comparison of carbon-11-acetate with fluorine-18-fluorodeoxyglucose for delineating viable...
TRANSCRIPT

,ACC Vol. 22, No . 6November 15 . 1993 : 1 587-97
Comparison of Carbon- I l-,".cetate
Auorline-18-Fluorodeoxygliacose Or rel .̀ "ZiAng V!z:)Ie Myocardium byPositron Emission TomographyROBERT J. GROPLER, MD, FACCM EDWARD M . GELTMAN, MD, FACC,tKONDAPURAM SAMPATHKUMARAN, DQ* JULIO E . PEREZ, MD, FACC,tKENNETH B. SCHECHTMAN, PHD,t ANDREA CONVERSANO, MD,*BURTON E . SOBEL, MD, FACC St STEVEN R. BERGMANN, MD, PIED, FACC,tBARRY A. SIEGEL, MD*Saint Louis, Missouri
Objectives. This study was designed to determine in patientswith advanced coronary disease whether prediction of recovery ofmechanical function after coronary revascularizallon could beaccomplished more effectively by positron emission tomography(PET) with carbon-11( 11C)-acetate than by PET with fluorine-18('"F)-fluorodeoxyglucose .
Background. Results of previous studies have demonstratedthat preservation of myocardial oxidative metabolism (measuredby PET with "C-acetate) is necessary for recovery of systolicfunction after coronary revascularizHon .
Methods. Myocardial oxidative metabolism was quantifiedbefore revascularization in 34 patients by the analysis of the rateof myocardial clearance of 11C-acetate. Metabolism of glucose wasassessed by analysis of uptake of 18F-fluorodeoxyglucose. Receiveroperating characteristic curves for predicting functional recoverywere derived for the measurements of oxidative metabolism andglucose metabolism . In addition, criteria for prediction of recov-ery of function based on measurements of oxidative metabolismand glucose metabolism were developed and compared .
Results. Analysis of receiver operating characteristic curves
Selection of patients with impaired left ventricular systolicfunction who would benefit from coronary revascularizationrequires accurate differentiation of myocardium that is hi-bernating or stunned but still viable from irreversibly in-jured, nonviable tissue (1) . We and others have explored the
From the *Division of Nuclear Medicine, Edward Mallinckrodt Instituteof Radiology ; the t Cardiovascular Division, Department of Internal Medicine ;and the Division of Biostatistics, Washington University School of Medicine,Saint Louis, Missouri. . This work was supported in part by a grant from theEdward Mallinckrodt, Jr. Foundation, Saint Louis, Missouri and by GrantsHL17646 (SCOR in Coronary and Vascular Diseases) and HL13851 from theNational Heart, Lung, and Blood Institute, National Institutes of HealthBethesda, Maryland . Dr. Gropler is the recipient of a Clinician-ScientistAward from the American Heart Association, Dallas, Texas .
Manuscript received October 2,1992 ; ievised manuscript received June 7,1993, accepted June 17, 1993 .
Address for correspondence : Dr. Robert J . Groplet, Mallinckrodt Institute ofRadiology, 5 10 South Kingshighway Boulevard, Saint Louis, Missouri 63110 .
01993 by the American College of Cardiology
MYOCARDIAL ISCHENHA
indicated that estimates of oxidative metabolism were more robustin predicting functional recovery than were estimates of glucosemetabolism (p < 0 .02) . Moreover, threshold criteria with "C .act-tale exhibited superior positive and negative predictive values(67% and 89%, respectively) than did the criteria with ' OF-fluorodeoxygincose (52% and 81%, respectively), p < 0.01 . Insegments with initially severe dysfunction, estimates of oxidativemetabolism tended to be more robust than estimates of glucosemetabolism in predicting functional recovery . Moreover, in suchsegments, the threshold criteria with "C-acetate tended to exhibitsuperior positive and negative predictive values (85% and 87%,respectively) than did the criteria with "T-fluorodeoxyglucose(72% and 82% respectively), although statistical significance wasnot achieved.
Conclusions . In patients with advanced coronary artery dis-ease, the extent to which functional recovery can be anticipatedafter coronary revascularization can be delineated accurately byquantification of regional oxidative metabolism by PET with11 C-acetate.
(J Am Coll Cardiol 1993,22 :1587- .97)
1587
feasibility of utilizing cardiac positron emission tomography(PET) for this purpose . Initial clinical efforts have focusedon quantifying myocardial utilization of glucose with theglucose analogue fluorine-l84uorodeoxyglucose in patientswith left ventricular dysfunction attributable to chronic coro-nary artery disease (2,3) . Persistent myocardial utRization ofglucose, reflected by accumulation of "F-fluorodeoxyglucose,has been shown to predict restoration of function after coro-nary revascularization . Conversely, diminished utilization con-cordant with the reduction in perfusion has been thought to beindicative of irreversible injury (2-6) . Unfortunately, however,PET with "3F-fluorodeoxyglucose overestimates the extent oftissue viability in as many as 32% of myocardial segments andunderestimates tissue viability in up to 22% of segments(2,3,6) . These discordances may in part reflect differences inthe pattern of substrates presented to the heart at the time ofmyocardial imaging with 18F-fluoredeoxyglucose . These re-
0735-100,7193/56 .00
1 588
GROPLER ET AL .VIABLE MYOCARDIUM DETERMINED BY "C-ACETATE TOMOGRAPHY
suits also probably reflect the failure of uptake of "F-fluorodeoxyglucose delineated with PET to identify meta-bolic processes underlying viability sufficient for restorationof myocardial systolic function (7) .
Under physiologic conditions, myocardial oxidative me-tabolism is required to support contractile function (8,9) . Inmyocardium rendered ischemic but ultimately salvaged byreperfusion, maintenance of oxidative metabolism is re-quired for subsequent functional recovery (10,11) . We andothers (12-14) have shown that PET with "C-acetate canaccurately quantify regional myocardial oxidative mc .abo-lism under conditions of normoxia, ischernia or reperfusionand under diverse ventricular loading conditions, Further-more, maintained oxidative metabolism has been found to bea more robust descriptor of functional recovery comparedwith maintained glucose utilization under several circum-stances (15,16). Accordingly, it appeared likely that differrendation of dysfunctional but viable myocardium from non-viable tissue could be accomplished more effectively byquantification of regional myocardial oxidative metabolismby PET with "C-acetate than by measuring myocardialutilization of glucose by PET with ' 8F-fluorodeoxyglucose .
MethodsStudy patients. The protocol was approved by the Hu-
man Studies Committee and the Radioactive Drug ResearchCommittee of Washington University School of Medicine,and written informed consent was obtained from each pa-tient. Thirty-four patients (26 men and 8 women ; mean age60 years range 30 to 77) who had left ventricular wall motionabnormalities secondary to angiographically documentedcoronary artery disease were studied . Twenty-one had bus-tamed at least one myocardial infarction from I I days to 10yon before enrollment in the study . In 17 patients, themyocardial infarction had occurred at I month before enroll-ment, Two patients had undergone coronary artery bypasssurgery 18 and 4 years earlier, respectively . Because thekinetics of "F-fluorodeoxyglucose in myocardium. have notbeen well delineated in patients with diabetes mellitus,patients with known diabetes were excluded .
CWTAIW catheterization and selective coronary angiogra-phy followed by coronary revascularization (coronary arterybypass stulery or coronary artery angioplasty) were per-Irmod in all patients. Eight had angiographically definedlesions in a single vessel, 8 had lesions in two vessels and 18had lesions in three vessels . In 24 patients, coronary arterybypass VaRing 'Ams performed, and 10 underwent percuta-Womus transluminal coronary angioplasty, The adequacy ofthe revascuMiation, procedure was verified by review ofthe operative reports documenting the successful placementof bypass grafts and, in the case of coronary angioplasty, byROgiW*ic documeitation of successful balloon dilation .None of the patients exhibited signs or symptoms of acutemyocardial infarction during the interval between the per-
W .̀C Vol. 22, No, 6November 15, M3 :1587-97
formance of the initial PET and waii motion studies andperformance of the follow-up wall motion stiv . 1y .
Assessment of ventricular function. For each patient, re-gional systolic function was assessed before (mean 18 days,range I to 65) and after (mean 2.0 months, range 0.5-7)coronary revascularization . In 20 patients . regional systolicfunction was assessed before and after revascularization bytwo-dimensional echocardiography . In six patients, contrastventriculography was performed before and two-dimen-sional echocardiography after revascularization . In six pa-tients, radionuclide ventriculography was performed beforeand after coronary revascularization . Two patients under-went left ventricular ancury%niectomy at the time of revas-cularization (see later) .
Regional systolic function was quantified as recentlydescribed (15,16). For the purposes of analysis, the leftventricular myocardium was segmented into eight regions(septal, anterobasal, anterior, apical, lateral, posterolateral,inferior and inferoposterior). With all three modalities (echo-cardiography, radionuclide ventriculography and contrastleft ventriculography), regional systolic function was gradedaccording to the scoring system recommended by the Amer-ican Society for Echocardiography (I = normal, 2 = hypo-kinetic, 3 = akinetic, 4 = dyskinetic and 5 = aneurysmal)(17). The wall motion analyses were performed by twoobservers blinded to both PET and clinical data . The averagewall motion score reflecting values assigned by both observ-ers was tabulated for each segment in each study .
As judged from the wall motion analyses, myocardialsegments were defined as: 1) normal ; 2) dysfunctional butviable (initially dysfunctional segments [wall motion scoree21 that subsequently exhibited an improved wall motionscore of at least one full grade after revascularization) ; or3) nonviable (persistently dysfunctional segments that didnot exhibit functional improvement) (15,16) . In the twopatients who underwent left ventricular aneurysmectomy,only those segments that were resected were included in theanalysis because of the potential for misregistration of seg-ments identified before and after revascularization conse-quent to the altered left ventricular geometry that typicallyoccurs after aneurysmectomy . Extensive transmural necro-sis and scarring were confirmed by gross and microscopicanalysis in each . Thus, the segments that were resected wereclassified as nonviable. In patients who underwent coronaryartery bypass surgery, the interventricular septum was ex-cluded from analysis because of abnormalities in contractileperformance independent of ischemia that occur frequentlyin this region after surgery .
Tomographic assessment of perfusion and metabolism .Tomographic assessments of perfusion and metabolism wereperformed in all patients before coronary revascularization(mean 12 days, range I to 38) . Positron emission tomo-graphic studies were performed on average within 8 days(range 1 to 56) of the assessments of systolic function .Tomographic studies (IN that delineated the effects ofrevascularization on myocardial perfusion, oxidative metab-
JACC Vol . 22, No. 6November 15 .1993 : 1 587-97
VIABLE MYOCAUSIUM DETERMINED BY 00C.ACETATE TOMOGRAPHY
olism and ghtcose .utilization in dysfunctional but viable andnonviable myoca -Aium have previously peen reported for 16of the patients in the current study .
The methods used to measure regional myocardial perfu-sion, oxidative metabolism and utilization of glucose havebeen reported recently in detail (15,16) . In brief, PET studieswere performed on standard PET instrumentation availableat Washington University (18-20). All subjects were studiedin the postprandial state after the consumption of a highcarbohydrate meal 2 to 3 h before and 75 g of glucose(Trutol) I to 2 h before the administration of ' 8 17 -fluorodeoxyglucose (15,16) . An initial transmission scan wasperformed to correct subsequent emission scans for attenu-ation . Carbon-i1-acetate (0.25 to 0.40 mCi/kg) was thenadministered intravenously, followed by an 1,800-s list modedata collection . Subsequently, ' 8 F-fluorodeoxyglucose (9 to10 mCi) was administered intravenously, with an 1101s listmode data collection performed 45 min later . To ensure thateach patient was positioned consistently within the PETsystem for all data collections, position was checked withthe use of a low energy laser and indelible marks placed onthe torso .
Regional myocardial perfusion in relative terms wasbased on the early myocardial uptake of "C-acetate. Resultsof previous studies by our group and others (21,22) havedemonstrated that the regional distribution of activity withinthe myocardium from 60 to 180 s after the administration of"C-acetate accurately reflects regional myocardial perfusionin relative terms. Myocardial oxidative metabolism wasquantified by determining the myocardial turnover rate con-stant of acetate (k,), which reflects the rate of clearance of"C activity from myocardium after the administration of"C-acetate and correlates closely with regional myocardialoxygen consumption (i2-14) . Regional myocardial utiliza-tion of glucose was assessed on the basis of compositeimages of relative "F-fluorodeoxyglucose activity .
Analysis of tomographic images was performed with anoperator-interactive method developed and validated in ourlaboratory (23). All myocardial images were reformattedfrom the transaxial orientation to true short-axis views, withthe heart divided into 8 to 12 tomographic slices on whichcircumferential profiles of myocardial uptake of "C-acetate,k, and '8F-fluorodeoxyglucose activity were generated foreach. The left ventricular myocardium was segmented as forstudies of wall motion, with distal slices comprising the leftventricular apex, middle slices comprising anterior, lateral,inferior and septal segments and basal slices comprising theanterobasal, posterolateral and inferoposterior segments . Byreorienting the myocardial images and limiting the segmen-tation of left ventricular myocardium to eight large seg-ments, the risk of misregistration of the tomographic esti-mates of perfusion and metabolism with the measurementsof regional wall motion was reduced .
Average values for myocardial uptake of "C-acetate, k,and 1117-fluorodeoxyglucose activity were calculated for eachsegment. Carbon-11 acetate myocardial uptake and 18F-
GROPLER ET AL
1599
fluorodeoxyglucose activity were normalized to peak myocar-dial activity for "C-acetate and 18F-fluorodeoxyglucose,respectively, to yield relative values for myocardial bloodflow and utilization of glucose . In addition, myocardialutilization of glucose was normalized to blood flow withineach segment by dividing normalized "F-Ruorodeoxy-glucose activity by normalized myocardial uptake of "C-acetate activity for the same segment, an approach analo-gous to that described by others (24) .
Data analysis. Generation of receiver operating charac-teristic curves . Receiver operating characteristic curves forpredicting functional recovery were derived from the indi-vidual estimates of regional myocardial oxidative metabo-lism, glucose metabolism and glucose metabolism normal-ized to flow in the dysfunctional segments . The shape ofthese curves reflects the performance of the measurementsof oxidative metabolism and glucose metabolism in predict-ing functional recovery over a wide range of observedvalues .
Generation of foinographic criteria of myocardial viabil-ity. Although receiver operating characteristic curve analy-sis is useful for evaluating the performance of a test, for thepurposes of clinical decision-making, threshold values mustbe used. Consequently, tomographic criteria of tissue viabil-ity and of nonviability were developed by referencing valuesfor oxidative metabolism and utilization of glucose to meanvalues obtained in control subjects for each of the eightsegments . The control group consisted of 10 healthy normalvolunter -s (9 men; mean age 24 ± 3 years) with no history ofand a low likelihood for coronary artery disease . As judgedfrom measures of myocardial oxidative metabolism, dys-functional but viable myocardium was considered presentwhen values for k, were within 2 SD of the mean value for aparticular segment in the control group . Conversely, non-viable myocardium was considered present when values fork, were lower than the mean value minus 2 SD in the controlgroup. These criteria were chosen on the basis of theobservation that in patients with chronic coronary arterydisease, the level of oxidative metabolism exhibited bydysfunctional but viable myocardium was comparable tothat exhibited by normal myocardium. In contrast, the levelof oxidative metabolism exhibited by nonviable myocardiumwas significantly lower than that in either normal or dysfunc-tional but viable myocardium (16) . In the control subjects,mean values and standard deviations for k, ranged from0.052 ± 0.007 min- ' in apical segments to 0.057 ±0.006 min - ' in inferior segments . Criteria using measure-ments of myocardial utilization of glucose to identify viablemyocardium were analogo-is to those developed and vali-dated by others (2,3) . Dysfunctional but viable myocardiumwas defined by values for regional myocardial utilization ofglucose within 2 SD of the mean value in the control group(mean values ranged from 85 ± 11% in septal segments to94 ± 7% in posterolateral segments) . Values for myocardialutilization of glucose normalized to flow that were >2 SDabove the mean value in the control group were defined as
JACC Vol . 22, No . 6VIABLE MYOCARDIUM DETERMINED BY 11C-ACETATE TOMOGRAPHY
November 15 . 1993 : 1 587-971590
GkJPLER ET AL .
indicative of dysfunctional but still viable myocardium . Inthe control subjects, mean values ranged from 0 .92 ± 0.07 ininferior segments to 0 .99 ± 0.14 in anterobasal segments .Conversely, reductions in myocardial utilization of glucose(values >2 SD below the mean value in the control group)that were not associated with increased utilization of glucosenormalized to flow were defined as indicative of nonviablemyocardium .
S ys . Continuous variables were assessedin terms of mean values and standard d^.viations. Thecomparisons of paired frequency data were performed with acontinuity-corrected McNemar test . Receiver operatingcharacteristic curves were compared with the methods ofHanley and McNeil (25,26) . With this approach, it is as-sumed that information is conveyed by a one-dimensionalvariable X, with tow values of X su esting that tissue isnonviable and high values suggesting that it is viable . Then ifN represents the distribution of the X values that areassociated with nonviable tissue and V represents the distri-bution of the X values for viable tissue, the area A under thereceiver operating characteristic curve is given by :
A
Probability (V > N) .
With this formulation, Hanley and McNeil (25) demon-stratcd that the area under the receiver operating character-istic curve along with the standard error of that area can becomputed with a standard Wilcoxon statistic . This is be-cause the Wilcoxon statistic is by definition a measure of theproportion of observed X values that are associated withviable tissue that exceed a given X value that is associatedwith nonviable tissue, summed over all X values that areassociated with nonviable tissue . Thus, the Wilcoxon statis-tic is completely analogous to the area under the receiveroperating characteristic curve as just described . With thisformula, it is a simple matter to compute the standard error(SE) of the difference between the areas under two uncorre-lated receiver operating characteristic curves as ,
SE (Al A2) $ 'SE' (A l) + SE 2 (A2),
and thereby to test the hypothesis of the equality of the areasunder two uncorrelated receiver operating characteristiccurves . In their second report, Hanley and McNeil (26)extended this computation of standard errors in a naturalway to the case that applies herein, where the receiveroperating characteristic curves being compared are derivedfrom the same subject and are therefore correlate± . Proba-bility (p) values < 0.05 were considered significant .
ResultsSystolic As judged from the wall motion analy-
ses, 131 segments were identified as normal and 141 seg-ments as dysfunctional . Twenty-five of the dysfunctionalsegments were excluded from fin-her analysis because of1) location in interveatricular septum in patients undergoingcoronary artery bypass surgery (n = 15) ; 2) location not
completely within the field of view of the scanner duringtomographic imaging (n = 4) ; 3) incomplete revasculariza-tion (n = 4) ; and 4) failure to completely characterizesystolic function before and after coronary revascularization(n = 2) . Among the 116 dysfunctional segments that wereincluded in the analysis, 46 were classified as dysfunctionalbut viable and 70 as nonviable . Before revascularization,both types of dysfunctional myocardium exhibited similarmechanical impairment, with dysfunctional but viable myo-cardium exhibiting an average wall motion score of 2 .72 ±0.74 and nonviable myocardium showing an average wallmotion score of 2 .68 ± 0.91 (p = NS) . After coronaryrevascularization, segments classified as dysfunctional butviable exhibited improvement in systolic wall function (inaccordance with our original definition), with au averagewall motion score of 1 .28 ± 0.56. Conversely, regional wallmotion in dysfunctional segments classified as nonviable didnot change appreciably as evidenced by an average wallmotion score after revascularization of 2 .08 ± 0.89 (meanchange 0.01 ± 0 .30). Severe systolic dysfunction waspresent in 26 segments (from 13 patients) classified asdysfunctional but viable ; these segments exhibited akineticto frank aneurysmal changes (wall motion score ~3) beforecoronary revascularization . Thirty-one segments (from 14patients) classified as nonviable exhibited similarly severeimpairment of function before coronary revascularization .
To determine the reproducibility of the estimates ofregional systolic function, the paired wall motion studiesfrom 10 paticats (six paired echocardiograms, two pairedradionuclide ventriculograms and two contrast left ventric-ulograms paired with echocardiograms) were chosen atrandom and reanalyzed . The wall motion analysis wasperformed by the same two observers who performed theinitial analyses and who were blinded to the tomographic andclinical data as well as the wall motion scores assignedinitially . In 38 dysfunctional segments, the average wallmotion score calculated on repeat analysis was comparableto that calculated initially both before (2 .46 ± 0.74 and2.64 ± 0.74, respectively, p = NS, average percent differ-ence 10.2 ± 19.0%) and after (1 .88 ± 0 .74 and 1 .89 ± 0 .81,respectively, p = NS, average percent difference betweenthe two measurements 7 .8 ± 17.5%®) coronary revasculariza-tion . Moreover, the changes in systolic function in responseto coronary revascularization calculated on the repeat anal-ysis (average change 0 .76 ± 0.63) were comparable to thoseestimated initially (0.82 ± 0.71, p = NS, average percentdifference between the two measurements (18 ± 30%) .
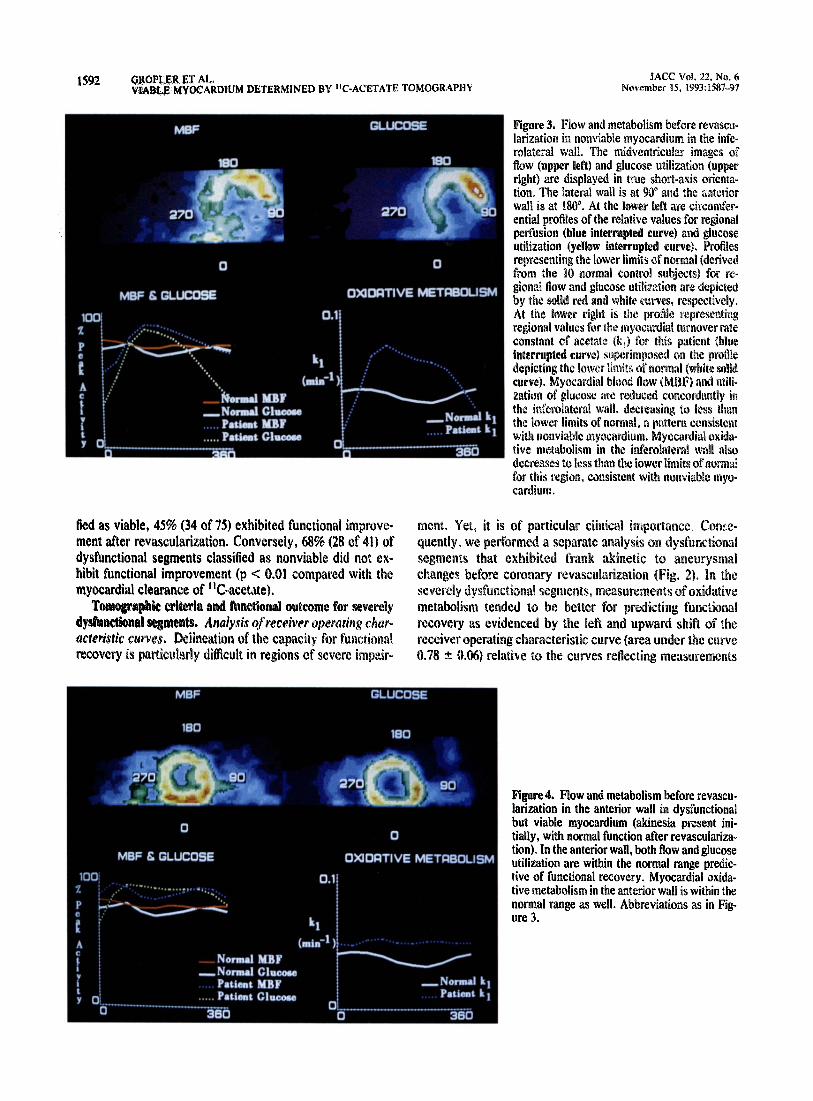
Tomographic criteria and functional outcome for all dys-functional segments. Analysis of receiver operating charac-teristic curves . The receiver operating characteristic curvesfor predicting functional recovery generated for the mea-surements of oxidative metabolism and glucose metabolismare shown in Figures 1 and 2 . Examples of dysfunctional butviable myocardium and nonviable myocardium are illus-trated in Figures 3 and 4, respectively. The receiver operat-ing characteristic curve reflecting measurements of regional
JACC vol . 22 . No . 6November 15, 19911587-97
1 .0
1
0.8
0• .6
0• .4
02
1.0
0.6
1
0 .2
0.4
0.6
False Positive Ratio
MSF. .-.° . Oxlttelivo Metabolism
Glucose Molabollsm Glucose MelabollsmIMaF
0.0
0.4
0
0.0
1.0False Positive Ratio
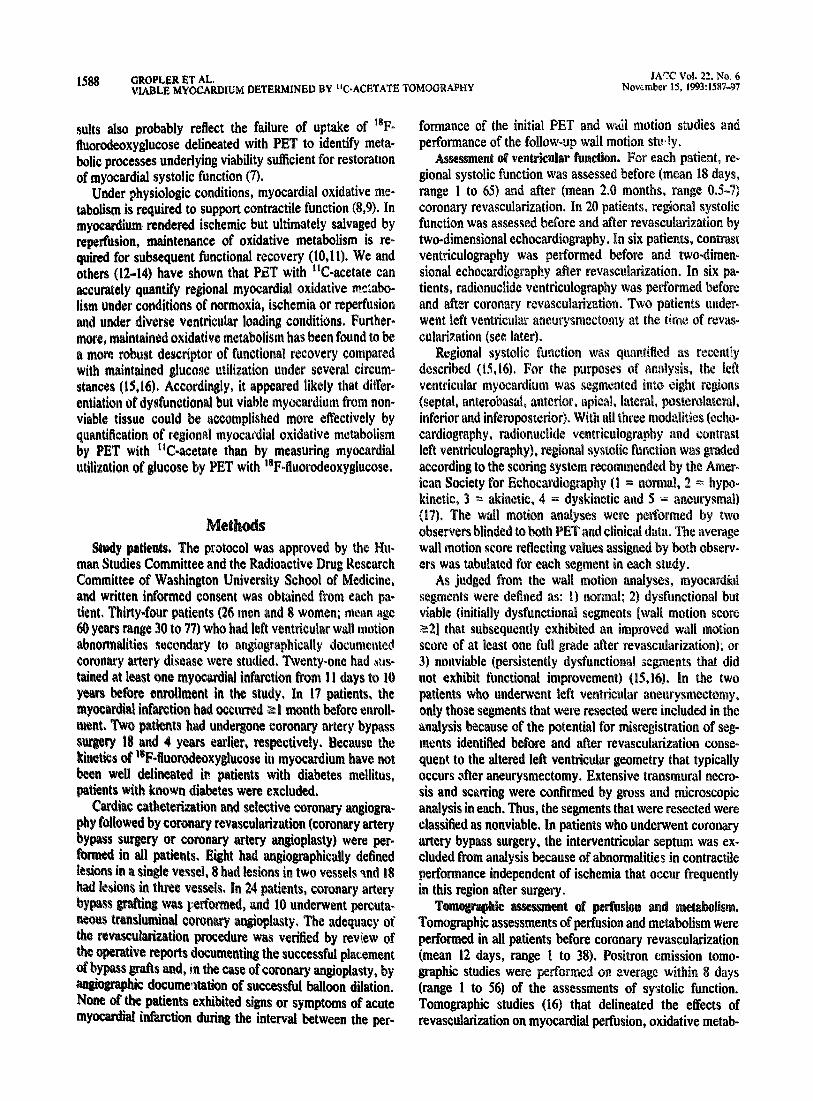
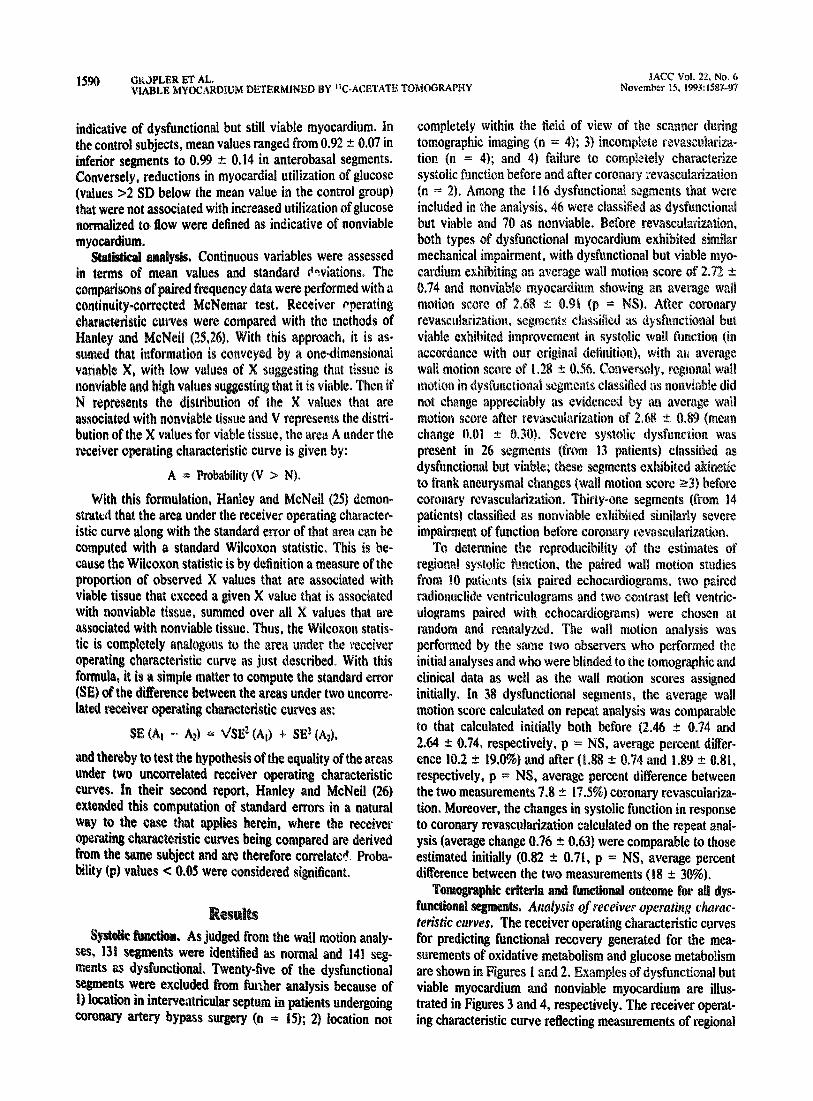
Figure 1 . Receiver operating characteristic curves for prediction o f
functional recovery based on measurements of regional myocardialblood flow (MBF), oxidative metabolism, glucose metabolism andglucose metabolism normalized to flow . Measurements of oxidativemetabolism were the most accurate as evidenced by the left andupward shift of the receiver operating characteristic curve for thesemeasurements (area under the curve 0 .79 ± 0.05) compared with thecurves reflecting estimates of myocardial blood flow (area underthe curve 0.58 ± 0 .06, p < 0.008), glucose metabolism (area under thecurve 0.63 ± 0 .05, p < 0 .007) and glucose metabolism normalized toflow (area under the curve 0 .63 ± 0.05, p < 0.02) .
perfusion are displayed for comparison purposes . The rela-tively linear shape of this curve (area under the curve 0 .580.06) suggests that measurements of relative flow alone werenot useful in delineating viable myocardium . Measurements
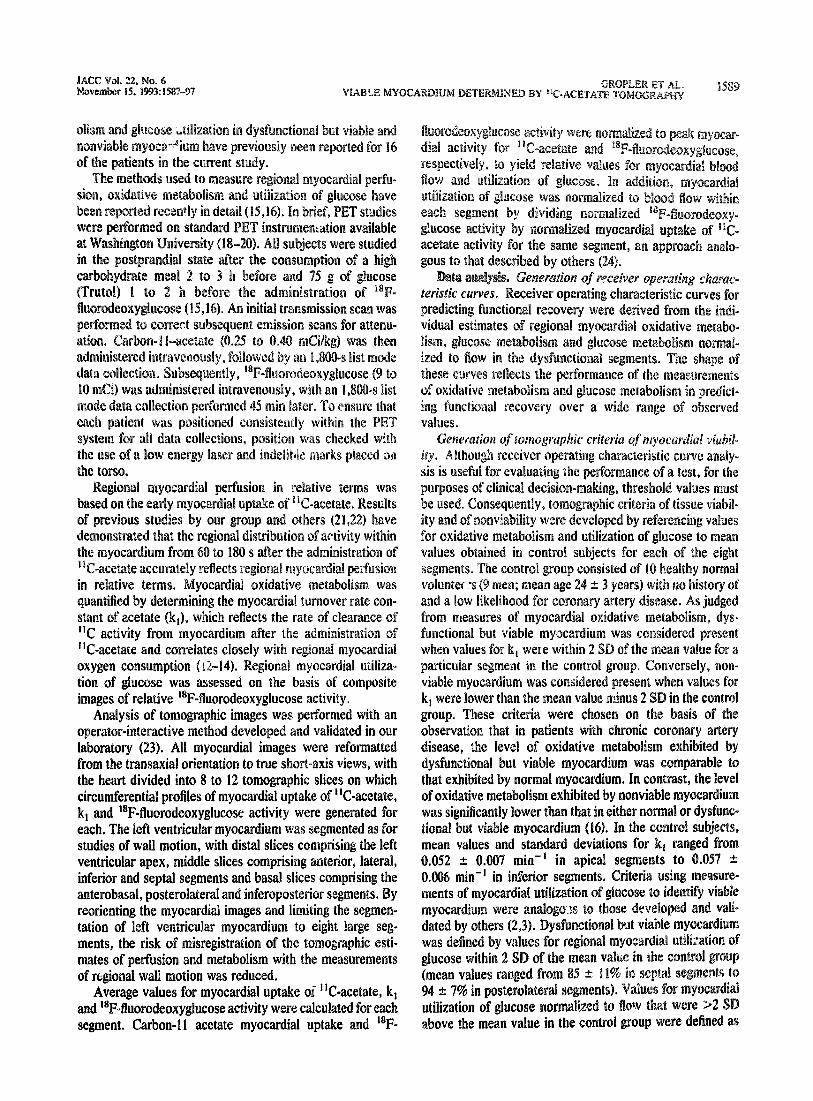
Figure 2 . Receiver operating characteristic curves for predictingfunctional recovery in segments exhibiting severe dysfunction ini-tially . Again, measurements of oxidative metabolism tend to be themost accurate in predicting functional recovery (area under thecurve 0.78 ± 0.06) relative to the curves reflecting measurements ofmyocardial blood flow (MBF) (area under the curve 0 .61 ± 0 .08, p <0.02), glucose metabolism (area under the curve 0 .72 ± 0.07, p =NS) and glucose metabolism normalized to flow (area under thecurve 0.64 ± 0.07, p = NS).
MBF- •- •- • Oxldallve Metabolism
Glucose Metabolism Glucose MelabollemIMBF
0.8
OROPLER FT AL .
1 59 1VIABLE MYOCARDIUM DETERMINE B °!C-ACETATE TOMOGRAPH Y
1 .0
•
0• .6
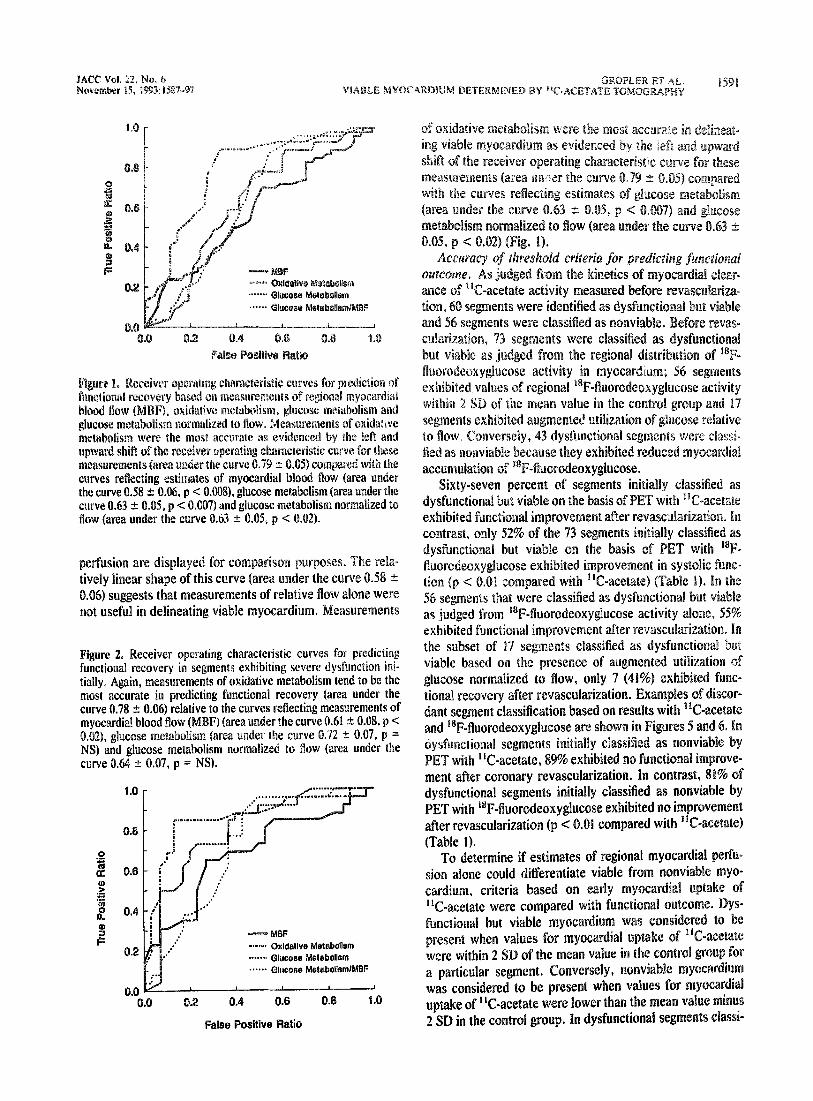
of oxidative metabolism were the most accurate in delineat-ing viable myocardium as evidenced by the left, and upwardshift of the receiver operating characteristic curve for thesemeasurements (area under the curve 0 .79 ± 0.05) comparedwith the curves reflecting estimates of glucose metabolism(area under the curve 0.63 ± 0.05, p < 0.007) and glucosemetabolism normalized to flow (area under the curve 0.630.05, p < 0.02) (Fig. 1) .
Accuracy of threshold criteria for predicting functionalolutcome . .A.s judged from the kinetics of myocardial clear-ance of "C-acetate activity measured before revasculariza-tion, 60 segments were identified as dysfunctional but viableand 56 segments were classified as nonviable . Before revas-cularization, 73 segments were classified as dysfunctionalbut viable as judged from the regional distribution of ' BF-fluorodeclxyglucose activity in myocardium ; 56 segmentsexhibited, values of regional ' BF-fluorodeoxyglucose activitywithin 2 SD of the mean value in the control group and 17segments exhibited augmented utilization of glucose relativeto flow . Conversely, 43 dysfunctional segments were classi-fied as nonviable because they exhibited reduced myocardialaccumulation of "1F-fluorodeoxyglucose.
Sixty-seven percent of segments initially classified asdysfunctional but viable on the basis of PET with 11 C-acetateexhibited functional improvement after revascalarization . Incontrast, only 52% of the 73 segments initially classified asdysfunctional but viable on the basis of PET with ' BF-fluorodeoxyglucose exhibited improvement in systolic func-tion (p < 0.01 compared with "C-acetate) (Table 1) . In the56 segments that were classified as dysfunctional but viableas judged from ' BF-fluorodeoxyglucose activity alone, 55%exhibited functional improvement after revascularization . Inthe subset of 17 segments classified as dysfunctional butviable based on the presence of augmented utilization ofglucose normalized to flow, only 7 (41%) exhibited func-tional recovery after revascularization . Examples of discor-dant segment classification based on results with "C-acetateand i8F-fluorodeoxyglucose are shown in Figures 5 and 6 . Indysfunctional segments initially classified as nonviable byPET with 11 C-acetate, 89% exhibited no functional improve-ment after coronary revascularization . In contrast, 81% ofdysfunctional segments initially classified as nonviable byPET with 18 F-fluorodeoxyglucose exhibited no improvementafter revascularization (p < 0 .01 compared with "C-acetate)(Table 1) .
To determine if estimates of regional myocardial perfu-sion alone could differentiate viable from nonviable myo-cardium, criteria based on early myocardial uptake of"C-acetate were compared with functional outcome . Dys-functional but viable myocardium was considered to bepresent when values for myocardial uptake of "C-acetatewere within 2 SD of the mean value in the control group fora particular segment . Conversely, nonviable myocardiumwas considered to be present when values for myocardialuptake of "C-acetate were lower than the mean value minus2 SD in the control group . In dysfunctional segments classi-
1 592
GROPI ER ET AL,
fled as viable, 45% (34 of 75) exhibited functional improve-ment after revascularization. Conversely, 68% (28 of 41) ofdysfunctional segments classified as nonviable did not ex-hibit functional improvement (p < 0 .01 compared with themyocardial clearance of 11C-acetate) .
Tomographic criteria and functional outcome for severelydyshndional segments . Analysis of receiver operating char-acteristic curves . Delineation of the capacity for functionalrecovery is particularly difficult in regions of severe impair-
JACC Vol, 22, No . 6VIABLE MYOCARDIUM DETERMINED BY "C-ACETATE TOMOGRAPHY
November 15,199-1 :1587-97
mew. Yet, it is of particular clinical importance . Con,--e-quently, we performed a separate analysis on dysfunctionalsegments that exhibited frank akinetic to aneurysmalchanges before coronary revascularization (Fig . 2) . In theseverely dysfunctional segments, measurements of oxidativemetabolism tended to be better for predicting functionalrecovery as evidenced by the left and upward shift of thereceiver operating characteristic curve (area under the curve0.78 ± 0.06) relative to the curves reflecting measurements
Figure 4. Flow and metabolism before revascu-larization in the anterior wall in dysfunctionalbut viable myocardium (akinesia present ini-tially, with normal function after revasculariza-tion) . In the anterior wall, both flow and glucoseutilization are within the normal range predic-tive of functional recovery . Myocardial oxida-tive metabolism in the anterior wall is within thenormal range as well . Abbreviations as in Fig-ure 3 .
Figure 3 . Flow and metabolism before revascu-larization in nonviable myocardium in the infe-rolateral wall . The midventricular images offlow (upper left) and glucose utilization (upperright) are displayed in true short-axis orienta-tion . The lateral wall is at 90° and the anteriorwall is at 180' . At the lower left are circumfer-ential profiles of the relative values for regionalperfusion (blue interrupted curve) and glucoseutilization (yellow interrupted curve) . Profilesrepresenting the lower limits of normal (derivedfrom the 10 normal control subjects) for re-gional flow and glucose utilization are depictedby the solid red and white curves, respectively .At the lower right is the profile representingregional values for the myocardial turnover rateconstant of acetate (k) for this patient (blueinterrupted curve) superimposed on the profiledc jiicting the lower limits of normal (white solidcurve) . Myocardial blood flow (MI3F) and utili-zation of glucose are reduced concordantly inthe inferolateral wall, decreasing to less thanthe lower limits of normal, a pattern consistentwith nonviable myocardium . Myocardial oxidu-live metabolism in the inferolateral wall alsodecreases to less than the lower limits of normalfor this region, consistent with nonviable myo-cardium .

MCC Vol . 22, No . 6November 15 . 1993:1587-97
Table 1. Tomographic Criteria of Myocardial Viability andFunctional Outcome
*p < 0 .01 compared with fluorine- 18-fluorodeoxyglucose .
of glucose metabolism nd glucose metabolism normalizedto flow (area under the curve 0 .72 ± 0.07 and 0 .64 ± 0.07,respectively), but these differences did not achieve statisticalsignificance,
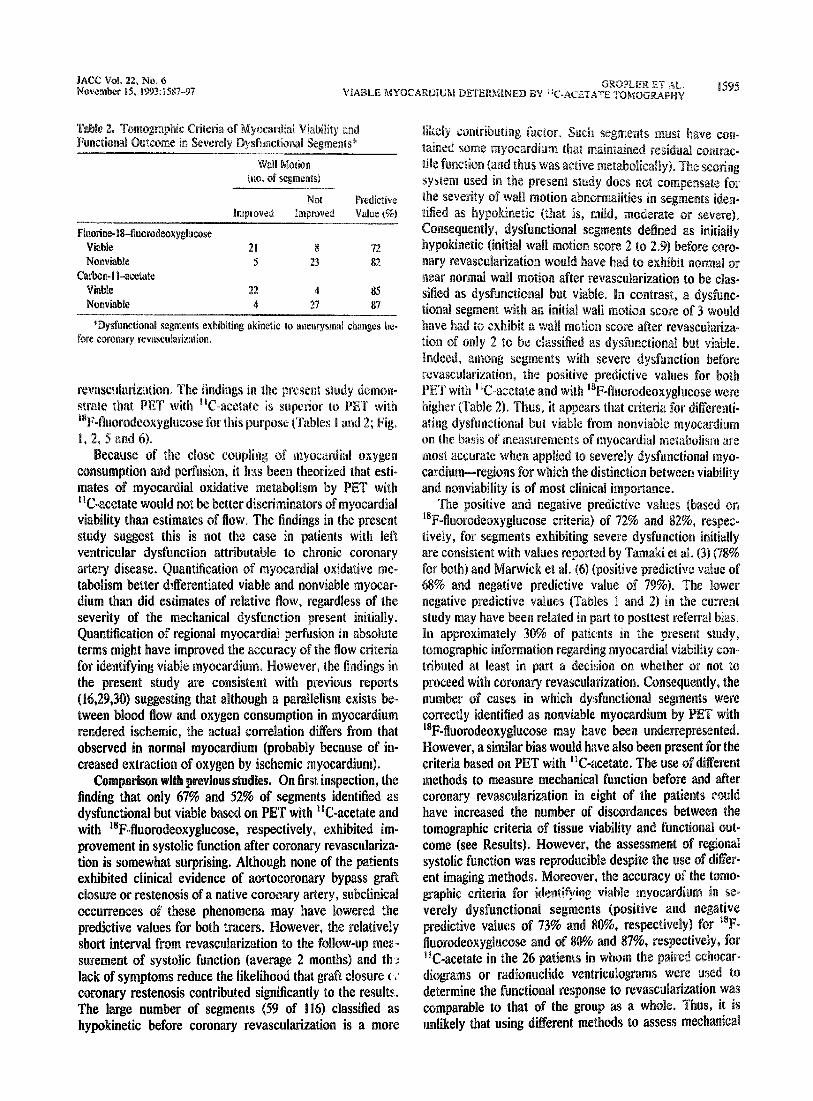
Accuracy of drreshold criteria fiw pr°edBiimy recovery of`finiction . Among segments exhibiting severe, impairment insystolic function before revascularization that were classi-fied as dysfunctional but viable by PET with "C-acetate,85% exhibited functional improvement after revasculariza-tion. However, among segments classified as dysfunctionalbut viable by PET with ' 8F-fluorodeoxyglucose before re-vascularization, only 72% exhibited improved systolic func-tion after reva .,cularization (p = NS) (Table 2) . Among the22 segments classified as dysfunctional but viable based onthe level of 18 17-fluorodeoxyglucose activity alone, 73% (n =16) exhibited functional improvement after revasculariza-tion. Among the seven segments classified as viable on thebasis of the presence of augmented utilization of glucosenormalized to flow, 71% (n = 5) exhibited functional recov-ery after revascularization .
In severely dysfunctional segments classified as nonvia-ble by PET with "C-acetate, 87% did not improve aftercoronary revascularization. Eighty-two percent of severelydysfunctional segments classified as nonviable by PET with' 8F-fluorodeoxyglucose failed to exhibit improvement insystolic function after revascularization (p = NS) .
In severely dysfunctional segments classified as viab le onthe basis of flow estimates, 56% (18 of 32) exhibited func-tional improvement after coronary revascularizatian . Sixty-eight percent (17 of 25) of severely dysfunctional -egmentsclassified as nonviable on the basis of flow estimates failed toexhibit improvement in mechanical function after revascu-larization (p < 0.05 compared with myocardial clearance ofG I I acetate) .
DiscussionOur results indicate that in patients with left ventricular
dysfunction attributable to predominantly chronic coronaryartery disease, regional estimates of overall myocardialoxidative metabolism by PET with 11C .-acetate can accu-
GROPLER ET AL-
1 593VIABLE MYOCARDIUM DE P : RMINED BY "C-ACETATE TOMOGRAPHY
rately identify dysfunctional but still viable myocardiumcapable of recovering systolic function after coronary revas-cularization . They indicate that the estimates are morerobust and superior to those acquired with a tracer that is notspecific for oxidative metabolism .
Delineation of viable myocardium by fluorine-18-fluorodeoxyglucose. Accelerated utilization of glucose (at-tributable to both anaerobic and aerobic glycolysis) is char-acteristic of myocardium rendered ischemic (27) .Consequently, initial efforts to delineate dysfunctional butviable myocardium by PET focused on assessing levelsof myocardial utilization of glucose with ' 8 F-fluorodcoxyglucose in relation to functional outcome (2,3) .In humans with left ventricular dysfunction attributable tochronic coronary artery disease, the persistence of myocar-dial utilization of glucose (whether or not hypoperfusion waspresent) identified myocardium capable of functional recov-ery after coronary artery bypass surgery in 78% to 85%of cases (2,3) . Conversely, reduced myocardial utilizationof glucose (concordant with reduced perfusion) identifieddysfunctional myocardium that failed to improve in 78%to 92% of cases (2,3) . Accordingly, PET with 180fluorodeoxyglucose has been considered by many to beuseful for differentiating dysfunctional but viable from non-viable myocardium (4-6) .
Recently, positive and negative predictive values of 68%and 79%, respectively, for identifying viable myocardiumwith this approach have been reported (6) . Thus, PEI" with`F-fluorodeoxyglucose will overestimate the extent of tis-sue viability in up to 32% of myocardial segments andunderestimate the extent of tissue viability in up to 22% ofsegments (3,6) . The discordances may be explained in partby the differences in the protocols used to standardize thesubstrate environment for myocardial imaging with "F-fluorodeoxyglucose in the various studies (for example,lower predictive values were reported when patients werestudied under fasting conditions than when they were stud-ied in the glucose-loaded state) (2,3,6) . However. theseinaccuracies probably also reflect the relative nonspecificityof myocardial kinetics of 18 F-fluorodeoxyglucose with re-spect to oxidative compared with nonoxidative myocardialglucose metabolism (7,28) . Indeed, it was recently shownthat myocardial accumulation of ' 4 C-deoxyglucose does notreflect glycolysis during reperfusion, whether or not hyper-glycemia was present initially (7) . Consequently, PET with
' S F-fluorodeoxyglucose may not be capable of specificallyidentifying those metabolic processes required for the recov-ery of function of myocardium rendered ischemic .
Oxidative metabolism and myocardial viability . Underphysiologic conditions, maintenance of myocardial oxidativemetabolism is required for continued contractile function(8,9) . In experimental animals subjected to myocardial isch-emia and successful reperfusion, recovery of contractileperformance is associated %,, ith recovery of oxidative metab-olism (10,11) . Until recently, the lack of availability ofmethods for measurement of regional myocardial oxidative
wall Motion(no . of segments)
ImprovedNot
unprovedPredictiveValue (70
Fluorine- 184uorodeoxyglucoseViable 38 35 52Nonviable 8 35 81
Carbon-11-acetateViable 40 20 67*Nonviable 6 50 89*
1594
GROPLER FT AL .VIABLE MYOCARDIUM DETERMINED BY "C-ACETATE TOMOGRAPHY
metabolism precluded assessments in human subjects. How-ever, results of studies by our group and others (12-14) havedemonstrated that PET with acetate can provide accurateestimates of regional overall myocardial oxidative metabo-lism under conditions of normoxia, ischemia and reperfu-sion. Using this approach in conjunction with PET and' IF-fluorodeoxyglucose, we demonstrated that preservationof overall myocardial oxidative metabolism is a necessarycondition for the recovery of function after revascularization
JACC Vol . 22 . No . 6November 15,1993:1587-97
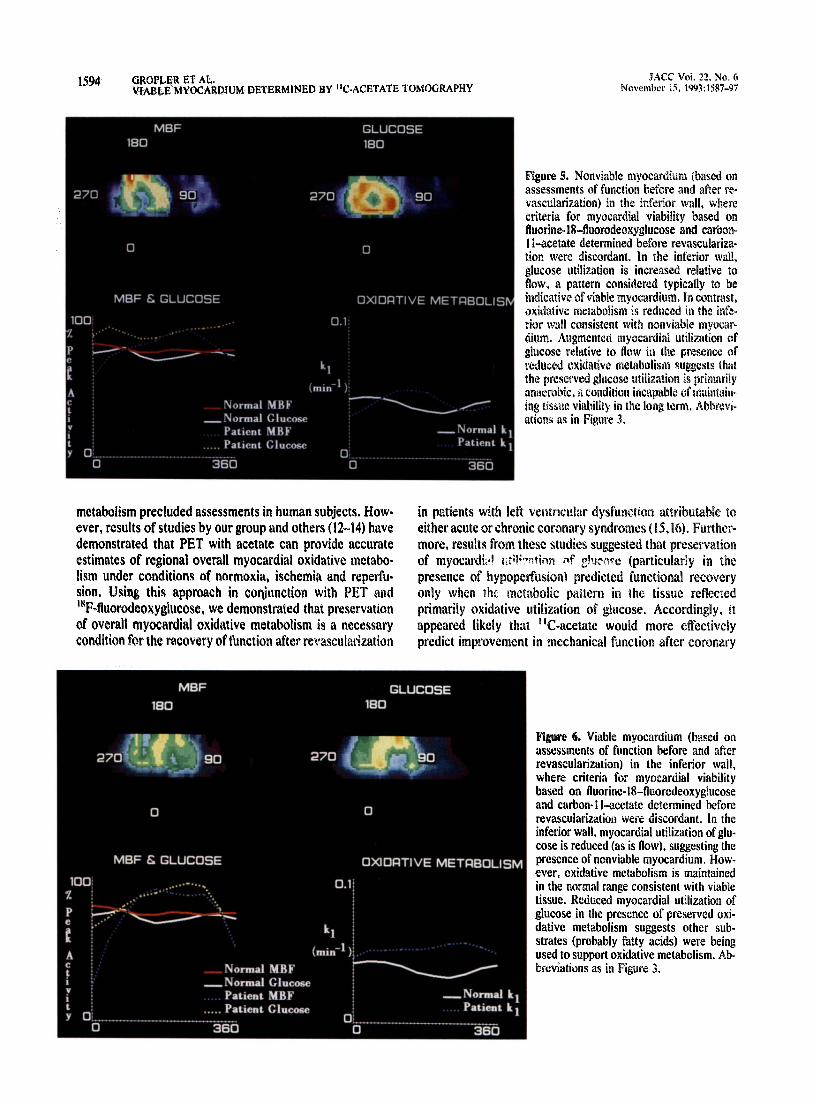
Figure 5. Nonviable myocardium (based onassessments of function before and after re-vascularization) in the inferior wall, wherecriteria for myocardial viability based onfluorine- I 8-fluorodeoxyglucose and carbon-1I-acetate determined before revasculariza-tion were discordant . In the inferior wall,glucose utilization is increased relative toflow, a pattern considered typically to beindicative of viable myocardium . In contrast,Oxidative metabolism is reduced in the infe-rior wall consistent with nonviable myocar-dium. Augmented myocardial utilization ofglucose relative to flow in the presence ofreduced oxidative metabolism suggests thatthe preserved glucose utilization is primarilyanaerobic, a condition incapable of maintain-ing tissue viability in the long term . Abbrevi-ations as in Figure 3,
in patients with left ventricular dysfunction attributable toeither acute or chronic coronary syndromes (15,16) . Further-more, results from these studies suggested that preservationof myocardial of glljco~e (particularly in thepresence of hypoperfusion) predicted functional recoveryonly when the metabolic pattern in the tissue reflectedprimarily oxidative utilization of glucose . Accordingly, itappeared likely that "C-acetate would more effectivelypredict improvement in mechanical function after coronary
Figure 6. Viable myocardium (based onassessments of function before and afterrevascularization) in the inferior wall,where criteria for myocardial viabilitybased on fluorine- 18-fluorodeoxyglucoseand carbon- I I-acetate determined beforerevascularization were discordant . In theinferior wall, myocardial utilization of glu-cose is reduced (as is flow), suggesting thepresence of nonviable myocardium . How-ever, oxidative metabolism is maintainedin the normal range consistent with viabletissue . Reduced myocardial utilization ofglucose in the presence of preserved oxi-dative metabolism suggests other sub-strates (probably fatty acids) were beingused to support oxidative metabolism . Ab-breviations as in Figure 3.
JACC Vol . 22, No . 6November 15, 1993 :1587-97
Table 2 . Toniographic Criteria of Myocardial viability andFunctional Outcome in Severely Dysfunctional Segments*
*Dysfunctional segments exhibiting akinelic to aneurysmal changes be-fore coronary revascularization .
revascularization . The findings in the present study demon-strate that PEI' with "C-acetate is superior to PET with"'F-fluorodeoxyglucose for this purpose (Tables I and 2 ; Fig .1, 2, 5 and 6) .
Because of the close coupling of myocardial oxygenconsumption and perfusion, it has been theorized that esti-mates of myocardial oxidative metabolism by PET with"C-acetate would not be better discriminators of myocardialviability than estimates of flow, The findings in the presentstudy suggest this is not the case in patients with leftventricular dysfunction attributable to chronic coronaryartery disease . Quantification of myocardial oxidative me-tabolism better differentiated viable and nonviable myocar-dium than did estimates of relative flow, regardless of theseverity of the mechanical dysfunction present initially .Quantification of regional myocardial perfusion in absoluteterms might have improved the accuracy of the flow criteriafor identifying viable myocardium . However, the findings inthe present study are consistent with previous reports(16,29,30) suggesting that although a parallelism exists be-tween blood flow and oxygen consumption in myocardiumrendered ischemic, the actual correlation differs from thatobserved in normal myocardium (probably because of in-creased extraction of oxygen by ischemic myocardium) .
Comparison with previous studies . On first inspection, thefinding that only 67% and 52% of segments identified asdysfunctional but viable based on PET with "C-acetate andwith "F-fluorodeoxyglucose, respectively, exhibited im-provement in systolic function after coronary revasculariza-tion is somewhat surprising. Although none of the patientsexhibited clinical evidence of aortocoronary bypass graftclosure or restenosis of a native coronary artery, subclinicaloccurrences of these phenomena may have lowered thepredictive values for both tracers . However, the relativelyshort interval from revascularization to the follow-up mea-surement of systolic function (average 2 months) and thlack of symptoms reduce the likelihood that graft closure (,,,coronary restenosis contributed significantly to the results .The large number of segments (59 of 116) classified ashypokinetic before coronary revascularization is a more
GROPLER ET AL,
1595VIABLE MYOCAREJtUM DETERMINED BY "C-ACETATE TOMOGRAPHY
likely contributing factor . Such segments must have con-tained some myocardium that maintained residual contrac-tile function (and thus was active metabolically) . The scoringsystem used in the present study does not compensate forthe severity of wall motion abnormalities in segments iden-tified as hypokinetic (that is, mild, moderate or severe) .Consequently, dysfunctional segments defined as initiallyhypokinetic (initial wall motion score 2 to 2 .9) before coro-nary revascularization would have had to exhibit normal ornear normal wall motion after revascularization to be clas-sified as dysfunctional but viable . In contrast, a dysfunc-tional segment with an initial wall motion score of 3 wouldhave had to exhibit a wall motion score after revasculariza-tion of only 2 to be classified as dysfunctional but viable .Indeed, among segments with severe dysfunction beforerevascularization, the positive predictive values for bothPET with "C .-acetate and with 18F-fluorodeoxyglucose werehigher (Table 2) . Thus, it appears that criteria for differenti-ating dysfunctional but viable from nonviable myocardiumon the basis of measurements of myocardial metabolism aremost accurate when applied to severely dysfunctional myo-cardium-regions for which the distinction between viabilityand nonviability is of most clinical importance .
The positive and negative predictive values (based on18F-fluorodeoxyglucose criteria) of 72% and 82%, respec-tively, for segments exhibiting severe dysfunction initiallyare consistent with values reported by Tamaki et al . (3) (78%for both) and Marwick et al . (6) (positive predictive value of68% and negative predictive value of 79%) . The lowernegative predictive values (Tables I and 2) in the currentstudy may have been related in part to posttest referral bias .In approximately 30% of patients in the present study,tomographic information regarding myocardial viability con-tributed at least in part a decision on whether or not toproceed with coronary revascularization . Consequently, thenumber of cases in which dysfunctional segments werecorrectly identified as nonviable myocardium by PET with' 8F-fluorodeoxyglucose may have been underrepresented.However, a similar bias would have also been present for thecriteria based on PET with 11C-acetate . The use of differentmethods to measure mechanical function before and aftercoronary revascularization in eight of the patients couldhave increased the number of discordances between thetomographic criteria of tissue viability and functional out-come (see Results) . However, the assessment of regionalsystolic function was reproducible despite the use of differ-ent imaging methods . Moreover, the accuracy of the tomo-graphic criteria for identifying viable myocardium in se-verely dysfunctional segments (positive and negativepredictive values of 73% and 80%, respectively) for 18F
efluorodeoxyglucose and of 80% and 87%, respectively, for1 &C-acetate in the 26 patients in whom the paired echocar-diograms or radionuclide ventriculograms were used todetermine the functional response to revascularization wascomparable to that of the group as a whole . Thus, it isunlikely that using different methods to assess mechanical
Wall Motion(no . of segments)
ImprovedNot
ImprovedPredictiveValue (%)
Fluorine- 18-fluorodeoxyglucoseViable 21 8 72Nonviable 5 23 82
Carbon- I I-acetateViable 22 4 85Nonviable 4 27 87
JACC Vol . 22, No. 6VIABLE MYOCARDIUM DETERMINED BY "C-ACETATE TOMOGRAPHY
November 15. 1993 :1587-971 596
GROPLER ET AL .
function before and after revascularization had a significantimpact on the accuracy of the tomographic criteria forviability .
Myocardial
with 11C-acetate: technical consider .In addition to improved accuracy in differentiating
dysfunctional but viable from nonviable myocardium, PETwith ITC-acetate affords logistic advantages relative to PETwith 1®F-fluorodeoxyglucose . The duration of a completetomographic study with 11C-acetate is approximately 45 min,during which both relative myocardial blood flow and re-gional myocardial oxidative metabolism can be assessed . Incontrast, a viability study with 15F-fluorodeoxyglucose re-quires 2 h and the use of another radiopharmaceutical (forexample, t 50-water, 1IN-ammonia or s2rubidium) for assess-ment of perfusion . The insensitivity of I IC-acetate kinetics inmyocardium to the pattern of substrate delivery (31) is anadditional advantage . However, these advantages are some-what counterbalanced by the need for more frequent synthe-sis of the radiopharmaccutical (physical half-life 20 .3 min forcarbon- l l vs . 109.9 min for fluorine- 18) and slightly moreintensive computer processing and data analysis,
The extent of improvement in global left ventricularfunction and clinical outcome after revascularization arerelated in part to the extent of dysfunctional but still viablemyocardium present initially (2,32,33). Positron emissiontomography and 18F-fluorodeoxygiucose can identify pa-tients with left ventricular dysfunction due to coronaryartery disease in whom successful coronary revasculariza-tion will result in an increase in left ventricular ejectiontraction and an improvement in functional class (2,33) .Moreover, patients who are at high risk for future cardiacevents can be identified (33). Thus, the improved identifica-tion of left ventricular segments that contain dysfunctionalbut still viable myocardium by PET with 11C-acetate shouldfacilitate the objective assessment of the need to revascular-ize myocardium and interventions designed to restore myo-cardial perfusion, thereby improving patient selection forcoronary revascularization,
rldt;r°ilI . Gropler RJ, Bergmann SR. Myocardial viability . What is the definition?
J Nucl Med 1991 ;33:I0-2 .2, Tillliiacch J, Brunken R, Marshall R, et al . Reversibility of cardiac wall
motion abnormalities predicted by positron tomography . N Engl J Med1986 ;314:884-a.
3, Tamaki N, Yonekura Y, Yamashita K, et al, Positran emission tomogra-phy using F-18-deoxygllucose in evaluation of coronary artery bypassgrafting, Am J Cardiol 1 ;64: -5.
4. Ronow R0. D lsiaian V, Cuccolo A, Bacharach SL. Identification ofmyocardium in patients with chronic coronary artery disease and
left ventricular dysfunction : comparison of thallium scintigraphy withreitjection and PET i with ra F-lluorodeoxyglucose . Circulation1991,83 .26-3Z
5 . Gould KL, Y h K, Hess MJ, Haynie M, Mullani N, Smalling RW.M metabolism of duorodeoxyglucose compared to cell mem-brane integrity for the potassium analogue rubidium-82 for assessinginfarct size in man by PET . J Nucl Med 1991 ;32:1-9.
6. Marwick TH. Maclntyre WJ. Lafont A, Nemec JJ, Salcedo EE. Meta-
bolic responses of hiberr°.ating and infarcted myocardium to revascular-ization . Circulation 1992 ;85 :1347-53.
7. Liedtke AJ, Renstiom B, Nellis SH . Correlation between [5- 3 H]glucoseand [U-14C]deoxyglucose as markers of glycolysis in reperfused myocar-dium . Circ Res 1992 ;71 :689-700.
8 . Sarnoff SJ, Braunwald E, Welch GH Jr . Case RB, Stainsby WN, MacrvzR. Hemodynamic determinants of oxygen consumption of the heart withspecial reference to the tension-time index . Am J Physiol 1958;192:148-56.
9. Graham TP Jr, Covell JW, Sonnenblick EH, Ross J Jr, Braunwald E .Control of myocardial oxygen consumption : relative influence of contrac-tile state and tension development . J Clin Invest 1968 ;47 :375.-85.
10. Taegtmeyer H, Roberts AFC, Raine AEG . Energy metabolism in reper-fused heart muscle : metabolic correlates to return of function . J Am CollCardiol 1985 ;6 :864Y70.
11 . Weinheimer CJ, Brown MA, Nohara R, Pdrez JE, Bergmann SR .Functional recovery after reperfusion is predicated on recovery of myo-cardial oxidative metabolism. Am Heart J 1993 ;125 :939--49.
12 . Brown MA, Marshall DR, Sobel BE. Bergmann SR . Delineation ofmyocardial oxygen utilization with carhop-I t-acetate . Circulation 1987 ;76 :687--96.
13 . Henes CO. Bergmann SR. Walsh MN, Sobel BE, Geltman EM. Assess-ment of myocardial oxidative metabolic reserve with positron emissiontomography and carbon-] I-acetate, J Nucl Mcd 1989 ;30 :1489-99.
14 . Armbrecht JJ, Buxton DB . Schelbert HR. Validation of [I- 11C1 acetate asa tracer for noninvasive assessment of oxidative metabolism with positronemission tomography in normal, ischemic, postischemic, and hyperemiccanine myocardium . Circulation I ;81 :1594-605 .
15 . Gropler RJ, Siegel BA, Santpathkumaran KS, et al . The dependence ofrecovery of contractile function on maintenance of oxidative metabolismafter myocardial infarction . J Am Coll Cardiol 1992 ;19:989-97 .
16 . Gropler RJ, Geltman EM, Sampathkumaran KS, et al . Functional recov-cry after revascularization for clr,oaic coronary artery disease is depen-dent on maintenance of oxidative metabolism. J Am Colt Cardiol 1992 .20 :569-77 .
17 . Schifler NO . Shah PM, Crawford M, et al. Recommendations for quan-litation of the left ventricle by two-dimensional echocardiography . J AmSoc Echocardiogr 1989 ;2 :358-67.
18 . Ter-Pogossian MM, Ficke DC, Yamamoto M, Hood JT . Super PETT 1 : apositron emission tomograph utilizing photon time-of-flight information .IEEE Trans Med Imaging 1982 ;3 :179-87 .
19 . Gropler RJ, Siegel BA, Lee ICJ, et al. Non-uniformity of myocardialaccumulation of fluorine-18-fluorodeoxyglucose in normal fasted humans .J Nucl Med 1990:31:1749-56 .
20. Ficke DC, Beecher DE, Bergmann SR, Hofman OR, Hood JT . Ter-Pogossian MM. Performance characterization of a whole body PETsystem designed for dynamic cardiac imaging . IEEE Trans Med Imaging1991 ;3:27-30.
21 . Gropier RI, Siegel BA, Geltman EM . Myocardial uptake of carbon-I1-acetate as an indirect estimate of regional myocardial blood flow . J NuclMed 1991 ;32 :245-5I .
22. Chan SY, Drunken RC, Phelps ME, Schelbert HR . Use of the metabolictracer carbon-I l-acetate for evaluation of regional myocardial perfusion .J Nucl Med 1991 ;32:665-72.
23. Sampathkumaran KS, Herrero P, Owens SE, et al . Image-analysissoftware to facilitate the processing of dynamic positron emission tomo-graphic studies of the heart [abstract] . J Am Coll Cardiol 1992 ;19 SuppiA: 12A.
24. Marshall RC, Tillisch J, Phelps ME, et al . Identification and differentia-tion of resting myocardial ischemia and infarction in man with positroncomputed tomography, "F-labeled fluorodeoxyglucose and N-13 ammo-nia . Circulation 1 2 ;67:766-78 .
25. Hanley JA, McNeil B.I. The meaning and use of the area under a receiveroperating characteristic (ROC) curve . Radiology 1982 ;143 :29-36.
26. Hanley JA, McNeil BJ . A method of comparing areas under receiveroperating characteristic curves derived from the same cases . Radiology1 3;148 :839-43.
27. Camici P, Ferrannini E, Opie LH . Myocardial metabolism in ischemicheart disease : basic principles and application to imaging by positronemission tomography . Prog Cavdiovasc Dis 1989 ;32 :217-38 .
28. Ratib 0, Phelps ME, Huang SC, Henze E, Seen CE, Shelbert HR .

JACC Vol. 22 . No. 6
GROPLER ET AL .
1597November 15, 1993 :1587-97
VIABLE MYOCARDIUM DETERMINED BY "C-ACETATE TOMOGRAPily
Positron tomography with deoxyglucose for estimating local my cardialglucose metabolism. J Nucl Med 1982 ;23 :577-86.
29. Weiss HR . Effect of coronary artery occlusion on regional arterial andvenous 0 2 saturation, 02 extraction, blood flow, and 0 2 consumption inthe dog heart. Cire Res 1980;47 :400-7.
30 . Messer JV, Wagman R), Levine 111, Neill WA, Krasnow N, Gorlin R .Patterns of human myocardial oxygen extraction during rest and exercise .J Clin Invest 1962 .41 :725-42.
31 . Brown MA, Myeats DW, Bergmann SR . Validity of estimates of myo-cardial oxidative metabolism with carbon-l1-acetate and positron emis-
sion tomography despite altered patterns of substrate utilization. J NuclMed 1989 ;30:187-93 .
32 . Gibson RS, Watson DD, Taylor GJ, et al . Prospective assessrneat ofregional myocardial perfusion before and after coronary revascularizationsurgery by quantitative thallium-201 scintigraphy . J Am Coll Cardiol1983 ;1 :804-15 .
33 . Eitzman D, Al-Aouar Z, Kanter ML, Vom Dahl J, Kirsh M, Deeb GM,Schwaiger M . Clinical outcome of patients with advanced coronary arterydisease after viability studies with positron emission tomography . J AmColl Cardiol 1992 ;20 :539-65 .