the role of carotid artery screening before coronary artery bypass graft surgery
TRANSCRIPT
1The Journal of Tehran Heart Center
Editor – in – Chief Abbasali Karimi, MD Tehran University of Medical Sciences, IRAN
Associate Editor Alimohammad Haji Zeinali, MDTehran University of Medical Sciences, IRAN
Editorial Board Hosein Ahmadi, MDTehran University of Medical Sciences, IRANShahin Akhondzadeh, PhD Tehran University of Medical Sciences, IRANZohair Yousef Al-halees, MD, FRCSKing Faisal Specialist Hospital & Research Centre Riyadh, SAUDI ARABIABahram Aminian, MDShiraz University of Medical Sciences, IRANHooshang Bolooki, MD, FRCS (C)University of Miami, USA Mohammad ali Boroumand, MDTehran University of Medical Sciences, IRANAhmad Reza Dehpour, PhDTehran University of Medical Sciences, IRANYadolah Dodg, PhD University of Neuchatel, SWITZERLANDAli Dodg –Khatami, MD, PhD University of Zurich, SWITZERLANDIradj Gandjbakhch, MDHopital pitie, Paris, FRANCEAlimohammad Haji Zeinali, MDTehran University of Medical Sciences, IRANOmer Isik, MDYeditepe University, Ankara, TURKEYSami S Kabbani, MD Damascus University, SYRIAKayvan Kamalvand, MD, FRCP, FACCGuy’s & St Thomas’ Hospital Trust, London, UK Abbasali Karimi, MDTehran University of Medical Sciences, IRANDavood Kazemi Saleh, MDBaghiatollah University of Medical Sciences, IRANMajid Maleki, MD Iran University of Medical Sciences, IRANMehrab Marzban, MD Tehran University of Medical Sciences, IRAN Ali Massumi, MDTexas Heart Institute, USACarlos A Mestres, MD, PhD University of Barcelona, SPAINSeyed Rasol Mirsharifi, MDTehran University of Medical Sciences, IRAN Ahmad Mohebi, MD Iran University of Medical Sciences, IRANMahmood Mirhoseini, MDMedical College of Wisconsin, USAMansoor Moghadam, MDTehran University of Medical Sciences, IRANSina Moradmand, MD Tehran University of Medical Sciences, IRAN Ebrahim Nematipoor, MDTehran University of Medical Sciences, IRANMohammed T Numan, MDHamad Medical Corporation, Doha, QATAR Ahmad S Omran, MD, FACC, FASEKing Abdulaziz Medical City, SAUDI ARABIARezayat Parvizi, MDTabriz University of Medical Sciences, IRANMasoud Pezeshkian, MDTabriz University of Medical SciencesHasan Radmehr, MDTehran University of Medical Sciences, IRANMehrdad Rezaee, MD, PhD Stanford University, USASaeed Sadeghian, MDTehran University of Medical Sciences, IRANMojtaba Salarifar, MDTehran University of Medical Sciences, IRANLee Samuel Wann, MDMedical College of Wisconsin, USA
The Journal of Tehran Heart Center Nizal Sarraf –Zadegan, MDIsfahan University of Medical Sciences, IRANAhmad Yaminisharif, MDTehran University of Medical Sciences, IRANMohammad Reza Zafarghandi, MDTehran University of Medical Sciences, IRANAli Akbar Zeinaloo, MDTehran University of Medical Sciences, IRAN
Managing EditorSeyed Hesameddin Abbasi, MDTehran Heart Center, Research Department, IRAN
Advisory Editors Kyomars Abbasi, MDTehran University of Medical Sciences, IRAN Seifollah Abdi, MDIran University of Medical Sciences, IRANMohammad Alidoosti, MDTehran University of Medical Sciences, IRAN Naser Aslanabadi, MDTabriz University of Medical Sciences , IRANAlireza Amirzadegan, MDTehran University of Medical Sciences, IRAN Sirous Darabian, MDTehran University of Medical Sciences, IRAN Gholamreza Davoodi, MDTehran University of Medical Sciences, IRAN Saeed Davoodi, MDTehran University of Medical Sciences, IRAN Iraj Firoozi, MDIran University of Medical Sciences, IRANSeyed Ebrahim Kassaian, MDTehran University of Medical Sciences, IRANSeyed Khalil Foroozannia, MDYazd University of Medical Sciences, IRANAli Ghaemian, MDSari University of Medical Sciences, IRAN Namvar Ghasemi Movahedi, MDTehran University of Medical Sciences, IRAN Abbas Ghiasi, MDTehran University of Medical Sciences, IRAN Mohammad Hashemi, MDIsfahan University of Medical Sciences, IRAN Ali Kazemi Saeed, MDTehran University of Medical Sciences, IRAN Jalil Majd Ardekani, MDTehran University of Medical Sciences, IRANFardin Mirbolook, MDRasht University of Medical Sciences, IRANMehdi Najafi, MDTehran University of Medical Sciences, IRAN Yoones Nozari, MDTehran University of Medical Sciences, IRANHamid Reza Poorhosseini, MDTehran University of Medical Sciences, IRAN Habibollah Saadat, MD Shahid Beheshti University of Medical Sciences, IRAN Hakimeh Sadeghian, MDTehran University of Medical Sciences, IRANAbbas Salehi Omran, MDTehran University of Medical Sciences, IRANAbbas Soleymani, MDTehran University of Medical Sciences, IRAN Mahmood Shabestari, MDMashhad University of Medical Sciences, IRAN Shapour Shirani, MDTehran University of Medical Sciences, IRANAbdolhosein Tabatabaei, MDTehran University of Medical Sciences, IRANArezoo Zoroofian, MDTehran University of Medical Sciences, IRAN
Office Shima SadeghiZahra Reshadati
In the name of God
Tel: +98 21 88 02 97 02Fax: +98 21 88 02 97 02E-mail: [email protected]
The Journal of Tehran Heart Center
2
ContentVolume: 1 Number: 1 Spring 2006
The Journal of Tehran Heart Center
Editorial
My Dear Colleagues, Editor in Chief .................................................................................................................................................3
Review Article
Antipsychotic Drugs and Sudden Death Seyed Hesameddin Abbasi, Khosro Afkham, Shahin Akhondzadeh……………………….………………………..….........................……….5
Original Articles
The Sheep as a Model for Coronary Artery Surgery Experiments on Beating Heart Drissi Boumzebra, Jan Otto Solem, Shaheen Nakeeb, Zohair Al Halees ……………....................................................................................... 11 Moderate Mitral Regurgitation and Coronary Disease: Treatment with Coronary Bypass Alone? Hakimeh Sadeghian, Abbassali Karimi, Hosein Ahmadi, Saeed Sadeghian, Mojtaba Salarifar, Kyomars Abbasi, Navid Paydari, Mohammad Majd………………………………........................................................................................................................17 Surgical Radiofrequency MAZE III Ablation for Treatment of Atrial Fibrillation During Open Heart Surgery Rezayat Parvizi, Fariborz Akbarzadeh ………………………………................................................................................................................23 The Role of Carotid Artery Screening Before Coronary Artery Bypass Graft Surgery Shapour Shirani, Mohammad Ali Boroumand, Seyed Hesameddin Abbasi, Negar Maghsoodi, Majid Shakiba, Abbasali Karimi, Saeed Davoodi, Maryam Esfandbod ………………………………………………………….….........................................29 . Cardiac Abnormalities in the Iranian Pediatric and Adolescent Population with Chronic Renal Failure Ali Akbar Zeinaloo, Abbas Madani, Mohammad Taqi Haqi Ashtiani ……………………………………........................................................33
Comparison of Specifications, Short Term Outcome and Prognosis of Acute Myocardial Infarction in Opium Dependent Patients and Nondependents Gholamreza Davoodi, Saeed Sadeghian, Shahin Akhondzadeh, Soodabeh Darvish, Mohammad Alidoosti, Alireza Amirzadegan ……………………………………………………………………………………………………...................……...………….43 Brief Communication Main Pulmonary Artery Hydatidosis with Seconday Involvement of the Lungs: a Shepherd Boy’s Story Ali Mohammad Haji Zeinali, Kyomars Abbasi, Hakimeh Sadeghian, Navid Paydari .......................................................................................49
Case Report
Bifurcating Radial Artery: a Useful Anatomic Variation for Coronary Artery Bypass Grafting Mehrab Marzban, Seyed Hesameddin Abbasi, Amirali Rahnemay Azar ……………………...........................................................................53
3The Journal of Tehran Heart Center
Editorial
Abbasali Karimi, MD* Editor in Chief
My Dear Colleagues Over the past two centuries, the industrial and technological revolutions and their associated economic and social
transformation have resulted in dramatic shifts in the diseases responsible for illness and death. Cardiovascular Disease (CVD) has emerged as the dominant chronic disease in many parts of the world, and early in the
21st century it is predicted to become the main cause of disability and death worldwide. At the beginning of the 20th century, CVD accounted for less than 10 percent of all deaths worldwide. At the beginning
of the 21st century CVD accounts for nearly half of all deaths in the developed world and a Quarter of all deaths in the developing world. By 2020 it is predicted that CVD will claim 25 million lives annually and Coronary Heart Disease (CHD) will surpass infectious disease as the world’s number one cause of death and disability. This global rise in CVD is the result of a dramatic shift in the health status of individuals around the world during the course of the 20th century.
Before 1900, infectious disease and malnutrition were the most common causes of death. These have been gradually supplanted in some (mostly developed) countries by chronic diseases such as CVD and cancer, thanks largely to improved nutrition and public health measures. As this trend spreads to developing countries, CVD will dominate as the major cause of death by 2020, accounting for at least one in every three deaths.
Continued improvements in living standards, urbanization and radical changes in the nature of work-related activities lead to dramatic life-style changes in diet, activity levels and behaviors such as smoking.
Easier access to less expensive foods and increased fat content increase total caloric intake, whereas mechanization results in lower daily caloric expenditure.
This disparity leads to a higher mean body mass index, Blood pressure and levels of plasma lipids and blood sugar. These changes set the stage for the emergence of hypertensive diseases and atherosclerosis.
In industrialized nations, however, major technological advances such as coronary care units, bypass surgery, percutaneous coronary interventions, and thrombolytic therapy are available to manage the acute manifestations of CVD. Preventive strategies such as smoking cessation and blood pressure management are widely implemented. As a result of better treatment and widespread primary and secondary prevention efforts, deaths are prevented among people with disease and primary event are delayed.
We are now halfway through a two-century transition in which CVD will dominate as the major cause of death and disease. Although CVD rates are declining in the developing countries, they are increasing in virtually every other region of the world. Each region of the world faces major challenges presented by the epidemic of CVD. There is no single global solution to the rising burden of CVD given the vast differences in social, cultural, and economic circumstances.
In Iran we must find ways to efficiently care for increasing numbers of individuals with CVD as well as to deploy low-cost preventive strategies.
Allocation of resources to less-expensive preventive strategies will likely be more less-expensive than dedicating resources to expensive measures.
*Associate Professor of Cardiac Surgery of Tehran University of Medical Sciences. Director of Tehran Heart Center, Tel: 88029722. Fax: 8802924. P.O.BOX: 14395-477. E-mail: [email protected]

4
5The Journal of Tehran Heart Center
Review Article
Antipsychotic Drugs and Sudden Death
Seyed Hesameddin Abbasi, MD1, Khosro Afkham, MD2, Shahin Akhondzadeh, PhD2*
1National Iranian Oil Company Central Hospital, Tehran, Iran.
2Psychiatric Research Center, Roozbeh Psychiatric Hospital, Tehran University of Medical Sciences, Tehran, Iran.
Abstract
Sudden, unexpected death may occur in apparently healthy individuals. Its occurrence in psychiatric patients has raised the concern that the use of psychotropics, especially antipsychotics, may be associated with an increased risk of sudden death. This concern is maintained even though not all psychiatric patients who have succumbed to sudden death have been on psychotropics. Early reports presented the concern that the use of chlorpromazine and thioridazine were associated with sudden death. More recently, the focus shifted to the more potent agents. Indeed, the FDA Advisory Committee discussed the possibility of a connection between sudden death and haloperidol. No decision could be reached by the FDA Committee be-cause of the enormous complexity of the problem. Nonetheless, since sudden death continues to catastrophically complicate the course of some patients, the scope of this review is to further investigate the relationship between antipsychotic agents and sudden death.
The Journal of Tehran Heart Center 1 (2006) 5-9
Keywords: Antipsychotic • QT prolongation • Sudden death
*Corresponding Author: Shahin Akhondzadeh, Psychiatric Research Center, Roozbeh Psychiatric Hospital, Tehran University of Medical Sciences, South Kargar Street, Tehran 13337, Iran. P.O.BOX: 1741. Tel: 98-21-55412222. Fax: +98-21-55419113. Email: [email protected].
There is widespread, serious concern about the hazards of psychotropic medication, particularly sudden death with high doses of antipsychotic (narcoleptic) drugs. This concern follows several reports of unexpected deaths in young people, usually males, where the concurrent prescription of antipsychotic drugs has been implicated. The public perception is that these deaths occur when the medication is used in high dosage in disturbed patients. There is some suspicion of an ethnic bias, with young men of Afro-Caribbean origin being more commonly involved, although no data exist to substantiate this. The death rate among psychiatric patients tends to be higher than that of the general population, but suicide and accidental deaths may account
for much of this excess.1,2 Sudden, unexpected death is perhaps more common in the general population than might be expected. It has been estimated that between 15–30% of all natural fatalities in the industrially developed world occur suddenly and unexpectedly.3,4 Davies has suggested that there are 50–100 sudden deaths in Britain every year that could be categorized as due to the sudden adult death syndrome, and for which there is no specific explanation.5,6 Nevertheless, it would seem that the cardiovascular mortality of patients with chronic schizophrenia exceeds that of the general population7 and the cardiovascular toxicity of neuroleptics may be a contributory factor.
Antipsychotic (neuroleptic) drugs have generally been

The Journal of Tehran Heart Center
6
regarded as a group of drugs with a good margin of safety, but there have been regular case reports of sudden death associated with these agents since the 1960s. Committee on Safety of Medicines have received reports of 31 cases of unexplained sudden death and 63 reports of fatal cardiac arrest/arrhythmias in association with people treated with various antipsychotic drugs, covering the period that each drug was introduced up to May 1996. The role played by antipsychotic drugs is often uncertain, but when sudden death occurs in previously healthy, young individuals a common conjecture is that medication played a part. It is essential that epidemiological evidence is gathered to determine the extent of this problem, and that the relevant pharmacological and physiological mechanisms are clarified. This is a key task, and has yet to be undertaken.
The first step in such an investigation would be to agree a definition of sudden death. Brown & Kocsis (1984) referred to “death occurs instantaneously or within 24 hours of the onset of acute illness”, excluding death by suicide, homicide or accident.7 The following definition is taken from Jusic & Lader (1994): Sudden, unexpected, unexplained death can be defined as death within one hour of symptoms8 (excluding suicide, homicide and accident)9 which is both unexpected in relation to the degree of disability before death10 and unexplained because clinical investigation and autopsy failed to identify any plausible cause.11
Schizophrenia
Schizophrenia is a relatively uncommon disease in the general population with prevalence between 1.4–4.6 per 1000 population at risk, an incidence rate for new cases in the range of 0.2–0.4 per 1000, and a morbid lifetime risk around 1% (12-14). It varies in its severity and its clinical course. Although the illness represents a major part of the workload of specialist psychiatric in-patient and out-patient practice, its management is not confined to psychiatrists. Many affected patients are treated exclusively in general practice while others are stabilized in specialist practice before being returned to their general practice for long-term follow-up and care. It is thought that a substantial proportion of the vagrant population is affected with schizophrenia-like illnesses. Among this subgroup the disease may be seen in its more florid form because of the lack of treatment. The main treatment is antipsychotic medication. The duration of treatment varies between patients, as does the dose that is required for control of the symptoms. None of the drugs currently available is free from the risk of adverse effects, all produce side-effects. The principal side-effects include extra pyramidal symptoms (Parkinsonism, akathisia, dystonia and tardive dyskinesia), hypotension, and interference with the temperature regulating system, the so-called neuroleptic malignant syndrome, and a number of idiosyncratic effects on the cardiac system.
Some of the side-effects and adverse effects are dose-related. Interactions between antipsychotics and other medication have been documented. For example, the concurrent use of phenothiazines and tricyclic antidepressants can result in a rise in the blood levels of the two drugs with a consequent increase in the risk of dose-related side-effects of both.12,15
Cardiac effects of antipsychotic drugs
Abnormalities of the electrocardiogram (ECG) are relatively common in people receiving neuroleptics, occurring in around 25%.16,18 There are numerous reports of ventricular arrhythmias associated with repolarisation disturbances such as prolonged QT intervals, widening of QRS complexes, depression of ST segments and most commonly abnormal T-morphology or large U-waves.19-27
They are observed more often in patients with pre-existing heart disease.28 The phenothiazine group of antipsychotics display electrophysiological properties like those of the class IA antiarrhythmic agents (quinidine-like), involving blockade of potassium and sodium channels, leading to a prolonged duration of the action potential (which also slows conduction), refractory period and QT interval. However, members of other antipsychotic classes such as haloperidol and droperidol, butyrophenones,29-31 pimozide, a diphenylbutylpiperidine,32 and sultopride, a substituted benzamide,33 have also been reported to cause QT prolongation. Warner et al (1996) found that QTc (QT interval corrected for heart rate) prolongation (>420 ms) was significantly more common (23%) in a sample of 111 chronic in-patients with schizophrenia receiving antipsychotic medication than in 42 age-matched, drug-free controls (2%).34 QTc prolongation was also significantly more likely in those patients receiving mega doses, that is, above 2000 mg chlorpromazine equivalents a day. A new antipsychotic drug, sertindole, introduced in July 1996, can also cause prolongation of the QT interval. The prescribing information for the drug states that it is contraindicated in patients with prolongation of the QT interval and that all patients should have an ECG performed before the drug is started and Thensubsequently at regular intervals. According to a report in the Lancet,35 there was disagreement over the safety of sertindole at the meeting of the Food and Drug Administration advisory committee at which the drug was approved. These ECG changes have commonly been considered benign, and even now there is no consensus on the clinical significance of prolonged QTc.36 However, QT prolongation with other compounds has been shown to produce serious arrhythmias that have sometimes proved fatal. Drug-induced QTc prolongation may be important even if the mean increase is not very large. For example, the drug terodiline was withdrawn after causing QT prolongation, torsade de pointes, and sudden death. In healthy volunteers, therapeutic plasma concentrations are associated with increases in mean QTc of only 23 ms, which are similar to the increases associated with quinidine and prenylamine. Nevertheless, much larger increases occurred in a minority
Seyed Hesameddin Abbasi et al

7The Journal of Tehran Heart Center
Antipsychotic Drugs and Sudden Death
of patients who developed arrhythmias. These included those predisposed by existing problems such as heart disease and congenital repolarisation abnormalities. Thus, apparently benign QT prolongation in one subject may indicate that another more susceptible patient might develop extreme QT prolongation and arrhythmias with the same drug at the same dose.
Furthermore, small increases in QT interval may increase the risk of VT/ torsade de pointes. Although the increased risk is probably small, because minor QT prolongation is common the risk is applied over a large population. The number of excess cases of sudden death in the large numbers of patients with minor QT prolongation may exceed those in the small numbers of patients with extreme QT prolongation. In his review of drug-induced QT prolongation, Thomas (1994) was of the opinion that neuroleptic drugs presented a particular hazard in terms of provoking dysrhythmias (proarrhythmia) as they are commonly prescribed “in high doses and in combination”, by psychiatrists who have little training in detecting such problems. A lack of ECG facilities and interpretation
May be particular problems.36. Thioridazine, and less frequently, chlorpromazine, have been particularly implicated in the development of ventricular tachycardia, primarily in patients taking overdoses.8
For example, Buckley et al (1995) investigated the clinical andelectrocardiographic features associated with neuroleptic poisoning and compared thioridazine with other neuroleptics.37 of 299 consecutive patients admitted with neuroleptic poisoning, the mostcommonly ingested drug was thioridazine (104 patients). The other antipsychotics taken were chlorpromazine,19 trifluoperazine,36 pericyazin35, haloperidol,33 prochlorperazine, 18 fluphenazine,8 or other neuroleptics.7 Sixteen patients who had ingested more than one neuroleptic were excluded from comparative analysis. After taking into account variables such as for age, sex, dose ingested and co-ingestion of tricyclic antidepressants or lithium, thioridazine was still found to be significantly more likely to cause tachycardia, a prolonged QT interval, prolonged QTc (> 450 ms), a widened QRS (> 100 ms) and arrhythmias. Fulop et al (1987) noted that ECG abnormalities had been found in 10% of patients treated with pimozide, leading to recommendations in the USA and UK for periodic ECGs in patients receiving this drug.38 They commented that the abnormalities included prolongation of the QTc interval which increases the risk of a potentially fatal arrhythmia. From 1971 to 1995, the Committee on Safety of Medicines received 40 reports (16 fatal) of serious cardiac reactions, predominantly arrhythmias, with pimozide.39 The recommendations to doctors included an annual ECG for patients receiving the drug, and if the QT interval were prolonged, review of whether to withdraw the treatment and continue under close supervision. Torsade de pointes is a particular cardiac problem related to antipsychotic medication that has been implicated as a possible cause of sudden death,
in those individuals with a past history of disturbances of cardiac rhythm or other cardiac symptoms. This arrhythmia is a variant of paroxysmal ventricular tachycardia associated with a prolonged QT interval or prominent U waves on the ECG.40-43 although torsade de pointes may remit spontane ously, it is potentially lethal in that it can progress to ventricular fibrillation.44 Torsade de pointes may be asymptomatic or cause self-limiting palpitations, while a minority of episodes may precipitate sudden death. This arrhythmia has been reported in association with antipsychotic drugs, specifically haloperidol45-50 and thioridazine.40,51
How do drugs lengthen the QT interval and produce ventricular arrhythmias?
The QT interval represents the combined duration of the action potential and the subsequent ventricular repolarisation phase. The action potential is caused by fast-activating and inactivating sodium and calcium currents. Its length is largely determined by an ensuing plateau phase. Repolarisation occurs when the net outward current becomes dominant. This current is regulated by potassium efflux and influx through six or more different channels. of these, three are dominant, iK1, iK, and iT0. The basal potassium current is determined by iK1, which is blocked by inorganic ions including magnesium, and quinidine, and modulated by vagal activity. The delayed rectifier current, iK, is modulated by beta receptor occupancy, stimulation of adenylate cyclase, and production of cAMP. IK and iT0-like currents are the target of most known Class III antiarrhythmic agents, such as amiodarone. Although our understanding of the electrophysiological effects of antipsychotics is incomplete, it seems that, in addition to general membrane stabilizing properties, antipsychotic drugs and their metabolites may have selective and differing effects on the ion channels which govern length of the QT interval. For example, thioridazine has been shown to decrease the velocity of the action potential upstroke without altering the resting potential, whereas chlorpromazine has a greater effect on the resting potential.52 One important prediction from this is that drugs would differ in their propensity to cause arrhythmias, although no comparative studies have yet been done. Whether a drug-induced QT prolongation results in an arrhythmia depends on the presence of one or both of
the following.31 Increased cellular excitability. Early after-depolarisations
are associated with abnormal repolarisation and interrupt the repolarisation process. Torsade de pointes characteristically interrupt terminal repolarisation of a markedly prolonged QT interval, especially in the presence ofbradycardia.52
Abnormal dispersion of prolonged ventricular repolarisation.
This would favour a re-entrant mechanism, as different parts of the ventricle remain refractory for differing periods.53 slow conduction also favours re-entry. Cardiac risk factors

The Journal of Tehran Heart Center
8
for torsade de pointes may also include frequent ventricular ectopics which may trigger the phenomenon by landing on a T wave. Also, QT dispersion is much larger after a ventricular premature contraction and this may increase the risk.
What other factors interact with drug-induced QT interval prolongation to increase the risk of sudden death?
Although QT interval prolongation is common, proarrhythmic events are rare, and death is rarer still.52 this seems in part to be because one or more additional cofactors may be required to trigger an arrhythmia in the pres ence of QT interval prolongation. These cofactors may be grouped as follows.
Cardiac
Congenital long QT syndromes (LQTS), such as Romano Ward, Jervell and LangeNielsen, ischaemic heart disease, myocarditis, sinus bradycardia <60 beats perminute.52
Other drugs Additively, by directly lengthening the QT interval, or indirectly, by altering the metabolism of drugs which directly lengthen
The QT interval.54 Drugs may also affect the risk of torsade de pointes by changing heart rate, as risks are higher at slower rates, or by altering sensitivity to catecholamines.
Metabolic
Hypokalaemia, hypomagnesaemia, hypocalc-emia, hypothermia. Causes of autonomic instability Stress and extremes of emotion,55 extremes of physical exertion, sudden shocks.56
Other cardiac mechanisms for sudden death
It has also been suggested that antipsychotic drugs may be responsible for atoxic cardiomyopathy, leading to death by ventricular fibrillation or cardiac arrest. Ultrastructural damage to the heart associated with circulating auto-antibodies, especially those to skeletal muscle, heart, DNA, mitochondria and smooth muscle, has been found in patients who have died from drug-related, fatal arrhythmias.57 Further, clozapine has been associated with myocarditis which has been found in cases of sudden death.58-60
Conclusion
From a neurocardiologic perspective, antipsychotic drugs have the potential for both increasing and decreasing
the risk of sudden death.61 This notion that drugs with electrophysiological properties similar to quinidine are as likely to reduce as to increase the risk of arrhythmias must be viewed with some circumspection. Simpson et al go on to state that “Ultimate outcome is probably determined by a multitude of interacting factors, and the role played by the drug in a given individual is difficult, if not impossible, to determine.61 Where there is limited information, the tendency to cite neuroleptics as the cause of death in cases of sudden death with negative findings at postmortem should be resisted, according to Laposata et al (1988). Otherwise, efforts to identify the correct cause of death in such cases, and clearly establish the risk of neuroleptic treatment, will be hindered.62
References1. Tsuang MT, Woolson RF. Excess mortality in schizophrenia and affective disorder. Do suicides and accidental deaths solely account for this excess? Archives of General Psychiatry 1978;35:1181–1185.2. Black DW. Mortality in schizophrenia. The Iowa record-linkage study: a comparison with general population mortality. Psychosomatics 1988;29:55-60.3. Kannel WB, Doyle JT, McNamara PM. Precursors of sudden coronary death. Factors related to the incidence of sudden death. Circulation 1975;51:606–613.4. Gullestad L, Kjekshus J. sudden cardiac death. Significance of beta-blockers. Tidsskr nor Laegeforen 1992;112:2843–2847.5. Davies MJ. Unexplained death in fit young people. British Medical Journal 1992;305:538–539.6. Skentelberry D. Junior doctor died of natural causes, says coroner (News). British Medical Journal 1994;309:1530.7. Brown RP, Kocsis JH. Sudden death and antipsychotic drugs. Hospital and Community Psychiatry 1984;35:486–491.8. Jusic N, Lader M. Post-mortem antipsychotic drug concentrations and unexplained deaths. British Journal of Psychiatry 1994;165:787–791.9. Newman SC, Bland RC. Mortality in a cohort of patients with schizophrenia: a record linkage study. Canadian Journal of Psychiatry 1991;36:239–245.10. Kuller L, Lilienfield A, Fisher R. An epidemiological study of sudden and unexpected deaths in adults. Medicine 1967;46:341–361.11. Hirsch CS, Martin DK. Unexpected death in young epileptics. Neurology 1971;21:682.12. Mohammadi MR, Akhondzadeh S. Schizophrenia: etiology and pharmacotherapy. IDRUGS 2001;4:1167-1172. 13. Akhondzadeh S. The 5-HT hypothesis of schizophrenia. IDRUGS 2001;4:295-300.14. Akhondzadeh S. Pharmacotherapy of schizophrenia: The past, present and future. Current Drug Therapy 2006;1:1-7. 15. Akhondzadeh S, Faraji H, Sadeghi M, Afkham K, Fakharzadeh H, Kamalipour A. Double blind comparison of fluoxetine and nortriptyline in the treatment of moderate to severe major depression. Journal of Clinical Pharmacy and Therapeutics 2003;28:379-384.16. Ban TA, St Jean A. The effect of phenothiazines on the electrocardiogram. Canadian Medical Association Journal 1964;91:537–540.
Seyed Hesameddin Abbasi et al
9The Journal of Tehran Heart Center
Antipsychotic Drugs and Sudden Death
17. Ban TA, St Jean A. Electrocardiographic changes induced by phenothiazine drugs. American Heart Journal 1965;70:575–576.18. Huston JR, Bell GE. The effects of thioridazine hydrochloride and chlorpromazine on the electrocardiogram. Journal of the American Medical Association 1966;198:16–20.19. Alexander CS, Nino A. Cardiovascular complications in young patients taking 20. Lapierre YD, Lapointe L, Bordeleau JM. Phenothiazine treatment and electrocardiographic abnormalities. Canadian Psychiatric Association Journal 1969;14:517–523.21. Ayd FJ. Cardiovascular effects of phenothiazines. International Drug Therapy Newsletter. V 1970;1–822. Crane GE. Cardiac toxicity and psychotropic drugs. Disease of the Nervous System 1970;31:534–539.23. British Medical Journal Cardiovascular complications from psychotropic drugs. British Medical Journal 1971;1:3.24. Raj MVJ, Benson R. Phenothiazines and the electrocardiogram. Postgraduate Medical Journal, 511975;65–68.25. Fowler NO, McCall D, Chou TC. Electrocardiographic changes and cardiac arrhythmias in patients receiving psychotropic drugs. American Journal of Cardiology 1976;37:223–230.26. Deglin SM, Deglin JM, Chung EK. Drug-induced cardiovascular diseases. Drugs 1977;14:29–40.27. Wijsenbeck H, Steiner M, Goldberg SC. Trifluoperazine: a comparison between regular and high doses. Psychopharmacologia 1974;36:147-150.28. Swett CP, Shader RI. Cardiac side-effects and sudden death in hospitalized psychiatric patients. Diseases of the Nervous System 1977;38:69–72.29. Aunsholt NA. Prolonged QT interval and hypokalaemia caused by haloperidol. Acta Psychiatrica Scandinavica 1989;79:411–412.30. Guy JM, Andre-Fouet X, Porte J. Torsades de pointes et allongement de la duree de l’intervalle QT apres injection de droperidol. Annales de Cardiologie et d’Angeiologie 1991;40:541-545.31. Thomas SHL. Drugs, QT interval abnormalities and ventricular arrhythmias. Adverse Drug Reactions and Toxicology Review 1994;13:77–102.32. Krahenbuhl S, Sauter B, Kupferschmidt H. Case report: reversible QT prolongation with torsade de pointes in a patient with pimozide intoxication. American Journal of Medical Science 1995;309:315–316.33. Lande G, Drouin E, Gauthier C. Effets arythmogenes du chlorydrate de sultopride: correlation clinique et electrophysiologique cellulaire. Ann Fr Anesth Reanim 1992;11:629–635.34. Warner JP, Barnes TRE, Henry J. Electrocardiographic changes in patients receiving neuroleptic medication. Acta Psychiatrica Scandinavica 1996;93:311–313.35. Barnett AA. Safety concerns over antipsychotic drug, sertindole. Lancet 1996;348:256.36. Thomas SHL. Drug-induced QT interval prolongation. British Journal of Clinical Pharmacology 1996;42:399.37. Buckley NA, Whyte IM, Dawson AH. Cardiotoxicity more common in thioridazine overdose than with other neuroleptics. Clinical Toxicology 1995 ;33:199–204.38. Fulop G, Phillips RA, Shapiro AK. EEG changes during haloperidol and pimozide treatment of Tourette’s disorder. American Journal of Psychiatry 1987;144:673–675.39. Committee on Safety of Medicines Cardiac arrhythmias with pimozide (Orap). Current Problems in Pharmacovigilance 1995;21:2.
40. Liberatore MA, Robinson DS. Torsade de pointes: A mechanism for sudden death associated with neuroleptic drug therapy? Journal of Clinical Psychopharmacology 1984;4:143-146.41. Keren A, Tzivoni D. Torsade de pointes: prevention and therapy. Cardiovascular Drugs and Therapy1991;5:509–513.42. Cleland JGF, Krickler DM. Torsade de pointes: chaos, sixteen years on? British Heart Journal 1992;7:1–3.43. Krickler GFC, Krickler DM. Torsade de pointes: chaos, sixteen years on? British Heart Journal1992;67:1–3.44. Krickler DM, Curry PVL. Torsades de pointes: an atypical ventricular tachycardia. British Heart Journal 1976;38:117–120.45. Zee-Cheng CS, Mueller CE, Seifert CF. Haloperidol and torsades de pointes. Annals of Internal Medicine 1985 ;102:418.46. Fayer SA. Torsade de pointes ventricular tachyarrhythmia associated with haloperidol. Journal of Clinical Psychopharmacology 1986;6:375–376.47. Kriwisky M, Perry GY, Tarchitsky D. Haloperidol-induced torsades de pointes. Chest 1990;98:482–484.48. Henderson RA, Lane S, Henry JA. Life-threatening ventricular arrhythmia (torsade de pointes) after haloperidol overdose. Human and Experimental Toxicology 1991;10:59–62.49. Wilt JL, Minnema AM, Johnson RF. Torsade de pointes associated with the use of intravenous haloperidol. Annals of Internal Medicin 1993;119:391–394.50. Metzger E, Friedman R. Prolongation of the corrected QT and torsades de pointes cardiac arrhythmias associated with intravenous haloperidol in the medically ill. Journal of Clinical Psychopharmacology 1993;13:128–132.51. Kiriike N, Maeda Y, Nishiwaki S. Iatrogenic torsade de pointes induced by thioridazine. Biological Psychiatry 1987;22:99–103.52. Zehender M, Hohnloser S, Just H. QT-interval prolonging drugs: mechanisms and clinical relevance of their arrhythmogenic hazards. Cardiovascular Drugs and Therapy 1991;5:515–530.53. Day CP, McComb JM, Campbell RW. QT dispersion: an indication of arrhythmic risk in patients with long QT intervals. British Heart Journal 1990;63:342–344.54. Committee on Safety of Medicines Drug-induced prolongation of the QT interval. Current Problems in Pharmacovigilance 1996;22:2-11.55. Huang MH, Ebey J, Wolf S. Responses of the QT interval of the electrocardiogram during emotional stress. Psychosomatic Medicine 1989;51:419–427.56. Schwartz PJ, Zaza A, Locati E. Stress and sudden death. The case of the long QT syndrome. Circulation, 1991; 83 (suppl.), 1171–1180.57. Guillan RA, Yang C-P, Hocker EV. Antibody phenothiazines. Multiple antibody screening of patients under high doses. Journal of the Kansas Medical Society 1977;8:221–227.58. Meeker JE, Herrmann PW, Som CW. Clozapine tissue concentrations following an apparent suicidal overdose of Clozaril. Journal of Analytical Toxicology 1992;16:54–56.59. Jensen VE, Gotzsche O. Allergic myocarditis in clozapine treatment. Ugeskrift for Laeger 1994;156:4151–4152.60. Lilleng P, Morild I, Hope M. Clozapine and myocarditis. Tidsskrift for den Norske Laegeforening 1995;115:3026–3027.61. Simpson GM, Davis J, Jefferson JW. Sudden Deaths in Psychiatric Patients: The Role of Neuroleptic Drugs. American Psychiatric Association Task Force Report, No 1987;27.62. Laposata EA, Hale PJr, Poklis A. Evaluation of sudden death in psychiatric patients with special reference to phenothiazine therapy. Journal of Forensic Science 1988;33:432–440.

10
11The Journal of Tehran Heart Center
Original Article
The Sheep as a Model for Coronary Artery Surgery Experiments on Beating Heart
Drissi Boumzebra, MD, Jan Otto Solem, MD, Shaheen Nakeeb, MD, Zohair Al Halees, MD*
King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia.
Abstract
Background: A good animal model for coronary surgery experiments has been difficult to establish. An ideal model should have the closest morphological resemblance to human beings. The objective of this study is to establish sheep as a model for these experiments.
Methods: The anatomical aspects of left anterior descending coronary artery (LAD) and right internal thoracic artery (RITA) in the sheep are studied. Coronary artery bypass grafting between the RITA and LAD coronary artery was performed. Patency of the anastomosis was evaluated by follow-up angiography.
On a beating heart, the RITA was anastomosed to the LAD in adult sheep. A left anterior thoracotomy in the fifth intercos-tals space gave good access to both vessels. Ventricular fibrillation (VF) was a major intra-operative problem. Its incidence and relation to ischemic time was studied. The anastomosis patency was tested immediately and at follow-up by a modified technique of angiography. The morphological anatomy of both LAD and RITA was studied in detail and analysed. Surviving sheep were studied for 6 months or more.
Results: RITA was easy to harvest. The most common anatomy for the LAD was presence of two diagonal branches and absence of an overlying vein. The incidence of ventricular fibrillation (VF) during LAD snaring was 10.8% (mean ischemic time before VF occurrence was 4 minutes). The modified angiography technique produced good quality angiograms. Wound infection was initially a problem but controlled with prophylactic antibiotics.
Conclusion: Favorability of RITA and LAD anatomy prove sheep as a good animal model for coronary artery surgery experiments. VF incidence is acceptable. Wound infection is controlled. Good quality follow-up is feasible.
The Journal of Tehran Heart Center 1 (2006) 11-15
KeyWords: Sheep • Model • Coronary artery surgery
* Corresponding Author: Zohair Al Halees, King Faisal Heart Institute (MBC #16). King Faisal Specialist Hospital & Research Centre. P.O. Box 3354, Riyadh 11211, Kingdom of Saudi Arabia. Tel: (966-1) 442-7470. Fax: (966-1) 442-7482. Email: [email protected]
Introduction
Coronary artery bypass surgery has been performed over the last 30 years in large numbers: Now the number of operations in the western world is closer to one million
per year. Despite the generally excellent results with this technique, there remains some associated mortality and morbidity particularly in patients with increased risk factors.1,2 Hence, over the last decade, there has been an intensive focus on less invasive surgery leading to the

The Journal of Tehran Heart Center
12
development of minimally invasive and off pump coronary surgery.3,4,5 To facilitate this, new approaches and instruments were developed. New techniques and technologies have to be tested on animal models before implementation in humans. A good animal model for coronary artery surgery has been difficult to establish. An ideal model should have the closest morphological resemblance to human being.
In spite of the fact that they are stressful animals, pigs have been used because of their heart’s similarities to human heart, including a small capacity for coronary collateral flow.6 The weight of dogs and the size of the coronary arteries are limiting factors for their use. Until now, nobody has reported on beating heart surgery with long term follow up in a sheep model. In our animal laboratory a new anastomotic device was tested in sheep. Data about the anastomotic device were published earlier.7 This paper aims to analyze the anatomical aspect of the left anterior descending coronary artery and the right internal thoracic artery in the sheep describing this experimental animal model in detail.
Methods
Animals
Coronary artery bypass between the right internal thoracic artery (RITA) and the left anterior descending artery (LAD), either by using an anastomotic device or by continuous 7-0 Polypropylene sutures, was carried out at our institution’s animal laboratory in 65 sheep. These were healthy sheep of the local Najdi and Naimi breeds, 8-12 months in age, corresponding to a body weight of 40-55 kg, chosen and obtained from the local market. They were taken to the Animal Care Facility of the, Research Centre, underwent physical Examination and routine laboratory workup, then given prophylactic penicillin or cephalosporin. After a period of at least two weeks and when their health had been determined to be satisfactory, they were used for experiments. The experimental protocol was approved by our Research Advisory Council and Animal Care and Use Committee. The animals were fasted for 24-36 hours with access to water until 8 hours prior to surgery. Before the procedure, 1 gram of intravenous cefazolin sodium (Keflin; Eli Lily; Indiana, USA) was given followed by Gentamycin (Gentamycin; American Pharmaceutical, Illinois, USA) 1gm/day for 5 days.
Surgical procedure
A central venous line was obtained by puncturing the external jugular vein. The right carotid artery was openly accessed and cannulated for monitoring the arterial pressure and obtaining arterial blood gas samples. The arterial blood gases were monitored every 30 minutes. Atropine sulphate (Atropisol; American Regent; New York) 0.2 mg/kg, was
given preoperatively and every 15-30 minutes during the procedure. For muscle relaxation, atracurium besylate (Tracrium; Calmic, UK or; Wellcome, USA), 0.2 mg/kg was given and for reversal neostigmine (Prostigmin; Roche; UK), 0.5-2.5 mg. Propofol (Diprivan; ICI Pharmaceuticals; UK), 4 mg/kg was used for induction and maintenance as required. Halothane (Fluothane; ICI Pharmaceuticals; UK), 0.8-1.5 vol. % was added after induction of anaesthesia. Extremity EKG and oximetry with a tongue probe were used for additional monitoring.
The sheep sternum was found too thick for a median sternotomy; it was difficult to split and achieve a stable closure. The internal thoracic artery was found to be located in the angle formed between the sternum and the ribs. A left thoracotomy in the 5th intercostal space was the approach of choice. It was extended half way across the sternum at the beginning of our experience. It allowed a good exposure of the heart and the right internal thoracic artery the pericardial cavity was found to be suspended by two ligaments-one to the diaphragm, and the other to the sternum.
When these ligaments had been split, the heart and the pericardium were mobile and the RITA was well exposed through an anterior opening in the right pleura. It was worth mentioning that an ample space was found retrosternally. The left internal thoracic artery was ligated and transacted.
The RITA was inspected and then harvested without pedicle. The morphological anatomy, the side branches and the size of the RITA were studied. Thereafter, 100 units/kg of heparin sodium (Unihep; Leo; United Kingdom) and 1 mg/kg/min. of Lidocaine (Lidocaine HCL injection; USP; USA) were given intravenously as a bolus, followed by 0.1 mg/kg/min of Lidocaine (Lidocaine HCL injection; USP; USA), Propranolol (Inderal; ICI Pharmaceuticals; United Kingdom), 1.6mg or esmolol (Brevibloc; DuPont; USA), 0.5-1 mg was given, as needed, to achieve a heart rate below 80 bmp, since the risk of ventricular fibrillation (VF) increases with higher heart rate.8 Five ml of Xylocaine 2% (Xylocaine; Astra; United Kingdom) was applied topically to the epicardium and instilled in the pericardial cavity. The LAD was explored. The number of diagonal branches and the presence or absence of overlying veins was noted. A 4-0 Polypropylene suture for snaring was placed around the proximal LAD. On the beating heart and without a stabilizer, the LAD was opened for approximately 6 mm. The LAD was snared proximal to the anastomotic site. Preferably, location for the snare was chosen distal to the first diagonal branch of the LAD to minimize the amount of ischemic muscle and the risk of VF. The size of the LAD was measured with coronary probes. The ischemic time before the appearance of any VF was recorded. In many instances, the LAD was located be hind the anterior cardiac vein, which resulted in bleeding when the LAD had been dissected free. The RITA was anastomosed to the LAD between the first and the second diagonal or distal to the second diagonal branch. After the release of the snare, the blood flow in the RITA was measured
Drissi Boumzebra et al
13The Journal of Tehran Heart Center
by a transit time flow meter (Transonic Systems, Inc. Ithaca, NY) usually using a 2.5 mm probe. Thereafter, the LAD was ligated proximal to the first diagonal branch. Two flows were measured - one, with the proximal LAD open, and the other with the proximal LAD closed. The survival criteria were: open anastomosis on fluoroscopy, detected RITA flow and stable hemodynamics at the end of the experiment.
In 3 sheep, a length of 10-15 mm of the LAD was dissected free from the surrounding tissue one centimetre proximal to the first diagonal and the LAD flow was measured using the same flow probe.
Fluoroscopy and follow up
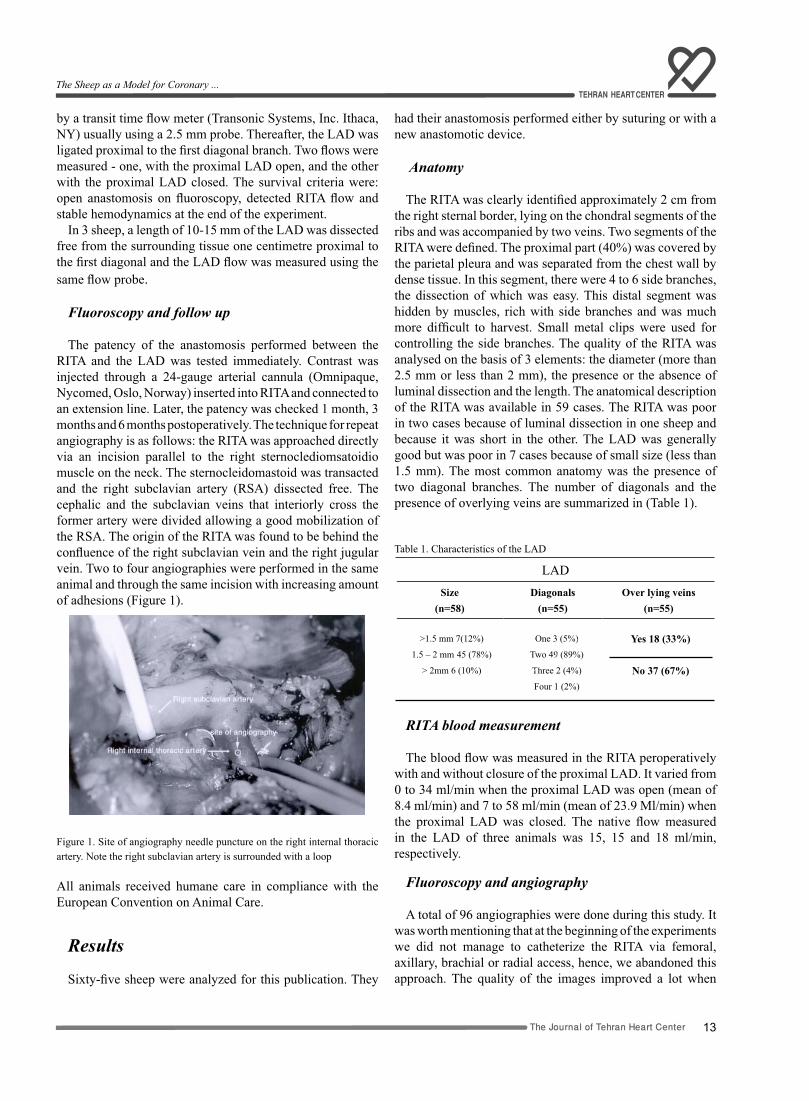
The patency of the anastomosis performed between the RITA and the LAD was tested immediately. Contrast was injected through a 24-gauge arterial cannula (Omnipaque, Nycomed, Oslo, Norway) inserted into RITA and connected to an extension line. Later, the patency was checked 1 month, 3 months and 6 months postoperatively. The technique for repeat angiography is as follows: the RITA was approached directly via an incision parallel to the right sternoclediomsatoidio muscle on the neck. The sternocleidomastoid was transacted and the right subclavian artery (RSA) dissected free. The cephalic and the subclavian veins that interiorly cross the former artery were divided allowing a good mobilization of the RSA. The origin of the RITA was found to be behind the confluence of the right subclavian vein and the right jugular vein. Two to four angiographies were performed in the same animal and through the same incision with increasing amount of adhesions (Figure 1).
Figure 1. Site of angiography needle puncture on the right internal thoracic artery. Note the right subclavian artery is surrounded with a loop
All animals received humane care in compliance with the European Convention on Animal Care.
Results
Sixty-five sheep were analyzed for this publication. They
had their anastomosis performed either by suturing or with a new anastomotic device.
Anatomy
The RITA was clearly identified approximately 2 cm from the right sternal border, lying on the chondral segments of the ribs and was accompanied by two veins. Two segments of the RITA were defined. The proximal part (40%) was covered by the parietal pleura and was separated from the chest wall by dense tissue. In this segment, there were 4 to 6 side branches, the dissection of which was easy. This distal segment was hidden by muscles, rich with side branches and was much more difficult to harvest. Small metal clips were used for controlling the side branches. The quality of the RITA was analysed on the basis of 3 elements: the diameter (more than 2.5 mm or less than 2 mm), the presence or the absence of luminal dissection and the length. The anatomical description of the RITA was available in 59 cases. The RITA was poor in two cases because of luminal dissection in one sheep and because it was short in the other. The LAD was generally good but was poor in 7 cases because of small size (less than 1.5 mm). The most common anatomy was the presence of two diagonal branches. The number of diagonals and the presence of overlying veins are summarized in (Table 1).
Table 1. Characteristics of the LAD
LADSize
(n=58) Diagonals
(n=55) Over lying veins
(n=55)
>1.5 mm 7(12%)
1.5 – 2 mm 45 (78%)
> 2mm 6 (10%)
One 3 (5%)
Two 49 (89%)
Three 2 (4%)
Four 1 (2%)
Yes 18 (33%)
No 37 (67%)
RITA blood measurement
The blood flow was measured in the RITA peroperatively with and without closure of the proximal LAD. It varied from 0 to 34 ml/min when the proximal LAD was open (mean of 8.4 ml/min) and 7 to 58 ml/min (mean of 23.9 Ml/min) when the proximal LAD was closed. The native flow measured in the LAD of three animals was 15, 15 and 18 ml/min, respectively.
Fluoroscopy and angiography A total of 96 angiographies were done during this study. It
was worth mentioning that at the beginning of the experiments we did not manage to catheterize the RITA via femoral, axillary, brachial or radial access, hence, we abandoned this approach. The quality of the images improved a lot when
The Sheep as a Model for Coronary ...

The Journal of Tehran Heart Center
14
we succeeded to catheterize the RITA directly as described above (Figure 1).
Mortality and morbidity
Twelve (18.5%) animals expired during the surgery. Three were sacrificed because they did not meet the survival criteria. The other 9 had ventricular fibrillation (VF) and died during surgery. The VF occurred during the snaring of the LAD in 7 cases and mainly during the performance of the first 33 anastomosis. The mean ischemic time before the occurrence of VF was 4 minutes ranging from 1.5 to 8 minutes? As our experience improved, we learned to avoid VF which occurred only in 2 cases during the second half of the study. Fifty-three sheep survived the surgery. Eight among them had chest wound infections (15%). In seven of these (87.5%), the wound infection complicated the extended thoracotomies to the sternum. Sixteen sheep died within 30 days following the procedure. The causes are summarized in (Table 2).
Table 2. Causes of late death (n = 16)
Causes Number
Bleeding 2
VF due to contrast 3
Chest Infections 4
Endocarditis 1
Arrhythmia 1
Heat Stroke 2
AMI 1
Undetermined 2
VF, Ventricular Fibrillation; AMI, Acute Myocardial Infarction
Thirty-seven animals were sacrificed according to the protocol, 4 had minor chest infection which did not compromise the quality of the angiographies.
Discussion
The sheep as an animal model has been used previously for cardiac valve surgery.9 the sheep grows slowly is docile and its coagulation system is similar to that of humans.10 although there has been an increasing interest for beating heart and minimally invasive surgery, the sheep was rarely used for coronary surgery experiments.
In order to test a newanastomotic device, 65 sheep underwent coronary artery procedures on the left anterior descending artery on a beatingheart. It was easy to approach the whole LAD through the fifth left intercostal space. David J. Farrar used the fourth intercostal space for implanting a prosthetic coronary artery bypass graft on the proximal
circumflex in a sheep model as well.11 the exposure was good without respecting any rib. At the beginning of our experience, we used to extend the incision half way across the sternum when the animal was fat. We later abandoned this extension, as we experienced recurrent and fatal chest wound infections in the extended incision animals. Actually, the sheep is an animal that rests on the sternum, which exposes the wound to fecal contamination of the floor. To prevent this complication, we adopted strict aseptic measures when dealing with sheep during anaesthesia and surgery, reduced the size of skin incisions and dressed the wound for 48 hours. In addition, prophylactic antibiotics were used for 5 days. This led to reduction in the wound infection rate. The administration of prophylactic antibiotics, after implantation of valve prosthesis until the wound became dry and healed, was used in dogs and sheep.12
The origin of the RITA is in the concavity of the right subclavian artery and at approximately 2 cm from the sternal border. It is accompanied by a pair of internal mammary veins. The RITA is covered by the parietal pleura only in its proximal one third; below this level, muscles separate the vessel from the pleura. In contrast to human anatomy, the majority and the largest side branches are located at this distal part of the RITA. We found it easier to harvest a skeletonized RITA rather than on a pedicle. All the branches were Secured with metal clips and cut in order to have a good mobilization, though it has been proven recently in pig models that patent side branches do not affect coronary blood flow in internal thoracic artery to left anterior descending anastomosis.13 a good length of the RITA proved to be important. In the follow up angiograms we found the distal RITA stenosis to be related to stretch conduits. In our study, the LAD of the sheep had two diagonals in 90% of cases. The anastomosis of RITA to LAD was generally done distal to the second diagonal. When the LAD was covered by a vein or was intra-mural, its dissection became difficult and bleeding from damaged veins was common. During the anastomosis, the LAD was snared distal to the first diagonal. This gave us enough time to perform the anastomosis, as most of the myocardium was still perfused by the first diagonal. While completing the anastomosis, we experienced many cases of ventricular fibrillation (10.8%), mainly when there was only one diagonal or when the second diagonal was dominant. The occurrence of VF decreased significantly as we became experienced to perform anastomosis with the new device. The incidence of VF after snaring of the proximal LAD in pigs has been reported to be between 71% and 100%.14 This difference in the VF occurrence when the LAD was snared inferred that the LAD of the sheep has more collaterals than that of the pig. The dog is less prone to VF after the occlusion of the proximal LAD because the circumflex supplies more myocardium than does the LAD in pigs.14 Moreover the dog has a rich capacity of collateral flow. The occurrence of arrhythmia after legation of a coronary artery probably depends on the amount of collateral flow. In pilot tests, we
Drissi Boumzebra et al

15The Journal of Tehran Heart Center
did acute experiments on dogs and were happy with the absence of VF but we were not satisfied with small size of the LAD.
When the anastomosis had been done and the flow had been measured, the LAD was ligated proximal to the first diagonal in order to avoid the competitive flow to the RITA from the proximal LAD.
At follow up, we recanalization of the ligated LAD, evident at angiography or at sacrifice. This problem was met even after we had changed the ligature used from polyprolene to silk. Because of this problem, in our last animals, we dissected and clipped the LAD at the origin. The elimination of the competitive blood coming from the proximal LAD allowed an undisturbed flow from the RITA.
In total, we performed 96 angiographies during the follow up. Early on we realized that it was very difficult to cannulate the RITA from a femoral, axillary, brachial or radial approach. Therefore, the approach was modified. The RITA was dissected and catheterized directly at its origin via an incision in the neck. Up to three angiographies were done using this same approach. During the third and fourth controls we encountered a lot of adhesions and experienced serious bleeding from around the superior vena cava and the right common carotid artery but never compromised the quality of the angiograms. In summary we present here the sheep as an animal model for coronary artery surgery. Its size is ideal; the coronary anatomy is suitable and is an easy animal to care for. Ventricular fibrillation is acceptable and is related to length of ischemia. Use of prophylactic antibiotics is recommended and should reduce the rate of wound infection. The retrosternal space is adequate enough to allow using the sheep for evaluating the newly developed endoscopic surgical techniques in cardiac surgery as interest in these is gaining a lot of momentum.
References1. Blauth CI, Cosgrove DM, Webb BW, Ratliff NB, Boylan M, Piedmonte MR. Artheroembolism from the ascending aorta: An emerging problem in cardiac surgery. J Thorac Cardiovasc Surg 1992;103:1104-1111.2. Loop FD, Lytle BW, Cosgrove DM, Mahfood S, McHenry MC, Goortmastic M, et al. Sternal wound complications after isolated coronary artery bypass grafting: Early and late mortality, morbidity, and cost of care. Ann Thorac Surg 1990;49:179-186..3. Benetti F, Ballester C, Boonstra P, Grandjean J. Video assisted coronary bypass surgery. J Card Surg 1995;10:620-625.4. Borst F, Santamore WP, Smedira NG, Bredee JJ. Minimally invasive coronary artery bypasses grafting: on beating heart and via l imited access. Ann Thorac Surg 1997;63:S1- S5.5. Cartier DBR. Off-pump revascularization of multivessel coronary artery diseases has decreased myocardial rate. Eur J Cardio-thorac Surg 1998;14:S20-S24.6. White FC, Roth DM, Bloor CM. The pig as a model for myocardial ischemia and exercise. Lab Anim Sci 1986;36:351-6.
7. Sole JO, Boumzebra D, Al Buraiki J, Nakeeb S, Rafeh W, Al Halees Z. Evaluation of a new device for quick Sutureless coronary artery anastomosis in surviving sheep. Eur J Cardio-thorac Surg 2000;17:312-318.8. Chadd KD, Bank VS, Hefant RH. Rate dependent ventricular ectopia following acute coronary occlusion. Circulation 1974;49:654-659.9. Ali ML, Kumar SP, Bjornstad K, Duran CMG. The sheep as an animal model for heart valve research. Cardiovascular Surgery 1996;4;543-549.10. Tillman P, Carson SN, Talken L. Platelet function and coagulation parameters in sheep during experimental vascular surgery. Lab Anim Sci. 1981;31:263-267.11. Farrar DJ. Developments of a prosthetic coronary artery bypass graft. The Heart Surgery Forum 2000;3:36-40.12. Irwin E, Lang G, Clark R, Cyr JS, Runge W, Foker J, Bianco R. Long-term evaluation of prosthetic mitral valves in sheep. J Investigative Surg 1993;6:133-141.13. Pragliola C, Gaudino M, Bombardieri G, Barilaro C, Bruno P, Varano C, Santoro T, Possati G. Patent side branches do not affect coronary blood flow in internal thoracic artery-left anterior descending anastomosis: an experiment study. J Thorac Cardiovasc Surg 1999;118:66-70.14. Verdouw PD, Hartog JM. Provocation and suppression of ventricular arrhythmias in domestic swine. In: Stanton HC, Merssmann HJ, eds. Swin in Cardiovascular Research, Florida, Boca-Raton, 1986. p. 122-156.
The Sheep as a Model for Coronary ...

16
17The Journal of Tehran Heart Center
Original Article
Moderate Mitral Regurgitation and Coronary Disease: Treat-ment with Coronary Bypass Alone?
Hakimeh Sadeghian, MD*, Abbasali Karimi, MD, Hosein Ahmadi, MD, Mojtaba Salarifar, MD, Saeed Sadeghian, MD, Nader Fallah, PhD, Navid Paydari, MD, Mohammad Majd, MD
Tehran Heart Center, Tehran University of Medical Sciences, Tehran, Iran.
Abstract
Background: In cases of moderate(2 or 3+ on a scale of 0 to 4+) nonorganic mitral regurgitation (MR) and coronary artery disease, operative strategy continues to be debated between coronary artery bypass grafting alone (CABG) or con-comitant valve repair. To clarify the optimal management of these patients, we evaluated the mid-term results of isolated CABG in the study group.
Methods: From March 2002 to February 2005, 40 consecutive patients (57.5% male, mean age: 62.45±8.7 years, mean ejection fraction: 44.15±12.6%, mean New York Heart Association class 2.5±0.78) with coronary artery disease and moder-ate MR without organic mitral valve disease (prolapse, rheumatism, etc.) underwent CABG alone. Thirty one (77.5%) pa-tients had either postoperative or follow-up transthoracic echocardiography with mean follow up time of 10.82±8.12 months. Patient’s pre and postoperative data were compared to evaluate the results of isolated CABG on moderate MR.
Results: MR was ischemic (with persistent wall motion abnormality) in 25(62.5%) patients and functional (without per-sistent wall motion abnormality) in 15(31.5%). Considering postoperative and follow up transthoracic echocardiography, 54.8% had no or mild MR (29% MR 1+, 25.8% no MR) and 45.2% had moderate MR (16.1% MR 3+, 29% MR 2+). Resolu-tion of MR was significant (p<0.001), but it had no correlation with ischemic MR (p=0.46), preoperative ejection fraction (p=0.09), LV systolic (p=0.70) and diastolic dimensions (p=0.80). Seven patients died, 2 in hospital and 5 later.
Conclusion: Although for coronary artery disease accompanying moderate nonorganic MR, CABG alone reduces sever-ity of MR significantly, many patients are left with moderate MR. Preoperative diagnosis of moderate nonorganic MR may warrant concomitant mitral repair.
The Journal of Tehran Heart Center 1 (2006) 17 -22
Keywords: CABG • Echocardiography • Mitral regurgitation
*Corresponding Author: Hakimeh Sadeghian, Department of echocardiography, Tehran Heart Center, North Kargar Street, Tehran, Iran 1411713138. Tel: +98-21-88029257. Fax: +98-21-88029256. E-mail: [email protected].
Introduction
Mitral regurgitation (MR) accompanying coronary artery disease (CAD) is a heterogeneous entity. Ischemic MR (IMR) is mitral insufficiency caused by myocardial infarction and associated with a persistent wall motion abnormality.1 The
term IMR excludes rheumatic, degenerative, myxomatous, infective and other organic causes of MR.
IMR must be distinguished from organic mitral valve disease with coexisting coronary artery disease, but sometimes it is
The Journal of Tehran Heart Center
18
very difficult to determine whether MR is ischemic or there is a coexisting of MR with coronary artery disease.
In IMR, does coronary artery bypass grafting (CABG) alone and revascularizing ischemic areas improve regional wall motion and correct the MR?
Although most surgeons would agree that severe MR should be corrected at the time of CABG and that trace to mild MR can probably be left alone, the optimal management of moderate ischemic MR remains controversial.
Those favoring a conservative approach, make several arguments:
First, revascularizing ischemic areas will improve regional wall motion and correct the MR.2,3,4
Second, several studies suggest that performing CABG alone does not affect long term survival or functional status.5,6,7,8,9
Many surgeons however, have advocated more liberal use of mitral annuloplasty in patients with moderate MR at the time of CABG.10
They argue that CABG alone will not correct moderate ischemic MR in many patients, especially those with scarring from myocardial infarction and those with annular and ventricular dilation.11
In addition, intervention on the mitral valve appears to benefit those with symptomatic heart failure.12 Some authors suggest repairing moderate mitral regurgitation in selected cases to improve long-term quality of life.13
This investigation was undertaken to study the influence of CABG alone on moderate non organ ic MR. For this purpose, we compared severity of MR before and after CABG and at follow up in patients with moderate MR.
Methods Between March 2002 and February 2005, patients with
moderate MR and coronary artery disease (CAD) who underwent CABG alone were identified from Tehran Heart Center surgery data base.
Moderate MR was defined as MR grade II or III with echocardiography or ventriculography.
Based on preoperative echocardiography, we excluded organic mitral valve diseases such as rheumatism, prolapse and infective endocarditis.
Patients with moderate MR and concomitant valve repair or replacement have been evaluated in another study.
MR was defined as ischemic if associated with persistent wall motion abnormality and as functional when there was not any persistent wall motion abnormality.
Parsonnet score was used before the operation to estimate the risk of mortality after CABG.
Echocardiography
A preoperative echocardiography was performed for all
patients. The assessment of mitral regurgitation severity was based on a number of variables (Table 1).14
Table 1. Assessment of the mitral regurgitation severity
RV (ml) ERO cm2
MR jet (%LA)
I Mild <30ml <0.2 <15
II 30-44ml 0.2-0.29 15-30
III 45-59ml 0.3-0.39 35-50
IV Severe ≥ 60ml >0.4 >50
RV, Regurgitation Volume (ml); ERO, Effective Regurgitation Orifice (cm2); MR jet (%LA), Mitral Regurgitation jet (% Left Atrium)
Ventriculography
MR grading based on ventriculography was done according to the following criteria:15
I. Mild: essentially clears with each beat and never opacifies the entire left atrium.
II. It does not clear with one beat and generally does opacity the entire Left atrium, it is opacified (albeit faintly) after several beats, however, opacification of Left atrium does not equal that of left ventricle.
III. The left atrium is completely opacified and achieves equal opacification of left ventricle.
IV. Severe: opacification of the entire left atrium occurs within one beat, the opacification becomes progressively denser with each beat, and contrast material can be seen refluxing into the pulmonary veins during systole.
Postoperative Transthoracic echocardiography A postoperative transthoracic echocardiography was
performed by a noninvasive cardiologist before discharge for 17/38 (45%) patients.
Follow up
Follow up was conducted in two periods. One between January and March 2004 and another between January and March 2005. Transthoracic echocardiography for follow up was completed in 21 patients. We can not find 5 patients because of change of their telephone NO. And their address, 7 patients interviewed by telephone, but they didn’t come for echocardiography and 7 patients were died (2 in hospital and 5 later). The date and cause of death were noted for cases who had died.
Data collection and analysis
Preoperative, operative, and postoperative data were collected prospectively in the division’s clinical database and confirmed by review of the actual medical records.
Hakimeh Sadeghian et al
19The Journal of Tehran Heart Center
Moderate Mitral Regurgitation ...
Statistical analysis was performed with the SPSS statistical package (SPSS Inc). All means in the text are expressed as mean ± SD.
Ordinal variables were compared with the nonparametric Mann-Whitney or Willcoxon signed ranks tests. Categorical Variables were compared with fisher’s exact test for2 X 2 contingency tables and Pearson’s x2 test for larger tables. A p value< 0.05 was considered statistically significant.
Results
Patient characteristics
Patient demographics, preoperative and postoperative data are presented in (Table 2).
Table 2. Patient characteristics
All patients Age, y
MeanRange
SexMale Female
Left ventricular function Normal (EF ≥ 50%) Mild dysfunction (EF 40- 49%)Moderate dysfunction (EF 30-39%) Severe dysfunction (EF <30%)
Ejection FractionMean Range
NYHA Function ClassMean Comorbid condition
Diabetes mellitus Hypertension Renal insufficiency COPD
Number of bypass grafts Mean Range
Aneurysmectomy Poor coronary arteries Left main stenosis (> 50%) Recent unstable angina Recent Myocardial infarction Preoperative IABP Recent pulmonary edemaCardiogenic shock Congestive heart failure
n = 40
62.45 ±8.744 - 78
57.5%42.5%
42.5%25%12.5%20%
44.15% ± 17.6%20% – 70%2.5 ± 0.78
30%52.5%5%25%
3.43 ± 1.011-55%7.5%7.5%32.5%15%7.5%5%2.5%10%
EF, Ejection Fraction; NYHA, New York Heart Association; COPD, Chronic Obstructive Pulmonary Disease; IABP, Intra Aortic Balloon Pump
Mean age was 62.45±8.7 years (range 44 to 78 years) and mean ejection fraction was44.15 ± 1 2.60% (range 20 to 70%). 25(62.5%) patients had persistent wall motion abnormality (Ischemic MR (IMR) group), while 15(31.5%) patients had no persistent wall motion abnormality (functional MR (FMR) group).
17(42.5%) patients had preserved left ventricular systolic function (EF ≥ 50%) and 23(57.5%) had left ventricular systolic dysfunction (EF < 50%), which 20 % of them had severe systolic dysfunction (EF < 30%). 10 % of patients had congestive heart failure. Recent unstable angina was detected in 32.5 %, recent myocardial infarction in 15%, recent pulmonary edema in 5 %. 7.5% had left main stenosis, 2.5% were in cardiogenic shock and intra aortic balloon pumps (IABP) were used in 7.5% of patients.
Significant non cardiac comorbid conditions, including diabetes mellitus (30%), renal insufficiency (5%) and chronic obstructive pulmonary disease (25%) were not uncommon.
Preoperative data
Preoperative data are shown in table 2. The mean number of bypass grafts was3.43±1.01. Aneurysmectomy was done for 5% and 7.5% had poor coronary arteries.
Mortality and functional class There were 2 (5%) in-hospital deaths and from the 33
patients whom were followed, late death occurred in5 (16.50%) patients.
All deaths were cardiac related. Overall mortality was 7 (20%) patients, 3 in the IMR group and 4 in functional MR (FMR) group. Mortality was not significantly different between IMR and FMR groups (12% vs. 26.7%, p=0.99). Preoperative ejection fraction (43.32± 13.59 vs. 47.14±10.74, p=0.48) and severity of MR (p=0.62) had no relation with mortality.
2 in-hospital deaths occured on the day of operation, one with reducing blood pressure not responding to IABP and the other with cardiac arrest. Of the 5 late deaths, one occurred 30 days after operation due to pulmonary thromboemboli, the 4 other deaths were documented through the telephone. The functional class improved from a preoperative mean of 2.5±0.78 to a postoperative mean of 1.53±0.79 (p=0.002).
Postoperative TTE
From 17 patients who had postoperative transthoracic echocardiography, 41.2% had no or mild MR and 58.9% had moderate MR (2 or 3+) (Table 3).
The Journal of Tehran Heart Center
20
Table 3. Mitral regurgitation (MR) severity by TTE or Ventriculography
Severity
of MR
Preoperative
N=40
Postoperative
TTE
N=17
Follow up
TTE
N=21
Postoperative or follow up
TTE
N=31
0+ 0% 29.4% 14.3% 25.8%
1+ 0% 11.8% 42.9% 29.0%
2+ 80% 47.1% 23.8% 29.0%
3+ 20% 11.8% 19.0% 16.1%
4+ 0% 0% 0% 0%
Mean severity
of MR 2.20±0.41 1.41±1.06 1.47±0.98 1.35±1.05
TTE, Transthoracic Echocardiography
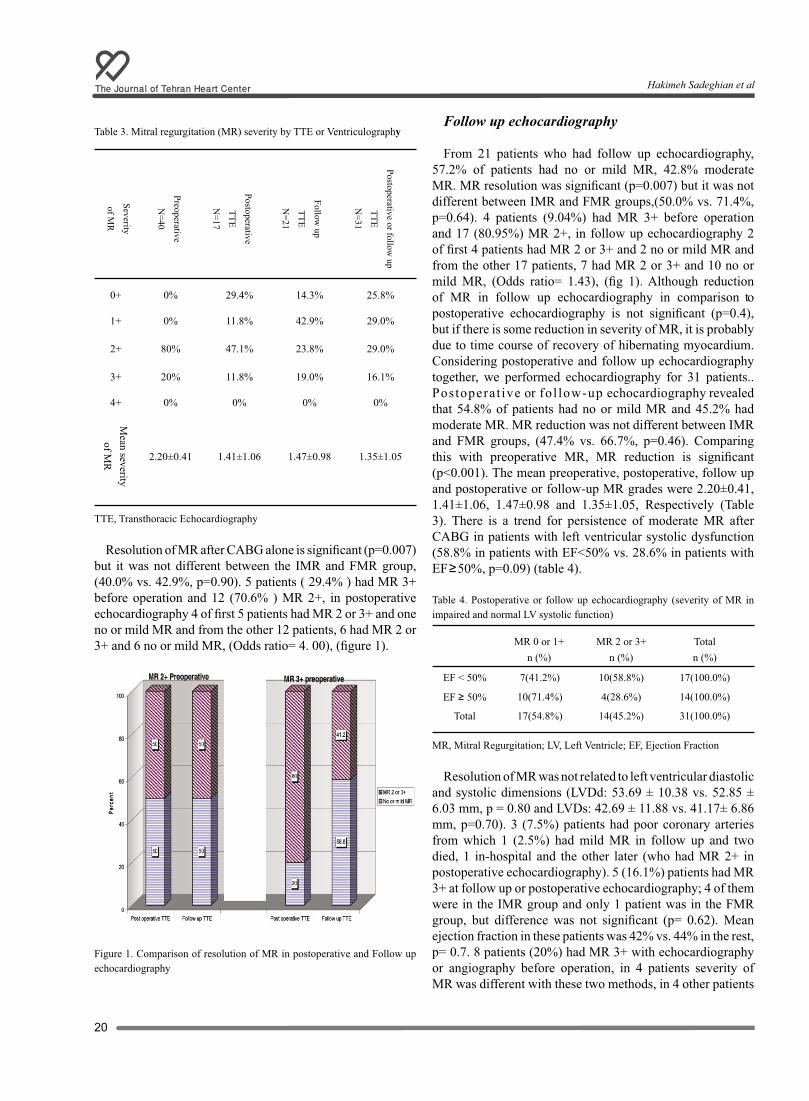
Resolution of MR after CABG alone is significant (p=0.007) but it was not different between the IMR and FMR group, (40.0% vs. 42.9%, p=0.90). 5 patients ( 29.4% ) had MR 3+ before operation and 12 (70.6% ) MR 2+, in postoperative echocardiography 4 of first 5 patients had MR 2 or 3+ and one no or mild MR and from the other 12 patients, 6 had MR 2 or 3+ and 6 no or mild MR, (Odds ratio= 4. 00), (figure 1).
Figure 1. Comparison of resolution of MR in postoperative and Follow up echocardiography
Follow up echocardiography
From 21 patients who had follow up echocardiography, 57.2% of patients had no or mild MR, 42.8% moderate MR. MR resolution was significant (p=0.007) but it was not different between IMR and FMR groups,(50.0% vs. 71.4%, p=0.64). 4 patients (9.04%) had MR 3+ before operation and 17 (80.95%) MR 2+, in follow up echocardiography 2 of first 4 patients had MR 2 or 3+ and 2 no or mild MR and from the other 17 patients, 7 had MR 2 or 3+ and 10 no or mild MR, (Odds ratio= 1.43), (fig 1). Although reduction of MR in follow up echocardiography in comparison to postoperative echocardiography is not significant (p=0.4), but if there is some reduction in severity of MR, it is probably due to time course of recovery of hibernating myocardium. Considering postoperative and follow up echocardiography together, we performed echocardiography for 31 patients..Postoperat ive or fol low-up echocardiography revealed that 54.8% of patients had no or mild MR and 45.2% had moderate MR. MR reduction was not different between IMR and FMR groups, (47.4% vs. 66.7%, p=0.46). Comparing this with preoperative MR, MR reduction is significant (p<0.001). The mean preoperative, postoperative, follow up and postoperative or follow-up MR grades were 2.20±0.41, 1.41±1.06, 1.47±0.98 and 1.35±1.05, Respectively (Table 3). There is a trend for persistence of moderate MR after CABG in patients with left ventricular systolic dysfunction (58.8% in patients with EF<50% vs. 28.6% in patients with EF≥50%, p=0.09) (table 4).
Table 4. Postoperative or follow up echocardiography (severity of MR in impaired and normal LV systolic function)
MR 0 or 1+ n (%)
MR 2 or 3+n (%)
Totaln (%)
EF < 50% 7(41.2%) 10(58.8%) 17(100.0%)
EF ≥ 50% 10(71.4%) 4(28.6%) 14(100.0%)
Total 17(54.8%) 14(45.2%) 31(100.0%)
MR, Mitral Regurgitation; LV, Left Ventricle; EF, Ejection Fraction
Resolution of MR was not related to left ventricular diastolic and systolic dimensions (LVDd: 53.69 ± 10.38 vs. 52.85 ± 6.03 mm, p = 0.80 and LVDs: 42.69 ± 11.88 vs. 41.17± 6.86 mm, p=0.70). 3 (7.5%) patients had poor coronary arteries from which 1 (2.5%) had mild MR in follow up and two died, 1 in-hospital and the other later (who had MR 2+ in postoperative echocardiography). 5 (16.1%) patients had MR 3+ at follow up or postoperative echocardiography; 4 of them were in the IMR group and only 1 patient was in the FMR group, but difference was not significant (p= 0.62). Mean ejection fraction in these patients was 42% vs. 44% in the rest, p= 0.7. 8 patients (20%) had MR 3+ with echocardiography or angiography before operation, in 4 patients severity of MR was different with these two methods, in 4 other patients
Hakimeh Sadeghian et al

21The Journal of Tehran Heart Center
Moderate Mitral Regurgitation ...
when our surgeons checked severity of MR in the time of operation, it seemed non significant and so they did not repair mitral valve. In follow up of these patients, 3 had MR3+ (one died later), 1 MR 2+, 1 MR 1 +, 2 no MR and another died later. From 5 patient who had MR 3+ after operation, 3 had MR3+ before operation, 1 MR 1+ and 1 MR 2+.
Intraoperative transesophageal echocardiography
From 3 patients who had intraoperative TEE (post-pump) 1 had moderate MR and she died on the day of operation, 2 had mild MR and upon follow up echocardiography one of them had mild MR and the other moderate MR.
Discussion
There are two key findings in this study: 1) although resolution of MR after CABG alone is statistically significant and 55% of patients had resolution of MR, but 45% continued to have moderate MR after CABG alone.
2) There is a trend for persistence of MR in patients with impaired LV systolic function. In addition, most patients with MR 3+ after CABG alone were in the IMR group.
Effect on mortality
In hospital mortality was 5% and overall mortality in the patients who were followed was 7/35 (20%).
Parsonnet score of these patients was 19.58 ± 9.77. According to the Parsonnet score, in-hospital mortality for a score between 15-20, is about 9.5 %16 so in-hospital mortality in this study is lower than comparable populations.
Late mortality in our study was 16.5 % which was comparable to the Ogus report (16%),4 but mean ejection fraction of their patients was lower (25±5%).
Clinical Implications
The present study addressed the specific question of whether CABG alone corrects moderate MR in the mid term.
Although many patients had some improvement in their MR, a significant proportion was left with moderate MR. The long term clinical implications of these results are not specifically addressed in the present study. Whether these results justify more liberal use of mitral annuloplasty depends on the answer to 2 follow up questions: 1) what is The long-term impact of residual MR on functional status and survival? 2) Does this MR gradually progress to severe MR and produce left atrial and ventricular dilation, elevate pulmonary pressure, increase the frequency of atrial fibrillation and need for reoperation?
Skeptics have argued that residual MR after CABG alone does not have an adverse effect on late functional status or survival.
In the Emory group study,6 5-and 10- year actuarial survival
was nearly identical to that of a control group without preoperative MR undergoing CABG during the same time period. One other study suggests that CABG alone does not affect long-term survival in patients with moderate ischemic MR.17
Two large studies18,19 in the 1980s suggest that MR is an independent risk factor for late death in patients undergoing CABG.
There is limited information in the literature on the late functional status of patients undergoing CABG alone for moderate ischemic MR. Mallidi et al reported that overall late survival was not affected by the presence of mild to moderate degrees of mitral regurgitation in patients undergoing CABG but These patient had poorer event-free survival and worse late functional status.13 The Emory study6 reported a trend toward more class III and IV angina (29% versus 6%) and congestive heart failure (14% versus 6%) compared with case-matched controls. On the other hand, Bolling et al20 reported that nearly all patients undergoing mitral valve repair at the time of CABG moved from class III or IV to class I or II.
These findings raise the possibility that even if the significant rate of residual MR noted in the present study does not result in decreased long term survival, it may adversely affect long-term functional status and quality of life. Concomitant mitral valve repair may therefore be justified, if it can be performed with relatively low operative risk, to improve long-term functional status. In our study, there is a trend for persistence of moderate MR in patients with left ventricular systolic dysfunction. In addition, of 5 patients with MR3+ after CABG, 4 were in the IMR group. Is there any association between Ischemic MR as the mechanism of MR and preoperative ejection fraction with resolution of MR after CABG alone? If this hypothesis could be proved, we can determine patients who need mitral valve repair by preoperative transthoracic echocardiography. For proving the hypothesis we need a prospective study with more patients.
Study Limitations
The primary limitation of the present study is that it is a retrospective analysis, susceptible to various sources of bias.
The second limitation is that decision to forgo concomitant mitral valve repair was not based on specific preoperative criteria but solely on surgeon preference.
Individual surgeons differed in their threshold for exploring the mitral valve based on their assessment of the literature, with some surgeons performing CABG alone as a matter of policy.
Conclusion Although CABG alone reduces MR severity significantly
in patients with moderate non organic MR, but about 45%

The Journal of Tehran Heart Center
22
of patients are left with moderate MR, so wider application of mitral annuluplasty may be warranted in these patients. More detailed analysis is necessary to determine preoperative factors that predict residual MR after CABG alone, and long-term follow up is necessary to determine the impact of residual MR on late symptoms and survival.
A prospective study with routine echocardiography is necessary to determine whether LV systolic function, persistent wall motion abnormality and scarring myocardium have any effect on residual MR after CABG in these patients.
References1. Gorman RC, Gorman III/L JH, Edmunds, Jr. H. Ischemic mitral regurgitation. In:Cohn LH, Edmunds, Jr. LH, eds. Cardiac surgery in the adults. New York: Mc GRAWHILL; 2003. p. 751-769.2. Balu V, Hershowitz S, Zaki Masud AR, Bhayana JN, Dean DC. Mitral regurgitation in coronary artery disease.Chest 1982;81:550-555. 3. Christenson JT, Simonet F, Bloch A, Maurice J, Velebit V, Schmuziger M. Should a mild to moderate ischemic mitral valve regurgitation in patients with poor left ventricular function be repaired or not? J Heart Valve Dis 1995;4:484-488.4. Ogus NT, Hulusi Us M, Ogus H, Islik O.Coronary artery bypass grafting alone for advanced ischemic left ventricular dysfunction with significant Mitral regurgitation: early and midterm outcomes in a small series. Tex Heart Inst J 2004;1:143-8. 5. Tolis GA., Korkolis DM, Kopf GS, Elefterades JA.. Revascularization alone (without mitral valve repair) suffices in patients with advanced ischemiccardiomyopathy and mild-to-moderate mitral regurgitation. Ann Thorac Surgery 2002;74:1476-81.6. Duarte IG, Shen Y, MacDonald MJ, Jones EL, Carver JM, Guyton RA.. Treatment of moderate mitral regurgitation and coronary disease by coronary bypass alone: late results. Ann Thorac Surg 1999;68:426-430.7. Connolly MW, Gelbfish JS, Jacobowitz IJ, Rose DM, Mendelsohn A, Cappabianca PM. Surgical results for mitral regurgitation from coronary artery disease. J Thorac Cardiovasc Surg 1986;91:379-388. 8. Arcidi JM Jr, Hebeler RF, Craver JM, Jones EL, Hatcher CR Jr, Guyton RA.. Treatment of moderate mitral regurgitation and coronary disease by coronary bypass alone. J Thorac Cardiovasc Surg 1988;95:951-959.9. Rydén T, Bech-Hanssen O, Brandrup-Wognsen G, Nilsson F, Svensson S, Jeppsson A. The importance of grade 2 ischemic mitral regurgitation in coronary artery bypass grafting. European Journal of Cardio-thoracic Surgery 2001;20:276-281.10. Aklog L, Filsoufi F, Flores KQ, Chen RH, Chon LH, Nathan NS, Byrne JG, Adams DH. Does coronary artery bypass grafting alone correct moderate ischemicmitral regurgitation? Circulation 2001;104[suppl I]: I-68-I-75.11. Czer LSC, Maurer G, Bolger AF, Derobertis M, Chaux RNA, JM Matloff. Revascularization alone or combined with suture annuloplasty for ischemic mitral regurgitation: evaluation by color Doppler echocardiography. Tex Heart Inst J 1996;23:270-278.12. Harris KM, Sundt Ш TM, Aeppli D, Sharma R, Brazilai B. Can
late survival of patients with moderate ischemic mitral regurgitation be impacted by intervention on the valve? Ann Thorac Surg 2002;74:1468-75.13. Mallidi HR. Pelletrier MP. Lamb j, Desai N, Sever j, Christakis GT. Late outcomes in patients with uncorrected mild to moderate mitral regurgitation at the time of isolated coronary artery bypass grafting. J throc cardiovasc Surg 2004;127:636-644.114. Feigenbaum H, Armstrong WF, Ryan T. Mitral valve Disease. In: Feigenbaum H, Armstrong WF, Ryan T, eds. Feigenbaum’s Echocardiography. 6th ed. Philadelphia: WILLIAMS and WILKINS; 2005. p. 306-385.15. Grossman W. Profiles in valvular heart disease. In: Baim D, Grossman W, eds. Cardiac catheterization, angiography, and intervention. Baltimore: Mc GRAW-HILL; 2001. p. 742-743.16. Lawrence DR, Valencia O, Smith EEJ, Murday A, Treasure T. Parsonnet score is a good predictor of the duration of intensive care unit stay following cardiacsurgery. Heart 2000;83:429-432.17. Hickey MS, Smith LR, Muhlbaier LH, Harrell FE Jr, Reves JG, Hinohara T, Califf RM, Pryor DB, Rankin JS. Current prognosis of ischemic mitral regurgitation: Implications for future management. Circulation 1988;78(suppl I): I-51-I-59.18. Adler DS, Goldman L, O’Neil A, Cook EF, Mudge GH Jr, Shemin RJ, DiSesa V, Cohn LH, Collins JJ Jr. Long-term survival of more than 2,000 patients after coronaryartery bypass grafting. Am J Cardiol 1986;58:195-202.19. Pinson CW, Cobanoglu A, Metzdorff MT, Grunkemeier GL, and Kay PH, Starr A.Late surgical results for ischemic mitral regurgitation: role of wall motion score andseverity of regurgitation. J Thorac Cardiovasc Surg 1984;88:663-672.20. Bolling SF, Deeb GM, Bach DS. Mitral valve reconstruction in elderly, ischemic patients. Chest 1996;109:35-40.
Hakimeh Sadeghian et al

23The Journal of Tehran Heart Center
Original Article
Surgical Radiofrequency MAZE III Ablation for Treatment of Atrial Fibrillation During Open Heart Surgery
Rezayat Parvizi, MD*, Fariborz Akbarzadeh, MD
Department of cardiothoracic surgery, Madani Heart Hospital.Tabriz University of Medical Sciences, Tabriz, Iran.
Abstract
Background: Atrial fibrillation is a common arrhythmia in patients with rheumatic mitral and other valve diseases who are candidates for valve repair surgeries. Conversion of rhythm to sinus has positive effects on quality of life and lower use of medications. The aim of this clinical study was to evaluate the effectiveness of the radiofrequency ablation Maze III pro-cedure in the treatment of atrial fibrillation associated with rheumatic heart valve disease.
Methods: We applied a modified Cox III Maze procedure using radiofrequency ablation in the treatment of atrial fibrilla-tion associated with rheumatic heart valve disease and evaluated the outcome of 20 patients of atrial fibrillation associated rheumatic valve disease who underwent radiofrequency ablation Maze III procedure plus heart valve surgery. Demographic, echocardiographic, Electrocardiographic and Doppler study data were calculated before surgery, six month and one year after surgery..
Results: No perioperative deaths occurred in the study group. Duration of additional time for doing radiofrequency ablation was about 22 minutes. Freedom from atrial fibrillation was 85% and 75% at six months and one year follow-up respectively...
Conclusions: The addition of the radiofrequency ablation Maze procedure to heart valve surgery is safe and effective in the treatment of atrial fibrillation associated with rheumatic heart valve disease..
The Journal Of Tehran Heart Center 1 (2006) 23-27
Keywords: Radiofrequency ablation • MAZE ablation • Atrial fibrillation
*Corresponding Author: Rezayat Parvizi, Department of cardiothoracic surgery, Madani heart hospital, Tabriz, Iran. P.O.BOX: 51665/404. Tel: +98 (411) 3361175. Fax: +98 (411) 3344021. E-mail: [email protected]
Introduction
Among the varieties of supraventricular arrhythmias that confront electrophysiologists, atrial fibrillation remains the most vexing affecting 0.4% of the general population and up to 10% of persons older than 65 years. Not only is atrial fibrillation extremely common, it is a progressive disorder that is often poorly controlled with antiarrhythmic medications.1, 2
More importantly, atrial fibrillation (AF) is often associated with other cardiac diseases that compromise the patient’s clinical outcome. 60% of patients admitted for mitral valve surgery and up to 5% of patients undergoing coronary revascularisation are known to have chronic AF. Restoration of sinus rhythm (SR) with atrioventricular resynchronization may be difficult in patients with chronic or permanent AF or

The Journal of Tehran Heart Center
24
other risk factors for AF.2,3 Over the past 5 years, increasing attention has been focused on the development of catheter ablation techniques and ablation systems to cure atrial fibrillation. The importance of this endeavor has been fueled by a number of factors including the clinical importance of atrial fibrillation because of its high prevalence in the general population, associated symptoms, stroke risk, and increased mortality; the limited efficacy, side effects, and risks associated with pharmacologic therapy; and demonstration of the feasibility of curing atrial fibrillation with open heart surgical procedures and also with catheter ablation techniques.4 Cox and colleagues developed and applied the Maze procedure successfully in patients with lone atrial fibrillation (AF). Although isolated AF itself has been reported to carry a low risk of thromboembolism, AF increases the risk significantly when associated with organic disease. Once AF becomes sustained in these patients, it usually persists even after otherwise successful operation for the underlying lesions. Because developing AF signifies pathologic degradation and symptomatic deterioration in these patients, simultaneous treatment of the rhythm and organic lesions has long been desired and expected to improve prognosis. Nonetheless, Adding the Maze procedure may increase the risk because of extensive atrial incision and reanastomosis requiring longer cardiac arrest and cardiopulmonary bypass time. For this reason, we used radiofrequency ablation and modified the Maze atriotomy so as to shorten the operating time and preserve the sinus node artery. Moreover, myocardial changes and fibrosis derived from underlying diseases may render the Maze procedure less effective than in lone AF.5,6 The operating time and preserve the sinus node artery. Moreover, myocardial changes and fibrosis Derived from underlying diseases may render the Maze procedure less effective than in lone AF.5, 6
Methods Patients
From October 2003 to January 2005, twenty consecutive patients with a history of at least one year duration of chronic atrial fibrillation (AF) caused by mitral valve (MV) and other valvular disorders underwent a radiofrequency modified maze III procedure combined with MV and other valvular surgeries and left atrial reduction surgery when needed. All patients had documented AF for at least one year before operation. Demographic, echocardiographic, angiographic and catheterization data were collected before surgery. The average size of the left atrium was measured on M-mode tracing taken from a two-dimensional parasternal long-axis view (E 850, Ving Med echocardiograph system). In all patients ventricular rate control medication, i.e. calcium blockers and/or digoxin, was allowed until the day before surgery. Oral anticoagulant therapy (warfarin) for the
prevention of thromboembolism secondary to chronic AF was discontinued 2 days before surgery. Beta-Adrenergic blockers were continued...
Surgical procedure Radiofrequency energy unipolar was used to create long
continuous endocardial lesions under direct vision with a hand-held cooled tip probe in all patients. The ablation procedure was done in a bloodless operating field and temperature guided energy applications were performed with a pre selected catheter tip temperature.
The heart was exposed through a median sternotomy and suspended in a pericardial cradle. Cardiopulmonary bypass was instituted using standard aortic and bicaval cannulation and moderate hypothermia. The operative procedure was based on the Maze III
procedure as described by Cox et al.6 In our RF modification, all atrial incisions currently used in the maze III were replaced by endocardial linear ablation lines as illustrated in Figure 1 except for the incisions to enter the left and right atrial cavity.
Figure 1. RF modified maze schematic view of the dorsal aspect of the heart. Line A, electrical activation: zig zag line B, incision in the atria; dotted line C, ablation lines. LAA, left atrial appendage; RAA, right atrial appendage; IVC, Inferior Vena Cava; SVC, Superior Vena Cava; LPV, Left Pulmonary Veins; RPV, Right Pulmonary Veins.
According to the original Maze III both appendages were
excised as well. The right-sided maze was performed on the beating heart without cross-clamp. The left-sided Maze procedure was started after the heart was arrested with cold cardioplegic solution and the aorta cross-clamped. Both left and right pulmonary veins were isolated separately. Concomitant procedures, e.g. tricuspid valve repair, were performed immediately after aortic cross-clamping and prior to completing the left-sided Maze and the mitral valve procedure. During rewarming the left atrium was closed and the cross-clamp released. The heart was then de-aired extensively prior to defibrillation and to closing of the right atrium. Occasionally atrial pacing or ventricular pacing was needed to wean off bypass.
Follow-up
Early postoperative care was similar to that for routine
Rezayat Parvizi et al
25The Journal of Tehran Heart Center
Surgical Radiofrequency MAZE III Ablation ...
open-heart surgery. Cardiac rhythm was continuously monitored after surgery until
stable rhythm returned. Temporary epicardial wire attached to the right ventricle was used to pace the patient in case of severe bradycardia. We started infusion of amiodarone after surgery (150 mg loading dose and 0.5 mg/min) during the first day of ICU care and 200 mg orally per day for 6 months.2 Postoperative atrial tachy arrhythmias were treated with additional doses of amiodarone and beta blockers which sometimes combined with DC cardioversion, if necessary. Patients were seen in the outpatient clinic monthly and at 6 months and one year after operation, or earlier when necessary. Antiarrhythmic drugs were tapered gradually after cardiac rhythm was considered stable. Amiodarone was stopped after 6 months. Transthoracic Doppler echocardiography was performed at 6 months and 1 year after surgery to assess atrial mechanical function. The AF after surgery is defined as AF which persists more than 48 hours.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation. Means were compared using Student’s t-test. In the case of non-normal distribution, the nonparametric Wilcoxon test was used. A P value less than 0.05 was considered statistically significant.
Results
Demographic data We studied twenty patients (nine men and 11 women);
mean age was 46.35 ± 10.6 years.
Operative data The mean time for doing radiofrequency ablation was
about 22±3 min.Concomitant cardiac procedures (Table 1) included mitral valve (MV) repair (n=2), MV replacement (n=18), tricuspid valve repair (n=3), aortic valve (AV) repair (n=1), AV replacement (n=9), and left atrial reduction (n=6). In three patients the surgery was redo operation. Atrial reduction (n=6). In three patients the surgery was redo operation.
Table 1: Operative data of patients
Patients MV Disease AV Disease TV Disease/therapy
TherapyMV
TherapyAV
MS MR AS AR OMVC MVR AV Rep AVRMen 9 4 0 5 2 0 9 0 5
Women 10 5 1 4 1 2 9 1 4Total 19 9 1 9 3 2 18 1 9
MV: Mitral valve, AV: Aortic valve, TV: Tricuspid valve, MS: Mitral stenosis, MR: Mitral regurgitation, AS: Aortic stenosis, AR: Aortic regurgitation, OMVC: Open MV comissurotomy, MVR: MV replacement, AV Rep: AV repair, AVR: AV replacement
Cardiac rhythm and atrial transport
Rhythm of all patients except one was sinus upon arriving to ICU and except two patients the rhythm of remaining patients were sinus at discharge. Two patients had low rate junctional rhythm during their stay in ICU, so amiodarone was discontinued and temporary ventricular pacing continued until patients’ rhythm converted to sinus. During ICU stay, rhythm of 4 patients changed to AF: For two of them cardioversion converted their rhythm to sinus, while in one patient rhythm converted to sinus automatically. Rhythm conversion to sinus was unsuccessful in one patient. During follow up, five patients underwent DC-shock therapy for treatment of AF, which was successful in three patients and converted their rhythm to sinus. Rhythm of two patients converted to sinus automatically. One of our patients got atrial flutter during follow-up which treated was successfully with DC-shock therapy. All patients completed six month follow up and 85% of patients were free of AF. At six months follow up in patients who were in sinus rhythm, left atrial transport and contractility were assessed by transthoracic Doppler study: 82% had left atrial contraction. In patients who were free of AF, amiodarone (200 mg/day) was discontinued after six months. In patients with AF whose rhythm didn’t convert to sinus by DC-shock or patients who were unwilling to undergo this rate control strategy.
At one year follow up, 75% of patients had sinus rhythm 24 hour ambulatory Electrocardiographic study and in patients with sinus, rhythm transthoracic Doppler study showed 80% atrial transport. The mean ejection fraction of patients was 51.25% ± 8.7 and 53.25% ± 6.3 before and one year after surgery: This difference was statistically significant (P= 0.035).. The LA size was 5.03 ± 0.74 before surgery which decreased to 4.4 ± 0.58 one year after surgery, which was statistically significant (P= 0.002) also.
Complication Hospital and ICU stay didn’t change significantly in our
patients. There was no major bleeding or need for permanent pacing..

The Journal of Tehran Heart Center
26
Discussion
In the majority of patients who undergo MV surgery in chronic AF at the time of operation, the arrhythmia will remain after surgical correction of the underlying cardiac disease.6,7,8 However, in patients with intermittent AF or AF duration of less than 1 year, MV surgery alone is sufficient to restore sinus rhythm in the majority of patients.6,7,9 In this study we included only patients with a history of AF of at least 1-year duration, in whom it was unlikely for sinus rhythm to be Regained after valve surgery. The Cox’s Maze procedure6,10,11 has apparently remained an universally applicable and potentially effective treatment to restore sinus rhythm in patients with chronic AF and concomitant structural heart disease.6,12,13 However, this surgical procedure involves extensive incision and suturing of the atria. In an attempt to simplify the original Maze, our group and others4,14,15 used Radiofrequcucy (RF) energy intraoperatively to create linear ablation lines endocardially - under direct visual guidance - to eliminate AF. The RF pattern we used is based on the maze III concept,11 and most of the atrial incisions of the original Maze procedure are replaced by RF lesions. As a consequence, the extra cardiac arrest time to complete the left-sided part of the Maze procedure was only 22 min.
The aim of AF surgery is restoration of sinus rhythm and reestablishment of atrial mechanical function. This was achieved in the majority of the patients in our study, which icomparable with the surgical maze III in patients with long-standing AF and structural heart disease.16,17 Swartz reported that sinus rhythm could be maintained in long-term follow-up in >70% of patients with this approach.1 Our study showed restoration of sinus rhythm in 75% of patients at one year follow up which is comparable with most other studies. Conduction gaps within the ablation lines may predispose patients to iatrogenic left atrial macro-reentrant arrhythmias that may necessitate a second ablation procedure in as many as 55% of patients,1 in our study, one of patients had atrial flutter during follow up which was treated successfully with DC shock cardioversion permanently. Cox and associates 18 Demonstrated that preservation of atrial transport function was 85.1% in the left atrium after the Maze III when evaluated by transthoracic Doppler echocardiography, although when additional techniques such as transesophageal Doppler echocardiography or magnetic resonance imaging, were used, preservation of transport function was 94% in the left atrium. The high percentage of atrial contractility in this patient group in contrast to other studies11,19,20 can be explained by the use of transesophageal Doppler echocardiography to assess atrial transport function while others have relied on transthoracic Doppler echocardiography as a means to show atrial contractility. Furthermore, we have observed recovery of left atrial function in the majority of patients undergoing intraoperative RF ablation which was about 80% with Doppler echocardiography study.21 There is no significant
difference in the postoperative sinus rhythm conversion rates between the classical ‘cut and sew’ and the alternative sources of energy, which were used to treat atrial fibrillation,22 so we conclude that our results are not significantly different from conventional Maze procedure. Finally, some studies reported better results of conversion to sinus rhythm by radiofrequency ablation applied at limited epicardial and or endocardial sites in patients with AF during MV surgery,14,23,24,25 but in contrast to our patient population, these studies also included patients with paroxysmal AF and AF duration
less than 1 year and, according to recent studies9,26 these patients have a higher likelihood to remain in sinus rhythm after surgery.
We are continuing doing RF ablation in our patients with AF who are otherwise candidates for cardiac surgery, so these results are preliminary results of patients during the last couple of years: Hopefully with increasing with increase in patient number we will be able to reach more reliable result and conclusions regarding this ongoing study.
Conclusion The Cox maze III radiofrequency ablation remains the
gold standard for the treatment of atrial fibrillation and has excellent long-term efficacy.
Acknowledgement
We would like to thanks all personnel of ICU, cardiac surgery room and echocardiography room of Shahid Madani heart center and all of other peoples who helped us to do this research.
References
1. Neal Kay G. Catheter Ablation of Atrial Fibrillation: Challenges and Promise. Am J Cardiol 2000;86(suppl):25K–27K.. 2. Guden M, Akpınar B, Sanisoglu I, Sagbas E, and Bayındır O. Intraoperative Saline-Irrigated Radiofrequency Modified Maze Procedure for Atrial Fibrillation. Ann Thorac Surg 2002;74:S1301–1306. 3. Deneke T, Khargi K, Hubert Grewe P, Dryander SV, Kuschkowitz F, Lawo T. Left Atrial Versus Bi-Atrial Maze Operation Using Intraoperatively Cooled-Tip Radiofrequency Ablation in Patients Undergoing Open-Heart Surgery Safety and Efficacy. American College of Cardiology 2002;39:1644-1650. 4. Calkins H, Hall J, Ellenbogen K, Walcott G, Sherman M, Bowe W. A New System for Catheter Ablation of Atrial Fibrillation. Am J Cardiol 1999;83:227–236. 5. Kawguchi A, Kosakai Y, Sasako Y, Eishi K, Nakano K, Kawashima Y. Risks and Benefits of Combined Maze Procedure for Atrial Fibrillation Associated With Organic Heart Disease. J Am Col Cardiol 1996;28:985-990. 6. Siea TH, Beukemaa WP, Ramdat Misiera AR, Elvana A, Ennemaa
Rezayat Parvizi et al

27The Journal of Tehran Heart Center
Surgical Radiofrequency MAZE III Ablation ...
JJ, Wellensb HJJ. The radiofrequency modi®ed maze procedure: A less invasive surgical approach to atrial fibrillation during open-heart surgery. European Journal of Cardio-thoracic Surgery 2001;19:443-447.7. Williams JM, Ungerleider RM, Loand GK, Cox JL. Left atrial isolation: new technique for the treatment of supraventricular arrhythmias. J Thorac Cardiovasc Surg 1980;80:373-380.. 8. Scheinmann MM, Morady F, Hess DS, Gonzalez R. Catheter induced ablation of the atrioventricular junction to control refractory supraventricular arrhythmias. J Am Med Assoc 1982;248:851-855. 9. Obaida JF, El Farra M, Bastien OH, Lievre M, Martelloni Y, Chassignolle JF. Outcome of atrial fibrillation after mitral valve repair. J Thorac Cardiovasc Surg 1997;114:179-185. . 10. Defauw JJAMT, Guiraudon GM, van Hemel NM, Vermeulen FEE, Kingma JH, De Bakker JMT. Surgical therapy of paroxysmal atrial fibrillation with the corridor operation. Ann Thorac Surg 1992;53:564-571. 11. Feinberg MS, Waggoner AD, Kater KM, Cox JL, Lindsay BD, Perez JE. Restoration of atrial function after the maze procedure for patients with atrial fibrillation: Assessment by Doppler echocardiography. Circulation 1994;90(Part2):II285-II292.. 12. Hioki M, Ikeshita M, Iedokoro Y, Nitta T, Harada A, Asano T, Tanaka S, Shoji T. Successful combined operation for mitral stenosis and atrial fibrillation. Ann Thorac Surg 1993;55:776-778... 13. Izumoto H, Kawazoe K, Kitahara H, Kamata J. Operative results after Cox/maze procedure combined with mitral valve operation. Ann Thorac Surg 1998;66:800-804.. 14. Melo J, Adraga P, Neves J, Ferreira M, TimoTeo A, Santiago T, Ribeiras R, Canada M. Endocardial and epicardial radiofrequency ablation in the treatment of atrial fibrillation with a new intra-operative device. Eur J Cardio-thorac Surg 2000;18:182-186.. 15. Chen MC, Guo GBF, Chang JP, Yeh KH, Fu M. Radiofrequency and cryoablation of atrial Fibrillation in patients undergoing valvular operations. Ann Thorac Surg 1998;65:1666-1672... 16. Kosakai Y, Kawaguchi AT, Isobe F, Sasako Y, Nakano K, Eishi K, Kito Y, Tanaka N, Kawashima Y. Cox maze procedure for chronic atrial fibrillation associated with mitral valve disease. J Thorac Cardiovasc Surg 1994;108:1049-1055... 17. Kamata J, Kawazoe K, Izumoto H, Kitahara H, Shiina Y, Sato Y, Nakai K, Kubo T, Tsuji I, Hiramori K. Predictors of sinus rhythm restoration after Cox Maze procedure concomitant with other cardiac operations. Ann Thorac Surg 1997;64:394-398.. 18. Cox JL, Boineau JP, Schuessler RB, Jaquiss RDB, Lappas DG. Modification of the maze procedure for atrial flutter and atrial fibrillation: Rationale and surgical results. J Thorac Cardiovasc Surg 1995;110:473-484.. 19. Kosakai Y, Kawaguchi AT, Isobe F, Sasako Y, Nakano K, Eishi K, Kito Y, Kawashima Y. Modified maze procedure for patients with atrial fibrillation undergoing simultaneous open heart surgery. Circulation 1995; 92(Suppl II):359-364. 20. Kim KB, Cho KR, Sohn DW, Ahn H, Rho JR. The Cox-maze III procedure for atrial fibrillation associated with rheumatic mitral valve disease. Ann Thorac Surg 1999;68:799-804.. 21. Beukema WP, Ramdat Misier AR, Sie HT, Ennema JJ, Wellens HJJ. Immediate and long term recovery of atrial function in patients with chronic atrial fibrillation 22. Khargia K, Huttenb BA, Lemkec B, Deneked T. Surgical treatment of atrial fibrillation; a systematic review. European Journal of Cardio-thoracic Surgery 2005;27:258–265.23. Benussi S, Pappone C, Nascimbene S, Oreto G, Caldarola A,
Stefano PL, Casati V, Alfieri O. A simple way to treat chronic atrial fibrillation during mitral valve surgery: the epicardial radiofrequency approach. Eur J Cardio-thorac Surg 2000;17:524±529. 24. Sie HT, Beukema WP, Ramdat Misier AR, Elvan AE, Ennema JJ, Haalebos MMP, Wellens HJJ, and Radiofrequency modified maze in patients with atrial fibrillation Undergoing concomitant cardiac surgery. J Thorac Cardiovasc Surg 2001;122:249-256.25. Guang Y, Zhen-jie C, Yong LW, Tong L, Ying L. Evaluation of clinical treatment of atrial fibrillation associated with rheumatic mitral valve disease by radiofrequency ablation. European Journal of Cardio-thoracic Surgery 2002;21:249–254.

28
29The Journal of Tehran Heart Center
Original Article
The Role of Carotid Artery Screening Before Coronary Artery Bypass Graft Surgery
Shapour Shirani, MD1, Mohammad Ali Boroumand, MD1, Seyed Hesameddin Abbasi, MD1,2, Negar Maghsoodi, MD1, Majid Shakiba, MD1, Abbasali Karimi, MD1, Saeed Dav-oodi, MD1, Maryam Esfandbod1
1Tehran Heart Center, Tehran University of Medical Sciences, Tehran, Iran. 2National Iranian Oil Company Central Hospital, Tehran, Iran.
Abstract
Background: The incidence of stroke is 2.1-5.2% in bypass surgery patients with a mortality of 0-38%. This study was designed to evaluate the incidence of significant carotid artery stenosis and its related risk factors in candidates for coronary artery bypass graft (CABG) surgery.
Methods: 1045 consecutive candidates for CABG underwent carotid artery Doppler examination in a prospective study. The relation of age, sex, smoking and diabetes as well as lipid profile and carotid stenosis was evaluated. . .
Results: In 1045 CABG candidates with the mean age of 60 years, the prevalence of significant carotid stenosis (>60%) was 6.9%. In the patients who aged 65 years and older, significant stenosis was12.5%. Age of 50 years and above, female gender, hypercholesterolemia and diabetes mellitus are independent risk factors for significant carotid stenosis.
Conclusion: Significant carotid stenosis has an earlier beginning in our study. Cost effectiveness studies are recommended for revising the previous screening protocols. .
The Journal of Tehran Heart Center 1 (2006) 29-32
Keywords: Carotid doppler • CABG • Carotid screening .
*Corresponding Author: Shapour Shirani, Radiology Department, Tehran Heart Center, Tehran University of Medical Sciences, Tehran, Iran 1411713138. Tel: 88029600-69. Fax: 88029731. E-mail: [email protected].
Introduction
Excluding intraoperative death, stroke is the most dreaded perioperative complication in patients that undergo coronary bypass surgery. The incidence of stroke is 2.1-5.2% in bypass surgery patients with a mortality of 0-38%.1 Shedding debris from carotid or aortic atherosclerotic plaques, embolization of the intracardiac clot and a decrease in perfusion pressure to <60 mmHg are the etiologic causes of stroke associated with bypass surgery.2 The carotid stenosis can be diagnosed
and managed preoperatively. Therefore, several studies recommend preoperative carotid screening in all bypass candidates.3, 4 However, some others recommend it only in high risk patients. The stated risk factors are: over 65 years of age,1 carotid bruit on physical examination,1,5,6 female gender, previous cerebrovascular accident or transient ischemic attack, peripheral vascular stenosis,1,7,8 hypertension,1 left main coronary stenosis, history of smoking,7,8 and diabetes
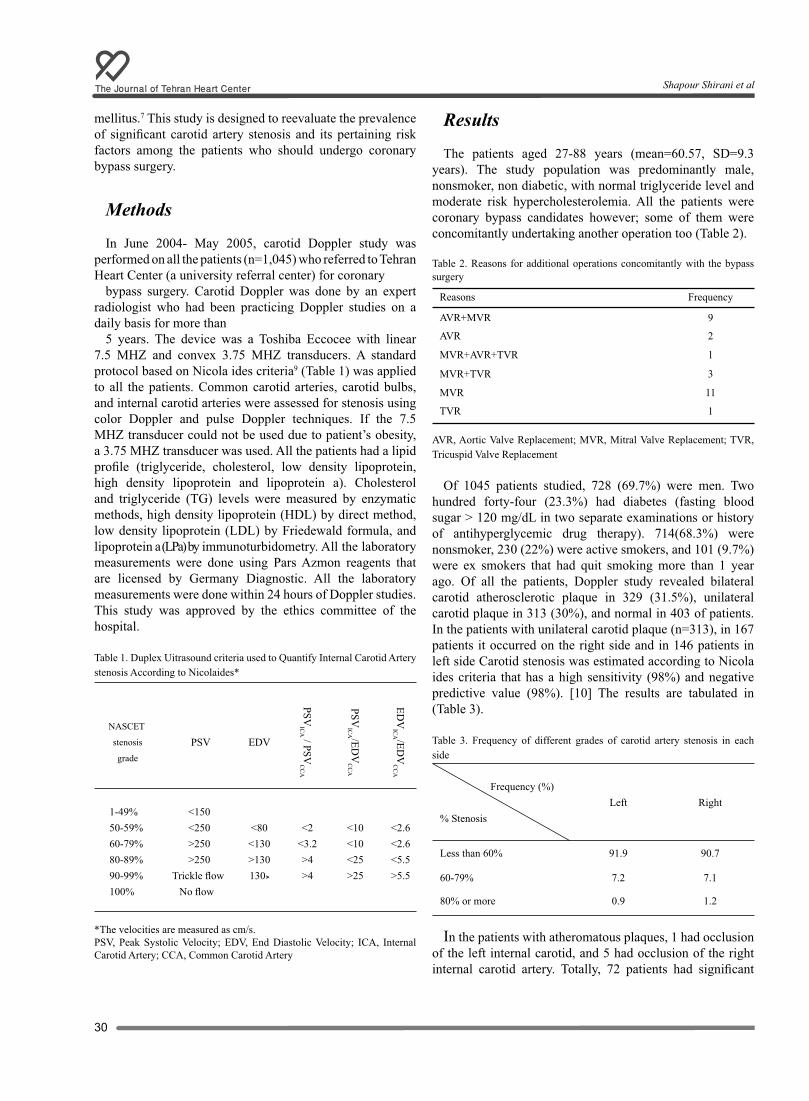
The Journal of Tehran Heart Center
30
mellitus.7 This study is designed to reevaluate the prevalence of significant carotid artery stenosis and its pertaining risk factors among the patients who should undergo coronary bypass surgery.
Methods
In June 2004- May 2005, carotid Doppler study was performed on all the patients (n=1,045) who referred to Tehran Heart Center (a university referral center) for coronary
bypass surgery. Carotid Doppler was done by an expert radiologist who had been practicing Doppler studies on a daily basis for more than
5 years. The device was a Toshiba Eccocee with linear 7.5 MHZ and convex 3.75 MHZ transducers. A standard protocol based on Nicola ides criteria9 (Table 1) was applied to all the patients. Common carotid arteries, carotid bulbs, and internal carotid arteries were assessed for stenosis using color Doppler and pulse Doppler techniques. If the 7.5 MHZ transducer could not be used due to patient’s obesity, a 3.75 MHZ transducer was used. All the patients had a lipid profile (triglyceride, cholesterol, low density lipoprotein, high density lipoprotein and lipoprotein a). Cholesterol and triglyceride (TG) levels were measured by enzymatic methods, high density lipoprotein (HDL) by direct method, low density lipoprotein (LDL) by Friedewald formula, and lipoprotein a (LPa) by immunoturbidometry. All the laboratory measurements were done using Pars Azmon reagents that are licensed by Germany Diagnostic. All the laboratory measurements were done within 24 hours of Doppler studies. This study was approved by the ethics committee of the hospital. . .
Table 1. Duplex Uitrasound criteria used to Quantify Internal Carotid Artery stenosis According to Nicolaides*
EDV
ICA /ED
VC
CA
PSVIC
A /EDV
CC
A
PSVIC
A / PSVC
CA
EDV PSVNASCET
stenosis
grade
<2.6<2.6<5.5>5.5
<10<10<25>25
<2<3.2>4>4
<80<130>130130>
1-49% <150 50-59% <250 60-79% >250 80-89% >250 90-99% Trickle flow 100% No flow
*The velocities are measured as cm/s. PSV, Peak Systolic Velocity; EDV, End Diastolic Velocity; ICA, Internal Carotid Artery; CCA, Common Carotid Artery
Results
The patients aged 27-88 years (mean=60.57, SD=9.3 years). The study population was predominantly male, nonsmoker, non diabetic, with normal triglyceride level and moderate risk hypercholesterolemia. All the patients were coronary bypass candidates however; some of them were concomitantly undertaking another operation too (Table 2). .
Table 2. Reasons for additional operations concomitantly with the bypass surgery
Reasons Frequency
AVR+MVR 9
AVR 2
MVR+AVR+TVR 1
MVR+TVR 3
MVR 11
TVR 1
AVR, Aortic Valve Replacement; MVR, Mitral Valve Replacement; TVR, Tricuspid Valve Replacement
Of 1045 patients studied, 728 (69.7%) were men. Two hundred forty-four (23.3%) had diabetes (fasting blood sugar > 120 mg/dL in two separate examinations or history of antihyperglycemic drug therapy). 714(68.3%) were nonsmoker, 230 (22%) were active smokers, and 101 (9.7%) were ex smokers that had quit smoking more than 1 year ago. Of all the patients, Doppler study revealed bilateral carotid atherosclerotic plaque in 329 (31.5%), unilateral carotid plaque in 313 (30%), and normal in 403 of patients. In the patients with unilateral carotid plaque (n=313), in 167 patients it occurred on the right side and in 146 patients in left side Carotid stenosis was estimated according to Nicola ides criteria that has a high sensitivity (98%) and negative predictive value (98%). [10] The results are tabulated in (Table 3). .
Table 3. Frequency of different grades of carotid artery stenosis in each side
Frequency (%)
% Stenosis Left Right
Less than 60% 91.9 90.7
60-79% 7.2 7.1
80% or more 0.9 1.2
In the patients with atheromatous plaques, 1 had occlusion of the left internal carotid, and 5 had occlusion of the right internal carotid artery. Totally, 72 patients had significant
Shapour Shirani et al

31The Journal of Tehran Heart Center
carotid stenosis (more than 60% stenosis) that constituted 6.9% of all the bypass surgery candidates. Of these patients, 59 had unilateral and 13 had bilateral significant stenosis. Ten patients had carotid stenosis more than 80%, 6 on the right side and 4 on the left. Six patients had obstruction in their internal carotid artery. Three hundred ninety-two patients aged 65 years and more, 49 (12.5%) of them had stenosis more than 60%, and 12 (3%) had stenosis more than 80%. . The most common site for atheromatous plaques was the carotid bulb (84% of the right-sided, and 78% left-sided plaques). The cervical portion of the internal carotid and common carotid arteries were other most common sites for plaques, respectively.
In the Chi2 test for association of gender, age, and diabetes with carotid stenosis of more than 60%: 13% of women and 4.3% of men had stenosis more than 60% (p=0.002, OR=1.4). Also, 11% of the patients with diabetes and 5.6% of nondiabetic patients had significant stenosis (p=0.003, OR=1.4). The prevalence of significant stenosis was 1.3% for less than 50 years of age, and 7.9% for 50 years and over (P<0.0001). Regarding the low number of female smokers in our study (16 active smokers and 6 ex smokers), the association of smoking and carotid stenosis was evaluated only among the men. Thus, 5.8% of the nonsmoker men had stenosis more than 60%. It was respectively 2.3% and 2.1% in active smokers and those with history of smoking (p=0.063).
The effect of atherogenic factors (triglyceride, cholesterol, LDL and LPa) were assessed in regard with carotid stenosis. Patients were grouped for LPa level as normal (< 30 mg/dL) and high (≥ 30 mg/dL), for cholesterol level as desirable (< 200 mg/ dL), moderate risk (200-240 mg/dL), and high risk (≥ 240 mg/dL), for triglyceride level as normal (<200 mg/dL), moderately high (200-400 mg/dL), and high (≥ 400 mg/dL), and for LDL level as normal (< 160 mg/ dL), and high (≥ 160 mg/dL). Accordingly, the significant stenosis was 7.1% in patients with normal LPa and 6.7% in the high LPa group (p=0.78). Normal LDL and high LDL groups had respectively 5.4% and 12.6% significant carotid stenosis (p=0.0006). Significant carotid stenosis occurred in 5.6% of desirable cholesterol levels, 4.6% in moderate risk, and in 13.4% of high risk groups (p=0.0001). Carotid artery stenosis of more than 60% was observed in 6.5% with normal TG, 7% with moderately high TG, and 17.4% with high TG (p=0.12). Only 23 patients had high (>400mg/dL) TG.
Discussion
In coronary bypass surgery candidates, carotid stenosis is the risk factor for stroke, in-hospital mortality and longer in-hospital stay.10 screening carotid arteries for stenosis combined with endarterectomy reduces perioperative as well as postoperative stroke. Screening also helps to discover and follow the significant carotid artery stenosis cases that do not
have neurological symptoms. . Presence of significant carotid artery stenosis can change the bypass schedule to a bypass with endarterectomy or endarterectomy and then bypass surgery.11 considering the costliness of carotid Doppler studies, it is important to determine those bypass candidates who would benefit from carotid screening. Age of more than 65 years,1 carotid bruit on examination,1,5,6 peripheral vascular stenosis,1,7,8 hypertension, 1 left main coronary stenosis,1,7,8 history of smoking,7,8 and diabetes mellitus7 have been stated as the risk factors associated with carotid stenosis in different studies. However, some other studies did not find any association between hypertension, hypercholesterolemia, smoking12 and diabetes1,12 with carotid stenosis. In regard with the fact that atherosclerosis is a multifactorial phenomenon with both genetic and environmental factors playing a role, and considering the fact that previous studies have shown coronary artery diseases are occurring at an earlier age in last decade,13,14 this study sought to assess the prevalence of carotid stenosis and its pertinent risk factors. Of 1,045 patients in this study with a mean age of 60.57 years, 72 patients (6.9%) had carotid stenosis of more than 60%. Significant stenosis was 12.5% in 65 year olds and above, which is in accordance with Berens11 and Faggioli’s12 results. Unlike Faggioli’s study that prevalence of carotid stenosis significantly increased after 60 years of age, we observed it at 50 (i.e. 1.3% at 50 years and less, and 7.9% at more than 50, p=0.002). Faggioli did not report hypercholesterolemia, hypertension, diabetes, and smoking as the risk factors for carotid stenosis, postoperative stroke and death. However, in our study high risk hypercholesterolemia (>240 mg/dL) and diabetes were associated with significant carotid stenosis (p=0.0001 and 0.003 respectively) and therefore were identified as risk factor. The risk of carotid stenosis is 17.4% with TG more than 400 mg/dL, and 6.5% with TG less than 200 mg/dL. However, the small number of the patient with TG more than 400 mg/dL in our study (33 out of 1,045) renders the statistical evaluation non conclusive. LDL level higher than 160 mg/dL was also a risk factor for carotid stenosis (p=0.0006). In the current study, smoking was not a risk factor for carotid stenosis, and hypertension was not studied. Identifying diabetes as a risk factor in our study is against the findings in Dunard’s study. Dunard observed that 32% of the patients with less than 70% carotid stenosis had a history of diabetes and the prevalence of diabetes was 34% in patients with stenosis of 70% and more. Female gender was known to be a risk factor by Dunard and Figgioli (p= <0.005 and 0.02 respectively). In our study this association was stronger (p< 0.0001). High serum LPa levels (more than 30 mg/dL) is a controversial atherogen factor. We did not find anassociation between high LPa and significant carotid stenosis.15
Conclusion
Fifty years of age and over, female gender, diabetes, and
The Role of Carotid Artery Screening ...

The Journal of Tehran Heart Center
32
hypercholesterolemia were identified the risk factors for carotid artery stenosis among our patients. In regard with the earlier occurrence of carotid stenosis in our patients by one decade, it is recommended to assess the cost effectiveness of carotid screening after the age of 50 in another study.
References1. Durand DJ, Perler BA, Roseborough GS, Grega MA, Borowicz LM Jr, Baumgartner WA, Yuh DD. Mandatory versus selective preoperative carotid screening: A retrospective analysis. Ann Thorac Surg 2004;78:159-166.2. Schwartz AE, Sandhu AA, Kaplon RJ, Young WL, Jonassen AE, Adams DC, Edwards NM, Sistino JJ, Kwiatkowski P, Michler RE. Cerebral blood flow is determined by arterial pressure and not cardiopulmonary bypass flow rate. Ann Thorac Surg 1995;60:165-169.3. Fukuda I, Gomi S, Watanabe K, Seita J. Carotid and aortic screening for coronary artery bypass grafting. Ann Thorac Surg 2000;70:2034-2039.4. Archbold RA, Barakat K, Magee P, Curzen N. Screening for carotid artery disease before cardiac surgery: is current clinical practice evidence based? Clin Cardiol 2001;24:26-32.5. Walker WA, Harvey WR, Gaschen JR, Appling NA, Pate JW, Weiman DS. Is carotid screening for coronary surgery needed? Am Surg 1996;62:308-310.6. Hill AB, Obrand D, Steinmetz OK. The utility of selective screening for carotid stenosis in cardiac surgery patients. J Cardiovasc Surg (Torino) 1999;40:829-836.7. D’Agostino RS, Svensson LG, Neumann DJ, Balkhy HH, Williamson WA, Shahian DM. Screening carotid ultrasonography and risk factors for stroke in coronary artery surgery patients. Ann Thorac Surg 1996;2:1714 -1723.8. Berens ES, Kouchoukos NT, Murphy SF, Wareing TH. Preoperative carotid artery screening in elderly patients undergoing cardiac surgery. J Vasc Surg 1992;15:313 -321.9. Nicolaides AN, Shifrin EG, Bradbury A, Dhanjil S, Griffin M, Belcaro G, Williams M. Angiographic and duplex grading of internal carotid stenosis: can we overcome the confusion? J Endovasc Surg 1996;3:58-65.10. Sabeti S, Schillinger M, Mlekusch W, Willfort A, Haumer M, Nachtmann T, Mullner M, Lang W, Ahmadi R, Minar E. Quantification of internal carotid artery stenosis with duplex US: comparative analysis of different flow velocity criteria. Radiology 2004;232:431-439.11. Berens ES, Kouchoukos NT, Murphy SF, Wareing TH. Preoperative carotid artery screening in elderly patients undergoing cardiac surgery. J Vasc Surg 1992;15:313-323.12. Faggioli GL, Curl GR, Ricotta JJ. The role of carotid screening before coronary artery bypass. J Vasc Surg 1990;12:724-729.13. Hajizeinali AM, Davoodi G, Sadeghian S, Alidoosti M, Dariaani S. Angiographic findings is 401 very premature CAD patients (age< 40). Iranian Heart J 2004;4:142-146.14. Sadeghian S, Darabian C, Hagizeinali AM , Karimi A, Amirzadegan A, Marzban M, Abbasi K, Hanafizadeh B. Relation between age and sex of CABG patients and kind and number of risk factors. Iranian Heart J 2004;4:129-133.15. Berglund L, Ramakrishnan R: Lipoprotein(a). An elusive
cardiovascular risk factor. Arterioscler Thromb Vasc Biol 2004;24:2219-2226.
Shapour Shirani et al
33The Journal of Tehran Heart Center
Original Article
Cardiac Abnormalities in the Iranian Pediatric and Adolescent Population with Chronic Renal Failure
Ali Akbar Zeinaloo, MD*, Abbas Madani, MD, Mohammad Taqi Haqi Ashtiani, MD, PhD
Children’s Hospital Medical Center, Tehran University of Medical Sciences, Tehran, Iran.
Abstract
Background: It has been well documented that left ventricular hypertrophy (LVH) is an independent factor for cardiac death in children. The epidemiologic information reveals that there is a very high prevalence of LVH in children with chronic renal failure (CRF). The purpose of this study was to evaluate the existence of left ventricular hypertrophy, its severity and other cardiac abnormalities in children and young adults with chronic renal failure (CRF), end stage renal disease (ESRD) on hemodialysis (HD) or post renal transplantation (RTx).
Methods: Sixty-three patients including 31 females and 32 males aged 1 to 18-year- old with defined causes for renal damage were enrolled in the study. Study patients were distributed in three groups: HD (n=45), CRF (9) and RTx (9). LVH and degree of hypertension were compared with an age and sex-matched control group (63 normal individuals). Left ven-tricular mass indexed for height (LVM/Ht and LVM/Ht2.7) and body surface area (LVM/BSA), and other related parameters were determined by echocardiography in both groups. Laboratory investigations were carried out at a reference laboratory for the study group.
Results: The index of LVM/BSA in CRF group was more (r=0.765) than the control group. The HD patients had signifi-cantly higher LV systolic and diastolic dimensions. Analysis of variance (ANOVA) showed the influence of groups on subject score on the LVM. A significant effect of groups on the mean score on the LVM was noted. An important finding of this study was the correlation between serum creatinine and LVM in the HD and RTx subjects by both linear and multiple regression analyses. There was also significant difference amongst groups with respect to blood parameters, which is discussed.
Conclusion: This study demonstrates that left ventricular hypertrophy and cardiac abnormalities are frequent findings in children with renal impairment or ESRD. The degree of hypertrophy is often severe, particularly following transplantation. Further studies to clarify the relationship between biochemical disturbances and ventricular abnormalities are suggested.
The Journal of Tehran Heart Center 1 (2006) 33-41
Keywords: Left ventricular mass • Cardiac abnormalities • End stage renal disease • Children and young adult
*Corresponding Author: Ali Akbar Zeinaloo, Department of Pediatric Cardiology, Children’s Hospital Medical Center (Markaz Tebbi Koodakan), Tehran University of Medical Sciences, Tehran, Iran. 1413914711. Tel: +98 21 66921185, 66911029. Fax: +98 21 88792552. E-mail: [email protected].
Introduction
Chronic renal failure (CRF) is a major cause of morbidity and mortality in children. The prevalence and incidence of
chronic renal failure in children has been reported in some countries. For instance, a recent study in Italy reported the

The Journal of Tehran Heart Center
34
mean incidence of CRF as 12.1 cases per million, and the point prevalence as 74.7 per million of the age-related population.1 It has been well documented that left ventricular abnormalities are frequent in children with end-stage renal disease. It has been shown that cardiovascular diseases cause 41% of deaths in less than 15- year-old children with renal failure2,3,4 to our knowledge, little has been written concerning the cardiac abnormalities in RF patients undergoing renal transplantation at a young age across the world. Young patients with end – stage renal disease (ESRD) suffer from an excessive cardiovascular mortality, which is increased 70-fold in patients undergoing dialysis and more than 10-fold after renal transplantation. Chronic renal failure is associated with hypertension, dyslipidemia, hyperphosphatemia, chronic inflammation, uremic toxins, hyperparathyroidism, hypoalbuminemia, hyperhomocysteinemia, severe chronic anemia and acid–base abnormalities which may in time lead to cardiovascular complications. Accelerated coronary arteropathy, manifested as myocardial dysfunction significantly contributes to morbidity and mortality in these children.5,6,7 the precise pathophysiology of cardiac involvement and myocardial dysfunction in CRF are not clear. To date, no studies adequately illuminate the role of any of these factors in the development of myocardial dysfunction in children. However it has been reported that cardiomyopathy in chronic uremia results from pressure and volume overload,7,8 and increased patients’ survival due to the advances in renal replacement therapy have subjected these children to prolonged exposure to multiple cardiovascular risk factors.9 Anemia has been associated with an increase in left ventricular mass (LVM) and with increased LV end diastolic diameter (LVdD) in hemodialysis patients and the correction of anemia by erythropoietin was followed by a decreased in ventricular volume and mass. The effect of rHuEpo on the myocyte cells appear to be related to the capacity of erythropoietin to stimulate Na, K+ -ATPase activity, likely secondary to the activation of tyrosine kinase and protein kinase C.10,11Although the etiologies for altered myocardial structure and performance in renal failure are multiple, there is evidence suggesting that disturbance of calcium, phosphorus and vitamin D metabolism caused by secondary hyperparathyroidism may play important roles in uremic cardiovascular disease.12 Further study demonstrated the high prevalence of LVH in patients with predialysis CRF with concentric hypertrophy as the main pattern of LVH.13,14,15 It should be noted that a report on management of renal failure in children in Europe indicated that 30% of children on continuous ambulatory peritoneal dialysis and 22% of transplant children had left ventricular abnormalities on echocardiographic examination.16,17 In Iran, there is no empirical evidence to evaluate LVH in pediatric chronic renal failure and its relation with factors such as anemia, blood pressure, hyperparathyroidism, which may influence Left Ventricular mass index. The purpose of this cross-sectional study was to investigate left ventricular hypertrophy, its severity and other patterns of cardiac abnormalities in
children and young adults with chronic renal failure (CRF), end stage renal disease (ESRD) on medication, hemodialysis (HD) or post renal transplantation (RTx).
Methods
Patients
Sixty three CRF patients on hemodialysis (HD) (n=45), CRF on medication (n=9) and RTx (n=9) were studied. Patients consisted of 31 females and 32 males with age between 1 and 18-year old, Inclusion criteria for CRF group were existence of CRF with serum creatinine greater than 2 SD above the mean for age persisting for at least six months and a defined cause for renal damage. The HD group had arterio-venous fistula, and were treated with r-HuEPO (EPReX), folic acid and active vitamin D supplements. In the transplant group, 7 patients had received Living related (matched) grafts and two had cadaveric grafts. The median time following transplantation at the time of study was 2.6 years (range: 0.8-5.2 years). Eight of nine patients in the RTx group used prednisone, Two out of 9 consumed Adalat and four were treated with Cyclosporine and Imuran. Existence of LVH and level of hypertension in the study patients were compared with 63 normal subjects including 29 females and 34 Males aged between 2 and 18 years as the control group.
Design
A cross -sectional study was carried out in a Tehran University affiliated hospital over a two- year period. All echocardiogarphic examinations were performed by an expert pediatric cardiologist using a Vingmed 750 ultrasound machine. M-mode measurements were performed according to recommendations of the American Society of Echocardiography (ASE).18 Echocardiograms were recorded on the tape by the investigator and two expert pediatric cardiologists examined the tracings to measure the following parameters: left ventricular end diastolic dimension (LVdD), left ventricular end systolic dimension (LVsD), ventricular posterior wall thickness (PWT), interventricular septal thickness (IVS), aortic root (AR) diameter, left atrial (LA) dimension, fractional shortening (FS), Ejection fraction (EF) and diastolic mitral inflow measuring; peak E wave flow and peak A wave flow and E:A ratio(E/A). Diastolic initial inflow velocities were measured by pulsed wave Doppler at the tips of the mitral valve leaflets, with the opening click of the mitral valve just audible.Valvular abnormalities were noted when present.19 Left ventricular mass was determined by M-mode echocardiography using the following formula: LVM (gm)= 0.8{1.04[(LVdD + PWT+IVS)3 - (LVdD) 3}+0.6(gm).20 Left ventricular size was measured at or just below the tips of the mitral valve leaflets at the largest left ventricular internal dimension. LVdD and PWT measurement were made at end-
Ali Akbar Zeinaloo et al
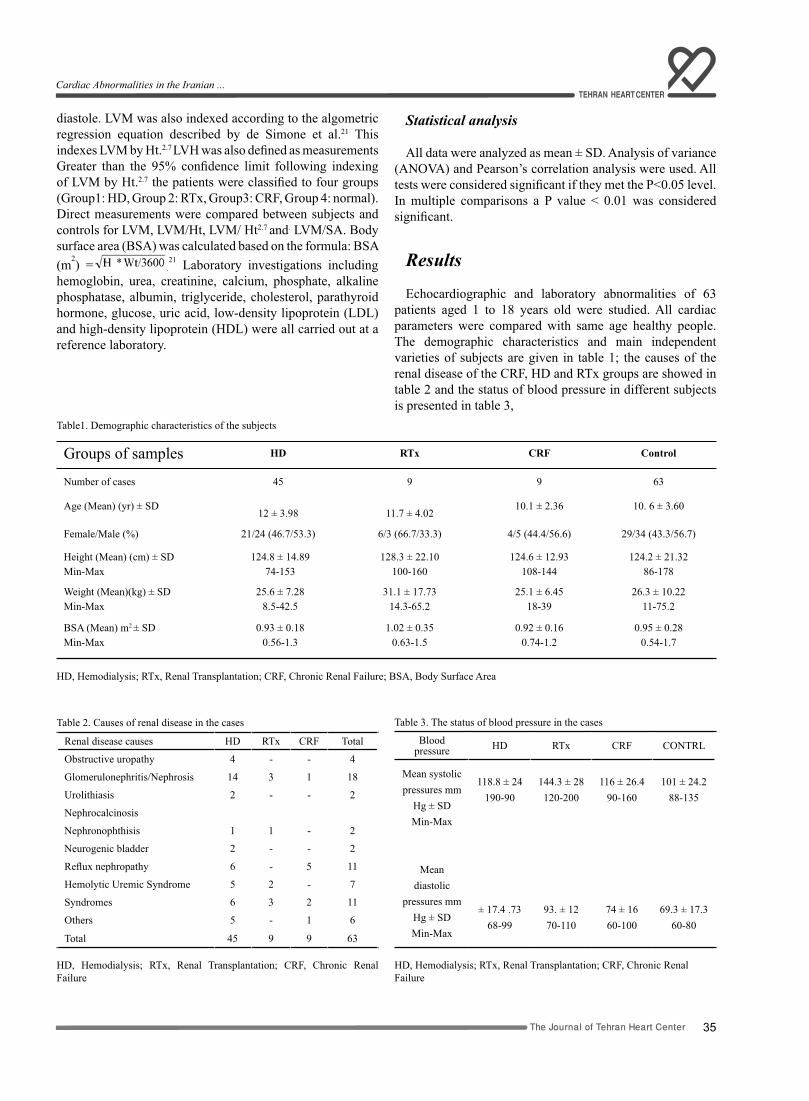
35The Journal of Tehran Heart Center
diastole. LVM was also indexed according to the algometric regression equation described by de Simone et al.21 This indexes LVM by Ht.2.7 LVH was also defined as measurements Greater than the 95% confidence limit following indexing of LVM by Ht.2.7 the patients were classified to four groups (Group1: HD, Group 2: RTx, Group3: CRF, Group 4: normal). Direct measurements were compared between subjects and controls for LVM, LVM/Ht, LVM/ Ht2.7 and. LVM/SA. Body surface area (BSA) was calculated based on the formula: BSA (m2) = .
21 Laboratory investigations including hemoglobin, urea, creatinine, calcium, phosphate, alkaline phosphatase, albumin, triglyceride, cholesterol, parathyroid hormone, glucose, uric acid, low-density lipoprotein (LDL) and high-density lipoprotein (HDL) were all carried out at a reference laboratory.
Statistical analysis
All data were analyzed as mean ± SD. Analysis of variance (ANOVA) and Pearson’s correlation analysis were used. All tests were considered significant if they met the P<0.05 level. In multiple comparisons a P value < 0.01 was considered significant.
Results
Echocardiographic and laboratory abnormalities of 63 patients aged 1 to 18 years old were studied. All cardiac parameters were compared with same age healthy people. The demographic characteristics and main independent varieties of subjects are given in table 1; the causes of the renal disease of the CRF, HD and RTx groups are showed in table 2 and the status of blood pressure in different subjects is presented in table 3,
Table1. Demographic characteristics of the subjects
Groups of samples HD RTx CRF Control
Number of cases 45 9 9 63
Age (Mean) (yr) ± SD 12 ± 3.98 11.7 ± 4.02
10.1 ± 2.36 10. 6 ± 3.60
Female/Male (%) 21/24 (46.7/53.3) 6/3 (66.7/33.3) 4/5 (44.4/56.6) 29/34 (43.3/56.7)
Height (Mean) (cm) ± SD Min-Max
124.8 ± 14.8974-153
128.3 ± 22.10100-160
124.6 ± 12.93108-144
124.2 ± 21.3286-178
Weight (Mean)(kg) ± SD Min-Max
25.6 ± 7.288.5-42.5
31.1 ± 17.7314.3-65.2
25.1 ± 6.4518-39
26.3 ± 10.2211-75.2
BSA (Mean) m2 ± SD Min-Max
0.93 ± 0.180.56-1.3
1.02 ± 0.350.63-1.5
0.92 ± 0.160.74-1.2
0.95 ± 0.280.54-1.7
HD, Hemodialysis; RTx, Renal Transplantation; CRF, Chronic Renal Failure; BSA, Body Surface Area
Table 2. Causes of renal disease in the cases
Renal disease causes HD RTx CRF Total
Obstructive uropathy 4 - - 4
Glomerulonephritis/Nephrosis 14 3 1 18
Urolithiasis 2 - - 2
Nephrocalcinosis
Nephronophthisis 1 1 - 2
Neurogenic bladder 2 - - 2
Reflux nephropathy 6 - 5 11
Hemolytic Uremic Syndrome 5 2 - 7
Syndromes 6 3 2 11
Others 5 - 1 6
Total 45 9 9 63
HD, Hemodialysis; RTx, Renal Transplantation; CRF, Chronic Renal Failure
Table 3. The status of blood pressure in the cases
Bloodpressure HD RTx CRF CONTRL
Mean systolic pressures mm
Hg ± SD Min-Max
Mean diastolic
pressures mmHg ± SD
Min-Max
118.8 ± 24190-90
± 17.4 .7368-99
144.3 ± 28120-200
93. ± 1270-110
116 ± 26.490-160
74 ± 1660-100
101 ± 24.288-135
69.3 ± 17.360-80
HD, Hemodialysis; RTx, Renal Transplantation; CRF, Chronic Renal Failure
Cardiac Abnormalities in the Iranian ...
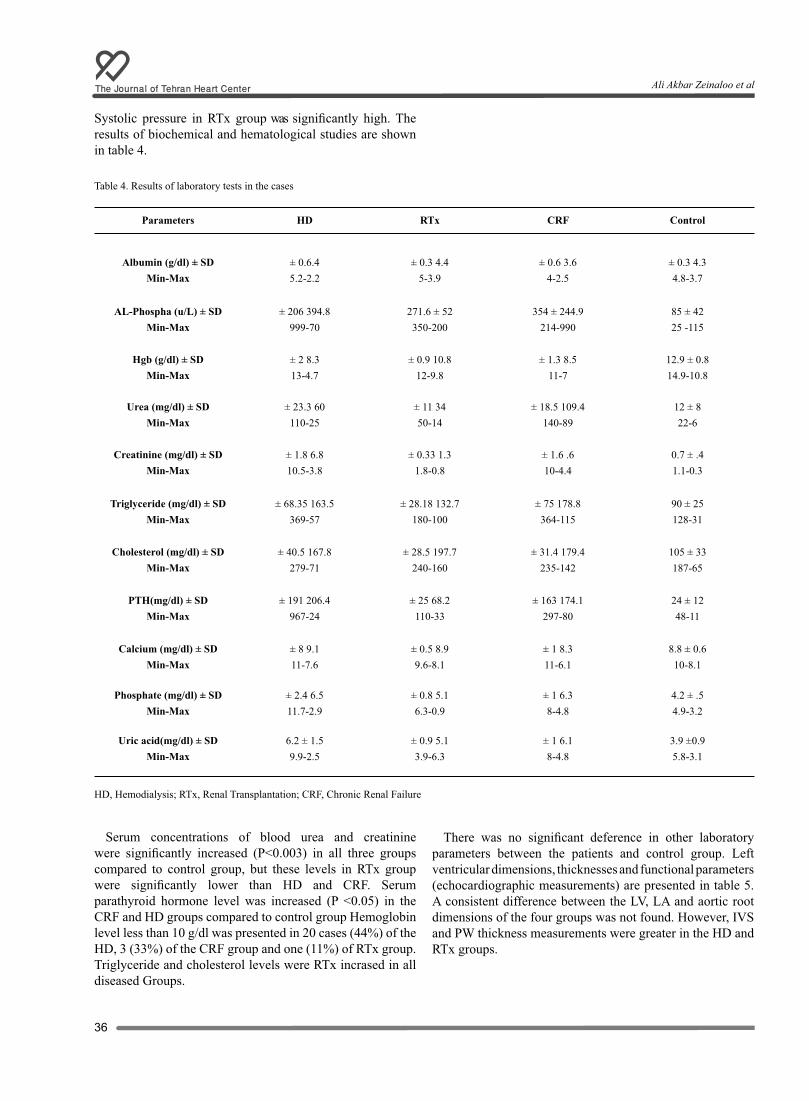
The Journal of Tehran Heart Center
36
Systolic pressure in RTx group was significantly high. The results of biochemical and hematological studies are shown in table 4.
Table 4. Results of laboratory tests in the cases
ControlCRFRTxHDParameters
± 0.3 4.34.8-3.7
± 0.6 3.64-2.5
± 0.3 4.45-3.9
± 0.6.45.2-2.2
Albumin (g/dl) ± SD Min-Max
85 ± 4225 -115
354 ± 244.9214-990
271.6 ± 52350-200
± 206 394.8999-70
AL-Phospha (u/L) ± SD Min-Max
12.9 ± 0.814.9-10.8
± 1.3 8.511-7
± 0.9 10.812-9.8
± 2 8.313-4.7
Hgb (g/dl) ± SD Min-Max
12 ± 822-6
± 18.5 109.4140-89
± 11 3450-14
± 23.3 60110-25
Urea (mg/dl) ± SD Min-Max
0.7 ± .41.1-0.3
± 1.6 .610-4.4
± 0.33 1.31.8-0.8
± 1.8 6.810.5-3.8
Creatinine (mg/dl) ± SD Min-Max
90 ± 25128-31
± 75 178.8364-115
± 28.18 132.7180-100
± 68.35 163.5369-57
Triglyceride (mg/dl) ± SD Min-Max
105 ± 33187-65
± 31.4 179.4235-142
± 28.5 197.7240-160
± 40.5 167.8279-71
Cholesterol (mg/dl) ± SD Min-Max
24 ± 1248-11
± 163 174.1297-80
± 25 68.2110-33
± 191 206.4967-24
PTH(mg/dl) ± SD Min-Max
8.8 ± 0.610-8.1
± 1 8.311-6.1
± 0.5 8.99.6-8.1
± 8 9.111-7.6
Calcium (mg/dl) ± SD Min-Max
4.2 ± .54.9-3.2
± 1 6.38-4.8
± 0.8 5.16.3-0.9
± 2.4 6.511.7-2.9
Phosphate (mg/dl) ± SD Min-Max
3.9 ±0.95.8-3.1
± 1 6.18-4.8
± 0.9 5.13.9-6.3
6.2 ± 1.59.9-2.5
Uric acid(mg/dl) ± SD Min-Max
HD, Hemodialysis; RTx, Renal Transplantation; CRF, Chronic Renal Failure
Serum concentrations of blood urea and creatinine were significantly increased (P<0.003) in all three groups compared to control group, but these levels in RTx group were significantly lower than HD and CRF. Serum parathyroid hormone level was increased (P <0.05) in the CRF and HD groups compared to control group Hemoglobin level less than 10 g/dl was presented in 20 cases (44%) of the HD, 3 (33%) of the CRF group and one (11%) of RTx group. Triglyceride and cholesterol levels were RTx incrased in all diseased Groups.
There was no significant deference in other laboratory parameters between the patients and control group. Left ventricular dimensions, thicknesses and functional parameters (echocardiographic measurements) are presented in table 5. A consistent difference between the LV, LA and aortic root dimensions of the four groups was not found. However, IVS and PW thickness measurements were greater in the HD and RTx groups.
Ali Akbar Zeinaloo et al
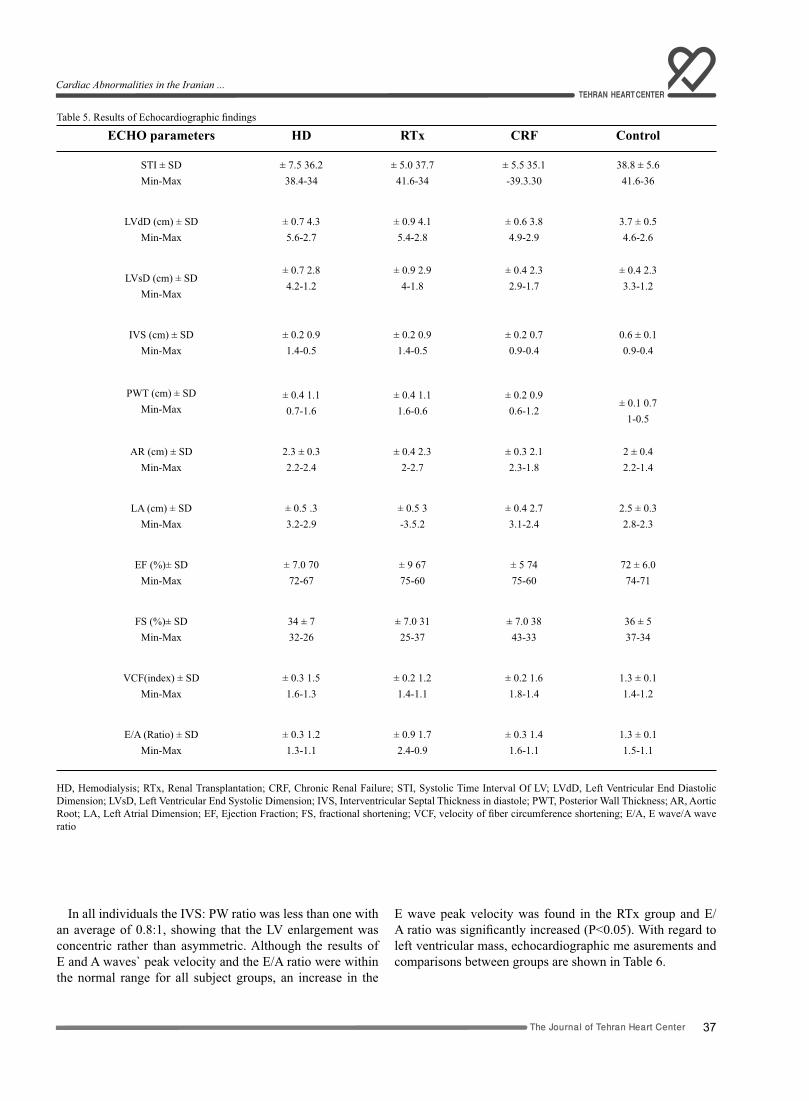
37The Journal of Tehran Heart Center
Table 5. Results of Echocardiographic findings
ControlCRFRTxHD ECHO parameters
38.8 ± 5.641.6-36
± 5.5 35.1-39.3.30
± 5.0 37.741.6-34
± 7.5 36.238.4-34
STI ± SDMin-Max
3.7 ± 0.54.6-2.6
± 0.6 3.84.9-2.9
± 0.9 4.15.4-2.8
± 0.7 4.35.6-2.7
LVdD (cm) ± SDMin-Max
± 0.4 2.33.3-1.2
± 0.4 2.32.9-1.7
± 0.9 2.94-1.8
± 0.7 2.84.2-1.2
LVsD (cm) ± SDMin-Max
0.6 ± 0.10.9-0.4
± 0.2 0.70.9-0.4
± 0.2 0.91.4-0.5
± 0.2 0.91.4-0.5
IVS (cm) ± SDMin-Max
± 0.1 0.71-0.5
± 0.2 0.90.6-1.2
± 0.4 1.11.6-0.6
± 0.4 1.10.7-1.6
PWT (cm) ± SDMin-Max
2 ± 0.42.2-1.4
± 0.3 2.12.3-1.8
± 0.4 2.32-2.7
2.3 ± 0.32.2-2.4
AR (cm) ± SDMin-Max
2.5 ± 0.32.8-2.3
± 0.4 2.73.1-2.4
± 0.5 3-3.5.2
± 0.5 .33.2-2.9
LA (cm) ± SDMin-Max
72 ± 6.074-71
± 5 7475-60
± 9 6775-60
± 7.0 7072-67
EF (%)± SDMin-Max
36 ± 537-34
± 7.0 3843-33
± 7.0 3125-37
34 ± 732-26
FS (%)± SDMin-Max
1.3 ± 0.11.4-1.2
± 0.2 1.61.8-1.4
± 0.2 1.21.4-1.1
± 0.3 1.51.6-1.3
VCF(index) ± SDMin-Max
1.3 ± 0.11.5-1.1
± 0.3 1.41.6-1.1
± 0.9 1.72.4-0.9
± 0.3 1.21.3-1.1
E/A (Ratio) ± SDMin-Max
HD, Hemodialysis; RTx, Renal Transplantation; CRF, Chronic Renal Failure; STI, Systolic Time Interval Of LV; LVdD, Left Ventricular End Diastolic Dimension; LVsD, Left Ventricular End Systolic Dimension; IVS, Interventricular Septal Thickness in diastole; PWT, Posterior Wall Thickness; AR, Aortic Root; LA, Left Atrial Dimension; EF, Ejection Fraction; FS, fractional shortening; VCF, velocity of fiber circumference shortening; E/A, E wave/A wave ratio
In all individuals the IVS: PW ratio was less than one with an average of 0.8:1, showing that the LV enlargement was concentric rather than asymmetric. Although the results of E and A waves` peak velocity and the E/A ratio were within the normal range for all subject groups, an increase in the
E wave peak velocity was found in the RTx group and E/A ratio was significantly increased (P<0.05). With regard to left ventricular mass, echocardiographic me asurements and comparisons between groups are shown in Table 6.
Cardiac Abnormalities in the Iranian ...
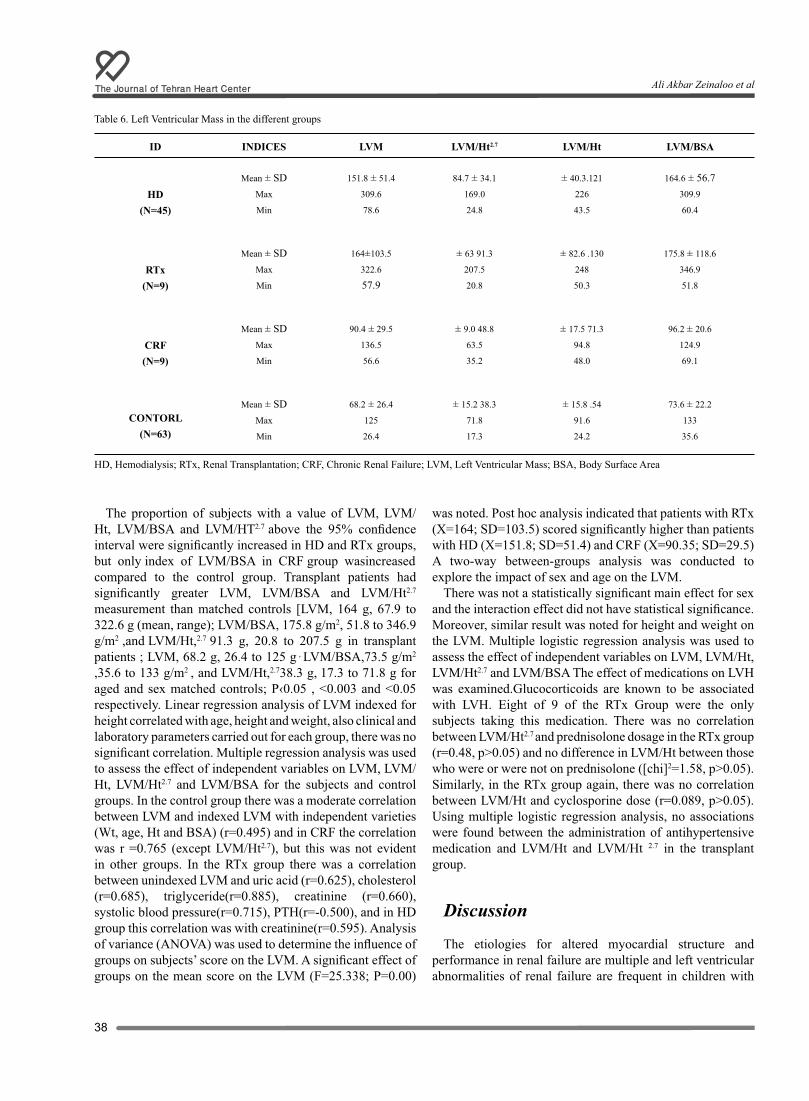
The Journal of Tehran Heart Center
38
Table 6. Left Ventricular Mass in the different groups
LVM/BSALVM/HtLVM/Ht2.7LVMINDICESID
164.6 ± 56.7309.9
60.4
± 40.3.121
226
43.5
84.7 ± 34.1
169.0
24.8
151.8 ± 51.4
309.6
78.6
Mean ± SD Max
MinHD
(N=45)
175.8 ± 118.6
346.9
51.8
± 82.6 .130
248
50.3
± 63 91.3
207.5
20.8
164±103.5
322.6
57.9
Mean ± SD Max
MinRTx
(N=9)
96.2 ± 20.6
124.9
69.1
± 17.5 71.3
94.8
48.0
± 9.0 48.8
63.5
35.2
90.4 ± 29.5
136.5
56.6
Mean ± SD Max
MinCRF(N=9)
73.6 ± 22.2
133
35.6
± 15.8 .54
91.6
24.2
± 15.2 38.3
71.8
17.3
68.2 ± 26.4
125
26.4
Mean ± SD Max
Min
CONTORL(N=63)
HD, Hemodialysis; RTx, Renal Transplantation; CRF, Chronic Renal Failure; LVM, Left Ventricular Mass; BSA, Body Surface Area
The proportion of subjects with a value of LVM, LVM/Ht, LVM/BSA and LVM/HT2.7 above the 95% confidence interval were significantly increased in HD and RTx groups, but only index of LVM/BSA in CRF group wasincreased compared to the control group. Transplant patients had significantly greater LVM, LVM/BSA and LVM/Ht2.7
measurement than matched controls [LVM, 164 g, 67.9 to 322.6 g (mean, range); LVM/BSA, 175.8 g/m2, 51.8 to 346.9 g/m2 ,and LVM/Ht,2.7 91.3 g, 20.8 to 207.5 g in transplant patients ; LVM, 68.2 g, 26.4 to 125 g , LVM/BSA,73.5 g/m2 ,35.6 to 133 g/m2 , and LVM/Ht,2.738.3 g, 17.3 to 71.8 g for aged and sex matched controls; P‹0.05 , <0.003 and <0.05 respectively. Linear regression analysis of LVM indexed for height correlated with age, height and weight, also clinical and laboratory parameters carried out for each group, there was no significant correlation. Multiple regression analysis was used to assess the effect of independent variables on LVM, LVM/Ht, LVM/Ht2.7 and LVM/BSA for the subjects and control groups. In the control group there was a moderate correlation between LVM and indexed LVM with independent varieties (Wt, age, Ht and BSA) (r=0.495) and in CRF the correlation was r =0.765 (except LVM/Ht2.7), but this was not evident in other groups. In the RTx group there was a correlation between unindexed LVM and uric acid (r=0.625), cholesterol (r=0.685), triglyceride(r=0.885), creatinine (r=0.660), systolic blood pressure(r=0.715), PTH(r=-0.500), and in HD group this correlation was with creatinine(r=0.595). Analysis of variance (ANOVA) was used to determine the influence of groups on subjects’ score on the LVM. A significant effect of groups on the mean score on the LVM (F=25.338; P=0.00)
was noted. Post hoc analysis indicated that patients with RTx (X=164; SD=103.5) scored significantly higher than patients with HD (X=151.8; SD=51.4) and CRF (X=90.35; SD=29.5) A two-way between-groups analysis was conducted to explore the impact of sex and age on the LVM.
There was not a statistically significant main effect for sex and the interaction effect did not have statistical significance. Moreover, similar result was noted for height and weight on the LVM. Multiple logistic regression analysis was used to assess the effect of independent variables on LVM, LVM/Ht, LVM/Ht2.7 and LVM/BSA The effect of medications on LVH was examined.Glucocorticoids are known to be associated with LVH. Eight of 9 of the RTx Group were the only subjects taking this medication. There was no correlation between LVM/Ht2.7 and prednisolone dosage in the RTx group (r=0.48, p>0.05) and no difference in LVM/Ht between those who were or were not on prednisolone ([chi]2=1.58, p>0.05). Similarly, in the RTx group again, there was no correlation between LVM/Ht and cyclosporine dose (r=0.089, p>0.05). Using multiple logistic regression analysis, no associations were found between the administration of antihypertensive medication and LVM/Ht and LVM/Ht 2.7 in the transplant group.
Discussion
The etiologies for altered myocardial structure and performance in renal failure are multiple and left ventricular abnormalities of renal failure are frequent in children with
Ali Akbar Zeinaloo et al

39The Journal of Tehran Heart Center
end-stage renal disease. The main finding of this study was that the proportion of subjects with a value of above the 95% confidence interval LVM, LVM/Ht, LVM/BSA and LVM/Ht2.7 were significantly increased in HD and RTx groups ,but only index of LVM/BSA in CRF group was increased compared to the control group. Transplant patients had significantly greater LVM, LVM/BSA and LVM/Ht2.7 measurement than matched controls. In this study the most common causes of CRF were glomerulonephritis (GN) (28.5%), reflux nephropathy (17%) and Hemolytic Uremic Syndrome (HUS) (11%). Radi M, et al22 studied 202 Jordanian children with mean age of 7.5 year with CRF and reported the urological abnormalities and malformations as the etiologic diseases in 42% of the of cases with CRF and hereditary renal disorders in 29.7%, GN in 14.4% and HUS in 4.5%. As shown in table 3, the transplant patients were more likely to be hypertensive than those in other groups. A greater proportion of individuals in this group required anti-hypertensive medication. Hypertension usually causes concentric ventricular hypertrophy which was found in this study. In the RTx group there was a correlation between unindexed LVM and systolic blood pressure(r=0.715), however, this study did not reveal a significant correlation between blood pressure and indexed LVM. Furthermore the AR and LA Dimensions were increased in the RTx group more than other diseased groups. Johnstone et al13 reported that AR dimension was not increased in the RTx group more than other diseased groups. In hypertensive heart disease the AR is usually dilated. Fagard et al23 on reviewing the literature found that correlation coefficients between LVM or LVM/Ht and blood pressure in the normal population were commonly less than 0.5, but this study suggests that hypertension is not the dominant cause of LVH in the under 18 renal transplanted patients. In our study transplant patients had significantly greater LVM, LVM/BSA and LVM/Ht2.7 measurement than matched controls. Daniels et al24 studied 334 young persons between the ages of 6 and 23 and determined the distribution of LVM, LVM corrected for height and LVM corrected for body surface area according to sex, no data were provided for LVM according to age. De Semine et al25 determined 95% confidence intervals for LVM according to sex and height in 444 individuals ranging from four months to 23 years of age. In their studies the indexing of LVM to Ht2.7 reduced the variability in LVM caused by weight differences better than indexing LVM to Ht or SA. It is well recognized in the pediatric age range that age, height and weight are all significantly associated with LVM. Johnstone et al 13 investigated 72 cases of children and young adults(less than 27 years old) with chronic renal failure and ESRD. In their study Left ventricular mass indexed for height was significantly increased in the chronic peritoneal dialysis (CPD) and transplant groups and further analysis using LVM/Ht2.7 confirmed their finding and demonstrated an Increase in LVM in all three subject groups.
In contrast, in our study linear regression analysis of
LVM indexed for height revealed no significant correlation and with multiple regression analysis, in the control group there was a moderately correlation between LVM and indexed LVM with independent varieties and in CRF the correlation was r=0.765 but this was not evident in other groups. Hemodialysis can alter cardiovascular function due to the presence of increased cardiac output associated with an arteriovenous fistula and to the larger changes in intravascular volume the patients experiencing pre- and post-dialysis.26 in dialysis patients, lower hemoglobin levels are associated with increased requenc of LVH, possibly through renin-angiotensin activation. There is a 30% increased risk of developing LV mass for each 0.5 g/dl drop in hemoglobin.27 In ESRD patients, the effect of rHuEpo on LVH may be dependent upon the degree of anemia prior to initiation of rHuEpo therapy.28 Kyle J et al have suggested rHuEpo is safe and effective in reducing LVH and increasing hemoglobin level.11 All the children studied by Morris et al were anemic (Hb < 9.0) and they had shown reduction in left ventricular mass following treatment with recombinant human erythropoietin.2 In our study, a hemoglobin level of less than 10 g/dl was detected in 20 cases (44%) in spite of r- HuEpo (EPReX) and folic acid therapy in all of them. In our opinion, although erythropoietin has been used in all HD patients, there are two questions: the first is whether all the cases have received sufficient doses of rHuEpo and the second one is how the level of hemoglobin was prior to initiation of rHuEpo therapy. Left ventricular hypertrophy was found most frequently after renal transplantation. Renal transplantation resulted in correction of uremia, anemia and secondary hyperparathyroidism. These consequences would be expected to reduce the severity of LVH. The transplant patients were more likely to be hypertensive than those in the other groups. Most of the RTx group was on prednisolone at the time of the study and all had prednisolone in the first nine months following transplantation. Despite lack of a clear relationship between LVM indexed to Ht or Ht2.7, there may have been an additive effect of steroid as reported in infants with lung disease or studies on exercise-induced cardiac hypertrophy.30 Two of the patients in the Transplant group were treated with antihypertensive drugs and none of these patients received an angiotensin converting enzyme (ACE) inhibitor. The incidence of renin-angiotensin-aldosterone mediated hypertension is high in transplant patients, originating from the native kidneys, graft artery stenosis or chronic rejection.31 there is a significant body of evidence in experimental animals that renin-angiotensin can cause myocardial hypertrophy and fibrosis.32 Angiotensin converting enzyme inhibitors would be expected to block this effect. This class of drug is avoided after transplantation because of the possibility of existence of a relative stenosis in the single graft renal artery resulting in impaired renal functionusing induced by the ACE inhibitor. The result of this research is consistent with Johnstone et al13 study. In our study, despite the more frequent finding of LVH in the RTx
Cardiac Abnormalities in the Iranian ...

The Journal of Tehran Heart Center
40
group, an increase in the E wave peak velocity was found and E/A ratio was significantly increased (P<0.05). This may be a reflection of recovery of diastolic function in these patients. It has been shown that renal transplant recipients have less severe diffuse intermyocardiocytic fibrosis than patients with advanced chronic renal failure, suggesting some improvement with correction of uremia.33 the combination of interstitial fibrosis and a reduction in capillary density may cause restrictive changes in myocardial compliance and ischemia. An important finding of this study was the correlation between serum creatinine and LVM in the HD and RTX subjects showed by both linear and multiple regression analyses, but no correlation was detected between urea level and unindexed and indexed LVM in diseased groups. Johnstone et al13
reported correlation between serum creatinine and LVM in the CRF patients. Biochemical study in the cases (as shown in Table 4) revealed high levels of PTH, phosphate, alkaline–phosphatase, cholesterol, triglyceride, LDL, uric acid and hypocalcaemia or normocalcaemia in HD and CRF groups. In RTx group, uric acid, calcium and phosphate were within normal limits and PTH declined to near normal level. In the RTx group there was a correlation between Unindexed LVM and systolic blood pressure(r=0.715), uric acid (r=0.625), cholesterol(r=0.685),triglyceride(r=0.885),creatinine(r=0.0), PTH (r=.500).
Hyperphosphatemia is a predictable consequence of ESRD. There is growing evidence to suggest that abnormalities in serum phosphate, calcium–phosphate product and parathyroid hormone (PTH) levels are resulting in vascular and visceral calcification leading to increased risk of cardiovascular morbidity and mortality in these patients.34 Secondary and tertiary hyperparathyroidism are often found to be independent risk factors for uremic calcification. PTH contributes to cardiovascular complications in many ways. It has a permissive role in arteriolar wall thickening myocardial interstitial fibrosis,35 promoting hyperlipidemia and hypertension.36 both primary and secondary hyperparathyroidism and their marker and elevated alkaline phosphatase level are also Associated with LVH and increased LV mass index. The mechanisms by which hyperparathyroidism could favor LVH are theoretically several and include direct trophic effects on myocardial cells and on interstitial fibroblasts and indirect effects such as an increase in blood pressure via hypercalcemia, anemia, and large and small vessel changes. PTH induces these changes by increasing protein synthesis and induction of creatine kinase and an elevation of the basal levels of cytosolic calcium on cardiac myocyte and induces toxic effects on the heart.12,37 We believe many effects of PTH on myocardiocytes, cardiac small vessel cells, calcium accumulation and metabolism, myocardial hypertrophy and fibrosis could be reversed or prevented by Ca-channel blockade. Many investigators suggest the use of calcium channel blockers early in the course of renal insufficiency since it may be beneficial in reducing cardiovascular accumulation of calcium, thus decreasing the risk of calcifying
of the myocardium, conduction system and small resistance arteries, thereby reducing the risk for myocardial ischemia, heart failure, arrhythmia, and death. Proper management of hyperparathyroidism would reduce the serum level of lipids and their pathologic effects on cardiac and vessel structures. Moreover, efforts should be made to reduce PTH secretion through strict phosphorus and oral supplementation with calcium or vitamin D derivatives into a range that is normal for uremic patients.
Conclusion
This study demonstrates that left ventricular hypertrophy is a frequent finding in children with renal impairment or ESRD. The degree of hypertrophy is often severe, particularly following transplantation. The finding of increased LVM could not be directly associated with hypertension even though hypertension was commonly found after transplantation, suggesting that other factors may be more important. Factors other than hypertension and uremia such as toxic effect of hyperparathyroidism and hyperphosphatemia, persistent profound chronic anemia, hyperlipidemia, are important. Follow-up Studies are required to determine the precise roles of these factors and the significance of increased LVM in premature cardiovascular morbidity and mortality among pediatric patients with chronic renal disease .Further studies to clarify the relationship between biochemical disturbances and heart abnormalities is suggested.
Acknowledgements We are deeply indebted to the attending staff and nursing
staff of nephrology department of Children’s Medical Center Hospital, without whose assistance this study could not have been performed. The authors gratefully thank Mr. Ali O. Zeinanloo and Mr. M. Zeinanloo for technical assistance with the statistical analysis.
References:1. Ardissino M. Epidemiology of chronic Renal Failure in children: Data from the Ital Kid Project. Pediatrics 2003;111:382- 387.2. Brunner FP. Demography of dialysis and transplantation in children in Europe: Report from the European Dialysis and Transplant Association Registry. Nephrol Dial Transplant 1988;3:235-243.3. O’Regan S. Cardiovascular abnormalities in paediatric with ESRD. In: Fine RN, Gruskin AB, eds. End-Stage Renal Disease in Children. Philadelphia: WB Saunders; 1984. p. 359-374.4. Scharer K, Ulmer HE. Cardiovascular complications of renal failure. In: Holiday MA, Barratt TM, Verneir RL, eds. Pediatric Nephrology. 2nd ed.. Baltimore: Williams Wilkins; 1985. p. 887-896.5. Foley RN, parfery PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney
Ali Akbar Zeinaloo et al

41The Journal of Tehran Heart Center
Dis1998;32[suppl 3]:112- 119.6. Locatilli F, Bommer j, London GM. Cardiovascular disease determinants in chronic renal failure: clinical approach and treatment. Nephral Dial Transplan 2001;16:459-468.7. Ulmer H, Heugel E, scharer K. Long-term evaluation of cardiac function using systolic time intervals in children with chronic renal failure. Int Pediatric nephrol 1982;3:79-83.8. London GM, Parfery PS. Cardiac disease in chronic uremia, pathogenesis. Advance Ren Replace Ther 1997;4:194-211.9. Wei Kin G. The Kidney’s contribution to a broken Heart. J nephrology 2000;8:12-15.10. Miroslaw S, shaul G.M. Uremic cardiomyopathy: Role of Parathyroid hormone 1997;52.Suppl62:S.12-S.14.11. Kyle J. Smith, Anthony J. Bleyer, William C.Little, David C.Sane. The cardiovascular effect of erythropoietin. J cardiovascular research 2003;59:538-548.12. Stephen GR and Tilman B.D. Parathyroid hormone, vitamin D, and cardiovascular disease in chronic renal failure. Kidney international 1999;56:383-392.13. Lilian M, Johnstone. Lott ventricular abnormalities in children, adolescents and young adults with renal disease. Kidney international 1996;6:998-1006.14. Jenny A.D, Cathrine MW. Description between echocardiographic measurements of left ventricular mass in a healthy adult population. Clinical Science 1999;97:377-383.15. Loirat C. Report on management of renal failure in children in Europe XXIII. Nephrol Dial Transplant 1994;S1:26-40.16. Mark M. Pediatric end-stage renal disease: Heart as a target. J Pediatrics 2002;141:162-64.17. Vogel Micheal, Staller W, Bublmeyer K. Left ventricular myocardial mass determined by cross-sectional echocardiography in normal newborns, infants and children. Pediat cardial 1991;12:143-149.18. Devereux RB, Reichek N. Echocardiographic determination of left ventricular mass in man: Anatomic validation of the methods, Circulation 1997;55:613-618.19. Devereux RB, Alanso DR, Lutas EM. Echocardiographic assessment of LV hypertrophy: comparison to necropsy finding. Am J cardial 1986;57:450-458.20. Deverex RB, Lutas EM, Casole PN. Standardization of M-Mode echocardiographic LV anatomic measurements. J Am coll cardiol 1984;4:1220-1230.21. Giovanni DE.S. LV mass and body size in normotensive children and adult. JACC 1992;20:1251-1260.22. Stephen RD, Meyer RA, Loggie JMH. Determinants of cardiac involvement in children and adolescent with essential hypertention. Circulation 1990;82:1243-1248.23. Radi MAH. The spectrum of chronic renal failure among Jordanian children. J Nephrology 2002;15:130-135.24. Fagard R, Lijness P, Staessen J, Thijs L, Amery A. Mechanical and other factors relating to left ventricular hypertrophy. Blood Pressure 1994;3:S5-S10.25. Daniels SR, Meyer RA, Liang Y, Bove KE. Echocardiographically determined left ventricular mass index in normal children, adolescents and young adults. J Am Coll Cardiol 1988;12:703-708.26. Soergel M, Machen MA, Azancot-Benisty A, Loirat C. Which hemodynamic factors influence left ventricular mass and dysfunction in pediatric patients on hemodialysis? (abstract) Pediatr Nephrol 1992;6:184. 27. Levin A, Thompson C, Ethler J. Left ventriclar mass index
increase in early renal disease: Impact of decline in hemoglobin. AM J Kidney Dis 1999;34:125-134.28. Sunder-plassmann G, Horl WH. Effect of erythropoietin on cardiovascular Disease. AM J Kidney dis 2001;38:20-25.29. Morris KP, Skinner JR, Hunter S, Coulthard MG. Cardiovascular abnormalities in end stage renal failure: The effect of anemia or uremia. Arch Dis Child 1994;71:119-122.30. Jurowski TT, Chatterton JR, Hickson RC. Glucocorticoid induced cardiac hypertrophy: Additive effects of exercise. J Appl Physiol 1984;527:514-519.31. Van Ypersele de Strihou C, Pochet JM. Hypertension in the transplant patient. In: Cameron S, Davidson AM, Gruenfeld J-P, Kerr D, Ritz E, eds. Oxford Textbook of Clinical Nephrology. Oxford: Oxford Medical Publications; 1992. p. 556-561.32. Schunkert H, Jackson B, Targ SS, Smits JF, Apstein CS, Lovell BH. Distribution and functional significance of cardiac angiotensin converting enzyme in hypertrophied rat hearts. Circulation 1993;87:1328-1339.33. Mall G, Huthen W, Schneider J, Lundin P, Ritz E. Diffuse intermyocardiocytic fibrosis in uraemic patients. Nephrol Dial Transplant 1990;5:39-44.34. Geoffrey AB, Friedrich KP. Re-evaluation of risks associated with hyperphosphataemia and hyperparathyroidism in dialysis patients: recommendation for a change in management. Am J Kin Dis 2000;35:1226-1237.35. Wessels S, Amman K, Toring J, Ritz E. Cardiovascular structural changes in uremia: Implications for cardiovascular function. Semin dial 1999;12:288-292.36. Nishizawa Y, Shoji T, Kawagishi T, Morii H. Atherosclerosis in uremia: possible roles of hyperparathyroidism and intermediate density lipoprotein accumulation. Kidney Int 1997;52(suppl 62):90- 92.37. Schluter KD, Piper HM. Trophic effect of catecholamines and PTH on adult ventricular cardiomyocytes. Am J Physhol 1992;263:1739-1746.
Cardiac Abnormalities in the Iranian ...
42
43The Journal of Tehran Heart Center
Original Article
Comparison of Specifications, Short Term Outcome and Progno-sis of Acute Myocardial Infarction in Opium Dependent Patients
and Nondependents
Gholamreza Davoodi, MD1*, Saeed Sadeghian, MD1, Shahin Akhondzadeh, PhD2, Sooda-beh Darvish, MD1, Mohammad Alidoosti, MD1, Alireza Amirzadegan, MD1
1Tehran Heart Center, Tehran University of Medical Sciences, Tehran, Iran.2Psychiatric Research Center, Roozbeh Psychiatric Hospital, Tehran University of Medical Sciences, Tehran, Iran.
Abstract
Background: The effects of opium dependence on prognosis and short term outcome of patients with acute myocardial infarction (AMI) are not clear yet.
Methods: From March 2004 to August 2004 all male patients admitted with diagnosis of AMI were enrolled. Patients who fulfilled DSM- IV-TR criteria were chosen as opium dependent patients (ODP). Demographic data, risk factors, peak enzyme levels, location of MI, mortality and ejection fraction were collected and analyzed.
We studied the mortality, readmission, functional class, performed revascularizations and coronary angiogram results in a short term follow-up (184 ± 37 days).
Results: A total number of 160 patients were enrolled, of which 45 (28.1%) were opium dependent. In 137 patients 6 months follow up was completed. Duration of admission was higher in O.D.P (11.3 days versus 8.7, P= 0.03) There was no significant difference in age, EF, location of MI, peak enzymes levels, angiographic findings, risk factors (except for cigarette smoking and triglyceride level), in-hospital mortality, need for readmission, 6 months mortality, functional class, and the need for revascularization.
Conclusion: In an unselected cohort of patients admitted with AMI, there was no significant difference in specifications, short term outcome and prognosis of AMI between ODP and nondependents except for duration of hospitalization.
The Journal Of Tehran Heart Center 1 (2006) 43-47
Keywords: Opium dependence • Acute myocardial infarction • Mortality • Angiographic findings
*Corresponding Author: Gholamreza Davoodi, Department of cardiology, Tehran Heart Center, North Kargar Street, Tehran, Iran 14111713138. Tel: 88029600-69. Fax: 88029731. E-mail: [email protected].
Introduction
Opium dependence is a major public health problem in some parts of the world including our country Iran. Opium has always been the most widely abused substance in Iran.
Unlike the pure opioids such as morphine; opium is a complex and variable mixture of substances. Daily amount used both by smoking and by mouth vary from less than 1 gram to

The Journal of Tehran Heart Center
44
more than 30 grams equivalent to 75-3000 mg of morphine. The effects of opium are essentially those of morphine. The major effects of opium are on central and autonomic nervous systems and the bowels, while it has certain influences on other organ systems including respiratory and cardiovascular systems.1 orthostatic hypotension has been reported after opium consumption. Several investigations about the effects of opioid peptides on cardiovascular system have also been performed. They show that hypotension, badycardia, peripheral vasodilatation or sometimes hypertension and tachycardia are among the cardiovascular effects of opioids2 which are produced mainly through their effects on K and Ca channels as well as adenylate cyclase.3 Opioid peptides of myocardial origin have also recently been shown to play a key role in local regulation of the heart. Ischemic preconditioning which reduces the infarct size is abolished in human and rat by blocking opioid peptide receptors with naloxone.4,5 Rats treated with morphine or selective delta agonist before ischemia, produced significant and similar reduction in infarct size when compared with vehicle.6 Induction of hypertrophy may also be associated with increased enkephalin production in the heart.7 There may be also effects on age-associated reduction in ß adrenergic responsiveness.8 A study in Iranian drivers showed significant lower cholesterol level, as well as lower diastolic blood pressure, which in combination with other effects of opium can influence the outcome of cardiovascular disease.9
Considering the above mentioned data there are beliefs among some people (including some medical staff) that opium consumption has protective effects in cardiovascular Disease, while others disagree and yet others believe that opium has harmful effects. There is no sufficient and reliable data regarding the Influences of opium dependence on the patient’s outcome after myocardial infarction which is the most important heart disease. Therefore, we decided to perform this study to evaluate the probable effects. The aim of the present study was to compare the specifications, short term outcome. Complications and prognosis of acute myocardial infarction in opium dependent patients and nondependent patients.
Methods
From March 2004 to August 2004 all male admitted patients with diagnosis of Acute Coronary Syndrome (ACS) in Tehran Heart Center (THC) were registered. Serial Eggs for the first 72 hours were recorded and compared with previous ECG recordings (if available). Creatinin kinase (MB) level, and Troponin I levels were checked 3 times during this first 72 hours. Patients were examined by our cardiologists and a complete history including the specifications and quality of their chest pain was obtained. Meanwhile they were asked about their history of opium dependence criteria. Those who fulfilled the ESC/ACC criteria for acute MI 10 were
identified.Patients who died prior to a possible enzyme rise who
had typical symptoms and ECG changes of AMI were also selected only if there was enough time to ask for the history of opium dependence.
Due to the low prevalence of opium dependence in our female patients (compared to male patients), they were excluded from this study. Patients admitted with AMI who had a history of PCI or CABG were also excluded from the study.
Patients who fulfilled the DSM - IV-TR criteria for opium dependence (by smoking or oral intake) were enrolled as Opium Dependent Patients (ODP).
The management strategy including indications for thrombolytic therapy, and the guidelines for use of Beta-blockers, ACE inhibitors, anti-platelets, Statins and identical for both ODP and non dependents. The following variables were collected: age-history of hypertension – history of cigarette smoking –history of diabetes- lipid profile (cholesterol, triglyceride, HDL and LDL by sampling in the first 24 hours of MI)– peak enzyme level(CK-MB and Troponin I within the first 72 hours)-ejection fraction(by echocardiography)- location of MI ( based on ECG changes as Diagnosed by cardiologists and categorized as inferior, anterior and non ST elevation MI) - duration of hospital admission and in-hospital mortality. The patients were followed for an average of 6 months and in the follow up performed by the cardiologist in charge, the following data were collected: mortality in the follow up period-readmission rate- the performed cases of CABG or PCI- the results of selective coronary angiography(SCA) including the location of involvement (with more than 50% stenosis) and the number of involved vessels(single, two or three vessels)-functional class of patient after 6 months (categorized and classified as asymptomatic or FC=1, mildly to moderately symptomatic (FC=2 and FC=3 ) and severely symptomatic (FC=4) respectively).
Statistical analysis
For continuous variables including age, lipid profile, enzyme levels, ejection fraction and number of involved vessels the values are expressed as mean ±standard deviation and in those marked by * as mean ±standard error mean. For discrete variables, values are expressed as percentages. This was a prospective study in which patients were followed for an average of 6 months. The calculated power of study based on ejection fraction and mortality was more than 85%.For continuous variables T-Test was used to assess the differences between two groups and for qualitative variables, Chi-Square test was used. For small sample sizes we used Fisher’s exact test. In order to determine the effects of confounder variables we used Mantel- Haenszel test.All statistical analyses were performed using SPSS for Windows 11.5.
Gholamreza Davoodi et al
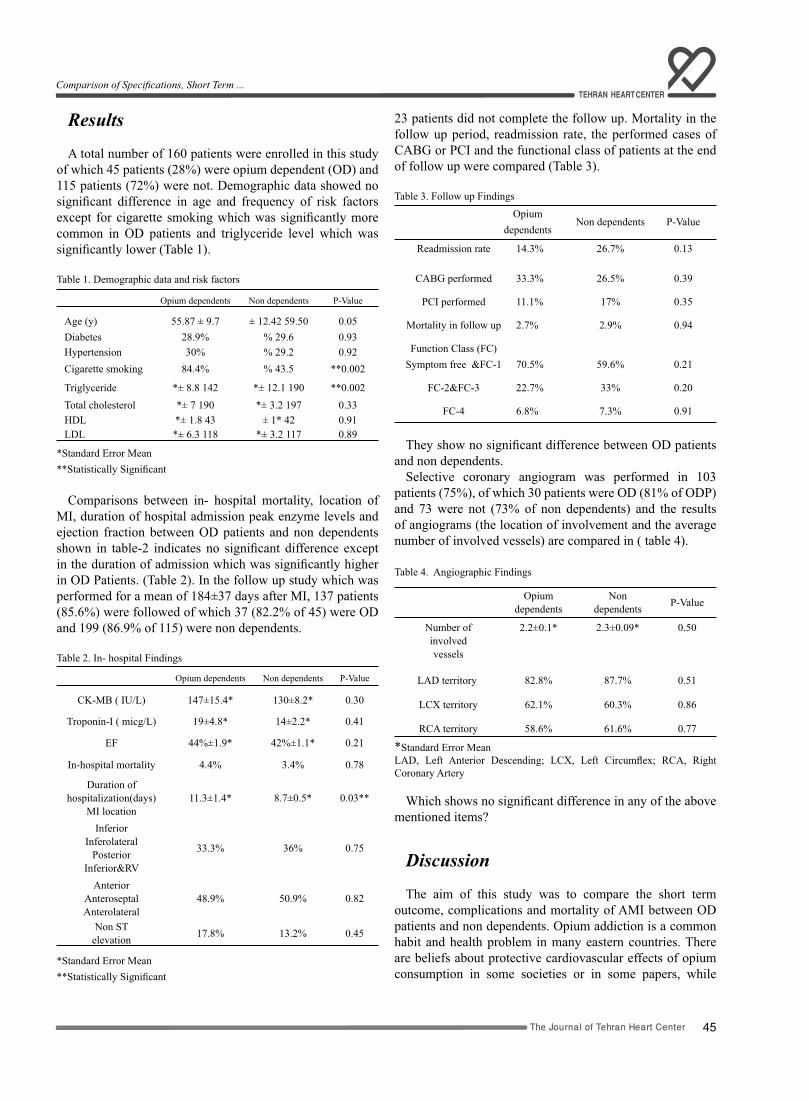
45The Journal of Tehran Heart Center
Comparison of Specifications, Short Term ...
Results A total number of 160 patients were enrolled in this study
of which 45 patients (28%) were opium dependent (OD) and 115 patients (72%) were not. Demographic data showed no significant difference in age and frequency of risk factors except for cigarette smoking which was significantly more common in OD patients and triglyceride level which was significantly lower (Table 1).
Table 1. Demographic data and risk factors
Opium dependents Non dependents P-Value
Age (y) 55.87 ± 9.7 ± 12.42 59.50 0.05Diabetes 28.9% % 29.6 0.93Hypertension 30% % 29.2 0.92Cigarette smoking 84.4% % 43.5 **0.002
Triglyceride *± 8.8 142 *± 12.1 190 **0.002Total cholesterol *± 7 190 *± 3.2 197 0.33HDL *± 1.8 43 ± 1* 42 0.91LDL *± 6.3 118 *± 3.2 117 0.89
*Standard Error Mean**Statistically Significant
Comparisons between in- hospital mortality, location of MI, duration of hospital admission peak enzyme levels and ejection fraction between OD patients and non dependents shown in table-2 indicates no significant difference except in the duration of admission which was significantly higher in OD Patients. (Table 2). In the follow up study which was performed for a mean of 184±37 days after MI, 137 patients (85.6%) were followed of which 37 (82.2% of 45) were OD and 199 (86.9% of 115) were non dependents.
Table 2. In- hospital Findings
Opium dependents Non dependents P-Value
CK-MB ( IU/L) 147±15.4* 130±8.2* 0.30
Troponin-I ( micg/L) 19±4.8* 14±2.2* 0.41
EF 44%±1.9* 42%±1.1* 0.21
In-hospital mortality 4.4% 3.4% 0.78
Duration of hospitalization(days)
MI location11.3±1.4* 8.7±0.5* 0.03**
InferiorInferolateral
PosteriorInferior&RV
33.3% 36% 0.75
AnteriorAnteroseptalAnterolateral
48.9% 50.9% 0.82
Non STelevation 17.8% 13.2% 0.45
*Standard Error Mean**Statistically Significant
23 patients did not complete the follow up. Mortality in the follow up period, readmission rate, the performed cases of CABG or PCI and the functional class of patients at the end of follow up were compared (Table 3).
Table 3. Follow up Findings
Opiumdependents
Non dependents P-Value
Readmission rate 14.3% 26.7% 0.13
CABG performed 33.3% 26.5% 0.39
PCI performed 11.1% 17% 0.35
Mortality in follow up 2.7% 2.9% 0.94
Function Class (FC)Symptom free &FC-1 70.5% 59.6% 0.21
FC-2&FC-3 22.7% 33% 0.20
FC-4 6.8% 7.3% 0.91
They show no significant difference between OD patients and non dependents.
Selective coronary angiogram was performed in 103 patients (75%), of which 30 patients were OD (81% of ODP) and 73 were not (73% of non dependents) and the results of angiograms (the location of involvement and the average number of involved vessels) are compared in ( table 4).
Table 4. Angiographic Findings
Opium dependents
Non dependents P-Value
Number of involved vessels
2.2±0.1* 2.3±0.09* 0.50
LAD territory 82.8% 87.7% 0.51
LCX territory 62.1% 60.3% 0.86
RCA territory 58.6% 61.6% 0.77
*Standard Error MeanLAD, Left Anterior Descending; LCX, Left Circumflex; RCA, Right Coronary Artery
Which shows no significant difference in any of the above mentioned items?
Discussion
The aim of this study was to compare the short term outcome, complications and mortality of AMI between OD patients and non dependents. Opium addiction is a common habit and health problem in many eastern countries. There are beliefs about protective cardiovascular effects of opium consumption in some societies or in some papers, while

The Journal of Tehran Heart Center
46
others mention it as an aggravating factor or even a probable risk factor for CAD. There is no definite answer to many of the questions regarding the cardiovascular effects of opium dependence.
First we had to identify OD patients. Since some of these patients may deny their dependence, there was a probability of under estimation of OD patients.On the other hand relying on urine test for opium would give a large number of false positive results because Most of our patients received narcotics among their drugs. Therefore we decided to directly ask the patients, through their cardiologist, about opium dependence in their first visit. Patients were informed that the data will be used only for this study and would not be mentioned elsewhere. In order to have an estimate of reliability of the answers, we performed urine test for opium in 18 patients who denied OD and did not receive narcotics (selected randomly), and all these tests were negative. This was a strong clue for reliability of patients’ answers to our question about OD.
We used DSM- IV-TR criteria for diagnosis of OD Therefore some patients who used opium infrequently were not enrolled as ODP. We did not separate patients who used opium by oral route or by smoking because of the similar pathologic or physiologic effects. On the other hand there is much cross over between ODP using each of these two methods of opium consumption. By this definition 28% of our patients were OD, which is significantly higher than the prevalence of opium dependence in our country mentioned in official reports. Also some studies in our country have reported dependence rate between 2.1% to 20% in different social groups.11-12
This may have some explanations; first; underestimation of opium dependence rates in the official reports which is probable. Second; opium dependence may be a risk factor or a predisposing factor for CAD or AMI. Finally; the most important factor seems to be the demographic specifications of our study group which is quite different from the whole population of our country and the study is performed only in men. Since this study was designed only for evaluation of effects of opium dependence on patients’ outcome after AMI, we can not give comments regarding these items.
The mortality, complications and outcome of patients with prior history of CABG or PCI who experience AMI is influenced by several other variables; therefore we excluded such patients from our study.
In-hospital mortality in ODP was 4.4 % and in non addicts was 3.4 % which is close to mortality rates reported in Global Registry of Acute Coronary Events (GRACE)13 and the Euro Heart Survey of Acute Coronary Syndrome (EHS-ACS).14
The results of elective coronary angiography (SCA) in our patients were also similar to the above mentioned studies and a newer study comparing Mortality rate inpatients with ST elevation versus non ST elevation acute MI.15 There was no significant difference between ODP and non dependents in angiographic results.
ODP were cigarette smokers in 84.4 % of cases but non dependents mentioned cigarette smoking (CS) in 43.5%. This is not surprising because most of the OD are smokers as well. We analyzed the probable effect of different CS frequency in the two groups and corrected it by Mantel –Hanzel statistics which revealed that the findings were still valid after correction for different levels of CS. fortunately the prevalence of diabetes and hypertension was similar in the two groups so the results of our study were not confounded by these factors. Mortality during 6 months follow up was 2.7% versus 2.9% and the differences were not significant. Our results resembled other large study results. Peak enzyme levels (CK-MB and Troponin I) which are reliable predictors of outcome and size of MI were compared in the two groups and were not significantly different.
Study limitations
As discussed above, although we tried to identify the OAP precisely, there may still be some under estimations. The other limitation of our study is inclusion of male patients only. The prevalence of opium addiction among our female patients was low and since there are demographic differences as well as differences in risk factors and prognosis between men and women after AMI, we excluded female patients in order to get more reliable results with a smaller sample size. The next limitation of this study is silent MI which is supposed to be more frequent in OAP (because of narcotic effects and pain relief). Since this study was performed only on patients admitted with ACS (and the final diagnosis of AMI) we can not give advices on this item either.
Conclusion
In an unselected cohort of patients admitted with AMI; specifications, location, prognosis and complications of AMI were similar in ODP and non dependents (both during their hospitalization, and after 6 months follow-up) except the longer duration of admission in OAP Cigarette smoking was much more frequent in ODP while their Triglyceride level was significantly lower. Angiographic findings were also similar in the two groups. Therefore we did not find any protective effect of opium in ODP after AMI.
Acknowledgements
The authors thank Navid Paydari MD and Dr Fallah for their expert assistance in data management and statistical analysis.
Gholamreza Davoodi et al

47The Journal of Tehran Heart Center
Comparison of Specifications, Short Term ...
References
1. Kalant H. Opium revisited: A brief review of its nature, composition, non-medical use and relative risks. Addiction 1997;92:(3).2. Ventura c, Spurgeon H, Lakatta EG. Kappa and delta opioid receptor stimulation effects cardiac myocyte function and Ca release from an intracellular pool in myocytes and neurons. Circ Res 1992;70:66-81.3. Brink O, Delbridge LM, Rosenfeldt F. Endogenous Cardiac Opioids: Enkefalins in adaptation and protection of the heart. Heart, Lung and Circulation 2003;12:178-187.4. Tomai F, Crea F, Gaspardone A. Effects of naloxone on myocardial ischemic preconditioning in human. J Am Coll Cardiol 1999;33:1863-1869.5. Karck M, Tanaka S, Bolling SF. Myocardial protection by ischemic preconditioning and delta-opioid receptor activation in the isolated working rat heart. J Thorac Cardiovasc Surg 2001;122:986-992.6. Gross ER, Hsu AK, Gross GJ. Opioid-induced cardioprotection occurs via Glycogen Synthase Kinase (beta) inhibition during reperfusion in intact rat heart. Circulation Research 2004;94:960-966.7. Hao JM, Rabkin SW. Increased cardiac ppENK m RNA in cardiac hypertrophy and effects on blood pressure of its peptide products. Am J Physiol 1997;272:2885-2894.8. Xiao R, Capogrossi M, Spurgeon H, Lakatta E. Stimulation of delta opioid receptors in single heart cell blocks beta- adrenergic receptor mediated increase in calcium and contraction. Mol Cell Cardiol 1991;23(suppl III):s83.9. Rajabizade G, Ramezani M, Shakibi M. Prevalence of opium addiction in Iranian drivers. J Med Sci 2004;4:210-213.10. The Joint European Society of Cardiology/America College of Cardiology Committee. for the Redefinition of Myocardial Infarction. Eur Heart J 2000;21:1502-1513.11. Ahmadi J, Arabi H, Mansouri Y. Prevalence of substance abuse among offspring’s of opioid addicts. Addictive Behav 2003;28:591-595.12. Ahmadi J, Hasani M. Prevalence of substance abuse among Iranian high school students. Addictive Behav 2003;28:375-379.13. Step PG, Goldberg RJ, Gore JM, Fox KA, Eagle KA, Flather MD, Sadiq I, Kasper R, Rushton-Mellor SK, Anderson FA. Baseline characteristics, management practices, and in- hospital outcomes of patients hospitalized with acute coronary syndrome in the Global Registry of Acute Coronary Events (GRACE). Am J Cardiol 2002;90:358-363.14. Hasdai D, Behar S, Wallentin L, Danchin N, Gitt AK, Boersma E, Fioretti PM, Simoons ML, Battler A. A prospective survey of the characteristics, treatment and outcomes of patients with acute coronary syndromes in Europe and Mediterranean basin: The Euro Heart Survey of Acute Coronary Syndromes (Euro Heart Survey ACS). Eur Heart J 2002;23:1190-1201.15. Terkelsen C, Lassen JF. Mortality rates in patients with ST-elevation vs non-ST-elevation acute myocardial infarction. European Heart Journal 2005;26:8-26.

48
49The Journal of Tehran Heart Center
Brief Communication
Main Pulmonary Artery Hydatidosis with Seconday Involvement of the Lungs: a Shepherd Boy’s Story1
Ali Mohammad Haji Zeinali, MD*, Kyomars Abbasi, MD, Hakimeh Sadeghian, MD, Navid Paydari, MD
Tehran Heart Center, Tehran University of Medical Sciences, Tehran, Iran.
Abstract
Cardiac hydatid cyst (CHC) is a rare disease that was endemic in some regions especially in sheep-raising areas. The most commonly accepted theory for the routes of heart involvement in hydatid cyst was infestation by the hexacanthus embryo through coronary arteries.
Here, we describe a case with the primitive cardiac hydatid cyst located around the pulmonary valve (PV) and main pul-monary artery (mPA) extended to right and left pulmonary arteries and metastasized to both lungs. Could it be possible for the embryo to adhere PV and mPA directly?
The Journal of Tehran Heart Center 1 (2006) 49-52
Keyword: Hydatid cyst • Pulmonary valve • Main pulmonary artery
Introduction
Cardiac echinococcosis is not a common lesion, the incidence reported ranges between 0.5 to 2 % of all human echinococcosis, and most cases have been reported from endemic regions like the Mediterranean basin, Australia, South America, Africa.1
Although many of the Cardiac echinococcosis cases are asymptomatic, chest pain, palpitation, dyspnea have been described.1,2 Faintness, angina, arrhythmia, pulmonary or systemic emboli were also reported, rarely.1-8
Case report
A 20 years old male patient from central Territory, Iran, was admitted in Tehran Heart Centre due to dyspnea, hemoptysis & syncope, on April 2003.
His coughing had started a year prior to and gradually hemoptysis had developed.
On February 2003, he had a few attacks of syncope & had been visited by a cardiologist, who referred him to our clinic due to detection of mPA cystic lesions in the patient’s two dimensional echocardiography (Figure 1).
*Corresponding Author: Ali Mohamma Haji Zeinali, Department of cardiology Tehran University of Medical Science Tehran Heart Center Karegar Ave, Tehran, Iran 1411713138. Tel: +98-21-88029702. Fax: 88029731. E-mail: [email protected]
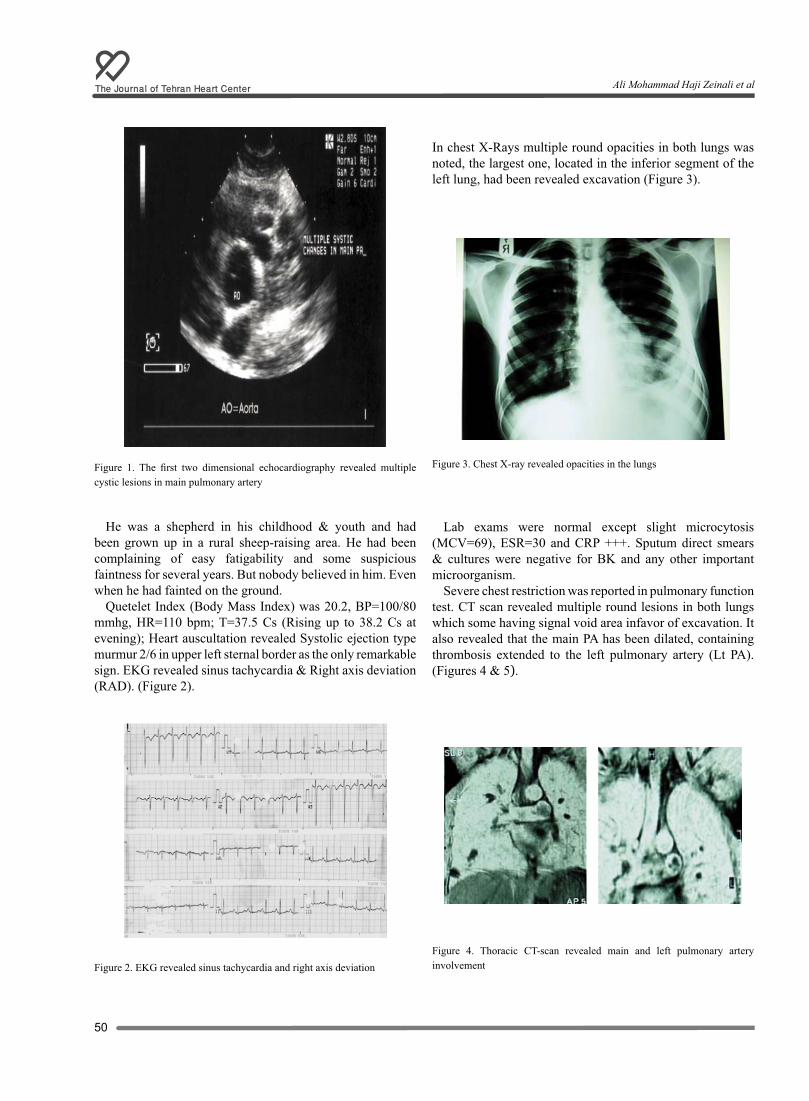
The Journal of Tehran Heart Center
50
Figure 1. The first two dimensional echocardiography revealed multiple cystic lesions in main pulmonary artery
He was a shepherd in his childhood & youth and had been grown up in a rural sheep-raising area. He had been complaining of easy fatigability and some suspicious faintness for several years. But nobody believed in him. Even when he had fainted on the ground.
Quetelet Index (Body Mass Index) was 20.2, BP=100/80 mmhg, HR=110 bpm; T=37.5 Cs (Rising up to 38.2 Cs at evening); Heart auscultation revealed Systolic ejection type murmur 2/6 in upper left sternal border as the only remarkable sign. EKG revealed sinus tachycardia & Right axis deviation (RAD). (Figure 2).
Figure 2. EKG revealed sinus tachycardia and right axis deviation
In chest X-Rays multiple round opacities in both lungs was noted, the largest one, located in the inferior segment of the left lung, had been revealed excavation (Figure 3).
Figure 3. Chest X-ray revealed opacities in the lungs
Lab exams were normal except slight microcytosis (MCV=69), ESR=30 and CRP +++. Sputum direct smears & cultures were negative for BK and any other important microorganism.
Severe chest restriction was reported in pulmonary function test. CT scan revealed multiple round lesions in both lungs which some having signal void area infavor of excavation. It also revealed that the main PA has been dilated, containing thrombosis extended to the left pulmonary artery (Lt PA). (Figures 4 & 5).
Figure 4. Thoracic CT-scan revealed main and left pulmonary artery involvement
Ali Mohammad Haji Zeinali et al
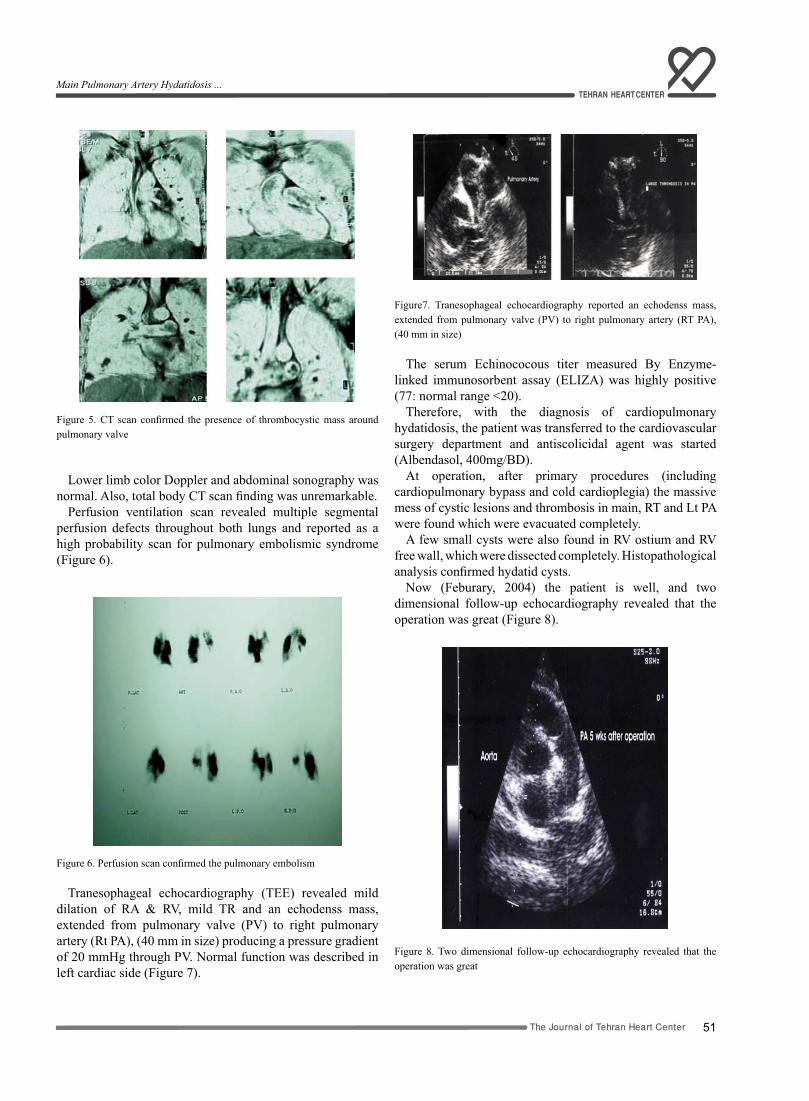
51The Journal of Tehran Heart Center
Figure 5. CT scan confirmed the presence of thrombocystic mass around pulmonary valve
Lower limb color Doppler and abdominal sonography was normal. Also, total body CT scan finding was unremarkable.
Perfusion ventilation scan revealed multiple segmental perfusion defects throughout both lungs and reported as a high probability scan for pulmonary embolismic syndrome (Figure 6).
Figure 6. Perfusion scan confirmed the pulmonary embolism
Tranesophageal echocardiography (TEE) revealed mild dilation of RA & RV, mild TR and an echodenss mass, extended from pulmonary valve (PV) to right pulmonary artery (Rt PA), (40 mm in size) producing a pressure gradient of 20 mmHg through PV. Normal function was described in left cardiac side (Figure 7).
Figure7. Tranesophageal echocardiography reported an echodenss mass, extended from pulmonary valve (PV) to right pulmonary artery (RT PA), (40 mm in size)
The serum Echinococous titer measured By Enzyme-linked immunosorbent assay (ELIZA) was highly positive (77: normal range <20).
Therefore, with the diagnosis of cardiopulmonary hydatidosis, the patient was transferred to the cardiovascular surgery department and antiscolicidal agent was started (Albendasol, 400mg/BD).
At operation, after primary procedures (including cardiopulmonary bypass and cold cardioplegia) the massive mess of cystic lesions and thrombosis in main, RT and Lt PA were found which were evacuated completely.
A few small cysts were also found in RV ostium and RV free wall, which were dissected completely. Histopathological analysis confirmed hydatid cysts.
Now (Feburary, 2004) the patient is well, and two dimensional follow-up echocardiography revealed that the operation was great (Figure 8).
Figure 8. Two dimensional follow-up echocardiography revealed that the operation was great
Main Pulmonary Artery Hydatidosis ...

The Journal of Tehran Heart Center
52
Also serial chest X-ray demonstrates that the pulmonary lesions were diminished in size by now.
In our story, the shepherd boy was right and at last, somebody believed in him before the wolf breaks his heart, completely.
Discussion
Although liver and lungs are the primary sites of hydatid cyst in 85- 90% of cases, it should be insisted that the cyst may involve any other organ in the body (including bone, brain, heart etc).2 Due to the work of Dévé,2,10 it is now commonly accepted that the main route of cardiac infestation with hexacanthus embryo of Echinococcus Granulosa was through the coronary Arteries.
Thus it is primitive and often unique lying in myocardial layers. Sometimes, after rupture of primitive hydatid cysts, the secondary cardiac lesions are developed. These secondary cysts can progress to the myocardium, where they tend to be numerous.11
Cardiac hydatidosis through coronary arteries often involves left ventricular freewall. However, questions persist regarding the predominance of left ventricular (LV) locations of CHCs. Several hypotheses have been offered: (1) dominance of the left coronary artery, (2) the more important myocardial mass in the LV offers better condition of development for parasite; and (3) different pressure regimens. All these factors seem to play roles, but none is likely to be a determining one.2,11 this report revealed a strange pattern of larva dissemination throughout heart & pulmonary arteries that could be known as a reverse dissemination of hydatid cyst (heart to lungs).
As reported, involvement started from a strange location, PV & mPA, extended throughout PV and developed pulmonary artery mass, then ruptured and made a mess of thrombosis and cystic lesions in this case. Then after daughter cysts were embolized through pulmonary arteries, lungs getinvolved. Therefore, there is a point. How could it be possible? & how could it be explained by Deve’s theories? Moreover, could the embryo be transmitted by blood stream to adhere endothelium of the PV and mPA directly and resist against blood flow?
Although in this case we do not have any clues to case histories and could not reject the possibility of PV congenital malformations; we think that, the routes of hytatid cyst dissemination must be re-evaluted.
In this case although two dimensional echocardiography was the golden tool for detection and follow up, severity of dissemination was demonstrated by TEE and CT scan, concomitantly. Each one of them revealed some aspects of patient’s cardiopulmonary involvement. TEE revealed right PA and CT scan reported left PA involvement and neither one could demonstrate right ventricular free wall involvement (maybe due to small size).
Although there is some controversy regarding CHCs`
treatment,12 we believe, in our experience, that the surgical approach concomitant with the medical treatment is the best one.
References1. Ruggero De Paulis. Cardiac Echinococcosis causing coronary artery disease. Ann Thorac Surgery 1999;67:1791-1793.2. Habib Thameur. Cardiopericardial hydatid cysts. World J Surg 2001;25:58-67.3. Adnan Usael. A multivesicular cardiac hydatid cyst with hepatic involvement. European Journal of Cardio-thoracic Surgery 1998;14:335-337.4. Cemil Gürgün, Sanem Nalbantgil, Cahide S. Çınar. Two cases of hydatid cyst with right and left ventricular involvement. International Journal of Cardiology 2001;78:193-195.5. V.M.Beshlyaga. echinococcos cyst of the left ventricle in 10-year-old patient. European Journal of cardio-thoracic Surgery 2002;21:87-91.6. Ahmed Bennis. Cardiac hydatid cyst revealed by complete heart block. Heart Vessels 2000;15:46-48.7. Maroto LC. Hydatid cyst of the interventricular septum in a 3.5-year- old child. Ann Thorac Surg 1998;66:2110-2111.8. Sarkis A.. Kyste hydatique du cœur simulant une ischemie coronarienne. Ann Cardiol Angéil 2001;50:206-210.9. Smith GJ, Irons S, Schelleman A. Hydatid Pulmonary emboli. Australasian Radiology 2001;45:508-511.10. Dévé F. Primitive & Secondire. ĽÉchinococcose Primitive. Paris, Masson Edit, 1949, pp. 21-27.11. Talmudi Kilani T. Kystes hydatique Les kystes hydatique du cœur droit. thés, Med.Marseille, 1978, pp. 36-40.12. Karunajeewa HA. Hydatid disease invading the inferior vena cava: successful combined medical and surgical treatment. ANZ J Surg 2002;72:159-160.
Ali Mohammad Haji Zeinali et al
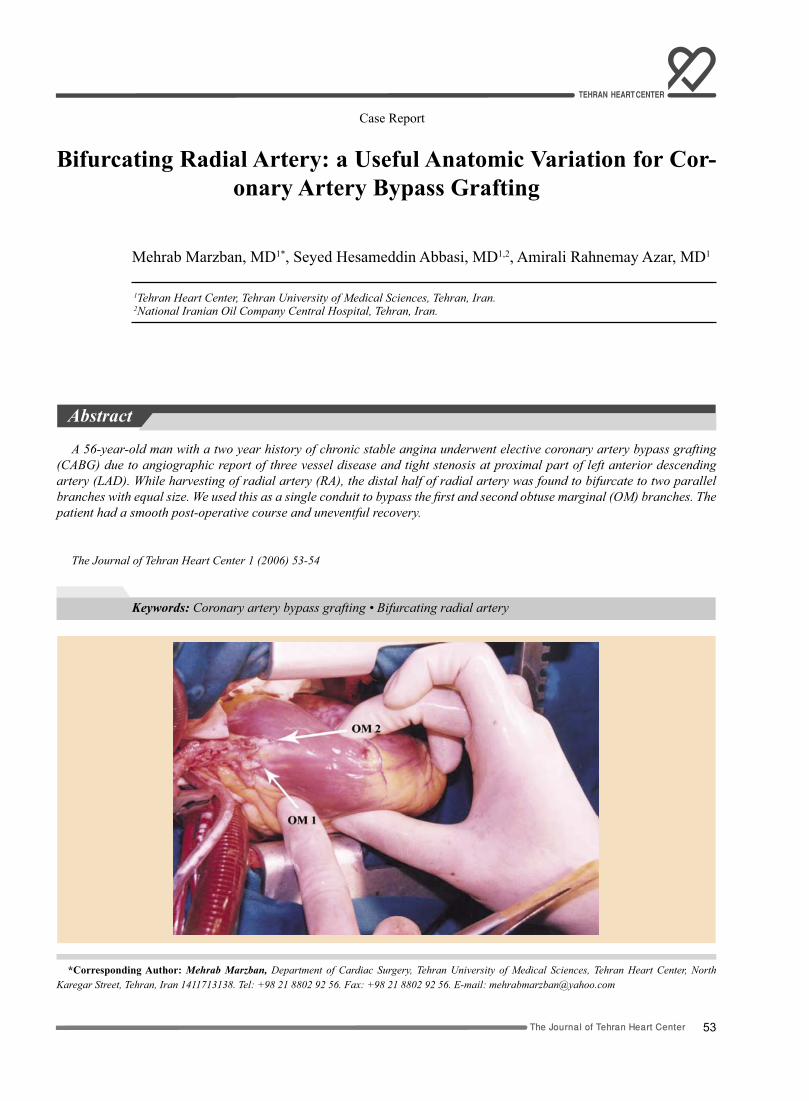
53The Journal of Tehran Heart Center
Case Report
Bifurcating Radial Artery: a Useful Anatomic Variation for Cor-onary Artery Bypass Grafting
Mehrab Marzban, MD1*, Seyed Hesameddin Abbasi, MD1,2, Amirali Rahnemay Azar, MD1
1Tehran Heart Center, Tehran University of Medical Sciences, Tehran, Iran. 2National Iranian Oil Company Central Hospital, Tehran, Iran.
Abstract
A 56-year-old man with a two year history of chronic stable angina underwent elective coronary artery bypass grafting (CABG) due to angiographic report of three vessel disease and tight stenosis at proximal part of left anterior descending artery (LAD). While harvesting of radial artery (RA), the distal half of radial artery was found to bifurcate to two parallel branches with equal size. We used this as a single conduit to bypass the first and second obtuse marginal (OM) branches. The patient had a smooth post-operative course and uneventful recovery.
The Journal of Tehran Heart Center 1 (2006) 53-54
Keywords: Coronary artery bypass grafting • Bifurcating radial artery
*Corresponding Author: Mehrab Marzban, Department of Cardiac Surgery, Tehran University of Medical Sciences, Tehran Heart Center, North Karegar Street, Tehran, Iran 1411713138. Tel: +98 21 8802 92 56. Fax: +98 21 8802 92 56. E-mail: [email protected]

The Journal of Tehran Heart Center
54
Introduction
Compared with saphenous vein graft, use of the internal mammary artery (IMA) as conduit has resulted in superior long-term results.1,2 On the basis of these findings, other arteries have been used in CABG and nowadays many cardiac surgeons favor total arterial revascularization,3,4 and the radial artery is their preferred conduit along with the IMA.5-8
In this article we report the case of a patient with bifurcating radial artery, a rare anatomic variation, and its use as a single conduit for CABG.
Case Report
A 56 years old man with two years history of chronic stable angina which was aggravated recently, underwent coronary arteriography in our institute which was indicative of three vessel disease and left ventricular ejection fraction (LVEF) of 45%. He scheduled for elective CABG. In pre-operative assessment both radial and ulnar artery pulsation was good and Allen’s test was negative. During the operation, we found that the radial artery bifurcated 7-8 cm proximal to styloid process of radius and the two branches ran parallel together and had equal size. We decided to use it as a single conduit and we anastomosed one end to the first branch of obtuse marginal and the second one to OM2, and its proximal end was anastomosed to the ascending aorta (figure 1). Also, LIMA was anastomosed to diagonal and LAD in sequential manner, and a vein graft was used to bypass the right coronary artery. Patient had smooth post-operative course and uneventful recovery. At 3-month follow up Patients was free of angina or hand complication. Theexercise test was negative and showed excellent functional capacity and echocardiography revealed LVEF of 50%.
Discussion
Since its re-introduction by Acar and Colleagues, the radial artery has Generated Considerable interest as an alternative conduit For CABG.9 The RA graft is rapidly gaining popularity because of its diameter length, safety and ease of harvest as well as the encouraging early and mid-to-long term results.5-8 Use of bilateral RA grafts has also been reported in many cases,2 this artery is used as a composite graft, forming part of a Y-graft or T-grafts. In a previous report of bifurcating RA, one of its branches was sacrificed,10 but we imagine this anatomical variation as a natural Y-graft that would excel over the composite Y-graft in terms of less thrombogenicity. Although pre-operative detection of such anomaly is difficult, but when encountering this, we can think of using it as a single conduit.
References
1. Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, Williams GW, Golding LA, Gill CC, Taylor PC, Sheldon WC. Influence of the internal-Mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med 1986;314:1-6.2. Karthik S, Srinivasan AK, Grayson AD, Jackson M, Mediratta NK. Left internal mammary artery to the left anterior descending artery: effect on morbidity and mortality and reasons for nonusage. Ann Thorac Surg 2004;78:142-148.3. Tatoulis J, Buxton BF, Fuller JA, Royse AG. Ann Thorac Surg 1999;68:2093- 2099. 4. Sundt TM 3rd, Barner HB, Camillo CJ, Gay WA Jr. Total arterial revascularization with an internal thoracic artery and radial artery T graft. Ann Thorac Surg 1999;68:399-404.5. Sajja LR, Mannam G, Pantula NR, Sompalli S. Role of radial artery graft in coronary artery bypass grafting. Ann Thorac Surg 2005;79:2180-2188.6. Tatoulis J, Buxton BF, Fuller JA. Patencies of 2127 arterial to coronary conduits over 15 years. Ann Thorac Surg 2004;77:93-101.7. Acar C, Ramsheyi A, Pagny JY, Jebara V, Barrier P, Fabiani JN, Deloche A, Guermonprez JL, A. The radial artery for coronary artery bypasses grafting: clinical and angiographic results at five years. J Thorac Cardiovasc Surg 1998;116:981-989.8. Possati G, Gaudino M, Alessandrini F, Luciani N, Glieca F, Trani C, Cellini C, Canosa C, Di Sciascio G. Midterm clinical and angiographic results of radial Artery grafts used for myocardial revascularization. J Thorac Cardiovasc Surg 1998;116:1015-1021.9. Acar C, Jebara VA, Portoghese M, Beyssen B, Pagny JY, Grare P, Chachques JC, Fabiani JN, Deloche A, Guermonprez JL. Revival of the radial artery for coronary artery bypasses grafting. Ann Thorac Surg 1992;54:652-659.10. Chamberlain MH, Taggart DP. Images in cardiothoracic surgery: Bifurcating radial artery. Ann Thorac Surg 2001;72:1399.
Mehrab Marzban et al
55The Journal of Tehran Heart Center
End DateStart DateCityTitle
28 January 200625 January 2006GarmischpartenkirchenHeart Failure Winter Research Meeting
29 January 200627 January 2006LillehammerAnnual Meeting of the Norwegian Society of Cardiology
28 January 200627 January 2006HelsinkiAnnual Business Meeting of the Finnish Cardiac Society
02 February 200631 January 2006KhobarThe 17 th Scientific Session of the Saudi Heart Association
01 February 200601 February 2006RotterdamThe first symposium on Biomechanics in Cardiovascular Disease : Shear Stress in Vascular Biology
04 February 200602 February 2006Brussels25 th Annual Scientific Meeting of the Belgian Society of Cardiology
10 February 200609 February 2006LeuvenMyocardial Velocity and Deformation Imaging in Clinical Practice
17 February 200615 February 2006VeniceII European Conference on Myocardial Diseases
12 March 200610 March 2006TripoliAnnual Meeting of the Libyan Cardiac Society
14 March 200611 March 2006AtlantaAmerican College of Cardiology Annual Meeting
25 March 200623 March 2006SydneyHeart Foundation Conference 2006
01 April 200630 March 2006Paris1st International Conference on Hypertension , Lipids, Diabetes and Stroke Prevention Interdisciplinary and Multifactorial Approach
International Cardiovascular Meetinges and Congresses Calender2006
The Journal of Tehran Heart Center
56
02 April 200631 March 2006Kuala Lumpur10 th National Heart Association of Malaysia Annual Scientific Meeting 2006
06 April 200602 April 2006Ascona
5thInternational Ascona Workshop on Cardiomyocyte Cell Biology : DIFFERENTIATION , STABILITY OF CYTOARCHITECTURE AND THERAPEUTIC POTENTIAL OF HEART MUSCLE CELLS
05 April 200603 April 2006RotterdamCardiology and Vascular Medicine Update and Perspective
07 April 200606 April 2006Nice4th European Conference on Management of Coronary Heart Disease
21 April 200620 April 2006AmsterdamSpring Congress of the Netherlands society of cardiology
22 April 200620 April 2006Mannheim72nd Annual Meeting of the German Cardiac Society
26 April 200622 April 2006VilamouraXXVII Annual Congress of the Portuguese Society of Cardiology
27 April 200624 April 2006GlasgowAnnual Scientific Conference of the British Cardiac Society
27 April 200625 April 2006LinkopingAnnual Meeting of the Swedish Society of Cardiology
27 April 200626 April 2006Tel Aviv53rdAnnual Conference of the Israel Heart Society
07 May 200603 May 2006CavtatDubrovnik14th Alpe Adria Cardiology Meeting &International Congress of the Croatian Cardiac Society
06 May 200604 May 2006SnekkerstenAnnual Meeting of the Danish Society of Cardiology
06 May 200605 May 2006Bergen6th Annual Spring Meeting of the ESC Working Group on Cardiovascular Nursing : New Frontiers in Cardiac Care
10 May 200607 May 2006Brno ( Fair Trade Exhibito Grounds)
Annual Meeting of the Czech Society of Cardiology
13 May 200610 May 2006dBalatonfureAnnual Meeting of the Hungarian Society of Cardiology
14 May 200611 May 2006St Petersburg55th International Congress of the European Society for Cardiovascular Surgery
13 May 200611 May 2006AthensEuroPRevent 2006
19 May 200616 May 2006ParisEuroPCR 2006
27 May 200624 May 2006Basel41st Annual Meeting of the Association for European Paediatric Cardiology (AEPC)
27 May 200626 May 2006RadenciAnnual Meeting of the Slovenian Society of Cardiology
03 June 200631 May 2006FlorenceAnnual Meeting of the Italian Association of Hospital (ANMCO ) Cardiologists
03 June 200601 June 2006WarsawPulmonary Circulation 2006 European Forum
03June 200601 June 2006Sophia AntipolisNuclear Cardiology in Practice
03 June 200601 June 2006Cannes3rd Global Cardiovascular Clinical Trialists Forum (CVCT Forum)

57The Journal of Tehran Heart Center
10 June 200607 June 2006SalzburgAnnual Meeting of the Austrian Society of Cardiology
09 June 200607 June 2006BaselAnnual Meeting of the Swiss Society of Cardiology
17 June 200614 June 2006Manchester26th Annual Scientific Meeting International Society for Heart Research ( ISHR-ES)
18 June 200615 June 2006CannesMEET 2005- Multidiciplinary European Endovascular Therapy
20 June 200617 June 2006HelsinkiHeart Failure 2006
24 June 200621 June 2006Ohrid3nd Macedonian Congress of Cardiology with international participation
28 June 200624 June 2006LisbonXXII World Congress of the International Union of Angiology
06 September 200602 September 2006BarcelonaWorld Congress of Cardiology 2006; Joint Congress of the European Society of Cardiology and the World Heart Federation
23 September 200620 September 2006ChisinauAnnual Meeting of the Moldavian Society of Cardiology
23 September 200621 September 2006GdanskyteicoS caidraC hsiloP eht fo ssergnoC lanoitanretnI htX
26 September 200623 September 2006Poiana Brasov45th National Congress of the Romanian Society of Cardiology
27 September 200625 September 2006London5th Advanced Symposium on Congenital Heart Disease in the Adult
07 October 200605 October 2006BratislavaAnnual Meeting of the Slovak Society of Cardiology
07 October 200606 October 2006Killarney,Co.KerryAnnual General Meeting of the Irish Cardiac Society
October 200612 10 October 2006MoscowAnnual Congress of the Society of Cardiology of the Russian
Federation
13 October 2006200611 rebotcO HelsinkiAutumn Meeting of the Finnish Cardiac Society
October 200621 18 October 2006MalagaAnnual Meeting of the Spanish Society of Cardiology
200620 rebotcO19 October 2006GrodnoAnnual Meeting of the Belorussian Scientific Society of Cardiologists
October 200624 21 October 2006PragueAcute Cardiac Care 2006
200628rebotcO200625ebotcOBeirut8th Cardiology Meeting of the Lebanese Society of Cardiology
28 October 200626 October 2006ErmeloAutumn Congress of the Netherlands Society of Cardiology
200629 rebotcO26 October 2006SofiaAnnual Meeting of the Bulgarian Society of Cardiology
29 October 200627 October 2006SofiaNational Congress of the Bulgarian Society of Cardiology
04 November200602 November 2006Athens27th Panhellenic Cardiological Congress
November200627 24 November2006AntalyaNational Congress of the Turkish Society of Cardiology
12 June 200709 June 2007HamburgHeart Failure 2007
05 September 200701 September 2007ViennaESC Congress 2007
03 September200830 August2008MunichESC Congress 2008
The Journal of Tehran Heart Center
58
Information for AuthorsScope of the journal
“The Journal of Tehran Heart Center” aims to publish the highest quality material, both clinical and scientific, on all aspects of Cardiovascular Medicine. It includes articles related to research findings, technical evaluations, and reviews. In addition, it provides a forum for the exchange of information on all aspects of Cardiovascular Medicine, including educational issues. “The journal of Tehran Heart Center” is an international, English language, peer reviewed journal concerned with Cardiovascular Medicine. It is an official journal of the Tehran Heart Center and is published quarterly. Papers submitted to this journal which do not adhere to the Instructions for Authors will be returned for appropriate revision to be in line with the Instructions for Authors. They may then be resubmitted. Submission of an article implies that the work described has not been published previously (except in the form of an abstract or as part of a published lecture or academic thesis), that it is not under consideration for publication elsewhere, that its publication is approved by all Authors and tacitly or explicitly by the responsible authorities where the work was carried out, and that, if accepted, it will not be published elsewhere in the same form, in English or in any other language, without the written consent of the publisher.
Article CategoriesThe Journal of Tehran Heart Center" accepts the following categories of articles:Guest Editorial Original Article
Clinical and pre-clinical papers based on either normal subjects or patients and the result of cardiovascular pre-clinical research will be Considered for publication provided they have an obvious clinical relevance.
Brief communication Case reportReview Article
"The Journal of Tehran Heart Center" publishes a limited number of scholarly, comprehensive reviews whose aims are to summarize and critically evaluate research in the field addressed and identify future implications. Reviews should not exceed 5000 words.
Letter to editor Letters to the editor must not exceed 500 words and should focus on a specific article published in "The Journal of Tehran Heart Center" within the preceding 12 weeks. No original data may be included. Authors will receive pre-publication proofs, and the authors of the article cited invited to reply.
Submission of manuscriptsFour double spaced copies on 8 1/2 × 11 in. paper should be sent to: Dr. A. Karimi, Editor in Chief, "The Journal of Tehran Heart Center", Tehran Heart Center, North Kargar Street, Tehran, Iran 1411713138 Photocopies or good reproductions of illustrations are acceptable only on the spare copies. Included also should be a set of the electronic files of the manuscript on floppy – disk or CD-ROM. For preparation of electronic files, see the instructions herein below. Authors can also e-mail their manuscripts to: [email protected].
Review of manuscripts All manuscripts correctly submitted to will first be reviewed by the Editors. Some manuscripts will be returned to authors at this stage if the paper is deemed inappropriate for publication in “The Journal of Tehran Heart Center”, if the paper does not meet submission requirements, or if the paper is not deemed to have a sufficiently high priority. All papers considered suitable by the Editors to progress futher in the review process will undergo appropriate peer review and all papers provisionally accepted for publication will undergo a detailed statistical review.
Preparation of manuscripts All submitted manuscripts must not exceed 5000 words, including References, Figure Legends and Tables. The number of Tables, Figures and References should be appropriate to the manuscript content and should not be excessive.Style and spelling Authors whose first language is not English are requested to have their manuscripts checked carefully before submission. This will help expedite the review process and avoid confusion. Abbreviations of standard SI units of measurement only should be used.Declaration of Helsinki
The Authors should state that their study complies with the Declaration of Helsinki that the locally appointed ethics committee has approved the research protocol and that informed consent has been obtained from the subjects (or their guardians).
59The Journal of Tehran Heart Center
Section of the manuscript Original articles should be divided into the following sections: (1) Title page, (2) Abstract and Keywords, (3) Introduction, (4) Methods, (5) Results, (6) Discussion, (7) Conclusion, (8) Acknowledgements, (9) References, (10) Figure legends, (11) Tables, (12) Figures.
General formatPrepare your manuscript text using a word processing package. Submissions of text in the form of PDF files are not permitted. Manuscripts should be double –spaced, including text, tables, legends and references. Number each page. Please avoid footnotes; use instead, and as sparingly as possible, parenthesis within brackets. Enter text in the style and order of the Journal. Type references in the correct order and style of the journal. Type unjustified, without hyphenation, except for compound words. Type headings in the style of the journal. Use the TAB key once for paragraph indents. Where possible use Times New Roman for the text font and Symbol for the Greek and special characters. Use the word processing formatting features to indicate Bold, Italic, Greek, Maths, Superscript and subscript characters. Clearly identify unusual symbols and Greek letters. Differentiate between the letter o and zero, and the letters I and i and the number 1. Mark the approximate position of each figure and table. Check the final copy of your paper carefully, as any spelling mistakes and errors may be translated into the typeset version.
Title pageThe title page should include the following: (1) the title, (2) the name (s) of authors and their highest degree ( no more than 12 authors are acceptable), (3) the institution (s) where work was performed, (4) institution, and location of all authors, (5) the address, telephone number, fax number and e-mail address of the corresponding author.
AbstractAll abstracts may not contain more than 250 words and should also be submitted as a separate file. The abstract should be formatted with the following heading: (1) Background, (2) Methods, (3) Results, (4) Conclusion. A maximum of six Keywords may be submitted.
FiguresThe review process will not begin until all figures are received. Figures should be limited to the number necessary for clarity and must not duplicate data given in tables or in the text. They must be suitable for high quality reproduction and should be submitted in the desired final printed size so that reduction can be avoided. Figures should be no larger than 125 (height) × 180 (width) mm (5× 7 inches) and should be submitted in a separate file from that of the manuscript.
Electronic submission of figures Figures should be saved in TIFF format at a resolution of at least 300 pixels per inch at the final printed size for colour figures and photographs, and 1200 pixels per inch for black and white line drawings. Although some other formats can be translated into TIFF format by the publisher, the conversion may alter the tones, resolution and contrast of the image. Digital colour art should be submitted in CMYK rather than RGB format, as the printing process requires colours to be separated into CMYK and this conversion can alter the intensity and brightness of colours. Therefore authors should be satisfied with the colours in CMYK (both on screen and when printed) before submission. Please also keep in mind that colours can appear differently on different screens and printers. Failure to follow these guides could result in complications and delays.. Photographs: Photographs should be of sufficiently high quality with respect to detail, contrast and fineness of grain to withstand the inevitable loss of contrast and detail inherent in the printing process. Please indicate the magnification by a rule on the photograph. Colour figures: There is a special charge for the inclusion of colour figures.. Figure legends: These should be on a separate, numbered manuscript sheet grouped under the heading “Legends” on a separate sheet of the manuscript after the References. Define all symbols and abbreviations used in the figure. All abbreviations and should be redefined in the legend..
TablesTables should be typed with double spacing, but minimizing redundant space and each should be placed on a separate sheet. Tables should be submitted, wherever possible, in portraits, as opposed to landscape, layout. Each Table should be numbered in sequence using Arabic numerals. Tables should also have a title above and an explanatory footnote below. All abbreviations and should be redefined in the Footnote.
AcknowledgementsAll sources of funding and support, and substantive contributions of individuals, should be noted in the Acknowledgements, positioned before the list of references.
Reference formatNumber references sequentially and use Arabic number in superscript to cite the reference in the text. All references should be compiled at the end of the article in the Vancouver style. Complete information should be given for each reference including the title of the article, abbreviated journal title and page numbers. All authors should be listed. Personal communications; manuscripts in preparation and other unpublished data should not be cited in the reference list but may be mentioned in parentheses in the text. Authors should get permission from the source to cite unpublished data.Titles of journals should be abbreviated in accordance with Index Medicus (see list printed annually in the January issue of Index Medicus). If a journal is not listed in Index Medicus then its name should be written out in full.Article citation example:Journal citation example: 1. Schroeder S, Baumbach A, Mahrholdt H. The impact of untreated coronary dissections on the acute and long-term outcome after intravascular ultrasound guided PTCA. Eur Heart J 2000;21:137-145.

The Journal of Tehran Heart Center
60
Chapter citation example: 2. Nichols WW, O’Rourke MF. Aging, high blood pressure and disease in humans. In: Arnold E, ed. McDonald’s Blood Flow in Arteries: Theoretical, Experimental and Clinical Principles. 3rd ed. London/Melbourne/Auckland: Lea and Febiger; 1990. p. 398-420.Webpage citation example: 3. Panteghini M. Recommendations on use of biochemical markers in acute coronary syndrome: IFCC proposals. eJIFCC 14. http://www.ifcc.org/ejifcc/vol14no2/1402062003014n.htm (28 May 2004). Where the date in parenthesis refers to the access date.
Statistics All manuscripts selected for publication will be reviewed for the appropriateness and accuracy of the statistical methods used and the interpretation of statistical results. All papers submitted should provide in their Methods section a subsection detailing the statistical methods, including the specific method used to summarize the data, the methods used to test their hypothesis testing and (if any) the level of significance used for hypothesis testing..
Conflict of interest At submission, the editors require authors to disclose any financial association that might pose a conflict of interest in connection with the submitted article. All sources of funding for the work should be acknowledged in a footnote on the title page and in the Acknowledgements within the manuscript, as should all the institutional affiliations of the authors (including corporate appointments). Other kinds of associations, such as consultancies, stock ownership or other equity interest or patent – licensing arrangements should be disclosed to the editors in the cover letter at the time of the of submission. If no conflict of interest exists, please state this in the cover letter.
ProofsPage proofs will be sent to the corresponding author. Please provide an e-mail address to enable page proofs to be sent as PDF files via e-mail. These should be checked thoroughly for any possible changes or typographic errors. Significant alterations instigated at this stage by the author will be charged to the author. It is the intention of the Editor to review, correct and publish your article as quickly as possible. To achieve this it is important that all of your corrections are returned to us in one all – inclusive mail or fax. Subsequent additional corrections will not be possible, so please ensure that your first communication is complete.

61The Journal of Tehran Heart Center
The Journal of Tehran Heart Center
62
Surname:First Name:Hospital or Organization: Date of subscription: Full mail address:
P.O.BOX: Tell: Fax:E-mail: The annual subscription and postage rate: 100/000 Rials for Iran and $ 100 US including postage for other countries.
Please liquidate the total amount of subscription and postal charges into: Bank: Refah Branch Code: 1232 Account: Tehran Heart Center Account Number: 200001.28and send the original bank slip along with duly completed form of subscription to the following address:
Tehran Heart Center,North Kargar Street,Tehran, Iran 1411713138Tel: +98 21 88029702FAX: +98 21 88029702E-mail: [email protected]
New Subscription: Continuation of Subscription:
Subscription Form
The Journal of Tehran Heart Center
Surname:First Name:Hospital or Organization: Date of subscription: Full mail address:
P.O.BOX: Tell: Fax:E-mail: The annual subscription and postage rate: 100/000 Rials for Iran and $ 100 US including postage for other countries.
Please liquidate the total amount of subscription and postal charges into: Bank: Refah Branch Code: 1232 Account: Tehran Heart Center Account Number: 200001.28and send the original bank slip along with duly completed form of subscription to the following address:
Tehran Heart Center,North Kargar Street,Tehran, Iran 1411713138Tel: +98 21 88029702FAX: +98 21 88029702E-mail: [email protected]
New Subscription: Continuation of Subscription:
Subscription Form
The Journal of Tehran Heart Center