contents contents contents - acem
TRANSCRIPT
|
Newsletter of the International Emergency Medicine Special Interest Group of ACEM
Contents
Editorial 2From the Editor Chris Curry 2
Message from the IEMSIG Chair Gerard O’Reilly 2International Scholarship Award 4International Development Fund 4New Website 4Accredited Training Time for Trainees in 2013 4International EM Opportunities 4Events 5IEMSIG ACEM Staff 5
Myanmar: EM development at Yangon General Hospital –Preparing for the South East Asian Games Dr Pa Pa 8Nepal: A New Training Program at BPKIHS - the development of a Fellowship in Emergency Medicine Gyanendra Malla 11Solomon Islands: Emergency Medicine in Solomon Islands Trina Sale 13
Fiji: EM Specialty Development Anne Creaton 17
Nursing Capacity Building for Emergency Care in PNG Georgina Phillips 23Emergency Medicine in Vanuatu: The View From Afar Brady Tassicker 25
Timor Leste Antony Chenhall 30Emergency care in Vietnam: The Alfred-Hue Emergency Care Partnership Project Gerard O’Reilly & Sally Chalton 31
Asia 32Bangladesh: A Glimpse of EM Reza Ali 32India: Emergency Medicine: Are We There Yet? Pankaj Arora & Anita Bhavnani 35Mongolia Simon Smith 40EM at B.P. Koirala Institute of Health Sciences, Dharan, Nepal Ros Taylor 41A Mountain to Climb – 11 Weeks in Nepal Brian O’Connell 42Progress for EM in Nepal Jennifer Rush 45
Sri Lanka Shane Curra
IEMSIG
IEMSIG
IEMSIG
Contents
Newsletter of the International Emergency Medicine Special Interest Group of
Newsletter of the International Emergency Medicine Special Interest Group of
ACEMNewsletter of the International Emergency Medicine Special Interest Group of
Accredited Training Time for Trainees in 2013New WebsiteInternational Development FundInternational Scholarship AwardMessage from the IEMSIG Chair
From the EditorEditorialACEM NEWS
Accredited Training Time for Trainees in 2013
International Development FundInternational Scholarship AwardMessage from the IEMSIG Chair
Gerard O’Reilly Chris Curry
4442222
for the South East Asian GamesMyanmar: EM development at Yangon General Hospital –Preparing
IEMSIG ACEM StaffEventsInternational EM OpportunitiesAccredited Training Time for Trainees in 2013
for the South East Asian GamesMyanmar: EM development at Yangon General Hospital –Preparing
IEMSIG ACEM Staff
International EM OpportunitiesAccredited Training Time for Trainees in 2013
Myanmar: EM development at Yangon General Hospital –Preparing
Accredited Training Time for Trainees in 2013
Dr Pa Pa
8
5544
Emergency Medicine in Vanuatu: The View From AfarNursing Capacity Building for Emergency Care in PNG
Fiji: EM Specialty Development
Solomon Islands: Emergency Medicine in Solomon IslandsFellowship in Emergency MedicineNepal: A New Training Program at BPKIHS - the development of a
Emergency Medicine in Vanuatu: The View From AfarNursing Capacity Building for Emergency Care in PNG
Fiji: EM Specialty Development
Solomon Islands: Emergency Medicine in Solomon IslandsFellowship in Emergency MedicineNepal: A New Training Program at BPKIHS - the development of a
Emergency Medicine in Vanuatu: The View From AfarNursing Capacity Building for Emergency Care in PNG
Solomon Islands: Emergency Medicine in Solomon Islands
Nepal: A New Training Program at BPKIHS - the development of a
Brady Tassicker Georgina Phillips
Anne Creaton
Trina Sale Gyanendra Malla
2523
17
1311
India: Emergency Medicine: Are We There Yet?Bangladesh: A Glimpse of EMAsia
Care Partnership ProjectEmergency care in Vietnam: The Alfred-Hue Emergency Timor Leste
India: Emergency Medicine: Are We There Yet?Bangladesh: A Glimpse of EM
Care Partnership ProjectEmergency care in Vietnam: The Alfred-Hue Emergency
India: Emergency Medicine: Are We There Yet?
Emergency care in Vietnam: The Alfred-Hue Emergency
Pankaj Arora & Anita Bhavnani Reza Ali
Gerard O’Reilly & Sally Chalton
Antony Chenhall
35Pankaj Arora & Anita Bhavnani 323231Gerard O’Reilly & Sally Chalton
30
Sri Lanka
Progress for EM in NepalA Mountain to Climb – 11 Weeks in NepalEM at B.P. Koirala Institute of Health Sciences, Dharan, NepalMongoliaIndia: Emergency Medicine: Are We There Yet?
Progress for EM in NepalA Mountain to Climb – 11 Weeks in NepalEM at B.P. Koirala Institute of Health Sciences, Dharan, Nepal
India: Emergency Medicine: Are We There Yet?
EM at B.P. Koirala Institute of Health Sciences, Dharan, Nepal
India: Emergency Medicine: Are We There Yet?
Shane Curra
Jennifer Rush Brian O’Connell Ros Taylor Simon Smith Pankaj Arora & Anita Bhavnani
4542414035Pankaj Arora & Anita Bhavnani
ContentsEDITORIAL
From the Editor Chris Curry 2Message from the IEMSIG Chair Gerard O’Reilly 2
INTERNATIONAL SCHOLARS’ PRESENTATIONS AT THE ACEM ASMMyanmar: Opening up doors – The first year of the new ED at YGH – challenges and successes. Rose Skalicky-Klein, Win Kyaw 4Myanmar: After the Games are over – The development of an ED at Nay Pyi Taw 1000 bedded Hospital Than Latt Aung 6Nepal graduates their first emergency medicine specialists Ramesh Maharjan 7PNG: Leading emergency medicine in Madang Province Taita Kila 7Vietnam: Emergency medicine development at Cho Ray Hospital, Ho Chi Minh City TônThanhTra,PhamThiNgocThao 9
PACIFICELS in the Pacific Andrew Bezzina 12Fiji – Perspectives on building an EM training program Anne Creaton 13PNG – Update on emergency medicine in Papua New Guinea Colin Banks 15Vanuatu – Wins for emergency medicine in Vanuatu Brady Tassicker 16
SOUTH EAST ASIAIndonesia – Bali and Lombok: the Methanol Education Program Di Brown 18Myanmar – Royal Children’s Hospital in Melbourne supports Myanmar Simon Young 20Thailand – Emergency Medicine update Jonathan Knott 21Timor Leste – An update from Dili Antony Chenhall 22Vietnam – The Alfred-Hue Emergency Care Partnership Project Gerard O’Reilly 23
ASIA and MIDDLE EASTMongolia – The Initial Emergency Care Program Simon Smith 24Nepal – Australian and New Zealand EPs support the first specialists Chris Curry 24India – EM training in India: Public and Private Pankaj Arora, Anita Bhavnani 25Sri Lanka – EM in Sri Lanka has progressed Shane Curran 27Qatar – Emergency Medicine update Shinu Varughese 27Israel – Towards a national training program George Braitberg 28
EUROPEHungary – The study of Oxyology and Central European challenges Peter Thompson 30Netherlands – Emergency Medicine update Naren Gunja 31
AFRICABotswana – Opportunities for TESL users and ACEM advanced trainees Megan Cox 32Kenya – Can you help a PEM and PCCM program? Mardi Steere, Jane Cocks 33
Volume 10 | Issue 2 | December 2014
IEMSIG | 32 | IEMSIG
international emergency care in 2015 include theWinter Symposium in Alice Springs, mid-year, theInternational Emergency Care Symposium and Coursein Melbourne in the last week of August, and theAnnual Scientific Meeting in Brisbane in November.
And there will be a significant change to ACEM’sgovernance structure for International EmergencyMedicine. Since 2004, the International EmergencyMedicine Special Interest Group (IEMSIG) has been abroad, organic, informative and flexible network. In2011 a dedicated committee, the InternationalDevelopment Fund Committee (IDFC), was formedfor the very specific task of developing the selectionmechanisms and determining the recipients of theannual IDF Grant. As of early 2015, there will be aone stop shop, the International Emergency MedicineCommittee (IEMC), which will bring together all thefunctions of the IEMSIG, the IDFC, and much more,including being an advisory body for the ACEMFoundation’s IEM pillar. The IEMSIG will remain thebroad network it has been, but will have a namechange: the International Emergency MedicineNetwork (IEMNet).
The broad remit of the IEMC has been captured by itsinaugural set of “responsibilities”, combining thehistorical terms of reference of the IEMSIG and theIDFC, and incorporated suggestions from IEMSIGmembers. The goal and responsibilities are asfollows:
The goal of the International Emergency MedicineCommittee is to facilitate the capacity of developingcountries to deliver safe and effective emergencycare. Where international health matters relate toemergency medicine in developing countries, thecommittee shall:
(a) be a repository of information that includesresources, networking, mentoring and careeradvice regarding international emergencymedicine
(b) be a liaison to ACEM and other relevantinstitutions regarding international emergencymedicine issues drawing on IEMC members’expertise
(c) assist in the establishment of emergency medicinetraining through facilitating:
• relevant educational activities in developingcountries
• support for emergency doctors based in
developing countries to enhance their skills incountry and abroad, and
• the development of sister hospital relationshipswith Australasian hospitals
(d) build Australasian emergency physician activitiesin developing countries by facilitatingopportunities for ACEM Fellows and trainees
(e) facilitate and encourage the inclusion of FACEMswho are resident in overseas development postsas members of the IEMC
(f) where appropriate, advise on and facilitate thecreation of training posts for ACEM advancedtrainees in international emergency medicine
(g) build awareness of international emergencymedicine issues across ACEM, other relevantinstitutions and the wider community throughpresentations, publications and events oninternational emergency medicine
(h) establish the criteria by which projects, grants andscholarships will be assessed. These criteria willbe aligned to the goals of the ACEM Foundationwith regard to building emergency medicinecapacity in developing countries
(i) oversee applications for funding and makerecommendations to the ACEM Foundationregarding international emergency medicineprojects, scholarships and grants
(j) promote and support the fund-raising activities ofthe ACEM Foundation.
Finally, it is with great pleasure that I welcome NeilFisher, in his role as the ACEM Foundation Manager,as the lead ACEM manager for the IEMC.
But sadly for ACEM IEM, we will officially be withoutSarah Smith as she takes on a senior managementrole for ACEM. As I mentioned at the recent IEMSIGdinner, Sarah has managed IEMSIG matters andfacilitated its many and varied activities for the last 3years including:
- responding to external and internal requests andqueries
- helping edit the IEMSIG Newsletter
- creation of selection criteria , budget andprocesses for the highly successful and valuedInternational Scholarship Awards
- developing links between Australian VolunteersInternational and Accredited IEM Training
Editorial
Chris Curry
This is the last issue of the chronicles of Australasianinvolvement in EM developments internationally thatwill be called the IEMSIG Newsletter. The first issueappeared in September 2004 with 3 authors; thisissue carries opportunities and outcomes from 28authors. So in ten years it would seem we haveoutgrown the term ‘Newsletter’. We have alsooutgrown ‘IEMSIG’ and in 2015 we will expand intoIEMC and IEMNet (International EM Committee andInternational EM Network).
Over the past decade Australians and NewZealanders have become increasingly active in ourregion, making substantial contributions towards thegraduation of the first emergency physicians in PNG,Thailand, Myanmar and Nepal. First trainees arenearing graduation in Sri Lanka, Fiji and Botswana.Australasians are spreading further afield, withexpanding engagements in the Pacific and Asia andin Europe and Africa.
In this, the second decade of ACEM engagement inEM developments internationally, there will be aneed for the consolidation of established trainingprograms and the development of still more newones. Of the 193 states that sit at the United Nations,fewer than 50 currently recognise emergencymedicine as a specialty. There is a great deal to do.
Message from the IEMSIG Chair
Gerard O’Reilly
From 2014 into 2015As you read this message, you will hopefully be freshfrom a recent break and re-energised for the yearahead. Following is a summary of the 2014 IEMSIGwrap-up from the Tuesday afternoon IEMSIG sessionof December’s Annual Scientific Meeting inMelbourne.
ACEM fellows and trainees have been helping toimprove the delivery of emergency care indeveloping countries for many years. As each yearpasses, the support coming from the College hasgrown considerably to better match and support theefforts of many individuals working in the field onshort or long-term programs.
2014 - Some highlightsMarch and October 2014 saw the graduation of thefirst emergency physicians in Myanmar and Nepalrespectively. Both programs have benefited frommajor Australasian emergency physician and traineework. Whilst emergency care remains in its infancy inboth settings, the building blocks are clearly there,with opportunities for ACEM fellows and trainees tocontribute. In Myanmar, for example, the secondDiploma for Emergency Medicine is half-complete,and the first Masters of Emergency Medicine has justcommenced.
In early 2014, the Department of Foreign Affairs andTrade (DFAT) directly approached ACEM forassistance in improving the delivery of emergencycare to the local population in the Solomon Islands.This led to the creation of a shared (ACEM and DFAT)Terms of Reference and Funding Agreementdocuments for a Scoping Mission and report whichwas successfully delivered in May 2015.Notwithstanding the major reduction of Australia’said budget, it is hoped that the next step will be theplanning and delivery of a funded and well-developed program of emergency care capacitydevelopment in the Solomon Islands.
The 3rd International Emergency Care symposiumwas held over two days in September. Manywonderful speakers spoke to topics linked to anoverall theme of “Can(‘t) we do better?” Similarly, thisyear’s Annual Scientific Meeting committed two fullsessions on the subject of International EmergencyMedicine, where, in addition to the IEMSIG session,we were privileged, with the annual support of theACEM Foundation, to hear wonderful presentationsfrom EM champions representing Myanmar, Nepal,Papua New Guinea and Vietnam. All of this rich IEMcontent was followed by a wonderful gathering ofmore than 50 guests at the annual IEMSIG dinner.
Of course, many unsung contributions and activitiesto improve the capacity of developing countries todeliver emergency care have continued.
2015 – What’s ahead?In addition to an array of activities, the details ofwhich were presented with country updates at boththe International Emergency Care symposium and theScientific Meeting, and in glorious photographicdetail in the pages of the IEMSIG Newsletter, thereare some specific activities worth highlighting.
Australasian events with an ongoing commitment to
IEMSIG | 54 | IEMSIG
A recent success story was a lady who arrived with a2-week history of increasing neck swelling. On arrivalat 2am she had a reduced conscious level, cyanosis,oxygen saturations 40% with signs of an obstructedairway. In the past she may have died. It was adifficult intubation but the EM specialist wassuccessful. She then went to ICU, with the surgeonsplanning to operate on the neck mass.
Our 3-category triage scale, although inconsistentlyimplemented at present, is still an improvement inprocess and is leading to many more success stories.
Our floor space is once again undergoing renovationsand we are hopeful that these improvements willhelp with the implementation of better workingfunctions and a more integrated approach betweenthe various units currently in the ED.
In treating patients one of the challenges has been thelack of supporting staff – initially maybe only anintern or resident to assist. Other staff would refuse tohelp. We have been able to teach and up-skill theinterns and residents and slowly assistance isimproving, but it is variable.
We have been able to increase the level of care in theED, but this is now highlighting some deficiencies inthe receiving areas for our patients.
Despite the successes we are mindful of manychallenges still facing the ED.
• With increasing patient load and casemix weneed more trained doctors and nurses who areable to work competently. With the upcomingMasters of EM and Diploma of EmergencyNursing this will happen, but it will be a slowbuild. We are trying to increase training of ourjunior medical and nursing staff but this teachingrole is difficult to balance with our clinicalworkload.
• Our workload is increasing and the nationalintroduction of the ‘Free of Charge’ care for EDpatients has increased it further.
• Many system processes have been used for manyyears, such as for patient registration and sorting.It will take time, perseverance and patience tonegotiate the changes required for the system tobe more patient centred and effective.
• Building relationships that are helpful not only tothe ED but also, more importantly, for patient careis important and does not always go smoothly.
• We are aware that the training of the Masters ofEM candidates will be important, but ourresources will be stretched.
• Because of low pay levels it is necessary for YGHdoctors to have additional work outside thegovernment hospital, to earn a living.
There are opportunities for the EM specialists to playa role in international gatherings, like ASEAN. We arehopeful that we can also play a meaningful role inroad trauma prevention policies, education andstrategies, and in developing an ambulance service.We see a role in developing good hospital careguidelines.
We are very thankful for ongoing internationalsupport, in particular via the Australian VolunteersInternational (AVI) programme. We see ongoingopportunities for people to help us:
• teaching for the Masters of EM
• training in specialist skill areas like ultrasound,
Posts for Trainees
- generation of the Solomon Islands EmergencyDepartment Improvement Project Scoping Mission,including the Funding Agreement between ACEMand DFAT
- creation of the IEMSIG Executive
- overseeing IEM components of the website update
- bringing structure and professionalism (includingagendas, meetings, transparency and minutes!) to abunch of freelancers, lefties, greenies, do-gooders,backpackers, trekkers, hippies and delinquentvolunteers masquerading as global hawkers of thegospel of emergency medicine!
- being a wonderful advocate for IEM in the corridorsof ACEM and elsewhere
- dealing with three passionate, quirky, and peskyIEMSIG Executive members.
Sarah has looked after many other aspects of ACEM’sengagement with IEM not listed here - and she hasachieved all of this with a constant, calm, gentle, andalways positive and passionate spirit andtemperament, perfect for the many cultures embracedby ACEM’s IEM work.
So on behalf of all IEM groupies and beneficiaries, Isay thank you to you, Sarah Smith.
And I say thank you all for your hard work in 2014for International Emergency Care; we all look forwardto our continued efforts in 2015. Best wishes.
With the successful conclusion of the first Diploma ofEmergency Medicine (EM) program in October 2013,the 18 graduating specialists were used in preparingand managing the emergency systems for the 2013South East Asia (SEA) Games. After the conclusion ofthe SEA Games 10 of those graduands remained full-time in EM and have been distributed throughout thecountry, with 4 specialists continuing at the YangonGeneral Hospital (YGH).
The YGH was established in 1899 and had the onlyrecognised ‘Accident & Emergency’ service in thecountry in 2009. At present it sees more than 70,000patients per year. Integrating a modern EM systemand department has been challenging. In 2014 the‘Accident & Emergency’ area was renamed the‘Emergency Department’ and the EM specialists weregiven responsibility over the department. However,functionally the ED is still run by the orthopaedictrauma service, medical unit and surgical unit.
The EM specialists’ role was to develop, equip andstaff the resuscitation room to cater for the triagecategory 1 patients. In parallel this has meant settingup a triage system to sort by acuity rather thanspecialty. This is a long term process and not yetconsistent, but despite this we are seeing dividendsfrom having a triage system.
Two EM specialists, along with new Diploma of EMcandidates, were present at YGH for much of the firsthalf of 2014, while others were on an observationaltrip in Japan. With limited staff, the ED ran an office-hours resuscitation service. Over this time 422patients were seen in the resuscitation room,70/month. Over half of the triage category 1 patientspresented with head injuries from road trauma orfalls. In August 2014 the resuscitation service became24/7, and still over half of the patients have severehead injury.
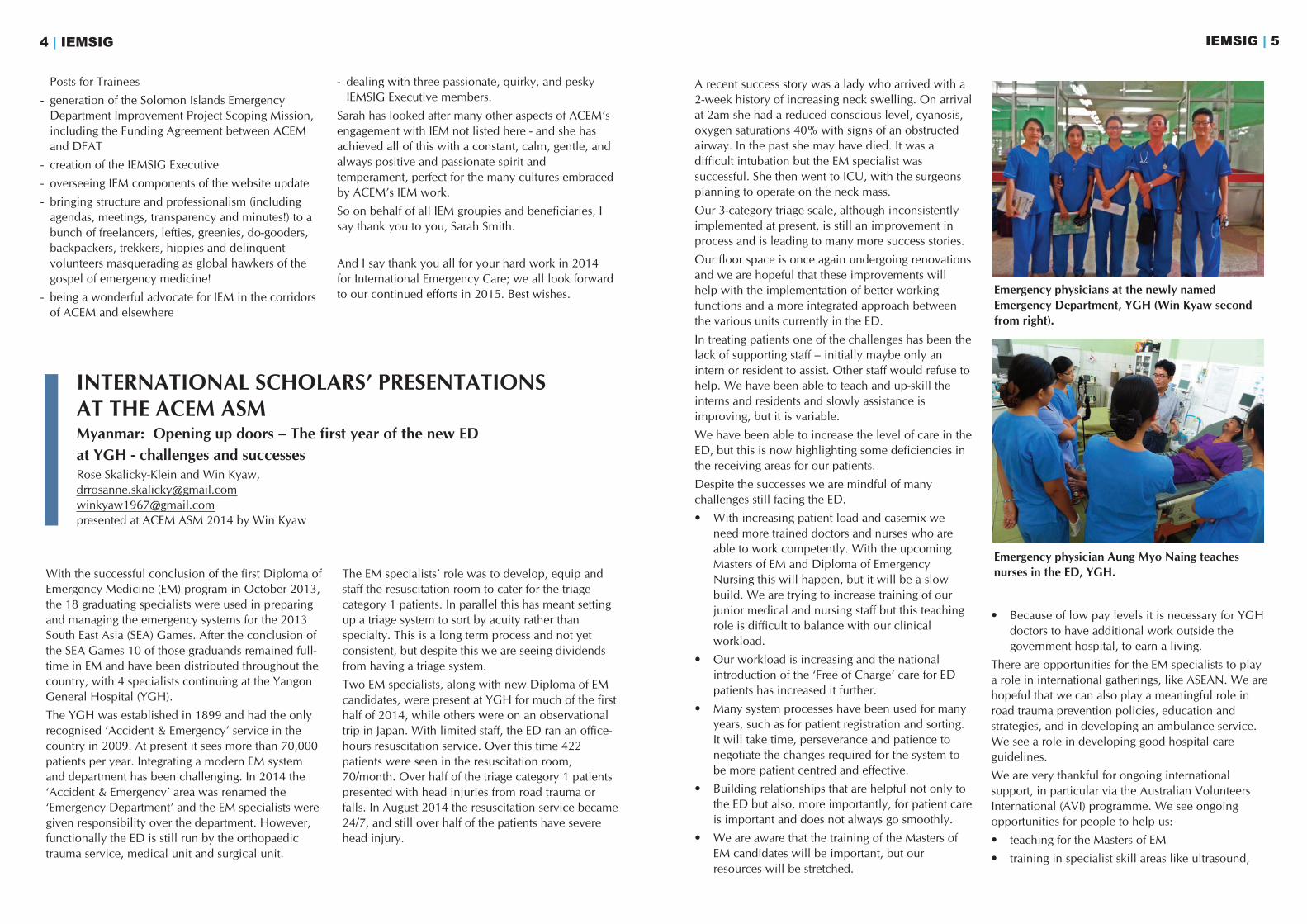
INTERNATIONAL SCHOLARS’ PRESENTATIONS AT THE ACEM ASMMyanmar: Opening up doors – The first year of the new ED at YGH - challenges and successes Rose Skalicky-Klein and Win Kyaw, [email protected]@gmail.compresented at ACEM ASM 2014 by Win Kyaw
Emergency physicians at the newly namedEmergency Department, YGH (Win Kyaw secondfrom right).
Emergency physician Aung Myo Naing teachesnurses in the ED, YGH.
IEMSIG | 76 | IEMSIG
Nepal graduates their first emergency medicine specialistsRamesh Maharjan
ABSTRACTBackground: The first program of emergencymedicine training in Nepal was launched by theInstitute of Medicine (IOM) at Tribhuvan UniversityTeaching Hospital (TUTH) in October 2011.
Objective: to describe the three year Doctorate ofMedicine in Emergency Medicine (DMEM) program.
Method: the period described is from October 2011to October 2014.
Results: The first Nepali emergency medicine trainingprogram was launched after a delegation of Dean,Campus Chief, Hospital Director and Professor ofGP&EM visited the ACEM office and several EDs inMelbourne in February 2011 and received offers ofsupport from FACEMs.
The Doctorate of Medicine in EM (DMEM) wasopened to Nepali doctors with a specialtyqualification, i.e. with 3 years of postgraduate(MD/MS) training after MBBS and internship.
Selection was on the basis of an entranceexamination. Two candidates were selected, bothwith the MDGP qualification and a background inGP&EM
The DMEM program included 2 years in the ED at TUTH, with 3 month rotations to Anaesthesia,Critical Care Medicine, Cardiology, and to the ED at CMC Vellore in India.
The ED training was under the supervision andmentoring of emergency physicians from Australiaand New Zealand. The rotations were conductedwith coordination between the relevant faculties atTUTH.
The program included the undertaking of substantialresearch, and the submission of a research thesis.
Final examinations were conducted in September andOctober 2014, with the two candidates meeting therequirements to be awarded DMEM.
Conclusion: The beginning of academic emergencymedicine training in Nepal has been possible throughcooperation with Australian and New Zealandemergency physicians. A challenge for the future willbe to develop this specialty for different levels ofhealthcare provision throughout the country.
Papua New Guinea: Leading emergencymedicine in Madang ProvinceTaita Kila
Papua New Guinea (PNG) graduated its first locallytrained emergency physician (EP) seven years ago.Today there is a total of 10 locally trained EPs, 7 ofwhom are in public practice. Two more have passedtheir final exams in October this year, making a totalof 12 EPs in 2015.
An emergency physician in Madang Province isessential for the support and continuation of alreadyexisting programs for nurses and health extensionofficers (HEOs) at the Nursing College and at DivineWord University. These students do their clinicalpractice at Modilon General Hospital. The EP is alsothe local supervisor for the ACEM advanced traineeswho do a rotation at Modilon General Hospital.
I transferred to Modilon General Hospital 9 monthsago to support the above programs.
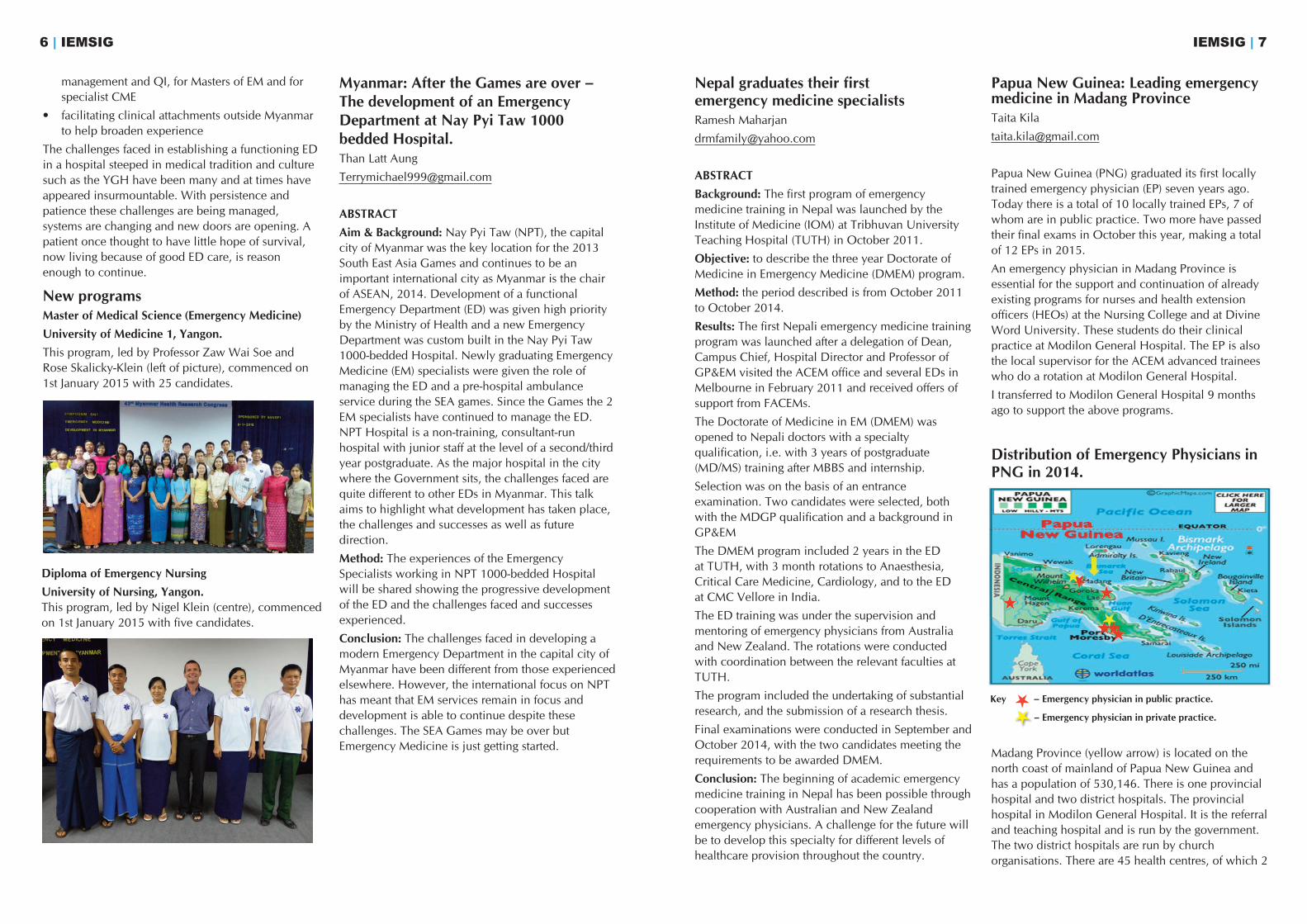
Distribution of Emergency Physicians inPNG in 2014.
Madang Province (yellow arrow) is located on thenorth coast of mainland of Papua New Guinea andhas a population of 530,146. There is one provincialhospital and two district hospitals. The provincialhospital in Modilon General Hospital. It is the referraland teaching hospital and is run by the government.The two district hospitals are run by churchorganisations. There are 45 health centres, of which 2
management and QI, for Masters of EM and forspecialist CME
• facilitating clinical attachments outside Myanmarto help broaden experience
The challenges faced in establishing a functioning EDin a hospital steeped in medical tradition and culturesuch as the YGH have been many and at times haveappeared insurmountable. With persistence andpatience these challenges are being managed,systems are changing and new doors are opening. Apatient once thought to have little hope of survival,now living because of good ED care, is reasonenough to continue.
New programsMaster of Medical Science (Emergency Medicine)University of Medicine 1, Yangon.This program, led by Professor Zaw Wai Soe andRose Skalicky-Klein (left of picture), commenced on1st January 2015 with 25 candidates.
Myanmar: After the Games are over – The development of an Emergency Department at Nay Pyi Taw 1000 bedded Hospital.Than Latt Aung
ABSTRACTAim & Background: Nay Pyi Taw (NPT), the capitalcity of Myanmar was the key location for the 2013South East Asia Games and continues to be animportant international city as Myanmar is the chairof ASEAN, 2014. Development of a functionalEmergency Department (ED) was given high priorityby the Ministry of Health and a new EmergencyDepartment was custom built in the Nay Pyi Taw1000-bedded Hospital. Newly graduating EmergencyMedicine (EM) specialists were given the role ofmanaging the ED and a pre-hospital ambulanceservice during the SEA games. Since the Games the 2EM specialists have continued to manage the ED.NPT Hospital is a non-training, consultant-runhospital with junior staff at the level of a second/thirdyear postgraduate. As the major hospital in the citywhere the Government sits, the challenges faced arequite different to other EDs in Myanmar. This talkaims to highlight what development has taken place,the challenges and successes as well as futuredirection.
Method: The experiences of the EmergencySpecialists working in NPT 1000-bedded Hospitalwill be shared showing the progressive developmentof the ED and the challenges faced and successesexperienced.
Conclusion: The challenges faced in developing amodern Emergency Department in the capital city ofMyanmar have been different from those experiencedelsewhere. However, the international focus on NPThas meant that EM services remain in focus anddevelopment is able to continue despite thesechallenges. The SEA Games may be over butEmergency Medicine is just getting started.
Diploma of Emergency NursingUniversity of Nursing, Yangon.This program, led by Nigel Klein (centre), commencedon 1st January 2015 with five candidates.
Key – Emergency physician in public practice.
– Emergency physician in private practice.
IEMSIG | 9
are closed, and 238 aid posts, of which 65 areclosed. Church organisations run 42% of thefacilities.
Modilon General Hospital (MGH)Modilon General Hospital has a bed capacity of 258and a total of 29 doctors. All the doctors and mostHEOs in the province work at this hospital. HEOshave responsibilities like doctors but are not doctors.
MGH supports two programs run by Divine WordUniversity:
1) Advanced Diploma in Emergency Medicine(ADEM), which is a postgraduate program for nursesand HEOs. The program has been runningsuccessfully since it started in 2008. About 40students have graduated and we expect another 10more graduates next year.
2) Undergraduate HEO program. The ACEMadvanced trainees are involved as clinical lecturers.
Some challenges in the Adults Outpatient, Accidentand Emergency Department.
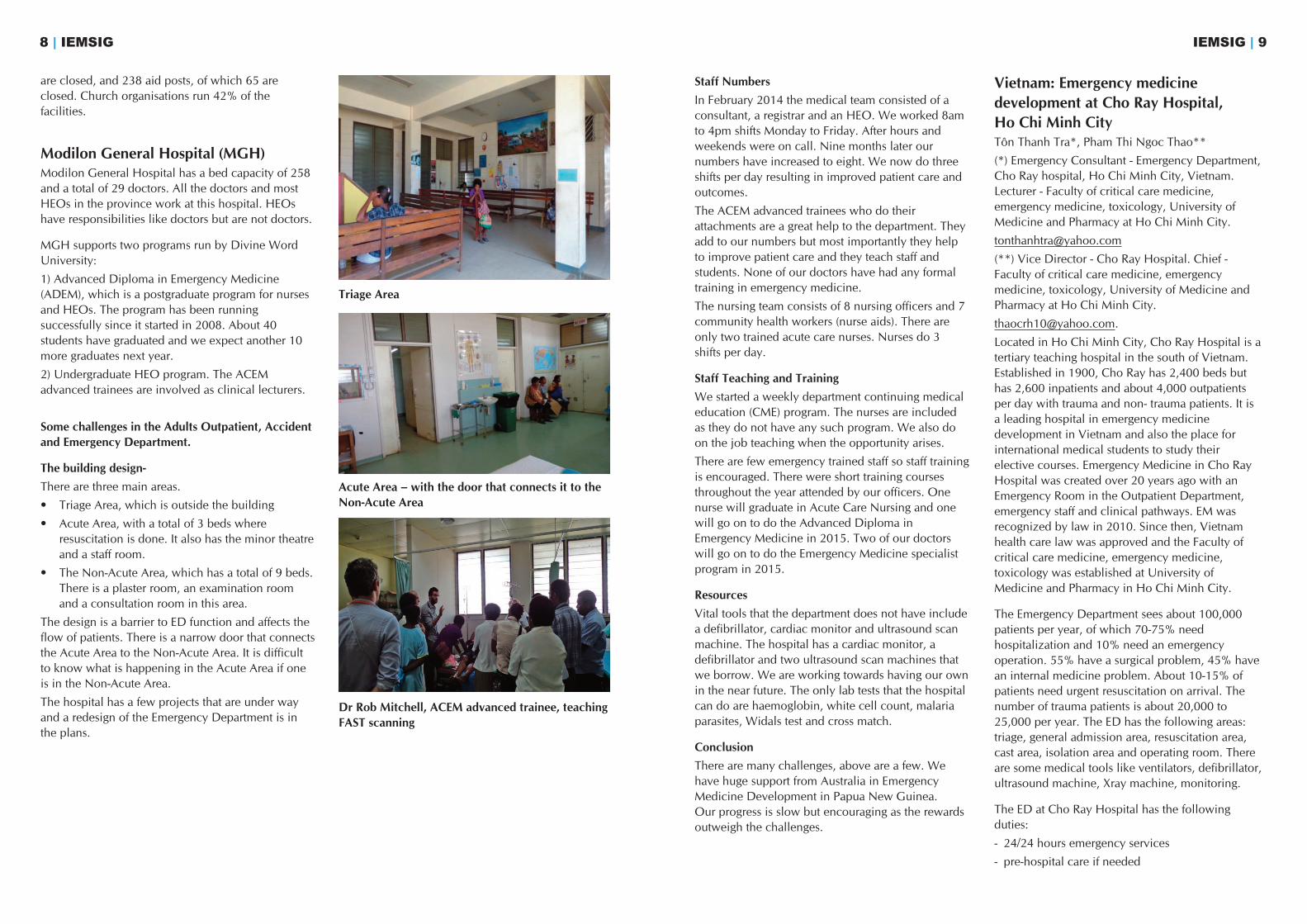
The building design-There are three main areas.
• Triage Area, which is outside the building
• Acute Area, with a total of 3 beds whereresuscitation is done. It also has the minor theatreand a staff room.
• The Non-Acute Area, which has a total of 9 beds.There is a plaster room, an examination roomand a consultation room in this area.
The design is a barrier to ED function and affects theflow of patients. There is a narrow door that connectsthe Acute Area to the Non-Acute Area. It is difficultto know what is happening in the Acute Area if oneis in the Non-Acute Area.
The hospital has a few projects that are under wayand a redesign of the Emergency Department is inthe plans.
8 | IEMSIG
Triage Area
Acute Area – with the door that connects it to theNon-Acute Area
Dr Rob Mitchell, ACEM advanced trainee, teachingFAST scanning
Staff NumbersIn February 2014 the medical team consisted of aconsultant, a registrar and an HEO. We worked 8amto 4pm shifts Monday to Friday. After hours andweekends were on call. Nine months later ournumbers have increased to eight. We now do threeshifts per day resulting in improved patient care andoutcomes.
The ACEM advanced trainees who do theirattachments are a great help to the department. Theyadd to our numbers but most importantly they helpto improve patient care and they teach staff andstudents. None of our doctors have had any formaltraining in emergency medicine.
The nursing team consists of 8 nursing officers and 7community health workers (nurse aids). There areonly two trained acute care nurses. Nurses do 3shifts per day.
Staff Teaching and TrainingWe started a weekly department continuing medicaleducation (CME) program. The nurses are includedas they do not have any such program. We also doon the job teaching when the opportunity arises.
There are few emergency trained staff so staff trainingis encouraged. There were short training coursesthroughout the year attended by our officers. Onenurse will graduate in Acute Care Nursing and onewill go on to do the Advanced Diploma inEmergency Medicine in 2015. Two of our doctorswill go on to do the Emergency Medicine specialistprogram in 2015.
ResourcesVital tools that the department does not have includea defibrillator, cardiac monitor and ultrasound scanmachine. The hospital has a cardiac monitor, adefibrillator and two ultrasound scan machines thatwe borrow. We are working towards having our ownin the near future. The only lab tests that the hospitalcan do are haemoglobin, white cell count, malariaparasites, Widals test and cross match.
ConclusionThere are many challenges, above are a few. Wehave huge support from Australia in EmergencyMedicine Development in Papua New Guinea. Our progress is slow but encouraging as the rewardsoutweigh the challenges.
Vietnam: Emergency medicine development at Cho Ray Hospital, Ho Chi Minh CityTôn Thanh Tra*, Pham Thi Ngoc Thao**
(*) Emergency Consultant - Emergency Department,Cho Ray hospital, Ho Chi Minh City, Vietnam.Lecturer - Faculty of critical care medicine,emergency medicine, toxicology, University ofMedicine and Pharmacy at Ho Chi Minh City.
(**) Vice Director - Cho Ray Hospital. Chief -Faculty of critical care medicine, emergencymedicine, toxicology, University of Medicine andPharmacy at Ho Chi Minh City.
Located in Ho Chi Minh City, Cho Ray Hospital is atertiary teaching hospital in the south of Vietnam.Established in 1900, Cho Ray has 2,400 beds buthas 2,600 inpatients and about 4,000 outpatientsper day with trauma and non- trauma patients. It isa leading hospital in emergency medicinedevelopment in Vietnam and also the place forinternational medical students to study theirelective courses. Emergency Medicine in Cho RayHospital was created over 20 years ago with anEmergency Room in the Outpatient Department,emergency staff and clinical pathways. EM wasrecognized by law in 2010. Since then, Vietnamhealth care law was approved and the Faculty ofcritical care medicine, emergency medicine,toxicology was established at University ofMedicine and Pharmacy in Ho Chi Minh City.
The Emergency Department sees about 100,000patients per year, of which 70-75% needhospitalization and 10% need an emergencyoperation. 55% have a surgical problem, 45% havean internal medicine problem. About 10-15% ofpatients need urgent resuscitation on arrival. Thenumber of trauma patients is about 20,000 to25,000 per year. The ED has the following areas:triage, general admission area, resuscitation area,cast area, isolation area and operating room. Thereare some medical tools like ventilators, defibrillator,ultrasound machine, Xray machine, monitoring.
The ED at Cho Ray Hospital has the followingduties:
- 24/24 hours emergency services
- pre-hospital care if needed
- The emergency medicine system in Vietnam is notcomprehensive and not uniform at all levels.
- There are no paramedic staffs in Vietnam.
- We do not have enough family doctors so thatpatients may come to the ED without anyemergency problems. Emergency staff cannot refusecare.
- The specialty of emergency medicine is not reallyrecognized by medical leaders and colleagues.
- Lastly, health care insurance does not cover all thepopulation and access to the medical system is notuniform.
Future plansTo practice emergency medicine well at Cho RayHospital and in Vietnam, we should developprofessional emergency staffs with postgraduateeducation. Training programs could includeSpecialty, Master degree, Philosophy degree inEmergency Medicine and continuing medicaleducations (CME), with hands-on training courses.
We should have some short training courses fordoctors and nurses who are working in EDs. We willtry to make a training curriculum for paramedics inVietnam to supply the human resources for pre-hospital care and medical evacuation. We mustdevelop an emergency medicine system that issuitable for Vietnam’s economic, cultural andmedical circumstances. We need to develop trainingcurricula for disaster management and we need todevelop specific emergency centres for trauma,surgery, internal medicine and toxicology. To do that,we need support from internal and internationalorganizations.
ConclusionThe emergency medicine system in Vietnam is still inits infancy and is not comprehensive. This specialty isvery hard work and has many challenges. Specialpolicies and regulations for professional developmentare necessary to meet community needs. Thedevelopment and implementation of modernemergency medicine is very urgent in Vietnam.
IEMSIG | 11
- training for Vietnamese and international medicalstudents, postgraduates.
- direction of healthcare activities
- international cooperation
As a leading hospital in Vietnam, the ED receivesmany severely ill patients from many hospitals and isa place of training for emergency staff and medicalstudents. To have a professional team is veryimportant in our activities. To achieve this purpose,the ED and the Faculty cooperate in activities andtraining. We have a lot of training courses:
- continuing medical education training for lowerlevels of emergency staff
- continuing medical education training for staff ofCho Ray Hospital
- postgraduate education for level 1 specialty incritical care medicine, emergency medicine,toxicology
- organizing of emergency medicine conferences
- writing emergency medicine books
- researching in emergency medicine
- supporting training in emergency medicine forremote areas
- developing an emergency medicine network
- training in disaster medicine for Cho Ray staff andother hospitals in Vietnam
- contributing to the Vietnam Society for EM (VSEM).
We have published 7 articles, including ultrasounddiagnosis of acute appendicitis by ED, FAST exam,ultrasound to estimate intravascular volume, masscasualty incidents, and the compliance of survivingsepsis campaign 2012 in the ED.
In 2010 Dr Tra received a scholarship fromQueensland University to study for 3 months as aclinical visitor at the Royal Brisbane and WomensHospital. In 2014 Dr Tra received an ACEM award toattend and present at the ACEM Annual ScientificMeeting in Melbourne Victoria, Australia. Thisopportunity generated linkages with ANZ EPs andoffers of support for the development of EM at ChoRay Hospital and more widely in Vietnam.
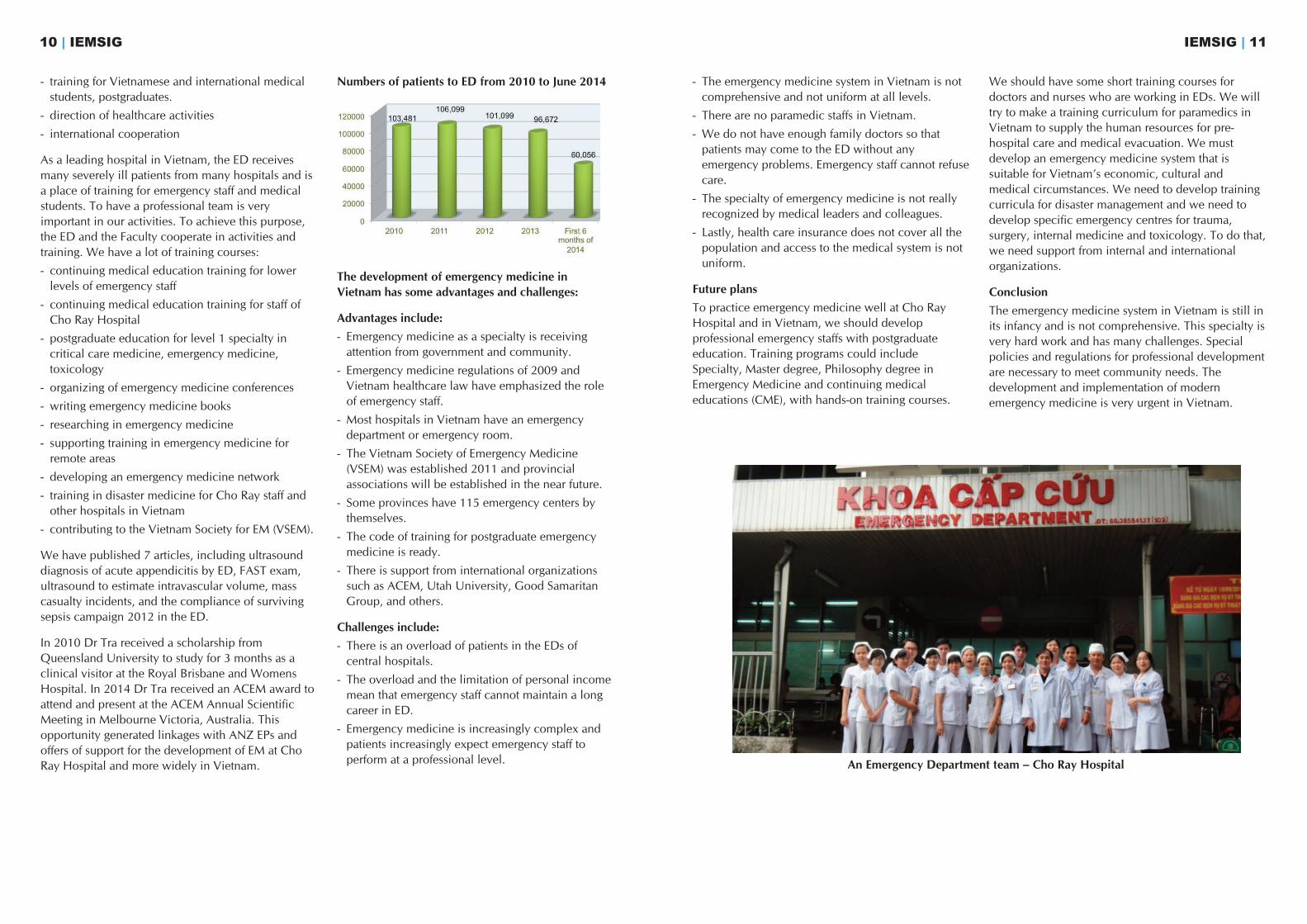
Numbers of patients to ED from 2010 to June 2014
The development of emergency medicine inVietnam has some advantages and challenges:
Advantages include: - Emergency medicine as a specialty is receivingattention from government and community.
- Emergency medicine regulations of 2009 andVietnam healthcare law have emphasized the roleof emergency staff.
- Most hospitals in Vietnam have an emergencydepartment or emergency room.
- The Vietnam Society of Emergency Medicine(VSEM) was established 2011 and provincialassociations will be established in the near future.
- Some provinces have 115 emergency centers bythemselves.
- The code of training for postgraduate emergencymedicine is ready.
- There is support from international organizationssuch as ACEM, Utah University, Good SamaritanGroup, and others.
Challenges include:- There is an overload of patients in the EDs ofcentral hospitals.
- The overload and the limitation of personal incomemean that emergency staff cannot maintain a longcareer in ED.
- Emergency medicine is increasingly complex andpatients increasingly expect emergency staff toperform at a professional level.
10 | IEMSIG
An Emergency Department team – Cho Ray Hospital
Constructing an emergency medicine (EM) trainingprogram in another country presents challenges.
Questions that arise include:
• content: relevance to global and local diseasepatterns, diagnostics and treatment
• delivery: what is desirable, what is possible?
• feedback and evaluation: are you meeting thelearners’ needs?
• translation into practice: can they practice whatthey learn?
It is important to consider the risks. The emergencydepartment is not an island and is highly dependent ona complex web of support and inpatient services. Forchanges to practice in the emergency space to beeffective, they must gain acceptance from otherstakeholders. This may take considerable time andeffort but is necessary to limit conflict and improve
care during the whole patient journey. Collaboratingwith other departments in education and qualityimprovement projects helps to build relationships,mutual understanding and respect. For impatientemergency clinicians the pace of change can seempainfully slow. One must persist to effect sustainablechange. Patience, acceptance, tolerance andunderstanding of local processes and power structuresare essential. Trust is key and local skepticism isunderstandable in places where many visit and lookbut few stay and help.
Structures and FluidityUniversities and hospitals provide structures fortraining. These structures may not be as straightforwardor as robust as they appear. Navigating foreignstructures and discovering how things work requires adegree of cultural assimilation that cannot be rushed
Brady Tassicker-Tasmanian; Nick Ryan - somewhere inthere is a mad Irishman; Craig Wallace - Kiwi Scot;Alan Tankel - Glaswegian Scot; Vincent Russell - trueAussie; Andrew Bezzina (convener) - a mongrel.Trina Sale from Honiara was the 7th member.
The SIREn courses were delivered by the above facultyminus Drs. Tankel and Russell, who had othercommitments. Trelly Samuel Patunvanu (Ni-Vanuatu)was an addition.
Whilst the courses were not fully subscribed, they
were very well received by the locals, with some staffattending the courses despite working night shiftsthroughout. If proof was needed, these coursesdemonstrated how important having ‘on the ground’organisational and political support is in maximisingaccess and benefits for the participants.
As is always the case in these circumstances, theAustralasian faculty continued to be impressed by thecapacity of the local clinicians in these environmentsto deliver a service to their communities.
IEMSIG | 1312 | IEMSIG
Fiji: Perspectives on building an EM Training program
Anne Creaton
PACIFIC
ELS in the Pacific
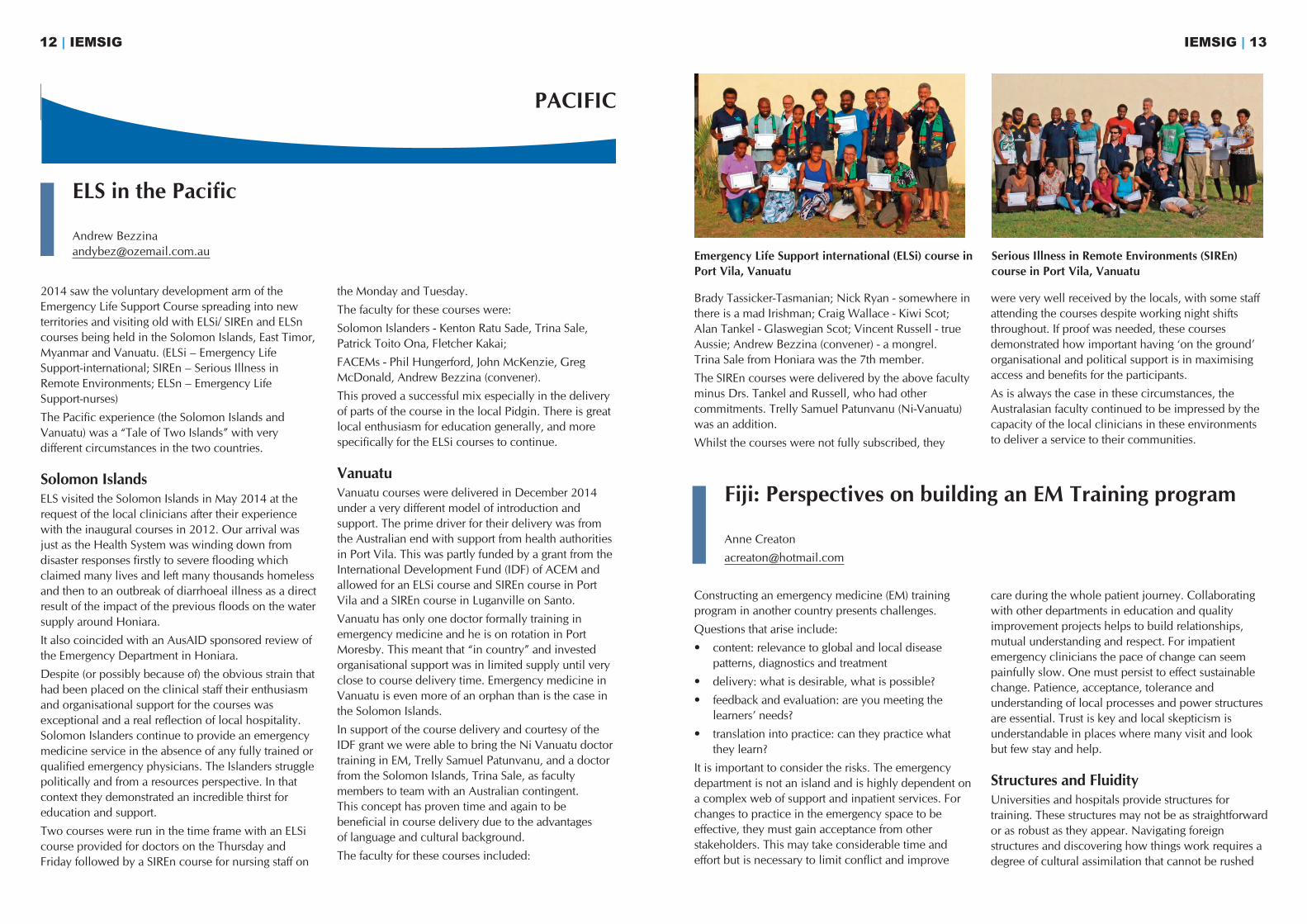
Andrew [email protected] Emergency Life Support international (ELSi) course in
Port Vila, VanuatuSerious Illness in Remote Environments (SIREn)course in Port Vila, Vanuatu
2014 saw the voluntary development arm of theEmergency Life Support Course spreading into newterritories and visiting old with ELSi/ SIREn and ELSncourses being held in the Solomon Islands, East Timor,Myanmar and Vanuatu. (ELSi – Emergency LifeSupport-international; SIREn – Serious Illness inRemote Environments; ELSn – Emergency Life Support-nurses)
The Pacific experience (the Solomon Islands andVanuatu) was a “Tale of Two Islands” with verydifferent circumstances in the two countries.
Solomon IslandsELS visited the Solomon Islands in May 2014 at therequest of the local clinicians after their experiencewith the inaugural courses in 2012. Our arrival wasjust as the Health System was winding down fromdisaster responses firstly to severe flooding whichclaimed many lives and left many thousands homelessand then to an outbreak of diarrhoeal illness as a directresult of the impact of the previous floods on the watersupply around Honiara.
It also coincided with an AusAID sponsored review ofthe Emergency Department in Honiara.
Despite (or possibly because of) the obvious strain thathad been placed on the clinical staff their enthusiasmand organisational support for the courses wasexceptional and a real reflection of local hospitality.Solomon Islanders continue to provide an emergencymedicine service in the absence of any fully trained orqualified emergency physicians. The Islanders strugglepolitically and from a resources perspective. In thatcontext they demonstrated an incredible thirst foreducation and support.
Two courses were run in the time frame with an ELSicourse provided for doctors on the Thursday andFriday followed by a SIREn course for nursing staff on
the Monday and Tuesday.
The faculty for these courses were:
Solomon Islanders - Kenton Ratu Sade, Trina Sale,Patrick Toito Ona, Fletcher Kakai;
FACEMs - Phil Hungerford, John McKenzie, GregMcDonald, Andrew Bezzina (convener).
This proved a successful mix especially in the deliveryof parts of the course in the local Pidgin. There is greatlocal enthusiasm for education generally, and morespecifically for the ELSi courses to continue.
VanuatuVanuatu courses were delivered in December 2014under a very different model of introduction andsupport. The prime driver for their delivery was fromthe Australian end with support from health authoritiesin Port Vila. This was partly funded by a grant from theInternational Development Fund (IDF) of ACEM andallowed for an ELSi course and SIREn course in PortVila and a SIREn course in Luganville on Santo.
Vanuatu has only one doctor formally training inemergency medicine and he is on rotation in PortMoresby. This meant that “in country” and investedorganisational support was in limited supply until veryclose to course delivery time. Emergency medicine inVanuatu is even more of an orphan than is the case inthe Solomon Islands.
In support of the course delivery and courtesy of theIDF grant we were able to bring the Ni Vanuatu doctortraining in EM, Trelly Samuel Patunvanu, and a doctorfrom the Solomon Islands, Trina Sale, as facultymembers to team with an Australian contingent. This concept has proven time and again to bebeneficial in course delivery due to the advantages of language and cultural background.
The faculty for these courses included:
The year 2014 has been significant for emergencymedicine (EM) in Papua New Guinea (PNG).Changes to the training program are afoot, there aretwo newly graduated emergency physicians andthere is now EM being practiced at specialist level infour provinces.
In PNG all specialty training is administered by theUniversity of PNG towards Masters of Medicine(MMed) degrees. The first year of MMed (EM) hasbeen spent as a surgical trainee, working as a surgicalregistrar and sitting surgical first part exams. This hasbeen necessary until now, but as of 2015, the firstyear will be spent as an emergency registrar workingin Port Moresby General Hospital and there will bean emergency medicine specific first part exam. Thiswill mean more accredited trainees present in theemergency department (ED), which should improvemorale, develop a more academic culture and
ultimately increase the standard of care. Anemergency medicine first part will be more relevantto the future emergency physicians of PNG.
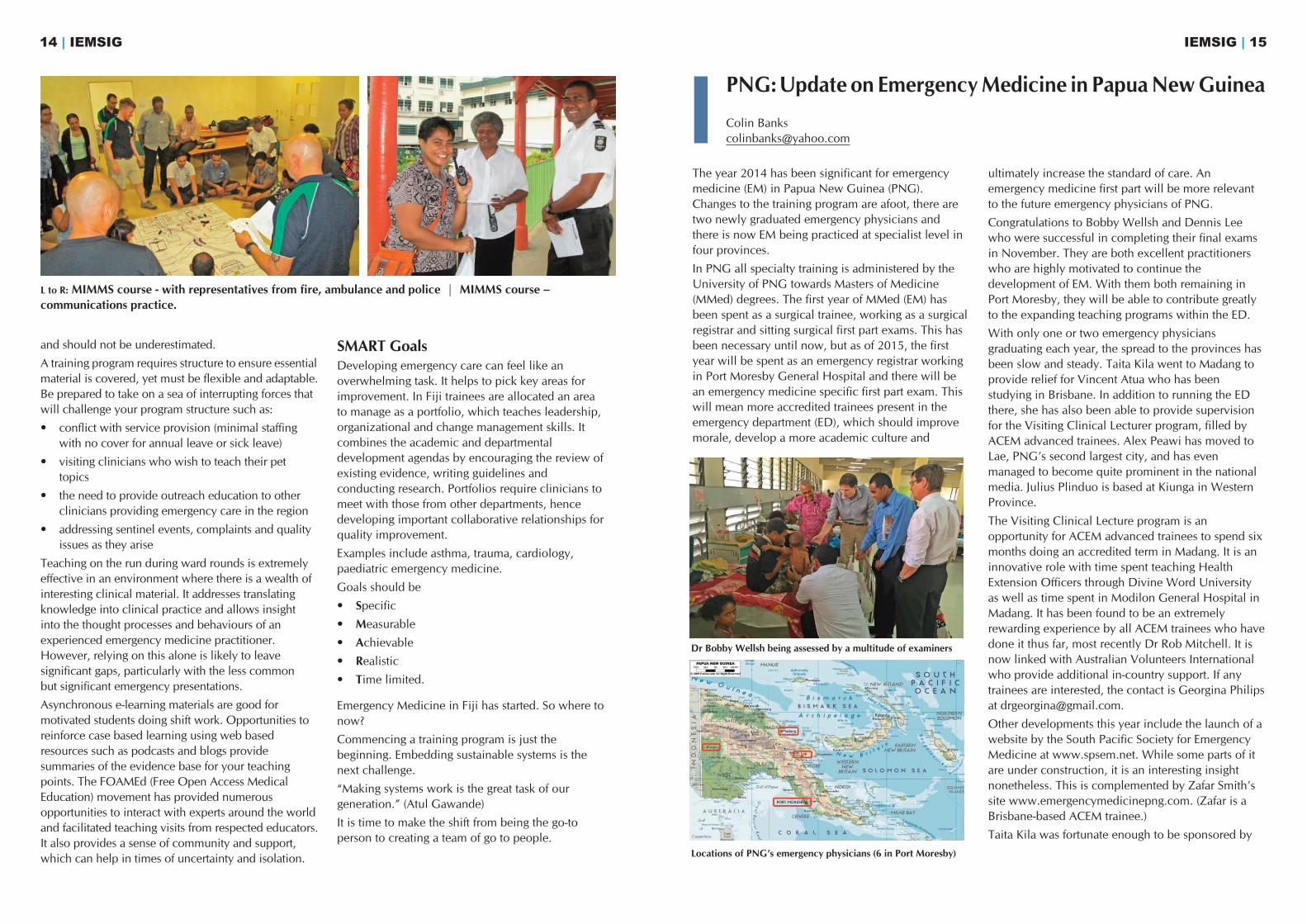
Congratulations to Bobby Wellsh and Dennis Leewho were successful in completing their final examsin November. They are both excellent practitionerswho are highly motivated to continue thedevelopment of EM. With them both remaining inPort Moresby, they will be able to contribute greatlyto the expanding teaching programs within the ED.
With only one or two emergency physiciansgraduating each year, the spread to the provinces hasbeen slow and steady. Taita Kila went to Madang toprovide relief for Vincent Atua who has beenstudying in Brisbane. In addition to running the EDthere, she has also been able to provide supervisionfor the Visiting Clinical Lecturer program, filled byACEM advanced trainees. Alex Peawi has moved toLae, PNG’s second largest city, and has evenmanaged to become quite prominent in the nationalmedia. Julius Plinduo is based at Kiunga in WesternProvince.
The Visiting Clinical Lecture program is anopportunity for ACEM advanced trainees to spend sixmonths doing an accredited term in Madang. It is aninnovative role with time spent teaching HealthExtension Officers through Divine Word Universityas well as time spent in Modilon General Hospital inMadang. It has been found to be an extremelyrewarding experience by all ACEM trainees who havedone it thus far, most recently Dr Rob Mitchell. It isnow linked with Australian Volunteers Internationalwho provide additional in-country support. If anytrainees are interested, the contact is Georgina Philipsat [email protected].
Other developments this year include the launch of awebsite by the South Pacific Society for EmergencyMedicine at www.spsem.net. While some parts of itare under construction, it is an interesting insightnonetheless. This is complemented by Zafar Smith’ssite www.emergencymedicinepng.com. (Zafar is aBrisbane-based ACEM trainee.)
Taita Kila was fortunate enough to be sponsored by
IEMSIG | 15
and should not be underestimated.
A training program requires structure to ensure essentialmaterial is covered, yet must be flexible and adaptable.Be prepared to take on a sea of interrupting forces thatwill challenge your program structure such as:
• conflict with service provision (minimal staffingwith no cover for annual leave or sick leave)
• visiting clinicians who wish to teach their pettopics
• the need to provide outreach education to otherclinicians providing emergency care in the region
• addressing sentinel events, complaints and qualityissues as they arise
Teaching on the run during ward rounds is extremelyeffective in an environment where there is a wealth ofinteresting clinical material. It addresses translatingknowledge into clinical practice and allows insightinto the thought processes and behaviours of anexperienced emergency medicine practitioner.However, relying on this alone is likely to leavesignificant gaps, particularly with the less common but significant emergency presentations.
Asynchronous e-learning materials are good formotivated students doing shift work. Opportunities toreinforce case based learning using web basedresources such as podcasts and blogs providesummaries of the evidence base for your teachingpoints. The FOAMEd (Free Open Access MedicalEducation) movement has provided numerousopportunities to interact with experts around the worldand facilitated teaching visits from respected educators.It also provides a sense of community and support,which can help in times of uncertainty and isolation.
SMART GoalsDeveloping emergency care can feel like anoverwhelming task. It helps to pick key areas forimprovement. In Fiji trainees are allocated an areato manage as a portfolio, which teaches leadership,organizational and change management skills. Itcombines the academic and departmentaldevelopment agendas by encouraging the review ofexisting evidence, writing guidelines andconducting research. Portfolios require clinicians tomeet with those from other departments, hencedeveloping important collaborative relationships forquality improvement.
Examples include asthma, trauma, cardiology,paediatric emergency medicine.
Goals should be
• Specific• Measurable
• Achievable• Realistic• Time limited.
Emergency Medicine in Fiji has started. So where tonow?
Commencing a training program is just thebeginning. Embedding sustainable systems is thenext challenge.
“Making systems work is the great task of ourgeneration.” (Atul Gawande)
It is time to make the shift from being the go-toperson to creating a team of go to people.
14 | IEMSIG
PNG:Update on EmergencyMedicine in PapuaNewGuinea
Colin [email protected]
L to R: MIMMS course - with representatives from fire, ambulance and police | MIMMS course –communications practice.
Dr Bobby Wellsh being assessed by a multitude of examiners
Locations of PNG’s emergency physicians (6 in Port Moresby)

IEMSIG | 17
The past year has seen some significant wins foremergency medicine in Vanuatu. The long-awaitednew emergency department (ED) in Vila CentralHospital, the tertiary referral hospital, has beencompleted (more on this later). The first ever Ni-Vanuatu emergency medicine registrar, Trelly SamuelPatunvanu, is progressing well through his training,and is due to commence employment in Canberra in2015, after which the final barrier to completion ofhis specialist EM training will be the examinations forMMedEM of UPNG. And an IDF grant from ACEMwas used to run the inaugural ELSi and SIREn courses(see report by Andrew Bezzina in this newsletter). Allof this has undoubtedly helped raise the profile ofemergency medicine within Vanuatu.
The Japanese government donated a new hospitalwing, with construction finished earlier this year, andthe Outpatients and ED have only recently movedinto this new facility. The comparison with the oldone is fantastic. Emergency care in Vanuatu, as inmuch of the world, continues to function as thoughoutpatients and emergency medicine were separateentities, assuming that patients have enough healthliteracy to know how urgent their clinicalpresentation is. The blurring of these boundaries wascompounded in the old department by the minglingof patients in a dark and poorly ventilated corridor,which confused patient flow.
The new layout continues this separation ofoutpatients and emergency, but in a way which ismuch more functional. There is a large open-air
waiting area for outpatients, and flow of patients iswell controlled by the layout of doors and rooms.Outpatients backs directly onto the ED, facilitatingease of transfer of patients between the two.
The ED itself is spacious, well ventilated and well lit.The department is well resourced, with dedicatedbarouches, monitors, and portable X-ray machine.
The model of care across both departments isunchanged: nurses and nurse practitioners with nodedicated medical staff. This reflects a shortage ofmedical staff generally, across the nation.
Even this shortage is likely to change in the nearfuture. There are a large number of Cuban-trained Ni-Vanuatu medical students due to start theirinternships in Port Vila over the next couple of years.This influx of medical staff will inevitably improve thestaffing model for the ED, and hopefully includesome emergency physicians of the future.
The next project being tackled involves trying tobring the inaugural Emergency Management ofSevere Burns course to Vanuatu. As with any projectin this environment, there will undoubtedly bechallenges in realizing this. The lessons learnt frompreparing the ELSi and SIREn courses will proveinvaluable in this.
Current development needs are broad. Any visitingdelegation is most likely to be successful if it includesboth medical and nursing representation. If anyone isinterested, please contact me on the email addressabove.
16 | IEMSIG
Vanuatu: Wins for emergency medicine in Vanuatu
Brady Tassicker
ACEM to come to the Annual Scientific Meeting inMelbourne just recently. She made an excellentpresentation, met some great people and then wenton to do an ultrasound course courtesy of StVincent’s Hospital in Melbourne. Thanks to everyoneat ACEM and St Vincent’s who facilitated this.
No-one quite knows what 2015 will hold in store inthe ‘land of the unexpected’. There are the newchanges to the MMed(EM), some excellent trainees
sitting the part two exam, and the EM community isinvolved with the South Pacific Games to be held inPort Moresby in July. There are some opportunities toget involved, particularly with teaching in PortMoresby, although the logistics can be challenging.
If you are interested then contact either myself [email protected] or the Chief EmergencyPhysician, Sam Yockopua [email protected].
New Outpatients and ED waiting area – Vila Central Hospital
New Emergency Department entrance
Resuscitation facilities
Building on the work done in 2013, in 2014 twostreams of educational programs about methanolpoisoning were developed: one focused oncommunity education (for the general communityand primary health centre staff) and the second forclinical staff within hospital settings. The programsare managed by the Lifesaving Initiatives AboutMethanol – LIAM - Charity, based in WesternAustralia, which works collaboratively with selectedstaff from both Sanglah Hospital and the PublicHealth School at Udayana University in Bali. Theclinicians from Australia are Di Brown RN(coordinator of the Sister Hospital Program betweenRoyal Darwin Hospital and Sanglah Hospital) andMalcolm Johnstone-Leek FACEM from the NationalCritical Care and Trauma Response Centre(NCCTRC). Mark Monaghan, FACEM toxicologist,provides long distance advice and mentoring fromPerth. Funding has come from NZAid, the LIAMCharity, the Methanol Institute and the NCCTRC.
https://www.facebook.com/pages/Lifesaving-Initiatives-About-Methanol-LIAM/389335401165731
http://indonesiaexpat.biz/other/lifesaving-initiatives-against-methanol/
http://methanol.org/blog/?p=407
http://www.methanol.org/
The community education program has initiallyfocused on 14 villages and 12 community healthcentres in the regions in Bali where the most arak-poisoning deaths have occurred. Initially thecommunities were suspicious about the motives forthe program as they suspected the aim was to closethe arak production down. To engage the localcommunities, Bondres - traditional Balinese folkdance - is used to convey the messages about
methanol poisoning. This has been well received andthe attendance at the workshops has been good.
Information is also provided by social media andlocal and national TV and newspapers, etc.The clinical education program has targeted themajor public hospitals and the main private hospitalsin both Bali and Lombok.
To date over 1000 people have received educationabout recognition and treatment for people whopresent with methanol poisoning. The program is
very relevant and topical as 117 people werepoisoned in western Java before Christmas 2014 andmore than 25 of them died.
In December 2014 a workshop of key stakeholders -from public health, food and liquor, tourism andpolice - was held at Udayana University to discussthe issues surrounding methanol poisoning. While allparticipants were willing to support the treatmentoptions that are available they are not able to do sountil there is written approval and a standardoperating procedure received from the Ministry ofHealth in Jakarta.
In 2015 the following is planned:
1. continue both streams of the education programin Bali and Lombok;
2. provide a national seminar in Jakarta to key policyand educational stakeholders with a view togetting changes in standard operating proceduresfor patients with methanol poisoning;
3. Malcolm Johnston-Leek and an emergency nursefrom the NCCTC will come to Lombok for 2months to work in the main Provincial Hospital totrain emergency staff and first responders there;
4. develop a position and training program in Java;
5. send suitable staff to Australia for training in triageand assessment of patients presenting to EDs (thiswill require funding).
There is no emergency medicine specialty inIndonesia and patients suffer because there is nosystematic triage and assessment process and becauseEDs are staffed by the most junior doctors.Opportunities for emergency physician involvementexist in EDs across the archipelago, but thedevelopment of any program will require carefulnegotiation and the systematic building ofrelationships. Di Brown is happy to be of assistance.
IEMSIG | 1918 | IEMSIG
SOUTH EAST ASIA
INDONESIABali and Lombok: the Methanol Education ProgramDi [email protected]
Bondres – telling the story with folk dance
Di Brown is interviewed by Bali TV during a workshop inBadung.
Montage from a workshop. Malcolm Johnston-Leek responds to questions from army medical personnel
The methanol team at a workshop in Lombok.

Thailand has a well established medical systembefitting its relatively strong economic position. Thereis a mix of private and public practice and mostmedical specialities are represented. Universal healthcare is provided and the Ministry of Public Healthoversees more than 1000 hospitals. Training istypically conducted along a mix of models consistentwith Western Europe and North America.
Whilst there were casualty departments and a nascentpre-hospital service, there was no speciality ofemergency medicine until the mid-2000s. Thischanged as a result of the 2004 Boxing Day SouthAsian tsunami that devastated the local Indonesianprovince of Aceh but also gravely affected manynations on the Indian Ocean boundaries. The Thaigovernment, recognising the gap in their medicalservices, tasked the Thai Association for EmergencyMedicine (TAEM) to fast-track the development ofemergency medicine (EM) as a speciality.
Following contact with ACEM, Dr SomchaiKanchanasut and Dr Pairoj Khruekarnchana teamedup with Associate Professor Marcus Kennedy and DrDon Liew at Royal Melbourne Hospital (RMH) to winthe first of several AusAid grants to help fund thedevelopment of Thai EM.
The program included:
• A 12 month project (2005) to bring the currentThai leaders in the nascent specialty of EM toRMH to be taught about the specialty, itsgovernance, administration, research andteaching.
• A follow-up project (2007) for the current cohortof advanced trainees, those doctors destined tobecome the first graduates in EM in Thailand.
• Establishment of a Thai Emergency Medicineresidency program. This has been supported withteaching and research forums by Australianfaculty.
• The first Thai / International Emergency Medicineconference, held in Bangkok.
The initial program culminated with the 1st Thai /International EM conference. The local response was
overwhelming with attendees far out strippingexpectations. Less surprising was the willingness ofkey speakers to come from around the globe tosupport the development of their specialty in a newcountry.
Relationships have been maintained with on-goingsupport for the resident research conferences,workshops in crisis resource management and directteaching when in country. Many of the originalexpatriate supporters have continued to stay closelyinvolved and many FACEMs have devoted time toassisting the Thai association fully develop theirspecialty. As well as alumni from RMH, contributorsinclude Glenn Harrison, Sol Zalstein and AlastairMeyer; fellows very familiar to IEMSIG include AnneCreaton, Marian Lee and Shane Curran.
Given a strong foundation, support from governmentin both Australia and Thailand and the enormousenthusiasm of the Thai doctors, it is unsurprising thata fully fledged speciality has been established soquickly. The future of EM in Thailand involves theconsolidation of specialist numbers as there iscurrently only a handful in the country. With manyactive residential programs this will soon be rectifiedbut current demand is high. Thailand is also wellplaced to be a regional leader in EM. Thai consultantshave been active in support for the speciality inneighbouring countries. Several of these are likely tohave a slower rate of development but should begreatly encouraged by what has been achieved inThailand.
IEMSIG | 21
The opportunity to host an overseas colleague in yourED is both a privilege and a pleasure, with thepotential for both parties to gain significantly from theexperience.
Last year I and the ED team at the Royal Children’sHospital (RCH) hosted Dr Aye Thiri Naing, aconsultant paediatrician from the Yangon Children’sHospital (YCH) who had just finished the trainingprogram for DipEM supported by ACEM. We werelucky in that we already knew Aye Thiri Naing,having been to Yangon and taught with her theprevious year. We had also been to her hospital anddepartment and had a good understanding of thechallenges she faced in developing paediatric EM inMyanmar. We were pretty certain that we couldprovide a professionally and socially successfulattachment for her. Achieving a successfulattachment, though, takes a bit of planning, andhaving done this a few times now, I would like toshare a few thoughts:
“The right person to the right place at the right time”principle is key. Aye Thiri Naing was indeed the rightperson: highly motivated, smart, committed to EMand in a senior position in the ED of the YCH.Knowing whether the proposed visitor is the right
person can bedifficult,especially if youhave not metthem. Personalreferences andrecommendationsare helpful but myadvice is alwaysmeet them first ifpossible.
Were we the rightplace? Well ofcourse my totallyunbiased andobjective opinionis “Yes”!!
Realistically though, many institutions around theworld could have hosted Aye Thiri Naing successfullyin a professional sense. What made Melbournedifferent was the social links that she already hadhere, specifically with people like Shona McIntyreand Michael Augello who had spent an extendedtime in Yangon. Clearly a comfortable, relaxed,interactive guest who feels welcome will absorb farmore than the alternative.
Professionally at the RCH we could offer Aye ThirNaing the chance to see a lot of what she had askedfor. There were examples of clinical medicine, triage,trauma team function, critical incident management,debriefing, registrar teaching, clinically basedresearch, and a whole range of other ED functions.Not all of these would be immediately relevant to herdepartment in Yangon but maybe some would be,maybe some would be aspirational and maybe shewould see some things best avoided!! We werecertainly aware the RCH could be seen as being tootertiary, too high tech, too well resourced to be ofuse, so visits to other hospitals in Sunshine andGeelong were organised to give balance.
And finally it was the right time. Emergency medicinein Myanmar, although still embryonic, wasdeveloping quickly with backing from theGovernment, ACEM and other professional bodies.People of influence and leadership were realising thebenefits of an effective ED with well trained staff andstrong leadership. Paediatric EM needed early supportand strong leadership so as to not lag behind, as ithas in a number of countries. Aye Thiri Naing andher department were ripe with opportunity!!
Having got the right person to the right place at theright time, the rest is forms, funding, logistics, forms,committees, visas, and of course more forms. Eachinstitution and State has different rules andregulations, none of which are insurmountable, but tocarry it off does take a bit of knowledge, time andpersistence – which of course an emeritus directorlike me has aplenty.
20 | IEMSIG
Myanmar: Royal Children’s Hospital in Melbourne supports MyanmarSimon [email protected]
Thailand: Emergency Medicine update
Jonathan [email protected]
2010 CRM course faculty and students
I am now into my 4th year living and working in Dili,Timor Leste (in two stints since 2009), long enough tosee a number of changes.
The Timor Leste health system now is very differentto 5 years ago and one of the more obvious changesis the number of Timorese doctors. There arecurrently approximately 850 Timorese doctors whichis almost a 20 fold increase since 2009 and this greatopportunity (and great challenge) has driven changesto the program I work for. The program goals are stillaround postgraduate medical education,strengthening in-country medical education capacityand hospital Quality Improvement but the program(at the request of the MoH) now has much more of afocus on Post Graduate Year 1 – 2 junior doctoreducation. QI (the systems change stuff) is stillhappening in the ED and elsewhere and it is still hardand still limited by systemic factors includingaccountability that need a hospital wide (or wider)approach. Maybe 2015 will be the year the ducksline up for some of that. Working towards thoseducks line up is probably the most important andeffective thing to do from a QI point of view, even iftechnically some would not see it as QI.
In the ED there are more medical staff and someshow an interest in staying in ED. Dr Todi will go toPNG for MMedEM next year, so there is a long termplan for department leaders. So a big shout out toColin Banks!
The major collaboration with Australasian FACEMsthis year has been in starting ELS courses, with the
ELS course forming a component of the junior doctortraining program. We had 2 visits from ELS trainersthis year. The plan is for two more next year. And abig shout out to Phil Hungerford and the ELS team!
Also a big thank you to the SMACC Gold team forlive streaming the conference into Timor Leste.
My role in the team has changed. I am now teamleader for a team of five specialist expatriateclinicians covering ED (me), anaesthesia, surgery,obstetrics and paediatrics. The much greater programplanning, implementing and managingresponsibilities do take some time away from EDwork but I still manage to get time in the ED everyday. Personally, the program redesign and teamleader position has led to a big learning curve onprogram design, monitoring and evaluation (M&E),etc, also the ways of Department of Foreign Affairsand Trade, so I feel professionally enriched - and a bittired.
Socially, Dili is a great place for family life with goodbeaches in town and fantastic beaches nearby. Thecycling in the nearby hills is great. And every year asDili changes and builds the hassles of domestic lifeare reducing.
Antony Chenhall is Team Leader, Australia Timor-Leste Program of Assistance in Secondary Services(ATLASS II). This is an Australian Government fundedprogram, delivered by the Royal Australasian Collegeof Surgeons (RACS) at Hospital Nacional GuidoValadares, Dili, Timor Leste.
Phone: +670 7756 2340. Skype: chenhall.aj
IEMSIG | 2322 | IEMSIG
Timor Leste: An update from DiliAntony [email protected]
Dr Pairoj in the Sim Centre Rajavithi Hospital ED, Bangkok
The Alfred-Hue Emergency Care Project wasdelivered by the Emergency and Trauma Centre staffof the Alfred Hospital in Melbourne, in Hue,Vietnam in 2013 and 2014. The completion of thisproject was made possible through the generoussupport of the ACEM International DevelopmentGrant (2013).
Emergency medicine is only just beginning todevelop in Vietnam. In March 2010 the first annualVietnam Symposium in Emergency Medicine washeld in Hue, Vietnam. In April 2012 two AlfredHospital Critical Care Nurses visited Hue UniversityHospital emergency department to provide training.Hue University Hospital has 300 beds and is usuallyovercrowded.
Important gaps identified within the emergencydepartment during a 2012 visit by Alfred emergencystaff, included: no triage system; no systematicassessment of patients; a lack of emergency medicineand emergency nursing knowledge; the under-utilisation and maintenance of equipment; andlimited education programs.
The primary aim of the Alfred-Hue Emergency CarePartnership Project was to develop the capacity toimprove emergency care in Hue. In September2013 and again in February 2014, Alfred teams oftwo emergency physicians and two emergency,critical care trained nurses delivered two weekprograms in Hue University Hospital and HueCentral Hospital. For each visit, there were morethan twenty emergency medical and nursing
participants. Following the delivery of the AlfredEmergency and Trauma Team Training Manual,translated into Vietnamese, the program consistedof predominantly emergency department bed-sidetraining with a two day formal training component.The focus of the program was on emergency triageand the systematic and team-based approach tomanaging the seriously ill or injured patient. Therewas large emphasis on scenario-based and realpatient-based learning. Evaluation was conductedvia written examinations, with formal and informalobservation of emergency scenarios. Self-ratingquestionnaires demonstrated that the all participantsbelieved they had improved across the key skills inmanaging the critically ill or injured patient.
In addition to the delivery of the Project in Hue,one emergency physician and two emergencynurses also attended the annual emergencymedicine conference for 2014, this time at Cho RayHospital in Ho Chi Minh City in early March, wherethe Alfred team joined with a large, predominantlyU.S.A. faculty and delivered skill stations focusedon the team-based approach to the assessment andmanagement of the severely injured patient.
The Project was also an excellent opportunity forcollaboration between the key emergency carestakeholders in Vietnam and emergency physiciansand emergency nurses from Australia. It is intendedthat there will be further engagement in the nearfuture in an effort to further develop emergency carecapacity in Vietnam.
Vietnam: The Alfred-Hue Emergency Care Partnership ProjectGerard O’[email protected]
The ACEM Annual Scientific Meeting in December2014 saw Ramesh Maharjan, one of the first two EPsin Nepal, present on “Nepal graduates their firstemergency medicine specialists”. (See his abstract inthis issue.)
This is the outcome of many years’ work, some ofwhich has been chronicled in IEMSIG Newsletterssince 2007 (see below).
The three years of the Doctorate of Medicine inEmergency Medicine program of the Institute ofMedicine at Tribhuvan University have been
supported by a large group of Australian and NewZealand emergency doctors. Contributions variedfrom days to months, all making a difference.
Thanks are extended to Sanj Fernando, PeterFreeman, Adrian Goudie, Jamie Hendrie, JoannaKoryzna, Tony Mattick, Mark Monaghan, TomMorton, Guru Nagaraj, Mike Nichols, BrianO’Connell, Jennifer Rush, Athol Steward, Ryan Tan,Ros Taylor, Kavita Varshney, Gina Watkins, MerleWeber.
Articles relating to EM in Nepal can be found in thefollowing issues of the IEMSIG Newsletter:
• Volume 3 / Issue 2 / April 2007
• Volume 5 / Issue 1 / May 2009
• Volume 7 / Issue 1 / April 2011
• Volume 7 / Issue 2 / December 2011
• Volume 8 / Issue 2 / December 2012
• Volume 9 / Issue 1 / July 2013
• Volume 9 / Issue 2 / December 2013
• Volume 10 / Issue 1 / July 2014
IEMSIG | 2524 | IEMSIG
Following the success of recent programs deliveredin Mongolia, the IEC (Initial Emergency Care)Program is planned to be delivered in Mongoliaagain in 2015. As previously described, the programis a 3 day course given to soum (rural) doctors tointroduce the concept of emergency medicine as adiscipline as part of a developing Mongolian HealthNetwork. The program is structured similar to othercourses in that there are a combination of lecturesand workshops delivered on core emergencymedicine topics relevant to Mongolian Healthcare.This program has backing from the MongolianHealth Ministry and is hopefully going to expandinto something more detailed and permanent in thefuture. IEC is run in conjunction with other similarprojects in the fields of anaesthesia, obstetrics andgynaecology.
We are looking for interested FACEMs to helpdevelop and expand the program. In 2015 it isplanned that two teams will travel to Mongolia inmid June to deliver the course in two separateAimags (regional centres) concurrently. Previouslythe courses have been challenging to deliver due tolanguage difficulties, however they are incrediblywell received and fun to be part of. The Mongoliansare incredibly appreciative of the efforts that havebeen made thus far, and ensure that in any sparetime the true Mongolia is experienced.
It is an exciting time to be involved in a program thatwill hopefully evolve into much more in the comingyears. I look forward to hearing from anyoneinterested, and am happy to be contacted if you haveany questions.
ASIA and MIDDLE EAST
Mongolia: The Initial Emergency Care Program
Simon Smith
Nepal: Australian and New Zealand EPs support the first specialistsChris [email protected]
Ramesh Maharjan and Ajay Thapa, the first two emergencyphysicians in Nepal
The majority of the health dollars spent in India goesto the private sector and helps the disproportionatelysmall wealthy population. The World HealthOrganization estimates that only 0.9 % of GDP isspent by India’s government on health in the publicsector whereas another 4.2% of GDP is spent onprivate health care. In comparison, 8.3 % ofAustralia’s GDP is spent in the public health sectorwhile 1.2 % of GDP is spent in the private healthsector. In other words, if an Australian spends adollar for health, the government spends 8 dollars; ifan Indian spends a dollar on health, the governmentspends 23 cents.
Medical training in India occurs both in the publicand the private sector; and hence there aregovernment and private hospital training programs.
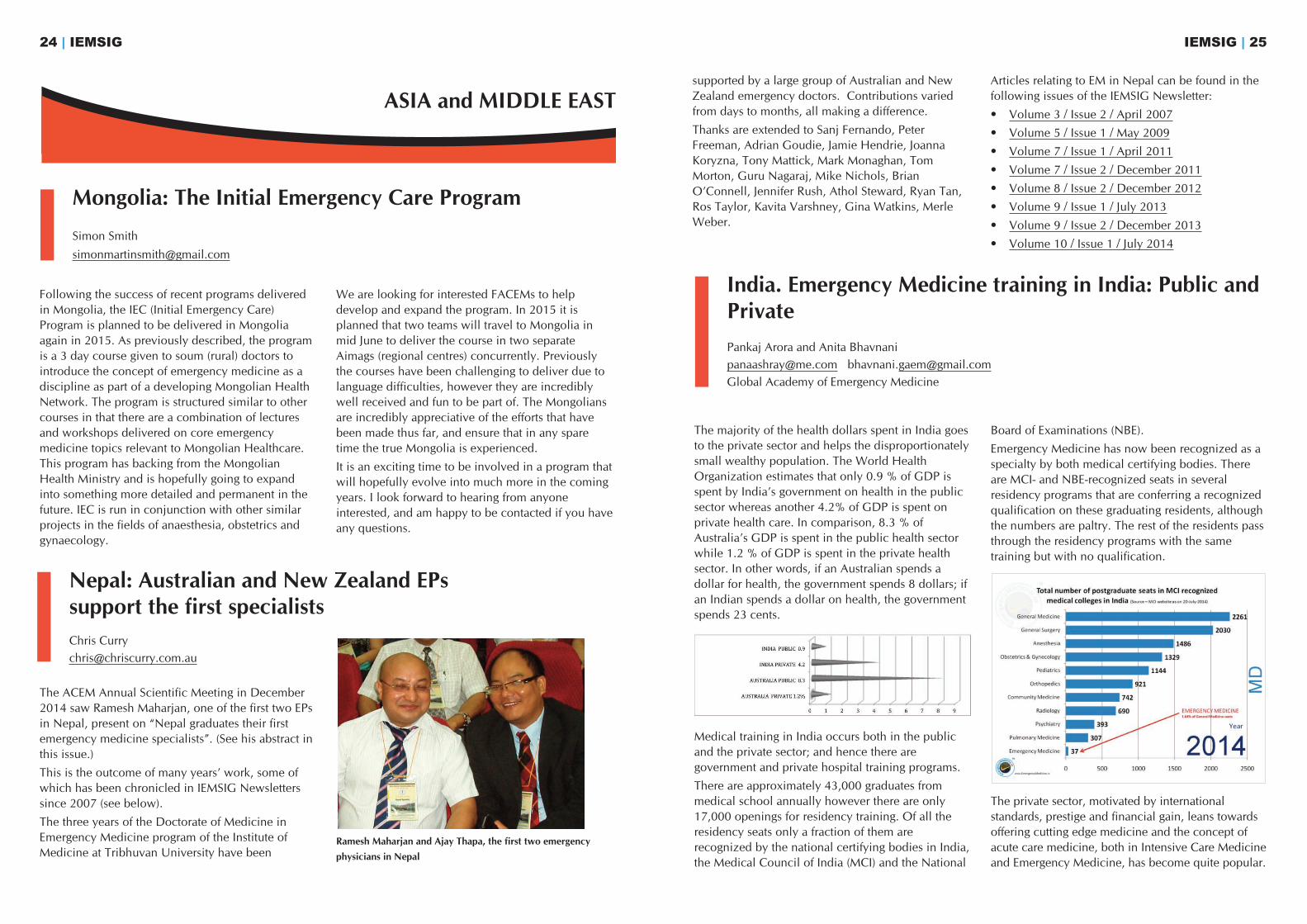
There are approximately 43,000 graduates frommedical school annually however there are only17,000 openings for residency training. Of all theresidency seats only a fraction of them arerecognized by the national certifying bodies in India,the Medical Council of India (MCI) and the National
Board of Examinations (NBE).
Emergency Medicine has now been recognized as aspecialty by both medical certifying bodies. Thereare MCI- and NBE-recognized seats in severalresidency programs that are conferring a recognizedqualification on these graduating residents, althoughthe numbers are paltry. The rest of the residents passthrough the residency programs with the sametraining but with no qualification.
The private sector, motivated by internationalstandards, prestige and financial gain, leans towardsoffering cutting edge medicine and the concept ofacute care medicine, both in Intensive Care Medicineand Emergency Medicine, has become quite popular.
India. Emergency Medicine training in India: Public andPrivatePankaj Arora and Anita [email protected] [email protected] Academy of Emergency Medicine
IEMSIG | 27
With regards to EM, the private sector has involvedinternational interest groups and foreign universitiesto create quality EM training. These programs aregraduating well-trained physicians many of whomhave become the leaders of EM in India and areinstrumental in maturing the specialty, howeverthese doctors have no national recognition orqualification. The debate in the EM academiccommunity centres around the value of having theprivate system of training which is putting outincreasing numbers of well-trained butunrecognized EPs, while the nationally-recognizedtracks are producing such small numbers of EPs thatit may very well take more than a century to havehalf the number that India requires.
Public training boasts large numbers of patientsconferring vast experience. The environmenthowever is often chaotic and overwhelming becauseof sheer volume and dearth of resources. Due to thelack of primary care medicine in this population,many patients present to the ED with primary careissues and the admission rates are as low as 25% inmany institutes. The supervisor to trainee ratio ismandated at 1:2 by the certifying bodies, but thereare few EM-trained supervisors. Residents have theopportunity to do many procedures, however thetraining is under-resourced, often leading to lack ofequipment available for procedures. Since thegraduates of these programs will hold recognizedqualifications, they will get prestigious postings andwill have the opportunity to continue in academicemergency medicine.
In the private system, the numbers of patients seenin the ED are much lower (per hospital) than in thepublic system, as low as one tenth of the numbersseen at a government hospital, with most of thepatients being referred or transferred patients.Admission rates are higher, in concurrence with theacuity, however there is significant attrition ofadmitted patients because of high cost. These EDsusually have state of the art equipment and otherspecialists that are eager to see patients and takeadmissions. There are many private trainingprograms that have international faculty and trainingin international practices. These graduates mostoften do not get national recognition orqualifications by the MCI or the NBE, but are findingwell paying jobs nationally and internationally.
Distribution of training positionsPrograms in Private SystemDNB Emergency Medicine MD Emergency Medicine International MEM Training initiated by local organisationsFEM
Programs in Public system MD Emergency Medicine inJIPMER Pondicherry AIIMS Delhi7 other government medical colleges
Major organisations involved National Board of ExaminationsVinayaka Missions UniversitySri Ramachandra Medical CollegeCMC VelloreGeorge Washington UniversitySUNY Upstate Medical UniversityUniversity of MarylandNorth Shore LIJSEMIAmerican Academy of EM IndiaGlobal Academy of Emergency Medicine
The question remains: Do we need both types ofprograms? And which is better? The follow upquestion is: what does better mean? Does bettermean better quality training? Better in the number ofgraduates trained? Better income opportunity andstatus for the graduates?
The Global Academy of Emergency Medicine(GAEM) is an academic endeavour of the AmericanAcademy of EM in India (AAEMI) and has been ableto collaborate with more than 40 EPs from ACEP,ACEM and CEM (UK), as well as several USUniversity-based programs, to commit to capacitybuilding in India. The training programs supported byGAEM are Mission Hospital Durgapur, ApolloHospital Calcutta, Jawaharlal Institute of PostgraduateMedical Education and Research (JIPMER) inPondicherry. GAEM is also working with PGI inChandigarh and Dayanand Medical College topromote EM and to build capacity.
There are several ways FACEMs can get involved: 1) participate in conferences2) participate in short courses3) approach individual organisations involved4) become a GAEM Faculty Scholar:
www.globalacademyem.org/faculty-interest.html
26 | IEMSIG
Sri Lanka: Emergency Medicine in Sri Lanka has progressed since my last report Shane [email protected]
Qatar: Emergency Medicine updateShinu [email protected]
The second intake of trainees has occurred to theMD in EM program, with the first intake now in theirthird year of training.
There is a nationwide EM strategy by thegovernment, with an extensive building programacross the country of new EDs financed by TheWorld Bank.
Ongoing education from international faculty is nowestablished. There are monthly video tutorialsfacilitated by Nilantha Lenora, an American EP. He isalso organizing a mentor program for EM trainees.
Emergency Life Care coursesThere have now been 6 sessions of the EmergencyLife Care course run, with the 200th candidatepassing in November 2014, including a doctor fromthe Maldives. November saw the first course to berun in Jaffna, with local medical staff indicating afirm desire for the course to be run there again. Apart from the mannequins we now have a full set ofequipment based in Sri Lanka owned by theSSCCEM, allowing portability of the course. Plans for2015 include taking the ELC course to Galle, and inthe second sessions in October taking it to the EastCoast.
SSCCEMActivities by the Sri Lankan Society of Critical Careand Emergency Medicine (SSCCEM) continue. InNovember 2014 there was a very successful AnnualScientific Meeting, with Professor Tony Browndelivering a keynote lecture via Skype from his livingroom! The SSCCEM ASM in 2015 will coincide withthe October sessions of the ELC course and againinvolve overseas faculty. Preliminary discussions arebeing held regarding running an ATLS course inconjunction with that ASM.
The SSCCEM has been invited to participate in theSri Lankan Medical Association annual meeting inJuly 2015 and Sally McCarthy has agreed to talk onbehalf of the Society as the international speaker.
I have recently had contact with the EPs in theMaldives about supporting their education efforts.
As always, I am keen to involve anyone who wishesto help. Opportunities include coming to Sri Lankaand teaching and/or talking at the SSCCEM ASM, orfrom home contributing to video tutorials and to thementoring program. At the moment we are short ofmentors.
Emergency medicine in Qatar has evolved rapidly inthe last decade. The primary focus of EM in Qatar isthe EDs of Hamad Medical Corporation. The ED atHamad General Hospital is the largest in Qatar, inthe largest tertiary care facility. The daily attendancestands at around 1500 patients, with around 200highly qualified emergency physicians from aroundthe world currently headed by Professor PeterCameron FACEM. Besides patient care, health careeducation and research is of paramount importance.A residency training program accredited by ACGME(Accreditation Council of Graduate Medical
Education, USA) and a postgraduate fellowshiptraining program both play a significant role indeveloping highly qualified emergency physicians toguide and support emergency health care in Qatarinto the future. Emphasis is on the delivery of carethat is on a par with that in other developedcountries of the world. The ED aspires to be a centreof excellence in the region for healthcare deliveryand medical education.
Shinu Varughese is an Acting Consultant, ED,Hamad Medical Corp, Doha-Qatar

Hashomer ED, and Merav Slotky, soon to take up theposition of ED Director at Kfar Saba Hospital.
The IAEM have an annual conference before Pesacheach year and I would encourage anyone interestedto attend. For further information I would be happy tobe contacted. The current President of the IAEM isAziz Darwashe, Director of Hadassah Hospital ED.
I must acknowledge the considerable assistance ofDanny Beneli, EP at Monash Health, who has beeninstrumental in developing the links to EM specialists
in Israel and mentoring the Israeli EPs who havecome to work in Australia.
Katz E, Ofek B, Adler J et al. Primary Blast Injury After aBomb Explosion in a Civilian Bus. Ann Surg. Apr 1989;209(4): 484–488
Halperin P, Waisman Y and Steiner IP. Development of thespecialty of emergency medicine in Israel: comparisonwith the UK and US models Emerg Med J 2004;21:533-536
IEMSIG | 29
Israeli physicians have considerable expertise in blastand penetrating trauma, burns and other injuries ofwar and terror. Israeli traumatologists such as Katz etal have even published on the likelihood andprevalence of injury after a bomb explosion on acivilian bus. In the past, Israelis have interpretedtrauma medicine as the equivalent of emergencymedicine thus hampering the development of thespecialty. However, for every person injured in apeguah or war there are many thousands that presentto emergency departments all over Israel with thesame conditions that are treated in our departmentsin Australia; infarcts, strokes, respiratory diseases,UTIs etc. The Israeli Emergency System must providefor the day to day needs of its population as well asmaintain a readiness to deal with the sad reality ofterrorism and war.
Halperin et al reported in the British Medical Journal(2004) that there were 27 EDs in Israel providingcare for 2.3 million annual ED visits. At that timemost EDs were staffed by a small number ofphysicians who called themselves emergencydoctors, with most of the staffing provided bydoctors rotating from other specialists with diversetraining backgrounds. On-call residents from medicaland surgical departments, often without directsupervision, were responsible for all patient carerelated decision-making after hours and onweekends. In 2014, little has changed; EDs remaincompartmentalised with specialties such as internalmedicine, paediatrics, obstetrics and gynaecology,general and orthopaedic surgery runningindependent and autonomous emergency rooms.The patient with an inferior infarct presenting withepigastric pain might find himself or herself beingcared for in the surgical ER by a surgical resident.
In the background, however, there has beensignificant change, culminating in the adoption of anational training curriculum by the Ministry ofHealth in late 2014. This has been driven by theIsraeli Association for Emergency Medicine (IAEM)formed in 1992. Emergency Medicine (EM) wasrecognised as a “super-specialty“ in 1999. Tobecome an emergency physician in Israel, a boardcertified physician in internal medicine, general
surgery, anaesthesiology, paediatrics, orthopaedicsurgery, or family medicine is required to undergofurther training in EM. Thus, the EM resident is aspecialist being “retrained” in the discipline of EM.Until now the EM training provided was by anacademic institution or health service with noconsensus on what to teach and what level ofknowledge should be sought from the trainee. The delivery of care to patients was potentially asfragmented as the courses offered to doctorsinterested in pursuing a career in EM.
With the adoption of a National Curriculum, allIsraeli EM trainees must complete the recognised twoyear modular Fellowship in Emergency Medicine. Itis now possible for physicians who choose EM toenter directly into the speciality without beingboarded in another. There are currently nearly 50trainees across Israel enrolled in the “direct”pathway.
I have been fortunate to work with a number oftalented and passionate Israeli EPs in writing theNational Curriculum for Emergency Medicine. It is built upon the Australasian curriculum and iscompetency based. The aim of the curriculum is toensure that all EPs trained in Israel achievecompetency in each of the core skills listed below:
1. specialty specific skills
2. personal and interpersonal skills
3. systems based practices
4. research and academic skills
5. managing emergency scenarios
6. core emergency medicine knowledge
Over the 2 years, the course is delivered in 40sessions with 240 contact hours via a combination ofhalf day and full day seminars and workshops. Thecourse director is Debra West (from Ichilov Hospital)assisted by content coordinators and theme leadersfrom across Israel. Three of the 12 theme leadersspent up to 18 months training with our own traineesat Monash Health and have returned to Israel inleadership positions; Moshe Sharist as Director orWoolfson ED, Ariel Bentacur, senior leader at Tel
28 | IEMSIG
Israel: Towards a national training programGeorge [email protected]
George Braitberg and Moshe Sharist, Director of Woolfson ED (South Tel Aviv)
George Braitberg, Aziz Darwashe, Director of Hadassah Hospital ED(Jerusalem), and Danny Beneli
2) assisting in educational projects for skills trainingand critical problem solving as part of theongoing professional development for specialistsas well as for the assistance in training the juniordoctors
3) collaborating in research projects throughSimmelweis University
4) offering secondments for trainees or specialistsfrom Hungary to be able to observe or doresearch work in Australasia.
Similar to many international areas of interest there is
no specific funding for our involvement in Hungarianemergency medicine. The opportunity exists to seekfunding through the European Union to help in thedevelopment of improved access to emergency care.
In March of 2015 there is the main Critical CareConference (SIASTOK) that is run throughSimmelweis University Hospital. This is on theoutskirts of Budapest from March 26-28th. AnyFACEM interested in attending and/ or providinginput can let me know and I can forward on orconnect you to the organising committee.
Emergency Medicine in the Netherlands has come along way from its inception in the 1990s. In 1999,the Netherlands Society of Emergency Physicians(http://www.nvsha.nl/) was formed, which has beeninstrumental in establishing a national curriculumand assessment framework. This has resulted in arobust three year training program, with partialrecognition as a specialty since 2008. Currently, anexpansion to five years is being considered.
A significant number of Dutch emergency physicianshave spent training time in various hospitals aroundAustralia and the UK. Several have even becomeFACEMs, and are expected to return to theNetherlands in the next few years.
In 2012, a group of Dutch and Australian EPsestablished a web-based CPD program, intended tohelp expand knowledge and skills for EPs aftercompletion of the Dutch EP training program. It iscalled 'MNSHA Masterclass' (Modulaire NascholingSEH-artsen) - http://www.mnsha.nl/en/. It consists of15 week, themed modules. Case-based self-study iscomplemented by web-based mentoring byFACEMs/FCEMs. There are several intense face-to-face days in which participants' knowledge isdiscussed, consolidated and challenged.
Opportunities for FACEMs include site visits andlecture schedules, as well as internet-basedmentoring of local EPs. FACEM contacts includeFemke Geijsel, Sander Manders, Kevin Lai, andNaren Gunja.
IEMSIG | 31
Hungary is a landlocked central European countrythat is full of the charm of old Europe together withthe challenges of developing a functional democracy.The population of the country is about ten millionwith approximately a fifth being based in Budapest-the capital. The current political environment ischallenging with a growth in the right wing,nationalist sector. From a political historicalperspective Hungary, along with several of theCentral European countries, is currently strugglingwith its transition between the European Union and agrowing Nationalist movement. The current concernis that aspects of Nationalist intolerance will riseagain. Several Health and Community groups areemphasising the importance of strong advocacyacross healthcare for equality, and access to care hasbeen seen as important.
Across Europe there are several differences in systemsprovided but there is an overarching organisation,EUsEM (European Society of Emergency Medicine),that works to ensure suitable collaboration andsharing of focus/ vision across the different systems.There is now a European Fellowship exam forEmergency Medicine and trainees within Hungary areable to work towards this. Currently EM is notregarded as a specialist practice in its own right andmost departments are linked to Anaesthetics and ICUas part of a Critical Care hub. The ability to developdoctors interested in acute and emergency care isdifficult owing to the lack of structure in training andthe limited number of specialists available. I have hadthe opportunity to spend two separate weeks last yearin Budapest to assist with some of the prehospitaleducation provided for the first response paramedicteams as well as to develop some links with theUniversity Emergency Department based in Budapest.
All of my communication is in English and most ofthe doctors are able to understand Englishadequately. Certainly an understanding andenthusiasm to use Hungarian is an advantage but itremains a tricky language to master- so English is fine.
The pre-hospital EMS is strong in some places and theopportunity for emergency physicians to be tasked toa prehospital setting is common. Final year medicalstudents often work as paramedics within EMS andhospital doctors will continue to provide additionalshifts to cover this work. Budgets are struggling andthe need for innovation and change in how thehealthcare system is coordinated, structured anddelivered has been identified but not funded.
During the years of Soviet domination in Hungary(1947-89) Oxyology was developed and this specialtyrepresents emergency medicine. It was described byone of the early pioneers of acute medicine withinthe country- Dr Aurel Gabor. He outlined the needfor urgent clinical care to be based upon soundscience and evidence and formulated Oxyology fromthe Greek oxys (quick) and logos (science).
The main Medical School in Budapest is Simmelweis.This academic institution is enthusiastic about agrowth in collaboration for developing the structuresof EM within the city and country. It is very early daysin developing this supportive link so assistance fromenthusiastic clinicians across the emergency spectrumwould be great. Paramedic and nursing educatorsrelated to emergency care are similarly helpful.
The opportunities for FACEMs who wish to helpsupport Hungarian emergency healthcare include:
1) mentoring the local emergency specialists andhelping in their strategic planning for servicedelivery
30 | IEMSIG
EUROPE
Hungary: The study of Oxyology and Central European challengesPeter [email protected]
Netherlands: Emergency Medicine updateNaren [email protected]
For the last 4 years Mardi has been living andworking in rural Kenya as the country's only PEMphysician. Kijabe Hospital is recognised as a nationaltraining site for the University of Nairobi in generalsurgery, pediatric surgery, orthopedics, nurseanesthesia, pediatric anesthesia and pediatricneurosurgery.
In Kenya, with 40 million people, there are 4 ICUs - aperpetually full public one and a private expensiveone in Nairobi, one in Eldoret 8 hours away, and oneat our hospital. Currently the only place to train inemergency and critical care is internationally. So weare keen to train pediatricians who will be workingrurally in emergency and critical care, and in how toset up a rural hospital to be able to provide criticalcare.
For the last 2 years Mardi has been liaising with theUniversity of Washington and with the paediatricintensivists and chair of pediatrics at the University ofNairobi to work on developing sub-Saharan Africa'sfirst 2 year fellowship in Pediatric Emergency andCritical Care.
Kenya has 3 pediatric intensivists, trained in Europeor South Africa, and now 2 PEM physicians, Mardiand Arianna Shirk who has just finished fellowship inthe USA. So we are looking for doctors to assist us asvisiting faculty in PEM and PCCM. Can you help?
Mardi Steere FRACP FACEP is Medical Director atAIC Kijabe Hospital. She was previously an EP atWomen’s and Children’s Hospital and with MedSTARretrieval service in Adelaide. www.kijabehospital.org
Jane Cocks FRACP FACEM FCICM works at Women’sand Children’s Hospital and at MedSTAR retrievalservice in Adelaide.
IEMSIG | 33
‘Dumela’ (Hello) from Gaborone.
Thanks for your interest in EM in Botswana. As ofJanuary 2015 there are 8 local emergency medicinetrainees and still only one emergency physician (me)in the country. Four of these are advanced trainees,moving temporarily to South Africa, as part of theBotswana program, to attempt the SA FCEM (SouthAfrican Fellowship of the College of EmergencyMedicine) in the next 18 months. The other 4 havejust excitedly started the program. I am hopeful thatBotswana will have its first local emergency physicianby 2016.
I work full time here for the University of Botswanaheading a team of two Cuban ICU specialists, a nurseanaesthetist running BLS and ACLS courses at theUniversity of Botswana, and many interested localhealth professionals in EMS, ICU and A&E. In August2014 the University of Botswana held the firstgraduation of locally taught medical studentsgraduating to doctors. They are now working with usas interns. There is also a formal rotation for EM inthe A&E for the local University of Botswana 5th yearmedical students. There is increasing interest fromInternational (especially Australian) medical studentsapplying for medical electives in EM and ICU here.
There will be two ACEM advanced trainees inBotswana in 2015, doing approved terms here. Theminimum time frame to consider for this is 3 months.I am very grateful for past and present ACEM
colleagues coming to assist me. Senior EM registrarsor FACEMs reading this who are considering usingtheir LSL, annual or study leave and would like toteach any of the following - basic sciences,ultrasound, EMS, retrieval skills, paediatric EM orcritical care, team work and leadership, clinical EM,simulation, or any type of research - would be muchappreciated. A minimum of 6 weeks is required, toallow for registration, orientation and familiarization.
If you or anyone you know would like to come andassist in the next 2 years, it would be a perfect timeframe. If you would like an African medicalexperience with little malaria, relatively peacefulsurroundings (especially compared to its neighbours),no ebola, lots of trauma, teaching and procedures ...please let me know!
If you enjoy child-friendly safaris, fabulous sunsets,great BBQs, SA wine and Namibian beer, goodimported food, 4W driving or visiting world heritagesites close by (Okavango Delta and Victoria Falls) thiswould help too...
For more insight, please visit this videohttp://vimeo.com/76859965Megan Cox is Assistant Program Director and ActingHead of Department, Department of EmergencyMedicine, Faculty of Medicine, University ofBotswana +267 76574766
32 | IEMSIG
Kenya: Can you help a Paediatric Emergency and Critical Care program?Mardi Steere and Jane [email protected] [email protected]
AFRICA
Botswana: Opportunities for TESL users and ACEM advanced traineesMegan Cox [email protected]