cuspal deflection in mod molars restored with bulk-fill
TRANSCRIPT
Cuspal Deflection in MOD Molars Restored with Bulk-fill
Versus Layered Resin Composite Restorations (A
Comparative in-vitro Study)
Dahlia Mowafaq Mohammed
1, Sawsan Hameed Aljubori
2
1Ninavah Health Directorate, Mosul, Iraq.
2Department of Conservative Dentistry, College of Dentistry, University of Mosul, Mosul, Iraq.
Email Address: [email protected]
Received: 20 Nov 2021, Revised: 23 Nov 2021, Accepted: 1 Dec 2021, Online: 26 Dec 2021
Abstract
Objectives: To evaluate the accuracy of the bulk-fill application technique with its effect on the cuspal
deflection of molars with class II MOD cavities filled with bulk-fill and conventional composite resin
restorations. Aims of the study: The aims of this study focused on comparing and evaluating the cuspal
deflection of bulk-fill composite resin materials (high and low viscosity) with conventional composite resin
material using incremental and bulk-fill application techniques by assessing shrinkage stress and elastic
modulus(E£). Materials and Methods: Thirty human molars teeth received standardized class II mesio-occlusal-
distal cavity preparation and were restored with three types of composites: [Filtek (Z350XT), 3M-ESPE (USA)],
[SDR surfil plus (DENSPLY)], [Tetric- Evoceram bulk- fill (Ivoclar viva-dent)]. Teeth were divided into three
groups (n=10) according to the type of composite resin, then each group was subdivided into two groups (n=5)
depending on the application techniques (Bulk-fill and Incremental filling). Filtek Z350XT composite was used
as a control group in incremental and bulk-fill techniques which was tested as a conventional incremental
material according to manufacture instruction represented as positive control subgroup and also as bulk-fill
product, represented as negative control subgroup. The buccal and palatal cuspal deflection was measured using
a strain measurement system, in addition, thirty specimens were prepared for each composite resin material and
used to evaluate and measure the elastic modulus (E£) by three-point bending test using a universal testing
machine (Gester, Total Testing Solution). Results: Teeth filled with bulk-fill composite resin restoration had
significantly lower total cuspal movement values compared with conventional composite resin restoration for all
groups ( incremental and bulk-fill application techniques). Incremental and bulk-fill application techniques
groups with low-viscosity SDR surefil plus and high-viscosity Tetric- Evoceram bulk-fill composite resin
restoration were not significantly different from each other. Bulk filled and incremental filled with low-
viscosity SDR surefil plus have a significantly lower cuspal movement than all other groups. P-value less than
or equal to 0.05 was considered statistically significant. Conclusion: Incremental application technique was the
best technique to lower the polymerization shrinkage stress and it's complication. Bulk-fill application technique
of low-stress bulk-fill composite resin restorations achieved comparable results to incremental application
technique. The use of the incremental technique with low polymerization shrinkage stress has dwindled but it is
safer to continue to use the incremental application technique, as a significant number of the bulk-fill and
conventional composite resins produced higher polymerization shrinkage stress without it.
Keywords: Bulk fill restorative material, Cuspal deflection, Intercuspal distance, Elastic modulus.
Journal of Global Scientific
Research
www.gsjpublications.com/jgsr
www.gsjpublications.com
Journal of Global Scientific Research (ISSN: 2523-9376)
6 (12) 2021/ 1952-1971

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1953
1. Introduction
Since the development of the composite
resin as an esthetic restoration alternative
to old-dental amalgam restoration in the
late 1950s. Composite resins are mercury-
free, adhered to the dental structure
through the dental adhesive system, low
thermal conductivity. The materials have
found increasing application in modern
preventive and conservative dentistry as
the material undergo catastrophic
development; alternative photo-initiators
system, application of nano- filler particles
technology, novel- resin monomer, blend –
resin monomer, and the development of
the translucent dental composite resin to
the blue light permit curing up to 4mm
thickness of the restorations and produce a
restoration with natural tooth appearance
with long term performance (Kalliecharan
et al., 2016; Ricci et al., 2019).
The incremental technique is based on
polymerizing with resin-based composite
layers < 2.0 mm thick to ensure a complete
polymerization, secure the adhesion of the
restoration to the cavity wall, and can help
achieve a good quality of the margin. The
incremental technique increasing the
unbounded area for each increment layer
allows for material to flow, maximizes the
relaxation of polymerization shrinkage
stress, minimized the stress on the
prepared cavity walls and its complications
(Deliperi and Bardwell, 2002;
Chandrasekhar et al., 2017 ).
The main disadvantages of the incremental
filling technique are time-consuming (as
multiple increments must be inserted and
individually light cured), lack of bond
between layers, technique sensitivity,
contamination, or incorporation of voids to
the mass of the restoration. Recently, the
concept of bulk-fill technique ( the
restoration placed in a 4.0-mm bulk in one
increment ) was introduced by some
authors not only to save time but also to
reduce stress at the cavosurface margins
and to reduce the potential for errors
(Giachetti et al., 2006; Menees et al.,
2015).
Cuspal deflection occurs in teeth restored
with composite resin materials as the result
of the interaction of polymerization
shrinkage stress in the composite resin
restoration and the compliance of the
remaining teeth structure after cavity
preparation that impact the adaptation of
the restoration to the cavity walls (Lee et
al., 2007; Hamama et al., 2011; Oskoee et
al; 2012).
The deformation occurred as a
combination of stresses in restoration,
across the tooth restoration interface and
the tooth structure. Cusp compliance is an
important factor that affects the amount of
cusp deflection, compliance is defined as a
change in dimension of the object to unit
force and has the opposite meaning to
stiffness, thus the degree of compliance
can affect the result of the measurement
stress. The teeth with high compliance,
that the cusps will deflect more easily, the
teeth with cavities exhibit relatively a high
compliance. Cuspal deflection may cause a
change in the occlusal contact relation of
the teeth and may cause postoperative
teeth sensibility or with greater magnitude
of this deflection lead to the greater degree
of micro deformation in tooth cusps and
consequently increase the possibility of
fracture under the stress far below the
maximum strength of the restored tooth
may occur (Oliveira et al; 2012; Kim et
al., 2016)
Inward displacement of the cusp was much
slower and longer than polymerization
shrinkage of composites therefore cuspal
deflection was used by many authors to
study the influence of restorative
procedures and restorative material
properties and provided indirect
quantifying measurements of
polymerization stress in the composite
being restricted by bonded to the cavity

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1954
walls, as the polymerization stress cannot
be directly and simply measured in
restored teeth cavities (McCullock and
Smith, 1986; Campodonico et al., 2011;
Karaman and Ozgunalty, 2013).
The measured cuspal deflections averaged
15μm to 50μm but varied according to the
technique used, the measurement method,
the cavity size, and tooth type. An absence
of standardization of tooth size, tooth
cavity preparation, and restoration
technique renders comparison of result
difficult since the cusps contraction
depends on the amount of the remaining
tooth structure. Some studies combined
cuspal deflection with microleakage
analysis for shrinkage stress determination
(Moorthy et al., 2012 and Kweon et al.,
2012).
Different inexpensive and simple
measurement devices had been used to
measure cuspal deflection included non-
contact and contact methods. Non-contact
methods such as; Digital image correlation
(DIC), Microscopy, Laser scanning, and
3D micro-computed tomography Contact
methods such as Twin-channel deflection
measurement gauge, Linear variable
displacement transducers (LVDT), Direct
current differential transformers (DCDTs),
the Deflection of metal strip with
microscopy indicated cusps alignment,
Digital micrometer, and Strain gauge
measurement system (Palin et al., 2005,
Faisal and Nashaat in 2018).
A modification of the strain gauge method,
which was developed in cooperation
between the engineering and dental staff
(Hamama et al., 2011). they were
relatively small grid areas of only a few
millimeters. Bonded on the external
surface of buccal and lingual cusps about
2.5mm from the cusp tips. It had been
reported that cusp fracture in restored teeth
commonly occurs in this area and it was
considered that this area was likely to be
the region subjected to the highest strains
(Lee et al., 2007; Shebl et al., 2018).
The strain gauge measurement system has
many computerized advantages and it
provided accurate quantitative and
qualitative measurements, details, a large
amount of data storage, and easy recall as
the process of micro deformation
experienced by the cusp led to the
covariance of electrical resistance later this
covariance was sent to the data acquisition
panel and conveyed into digital signs,
which displayed in curve format which
was consisted of peaks and valleys which
read in specified software and could be
provided a further expression in future
studies. The accuracy of these
measurements is more reliable than with
conventional measuring systems (in which
the measurements were based only on
deflection range values or difference
between the post-curing and pre-curing
values) as the data are automatically
calculated by a specified software program
(SI Prog). In addition, the result from
measurements showed that the highest
levels of strain were produced during
exposure of the restoration to the light-
curing source for polymerization
(Hamama et al., 2011; Nashaat and
Mohammed, 2018).
The main limitation of this measurement
system is that it was needed to obtain two
symmetric channels buccally and lingually
to judge whether the contraction occurs
simultaneously in both cusps or one cusp
more than the other. In addition, a greater
variety of micro deformation results might
occur due to the influence of a greater
number of factors. Factors that could
influence or interfere with the passage of
the current strain gauge measurement
system might include: the orientation of
the strain gauge sensor during the bonding
on the external surface of the cusp, thermal
vacillations, and the number of
information that might be lost in the path
between the strain gauge sensor and the

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1955
entrance device (data acquisition) (
Hamama et al., 2011; Rocha et al., 2013;
Shebl et al., 2018).
The purpose of this study was intended to
evaluate the effect of different application
techniques ( bulk-fill ⁄ incremental ) of
bulk-fill (low and high viscosity) and
conventional composite materials and their
roles to reduce the shrinkage stress by
assessing the cuspal deflection of class II
media-occluso-distal composite resin
restorations. The cuspal deflection was
measured using a strain measurement
system. The influence of the elastic
modulus of the different types of
composite resin restoration on the
polymerization shrinkage stress is also
verified.
2. Materıals and Methods
Materials:
The main materials used in this study: [
Filtek (Z350XT), 3M-ESPE(USA)],[ SDR
surfil plus (DENSPLY)], [Tetric-
Evoceram bulk- fill (Ivoclar viva-dent)],[ OptiBond FL (Kerr)].
Methods:
Selection of Teeth
Thirty extracted sound human third molars
(n=30) have been collected within four
months for this study. The teeth collected
from patients ranged from 18-33 years.
The inclusion criteria that the selected
teeth were free from .decay, cracks,
.attrition, previous restoration, any
malformation defects, and any visible teeth
defect resulting from the extraction, the
teeth with a complete root formation. The
teeth were selected to have nearly
standardized intercuspal width and
mesiodistal length which were measured
with a digital caliper, within a maximum
mean of deviation of 10%, from their
respective specific mean (9.5-10.5mm and
10.5-11.5mm).
The teeth were debrided from blood,
saliva. rinsed with water, the teeth were
disinfected in 0.1% thymol solution ( as it
alters less the conditions of dental
structures for adhesion) and after that
stored in distal water at room temperature
to keep the specimens hydrated until the
time of the study was carried out.
Preparation of the Mold and Mounting of
Teeth
Each tooth was marked 2±0.5mm above
the (CEJ) amelo-cemental junction with an
indelible pen. Polyvinyl chloride (PVC)
retentive tube, with two centimeters in
diameter and two centimeters in length,
was used as a mold for mounting the teeth,
Figure (1a). Each tube was filled with
polyvinyl siloxane impression material
(Dursoil putty addition polyvinyl siloxane
impression material, Germany), and by
aiding of surveyor mounted the occlusal
surface of the teeth with sticky wax so the
roots of each tooth had been positioned at
the center of the retentive tube, with the
long axis of the tooth parallel to the sides
of (PVC) were extended 2± 0.5mm below
the cement-enamel junction.
For the proximal cavities, to facilitate the
material placement, improve the
restorative material adaptation and shorten
the finishing steps, an impression for the
tooth crown was made prior to cavity
preparation with polyvinyl silicone which
was placed in a (1.5cm) diameter
cylindrical plastic tube used as a tray to
create a custom matrix for restoring
proximal box, Figure (1b). After setting
the impression material the plastic tube
was removed and trimmed of all the
material overlaying the occlusal surface of
the tooth, Figure (1c).

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1956
Grouping of the Specimens
Thirty prepared teeth were selected
randomly for strain measurements and
distributed into three experimental groups
according to composite material (n=10),
then each group was subdivided into two
equal subgroups according to filling
technique (n=5): Incremental and bulk-fill
technique.
Preparation of the Teeth
Standardized large slot (MOD) cavities
were prepared without proximal boxes in
order to reduce the preparation variation.
Cavities were prepared in each tooth by
using of milling machine (Bio-art), Figure
(2), flat-ended fissure bur (HP559S31)
(diameter 1.20mm) is mounted in a
straight handpiece with coolant water, the
cavity preparation was carried within a
stainless steel frame which is referred to it
as "guiding frame".
The guiding frame was attached to the
acrylic mold fixture by an adjusting screw
and was adjusted to be as near as possible
over the occlusal surface of the tooth and
the vertical part of the "guiding frame"
over the marginal ridge to ensure
standardization of the cavity in all
preparation. The result is nearly
standardized cavity width (4±0.3) and the
cavity depth was (4±0.3), Figure(3), the
bur was replaced every five preparation to
ensure high cutting efficiency. The
accuracy of cavity measurements was
aided by using a periodontal probe, using
dental magnifier loops with (2.5x
magnification).
Figure (1): A: The teeth mounted in polyvinyl chloride (PVC) retentive tube, B: A
cylindrical plastic tube of (1.5cm) in diameter used as a tray , C: custom matrix
for restoring proximal box.
A C B
Figure (2):Bio-art milling
machine.
Figure (3): Standardized
large slot (MOD) cavity.
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1957
Restorative Application
After standard class II cavities were
prepared for each sample, samples were
acid-etched and bonded using the same
total-etch system (Kerr Gel Etchant and
OptiBond FL, Kerr) to reduce the number
of variables. The silicon putty band which
was previously prepared for each
respective tooth has been used. Cavities
were encircled with silicon putty matrix
band with a mylar strip was adapted
against the proximal aspect on the teeth
being restored. Cavities were then restored
with resin composite restoration.
Composite in all groups applied in the
prepared cavities depending on the filling
techniques. In an incremental technique
(horizontal incremental technique) two
layers ( the thickness of each increment of
resin composite is not more than 2mm).
Each increment should be fully
polymerized before the next one is inserted
into the cavity for (20) seconds. For the
bulk-fill technique, the cavity filled in one
increment, the thickness of the increment
of resin composite is 4mm thickness which
was verified by the using periodontal
probe. Then light cured for (20) seconds,
using the light emitting diode (LED)
(eighteenth) at an irradiance of
(1500mw/cm²), the intensity of light cure
measured by radiometer before application
with a wavelength range between (380-
515). The light-curing tip touching the
slopes of the cusp tips of the teeth for
standardized the position of the light cure .
After removal the impression matrix
additional curing from the facial and
lingual aspect of the proximal boxes to
ensure complete polymerization. The
intensity of (LED) light source was
monitored before and after curing
throughout the study with a radiometer.
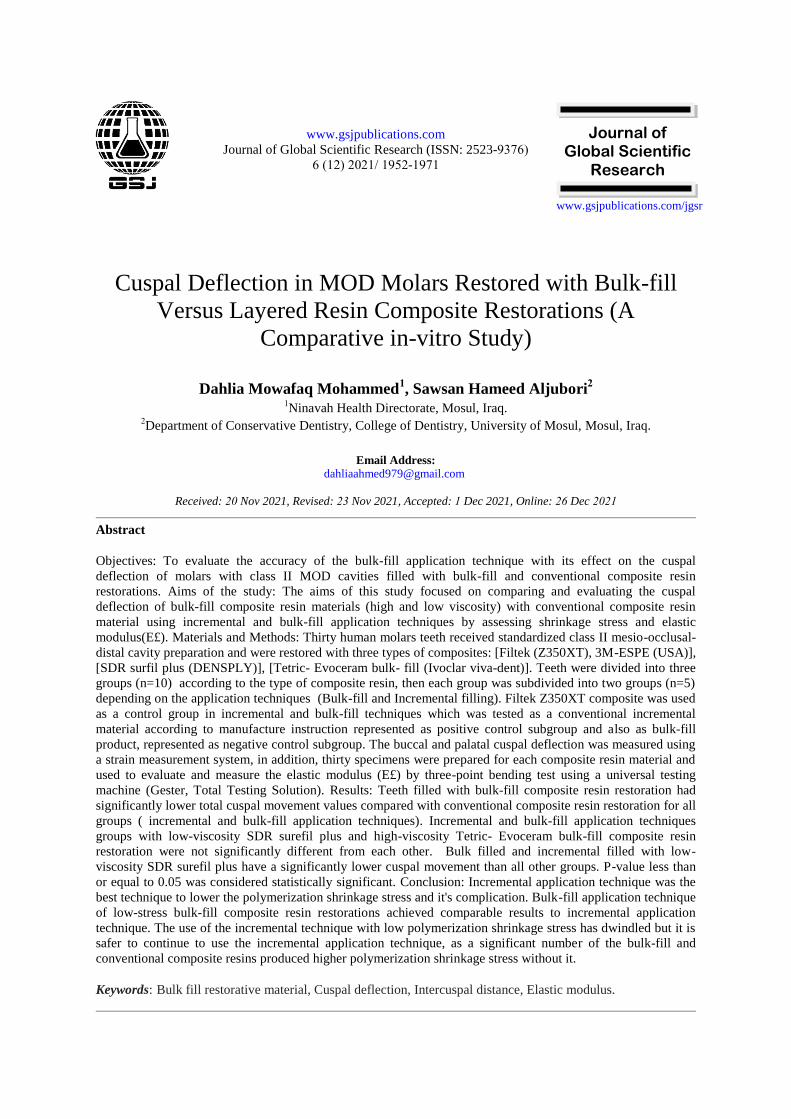
Strain Measurement System
The strain measurement system consists of
a four-channel amplifier circuit
(SunFounder-5V-4-Channel-Relay-
Module,15-20 mA), analog to digital
converter (AD) card (SunFounder AD
analog to Digital Convertermcp3004),
personal computer (Lenovo, L420) with
strain indicator program ( SIProg, Data
loger 4 channel ver.) and strain gauge
sensor, Figure (4) which designed for this
study by the technical engineer Nazar
Ahmed.
A
Figure (4) Strain measurement system: A: Four channel amplifier circuit,
B:Analog to digital converter (AD) card, CPersonal computer, D:Strain
Indicator Program ( SIProg), E: Strain gauge sensor
B C
D E

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1958
The cuspal strain was measured with strain
gauges (PA-06-060CC-350L) with pre-
attached thin copper cables which had
internal electrical resistance of 350Ω, a
gauge factor of 2.00-2.20, gauge grid
dimensions 3.2 x 3.06mm², small size,
mass, easy attachment, high sensitive to
strain, low cost and low sensitive to
temperature and other ambient conditions.
For strain gauge installation, it is important
that the external surface of the test
specimen on which the strain gauge
bonded should be cleaned. To do so, the
strain gauge's bonding site on the external
buccal and lingual surfaces of each tooth
should be carefully sandblasted with
abrasive paper (no 0.320), Figure (5a), the
abraded area should be fin cleaned by
soaking the area with a cloth dampened in
a small amount of acetone, this preparation
aided to obtain a sleekly, shiny surface,
and somewhat large braded area ( 20mm to
30mm) larger than the instillation area,
which provides a careful adaptation of
strain gauge on the tooth contour and
provides more security bonding and
stability during measurement without
interference with the boundaries of the
restoration and impression matrix band.
Two precision strain gauges were bonded
on the decontaminated external surface of
the buccal and lingual cusps of each
unrestored tooth with adhesive (super glue,
INGCO) and polythene sheet onto the
gauge and pressed down with thumb to the
cervical area of the cavity's external walls,
Figure (5b) In addition, to compensate for
any dimensional deviations due to
temperature effects, with the same
procedure two strain gauges were bonded
on the external surface of another tooth
performed with the same cavity dimension
but free from restoration ( acts as a passive
control sample) and connected to the
analog to digital converter card.
The upper portion of buccal and lingual
surfaces of polyvinyl siloxane impression
matrix that was encircled the tooth was
customized without encircling the cervical
portion of buccal and lingual surfaces,
Figure (6a) to avoid hocking the placement
of strain gauge and wrong measurement
due to pre-stress from the impression band,
later the specimens were placed on
specialized 3D printing stage for
standardized the position of the specimen,
Figure (6b).
A B
B
Figure (5): A: Sand- blasted the external surface of
tooth, B: strain gauge were bonded on the external
tooth surface with adhesive.

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1959
The strain gauge constituted two thin lead-
terminals, one-terminal connected to the
full-bridge while the other end had been
connected to the (SI Prog) strain indicator
program. Full bridge wheat stone bridge
circuits, it may be advantageous to make
all four elements of the bridge "active" for
even greater sensitivity (provided that the
change in resistance caused by the applied
force is equal for all four strain gauges).
However, the output voltage is directly
proportional to an applied force.
SI Prog ( Data loger 4 channel ver.) was
fully written in homestead using Matlab
packages. It consists of a Title bar is the
name of this program strain indicator
program. The menu bar from which the SI
Prog is processed by clicking on the start
option also can select other options in this
bar either running or running continuously.
The options panel contains the waveform
chart box and CH1-CH4 boxes from which
the number of operating channels can
select. The measuring information panel
when the scientific name of the material is
inserted in the VISA resource name
cabinet also contains the stop pushbuttons
cabinet. The display area in which the
collecting data appeared as a curve
between the time in minutes and the strain
in the microstrain unit (με).
The strain gauge recorded the data (the
changes in voltage signals) during the
polymerization process then amplified by
recording system, the amplified signals
were transferred using an analog-to-digital
converter (AD) card to a (SI Prog) for
analysis of the measurements that recorded
up to (180s) following the initiation of
light irradiation, no further cuspal recoil of
the buccal and lingual cusp occurred
following 180s post-irradiation, then by
clicking on the stop pushbuttons in the
measuring information panel
corresponding graphs are displayed of the
buccal and lingual cusp area the strain
reading is displayed as a graph
representing the relation between the strain
measurement and corresponding voltage.
The collecting data for both buccal and
lingual cuspal deflection were recorded
and tabulated to a Microsoft Excel ( 2010)
software program.
The collecting data appeared as a curve
between the time in second (sec) and the
strain in the microstrain unit (με). These
readings for the full wheat stone bridge are
directly proportional to the internal cuspal
contraction of the buccal and lingual cusps
of tested specimens. The sum of the buccal
and lingual cuspal contraction or
deflection measurements by microstrain
(με) also was calculated for each
specimen.
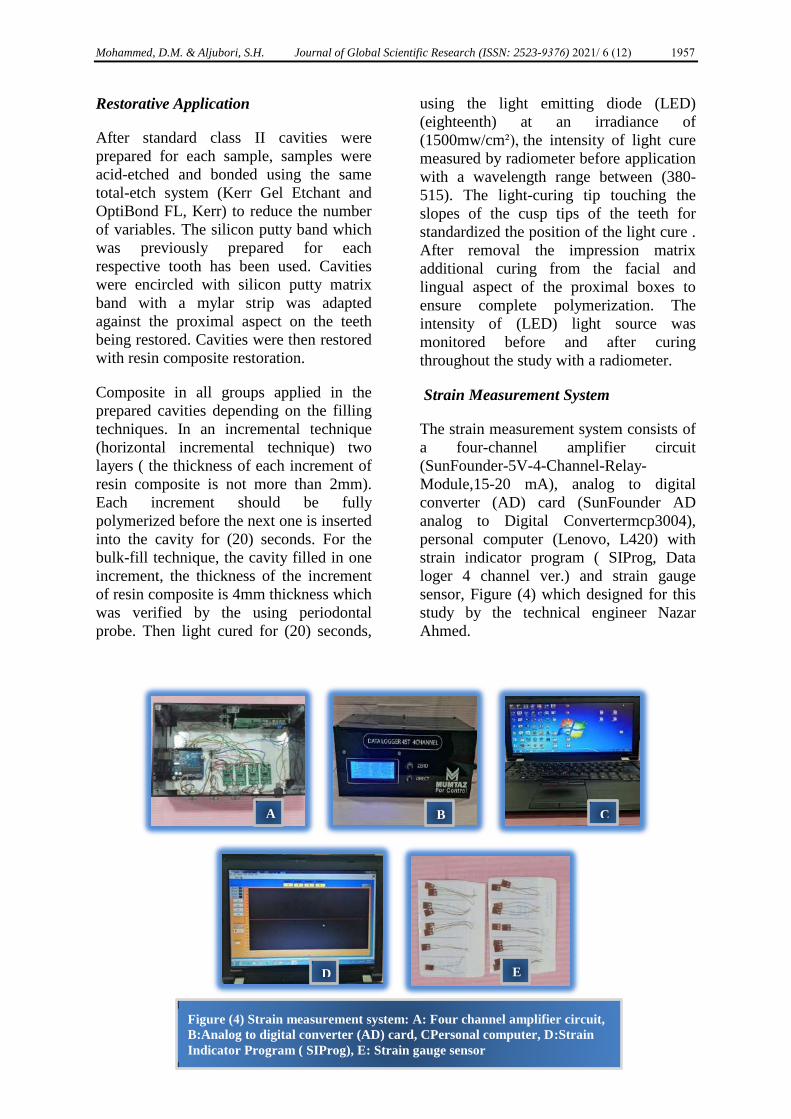
Flexural Modulus (ES)
Composites resin materials were prepared
in a half-spilt stainless-steel mold with
dimension 2.0 (depth) x 2.0 (width) x 25.0
A B
Figure (6): (A) impression matrix was customized without encircle the upper portion of buccal
surface, (B) Specialized 3D printing stage for standardized the position of the specimen.
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1960
(length) mm³, with metallic base, Figure
(7a) For packing of composite into the
mold amylar strip and a glass slid
microscope was used to make a flat
surface of the specimen and prevent the
interfering of oxygen with the most
superior layer of the composite material.
The specimen were then polymerized, the
light curing procedure was performed with
3 overlapping sessions, to cure the entire
length of the specimen with 20 seconds for
each secssion, by LED (eighteenth ) with
light intensity (1500) mw/cm², wave
length of (380-515) nm. This procedure
was repeated on the opposite side after
removal the metallic base.
Ten specimens were prepared for each
group. After light curing, the specimens
were then free from the mold, Figure (7b)
then gently wet-ground (stand paper no
0.320) to remove any accessories or flash.
Specimen's dimensions were measured by
digital caliper to an accuracy of 0.01mm,
measurements were performed at 3 points
for the width, height, and their (average
values were used in the calculation of
bending strength), then transferred to distal
water kept at 37ºC for 24 hours.
The three-point bending fixture was
performed according to ISO No.4049:2009
that consisted of 2 rods (diameter 2mm)
mounted parallel with 20mm between their
center (support span 20mm) the test was
performed immediately after removing the
specimens from the distilled water and
without drying the specimens. For a three-
point flexural test, a rectangular sample of
the resin composite material is supported
at its two ends, in the middle there is no
support but the ends are sturdy a load or
force is applied to the middle section until
the material breaks, or permanently bend
.With a 2mm diameter of the loading
piston and cross-head speed of 0.5
mm/min until failure occured (Universal
testing Machine, Gester, total testing
solution), using a preloaded of 0.5N.
The flexural strength values were recorded
with computer software (ver.1.6.4.9), the
modulus of elasticity (E£) was calculated
from the slope of the linear part of the
diagram of the force-deflection using the
following equation:
E = FL³ / 4BH³d
F: is the maximum load (Newton's), L: is
the distance between the arms
(millimeters), B: is the width of the
samples (millimeters), H: is the height of
the specimen (in millimeters), D: is the
deflection corresponding to the load F.
After collecting the data, the elastic
modulus (E£) have been calculated and
measured in (GPa).
A B
Figure (7): A: stainless-steel mold, B:
specimens were free from the mold.
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1961
Statistical Analysis
The data for this study were collected,
tabulated, and statically analyzed by using
a compatible personal computer with a
statistical package for social. science IBM
SPSS( SPSS for Windows, IBM Corp.,
Version 25) for statistical analysis.
Normality of data distributions and
homogeneity of variance tests was
assessed with Kolmogorov-Smirnov and
Shapiro-Wilk at the significances level of
(P≤ 0.05). All data passed the tests and
was distributed normally, they were
subjected to the parametric statistical
analysis.
Thirty tooth specimens were tested for
cuspal deflection. Cuspal deflection of
each specimen of the same group was
statistically analyzed using paired sample-
t-test for both buccal and lingual cusps
comparison and the independent-sample t-
test for comparison of two application
techniques. One-Way ANOVA Test and
Duncan's Multiple Rane Test for
comparison of the cuspal deflection of
three types of composite materials using
incremental and bulk fill application
technique, Significant differences were
considered when (P≤ 0.05).
Thirty specimens of the testing materials
were prepared for flexural modulus. One-
way ANOVA test and Duncan's Multiple
Rane Test were performed to identify the
significance of the flexural modulus
among composite resin materials groups at
( p≤0.05).
3. Results
Cuspal Deflection Measurements
The behavior of the cuspal deflection of
each specimen of the same group consisted
of summation of both buccal and lingual
cuspal deflection were statistically
analyzed using paired-sample- t-test and
the independent-sample t-test of two
application techniques shown in Table(1),
the results indicated there was a significant
difference between buccal and lingual
cusps, with the lingual cusp has higher
cuspal deflection than the buccal cusp.
The results of the application techniques
for (FiltekZ350XT) there is significant
differences between incremental (control
positive group) and bulk fill (control
negative group) application technique at (P
≤ 0.05), while there are no significant
differences between bulk fill and
incremental application technique for
(Tetric EvoCeram Bulk fill ) and (SDR
Surefill Plus) at (P ≤ 0.05) as shown in.
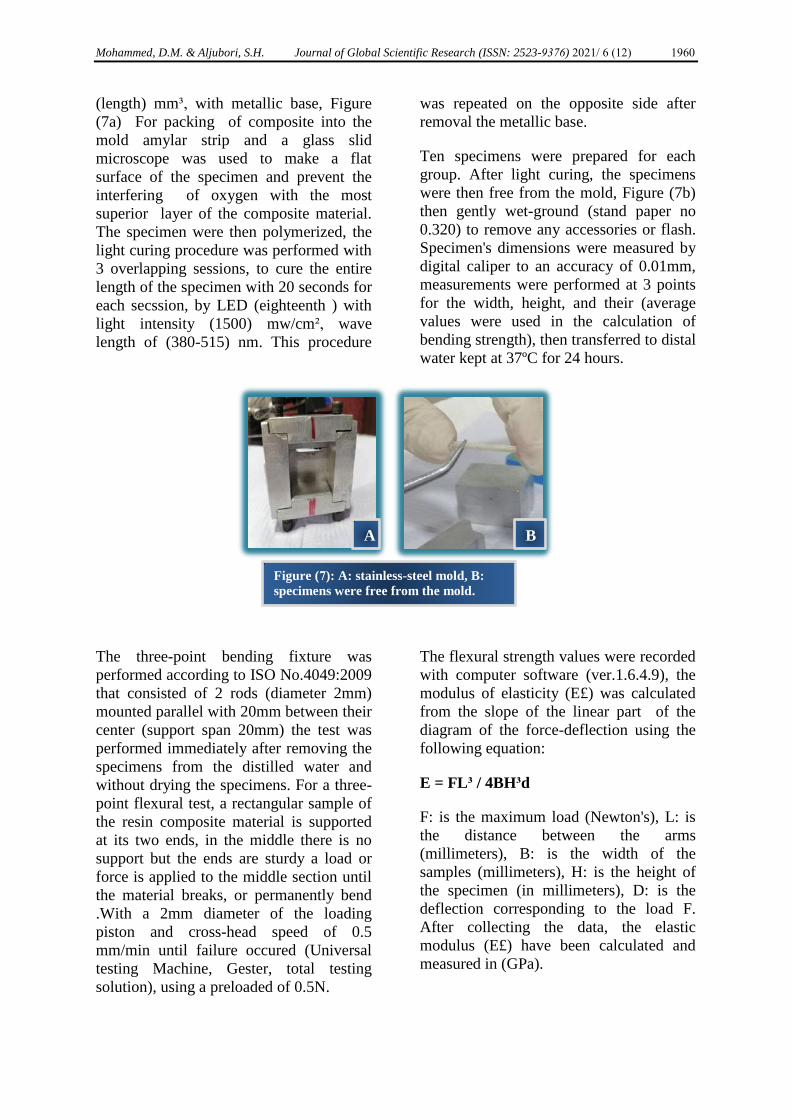
Table (1) Comparison of cuspal deflection
in specimens with bulk fill and
incremental application technique for
conventional and bulk-fill composite
resins.
N: number of specimens; SD: stander of deviation.
Composite Resin
Materials
Application
Techniques
N
Mean(μs) and SD
of Buccal cusp
Mean(μs) and SD
of Lingual cusp Sig.
(2-tailed)
(FiltekZ350XT) Bulk -fill 5 519.52±11.17 564.42±20.21 0.004
Incremental 5 321.16±11.14 367.55±8.23 0.000
Tetric EvoCeram
Bulk fill
Bulk -fill 5 271.68±2.57 328.50±10.69 0.000
Incremental 5 262.34±19.53 328.18±13.20 0.001
SDR Surefill
Plus
Bulk -fill 5 167.10±2.88 272.25±6.14 0.000
Incremental 5 164.34±90 263.85±19.22 0.001
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1962
Table (2) Descriptive statistic of elastic modulus(GPa) for each group.
Composite Resin
Materials
N
Minimum
Median
Maximum
Mean
SD
FiltekZ350XT
10
6.73
8.06
9.54
8.01
0.95
Tetric Evo Ceram
Bulk fill
10
4.88
7.03
7.81
6.61
1.03
SDR Surefill
Plus
10
2.72
3.24
3.63
3.16
0.29
N: number of specimens; SD: stander of deviation.
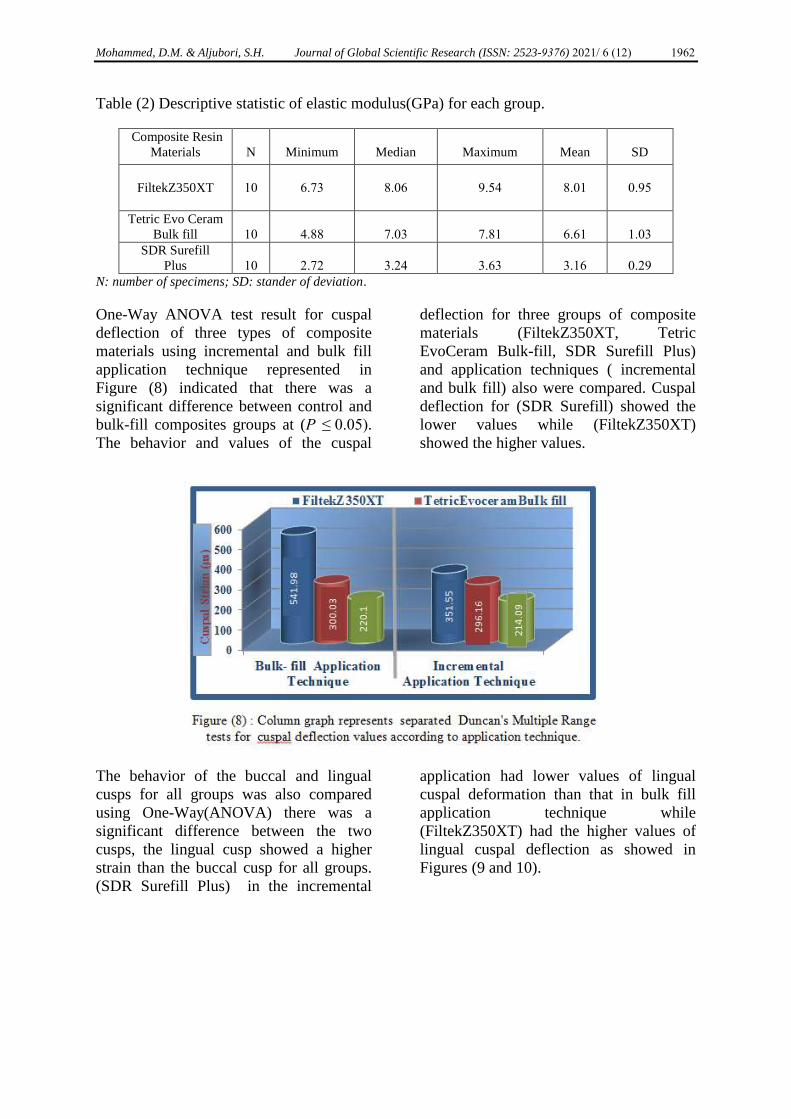
One-Way ANOVA test result for cuspal
deflection of three types of composite
materials using incremental and bulk fill
application technique represented in
Figure (8) indicated that there was a
significant difference between control and
bulk-fill composites groups at (P ≤ 0.05).
The behavior and values of the cuspal
deflection for three groups of composite
materials (FiltekZ350XT, Tetric
EvoCeram Bulk-fill, SDR Surefill Plus)
and application techniques ( incremental
and bulk fill) also were compared. Cuspal
deflection for (SDR Surefill) showed the
lower values while (FiltekZ350XT)
showed the higher values.
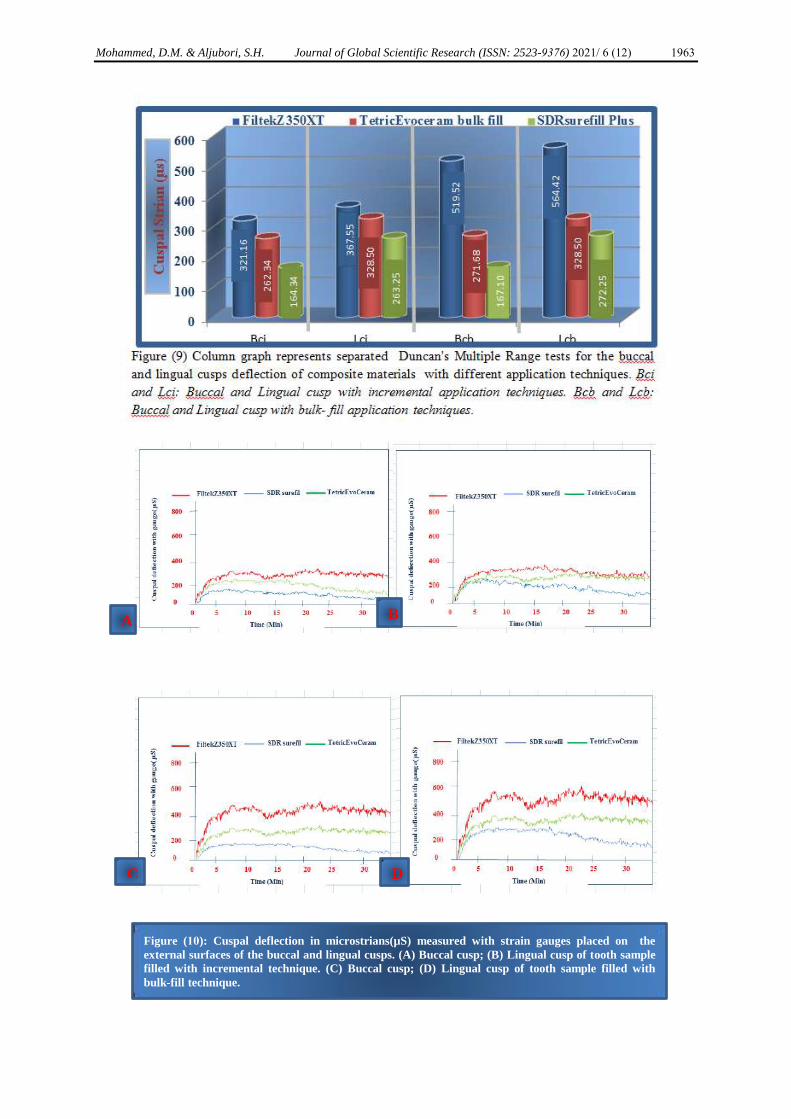
The behavior of the buccal and lingual
cusps for all groups was also compared
using One-Way(ANOVA) there was a
significant difference between the two
cusps, the lingual cusp showed a higher
strain than the buccal cusp for all groups.
(SDR Surefill Plus) in the incremental
application had lower values of lingual
cuspal deformation than that in bulk fill
application technique while
(FiltekZ350XT) had the higher values of
lingual cuspal deflection as showed in
Figures (9 and 10).
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1963
A B
C D
Figure (10): Cuspal deflection in microstrians(µS) measured with strain gauges placed on the
external surfaces of the buccal and lingual cusps. (A) Buccal cusp; (B) Lingual cusp of tooth sample
filled with incremental technique. (C) Buccal cusp; (D) Lingual cusp of tooth sample filled with
bulk-fill technique.
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1964
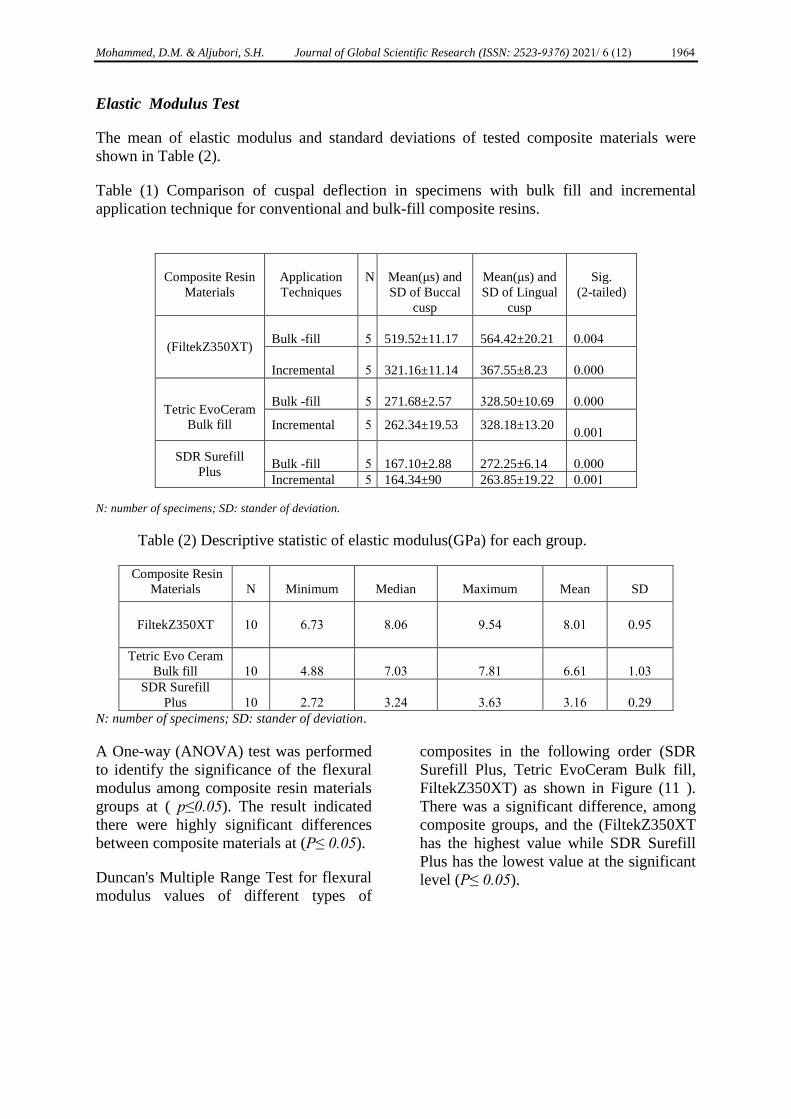
Elastic Modulus Test
The mean of elastic modulus and standard deviations of tested composite materials were
shown in Table (2).
Table (1) Comparison of cuspal deflection in specimens with bulk fill and incremental
application technique for conventional and bulk-fill composite resins.
N: number of specimens; SD: stander of deviation.
Table (2) Descriptive statistic of elastic modulus(GPa) for each group.
Composite Resin
Materials
N
Minimum
Median
Maximum
Mean
SD
FiltekZ350XT
10
6.73
8.06
9.54
8.01
0.95
Tetric Evo Ceram
Bulk fill
10
4.88
7.03
7.81
6.61
1.03
SDR Surefill
Plus
10
2.72
3.24
3.63
3.16
0.29
N: number of specimens; SD: stander of deviation.
A One-way (ANOVA) test was performed
to identify the significance of the flexural
modulus among composite resin materials
groups at ( p≤0.05). The result indicated
there were highly significant differences
between composite materials at (P≤ 0.05).
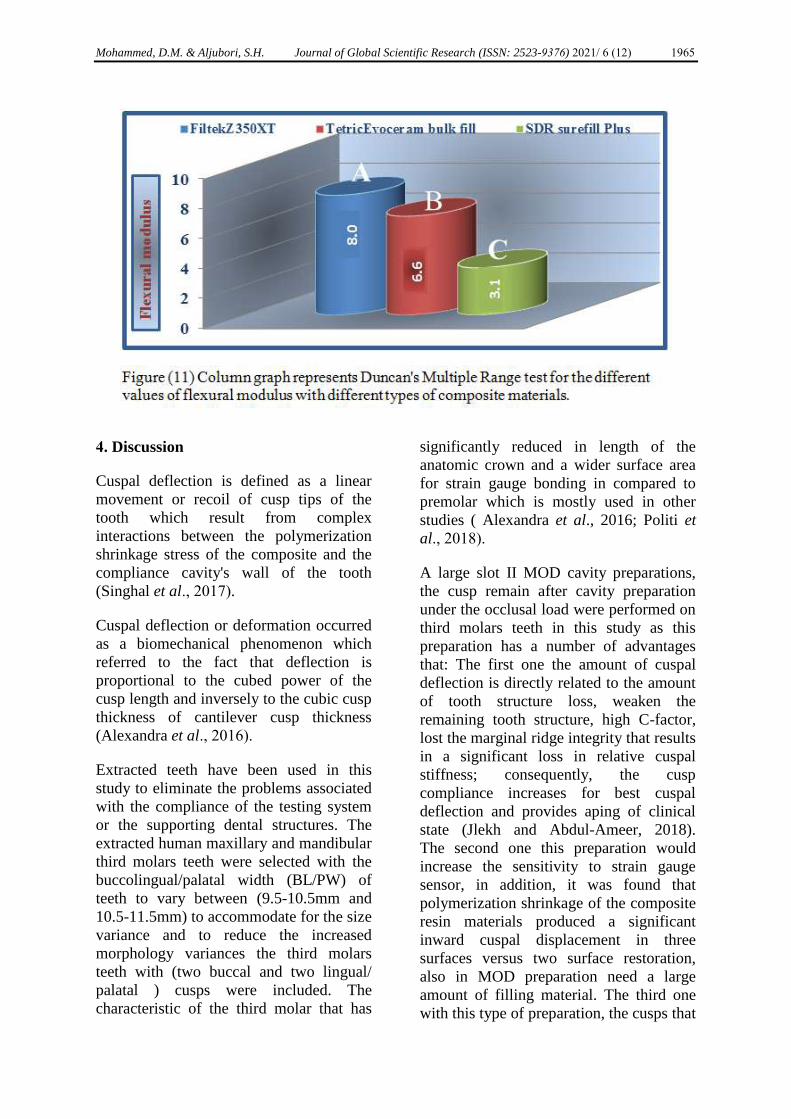
Duncan's Multiple Range Test for flexural
modulus values of different types of
composites in the following order (SDR
Surefill Plus, Tetric EvoCeram Bulk fill,
FiltekZ350XT) as shown in Figure (11 ).
There was a significant difference, among
composite groups, and the (FiltekZ350XT
has the highest value while SDR Surefill
Plus has the lowest value at the significant
level (P≤ 0.05).
Composite Resin
Materials
Application
Techniques
N
Mean(μs) and
SD of Buccal
cusp
Mean(μs) and
SD of Lingual
cusp
Sig.
(2-tailed)
(FiltekZ350XT)
Bulk -fill
5
519.52±11.17
564.42±20.21
0.004
Incremental
5
321.16±11.14
367.55±8.23
0.000
Tetric EvoCeram
Bulk fill
Bulk -fill
5
271.68±2.57
328.50±10.69
0.000
Incremental 5 262.34±19.53 328.18±13.20
0.001
SDR Surefill
Plus
Bulk -fill
5
167.10±2.88
272.25±6.14
0.000
Incremental 5 164.34±90 263.85±19.22 0.001
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1965
4. Discussion
Cuspal deflection is defined as a linear
movement or recoil of cusp tips of the
tooth which result from complex
interactions between the polymerization
shrinkage stress of the composite and the
compliance cavity's wall of the tooth
(Singhal et al., 2017).
Cuspal deflection or deformation occurred
as a biomechanical phenomenon which
referred to the fact that deflection is
proportional to the cubed power of the
cusp length and inversely to the cubic cusp
thickness of cantilever cusp thickness
(Alexandra et al., 2016).
Extracted teeth have been used in this
study to eliminate the problems associated
with the compliance of the testing system
or the supporting dental structures. The
extracted human maxillary and mandibular
third molars teeth were selected with the
buccolingual/palatal width (BL/PW) of
teeth to vary between (9.5-10.5mm and
10.5-11.5mm) to accommodate for the size
variance and to reduce the increased
morphology variances the third molars
teeth with (two buccal and two lingual/
palatal ) cusps were included. The
characteristic of the third molar that has
significantly reduced in length of the
anatomic crown and a wider surface area
for strain gauge bonding in compared to
premolar which is mostly used in other
studies ( Alexandra et al., 2016; Politi et
al., 2018).
A large slot II MOD cavity preparations,
the cusp remain after cavity preparation
under the occlusal load were performed on
third molars teeth in this study as this
preparation has a number of advantages
that: The first one the amount of cuspal
deflection is directly related to the amount
of tooth structure loss, weaken the
remaining tooth structure, high C-factor,
lost the marginal ridge integrity that results
in a significant loss in relative cuspal
stiffness; consequently, the cusp
compliance increases for best cuspal
deflection and provides aping of clinical
state (Jlekh and Abdul-Ameer, 2018).
The second one this preparation would
increase the sensitivity to strain gauge
sensor, in addition, it was found that
polymerization shrinkage of the composite
resin materials produced a significant
inward cuspal displacement in three
surfaces versus two surface restoration,
also in MOD preparation need a large
amount of filling material. The third one
with this type of preparation, the cusps that

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1966
remain after cavity preparation were
reported to act under the occlusal load as a
cantilever beam, which increases the depth
of the prepared cavity, while the prepared
cavity floor acts for cusp bending as a
fulcrum.
The factors influencing the stress
formation included: polymerization
shrinkage stress, the elastic modulus of the
composite resins, C-factors of the restored
cavity, the curing mode, and the type of
the dentin adhesive system. In this study,
the size and the shape of the cavity, curing
mode, and the dentin adhesive system was
standardized for all specimens.
The main variables causing the difference
between the cuspal deflection values of
conventional composite and bulk-fill
composites may be due to two factors of a
combination thereof. The first factor was
materials' chemical composition of the
different groups of composites
(conventional and bulk-fill composites)
and the second factor was the type of
application technique: Incremental (two
layers and two sessions of light-curing)
Bulk-fill (one layer and one session of
light-curing) application techniques
(Elsharkasi et al., 2018; Oliveria et al.,
2018).
The matrix band placement on teeth
prepared with MOD cavities may cause
cuspal bending and pre-stress the tooth
prior to polymerization of composite
restoration (Mohammed and Nashaat,
2018) therefore in this study impression
matrix band with modification on the
buccal and lingual surface has been used
during the restorative procedure to prevent
the interference with the adaptation of
strain gauge sensor.
After the tooth restoration, the initial
period of negative cuspal deflection is
critical value because during this period
occlusal contact is normally adapted,
which could cause a greater tendency to
tooth fracture till a period of relaxation
reaches (Gonzalez-Lopez et al., 2006 a).
The result of this study showed that after
completing the restorative procedure an
inward cuspal deflection for all groups this
deflection was continued for several
minutes( at time intervals of 0.5 min to 3
min) and there is no further cuspal
movement for both cusps occurred after 3
min or (180s) post-irradiation this result
can be explained: inward cuspal
deflection, might be attributed to the
amount of the remaining free radicals,
double bonds in the resin base composite
restoration which persisted to react after
the polymerization reaction process
consequence, the polymerization stress
developed and causes inward recoil of
both cusps (McHugh et al., 2017;
Elsharkasi et al., 2018; Jlekh et al., 2018).
The present study compared the influence
of application technique ( incremental and
bulk-fill) on the mean of cusp deflection
for conventional and bulk-fill ( high and
low viscosity) composites resin. The
results showed that in (Filtek ZX50XT)
groups there is a significant difference (p ≤
0.05) between incremental and bulk-fill
techniques, the incremental technique
show less cuspal deflection compared with
bulk-fill technique, and this could explain
as a recommended maximum depth of cure
is about 2mm for each incremental layered
of composites resin materials. Therefore,
in the bulk-fill technique, the depth of
polymerization might not be totally
completed causes internal stress to be
developed within the structure of the
material as well as more cuspal recoil, so
the clinical application of the conventional
composite with bulk-fill technique may not
be applicable, the bulk-fill technique with
conventional composite not recommended
for clinical use, these findings are in
agreement with (Park et al., 2008) reported
that when the conventional composite used
in both incremental and bulk-fill
application techniques, the increment

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1967
technique was shown considerably lower
cuspal deflection than that for bulk-fill
technique implying that the bulk-filling
technique led to significant more cuspal
deflection than did the incremental filling
technique with no significant differences
between oblique and horizontal layered
techniques.
On the other hand for (Tetric Evo Ceram
Bulk-fill) and (SDR surefill Plus) groups,
there was no significant difference (p
≥0.05) between the mean of cuspal
deflection for both incremental and bulk-
fill application techniques, this could be
explained as the bulk-fill composite resin
that used in this study according to the
level of polymerization shrinkage stress
can be classified into: low-viscosity bulk-
fill with low stress (SDR surefill Plus) and
high-viscosity bulk-fill with low stress
(Tetric Evo Ceram Bulk-fill).
(SDR surefill Plus) is based on "Stress
Decrease Resin" technology, which means
that in the backbone of the polymerizable
resin a substance that is chemically
embedded known as a "polymerization
modulator" has an appositive effect in
lowering the development elasticity
modulus, allowing for the reduction in the
polymerization stress without any negative
effect in the rate of the polymerization
reaction and the degree of conversion and
this effect occurred as a result of the
synergistically interacts between the
polymerization modulator and the
camphoroquinone photo-initiator (Patel et
al., 2016; Al-Bargash et al., 2017;
Tsujimoto et al., 2020).
Tetric Evo Ceram Bulk-fill composites
resin is known to have filler within the
matrix of the composite resin, which is
partially functionalized by silane known
a special stress reliever״ allowing reliable
polymerization and depth of cure at 4mm
depth for posterior restoration, in addition,
to di-benzoyl germanium which a newly
patented light initiator. Furthermore, this
bulk-fill composite contains ″Ivocerin״
which provide a high absorption
coefficient and consequence increase the
efficiency of the quantum, Ivocerin also
characterized by high reactivity to the light
provide rapid polymerization reaction with
lead an increase in the depth of cure (Patel
et al., 2016; Al-Bargash et al., 2017;
Tsujimoto et al., 2020).
Although the difference in the viscosity of
the two bulk-fill between low-viscosity
and high-viscosity bulk-fill composite
resin but both materials have low stress. In
this study, the incremental application
technique doesn't appear to offer any
advantages over the bulk fill application
technique for both (SDR surefill Plus)
(Tetric Evo Ceram Bulk-fill composites
resin). Thus in the low-stress bulk-fill
resins, the effect of the incremental
technique on the polymerization stress has
a minimal influence and the advance in the
chemical composition of the composite
resin materials are more important in
reducing the generated polymerization
shrinkage stress than the choice of the type
of the application technique this result was
supported by ( Shimatani et al., 2018)
which suggests that the cuspal deflection
of the composites resin materials is
primarily influenced by materials
chemical composition rather than the
application filling technique.
This result also came in agreement with (
Meeries et al., 2018) provided a systemic
review of polymerization shrinkage stress
of resin composites which found that
modification of composite resin matrix had
the largest redounding on minimizing
stress development and also this result
came in agreement with the study carried
by (Műnchow et al., 2018) showed in
those reviews, the technique protocols for
application of composite resin materials no
longer impacted with a great contribution
to polymerization shrinkage stress and the
consequence complication associated with
cuspal deflection and had fewer influences

Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1968
than light-curing method. On the other
hand to minimize the development of the
polymerization shrinkage the amending in
the resin matrix made the largest effects.
Also, this result came in agreement with
(Tsujimoto et al., 2020) which concluded
that the cuspal deflection of some high and
low-viscosity bulk-fill resin was
significantly reduced by using incremental
techniques, however, the resultant
improvement of incremental techniques
was not applicable to all the bulk-fill
resins, so the effect of incremental
techniques on polymerization shrinkage
stress of low-and high bulk-fill resins was
material predicated. Thus, the use of the
incremental technique with low
polymerization shrinkage stress has
dwindled but it is safer to continue to use
the incremental application technique, as a
significant number of the bulk-fill and
conventional composite resins produced
higher polymerization shrinkage stress
without it.
The lingual cusps had higher cuspal
deflection than buccal cusps for all
experimental groups. This can be
explained by that the amount of cuspal
deflection being influenced by the amount
of remaining tooth structure. The cervical
areas of third molars narrower lingually,
and less amount of the remaining tooth
structure than they did buccally, and, thus,
the less stiff could be expected of the
lingual cusps than the buccal cusps this
result came in agreement with (Bicalho et
al., 2014) found that when cuspal
deflection measured with strain gauge
sensor validated the finite element analysis
on the third molars the lingual cusps had a
significant higher cuspal deflection in
compared to the buccal cusp also reported
that the negative effect of the residual
polymerization shrinkage stress can
minimize through the combination of the
low-post-gel shrinkage composite resins
and incremental application techniques
that provides appropriately polymerized
the restoration, but without increasing in
the number of increment, with the
thickness of increment layer that is large
enough but not exceeding 2mm.
Moreover, the effect of the filling
techniques ( incremental and bulk-fill) was
proved by measuring the flexural modulus
of the tested composite resin materials.
The ( SDR surefil Plus) has the lowest
elastic modulus values, in (Tetric Evo
Ceram Bulk-fill) the moderate elastic
modulus and the highest elastic modulus in
( Filtek Z350XT). During the
polymerization process, the elastic
modulus of the material plays an important
role in the generation of polymerization
stress, it was found that the viscosity of the
resin base materials increase during the
polymerization reaction with the formation
of bonded cross-linked network
accompanied by a rapid increase in the
material rigidity, while the volumetric
changes of the materials occurred it was
restricted with the perimeter of the
surrounding tooth structure lead to
increase the stress in the internal structure
of the material (Shebl et al., 2018).
According to the present study the bulk-fill
composite resin has shown less
polymerization shrinkage stress than the
conventional composite resin, with ( SDR
surefil Plus) has the lowest cuspal
deflection and (FiltekZ350XT) the highest
cuspal deflection, the possible explanation
for the positive result of SDR surefill Plus
may be despite its contain a lower filler
volume with higher polymerization
contraction values, but the resin matrix
contains high molecular weight
polymerization modulators, with greater
flexibility of the urethane modulators
groups lead to more uniform network
formation with a delay in the rate of
contraction reaction which allows to
compensate the effect of the
polymerization contraction and result in
low stress. The low elastic modulus and
the low stress generated have a synergetic
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1969
effect in reducing the amount of cuspal
deflection. Conversely, (Tetric Evo Ceram
Bulk-fill) which shows moderate values
for the elastic modulus, though having a
high filler content, the Tetric Evo Ceram
Bulk-fill contains pre-polymerized fillers
(with a modulus of elasticity 10MPa) that
are included in the total filler amount
consequently lower fraction of inorganic
filler thus their effect increases the elastic
modulus is concordantly lower, these
fillers act as a ″shrinkage stress reliever"
improved the elasticity of the material
through keeping a chemical cushion
between the coarse filler particles.
FiltekZX350 showed higher stress because
of higher elastic modulus and higher post-
gel shrinkage (Ilie et al., 2013; Kim et al.,
2015). This finding came in agreement
with (Braga et al., 2018) that indicated the
composite resin materials with high elastic
modulus values and the polymerization
shrinkage restricted by bonding to the
cavity walls, deformed less when they are
stressed, and produced more rigid
restoration will result in higher shrinkage
stress.
As ( SDR surefil Plus) produced lower t
modulus of elasticity compared to (Tetric
Evo Ceram Bulk-fill), so the cuspal
deflection was lower due to
polymerization stress that generated by (
SDR sure fil Plus) is lower than (Tetric
Evo Ceram Bulk-fill) this could be
explained by the resin composite with a
higher elastic modulus has limited flow
generate higher polymerization stress. This
result came in conformed with (Olafsson
et al., 2017 and Jlekh and Abdul-Ameer,
2018 ) reported that the incrementally
placed conventional composite resin
resulted in greater cuspal deflection when
compared with bulk-fill resin-based
material and the amount of cuspal
deflection in the bulk-fill resin-based
material, depends on the type of composite
resin material, the lower cuspal deflection
attribute to that the new bulk-fill
composite resins are produced lower
polymerization shrinkage stress than those
of conventional composite resins through
the incorporation of "stress-reliever" to
change the dynamic of the polymerization
reaction using either; novel chemistry,
increase filler loading, decrease resin
matrix.
5. Conclusion
Bulk fill composite resin of all
groups (incremental and bulk-fill
application techniques) have shown
less cuspal deflection than the
conventional composite resin, with (
SDR surefill Plus, low viscosity
bulk-fill) having the lowest cuspal
deflection and (FiltekZ350XT) the
highest cuspal that generated by
polymerization shrinkage stress.
Although the incremental application
technique decreased the
polymerization shrinkage stress and
it's a complication associated with
cuspal deflection better than the
bulk-fill application technique in
comparing between the control
groups (conventional composite resin
material) but doesn't appear to offer
any advantages over bulk-fill
technique for both low stress (SDR
surefil Plus) and (Tetric Evo Ceram
Bulk-fill composites resin) bulk-fill
composite resin.
The result of the present study cuspal
deflection is primarily influenced by
materials' chemical composition and
properties rather than the type of the
application technique.
It is preferable always to use the
incremental application technique. A
significant number of composite
resins produced higher
polymerization shrinkage stress.
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1970
6. References
[1]. Kalliecharan, E., Keskin, B., and Inan, U.
(2016). Three-years clinical evolution of
class II posterior composite placed with
different application techniques and
flowable composite linings in
endodontically treated teeth. Clin Oral
Invest.21(2): 709-16.
[2]. Ricci, W., Alfona, P., Pamato, S., Cruz, C.,
and Pereira, J. (2019). Mechanical
degradation of different classes of composite
resins in water, air and oil. Bio. Med. Res
Inter. 19: 1-7.
[3]. Deliperi, S., and Bardwell, D. (2002). An
alternative method to reduce polymerization
shrinkage in direct posterior composite
restorations. J Am Dent Assoc. 133(10):
1387- 1398.
[4]. Chandrasekhar, V., Rudrapati, L., and
Tummala, M. (2017). Incremental
techniques in direct composite restoration. J
of Conserve Dent. 20(6):386-391.
[5]. Giachetti, L., Scaminaci, R., Bambi, C., and
Grandini, R. (2006). A review of
polymerization shrinkage stress: Current
techniques for posterior direct resin
restorations. J Contemp Dent Pract. 7:79–
88.
[6]. Menees, T., Lin, C., Kojic, D., Burgess, J.,
and Lawson, N. (2015). Depth of cure of
bulk fill composites with monowave and
polywave curing lights. Am J Dent.
28(6):357-361.
[7]. Lee, M., Cho, B., Son, H., Um, C., and Lee,
I. (2007). Influence of the cavity dimension
and restoration methods on the cusp
deflection of premolars in composite
restoration. Dent Mater. 23(3): 288-95.
[8]. Hamama, H., Zaghloul, N., Abonelatta, O.,
and El-Embaby, A. (2011). Determining the
influence of flowable composite Resin
application on cuspal deflection using a
computerized Modification of the strain
gauge method. The Amer J of Esth Dent.
1(1): 48-59.
[9]. Oskoee, S., Oskoee, O., Siavash, S.,
Nanimipour, E. (2012). The effect of
composite fiber insertion along with low
shrinking composite resin on cuspal
deflection of root-filled maxillary premolars.
J of Contemp Dent Pra.13(5): 20-12.
[10]. Oliveria, K., Consani, S., Goncalves, L.,
Brandt, W., and Ccahuana-Vasquez, R.
(2012). Photoelastic evaluation of the effect
of composite formulation on polymerization
shrinkage stress. Braz Oral Res. 26(3): 202-
208.
[11]. Kim, Y., Kim, R., Ferracane, J., and Lee, I.
(2016). Influence of the compliance and
layering method on the wall deflection of
simulated cavities in bulk-fill composite
restoration. Oper Dent. 41(6): 183-194.
[12]. McCullock, A., and Smith, B. (1986). "in
vitro studies of cuspal movement produced
by adhesive restorative materials". British
Dent.161(11): 405-409.
[13]. Campodonico, C., Tantbirojn, D., Olin, P,.
and Versluis, A. (2011). Cuspal deflection
and depth of cure in resin-based composite
restorations filled by using bulk, incremental
and tooth-illumination techniques. J Am
Dent Assoc.142(10): 1176-82.
[14]. Karaman, E., and Ozgunaltay, G. (2013).
Cuspal deflection in premolar teeth restored
using current composite resins with and
without resin modified glass ionomer liner.
Oper Dent. 38(2) :282-289.
[15]. Moorthy, A., Hogg, C., Dowling, A.,
Grufferty, B., Benetti, A., and Fleming, G.
(2012). Cuspal deflection and microleakage
in premolar teeth restored with bulk-fill
flowable resin-based composite base
materials. J of Dent. 40(6): 500-505.
[16]. Kweon, H., Ferracane, J., Kang, K., Dhont,
J., and Lee, I.B. (2012). Effect of layering
methods, composite type and flowable liner
on the polymerization shrinkage stress of
light cured composites. Dent Mater. 28(7):
801-809.
[17]. Palin, W., Fleming, G., Nathwani, H.,
Burker, F., and Randall, R. (2005). In vitro
cuspal deflection and micro-leakage of
maxillary premolars restored with novel
low-shrink dental composites. Dent. Mater.
21(4): 324-335.
[18]. Faisal, M., and Nashaat, M. (2018). Cuspal
deflection of Bulk-fill versus layered Resin
composite Restorations. IOSR J of Dent
Med Scie. 17(4): 26-32.
[19]. Shebl, S., Abdel-Karim, U., Abdalla, A.,
and Elkafrawy, H. (2018). Shrinkage stress
of High and low viscosity bulk-fill
composites with incremental and bulk-fill
techniques. Tanta Dent J. 15(4): 224-233.
[20]. Rocha, M., Liliana, G., Joȁo, M., and Maria,
P. (2013). Cuspal deflection od directly and
indirectly restorated teeth. Braz Dent Sci.
16(4): 34-40.
[21]. Singhal, S., Gurtu, A., Singhal, A., Bansal,
R., Mohan, S. (2017)."Effect of different
composite restorations on the cuspal
deflection of premolar restored with
different insertion techniques-An in vitro
study. J of clin and diagn Res. 11(8): 67-70.
[22]. Alexandra, V., Joao, R., Sofa, A., Ana, M.,
Nelia, A., and Rogerio, N. (2016). Cuspal
Displacement Induced by Bulk Fill Resin
Composite Polymerization: Biomechanical
Mohammed, D.M. & Aljubori, S.H. Journal of Global Scientific Research (ISSN: 2523-9376) 2021/ 6 (12) 1971
Evaluation Using Fiber Bragg Grating
Sensors. Inter J of BioMater. (9): 7134283.
[23]. Politil, I., Mchugh, L., AL-fodeh, R.,
Fleming, G. (2018). Modification of the
restoration protocol for resin- based
composite(RBC) restoratives (conventional
and bulk-fill) on cuspal movement and
microleakage score in molar teeth. Dent
Mater. 33: 329-335.
[24]. Elsharkasi, M., Platt, J., Cook, N., Yassen,
G., and Matis, B. (2018). Cuspal deflection
in premolar teeth restored with bulk-fill
resin-based composite materials. Oper Dent.
43(1) :1-9.
[25]. Oliveria, L., Braga, S., Bicalho, A., Ribeiro,
M., Price, R., and Soares, C. (2018). Molar
cusp deformation evaluated by micro-CT
and enamel crack formation to compare
incremental and bulk-filling techniques. J of
Dent. 74(19): 71-78.
[26]. Gonzalez-Lopez, S., Sanz Chinesta, M.,
Ceballos, G., de Haro, G., and Gonzalez-
Rodiguez, M. (2006a). Influence of cavity
type and size of composite restorations on
cuspal flexure. Med oral patol Oral Cir
Bucal. 11(6) 536-540. [27]. McHugh, L., Politi, I., Al-Fodeh, R., and
Fleming, G. (2017). Implications of resin-
based composite restoration on cuspal
deflection and microleakage score in molar
teeth: placement protocol and restorative
material. Dent Mater. 33: 329-335.
[28]. Jlekh, Z., and Abdul-Ameer, M. (2018).
Evaluation of the cuspal deflection of
premolars restored with different types of
bulk-fill composite Restorations (A
comparative in vitro study. Biomed and
Pharmacal J. 11(2): 751-757.
[29]. Park, J., Chang, J., Ferracane, J., and Lee, I.
(2008). How should composite be layered to
reduce shrinkage stress: incremental or
bulk-filling?. Dent Mater 24(11): 1501-1505.
[30]. Patel, P., Shah, M., Agrawal, N., Desia, P.,
Tailorm, K., and Patel, K. (2016).
Comparative evaluation of micro leakage of
class II cavities restored with different bulk-
fill composite restorative systems: An in
vitro study. J Res Adv Dent. 5:52-62.
[31]. Al-Bargash, A., Al-Omari, A., Naseem, M.,
Abduljabbar, T., and Vohra, F. (2017).
Influence of the placement techniques on the
micro leakage of class II composite
restorations. BioMater and Tissue En. 7:1-7.
[32]. Tsujimoto, A., Jurado, C., Barkmeier, W.,
Sayed, M., Takamizawa, T., Latta, M.,
Miyazaki, M., and Garcia-Godoy, F. (2020).
Effect of layering on polymerization
shrinkage stress of high-and low-viscosity
Bulk-fill Resins. Oper Dent. 45(6): 655-663.
[33]. Shimatani, Y., Tsujimoto, A., Barkmeier,
W., Fischer, N., Nagura, Y., Takamizawa,
T., Latta, M., and Miyazaki, M. (2018).
Simulated cuspal deflection and flexural
properties of Bulk-Fill and conventional
flowable Resin composites. Oper Dent. 45
(5): 537–546.
[34]. Meereis, C., Munchow, E., deOliveira
daRosa, W., daSilva, A., and Piva, E.
(2018). Polymerization shrinkage stress of
resin-based dental materials: a systematic
review and meta-analyses of composition
strategies. J of the Mechan Behavior of
BioMed Mater. 82(36): 268-281.
[35]. Munchow, E., Meereis, C., deOliveira
daRosa, W., daSilva, A., and Piva, E.
(2018). Polymerization shrinkage stress of
resin-based dental materials: A systematic
review and meta-analyses of technique
protocol and photo-activation strategies. J
of the Mechan behavior of BioMed Mater.
82:77-86.
[36]. Bicalho, A., Pereira, R., Zanatta, R., Franco,
S., Tantbirojn, D., Versluis, A., and Soares,
C. (2014a) Incremental filling technique and
composite material-part I: cuspal
deformation, Bond strength, and physical
properties. Oper Dent. 39(2): 71-82.
[37]. Ilie, N., Bucuta, S., and Draenert, M. (2013).
Bulk-fill resin-based composites: An in vitro
assessment of their mechanical
performance. Oper Dent. 38(6): 618-625.
[38]. Kim, R., Kim, Y., Choi, N., and Lee, I.
(2015). Polymerization shrinkage, modulus
and shrinkage stress related to tooth-
restoration interfacial debonding in bulk-fill
composites. J of Dent. 43(4): 430-439.
[39]. Braga, S., Oliveira, L., Rodrigues, R.,
Bicalho, A., and Novais, V. (2018). The
effect of cavity preparation and composite
resin on bond strength and stress
distribution using the Micro tensile Bond
Test. Oper Dent. 43(1):81-89.
[40]. Olafsson, J., Vilhelm, G., and Elsharkasi, M.
(2017). Effect of composite type and
placement technique on cuspal strain .J of
Esth and Rest Dent.30(1): 30-38.
[41]. Ahmed, D. K., Al-jabar, M. A. (2021).
Effect of Different Storage Temperatures
and LED Light Curing Units on Color
Stability of Bulk Fill Composite Resin; an in
Vitro Study. Journal of Global Scientific
Research. 6 (4): 1285-1296.