blood-injury phobia
TRANSCRIPT

Pergamon Clinical Psychology Review, Vol. 14, No. 5, pp. 443-461, 1994
Copyright 0 1994 Elsevier Science Ltd Printed in the USA. All rights reserved
0272-7358194 $6.00 + .OO
0272-7358(94)00022-O
BLOOD-INJURY PHOBIA
Andrew C. Page
Clinical Research Unit for Anxiety Disorders, St. Vincent’s Hospital
ABSTRACT. Blood-injury phobia is an atypical speczfic phobia. Sufferers exhibit irrational or
excessive anxiety and a desire to avoid specific feared objects and situations, to the point of avoiding
potentially life-saving medical procedures. In addition, blood-injury phobics are liable to faint in the
presence of blood or injury. Such fainting complicates the clinical picture, the etiological models, and the
forms of treatment o@ed. This article reviews evidence for the etiology of blood-injtry phobia and
concludes that the disorder is the product of two separate but related etiologies: one underlying fealful
avoidance, the other fainting. The vulnerability to blood-injury fears and avoidance may involve elevated
trait anxiety and the vulnerability to faint in the presence of blood and injury may involve elevated disgust
sensitivity. Available treatments are discussed in light of the separation offear andfainting.
Blood-injury phobia is similar to other specific phobias in many ways (American Psy- chiatric Association, 1987, World Health Organisation, 1991). Sufferers report fear on exposure to a specific class of stimuli that include blood, injury, injections, etc.’ They also avoid or endure such exposure with distress, identifying the associated fear and avoidance as excessive or irrational. In contrast to the case in other specific phobias, 4 out of 5 people with blood-injury phobia faint in phobic situations (Ost, Lindahl, Sterner, & Jerremalm, 1984; Thyer, Himle, & Curtis, 1985). C onnolly, Hallam, and Marks (1976) drew attention to the specificity of fainting when they found that only 0.02% of mixed phobics reported fainting in the presence of feared stimuli, whereas 100% of their sample of blood-injury phobics reported such fainting. This “emotional fainting,” or vasovagal
syncope (Callahan, Edelman, Smith, & Smith, 1963; Graham, Kabler, & Lunsford, 1961; Lewis, 1932; Poles & Boycott, 1942; Ruetz, Johnson, Callahan, Meade, & Smith, 1967), occurs when blood pressure drops dramatically following an initial increase, apparently as blood is directed toward skeletal musculature. The redirection of blood is witnessed by increasing facial pallor. Breathing rate may temporarily increase and become shallow.
Correspondence should be addressed to Andrew Page Ph.D., Department of Psychology, Univer- sity of Western Australia, Nedlands WA 6009 Australia.
‘The term blood-injury phobia is used to describe the pathological response not only to blood and injury but also to conceptually related stimuli (e.g., injections, mutilation, medical paraphernalia, etc.) although it is acknowledged that further subtyping may prove necessary.
443

444 A. C. Page
Individuals report feelings of heat, dizziness, confusion, nausea, epigastric discomfort, yawning, and may lose consciousness. Respiration becomes slow and deep, and sweating is almost inevitable. Recovery is slow, leaving persons weak, inert, and pale with heart rate and blood pressure remaining suppressed.
The stimuli that individuals with blood-injury phobia avoid or find distressing at first inspection suggest commonality, but more detailed analysis reveals some distinctions. Listings of feared situations include a group of items that involve blood, mutilation, injury, injections, medical paraphernalia, medical or dental environments, and illness. It is possible to separate these related items into two groupings. Kleinknecht (1988) exam- ined the correlations between the Mutilation Questionnaire (MQ Klorman, Hastings, Weerts, Melamed, & Lang, 1974) and fainting in a student sample, while partialling out the variance attributable to fear. They identified that the MQcomprised two independent components. One component relating to general blood and injury fears and another to fainting in the presence of blood and injury. Empirical investigations of the meanings attributed to blood and injury concord with the components identified in the MQ. Sledge (1978) found an association between the perception of two types of threat and fainting in a medical context. One cluster of perceived threats involved the anticipation of painful consequences (e.g., a patient believed that his stitches were to be removed too early and the wound would re-open). A second cluster of threats involved a resignation to the consequences of fainting (e.g., embarrassment or humiliation).
In summary, two different response patterns characterize blood-injury phobia. The first set of changes is the classic fight or flight response (Cannon, 1927) which is common to all phobic disorders (Andrews, Crino, Hunt, Lampe, & Page, in press; Barlow, 1988; Gray, 1987). Persons report feeling afraid and become physically aroused in preparation for flight or fight. The second pattern of responding involves the emotional fainting just described (Connolly et al., 1976) This distinction suggests a separation between two processes leading ultimately to fearful avoidance and/or fainting that etiological models need to address.
EPlDEMiOLOCY
An accurate estimate of the prevalence of blood-injury phobia is not possible because no study has adequately assessed the frequency of blood and injury fainting in addition to fear. Nevertheless, it is possible to estimate that the frequency of fainting in the presence of blood and injury is between 5 ‘$% and 15 %. By way of explanation, between 13 % and 19% of late adolescents report fainting in the presence of blood or injury (Kleinknecht, 1987; 1988; Kleinknecht & Lenz, 1989). To the extent that these figures accurately reflect the lifetime prevalence of blood-injury fainting in a population sample, they indicate an upper boundary of prevalence. An indication of the lower limit of fainting in the presence of blood and injury can be drawn from the rate of fainting in blood donation units, that is around 5% (Callahan et al., 1963; Poles & Boycott, 1942; Subcommittee of the Blood Transfusion Research Committee, 1944). Because people who anticipate fainting in med- ical situations may avoid these contexts, and because observed fainting rates assess point prevalence rather than lifetime prevalence, these figures represent a lower boundary of the occurrence of blood-injury fainting.
Although between 5 % and 15 % of the population have fainted in the presence of blood and injury, not all of these individuals will have blood-injury phobia. However, because the majority of blood-injury phobics have fainted (Ost et al., 1984), those with the phobia will form a subgroup of those who faint. Therefore, the actual rate of blood-injury phobia should be lower than the rate of blood-injury fainting. Consistent with this expectation,

Blood-Injury Phobia 445
Agras, Sylvester, and Oliveau (1969) found that the population prevalence of blood- injury phobia was 3.1% , with a slightly higher rate for females (2.2 % of males and 3.9 % of females). Costello (1982) reported a similar rate of 4.5 % in an all female sample. These two studies only asked about blood-injury fears. Therefore, it remains to discover the prevalence of blood-injury phobia that involves fainting as well as fear.
These global population rates do not give any information about changes in prevalence at different ages. Developmental studies point to a general trend for blood and injury fears to rise in early childhood and subsequently decrease with age. Mild blood-injury fears have been found in 44% of 6- to 8-year-olds but only in 27% of 9- to 12-year-olds (Lapouse & Monk, 1959). Estimates of the prevalence of blood-injury phobia show a similar pattern, rising to 13% by age 10 and decreasing progressively until age 60, with a mean age of onset at age seven (Agras et al., 1969; Ost et al., 1984).
What is not clear from these statistics is the frequency and consequences of avoidance among individuals with blood-injury phobia. The only available study examined univer- sity students and found that of those who reported fainting, 25% avoided consultations with doctors (Kleinknecht & Lenz, 1989). Although the study involved a detailed assess- ment of the presentation and etiology of blood-injury fears and fainting, generalization of these findings is limited. The sample is not necessarily representative of the general population and there was no attempt to investigate whether avoiding subjects met diag- nostic criteria for a phobia. Furthermore, these was no examination of the impact of avoidance on a subject’s health. Therefore, it remains to assess the health consequences of avoidance among blood-injury phobics.
Research into the health consequences may seem unwarranted at first. Whereas avoid- ance of blood, injections, and injury may limit a person’s life, it is not dangerous. However, phobic avoidance becomes serious when it precludes an individual securing appropriate medical care. When a potentially life-threatening condition co-exists with blood-injury phobia, it is irrelevant how effective available treatments for the disease are; the irrational avoidance may circumvent the entire treatment process. For instance, of the last four consecutive blood-injury phobia referrals to the Anxiety Disorders Unit, one patient avoided investigations for a potentially carcinomic lump in the breast, another for removal of a mole consistent with malignant melanoma, another for extraction of im- pacted wisdom teeth, and an HIV positive individual refused to give blood samples to investigate an unexpectedly rapid progression towards AIDS. In each case, treatment was clear and could prevent disease progression. To reduce the incidence of such complica- tions it is necessary to identify the etiology of the disorder and ultimately to develop and refine effective treatments.
ETIOLOGY
The Etiology of Fear
The inclusion of “blood-injury phobia” within the category of specific or simple phobias in classificatory systems reflects a perception that fear has a primary role in the disorder. Consistent with this assumption, blood-injury phobia appears to share a common etiology with other phobias. Kendler, Neale, Kessler, Heath, and Eaves (1992) have argued from data comparing monozygotic with dizygotic twins that the genetic factor common to all phobias (agoraphobia, social phobia, and specific phobias), strongly predisposes a person to specific phobias. The recognition of an inherited vulnerability common to all phobias is consistent with the notion that elevated trait anxiety predisposes one to anxiety disorders (Andrews, Stewart, Morris-Yates, Holt, & Henderson, 1990). Andrews and his group
446 A. C. Page
examined Eysenck’s proposition that an inherited predisposition toward excessive arousal under stress (or elevated trait anxiety) predisposes a person to anxiety disorders. They found that trait anxiety (measured by the neuroticism subscale of the Eysenck Personality Questionnaire; Eysenck & Eysenck, 1975) explained a large proportion of the variance in stable factors predisposing a person to anxiety disorders (Andrews, 1991; Andrews et al., 1990). Although they did not examine blood-injury phobics separately, Schmidt (1975) similarly found that blood-injury phobics have higher trait anxiety scores than normal controls.
Acknowledging findings such as these, most etiological theories of anxiety disorders acknowledge the important role of elevated trait anxiety. Taking one influential account, Barlow (1988) argued that anxiety disorders arise from an inherited proneness to high anxiety. Certain environmental events then serve to activate and release the inherited tendency toward excessive affective reactivity. Trait anxiety thereby provides a back- ground of affective arousal that permits a more rapid activation of the fight or flight response.
With respect to specific activating events, conditioning is one way that stimuli become able to elicit anxiety (Rachman, 1991). Accordingly, painful experiences can condition fear to blood-injury stimuli. Investigators typically classify around 60% of self-reported onsets of blood-injury phobia as beginning with conditioning experiences (Ost, 1991; Ost, 1992; Ost & Hugdahl, 1985; Thyer et al., 1985). However, examinations of available case-by-case verbal summaries call into question the conclusion that conditioning episodes are as prevalent as reported (see Mattick, Page, & Lampe, in press). For example, Thyer et al. (1985) identified a conditioning episode when a “patient received an injection at age 13 and fainted” (p. 455), and in another person when ‘at age six she heard her elementary school teacher give a talk on the circulatory system. This frightened the patient to the point of syncope” (Thyer et al., 1985; p. 455). In these examples there are no apparent unconditioned stimuli. Injections do not unconditionally lead to fainting and if these episodes represent the onset of the blood-injury phobia, why did the children faint in the first instance? It is more likely that the fainting itself is a manifestation of a pre-existing problem. Excluding cases in which aversive experiences may reflect a pre-existing prob- lem with blood and injury decreases the rate of conditioning episodes from 60% to 45 % .
This is not to say that fainting is not aversive. Rather, perhaps people at risk of developing blood-injury phobia are more likely to faint in the presence of blood and injury. Having fainted, perhaps causing injury or embarrassment, the person may come to fear stimuli that appear to trigger these aversive events. A cycle characterized by “fear of fainting” may be initiated, that then exacerbates the problem in much the same way that “fear of fear” appears to exacerbate panic attacks (Clark, 1986, 1988). Support for this proposition exists in data reported by Kleinknecht and Lenz (1989) regarding the development of fear following fainting episodes. Present avoidance was predicted by the number of past faints and expectations of the probability of future fainting.
In summary, inherited anxiety proneness and painful conditioning episodes may be involved in the etiology of blood-injury phobia in much the same way that they are in other phobias. Fainting may serve as an additional aversive event operating only in blood-injury phobia. Although vasovagal syncope is not unique to individuals with a blood-injury phobia, when this tendency is particularly strong, the probability of fainting around blood and injury may increase. To the extent that these fainting experiences are aversive, stimuli may become associated with avoidance. Nonetheless, whereas explana- tions in terms of anxiety proneness and conditioning make reference to the etiology of fear, they do not address the etiology of fainting.
Blood-Injury Phobia 447
The Etiology of Fainting
Lewis (1932) offered the phrase “vasovagal syncope” as the one most descriptive of the mechanism of emotional fainting. He suggested that the first of the two processes was vagally mediated cardiac slowing. The vagus is a parasympathetic nerve that innervates the chest and upper abdomen and, among other things serves to decrease heart rate. However, slowing of the heart rate to 40-50 beats per minute is insufficient to induce unconsciousness and Lewis therefore postulated involvement of the vasculature. He sug- gested that a concomitant fall in blood pressure was the necessary cause of the cerebral ischemia that precipitated syncope. Vagal involvement added to the clinical picture rather than being the primary cause of fainting. Subsequent research has provided some support for these assertions and has clarified the mechanisms of vasovagal syncope.
A balance between cardiac output and peripheral resistance maintains arterial blood pressure. A fall in peripheral resistance will not normally produce a corresponding decline in arterial blood pressure, owing to a compensatory increase in cardiac output. One of the puzzles regarding vasovagal syncope was that cardiac output failed to increase despite decreased peripheral resistance. Weissler, Warren, Estes, McIntosh, and Leonard (1957) hypothesized that the absence of a compensatory rise in cardiac output may be due to a vagally mediated myocardial slowing. Alternatively, they suggested that insufficient ve- nous return to the heart may prevent a rise in cardiac output.
Weissler et al. (1957) tested the hypothesis of vagal inhibition by examining the effect of atropine on cardiac output. By acting on the heart, atropine usually serves to reverse bradycardia. However, cardiac output among subjects administered atropine was no different from that among control subjects without atropine. This result confirmed Lew- is’s claim that vagal inhibition of heart rate was neither the primary factor limiting cardiac output, nor a necessary cause of syncope. In a second set of experiments, the same experimenters examined the effects of procedures that increase cardiac output, one of which included inflation of an antigravity suit surrounding the subject. Inflation of the suit immediately terminated syncope, by reversing hypotension and thereby elevating cardiac output. They suggested, on the basis of these findings, that limited venous inflow to the heart plays a significant role in the restriction of cardiac output in syncope. Subse- quent investigators have begun the search for causes of the decrease in blood pressure, initially using blood donors as subjects.
Research with blood donors permits comparisons between those who do and those who do not faint. Blood donors who do not faint, typically demonstrate a rise in systolic and diastolic blood pressure during the preparations for venepuncture. Heart rate, respiratory rate, and cardiac output increase during the first half of blood withdrawal and fall in the latter half. Blood pressure, heart rate, respiratory rate, cardiac output, and peripheral resistance tend to fall slightly after bleeding (Logic, Johnson, & Smith, 1963). Blood donors who faint, differ principally from nonfainters only after withdrawal of blood. They exhibit a greater and more rapid fall in heart rate, pulse pressure, peripheral resistance, and they demonstrate minimal changes in cardiac output after bleeding (Goldstein et al., 1982; Glick & Yu, 1963; Logic et al., 1963; Ost, Sterner, & Lindahl, 1984; Ruetz et al., 1967). The drop in blood pressure (particularly diastolic) correlates positively with de- creases in heart rate and increases in fainting (Ogata, Iinuma, Nagashima, & Akabane, 1980; Ruetz et al., 1967). The hypotension appears to be due to active sympathetic vasodilatation in the skeletal musculature (Barcroft, Edholm, McMichael, Sharpey- Schafer, 1944; Engel, 1962, 1978; Greenlield, 1951; Wallin & Sundlof, 1982; Roddie, 1977). Thus, general physiological indices suggest that vasovagal syncope involves an

448 A. C. Page
initial increase in arousal followed by an excessive decrease in arousal. Examination of the biochemical changes associated with syncope suggests that the sympathetic nervous system may mediate increases in arousal and that the parasympathetic nervous system may mediate decreases in arousal. Catecholamines (adrenalin and noradrenaline) in- crease during fear (and prior to fainting) and noradrenaline levels decrease with fainting (Chosy & Graham, 1965; Vingerhoets, 1984). However, a purely physiological descrip- tion fails to explain what triggers the physiological response in the first place. Further- more, it is not clear why only a relatively small subset of stimuli trigger vasovagal syncope. Research has therefore focussed on the variables that engage the autonomic processes responsible.
Investigations of the processes responsible for fear and fainting include studies of the heritability of each. Phobic fear has a moderately strong heritable component (Andrews et al., 1990; Kendler et al., 1992; cf. Skre, Onstad, Torgersen, Lygren, & Kringlen, 1993). However, because fainting involves distinct processes to fear, differential heritabil- ities may be expected. Consistent with this notion, Kleinknecht and Lenz (1989) identi- lied a strong parent-child correspondence in a nonphobic sample with blood-injury con- cerns; the heritability estimates being higher for fainting than for fear. Clinical samples yield similar results, with estimates of the number of patients reporting a positive family history ranging from 27% to 68% (Kozak & Montgomery, 1981; Marks, 1988; Ost et al., 1984). These results contrast with the lower positive family histories for specific phobias more generally, ranging from 11% to 31% (Fyer et al., 1990; Marks, 1987; Marks & Herst, 1979; Ost et al., 1984). One possible reason for the elevated heritability of blood-injury phobia may be that the tendency to faint is more highly heritable than the tendency to become afraid. Along these lines, Ost (1992) divided blood-injury phobics into two groups; those who feared blood and those who feared injections. Blood phobics were more likely to report an episode of fainting (70%) than injection phobics (56%). In turn, blood phobics were more likely to report having a first degree relative with the same phobia (61%) than injection phobics (29%).
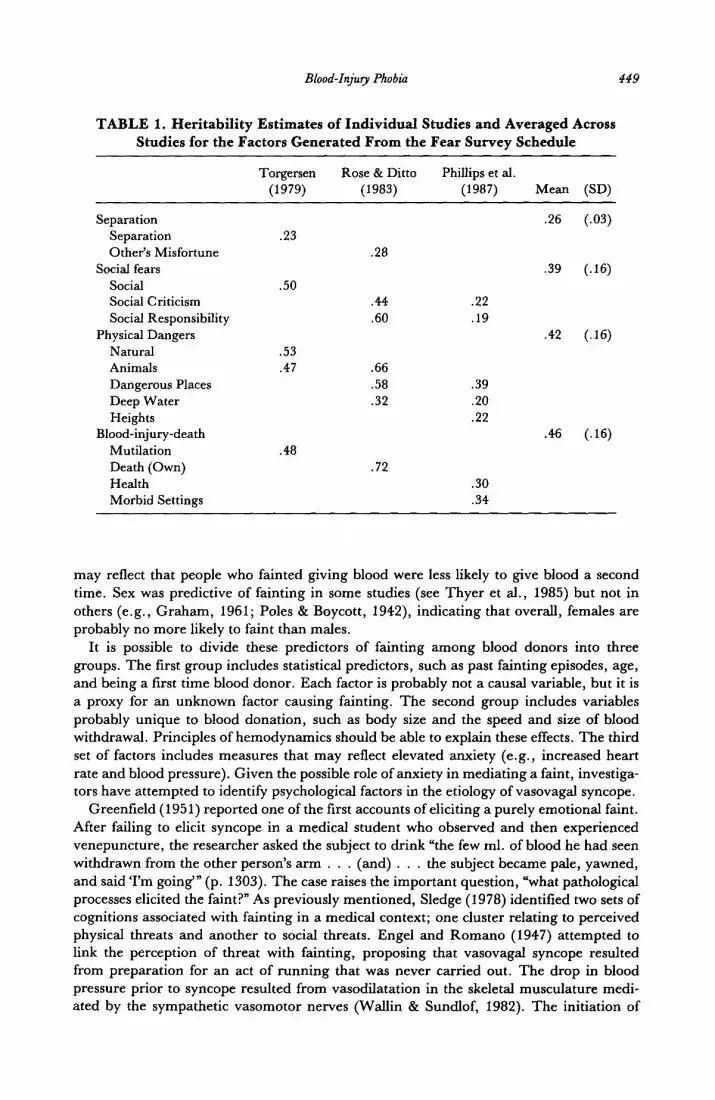
Although the aforementioned studies are consistent with the existence of a heritable predisposition, they are also consistent with some form of environmental transmission (e.g., vicarious learning). However, some confidence in a genetic interpretation can be drawn from the observation that fainting subjects are not able to reliably identify whether their parents have fainted in response to blood and injury (Kleinknecht & Lenz, 1989). Thus, transmission of the vulnerability is not by any obvious environmental means. A genetic interpretation of the family studies receives additional support from twin studies. It is evident from data summarized in Table 1 that blood-injury fear has a heritable component at least comparable to other specific phobias. It is probably over-interpreting the small difference to conclude that the heritability is highest for blood-injury fears. Nevertheless, findings from family studies, suggesting that fainting is more heritable than fear, imply that a division of blood-injury phobics on these grounds would produce higher heritabilities for blood-injury phobics with a history of fainting than for phobics more generally.
Despite the absence of data regarding a specific heritability of fainting, there are a variety of accounts of the physiological processes responsible for fainting. Much early research was conducted with blood donors and therefore the initial theories of vasovagal syncope implicated blood loss. Some factors predictive of fainting among blood donors were the amount and speed of blood withdrawal, a history of fainting, low body weight, and a higher blood pressure and pulse rate prior to the procedure (Callahan et al., 1963; Graham, 1961; Ogata et al., 1980). Y ounger patients were more likely to faint (Callahan et al., 1963), as were first time donors (Poles & Boycott, 1942). However, these effects
Blood-Injury Phobia 449
TABLE 1. Heritability Estimates of Individual Studies and Averaged Across
Studies for the Factors Generated From the Fear Survey Schedule
Separation
Separation
Other’s Misfortune
Social fears
Social Social Criticism
Social Responsibility
Physical Dangers
Natural
Animals
Dangerous Places
Deep Water
Heights Blood-injury-death
Mutilation
Death (Own)
Health
Morbid Settings
Torgersen
(1979)
.23
.50
.53
.47
.48
Rose & Ditto Phillips et al.
(1983) (1987) Mean (SD)
.26 (.03)
.28
.39 (.16)
.44 .22
.60 .19
.66
.58 .39
.32 .20
.22
.72
.30
.34
.42 (.16)
.46 (.16)
may reflect that people who fainted giving blood were less likely to give blood a second time. Sex was predictive of fainting in some studies (see Thyer et al., 1985) but not in others (e.g., Graham, 1961; Poles & Boycott, 1942), indicating that overall, females are probably no more likely to faint than males.
It is possible to divide these predictors of fainting among blood donors into three groups. The first group includes statistical predictors, such as past fainting episodes, age, and being a first time blood donor. Each factor is probably not a causal variable, but it is a proxy for an unknown factor causing fainting. The second group includes variables probably unique to blood donation, such as body size and the speed and size of blood withdrawal. Principles of hemodynamics should be able to explain these effects. The third set of factors includes measures that may reflect elevated anxiety (e.g., increased heart rate and blood pressure). Given the possible role of anxiety in mediating a faint, investiga- tors have attempted to identify psychological factors in the etiology of vasovagal syncope.
Greenfield (1951) reported one of the first accounts of eliciting a purely emotional faint. After failing to elicit syncope in a medical student who observed and then experienced venepuncture, the researcher asked the subject to drink “the few ml. of blood he had seen withdrawn from the other person’s arm . . . (and) . . . the subject became pale, yawned, and said ‘I’m going”’ (p. 1303). The case raises the important question, “what pathological processes elicited the faint?” As previously mentioned, Sledge (1978) identified two sets of cognitions associated with fainting in a medical context; one cluster relating to perceived physical threats and another to social threats. Engel and Roman0 (1947) attempted to link the perception of threat with fainting, proposing that vasovagal syncope resulted from preparation for an act of running that was never carried out. The drop in blood pressure prior to syncope resulted from vasodilatation in the skeletal musculature medi- ated by the sympathetic vasomotor nerves (Wallin & Sundlof, 1982). The initiation of

450 A. C. Page
physical exercise would increase venous return to the heart and no drop in blood pressure would result. In the absence of running, a precipitous drop in blood pressure would occur, leading to syncope. Vasovagal syncope occurred in blood donation units because individuals were anxious and prepared to flee, but the social context prohibited them for doing so.
The main objection to Engel and Romano’s (1947) argument is that the majority of subjects who faint during simple venepuncture do so after withdrawal of the needle (Ruetz et al., 1967). Fainting cannot be a preparation for escape from danger if it is most likely to occur after removal of the threat. In response to this difficulty Graham (1961; Graham et al., 1961) suggested that the fainting response is diphasic. The first phase was, as Engel suggested, a preparation for flight. However, the second phase was relief at the passing of a threat. This explained why some people fainted after the needle had entered the vein (if initial pain was the perceived threat) and why most fainted upon removal of the needle (if withdrawal of blood was the perceived threat). The account explained why fainters tended to be nervous (because perception of threat triggered sympathetic arousal present in the first phase) and why bradycardia was the response observed in the second phase (because when the person relaxed as the danger passed, compensatory parasympa- thetic activity dominated). Also consistent with postulation of a diphasic response are an acute rise in blood and pulse pressures followed by decreases in indexes of cardiac func- tion, systemic resistance, and blood pressure (Curtis & Thyer, 1983; Foulds, 1993; Glick & Yu, 1963; Thyer & Curtis, 1985). Biochemical changes similarly reflect a succession of sympathetic and parasympathetic response (Goldstein et al., 1982; Henry, 1984; Vinger- hoets, 1984).
The increasing amount of data attesting to a diphasic response has ensured its retention within more recent theories. Each acknowledges the existence of a diphasic response but variations exist regarding the identified triggering mechanism. The revisions have been prompted by difficulties with Graham’s original account. Primarily, although nervousness and anxiety precede vasovagal syncope, there is no evidence of a rapid reduction in anxiety prior to syncope. If anything, anxiety appears to continue to rise until loss of consciousness (Curtis & Thyer, 1983). A further difficulty with assuming that vasovagal syncope is concomitant with anxiety relief becomes evident when considering other anxi- ety disorders. The sharp rise in sympathetic arousal on exposure to feared stimuli is common to all phobias and so is the rapid decrease in anxiety following removal of the feared stimulus. So ubiquitous is the phenomenon that it has been postulated as sufficient to maintain phobic avoidance (Marks, 1987; Mowrer, 1950). Therefore, if anxiety relief causes vasovagal syncope, it is not clear why fainting is unique to blood-injury phobia.
In an effort to accommodate such difficulties, Engel (1978) argued that vasovagal syncope involves a diphasic reaction comprising a fight-flight and a conservation-with- drawal response. Engel emphasises that rather than a systematic progression from one response to another, physiological control is disorganized. When an organism experiences a novel danger, when environmental circumstances prohibit a typical response (e.g., physical restraint), or when past experience has taught the futility of a certain response, a condition of unresolvable uncertainty about appropriate responding exists. Simultaneous activation or rapid alternation between sympathetic and parasympathetic responses re- flects the uncertainty.
A similar conceptualization of the diphasic response has developed from the notion that fainting is an adaptive response to a threat. Vingerhoets (1984) suggested that the dipha- sic response involves a rapid succession of two kinds of stress reactions. The first reaction is a flight-fight response. The second reaction is a conservation-withdrawal response. Both reactions are active strategies for coping with stress (see Henry, 1976). In the first

Blood-Injury Phobia 451
phase (mediated via the orbital frontal cortex and the amygdala), behavior involves aggression and flight. Mobilization of resources serves to prepare for the necessary motor activity. In the second phase (mediated by the pituitary-adrenal axis), behavior involves inhibition and decreased mobility. The organism disengages and withdraws, becoming inactive to conserve energy. The latter pattern of behavior decreases engagement with the threat and the organism may be less conspicuous to potential predators.
Along similar lines, vasovagal syncope may increase the probability of survival. Car- diac slowing in response to blood and injury may be an adaptive reflex that evolved under circumstances in which immobility produced less risk than did flight (Henry, 1984; Marks, 1988). As a predator lost interest in the immobile prey, the organism could flee. Marks suggested that similar central nervous system structures (the depressor area) medi- ate human fainting and tonic immobility (i.e., playing dead). For example, stimulation of a cat’s cingulate gyrus results in a pattern of responding similar to vasovagal syncope. The behavior includes freezing, vasodilatation of skeletal musculature, a fall in blood pressure, and decreased respiration (Lofving, 1961). H owever, the patterns of responding within vasovagal syncope and tonic immobility are different in one important respect. A tonically immobile organism, although stationary, is highly aroused and ready for action. It will flee as soon as the predator leaves or relaxes its grip (Gallup & Maser, 1977). During vasovagal syncope the person loses consciousness. If a predator was to leave or relax its grip, the organism would be completely unaware. Furthermore, Steptoe and Wardle (1988) found that subjects who fainted were more likely to attend to bodily sensations than those who did not faint. If vasovagal syncope was a form of tonic immobil- ity, subjects who fainted should be more likely to focus on the threat.
Barlow (1988) acknowledged some of these difficulties and argues that a different physiological response to both tonic immobility and the flight or fight response may mediate fainting. He suggests that our ancestors who responded to injury and bleeding with a dramatic drop in blood pressure would minimize blood loss and the danger of shock. For these reasons they would be more likely to survive an attack. Although appeal- ing, the account fails to acknowledge a commonly observed response in emergency wards. When individuals sustain severe tissue damage and blood loss, the decrease in venous return to the heart leads to increases in heart rate and systemic vasoconstriction, thereby pumping more blood around the body (see Poles & Boycott, 1942). The cardiac slowing referred to occurs after loss of 30% of total blood volume (see Appenzeller, 1990). It is difficult to see how little or no blood loss by a blood-injury phobic could trigger a response that serves to minimize severe blood loss, especially when the normal reaction to small losses of blood is in the opposite direction to that evident during syncope. For instance, Klorman, Weissberg, and Wiesenfeld (1977) reported that blood-injury phobics exhibited a pattern of results opposite to those expected if the response to blood and injury involved exaggerated cardiac deceleration. Individuals with low scores on the MQ demonstrated reduced heart rate in response to slides of mutilation. In contrast, individuals with high scores on the questionnaire showed increases in heart rate to the slides (although a cardiac deceleration consistent with a diphasic response occurred later in the trial). Thus, the adaptive advantage of vasovagal syncope remains obscure. Indeed, vasovagal syncope may serve no adaptive advantage. The behavior may even be a counterproductive re- sponse gradually being bred out of our species as predators killed those with a tendency to faint.
Another possibility is that vasovagal syncope has multiple determinants. For example, Lumley and Melamed (1992) found that blood pressure did not correlate with self- reported faintness. These data could imply that a factor other than reductions in blood pressure may be contributing to the prodrome of vasovagal syncope. One possible factor
452 A. C. Page
is hyperventilation. Foulds (1993) measured heart rate and cerebral blood flow in a single blood-injury phobic under various conditions. When exposed to a slide of a severed linger, the patient exhibited a typical diphasic pattern of responding. However, the patient also exhibited a reduction in cerebral blood flow that preceded cardiac decelera- tion. In a pre-test, Foulds found an association between reductions in cerebral blood flow and hyperventilation. He suggested that hyperventilation may have complicated the clinical picture by producing dizziness, feelings of faintness, and reduced cerebral blood flow (see Papp, Klein, & Gorman, 1993). Although Foulds did not record breathing during exposure, an examination of earlier studies lends support to his claim. Ruetz et al. (1967) examined pulmonary alveolar gas tensions before and after phlebotomy and found results consistent with a hyperventilation hypothesis. They found that fainters evidenced a decrease in pC0, values relative to controls. They also noted that inhalation of 5% COP, which should restore pC0, values, can produce a rapid and notable clinical im- provement in syncope (see McHenry, Fazekas, & Sullivan, 1961). Although respiration is a relatively insensitive index of hyperventilation, Logic et al. (1963) found similar increases in respiration rate among blood donors who fainted (cf. Steptoe & Wardle, 1988). Because all of these studies used blood donors as subjects, it is important to investigate Foulds’s interesting suggestion within a phobic sample. Nevertheless, even if hyperventilation turns out to be a further factor complicating fainting, it remains to identify a comprehensive account of the two phases of vasovagal syncope.
Disgust Sensitivity and Fainting
A speculative proposition is that vasovagal syncope has little to do with fear. Fainting may be subserved by the same psychological and physiological processes as those that underlie disgust. When the (parasympathetic) processes underlying disgust combine with a homeostatic increase in parasympathetic activity (which counteracts the sympathetically mediated light or flight response), the joint effect may produce a pattern of vascular and vagal responding responsible for fainting.
Matchett and Davey (1991) measured disgust sensitivity (using a 24-item scale investi- gating responses to contamination of otherwise highly desirable foods; Rozin, Fallon, & Mandell, 1984) and various fears (using the Fear Survey Schedule, FSS; Wolpe 8z Lang, 1964). They found a low correlation (r = 0.16) between a blood-injury factor of the FSS and trait anxiety. In contrast, disgust sensitivity correlated positively (r = 0.33) with the blood-injury factor. Similarly, Grassick (1990) described a 22-year-old female presenting with anxiety about injections. The patient also manifested a heightened disgust sensitiv- ity, indicated by aversions to nude males, dirt, and spiders. The patient reported that she felt dizzy and nauseous when painting a nude model in an art class, a pattern of respond- ing similar to that which occurred when receiving an injection. Indeed, she “stated that she found close examination of her ‘flesh’ distasteful and even disgusting,” especially her veins (Grassick, 1990; p. 284, italics added). Although correlational data and a case report do not provide strong evidence that disgust sensitivity may relate to fainting, there are several reasons for expecting that disgust mediates the relationship between fainting and blood-injury phobia.
Disgust is a fundamental emotion defined as “revulsion at the prospect of (oral) incorpo- ration of an offensive object. The offensive objects are contaminants; that is, if they even briefly contact an acceptable food, they tend to render that food unacceptable” (Rozin & Fallon, 1987; p. 23). Disgust serves to protect omnivors from the risk of poisoning by creating strong affective responses to seemingly edible foods. Rozin and Fallon therefore argued that this is why almost all objects rated as disgusting are animals (and parts

Blood-Injury Phobia 453
thereof) or animal bodily products (e.g., faeces, urine, and mucus; Angyal, 1941).2 One attribute of such bodily products is that they have an unusual status with respect to the self. For instance, Allport (1955) noted that saliva in the mouth does not elicit disgust, but saliva is able to elicit disgust once it leaves the body (see Rozin, Millman, & Nemer- off, 1986).
Blood and injury comprise part of the class of objects identified by Rozin and Fallon as disgusting. Blood is an animal bodily product and as such it is treated in the same way as other bodily products. For instance, Allport’s (1955) comment that saliva becomes dis- gusting as it leaves the body is equally applicable to blood. Indeed, he noted that sucking blood from a cut finger is less distressing than tasting the same blood after it has left the body and passed onto a bandage. There is also much evidence from anthropological studies regarding the similar treatment of blood and disgusting substances. For instance, Kwaio people designed settlements so that “polluted” areas were downhill from the “sa- cred” areas. At the lowest point of the settlement was a hut dedicated for use by females during menstruation (Keesing, 1981).
However, to successfully argue that disgust mediates vasovagal syncope, it is necessary to do more than suggest that blood and injury can elicit disgust. It is necessary to demonstrate first, that fainting and disgust co-occur and second, that vasovagal syncope and disgust involve identical physiological processes. Addressing the first point, there does not appear to be any published research explicitly examining the relationship be- tween fainting and disgust. Nevertheless, Greenfield’s (1951) study could be a case in point, when he demonstrated that fainting could be triggered by a request to drink another person’s blood. Although fear of contamination may have been mediating the person’s reaction, it is equally plausible that the subject found the prospect of consuming another’s blood disgusting.
Addressing the second point, that disgust and fainting recruit similar physiological processes, it is necessary to again draw on research not designed to test the hypothesis in question. Broadly speaking, disgust and vasovagal syncope are both mediated by parasympathetic processes involving the vagus nerve. The vagus nerve not only inner- vates the heart but also the smooth muscles of much of the digestive system (e.g., oesopha- gus, stomach, intestines, etc.). Therefore, the vagus serves a dual role in the regulation of cardiac and digestive function. Although it is probably premature to speculate about common neurophysiological structures, it is noteworthy that the nucleus of the solitary tract participates in cardiovascular control, the monitoring of tastes, and the rejection of otherwise palatable foods (Scott, 1992). Similarly, the medulla, via its vagal afferents, controls cardiac slowing as well as nausea and vomiting (Sanford, 1982). Therefore, eliciting disgust involves activation of the parasympathetic nervous system that serves to reduce blood pressure.
Taking the suggestion that blood and injury elicit disgust, a dual process account of vasovagal syncope is possible. It was argued earlier that blood and injury are capable of eliciting fear and avoidance. This implies that one process involved in the phobic reaction is a sympathetically mediated fight or flight response. The processes responsible will be similar to those involved in other phobias. Exposure to a phobic stimulus will elicit sympathetic arousal that will either habituate with the passage of time or decrease on removal of the stimulus. However, because the two branches of the autonomic nervous system operate in an antagonistic manner, the sympathetic activity will reduce, in part,
*Disgust of an interpersonal nature is beyond the scope of the present discussion, the interested
reader is referred to Rozin and Fallon (1987).
454 A. C. Page
due to a relative increase in parasympathetic activity. Assuming that blood and injury can elicit disgust, the second process in the diphasic reaction should involve a parasympa- thetically mediated disgust response. Observable responding will reflect the more domi- nant of the two processes.
Exposure to blood and injury will elicit a rapid sympathetic response ensuring that an organism is in a position to flee or light. These processes will initially mask any concur- rent parasympathetic activity (i.e., disgust). When homeostatic (i.e., parasympathetic) processes are recruited, either in the course of habituation or upon the removal of the stimulus, a summation may occur. The antagonistic increase in parasympathetic activity (to counter the sympathetically mediated light of flight response) may sum with the parasympathetic activity already activated to produce a disgust response. Consequently, an excessively strong parasympathetic response will produce a drop in blood pressure, thereby setting the stage of vasovagal syncope.
A dual process account permits explanation of a variety of scenarios. It may be that a person continues to perceive a threat at the same time as a disgust response is elicited (thus inhibiting habituation by continually reactivating the sympathetic response). Individuals would then exhibit the apparent confusion or rapid alternation between sympathetic and parasympathetic activity noted by Engel (1978). Because the initial sympathetic response would mask any parasympathetic involvement, fainting would not occur until the homeo- static parasympathetic activation summated with the disgust response to reduce blood pressure. Fainting would therefore tend to occur on removal of a perceived threat (Gra- ham, 1961; Graham et al., 1961).
To adopt a dual process account of blood-injury phobia means that three subtypes of blood-injury phobia should be identifiable. The first subtype includes fearful blood-injury phobics. Such individuals would exhibit elevated trait anxiety and anticipatory anxiety regarding exposure to blood and injury. The second subtype includes the fainting blood- injury “phobics,” who experience feeling of faintness in the presence of blood and injury due to elevated disgust sensitivity. Such people will avoid blood and injury stimuli be- cause they anticipate becoming faint. The final subtype includes the fearful fainting blood-injury phobics. Among these individuals, the avoidance of blood and injury will occur as a combination of the two mechanisms just described. For instance, an elevated disgust sensitivity leading to early aversive fainting experiences may provide the basis for the development of fearful anticipation. This three-fold classification is consistent with Kleinknecht and Lenz’s (1989) data, but it adds that the processes underlying fear and fainting are the mechanisms involved in triggering of the fight or flight response and the disgust response.
Although the aforementioned explanation is presently speculative, it is possible to generate several testable predictions. First, two symptom patterns should be distinguish- able among people who report fear or fainting in the presence of blood and injury. Second, one of the symptom patterns should correlate with elevated trait anxiety and the other with elevated disgust sensitivity. Feelings of faintness should be lowest in “fearful phobic2 and highest in “fearful faintness.” Third, treatments should be differentially sensitive. Individuals with elevated trait anxiety would benefit most from treatments that reduce sympathetic activity (i.e., fear control). Individuals with elevated disgust sensitiv- ity should benefit most from treatments that reduce parasympathetic activity (i.e., faint- ing control). Another prediction is that fainting may not be unique to blood-injury phobia. Disgust sensitivity is associated with certain types of animal phobias. Specifically, possible predators (e.g., sharks) elicit less disgust than nonpredators (e.g., slugs; Davey, Forster, & Mayhew, 1993; Matchett & Davey, 1991). Feelings of faintness should be more prevalent among animal phobics who avoid “disgusting” animals, than among

Blood-Injury Phobia 455
animal phobics who avoid “dangerous” animals. It should also be possible to indepen- dently vary the perceived threat and disgustingness of blood or injury and examine the effect on fear and fainting. For instance, one’s own blood carries much the same risk of contamination whether on one’s skin or on a bandage, yet its ability to elicit disgust increases with greater proximity from the body. Therefore, fear should be unmodified by the distance from the body, but feelings of faintness should increase. In addition, because disgust sensitivity (Davey et al., 1993; Rozin, Fallon, & Mandell, 1984) and trait anxiety are both likely to be inherited (Andrews et al., 1990), blood-injury phobia will be inher- ited to the extent that it is a combination of these two vulnerabilities. Disgust sensitivity should be most predictive of fainting in the presence of blood and injury and trait anxiety should be most predictive of fear in the presence of blood an injury.
TREATMENT
If blood-injury phobia involves two potentially separable and etiologically distinct compo- nents, at least two treatment approaches should be effective. Furthermore, matching treatment to the underlying mechanism should maximize the outcome of therapy. Until recently, blood-injury phobia was conceptualized and treated in a similar way to other specific phobias. Treatments involved exposure to feared stimuli (see Fyer, 1987) and the conduct of therapy was similar to that offered for other specific phobias (e.g., Page, 1993). Fainting was inconvenient because it could hinder exposure exercises and the key determinant of treatment success was fear reduction.
Indeed, exposure has been successful in the treatment of blood-injury phobia (Curtis & Thyer, 1983; Lloyd & Deakin, 1975). It has also been successful when combined with participant modelling or relaxation training to facilitate anxiety reduction (Elmore, Wild- man, &Westfield, 1980; Nimmer & Kapp, 1977; Taylor, Ferguson, & Wermuth, 1977). Having patients place their heads between their knees when necessary (Yule & Fernando, 1980) overcame the inconvenience of fainting. Alternatively, conducting exposure with patients in a supine position enabled gradual progression until they were able to stand and face their phobic objects (Marks, 1988). Although fainting appears to extinguish (or habituate) during treatment, the extent to which fainting continues to trouble patients after treatment is not apparent. The dual process model developed in the current paper predicts that individuals with a history of fainting would be more likely to relapse because future aversive fainting episodes may re-elicit fear.
A more recent development in treatment has been the inclusion of components to modify vasovagal syncope. Wardle and Jarvis (1981) suggested on the basis of a single case, that cognitive therapy aimed at modifying beliefs about blood and injury caused cardiac changes that ultimately decreased the probability of fainting. Although an appeal- ing proposition, subsequent research has not taken up this question (see Kaloupek, Scott, & Khatami, 1985; Kaloupek, White, & Wong, 1984). Interest has instead focussed on an intervention identified by Cohn, Kron, and Brady (1976) when they had difficulty treat- ing a blood-injury phobic with graded exposure combined with relaxation. The hypothe- sized reason for failure was that vasovagal syncope involved a pattern of responding similar to that induced during relaxation. When the treatment strategy changed, to inducing a state of anger during exposure, the patient improved. Using a similar ap- proach, Babcock and Powell (1982) successfully treated an individual using a modified version of reciprocal inhibition. Rather than the usual anxiety-reducing strategies, the patient imagined acting aggressively to fend off attackers.
According to a similar rationale, Kozak and Montgomery (1981) identified a simple technique to prevent fainting during exposure, that is now called applied tension. They

456 A. C. Pafe
assumed that any activity incompatible with syncope would prevent fainting. For exam- ple, because anger involves increases in heart rate and blood pressure, its elicitation should be incompatible with syncope. Rapid and frequent contraction of skeletal muscula- ture should likewise increase venous return, enhance cardiac output, and thereby prevent or reverse syncope (see Engel & Romano, 1947). Consistent with this rationale, Kozak and Montgomery (1981; see also Kozak & Miller, 1985) successfully treated a group of blood-injury phobics with graded exposure after being taught to contract musculature in a manner that they assumed would increase blood pressure and cerebral blood flow. Supporting the theoretical explanation of why applied tension may militate against syn- cope, Foulds, Weidmann, Patterson, and Brooks (1990; although cf. Foulds, 1993) found that heart rate and cerebral blood flow velocity increased during muscle tensing exercises to a greater degree than that observed during mental arithmetic or relaxation. These data concord with measures taken by Ost and Sterner (1987), who found that systolic blood pressure increased by 14 mm Hg following applied tension.
Although these case studies may help to identify characteristics of an individual that relate to relatively greater success with one technique as opposed to another, they cannot establish relative treatment efficacy without adequate controls. In this context, Ost et al. (1984) compared exposure alone to exposure plus training in applied “relaxation.” Sub- jects relaxed before exposure to feared stimuli, but tensed skeletal musculature whenever fainting was imminent. The more complicated procedure was no more effective than exposure alone. Later, Ost and Sterner (1987) f ound that they were able to successfully treat individuals using graded exposure plus applied tension (without the relaxation com- ponent) in five sessions. The shorter number of sessions required when treatment focus- sed on fainting could support the treatment’s validity. However, the absence of a control group prohibited drawing such conclusions. More recently, Ost, Sterner, and Fellenius (1989) compared graded exposure when combined with applied relaxation or applied tension. There were no differences between groups at post-treatment or follow-up (al- though there was a trend in the favor of applied tension). Both treatments were very effective, with three quarters of each group being much improved.
Apparently inconsistent with the dual process model developed here is the absence of evidence from controlled trials that applied tension enhances the efficacy of graded expo- sure. One possibility is that although exposure is effective with subjects who rarely or never faint, fainting control skills are effective with patients who have a tendency to faint. Ost et al. (1989), however, failed to find any superior efficacy of applied tension among patients who fainted. One possibility is that some of the nonfainters reported in the study were misclassified. They identified fainters as those who “either fainted or were on the edge of doing so” (p. 118) during the pre-treatment assessment. It is possible that many of the nonfainters had actually fainted at other times but did not do so during the pre- treatment assessment. The alternative explanation derives additional support from a comparison of the finding that 80% of blood-injury phobics report a past history of fainting in response to relevant stimuli (Ost et al., 1984; Thyer et al., 1985) with the data of Ost et al. (1989), that only identified 37% of fainters. Perhaps use of a different criterion, such as reports of two prior episodes of fainting in response to blood injury stimuli, may have revealed that fainters responded better to applied tension than non- fainters.
Ost, Fellenius, and Sterner (1991) h ave since addressed an important issue, examining the extent to which exposure is mediating the effects of applied tension. They compared groups given exposure alone, applied tension alone, and applied tension training during exposure to blood and injury slides. They found that both groups given training in applied tension exhibited temporary increases in blood pressure. After treatment, and at

Blood-Injury Phobia 457
follow-up, the two tension groups were superior to the exposure alone group in terms of a behavioral avoidance as well as observer ratings of fainting behavior. These data support the authors’ conclusion that “it is the coping skill that is crucial component in the applied tension package, and that exposure to the phobic stimuli does not seem to be necessary” (p. 571). However, this same conclusion does not receive support from their data regard- ing state anxiety, where all groups improved to an equivalent degree. Rather, it appears that exposure can reduce state anxiety as effectively as applied tension (with and without exposure), but it is not as successful in reducing fainting. behavior. Assuming that de- creased avoidance reflects reductions in fear and fainting, applied tension is the most effective treatment because it reduces both the fear and the fainting leading to avoidance. Exposure alone is of lesser efficacy because it only reduces fear.
In summary, individual case studies and controlled treatment trials are generally con- sistent with the hypothesis that two etiological pathways characterize blood-injury phobia; one underlying fear and another fainting. Fainting control skills assist in treatment but there is presently no convincing evidence from controlled trials that the effects are strong- est among patients who faint. One way to increase the power of subsequent investigations is to allocate subjects to groups on the basis of the factor that predisposes a person to vasovagal syncope. If disgust sensitivity is indeed the vulnerability factor underlying observed fainting, then measures of the construct will be potentially more informative and discriminatory than fainting behavior.
A PROGRAM OF FUTURE RESEARCH
Blood-injury phobia is an atypical phobia because it involves vasovagal syncope as well as phobic fear. This descriptive separation of fear from fainting serves to provide an overall framework for future research. Without restating the individual research questions dis- cussed earlier, an overall program of research needs to extend the separation of fear from fainting. It is necessary to identify the symptoms that discriminate between blood-injury phobics who are high on fear from those who are high on fainting. Following this diagnos- tic subtyping, it will be possible to investigate correlates of the particular symptom pat- terns, thereby identifying etiological variables. It was suggested that trait anxiety may correlate with blood and injury fears and avoidance, while disgust sensitivity may corre- late with fainting. If future research supports these two etiological variables, it may be possible to refine existing therapies and develop new treatments accordingly. Broadly speaking, applied tension aims to overcome fainting by increasing sympathetic activity. An, as yet unexplored alternative, would be to generate treatments that directly decrease parasympathetic activity. In this way, a deeper understanding of the mechanisms respon- sible for the unusual aspects of blood-injury phobia will guide uniquely focussed treat- ments for this potentially life-threatening disorder.
Acknowledgements-This work was supported in part by the Government Employees and Medical
Research Fund. I am grateful for the helpful comments of Gavin Andrews and two anonymous
reviewers on earlier drafts.
REFERENCES
Agras, S. W., Sylvester, D., & Oliveau, D. (1969). The epidemiology ofcommon fears and phobias. Comprchm-
sive Psychiatry 10, 439-447.
Allport, G. W. (1955). Becoming: Basic cotrtiderationsforapsycholo~ ofpemoanlily. New Haven, CT: Yale University
Press.

458 A. C. Page
American Psychiatric Association (1987). Diagnostic and statistical manual of the mental disorders (3rd cd. rev.). Washington, DC: Author.
Andrews, G. (1991). Anxiety, personality, and anxiety disorders. Zntemational Rmicm of Psychiatry, 3, 293-302.
Andrew, G., Crino, R., Hunt, C., Lampe, L., & Page, A. (in press). Treatment of anxiety disorders: Clinician’s guide andpatient manuals. New York: Cambridge University Press.
Andrew, G., Stewart, G. W., Morris-Yates, A., Holt, P. E., & Henderson, A. S. (1990). Evidence for a
general neurotic syndrome. British Journal of Psychiatry, 157, 6-12. Angyal, A. (1941). Disgust and related aversions. Journal ofAbnormal Psychology, 36, 393-412. Appenzeller, 0. (1990). The autonomic nervozu system: An introduction to basic and clinical concepts. Amsterdam:
Elsevier.
Babcock, H. H., & Powell, D. H. (1982). Vasovagal fainting: Deconditioning an autonomic syndrome. Psychosomatics, 23, 969-970.
Babcock, H., Edholm, 0. G., McMichael, J., & Sharpey-Schafer, E. P. (1944). Post-hemorrhagic fainting: Study by cardiac output and forearm flow. Lancet, 1, 489-493.
Barlow, D. H. (1988). Anrie~ and its disordns: The nature and treatment of anxiety and panic. New York: Guilford Press.
Callahan, R., Edelman, E. B., Smith, M. S., & Smith, J. J. (1963). Study of the incidence and characteristics of blood donor “reactions.” Transfusion, 3, 76-82.
Cannon, W. B. (1927). The James-Lange theory of emotion: A critical examination and an alternative theory.
American Journal of Psychology, 39, 106- 124. Chosy, J. J., & Graham, D. T. (1965). Catecholamines in vasovagal fainting. Journal of Psychosomatic Research,
9, 189-194.
Clark, D. M. (1986). A cognitive approach to panic. Bchaviour Research and Therapy, 24, 461-470. Clark, D. M. (1988). A cognitive model of panic attacks. In S. Rachman, &J. D. Maser (Eds.), Panic:
Psychological perspectives. Hillsdale, NJ: Erlbaum. Cohn, C. K., Kron, R. E., & Brady, J. P. (1976). A case of blood-illness-injury phobia treated behaviorally.
The Journal of Nervous and Mental Disease, 162, 65-68. Connolly, J., Hallam, R. S., & Marks, I. M. (1976). Selective association of fainting with blood-injury-illness
fear. Behavior Therapy, 7, 8- 13.
Costello, C. G. (1982). Fears and phobias in women: A community study. Journal of Abnormal Psychology, 91, 280-286.
Curtis, G. C., & Thyer, B. (1983). Fainting on exposure to phobic stimuli. Am&an Journal of Psychiatry, 140, 771-773.
Davey, G. C. L., Forster, L., & Mayhew, G. (1993). Familial resemblances in disgust sensitivity and animal
phobias. Behaviour Research and Therapy, 31, 41-50. Elmore, R. T., Wildman, R. W., & Westfield, J. S. (1980). The use of systematic desensitization in the
treatment of blood phobia. Journal of Behaviour Therapy and Experimmlol Psychiatry, 11, 277-279. Engel, G. L. (1962). Fain&g (2nd cd.). Springfield, IL: Charles Thomas.
Engel, G. L. (1978). Psychologic stress, vasodepressor (vasovagal) syncope, and sudden death. Annals of Internal
Medicine, 89, 403-412.
Engel, G. L., & Romano, J. (1947). Studies of syncope. IV. Biologic interpretation of vasodepressor syncope. Psychosomatic Medicine, 9, 288-294.
Eysenck, H. J., & Eysenck, S. B. G. (1975). Manual of the Eyscnck Personality Qustionnaire (Junior and Adult).
Essex: Hodder & Stoughton. Foulds, J. (1993). Cerebral circulation during treatment of blood-injury phobia: A case study. Bchavioural
Psychotherapy, 21, 137- 146.
Foulds, J., Wiedmann, K., Patterson, J., & Brooks, N. (1990). The effects of muscle tension on cerebral
circulation in blood-phobic subjects and non-phobic subjects. Behavivur Research and Therapy, 28, 481-486. Fyer, A. J, (1987). Simple phobia. Modern Probltms in Phanacopsychiatry, 22, 174-192. Fyer, A. J., Mannuzza, S., Gallops, M. S., Martin, L. Y., Aaronson, C., German, J. M., Liebowitz, M. R.,
& Klein, D. F. (1990). Familial transmission of simple phobias and fears. Archives of General Psychiatry, 47,
252-256. Gallup, G. G., & Maser, J. D. (1977). Tonic immobility: Evoluntionary underpinnings of human catalepsy
and catatonia. In J. D. Maser, & M. E. P. Seligman (Eds.), Psychopathology: Experimental mod& (pp. 334-357). San Francisco, CA: Freeman.
Glick, G., & Yu, P. N. (1963). Hemodynamic changes during spontaneous vasovagal reactions. American Journal
of Medicine, 34, 42-5 1. Goldstein, D. S., Spanarkel, M., Pitterman, A., Toltzis, R., Gratz, E., Epstein, S., & Keisser, H. R. (1982).
Circulatory control mechanisms in vasodepressor syncope. American Heart Journal, 104, 1071-1075. Graham, D. T. (1961). Prediction of fainting in blood donors. Circulation, 23, 901-906.

Blood-Injury Phobia 459
Graham, D. T., Kabler, J. D., & Lunsford, L. (1961). Vasovagal fainting: A diphasic response. Psychosomatic
Medicine, 23, 493-507.
Grassick, P. (1990). The fear behind the fear: A case study of apparent simple injection phobia. foumul of
Behavior Therapy and Exfmimental Psychiatry, 21, 28 l-287.
Gray, J. A. (1987). Fear andstress (Zndcd.). Cambridge, MA: Cambridge University Press. Greenlield, A. D. M. (1951). An emotional faint. Lancet, I, 1302-1303.
Henry, J. P. (1976). Understanding the early pathophysiology of essential hypertension. Geriatrics, 31, 59-72.
Henry, J. P. (1984). On the triggering mechanism of vasovagal syncope. Psychosomatic Medicine, 46, 91-93.
Kaloupek, D. G., Scott, J. R., & Khatami, V. (1985). Assessment of coping strategies associated with syncope in blood donors. Journal of Psychosomatic Research, 29, 201-214.
Kaloupek, D. G., White, H., & Wong, M. (1984). Multiple assessment of coping strategies used by volunteer
blood donors: Implications for preparatory training. Journal ofBehauioura1 Medicine, 7, 35-60.
Keesing, R. M. (1981). Cultural anthropolou: A contemporary pemfiectioe. New York: Holt Rinehart & Winston. Kendler, K. S., Neale, M. C., Kessler, R. C., Heath, A. C., & Eaves, L. J. (1992). The genetic epidemiology
of phobias in women: The interrelationship of agoraphobia, social phobia, situational phobia, and simple
phobia. Archives of Gemal Psychiatry, 49, 273-281.
Kleinknecht, R. A. (1987). Vasovagal syncope and blood/injury fear. Behaviour Research and Therapy, 25, 175-
178.
Kleinknecht, R. A. (1988). Specificity and psychosocial correlates of blood/injury fear and fainting. Behaoiour
Research and Thmapy, 26, 303-309.
Kleinknecht, R. A., & Lena, J. (1989). Blood/injury fear, fainting and avoidance of medically-related situa-
tions: A family correspondence study. Behaoiour Research and Therapy, 27, 537-547.
Klorman, R., Hastings, J., Weerts, T., Melamed, B., & Lang, P. (1974). Psychometric description of some
specific-fear questionnaires. Bebaoior Therapy, 7, 35-60.
Klorman, R., Weissberg, R. P., & Wiesenfeld, A. R. (1977). Individual differences in fear and autonomic reactions to affective stimulation. Psychophysiology, 14, 45-51.
Kozak, M. J., & Miller, G. A. (1985). The psychophysiological process of therapy in a case of injury-scene-
elicited fainting. Journal of Behaviour Therapy and Experimental Psychiatry 16, 139-145.
Kozak, M. J., & Montgomery, G. K. (1981). Multimodal behavioral treatment of recurrent injury-scene-
elicited fainting (vasodepressor syncope). Behavioural Psychothmapy, 9, 316-321.
Lapouse, R., & Monk, M. A. (1959). Fears and worries in a representative sample of children. American Journal
of Orthopsychiatry, 29, 803-818.
Lewis, T. (1932). Vasovagal syncope and the carotid sinus mechanism. Bri>ish MedicalJournal, I, 873-876.
Lloyd, G. G., & De&n, H. G. (1975). Phobias complicating treatment of uterine carcinoma. British Medical
Journal, 4, 440.
Lofving, B. (1961). Cardiovascular adjustments induced from the rostral cingulate gyrus with special reference
to sympatho-inhibitory mechanisms. Acta Psychiatrica Scandinaoica, 184(&p@), l-82. Logic, J. R., Johnson, S. A., & Smith, J. J. (1963). Cardiovascular and hematologic responses to phlebotomy
in blood donors. Transfmion, 3, 83-93.
Lumley, M. A., & Melamed, B. G. (1992). Blood phobics and nonphobics: Psychological differences and affect
during exposure. Behaviour Research and Therapy, 30, 425-434.
Marks, I. M. (1987). Fears, phobias, and rituals: Panic, anxiety, and their disordns. Oxford: Oxford University Press.
Marks, I. M. (1988). Blood-injury phobia: A review. Am&an Journal of Psychiatry, 145, 1207-1213.
Marks, I. M., & Herst, E. R. (1970). A survey of 1200 agoraphobics in Britain. Social Psychiatry, 5, 16-24.
Matchett, G., & Davey, G. C. L. (1991). A test of a disease-avoidance model of animal phobias. Be/&our
Research and Therapy, 29, 91-94.
Mattick, R. P., Page, A. C., & Lampe, L. (in press). Cognitive and behavioural theories and treatments of
social phobia. In M. B. Stein (Ed.), Social phobia: Clinical and research pcrspectiocs. Washington, DC: American Psychiatric Press.
McHenry, L. C., Fazekas, J. F., & Sullivan, J. F. (1961). Cerebral hemodynamics of syncope. Amian Journal
of Medical Science, 241, 173- 179.
McNally, R. J. (1990). Psychological approaches to panic disorder: A review. Psychological Bulletin, 108, 403-
419.
Mower, 0. H. (1950). Learning theory and the personality dynamics. New York: Arnold Press.
Nimmer, W. H., & Kapp, R. A. (1974). A multiple impact program for the treatment of injection phobias. Journal of Behaviour Therapy and Experimental Psychiatry 5, 257-258.
Ogata, H., Iinuma, N., Nagashima, K., & Akabane, T. (1980). Vasovagal reactions in blood donors. Tram&-
sion, 20, 679-683.
Ost, L-G. (1991). Acquisition of blood and injection phobia and anxiety response patterns in clinical patients. Behaviour Research and Therapy, 29, 323-332.

460 A. C. Page
Ost, L-G. (1992). Blood and injection phobia: Background and cognitive, physiological, and behavioral vari- ables. JOUTW~ of Abnoml Psychology, 101, 68-74.
Ost, L-G., Fellenius, J., & Sterner, U. (1991). Applied tension, exposure in viva, and tension only in the
treatment of blood phobia. Behmiour Research and Therapy, 29, 561-574.
Ost, L-G., & Hugdahl, K. (1985). Acquisition of blood and dental phobia and anxiety response patterns in clinical patients. Behaviour Research and Thnapy, 23, 27-34.
Ost, L-G., Lindahl, I-L, Sterner, U., & Jerremalm, A. (1984). Exposure in viva vs. applied relaxation in the
treatment of blood phobia. Behaviour Research and Therapy, 22, 205-216.
Ost, L-G., & Sterner, U. (1987). A specific behavioral method for treatment of blood phobia. Behaoiour Research
and Therapy, 25, 25-29.
Ost, L-G., Sterner, U., & Fellenius, J. (1989). Applied tension, applied relaxation, and the combination in the
treatment of blood phobia. Behaoiour Research and Therapy, 27, 109-121.
Ost, L-G., Sterner, U., & Lindahl, I-L. (1984). Physiological responses in blood phobics. Behaviour Research and
Therapy, 22, 109-117.
Page, A. C. (1991). Simple phobias. Zntemational Review of Psychiatry, 3, 175-188.
Page, A. C. (1993). Don’tpanic: Overcoming anxie&, phobias, and tension. Sydney: Gore and Osment.
Papp, L. A., Klein, D. F., & German, J. M. (1993). Carbon dioxide sensitivity, hyperventilation, and panic disorder. American Journal of Psychiatry, 150, 1149- 1157.
Phillips, K., Fulker, D. W., & Rose, R. J. (1987). Path analysis of seven fear factors in adult twin pairs and sibling pairs and their parents. Genetic Epidemiolo~, 4, 345-355.
Poles, F. C., & Boycott, M. (1942). Syncope in blood donors. Lance& 2, 531-535.
Rachman, S. (1991). Neo-conditioning theory and the classical theory of fear acquisition. Clinical Psychology
Review, 11, 155-174.
Roddie, I. C. (1977). Human responses to emotional stress. Irish JournalMedical Science, 146, 395-417.
Rose, R. J., & Ditto, B. (1983). A development-genetic analysis of common fears from early adolescence to early adulthood. Child Development, 54, 361-368.
Rozin, P., & Fallon, A. E. (1987). A perspective on disgust. Psychological Review, 94, 23-41.
Rozin, P., Fallon, A. E., & Mandell, R. (1984). F amily resemblance in attitude to foods. Developmental Psychol-
ogy, 21,1075-1079.
Rozin, P., Millman, C., & Nemeroff, C. (1986). Operation of the laws of sympathetic magic in disgust and
other domains. Journal of Personality and Social Psychology, 50, 703-712.
Ruetz, P. P., Johnson, S. A., Callahan, R., Meade, R. C., & Smith, J. J. (1967). Fainting: A review of its
mechanisms and a study in blood donors. Medicine, 46, 363-384.
Sanford, P. A. (1982). Digestive systemphysiolou. London: Edward Arnold.
Schmidt, R. T. (1975). Personality and fainting. Journal of Psychosomatic Research, 19, 21-25.
Scott, T. R. (1992). Taste, feeding, and pleasure. Propess in Psychobiology and Physiological PsychololLy 15, 231-
291.
Skre, I., Onstad, S., Torgersen, S., Lygren, S., & Kringlen, E. (1993). A twin study of DSM-III-R anxiety
disorders. Acta Psychiatra Scandinavica, 88, 85-92.
Sledge, W. H. (1978). Antecedent psychological factors in the onset ofvasovagal syncope. Psychosomatic Medicine,
40,568-579.
Steptoe, A., & Wardle, J. (1988). Emotional fainting and the psychologic response to blood and injury: Autonomic mechanisms and coping strategies. Psychosomatic Medicine, 50, 402-417.
Subcommittee of the Blood Transfusion Research Committee. (1944). Fainting in blood donors. British Medical
Journal, 1, 279-283.
Taylor, C. B., Ferguson, J. M., & Wermuth, B. M. (1977). Simple techniques to treat medical phobias.
Postpaduate Medical Journal, 53, 28-32.
Thyer, B. A., &Curtis, G. C. (1985). On the diphasic nature ofvasovagal fainting associated with blood-injury-
illness phobia. Paolooian Journal of Biological Science, 20, 84-87.
Thyer, B. A., Himle, J., & Curtis, G. C. (1985). Blood-injury-illness phobia: A review. Journal of Clinical
Psychology, 41, 45 l-459. Torgersen, S. (1979). The nature and origin of common phobic fears. British Journal of Psychiatry, 134, 343-351.
Vingerhoets, A. J, J. M. (1984). Biochemical changes in two subjects succumbing to syncope. Psychosomatic
Medicine, 46, 95-103. Wardle, J., & Jarvis, M. (1981). The paradoxical fear response to blood, injury and illness-A treatment
report. Behavioural Psychotherapy, 9, 13-24. Wallin, B. G., & Sundlof, G. (1982). Sympathetic outflow to muscles during vasovagal syncope. Journal of the
Autonomic N~~VOW System, 6, 287-291. Weissler, A. M., Warren, J. V., Estes, E. H., McIntosh, H. D., & Leonard, J. J. (1957). Vasodepressor
syncope: Factors affecting cardiac output. Circulation, 15, 875-882.

Blood-Injury Phobia 461
Wolpe, J., & Lang, P. J. (1964). A fear survey schedule for use in behaviour therapy. Bchaviour Research and Therapy, 2, 27-30.
World Health Organization (1991). Tlu intemationalclarsification of diseases (10th cd.). Geneva: Author.
Yule, W., & Fernando, P. (1980). Blood phobia-beware. Bchaviour Research and Therapy, 18, 587-590.