, IVM has been underontinuous evolution. The implantation rate was initially low3, 4). However, the rates significantly improved by priminghe immature oocytes with hCG prior to retrieval (5, 6). Inecent years, clinical pregnancy rates exceeding 35% perycle with implantation rates of almost 15% per embryoave been reported in women less than 35 years of age (5, 6,1).
Cha et al. (12) reported that the miscarriage rate, length ofestation and birth weight of the infants, and obstetric com-lications of pregnancies conceived by IVM in women withCOS were comparable to those treated by conventionalVF. We recently reported that the mean gestational age atelivery, the obstetric outcomes, and the rate of congenitalalformations after IVM treatment were not significantly
ifferent from those in women who spontaneously conceived13).
The IVM success rates are obviously correlated with theumber of GV oocytes collected. Patients in whom the AFC
s high will have more GV oocytes, more embryos availables after IVM Vol. 87, No. 5, May 2007

fTur
ctc
ccptd
pphsf
stw
R
F
or transfer, and eventually a higher pregnancy rate (14).herefore the ideal candidates for IVM are women withltrasound findings of PCO. All the patients in the presenteport had PCO. Gonadotropin stimulation in these patients
TABLE 1Number of antral follicle counts (AFC), number onumber of embryos transfered, cumulative embrwho had repeated pregnancies after in vitro mat
Case. no. No. cycle Date of IVMInitial age
(yrs) No. AFC Day of hCG
1 1 May ’99 27 45 132 Oct. ’01 103 Feb. ’02 84 Feb. ’05 10
2 1 Jan. ’99 35 22 82 July ’00 73 June ’02 94 Mar. ’03 9
3 1 Jan. ’00 29 21 92 Jan. ’02 7
4 1 Oct. ’98 30 20 82 Nov. ’98 113 Nov. ’00 10
5 1 Jan. ’01 27 37 92 Nov. ’02 103 May. ’05 10
6 1 May. ’03 27 40 102 Mar. ’05 9
Note: GV � germinal vesicle.
Al-Sunaidi. Repeated pregnancies and live births after IVM. Fertil Steril 2007.
TABLE 2Profile of the newborns of the mother whoconceived after in vitro maturationtreatment.a
Casenumber
Gestationalage (wks) Weight (g) Gender
1 39 3719 Male40) 4082 Female
37 (twin) 2812, 2630 Male,Male
2 39 3492 Female38 3628 Female
3 38 3583 Female37 (twin) 3265, 3084 Male,
Female4 39 3356 Male
40 3175 Female5 40 4173 Male
39 3674 Female6 40 2902 Male
39 2812 Femalea All babies are healthy and normal.
Al-Sunaidi. Repeated pregnancies and live births after IVM. Fertil Steril
2007.ertility and Sterility�
arried a considerable risk for developing OHSS. Instead,hey underwent a simple treatment with fewer risks andosts.
The initial success in conceiving and delivering a healthyhild in our patients encouraged both the couples and us tohoose IVM again as the treatment of choice for subsequentregnancy. Indeed, the repetitive success of these six pa-ients establishes IVM as a treatment that results in repro-ucible success in the same patients.
It should be noted that three of the present patients hadreviously failed to conceive after IVF. Two of them hadroduced a suboptimal response to ovarian stimulation andad produced a high number of poor-quality embryos. Thisuggests that IVM may be offered as an appropriate therapyor a small number of patients who have failed IVF cycles.
We conclude that IVM may be an effective treatment forome women, especially those with a high AFC. It can leado repetitive success and may be effective in some womenho have failed IVF treatment.
EFERENCES1. Trounson A, Wood C, Kausche A. In vitro maturation and the
fertilization and developmental competence of oocytes recoveredfrom untreated polycystic ovarian patients. Fertil Steril 1994;62:353– 62.
2. Barnes FL, Crombie A, Gardner DK, Kausche A, Lacham-Kaplan O,Suikkari AM, et al. Blastocyst development and birth after in-vitromaturation of human primary oocytes, intracytoplasmic sperm injectionand assisted hatching. Hum Reprod 1995;10:3243–7.
3. Barnes FL, Kausche A, Tiglias J, Wood C, Wilton L, Trounson A.Production of embryos from in vitro–matured primary human oocytes.
cytes retrieved, matured, and fertilized,core (CES), and clinical outcome in six patientsion treatment.
Vested
No. eggsmatured
No. eggsfertilized
No. embryostransfered CES Outcome
8 7 3 56 Single live birth16 9 4 92 No pregnancy11 6 4 50 Single live birth17 17 4 120 Twin live birth5 4 4 50 Single live birth6 4 4 48 No pregnancy6 5 4 96 No pregnancy6 4 3 43 Single live birth8 5 3 39 Single live birth
13 5 4 48 Twin live birth2 2 2 14 No pregnancy8 7 3 48 Single live birth
11 10 4 87.5 Single live birth13 13 4 92 Biochemical pregnancy25 17 6 75 Single live birth16 11 6 93 Single live birth14 5 4 79 Single live birth17 14 4 66.5 Single live birth
f ooyo surat
No. Goocyt
collec
1028222910129
1010183
10181436391727
Fertil Steril 1996;65:1151–6.
1212.e11

1
1
1
1
1
4. Trounson A, Anderiesz C, Jones GM, Kausche A, Lolatgis N, Wood C.Oocyte maturation. Hum Reprod 1998;13:52–62.
5. Chian RC, Gulekli B, Buckett WM, Tan SL, Priming with humanchorionic gonadotropin before retrieval of immature oocytes in womenwith infertility due to the polycystic ovary syndrome. N Engl J Med1999;341:1624–6.
6. Chian RC, Buckett WM, Tulandi T, Tan SL. Prospective randomizedstudy of human chorionic gonadotrophin priming before immatureoocyte retrieval from unstimulated women with polycystic ovariansyndrome. Hum Reprod 2000;15:165–70.
7. Rao GD, Tan SL. In vitro maturation of oocytes. Semin Reprod Med2005;23:242–7.
8. MacDougall MJ, Tan SL, Balen A, Jacobs HS. A controlled studycomparing patients with and without polycystic ovaries undergoingin-vitro fertilization. Hum Reprod 1993;8:233–7.
9. Brinsden P, Wada I, Tan SL, Balen A, Jacobs HS. Diagnosis, preven-tion and management of ovarian hyperstimulation syndrome. Br J
Obstet Gynecol 1995;102:767–72.1212.e12 Al-Sunaidi et al. Repeated pregnancies and live birth
0. Orvieto, R. Can we eliminate severe ovarian hyperstimulation syn-drome? Hum Reprod 2005;20:320–2.
1. Chian RC. In-vitro maturation of immature oocytes for infertile womenwith PCOS. Reprod Biomed Online 2004;8:547–52.
2. Cha KY, Chung HM, Lee DR, Kwon H, Chung MK, Park LS, et al.Obstetric outcome of patients with polycystic ovary syndrome treatedby in vitro maturation and in vitro fertilization–embryo transfer. FertilSteril 2005;83:1461–5.
3. Buckett WM, Chian R, Holzer H, Usher R, Tan SL. Congenitalabnormalities and perinatal outcome in pregnancies following IVM,IVF, and ICSI delivered in a single center; 61st Annual Meeting ofthe American Society for Reproductive Medicine, Montreal, Can-ada, Abstract O-196. Fertil Steril 2005;84 Suppl 1:S80 –1.
4. Tan SL, Child TJ, Gulekli B. In vitro maturation and fertilization ofoocytes from unstimulated ovaries: predicting the number of immatureoocytes retrieved by early follicular phase ultrasonography. Am J
Obstet Gynecol 2002;186:684–9.s after IVM Vol. 87, No. 5, May 2007

Occiacot
stcpeaa
R
R
CASE REPORT
0d
A new approach to preserve fertility by using a coatednitinol stent in a patient with recurrent cervical stenosisDorothee Grund, M.D.,a Christhardt Köhler, M.D.,a Holger Krauel, M.D.,b
and Achim Schneider, M.D., M.P.H.a
a Department of Gynecology, Charité–Universitätsmedizin Berlin, Berlin; and b Department of Medicine, Asklepios KlinikenWeissenfels-Hohenmölsen, Weissenfels, Germany
Objective: The incidence of hematometra caused by cervical stenosis after conization is �1%. Nevertheless, ifdilatation was unsuccessful, further therapy often remains unclear, and the clinical consequences can be severe,including hysterectomy.Design: Case report.Setting: University hospital.Patient(s): A 33-year old patient who developed recurrent cervical stenosis with consecutive hematometra aftertwo conizations during lactation amenorrhea that could not be treated by dilatation and insertion of a temporaryplastic catheter according to the manufacturer’s instructions.Intervention(s): Insertion of a coated nitinol stent in the cervical canal after dilatation and hysteroscopic removalof the hematometra.Main Outcome Measure(s): Normal menstruation, future pregnancy.Result(s): The patient was free of symptoms, had a normal menstruation, and has become pregnant.Conclusion(s): The insertion of a coated vessel stent in the uterine cervix appears to be a valid alternative inpatients with recurrent cervical stenosis and hematometra after conization to preserve childbearing function.(Fertil Steril� 2007;87:1212.e13–16. ©2007 by American Society for Reproductive Medicine.)
Key Words: Hematometra, cervical stenosis, laser conization, coated stent
skg
CA(ccndcs
anhflctt
ne of the well-known complications after cervicalonization is stenosis of the cervix. Complete occlusionombined with hematometra, however, is rare and occursn �1% of all conizations. Nevertheless, among those it is
severe complication that may lead to abdominal pain,ramping, fertility problems, and uterine infections. If allther options fail, even hysterectomy is recommended tohese patients.
Effective and reliable treatment options for high-gradetenosis after conization are not available to date. Use of aemporary indwelling plastic stent, placed in the cervicalanal and sutured to the cervical wall after dilatation torevent a new postoperative stenosis, has been discussedlsewhere (1). However, these stents have to be removedfter 1 or 2 weeks. Cervical stenosis can occur again, alsofter periods of normal menstruations.
eceived May 14, 2006; revised September 25, 2006; accepted October11, 2006.
eprint requests: Achim Schneider, M.D., M.P.H., Department of Gynecol-ogy, Charité Universitätsmedizin Berlin, Campus Benjamin Franklin, 12200Berlin, Germany (FAX: 49-30-84454477; E-mail: achim.schneider@
ccharite.de).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.10.008 Copyright ©2007 American Society
Different types of stents are used in urology, vascularurgery, intervention radiology, or gastroenterology. To ournowledge, the use of the self-expanding metal stent inynecology has never been described before.
ASE REPORT33-year-old woman was diagnosed with Papanicolaou
PAP) IVa and IVb 3 months after giving birth to a child viaesarean section. The patient underwent laser conization andurettage. During these procedures, a cervical intraepithelialeoplasia grade III lesion with non in sano resection wasiagnosed. Three months later, reconization and cervicalurettage were performed. Histology revealed a circum-cribed, completely resected adenocarcinoma in situ.
Meanwhile, the patient was breastfeeding and thereforemenorrheic. After weaning, she developed severe abdomi-al cramping without any bleeding. Cervical stenosis andematometra were diagnosed with ultrasound: the ante-ected uterus showed an intrauterine hematometra of 6 � 3m. The patient underwent cervical dilatation that indicatedhe cervical canal to be completely blocked. After dilatation,he hematometra was evacuated. In this session, a laparos-
opy was performed to confirm hematosalpinx.1212.e13Fertility and Sterility� Vol. 87, No. 5, May 2007for Reproductive Medicine, Published by Elsevier Inc.

aTiw
eFTa
hdcew
oncswlw(
fpTpodcsCm
gg2cafscTnr
occtTdows
At the time of the expected next menstruation, the patientgain developed abdominal cramping without any bleeding.he operative procedure was repeated with the additional
nsertion of a Fehling catheter into the cervix. The catheteras removed 4 days later. This time, no biopsy was taken.
Four weeks later, the patient had similar symptoms. Op-ration (dilatation of the cervical canal and insertion of aehling catheter) was repeated under hysteroscopic control.he dilatation was to Hegar 7. This time, the patient receivedntibiotic prophylaxis.
After the removal of the Fehling catheter, the patient againad abdominal pain and cramping. For a third time, a cervicalilatation was tried but was aborted because two cervix-likeanals were detected and neither could be dilatated properly,ven under ultrasonographic control. At this time, hysterectomyas recommended to the patient.
When we saw the patient initially, we found a totallyccluded and shortened residual cervix. On magnetic reso-ance imaging, the uterus was enlarged up to a length of 10m and a maximal diameter of 4.5 cm proximal to thetenosis in the cervical canal. The total length of the cervixas 4 cm, and the stenotic area of the cervix was 1.5 cm
ong. Uterus and cervix were filled with blood. The ovariesere normal, but hematosalpinx was found on both sides
Fig. 1).
FIGURE 1
Preoperative magnetic resonance imaging of thepelvis demonstrates hematometra andhematocervix.
aGrund. Use of vessel stents in cervical stenosis. Fertil Steril 2007.
1212.e14 Grund et al. Use of vessel stents in cervical stenosis
Because of the patient’s very strong wish to preserveertility, we discussed with her several options such as re-eated conization, cervicoplastic, and insertion of a stent.he patient was informed about the lack of reliable data andossible complications like infection, dislocation, and failuref the planned treatment. In consent with the patient, weecided to dilate the cervical canal and insert a self-expanding,oated nitinol stent used in interventional radiology for thetenting of vessels. The stent (Symphony; Boston Scientificorporation, United Kingdom) was 6 mm in diameter and 40m in length (Fig. 2).
The external os of the uterine cervix was fixed with tworasping forcipes and dilated to Hegar 10 under ultrasono-raphic control (Fig. 3). After evacuation of approximately0 mL of old blood, the uterus was examined hysteroscopi-ally, and the cavum of the uterus was irrigated. The cavumppeared normal on hysteroscopy. Taking into account theormer histological finding of adenocarcinoma in situ, biop-ies from the posterior cervical wall were taken, and cervicalurettage was performed. Specimens were sent to pathology.he stent was inserted by using its self-expanding mecha-ism, and it was fixed to the external cervical os with threeesorbable sutures (Fig. 4).
The localization of the stent was controlled each of post-perative days 1 to 4 by abdominal sonography (Fig. 5). Itsorrect function was confirmed by vaginal bleeding, whichontinued for 1 week. The patient did not show any symp-oms of hematometra, such as cramping or abdominal pain.o prevent infection, antibiotic prophylaxis was given for 5ays. The patient was instructed to measure her vaginal pHn her own every day and to see her gynecologist if thereere any changes in vaginal discharge. The following men-
truation happened 35 days after surgery and did not cause
FIGURE 2
Stent in comparison with a match.
Grund. Use of vessel stents in cervical stenosis. Fertil Steril 2007.
ny pain or disorders.
Vol. 87, No. 5, May 2007

pwtw
DTcps
ecSsm
sbri
mps
viitsdmftro
pitpc
o
F
After 9 months, the stent was removed without any com-lications. At first the patient had a normal menstruationithout any complications. Two months after the removal of
he stent, the patient became pregnant. Up to the time of thisriting, there have not been any problems during pregnancy.
ISCUSSIONhe incidence of hematometra after stenosis of the cervicalanal as a result of conization is a rare event (�1%), de-ending on the method used (2, 3). Baldauf et al. (4) as-umed that cervical stenosis occurs less frequently after loop
FIGURE 3
Intraoperative abdominal ultrasound confirmscomplete evacuation of the hematometra.
Grund. Use of vessel stents in cervical stenosis. Fertil Steril 2007.
FIGURE 4
Inserted stent in the cervical canal.
Grund. Use of vessel stents in cervical stenosis. Fertil Steril 2007.
ertility and Sterility�
lectrosurgical excision procedure. Cervical stenosis mayause menstrual disorders and adversely affects fertility.ome of the women develop stenosis of the cervical canaleveral months postoperatively, after having resumed normalenstruation at first.
It is unclear whether our patient had a primary or aecondary stenosis because she was amenorrhoic whilereast feeding. After stopping breast feeding she did notesume menstruation but had dysmenorrhea without bleed-ng. Shortly thereafter, the stenosis was diagnosed.
Repeated dilatation failed, and hysterectomy was recom-ended as a last resort. Because of the young age of the
atient and her very strong wish to have children, weearched for another method of uterus-preserving therapy.
In the literature, hardly any treatment modalities for cer-ical stenosis are described. Luesley et al. (1) tried to min-mize the stenosis of the residual cervix by using a temporaryndwelling plastic cervical support stent that was sutured intohe exposed cone bed immediately after excising the conepecimen and then was removed 2 weeks later. The proce-ure was performed in 33 patients. After 6 months, thisethod failed only in 6% of patients. In this study, no
ollow-up data regarding fertility are specified. All patientsreated with this method had primary stenosis. Because theate of relapse is increasing in accordance with the number ofccurred stenoses, we decided not to use this method.
Martius (5) described “metrotomia” as an operativerocedure for stenotic cervical canals that uses deep cutsn the cervix and resuturing of these incisions. Accordingo that investigator, this method may be associated withossible complications, such as infections, relapse, orervical insufficiency.
Another feasible approach is reconization, with the aim topen the cervical canal. After two former conizations for our
FIGURE 5
Postoperative ultrasound with stent.
Grund. Use of vessel stents in cervical stenosis. Fertil Steril 2007.
1212.e15

pi
budaitftPr
tRbpitt
tdsate
R1
2
3
4
5
atient, this was not an option because of the risk of cervicalnsufficiency.
Thus, inserting a permanent indwelling stent appeared toe the only practicable solution. The coated nitinol stent wesed was 6 mm in diameter and 40 mm in length. Theeployment of the stent is facilitated by its indwelling mech-nism, which opened to 6 mm. Because of its funnel, locatedn the cavum of the uterus, and three additional sutures onhe ectocervix, the stent could not migrate. As a safetyeature, the stent was equipped with radiopaque markers sohat it could be easily found if it did migrate. We also tied arolene string to the external end of the stent to allow itsemoval in case of pregnancy.
To ensure opening of the cervical canal, we calculate thathe stent should be maintained in position for 10 months.emoval of the stent afterwards should not be a problemecause of its coating and its noninvasive anchorage. Theersistent opening of the external os could cause uterusnfections. To prevent infection, the patient should measurehe vaginal pH every day. Up to the present, this complica-
ion has not yet been observed.1212.e16 Grund et al. Use of vessel stents in cervical stenosis
In conclusion, the use of a vascular nitinol stent forreatment of cervical stenosis of the uterus has not beenescribed previously. Insertion of a permanent coated nitinoltent designed for vascular application appears to be a validlternative in the treatment of hematometra that is secondaryo cervical stenosis after conization. Because of its self-xpanding mechanism, the stent can be placed easily.
EFERENCES. Luesley DM, Redman CW, Buxton EJ, Lawton FG, Williams DR.
Prevention of post-cone biopsy cervical stenosis using a temporarycervical stent. Br J Obstet Gynaecol 1990;97:334–7.
. Mathevet P, Chemali E, Roy M, Dargent D. Long-term outcome of arandomized study comparing three techniques of conization: cold knife,laser and LEEP. Eur J Obstet Gynecol Reprod Biol 2003;106:214–8.
. Brun JL, Youbi A, Hocke C. Complications, sequelae and outcome ofcervical conizations: evaluation of three surgical techniques. J GynecolObstet Biol Reprod 2002;31:558–64.
. Baldauf JJ, Dreyfus M, Ritter J, Meyer P, Philippe E. Risk of cervicalstenosis after large loop excision or laser conization. Obstet Gynecol1996;88:933–8.
. Martius H. Die Gynäkologischen Operationen. Leipzig, Germany: Georg
Thieme Verlag, 1942:223–4.Vol. 87, No. 5, May 2007
Sr(iaMfcf
orts
mmtaSi
RR
CASE REPORT
0d
Supernumerary minute ring chromosome 14 in a manwith primary infertility and left varicoceleBrandon C. Stahl, M.D.,a Shivanand R. Patil, Ph.D.,b Craig H. Syrop, M.D.,c
Amy E. T. Sparks, Ph.D.,c and Moshe Wald, M.D.a
Departments of a Urology, b Pediatrics, and c Obstetrics and Gynecology, University of Iowa, Iowa City, Iowa
Objective: To describe a case of supernumerary minute ring chromosome (SMRC) in an infertile man, with theconcurrent finding of a left varicocele.Design: Case report.Setting: Urologic infertility clinic in a university hospital.Patient(s): Male patient presenting with primary infertility.Intervention(s): Karyotyping, genetic counseling, and microsurgical left varicocelectomy.Main Outcome Measure(s): Sperm concentration and motility, chromosomal number and structure.Result(s): Fluorescence in situ hybridization revealing SMRC 14. Sperm concentration and motility improvedafter left varicocele repair.Conclusion(s): A karyotype should be included in the evaluation of severe oligospermia. Although SMRC 14 maybe associated with fertility problems, repair of a coexisting varicocele should be considered in these patients.(Fertil Steril� 2007;87:1213.e1–3. ©2007 by American Society for Reproductive Medicine.)
Key Words: Infertility, male, sex chromosome disorders, oligospermia, varicocele, karyotyping
CAecrt
fnn
pmenn
r7mltt
upernumerary minute ring chromosomes (SMRC) are aare finding, occurring in 3 to 4 of every 10,000 live births1, 2). This incidence is increased to 17 per 10,000 newbornsn subfertile individuals (2). There is a variable phenotypessociated with SMRC, from normal to severely abnormal.ost SMRC are seen in normal, healthy individuals and are
amilial. They can be seen in mosaic condition, that is, someells with and some cells without. The majority originaterom acrocentric chromosomes 13, 14, 15, 21, and 22.
In a review of the literature, Crolla (3) identified 25 casesf SMRC 14, of which 16% (4/25) were associated witheproductive problems. Only 1 of these, however, was iden-ified as having abnormal semen parameters, described asevere oligoasthenospermia (4).
As fluorescence in situ hybridization techniques becomeore widely used in determining possible genetic factors forale-factor infertility, the need to counsel patients regarding
he meaning of SMRC will continue to grow. Our reportdds to the existing literature of the phenotypic expression ofMRC 14 and advances the concept that this may be a factor
n male-factor infertility.
eceived June 7, 2006; revised and accepted September 19, 2006.eprint requests: Moshe Wald, M.D., Department of Urology, Universityof Iowa, 200 Hawkins Drive, 3 RCP, Iowa City, Iowa 52242-1089 (FAX:
e319-356-3900; E-mail: [email protected]).
015-0282/07/$32.00oi:10.1016/j.fertnstert.2006.09.008 Copyright ©2007 American Societ
ASE REPORT32-year-old man presented to our male-infertility clinic for
valuation of primary infertility and oligospermia after 5onsecutive years of inability to conceive with his wife. Heeported good libido and no erectile or ejaculatory dysfunc-ion, and he had fathered no prior children.
His history was remarkable for previous surgery in 1996,or right inguinal hernia repair using mesh. He was takingo medications. Complete physical examination revealedormal-appearing male genitalia.
His penis was circumcised, meatus normal, with nolaques or curvature. His testes were descended bilaterally,easuring 4.9 cm on the right and 4.3 cm on the left. His
pididymides and vasa deferentia were present and wereormal to palpation bilaterally. A small left varicocele wasoted only with the Valsalva maneuver.
His referring physician obtained a semen analysis thatevealed a semen volume of 2.1 mL, sperm concentration of.4 million per milliliter, and motility of 54%, with a totalotile sperm count of 8.4 million. A repeat sample 2 weeks
ater showed a semen volume of 1.8 mL, sperm concentra-ion of 5.5 million per milliliter, and motility of 15%, with aotal motile sperm count of 1.5 million.
Additional laboratory tests included FSH, 8.4 mIU (refer-
nce range, 1.5–12.4) and a total T level of 331 ng/dL1213.e1Fertility and Sterility� Vol. 87, No. 5, May 2007y for Reproductive Medicine, Published by Elsevier Inc.

(tAss
isc3bt[
anfpwl
ttm
swm
DAoTss
rs
hrtsm8dte
reference range, 280–800). A Y-chromosome microdele-ion assay was performed, with no microdeletions in theZFa, AZFb, or AZFc regions. Routine G-banded chromo-
ome analysis revealed a 47,XY karyotype with an extra-mall marker chromosome (Fig. 1).
Subsequent fluorescence in situ hybridization analysis us-ng centromere probe and the whole-chromosome painthowed that this small ring chromosome originated fromhromosome 14. The ring chromosome 14 was present in all0 cells analyzed. It was difficult to determine the precisereakpoint, but it appeared that it contained mostly pericen-romeric area, with breakpoints at 14p11.1 and 14q11.247,XY,�r(14)(p11.2q11.2)].
The patient then was referred for genetic counselingnd was advised that if a conception should occur, am-iocentesis should be conducted to rule out a possibleetal karyotype abnormality. It also was suggested to theatient that he obtain a karyotype of his parents to seehether this is possibly a familial abnormality and thus
ikely to be inconsequential.
In hope of improving his semen parameters, he was takeno the operating room for a microsurgical left varicocelec-omy. Five dilated veins were isolated and ligated. He had a
FIGURE 1
Karyotype demonstrating the presence of a ring chroanalysis determined the origin to be chromosome 14
Stahl. Supernumerary minute ring chromosome 14. Fertil Steril 2007.
uch-improved 3-month postoperative semen analysis, n
1213.e2 Stahl et al. Supernumerary minute ring chromosome 1
howing a sperm concentration of 15.8 million per milliliter,ith motility of 32.9% and a total motile sperm count of 19.8illion.
ISCUSSIONny male patient presenting to a urologist with a complaintf infertility with oligospermia warrants a full evaluation.his includes a complete history and physical examination,tandard laboratory tests, and genetic screening in cases ofevere oligospermia.
It is extremely difficult to establish the origin of SMRC byoutine cytogenetic analysis alone. However, fluorescence initu hybridization methods are well suited and must be used.
Seven cases with SMRC derived from chromosome 14ave been reported to be phenotypically normal, with agesanging from newborn to 21 years old (5–8). Only three ofhese were de novo. A case of de novo mosaic ring chromo-ome 14 was among a series of supernumerary small ringarker autosomes by fluorescence in situ hybridization in an
-year boy with moderate retardation, hypotonia, and speechelay (9). Callen et al. (10) described a de novo case ofrisomy 21 plus ring 14. It has been estimated that thempirical risk for abnormal phenotype associated with de
ome. Subsequent fluorescence in situ hybridization
mos.ovo SMRC is approximately 15% (11).
4 Vol. 87, No. 5, May 2007

mpalos
cftornowcic
1cswiooa
R
1
1
1
1
1
F
The frequency of chromosome abnormalities in cases ofale infertility is about 5% (12). Shi and Martin (13) re-
orted that infertile men with constitutional chromosomebnormalities have an increased frequency of chromosoma-ly abnormal spermatozoa and offspring. Men with severeligospermia showed a significantly higher frequency ofex-chromosome aneuploidy (14).
As awareness of male-factor infertility continues to in-rease, so too will the number of cytogenetic tests per-ormed, possibly leading to the detection of more SMRC inhis particular patient population. At this time, given theverall rarity of SMRC 14 and relative paucity of literatureegarding its correlation to fertility status, each case willeed to be evaluated and treated on an individual basis. Inur report, a concomitant small varicocele was detected,ith a marked improvement of semen parameters after mi-
rosurgical correction. Whether this was a phenotypic man-festation of SMRC 14 that resulted in infertility or simply aoincidental finding cannot, at this time, be determined.
For infertile male patients who are diagnosed with SMRC4, we recommend a thorough physical examination, with aareful assessment of any possible varicoceles. Patientshould be counseled that although we do not yet knowhether there is a direct cause-and-effect relationship, exist-
ng data suggest that SMRC 14 may be a factor. Treatmentptions remain limited to the existing standard treatmentptions for infertility, including a microsurgical approach tony coexisting varicoceles.
EFERENCES1. Crolla JA, Long F, Rivera H, Dennis NR. FISH and molecular study of
autosomal supernumerary marker chromosomes excluding those de-rived from chromosomes 15 and 22: I. Results of 26 new cases. Am J
Med Genet 1998;75:355–66.ertility and Sterility�
2. Liehr T, Claussen U, Starke H. Small supernumerary marker chromo-somes (sSMC) in human. Cytogenet Genome Res 2004;107:55–7.
3. Crolla JA. FISH and molecular studies of autosomal supernumerarymarker chromosomes excluding those derived from chromosome 15: II.Review of the literature. Am J Med Genet 1998;75:367–81.
4. Gentile M, Susca F, Resta N, Stella A, Cascone A, Guanti G. Infertilityin carriers of two bisatellited marker chromosomes. Clin Genet 1993;44:71–5.
5. Stetten G, Blakemore KJ, Courter AM, Coss CA, Jabs EW. Prenatalidentification of small mosaic markers of different chromosomal ori-gins. Prenat Diagn 1992;12:83–91.
6. Gravholt CH, Friedrich U. Molecular cytogenetics study of supernu-merary marker chromosomes in an unselected group of children. Am JMed Genet 1995;56:106–11.
7. Ning Y, Laundon CH, Schrock E, Buchanan P, Ried T. Prenataldiagnosis of a mosaic extra structurally abnormal chromosome byspectral karyotyping. Prenat Diagn 1999;19:480–2.
8. Starke H, Nietzel A, Weise A, Heller A, Mrasek K, Belitz B, et al. Smallsupernumerary marker chromosomes (SMCs): genotype-phenotype corre-lation and classification. Hum Genet 2003;114:51–67.
9. Daniel A, Malafiej P. A series of supernumerary small ring markerautosomes identified by FISH with chromosome probe arrays andliterature review excluding chromosome 15. Am J Med Genet A2003;117:212–22.
0. Callen DF, Eyre HJ, Ringenbergs ML, Freemantle CJ, Woodroffe P,Haan EA. Chromosomal origin of small ring marker chromosomes inman: characterization by molecular genetics. Am J Hum Genet 1991;48:769–82.
1. Warburton D. De novo balanced chromosome rearrangements and extramarker chromosomes identified at prenatal diagnosis: clinical signifi-cance and distribution of breakpoints. Am J Hum Genet 1991;49:995–1013.
2. Van Assche E, Bonduelle M, Tournaye H, Joris H, Verheyen G,Devroey P, et al. Cytogenetics of infertile men. Hum Reprod 1996;11(Suppl 4):1–24.
3. Shi Q, Martin RH. Aneuploidy in human spermatozoa: FISH analysis inmen with constitutional chromosomal abnormalities, and in infertilemen. Reproduction 2001;121:655–6.
4. Miharu N. Chromosome abnormalities in sperm from infertile men withnormal somatic karyotypes: oligozoospermia. Cytogenet Genome Res
2005;111:347–51.1213.e3

Herriasaa
ciAoccitaaed
muT(it
RWR
CORRESPONDENCE
1
Heat-shock proteins modulate the incidence ofapoptosis and oxidative stress in preimplantationmouse embryos
We investigated the effect of antibodies to heat-shock proteins 60 and 70 on development, reactive oxygenspecies production, and incidence of apoptosis in preimplantation mouse embryos. Supplementation of culturemedia with antibodies to heat-shock proteins 60 and 70 resulted in significantly lower blastocyst development,hatching rate, reduced total cell number, and trophectoderm cell number, and increased the incidence ofapoptosis in blastocysts compared to the control group. (Fertil Steril� 2007;87:1214–7. ©2007 by American
Society for Reproductive Medicine.)aHmlrmi1m3Etf
h(L�pdettwaw0Twfwd
nG
eat-shock proteins (HSPs) are a group of constitutivelyxpressed inducible proteins (1, 2) that are produced inesponse to a wide range of environmental stresses such asapid cell growth and differentiation, inflammation andnfection, toxic chemicals, and oxidative stress (3). HSPsre among the first proteins produced during embryogene-is (4, 5). Several studies have shown that Hsp70, Hsp90,nd Hsp27 protect against cell death through apoptosis byvariety of stressors including oxidative stress (6).
Oxidative stress is a result of the relatively high oxygenoncentrations in the in vitro microenvironment surround-ng preimplantation embryos that may trigger apoptosis (7).lthough apoptosis takes place as a normal part of embry-nic development to eliminate defectively differentiatedells, it is more likely to occur during in vitro embryoulture because of suboptimal conditions (8). The higherncidence of apoptosis is detrimental to blastocyst forma-ion, and leads to preimplantation embryo death (9). Theim of the present study was to determine the effect ofntibodies to HSP 60 and 70 on preimplantation mousembryo development, reactive oxygen species (ROS) pro-uction, and apoptosis.
A total of 222 normal appearing two-cell (B6C3F1ouse crossed with B6D2F1) cryopreserved embryos were
sed (Embryotech Laboratories, Inc. Wilmington, MA).he embryos were transferred to 1 mL of human tubal fluid
HTF, Irvine Scientific, Santa Ana, CA) medium contain-ng 10% serum substitute supplement (SSS, Irvine Scien-ific) and 100 �g/mL of mouse monoclonal antibodies was
eceived April 5, 2006; revised and accepted July 28, 2006.ebsite: http://www.ClevelandClinic.Org/ReproductiveResearchCentereprint requests: Rakesh K. Sharma, Ph.D., Desk A19.1, Centre forAdvanced Research in Human Reproduction, Infertility, and SexualFunction, Department of Obstetrics-Gynecology, 9500 Euclid Ave-nue, Cleveland, Ohio 44195 (FAX: 216-445-6049; E-mail:
214 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
dded to either HSP60 (SPA-806, isotype IgG1; n � 51) orSP70 (SPA-820, isotype IgG1; n � 46). Because theonoclonal anti-HSP antibodies belong to immunoglobu-
in G1 (IgG1) subclass, HTF–SSS supplemented with pu-ified monoclonal mouse IgG1 was used as a control im-unoglobulin (n � 54). Embryos simultaneously cultured
n HTF–SSS were used as control (n � 71). Groups of 8 to0 embryos were randomly added to 1 mL of cultureedium in center-well culture dishes and incubated at
7°C under a humidified atmosphere of 5% CO2 in air.mbryos were monitored daily for cleavage, fragmenta-
ion, regularity of blastomeres, compaction, and cavitationor 72 hours.
Levels of ROS in culture media were measured after 24ours, 48 hours, and 72 hours by a Berthold luminometerAutolumat LB 953, Wallace Inc., Gaithersburg, MD) (10).evels of ROS were recorded for 15 minutes, expressed as104 counted photons per minute (cpm). To detect apo-
tosis, individual embryos were stained by the terminaleoxynucleotidyl transferase (TdT)-mediated dUTP nicknd labeling (TUNEL) technique (in situ cell death detec-ion system; Roche Diagnostic GmbH, Germany). To dis-inguish apoptosis from necrosis, embryos were stainedith 20 �g/mL propidium iodide, a membrane-imperme-
ble stain that is excluded from viable cells. Embryos wereashed three times in phosphate-buffered saline containing.3% polyvinyl pyrrolidone, and permeabilized in 0.5%riton X-100 on ice for 2 minutes. The embryos wereashed and incubated in TUNEL reaction cocktail at 37°C
or 1 hour in the dark. Total blastomere count per embryoas determined by staining with bisbenzimide (Hoechstye 33258).
Images were collected with a Leica TCS-SP2 laser scan-ing spectral confocal microscope (Leica LasertechnikmbH, Heidelberg, Germany). Each optical section of the
lastocyst was analyzed for total number of nuclei, necrotic0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.07.1536

bcb
dmwetscdgs
wpa8brhctwaIHa
sv
cmScHIwst
Hhg
slaoasccwb
Fe
lastomers, and number of TUNEL-labeled nuclei in innerell mass (ICM) and trophoectoderm (TE), and identifiedased on their size and intensity of stain (11).
Per-embryo findings were clustered with other embryosuring each trial. Therefore, comparisons between treat-ents utilized treatment as the sole independent variable,ith embryos treated as clustered observations within each
xperiment. Statistical significance was assessed with two-ailed tests, using P�.05 as Type I error rates. The sampleize had 90% power to detect a difference of 1.5 apoptoticells per blastocyst between groups, and 90% power toetect a 0.17 � 104 cpm difference in ROS levels betweenroups. Calculations were performed with SAS version 8.1oftware (SAS Institute Inc., Cary, NC).
The blastocyst formation rate after 48 hours and 72 hoursas not significant for embryos cultured in HTF–SSS com-ared to those cultured in HTF–SSS-supplemented IgG1fter 48 hours (32% and 22.2%) and 72 hours (92% and8.9% consecutively). However, the percentage of em-ryos undergoing blastocyst formation was significantlyeduced by anti-HSP 60 and 70 supplementation after 48ours (13.7% and 0%) and 72 hours (39.2% and 15.2%onsecutively). The hatching rate was significantly lower inhe presence of antibodies compared to the embryos thatere cultured in the HTF–SSS (P�.05). Growth-retarded/
rrested embryos before the morula stage were observed ingG group (6 of 54, 9%), HSP60 (9 of 51, 17.6%) andSP70 (19 of 46, 41.3%). However, the effect of HSP
ABLE 1The allocation of inner cell mass (ICM) and trophblastocysts cultured in HTF–SSS alone and in the
Variable
Control IgG1 a
(n � 71) (n � 54)
TCNa 54.5 (41.0, 65.0)b 57.0 (51.0, 59.0) 41ICMa 13.0 (11.0, 16.0) 15.0 (13.0, 16.0) 12TEa 40.0 (33.0, 44.0) 43.0 (38.5, 45.0) 29ICM/TE 0.4 (0.3, 0.4) 0.4 (0.3, 0.4) 0Apoptotic cell/blastocyst (%) 4.9 10.6Apoptosis in TCNa 2.3 (2, 3.3) 5 (4, 7) 4Apoptosis in ICMa 1.4 (1.2, 1.6) 3.5 (2, 6)Apoptosis in TEa 1 (0.95, 1.4) 1.5 (1, 3)
Note: HTF � Human tubal fluid; SSS � Serum substitute supplement.a TCN � Total cell number, ICM � Inner cell mass, TE � Trophectoderm.b Values are median and interquartile range.
A � Comparison between control group and IgG1.B � Comparison between control group and anti-HSP60.C � Comparison between control group and anti-HSP70.D � Comparison between group IgG1 and anti-HSP60.E � Comparison between group IgG1 and anti-HSP70.F � Comparison between anti-HSP60 and group anti-HSP70.
c P�0.05 was considered significant using mixed model analysis of varian
Esfandiari. Heat shock proteins and preimplantation embryos. Fertil Steril 2007.
ntibodies are more evident at the morula–blastocyst tran- R
rtility and Sterility�
ition where 63% of morula stage embryos failed to de-elop to blastocyst in HSP60 and 74% in HSP70 groups.
The total cell number (TCN) for the embryos that wereultured in the four groups are shown in Table 1. Theedian and interquartile (IQR) range for TCN in the HTF–SS group was similar to that of the blastocysts that wereultured in the presence of IgG1. The ICM number in theTF–SSS group was similar to other groups, and the
CM/TE ratio in IgG1 and HSP60 groups was comparableith the HTF–SSS group. The number of TE cells was
ignificantly lower in HSP60 and 70 groups compared tohe control group (P�.001, and .0001 consecutively).
The median (IQR) level (104 cpm) of ROS for IgG1,SP 60, and HSP 70 groups at 24 hours, 48 hours, and 72ours were comparable to those observed in the HTF–SSSroup.
Positive TUNEL labeling in apoptotic cells was ob-erved in the blastocysts of all groups. However, a positiveabeling could not be identified in the growth-retarded orrrested embryos before the morula stage. Supplementationf culture media with antibodies increased the incidence ofpoptosis in the cultured embryos as evidenced by theignificantly higher percentage of apoptosis in the blasto-ysts and in the higher median and IQR values of apoptoticells per blastocyst (Table 1). Positive TUNEL labelingas seen in ICM and TE in both groups. Cell death in thelastocysts occurred primarily in the ICM in both groups.
No significant correlation was seen between the levels of
toderm (TE) and incidence of apoptosis inesence of antibodies.
SP60 anti-HSP70 P valuec
51) (n � 46) A B C D E F
.0, 48.0) 32.0 (29.0, 35.0) NS .0001 .0001 .0001 .0001 .03
.0, 13.0) 10.0 (9.0, 10.0) NS NS NS .045 .11 .99
.0, 36.0) 23.0 (20.0, 26.0) .02 .001 .0001 .0001 .0001 .002, 0.4) 0.4 (0.3, 0.5) NS NS .004 NS .003 .002.8 13.4 .0001 .0001 .0001 .4 .004 .086) 3.5 (2, 5) .0001 .002 .04 .2 .02 .214) 3 (2, 4) .001 .08 .2 .18 .23 .92) 1 (1, 2) .0001 .0002 .007 .74 .84 .70
Toecpr
nti-H
(n �
.0 (37
.0 (11
.0 (26
.4 (0.412
.5 (3,3 (2,2 (1,
ce.
OS at 24 hours, 48 hours, and 72 hours, and embryo
1215

pLc�tttPc
tatathhntmc
aHtomnpcepHmthb6
phcoanlnh
ecobo
ekatmtni
d(pbeatfOev
atfspvcevam(
pIccwatm
1
arameters in the control (HTF–SSS) and HSP 60 group.evels of ROS at 24 hours and 48 hours were negativelyorrelated with the number of ICM in IgG1 group (r �0.8 and �0.81, P�.02 and .02 respectively). However, in
he HSP 70 group, a positive correlation was seen betweenhe levels of ROS at 24 hours and number of cells in ICM,he ICM/TE ratio, and the incidence of apoptosis (r � 1,�.0001). The level of ROS at 48 hours was negativelyorrelated with blastocyst formation (r � �1, P�.0001).
In the present study, we have shown that supplementa-ion of embryo culture media with anti-HSP antibodiesdversely affects embryo development in different transi-ion stages including cleavage-morula, morula-blastocyst,nd hatching. It also increases the incidence of apoptosis inhe cultured embryos as evidenced by the significantlyigher percentage of apoptosis in the blastocysts and in theigher apoptotic cells per blastocyst. However, there waso significant effect on the level of ROS production, andhe higher amount of ROS in the control and IgG1 groupsay be largely because of the number of blastocysts in the
ulture.
The molecular mechanism(s) involved in inhibition ofpoptosis by HSPs is still undefined. It is proposed thatSPs following stress may move from the cytoplasm into
he nucleus and confer some protective effects againstxidant-induced DNA damage (12). HSP70 can preventitochondrial membrane depolarization, although it does
ot exert its protective effect by scavenging ROS or byreventing cell damage. Rather, it appears to modulate theellular response to the toxic insult (13). The beneficialffects of HSP in embryo development have been shown inrevious studies (14, 15). By limiting the expression ofSP70 in four-cell embryos, in vitro blastocyst develop-ent was reduced with increased embryo sensitivity to
oxic agents. Significantly diminished development ofatched blastocysts was reported in two-cell mouse em-ryos cocultured with monoclonal antibodies against HSP0 and 70.
Upon differentiation at the early blastocyst stage, tro-hectoderm secretes zona lysin that is necessary for zonaatching (16). However, continued exposure to unbalancedulture environment, the presence of IgG or anti-HSP, as inur study, and the signals produced by some embryos thatre arrested at the cellular or morula stage could affectormal cell function. This results in a decrease in the totalysin production by TE cells below the threshold levelecessary to promote zona thinning and subsequently in-ibiting the blastocyst hatching (17).
Although HSPs were, until recently, assumed to localizexclusively at various intracellular sites, it has been re-ently reported that several HSP molecules are expressedn the outer cellular membranes and show cell surfaceinding and/or cellular uptake (18, 19). The zona pellucida
f mouse oocytes and zygotes is permeable to macromol-216 Esfandiari et al. Correspondence
cules up to 170 kDa (20), that is, larger than IgG (150Da) (21). Therefore, it is plausible to assume that antiHSPntibodies can pass through the zona and attach to HSPs onhe surface of blastomeres to exert their effect. Theseolecules are now recognized as participants in signal
ransduction pathways, and some studies show active sig-aling by HSP for induction of cytokine secretion by var-ous cell types (22).
Apoptosis is more likely to occur to a greater degreeuring in vitro embryo culture due to suboptimal conditions23). Nutrient imbalance, oxygen tension, variation of tem-erature, altered cellular environment, manipulation of em-ryos in culture, extra-uterine environment, and the nutri-nts for six to eight cell-stage embryos may not be optimal,nd all these may cause additional stress. All these condi-ions cause apoptosis in cultured embryos and the HSPamily; Hsp70 especially may protect against apoptosis.verexpression of HSP, up to 15-fold higher, in cultured
mbryos is reported to have beneficial effects on the de-eloping embryos (24).
Women undergoing in vitro fertilization who have localnd systemic immunity to human HSP60 following infec-ions, show an increased prevalence of in vitro fertilizationailure (25). During an infection, enhanced microbial HSPynthesis may be part of the protective response of theathogen to host defenses, and can contribute to microbialirulence. This is important for reproduction because manyouples seeking infertility treatment have had a previousxposure to microbial pathogens. Several studies have re-ealed that sensitizing HSP60 to Chlamydia trachomatisnd subsequent expression of the highly homologous hu-an HSP60 can lead to unsuspected infertility problems
25).
In conclusion, this study provides evidence that HSPslay an essential role in mammalian embryo development.nhibition of HSP function by antibodies causes a signifi-ant reduction in blastocyst development and an increase inell death. HSP-mediated regulation of the apoptotic path-ays probably constitutes a fundamental protective mech-
nism that decreases cellular sensitivity to damaging eventso allow cells to escape the otherwise inevitable engage-ent of apoptosis
Navid Esfandiari, D.V.M., Ph.D.a
Tommaso Falcone, M.D.a
Jeffrey M. Goldberg, M.D.a
Ashok Agarwal, Ph.D.a,b
Rakesh K. Sharma, Ph.D.a,b
a Center for Advanced Research in HumanReproduction, Infertility, and Sexual Function,Department of Obstetrics Gynecology andb Glickman Urological Institute, The Cleveland
Clinic Foundation, Cleveland, OhioVol. 87, No. 5, May 2007

R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
Fe
EFERENCES1. Lindquist S, Craig EA. The heat-shock proteins. Annu Rev Genet
1988;22:631–77.2. Nollen EAA, Morimoto RI. Chaperoning signaling pathways: molec-
ular chaperones as stress-sensing “heat shock” proteins. J Cell Sci2002;115:2809–16.
3. Burdon RH, Gill VM, Rice-Evans C. Oxidative stress and heat shockprotein induction in human cells. Free Radic Res Commun 1987;3:129–39.
4. Bensaude O, Babinet C, Morange M, Jacob F. Heat shock proteins,first major products of zygotic gene activity in mouse embryo. Nature1983;305:331–3.
5. Liu CH, Yang CC, Lin DP, Wu MH, Tsai KJ. Stored of Hsp72/Hsp73in germinal vesicle-stage mouse oocytes. Reprod Domest Anim 2004;39:19–24.
6. Yamagishi N, Saito Y, Ishihara K, Hatayama T. Enhancement ofoxidative stress-induced apoptosis by Hsp105alpha in mouse embry-onal F9 cells. Eur J Biochem 2002;269:4143–51.
7. Finkel T. Oxygen radicals and signaling. Curr Opin Cell Biol 1998;10:248–53.
8. Matwee C, Betts DH, King WA. Apoptosis in the early bovineembryo. Zygote 2000;8:57–68.
9. Hardy K. Apoptosis in the human embryo. Rev Reprod 1999;4:125–34.0. Kobayashi H, Gil-Guzman E, Mahran AM, Sharma RK, Nelson DR,
Thomas AJ Jr, et al. Quality control of reactive oxygen speciesmeasurement by luminol-dependent chemiluminescence assay. J An-drol 2001;22:568–74.
1. Brison DR, Schultz RM. Increased incidence of apoptosis in trans-forming growth factor alpha-deficient mouse blastocysts. Biol Reprod1998;59:136–44.
2. Hirvonen MR, Brune B, Lapetina EG. Heat shock proteins andmacrophage resistance to the toxic effects of nitric oxide. Biochem J1996;315:845–9.
3. Bellmann K, Jaattela M, Wissing D, Burkart V, Kolb H. Heat shockprotein hsp70 overexpression confers resistance against nitric oxide.
FEBS Lett 1996;391:185–8.rtility and Sterility�
4. Dix DJ, Garges JB, Hong RL. Inhibition of hsp70-1 and hsp70-3expression disrupts preimplantation embryogenesis and heightensembryo sensitivity to arsenic. Mol Reprod Dev 1998;51:373–80.
5. Neuer A, Mele C, Liu HC, Rosenwaks Z, Witkin SS. Monoclonalantibodies to mammalian heat shock proteins impairs mouse embryodevelopment in vitro. Hum Reprod 1998;13:987–90.
6. Perona RM, Wassarman PM. Mouse blastocysts hatch in vitro byusing a trypsin-like proteinase associated with cells of mural trophec-toderm. Dev Biol 1986;14:42–52.
7. Schiewe MC, Hazeleger NL, Sclimenti C, Balmaceda JP. Physiolog-ical characterization of blastocyst hatching mechanisms by use of amouse antihatching model. Fertil Steril 1995;63:288–294.
8. Arnold-Schild D, Hanau D, Spehner D, Schmid C, Rammensee HG,de la Salle H, et al. Receptor-mediated endocytosis of heat shockproteins by professional antigen-presenting cells. J Immunol 1999;162:3757–60.
9. Wassenberg JJ, Dezfulian C, Nicchitta CV. Receptor mediatedand fluid phase pathways for internalization of the ER Hsp90chaperone GRP94 in murine macrophages. J Cell Sci 1999;112:2167–75.
0. Legge M. Oocyte and zygote zona pellucida permeability to macro-molecules. J Exp Zool 1995;271:145–50.
1. Sellens MH, Jenkinson EJ. Permeability of the mouse zona pellucidato immunoglobulin. J Reprod Fertil 1975;42:153–7.
2. Kol A, Lichtman AH, Finberg RW, Libby P, Kurt-Jones EA. Heatshock protein (HSP) 60 activates the innate immune response: CD14is an essential receptor for HSP60 activation of mononuclear cells.J Immunol 2000;164:13–17.
3. Hardy K. Cell death in the mammalian blastocyst. Mol Hum Reprod1997;3: 919–25.
4. Christians E, Campion E, Thompson EM, Renard JP. Expression ofthe HSP 70.1 gene, a landmark of early zygotic activity in the mouseembryo, is restricted to the first burst of transcription. Development1995;121:113–22.
5. Neuer A, Spandorfer SD, Giraldo P, Dieterle S, Rosenwaks Z, WitkinSS. The role of heat shock proteins in reproduction. Hum Reprod
Update 2000;6:149–59.1217

Efetfgvltu
btmq1fppbte
cHowtetcotim
RR
1
Prolonged duration of transfer does not affectoutcome in cycles with good embryo quality
The objective of investigating the impact of the time that embryos remain in the catheter on the outcome ofcycles was assessed by measuring the period between loading the catheter and discharging the embryos in 300transfer cycles. The pregnancy and implantation rates were similar in cycles with good embryo qualityregardless of transfer duration. (Fertil Steril� 2007;87:1218–21. ©2007 by American Society for Reproduc-
tive Medicine.)tc2epw[pcntoe
tbATaddwtuiRIaa
(scfcktcc
mbryo transfer is considered to be of utmost importanceor the success of assisted reproduction treatment (1). How-ver, although the technology of IVF has developed overhe years, the practice of embryo transfer has undergoneew alterations. Some modifications that have been sug-ested to be of importance in improving outcome areisualization of the uterine cavity by ultrasound (2, 3),oading the catheter without air (4), causing minimalrauma (3, 5–8), increasing speed of the procedure (9), andsing soft catheters (10).
Although the success of a transfer technique appears toe largely dependent on the skills of the physician (1, 11),he impact of operator variability has been disregarded inany studies; for example, 15 physicians in (7). Embryo
uality is another important variable in the assessment (12,3). Recent studies showed that day 2 embryos displayingour mononucleated blastomeres possessed a higher im-lantation potential than others (14, 15). Hence, a betterrediction of the effect of embryo quality on outcome haseen enabled, and evaluation of the impact of the transferechnique after minimizing possible interference of thembryo factor became possible.
Two physicians, each carrying out approximately 2,000ycles per year, perform embryo transfers in our center.ence, the situation can be regarded as “minimal impact ofperator skills on outcome” compared to those clinics inhich many physicians perform the transfers. However, the
ime that embryos spend in the catheter before they arexpelled into the uterus differs among physicians and pa-ients, because of the speed of the manipulation or to otheronditions, such as anatomy of the cervical canal, and son. The outcome may be influenced by the transfer dura-ion, as the microenvironment to which embryos is exposedn the period between loading and discharging the catheteray have a negative impact on their implantation capacity.
eceived April 8, 2006; revised and accepted August 4, 2006.eprint requests: Mustafa Bahceci, M.D., Azer Is Merkezi 44/17 Kat 6,Abdi Ipekci Cad., Nisantasi 80200, Istanbul, Turkey (FAX: 90
w2122303990; E-mail: [email protected]).
218 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
Therefore, the present study investigated the impact ofhe time that embryos remain in the catheter on the out-ome of cycles for a period of three months (October 1,005–December 31, 2005). To minimize potential interfer-nce on the results of parameters other than the transferrocedure itself, only cycles that met the following criteriaere taken into the survey: [1] women of �39 years of age,
2] �2 previous failed attempts in our unit, [3] no Preim-lantation Genetic Diagnosis (PGD) cycles, [4] no thawycles, and [5] at least one motile sperm used for insemi-ation. No consent has been obtained from the patients orhe ethics committee, because no additional manipulationsther than the routine have been applied to gametes and/ormbryos.
The procedures for patient preparation and embryo cul-ure have been described elsewhere (16–18). Briefly, em-ryos were cultured individually in 20 �L of Quinn’sdvantage Plus Medium (Sage In-Vitro Fertilization Inc.,rumbull, CT) covered with sterile mineral oil. Zygotesnd embryos were evaluated for early cleavage, day 2 anday 3 morphologies. Embryo transfers were performed atays 2 and 3 according to the indications described else-here (19). Two physicians (S.T. and A.M.) performed
ransfers on a weekly basis to patients with full bladdernder ultrasound guidance. Two embryologists participatedn the study (H.N.C. and O.H.). Only Wallace Embryoeplacement catheters (18 mm or 23 mm, Smiths Medical
nt. Ltd., Kent, UK) were used. In none of the transfers wasdditional equipment (forceps, tenaculum, hysterometer,nd so on) needed.
The embryos were drawn into the catheter without air4). As soon as the catheter was loaded, a digital timer waset. The physician introduced the catheter gently into theervical canal and expelled embryos smoothly 1 to 2 cmrom the fundus. If there were no retained embryos in theatheter, the timer was stopped. Otherwise, the timer wasept running until retained embryos were expelled. Easyransfers were those in which no blood or mucus in theatheter was observed, and there was no reloading orhange of catheter. Transfers with other characteristics
ere described as difficult. Reloading occurred when there0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.100
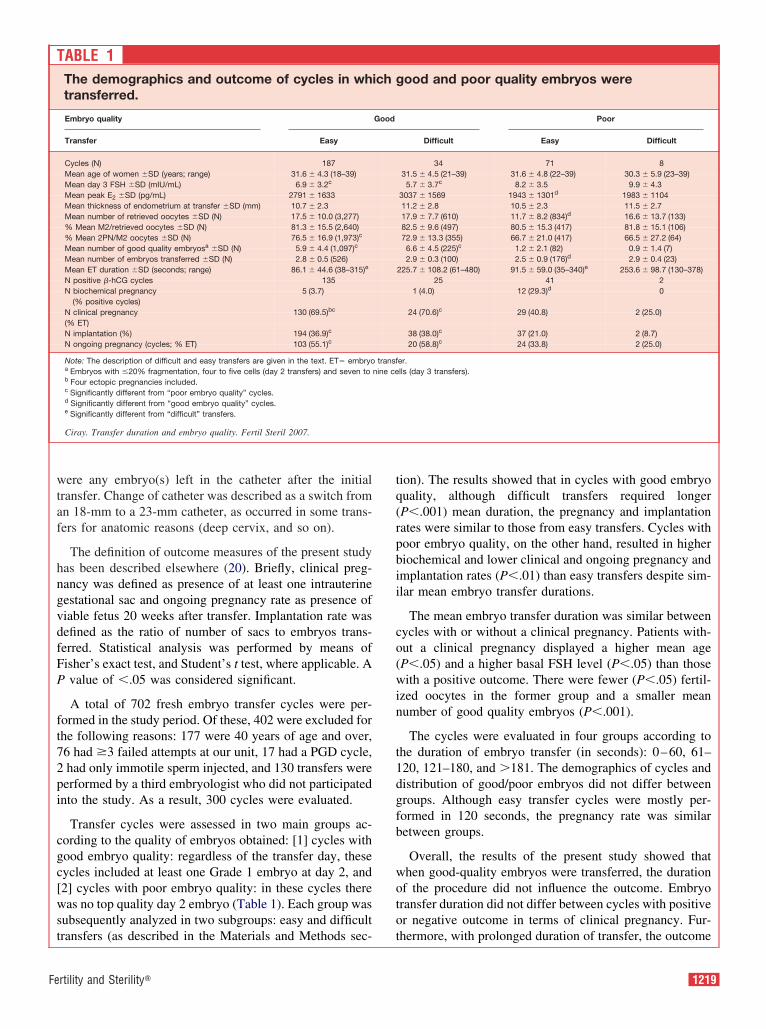
wtaf
hngvdfFP
ft72pi
cgc[wst
tq(rpbii
co(win
t1dgfb
woto
Fe
ere any embryo(s) left in the catheter after the initialransfer. Change of catheter was described as a switch fromn 18-mm to a 23-mm catheter, as occurred in some trans-ers for anatomic reasons (deep cervix, and so on).
The definition of outcome measures of the present studyas been described elsewhere (20). Briefly, clinical preg-ancy was defined as presence of at least one intrauterineestational sac and ongoing pregnancy rate as presence ofiable fetus 20 weeks after transfer. Implantation rate wasefined as the ratio of number of sacs to embryos trans-erred. Statistical analysis was performed by means ofisher’s exact test, and Student’s t test, where applicable. Avalue of �.05 was considered significant.
A total of 702 fresh embryo transfer cycles were per-ormed in the study period. Of these, 402 were excluded forhe following reasons: 177 were 40 years of age and over,6 had �3 failed attempts at our unit, 17 had a PGD cycle,had only immotile sperm injected, and 130 transfers wereerformed by a third embryologist who did not participatednto the study. As a result, 300 cycles were evaluated.
Transfer cycles were assessed in two main groups ac-ording to the quality of embryos obtained: [1] cycles withood embryo quality: regardless of the transfer day, theseycles included at least one Grade 1 embryo at day 2, and2] cycles with poor embryo quality: in these cycles thereas no top quality day 2 embryo (Table 1). Each group was
ubsequently analyzed in two subgroups: easy and difficult
ABLE 1The demographics and outcome of cycles in whtransferred.
Embryo quality
Transfer Easy
Cycles (N) 187Mean age of women �SD (years; range) 31.6 � 4.3 (18–39)Mean day 3 FSH �SD (mIU/mL) 6.9 � 3.2c
Mean peak E2 �SD (pg/mL) 2791 � 1633Mean thickness of endometrium at transfer �SD (mm) 10.7 � 2.3Mean number of retrieved oocytes �SD (N) 17.5 � 10.0 (3,277)% Mean M2/retrieved oocytes �SD (N) 81.3 � 15.5 (2,640)% Mean 2PN/M2 oocytes �SD (N) 76.5 � 16.9 (1,973)c
Mean number of good quality embryosa �SD (N) 5.9 � 4.4 (1,097)c
Mean number of embryos transferred �SD (N) 2.8 � 0.5 (526)Mean ET duration �SD (seconds; range) 86.1 � 44.6 (38–315)e
N positive �-hCG cycles 135N biochemical pregnancy 5 (3.7)
(% positive cycles)N clinical pregnancy 130 (69.5)bc
(% ET)N implantation (%) 194 (36.9)c
N ongoing pregnancy (cycles; % ET) 103 (55.1)c
Note: The description of difficult and easy transfers are given in the text. ET� embryoa Embryos with �20% fragmentation, four to five cells (day 2 transfers) and seven tob Four ectopic pregnancies included.c Significantly different from “poor embryo quality” cycles.d Significantly different from “good embryo quality” cycles.e Significantly different from “difficult” transfers.
Ciray. Transfer duration and embryo quality. Fertil Steril 2007.
ransfers (as described in the Materials and Methods sec- t
rtility and Sterility�
ion). The results showed that in cycles with good embryouality, although difficult transfers required longerP�.001) mean duration, the pregnancy and implantationates were similar to those from easy transfers. Cycles withoor embryo quality, on the other hand, resulted in higheriochemical and lower clinical and ongoing pregnancy andmplantation rates (P�.01) than easy transfers despite sim-lar mean embryo transfer durations.
The mean embryo transfer duration was similar betweenycles with or without a clinical pregnancy. Patients with-ut a clinical pregnancy displayed a higher mean ageP�.05) and a higher basal FSH level (P�.05) than thoseith a positive outcome. There were fewer (P�.05) fertil-
zed oocytes in the former group and a smaller meanumber of good quality embryos (P�.001).
The cycles were evaluated in four groups according tohe duration of embryo transfer (in seconds): 0–60, 61–20, 121–180, and �181. The demographics of cycles andistribution of good/poor embryos did not differ betweenroups. Although easy transfer cycles were mostly per-ormed in 120 seconds, the pregnancy rate was similaretween groups.
Overall, the results of the present study showed thathen good-quality embryos were transferred, the durationf the procedure did not influence the outcome. Embryoransfer duration did not differ between cycles with positiver negative outcome in terms of clinical pregnancy. Fur-
ood and poor quality embryos were
Poor
Difficult Easy Difficult
34 71 831.5 � 4.5 (21–39) 31.6 � 4.8 (22–39) 30.3 � 5.9 (23–39)
5.7 � 3.7c 8.2 � 3.5 9.9 � 4.33037 � 1569 1943 � 1301d 1983 � 110411.2 � 2.8 10.5 � 2.3 11.5 � 2.717.9 � 7.7 (610) 11.7 � 8.2 (834)d 16.6 � 13.7 (133)82.5 � 9.6 (497) 80.5 � 15.3 (417) 81.8 � 15.1 (106)72.9 � 13.3 (355) 66.7 � 21.0 (417) 66.5 � 27.2 (64)6.6 � 4.5 (225)c 1.2 � 2.1 (82) 0.9 � 1.4 (7)2.9 � 0.3 (100) 2.5 � 0.9 (176)d 2.9 � 0.4 (23)
225.7 � 108.2 (61–480) 91.5 � 59.0 (35–340)e 253.6 � 98.7 (130–378)25 41 2
1 (4.0) 12 (29.3)d 0
24 (70.6)c 29 (40.8) 2 (25.0)
38 (38.0)c 37 (21.0) 2 (8.7)20 (58.8)c 24 (33.8) 2 (25.0)
er.lls (day 3 transfers).
Tich g
Good
transfnine ce
hermore, with prolonged duration of transfer, the outcome
1219

do
ifcccffingofoc
lahssetdaiutadHitoTnsspscp
rltnps(swa
factotvdbWwt
R
1
1
1
1
id not differ when the groups included similar proportionf cycles with good embryo quality.
To our knowledge, this is the first study in which nonfluence of transfer duration to the outcome has beenound when good-quality embryos were available. Thelinical pregnancy and implantation rates were lower inycles with poor embryo quality regardless of transferharacteristics, although the transfer duration did not differrom respective cycles with good embryo quality. Thisnding, taken together with a higher biochemical preg-ancy rate in the poor compared to good embryo qualityroup, indicate the importance of embryo quality on theutcome in similar transfer durations. The impact of trans-er duration on the outcome of poor embryo quality cycles,n the other hand, remains to be further investigated be-ause of low number of cycles in the assessed groups.
It has previously been reported that the duration betweenoading and discharging embryos affected the pregnancynd implantation rates (9). Durations over 120 secondsave been found to result in poor outcome, and therefore,hould be avoided when possible. The conclusion of thattudy was “the duration of interval loading–dischargingmbryos was a prognostic factor of IVF, independent ofransfer difficulty.” The results of the present study contra-ict this statement. Possible explanations for this discrep-ncy could be: [1] there was no transfer in the present studyn which a cervical tenaculum and/or hysterometer wassed. In the study by Matorras et al. (9), easy transfers werehose in which no cervical tenaculum was used, and use oftenaculum with or without hysterometer was defined as aifficult or moderately difficult transfer, respectively.ence, any potential traumatic effect arisen from use of
nstruments during the transfer (5, 7, 8) was minimized inhe present compared to the earlier study, and the durationf the procedure had a greater effect on the outcome. [2]he impact of operator variability, in other words, theumber of physicians performing embryo transfers was nottated in the study by Matorras et al. (9). However, theuccess of a transfer technique appears to be largely de-endent on the skills of the physician (1, 11). The presenttudy minimizes any impact of operator skills on the out-ome compared to most of the clinics in which manyhysicians perform transfers.
Transfer embryos can be vulnerable to the microenvi-onment to which they are exposed in the period betweenoading and discharging the catheter. It can be expectedhat with prolonged durations, their metabolism will beegatively influenced, and possibly, the implantation ca-acity of the embryo will be compromised. In the presenttudy, the outcome of transfers lasting up to 459 secondsapproximately 7.5 minutes) was evaluated, and these re-ulted in a clinical pregnancy when good-quality embryosere present. Good-quality embryos may be resistant to
lterations in the microenvironment, and prolonged trans-
220 Ciray et al. Correspondence
ers may not be detrimental to the outcome if performedtraumatically. Recent evidence suggested that althoughulture conditions during bovine in vitro embryo produc-ion could impact somewhat on the developmental potentialf the early embryo, the intrinsic quality of the oocyte washe key factor determining the proportion of oocytes de-eloping to the blastocyst stage (21). Therefore, embryoseriving from good-quality oocytes could be less vulnera-le to environmental conditions than those of poor quality.hether the implantation capacity of poor-quality embryosas compromised with prolonged transfer duration remains
o be investigated.
H. Nadir Ciray, M.D., Ph.D.Suleyman Tosun, M.D.Oguzhan HacifazliogluAli Mesut, M.D.Mustafa Bahceci, M.D.Bahceci Women’s Health Care Center and German
Hospital IVF Unit, Istanbul, Turkey
EFERENCES1. Hearns-Stokes RM, Miller BT, Scott L, Creuss D, Chakraborty PK,
Segars JH. Pregnancy rates after embryo transfer depend on theprovider at embryo transfer. Fertil Steril 2000;74:80–6.
2. Schoolcraft WB, Surrey ES, Gardner DK. Embryo transfer: tech-niques and variables affecting success. Fertil Steril 2001;76:863–70.
3. Matorras R, Urquijo E, Mendoza R, Corcostegui B, Exposito A,Rodriguez-Escudero FJ. Ultrasound-guided embryo transfer improvespregnancy rates and increases the frequency of easy transfers. HumReprod 2002;17:1762–6.
4. Meldrum DR, Chetkowski R, Steingold KA, de Ziegler D, Cedars MI,Hamilton M. Evolution of a highly successful in vitro fertilization–embryo transfer program. Fertil Steril 1987;48:86–93.
5. Mansour R, Aboulghar M, Serour G. Dummy embryo transfer: atechnique that minimizes the problems of embryo transfer and im-proves the pregnancy rate in human in vitro fertilization. Fertil Steril1990;54:678–81.
6. Goudas VT, Hammitt DG, Damario MA, Session DR, Singh AP,Dumesic DA. Blood on the embryo transfer catheter is associatedwith decreased rates of embryo implantation and clinical pregnancywith the use of in vitro fertilization-embryo transfer. Fertil Steril1998;70:878–82.
7. Tomas C, Tikkinen K, Tuomivaara L, Tapanainen JS, Martikainen H.The degree of difficulty of embryo transfer is an independent factorfor predicting pregnancy. Hum Reprod 2002;17:2632–5.
8. Lesny P, Killick SR, Tetlow RL, Robinson J, Maguiness SD. Uterinejunctional zone contractions during assisted reproduction cycles.Hum Reprod Update 1998;4:440–5.
9. Matorras R, Mendoza R, Exposito A, Rodriguez-Escudero FJ. Influ-ence of the time interval between embryo catheter loading and dis-charging on the success of IVF. Hum Reprod 2004;19:2027–30.
0. van Weering HG, Schats R, McDonnell J, Vink JM, Vermeiden JP,Hompes PG. The impact of the embryo transfer catheter on thepregnancy rate in IVF. Hum Reprod 2002;17:666–70.
1. Karande VC, Morris R, Chapman C, Rinehart J, Gleicher N. Impactof the “physician factor” on pregnancy rates in a large assistedreproductive technology program: do too many cooks spoil the broth?Fertil Steril 1999;71:1001–9.
2. Diedrich K, van der Ven H, al-Hasani S, Krebs D. Establishment ofpregnancy related to embryo transfer techniques after in-vitro fertil-
ization. Hum Reprod 1989;4:111–4.Vol. 87, No. 5, May 2007

1
1
1
1
1
1
1
2
2
Fe
3. Giorgetti C, Terriou P, Auquier P, Hans E, Spach JL, Salzmann J,et al. Embryo score to predict implantation after in-vitro fertiliza-tion: based on 957 single embryo transfers. Hum Reprod 1995;10:2427–31.
4. Moriwaki T, Suganuma N, Hayakawa M, Hibi H, Katsumata Y,Oguchi H, et al. Embryo evaluation by analysing blastomere nuclei.Hum Reprod 2004;19:152–6.
5. Saldeen P, Sundstrom P. Nuclear status of four-cell preembryospredicts implantation potential in in vitro fertilization treatment cy-cles. Fertil Steril 2005;84:584–9.
6. Akman MA, Erden HF, Tosun SB, Bayazit N, Aksoy E, BahceciM. Comparison of agonistic flare-up-protocol and antagonisticmultiple dose protocol in ovarian stimulation of poor responders:results of a prospective randomized trial. Hum Reprod 2001;16:868 –70.
7. Ulug U, Jozwiak EA, Mesut A, Berksoy MM, Bahceci M. Survival
rates during the first trimester of multiple gestations achieved byrtility and Sterility�
ICSI: a report of 1448 consecutive multiples. Hum Reprod2004;19:360 – 4.
8. Ciray HN, Karagenc L, Ulug U, Bener F, Bahceci M. Use of bothearly cleavage and day 2 mononucleation to predict embryos withhigh implantation potential in intracytoplasmic sperm injection cy-cles. Fertil Steril 2005;84:1411–6.
9. Bahceci M, Ulug U, Ciray HN, Akman MA, Erden HF. Efficiency ofchanging the embryo transfer time from day 3 to day 2 among womenwith poor ovarian response: a prospective randomized trial. FertilSteril 2006;86:81–5.
0. Zegers-Hochschild F, Nygren KG, Adamson GD, de Mouzon J,Lancaster P, Mansour R, et al. The International Committee Moni-toring Assisted Reproductive Technologies (ICMART) glossary onART terminology. Fertil Steril 2006;86:16–9.
1. Lonergan P, Fair T, Corcoran D, Evans AC. Effect of culture envi-ronment on gene expression and developmental characteristics in
IVF-derived embryos. Theriogenology 2006;65:137–52.1221

Tu(wicuimtiuret8ud
wOocuassttef
yp
RR
1
Ureteral suspension facilitates surgery for deeppelvic endometriosis
This study describes a technique that facilitates the identification of the ureter during radical excision ofendometriosis. After dissection of the ureter, a biocompatible silicone sling is introduced into the pelvisthrough the trocar; the sling is applied around the ureter and the two ends of the sling are pulled until adequatetraction on the ureter is obtained. Ureteral suspension was performed in 126 consecutive women withendometriotic lesions involving the ovarian fossa and/or the uterosacral ligaments. This surgical techniquefacilitated the identification of the ureter, preventing injuries. (Fertil Steril� 2007;87:1222–4. ©2007 by
American Society for Reproductive Medicine.)dgwwf4Ppfetb(potewt
7aoriucobrfmcottfi
he presence of endometriotic glands and stroma in thereteral wall (intrinsic ureteral endometriosis) is very rare1), and it is estimated to occur in about 0.08% to 1% ofomen with endometriosis (2). More frequently, the ureter
tself is not invaded by endometriosis, but it is encircled byonstrictive fibrosis caused by the disease of the adjacentterosacral ligament (3). Typically, endometriotic lesionsnvolving the pelvic sidewall determine a medial displace-ent of the ureter toward the uterosacral ligament (4) and
hicken the peritoneum, making difficult the direct visual-zation of the ureter; in the presence of these conditions, thereter is susceptible to surgical injury (5–7). Therefore,etroperitoneal dissection of the ureter is required whenxcising deep endometriotic lesions of the ovarian fossa,he uterosacral ligaments, and the rectovaginal septum (3,). The current study aims to describe a technique ofreteral suspension that may facilitate its identificationuring excision of deep endometriotic lesions.
This study included 126 consecutive women who under-ent laparoscopy because of symptomatic endometriosis.nly women with endometriotic lesions involving thevarian fossa and/or the uterosacral ligaments were in-luded in the study. A four-port laparoscopic technique wassed with an umbilical 10-mm port for the scope and threedditional 5-mm operating ports (two lateral to the rectusheath and one in the midline in the suprapubic area). Inome cases surgery was started vaginally by circumscribinghe lesion with electrosurgery until the soft areolar tissue ofhe rectovaginal septum was encountered (3). If ovarianndometriotic cysts were present, they were removed be-ore suspending the ovaries to the abdominal wall (9).
Before excision of deep endometriotic lesions, ureterol-sis was started high on the pelvic sidewall in normaleritoneum overlying the ureter and then continued in the
eceived April 13, 2006; revised and accepted August 19, 2006.eprint requests: Simone Ferrero, M.D., Department of Obstetrics andGynaecology, San Martino Hospital, University of Genoa, Largo R.Benzi 1, 16132 Genoa, Italy. (FAX: 011-39-010-51-1525; E-mail:
222 Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ©2007 American Society for Reproductive Medicine,
irection of the uterosacral ligament. The ureter was pro-ressively freed up by sharp and blunt dissection combinedith small cutting and bipolar coagulation. In some cases itas necessary to sacrifice the uterine artery to completely
ree the ureter. When the ureter was completely free, a0-cm biocompatible silicone sling (Medical Biomaterialroducts, Neustadt-Glewe, Germany) was introduced in theelvis through the ipsilateral trocar by using atraumaticorceps. The sling was applied around the ureter. The twonds of the sling were pulled until adequate traction onhe ureter was obtained, and the two ends of the sling wererought out of the pelvis via the ipsilateral trocar sleeveFig. 1). The sleeve was removed and was replaced in theeritoneal cavity next to the sling. The sling was securedutside the abdomen. The same procedure was repeated onhe opposite side if required. The surgery continued with anasy identification of the ureters, which were pushed out-ard by placing an extracorporeal traction on the slings. At
he end of the surgical procedure, the sling was removed.
Ureteral suspension was performed monolaterally in0.6% of the patients (n � 89; on the left side in 55 casesnd on the right side in 34 cases) and bilaterally in 29.4%f the subjects (n � 37). In 125 (99.2%) cases the fibroticing surrounding the ureter was completely removed, leav-ng the ureter in total safety and without opening thereteral lumen. In four cases (3.2%) the uterine arteryrossing the lowest part of the ureter was coagulated. Inne case (0.8%), the muscularis of the ureter was invadedy endometriosis; resection of a portion of the ureter wasequired and laparoscopic uretero-ureterostomy was per-ormed. This patient underwent intraoperative stent place-ent, and the catheter was left in place for 3 months. No
omplication resulting from the ureteral suspension wasbserved. The technique was easy to perform and normallyook �5 minutes to be completed on both sides. In all caseshe endometriotic nature of the removed nodules was con-rmed at histologic examination.
Prevention of ureteric injuries is a primary goal during
ajor laparoscopic pelvic surgery, particularly in the pres-0015-0282/07/$32.00Published by Elsevier Inc. doi:10.1016/j.fertnstert.2006.08.116

espsiernitcme
iaitpwj
ampap
ttpofTdassm
p
A
Fe
nce of predisposing conditions such as pelvic adhesionsecondary to endometriosis or previous pelvic operations,elvic malignancy, and previous pelvic irradiation. Duringurgery for deep endometriosis, the risk of ureteral injuriess greater when lesions of the uterosacral ligament arexcised. In fact, when the ureter is not identified, there is aelevant risk of inadvertent lacerations or resection. Alter-atively, burn injuries and necrosis can occur when bleed-ng in this area induces the surgeon to use electrical,hermal, or laser energy. Even the use of bipolar electro-oagulation around the ureter may be problematic becauseany coagulator paddles are too large to apply a small
nergy footprint (3).
Ureteric lesions may cause significant morbidity, includ-ng ureteric stenosis or obstruction, uterovaginal fistula,nd in some cases hydronephrosis and variable degrees ofmpaired renal function. Donnez et al. (10) suggested thathe placement of ureteral stents just before surgery im-roves the intraoperative recognition of the ureters inomen with endometriosis. When ureteral dissection is
IGURE 1
urgical steps in ureteral suspension. (A) Ureterolysiseritoneum overlying the left ureter, and it is then coreter was progressively freed. (B) The silicone slingrocar by using atraumatic forceps. (C) The sling is are pulled until adequate traction on the ureter is obtreter.
lessandri. Ureteral suspension in endometriosis. Fertil Steril 2007.
udged to be not required, for example during laparoscopy- i
rtility and Sterility�
ssisted vaginal hysterectomy, the chance of ureteral injuryay be reduced by creating a window over the anterior and
osterior broad ligaments and pushing inferolaterally thereolar tissue (in which the ureter is embedded) on theosterior broad ligament (11).
Ureteral suspension with a silicone sling may facilitatehe dissection because it allows the surgeon to modulate theraction on the ureter during the procedure. An importantroperty of the silicone sling is its slipperiness; in fact notnly it can be easily inserted, but also it slides with minimalriction even when it is placed next to the trocar sleeve.heoretically, friction during movements of the sling mayetermine damages to the surrounding tissues (ureter andbdominal wall). The use of a silicone sling in the currenttudy was based on the previous demonstration thatilicone-based materials show the greatest ease of move-ent because of the lower friction (12).
In conclusion, we describe a technique of ureteral sus-ension that not only gave us the opportunity to easily
tarted high on the pelvic sidewall in the normaled in the direction of the uterosacral ligament; thetroduced into the pelvis through the ipsilaterald around the ureter. (D) The two ends of the slingd. (E) The same procedure is repeated on the right
F
S is sp ntinuu is int ppliea aineu
dentify the ureter, but also facilitated the excision of
1223

et
R1
1
1
1
ndometriosis through the traction exerted on the ureter byhe sling.
Franco Alessandri, M.D.Davide Lijoi, M.D.Emanuela Mistrangelo, M.D.Simone Ferrero, M.D.Nicola Ragni, M.D.Valentino Remorgida, M.D.Department of Obstetrics and Gynecology, San
Martino Hospital and University of Genoa, Genoa,Italy
EFERENCES1. Donnez J, Squifflet J, Smets M, Jadoul P. Severe endometriosis
involving the urogenital system. In: Sutton C, Jones K, Adamson GD,eds. Modern management of endometriosis. Abington, UK: Taylorand Francis, 2005:205–13.
2. Nezhat C, Nezhat F, Nezhat CH, Nasserbakht F, Rosati M, SeidmanDS. Urinary tract endometriosis treated by laparoscopy. Fertil Steril1996;66:920–4.
3. Redwine DB. Endometriosis of the urinary tract. In: Redwine DB, ed.Surgical management of endometriosis. London: Martin Dunitz, Tay-
lor and Francis Group, 2004:191–203.224 Alessandri et al. Correspondence
4. Nackley AC, Yeko TR. Ureteral displacement associated with pelvicperitoneal defects and endometriosis. J Am Assoc Gynecol Laparosc2000;7:131–3.
5. Cheng YS. Ureteral injury resulting from laparoscopic fulguration ofendometriotic implant. Am J Obstet Gynecol 1976;126:1045–6.
6. Grainger DA, Soderstrom RM, Schiff SF, Glickman MG, DeCherneyAH, Diamond MP. Ureteral injuries at laparoscopy: insights intodiagnosis, management, and prevention. Obstet Gynecol 1990;75:839–43.
7. Saidi MH, Sadler RK, Vancaillie TG, Akright BD, Farhart SA, WhiteAJ. Diagnosis and management of serious urinary complications aftermajor operative laparoscopy. Obstet Gynecol 1996;87:272–6.
8. Chapron C, Dubuisson JB. Laparoscopic treatment of deep endome-triosis located on the uterosacral ligaments. Hum Reprod 1996;11:868–73.
9. Cutner AS, Lazanakis MS, Saridogan E. Laparoscopic ovarian sus-pension to facilitate surgery for advanced endometriosis. Fertil Steril2004;82:702–4.
0. Donnez J, Suifflet J. Ureteral endometriosis: a complication of rec-tovaginal adenomyosis. In: Jain N, ed. Atlas of endoscopic surgery ininfertility and gynecology. New York: McGraw-Hill, 2004:192–200.
1. Koh LW, Koh PH, Lin LC, Ng WJ, Wong E, Huang MH. A simpleprocedure for the prevention of ureteral injury in laparoscopic-as-sisted vaginal hysterectomy. J Am Assoc Gynecol Laparosc 2004;11:167–9.
2. Jones DS, Garvin CP, Gorman SP. Relationship between biomedicalcatheter surface properties and lubricity as determined using texturalanalysis and multiple regression analysis. Biomaterials 2004;25:
1421–8.Vol. 87, No. 5, May 2007

TimcTcaeltc
cuctlpdGtmopctd
mdwwlema
R
R
00do
Simple vaginal mold for use in the postoperativecare of patients with a transverse vaginal septum
Severe vaginal stenosis is a potentially disabling complication of transverse vaginal septum resection due tothe constriction of the resulting circular scar. We describe a vaginal mold that can be easily created by anoccupational therapist, and used as a long-term stent of the vagina in young girls. (Fertil Steril� 2007;87:
1225–6. ©2007 by American Society for Reproductive Medicine.)dmmtosm
miIcutwtopstbwetVNoialwp
haagTmhw
he surgical management of obstructing vaginal abnormal-ties varies in complexity, from the fairly straightforwardanagement of an imperforate hymen to the more difficult
orrection of mid-to-high transverse vaginal septums.hese latter entities are fraught with the postoperativeomplication of vaginal stenosis, which may occur monthsfter the surgery. Because of the rarity of this condition,stimated at 1 in 70,000 females (1), information from theiterature mainly consists of case reports. In one report ofhree patients, two required repeat surgical procedures be-ause of vaginal stenosis (2).
Strategies for preventing postoperative vaginal stenosis in-lude a unique surgical approach combined with long-termse of a vaginal mold to maintain the diameter of the vaginalanal. For surgery, a circumferential Z-plasty is used (3), suchhat scarring along the suture line contracts the incision in aongitudinal more than a transverse direction. If the patient’sain from the hematocolpos is manageable, surgery may beelayed (4), with suppression of endometrial activity by anRH agonist or continuous oral contraceptive. This allows
ime for dilatation of the lower vaginal segment, yieldingore tissue for an easier anastomosis. Initial decompression
f the hematocolpos with percutaneous aspiration was re-orted (5), but requires significant antibiotic prophylaxis be-ause of the substantial risk of infection. Although theseechniques likely decrease the chance of vaginal stenosis, theyo not always eliminate the need for a vaginal mold.
Scant information is provided in the literature concerningolds used after resection of vaginal septums. In the original
escription by Rock, a hollow Lucite form was used whichould allow for menstrual egress (6). These Lucite formsere commercially made and, to our knowledge, are no
onger available. Also, little information is available about theasiest methods for retaining vaginal molds. Characteristics ofolds for transverse septums are different from those used
fter a McIndoe vaginoplasty. After resolution of the initial
eceived May 29, 2006; revised September 25, 2006; accepted No-vember 6, 2006.
eprint requests: Thomas M. Price, M.D., Department of Obstetrics andGynecology, Duke University Medical Center, 5704 Fayetteville Road,Durham, North Carolina 27710 (FAX: 919 681-7904; E-mail: price067@
dmc.duke.edu).
15-0282/07/$32.00i:10.1016/j.fertnstert.2006.11.013 Copyright ©2007 American Soc
ischarge from the healing of a vaginoplasty skin graft, a solidold may be used, because there is no uterus. These moldsay be small enough to fit above the levator ani muscles, and
hus be self-retained. In contrast, the mold used after resectionf a transverse septum is ideally hollow and long enough topan the anastomosis site. This requires some type of belt toaintain position.
Over the past 2 years, we have cared for three cases ofid-to-high transverse vaginal septums, and this has resulted
n novel ideas for an acceptable long-term vaginal mold.deally, the mold would be inexpensive, easy to make, and asomfortable as possible. Figure 1 shows the mold and the beltsed to secure it. The mold is made from low-temperaturehermoplastic splint material by an occupational therapist,ith a length of 10.5 cm and a diameter of 2.6 cm. Edges of
he insertion end are slightly rounded, and there is a slight flaref the end remaining at the introitus. Four small holes arelaced at the 2, 4, 8, and 10 o’clock positions. The mold isterilized with ethylene oxide. All materials for the belt usedo hold the mold in place were purchased from Wal-Mart. Theelt was constructed of 1-inch-wide elastic around the waist,ith a plastic buckle. In total, four half-inch-wide pieces of
lastic were attached to the waist band: two in the front, andwo in the back. At the end of each strip of elastic, twoelcoin hook patches (Velcro Industries B.V., Manchester,H) were placed 4.5 cm apart, with the last being at the endf the strip. The mold is secured to the belt with one-quarter-nch-wide Penrose drains (Bard Medical, Covington, GA)ttached via the small holes. After determining the necessaryength, a Velcoin loop patch is stitched to the Penrose drain,hich is then sandwiched between the two Velcoin hookatches on each elastic strip.
Of the three patients with transverse vaginal septum that weave cared for in the last 2 years, one was lost to follow-up,nd the remaining two continue to be followed. Both patientsre virginal teenagers. One patient is now 18 months postsur-ery, and only uses her mold while sleeping 3 nights a week.he other patient is 12 months out postsurgery, and uses herold while sleeping. Based on their experience, each patient
as learned what length of time they may leave the mold outithout subsequent difficulty in replacing it. They have had no
ifficulty with urination or bowel movements with the mold in1225Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

piirrc
R1
2
3
4
5
6
L
1
lace. They are able to perform most activities with the moldn place, except for exercises that could result in a straddlenjury. Both the mold and the belt are inexpensive and easilyeplicated. Most important, the molds may be custom-made inegard to length and width, allowing for improved patientomfort and thus compliance.
Judith Lacy, M.D.a
Gretchen R. Correll, O.T.R./L., C.H.T.b
David K. Walmer, M.D., Ph.D.a
Thomas M. Price, M.D.aa Department of Obstetrics and Gynecology, and
b Department of Physical and OccupationalTherapy, Duke University Medical Center, Durham,
IGURE 1
vaginal mold (left), constructed of low-temperaturehe mold is secured to the belt with Velcoin patches
acy. Vaginal mold after vaginal septum repair. Fertil Steril 2007.
North Carolina
226 Lacy et al. Correspondence
EFERENCES. Banerjee R, Laufer D. Reproductive disorders associated with pelvic
pain. Semin Pediatr Surg 1998;7:52.. Joki-Erkkila M, Heinonen P. Presenting and long-term clinical impli-
cations and fecundity in females with obstructing vaginal malforma-tions. J Pediatr Adolesc Gynecol 2003;16:307–12.
. Wierrani F, Bodner K, Spangler B, Grunberger W. “Z”-plasty of thetransverse vaginal septum using Garcia’s procedure and the Grun-berger modification. Fertil Steril 2003;79:608–12.
. Beyth Y, Klein Z, Weinstein S, Tepper R. Thick transverse vaginalseptum: expectant management followed by surgery. J Pediatr AdolescGynecol 2004;17:379–81.
. Hurst B, Rock J. Preoperative dilatation to facilitate repair of the hightransverse vaginal septum. Fertil Steril 1992;57:1351–3.
. Rock J. Surgery for anomalies of the Mullerian ducts. In: Rock J, Thomp-son J, eds. TeLinde’s operative gynecology. Philadelphia: Lippincott-
rmoplastic splint material with an elastic belt (right).n to Penrose drains.
F
A theT sew
Raven, 1997:687–792.
Vol. 87, No. 5, May 2007

MMgtMamwmr[aws
rdb(laMr[ymfi
boM
R
T
R
00do
Serum and ovarian Müllerian inhibiting substance,and their decline in reproductive aging
The objectives of this study were to identify whether there is a decline in Müllerian inhibiting substance (MIS)in the female rat during chronological aging, and to define the physiological basis of aging-related changes inMIS. The results demonstrate that there is an exponential decline in both serum and ovarian levels of MIS withincreasing female age, and that the histologic origin for the reduction in serum levels of MIS is a decline inthe number of small ovarian follicles expressing MIS. (Fertil Steril� 2007;87:1227–30. ©2007 by American
Society for Reproductive Medicine.)rwc
ndftipt
b(bnofsPBotf
EcuetQpdtb
so
üllerian inhibiting substance (MIS; also known as anti-üllerian hormone) is a member of the transforming
rowth factor-� superfamily (1). It was localized in prean-ral and small antral follicles (2–10). In experiments using
IS knockout mice, the null females had more preantralnd small antral follicles at 25 days and 4 months, but at 13onths, the null females had almost no primordial follicles,hich suggested that they had an early depletion of pri-ordial follicles (11). Further data indicated that MIS
egulates the development of early follicles in two ways:1] as a negative stimulator of follicular maturation, and [2]s an inhibitor of FSH sensitivity of growing follicles,hich serves to negatively modulate the FSH-dependent
election of dominant follicles (12–14).
Ovarian reserve is a term used to denote the potential foreproduction (15, 16). A number of investigators presentedata to support the hypothesis that MIS could be used as aiomarker of ovarian age and ovarian reserve in humans17–27). In humans, findings showed [1] that serum MISevels decline with increasing reproductive age, [2] thatfter oophorectomy there is a precipitate drop in levels ofIS, [3] that after gonadotropin stimulation for assisted
eproductive technologies, the levels of MIS decline, and4] that the follicular-fluid MIS levels differ betweenounger patients and older patients (17–28). Kevenaar et al.easured serum MIS in mice, and the decline in MIS levels
ound in aging mice is consistent with the results obtainedn humans (29).
It was hypothesized in this study that the physiologicalasis of the age-dependent decline in serum MIS is becausef a decrease in the number of ovarian follicles expressingIS. We sought to determine how the levels of MIS in the
eceived June 16, 2006; revised September 20, 2006; accepted Octo-ber 26, 2006.
his work was presented, in part, as an abstract at the Conference onSystems Biology of Mammalian Cells, Heidelberg, Germany, 2006.
eprint requests: John Yeh, M.D., Department of Gynecology-Ob-stetrics, University of Buffalo, The State University of New York,219 Bryant Street, Buffalo, New York 14222 (FAX: 716-888-3833;
wE-mail: [email protected]).
15-0282/07/$32.00i:10.1016/j.fertnstert.2006.11.011 Copyright ©2007 American Soc
at might change during ovarian chronological aging, ande looked for specific histologic features leading to MIS
hanges in aging.
Female Sprague-Dawley rats were used (Harlan, India-apolis, IN) (30). The animals studied were immature (26ays old; “young”) females, adult (65–75 days old; “adult”)emales, and retired breeders (8–9 months old; “reproduc-ive aging;” retired breeders have smaller litter sizes orncreased estrous-cycle irregularity). This study was ap-roved by the Institutional Animal Care and Use Commit-ee of the University at Buffalo (protocol GYN07042N).
The adult and reproductive-aging animals were studiedoth as estrous-cycle staged and as estrous-cycle nonstaged31). The females of the three age groups were examined ataseline, and were given an ovarian challenge with preg-ant mare serum gonadotropin (PMSG) to replicate pre-vulatory conditions, so as to further distinguish the dif-erences in the three age groups. Therefore, the rats wereacrificed at 0 hours and at 54 hours, after an injection ofMSG (1 IU/g body weight; Sigma, St. Louis, MO) (32).lood was collected via terminal cardiac puncture. Thevaries were collected, with one ovary snap-frozen andhen stored at �80°C, and the other ovary fixed in 10%ormalin for paraffin sectioning.
For measurement of serum MIS, the DSL-10-14400 MISLISA kit was used (DSL, Webster, TX). We used thisommercial kit because it was the intent of this study tonderstand the relative changes of rat MIS levels in differ-nt conditions. Whole ovaries were used for the MIS pro-ein analysis, as prepared by the protocol of Yeh et al. (33).uantitative analysis of MIS levels in ovarian lysates waserformed with the DSL-10-14400 MIS ELISA kit, asescribed. The final results were normalized to “ng/mgotal protein,” to allow comparisons of MIS concentrationsetween the three age groups.
The Western blot method followed a previously de-cribed method (33, 34). Reducing conditions were used toptimize the visualization of MIS proteins. The membranes
ere incubated with goat anti-MIS antibody (1:200, C-20:1227Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

sM
uMSpne(pao
m(uP
slarHcaa
1
c-6886; Santa Cruz Biotechnology, Santa Cruz, CA).
FIGURE 1
Y A RA 0h
Actin
MIS 65 kDa
Y A RA 54h
MIS Positive Follicles
Num
ber o
f MIS
Pos
itive
Fol
licle
s
0
5
10
15
20
25
C
n=6
n=14
n=11
n=6
n=11
n=15
0h 54h
***‡
MIS Levels in Ovarian Lysatesby Western Blot
MIS
Rel
ativ
e B
and
Inte
nsity
0
2000
7000
8000
9000
n=4
B
n=5
n=5
n=4
n=4
n=4
***
***
***
0h 54h
‡‡ ‡‡
Serum MIS Levels M
IS n
g/m
l
01234567 Young
Adult Aging
n=19
n=22
n=36
n=44
n=44
n=24
A
***
*** ***
§§§
§§
0h 54h
###
‡‡
‡‡‡
Yeh. MIS in reproductive aging. Fertil Steril 2007.
embranes were reprobed for actin for normalization. r
228 Yeh et al. Correspondence
Immunofluorescence studies were performed with these of previously described methods (33), with goat anti-IS as primary antibody (1:100 dilution; C-20: sc-6886;
anta Cruz Biotechnology). For the negative control ex-eriments, preimmune serum was applied. To quantify theumber of positive MIS follicles, each ovarian follicle wasvaluated by the criteria of Liao et al. (35) and Yeh et al.33) to obtain a final immunofluorescent score. Two inde-endent observers reviewed the ovarian sections. To obtainrelative ovarian follicle count, a count was obtained in thevarian sections of each age group.
The results are presented as mean � SEM. The experi-ents were repeated 3–6 times. Analysis of variance
ANOVA), followed by Scheffé’s post hoc analysis, wassed for comparison of different groups, when appropriate.�.05 was considered significant.
The serum MIS results show that basal serum MIS levelspontaneously declined in the rat with increasing chrono-ogical age. After the animals were challenged with PMSG,decline in the serum levels of MIS for the young and adult
ats was found (0 hours versus 54 hours, P�.05; Fig. 1A).owever, after stimulation with PMSG, there was no
hange in serum MIS levels in the reproductive-agingnimals (P�NS). In addition, when comparing the rel-tive MIS levels at 54 hours for the young, adult, and
FIGURE 1 CONTINUED
(A) Serum MIS levels in young, adult, andreproductive-aging females, at 0 hours and 54hours after PMSG ovarian stimulation.(B) Ovarian MIS levels in young, adult, andreproductive-aging females. Western blotanalysis of ovarian lysates in young, adult, andreproductive-aging females at 0 hours and 54hours after ovarian stimulation with PMSG.Y, young; A, adult; RA, reproductive aging.(C) Analysis of MIS-positive follicles at baselineand 54 hours after PMSG ovarian stimulation,showing the number of follicles in randomsections that were positively stained for MIS.n � total number of animals studied in a givenage group. ***P�.001, compared with young at0 hours. §§P�.01, compared with young at 54hours. §§§P�.001, compared with young at 54hours. ‡P�.05, compared with adult at 0 hours.‡‡P�.01, compared with adult at 0 hours.‡‡‡P�.001, compared with adult at 0 hours.###P�.001, compared with adult at 54 hours.Comparisons of groups were performed with theuse of ANOVA, followed by Scheffé’s post hocanalysis, when appropriate.
eproductive-aging females, there was still a compara-
Vol. 87, No. 5, May 2007

tnltatsb
qmhamo(fw
ai0mrl
glofMd(s6mi35pfa
idrfalMfani
da
eaMcdrsTiasta
ilMvcsii
cseatFttlfiafMeb
R
Fe
ive stepwise fall in MIS serum levels with rising chro-ological age after PMSG challenge (P�.01). The serumevels of MIS in all stages of the estrous cycle showedhat the serum MIS measurement distinguishes betweendult and reproductive-aging females at every stage ofhe estrous cycle and that, after PMSG stimulation,erum MIS levels continued to be able to differentiateetween the adult and reproductive-aging females.
The ovaries were analyzed by two different methods touantify MIS protein levels. First, ovarian lysates wereeasured for MIS levels by using ELISA. At baseline (0
ours), there was a reduction with increasing chronologicalge (P�.05). Furthermore, for the young and adult fe-ales, there was a decline from 0-hour levels in the
varian lysates 54 hours after stimulation with PMSGP�.05). No decline in the ovarian lysate MIS level wasound in reproductive-aging females after stimulationith PMSG (P�NS).
Western blot analysis showed that at 0 hours, there wasstepwise drop in the 65-kDa MIS protein level with
ncreasing chronological age (P�.05). In addition, the-hour results of the MIS ELISA and Western blot analysisatched the serum results in which the young, adult, and
eproductive-aging ovaries had progressively diminishingevels of MIS (Fig. 1B).
Immunofluorescence showed that for all three ageroups studied, the primary follicles and small antral fol-icles had the most intense staining for MIS. After PMSGvarian stimulation, the primary follicles and small antralollicles continued to have the most intense staining for
IS. The number of the MIS positively stained folliclesecreased with increasing chronological age at 0 hoursP�.001; Fig. 1C). In contrast, the percentage of positivetaining follicles for MIS was relatively constant at 50%–0% for all three age groups at 0 hours (P�NS). Further-ore, after stimulation with PMSG, the percentage of
mmunoreactive follicles declined to the range of 20%–0% for all three age groups (P�.05 for 0 hours versus4 hours, by ANOVA). The decline in number of MIS-ositive small follicles mirrored the stepwise decreaseound in serum MIS levels with increasing chronologicalge.
To our knowledge, the results presented here are the firstn the rat to show that serum and ovarian MIS levelsecline with increasing chronological age. Importantly, theesults described here confirm that the physiological basisor the decline in serum MIS found in aging is likely due todecrease in the total number of MIS-positive small fol-
icles, and not because of a loss in the percentage ofIS-positive follicles. This is in agreement with the results
ound in mice by Kevenaar et al. (29). Their work showedclear association between serum MIS levels and the
umber of small follicles in the aging process. The decline
n levels of serum MIS was highly correlated with thertility and Sterility�
ecline in number of primordial and growing follicles inging mice up to 18 months of age.
Building on the work of Kevenaar et al. (29), our workxtends the understanding of the decline of serum MIS inging in three respects. First, we showed by quantitativeIS Western blot analysis that ovarian MIS protein de-
lined in parallel to the serum MIS changes. Second, weemonstrated that gonadotropin stimulation of the ovariesesulted in a decline in serum MIS levels after ovariantimulation only in the younger reproductive age groups.hird, we showed that the number of MIS-positive follicles
n aging, as demonstrated by immunohistochemistry, par-lleled the serum MIS decline in aging. Thus, our workupports the findings of Kevenaar et al. (29), and extendshe association between serum levels of MIS and aging-ssociated changes found in the ovary.
From the rat data generated in this study, the mathemat-cal curves in chronological aging for both serum MISevels and total ovarian MIS levels could be calculated.
odeling of the decline in MIS with increasing age re-ealed that both calculated curves are exponential decayurves. Our extrapolation is in agreement with the conclu-ions of de Vet et al. (17) and Visser et al. (36), that MISs an early marker of ovarian aging, and that MIS mayndicate ovarian aging earlier than FSH.
The histological basis of the decline in serum MIS inhronological aging had not been characterized until thistudy. In human studies by de Vet et al. (17) and Fanchint al. (19), as subsequently reviewed by Visser et al. (36),correlation was observed between serum MIS levels and
he antral follicle count as determined by ultrasonography.urther, Fanchin et al. (26) showed a correlation between
he ultrasonographically defined small follicle count andhe serum MIS level, and concluded that the serum MISevel may reflect per-follicle MIS follicle production. Thendings reported in this study extend the previous studies,nd show histologically that it is the total number of smallollicles that are MIS-positive that is related to the serum
IS level. Moreover, the present data demonstrate thatven after ovarian stimulation, MIS level reflects the num-er of MIS-positive small follicles.
John Yeh, M.D.Beomsu Kim, Ph.D.Jennifer Peresie,Yuan Jing Liang, Ph.D.Armando Arroyo, M.D.Department of Gynecology-Obstetrics, University at
Buffalo, The State University of New York, Buffalo,New York
EFERENCES1. Lee MM, Donahoe PK. Müllerian inhibiting substance: a gonadal
hormone with multiple functions. Endocr Rev 1993;14:152–64.
1229

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
1
2. Bezard J, Vigier B, Tran D, Mauleon P, Josso N. Immunocytochem-ical study of anti-Müllerian hormone in sheep ovarian follicles duringfetal and post-natal development. J Reprod Fertil 1987;80:509–16.
3. Ueno S, Kuroda T, Maclaughlin DT, Ragin RC, Manganaro TF,Donahoe PK. Müllerian inhibiting substance in the adult rat ovaryduring various stages of the estrous cycle. Endocrinology 1989;125:1060–6.
4. Ueno S, Takahashi M, Manganaro TF, Ragin RC, Donahoe PK.Cellular localization of Müllerian inhibiting substance in the devel-oping rat ovary. Endocrinology 1989;124:1000–6.
5. Baarends WM, Uilenbroek JT, Kramer P, Hoogerbrugge JW, vanLeeuwen EC, Themmen AP, et al. Anti-Müllerian hormone andanti-Müllerian hormone type II receptor messenger ribonucleic acidexpression in rat ovaries during postnatal development, the estrouscycle, and gonadotropin-induced follicle growth. Endocrinology 1995;136:4951–62.
6. Hirobe S, He WW, Gustafson ML, MacLaughlin DT, Donahoe PK.Müllerian inhibiting substance gene expression in the cycling ratovary correlates with recruited or Graafian follicle selection. BiolReprod 1994;50:1238–43.
7. Weenen C, Laven JS, Von Bergh AR, Cranfield M, Groome NP,Visser JA, et al. Anti-Müllerian hormone expression pattern in thehuman ovary: potential implications for initial and cyclic folliclerecruitment. Mol Hum Reprod 2004;10:77–83.
8. Stubbs SA, Hardy K, Da Silva-Buttkus P, Stark J, Webber LJ,Flanagan AM, et al. Anti-Müllerian hormone protein expression isreduced during the initial stages of follicle development in humanpolycystic ovaries. J Clin Endocrinol Metab 2005;90:5536–43.
9. Themmen AP. Anti-Müllerian hormone: its role in follicular growthinitiation and survival and as an ovarian reserve marker. J Natl CancerInst Monogr 2005;34:18–21.
0. Visser JA, Themmen AP. Anti-Müllerian hormone and folliculogen-esis. Mol Cell Endocrinol 2005;234:81–6.
1. Durlinger AL, Kramer P, Karels B, de Jong FH, Uilenbroek JT,Grootegoed JA, et al. Control of primordial follicle recruitment byanti-Müllerian hormone in the mouse ovary. Endocrinology 1999;140:5789–96.
2. Durlinger AL, Gruijters MJ, Kramer P, Karels B, Ingraham HA,Nachtigal MW, et al. Anti-Müllerian hormone inhibits initiation ofprimordial follicle growth in the mouse ovary. Endocrinology 2002;143:1076–84.
3. Durlinger AL, Gruijters MJ, Kramer P, Karels B, Kumar TR, MatzukMM, et al. Anti-Müllerian hormone attenuates the effects of FSH onfollicle development in the mouse ovary. Endocrinology 2001;142:4891–9.
4. Durlinger AL, Visser JA, Themmen AP. Regulation of ovarian func-tion: the role of anti-Müllerian hormone. Reproduction 2002;124:601–9.
5. Arroyo A, Yeh J. Understanding the menopausal transition, andmanaging its clinical challenges. Sex Reprod Menopause 2005;3:12–7.
6. Practice Committee of the American Society for Reproductive Med-icine. Aging and infertility in women. Fertil Steril 2004;82(Suppl 1):S102–6.
7. de Vet A, Laven JS, de Jong FH, Themmen AP, Fauser BC. Anti-Müllerian hormone serum levels: a putative marker for ovarian aging.Fertil Steril 2002;77:357–62.
8. van Rooij IA, Broekmans FJ, te Velde ER, Fauser BC, Bancsi LF, deJong FH, Themmen AP. Serum anti-Müllerian hormone levels: anovel measure of ovarian reserve. Hum Reprod 2002;17:3065–71.
9. Fanchin R, Schonauer LM, Righini C, Guibourdenche J, Frydman R,Taieb J. Serum anti-Müllerian hormone is more strongly related toovarian follicular status than serum inhibin B, estradiol, FSH and LH
on day 3. Hum Reprod 2003;18:323–7.230 Yeh et al. Correspondence
0. Hazout A, Bouchard P, Seifer DB, Aussage P, Junca AM, Cohen-Bacrie P. Serum anti-Müllerian hormone/Müllerian-inhibiting sub-stance appears to be a more discriminatory marker of assisted repro-ductive technology outcome than follicle-stimulating hormone,inhibin B, or estradiol. Fertil Steril 2004;82:1323–9.
1. van Rooij IA, Tonkelaar I, Broekmans FJ, Looman CW, Scheffer GJ,de Jong FH, et al. Anti-Müllerian hormone is a promising predictorfor the occurrence of the menopausal transition. Menopause 2004;11:601–6.
2. Fanchin R, Taieb J, Lozano DH, Ducot B, Frydman R, Bouyer J. Highreproducibility of serum anti-Müllerian hormone measurements sug-gests a multi-staged follicular secretion and strengthens its role in theassessment of ovarian follicular status. Hum Reprod 2005;20:923–7.
3. Pastor CL, Vanderhoof VH, Lim LCL, Calis KA, Premkumar A,Guerrero NT, et al. Pilot study investigating the age-related decline inovarian function of regularly menstruating normal women. FertilSteril 2005;84:1462–9.
4. Tremellen KP, Kolo M, Gilmore A, Lekamge DN. Anti-Müllerianhormone as a marker of ovarian reserve. Aust N Z J Obstet Gynaecol2005;45:20–4.
5. van Rooij IA, Broekmans FJ, Scheffer GJ, Looman CW, HabbemaJD, de Jong FH, et al. Serum anti-Müllerian hormone levels bestreflect the reproductive decline with age in normal women withproven fertility: a longitudinal study. Fertil Steril 2005;83:979–87.
6. Fanchin R, Louafi N, Lozano DH, Frydman N, Frydman R, Taieb J.Per-follicle measurements indicate that anti-Müllerian hormone se-cretion is modulated by the extent of follicular development andluteinization and may reflect qualitatively the ovarian follicular status.Fertil Steril 2005;84:167–73.
7. Muttukrishna S, McGarrigle H, Wakim R, Khadum I, Ranieri DM,Serhal P. Antral follicle count, anti-Mullerian hormone and inhibin B:predictors of ovarian response in assisted reproductive technology?Br J Obstet Gynaecol 2005;112:1384–90.
8. La Marca A, De Leo V, Giulini S, Orvieto R, Giannella L, Volpe A.Anti-Müllerian hormone in premenopausal women and after sponta-neous or surgically induced menopause. J Soc Gynecol Invest 2005;12:545–8.
9. Kevenaar ME, Meerasahib MF, Kramer P, van de Lang-Born BMN,de Jong FH, Groome NP, et al. Serum anti-Müllerian hormone levelsreflect the size of the primordial follicle pool in mice. Endocrinology2006;147:3228–34.
0. Palumbo A, Yeh J. In situ localization of apoptosis in the rat ovaryduring follicular atresia. Biol Reprod 1994;51:888–95.
1. Marcondes FK, Bianchi FJ, Tanno AP. Determination of the estrouscycle phases of rats: some helpful considerations. Braz J Biol 2002;62:609–14.
2. Soodak LK, Behrman HR. Mitochondria mediate amplification ofluteinizing hormone action by adenosine in luteal cells. Endocrinol-ogy 1988;122:1308–13.
3. Yeh J, Kim B, Liang YJ, Peresie J. Müllerian inhibiting substance asa novel biomarker of cisplatin-induced ovarian damage. BiochemBiophys Res Commun 2006;348:337–44.
4. Khan SM, Oliver RH, Yeh J. Epidermal growth factor receptorinhibition by tyrphostin 51 induces apoptosis in luteinized granulosacells. J Clin Endocrinol Metab 2005;90:469–73.
5. Liao Y, Abel U, Grobholz R, Hermani A, Trojan L, Angel P, et al.Up-regulation of insulin-like growth factor axis components in humanprimary prostate cancer correlates with tumor grade. Hum Pathol2005;36:1186.
6. Visser JA, de Jong FH, Laven JSE, Themmen APN. Anti-Müllerianhormone: a new marker for ovarian function. Reproduction 2006;131:
1–9.Vol. 87, No. 5, May 2007

Iut(cwidtaaft
tecpLpntariipd6
idp
RT
R
00do
The levonorgestrel-releasing intrauterine systemand endometriosis staging
This study aims to determine whether the levonorgestrel-releasing intrauterine system can influence AmericanSociety for Reproductive Medicine endometriosis staging scores, as assessed through second-look laparos-copies, and to compare the results with those obtained with a GnRH agonist. Both treatments reduced theextent of pelvic endometriotic lesions in patients with chronic pelvic pain. (Fertil Steril� 2007;87:1231–4. ©
2007 by American Society for Reproductive Medicine.)ulspteapwftptsmpmbnoWop(tPiisdnFid
rbtbm
t has been shown that the levonorgestrel-releasing intra-terine system (LNG-IUS) is a viable therapeutic option forhe treatment of pelvic pain in patients with endometriosis1–3). The drugs previously used to treat such pain in-luded progestagens (such as danazol and gestrinone),hich have an antiestrogen effect, as well as drugs that
nduce pseudomenopause (e.g., GnRH agonists) or pseu-opregnancy (e.g., combined oral contraceptives). Al-hough effective, most of these options have been associ-ted with systemic side effects that can affect treatmentdherence and preclude long-term use. In addition, the needor repeated or regular administration also compromisesreatment adherence and therefore efficacy.
The LNG-IUS release of levonorgestrel (a 19-C proges-ogen) into the uterine cavity restricts its effects almostxclusively to within the endometrium, where the highoncentrations of levonorgestrel induce atrophy andseudodecidualization (4, 5). It is well established thatNG-IUS treatment reduces the chronic pelvic pain accom-anying endometriosis. However, only one observational,oncomparative study, in which patients were treated withhe LNG-IUS for 6 months, has shown a favorable alter-tion in the staging of endometriosis (6). Therefore, aandomized, controlled clinical study was conducted tonvestigate the efficacy of 6 months of LNG-IUS treatmentn the symptomatic relief of endometriosis, as well as theosttreatment changes in the laparoscopic staging of theisease, and to compare the results to those obtained aftermonths of treatment with a GnRH agonist (GnRHa).
Twenty-two female patients ages 18 to 40 years werencluded in this controlled clinical study, which was con-ucted from February 2003 to May 2005. All participatingatients were under treatment at the pelvic pain clinic of a
eceived June 8, 2005; revised and accepted November 8, 2006.he levonorgestrel-releasing intrauterine system (Mirena) and GnRH-agonist ampules were provided free of charge by Schering, SãoPaulo, Brazil.
eprint requests: Rui Alberto Ferriani, M.D., Departamento de Gineco-logia e Obstetrícia, Faculdade de Medicina de Ribeirão Preto–USP,Avenue Bandeirantes, 3900 8° Andar, Ribeirão Preto–SP, Brasil (FAX:
V16-3633-9633; E-mail: [email protected]).
15-0282/07/$32.00i:10.1016/j.fertnstert.2006.11.044 Copyright ©2007 American Soc
niversity hospital. Initial inclusion criteria were havingaparoscopically and histologically confirmed endometrio-is (made 3 months before enrollment in the study) andresenting chronic pelvic pain that was cyclic. In addition,he visual analog scale (VAS), which consists of subjectivevaluation of pain on a scale from 0 to 10 (0 being no painnd 10 being the most severe pain), was applied during theretreatment phase, and only those patients scoring � 3ere included in the study. All subjects gave written in-
ormed consent, and the study protocol was approved byhe institutional review boards of the university. All of theatients had been having regular menstrual periods (at 25-o 35-day intervals) for � 3 months before entering thetudy, had not used any hormonal therapy for at least 3onths before the study, and had not taken long-acting
rogestins or GnRHa therapy within the preceding 9onths. None of the patients had been breastfeeding or had
een pregnant during the 3 months preceding the study, andone had a history of osteoporosis, coagulation disorders,r contraindications to the LNG-IUS as defined by theorld Health Organization. A computer-generated system
f sealed envelopes was used to randomly allocate theatients to receive 6 months of treatment with an LNG-IUSMirena; Schering Oy, Helsinki, Finland) or 6 months ofreatment with a GnRHa (Lupron depot 3.75 mg; TAPharmaceuticals, Lake Forest, IL), the latter administered
n 6 doses (1 ampule IM every 28 � 3 days). Each groupnitially consisted of 11 patients. The LNG-IUS was in-erted or GnRHa treatment was initiated within the first 7ays of the menstrual cycle. Patients were instructed to useo medication other than that provided during the study.ollow-up visits were scheduled every 28 � 3 days after
nitiation of treatment to have at least six completed visitsuring the study period.
Pain was evaluated by comparing the mean VAS scoreecorded each month with that registered in the monthefore the study outset. In addition, the patients recordedhe daily occurrence and intensity of their pain in a VAS-ased pain diary (3). The score was recorded in the diary byarking a single point along a 10-cm line. The monthly
AS-based pain diary score was calculated as the sum of1231Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

to
ltSTasct
IunawpV
ielddpm3Gssbms
i(pT�a(ia
tsm(eilt
Vt1pm(G�ibom
sascstLcfiiawss
1
he daily scores divided by the number of days in eachbservation period.
In the baseline laparoscopy, as well as in the second-lookaparoscopy, the disease was staged, with video documen-ation, according to the criteria established by the Americanociety for Reproductive Medicine (ASRM) in 1997 (7).he pretreatment and posttreatment clinical evaluationsnd surgical procedures were performed by different phy-icians. Therefore, those performing the second-look pro-edures and evaluations were blinded regarding the pre-reatment endometriosis staging.
The GraphPad Prism 2.01 program (GraphPad Softwarenc., San Diego, CA) was used for the statistical analysis,sing Student’s t test for the quantitative variables withormal distribution. For qualitative variables, Fisher’s ex-ct test was used. Values at the time of insertion of the IUSere compared with those at 6 months after insertion usingaired Student’s t test or the Wilcoxon test, as appropriate.alues of P�.05 were considered statistically significant.
Of the 22 female patients initially selected for study, 4 (1n the LNG-IUS group and 3 in the GnRHa group) werexcluded for having refused to be submitted to the second-ook laparoscopy. There were no statistically significantifferences between the two groups with respect to baselineata, including age, stage of endometriosis, smoking habits,arity, and use of medication before the study outset. Theean age of the remaining subjects was 29.2 � 5.5 and
2.6 � 5.3 years, respectively, in the LNG-IUS andnRHa groups. In the LNG-IUS group, three patients
cored between 3 and 7 on the pretreatment VAS, whereaseven patients scored �7. In the GnRHa group, six scoredetween 3 and 7, whereas two scored �7, on the pretreat-ent VAS. The difference between the two groups was not
tatistically significant (P�.0698).
After 6 months of treatment, the ASRM stage was lowern 6 (60%) of the 10 LNG-IUS group patients and in 337.5%) of the 8 GnRHa group patients (P�.1698). Theretreatment and posttreatment ASRM stages are shown inable 1. The mean ASRM scores decreased from 34
27.9 to 21.3 � 20.5 in the LNG-IUS group (P�.1612)nd from 42.4 � 30.3 to 30.8 � 22.8 in the GnRHa groupP�.0546), with no intergroup difference. Only one patientn each group presented an increase in the ASRM scorefter treatment.
Mean pretreatment VAS pain scores were 7.9 � 1.2 inhe LNG-IUS group and 6.5 � 1.1 in the GnRHa group. Aignificant reduction in this score was achieved after 6onths of treatment: 2.1 � 2.7 (P�.0001) and 0.4 � 1.1
P�.0001), respectively. There was no intergroup differ-nce. Pain was found to have been reduced in all patients,n those who presented improved staging in the second-ook laparoscopy, as well as in those who did not. Among
he patients who presented such an improvement, the mean t232 Gomes et al. Correspondence
AS pain score decreased from 8.1 � 1.2 to 2.1 � 2.9 inhe LNG-IUS group (P�.0313) and from 5.7 � 0.6 cm to
� 1.7 cm (P�.25) in the GnRHa group. Among theatients who presented no improvement in staging, theean VAS pain score decreased from 7.5 � 1.3 to 2 � 2.8
P�.125) in the LNG-IUS group and from 7 � 1 to 0 in thenRHa group. All posttreatment VAS pain scores were3, with the exception of those reported by three patients
n the LNG-IUS group, who presented VAS pain scoresetween 3 and 7 after 6 months of treatment. For all threef those patients, the endometriosis was staged as mild orinimal in the second-look laparoscopy.
To the best of our knowledge, this is the first randomizedtudy comparing the LNG-IUS with a GnRHa and evalu-ting the effect of these two drugs on the laparoscopictaging of endometriosis and on endometriosis-associatedhronic pelvic pain. Despite the fact that we found noignificant reduction in the ASRM endometriosis score inhe second-look laparoscopy, 60% of the patients in theNG-IUS group presented altered (lower) disease stage,ompared with 37.5% of those in the GnRHa group. Thisnding is corroborated by the results of uncontrolled clin-
cal trials, in which significant improvements in stagingfter the isolated use of a GnRHa (8) or of the LNG-IUS (6)ere found. It is likely that the lack of a statistically
ignificant difference in the present study is related to themall size of the study sample. The reduction in endome-
TABLE 1Laparoscopic staging of endometriosisaccording to ASRM criteria before and after6 months of treatment with the LNG-IUS ora GnRHa in female patients with chronicpelvic pain.
GroupBaselinestage (n)
Second-lookstage (n)
LNG-IUS Mild (3) Minimal (2)Improvement in 6
(60%) of the 10Mild (1)
Moderate (3) Mild (1)Moderate (1)Severe (1)
Severe (4) Mild (1)Moderate (2)Severe (1)
GnRHa Mild (1) Moderate (1)Improvement in 3
(37.5%) of the 8Moderate (3) Mild (2)
Moderate (1)Severe (4) Moderate (1)
Severe (3)Gomes. The LNG-IUS and endometriosis staging. Fertil Steril 2007.
riosis score and staging in the patients treated with the
Vol. 87, No. 5, May 2007

GeaiTdttwatppt(di
s(mtitbue
tClcbs(ioIotitbr
ataNvtrti
lctptb
R
1
1
1
1
Fe
nRHa is probably attributable to the intense antiestrogenffect of the drug (9) because endometriosis is known to ben estrogen-dependent disease (10), a fact that would implynhibition of the proliferation of ectopic endometrial tissue.herefore, the GnRHa was shown to be efficacious inecreasing endometriosis proliferation by increasing apop-osis (11), which is typically minimal in endometrioticissue. It must be borne in mind that the clinical treatment,hether with the LNG-IUS or with the GnRHa, was not
dministered in isolation. Therein lies the importance ofesting a new treatment modality (the LNG-IUS) in com-arison with a classic treatment (a GnRHa). All of theatients had previously undergone laparoscopy, which, al-hough primarily diagnostic, had a therapeutic functioncauterization of the peritoneal lesions and excision of theeeper endometriotic lesions), thereby influencing the stag-ng in the second-look laparoscopy.
No correlation has been found between endometriosistage and the intensity of the accompanying pelvic pain12). Therefore, we cannot infer that the clinical improve-ent in the level of pelvic pain in endometriosis patients
reated with the LNG-IUS is directly related to a reductionn the number and extent of the lesions. However, produc-ion of some serum markers, such as CA-125, that seem toe related to endometriosis progression is reduced by these of LNG-IUS (13), suggesting that the system has anffect on endometriosis lesions.
The exact mechanism by which the LNG-IUS influenceshe course of endometriosis remains unclear. According toritchley et al. (14), the LNG-IUS releases high doses of
evonorgestrel into the uterine cavity, promoting rapid de-idualization of the endometrial stroma. In addition, it haseen shown that the LNG-IUS induces a decrease in andubsequent blockage of DNA synthesis and mitotic activity15), suggesting that progesterone plays a moderating rolen the endometrial proliferation. Such moderation was alsobserved by Vereide et al. (16), who found that the LNG-US promotes endometrial apoptosis by reducing expressionf the Bcl-2 gene, which has an antiapoptotic effect. Althoughhe effect of levonorgestrel is primarily local, it is also foundn the peritoneal fluid of its users (17). Therefore, the effectshat levonorgestrel has on the normal endometrium might alsoe seen in the ectopic endometrium, which could explain theeduced disease progression.
In this study, we found that treatment with the LNG-IUSnd with the GnRHa provided similar results, presenting aendency toward improvement in the endometriosis stage,s assessed after 6 months in the second-look laparoscopy.evertheless, the potential influence of the surgical inter-ention performed during the initial laparoscopy must beaken into consideration. In addition, it is of note thateduced pelvis pain was not found to be necessarily relatedo altered ASRM score or endometriosis surgical staging. It
s possible that further studies of these drugs, involvingrtility and Sterility�
arger patient samples, would show a statistically signifi-ant improvement in the laparoscopic staging of endome-riosis. However, the LNG-IUS can be used for longereriods and is more cost-effective, making it a more attrac-ive option for the treatment of chronic pelvic pain causedy endometriosis.
Mariana Kefalás Oliveira Gomes, M.D.Rui Alberto Ferriani, M.D.Júlio Cesar Rosa e Silva, M.D.Ana Carolina Japur de Sá Rosa e Silva, M.D.Carolina Sales Vieira, M.D.Francisco José Cândido dos Reis, M.D.Department of Gynecology and Obstetrics, University
of São Paulo at Ribeirão Preto School of Medicine,Ribeirão Preto, Brazil
EFERENCES1. Vercellini P, Frontino G, De Giorgi O, Aimi G, Zaina B, Crosignani
PG. Comparison of a levonorgestrel-releasing intrauterine deviceversus expectant management after conservative surgery for symp-tomatic endometriosis: a pilot study. Fertil Steril 2003;80:305–9.
2. Lockhat FB, Emembolu JO, Konje JC. The efficacy, side-effects andcontinuation rates in women with symptomatic endometriosis under-going treatment with an intra-uterine administered progestogen(levonorgestrel): a 3-year follow-up. Hum Reprod 2005;20:789–93.
3. Petta CA, Ferriani RA, Abrao MS, Hassan D, Rosa e Silva JC,Podgaec S, et al. Randomized clinical trial of a levonorgestrel-releasing intrauterine system and a depot GnRH analogue for thetreatment of chronic pelvic pain in women with endometriosis. HumReprod 2005;20:1993–8.
4. Silverberg SG, Haukkamaa M, Arko H, Nilsson CG, LuukkainenT. Endometrial morphometry of women during long term use oflevonorgestrel intrauterine system. Int Gynaecol Pathol 1986;5:235– 41.
5. Maruo T, Laoag-Fernandez JB, Pakarinen P, Murakoshi H, Spitz IM,Johansson E. Use of a levonorgestrel intrauterine system on prolifer-ation and apoptosis in the endometrium. Hum Reprod 2001;16:2103–8.
6. Lockhat FB, Emembolu JO, Konje JC. The evaluation of the effec-tiveness of an intrauterine-administered progesterone (levonorgestrel)in the symptomatic treatment of endometriosis and in the staging ofthe disease. Hum Reprod 2004;19:179–84.
7. Revised American Society for Reproductive Medicine classificationof endometriosis: 1996. Fertil Steril 1997;67:817–21.
8. Mettler L, Steinmuller H, Schachner-Wunschmann E. Experiencewith a depot GnRH-agonist (Zoladex) in the treatment of genitalendometriosis. Hum Reprod 1991;6:694–8.
9. Casper RF. Clinical uses of gonadotropin-releasing hormone ana-logues. CMAJ 1991;144:153–8.
0. Bruner KL, Matrisian LM, Rodgers WH, Gorstein F, Osteen KG.Suppression of matrix metalloproteinases inhibits establishment ofectopic lesions by human endometrium in nude mice. J Clin Invest1997;99:2851–7.
1. Meresman GF, Bilotas MA, Lombardi E, Tesone M, Sueldo C,Baranao RI. Effect of GnRH analogues on apoptosis and release ofinterleukin-1beta and vascular endothelial growth factor in endome-trial cell cultures from patients with endometriosis. Hum Reprod2003;18:1767–71.
2. Whiteside JL, Facone T. Endometriosis-related pelvic pain: what isthe evidence? Clin Obstet Gynecol 2003;46:824–30.
3. Rosa e Silva ACJS, Rosa e Silva JC, Nogueira AA, Petta CA, Abrão
MA, Ferriani RA. The levonorgestrel-releasing intrauterine device1233

1
1
1
1
1
reduces CA-125 serum levels in patients with endometriosis. FertilSteril. In press.
4. Critchley HO, Wang H, Jones RL, Kelly RW, Drudy TA, Gebbie AE,et al. Morphological and functional features of endometrial decidu-alization following long-term intra-uterine levonorgestrel delivery.Hum Reprod 1998;13:1218–24.
5. Bergeron C. Morphological changes and protein secretion induced byprogesterone in the endometrium during the luteal phase in prepara-
tion for nidation. Hum Reprod 2000;15 Suppl 1:119–28.234 Gomes et al. Correspondence
6. Vereide AB, Kaino T, Sager G, Orbo A, Scottish GynaecologicalClinical Trials Group. Bcl-2, BAX, and apoptosis in endometrialhyperplasia after high dose gestagen therapy: a comparison ofresponses in patients treated with intrauterine levonorgestrel andsystemic medroxyprogesterone. Gynecol Oncol 2005;97:740 –50.
7. Lockhat FB, Emembolu JE, Konje JC. Serum and peritoneal fluidlevels of levonorgestrel in women with endometriosis who weretreated with an intrauterine contraceptive device containing levonorg-
estrel. Fertil Steril 2005;83:398–404.Vol. 87, No. 5, May 2007

Tahbtwdpt
RpstIa8yhabcwdusrfa
pO
RR
00do
The influence of abdominal ultrasound-guidedembryo transfer on pregnancy rate: a preliminaryreport
To determine whether the use of abdominal ultrasound-guided embryo transfer improves the clinical preg-nancy rate in patients undergoing in vitro fertilization, 50 fresh cycles with day 3 embryo transfer werestudied; 27 patients were randomized to ultrasound-guided transfers, and 23 patients were randomized toclinical touch transfers. Although the clinical pregnancy rate was not statistically different (18.5% in theultrasound-guided group vs. 17.4% in the clinical touch group), the use of abdominal ultrasound during theembryo transfer procedure provided a greater degree of confidence and satisfaction to both patients and
physicians. (Fertil Steril� 2007;87:1235–7. ©2007 by American Society for Reproductive Medicine.)ncIG3saflwd(TioaBn
FweIgmuo(CstttitT
he use of ultrasound guidance during embryo transfer inn effort to improve the pregnancy rate has been suggested;owever, a significantly higher rate of pregnancy has noteen consistently demonstrated (1–12). The objective ofhe present prospective controlled study was to determinehether the use of abdominal ultrasonographic guidanceuring embryo transfer improves the pregnancy rate com-ared with the current practice of clinical touch embryoransfer.
This study was approved by the Committee of Medicalesearch Reviewing of Cathay General Hospital, and allatients participating in the study gave their informed con-ent. Fifty patients who were candidates for day 3 embryoransfer were enrolled between June 2002 and May 2003.nclusion criteria were: 1) at least 1 grade 2 embryo avail-ble for transfer; and 2) the embryo to be transfered at the-cell stage. Exclusion criteria were: 1) patient age �40ears; 2) cleaved embryos with less than 8 cells; 3) patientistory of three previous failed assisted conception cycles;nd 4) anticipated difficulty with the embryo transfer. Em-ryo scoring was established by reference to the number ofells and the percentage of cytoplasmic fragments. Patientsere randomized by means of a computer-generated ran-om number sequence at the time their cycles were sched-led. Twenty-seven patients were randomized to the ultra-ound-guided embryo transfer group, and 23 patients wereandomized to the clinical touch group. All embryo trans-ers were fresh cycles and were performed by the samettending physician.
Patients were down-regulated with GnRH analog (Lu-ron [leuprolide acetate], 0.2 �g/day SC; Takeda, Japan).n day 3 of the treatment cycle, recombinant FSH (Go-
eceived March 4, 2006; revised and accepted November 9, 2006.eprint requests: Tsung-Hsuan Lai, M.D., Department of Obstetricsand Gynecology, Cathay General Hospital, 280, Ren-Ai Road,Section 4, Taipei 106, Taiwan (Fax: �886 –2-27092063; E-mail:
15-0282/07/$32.00i:10.1016/j.fertnstert.2006.11.026 Copyright ©2007 American Soc
al-F; Serono, Switzerland) at a dose of 225–300 IU/day,ombined with hMG (Pergonal; Serono) at a dose of 150U/day, was administrated for 3 days. From cycle day 6,onal-F was independently administered at a fixed dose of00 IU/day for 4 days. Ovarian response was monitored byerial transvaginal ultrasound scanning and serum E2, LH,nd P measurement. Human chorionic gonadotrophin (Pro-asi; Serono), 10,000 IU, was given IM when the twoeading follicles reached 18 mm in mean diameter and thereere at least two other follicles greater than 14 mm in meaniameter. Transvaginal ultrasound-guided oocyte retrievalAloka SSD-650 with a 5-MHz transducer; Aloka Co.,okyo, Japan) was scheduled 36 hours after the hCG
njection. Embryo transfer was performed on day 3 afterocyte retrieval. Luteal phase was supported by vaginaldministration of 600 mg/day micronized P (Utrogestan;esins International Belgique, Beinheim, France) begin-ing on the day of oocyte retrieval.
After preparation of the external genitalia and cervix, arydman soft catheter (Laboratoires C.C.D., Paris, France)as loaded by introducing a 1-�L air gap into the proximal
nd of the catheter, followed by 15 �L Medicult UniversalVF medium (catalog number 1031; Medicult, Copenha-en, Denmark) containing the embryos, and finally a ter-inal 1-�L air gap at the distal end of the catheter. In the
ltrasound-guided group, both the insertion and positioningf the catheter were facilitated by abdominal ultrasoundAloka SSD-500 with a convex 3.5-MHz transducer; Alokao.). The embryos were slowly released when the ultra-
ound scan revealed the tip of the catheter within 1 cm ofhe fundus. Ultrasonography also permitted visualization ofhe transfer bubble after the embryos had been expelled. Inhe clinical touch group, the embryos were released accord-ng to the attending physician’s judgment that the catheterip was as close to the fundus as possible without contact.hree to five embryos were transfered in each patient,
epending on the age of the patient, the number of previous1235Fertility and Sterility� Vol. 87, No. 5, May 2007iety for Reproductive Medicine, Published by Elsevier Inc.

ea
ocplp
totottbWmS(w(
tmitun
rdmftum
sbcfau
1
mbryo transfers, and the number and quality of embryosvailable for transfer.
A positive serum �-hCG test performed 2 weeks afterocyte recovery (11 days after the embryo transfer), wasonsidered to be a positive pregnancy outcome. Clinicalregnancy was confirmed by an ultrasound scan showing ateast 1 sac in the uterine cavity 2 weeks after the positiveregnancy test.
There were no statistically significant differences be-ween the 2 groups with respect to age, causes of infertility,r characteristics of IVF (Table 1). Additionally, althoughhe power calculation for this study is relatively low (8%)wing to the limited number of cases, there was no statis-ically difference in the clinical pregnancy rate between thewo groups of patients. (Power estimation was calculatedy the program Power and Samples Size Calculation, byilliam D. Dupont et al., Division of Biostatistics, Depart-ent of Preventive Medicine, Vanderbilt Universitychool of Medicine, 1996.) In the ultrasound group, 18.5%5 out of 27) of the patients became pregnant, comparedith 17.4% (4 out of 23) in the clinical touch group
ABLE 1Characteristics of IVF patients.
CharacteristicUltras
gro
Age (yrs) 34Cause of infertility (%)
Tubal 22Ovarian 11Male 14Endometriosis 18Multiple 25Unexplained 7
Day 3 FSH (mIU/mL) 4Day 3 LH (mIU/mL) 3Day 3 E2 (pg/mL) 16Number of follicles 18Day 9 LH (mIU/mL) 3Day 9 E2 (pg/mL) 1,869Day 9 P (pg/mL) 1Endometrium (mm) 12hCG day LH (mIU/mL) 104hCG day E2 (pg/mL) 2,136hCG day P (pg/mL) 6Oocytes retrieved 10Embryos transfered 5Pregnancy rate (%) 18Note: Values are mean � standard deviation unless other
Chen. Ultrasound-guided embryo transfer. Fertil Steril 2007.
P�.918). a
236 Chen et al. Correspondence
There is a growing body of evidence indicating that theraditional method of embryo transfer is inadequate anday contribute to decreased IVF success (13, 14). A lim-
ted number of studies have addressed the technical aspectshat might influence the outcome of embryo transfer, andltrasound-guided embryo transfer has been evaluated by aumber of clinicians, with conflicting results (1–12).
In one large serial study, Tang et al. (4) reported aandomized controlled trial comparing embryo transfer un-er ultrasound guidance (n � 400) vs the clinical touchethod (n � 400). A total of 441 fresh cycles and 359
rozen-thawed cycles were included in the study. Althoughhe overall implantation rate was significantly higher in theltrasound-guided group, there was no significant improve-ent in the pregnancy rate.
Compared with the traditional method, abdominal ultra-ound-guided embryo transfer has a number of potentialenefits. First, with the guidance of ultrasound, the catheteran be bent to easily pass through the cervical canal andollow the uterine axis, which helps avoid overstimulationnd injury to the cervix and uterus, because excessiveterine contraction at the time of embryo transfer has been
d-guidedn � 27)
Clinical touchgroup (n � 23)
3.6 32.6 � 3.6
/27) 26.1 (6/23)/27) 17.4 (4/23)/27) 13.0 (3/23)/27) 4.3 (1/23)/27) 17.4 (4/23)/27) 21.7 (5/23)1.5 4.2 � 2.23.3 3.6 � 2.98.8 20.6 � 10.98.5 17.7 � 8.52.9 3.9 � 2.81,169.9 1,996.3 � 1,298.51.0 1.2 � 0.82.6 11.5 � 2.327.3 97.9 � 27.71,283.9 2,275.0 � 1,350.46.5 7.4 � 5.77.3 11.7 � 6.91.6 4.5 � 1.7/27) 17.4 (4/23)stated.
T
ounup (
.0 �
.2 (6
.1 (3
.8 (4
.5 (5
.9 (7
.4 (2
.1 �
.8 �
.9 �
.9 �
.5 �
.1 �
.2 �
.1 �
.9 �
.4 �
.9 �
.6 �
.0 �
.5 (5wise
ssociated with lower clinical pregnancy rates (15, 16).
Vol. 87, No. 5, May 2007

StearfecrcTsccf
upofsiScacspf
fntsgtuomuti
ACt
R
1
1
1
1
1
1
1
1
Fe
econd, the entire process of catheterization and release ofhe embryos can be visualized, making it easier to place thembryos in the correct position within the uterus. Pope etl. (17) reported that implantation and clinical pregnancyates are significantly influenced by the transfer distancerom the uterine fundus, i.e., for every additional millimetermbryos are deposited away from the fundus, the odds oflinical pregnancy increases by 11%. Kojima et al. (11)eported that 1.5 cm was a more suitable distance than 1m, and significantly improves the clinical pregnancy rate.hey also found that a distance less than 1 cm decreases theuccess of embryo implantation. Finally, accurate uterineavity depth measurement by ultrasound before transfer islinically useful to avoid contact of the catheter tip with theundus.
In the present randomized prospective study, the use ofltrasound-guided embryo transfer did not lead to an im-roved pregnancy rate. There are several original featuresf this study that minimize the influence of potential con-ounding variables. First, the two groups of patients wereimilar with respect to the known clinical factors thatnfluence pregnancy rate in fresh embryo transfer cycles.econd, all transfers were carried out by the same physi-ian, thus avoiding the impact of an operator factor. Third,ll embryo transfers were performed in artificially preparedycles with prior pituitary suppression. Finally, we used theame soft transfer catheter according to a standardizedrotocol to avoid confounding effects resulting from dif-erent instruments.
In conclusion, in the present study embryo transfer per-ormed under abdominal ultrasound guidance did not sig-ificantly improve the clinical pregnancy rate for patientsreated with IVF. However, the use of abdominal ultra-ound during the embryo transfer procedure provided areater degree of confidence and satisfaction to both pa-ients and physicians. Under the guidance of abdominalltrasound the entire process of catheterization and releasef the embryos can be visualized, thus guaranteeing place-ent of the embryos at the optimal location within the
terus. In addition, it is possible that minimizing endome-rial trauma may decrease myometrial contractions, whichn turn may enhance implantation.
cknowledgments: We are grateful to Dr. Pa-Chun Wang and Ya-Huihen, M.H.A., of the Medical Research Institute, Cathay General Hospi-
al, Taipei, Taiwan, for statistical evaluation of the data.
Su-Chee Chen, M.D.a
Tsung-Hsuan Lai, M.D.a,b
Fa-Kung Lee, M.D.ca Assisted Reproductive Unit, Department of Obstetrics
and Gynecology, Cathay General Hospital, Taipei,
rtility and Sterility�
Taiwan; b Fu Jen Catholic University School ofMedicine, Taipei, Taiwan; and c Department ofObstetrics and Gynecology, HsinuChu Branch,Cathay General Hospital, Hsin Chu, Taiwan
EFERENCES1. Strickler RC, Christianson C, Crane JP, Curato A, Knight AB, Yang
V. Ultrasound guidance for human embryo transfer. Fertil Steril1985;43:54–61.
2. Kan AK, Abdalla HI, Gafer AH, Nappi L, Ogunyemi BO, Thomas A,et al. Embryo transfer: ultrasound-guided versus clinical touch. HumReprod 1999;14:1259–61.
3. Coroleu B, Carreras O, Veiga A, Martell A, Martinez F, Belil I, et al.Embryo transfer under ultrasound guidance improves pregnancy ratesafter in-vitro fertilization. Hum Reprod 2000;15:616–20.
4. Tang OS, Ng EH, So WW, Ho PC. Ultrasound-guided embryotransfer: a prospective randomized controlled trial. Hum Reprod2001;16:2310–5.
5. Matorras R, Urquijo E, Mendoza R, Corcostegui B, Exposito A,Rodriguez-Escudero FJ. Ultrasound-guided embryo transfer improvespregnancy rates and increases the frequency of easy transfers. HumReprod 2002;17: 1762–6.
6. Li R, Lu L, Hao G, Zhong K, Cai Z, Wang W. Abdominal ultrasound-guided embryo transfer improves clinical pregnancy rates after invitro fertilization: experiences from 330 clinical investigations. JAssist Reprod Genet 2005;22: 3–8.
7. Garcia-Velasco JA, Isaza V, Martinez-Salazar J, Landczabal A, Re-quena A, Remohi J, et al. Transabdominal ultrasound-guided embryotransfer does not increase pregnancy rates in oocyte recipients. FertilSteril 2002;78:534–9.
8. Hurley VA, Osborn JC, Leoni MA, Leeton J. Ultrasound-guidedembryo transfer: a controlled trial. Fertil Steril 1991;55:559–62.
9. al-Shawaf T, Dave R, Harper J, Linehan D, Riley P, Craft I. Transferof embryos into the uterus: how much do technical factors affectpregnancy rates? J Assist Reprod Genet 1993;10:31–6.
0. Lindheim SR, Cohen MA, Sauer MV. Ultrasound guided embryotransfer significantly improves pregnancy rates in women undergoingoocyte donation. Int J Gynaecol Obstet 1999;66:281–4.
1. Kojima K, Nomiyama M, Kumamoto T, Matsumoto Y, Iwasaka T.Transvaginal ultrasound-guided embryo transfer improves pregnancyand implantation rates after IVF. Hum Reprod 2001;16:2578–82.
2. Flisser E, Grifo JA, Krey LC, Noyes N. Transabdominal ultrasound-assisted embryo transfer and pregnancy outcome. Fertil Steril 2006;85:353–7.
3. Kovacs GT. What factors are important for successful embryo trans-fer after in-vitro fertilization? Hum Reprod 1999;14:590–2.
4. Schoolcraft WB, Surrey ES, Gardner DK. Embryo transfer: tech-niques and variables affecting success. Fertil Steril 2001;76:863–70.
5. Sallam HN, Agameya AF, Rahman AF, Ezzeldin F, Sallam AN.Ultrasound measurement of the uterocervical angle before embryotransfer: a prospective controlled study. Hum Reprod 2002;17:1767–72.
6. Goudas VT, Hammitt DG, Damario MA, Session DR, Singh AP,Dumesic DA. Blood on the embryo transfer catheter is associatedwith decreased rates of embryo implantation and clinical pregnancywith the use of in vitro fertilization–embryo transfer. Fertil Steril1998;70:878–82.
7. Pope CS, Cook EK, Arny M, Novak A, Grow DR. Influence ofembryo transfer depth on in vitro fertilization and embryo transfer
outcomes. Fertil Steril 2004;81:51–8.1237

BOOK REVIEW
Christine Evans, editor. Genetic Counselling: A Psycholog-ical Approach. New York, NY: Cambridge UniversityPress, 2007:1–197. Price: $45.00.
As we stand on the brink of the much anticipated era of ge-netic medicine, with more people considering genetic testingfor an increasing number of diseases, Genetic Counselling:A Psychological Approach by Christine Evans is an excellentbook to sensitize all health care professionals to this emotion-ally charged process. Although written primarily for geneticcounselors, it can teach each of us who is in the position ofgiving potentially upsetting or anxiety-provoking news topatients how to do this more effectively and with greatercompassion.
Dr. Evans, a psychiatrist and psychotherapist, has workedwith genetic counselors for ten years integrating psychologicand physical aspects of medicine. While the focus of the bookis on helping patients make decisions about genetic testingfor both potentially curable diseases (e.g., breast cancer)and incurable ones (e.g., Huntington’s disease), it presentspsychotherapeutic concepts and gives many examples of im-plementation to try to achieve psychologic attunement withpatients. I found that much of the information could beextrapolated to work with patients struggling with fertilityissues and pregnancy losses, as well as those consideringprenatal testing or preimplantation genetic diagnosis. Infact, Dr. Evans’s approach would be applicable to all healthcare professionals working with patients who may be feelingvulnerable and exposed.
When people consider genetic testing, they are really facedwith coming to terms with the psychologic implications ofwhat that knowledge does for them, their families, and theirfuture children. Dr. Evans encourages genetic counselors tobecome well grounded in psychology and the psychothera-peutic process, because providing information and probabil-ity statistics are only the beginning of their job with patients.Because respect of patient autonomy has resulted in a morecollaborative relationship between health care professionalsand patients, it is no longer seen as appropriate for the medicalprofessional to make decisions for the patient. Rather, the roleof the medical professional is to guide and facilitate thepatient’s decision-making process. In taking this position,the genetic counselor can, by effectively listening to thepatient on a deeper level, assist the patient in deciding whetheror not to undergo testing, how to involve family members,how to contain their test-related anxiety, and how to copewith positive test results.
Intense anxiety can often be felt both by patients consider-ing genetic testing and by those seeing a reproductive endo-crinologist for information regarding their fertility potential,and it can be debilitating. Recognizing this in our patients
Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ª2007 American Society for Reproductive Medicine
1238
allows us to assist them in containing their anxiety and putsthem in a better position to process the information we sharewith them and to work toward decision making. Dr. Evansaptly points out how medical personnel may sometimesfeel more comfortable hiding behind their technical exper-tise, relying too much on conveying scientific informationwhen, in fact, emotional interventions may be needed.
Chapters 1–3 of the book present an overview of geneticcounseling, framing genetic testing as a psychologic stressor,presenting Dr. Evans’s client-centered approach with pa-tients, and using attachment theory to explain differences inpatient coping with both the testing and the receipt of the re-sults. Chapter 4 explains psychotherapeutic skills necessaryto establish a collaborative relationship with a patient, andChapter 5 applies this to working with various patient reac-tions to genetic testing, such as anxiety, grief, defensive reac-tions, and hopelessness. Chapter 6 introduces the reader tofamily systems theory and the impact of genetic informationon the rest of the family, present and future. Chapter 7 focuseson working with parents and children who either have a ge-netic disease or may be carriers. Chapter 8 focuses on geneticcounseling in the areas of prenatal diagnosis, Huntington’sdisease, cancer screening, and dysmorphology. The geneticcounselor’s own emotional reactions to the patients in a situ-ation where they may feel guilt or failure for not being able to‘‘cure’’ the patient, is covered in Chapter 9, along with therecommendation that genetic counselors obtain supervisionto assist with self-care, self-awareness, and professionalgrowth in this emotion-laden field. The final chapter reflectson the difficulty of remaining nondirective in the face ofintense patient anxiety and the frequently asked question,‘‘What would you do?’’
Throughout the book, it is suggested that genetic counselorsask patients their preference for receiving information asa way of being responsive to patient needs and information-processing styles as well as giving them some control in anoverwhelming situation. Checking on the patient’s under-standing of shared information, rather than assuming compre-hension, and responding to feelings that may be expresseddirectly or indirectly or are absent (but thought to be a possibil-ity based on the professionals’ prior experience with patientsas well as their experience of the particular patient) is alsorecommended.
For those who are not already well versed in psychothera-peutic techniques to engage with and respond to patients inemotional crisis, the book may try to cover too much. There’sa good deal of psychologic jargon as well, but most is quitewell explained to the reader unfamiliar with the terminology.Typographic errors throughout the book necessitates a secondreading of some sentences to understand what is trying to beconveyed, but Dr. Evans’s examples clearly demonstrate the
0015-0282/07/$32.00, Published by Elsevier Inc.

concepts she presents. The take-home message of this book isthat our patients are unique human beings with individual his-tories which affect their ability to cope with the informationwe present to them. When this information requires an adjust-ment in their appraisal of themselves as invulnerable andhealthy, neither genetic counseling nor any other interactionwith patients should be viewed as a one-size-fits-all proposi-tion. This book is an excellent reminder of this as well as
Fertility and Sterility�
a brief guide to developing the skills needed to address thevery real human emotions arising in the everyday interactionsbetween medical professionals and patients.
Joann Paley Galst, Ph.D.New York, New York
doi:10.1016/j.fertnstert.2007.01.004
1239

LETTERS TO THE EDITORPaul G. McDonough, M.D.Associate Editor
Reply of the Author:
We thank Shahine and colleagues for their interest in ourmeta-analysis and for their review of the original articles.However, more careful reading of our article and of the orig-inal articles would have prevented them from making errorsin their interpretation.
Contrary to what they state herein, Piacquadio et al. de-scribed two women taking phenformin and only one takingmetform in (1). The atr ial septal defe ct happened with phen-formin (Table 1) and not with metformin, as claimed byShahine and colleagues.
In a similar manner Shahine et al. claimed that we missedthe 2001 study by Gl uek et al. (2) becau se of our search strat-egy. Not so; the study by Gluek et al. was found by us but wasexcluded because a year later the same group describeda larger group from the same center, and in such casesmeta-analysis has to assume overlap and to choose the later,and larger, study.
Gideon Koren, M.D.Motherisk Program, University of TorontoToronto, Ontario, Canada
February 12, 2007
REFERENCES1. Piacquadio K, Hollingsworth DR, Murphy H. Effects of in-utero exposure
to oral hypoglycaemic drugs. Lancet 1991;338:866–9.
2. Glueck CJ, Phillips H, Cameron D, Sieve-Smith L, Wang P. Continuing
metformin throughout pregnancy in women with polycystic ovary
syndrome appears to safely reduce first-trimester spontaneous abortion:
a pilot study. Fertil Steril 2001;75:46–52.
doi:10.1016/j.fertnstert.2007.03.022
Metformin and fetal malformations
To the Editor:
Gilbert et al. (1) published a meta-analysis concerningpregnancy outcome and fetal malformations after first-tri-mester exposure to metformin. These data could be importantbecause many practitioners treat infertility in polycysticovary syndrome (PCOS) with metformin and continue itinto the first trimester of pregnancy.
One of the inclusion criteria for meta-analysis was first-tri-mester exposure to metformin; however, not all includedstudies met criteria. In one study, patients stopped metforminon the day of hCG trigger (2).
The authors of the meta-analysis show in their tables that0 of 1 infant exposed to metformin in the first trimester hada malformation when describing data taken from Piacquadioet al. (3). The study by Piacquadio et al. states that of the threewomen exposed to metformin during the first 7 weeks ofgestation, one infant had an atrial septal defect. Althoughthe authors note that this defect is unlikely to be a result ofmetformin exposure because the mother had a hemoglobinA1C level of 14.2%, it should probably be included as a mal-formation in an infant exposed to metformin for the meta-analysis. From another study (4), Gilbert et al. includedachondroplasia, which is hereditary, as a malformation intheir analysis (1).
Gilbert et al. did not use ‘‘malformation’’ as a search termwhen this is the main outcome of interest (1). If they had, theymight have found an additional study (5) in which rates ofmiscarriage and malformations were examined in 22 patientswith PCOS taking metformin throughout pregnancy com-pared with 125 women with PCOS who achieved pregnancywithout metformin.
The safety of metformin exposure in the first trimester isan important topic. However, we wonder whether data frompersons with type 2 diabetes can be extrapolated to patientswith PCOS. Poorly controlled blood sugar is a teratogen.Had the data used in the meta-analysis included the missedfetal abnormality, it is questionable whether the findingswould have remained statistically significant. It shouldalso be stated that the PCOS data alone do not appear to besignificant.
Lora Shahine, M.D.Ruth B. Lathi, M.D.Michael H. Dahan, M.D.Stanford UniversityStanford, California
December 5, 2006
Fertility and Sterility� Vol. 87, No. 5, May 2007Copyright ª2007 American Society for Reproductive Medicine
1240
REFERENCES1. Gilbert C, Valois M, Koren G. Pregnancy outcome after first-trimester
exposure to metformin: a meta-analysis. Fertil Steril 2006;86:658–63.
2. Sahin Y, Yirmibes U, Kelestimur F, Aygen E. The effects of metformin on
insulin resistance, clomiphene-induced ovulation and pregnancy rates in
women with polycystic ovary syndrome. Eur J Obstet Gynecol Reprod
Biol 2004;113:214–20.
3. Piacquadio K, Hollingsworth DR, Murphy H. Effects of in-utero exposure
to oral hypoglycaemic drugs. Lancet 1991;338:866–9.
4. Jakubowicz DJ, Iuorno MJ, Jakubowicz S, Roberts KA, Nestler JE.
Effects of metformin on early pregnancy loss in the polycystic ovary
syndrome. J Clin Endocrinol Metab 2002;87:524–9.
5. Glueck CJ, Phillips H, Cameron D, Sieve-Smith L, Wang P. Continuing
metformin throughout pregnancy in women with polycystic ovary syn-
drome appears to safely reduce first-trimester spontaneous abortion: a pilot
study. Fertil Steril 2001;75:46–52.
doi:10.1016/j.fertnstert.2007.03.021
0015-0282/07/$32.00, Published by Elsevier Inc.

Reply of the Authors:
We carefully read the comments raised by Bujan and col-leagues regarding our correspondence published in Fertilityand Sterility entitled ‘‘The Effectiveness of Modified SpermWashes in Severely Oligoasthenozoospermic Men InfectedWith Human Immunodeficiency and Hepatitis C Viruses’’(1).
In the above-mentioned article, we aimed to describe thepossibilities of men with severe oligoasthenozoospermia in-fected with HIV to reach fatherhood with their own sperm
Trying to avoid the transmission of humanimmunodeficiency virus particles in sperm ejaculates
To the Editor:
Garrido et al. reported in a recent issue of Fertility andSterility a modified sperm washing method adapted for menwith severe oligoasthenozoospermia infected with HIV andhepatitis C virus (HCV) (1). To date, several assisted reprodu-ctive technology programs have been reported (2). However,classic sperm washing methods are not possible if the manhas severe oligospermia. In this context, the relevant aim ofthe study of Garrido et al. was to determine whether lessrigorous sperm washing methods eliminate viral particles.
Seven men provided eight semen samples. Semen waswashed only twice. All viral tests were negative, and theauthors conclude, ‘‘thus demonstrating the effectiveness ofthe technique of washing sperm by means of seminal plasmaelimination after centrifugation.’’
Several considerations limit the results and conclusion ofthis study. The major consideration is the lack of viral dataconcerning seminal plasma or native sperm. To assess thetrue effectiveness of sperm washing, it would have beenmore relevant to choose patients with detectable seminal viralload before sperm washing. To date, HIV-1 presence in se-men has been well documented, and several factors associ-ated with HIV semen shedding have been studied, that is,genital infection, HIV-1 infection state, semen polynuclearcells, blood and seminal viral load (3, 4). It is very likely,therefore, that the patients from the study by Garrido et al.had an undetectable seminal viral load.
Moreover, all but two of the patients were receiving activeantiretroviral treatment, and only one patient had a detectableHIV blood load. Some patients could be infected by undetect-able variant HIV-1 strains, because it is not stated whether un-treated patients had an undetectable viral load. It is thenimportant to ensure that the molecular tests used are able todetect HIV genomes in all infected patients, thus avoidingpossible false negative results. Last, the small number of pa-tients impaired the validity of the authors’ conclusion.
Nevertheless, the use of intracytoplasmic sperm injection(ICSI) resulting from severe oligoasthenospermia probablycontributed in reducing the risk of infection, as only one iso-lated spermatozoon was used per oocyte. Indeed, althoughthe debate on HIV presence in spermatozoa is probably notdefinitively closed, several studies using highly sensitive mo-lecular assays argue against it (3, 4). The hypothetical risklies in HIV adhesion to sperm membrane, thus allowingHIV to enter the oocyte during ICSI. However, ICSI hasbeen performed in serodiscordant couples without virologi-cal tests on spermatozoa fractions (5).
From a clinical point of view, we suggest that ICSI couldbe used in oligoasthenozoospermic HIV-1 infected patients,after [1] introduction or optimization of treatment, usingantiretroviral molecules with good diffusion in the genital
Fertility and Sterility�
compartment to obtain, at the least, a drastic reduction inblood and seminal viral loads, or [2] sperm washes followedby rinsing of selected microaspirated spermatozoa in mediumbefore ICSI. All these methods reduce the risk of HIV re-maining on spermatozoa fractions after washes.
We believe, in the light of present scientific knowledge,that the conclusion of Garrido’s study should be interpretedwith great caution and that patients should be informed thatalthough the methods proposed above drastically reduce therisk, a hypothetical risk nevertheless persists.
Louis Bujan, M.D.Nathalie Moinard, Pharm.D.Myriam Daudin, M.D.CECOS Midi-PyreneesUniversite Toulouse-III Paul SabatierResearch Group on Human FertilityHospital Paule de Viguier
Christophe Pasquier, Ph.D.Department of VirologyUniversity Hospital PurpanToulouse, France
February 5, 2007
REFERENCES1. Garrido N, Remohi J, Pellicer A, Meseguer M. The effectiveness of mod-
ified sperm washes in severely oligoasthenozoospermic men infected with
human immunodeficiency and hepatitis C viruses. Fertil Steril 2006;86:
1544–6.
2. Gilling-Smith C, Nicopoullos JD, Semprini AE, Frodsham LC. HIV and
reproductive care—a review of current practice. Br J Obstet Gynaecol
2006;113:869–78.
3. Bujan L, Daudin M, Matsuda T, Righi L, Thauvin L, Berges L, et al. Fac-
tors of intermittent HIV-1 excretion in semen and efficiency of sperm
processing in obtaining spermatozoa without HIV-1 genomes. AIDS
2004;18:757–66.
4. Dejucq-Rainsford N, Jegou B. Viruses in semen and male genital tis-
sues—consequences for the reproductive system and therapeutic perspec-
tives. Curr Pharm Des 2004;10:557–75.
5. Sauer MV, Chang PL. Establishing a clinical program for human immuno-
deficiency virus 1–seropositive men to father seronegative children by
means of in vitro fertilization with intracytoplasmic sperm injection.
Am J Obstet Gynecol 2002;186:627–33.
doi:10.1016/j.fertnstert.2007.03.023
1241

and without horizontal or vertical transmission. Maybe thelimited length of the article left some issues poorly explained.
We thank Bujan et al. for their comments, and we will clar-ify point by point all their questions. We agree with the affir-mation that classic sperm washes (2) cannot be used for thesesamples. These extremely astringent methods will lead torecovering no sperm after the preparation. Nevertheless,because of the strong request from our patients in these situ-ations we were forced to try new protocols to guarantee theabsence of viral particles while maintaining some motilesperm. In this sense, we performed consecutive dilutions ofthe ejaculates, divided the samples in two equal volumes,and analyzed one while the other remained frozen until a neg-ative polymerase chain reaction (PCR) result was confirmed.
We also agree that this is not a direct demonstration of theremoval of viral particles from the ejaculates, because noPCR from the fresh sample was performed confirming thepresence of HIV. Whether no detectable blood virus load ispresent in our patients, HIV presence in ejaculated spermcould be confirmed with difficulty, but we follow one mainendpoint, which is to demonstrate that the sperm fraction tobe used in the assisted reproductive technologies is virusfree. It is unlikely that there would be patients with undetect-able viral strains given that the amplification protocols werefocused in a highly conserved region of the virus present in allHIV-1 groups (3).
The small number of patients led us to send the manuscriptas correspondence but conversely offered us the possibility ofshowing these results promptly to other groups treating HIV-infected men, because it is not frequent to find men with thesecharacteristics (HIV-infected men are not intrinsically infer-tile themselves) (2). Intracytoplasmic sperm injection obvi-ously reduces the infection risk, and this is our choice,always after PCR confirmation of the viral absence, but weprofoundly disagree with the groups performing ICSI withoutthe previous PCR confirmation as stated elsewhere (4). Thehypothetical risk does not lie in the adhesion to the spermmembrane: all nucleic acids of a sperm sample arechemically extracted, independently from their location.Subsequently, the PCR amplification should detect them.Moreover, among all the HIV treatments for serodiscordant
couples worldwide, just occasional infections have been re-ported, and only after intrauterine inseminations.
Finally, from the clinical point of view, antiretroviral treat-ments are unnecessary to manage reproductive wishes (2),given that this does not increase the possibility of having un-detectable HIV levels after sperm wash (2). Rinsing microas-pirated spermatozoa is not needed on the basis of the nucleicacid extraction followed by double PCR (nested), which isable to detect up to one copy of the virus. Nevertheless, weagree that our conclusion must be kept with caution, and ob-viously all patients should be informed that a 0% risk is non-existent in biology and must sign adequate informed consentsbefore any procedure is planned.
Nicolas Garrido, Ph.D.Andrology Laboratory and Sperm BankInstituto Universitario IVIValencia, Spain
Marcos Meseguer, Ph.D.IVF LaboratoryInstituto Universitario IVIValencia, Spain
February 9, 2007
REFERENCES1. Garrido N, Remohi J, Pellicer A, Meseguer M. The effectiveness of mod-
ified sperm washes in severely oligoasthenozoospermic men infected with
human immunodeficiency and hepatitis C viruses. Fertil Steril 2006;86:
1544–6.
2. Garrido N, Meseguer M, Remohi J, Simon C, Pellicer A. Semen charac-
teristics in human immunodeficiency virus (HIV)– and hepatitis C
(HCV)–seropositive males: predictors of the success of viral removal after
sperm washing. Hum Reprod 2005;20:1028–34.
3. Meseguer M, Garrido N, Gimeno C, Remohi J, Simon C, Pellicer A. Com-
parison of polymerase chain reaction–dependent methods for determining
the presence of human immunodeficiency virus and hepatitis C virus in
washed sperm. Fertil Steril 2002;78:1199–202.
4. Garrido N, Meseguer M. Use of washed sperm for assisted reproduction in
HIV-positive males without checking viral absence. A risky business?
Hum Reprod 2006;21:567–8. author reply 568.
doi:10.1016/j.fertnstert.2007.03.024
1242 Letters to the Editor Vol. 87, No. 5, May 2007