burn injury
TRANSCRIPT
BURN INJURY
Budhi Arifin Noor, Dion Ade Putra, Oktaviati, Ridho Ardhi Syaiful, RizkyAmaliah, MursidTranslator: Adrian Salim, Andrio Wishnu Prabowo, Arnetta Naomi L. Lalisang,Julistian, Muliyadi, Sony Sanjaya, Stefanny, Zamzania Anggia Shalih.
General Surgery Department, FKUI/RSCM, Jakarta, Indonesia, May 2011.
CASE ILLUSTRATIONA man, 43 years old came with complaint of burn injury 8 hoursbefore hospital admission. The patient was exposed to flamesparks on the face, body and both upper trunk while working asa construction worker. Patient was holding steel when thesteel was exposed to electrical wires and caused fire. Thepatient was unconscious for 5 minutes and taken to a privatehospital, there patient treated with MEBO, RL 1 kolf infusion,urinary catheters, anti-tetanus and analgesics. The patientwas then referred to the RSCM due to limited facility.
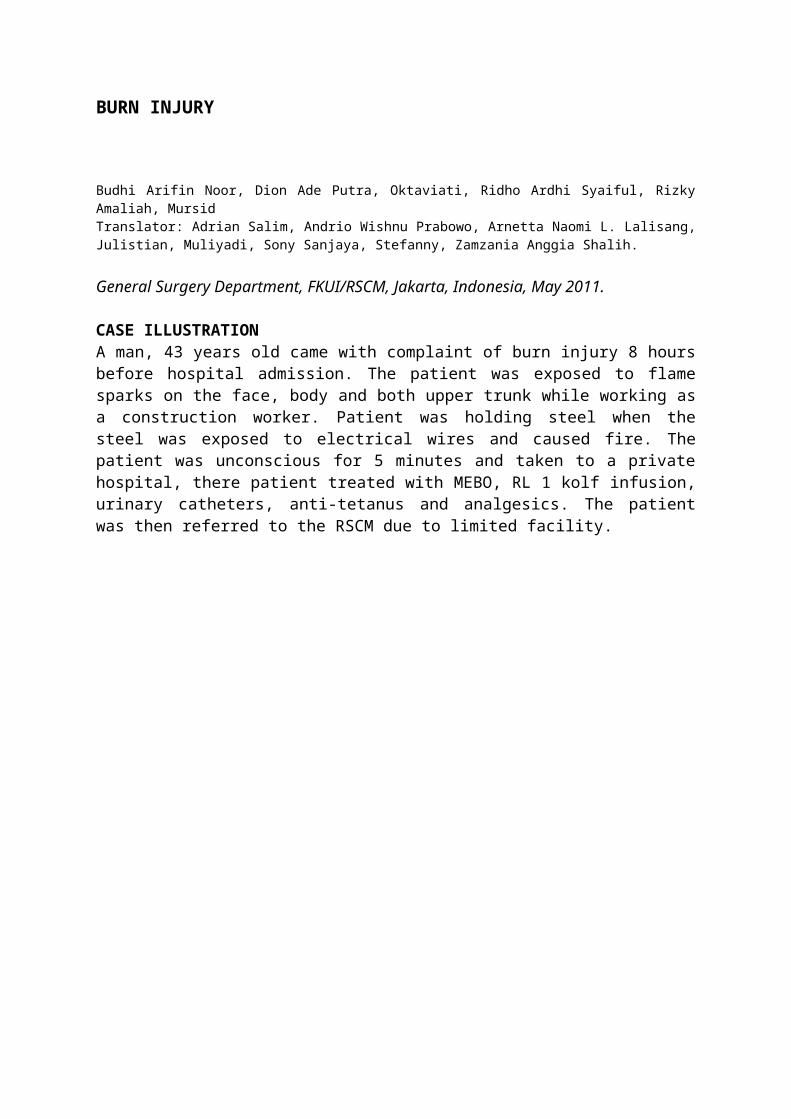
The primary survey during physical examination was clearairway, spontaneous breathing, vital signs was within normallimits, with GCS 15 (E4M6V5), and on secondary survey therewas found burn wounds on the face, neck and chest (see localstatus). Other physical examinations were within normal limitswith height 165 cm, and weight 62 kg. Laboratory tests resultshowed hemoglobin level of 12.2 g / dL, hematocrit 35%,leukocytes 10,480 / ul, 82.2 fl platelets, albumin 2.2, randomblood glucose 152 mg / dl, procalsitonin 16.06 and otherlaboratory results within normal result. The diagnosis forthis patient was second degree burn injury 37.5% wide.
Patient was treated with fluid resuscitation (37.5 x 4 x 62)9300 ml, 4650 ml within the first 8 hours, and continued with4650 ml in the next 16 hours and then titrated until the urineoutput reached 0.5 to 1 ml / kg / hour. Patients were alsogiven co-amoksiklav injection of 3 x 1 gram, ketorolac
injection of 3 x 300 mg, ranitidine injection of 3 x 150 mg,and vitamin E injection of 1 x 400 mg. Patients were thenconsulted to anesthesiologist for CVP installation. After 1day of treatment in the ER patients were then moved to theRSCM Burn Unit.
LITERATURE REVIEW
Burn injuries can be caused by fire, exposure to hightemperature such as the sun, electrocution, chemicals andradiation. Most of burn injuries admitted to RSCM are causedby fire with 56% of the total case, 40% of boiling water, 3%of electrocution and 1% of chemicals.5
I. PATHOPHYSIOLOGY Areas of burn wounds are divided into three zones, which arecoagulation zone, stasis zone and hyperemic zone.1,2
a. Coagulation zone The tissue in this zone is irreversibly damaged during traumatic burn.b. Stasis zone There are moderate perfusion disturbances in the area surrounding the necrotic zone. In the stasis zone, there is vascular damage thus causes vascular leakage. c. Hyperemic zone The character of the hyperemic zone is vasodilatation due to inflammation process.
Burn Injury Phases5
Acute Phase / shock phase. The patients may experiencedisturbance in the airway, breathing and circulation.
Sub-acute phase, which takes place after the shock phaseis resolved. Lost or damaged tissue resulting fromcontact with the heat source will cause inflammatoryprocess with exudation of plasma protein and infectionthat can cause sepsis.
Late Phase occurred after wound closure until maturation.The problem that arises during this phase are scarring,contractures and deformities due to the fragility oftissue or structured organ.
II. DIAGNOSISa. Total burn surface area can be evaluated with:i. Palmar surface method : the patient’s palmar (includingthe fingers)
measured as 1% of Total Body Surface Area (TBSA). ii. Wallace’s Rule Of Nineiii. Lund and Browder charts: to measure body shape differencesin patient
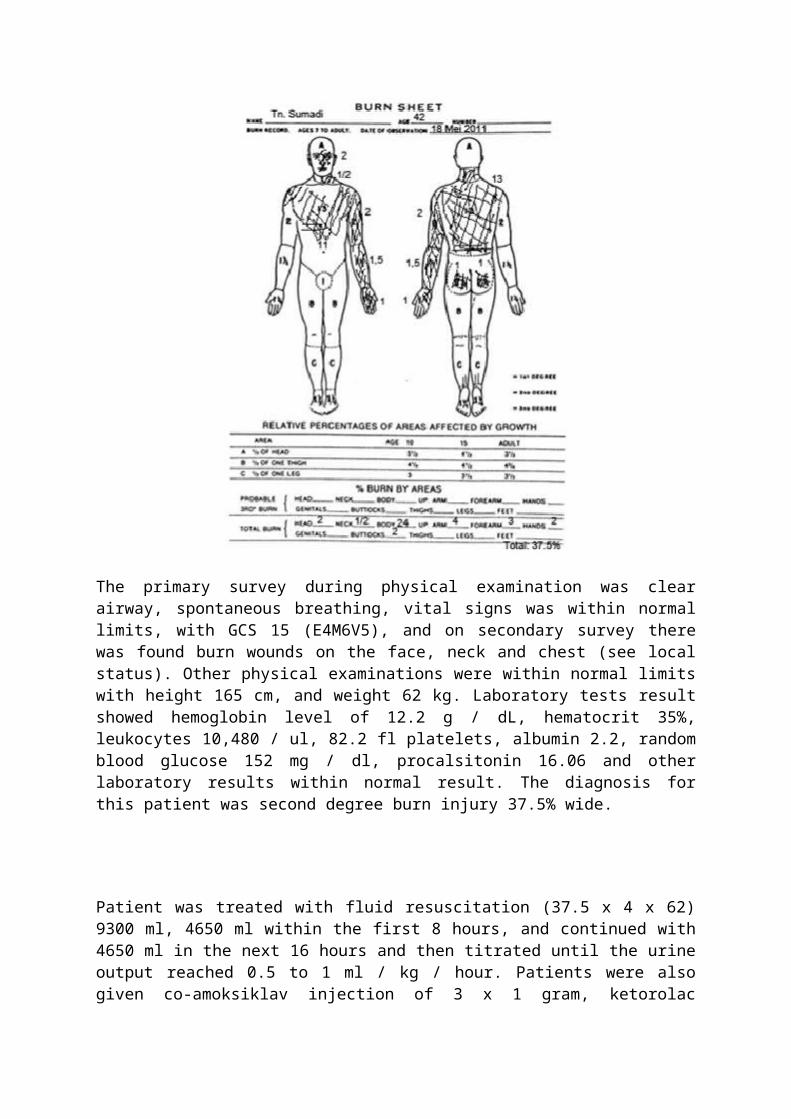
age and asses precise score in burn children.b. Age : Infant, children, and adultc. Burn Wound Depthd. Circumferential Grade II and III Burn Injury cause blood
flow restriction at extremities, disturb respiration process if located at
chest, therefore escharotomy is needed.
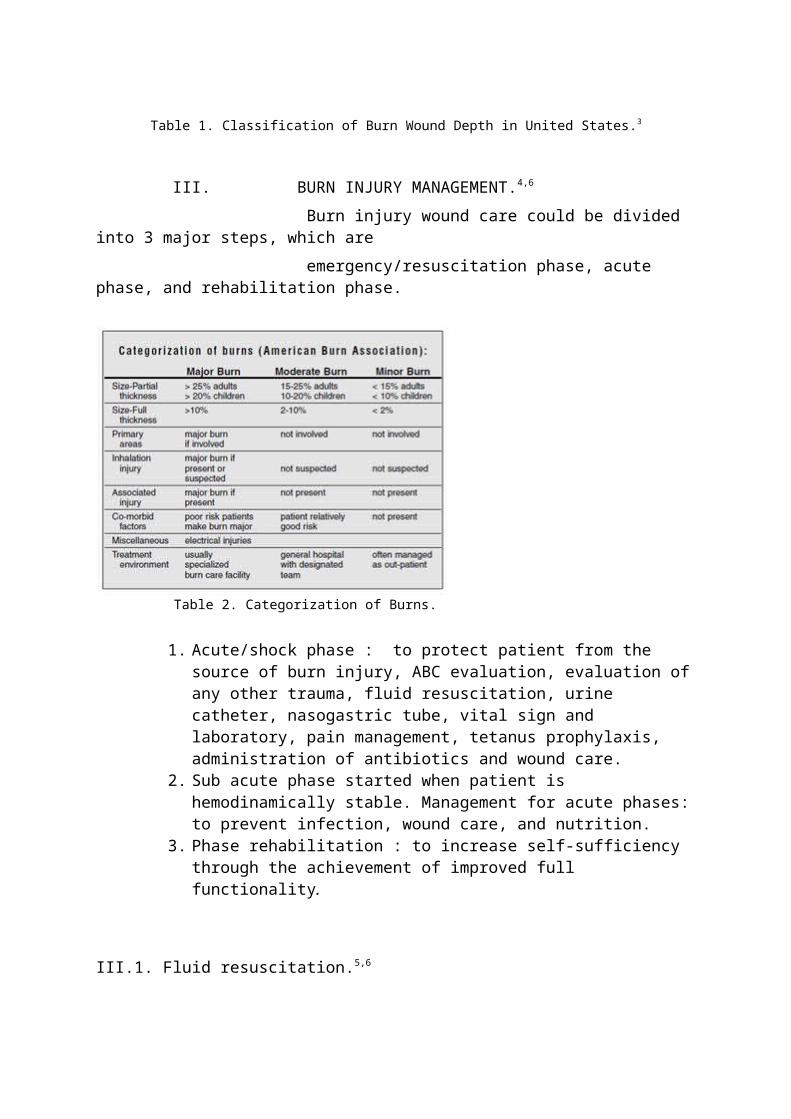
Table 1. Classification of Burn Wound Depth in United States.3
III. BURN INJURY MANAGEMENT.4,6
Burn injury wound care could be divided into 3 major steps, which are emergency/resuscitation phase, acute phase, and rehabilitation phase.
Table 2. Categorization of Burns.
1. Acute/shock phase : to protect patient from the source of burn injury, ABC evaluation, evaluation ofany other trauma, fluid resuscitation, urine catheter, nasogastric tube, vital sign and laboratory, pain management, tetanus prophylaxis, administration of antibiotics and wound care.
2. Sub acute phase started when patient is hemodinamically stable. Management for acute phases:to prevent infection, wound care, and nutrition.
3. Phase rehabilitation : to increase self-sufficiency through the achievement of improved full functionality.
III.1. Fluid resuscitation.5,6
III.2. Indication for fluid therapyGrade 2 or 3 > 25% in adult, burn injury in the face withinhalation trauma and if the patient can not drink. Whereas inchildren and elderly burn injury grade II or III >15%, theintravenous fluid resuscitation is generally required.
Baxter formula
First day : TBSA x body weight (kg) x 4 cc (RL) Second day : coloid : 500-2000cc + glucose 5% to maintain
the fluid.Half the fluid volume is given in the first 8 hours andanother halfis given in the next 16 hours.
III.3. Indications for hospitalization- Grade 2 over 15% in adults and over 10% in children - Grade 2 on the face, hands, feet and perineum - Grade 3 more than 2% in adults and every grade 3 in
children- Burns with viscera trauma, bones and airway
III.4. Wound management.5,7
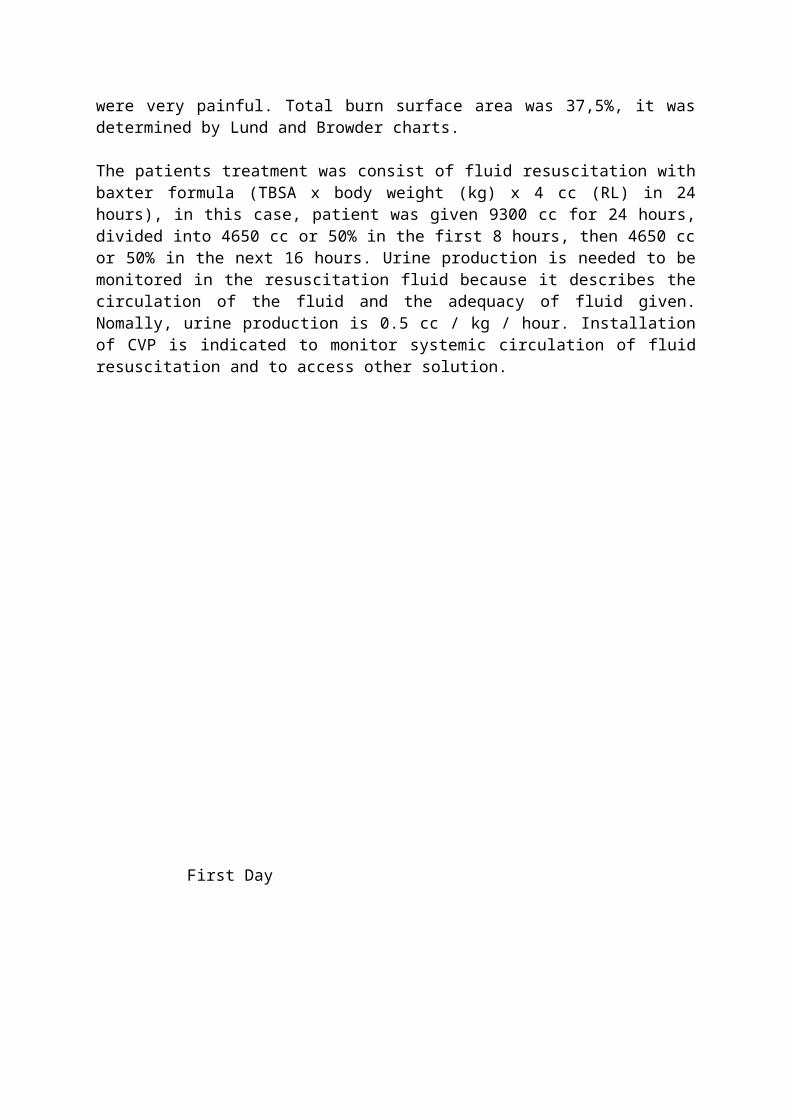
First burn wound should be washed with a solution of dilutedetergent (baby soap), debride the skin that has been damaged.Dry the wound and apply mecurochrom or silver sulfa diazine.In handling the wound required protective material to createan optimal environment for wound healing, protect the woundfrom bacteria, from the friction and absorb the exudat, thisis what we called dressing. There are many kinds of dressings,starting from the traditional (honey) conventional/passiveocclusive dressing (opened: mebo cream, silversulfadiazinecream; closed: wet gauze, dry gauze, pembebatan) moderndressing/active occlusive dressing (absorbent cellulosicmaterial, tulle grass dressing and film dressing).
IV. DISCUSSIONIn this patient, the diagnosis of Burn injury Grade II A-B wasupheld on the grounds that the injuries occurred on dermis;there were blisters, and reddish white colored injury that
were very painful. Total burn surface area was 37,5%, it wasdetermined by Lund and Browder charts.
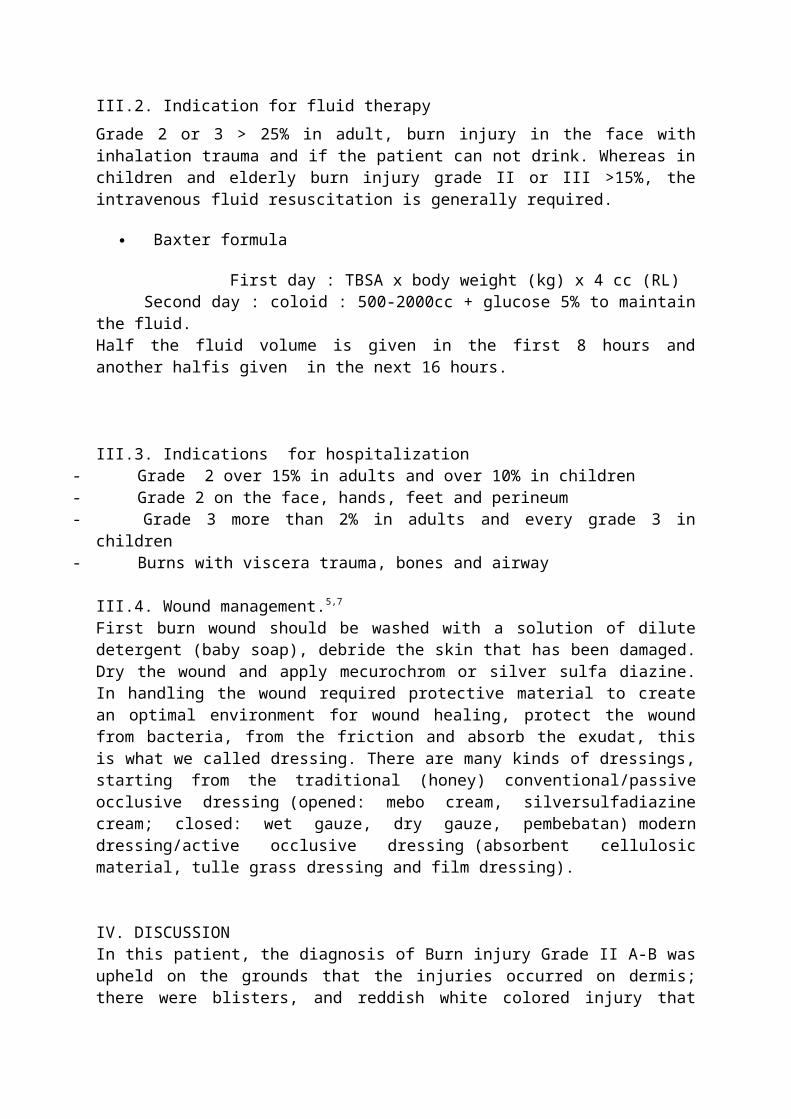
The patients treatment was consist of fluid resuscitation withbaxter formula (TBSA x body weight (kg) x 4 cc (RL) in 24hours), in this case, patient was given 9300 cc for 24 hours,divided into 4650 cc or 50% in the first 8 hours, then 4650 ccor 50% in the next 16 hours. Urine production is needed to bemonitored in the resuscitation fluid because it describes thecirculation of the fluid and the adequacy of fluid given.Nomally, urine production is 0.5 cc / kg / hour. Installationof CVP is indicated to monitor systemic circulation of fluidresuscitation and to access other solution.
First Day
Wound dressing
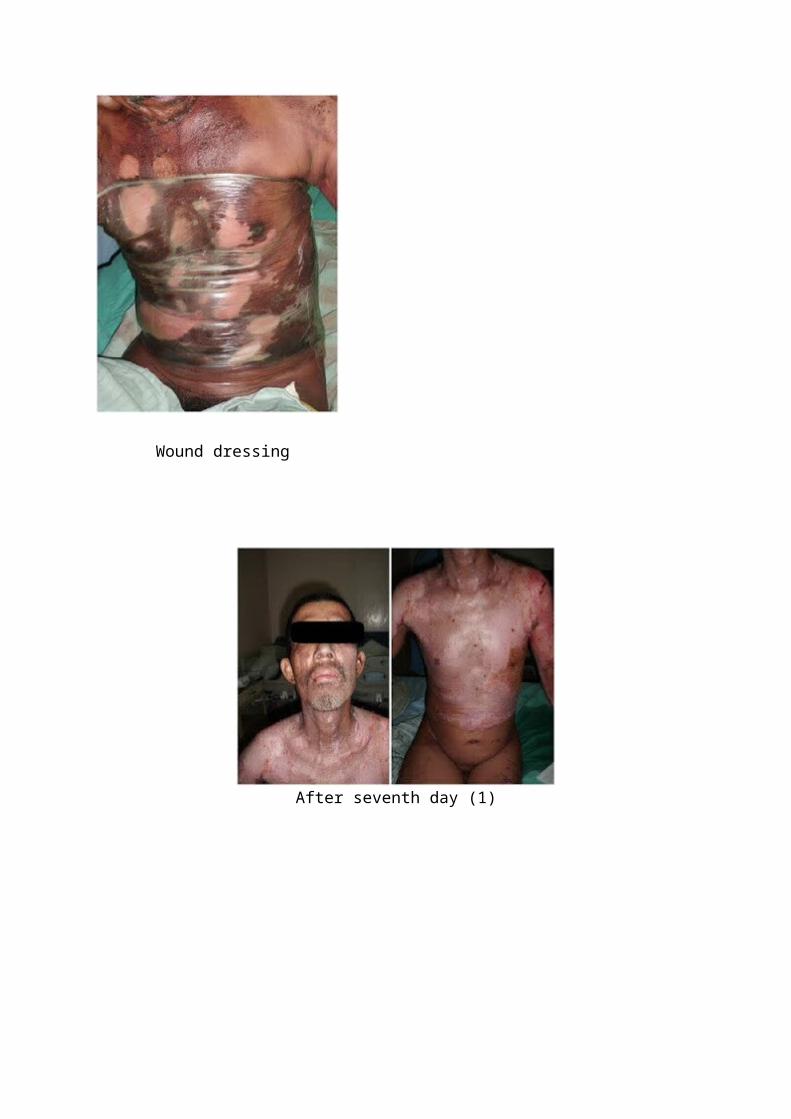
After seventh day (1)
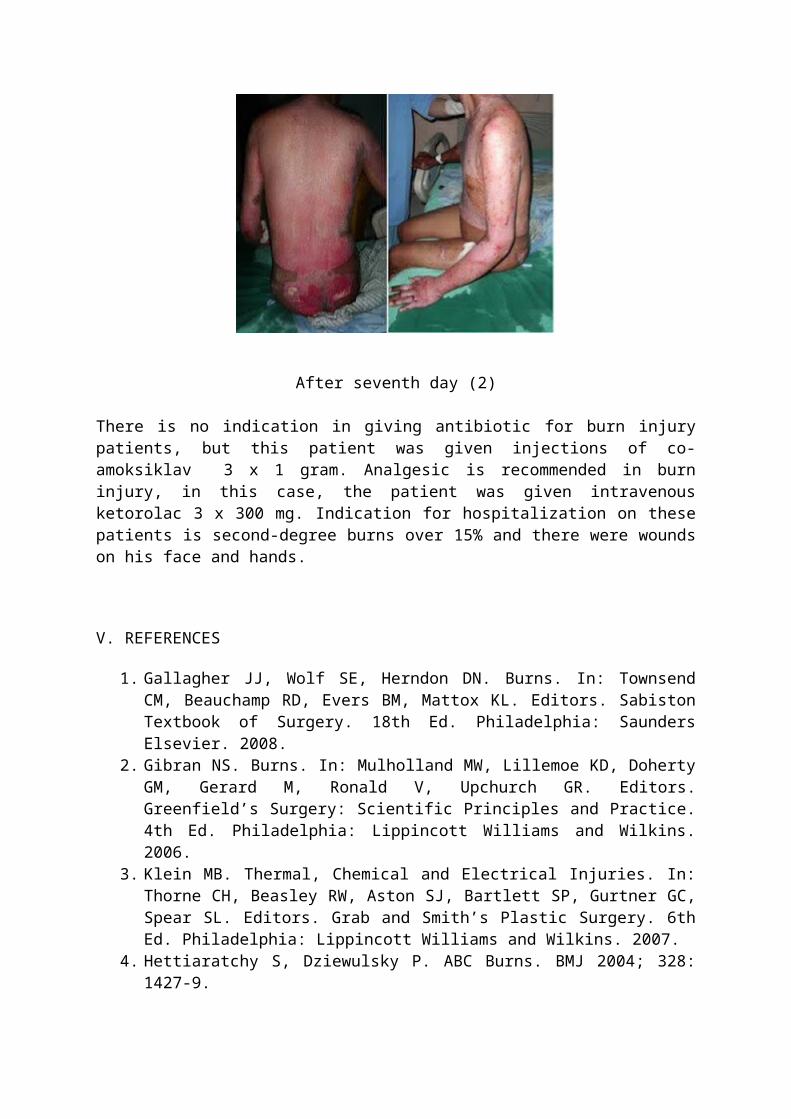
After seventh day (2)
There is no indication in giving antibiotic for burn injurypatients, but this patient was given injections of co-amoksiklav 3 x 1 gram. Analgesic is recommended in burninjury, in this case, the patient was given intravenousketorolac 3 x 300 mg. Indication for hospitalization on thesepatients is second-degree burns over 15% and there were woundson his face and hands.
V. REFERENCES
1. Gallagher JJ, Wolf SE, Herndon DN. Burns. In: TownsendCM, Beauchamp RD, Evers BM, Mattox KL. Editors. SabistonTextbook of Surgery. 18th Ed. Philadelphia: SaundersElsevier. 2008.
2. Gibran NS. Burns. In: Mulholland MW, Lillemoe KD, DohertyGM, Gerard M, Ronald V, Upchurch GR. Editors.Greenfield’s Surgery: Scientific Principles and Practice.4th Ed. Philadelphia: Lippincott Williams and Wilkins.2006.
3. Klein MB. Thermal, Chemical and Electrical Injuries. In:Thorne CH, Beasley RW, Aston SJ, Bartlett SP, Gurtner GC,Spear SL. Editors. Grab and Smith’s Plastic Surgery. 6thEd. Philadelphia: Lippincott Williams and Wilkins. 2007.
4. Hettiaratchy S, Dziewulsky P. ABC Burns. BMJ 2004; 328:1427-9.
5. Reksoprodjo S dkk (ed). Kumpulan Kuliah Ilmu Bedah.Jakarta: Binarupa Aksara Publisher.
6. Herndon, David N. Total Burn Care 3rd edition. SaundersElsevier.
7. Grunwald TB, Garner WL. Acute Burns Plast Reconstr Surg.2008(121):311.