circulating micrornas in patients with coronary artery disease
TRANSCRIPT

ISSN: 1524-4571 Copyright © 2010 American Heart Association. All rights reserved. Print ISSN: 0009-7330. Online
TX 72514Circulation Research is published by the American Heart Association. 7272 Greenville Avenue, Dallas,
DOI: 10.1161/CIRCRESAHA.109.215566 2010;107;677-684; originally published online Jul 1, 2010; Circ. Res.
Müller-Ardogan, Angelika Bonauer, Andreas M. Zeiher and Stefanie Dimmeler MargaFischer, Christoph Liebetrau, Michael Weber, Christian W. Hamm, Tino Röxe,
Stephan Fichtlscherer, Salvatore De Rosa, Henrik Fox, Thomas Schwietz, Ariane Circulating MicroRNAs in Patients With Coronary Artery Disease
http://circres.ahajournals.org/cgi/content/full/CIRCRESAHA.109.215566/DC1Data Supplement (unedited) at:
http://circres.ahajournals.org/cgi/content/full/107/5/677
located on the World Wide Web at: The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at
[email protected]. E-mail:
Fax:Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters
http://circres.ahajournals.org/subscriptions/Subscriptions: Information about subscribing to Circulation Research is online at
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Clinical/Translational Research
Circulating MicroRNAs in Patients With CoronaryArtery Disease
Stephan Fichtlscherer, Salvatore De Rosa, Henrik Fox, Thomas Schwietz, Ariane Fischer,Christoph Liebetrau, Michael Weber, Christian W. Hamm, Tino Roxe, Marga Muller-Ardogan,
Angelika Bonauer, Andreas M. Zeiher, Stefanie Dimmeler
Rationale: MicroRNAs are small RNAs that control gene expression. Besides their cell intrinsic function, recentstudies reported that microRNAs are released by cultured cells and can be detected in the blood.
Objective: To address the regulation of circulating microRNAs in patients with stable coronary artery disease.Methods and Results: To determine the regulation of microRNAs, we performed a microRNA profile using
RNA isolated from n�8 healthy volunteers and n�8 patients with stable coronary artery disease that receivedstate-of-the-art pharmacological treatment. Interestingly, most of the highly expressed microRNAs that werelower in the blood of patients with coronary artery disease are known to be expressed in endothelial cells (eg,miR-126 and members of the miR-17�92 cluster). To prospectively confirm these data, we detected selectedmicroRNAs in plasma of 36 patients with coronary artery disease and 17 healthy volunteers by quantitative PCR.Consistent with the data obtained by the profile, circulating levels of miR-126, miR-17, miR-92a, and theinflammation-associated miR-155 were significantly reduced in patients with coronary artery disease comparedwith healthy controls. Likewise, the smooth muscle–enriched miR-145 was significantly reduced. In contrast,cardiac muscle–enriched microRNAs (miR-133a, miR-208a) tend to be higher in patients with coronary arterydisease. These results were validated in a second cohort of 31 patients with documented coronary artery diseaseand 14 controls.
Conclusions: Circulating levels of vascular and inflammation-associated microRNAs are significantly downregu-lated in patients with coronary artery disease. (Circ Res. 2010;107:677-684.)
Key Words: microRNAs � endothelial function � atherosclerosis
MicroRNAs (miRNAs) are small (�22-nucleotide) non-coding RNAs regulating gene expression on the post-
transcriptional level by binding to the target mRNA, leadingeither to degradation or to translational repression.1 MiRNAscontrol development and are critically involved in manybiological processes in health and disease including cardio-vascular diseases.1,2 The crucial role of miRNAs in thecardiovascular system is supported by the finding that deple-tion of the miRNA-processing enzyme Dicer leads to defectsin angiogenesis, vessel formation, and cardiac development.1
In endothelial cells, several specific miRNAs have beenidentified to stimulate (let-7f, miR-27b, miR-130a) or inhibit(miR-221 and miR-222) angiogenesis in vitro.3,4 In particular,miR-126 was shown to be highly enriched in endothelialcells, and the expression of miR-126 is essential for vasculardevelopment.5,6 Moreover, members of the miR-17�92 clus-
ter were shown to modulate angiogenesis.7,8 The microRNAsmiR-143 and miR-145 are highly expressed in smooth musclecells and alter smooth muscle cell maintenance.9–11 MiR-1and miR-133 are enriched in cardiomyocytes and controlmyogenesis, cardiac development, and hypertrophy.12,13 Finally,miR-208a and miR-208b are cardiac-specific miRNAs that areexpressed by introns of myosin heavy chains and are involved instress-dependent cardiac growth and gene expression.14
MiRNAs were considered to act as intracellular RNAs tocontrol gene expression on a posttranscriptional level. How-ever, recent studies demonstrated that miRNAs can be de-tected in circulating blood and may be useful as biomarkersfor disease.15,16 Surprisingly, miRNAs are present in serum orplasma in a remarkably stable form that even withstandsrepetitive freezing/thawing cycles and are protected againstRNases.15,17 When human tumors were implanted in mice,
Original received December 21, 2009; revision received June 10, 2010; accepted June 21, 2010. In May 2010, the average time from submission tofirst decision for all original research papers submitted to Circulation Research was 14.6 days.
From the Division of Cardiology, Department of Medicine III (S.F., S.D.R., H.F., T.S., T.R., M.M.-A., A.M.Z.); and Institute for CardiovascularRegeneration, Center of Molecular Medicine (A.F., A.B., S.D.), Goethe University Frankfurt; and Department of Cardiology (C.L., M.W., C.W.H.),Kerckhoff Heart Center, Bad Nauheim, Germany.
This manuscript was sent to Deepak Srivastava, Consulting Editor, for review by expert referees, editorial decision, and final disposition.Correspondence to Stefanie Dimmeler, PhD, Institute for Cardiovascular Regeneration, Goethe University Frankfurt, Theodor Stern Kai 7, 60590
Frankfurt, Germany. E-mail [email protected]© 2010 American Heart Association, Inc.
Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/CIRCRESAHA.109.215566
677 by on September 3, 2010 circres.ahajournals.orgDownloaded from

specific human tumor-derived miRNAs have been detected inplasma.15 Recent studies additionally suggested that circulat-ing myocardial-derived miRNAs might be useful as potentialbiomarkers for infarction.18–22 In experimental acute myocar-dial infarction models and in patients, Wang et al showed thatthe muscle enriched miR-1, miR-133a, and miR-499, as wellas the cardiac-specific miR-208, are elevated in the plasma.18
Likewise, miR-499,19 miR-1,20,21 miR-133a/b, and miR-20821,22
were shown to be increased in small cohorts of humans afteracute myocardial infarction. In patients with heart failure,circulating miR-423 was recently identified as potentially prom-ising prognostic marker.23 In patients with coronary arterydisease (CAD), several miRNAs were shown to be dysregulatedin isolated peripheral blood mononuclear cells.24
The mechanism of how circulating miRNAs are releasedinto the circulation is unclear. However, increasing evidencesuggests that miRNAs are actively secreted in mi-crovesicles.16,25,26 Although the stimuli that trigger miRNAsecretion are unclear, a recent study demonstrated that serumdeprivation leads to the release of microRNAs in cell culturestudies,27 and miRNAs were detected in endothelial cell–derived apoptotic bodies.26 RNA or miRNAs, which havebeen incorporated in microvesicles or apoptotic bodies, wereshown to be delivered into recipient cells.16,26,28 However,
whether the endogenous levels of circulating miRNAs regu-late systemic gene expression needs to be further elucidated.
CAD is still the leading cause of death in the Westernworld. Endothelial activation is considered a first step in thedevelopment of atherosclerotic lesion, followed by invasionof proinflammatory cells and proliferation and dedifferentia-tion of smooth muscle cells.29,30 Several risk factors, such ashypercholesterolemia, are known to promote atherosclerosis,and various biomarkers were shown to identify patients atrisk for CAD. However, the influence of endothelial activa-tion and atherosclerotic disease, as well as the influence ofcurrent vasculoprotective therapy, on levels of circulatingmiRNAs is unknown. Therefore, we determined the levels ofcirculating miRNAs in patients with CAD.
MethodsStudy PopulationThirty-six patients with CAD were included in the initial studycohort (derivation cohort) after angiographic documentation ofCAD. Patients with impaired ejection fraction, heart failure, unstableCAD, or acute myocardial injury were excluded. Seventeen healthyvolunteers without any evidence of CAD or inflammatory disordersserved as the control group. General exclusion criteria were a knownhistory of leukopenia, thrombocytopenia, or severe hepatic or renaldysfunction, as well as evidence for inflammatory or malignantdisease. The results obtained in the derivation cohort were thenprospectively tested in a validation cohort of 14 controls withangiographic exclusion of CAD and 31 patients with angiographi-cally documented stable CAD. The ethics review board of theGoethe University Frankfurt, Germany, and the Landesärzk KammerHeasen approved the protocols, and the study was conducted inaccordance with the Declaration of Helsinki. Written informedconsent was obtained from each individual (German Clinical TrialsRegister No. DRKS00000207).
RNA IsolationRNA was isolated by using a TRIzol-based miRNA isolationprotocol (TRIzol BD from Sigma). Because of high phenol contam-
Figure 1. Profile of circulating miRNAsin patients with CAD vs healthy volun-teers. RNA was isolated from EDTA-plasma from healthy volunteers (n�8) orpatients with CAD (n�8). A heat mapdiagram is shown clustering the differen-tially expressed miRNAs.
Non-standard Abbreviations and Acronyms
CAD coronary artery disease
miR microRNA
miRNA microRNA
qPCR quantitative PCR
678 Circulation Research September 3, 2010
by on September 3, 2010 circres.ahajournals.orgDownloaded from

ination in these samples, additional isopropanol or ammoniumprecipitation steps were included. In addition, we used an miRNA kitprovided by Qiagen (miRNeasy), which combines phenol/guanidine-based lysis of samples and silica membrane–based purification oftotal RNA (�18 nucleotides) in combination with the blood deri-vate–specific TRIzol BD from Sigma. These methods were tested inserum and plasma samples from healthy controls. The optimizedprotocol using the Qiagen miRNA kit was then used for allsubsequent studies with 250 �L of EDTA-plasma or serum. To date,no housekeeping miRNA has been established and validated tonormalize for the miRNA content. Therefore, we supplemented thesamples (after addition of TRIzol) with 5 nmol/L Caenorhabditiselegans miR-39 (cel-miR-39) as described previously.15 We demon-strate that the cel-miR-39 can be used for normalization of the RNApreparation (Online Figure I, available at http://circres.ahajournals.org).
miRNA ProfileMiRNA profiles were obtained by hybridizing RNA from healthyvolunteers and patients to a Geniom Biochip MPEA homo sapiens byFebit biomed GmbH (Heidelberg, Germany). The RNA concentra-tion (optical density, 260/280) was similar between the patients andhealthy volunteers. Data were corrected for background and werenormalized by the mean intensity.
Detection and Quantification of miRNAs byQuantitative PCRRNA was obtained as outlined above and diluted 1:10 (for allmiRNAs except miR-208, which was added without dilution).Diluted RNA (5 �L) was reverse transcribed using the TaqManmicroRNA Reverse Transcription kit (ABI) according to the instruc-tions of the manufacturer. Subsequently, 3 �L of the product wasused for detecting miRNA expression by quantitative (q)PCR usingTaqMan microRNA Assay kits (ABI) for the corresponding mi-
croRNA. For the derivation cohort, values were normalized tocel-miR-39 and are expressed as 2�(CT[microRNA]�CT[cel-miR-39]). Forthe validation cohort, we additionally used recombinant miRNAs toallow quantification of the circulating miRNAs (Online Figure II).Values are given in picomolar concentrations of the miRNA andwere normalized to cel-miR-39.
StatisticsAll results for continuous variables are expressed as means�SEM, ifnot stated otherwise. For group-wise comparisons, Mann–Whitneytest (2 groups), ANOVA, Kruskal–Wallis test (n groups), or Stu-dent’s t test (2 groups) were used as appropriate. For categoricalvariables, Fischer’s exact test or the �2 test were used. Spearman rankcorrelation or Pearson correlation were used to compare levels ofmicroRNAs with classic clinical risk factors. All tests were performed2-sided and a significance level of P�0.05 was considered to indicatestatistical significance.
For all statistical analyses, the statistical software SPSS 15.0(Statistical Package for the Social Sciences, Chicago, Ill) for Win-dows was used.
ResultsDetection of Circulating miRNAsTo measure circulating miRNAs, we tested several miRNAisolation methods in serum and plasma samples from healthycontrols. As shown in Online Figure III, the miRNA isolationkit (miRNeasy kit, Qiagen) revealed the best results to isolatemiRNAs from EDTA-plasma or serum. These results werealso confirmed for other miRNAs (miR-126) (data notshown). EDTA-plasma or serum also was superior to citrateplasma (data not shown). Although miRNAs were reliably
Table. Circulating miRNAs in Healthy Controls and Patients With CAD
Healthy Controls CAD
Fold t TestMean SEM Median 95% CI Mean SEM Median 95% CI
Endothelial-expressed miRNAs
hsa-miR-126 10.94 0.46 11.04 9.86–12.02 7.62 0.60 7.18 6.21–9.03 0.70 0.00
hsa-miR-17 10.02 0.40 9.97 9.06–10.97 6.85 0.61 6.46 5.42–8.29 0.68 0.00
hsa-miR-20a 9.11 0.39 8.72 8.19–10.01 7.19 0.52 6.81 5.95–8.42 0.79 0.01
hsa-miR-92a 10.39 0.39 10.60 9.48–11.30 8.41 0.57 8.41 7.07–9.75 0.81 0.01
hsa-miR-221 6.8 0.8 6.70 4.94–8.71 3.6 0.6 3.04 2.19–4.94 0.52 0.01
hsa-miR-199a-5p 6.7 0.6 6.56 5.41–8.04 3.4 0.6 3.19 1.99–4.77 0.50 0.00
hsa-miR-27a 8.1 0.5 8.01 7.06–9.21 5.8 0.3 5.90 4.94–6.55 0.71 0.00
hsa-miR-130a 9.51 0.35 9.48 8.68–10.34 7.17 0.42 6.81 6.19–8.15 0.75 0.00
hsa-let-7d 8.57 0.67 8.24 6.99–10.15 4.97 0.84 4.30 2.99–6.95 0.58 0.00
hsa-miR-21 8.36 0.41 8.04 7.39–9.33 6.34 0.37 6.46 5.47–7.22 0.76 0.00
Cardiac- and skeletal muscle–expressed miRNAs
hsa-miR-1 3.38 0.15 3.37 3.02–3.75 3.46 0.39 3.83 2.53–4.39 1.02 0.86
hsa-miR-133a 5.02 0.46 4.97 3.94–6.10 5.79 0.24 5.60 5.22–6.35 1.15 0.16
hsa-miR-133b 3.64 0.20 3.54 3.18–4.11 3.83 0.37 4.16 2.95–4.71 1.05 0.66
hsa-miR-208b 3.85 0.25 3.90 3.25–4.44 5.62 0.14 5.62 5.27–5.96 1.46 0.00
hsa-miR-208a 5.76 0.36 5.94 4.91–6.61 6.23 0.22 6.37 5.72–6.74 1.08 0.29
hsa-miR-499–3p 5.19 0.41 5.08 4.21–6.16 5.61 0.35 5.72 4.78–6.44 1.08 0.45
hsa-miR-499–5p 3.97 0.30 3.89 3.26–4.67 4.02 0.26 4.09 3.41–4.63 1.01 0.89
Smooth muscle miRNAs
hsa-miR-143 6.65 0.52 7.16 5.42–7.88 6.08 0.24 6.17 5.52–6.64 0.91 0.34
hsa-miR-145 4.72 0.36 4.54 3.87–5.57 5.36 0.23 5.45 4.81–5.90 1.13 0.16
Circulating miRNAs were detected by Geniom Biochips in RNA isolated from EDTA-plasma obtained from healthy volunteers (n�8) or patients with CAD (n�8).
Fichtlscherer et al Circulating MicroRNAs in Coronary Artery Disease 679
by on September 3, 2010 circres.ahajournals.orgDownloaded from

measurable, the absolute concentration of circulating miR-NAs was �0.5% of the concentrations measured in hearttissue (Online Table I).
Study Population of the Derivation CohortA total of 53 subjects were studied. Thirty-six patients hadangiographically documented CAD. Seventeen individualswithout evidence for CAD were selected as the controlcohort. The clinical characteristics of the 2 study populationsare summarized in Online Table II.
miRNA Profiles in Patients VersusHealthy VolunteersTo determine the influence of CAD on the levels of circulat-ing miRNAs, we performed an miRNA profile using RNAisolated from n�8 patients with CAD and n�8 healthycontrols. The clinical characteristics of the subgroups areshown in Online Table III. The levels of circulating miRNAsprofoundly differed between patients and healthy controls, asillustrated in the heat map diagram shown in Figure 1.Quantification revealed that multiple miRNAs were signifi-cantly downregulated in patients compared with healthycontrols (Online Table IV). Although the absolute number ofsignificantly downregulated miRNAs prevailed, some circu-
lating miRNAs were identified demonstrating increased lev-els in patients (Online Table V). Interestingly, most if not allof the highly expressed and significantly downregulatedmiRNAs in patients with CAD are known to be expressed inthe vascular wall, particularly in endothelial cells. Theseendothelial miRNAs include miR-126, members of the miR-17�92 cluster (miR-17, miR-20a, miR-92a), miR-130a, miR-221, members of the let-7 family (let-7d), and miR-21(Table). In contrast to the high levels and profound regulationof endothelial and vascular miRNAs, cardiac miRNAs weredetected at lower levels and were not downregulated. Inter-estingly, miR-208b was significantly upregulated in patientscompared with healthy volunteers (Table). The establishedsmooth muscle–enriched miRNAs miR-143 and miR-145 didnot differ between healthy controls and CAD patients in theprofile (Table).
To confirm the findings obtained by analyzing the miRNAprofile, we measured the expression of selected miRNAs inthe entire cohort of n�53 subjects by using TaqMan qPCR.As shown in Figure 2, the predominantly endothelial ex-pressed miRNAs miR-126, miR-17, and miR-92a, as well asthe smooth muscle–enriched miR-145, were significantlyreduced in patients with CAD, whereas cardiac muscle–enriched miRNAs, such as miR-133 and miR-208a, were
Figure 2. Circulating miRNAs inpatients with CAD vs healthy volun-teers. Expression of selected miRNAs inEDTA-plasma obtained from patients withCAD (n�36) and healthy volunteers (HC;n�17), as determined by TaqMan PCR.
680 Circulation Research September 3, 2010
by on September 3, 2010 circres.ahajournals.orgDownloaded from

increased (Figure 2). In summary, these data demonstrate thatCAD is associated with a significant decrease of circulatingmiRNAs that are preferentially expressed in endothelial cellsor the vasculature, whereas prototypic muscle–enriched miR-NAs were increased. In addition, we measured the expressionof miR-155, which is processed from BIC, a noncodingtranscript highly expressed in both activated B and T cellsand in monocytes/macrophages but only weakly expressed inendothelial cells.31 Circulating levels of miR-155 were sig-nificantly downregulated in patients with CAD, indicatingthat the downregulation of circulating miRNAs is not re-stricted to endothelial or vascular miRNAs.
Factors Influencing Circulating Levels ofEndothelial miRNAs in Patients With CADTo determine factors that influence the levels of circulatingmiRNAs, we analyzed the association with specific riskfactors for CAD. Age was inversely correlated with the levelsof circulating miR-155, and miR-155 was higher in females(Online Table VI). None of the other circulating miRNAs wassignificantly associated with age or gender. MiR-155, miR-17, and miR-199 were significantly lower in diabetic patients(Online Table VI). However, when only patients were in-cluded in the analysis, these miRNAs were not significantlydifferent in patients with or without diabetes (data notshown). None of the miRNAs was associated with leukocytecounts. Interestingly, vascular and inflammation-linked
miRNA (but not the cardiac-specific miR-208a) were highlyinfluenced by vasculoprotective therapy with inhibitors of therenin–angiotensin system, aspirin and statins (Online TableVI). When the group of patients was selectively analyzed, statintherapy remained a significant factor (Online Table VII), and atrend toward lower levels of miR-17, miR-92a, and miR-126was detected in patients with statin therapy compared withpatients without statin therapy (data not shown).
Validation StudyTo verify the reduction of vascular and inflammation associ-ated miRNAs in patients with CAD and to confirm the factorsinfluencing the levels of circulating miRNAs, we prospec-tively measured circulating miRNAs in a validation cohort ofcontrol subjects without CAD (n�14) and patients withdocumented stable CAD (N�31) (Online Table VIII). Asshown in Figure 3, vascular and leukocyte-derived miRNAwere significantly reduced in patients with CAD comparedwith controls, whereas cardiac miRNAs were slightly in-creased. Consistent with the influence of age and gender onmiR-155 detected in the derivation cohort, females showed asignificantly higher level of circulating miR-155 comparedwith males in the validation cohort (Figure 4A), and age wasnegatively associated with circulating miR-155 levels(P�0.001). Diabetes, again, was associated with significantlyreduced levels of some vascular miRNAs in the entirevalidation cohort (miR-17 and miR-145: P�0.05). However,
Figure 3. Circulating miRNAs in the vali-dation cohort. Expression of selectedmiRNAs in serum obtained from patientswith CAD (n�31) and control subjects(CON) (n�14), as determined by TaqManPCR. Values were quantified by usingrecombinant miRNAs to generate a standardcurve (see Online Figure II), and values werenormalized to cel-miR-39. Probability valueswere calculated by Mann–Whitney test com-pared with controls.
Fichtlscherer et al Circulating MicroRNAs in Coronary Artery Disease 681
by on September 3, 2010 circres.ahajournals.orgDownloaded from

when directly comparing the patients with or without diabe-tes, a trend can only be seen in miR-145 levels, which werefurther reduced in diabetic patients compared with patientswith CAD but without diabetes (Figure 4B). Finally, confirm-ing the results of our original cohort, statin treatment wasassociated with reduced levels of vascular miRNAs (miR-17:P�0.001; miR-145: P�0.05) and miR-155 (P�0.05). How-ever, only miR-17 was significantly different, when exclu-sively CAD patients with statin therapy were compared withCAD patients without statin therapy (36�14% percent reduc-tion; P�0.024).
DiscussionThe present study demonstrates that circulating vessel wall–and inflammatory cell–derived miRNAs can be detected inthe blood and are regulated in patients with CAD. Interest-ingly, cardiac muscle– or skeletal muscle–derived miRNAwere differentially regulated and tend to increase in stablepatients with CAD.
The data of the present study confirm previous reportsshowing that circulating miRNAs can be reliably isolated andmeasured in humans.15,20 The levels of miRNAs detected inplasma were slightly higher compared with serum, whereasothers reported that similar concentrations of miRNAs can beisolated from plasma and serum.15 However, the levels werecorrelating with each other and the dysregulation of miRNAsin CAD patients was detected when using both either plasmaor serum to isolate miRNAs (see Figures 2 and 3, respec-tively). Among the different plasma preparations studied,EDTA-plasma yielded the best results compared with citrate-and heparin-plasma (data not shown). By supplementing theEDTA-plasma or serum samples with recombinant C elegansmiRNAs, which can be specifically detected by TaqMan
qPCR, differences in the efficiency of RNA isolation can benormalized. However, because of the profound regulation ofmultiple miRNAs and the unknown impact of factors thatmodulate circulating miRNA levels, we were unable tonormalize the levels of circulating miRNAs by a “house-keeping” miRNA. Because “vascular” miRNAs were differ-entially regulated compared with cardiac miRNAs, unequalRNA concentration in the plasma appears unlikely to underliethe changes in expression levels detected between the groupsin the present study.
Consistent with the exposure of the vasculature and inflam-matory cells to the circulating blood, vascular wall–derivedand leukocyte-derived miRNAs were detected in higherconcentrations compared with skeletal or cardiac muscle–derived miRNAs in healthy volunteers, as well as in patientswith CAD. Vascular miRNAs, including endothelial-enrichedmiRNAs (such as miR-126) or miRNAs that are highlyexpressed in endothelial cells (such as the miR-17�92cluster), were downregulated in patients with CAD, as shownin the miRNA profile, as well as in the derivation andvalidation study cohorts. Smooth muscle miRNAs were notsignificantly regulated in the profile, but we could detect asignificant downregulation in the larger cohorts of patients.This discrepancy is likely attributable to the small sample sizeused to profile the miRNA levels. In contrast to the down-regulation of most vascular-derived miRNAs in patients withCAD, circulating levels of skeletal muscle– or cardiac–derived miRNAs showed a trend toward increased levels inpatients with CAD. Although recent experimental studiesshowed that cardiac miRNAs are released after acute myo-cardial infarction, the increased levels are unlikely attribut-able to cardiac events, because the patients included in thepresent study had stable CAD and none of them showed
Figure 4. Effect of gender and diabetes on selected miRNAs. miRNAs were detected in the derivation and validation cohort by PCRand were normalized to cel-miR-39. A, miR-155 levels were detected in the derivation cohort (n�22 females, n�31 males) and the vali-dation cohort (n�19 females, n�26 males). B, Influence of diabetes on circulating miRNA levels in the derivation cohort in healthy con-trols (HC) (N�17), CAD (N�27), and CAD with diabetes (N�9) and in the validation cohort in healthy controls (N�12), CAD (N�23) andCAD patients with diabetes (N�8). Note that the 2 individuals with diabetics but without CAD in the control group were excluded.Probability values are calculated by Mann–Whitney test in A and ANOVA in B.
682 Circulation Research September 3, 2010
by on September 3, 2010 circres.ahajournals.orgDownloaded from

elevated troponin T levels. However, we cannot exclude thatthe slight increase might be caused by a low grade of cardiacmyocyte injury.
The reduced concentration of circulating vascular miRNAsdetected in patients with CAD was surprising, because onewould expect that endothelial activation, as it occurs inpatients with CAD, induces the release of microparticles andremnants of apoptotic cells, thereby elevating the levels ofmiRNAs. However, recent experimental studies demonstratethat miRNA can be delivered by apoptotic bodies to athero-sclerotic lesion.26 Therefore, one may speculate that thereduction of circulating miRNAs detected in patients withCAD might be caused by an uptake of circulating miRNAsinto atherosclerotic lesions.
One limitation of the present study is that we cannot providemolecular insights into the cause of the dysregulation. The levelsof circulating miRNAs may be affected by multiple parame-ters such as the change in expression in the tissue, the releaseof the miRNAs by the cells into the circulation and thestability of miRNAs in the plasma. The simultaneous regu-lation of many vascular miRNAs may also reflect a modula-tion of miRNA processing, as it is known that cellularstressors can affect the expression of the enzyme Dicer that isessential for the biogenesis of mature miRNAs.32 Furtherexperimental studies are necessary to explore the mecha-nism(s), by which CAD and therapies affect tissue versuscirculating miRNA levels.
In summary, the present study provides first insights intothe levels of circulating miRNAs in patients with CAD.Besides confirming studies demonstrating the reliable mea-surement of circulating miRNAs, our study specificallyaddressed the levels and regulation of vascular and muscle-derived miRNAs and shows that, in particular, miRNAs thatare highly expressed by endothelial cells can be detected inhigh concentrations in the circulation. Moreover, alteredlevels of miRNAs in CAD patients were detected in 2 patientcohorts. However, these data surely need to be confirmed inlarger clinical populations, particularly because the analysisof single risk factors (such as diabetes) or therapeutic inter-ventions is hampered by small numbers of patients availablein these subcohorts. Furthermore, the mechanisms underlyingthe dysregulation, as well as the putative impact of thechanges in circulating miRNAs levels in the physiology orpathophysiology, remains to be determined. Prospectivelarge-scale studies are required to determine the potential useof circulating endothelial or vascular miRNAs as biomarkersfor the development of CAD.
Sources of FundingThis study was supported by the Deutsche Forschungsgemeinschaft(SFB 834; project B1 to S.F. and S.D.), the Excellence Cluster Exc147-1 (to S.D., S.F., C.W.H., and A.M.Z.), and the EuropeanResearch Council (Angiomir to S.D.).
DisclosuresNone.
References1. van Rooij E, Olson EN. MicroRNAs: powerful new regulators of heart
disease and provocative therapeutic targets. J Clin Invest. 2007;117:2369–2376.
2. Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function.Cell. 2004;116:281–297.
3. Kuehbacher A, Urbich C, Zeiher AM, Dimmeler S. Role of Dicer andDrosha for endothelial microRNA expression and angiogenesis. Circ Res.2007;101:59–68.
4. Urbich C, Kuehbacher A, Dimmeler S. Role of microRNAs in vasculardiseases, inflammation, and angiogenesis. Cardiovasc Res. 2008;79:581–588.
5. Wang S, Aurora AB, Johnson BA, Qi X, McAnally J, Hill JA, RichardsonJA, Bassel-Duby R, Olson EN. The endothelial-specific microRNAmiR-126 governs vascular integrity and angiogenesis. Dev Cell. 2008;15:261–271.
6. Fish JE, Santoro MM, Morton SU, Yu S, Yeh RF, Wythe JD, Ivey KN,Bruneau BG, Stainier DY, Srivastava D. miR-126 regulates angiogenicsignaling and vascular integrity. Dev Cell. 2008;15:272–284.
7. Bonauer A, Carmona G, Iwasaki M, Mione M, Koyanagi M, Fischer A,Burchfield J, Fox H, Doebele C, Ohtani K, Chavakis E, Potente M, TjwaM, Urbich C, Zeiher AM, Dimmeler S. MicroRNA-92a controls angio-genesis and functional recovery of ischemic tissues in mice. Science.2009;324:1710–1713.
8. Suarez Y, Fernandez-Hernando C, Yu J, Gerber SA, Harrison KD, PoberJS, Iruela-Arispe ML, Merkenschlager M, Sessa WC. Dicer-dependentendothelial microRNAs are necessary for postnatal angiogenesis. ProcNatl Acad Sci U S A. 2008;105:14082–14087.
9. Elia L, Quintavalle M, Zhang J, Contu R, Cossu L, Latronico MV,Peterson KL, Indolfi C, Catalucci D, Chen J, Courtneidge SA, CondorelliG. The knockout of miR-143 and -145 alters smooth muscle cell main-tenance and vascular homeostasis in mice: correlates with human disease.Cell Death Differ. 2009;16:1590–1598.
10. Xin M, Small EM, Sutherland LB, Qi X, McAnally J, Plato CF, Rich-ardson JA, Bassel-Duby R, Olson EN. MicroRNAs miR-143 andmiR-145 modulate cytoskeletal dynamics and responsiveness of smoothmuscle cells to injury. Genes Dev. 2009;23:2166–2178.
11. Boettger T, Beetz N, Kostin S, Schneider J, Kruger M, Hein L, Braun T.Acquisition of the contractile phenotype by murine arterial smoothmuscle cells depends on the Mir143/145 gene cluster. J Clin Invest.2009;119:2634–2647.
12. Zhao Y, Ransom JF, Li A, Vedantham V, von Drehle M, Muth AN,Tsuchihashi T, McManus MT, Schwartz RJ, Srivastava D. Dysregulationof cardiogenesis, cardiac conduction, and cell cycle in mice lackingmiRNA-1–2. Cell. 2007;129:303–317.
13. Care A, Catalucci D, Felicetti F, Bonci D, Addario A, Gallo P, Bang ML,Segnalini P, Gu Y, Dalton ND, Elia L, Latronico MV, Hoydal M, AutoreC, Russo MA, Dorn GW II, Ellingsen O, Ruiz-Lozano P, Peterson KL,Croce CM, Peschle C, Condorelli G. MicroRNA-133 controls cardiachypertrophy. Nat Med. 2007;13:613–618.
14. van Rooij E, Sutherland LB, Qi X, Richardson JA, Hill J, Olson EN.Control of stress-dependent cardiac growth and gene expression by amicroRNA. Science. 2007;316:575–579.
15. Mitchell PS, Parkin RK, Kroh EM, Fritz BR, Wyman SK, Pogosova-Agadjanyan EL, Peterson A, Noteboom J, O’Briant KC, Allen A, LinDW, Urban N, Drescher CW, Knudsen BS, Stirewalt DL, Gentleman R,Vessella RL, Nelson PS, Martin DB, Tewari M. Circulating microRNAsas stable blood-based markers for cancer detection. Proc Natl Acad SciU S A. 2008;105:10513–10518.
16. Skog J, Wurdinger T, van Rijn S, Meijer DH, Gainche L, Sena-EstevesM, Curry WT Jr, Carter BS, Krichevsky AM, Breakefield XO. Glio-blastoma microvesicles transport RNA and proteins that promote tumourgrowth and provide diagnostic biomarkers. Nat Cell Biol. 2008;10:1470–1476.
17. Gilad S, Meiri E, Yogev Y, Benjamin S, Lebanony D, Yerushalmi N,Benjamin H, Kushnir M, Cholakh H, Melamed N, Bentwich Z, Hod M,Goren Y, Chajut A. Serum microRNAs are promising novel biomarkers.PLoS ONE. 2008;3:e3148.
18. Wang GK, Zhu JQ, Zhang JT, Li Q, Li Y, He J, Qin YW, Jing Q.Circulating microRNA: a novel potential biomarker for early diagnosis ofacute myocardial infarction in humans. Eur Heart J. 2010;31:659–666.
19. Adachi T, Nakanishi M, Otsuka Y, Nishimura K, Hirokawa G, Goto Y,Nonogi H, Iwai N. Plasma microRNA 499 as a biomarker of acutemyocardial infarction. Clin Chem. 2010;56:1183–1185.
20. Ai J, Zhang R, Li Y, Pu J, Lu Y, Jiao J, Li K, Yu B, Li Z, Wang R, WangL, Li Q, Wang N, Shan H, Yang B. Circulating microRNA-1 as apotential novel biomarker for acute myocardial infarction. BiochemBiophys Res Commun. 2010;391:73–77.
Fichtlscherer et al Circulating MicroRNAs in Coronary Artery Disease 683
by on September 3, 2010 circres.ahajournals.orgDownloaded from

21. Bostjancic E, Zidar N, Stajer D, Glavac D. MicroRNAs miR-1,miR-133a, miR-133b and miR-208 are dysregulated in human myocardialinfarction. Cardiology. 2010;115:163–169.
22. Ji X, Takahashi R, Hiura Y, Hirokawa G, Fukushima Y, Iwai N. PlasmamiR-208 as a biomarker of myocardial injury. Clin Chem. 2009;55:1944–1949.
23. Tijsen AJ, Creemers EE, Moerland PD, de Windt LJ, van der Wal AC,Kok WE, Pinto YM. MiR423–5p as a circulating biomarker for heartfailure. Circ Res. 2010;106:1035–1039.
24. Hoekstra M, van der Lans CA, Halvorsen B, Gullestad L, Kuiper J,Aukrust P, van Berkel TJ, Biessen EA. The peripheral blood mononuclearcell microRNA signature of coronary artery disease. Biochem BiophysRes Commun. 2010;394:792–797.
25. Hunter MP, Ismail N, Zhang X, Aguda BD, Lee EJ, Yu L, Xiao T,Schafer J, Lee ML, Schmittgen TD, Nana-Sinkam SP, Jarjoura D, MarshCB. Detection of microRNA expression in human peripheral bloodmicrovesicles. PLoS ONE. 2008;3:e3694.
26. Zernecke A, Bidzhekov K, Noels H, Shagdarsuren E, Gan L, DeneckeB, Hristov M, Koppel T, Jahantigh MN, Lutgens E, Wang S, Olson
EN, Schober A, Weber C. Delivery of microRNA-126 by apoptoticbodies induces CXCL12-dependent vascular protection. Sci Signal.2009;2:ra81.
27. Wang K, Zhang S, Weber J, Baxter D, Galas DJ. Mammalian cells inculture actively export specific microRNAs. Nature Precedings. hdl:10101/npre.2009.3718.1.
28. Deregibus MC, Cantaluppi V, Calogero R, Lo Iacono M, Tetta C,Biancone L, Bruno S, Bussolati B, Camussi G. Endothelial progenitor cellderived microvesicles activate an angiogenic program in endothelial cellsby a horizontal transfer of mRNA. Blood. 2007;110:2440–2448.
29. Lerman A, Zeiher AM. Endothelial function: cardiac events. Circulation.2005;111:363–368.
30. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis.Circulation. 2002;105:1135–1143.
31. Tili E, Croce CM, Michaille JJ. miR-155: on the crosstalk betweeninflammation and cancer. Int Rev Immunol. 2009;28:264–284.
32. Wiesen JL, Tomasi TB. Dicer is regulated by cellular stresses and inter-ferons. Mol Immunol. 2009;46:1222–1228.
Novelty and Significance
What Is Known?
● MicroRNAs (miRNAs) are short, noncoding RNAs that control geneexpression on a posttranslational level.
● Recent studies show that miRNA can be detected in circulating blood andthat these circulating microRNAs might be useful disease biomarkers,eg, for certain forms of cancer or cardiovascular diseases.
● Circulating levels of cardiac or muscle-derived miRNAs were elevatedin the blood after acute myocardial infarction.
What New Information Does This Article Contribute?
● We demonstrate that circulating levels of miRNAs are dysregulated inpatients with stable coronary artery disease.
● In patients with stable coronary artery disease, vascular-derivedmiRNAs were significantly downregulated, whereas muscle-derived miRNAs tended to be higher.
Here, we demonstrate that in 2 patient cohorts with stablecoronary artery disease, circulating levels of miRNAs are differ-entially regulated compared with individuals without coronaryartery disease. Thereby, miRNAs that are highly expressed in thevascular wall (eg, miR-17, miR-92a or miR-126) were signifi-cantly downregulated in the circulating blood, suggesting thatthese miRNAs are reduced in expression, are degraded, or aretaken up in diseased vessels. In contrast, miRNAs that are highlyexpressed in muscle tissue tend to be higher in the circulationof patients with coronary artery disease. These data are the firstto report a differential regulation of vascular- versus muscle-derived miRNAs in patients with coronary artery disease. Furtherstudies must elucidate the underlying mechanism(s) and thepotential use of selected miRNAs as biomarkers for riskstratification.
684 Circulation Research September 3, 2010
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Supplement Material
Online figure I
1,0E‐08
1,0E‐07
1,0E‐06
1,0E‐05
-CT
1,0E‐12
1,0E‐11
1,0E‐10
1,0E‐09
1250 125 12,5 1,25 0,125
C l iR 39 ( M)
2
Cel‐miR‐39 (pM)
Online figure I: Recombinant C.elegans miRNA cel‐miR‐39 was added to EDTA‐plasma (after trizol) and RNA was isolated with the miRNeasy kit. Cel‐miR‐39 was detected by Taqman PCR.
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online figure II
C l 39 92 126C.elegans-39 miR-92a miR-126
miR-17 miR-133a miR-155
pM pM pM
miR-208a miR-145 miR-199a
pM pM pM
pM pM pM
Online figure II: Recombinant miRNA was detected by TaqMan PCR
p p p
by on September 3, 2010 circres.ahajournals.orgDownloaded from
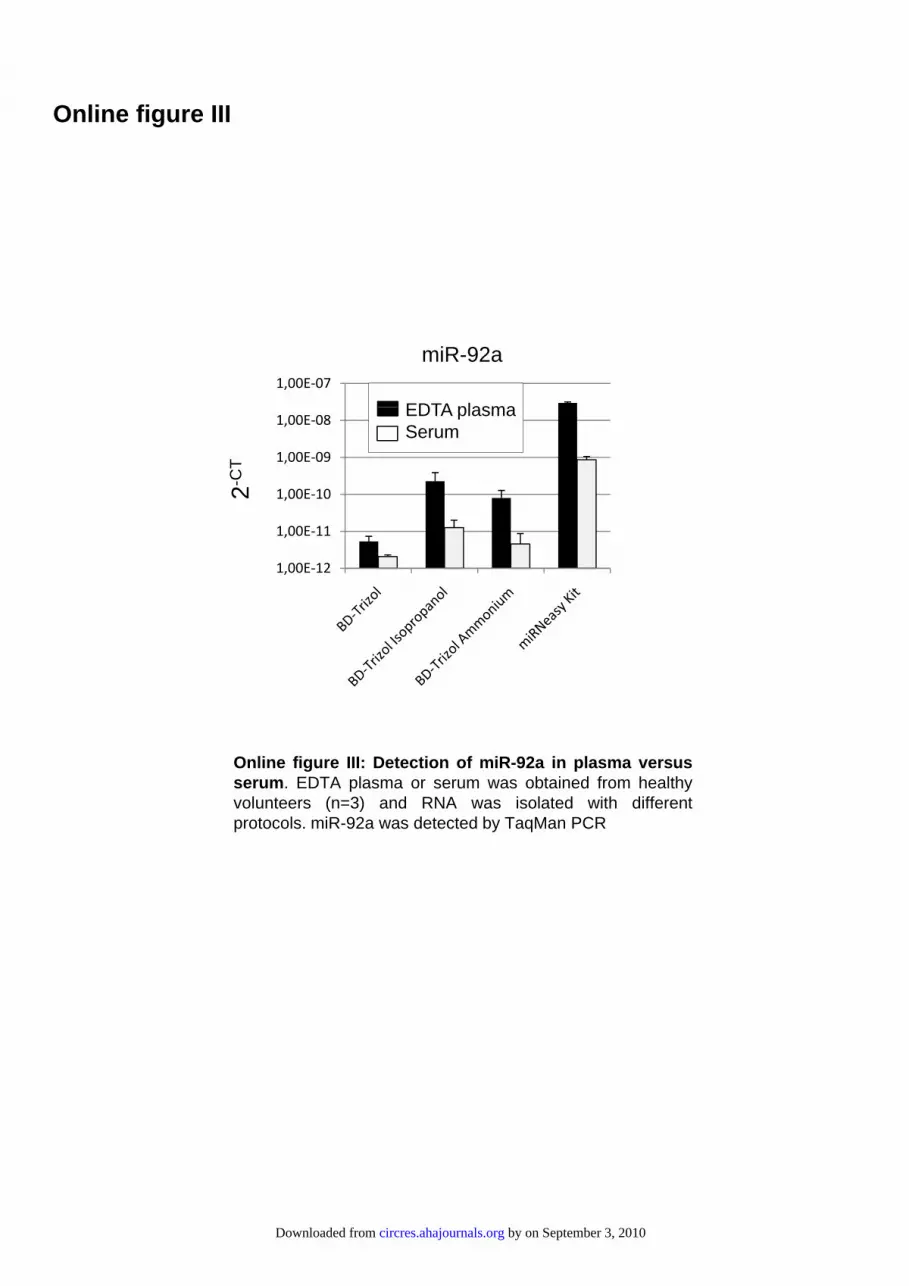
Online figure III
1,00E‐07
miR-92a
EDTA plasma
1 00E 12
1,00E‐11
1,00E‐10
1,00E‐09
1,00E‐08EDTA plasmaSerum
2-C
T
1,00E‐12
Online figure III: Detection of miR-92a in plasma versusserum. EDTA plasma or serum was obtained from healthyvolunteers (n=3) and RNA was isolated with differentprotocols. miR-92a was detected by TaqMan PCR
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online Table I
pM (in plasma or tissue) Mean SEMmiR-92a Plasma 3,92229863 0,41583282 Heart 1395,83841 74,8045852miR-126 Plasma 1,16092477 0,25368308 Heart 9648,63215 271,568527miR-208 Plasma 0,00302676 0,00057167 Heart 5197,73941 219,915659
Online table I: RNA was isolated of 250 µl EDTA plasma with the Qiagen miRNA kit or of 50 mg mouse hearts with the miRNeasy kit (Qiagen) using Qiazol instead of Trizol BD. miRNA were quantified using Taqman PCR and recombinant miRNAs were used for calibration. Data are mean + SEM from n=3 samples
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online Table II: Characteristics of study cohort
Healthy volunteers
(n=17)
Patients with CAD
(n=36)
P-value
Gender Male 6 (35.3%) 25 (69.4%) 0.020
Age (years) 32.18 ± 8.78 67.69 ± 11.07 0.000
Stable CAD for at least 4 months 0 100% 0.000
Number of vessels
(CAD) 0
I: 7 (19.4%)
II: 11 (30.6%)
III: 18 (50.0%)
0.000
0.000
0.000
Hypertension 0 32 (91.4%) 0.000
Active smoker 3 (30.0%) 8 (30.8%) 0.647
Adipositas (BMI > 25) 4 (23.5%) 12 (38.7%) 0.230
Diabetes mellitus 0 9 (25.0%) 0.021
History of
AMI/PCI/ACVB/PTA/Stroke 0 100% 0.000
Concurrent medication:
Beta - blocker
Aspirin / Clopidogrel
ACE-Inhibitor / ATRB
Diuretics
Statin therapy
0
0
0
0
0
31 (88.6%)
100%
30 (83.3%)
12 (33.3%)
31 (86.1%)
0.000
0.000
0.000
0.005
0.000
Total cholesterol (mg/dl) 192.63 ± 38.61 176.14 ± 37.82 0.156
LDL cholesterol (mg/dl) 103.00 ± 38.87 93.00 ± 31.31 0.335
Triglycerides (mg/dl) 92.38 ± 59.27 172.64 ±117.67 0.013
HDL cholesterol (mg/dl) 65.12 ± 19.20 49.21 ± 12.68 0.001
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online Table III: Characteristic of the subcohort used for miRNA profiling
Healthy volunteers
(n=8)
Patients with CAD (n=8)
P-value
Gender Male 4 (50%) 4 (50%) 0.690
Age (years) 35.0 ± 5.99 66.5 ± 3.95 0.001
Stable CAD for at least 4 months 0 8 (100%) 0.000
Number of vessels
(CAD)
0
0
0
I: 1 (12.5%)
II: 5 (62.5%)
III: 2 (25.0%)
0.190
0.180
0.110
Hypertension 0 6 (75.0%) 0.003
Active smoker 2 (25.0%) 5 (62.5%) 0.157
Adipositas (BMI > 25) 2 (25.0%) 3 (37.5%) 0.500
Diabetes mellitus 0 2 (25.0%) 0.230
History of
AMI/PCI/ACVB/PTA/Stroke
0
100%
0.000
Concurrent medication:
Beta - blocker
Aspirin / Clopidogrel
ACE-Inhibitor/ATRB
Diuretics
Statin therapy
0
0
0
0
0
6 (75.0%)
100%
100%
4 (50.0%)
5 (62.5%)
0.003
0.000
0.000
0.038
0.013
Total cholesterol (mg/dl) 180.57 ± 38.15 181.38 ± 35.89 0.967
LDL cholesterol (mg/dl) 103.57 ± 38.94 103.63 ± 37.20 0.998
Triglycerides (mg/dl) 77.57 ± 77.27 125.63 ± 48.66 0.167
HDL cholesterol (mg/dl) 61.67 ± 22.47 52.84 ± 14.91 0.380
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online table IV: Down‐regulated miRNAs in patients with CAD
Healthy controls CAD
microRNA MW SEM MW SEM fold t-test hsa-miR-199a-5p 6,7 0,6 3,4 0,6 0,50 0,00 hsa-miR-221 6,8 0,8 3,6 0,6 0,52 0,01 hsa-let-7d 8,6 0,7 5,0 0,8 0,58 0,00 hsa-miR-23a 11,2 0,5 6,8 0,9 0,61 0,00 hsa-miR-548b-3p 5,1 0,4 3,3 0,4 0,64 0,01 hsa-miR-23b 10,9 0,4 7,0 0,7 0,64 0,00 hsa-miR-26a 11,4 0,5 7,4 0,7 0,65 0,00 hsa-miR-106b 8,2 0,4 5,5 0,4 0,67 0,00 hsa-miR-106a 10,0 0,4 6,7 0,7 0,67 0,00 hsa-miR-320a 10,1 0,4 6,9 0,6 0,68 0,00 hsa-miR-17 10,0 0,4 6,9 0,6 0,68 0,00 hsa-miR-616Star 5,3 0,3 3,6 0,4 0,69 0,01 hsa-miR-126 10,9 0,5 7,6 0,6 0,70 0,00 hsa-miR-361-5p 7,6 0,5 5,3 0,5 0,70 0,01 hsa-miR-181a 8,2 0,3 5,8 0,3 0,70 0,00 hsa-miR-27a 8,1 0,5 5,7 0,3 0,71 0,00 hsa-miR-199b-3p 8,3 0,3 5,9 0,2 0,71 0,00 hsa-miR-151-5p 9,3 0,4 6,7 0,5 0,72 0,00 hsa-miR-191 10,7 0,5 7,7 0,6 0,72 0,00 hsa-miR-320b 7,2 0,4 5,3 0,5 0,74 0,01 hsa-miR-603 7,7 0,1 5,8 0,3 0,75 0,00 hsa-miR-130a 9,5 0,4 7,2 0,4 0,75 0,00 hsa-miR-25 8,4 0,3 6,4 0,5 0,75 0,00 hsa-miR-30d 8,4 0,3 6,4 0,4 0,76 0,00 hsa-miR-21 8,4 0,4 6,3 0,4 0,76 0,00 hsa-miR-1469 8,1 0,2 6,1 0,5 0,76 0,01 hsa-miR-93 8,5 0,5 6,5 0,2 0,77 0,00 hsa-miR-484 7,8 0,4 6,0 0,2 0,77 0,00 hsa-miR-1305 7,8 0,1 6,1 0,2 0,78 0,00 hsa-miR-20a 9,1 0,4 7,2 0,5 0,79 0,01 hsa-miR-150 7,8 0,3 6,2 0,2 0,79 0,00 hsa-miR-1254 7,7 0,2 6,1 0,2 0,80 0,00 hsa-miR-29c 6,7 0,2 5,4 0,3 0,80 0,00 hsa-miR-142-5p 7,8 0,3 6,3 0,2 0,80 0,00 hsa-miR-301a 8,0 0,2 6,5 0,3 0,80 0,00 hsa-miR-1249 10,2 0,4 8,2 0,5 0,80 0,01 hsa-miR-29a 7,3 0,4 5,9 0,2 0,81 0,01 hsa-miR-92a 10,4 0,4 8,4 0,6 0,81 0,01 hsa-miR-15b 10,6 0,4 8,6 0,5 0,81 0,01 hsa-miR-335 8,6 0,2 7,0 0,2 0,81 0,00 hsa-miR-29b 7,6 0,1 6,2 0,2 0,82 0,00 hsa-miR-32 8,2 0,1 6,7 0,2 0,82 0,00 hsa-miR-139-5p 8,2 0,1 6,7 0,1 0,82 0,00 hsa-miR-199a-3p 8,0 0,4 6,6 0,1 0,82 0,01 hsa-miR-296-5p 8,0 0,2 6,5 0,1 0,82 0,00 hsa-miR-424 7,5 0,3 6,2 0,3 0,82 0,01 miRNAs were detected by GeniomeR Biochips in healthy controls (n=8) or patients with CAD (n=8). miRNAs shown in the table were selected by basal expression level in healthy controls (cut off >5) and statistical difference between groups ( p<0.01 ; t‐test).
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online Table V: Up‐regulated miRNAs
Healthy controls CAD microRNA MW SEM MW SEM fold t-test hsa-miR-185Star 4,4 0,3 6,7 0,5 1,52 0,00hsa-miR-208b 3,8 0,3 5,6 0,1 1,46 0,00hsa-miR-571 4,1 0,2 5,8 0,2 1,43 0,00hsa-miR-1303 3,9 0,3 5,4 0,3 1,41 0,00hsa-miR-541 4,5 0,4 6,2 0,2 1,38 0,01hsa-miR-573 4,1 0,3 5,6 0,2 1,37 0,00hsa-miR-224 3,7 0,3 5,0 0,2 1,36 0,00hsa-miR-615-5p 3,8 0,2 5,1 0,2 1,35 0,00hsa-miR-1252 3,3 0,1 4,4 0,2 1,35 0,00hsa-miR-300 3,8 0,3 5,1 0,3 1,34 0,01hsa-miR-548g 3,9 0,3 5,0 0,1 1,30 0,01hsa-miR-659 4,6 0,4 5,9 0,2 1,30 0,01hsa-miR-487a 4,6 0,3 5,9 0,2 1,29 0,00hsa-miR-1323 4,2 0,3 5,3 0,3 1,28 0,01hsa-miR-920 3,8 0,2 4,9 0,3 1,28 0,01hsa-miR-1292 4,3 0,3 5,5 0,2 1,27 0,00hsa-miR-1296 4,3 0,1 5,5 0,2 1,26 0,00hsa-miR-34bStar 4,8 0,3 6,0 0,2 1,25 0,01hsa-miR-668 4,2 0,2 5,3 0,2 1,24 0,01hsa-miR-592 4,9 0,2 5,9 0,3 1,21 0,01
miRNAs were detected by GeniomeR Biochips in healthy controls (n=8) or patients with CAD (n=8). miRNAs shown in the table were selected for >1.2‐fold increased expression in patients with CAD compared to healthy controls and p<0.01 (t‐test).
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online Table VI:
Correlation of circulating miRNAs with baseline characteristics (analysis includes patients and health volunteers)
miR‐ 126
miR‐ 17
miR‐92a
miR‐199a
miR‐155
miR‐145
miR‐133a
miR‐208a
Age (Pearson)
R=‐.109 P=.435 N=53
R=‐.119 P=.396 N=53
R=‐.110P=431 N=53
R=‐.181P=.194 N=53
R=‐.395P=0.003 N=53
R=‐.205 P=.154 N=50
R=.036 P=.800 N=53
R=.157P=.261 N=53
Gender (Spearman)
R=225P=.105 N=53
R=.173 P=.216 N=53
R=.045P=.749 N=53
R=.148P=.291 N=53
R=.401P=0.003 N=53
R=.240 P=.093 N=50
R=.208 P=.135 N=53
R=‐.252P=.069 N=53
Cholesterol (Pearson)
R=.156P=.269 N=52
R=.124 P=.379 N=52
R=.237P=.091 N=52
R=.076P=.591 N=52
R=. 363P=0.008 N=52
R=.053 P=.718 N=49
R=.012 P=.932 N=52
R=‐.108P=.444 N=52
HDL (Pearson)
R=.071P=.617 N=52
R=.124 P=.381 N=52
R=.254P=0.07 N=52
R=.085P=.548 N=52
R=.376P=0.006 N=52
R=.094 P=.522 N=49
R=‐.058 P=.684 N=53
R=‐.316P=0.023 N=53
LDL (Pearson)
R=.184P=.202 N=50
R=.122 P=.399 N=50
R=.201P=.161 N=50
R=.032P=.824 N=50
R=.325P=.021 N=50
R=.061 P=.684 N=47
R=.088 P=.544 N=50
R=‐.062P=.670 N=50
Triglyceride (Pearson)
R=‐.107 P=.451 N=52
R=‐.113 P=.424 N=52
R=‐.069P=.629 N=52
R=‐.090P=.524 N=52
R=‐.169P=.232 N=52
R=‐.157 P=.280 N=49
R=‐.055 P=.701 N=52
R=.121P=.391 N=52
Creatinin (Pearson)
R=‐.321 P=.056 N=36
R=‐.260 P=.126 N=36
R=‐.211P=.217 N=36
R=.005P=.979 N=36
R=‐.390P=.019 N=36
R=‐.278 P=.117 N=33
R=‐.354 P=.034 N=36
R=.018P=.919 N=36
Urea (Pearson)
R=‐.150 P=.381 N=36
R=‐.247 P=.147 N=36
R=‐.163P=.343 N=36
R=‐.106P=.540 N=36
R=‐.393P=.018 N=36
R=‐.346 P=0.049 N=33
R=‐.226 P=.185 N=36
R=.016P=.926 N=36
Diabetes (Spearman)
R=‐.243 P=.079 N=53
R=‐.312 P=.023 N=53
R=‐.263P=.057 N=53
R=‐.279P=.043 N=53
R=‐.315P=.021 N=53
R=‐.265 P=.063 N=50
R=‐.174 P=.212 N=53
R=‐.007P=.959 N=53
Leukocytes (Pearson)
R=.064P=.713 N=36
R=.086 P=.616 N=36
R=‐.123P=.474 N=36
R=.149P=.385 N=36
R=.194P=.257 N=36
R=.245 P=.170 N=33
R=.041 P=.810 N=36
R=.194P=.258 N=36
Statins (Spearman)
R=‐.551 P=.000 N=53
R=‐.503 P=.000 N=53
R=‐.393P=.004 N=53
R=‐.538P=.000 N=53
R=‐.528P=.000 N=53
R=‐.475 P=.000 N=50
R=‐.333 P=.015 N=53
R=‐.260P=.06 N=53
ACE/AR‐Blockers (Spearman)
R=‐.381 P=.005 N=53
R=‐.331 P=.015 N=53
R=‐.164P=.240 N=53
R=‐.453P=.001 N=53
R=‐.331P=.015 N=53
R=‐.335 P=.017 N=53
R=‐.219 P=.115 N=53
R=.052P=.713 N=53
Aspirin (Spearman)
R=‐.469 P=.000 N=53
R=‐.403 P=.003 N=53
R=‐.318P=.020 N=53
R=‐.522P=.000 N=53
R=‐.494P=.000 N=53
R=‐.473 P=.001 N=50
R=‐.328 P=.017 N=53
R=.185P=.185 N=53
Red indicates significant correlations, gray background indicates no significant correlation. All patients classified as on statin therapy received statins for > 3 months.
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online Table VII: Correlation of circulating miRNAs with baseline characteristics (analysis includes only patients)
mir126 mir17 mir92a mir199a mir155 mir145 mir133a mir208a Statins r= -,336(*) -0,321 -0,313 -0,205 -0,197 -0,186 -0,135 0,208
p= 0,045 0,056 0,063 0,231 0,249 0,299 0,431 0,223N= 36 36 36 36 36 33 36 36
ACE/AR Blockers
r= -0,022 0,014 0,222 -0,072 -0,237 -0,008 0 -0,083p= 0,901 0,934 0,192 0,678 0,164 0,964 1 0,629N= 36 36 36 36 36 33 36 36
Asprin r= -0,196 -0,136 -0,153 -0,238 -0,111 -0,185 -0,102 0,036 p= 0,253 0,429 0,373 0,162 0,521 0,302 0,553 0,835 N= 36 36 36 36 36 33 36 36
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Online Table VIII: Characteristics of validation study cohort
Controls
(n=14)
Patients with CAD
(n=31)
P-value
Gender Male 5 (36%) 21 (68%) 0.057
Age (years) 39.28 ± 17.52 68.06 ± 9.66 0.000
Stable CAD for at least 4 months 0 31 (100%) 0.000
Number of vessels
(CAD) 0
I: 4 (13.8%)
II: 10 (34.5%)
III: 15 (51.7%)
0.000
0.000
0.000
Hypertension 3 (21.4%) 30 (96.8%) 0.000
Active smoker 7 (53.8%) 8 (25.8%) 0.076
Diabetes mellitus 2 (14.3%) 8 (25.8%) 0.469
History of
AMI/PCI/ACVB/PTA/Stroke 0 31 (100%) 0.000
Concurrent medication:
Beta - blocker
Aspirin / Clopidogrel
ACE-Inhibitor / ATRB
Statin therapy
2 (14.3%)
4 (28.6%)
3 (21.4%)
1 (7.1%)
20 (64.5%)
31 (100%)
24 (77.4%)
15 (48.4%)
0.003
0.000
0.001
0.007
Total cholesterol (mg/dl) 207.36 ± 32.21 201.68 ± 48.86 0.694
LDL cholesterol (mg/dl) 114.29 ± 40.22 112.93 ± 38.79 0.915
Triglycerides (mg/dl) 108.71 ± 42.05 181.19 ± 91.14 0.007
HDL cholesterol (mg/dl) 65.19 ± 18.52 51.48 ± 16.23 0.016
by on September 3, 2010 circres.ahajournals.orgDownloaded from

Extended method section
RNA isolation
RNA was isolated by using a trizol-based miRNA isolation protocol (Trizol BD from Sigma).
Due to high phenol contamination in these samples, additional isopropanol or ammonium
precipitation steps were included. In addition, we used a miRNA kit provided by Qiagen
(miRNeasy), which combines phenol/guanidine-based lysis of samples and silicamembrane-
based purification of total RNA (>18 nt) in combination with the blood derivate-specific Trizol
BD from Sigma. In detail, 250 µl plasma or serum were mixed with 700 µl Trizol BD,
incubated for 5 min at room temperature and subsequently mixed with 140 µl chloroform.
The organic and aqueous phase was separated by centrifugation. The aqueous phase
containing the RNA was carefully removed and RNA was precipitated by addition of 100%
ethanol. The mixture was applied to a RNeasy Mini spin column, washed several times and
RNA was eluted by addition of 25 µl RNase-free water. All methods were tested in serum
and plasma samples from healthy controls. The optimized protocol using the Qiagen miRNA
kit was then used for all subsequent studies with 250 µl EDTA plasma or serum.
by on September 3, 2010 circres.ahajournals.orgDownloaded from