biased processing of neutral facial expressions is associated with depressive symptoms and suicide...
TRANSCRIPT

�������� ����� ��
Biased processing of neutral facial expressions is associated with depressivesymptoms and suicide ideation in individuals at risk for major depression dueto affective temperaments
Roberto Maniglio, Francesca Gusciglio, Valentina Lofrese, Martino BelvederiMurri, Antonino Tamburello, Marco Innamorati
PII: S0010-440X(13)00309-XDOI: doi: 10.1016/j.comppsych.2013.10.008Reference: YCOMP 51170
To appear in: Comprehensive Psychiatry
Received date: 15 July 2013Revised date: 9 October 2013Accepted date: 14 October 2013
Please cite this article as: Maniglio Roberto, Gusciglio Francesca, Lofrese Valentina,Murri Martino Belvederi, Tamburello Antonino, Innamorati Marco, Biased processing ofneutral facial expressions is associated with depressive symptoms and suicide ideationin individuals at risk for major depression due to affective temperaments, ComprehensivePsychiatry (2013), doi: 10.1016/j.comppsych.2013.10.008
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Biased processing of neutral facial expressions is associated with depressive
symptoms and suicide ideation in individuals at risk for major depression due to
affective temperaments
Roberto Maniglioa, Francesca Gusciglio
b, Valentina Lofrese
b, Martino Belvederi
Murrid, Antonino Tamburello
b,c, Marco Innamorati
b,c,d
a University of Salento, Italy
b European University of Rome, Italy
c Skinner Institute, Naples, Italy
d University of Parma, Italy
Corresponding author. Roberto Maniglio, Psy.D., Ph.D., Department of History,
Society, and Human Studies, University of Salento, Via Stampacchia 45/47, 73100
Lecce, Italy. E-mail address: [email protected]
Short title: Emotion processing and affective temperaments
Key words: depression; suicide; affective temperaments; facial emotion processing;
etiology; risk factors
Word count for text only: 3,258

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Abstract
Background: To elucidate whether abnormal facial emotion processing represents a
vulnerability factor for major depression, some studies have explored deficits in
emotion processing in individuals at familial risk for depression. Nevertheless, these
studies have provided mixed results. However, no studies on facial emotion processing
have been conducted in at-risk samples with early or attenuated signs of depression,
such as individuals with affective temperaments who are characterized by subclinical
depressive moods, cognitions, and behaviors that resemble those that occur in patients
with major depression.
Methods: Presence and severity of depressive symptoms, affective temperaments,
death wishes, suicidal ideation, and suicide planning were explored in 231 participants
with a mean age 39.9 years (SD = 14.57). Participants also completed an emotion
recognition task with 80 emotional face stimuli expressing fear, angry, sad, happy, and
neutral facial expressions.
Results: Participants with higher scores on affective temperamental dimensions
containing a depressive component, compared to those with lower scores, reported more
depressive symptoms, death wishes, suicide ideation and planning, and an increased
tendency to interpret neutral facial expressions as emotional facial expressions; in
particular, neutral facial expressions were interpreted more negatively, mostly as sad
facial expressions. However, there were no group differences in identification and
discrimination of facial expressions of happiness, sadness, fear, and anger.
Conclusions: A negative bias in interpretation of neutral facial expressions, but not
accuracy deficits in recognizing emotional facial expressions, may represent a
vulnerability factor for major depression. However, further research is needed.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Introduction
A large amount of studies has reported abnormal processing of facial expressions of
emotions, especially a negative response bias in interpretation of facial expressions (i.e.
an increased tendency to interpret ambiguous, neutral, or other emotional expressions
negatively), in clinical and nonclinical samples of participants with major depression
(for reviews, see [1-3]).
However, it is unclear whether a biased processing of facial expressions of emotions
is a cause or an effect of depression [1]. To elucidate whether abnormal facial emotion
processing represents a vulnerability factor for major depression, some studies have
explored whether deficits and biases in the processing of facial expressions of emotions
are present in nonclinical samples of unaffected participants who are presumed to be at
risk for depression due to a family history of the illness. Nevertheless, these studies
have provided mixed results. Specifically, there is some evidence of an attentional bias
toward negative facial expressions [4-6] and emotion specific deficits in identification
and discrimination accuracy of facial expressions [7-9]; in contrast, evidence of a
negative bias in interpretation of ambiguous or neutral facial expressions is scant [9,10].
It is clear that further research is required. Importantly, future investigations should
address also other populations who may be at risk for depression, such as individuals
displaying early signs that resemble attenuated symptoms of the illness. In fact, these at-
risk samples of participants with early or attenuated signs of possible psychopathology
have been investigated by several studies aimed at exploring facial emotion processing
in other psychiatric disorders. For example, many of these studies have addressed
individuals considered at risk for schizophrenia, such as individuals from the general

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
population who demonstrate relatively high levels of schizotypy or signs that resemble
attenuated symptoms of schizophrenia and treatment-seeking individuals in the putative
prodrome to schizophrenia who are displaying early clinical signs of possible psychosis
(for a review, see [11]).
However, it is surprising that, to our knowledge, no studies on facial emotion
processing have been conducted in at-risk samples of participants with early or
attenuated signs of possible depression, such as individuals with affective
temperaments. In fact, individuals with temperaments containing a depressive
component (i.e. depressive, cyclothymic, and irritable temperaments, and, to a lesser
extent, anxious temperament) are characterized by some affective signs such as
subclinical depressive moods, cognitions, and behaviors (e.g., dejection, unhappiness,
irritability, low self-esteem, negativism, pessimism, hypercriticism, introversion,
dependency, shyness, insecurity, apathy, or low energy levels) that resemble those that
occur in patients with major depression [12]. Therefore, these affective temperaments
are considered to be subclinical manifestations and precursors of major depression [13].
In fact, research findings from several studies on both clinical and nonclinical
populations have shown that there is a continuum between affective temperaments and
affective disorders, clearly supporting that depressive, cyclothymic, and irritable
temperaments, and, to a lesser extent, anxious temperament, may play an important role
in the development of major depression (for reviews, see [12,14]).
Despite a considerable body of literature suggesting that individuals with affective
temperaments are at increased risk for depression, there is little understanding of the
factors and mechanisms that contribute to this elevated risk [14]. However, it is possible
to hypothesize that emotion processing might be related to affective temperaments,

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
given that emotions and temperaments are strictly related. In fact, affective
temperaments refer to the emotional domain of personality [14] and have a profound
and central role in emotional communication [13,15].
In sum, much more research on the etiology of depressive disorders is required in
order to implement prevention and treatment efforts, since depression can have adverse
effects on a person’s general health and quality of life [16]. In particular, depressed
people are at higher risk for suicidal ideation and behavior [17]. Awareness of these
negative effects should be reflected in the increase in research on risk factors for major
depression in order to understand how and why some people develop the illness.
To better understand the etiology of depression and implement research and
treatment strategies, it is important to clarify whether deficits and biases in facial
emotion processing represent a risk factor for major depression. Thus, for the first time,
the present study explored whether never-depressed individuals who were at risk for
depression due to significantly higher scores on affective temperamental dimensions
containing a depressive component differed from individuals with lower scores in the
processing of facial expressions of emotions.
Methods
The sample was composed of 231 participants (139 females and 92 males). All
participants were nonrandomly recruited from the general population between March
2012 and September 2012 through advertisement posted in established community
groups and university campuses located in Central and Southern Italy. Participants were
included if they were 18 years or older and provided written informed consent, while
they were excluded if they had a severe disabling condition or intellectual deficits

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
affecting the ability to take the assessment, such as a severe medical diagnosis, any
major disorder of the central nervous system (e.g., dementia), and current florid
psychotic symptoms. All participants completed the assessment on a voluntarily basis
without receiving any honorarium. The study design was approved from the local ethics
committee.
Psychometric measures
Participants were administered the Beck Depression Inventory – II (BDI-II [18]), the
Temperament Evaluation of Memphis, Pisa, Paris, and San Diego – auto-questionnaire
(TEMPS-A [19]), and the Suicidal History Self-Rating Screening Scale (SHSS [20]).
The BDI-II is a 21-item self-report inventory designed to assess the presence and
severity of depressive symptoms according to the DSM-IV criteria. Respondents have
to endorse specific statements that reflect their feelings over the last two weeks. Each
statement is rated on a 4-point Likert-type scale ranging from 0 to 3 on the basis of
symptom severity. In the current study, the Cronbach’s alpha was .90.
The TEMPS-A is a 110-item self-report measure of the affective temperament that
defines the bipolar spectrum, with depressive, cyclothymic, hyperthymic, irritable, and
anxious subscales [21]. The TEMPS-A has demonstrated to be not affected by current
mood state (e.g., depressive vs. manic), while it is able to reliably identify
temperamental profiles in psychiatric patients [22].
The SHSS is a 16-item (Yes/No) questionnaire developed to obtain information
about lifetime or past-year suicidal ideation, suicide planning, and suicide attempts. For
the present study the participants responded to items measuring death wishes (“Have
you ever felt tired of living or have you ever thought that life wasn’t worth living during

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
the last twelve months?” and “During the last twelve months, have you ever thought that
for you, for your family or for your friends, it would be better if you were dead?”),
suicidal ideation (“During the last twelve months, have you ever thought about taking
your own life?”), and suicide planning (“During the last twelve months, have you ever
planned a way of taking your own life?”) experienced in the past 12 months.
Cognitive task
Digitized color emotional face stimuli from the 2D Facial Emotional Stimuli
database [23] were used. Eighty stimuli expressing fear, angry, sad, happy, and neutral
facial expressions were presented to each participant. Eight stimuli at two different
levels of intensity (moderate intensity and full intensity) were presented for each
emotion and sex. Each trial consisted of a single stimulus presented for 10 s, and
participants were instructed to make mouse button presses with equal emphasis on
speed and accuracy to choose between five answers representing the classes of stimuli
presented. After the participant pressed the button, or after ten seconds from the
appearance of the stimulus, another stimulus was presented with an inter-trial-interval of
800±200 ms between two consecutive stimuli. Stimuli were presented with Affect 4.0
software for windows [24] using a portable PC with a 15 inches screen.
Statistical analysis
To measure prevalent affective temperaments, we calculated z-scores for all the
dimensions of the TEMPS-A. We considered prevalent the temperament having z-
scores of 1 or higher and being the highest in the profile of the individual. In this sense,
a participant had a prevalent affective temperament when he had scores on a specific

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
dimension of the TEMPS-A equal or greater than the mean plus 1 standard deviation
scores obtained by the whole sample.
To measure recognition accuracy of facial expressions of emotions, we computed
percentages of correct responses for each emotional category and also reported accuracy
in the recognition of emotional facial expression as deviation from the accuracy in the
recognition of neutral facial expression using the following formula:
[(% of correct responses for emotional stimuli) – (% of correct responses for neutral
stimuli) / % of correct responses for neutral stimuli] x 100.
Negative scores indicate that the participant is more accurate in recognizing neutral
facial expressions than the emotional ones, while positive scores indicate that the
participant is more accurate in recognizing emotional facial stimuli than the neutral
ones. Higher scores indicate greater differences in recognition accuracy of emotional
and neutral facial expressions.
In order to reveal temperamental groupings (or clusters) within the data set, we used
a two Step Cluster Analysis procedure. This procedure can handle categorical and
continuous variables, using a likelihood distance measure which assumes that variables
in the cluster model are independent. For the analysis, we let the procedure
automatically determine the number of clusters. One-way ANOVAs were used for
comparisons between groups of participants on dimensional variables and chi-squared
tests (χ2) were used for NxN contingency tables; post-hoc comparisons between pairs of
groups were performed with the Tamhane’s T2 procedure.
All the variables significant at the bivariate analysis were entered as independent
variables in a series of multinomial logistic regression analyses with the groups as
dependent variable. Odds ratios (OR) and their 95% confidence interval (95% CI) were

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
reported as measure of association. To reduce the problem of multicollinearity among
variables measured at the emotional test, those dimensions which were significant at the
bivariate analyses were inserted in a principal axis factoring analysis to extract common
factors explaining covariance among variables and factor scores were calculated and
used in the analyses.
Statistical analyses were performed with the Statistical Package for Social Sciences
for Windows 20.0 (IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM
Corp.).
Results
Characteristics of the sample
The mean age of the participants was 39.9 years (SD = 14.57; range: 47). In line with
the nonclinical nature of the sample, only 4.3% of the participants reported scores of 20
or higher on the BDI-II, suggestive of moderate to severe depression. Twenty-four
participants (10.4% of the sample) reported death wishes, 7 (3.0% of the sample)
reported suicidal ideation, and 3 (1.3% of the sample) reported suicide planning.
Regarding affective temperaments, while 54.5% of the sample had no prevalent
temperaments, 9.1% had a prevalent depressive temperament, 7.4% a cyclothymic
temperament, 10.0% a hyperthymic temperament, 8.2% an irritable temperament, and
10.8% an anxious temperament.
Factors associated with a dysregulated temperamental profile
The Two Step Cluster Analysis, performed to reveal natural groupings within the
participants’ response set, indicated a 3-cluster solution: the first group included 83

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
participants (35.9% of the sample), the second group 100 participants (43.3% of the
sample), and the third group 48 participants (20.8% of the sample). The three groups
differed for all the TEMPS-A dimensions with a depressive-dysregulated component
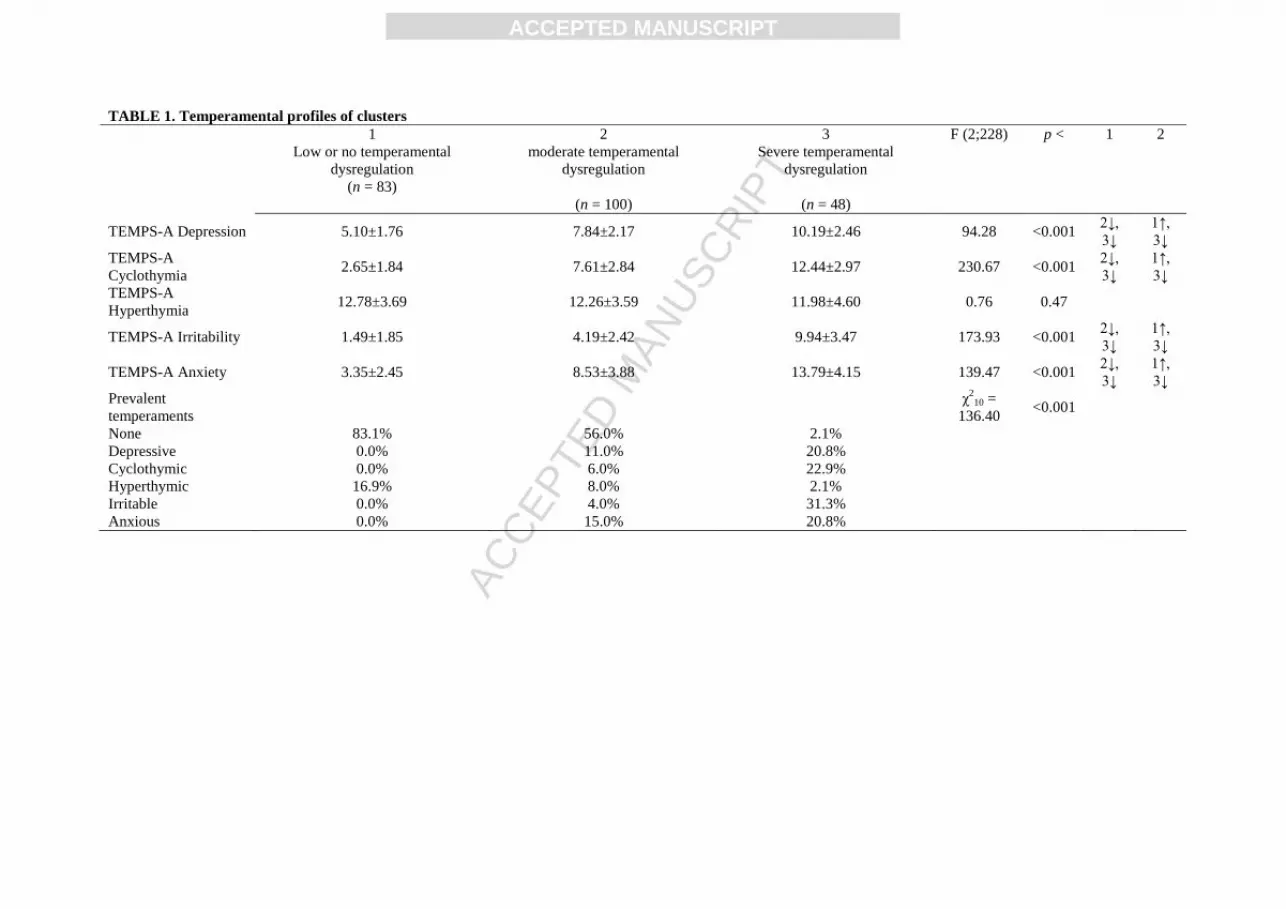
(depression, cyclothymia, irritability, and anxiety) but not for hyperthymia (Table 1).
Participants included in the first cluster reported low or no temperamental
dysregulation. They had significantly lower mean scores on all the temperaments with a
depressive-dysregulated component when compared to the other groups. No participants
included in this group had a prevalent dysregulated temperament. The second group
included participants with a moderate temperamental dysregulation. They had higher
mean scores on all the affective temperaments with a depressive-dysregulated
component when compared to the first group and lower mean scores when compared to
participants included in the third group. The third group included participants with a
more severely dysregulated depressive component; about 96% of them had a
dysregulated prevalent temperament.
Groups of participants with different temperamental profile differed for several
variables (see Tables 2-4), although they did not differ for sex and age. Compared to the
other groups, participants with severe temperamental dysregulation reported more
frequently death wishes, suicidal ideation, and suicide planning and more depressive
symptoms (Table 2).
Groups also differed for the accuracy in recognizing fear and happy facial
expressions (at full intensity) and neutral facial expressions (Table 3). Participants with
moderate temperamental dysregulation were more accurate than those with low or no
dysregulation in recognizing fear and happy facial expressions, while participants with

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
severe dysregulation were less accurate than those with moderate dysregulation in
recognizing neutral facial expressions.
When analyzing accuracy in recognizing emotional facial expressions as deviation
from accuracy in recognizing neutral facial expressions (Table 4), groups differed for
angry and fear facial expressions at their full intensity and for happy and sad facial
expressions at both moderate and full intensity. Participants with severe temperamental
dysregulation had the highest mean scores on all the categories, despite post-hoc
differences were significant only for comparisons between this group and participants
with moderate dysregulation for angry and sad facial expressions at their full intensity.
These analyses indicated that participants with low to moderate dysregulation were
similarly accurate when asked to recognize emotional and neutral facial expressions,
whereas participants with severe dysregulation were more accurate when asked to
recognize emotional facial expressions than when facing neutral facial expressions
which were interpreted as emotional facial expressions. Of nearly 1,500 errors in
interpreting neutral facial expressions, 64% were characterized by a negative
interpretative bias (i.e. neutral facial expressions were interpreted as sad facial
expressions) (not reported in the tables).
Multinomial logistic regression analyses with variables measuring accuracy in
recognizing emotional and neutral facial expressions that differentiated groups at the
bivariate analyses as independent variables and the groups as dependent variable (Table
5) indicated that participants with severe dysregulation, but not those with moderate
dysregulation (OR = 1.04; 95% CI = 0.99/1.02; p = 0.61), were less accurate in
recognizing neutral facial expressions than those with no or low dysregulation (OR =

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
0.98; 95% CI = 0.96/0.997; p < 0.05) even when controlling for the severity of current
depressive symptoms.
A principal factor analysis of variables measuring accuracy in recognizing emotional
facial expressions (reported as deviation from the accuracy in recognizing neutral facial
expressions) indicated the presence of a single latent factor with eigenvalue higher than
1 which explained 92.4% of the variability of the data. All the variables inserted in the
analysis loaded on this factor with loading of 0.91 and higher (not reported in the
tables). Multinomial logistic regression analysis with the factor measuring accuracy in
recognizing emotional facial expressions as deviation from the accuracy in recognizing
neutral facial expressions, BDI-II scores, and suicidality as independent variables and
groups as dependent variable (Table 6) indicated that participants with severe
temperamental dysregulation were 1.6 times more likely to have higher scores on this
factor (95% CI OR = 1.01/2.54; p < 0.05).
Discussion
This study was aimed to investigate whether abnormal facial emotion processing
represents a vulnerability factor for depression by investigating whether unaffected
individuals at risk for depression due to affective temperaments carrying a depressive
component are characterized by deficits and biases in recognition and interpretation of
facial expressions of emotions.
Participants with a more severely dysregulated depressive profile (i.e. higher scores
on affective temperaments containing a depressive component), compared to those with
low or moderate dysregulation, reported more depressive symptoms, death wishes, and
suicide ideation and planning. These results are consistent with literature revealing that

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
affective temperaments are significantly related to depression and suicidal behavior (for
reviews, see [12,14]). In particular, the results of the present study are consistent with
those from investigations suggesting that depression and/or suicidal ideation or behavior
are strongly related not only to depressive, cyclothymic, and irritable temperaments but
also to the anxious temperament (e.g. [25-29]). Since these affective temperaments
containing more or less of a depressive component provide a typical pattern of
cyclothymic-depressive-irritable-anxious temperamental constellation clearly associated
with depression and suicidal ideation or behavior, they represent a dysphoric-
dysregulated depressive profile.
Compared to participants with low temperamental dysregulation, participants with a
more severely dysregulated depressive component were not less accurate in recognizing
facial expressions of happiness, sadness, anger, and fear. A recent systematic review has
shown that evidence of reduced general or emotion-specific recognition accuracy of
facial emotion expressions is inconsistent, given that several studies have found no
group differences between depressed patients and healthy controls in identification and
discrimination of facial expressions of happiness, sadness, fear, anger, disgust, and
surprise [1]. Evidence of reduced identification accuracy of facial emotion expressions
is inconsistent also in studies on individuals at familial risk for depression [7-10]. In
fact, two studies have found that adult relatives of depressed patients did not differ from
controls in their identification and categorization of facial expressions of emotions with
varying intensities [8,10]. In contrast, two other studies have provided mixed results
[7,9]. Specifically, in one of these studies, high-risk girls, compared to low-risk girls,
needed more intensity to correctly identify sad expressions and made more errors when
identifying low-intensity angry expressions [7]. In the other study, high-risk boys, but

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
not high-risk girls, identified sadness at significantly lower levels of emotional intensity
than did their low-risk peers, while the high and low-risk groups did not differ with
regard to identification of anger [9].
However, in the present study, participants with severe affective temperament
dysregulation were less accurate in recognizing neutral facial expressions which were
interpreted as emotional facial expressions; in particular, neutral facial expressions were
interpreted more negatively, mostly as sad facial expressions. These results are
consistent with literature suggesting a negative response bias in interpretation of
ambiguous and neutral facial expressions in individuals with major depression, so that
neutral or ambiguous facial expressions tend to be evaluated as more sad or less happy
compared with healthy control groups (for a review, see [1]). Nevertheless, the only two
studies that, to our knowledge, have addressed the hypothesis of a negative
interpretative bias for ambiguous and neutral facial expressions in individuals at familial
risk for depression have found that relatives of depressed patients did not differ from
controls in their interpretation of ambiguous and neutral facial expressions [9,10].
In sum, the results of the present study do not support the hypothesis that accuracy
deficits in recognizing facial expressions of emotions may represent a risk factor for
major depression. In fact, at present, evidence of deficits in recognition accuracy of
facial emotion expressions in either individuals who have current or past diagnosis of
major depression or unaffected individuals at risk for depression is scant or conflicting.
Nevertheless, the results of the present study show that a negative bias in interpretation
of neutral facial expressions, specifically an increased tendency to interpret neutral
facial expressions negatively, may exist in individuals at risk for depression. As such,
this may represent a vulnerability factor for major depression.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Although the results of the present study may have important implications for the
development of appropriate prevention and treatment strategies, they should be
interpreted with caution and conclusions cannot be definitively drawn, given that, to our
knowledge, this is the first investigation of processing of facial expressions of emotions
in individuals with affective temperaments. Additionally, this study has some important
limitations, such as the use of a convenience sample and a cross-sectional design, that
might limit causal inferences and the generalizability of the findings. Therefore, further
research is needed. Importantly, since multiple biological, psychological, or social risk
factors contribute to the development of depressive symptoms and disorders [30-35],
future investigations should include facial emotion processing in more comprehensive,
multifactorial etiological models in order to explain how risk factors work together to
promote the onset and/or maintenance of major depression.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
Acknowledgments
This study has no external funding source and was not financial supported. The
authors report no financial interests, affiliations, conflicts of interest, or other
relationship relevant to the subject matter of this paper.
Author contributions: All authors had full access to all data in the study and take
responsibility for the integrity of the data and the accuracy of the data analysis. All
authors made substantial contributions to study concept and design, acquisition of data,
analysis and interpretation of data, drafting of the manuscript, critical revision of the
manuscript for important intellectual content, study supervision, and final approval of
the version to be published.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
References
[1]. Bourke C, Douglas K, Porter R. Processing of facial emotion expression in major
depression: a review. Aust N Z J Psychiatry 2010;44:681-696.
[2]. Kohler CG, Hoffman LJ, Eastman LB, Healey K, Moberg PJ. Facial emotion
perception in depression and bipolar disorder: a quantitative review. Psychiatry Res
2011;188:303-309.
[3]. Stuhrmann A, Suslow T, Dannlowski U. Facial emotion processing in major
depression: a systematic review of neuroimaging findings. Biol Mood Anxiety
Disord 2011;1:10.
[4]. Hankin BL, Gibb BE, Abela JRZ, Flory K. Selective attention to affective stimuli
and clinical depression among youths: role of anxiety and specificity of emotion. J
Abnorm Psychol 2010;119:491-501.
[5]. Joormann J, Talbot L, Gotlib IH. Biased processing of emotional information in
girls at risk for depression. J Abnorm Psychol 2007;116:135-143.
[6]. Kujawa A, Torpey D, Kim J, Hajcak G, Rose S, Gotlib I. et al. Attentional biases
for emotional faces in young children of mothers with chronic or recurrent
depression. J Abnorm Child Psychol 2011;39:125-135.
[7]. Joormann J, Gilbert K, Gotlib IH. Emotion identification in girls at high risk for
depression. J Child Psychol Psychiatry 2010;51:575-582.
[8]. Le Masurier M, Cowen PJ, Harmer CJ. Emotional bias and waking salivary cortisol
in relative of patients with major depression. Psychol Med 2007;37:403-410.
[9]. Lopez-Duran NL, Kuhlman KR, George C, Kovacs M. Facial emotion expression
recognition by children at familial risk for depression: high-risk boys are
oversensitive to sadness. J Child Psychol Psychiatry 2013;54:565-574.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
[10]. Mannie ZN, Bristow GC, Harmer CJ, Cowen PJ. Impaired emotional
categorisation in young people at increased familial risk of depression.
Neuropsychologia 2007;45:2975-2980.
[11]. Phillips LK, Seidman LJ, Emotion processing in persons at risk for schizophrenia.
Schizophr Bull 2008;34:888-903.
[12]. Vázquez GH, Gonda X. Affective temperaments and mood disorders: a review of
current knowledge. Curr Psychiatry Rev 2013;9:21-32.
[13]. Akiskal KK, Akiskal HS. The theoretical underpinnings of affective
temperaments: implications for evolutionary foundations of bipolar disorder and
human nature. J Affect Disord 2005;85:231-239.
[14]. Rihmer Z, Akiskal KK, Rihmer A, Akiskal HS. Current research on affective
temperaments. Curr Opin Psychiatry 2010;23:12-18.
[15]. Akiskal HS. Dysthymia, cyclothymia and related chronic subthreshold mood
disorders. In: Gelder M, Lopez-Ibor J, Andreasen N, editors. New Oxford Textbook
of Psychiatry. London: Oxford University Press; 2000:736-749.
[16]. IsHak WW, Greenberg JM, Balayan K, Kapitanski N, Jeffrey J, Fathy H. et al.
Quality of life: the ultimate outcome measure of interventions in major depressive
disorder. Harv Rev Psychiatry 2011;19:229-239.
[17]. Hawton K, Casañas I Comabella C, Haw C, Saunders K. Risk factors for suicide
in individuals with depression: a systematic review. J Affect Disord 2013;147:17-28.
[18]. Beck AT, Steer RA, Brown GK. Manual for the Beck Depression Inventory-II.
San Antonio: Psychological Corporation; 1996.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
[19]. Akiskal HS, Mendlowicz MV, Jean-Louis G, Rapaport MH, Kelsoe JR, Gillin JC,
et al. TEMPS-A: validation of a short version of a self-rated instrument designed to
measure variations in temperament. J Affect Disord 2005;85:45-52.
[20]. Innamorati M, Pompili M, Serafini G, Lester D, Erbuto D, Amore M, et al.
Psychometric properties of the suicidal history self-rating screening scale. Arch
Suicide Res 2011;15:87-92.
[21]. Akiskal HS, Akiskal KK. TEMPS: Temperament Evaluation of Memphis, Pisa,
Paris and San Diego. J Affect Disord 2005;85:1-2.
[22]. Akiskal HS, Akiskal KK, Haykal RF, Manning JS, Connor PD. TEMPS-A:
progress towards validation of a self-rated clinical version of the Temperament
Evaluation of the Memphis, Pisa, Paris, and San Diego Autoquestionnaire. J Affect
Disord 2005;85:3-16.
[23]. Gur RC, Ragland JD, Moberg PJ, Turner TH, Bilker WB, Kohler C, et al.
Computerized neurocognitive scanning: I. Methodology and validation in healthy
people. Neuropsychopharmacology 2001;25:766-776.
[24]. Spruyt A, Clarysse J, Vansteenwegen D, Baeyens F, Hermans D. Affect 4.0: a free
software package for implementing psychological and psychophysiological
experiments. Exp Psychol 2010;57:36-45.
[25]. Girardi P, Pompili M, Innamorati M, Serafini G, Berrettoni C, Angeletti G, et al.
Temperament, post-partum depression, hopelessness, and suicide risk among women
soon after delivering. Women Health 2011;51:511-524.
[26]. Pompili M, Innamorati M, Rihmer Z, Gonda X, Serafini G, Akiskal H, et al.
Cyclothymic-depressive-anxious temperament pattern is related to suicide risk in 346
patients with major mood disorders. J Affect Disord 2012;136:405-411.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
[27]. Rihmer A, Rozsa S, Rihmer Z, Gonda X, Akiskal KK, Akiskal HS. Affective
temperaments, as measured by TEMPS-A, among nonviolent suicide attempters. J
Affect Disord 2009;116:18-22.
[28]. Scuderi G, Pompili M, Innamorati M, Pasquale N, Pontremolesi S, Erbuto D, et al.
Affective temperaments are associated with higher hopelessness and perceived
disability in patients with open-angle glaucoma. Int J Clin Pract 2011;65:976-984.
[29]. Serafini G, Pompili M, Innamorati M, Fusar-Poli P, Akiskal HS, Rihmer Z, et al.
Affective temperamental profiles are associated with white matter hyperintensity and
suicidal risk in patients with mood disorders. J Affect Disord 2011;129:47-55.
[30]. Alloy LB, Abramson LY, Walshaw PD, Neeren AM. Cognitive vulnerability to
unipolar and bipolar mood disorders. J Soc Clin Psychol 2006;25:726-754.
[31]. Mandelli L, Serretti A. Gene environment interaction studies in depression and
suicidal behavior: An update. Neurosci Biobehav Rev 2013; doi:pii: S0149-
7634(13)00182-6. 10.1016/j.neubiorev.2013.07.011. [Epub ahead of print].
[32]. Maniglio R. Child sexual abuse in the etiology of depression: a systematic review
of reviews. Depress Anxiety 2010;27:631-642.
[33]. Maniglio R. The role of child sexual abuse in the etiology of suicide and non-
suicidal self-injury: a systematic review of reviews. Acta Psychiatr Scand
2011;124:30-41.
[34]. Mazure CM. Life stressors as risk factors in depression. Clin Psychol Sci Pract
1998;5:291-313.
[35]. Pompili M, Serafini G, Innamorati M, Möller-Leimkühler AM, Giupponi G,
Girardi P, et al. The hypothalamic-pituitary-adrenal axis and serotonin abnormalities:

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
a selective overview for the implications of suicide prevention. Eur Arch Psychiatry
Clin Neurosci 2010;260:583-600.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
TABLE 1. Temperamental profiles of clusters
1
Low or no temperamental
dysregulation
(n = 83)
2
moderate temperamental
dysregulation
(n = 100)
3
Severe temperamental
dysregulation
(n = 48)
F (2;228) p < 1 2
TEMPS-A Depression 5.10±1.76 7.84±2.17 10.19±2.46 94.28 <0.001 2↓,
3↓
1↑,
3↓
TEMPS-A
Cyclothymia 2.65±1.84 7.61±2.84 12.44±2.97 230.67 <0.001
2↓,
3↓
1↑,
3↓
TEMPS-A
Hyperthymia 12.78±3.69 12.26±3.59 11.98±4.60 0.76 0.47
TEMPS-A Irritability 1.49±1.85 4.19±2.42 9.94±3.47 173.93 <0.001 2↓,
3↓
1↑,
3↓
TEMPS-A Anxiety 3.35±2.45 8.53±3.88 13.79±4.15 139.47 <0.001 2↓,
3↓
1↑,
3↓
Prevalent
temperaments
χ210 =
136.40 <0.001
None 83.1% 56.0% 2.1%
Depressive 0.0% 11.0% 20.8%
Cyclothymic 0.0% 6.0% 22.9%
Hyperthymic 16.9% 8.0% 2.1%
Irritable 0.0% 4.0% 31.3%
Anxious 0.0% 15.0% 20.8%

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
TABLE 2. Differences between groups for depression scores and suicide ideation and wishes
Low or no temperamental
dysregulation
(n = 83)
Moderate temperamental
dysregulation
(n = 100)
Severe temperamental
dysregulation
(n = 48)
F (2;228) p < 1 2
Men 43.4% 37.0% 39.6% χ
22 =
0.77 0.68
Age 42.23±13.68 39.31±15.29 37.10±14.20 2.05 0.13
BDI-II 2.36±3.01 6.70±4.56 12.90±8.44 62.79 <0.001 2↓,
3↓
1↑,
3↓
SHSS 0.05±0.31 0.16±0.44 0.50±0.95 10.49 <0.001 3↓
Death wishes 2.4% 12.0% 20.8% χ
22 =
11.58 0.003
For family’s and friends’ sake, I have
better to be dead 1.2% 3.0% 12.5%
χ22 =
10.12 0.006
Suicidal ideation 1.2% 1.0% 10.4% χ
22 =
11.26 0.004
Suicidal planning 0.0% 0.0% 6.3% χ
22 =
11.59 0.003

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
TABLE 3. Accuracy in emotional stimuli recognition
Low or no temperamental
dysregulation
(n = 83)
Moderate temperamental
dysregulation
(n = 100)
Severe temperamental
dysregulation
(n = 48)
F
(2;228)
p < 1 2
Anger – moderate intensity 18.22±17.27 21.38±18.83 19.01±19.29 0.72 0.49
Anger – full intensity 83.28±15.03 79.88±15.17 78.91±17.52 1.57 0.21
Fear – moderate intensity 53.61±20.71 56.88±17.17 51.82±17.86 1.39 0.25
Fear – full intensity 72.14±23.37 80.63±19.49 73.70±21.30 3.99 0.05 2↓ -
Happiness – moderate
intensity
93.07±12.23 95.00±9.57 93.23±13.63 0.75 0.47
Happiness – full intensity 91.27±12.91 95.88±9.58 91.41±14.62 4.10 0.05 2↓ -
Neutral 67.62±24.60 71.44±21.36 56.25±28.68 6.45 0.01 - 3↑
Sadness – moderate intensity 70.78±18.34 71.63±18.45 72.40±25.13 0.10 0.90
Sadness – full intensity 78.16±20.18 75.75±19.45 79.43±23.84 0.60 0.55

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
TABLE 4. Accuracy in emotional stimuli recognition (as deviation from accuracy in recognition of neutral stimuli)
Low or no temperamental
dysregulation
(n = 83)
Moderate temperamental
dysregulation
(n = 100)
Severe temperamental
dysregulation
(n = 48)
F
(2;228)
p < 1 2
% of correct responses for anger –
moderate intensity -64.85±52.45 -62.27±65.15 -58.13±49.14 0.20 0.82
% of correct responses for anger – full
intensity 48.99±104.36 26.52±81.59 117.00±232.40 7.37 0.001 3↓
% of correct responses for fear – moderate
intensity -3.20±82.96 -7.35±68.68 26.39±105.97 2.83 0.06
% of correct responses for fear – full
intensity 23.05±70.53 29.89±103.32 98.42±220.21 5.92 0.01
% of correct responses for happiness –
moderate intensity 65.40±106.96 57.51±155.98 148.25±247.65 5.25 0.01
% of correct responses for happiness – full
intensity 61.39±100.17 57.27±137.62 135.48±222.55 4.96 0.01
% of correct responses for sadness –
moderate intensity 23.45±78.06 17.00±101.53 105.34±261.88 6.62 0.01
% of correct responses for sadness – full
intensity 32.54±77.79 18.31±80.79 119.01±258.91 9.09 <0.001 3↓

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
TABLE 5. Multinomial regression analysis (group with low or no temperamental dysregulation is the reference category)
B Std. Error Wald df Sig.
Odds
ratio
95% Confidence
Interval for odds ratio
Lower
Bound
Upper
Bound
Moderate temperamental
dysregulation
BDI-II 0.32-0.35 0.06
31.89-
34.06 1 <0.001 1.38-1.41 1.24-1.26 1.55-1.59
Suicidality -0.30
–
-0.44
0.50-0.51 0.37-0.75 1 0.39-0.54 0.65-0.74 0.24-0.28 1.74-1.96
Fear – full intensity 0.02 0.01 4.04 1 0.05 1.02 1.00 1.03
Happiness – full intensity 0.05 0.02 7.87 1 0.01 1.05 1.01 1.08
Neutral 0.004 0.01 0.26 1 0.61 1.04 0.99 1.02
Severe temperamental
dysregulation
BDI-II 0.49-0.50 0.07-
53.79-
54.21 1 <0.001 1.63-1.65 1.43-1.45 1.86-1.89
Suicidality -0.40-
-0.44 0.55-0.56 0.52-0.64 1 0.42-0.47 0.64-0.67 0.22-0.29 1.91-1.98
Fear – full intensity 0.00 0.01 0.00 1 0.99 1.00 0.98 1.02
Happiness – full intensity 0.03 0.02 1.85 1 0.17 1.03 0.99 1.07
Neutral -0.02 0.01 4.94 1 0.05 0.98 0.96 0.997
Model fitting criteria
Final models: -2 Log Likelihood = 191.23-239.79; Likelihood Ratio χ26 = 117.69-122.17; all significant for p < 0.001; Nagelkerke R
2 = 0.45-0.47.
Reduced models: BDI-II: -2 Log Likelihood = 285.20-391.06; Likelihood Ratio χ22 = 91.48-93.97; all significant for p < 0.001; Suicidality: -2 Log Likelihood =
191.96-297.74; Likelihood Ratio χ22
= 0.50-0.73; p = 0.70-0.78; Fearfull: -2 Log Likelihood = 245.61; Likelihood Ratio χ
22 = 5.83; p = 0.054; Happinessfull: -2 Log
Likelihood = 200.18; Likelihood Ratio χ2
2 = 8.95; p < 0.05; Neutral: -2 Log Likelihood = 307.52; Likelihood Ratio χ
22
= 10.31; p < 0.01.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
TABLE 6. Multinomial regression analysis (group with low or no temperamental dysregulation is the reference category)
B Std. Error Wald df Sig.
Odds
ratio
95% Confidence
Interval for odds ratio
Lower
Bound
Upper
Bound
Moderate temperamental
dysregulation
BDI-II 0.34 0.06 34.47 1 <0.001 1.41 1.26 1.58
Suicidality -0.37 0.51 0.55 1 0.46 0.69 0.26 1.85
Accuracy in emotional
recognition as deviation from
accuracy in the recognition of
neutral stimuli
-0.18 0.28 0.44 1 0.51 0.83 0.48 1.43
Severe temperamental
dysregulation
BDI-II 0.49 0.07 52.77 1 <0.001 1.64 1.43 1.87
Suicidality -0.31 0.56 0.31 1 0.58 0.73 0.25 2.19
Accuracy in emotional
recognition as deviation from
accuracy in the recognition of
neutral stimuli
0.47 0.23 4.01 1 0.05 1.60 1.01 2.54
Model fitting criteria
Final model: -2 Log Likelihood = 363.50; Likelihood Ratio χ2
6 = 117.84; p < 0.001; Nagelkerke R
2 = 0.46.
Reduced models: BDI-II: -2 Log Likelihood = 452.88; Likelihood Ratio χ2
2 = 89.38; p < 0.001; Suicidality: -2 Log Likelihood = 364.02; Likelihood Ratio χ
22 =
0.53; p = 0.77; Accuracy in emotional recognition as deviation from accuracy in recognition of neutral stimuli: -2 Log Likelihood = 371.75; Likelihood Ratio
χ2
2= 8.25; p = 0.05.