endovascular repair of abdominal aortic aneurysms: device-specific outcome
TRANSCRIPT
Endovascular Repair of Abdominal Aortic AneurysmsRisk Stratified Outcomes
Elliot L. Chaikof, MD, PhD, Peter H. Lin, MD, William T. Brinkman, MD, Thomas F. Dodson, MD, Victor J. Weiss, MD,Alan B. Lumsden, MD, Thomas T. Terramani, MD, Sasan Najibi, MD, Ruth L. Bush, MD, Atef A. Salam, MD,and Robert B. Smith, III, MD
From the Division of Vascular Surgery, Emory University School of Medicine, Atlanta, Georgia
ObjectiveThe impact of co-morbid conditions on early and late clinicaloutcomes after endovascular treatment of abdominal aorticaneurysm (AAA) was assessed in concurrent cohorts of pa-tients stratified with respect to risk for intervention.
Summary Background DataAs a minimally invasive strategy for the treatment of AAA, en-dovascular repair has been embraced with enthusiasm for allprospective patients who are suitable anatomical candidatesbecause of the promise of achieving a durable result with areduced risk of perioperative morbidity and mortality.
MethodsFrom April 1994 to March 2001, endovascular AAA repairwas performed in 236 patients using commercially availablesystems. A subset of patients considered at increased risk forintervention (n � 123) were categorized, as such, based on apreexisting history of ischemic coronary artery disease, withdocumentation of myocardial infarction (60%) or congestiveheart failure (35%), or due to the presence of chronic obstruc-tive disease (21%), liver disease, or malignancy.
ResultsPerioperative mortality (30-day) was 6.5% in the increased-risk patients as compared to 1.8% among those classified aslow risk (P � NS). There was no difference between groups inage (74 � 9 years vs. 72 � 6 years; mean � SD), surgicaltime (235 � 95 minutes vs. 219 � 84 minutes), blood loss
(457 � 432 mL vs. 351 � 273 mL), postoperative hospitalstay (4.8 � 3.4 days vs. 4.0 � 3.9 days), or days in the ICU(1.3 � 1.8 days vs. 0.5 � 1.6 days). Patients at increased riskof intervention had larger aneurysms than low-risk patients(59 � 13 mm vs. 51 � 14 mm; P � .05). Stent grafts weresuccessfully implanted in 116 (95%) increased-risk versus107 (95%) low-risk patients (P � NS). Conversion rates toopen operative repair were similar in increased-risk and low-risk groups at 3% and 5%, respectively. The initial endoleakrate was 22% versus 20%, based on the first CT performed(either at discharge or 1 month; P � NS). To date, increased-risk patients have been followed for 17.4 � 15 months andlow-risk patients for 16.3 � 14 months. Kaplan-Meier analysisfor cumulative patient survival demonstrated a reduced prob-ability of survival among those patients initially classified as atincreased risk for intervention (P � .05, Mantel-Cox test).Both cohorts had similar two-year primary and secondaryclinical success rates of approximately 75% and 80%,respectively.
ConclusionsEarly and late clinical outcomes are comparable after endovas-cular repair of AAA, regardless of risk-stratification. Notably, 2years after endovascular repair, at least one in five patients wasclassified as a clinical failure. Given the need for close life-longsurveillance and the continued uncertainty associated with clini-cal outcome, caution is dictated in advocating endovasculartreatment for the patient who is otherwise considered an idealcandidate for standard open surgical repair.
With the advent of an endovascular treatment option forthe abdominal aortic aneurysm (AAA), defining an appro-
priate strategy for the referral of patients to either open orendovascular repair remains a complex clinical endeavor.For example, patients who were otherwise appropriate sur-gical candidates for standard open repair have populatedmost, if not all, industry-sponsored clinical trials conductedDr. Chaikof has been paid a consulting fee and received clinical research
funding from Guidant. Dr. Lumsden has been paid a consulting fee andreceived clinical research funding from Meditronic and W. L. Gore.
Correspondence: Elliot L. Chaikof, MD, PhD, 1639 Pierce Drive, Room5105, Emory University, Atlanta, GA 30322.
E-mail: [email protected]
Presented at the 113th Annual Session of the Southern Surgical Associa-tion, December 3–5, 2001, Hot Springs, Virginia.
Accepted for publication December 2001.
ANNALS OF SURGERYVol. 235, No. 6, 833–841© 2002 Lippincott Williams & Wilkins, Inc.
833

in the United States.1–3 Among these patients, a significantreduction in hospital stay has been demonstrated, with earlyreturn to preoperative levels of activity. Enthusiasm forendovascular treatment for the patient at low risk has alsobeen coupled with the proposition that endovascular therapyprovides an ideal approach for patients in whom standardoperative repair carries an increased risk of perioperativemorbidity and mortality.4 Indeed, endovascular treatmenthas increased the proportion of patients now referred forAAA repair by providing therapy for patients who havebeen deemed inoperable because of the presence of signif-icant comorbid conditions. Nonetheless, the widespread ad-vocacy of endovascular grafting as a preferred option toopen surgery for potentially all anatomically suitable pa-tients continues during a period when most studies havereported outcomes that are largely confined to early inter-vals after intervention.
We recently reported the clinical experience with endo-vascular AAA repair at our institution.5 This updated reportreviews our mid-term experience with endovascular AAArepair over a 7-year period by examining early and lateclinical outcome in concurrent cohorts of patients stratifiedeither as patients at low risk, who would otherwise beconsidered ideal open surgical candidates, or as those whoare at increased risk for intervention. In these two groups ofpatients, we assessed perioperative morbidity and mortality,technical success, and late clinical success rates and patientsurvival.
METHODS
Patient Selection
Data for 236 consecutive patients undergoing electiveendovascular AAA repair at Emory University Hospital(Atlanta, GA) were retrospectively collected from April1994 through March 2001. An endovascular program wasinitially instituted at Emory University as part of an inves-tigator-sponsored, investigational trial (Endovascular Tech-nologies, Inc, Menlo Park, Calif/Guidant, Inc, Indianapolis,ID). This program expanded in 1999 to include a secondinvestigational device (Excluder, WL Gore and Associates,Inc, Flagstaff, AZ). We have also used the AneuRx(Medtronic, Inc, Sunnyvale, CA) endograft system after itsapproval by the Food and Drug Administration for com-mercial use in September 1999. During the study period,implanted endografts included the EVT/Guidant endograft(n � 150), the AneuRx stent graft system (n � 58), and theExcluder endograft (n � 28). The EVT/Guidant endograftsincluded tube (n � 26), bifurcated (n � 109), and aortoiliacendografts combined with a femorofemoral bypass graft(n � 15). The Gore endografts were all phase II devices.
Patients were considered at increased risk for interventionif there was 1) documentation of previous myocardial in-farction (MI) or congestive heart failure; 2) significant re-spiratory disease as demonstrated by a forced expiratory
volume in 1 second of � 1 liter/min or a requirement forhome oxygen therapy; 3) chronic liver disease with docu-mented cirrhosis or portal hypertension, or; 4) the presenceof concurrent or recent malignancy. Of note, all patientsunderwent preoperative cardiac risk assessment that in-cluded dobutamine echocardiography or persantine thalliumscanning.
Endograft Implantation
All endovascular AAA repairs were performed in a stan-dard operating room environment with complete angio-graphic capability by a team of vascular surgeons andinterventional radiologists. The techniques of transfemoralendovascular AAA prosthesis implantation have been de-scribed previously.1–4,6 Fluoroscopic guidance (OEC 9600,OEC Medical Systems, Inc, Thousand Oaks, CA) was usedfor placement of the endoprosthesis, and most of the pro-cedures were performed with the patients under generalanesthesia. All patients underwent systemic anticoagulationwith 100 U/kg heparin. Postimplantation aortography wasperformed to assess graft positioning, vessel patency,periprosthetic leakage, and graft limb stenosis. Type I en-doleaks, (leakage around the proximal or distal attachmentsite) were treated during the operation with additional en-dovascular measures. Type II endoleaks (those through ret-rograde lumbar or inferior mesenteric arteries) were ob-served and monitored with serial CT scans. At the discretionof the attending physician, this type of endoleak was treatedwith coil embolization of the patent collateral pathway.
Clinical Follow-up
Contrast-enhanced CT was performed either in the im-mediate postoperative period or within 1 month of endograftplacement. Additional imaging studies including CT, du-plex ultrasound scanning, and plain abdominal x-ray eval-uation were performed at 6 months, 12 months, and thenannually thereafter. If an endoleak was visualized, morefrequent surveillance imaging was performed as clinicallyindicated.
Definitions
All perioperative complications are described. However,major morbidity was defined as any complication that re-sulted in an increase in hospital stay, a secondary surgery, ora significant disability. The definitions of technical success,clinical success, and continuing success as described by theSociety for Vascular Surgery/International Society for Car-diovascular Surgery (SVS/ISCVS) Ad Hoc Committee onReporting Standards for Endovascular AAA Repair wereused.7 In brief, 30-day technical success was defined on anintent-to-treat basis as successful endograft deploymentwithout death, need for standard aortic reconstruction for 30days, or evidence of persistent (�48 hours) endoleak. Clin-
834 Chaikof and Others Ann. Surg. ● June 2002
ical success was inclusive of those patients who at 6 monthsafter implantation had spontaneously sealed a persistentendoleak and had demonstrated no evidence of aneurysmenlargement. Secondary clinical success was used if addi-tional endovascular techniques were required to seal anendoleak. Continuing success was defined as the mainte-nance of both clinical and technical success without evi-dence of graft thrombosis, infection, endoleak, or aneurysmexpansion of greater than 0.5 cm. Any late graft complica-tion that was successfully treated by an endovascular tech-nique was classified as a secondary continuing success.Other outcomes analyzed included successful graft deploy-ment irrespective of the presence or absence of endoleak,surgical time, operative blood loss, duration of stay in anintensive care unit, length of hospital stay, and patientsurvival.
Statistical Analysis
Descriptive data are expressed as mean � SD. Continu-ous variables were compared with the use of the Student
t-test. Nominal variables were analyzed by contingencytables. The Kaplan-Meier method with Mantel-Cox (log-rank) posthoc analysis was used to determine success andsurvival rates. P � .05 was considered statistically signifi-cant. An SAS statistical package was used for analysis(Version 5.0, Abacus Concepts, Berkeley, CA).
RESULTS
Between April 1994 and March 2001, elective endovas-cular repair of infrarenal AAA was carried out on 236patients, with 123 (52%) procedures conducted in patientsclassified at increased risk and 113 (48%) procedures per-formed in patients considered low risk for major morbidityor mortality. The incidence of comorbid conditions amongpatients deemed at increased risk for intervention is pre-sented in Table 1. Patient and procedural characteristics forthese two groups are summarized in Table 2, and the typesof endografts implanted are described in Table 3.
Notably, cardiac disease was a major indication for thecategorization of patients at increased risk for intervention.To obtain a more precise determination of the severity of
Table 1. CHARACTERISTICS DEFININGPATIENTS AT INCREASED RISK FOR
INTERVENTION (n � 123)*
Characteristic No (%)
Congestive heart failure 43 (35)Myocardial infarction 74 (60)Respiratory disease† 26 (21)Chronic liver disease-cirrhosis/portal hypertension†† 7 (6)Malignancy§ 9 (7)
* Patients may have had more than one factor increasing the risk of intervention.† Chronic obstructive pulmonary disease documented by pulmonary function
testing with a forced expiratory volume in 1 second �1 L/min or the need forhome oxygen therapy.
†† Child’s class B.§ Primary lung cancer (n � 5), metastatic colon cancer (n � 2; Duke’s stage D),
laryngeal cancer (n � 1), transitional cell carcinoma of the bladder (n � 1).
Table 2. COMPARISON OF PATIENT SUBGROUPS UNDERGOING ENDOVASCULARAAA REPAIR
CharacteristicIncreased-risk group
(n � 123)Low-risk group
(n � 113) P Value
Age (y) 73.9 � 9.2 72.1 � 6.3 NSAAA size (mm) 59.2 � 13.3 51.2 � 13.9 .007Preprocedure serum creatinine level (mg/dL) 1.2 � 0.5 1.1 � 0.6 NSOperative time (min)* 235 � 95 219 � 84 NSBlood loss (mL)* 457 � 432 351 � 273 NSPostoperative stay (days)* 4.8 � 3.4 4.0 � 3.9 NSICU stay (days)* 1.3 � 1.8 0.5 � 1.6 NS
Mean � SD.NS, No statistical significance; ICU, intensive care unit.* Includes only patients having successful endograft deployment.
Table 3. TYPES OF ENDOGRAFTSIMPLANTED
Graft TypeIncreased-risk Group
(n � 123) (%)Low-risk Group
(n � 113) (%)
Bifurcated (Guidant) 54 (44) 52 (46)Tube (Guidant) 9 (7) 19 (17)Aortoiliac* (Guidant) 13 (11) 3 (2)AneuRx (Medtronic) 37 (30) 21 (19)EXCLUDER (Gore) 17 (14) 11 (10)Conversions† 3 (2) 6 (5)Aborted procedures† 4 (3) 0 (0)
* Aortoiliac endograft performed in conjunction with contralateral common iliacartery occlusion and femorofemoral cross-over graft.
† No significant difference when analyzed by Fischer’s exact test.
Vol. 235 ● No. 6 Endovascular Repair of Abdominal Aortic Aneurysms 835

cardiac disease in our population, additional risk stratifica-tion of patients was performed with the SVS/ISCVS Car-diac Grading System.8 In brief, cardiac status is graded witha 0 to 3 flat scale where grade 0 indicates a patient with nosymptoms and a normal electrocardiogram (ECG); grade 1is used for a patient with no symptoms and a history of aremote MI (� 6 months), occult MI by ECG, or fixed defecton dipyridamole thallium or similar scan; grade 2 is used forthe patient with stable angina, the presence of a significantreversible perfusion defect on dipyridamole thallium scan,ejection fraction of 25% to 45%, controlled ectopy/arrhyth-mia, or compensated congestive heart failure; and grade 3 isused for patients with unstable angina, ejection fraction ofless than 25%, symptomatic or poorly controlled ectopy/arrhythmia, poorly compensated or recurrent congestiveheart failure, or MI within 6 months. Patients in the studyclassified as low risk (n � 113) had an SVS/ISCVS cardiacscore of 0, whereas patients categorized at increased risksolely by a history of cardiac disease had a score of 1.82 �0.53 (n � 71). Of note, most patients with cardiac diseasehad a score of 2 (58%; 41 of 71) or 3 (8%; 6 of 71).
Technical and Clinical Success
Endovascular stent graft deployment was successful in116 (95%) of 123 of patients at increased risk and in 107(95%) of 113 patients at low risk, with conversion rates of2.4% and 5.3%, respectively. No intraoperative deaths oc-curred. Intraoperative conversions to open repair and/oraborted procedures all occurred during attempted implanta-tion of EVT/Guidant endografts, except one case of at-tempted AneuRx endograft placement. These technical fail-ures were not clustered during any given time period. In theincreased-risk group, there were three immediate conver-sions to open repair and four aborted procedures. The solecase of AneuRx endograft conversion occurred when acontralateral catheter was caught in the nitinol strut and wasunable to be removed. In the second case of immediateconversion, the distal attachment hooks of an EVT/Guidanttube graft became caught on the aortic bifurcation and wereunable to be released. In the third case, a device twist wasnot resolvable with endoluminal techniques. Two abortedprocedures occurred in patients with tortuous, heavily cal-cified iliac arteries. One patient subsequently died of pro-gressive congestive heart failure several weeks after hospi-tal discharge, while the other patient declined open repair.The third and fourth aborted procedures were also related toan inability to access the aneurysm. The third patient de-clined open repair and subsequently had a fatal aneurysmrupture, and the fourth patient died 6 months later. The causeof death in this patient was not determined. A late conversionalso occurred in this group at 30 months. A patient whounderwent implantation with the original EGS (EVT, Inc.)system had attachment system failure in the form of a hookfracture. This was recognized because of the presence of apersistent endoleak and aneurysm enlargement.
The results for the low-risk group were similar, with sixconversions. Two were related to iliac artery injury and twoto the inability to access the aneurysm because of narrowedand calcified iliac arteries. Two cases of EVT/Guidant de-vice malfunction occurred during deployment. In all sixcases that required conversion, successful open repair wasperformed without postoperative complications. Two lateconversions occurred in the low-risk group, one a conse-quence of a hook fracture identified at 26 months and theother of a graft infection at 2 months.
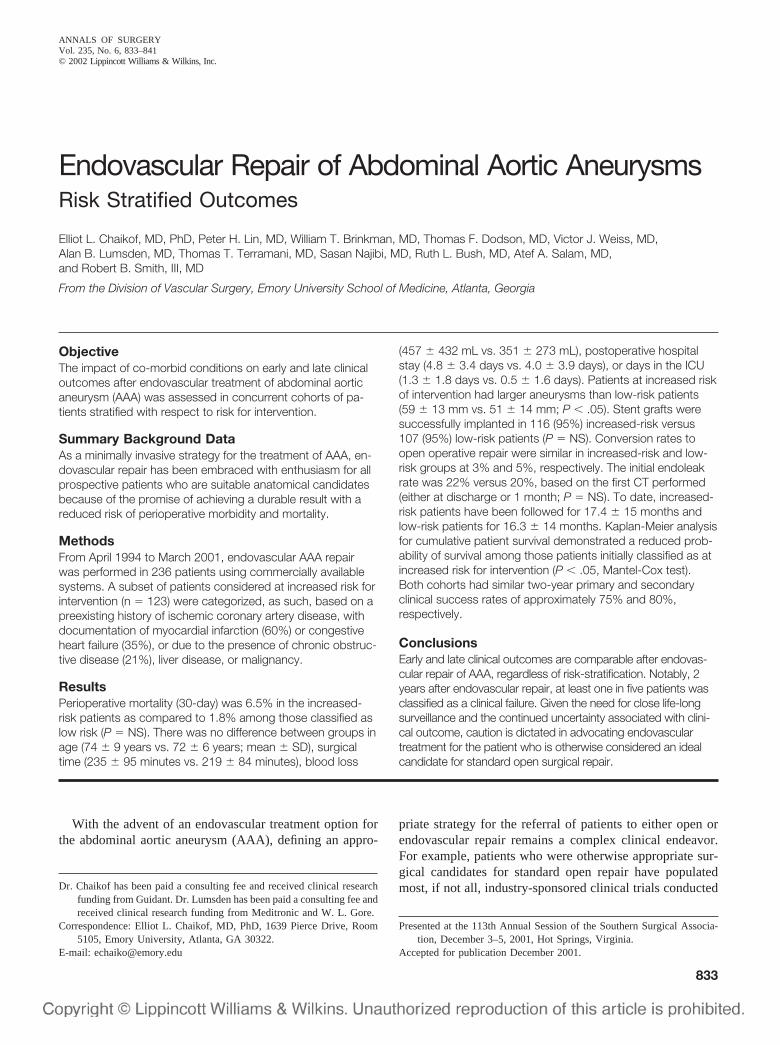
The 30-day technical success rates as defined by theSVS/ISCVS reporting standards were 73% for the in-creased-risk group and 78% for the low-risk group (P �NS). At 1 month after implantation, 25 (20.3%) patients atincreased risk and 21 (19.6%) at low risk had endoleaksdetected by CT imaging. These results remained essentiallyunchanged at 6 months, with clinical success rates at 6months of 83% for the patients at increased risk and 80% forthe low-risk cohort. Thirteen patients at increased risk andfive at low risk had spontaneous sealing of their endoleaks.All remaining endoleaks were observed during this period,and no further intervention was taken in this regard. Astatistically significant relationship between Type I and IIendoleaks and graft type was not detected. Continuing pri-mary and secondary success as defined by the SVS/ISCVSreporting standards are represented in Figure 1 and were73.5% � 10.2% and 76.5% � 9.3% for increased-risk andlow-risk groups, respectively, at 24 months. If the definitionof clinical success is revised to exclude the presence of aType II endoleak, Kaplan-Meier analysis revealed clini-cal success rates at 24 months of 76.2% � 19.60% and82.3% � 11.50% for increased-risk and low-risk groups,respectively.
Adjunctive endovascular techniques were used in bothgroups to facilitate graft implantation and aneurysm exclu-sion. In 11 patients with increased risk, one or both limbs ofa bifurcated graft had intraluminal stents placed for fabricfolds observed with either intravascular ultrasound scanningor angiography at the time of endograft deployment. Intralu-minal stents were also placed in 19 patients at low risk.Internal iliac arteries were unilaterally embolized in 13patients (seven at high risk, six at low risk) for the exclusionof ectatic or aneurysmal common iliac arteries. Iliac arterydissection was noted in one patient in each study group atthe time of graft implantation and was treated successfullyin both cases with stent coverage.
Complications
The perioperative complication rate was 17.5% and15.0% in the increased- and low-risk groups, respectively(Table 4). All wound infections were superficial and suc-cessfully treated on an outpatient basis with local woundcare and antibiotic therapy. Two patients developed acuterenal failure necessitated hemodialysis. Overall, major mor-bidity necessitating an increase in hospital stay or signifi-
836 Chaikof and Others Ann. Surg. ● June 2002
cant disability occurred in 4% (5 of 123) of patients atincreased risk and 6% (7 of 113) of patients at low risk.
Follow-up
Follow-up data were complete for all patients, with amean follow-up interval of 17.4 � 15 months for patients athigh risk and 16.3 � 14 months for the low-risk group. Nopatient was lost to follow-up. The perioperative (30-day)mortality rates were 6.5% and 1.8% for the increased-riskand low-risk groups, respectively (P � .2013, Fisher exacttest). Eight perioperative deaths occurred in the group atincreased risk for intervention. One death occurred in apatient who required conversion from endovascular repairto open repair and one in a patient who had an abortedprocedure and severe coronary artery disease. The thirddeath occurred in a patient who had a successful endovas-cular repair without evidence of postoperative endoleak. Amalignant arrhythmia was the presumed cause of death.Two deaths occurred due to postoperative myocardial isch-emia. One patient with severe chronic obstructive pulmo-nary disease and emphysema developed pneumonia postop-eratively. He developed adult respiratory distress syndromethat eventually contributed to his death. The seventh patientdeveloped acute renal failure and pneumonia postopera-tively and died two weeks following the endovascular an-eurysm repair. The eighth patient died of severe heart failureafter hospital discharge. Endograft deployment had beensuccessful in this patient, and no endoleak had been detectedby CT scanning at the time of discharge. Fifteen otherpatients died during the follow-up period.
In the low-risk group, two perioperative and nine latedeaths occurred. One death was due to intraoperative hem-orrhage and another death occurred due to presumed post-
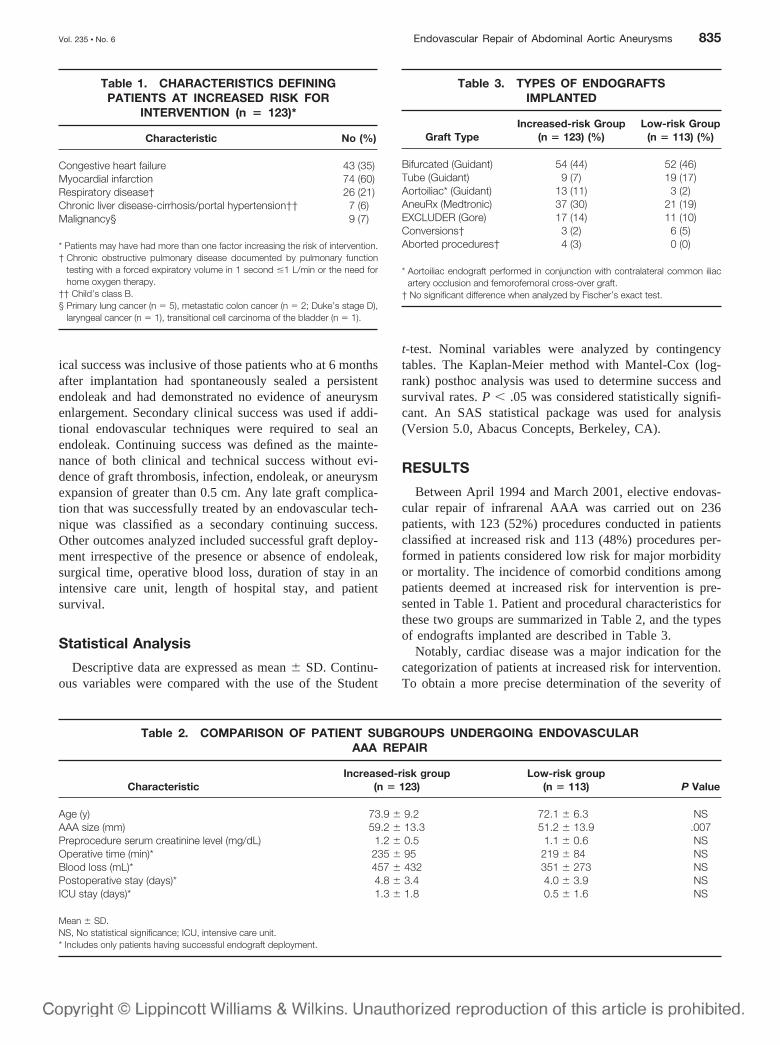
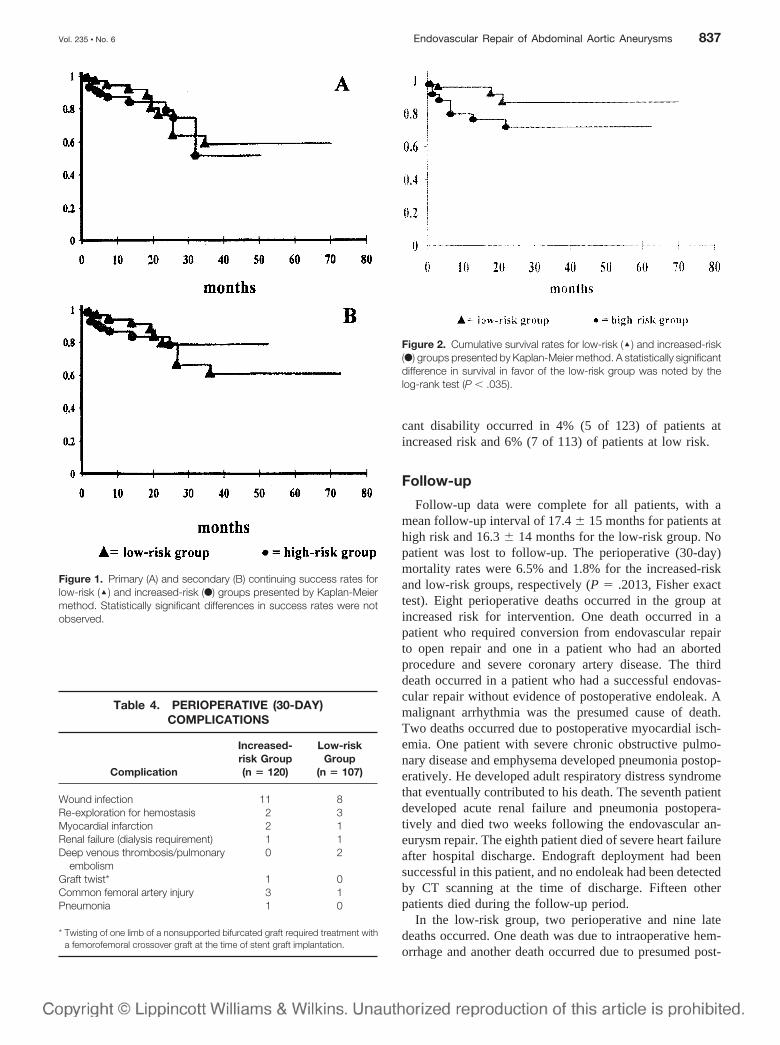
Figure 2. Cumulative survival rates for low-risk (‘) and increased-risk(F) groups presented by Kaplan-Meier method. A statistically significantdifference in survival in favor of the low-risk group was noted by thelog-rank test (P � .035).
Figure 1. Primary (A) and secondary (B) continuing success rates forlow-risk (‘) and increased-risk (F) groups presented by Kaplan-Meiermethod. Statistically significant differences in success rates were notobserved.
Table 4. PERIOPERATIVE (30-DAY)COMPLICATIONS
Complication
Increased-risk Group(n � 120)
Low-riskGroup
(n � 107)
Wound infection 11 8Re-exploration for hemostasis 2 3Myocardial infarction 2 1Renal failure (dialysis requirement) 1 1Deep venous thrombosis/pulmonary
embolism0 2
Graft twist* 1 0Common femoral artery injury 3 1Pneumonia 1 0
* Twisting of one limb of a nonsupported bifurcated graft required treatment witha femorofemoral crossover graft at the time of stent graft implantation.
Vol. 235 ● No. 6 Endovascular Repair of Abdominal Aortic Aneurysms 837

operative pulmonary embolism. Kaplan-Meier cumulativesurvival curves are shown in Figure 2. The two-year mor-tality rates were 26.5% � 8.1% and 14.2% � 7.5% for theincreased- and low-risk groups, respectively. A significantdifference between the two patient cohorts was noted by theMantel-Cox (log-rank) test (P � .035). None of the reportedlate deaths in our series were related to the initial endovas-cular procedure, device failure, or late aneurysm rupture.
DISCUSSION
The introduction of endovascular grafting was a mile-stone in the treatment of patients with AAA in that itprovided a treatment option for those patients with largeaneurysms who had been deemed inoperable because of thepresence of significant medical comorbidities.4 In the ex-tension of this technology to all patients with aneurysmaldisease, clinical investigations have confirmed that com-pared with open surgery, an early benefit in quality of lifecan be achieved, as it relates to reducing hospital stay andrecovery period.1,2 Nonetheless, even minimally invasiveinterventions may be associated with an adverse early out-come, and the presumption that an endovascular approachreduces perioperative mortality in patients at low risk com-pared with the results of standard surgery remains unproven.Moreover, an early benefit in quality of life may be offset bya lower level of late clinical success that carries with it arequirement for more intensive long-term surveillance, in-creased rates of reintervention, and higher costs and psy-chological stress. Thus, in advocating endovascular treat-ment for patients who are at low risk for operative repair, acritical analysis of late outcomes is required.
In our retrospective analysis, patients classified at lowrisk for intervention with accepted clinical and laboratorycriteria exhibited a 30-day mortality rate of 1.8% afterendovascular intervention. This result is of particular inter-est in the context of a recent review of open aortic surgeryperformed on 856 patients at our institution between 1986and 1996.9 The in-hospital mortality rate was 1.3%, with amajor complication rate of 15.9%. Thus, although the datagenerated by these two distinct reviews at the Emory Uni-versity Hospital are not strictly comparable, our experiencesuggests that in the patient at low risk, endovascular treat-ment of the infrarenal AAA is not associated with a reduc-tion in perioperative mortality compared with standard sur-gical repair.
Many reports, nevertheless, confirm that endovascularstrategies do offer unique advantages among those patientswhose comorbid conditions increase the risk of major com-plications including death. For example, May et al.10 com-pared outcomes of patients treated concurrently with eitheropen or endovascular repair. Although more than 40% ofpatients treated with endografts had been declined openrepair because of comorbid illness, no significant differencein perioperative mortality rates or long-term survival wasobserved. In addition, Chuter et al.11 observed a 30-day
mortality rate of 1.7% in their review of patients treated byendovascular approaches that had otherwise been refusedconventional AAA repair. In their patient population, cor-onary artery disease was present in 81%, congestive heartfailure in 34%, and respiratory disease in 49%. These re-ports compare favorably with published studies of conven-tional open aneurysmectomy in patients at high risk thathave been associated with mortality rates of up to 40%.12–14
Our review does reemphasize, however, that conversionto an open repair and the aborting of an endograft proceduremay not be well tolerated among those patients with signif-icant comorbidities. This is consistent with results reportedby May et al.,10,15 who have noted mortality rates of 18% to43% when primary conversion was required for patientsconsidered at prohibitive risk for standard surgery. It is ourview that both the prolonged anesthesia time and the bloodloss incurred during a preliminary attempt at endovascularrepair before conversion are important contributing factorsto these poor results. Therefore, a cautious approach shouldbe adopted in recommending endovascular repair for thepatient at high risk in the presence of anatomical constraints,which might reduce the potential for successful endograftdeployment.
With SVS/ISCVS-recommended reporting standards, 30-day primary technical success, 6-month clinical success,and 24-month primary and secondary continuing clinicalsuccess rates were all approximately 75% in both studysubgroups. Our 30-day primary technical success rate issimilar to the 77% rate reported by Zarins et al.2 for190 patients treated as part of the multicenter MedtronicAneuRx stent graft trial. Likewise, our 24-month successrate is comparable to that recently reported by May et al.16
for second-generation endovascular prostheses used in 148patients. Thus, although these results are encouraging andwill undoubtedly improve in coming years, the success ofendovascular repair remains uncertain in a significant pro-portion of patients. Two years after endograft implantation,25% of all patients were classified as failures with theSVS/ISCVS reporting standards definition.7 Therefore, inadvocating an aggressive approach for endovascular inter-vention in the patient who is an otherwise ideal surgicalcandidate, it is also important to recognize that significantlimitations to endovascular repair remain. Moreover, theimpact of this failure rate on increasing costs and reducingpatient quality of life is probably significant but admittedlywas not defined in this report.
It is notable that all reported late deaths in our series wereunrelated to the initial endovascular procedure, device fail-ure, or late aneurysm rupture. Although late survival wassignificantly compromised in those patients who weredeemed at increased risk for intervention, 75% were alive at2 years. These results are not unexpected, and others havereported similar late mortality rates for patients initiallyconsidered poor surgical candidates.11 Nonetheless, all ofthis suggests that the benefit of endovascular repair may belimited for patients who have a compromised life expect-
838 Chaikof and Others Ann. Surg. ● June 2002

ancy. In this regard, patients with a concomitant history ofrecent or concurrent malignant disease are a subgroup ofparticular interest. Of the nine patients in this group, twodied of progressive cancer 12 months after endovascularAAA repair. However, the six remaining patients were aliveat the time of last follow-up (12.4 � 8.2 months). Thus,given the imprecision in predicting the risk of AAA ruptureand long-term survival either in response to cancer therapyor other major medical illness, decisions to proceed withendovascular repair must be carefully individualized. In thisregard, we presently advocate endovascular intervention forthe patient with significant medical comorbidity only whenaneurysm size is equal to or exceeds 6 cm in diameter andpatient life expectancy is estimated to exceed 2 years. Webelieve this to be a prudent recommendation given respec-tive annual rates of rupture of approximately 6.6% and 19%for untreated patients with 5.7-cm and 7.0-cm diameteraortic aneurysms17 and our combined major morbidity and30-day mortality rate of 12% for the patient at increased riskfor intervention.
In summary, our analysis suggests that endovascular an-eurysm repair currently remains most appropriate for thosepatients with large aneurysms who are otherwise prohibitiveoperative candidates. It is significant that endovasculargrafting provides these patients with a treatment optionwhen one was not previously available. Advocating endo-vascular treatment for the patient who is at low risk forstandard operative intervention remains problematic. Al-though clinical success can be achieved in most patients,inadequate results continue to be observed in a significantportion. In deciding on a course of treatment, an informeddecision on the part of the patient requires a consideration ofthese data and an appreciation that endovascular aorticaneurysm repair remains in a relatively early stage ofdevelopment.
References
1. Moore WS, Rutherford RB. Transfemoral endovascular repair of ab-dominal aortic aneurysm: results of the North American EVT phase 1trial. EVT Investigators. J Vasc Surg 1996; 23:543–53.
2. Zarins CK, White RA, Schwarten D, et al. AneuRx stent graft versusopen surgical repair of abdominal aortic aneurysms: multicenter pro-spective clinical trial. J Vasc Surg 1999; 29:292–305; discussion306–8.
3. White RA, Donayre CE, Walot I, et al. Modular bifurcation endopros-thesis for treatment of abdominal aortic aneurysms. Ann Surg 1997;226:381–9; discussion 389–91.
4. Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal graftimplantation for abdominal aortic aneurysms. Ann Vasc Surg 1991;5:491–9.
5. Bush RL, Lumsden AB, Dodson TF, et al. Mid-term results afterendovascular repair of the abdominal aortic aneurysm. J Vasc Surg2001; 33:S70–6.
6. Harris EJ. Modular systems in the treatment of abdominal aorticaneurysms: lessons learned in the development of designer endografts.Semin Vasc Surg 1999; 12:170–5.
7. Ahn SS, Rutherford RB, Johnston KW, et al. Reporting standards forinfrarenal endovascular abdominal aortic aneurysm repair. Ad Hoc
Committee for Standardized Reporting Practices in Vascular Surgeryof The Society for Vascular Surgery/International Society for Cardio-vascular Surgery. J Vasc Surg 1997; 25:405–10.
8. Rutherford RB, Baker JD, Ernst C, et al. Recommended standards forreports dealing with lower extremity ischemia: revised version. J VascSurg 1997; 26:517–38.
9. Berry A, Smith RB, 3rd, Weintraub W, et al. Age versus comorbiditiesas risk factors for complications after elective abdominal aortic recon-structive surgery. J Vasc Surg 2001; 33:345–52.
10. May J, White GH, Yu W, et al. Concurrent comparison of endoluminalversus open repair in the treatment of abdominal aortic aneurysms:analysis of 303 patients by life table methods. J Vasc Surg 1998;27:213–21.
11. Chuter TA, Reilly LM, Faruqi RM, et al. Endovascular aneurysmrepair in high-risk patients. J Vasc Surg 2000; 31:122–33.
12. Sterpetti AV, Schultz RD, Feldhaus RJ, et al. Abdominal aortic aneu-rysm in elderly patients. Selective management based on clinical statusand aneurysmal expansion rate. Am J Surg 1985; 150:772–6.
13. Morishita Y, Toyohira H, Yuda T, et al. Surgical treatment of abdom-inal aortic aneurysm in the high-risk patient. Jpn J Surg 1991; 21:595–9.
14. Hollier LH, Reigel MM, Kazmier FJ, et al. Conventional repair ofabdominal aortic aneurysm in the high-risk patient: a plea for aban-donment of nonresective treatment. J Vasc Surg 1986; 3:712–7.
15. May J, White GH, Yu W, et al. Conversion from endoluminal to openrepair of abdominal aortic aneurysms: a hazardous procedure. Eur UEndovasc Surg 1997; 14:4–11.
16. May J, White GH, Waugh R, et al. Comparison of first- and second-generation prostheses for endoluminal repair of abdominal aorticaneurysms: a 6-year study with life table analysis. J Vasc Surg 2000;32:124–9.
17. Taylor LM, Porter JM. Basic data related to clinical decision-makingin abdominal aortic aneurysms. Ann Vasc Surg 1987; 1:502–4.
Discussion
DR. GREGORIO A. SICARD (St. Louis, MO): I would like to thank Dr.Dodson and Dr. Chaikof and the Emory University Division of VascularSurgery for allowing me to discuss this excellent paper as well as for thetimely copy of the manuscript to review.
Over the last 10 years since the initial description by Juan Parodi,endoluminal repair of abdominal aortic aneurysm has undergone extensivescrutiny evaluating its efficacy and safety. Despite the phase 2 FDA trialsof various devices, no prospective, randomized trial comparing open toendoluminal elective repair of aneurysm has been conducted, making ascientifically valid comparison unfeasible.
In this excellent report by Dr. Chaikof and the Emory UniversityVascular Surgery Group they extend the scrutiny of endoluminal grafts bycomparing patients of high and low risk and ask the question to whomshould it be offered. The excellent results presented reflect the experienceof the Emory Group in performing endovascular repair of abdominal aorticaneurysm that may not be duplicable in most clinical settings. A fewquestions:
Did you notice any difference in your results in your earlier 2 or 3 yearsof experience comparing it to the last 4 or 5 years? In other words, what doyou think is the learning curve for this procedure?
Several endografts were used in your series, with the largest numberbeing the two currently commercially available grafts, the Ancure(Guidant) and the AneuRx Medtronic. Did you find any differences be-tween these two grafts in technical and clinical success, complications,long-term survival, in either the low or high-risk groups.
I also notice in your presentation and manuscript that advanced age wasnot an indicator of high-risk status. Our recently published institutionalexperience comparing open versus endoluminal repair for elective aneu-rysm repair in 470 patients, 260 performed endoluminally and 210 open,showed that although there was not a significant difference in mortalitybetween octogenarians and the younger-than-80 groups, although it was
Vol. 235 ● No. 6 Endovascular Repair of Abdominal Aortic Aneurysms 839

lower in the younger-than-80 group, there was a significant difference inthe perioperative complication rate being significantly higher in the octo-genarians compared to those younger than 80 years of age for both open aswell as endoluminally repaired aneurysms. Did you evaluate your data forresults in octogenarians? If so, did you find any differences?
Because of the high incidence of abdominal aortic aneurysms in men, aswell as, anatomical constraints, women tend to be recipients of endograftsless frequently than men. Could you comment about what percent of yourpatients in both either low- or high-risk groups were women and was therea difference in complication rate and long-term survival?
Finally, I would like to get your opinion: where do you think theindications and application of this novel approach for aneurysm repair isheading? We are currently using first and second-generation endografts. Asthese devices become smaller and easier to use and as procedure-relatedcomplications decrease, do you think that this technology should be limitedto high-risk patients or that both patient predilection as well as increasedtechnical success will make endoluminal treatment of abdominal aneurysmthe treatment of choice in anatomically suited both high and low riskpatients?
I really appreciate the opportunity to comment on this paper and theprivilege of the floor.
DR. JAMES M. SEEGER (Gainesville, FL): I also want to compliment Dr.Dodson on his nice presentation and the Emory Group for sending me theirpaper in a timely fashion to review.
Dr. Dodson presented results from a retrospective review of a relativelylarge number of patients undergoing endovascular aneurysm repair in asingle institution. Furthermore, he has assessed and compared the out-comes in these patients categorized as low risk and increased risk groups,categories that seem clinically relevant to the decision-making concerningendograft repair of abdominal aortic aneurysms. The reported results arevery acceptable and, as pointed out in the manuscript, very similar to othersingle institutional trials.
Beyond that, what have we really learned from this review? To me, thereare three things: One, that attempted but unsuccessful stent graft repair ofabdominal aortic aneurysms is associated with not inconsequential risk,particularly in patients with significant comorbidities. Second, that stentgraft repair even in low risk patients is not risk free. And finally, thatcontinuing clinical success defined as the percentage of patients survivingwith continuing aneurysm exclusion in the Emory experience is about 80%at two years.
Like carotid endarterectomy, elective aortic aneurysm repair is a pro-phylactic procedure and thus to be beneficial must result in better outcomesthan the natural history of the disease without treatment. It has beenpresumed that stent graft repair will be less morbid and thus would improvethe benefit of intervention in the aneurysm disease. To date that has notbeen conclusively demonstrated. Therefore, given results such as thosepresented today, how should we currently choose the patients to whomstent graft repair of aortic aneurysm should be offered? As previouslymentioned, I think that considering the patients in two different groups, lowrisk and high risk for open surgical repair, is valuable, as the risk-benefitratio, and thus the decision to offer repair is different in these two groups.This raises several questions:
First, your definition of increased risk seems to me a bit broad. Witheven a history of MI or stable angina being included – and in fact, as notedin the manuscript, representing the majority of patients who were in theincreased risk group, does this skew your results in the increased risk groupand did the complications in this group of patients actually occur in thepatient’s more severe comorbidities? If this is true, this to me makes itdifficult to compare these results of endograft repair to previously reportedresults of open surgical repair inpatient judged high risk of open repair.
Second, as you point out in your manuscript, from a recent review ofopen surgical repair in your institution, the mortality associated with opensurgical repair of infra-renal aortic aneurysms was equal to that in thelow-risk patients undergoing endograft repair. However, I suspect that allyour patients undergoing open repair were not without any clinical evi-dence of heart disease as it appeared from your manuscript that your lowrisk patients were. This would make the outcome of endograft repair in
low-risk patients, who presumably were very good surgical candidates foropen repair, less compelling when compared to the results of open surgicalrepair.
Finally, on a little bit more philosophical note – and this is, I think,where we all stand in trying to understand this – how do we evaluate thisnew approach to the treatment of aneurysm disease in two patient groups?Chris Zarins, for one, has suggested using the concept of rupture-freesurvival as the best method of assessing benefit after aneurysm treatment,much like we assess stroke-free survival in patients with carotid diseaseundergoing intervention. Based on your endograft results presented hereand your open surgical reports reported in your paper, are you benefitingthe high risk and the low risk patients when you use this method ofcomparing them? Using your numbers, my calculation suggests that youlikely are benefiting the high-risk patients compared to no intervention andpotentially even to open surgical repair. In contrast, surprisingly, theoutcome at 2 years is essentially equivalent in the low-risk patients under-going either endograft or open surgical repair. Calculating the rupture-freeoutcome in these groups, at least by my calculations, I saw only one patientin the surgical group that would have survived that would not havesurvived in the endograft group. I would appreciate your comments on thisand your thoughts, as Dr. Sicard has suggested, on how these results aregoing to influence your selection of patients for endograft repair.
DR. RAYMOND S. MARTIN, III (Nashville, TN): I enjoyed hearing thereport of the Emory Group and found the outcomes similar to our own. Ihave a couple of additional questions:
First, did you find a difference in endoleak or other complications whenusing component versus unibody devices?
Second, was there a difference in the mean diameter or the complicationrates in these patients and those treated by the open technique during thesame time period?
Third, we found that some of our perioperative complications are re-lated, in retrospect, to stretching the limits of the devices in terms of aorticneck diameter or iliac size, particularly small iliacs and tortuosity. Haveyou experienced the same thing? And do you think there is a role forendovascular repair in low risk patients using conservative criteria; that is,the best patients anatomically?
Finally, one of the disadvantages of the endograft procedure is theburdensome follow-up process. This alone is a reason to consider using theopen procedure in patients with long life expectancies. Do you think thatyearly CT scans are really necessary in patients after 2 or 3 years ofstability?
DR. IAN HAMILTON (Chattanooga, TN): Whether it is open aneurysmrepair with simultaneous renal artery revascularization or, as we see today,endograft repair, we continue to look to Emory for leadership in vascularsurgery. I enjoyed the paper. A couple of questions:
With a young endograft program in Chattanooga, we have been coun-seled to try to apply this technology to our anatomically low-risk patientson the front end of our learning curve. I wonder if the similarities betweenhigh and low-risk patients in this group may reflect a disproportionatetiming of low-risk patients that are being treated early in the learning curveof three different devices.
The other issue that is not addressed in the paper has to do withpostendograft versus postopen aneurysm repair quality of life. I waswondering if the authors have any insight into those quality of life issues.
DR. GARY MAXWELL (Wilmington, NC): I have a question about whatmay come to be called “incidental” renal artery angioplasties. As I enterdata into our vascular registry, I have noted about 30% of patients arereceiving renal artery angioplasty. Whether it is “incidental” or not, I can’tbe sure from the data, since I cannot identify the indications for the renalangioplasty.
My question is, how many of these patients have had concomitantangioplasty, and do you have any opinion about whether we are helping orhurting patients with regard to their hypertension? Do you have any datathat speaks to that question?
DR. ELLIOT L. CHAIKOF (Atlanta, GA): I would like to thank the discus-sants for their insightful comments and probing questions. Dr. Sicardinquired as to whether our technical success rates improved as our expe-
840 Chaikof and Others Ann. Surg. ● June 2002

rience with endovascular devices grew. To some degree this has been thecase, with a commensurate improvement in our experience in both patientselection and device deployment. Overall, technical success rates remainhigher among lower profile devices, such as those produced by Medtronicand W. L. Gore, as compared to the higher profile Ancure system producedby Guidant, Inc. Nonetheless, we continue to believe that hook fixation,which is associated with the Ancure device, is an important feature forendograft stabilization. Overall, each of these devices has their own re-spective advantages and limitations.
Dr. Sicard requested information regarding our results among patientsover 80 years of age and among women. There were 30 octogenarians inan intent-to-treat subgroup and successful deployment was achieved in 28.Significantly, major postoperative morbidity occurred in only two or 7% ofthese patients. Thus, a reduction in major postoperative morbidity, thecapacity for patients to rapidly return to their preoperative quality of life,and a reduction in hospital stay continues to drive our interest in endovas-cular approaches to AAA repair. Although not demonstrated by random-ized trail, we also believe that a reduction in major adverse postoperativeevents is inherently associated with a reduction in mortality among patientsat increased risk for open repair. With regards to the distribution of maleand female patients, access to an aortic aneurysm using an endovasculardevice is currently difficult or impossible with available commercial de-vices unless at least one iliac artery is at least 7 millimeters in diameter orlarger. Most women with aneurysmal disease have relatively small iliacarteries and, therefore, are often excluded from consideration for endovas-cular repair. As a consequence, most of the patients in this report were men.
Dr. Seeger questioned whether our complications may have been dis-proportionately localized to a small group of patients at especially high riskfor intervention and inquired as to whether rupture-free survival is anappropriate form for reporting results of endovascular AAA repair. In brief,complications in our analysis were evenly distributed among all patients. It
bears reemphasis that the overall incidence of major postoperative mor-bidity was relatively modest, on the order of 5% among patients atincreased risk for intervention, which compares to reported incidences inthe literature of at least 10 to 15% for patients treated with open repair.Admittedly, reports that include rupture-free survival as a sole measure ofsuccess are limited by the inherent heterogeneity of aneurysm size withinthe study population and, as a consequence, varying risks of rupture fromone treatment to another. Thus, use of this outcome measure alone wouldbe comparable to an analysis of two different treatment strategies forcancer management without stratification with respect to tumor burden oroverall stage of disease.
As a final comment, our indications for aneurysm intervention have notchanged with the advent of endovascular approaches for repair. For thelow-risk patient, intervention is recommended for aneurysms of at least 5centimeters in diameter and for those at higher risk, treatment is recom-mended for aneurysms of at least 6 centimeters in diameter. Of course, theone exception to this statement is the patient with a large aneurysm andsignificant comorbidities who, before the introduction of endoprostheses,was not considered a treatment candidate. The utility of endografts forthese patients is quite clear. In summary, it should be noted that amongpatients with suitable anatomy there are no absolute contraindications forendovascular AAA repair. Nonetheless the need for lifelong surveillance,secondary interventions, the risk of late device failure, and the absence oflong-term data in large numbers of patients, has tempered our enthusiasmfor this approach in the young patient with a long life expectancy who isotherwise at low risk for standard surgery. For the time being, the watch-word associated with the implantation of an endovascular device in thelow-risk patient, particularly those under 70 years of age, must remaincaveat emptor. In contrast, for the patient at increased risk for standardsurgery, the positive impact of endovascular repair is clear andunequivocal.
Vol. 235 ● No. 6 Endovascular Repair of Abdominal Aortic Aneurysms 841