evaluation of 133xe washout kinetics by controlled pig liver perfusion in vivo
TRANSCRIPT

JOURNAL OF SURGICAL RESEARCH 32, 586-597 (1982)
Evaluation of 133 Xe Washout Kinetics by Controlled Pig Liver Perfusion in Viwo
ULRICH PASCHEN,MANFRED J. MILLER, ANDHANS J. SEITZ With the technical assistance of Angelika Harneit, Dagmar Luda, and Gunter Lutz
Institut fir Physiologische Chemie. Universitiits-Kronkenhaus Eppendorf; UniversiMt Hamburg, Mortinistrosse 52, 2000 Homburg 20, Federal Republic of Germany
Submitted for publication February 27, 1981
The interpretation of multiexponential curves from hepatic tracer washout for estimation of hepatic blood flow (THBF) was investigated, using hepatic ‘33Xe washout during controlled portal and arterial perfusion of liver in anesthetized pigs. Variations of (I) THBF from 25 to 210 ml/min X 100 g, (2) the proportion of portal to arterial flow, and (3) the site of tracer application were performed. After portal injection the tracer curves were in most cases multiexponential; their analysis revealed that calculation of THBF using k values based on the monocompartmental hypothesis always grossly overestimated total flow. Estimation of THBF by height/area (H/A), however, reflected the total
flow in all cases. Only when hypoventilation or elevation of hepatic venous pressure was performed, did calculation of THBF from k values and H/A values reveal similar results. THBF when estimated from H/A and from indocyanine green dye extraction gave identical results, both in the controlled perfused liver and in the intact animal. Washout curve analysis after arterial Xe application showed neither a correlation with the total nor with the arterial flow, indicating incomplete mixing of both blood flow components. It is concluded that liver perfusion is multicompartmental and blood flow through the portal and arterial vascular bed is incompletely mixed. Therefore, THBF can be cal- culated only after portal tracer injection and when the mean transit time concept is applied.
INTRODUCTION
Since inert gases were introduced for or- gan blood flow measurement, interpretation of the washout curves has been a main topic of discussion. When bi- or multiexponential curves were obtained as for instance from brain or kidney, the different components of the tracer washout curve were interpreted to indicate different functional compart- ments of the organ [ 121. Consequently, from organs with homogeneous perfusion such as liver or muscle, solely monoexponential curves have been predicted. However, all in- vestigators studying liver blood flow with in- ert gases described, in addition to mono-, multiexponential curves. The slow compo- nents were ascribed to extrahepatic sites and, therefore, were substracted from the original curve [S]. Other authors attributed the multiexponential curve to a multicom- partmental tracer clearance, reflecting dif- ferent velocities of tracer washout from por- tal and arterial vascular bed of the liver [4,
81, as a consequence of incomplete mixing within the organ. Thus, THBF calculation differed up to 100% by either including or excluding the slow component(s) of the tracer washout kinetic [ 171. As in these ex- periments the actual blood flow was not re- corded simultaneously, we evaluated the ‘33Xe kinetics by controlled perfusion of pig liver in vivo. This model permits (i) accurate delivery of blood flow in vivo by two cali- brated pumps; (ii) systematic alteration of the THBF over a wide range in the sume animal, (iii) variation of arterial and portal parts of THBF independently of each other, thus varying the mixture ratio.
Our ‘33Xe washout data provide strong evidence that the portal and arterial perfu- sion are incompletely mixed and, therefore, reasonable correspondence with actual liver perfusion can only be obtained when the tracer is injected in the portal vein and when the multiexponential decay curve is consid- ered as originating totally from intrahepatic washout.
0@22-4804/82/060586- 12$01.00/O Copyrigt 0 1982 by Academic Press, Inc. All rights of reproduction in any form reserved.
586

PASCHEN, MOLLER, AND SEITZ: HEPATIC “‘Xe WASHOUT KINETICS 587
METHODS Operative Procedures and Liver Blood
Experiments were performed on 2 1 female pigs (19.5 + 4.5 kg) of German Landrace, fasted 24 hr prior to the experiments. An- aesthesia was induced by intraperitoneal in- jection of 1.25 mg/kg azaperon (Stresnil, Janssen GmbH, Dusseldorf, FRG) and 10 mg/kg metomidat (Hypnodil, Janssen GmbH, Dusseldorf, FRG) and, following endotracheal intubation, was maintained with nitrous oxide/oxygen (3: 1) and supple- mentary doses of 0.1 mg/kg metomidat as necessary. The animals were ventilated in an open circuit using an Engstriim respirator with an outlet vented to the outside to pre- vent buildup of ‘33Xe in the laboratory at- mosphere. The tidal volume was adjusted to yield normal pOZ and pC02 values. pH was corrected if necessary by intravenous injec- tion of sodium bicarbonate. Rectal temper- ature was maintained at 36-37°C by use of radiant heat lamps and heating mattress. Systemic blood pressure, portal pressure, and hepatic vein pressure were monitored continuously by electromagnetic transducers (Type P 23Db, Statham, Hato Rey, Puerto Rico) and a three-channel oscilloscope (F. Liechti AG, Bern, Switzerland).
Flow Measurements
Under sterile conditions midline laparot- omy was performed to expose the liver and its supporting vessels. The portal vein was mobilized between splenic vein and the bi- furcation of its right and left liver branch; the gastroduodenal vein was catheterized with a catheter (polyvinyl, outer diameter 1.5 mm) and subsequently ligated. The he- patic artery was isolated by careful dissec- tion; all branches to gastric or duodenal areas were tied to assure that all blood from the common hepatic artery reached the liver directly. A further catheter (polyvinyl, outer diameter 1.5 mm) was inserted into the A. gastrica sinistra and the vessel ligated. The jugular vein was cannulated (polyvinyl, outer diameter 2.5 mm) for drug and fluid ad- ministration. A branch of A. carotis was can- nulated for blood pressure measurement and withdrawal of blood for blood gas analysis.
In two experiments another catheter (polyvinyl, outer diameter 2.5 mm) was in- serted into the common bile duct for mea- surement of bile flow.
Controlled liver perfusion by peristaltic pumps. Two independently running peri-
133 Xe - Injection --
withdrawal of portal blood and pressure measurement
Balloon catheter for alteration of hepatic outflow pressure
Withdrawal of hepatic venous blood and pressure measurement
arterial pressure measurement
ARTERIA CAROTIS
PORTAL VEIN
FIG. 1. Diagram showing the experimental arrangement of the controlled pig liver perfusion in vivo by two peristaltic pump systems.

588 JOURNAL OF SURGICAL RESEARCH: VOL. 32, NO. 6, JUNE 1982
0 60 120 180 240
TIME I MINUTES )
FIG. 2. Effect of in vivo controlled perfusion of pig liver during 240 min at various blood flows (20- 150 ml/ min X 100 g) on biochemical parameters of the organ and on physiological data of the animal. Data are given as means from three. representative experiments.
staltic pumps (model Eppendorf, Dreissen, Machine, Apparatenbuow, Hellevoetsluis, Holland) were used to perform a controlled liver perfusion via the arterial and portal route independent of actual cardiac output or systemic pressure. For arterial perfusion blood was conducted from A. carotis to a reservoir, situated in a waterbath at 37°C. From the reservoir blood was pumped via an “arterial outflow set” (Avon Medicals Ltd., Birmingham, England), containing an air trap and a blood filter. Blood reached the A. hepatica via a canula (polyvinyl, diameter 2.1 mm). Using a similar tube system portal venous blood was taken from the distal part of the portal vein and pumped into the prox- imal root after clamping off, cutting the por- tal vein and inserting special designed can- nulas (glassware, outer diameter 10 mm; inner diameter 8 mm). Because arterial con- trolled perfusion was started before the clamping of the portal vein, anoxia of the liver was avoided. The clamp time for each vessel was about 3 min. The spotting of the organ with dark patches as observed after arterial ligation described for dogs was not observed. The roller pump system was primed with 200 ml of Ringer-lactate solution con- taining heparin (crystalline, solved in saline solution), 200 U/kg body weight. Half of this dose was administered intravenously each 50 min. Care was taken that no air bubbles could enter the liver. The peristaltic pumps were calibrated with fresh pig blood and were found to be accurate (< +5%) over the range used in the experiments and up to an outflow pressure of 100 mm Hg. The cal- ibration was controlled at the end of each experiment.
In some experiments the outflow pressure of the liver was enhanced by inflating a bal- loon catheter (Fogarty Arterial Embolec- tomy cath 3F, inflated diameter 5 mm, Ed- wards Laboratories, Santa Ana, Calif.), inserted into the V. cava inf. via jugular vein. Thus it was possible to alter systematically the pressure in the hepatic veins. The pres- sure was continuously recorded by a catheter inserted in the main stem of the hepatic vein
of the left lobe according to Shoemaker et al. [ 19 1. As the zero reference point the right heart atrium was chosen. The experimental arrangement is illustrated diagramatically in Fig. 1. After finishing the operative pro- cedures the abdomen was closed, the tubes leaving the abdomen through holes in the abdominal wall. Heating lamps were piaced over the animal, which was allowed to re- cover for about 30 min (body temperature during anesthesia <37’C). The altered body temperature had no influence on the decay curves and their analyses, as it was con- trolled by cooling the reservoir in the per- fusion system and altering the temperature from 37 to 27’C.
The pig liver in vivo perfusion system could be kept for at least 240 min without evident damage as indicated by the constant oxygen consumption, the lactate extraction in parallel with arterial lactate concentra- tion, the unaltered bile flow, and the only
PASCHEN, MULLER, AND SEITZ: HEPATIC 13Xe WASHOUT KINETICS 589
slight increase in the activity of glutamate oxaloacetate transaminase (compare Fig. 2).
Zndocyanine green extraction. Total liver blood flow was estimated with indocyanine green (ICG, Hynson, Westcott and Dun- ning, Inc., Baltimore, Md.) according to Ketterer [ 101. ICG solution was always freshly prepared by dissolving ICG in sterile 5% human albumin (Behring, Marburg/ Lahn, FRG): ICG was given as a priming dose of 500 rg/kg body weight, followed by a continuous intravenous infusion of 10 pg/ kg X min resulting in a constant dye con- centration within 20 min. The arterial level was always cl.6 pg/ml plasma. Blood was withdrawn from arterial and hepatic venous line, centrifuged (10 min, 5000 rpm, 2”C), and immediately measured at 805 nm in a Zeiss PMQ III spectrophotometer. The dye concentration was read from a standard curve prepared for each animal. Then, THBF was calculated according to the formula:
THBF = ICG infusion rate
[(arterial cont.) - (hepatic venous cont.)] X [ 1 - Hct] ’ (1)
Recording of ‘33Xe washout. To record the ‘33Xe washout a NaJ scintillation detector (Type 8S8) combined with a ratemeter (Type 700A) (equipment Friesecke und Hopfner, Erlangen, FRG) was used: lead collimator window, 3 cm in diameter; rate- meter constant, 2.4 sec. The photomultiplier was tested for gain instability and was found to be less than 2%. The ratemeter was con- nected to a teletype. 133Xe in 1 ml saline solution (200 &i) (Amersham Radiochem- ical Centre, Amersham, England) was in- jected as instantaneous bolus. The catheter was flushed immediately with 2 ml saline solution. Peak count rates were approxi- mately 5OOO/sec. The washout curve was recorded over a 15-min period. The detector was placed over the lower part of the right liver lobe. After tracer injection into the pul- monary artery only a few counts were mea- sured, indicating that only minimal recir- culation occurred in our system, and no
relevant part of the lung was seen by the detector. When the detector was placed over the gut and the tracer injected into the portal vein, counting rate did not increase.
At the end of the experiments the animals were sacrificed, the liver removed, bled, and freed from gall bladder and all connective tissue. Liver weight was measured and the ratio of liver weight/body weight was found to be 24 g/kg, which was slightly lower than given in the literature [ 81, indicating that no major edema occurred. The routine esti- mation of hepatic lipid content always re- vealed a value less than 4.5 mg%.
Biochemical Analyses
pOz, pCO,, and pH were measured by a BMS3-MK2 (Radiometer Copenhagen). Oxygen saturation was read from the curve given by Bartels and Harms [2] for the pig; oxygen capacity was 1.34 times hemoglobin

590 JOURNAL OF SURGICAL RESEARCH: VOL. 32, NO. 6, JUNE 1982
v) SW0 . -~“oooooo 000
000 ARTERIAL 133 Xe - INJECTION f . ~"o~-oe L DETECTOR OVER THE LIVER
. PORTAL '-XC'- INJECTION .*. - - . a' *. .
.: l .oo
PORTAL 133 . . . . .
DETECTOROVERTHE LIVER
Xe - INJECTION . . l 0’ .O. .
. . .* *’ , . .
DETECTOR OVER THE LUNG . . * . a.. ..*.
. * . . * . . . . .
l .
*. ?*O. .:* .
. * . . .
t . .
101 1 I I 1 1 I 1 I I I
0 L I 3 4 5 6 7 I 9 LU 1, 12
7 I M F. , MlNUTES ,
FIG. 3. ‘33Xe washout curves recorded over the liver after tracer injection (0) into the arterial route and (0) into the portal route. For comparison the “‘Xe washout curve recorded over the lung (*) after tracer injection into the portal route was inserted. Experimental details: ‘33Xe injection, 0.2 mCi: total pumped flow: 115 ml/min X 100 g; arterial route, 38 ml/min X 100 g; portal route; 77 ml/min X 100 g.
concentration. Oxygen consumption was cal- culated using
V02 = [portal oxygen content X portal flow
+ arterial oxygen content X arterial flow]
- [ hepatic venous oxygen content
X total liver blood flow]. (2)
By routine clinical methods hemoglobin and hematocrit were estimated. Routine enzy- matic procedures [3] were applied to deter- mine blood lactate concentration and the activity of glutamate oxaloacetate trans- aminase, glutamate pyruvate transaminase, lactate dehydrogenase, and glutamate de- hydrogenase in plasma. In order to measure hepatic lipid content, about 500 mg liver was extracted according to Folch et al. [7] and washed twice with fresh upper layer; after saponification of the triglycerides glycerol was determined enzymatically [ 31. Reagents were purchased from Boehringer, Mann- heim, and Merck AG, Darmstadt.
Curve Analysis
Determination of the k value. The printed data (counts/2.4 set) corrected by subtrac- tion of the background level were drawn
TABLE 1
EFFECTOFDIFFERENTPROPORTIONSOF HEPATIC ARTERYANDPORTALVEINFLOWONTHE
CALCULATIONOFTHBF(BASEDON H/A VALUES) AFTERARTERIALORPORTALX~ INJECTION
Calculated total
THBF after
Pumped arterial
now
Pumped
portal now
Pumped Arterial
total XC Bow injection
Portal xc injection
ml/ 100 g X min
6 117 123 44 87 13 II0 123 54 118 19 104 123 47 I26
26 97 I23 53 II5 32 91 123 69 121
38 85 I23 68 125 45 78 I23 64 I03
51 72 123 65 I18 64 59 123 76 I18

PASCHEN, MOLLER, AND SEITZ: HEPATIC ‘j3Xe WASHOUT KINETICS 591
manually on semilogarithmic paper versus THBF = k X X X 100 time (up to about 12-15 min) and a straight line was drawn through the steepest part of (ml/min X 100 g). (4) the curve (“steepest slope”) by simple in- spection. The rate constant k, was then cal-
Using the height over area value total liver
culated from blood flow was derived from
In addition, in all experiments the “fast com- ponent” was determined by the “curve peel- ing” procedure and kF estimated according to Eq. (3).
Measurement of height over area. The height of the curve, H, was taken as the height of the plateau. The area, A, was cal- culated by adding all count values until background was reached (usually within 12 min) and multiplying with the time interval.
Using k, or kF total liver blood flow was derived from
4oc
_ 350 M
x
x .9 300
E
z 250
ii X l- 200
m
2 d ; 150
2
:
: 100 x
z 4
50
0
1 -
I -
, -
k - VALUE / HEIGHT / AREA - VALUE
l 0
‘/
/
THBF = H/A X X X 100
(ml/min X 100 g). (5)
X, representing the partition coefficient for ‘33Xe between blood and liver tissues, was taken from [ 11, including the correction for hematocrit:
x Hctx = 0.72 1.69
1.05 + 0.013 Hctx ’ (6)
Statistics
All values are expressed as means + SEM.
T
0 50 100 150 200 250 0 50 100 150 200 250
PUMPED TOTAL HEPATIC BLOOD FLOW ( ml / min x 100 g )
400
350 ̂m
z
300 ;
E
250 2 _
ii
200 :
0 aI
; 150 ;
”
:
100 : x
z
50
0
FIG. 4. Relationship between controlled liver perfusion and calculated THBF based on k values (left) (r = 0.88. P < 0.0001) or on height/area values (right) (r = 0.91, P < 0.0001). Values were taken from nine different experiments (n = 69) with a ratio of arterial to portal flow of approximately 1:3. Line of identity is inserted (-).

592 JOURNAL OF SURGICAL RESEARCH: VOL. 32, NO. 6, JUNE 1982
k - VALUE HEIGHT 1 AREA - VALUE
0
400
0
PUMPED TOTAL HEPATIC BLOOD FLOW ( ml / min x 100 B )
FIG. 5. Effect of different parts of hepatic artery flow on the relationship between controlled liver perfusion and calculated THBF based on k values (r = 0.96, P < 0.0001, n = 25) or on H/A values (r = 0.96, P < 0.0001, n = 25). Arterial flow: 10 ml/min X 100 g (A), 27 ml/min X 100 g (O), 54 ml/ min X 100 g (M). Line of identity is inserted (-).
RESULTS
Recording and Data Analysis of the Decay Curves after Arterial and Portal Tracer Injection
The results from the different ‘33Xe in- jection sites are depicted in Fig. 3. The ar- terial ‘33Xe injection resulted in a slow and nearly monoexponential decay rate (T/2 = 81 set, k = O.Sl/min). As shown in Table 1, after arterial tracer injection the decay curve neither reflected pumped arterial nor pumped total flow. After portal tracer injec- tion, yielding a multiexponential curve, the estimation of liver blood flow based on k values led to an overestimation of both portal and total liver blood flow (220 ml/min X 100 g). This overestimation was further in- creased, when the k values were obtained from the “fast component” by peeling off the slow component from the “steepest slope” (calculated value: 247 ml/min X 100
g). If the H/A procedure was applied to the decay curve, after portal tracer injection THBF was in the same range (120 ml/min x 100 g).
When the collimator was placed entirely over the lung, only low activity was recorded after tracer injection into the portal vein (Fig. 3). The peak value amounted to less than 10% of the activity recorded over the liver and showed a rapid decline. All ob- served phenomena were independent of the position of the collimator over different liver lobes.
Data Analysis of Decay Curves after Variation of Controlled Liver Perfusion
At a constant ratio of arterial to portal flow of approximately 1:3 the controlled liver perfusion was varied in nine different ani- mals. Flow/tissue ratios from 25 to 210 ml/ min X 100 g could be achieved. As shown in Fig. 4 a significant correlation (r = 0.88, P
PASCHEN, MULLER, AND SEITZ: HEPATIC “‘Xe WASHOUT KINETICS 593
300
M
0”
; 250
4 E
.
2 200
k
E
‘CI 150
2
”
:
; 100
P ”
50
NORMO- VENTILATION
,/
/
Lu 1 50 100 150 200
HYPO- VENTILATION
50 100 150 200
PUMPED TOTAL HEPATIC BLOOD FLOW (ml / min x 1OOg)
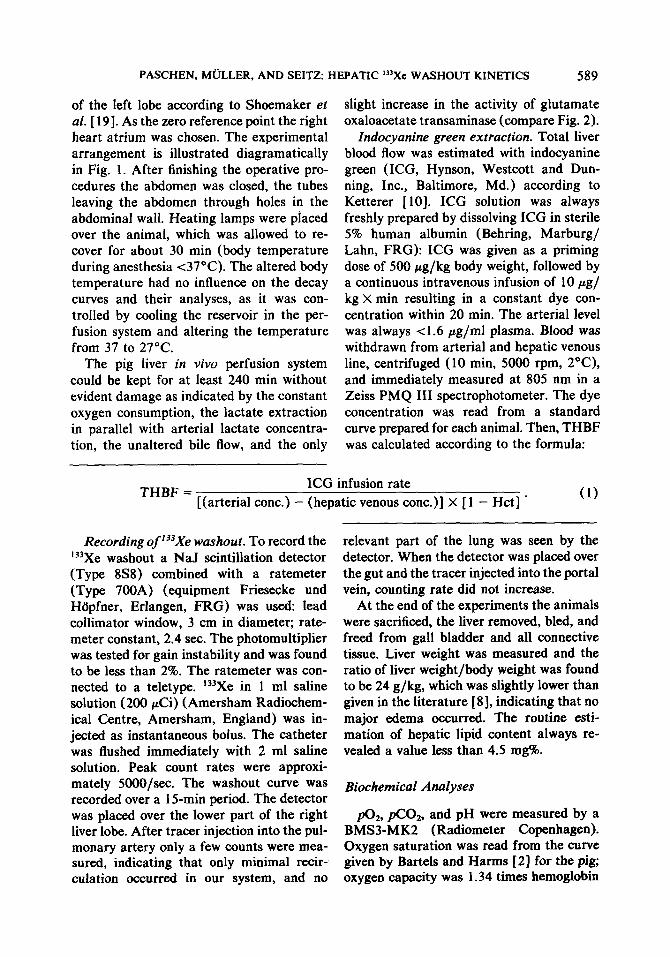
FIG. 6. Effect of hypoventilation on the calculation of THBF based on k values (A) or on H/A values (0). Hypoventilation (&Or = 60-80 mm Hg) was achieved by decreasing the tidal volume after col- lecting the data for normoventilation (pCOs = 35-40 mm Hg) in the animal (n = 3). Arterial to portal flow ratio was kept constant at approximately 1:3. Statistical analysis: (1) Normoventilation: controlled perfusion and calculated THBF based on k values, r = 0.97, P < 0.0005, n = 8; based on H/A values; r = 0.98, P < 0.0005, n = 8. (2) Hypoventilation: controlled perfusion and calculated THBF based on K values, r = 0.95, P < 0.0005, n = 9; based on H/A values; r = 0.93, P < 0.0005, n = 9. Line of identity is inserted (-).
< 0.0001, n = 69) was obtained between THBF by k values (steepest slope data) re- controlled liver perfusion and THBF cal- sulted in a large overestimation (Fig. 5). The culated from k values derived from “steepest different parts of arterial flow had no influ- slope.” However, the calculated flow greatly overestimated the pumped flow when cor- rected to liver weight. When the data anal- - ysis was performed for H/A again a corre- z lzo - lation between controlled perfusion and ; _ b ‘. . . calculated THBF could be demonstrated,
.g 100 -
.
which was in close relationship with the line \ , of identity (r = 0.91, P < 0.0001, n = 69).
i \ 2 \
\
Data Analysis of Decay Curves after 60 -
L4 5 \
\ ---_ Variation of the Arterial and Portal
\ m -N \
Flow X -a b 60 -
In order to investigate the influence of #
3 different proportions of arterial and portal L....l....I....
flows on the 133Xe washout kinetics after 5 10 15 20
portal tracer injection in three experiments HEPATIC OUTFLOW PRESSURE ( mmHg )
the arterial part of controlled liver perfusion FIG. 7. Effect of enhancing the hepatic outflow pres-
was varied from low to high values (lo-54 sure on the calculation of THBF based on k values
ml/min X 100 g) with a constant total per- (A) or on H/A values (0) at a constant pumped THBF of 72 ml/min X 100 g (m). Arterial to portal flow ratio
fusion volume. Again the calculation of was kept constant at approximately 1:3.
594 JOURNAL OF SURGICAL RESEARCH: VOL. 32, NO. 6, JUNE 1982
240
210
& m 2
120
D ai
m _ 90 1 0
m 0 ’ 60
; L?
/A A /
A / /
A/ A /AA
/ / : -
ICG-THBF (ml/minx 101
6
30
0 0 30 60 90 12c 0 30 60 90 120
PUMPED TOTAL HEPATIC BLdoD FLOW ( ml / min x 100 g )
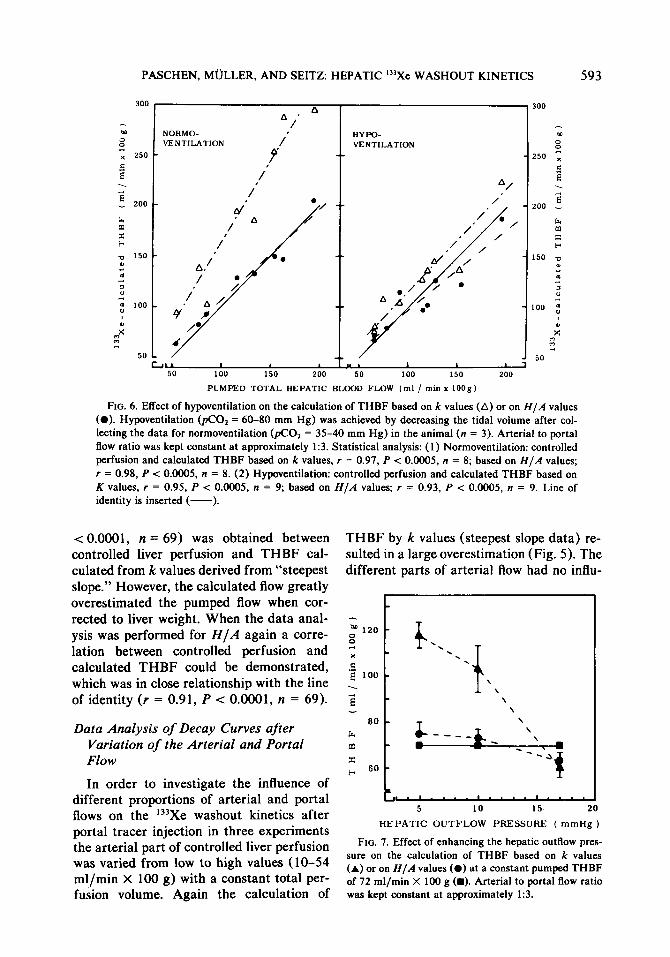
FIG. 8. Comparison between controlled liver perfusion and calculated THBF using “‘Xe washout (A) and the indocyanine green (ICG) dye extraction method (B) simultaneously in a single perfusion experiment. (A) Calculated THBF based on k values (A) and on height/area values (0); (B) calculated THBF based on ICG dye extraction method (m); (C) demonstration of the correlation between calculated THBF based on ICG dye extraction and based on “‘Xe washout (H/A data) at various pumped total liver blood flows. Values were obtained with ratio of arterial to portal flow of approximately 1:3. Statistical analysis (n = 11): pumped liver blood flows vs “‘Xe washout kinetic based on k values, r = 0.89, P < 0.0005; pumped liver blood flow vs I’Xe washout kinetic based on H/A values, r = 0.90, P < 0.0005; pumped liver blood flow vs ICG dye extraction, r = 0.94, P < 0.0005; ICG dye extraction vs ‘33Xe washout kinetic based on height/area values, r = 0.92, P < 0.0005. Line of identity is inserted (----).
ence on this phenomenon. The calculation cedure was unaffected by the state of ven- of THBF by H/A was in close agreement tilation (Fig. 6). Decay curves during hy- with the line of identity. perventilation (pCOz - 20 mm Hg) gave
data as observed during normoventilation Effect of Ventilation on Decay Curves (data not shown).
In two experiments controlled liver perfusion was performed during hypo-, Data Analysis of Decay Curves after
normo-, and hyperventilation. Hypoventila- Variation of the Hepatic Venous
tion (pC0, > 60 mm Hg) led to a shift of Outflow Pressure
the overestimation of THBF calculated from To investigate the influence of hepatic ve- k values (Fig. 6) toward the line of identity. nous outflow pressure on washout curve and The calculation of THBF by the H/A pro- its analysis the outflow pressure was altered

PASCHEN, MijLLER, AND SEITZ: HEPATIC 13’Xe WASHOUT KINETICS 595
z ,” ,I0 ICC calculated THBF (ml / min x 1OOg )
FIG. 9. Relationship between calculated THBF based on ICG dye extraction and on lJ3Xe washout (H/A val- ues) in anesthetized pigs. For experimental details see Methods. Statistical analysis: r = 0.92, P < 0.0005, n = 21.
systematically in three experiments (for de- tails see Methods). At a constant controlled liver perfusion of 70 ml/min X 100 g THBF was calculated from k values as well as from H/A values. As shown in Fig. 7 a good cor- respondence between pumped flow and H/ A values was found, whereas k values were only in line with pumped flow at increased outflow pressure.
Comparison of Liver Blood Flow Measurement by “‘Xe Washout Kinetics and KG Dye Extraction
A further series of controlled liver per- fusion was used to investigate the validity of ICG dye extraction. A close relationship between pumped flow and THBF calculated from ICG was obtained (Fig. 8B). As ex- pected the simultaneously recorded ‘33Xe washout kinetics gave only for H/A analysis liver blood flow values within the same range (Fig. 8A). Paired values of 13’Xe and ICG are depicted in Fig. 8C.
Without a controlled liver perfusion sys- tem, seven pigs were investigated under sli.ght anaesthesia: liver blood flow measure- ment was performed simultaneously with ‘33Xe washout kinetics (H/A values) and ICG dye extraction. A good correlation with
these two indirect methods was obtained (Fig. 9).
DISCUSSION
The essential finding of this study is the demonstration that the calculation of liver blood flow from Xe washout curves using the steepest slope as proposed by Leiberman et al. [ 131 resulted in a large overestimation of the actual flow (Fig. 4). This overesti- mation increased further after subtracting the slow component from the decay curve (calculation based on “fast component” ac- cording to Darle [ 53). When, however, THBF was calculated according to the mean transit time concept [20], a general approach to exponential curve analysis (for details of the theory see Lassen and Per1 [ 12]), an ex- cellent correlation with the actual flow from 25 to 210 ml/100 g X min (Fig. 4) was ob- served and in addition at different propor- tions of the arterial flow (Fig. 5), at different hepatic venous pressures (Fig. 7), and in hypoventilation (Fig. 6). Furthermore, in our experimental arrangement minimizing activity from extrahepatic sites such as in- testine and lung, only the H/A-calculated flow correlated well with THBF estimated by ICG dye extraction, as demonstrated in the controlled perfused liver (Fig. 8) as well as in the intact animal (Fig. 9). Thus, our results provide strong evidence that from the exponential curve not only the first compo- nent (k,) but also the others (k,, k3, . . . ) k,) reflect tracer washout from liver tissue. This result questions the suggestion of others, who argued that the slow com- ponents are extrahepatic in origin (lung and catheter [ 51 or intestine [ 14]), and therefore, should be neglected or subtracted, in order to obtain a monoexponential washout curve, which fits a monocompartmental perfusion model.
Contrary to our observations, reasonably good correlations between THBF, measured by electromagnetic flow meter and simul- taneously calculated (k, = k,) values, have been published recently [ 13, 151. This may
596 JOURNAL OF SURGICAL RESEARCH: VOL. 32, NO. 6, JUNE 1982
be due to two complementary, additive ex- tern of sinusoidal arrangements may cause perimental uncertainties: (i) as observed by preferential high-flow thoroughfare channels others and by us, on technical reasons the and numerous secondary sinusoids [ 61. Third, electromagnetic flow meter device often overestimates the blood flow, especially of the portal vein. Accordingly, recalculation of the published [ 13, 151 flow/tissue ratio (derived from flow values and body weight data) exceeded the ratio as given by Green- way and Stark [ 81 up to about 100%. (ii) The lack of X correction for hematocrit [ 13, 151 resulted in an underestimation of the previously calculated Xe flow by at least 10%.
Darle reported an excellent correlation between THBF, recorded with an outflow system, and the Xe-calculated flow from k values. This, however, might be the conse- quence of a number of factors: (i) THBF outflow was enhanced by (incorrect) inclu- sion of blood flow through the diaphragm; (ii) most probably the outflow recording sys- tem was accompanied by a considerable in- crease in the hepatic venous pressure, thus leading to an alteration of the Xe washout curve and consequently to a decrease in THBF calculation based on (k, = k,) values (Fig. 7); (iii) in Darle’s experiments nor- moventilation was not assured by artificial respiration and pCOz measurement. Espe- cially under phenobarbital anaesthesia, and after abdominal surgery in dorsal recum- bency, considerable hypoventilation usually occurs [ 181. In our experiments hypoventi- lation was followed by a shift of THBF de- rived from k. values from overestimation to- wards the line of identity (Fig. 6). Last, it should be mentioned that Darle [5] replac- ing his outflow- by an inflow-recording sys- tem, also observed an overestimation of THBF, derived from (k, = k,) values, as in our experiments.
As hepatic tracer washout is obviously of multicompartmental character, it is tempt- ing to speculate about the underlying reasons for the different passages through the organ: first, the varying extensions of the liver lobes may involve varying distances between inlet and outlet. Second, the “ladder-rung” pat-
it is evident from our results that the portal and arterial portions of blood flow are in- completely mixed: while after portal Xe in- jection the H/A-calculated flow correlated with the actual flow as well at low as at high arterial proportions (Fig. 5) conversely, af- ter arterial tracer injection no such corre- lation was observed-this route of applica- tion always led to gross overestimation of the arterial and underestimation of the arterial and portal flow (Fig. 3) measured at various arterial proportions (Table 1).
In conclusion, hepatic perfusion is of mul- ticompartmental character without distinct compartments, and liver arterial and portal flow are incompletely mixed. Thus, for liver blood flow measurement using inert gas washout (i) the tracer has to be injected into the portal vein and (ii) for curve analysis the general approach of the mean transit time concept should be applied.
ACKNOWLEDGMENTS
The cooperation and advice of Prof. Dr. G. Rodewald (Chirurgische Klinik), Prof. Dr. K. D. Voigt (II. Medi- zinische Klinik), and Dr. P. Dimigen, veterinarian, are gratefully acknowledged. We thank Mrs. B. Nippa for expert typing of the manuscript. This work was sup- ported by Deutsche Forschungsgemeinschaft (Sonder- forschungsbereich -34-).
1.
2.
3.
4.
5.
6.
7.
REFERENCES Andersen, A. M., and Ladefoged, J. Relationship between hematocrit and solubility of ‘r3Xe in blood. J. Pharm. Sci. 54: 1684, 1965. Bartels, H., and Harms, H. Sauerstoffdissoziations- kurven des Blutes von Sgugetieren. PJiigers Arch. 268: 334, 1959. Bergmeyer, H. U. Methoden der enzymatischen Ann&se. Weinheim: Verlag Chemie, 1974. Birtch. A. G., Casey, B. H., and Zakheim, R. M. Hepatic blood flow measured by the krypton-85 clearance technique. Surgery 62: 174, 1967. Darle, N. Xenon 133 clearance and liver blood flow. An experimental study in the cat. Acta Chir. &and. Suppl. 407, 1970. Elias, H., and Sherrick, J. C. Morphology of the Liver. New York Academic Press, 1969. Folch, J., Lees, M., and Sloane Stanley, G. H. A simple method for the isolation and purification of

PASCHEN, MfjLLER, AND SEITZ: HEPATIC 13’Xe WASHOUT KINETICS 597
total lipids from animal tissues. J. Biol. Chem. 226: of xenon133 clearance curves. Acta Chir. Sand. 142: 497, 1957. 519, 1976.
8. Greenway, C. V., and Stark, R. D. Hepatic vascular bed. Physiol. Rev. 51: 23, 1971.
9. Hollenberg, M., and Dougherty, J. Liver blood flow measured by portal venous and hepatic arterial routes with Kr”. Amer. J. Physiol, 210: 926, 1966.
10. Ketterer, S. G., Wiegand, B. D., and Rapaport, E. Hepatic uptake and biliary excretion of indocyanine green and its use in estimation of hepatic blood flow in dogs. Amer. J. Physiol. 199: 48 1, 1960.
11. Kety, S. S. The theory and applications of the ex- change of inert gas at the lungs and tissues. Pharm. Rev. 3: 1, 1951.
15. Mathie, R. T., Hughes, R. L., Harper, A. M., and Blumgart, L. H. A comparative study of liver blood flow using ‘)‘Xenon clearance and electromagnetic gowmeter measurements. Acta Chir. Sand. 144: 481, 1978.
12. Lassen, N. A., and Perl, W. Tracer Kinetic Me- thods in Medical Physiology. New York: Raven Press, 1979.
13. Leiberman, D. P., Mathie, R. T., Harper, A. M., and Blumgart, L. H. Measurement of liver blood flow in the dog using krypton-85 clearance: A com- parison with electromagnetic flowmeter measure- ments. J. Surg. Res. 25: 147, 1978.
14. Mackenzie, R. J., Leiberman, D. P., Mathie, R. T., Rice, G. C., Harper, A. M., and Blumgart, L. H. Liver blood flow measurement: The interpretation
16. Peters, A. M., and Richards, T. G. Radioxenon washout from the dog liver. Pfliigers Arch. 384: 75, 1980.
17. Rees, R. J., Redding, V. J., and Ashfield, R. Hepatic blood flow measurement with Xenon’33: Evidence for separate hepatic arterial and portal-venous path- ways. Lancer 2: 562, 1964.
18. Scholtholt, J. Das Verhalten der Durchblutung der Leber bei Steigerung des Sauerstoffverbrauches der Leber. Pjtigers Arch. 318: 202, 1970.
19. Shoemaker, W. S., Walker, W. F., van Itallie, T. B., and Moore, F. D. A method for simultaneous catheterization of major hepatic vessels in a chronic canine preparation. Amer. J. Physiol. 196: 311, 1959.
20. Zierler, K. L. Equations for measuring blood flow by external monitoring of radioisotopes. Circ. Res. 16: 309, 1965.