autologous bone marrow cells transplantation in patients with advanced critical limb ischemia: no...
TRANSCRIPT

1909
Cell Transplantation, Vol. 21, pp. 1909–1918, 2012 0963-6897/12 $90.00 + .00Printed in the USA. All rights reserved. DOI: http://dx.doi.org/10.3727/096368912X636948Copyright 2012 Cognizant Comm. Corp. E-ISSN 1555-3892 www.cognizantcommunication.com
Received June 13, 2011; final acceptance October 22, 2011. Online prepub date: April 2, 2012.Address correspondence to Juraj Madaric, M.D., Ph.D., Department of Cardiology and Angiology, National Cardiovascular Institute, Pod Krasnou horkou 1, 833 48 Bratislava, Slovakia. Tel: 00421259320276; E-mail: [email protected]
No Difference in Intra-Arterial and Intramuscular Delivery
of Autologous Bone Marrow Cells in Patients With
Advanced Critical Limb Ischemia
Andrej Klepanec,*† Martin Mistrik,‡ Cestmir Altaner,§ Martina Valachovicova,* Ingrid Olejarova,† Roman Slysko,† Tibor Balazs,† Terezia Urlandova,† Daniela Hladikova,† Branislav Liska,†
Jan Tomka,† Ivan Vulev,*† and Juraj Madaric*†
*Slovak Medical University, Bratislava, Slovakia
†National Cardiovascular Institute, Bratislava, Slovakia
‡Clinic of Haematology and Transfusiology, Faculty Hospital, Bratislava, Slovakia
§Institute of Experimental Oncology, Slovak Academy of Science, Bratislava, Slovakia
Stem cell therapy has been proposed to be an alternative therapy in patients with critical limb ischemia (CLI), not eligible for endovascular or surgical revascularization. We compared the therapeutic effects of intramuscular (IM) and intra-arterial (IA) delivery of bone marrow cells (BMCs) and investigated the factors associated with thera-peutic benefits. Forty-one patients (mean age, 66 ± 10 years; 35 males) with advanced CLI (Rutherford category, 5 and 6) not eligible for revascularization were randomized to treatment with 40 ml BMCs using local IM (n = 21) or selective IA infusion (n = 20). Primary endpoints were limb salvage and wound healing. Secondary endpoints were changes in transcutaneous oxygen pressure (tcpO
2), quality-of-life questionnaire (EQ5D), ankle–brachial
index (ABI), and pain scale (0–10). Patients with limb salvage and wound healing were considered to be respond-ers to BMC therapy. At 6-month follow-up, overall limb salvage was 73% (27/37) and 10 subjects underwent major amputation. Four patients died unrelated to stem cell therapy. There was significant improvement in tcpO
2
(15 ± 10 to 29 ± 13 mmHg, p < 0.001), pain scale (4.4 ± 2.6 to 0.9 ± 1.4, p < 0.001), and EQ5D (51 ± 15 to 70 ± 13, p < 0.001) and a significant decrease in the Rutherford category of CLI (5.0 ± 0.2 to 4.3 ± 1.6, p < 0.01). There were no differences among functional parameters in patients undergoing IM versus IA delivery. Responders (n = 27) were characterized by higher CD34+ cell counts in the bone marrow concentrate (CD34+ 29 ± 15×106 vs. 17 ± 12×106, p < 0.05) despite a similar number of total nucleated cells (4.3 ± 1.4×109 vs. 4.1 ± 1.2×109, p = 0.66) and by a lower level of C-reactive protein (18 ± 28 vs. 100 ± 96 mg/L, p < 0.05) as well as serum leukocytes (8.3 ± 2.1×109/L vs. 12.3 ± 4.5×109/L, p < 0.05) as compared with nonresponders (10 patients). Both IM and IA delivery of autologous stem cells are effective therapeutic strategies in patients with CLI. A higher concentration of CD34+ cells and a lower degree of inflammation are associated with better clinical therapeutic responses.
Key words: Autologous stem cells; Critical limb ischemia; Angiogenesis; Intramuscular delivery; Intra-arterial delivery
Several preclinical and clinical studies showed that
delivery of autologous bone marrow cells (BMCs) can
improve blood circulation and tissue perfusion and
thus prevent amputation via the induction of collat-
eral and capillary growth in a process called “thera-
peutic angiogenesis” (2,5,12,18,22,31,35). However,
the optimal route of administration of cells remains
unclear. Intra-arterial (IA) as well as intramuscular
(IM) delivery methods have shown promising results
in promoting neoangiogenesis (2,5,12,35), although
direct comparison between both routes of BMC deli-
v ery is lacking. Accordingly, we conducted a randomized
INTRODUCTION
Critical limb ischemia (CLI) is the end stage of periph-
eral arterial disease (PAD) characterized by ischemic rest
pain, ulcers, or gangrene, with a significant risk of loss
of the affected limb. The therapeutic options for patients
with failed endovascular or surgical revascularization or
in those in which these procedures cannot be carried out
(20–30% of CLI patients) are very limited. About 40%
of these high-risk patients will require amputation within
6 months of the initial diagnosis, whereas 20% will die
(23). The quality of life (QoL) of these patients is poor
and comparable to those with terminal cancer (1).

1910 KLEPANEC ET AL.
clinical study to compare IM versus IA delivery of autol-
ogous BMCs in “no-options” patients with advanced CLI.
To understand the underlying mechanism of the thera-
peutic effects of stem cells, we sought to address fac-
tors associated with therapeutic benefit in response to
cell therapy.
MATERIALS AND METHODS
Patients
Between October 2009 and August 2010, 41 patients
(mean age, 66 ± 10 years; 35 males) with advanced CLI
(Rutherford category, 5 or 6) after failed or impossible
revascularization were randomized to application of 40 ml
of bone marrow concentrate via the local IM route (n = 21)
or via selective IA infusion (n = 20).
Inclusion Criteria. (1) Patients over 18 years of age
with ischemic skin lesions (ulcers or gangrene) with
a CLI Rutherford category of 5 or 6 according to the
TransAtlantic InterSociety Consensus (TASC) classifica-
tion (minor or major tissue loss) (23). (2) CLI defined
by ankle–brachial index ≤ 0.4, or ankle systolic pressure
< 50 mmHg, or toe systolic pressure < 30 mmHg, or tran-
scutaneous oxygen pressure (tcpO2) < 30 mmHg. (3) No
option for endovascular or surgical revascularization
assessed by a vascular surgeon and interventionalist. (4)
Failed revascularization defined as no change of clinical
status with the best standard care 4 weeks after endovas-
cular or surgical revascularization.
Exclusion Criteria. (1) Life expectancy < 6 months.
(2) Evidence of malignancy during last 5 years. (3)
Proliferative retinopathy. (4) Critical coronary artery dis-
ease or unstable angina pectoris. (5) End-stage kidney
disease and patient on dialysis. (6) Bone marrow disease
(e.g., myelodysplastic syndrome, severe anemia, leuko-
penia, and thrombocytopenia).
Method of BMC Isolation. Isolation of stem cells
was undertaken under analgosedation with propofol. A
total of 240 ml of bone marrow from both posterior iliac
crests was harvested using a standard disposable needle
for bone marrow aspiration. Bone marrow aspirate was
processed using a SmartPreP2 Bone Marrow Aspirate
Concentrate System (Harvest, Plymouth, MA, USA),
which uses gradient density centrifugation to provide
40 ml of bone marrow-rich product for all blood ele-
ments within 15 min. The biological potential of this
system has been evaluated in a mouse model of hind-
limb ischemia with similar or greater functional activ-
ity compared with the Ficoll isolation procedure as the
current “gold standard” (10) and has also been tested in
several trials in patients with CLI (2,25).
Administration of Stem Cells. Immediately after the
harvesting and centrifugation of stem cells, BMCs were
administered by IM (group A) or IA (group B) methods.
In group A, 40 ml of BMCs were administered under anal-
gosedation with propofol by deep injections with a 23-G
needle into the muscles of the affected limb along the
crural arteries, with each injection being ~1 ml. In group
B, IA injection of 40 ml of BMCs was undertaken from
a percutaneous retrograde contralateral femoral approach
or antegrade femoral approach under local anesthesia at
the site of arterial occlusion of the affected limb using a
4-F catheter at 800 ml/h. The duration of procedures in
both groups was ~1 h.
Preprocedure Assessment and Follow-up. All patients
were examined before, 90 days, and 6 months after BMC
delivery. Peripheral blood tests such as blood count and
basal serological parameters (including C-reactive pro-
tein, CRP) were assessed. The total concentration of
mononuclear cells (BMMCs/MNCs) and CD34+ cells in
bone marrow concentrates was evaluated.
Digital subtraction angiography (DSA) was under-
taken 1 day before transplantation and 6 months after
transplantation with strictly fixed parameters of the
amount of contrast medium, constant speed of injec-
tion of contrast medium, catheter size, and position
of catheter tip. Two experienced operators evaluated
the development of new vessels in a blinded fashion
by semiquantitative analyses as reported elsewhere (31).
New collateral vessels were assessed as +0 (no develop-
ment of collateral vessels), +1 (slight), +2 (moderate),
or +3 (rich).
Measurement of the resting ankle–brachial index (ABI)
was done according to validated standards (27). It was cal-
culated as the quotient of the highest ankle pressure and
highest brachial systolic blood pressure (normal values,
0.95–1.2). Transcutaneous oxygen pressure (tcpO2) of the
affected limb was assessed using a TCM400 Mk2 moni-
tor (Radiometer Medical ApS, Copenhagen, Denmark).
TcpO2 was measured at the forefoot in the supine position
with an electrode temperature of 44°C. Wound character-
istics were documented by digital photography. Wound
healing was evaluated by two independent physicians.
Pain scale was measured with a visual analog scale (VAS)
graded form 0 to 10.
Patients were discharged the day after the procedure
on dual antiplatelet therapy (aspirin and clopidogrel) and
statin therapy. All patients received conventional wound
care during follow-up.
QoL before, 3 months, and 6 months after BMC appli-
cation was assessed by the EuroQol questionnaire (6).
Using a VAS, patients rated their overall health status
from 0 (“worst”) to 100 (“best”) imaginable health.
Endpoints. The primary endpoint was limb salvage and
improvement in wound healing within 6-month follow-up.
Patients with limb salvage and wound healing were con-
sidered to be responders to BMC therapy. Secondary

STEM CELL DELIVERY IN CRITICAL LIMB ISCHEMIA 1911
endpoints were change in tcpO2, Rutherford category,
QoL, and pain VAS after BMC transplantation.
The study design was approved by the local ethical
committee of National Cardiovascular Institute, Bratislava.
All included patients were informed about the nature of the
study and gave their written informed consent.
Statistical Analyses
Data evaluation was undertaken using a statistical
software package SPSS 13.0 (SPSS Inc., Chicago, IL,
USA). Discrete variables are presented as counts and
percentages. Continuous variables are presented as mean
values ± SD. Gaussian distributions of data were tested
by the Kolmogorov–Smirnov test. The paired t test was
used to compare values before and after BMC trans-
plantation. The frequencies of categorical variables
were compared using Fisher‘s exact test. Mean values
for continuous parameters were compared using the
Student‘s t test and Mann–Whitney test as appropriate.
Multivariate logistic regression analysis (binary logis-
tic regression) was used to study predictors of clinical
benefit after BMC application. For all analyses, p < 0.05
was considered significant.
RESULTS
Baseline Characteristics and Overall Results
The baseline characteristics of both groups are given
in Table 1. In all 41 patients, the underlying cause of
obstructive arterial disease was atherosclerosis. During
follow-up, four patients died (two due to heart failure,
one due to myocardial infarction, and one as a result of
pneumonia). At 6-month follow-up, the combined pri-
mary endpoint of limb salvage and wound healing was
met in 27 of the surviving 37 patients (73%). However,
in 10 patients, major amputation was required due to CLI
progression. Importantly, most cases of amputation (7/10)
happened during the first month after BMC delivery.
Table 2 shows the functional results of BMC appli-
cation in patients with limb salvage at 6 months in all
patients and that in the IA group and IM group. There was
significant improvement in wound healing, tcpO2, pain
scoring, and QoL, as well as in CLI Rutherford category
at 3-month follow-up, and the results were sustained or
even more pronounced at 6 months (Figs. 1 and 2).
DSA did not reveal detectable development of new
collateral vessels after 6 months compared with baseline
angiograms (grades 0 to +3: 0.21 ± 0.43) (Fig. 3).
Intramuscular Versus Intra-Arterial Application
Table 3 shows a comparison of functional outcomes
after IM and IA delivery of BMCs in patients with limb
salvage. Both procedures were well tolerated without
periprocedural complications. There were no differences
in IM versus IA application in either endpoint. The preva-
lence of limb salvage at 6 months was 72% in the IM
group compared with 74% in the IA group ( p = 0.94).
Similarly, wound healing was observed in 13 patients
(72%) in the IM group compared with 14 patients (74%)
Table 1. Baseline Characteristics of Patients
All Patients
(n = 41)
Group A
(IM, n = 21)
Group B
(IA, n = 20)
p
(IM vs. IA)
Age (years) 66 ± 10 66 ± 10 66 ± 11 0.86
Sex (males) 35 (85%) 17 (81%) 18 (90%) 0.41
Diabetes mellitus 28 (68%) 15 (71%) 13 (65%) 0.67
Arterial hypertension 33 (80%) 17 (81%) 16 (80%) 0.62
Hyperlipidemia 21 (51%) 13 (62%) 8 (40%) 0.96
BMI 28 ± 4 29 ± 4 26 ± 4 0.06
LVEF (%) 56 ± 8 60 ± 9 55 ± 7 0.43
Smoking 17 (41%) 9 (43%) 8 (40%) 0.85
Rutherford category 5.0 ± 0.2 5.0 5.1 ± 0.3 0.16
Creatinine (µmol/L) 94 ± 49 99 ± 66 88 ± 19 0.47
CRP (mg/L) 38 ± 60 44 ± 73 31 ± 42 0.50
Leu (109/L) 9.2 ± 3.3 9.2 ± 3.3 9.2 ± 3.5 0.99
Fbg (g/L) 4.1 ± 0.9 3.9 ± 1.0 4.3 ± 0.7 0.11
BMMC count (109 cells) 4.2 ± 1.4 4.4 ± 1.5 4.0 ± 1.3 0.45
CD34+ count (106 cells) 26 ± 14 28 ± 17 23 ± 11 0.30
Previous PTA/surgery 29 (71%) 14 (67%) 15 (75%) 0.73
Previous CABG/PCI 6 (15%) 3 (14%) 3 (15%) 1.0
Post-MI 13 (32%) 6 (29%) 7 (35%) 0.74
BMI, body mass index; BMMC, bone marrow mononuclear cells; CABG, coronary artery bypass grafting; CRP, C-reactive protein; Fbg, fibrinogen; IA, intra-arterial; IM, intramuscular; Leu, leukocyte level in peripheral blood; LVEF, left ventriclar ejection fraction; MI, myocardial infarction; PCI, percutaneous coronary intervention.
1912 KLEPANEC ET AL.
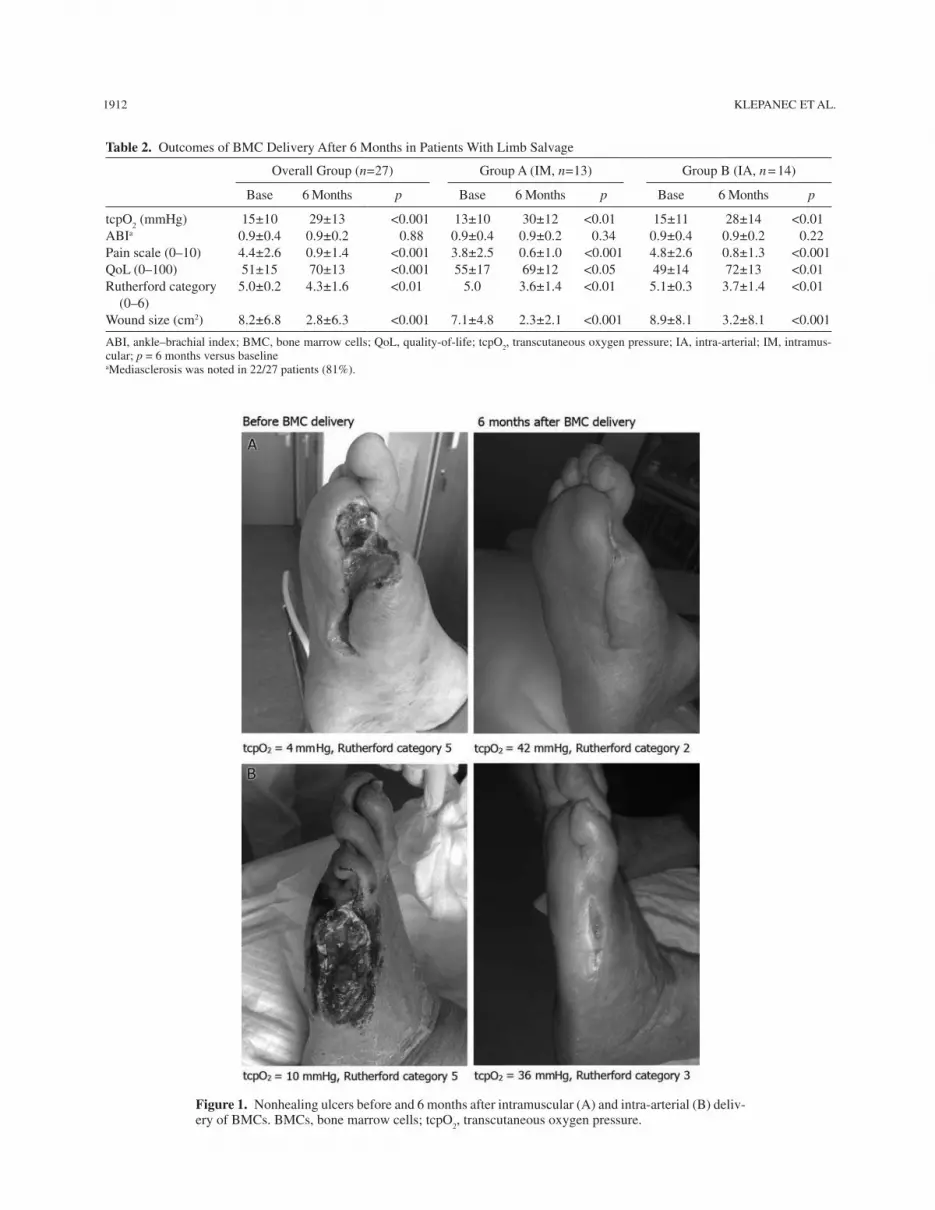
Figure 1. Nonhealing ulcers before and 6 months after intramuscular (A) and intra-arterial (B) deliv-ery of BMCs. BMCs, bone marrow cells; tcpO
2, transcutaneous oxygen pressure.
Table 2. Outcomes of BMC Delivery After 6 Months in Patients With Limb Salvage
Overall Group (n = 27) Group A (IM, n = 13) Group B (IA, n = 14)
Base 6 Months p Base 6 Months p Base 6 Months p
tcpO2 (mmHg) 15 ± 10 29 ± 13 <0.001 13 ± 10 30 ± 12 <0.01 15 ± 11 28 ± 14 <0.01
ABIa 0.9 ± 0.4 0.9 ± 0.2 0.88 0.9 ± 0.4 0.9 ± 0.2 0.34 0.9 ± 0.4 0.9 ± 0.2 0.22
Pain scale (0–10) 4.4 ± 2.6 0.9 ± 1.4 <0.001 3.8 ± 2.5 0.6 ± 1.0 <0.001 4.8 ± 2.6 0.8 ± 1.3 <0.001
QoL (0–100) 51 ± 15 70 ± 13 <0.001 55 ± 17 69 ± 12 <0.05 49 ± 14 72 ± 13 <0.01
Rutherford category
(0–6)
5.0 ± 0.2 4.3 ± 1.6 <0.01 5.0 3.6 ± 1.4 <0.01 5.1 ± 0.3 3.7 ± 1.4 <0.01
Wound size (cm2) 8.2 ± 6.8 2.8 ± 6.3 <0.001 7.1 ± 4.8 2.3 ± 2.1 <0.001 8.9 ± 8.1 3.2 ± 8.1 <0.001
ABI, ankle–brachial index; BMC, bone marrow cells; QoL, quality-of-life; tcpO2, transcutaneous oxygen pressure; IA, intra-arterial; IM, intramus-
cular; p = 6 months versus baselineaMediasclerosis was noted in 22/27 patients (81%).

STEM CELL DELIVERY IN CRITICAL LIMB ISCHEMIA 1913
Figure 2. Improvement in trancutaneous oxygen pressure and pain scale 3 and 6 months after BMC delivery: IM versus IA group. BMC, bone marrow cells; IA, intra-arterial; IM, intramuscular; tcpO
2, transcutaneous oxygen pressure. *p = NS IM versus IA; †p < 0.005 baseline
versus 6 months.
in the IA group (p = 0.94). There were no procedure-
related complications in either group.
Responders Versus Nonresponders to Cell Therapy
Table 4 shows the characteristics of responders ver-
sus nonresponders to BMC therapy. Responders (n = 27)
were characterized by a higher CD34+ cell count in the
BMC product (29 ± 15 × 106 vs. 17 ± 12 × 106, p < 0.05)
despite having a similar number of total nucleated cells
(4.3 ± 1.4 × 109 vs. 4.1 ± 1.2 × 109, p = 0.66). Responders
had lower CRP levels (18 ± 28 vs. 100 ± 96 mg/L, p < 0.05)
and peripheral blood leukocyte count (8.3 ± 2.1 × 109/L
vs. 12.3 ± 4.5 × 109/L, p < 0.05) as compared with nonre-
sponders (10 patients).
Upon univariate analysis, a CD34+ cell count >20 × 106
was associated with a positive therapeutic response to
stem cell therapy [p = 0.015, odds ratio (OR) 4.7, 95%
confidence interval (CI) 1.15–19.24], and peripheral
blood leukocyte count >10 × 109/L was associated with
a negative therapeutic response (p = 0.006, OR 2.1,
95% CI 1.06–4.1), similar to the effect of CRP level
>10 mg/L ( p = 0.038, OR 1.54, 95% CI 1.01–2.32).
Upon multivariate analysis (binary logistic regression),
the number of administrated CD34+ cells >20 × 106
emerged as an independent predictor of clinical benefit
after BMC application ( p = 0.03). A peripheral leukocyte
count >10 × 109/L was shown to be an independent pre-
dictor of negative therapeutic response to cell therapy
( p = 0.048). According to the receiver operating charac-
teristic (ROC) analysis, a cutoff limit for CD34+ cells of
20 × 106 in delivered bone marrow concentrate was pre-
dictive for a positive clinical response with 80% specific-
ity and 65% sensitivity (Fig. 4).
DISCUSSION
The present study investigates the effects of two meth-
ods of delivery of autologous BMCs on the progression
of advanced CLI. The main findings can be summarized
as follows: (1) IM and IA delivery routes are effective and
comparable in inducing a therapeutic effect in CLI and (2)
higher CD34+ cell counts and a lower degree of inflam-
mation are associated with a better clinical response to
BMC administration.
Delivery of Autologous BMCs in Patients With CLI
Several authors have reported the clinical benefit of
administration of autologous BMCs in patients with CLI
(2,5,12,18,22,31,35). BMC delivery has been associated
with limb salvage, increase in tcpO2, blood flow perfu-
sion, or the ABI. The results of the present study cor-
roborate the positive effects of BMC therapy on wound
healing, tcpO2, pain scoring, Rutherford category, as
well as QoL. Conversely, the ABI did not differ after 6
months in the present study, similar to the findings in the
PROVASA trial (35). Of note, most of our patients suf-
fered from diabetes mellitus, with the high prevalence of
mediasclerosis [22/27 subjects (81%) in the responders
group], where noncompressible ankle arteries precluded
meaningful determination of the ABI. Importantly, the
prevalence of limb salvage 73% in the present study was
similar to that of other studies reporting the effects of cell
therapy at 6 months (15,37).
Intramuscular Versus Intra-Arterial Routes
of BMC Delivery
There is ongoing discussion about the optimal method
of cell delivery in CLI. IM as well as IA methods of

1914 KLEPANEC ET AL.
Figure 3. Digital subtraction angiography before and 6 months after BMC delivery: IM (A) versus IA (B) group.
administration of stem cells have shown promising results
in achieving therapeutic benefit (2,5,12,25,35).
One potential advantage of IM delivery is creation
of “local depots” of implanted cells with increased
local paracrine activity in the ischemic area. However,
the prevalence of cell retention and survival times after
IM injection into ischemic limb muscle is not known.
For IA delivery, the homing of administrated BMCs in
the zone of ischemia is crucial (4). With selective IA
delivery, stem cells can reach the border zone of maxi-
mum ischemia by blood flow, although the degree of
cell uptake from the circulation and from engraftment
is unknown.
In the clinical setting, the question of the optimal
route of BMC delivery has been addressed only in small
studies (8,32). Our results from direct head-to-head
comparison of different administration routes indicate
that IM as well as IA methods of BMC delivery are
effective in limb salvage and wound healing, with no
significant differences in various functional surrogate
endpoints between the techniques. Our clinical obser-
vations corroborate experimental findings of a similar
level of angiogenic activity after IM and IA injections in
the rat ischemic hind-limb model (36). Likewise, they
are in agreement with a recent study showing no differ-
ences in the extent of perfusion improvement after IM

STEM CELL DELIVERY IN CRITICAL LIMB ISCHEMIA 1915
administration or combined IM and IA administration in
patients with CLI (32).
There are various techniques of IM or IA administra-
tion of stem cells. For IA methods, slow delivery over
3 min upon injection into the superficial femoral artery
(19) or IA infusion at 900 ml/h (5) has been described.
We undertook selective IA delivery of BMCs at a con-
trolled rate of 800 ml/h at the site of arterial occlusion.
For IM administration, in most clinical trials, injection
has usually been done using a symmetric grid with a fixed
number of injections (2,25). In the present study, BMC
administration into the muscles of the affected limb was
carried out along the crural arteries.
Functional improvement after IM and IA adminis-
tration was observed in the absence of macrovascular
changes of visible collaterals or arteriogenesis of the
affected limb upon DSA. This finding supports the con-
cept that the therapeutic effects of BMCs in CLI are pri-
marily exerted at the microcirculation and that DSA is
not a suitable method for the evaluation of therapeutic
angiogenesis (33).
Predictors of Therapeutic Responses to Delivery of
Autologous BMCs
The potential predictors of the therapeutic response
to cell-based therapy in CLI have not been clearly eluci-
dated. In the present study, two factors were predictive of
the response to cell therapy. The number of administrated
CD34+ cells, but not the total number of nucleated cells
(bone marrow mononuclear cells, BMMCs), was strongly
related to clinical benefit. This result partially contradicts
recent findings in the PROVASA trial in which CD34+
cells and BMMC numbers were independent predictors of
improved ulcer healing (35). Conversely, they are consis-
tent with various studies demonstrating the superior effects
of enriched CD34+ cells as compared with BMMCs. In
fundamental studies, the surface expression of CD34,
CD133 and vascular endothelial growth factor receptor-2
[VEGFR-2/kinase insert domain receptor (KDR)] identi-
fied a population of endothelial progenitor cells (EPCs)
with enhanced potency for neovascularization of isch-
emic tissue (7,14,16,24). Likewise, CD34+ cells could
restore the microcirculation and improve tissue perfusion
in preclinical models (13,14) as well as in clinical series
(21,28) that appeared to be superior to BMMCs alone (13).
Furthermore, enriched CD133+ progenitor cells demon-
strated positive functional effects in patients with chronic
as well as recently infarcted myocardium (3,29). Evidence
that CD34+ cells may be pivotal for therapeutic benefits is
supported by the notion that mononuclear cells depleted
of CD34+ cells do not improve myocardial function in a
murine infarct model (16). Nevertheless, it is likely that
nonhematopoietic stem cells (mesenchymal or stromal
cells), with their high paracrine ability, could also contrib-
ute to the beneficial effect of cell therapy. Mesenchymal
cells, although found in low numbers in mononuclear cell
fractions, are a potent source of trophic cytokines and have
been shown to exert pro-angiogenic effects regardless of
bone marrow or adipose origin (9,17). In addition, the
composition of the bone marrow concentrate used in the
present study included a small portion of an erythrocyte
layer together with a high number of platelets. Platelets, as
a rich source of paracrine activity, have been shown to aug-
ment the formation of collateral vessels in ischemic tissue
in the presence of mononuclear cells (11).
Second, elevated inflammatory markers (e.g., leukocyte
count, CRP levels) were predictive of a negative thera-
peutic response to cell delivery. CRP is considered to be
one of the strongest predictors of vascular death (26) and
appears to be an important mediator of atherogenesis (30).
It can exert a harmful effect on EPC function, resulting in
impaired repair of vessels and impaired neovasculariza-
tion of ischemic tissues (34). Accordingly, a reduced CRP
level has been shown to be a major predictor of successful
outcome in percutaneous transluminal angioplasty in dia-
betic patients with infected foot ulcers (20). Our findings
Table 3. Six-month Comparison of Functional Outcomes of
BMC Delivery in Patients With Limb Salvage
Group A
(IM, n = 13)
Group B
(IA, n = 14)
p
(IM vs. IA)
∆ tcpO2 (mmHg) 13.4 ± 12.4 13.5 ± 13.4 0.66∆ tcpO
2 > 15% 7 (70%) 9 (69%) 1.0∆ ABI 0.05 ± 0.23 –0.12 ± 0.30 0.25∆ Pain scale (0–10) –3.7 ± 2.1 –3.6 ± 2.8 0.63∆ QoL (0–100) 18 ± 13 22 ± 17 0.56∆ Rutherford
category (1–6)
–1.28 ± 1.70 –1.36 ± 1.43 0.46
∆ Wound size (cm2) –4.8 ± 3.2 –5.8 ± 5.4 0.59
ABI, ankle–brachial index; BMC, bone marrow cells; QoL, quality-of-life; tcpO
2, transcutaneous oxygen pressure; IA, intra-arterial; IM,
intramuscular; ∆, baseline value at 6 months.
Table 4. Characteristics of Responders Versus Nonresponders
to BMC Delivery
Responders
(n = 27)
Nonresponders
(n = 10) p
BMMC (109) 4.3 ± 1.4 4.1 ± 1.2 0.66
CD34+ (106) 29 ± 15 17 ± 12 0.03
CRP (mg/L) 18 ± 28 100 ± 96 0.03
Leu (109/L) 8.3 ± 2.1 12.3 ± 4.5 0.02
Tr (109/L) 290 ± 107 352 ± 163 0.33
tcpO2 baseline (mmHg) 15 ± 10 9 ± 8 0.07
Wound size (cm2) 8.2 ± 6.8 14.1 ± 10.3 0.12
BMC, bone marrow cells; BMMC, bone marrow mononuclear cells; CRP, C-reactive protein; Leu, leukocytes in peripheral blood; tcpO
2,
transcutaneous oxygen pressure; Tr, thrombocytes in peripheral blood.

1916 KLEPANEC ET AL.
corroborate the clinical results of the PROVASA trial
whereby patients with Rutherford classification of 6 CLI
(gangrene or major loss of tissue) at baseline (typical by
the highest inflammatory burden) did not respond to cell
therapy (35). Advanced local inflammation of ischemic tis-
sue acts as a hostile environment for delivered stem cells.
Hence, the question of appropriate timing of stem cell ther-
apy with regard to the deleterious inflammatory setting is
one of the key factors of clinical success.
LIMITATIONS
A relatively small number of patients in individual groups
could be considered to be one of the limitations; the findings
of the present study need to be confirmed in larger, prospec-
tively designed cohorts. Second, absence of a control group
cannot exclude the possibility of spontaneous improvement
in some patients. However, the significant improvements in
tcpO2 as an objective parameter in patients with no options
for surgical or endovascular revascularization are unlikely to
be the result of placebo or spontaneous improvement.
CONCLUSIONS
Both intramuscular and intra-arterial delivery of autolo-
gous BMCs is effective and a comparable therapeutic strategy
for patients with CLI who are not suitable for endovascular
or surgical revascularization. A higher concentration of
CD34+ cells and a lower degree of inflammation are associ-
ated with a better therapeutic response to BMC therapy.
ACKNOWLEDGMENTS: This study was sponsored with a grant from European Regional Development Funding (ITMS code: 26240220023). Authors declare no conflicts of interest.
REFERENCES
Albers, M.; Fratezzi, A. C.; De Luccia, N. Assesment of 1. quality of life of patients with severe ischemia as a result of infrainguinal arterial occlusive disease. J. Vasc. Surg. 6:54–59; 1992.Amann, B.; Luedemann, C.; Ratei, R.; Schmidt-Lucke, 2. J. A. Autologous bone marrow cell transplantation increases leg perfusion and reduces amputations in patients with advanced critical limb ischemia due to peripheral artery disease. Cell Transplant. 18:371–380; 2009.Bartunek, J.; Vanderheyden, M.; Vandekerckhove, B.; 3. Mansour, S.; De Bruyne, B.; De Bondt, P.; Van Haute, I.; Lootens, N.; Heyndrickx, G.; Wijns, W. Intracoronary injec-tion of CD133-positive enriched bone marrow progenitor cells promotes cardiac recovery after recent myocardial infarction: Feasibility and safety. Circulation 112:I178–183; 2005.Chavakis, E.; Aicher, A.; Heeschen, C.; Sasaki, K.; Kaiser, R.; 4. El Makhfi, N.; Urbich, C.; Peters, T.; Scharffetter-Kochanek, K.; Zeiher, A. M.; Chavakis, T.; Dimmeler, S. Role of beta2-integrins for homing and neovascularization capacity of endothelial progenitor cells. J. Exp. Med. 201:63–72; 2005.
Figure 4. Receiver operating characteristic of CD34+ cells, BMMC count, CRP, and leukocyte levels for the prediction of the BMC therapeutic response. Area under the receiver operating characteristic (ROC) curve: CD34+ = 0.75 (CI 0.57–0.94, p = 0.02); mononuclear cell (MNC) = 0.55 (CI 0.35–0.75, p = 0.65); c-reactive protein (CRP) = 0.26 (CI 0.04–0.47, p = 0.03); leukocyte (leu) = 0.21 (CI 0.01–0.4, p = 0.007)

STEM CELL DELIVERY IN CRITICAL LIMB ISCHEMIA 1917
Chochola, M.; Pytlík, R.; Kobylka. P.; Skalická, L.; 5. Kideryová, L.; Beran, S.; Varejka, P.; Jirát, S.; Køivánek, J.; Aschermann, M.; Linhart, A. Autologous intra-arterial infusion of bone marrow mononuclear cells in patients with critical limb ischemia. Int. Angiol. 27:281–290; 2008.Dolan, P. Modeling valuations for EuroQol health states. 6. Med. Care 35:1095–1108; 1997.Gehling, U. M.; Ergün, S.; Schumacher, U.; Wagener, C.; 7. Pantel, K.; Otte, M.; Schuch, G.; Schafhausen, P.; Mende, T.; Kilic, N.; Kluge, K.; Schäfer, B.; Hossfeld, D. K.; Fiedler, W. In vitro differentiation of endothelial cells from AC133-positive progenitor cells. Blood 95:3106–3112; 2000.Gu, Y. Q.; Zhang, J.; Guo, L. R.; Qi, L. X.; Zhang, S. W.; 8. Xu, J.; Li, J. X.; Luo, T.; Ji, B. X.; Li, X. F.; Yu, H. X.; Cui, S. J.; Wang Z. G. Transplantation of autologous bone mar-row mononuclear cells for patients with lower limb isch-emia. Chin. Med. J. 121:963–967; 2008.Hare, J. M.; Traversek, J. H.; Henry, T. D.; Dib, N.; Strumpf, 9. R. K.; Schulman, S. P.; Gerstenblith, G.; DeMaria, A. N.; Denktas, A. E.; Gammon, R. S.; Hermiller Jr., J. B.; Reisman M. A.; Schaer, G. L.; Sherman, W. A randomized, double-blind, placebo-controlled, dose-escalation study of intravenous adult human mesenchymal stem cells (prochy-mal) after acute myocardial infarction. J. Am. Coll. Cardiol. 54:2277–2286; 2009.Hermann, P. C.; Huber, S. L.; Herrler, T.; von Hesler, C.; 10. Andrassy, J.; Kevy, S. V.; Jacobson, M. S.; Heeschen, C. Concentration of bone marrow total nucleated cells by a point-of-care device provides a high yield and preserves their functional activity. Cell Transplant. 16:1059–1069; 2008.Iba, O.; Matsubara, H.; Nozawa, Y.; Fujiyama, S.; Amano, K.; 11. Mori, Y.; Kojima, H.; Iwasaka, T. Angiogenesis by implanta-tion of peripheral blood mononuclear cells and platelets into ischemic limbs. Circulation 106:2019–2025; 2002.Idei, N.; Soga, J.; Hata, T.; Fujii, Y.; Fujimura, N.; Mikami, 12. S.; Maruhashi, T.; Nishioka, K.; Hidaka, T.; Kihara, Y.; Chowdhury, M.; Noma, K.; Taguchi, A.; Chayama, K.; Sueda, T.; Higashi, Y. Autologous bone-marrow mononu-clear cell implantation reduces long-term major amputation risk in patients with critical limb ischemia: A comparison of atherosclerotic peripheral arterial disease and Buerger disease. Circ. Cardiovasc. Interv. 4:15–25; 2011.Iwasaki, H.; Kawamoto, A.; Ishikawa, M.; Oyamada, A.; 13. Nakamori, S.; Nishimura, H.; Sadamoto, K.; Horii, M.; Matsumoto, T.; Murasawa, S.; Shibata, T.; Suehiro, S.; Asahara, T. Dose-dependent contribution of CD34-positive cell transplantation to concurrent vasculogenesis and cardio-myogenesis for functional regenerative recovery after myo-cardial infarction. Circulation 113:1311–1325; 2006.Kawamoto, A.; Iwasaki, H.; Kusano, K.; Murayama, T.; 14. Oyamada, A.; Silver, M.; Hulbert, C.; Gavin, M.; Hanley, A.; Ma, H.; Kearney, M.; Zak, V.; Asahara, T.; Losordo, D. W. CD34-positive cells exhibit increased potency and safety for therapeutic neovascularization after myocar-dial infarction compared with total mononuclear cells. Circulation 114:2163–2169; 2006.Kawamura, 15. A.; Horie, T.; Tsuda, I.; Ikeda, A.; Egawa, H.; Imamura, E.; Iida, J.; Sakata, H.; Tamaki, T.; Kukita, K.; Meguro, J.; Yonekawa, M.; Kasai, M. Prevention of limb amputation in patients with limbs ulcers by autologous peripheral blood mononuclear cell implantation. Ther. Apher. Dial. 9:59–63; 2005.Kocher, A. A.; Schuster, M. D.; Szabolcs, M. J.; Takuma, 16. S.; Burkhoff, D.; Wang, J.; Homma, S.; Edwards, N. M.;
Itescu, S. Neovascularization of ischemic myocardium by human bone-marrow-derived angioblasts prevents cardio-myocyte apoptosis, reduces remodeling and improves car-diac function. Nat. Med. 7:430–436; 2001.Kondo, K.; Shintani, S.; Shibata, R.; Murakami, H.; 17. Murakami, R.; Imaizumi, M.; Kitagawa, Y.; Murohara, T. Implantation of adipose-derived regenerative cells enhances ischemia-induced angiogenesis. Arterioscler. Thromb. Vasc. Biol. 29:61–66; 2009. Lara-Hernandez, 18. R., Lozano-Vilardell, P.; Blanes, P.; Torreguitart-Mirada, N.; Galmés, A.; Besalduch, J. Safety and efficacy of therapeutic angiogenesis as a novel treat-ment in patients with critical limb ischemia. Ann. Vasc. Surg. 24:287–294; 2010.Lenk, K.; Adams, V.; Lurz, P.; 19. Erbs, S.; Linke, A.; Gielen, S.; Schmidt, A.; Scheinert, D.; Biamino, G.; Emmrich, F.; Schuler, G.; Hambrecht, R. Therapeutical potential of blood-derived progenitor cells in patients with peripheral arterial occlusive disease and critical limb ischaemia. Eur. Heart J. 26:1903–1909; 2005.Lin, C. 20. W.; Hsu, L. A.; Chen, C. C.; Yeh, J. T.; Sun, J. H.; Lin, C. H.; Chen, S. T.; Hsu, B. R.; Huang, Y. Y. C-reactive protein as an outcome predictor for percutaneous translu-minal angioplasty in diabetic patients with peripheral arte-rial disease and infected foot ulcers. Diabetes Res. Clin. Pract. 90:167–172; 2010.Losordo, D. W.; Schatz, R. A.; White, C. J.; Udelson, J. E.; 21. Veereshwarayya, V.; Durgin, M.; Poh, K. K.; Weinstein, R.; Kearney, M.; Chaudhry, M.; Burg, A.; Eaton, L.; Heyd, L.; Thorne, T.; Shturman, L.; Hoffmeister, P.; Story, K.; Zak, V.; Dowling, D.; Traverse, J. H.; Olson R. E.; Flanagan, J.; Sodano, D.; Murayama, T.; Kawamoto, A.; Kusano, K. F.; Wollins, J.; Welt, F.; Shah, P.; Soukas, P.; Asahara, T.; Henry, T. D. Intramyocardial transplantation of autolo-gous CD34+ stem cells for intractable angina: A phase I/IIa double-blind, randomized controlled trial. Circulation 115:3165–3172; 2007.Miyamoto, K.; Nishigami, K.; Nagaya, N.; Akutsu, K.; 22. Chiku, M.; Kamei, M.; Soma, T.; Miyata, S.; Higashi, M.; Tanaka, R.; Nakatani, T.; Nonogi, H.; Takeshita, S. Unblinded pilot study of autologous transplantation of bone marrow mononuclear cells in patients with thromboangiitis obliterans. Circulation 114:2679–2684; 2006.Norgren, L.; Hiatt, W. R.; Dormandy, J. A.; Nehler, M. R.; 23. Harris, K. A.; Fowkes, F. G.; TASC II Working Group; Bell, K.; Caporusso, J.; Durand-Zaleski, I.; Komori, K.; Lammer, J.; Liapis, C.; Novo, S.; Razavi, M.; Robbs, J.; Schaper, N.; Shigematsu, H.; Sapoval, M.; White, C.; White, J.; Clement, D.; Creager, M.; Jaff, M.; Mohler, 3rd., E.; Rutherford, R. B.; Sheehan, P.; Sillesen, H.; Rosenfield, K. Inter-society consensus for the management of periph-eral arterial disease (TASC II). Eur. J. Vasc. Endovasc. Surg. 33 Suppl 1:S1–75; 2007. Peichev, M.; Naiyer, A. J.; Pereira, D.; Zhu, Z.; Lane, W. J.; 24. Williams, M.; Oz, M. C.; Hicklin, D. J.; Witte, L.; Moore, M. A.; Rafii, S. Expression of VEGFR-2 and AC133 by circulating human CD34(+) cells identifies a population of functional endothelial precursors. Blood 95:952–958; 2000.Procházka, V.; Gumulec, J.; Jaluvka, F.; Salounová, D.; 25. Jonszta, T.; Czerny, D.; Krajca, J.; Urbanec, R.; Klement, P.; Martinek, J.; Klement, G. L. Cell therapy, a new standard in management of chronic critical limb ischemia and foot ulcer. Cell Transplant. 19:1413–1424; 2010.

1918 KLEPANEC ET AL.
Ridker, P. M. High-sensitivity C-reactive protein: Potential 26. adjunct for global risk assessment in the primary prevention of cardiovascular disease. Circulation 103:1813–1818; 2001.Rutherford, R. B.; Baker, J. D.; Ernst, C.; Johnston, K. W.; 27. Porter, J. M.; Ahn, S.; Jones, D. N. Recommended stan-dards for reports dealing with lower extremity ischemia: Revised version. J. Vasc. Surg. 26:517–538; 1997.Saigawa, T.; Kato, K.; Ozawa, T.; 28. Toba, K.; Makiyama, Y.; Minagawa, S.; Hashimoto, S.; Furukawa, T.; Nakamura, Y.; Hanawa, H.; Kodama, M.; Yoshimura, N.; Fujiwara, H.; Namura, O.; Sogawa, M.; Hayashi, J.; Aizawa, Y. Clinical application of bone marrow implantation in patients with arteriosclerosis obliterans, and the association between efficacy and the number of implanted bone marrow cells. Circ. J. 68:1189–1193; 2004.Stamm, C.; Westphal, B.; Kleine, H. D.; Petzsch, M.; Kittner, 29. C.; Klinge, H.; Schumichen, C.; Nienaber, C. A.; Freund, M.; Steinhoff, G. Autologous bone marrow stem-cell transplanta-tion for myocardial regeneration. Lancet 361:45–46; 2003.Szmitko, P. E.; Wang, C. H.; Weisel, R. D.; 30. de Almeida, J. R.; Anderson, T. J.; Verma, S. New markers of inflam-mation and endothelial cell activation: Part 1. Circulation 108:1917–1923; 2003.Tateishi-Yuyama, E.; Matsubara, H.; Murohara, T.; Ikeda, U.; 31. Shintani, S.; Masaki, H.; Amano, K.; Kishimoto, Y.; Yoshimoto, K.; Akashi, H.; Shimada, K.; Iwasaka, T.; Imaizumi, T. Therapeutic angiogenesis for patients with limb ischaemia by autologous transplantation of bone-marrow cells: A pilot study and a randomised controlled trial. Lancet 360:427–435; 2002.Van Tongeren, R. 32. B.; Hamming, J. F.; Fibbe W. E.; Van Weel, V.; Frerichs, S. J.; Stiggelbout, A. M.; Van Bockel, J. H.; Lindeman, J. H. Intramuscular or combined intramuscular/intra-arterial administration of bone marrow mononuclear
cells: A clinical trial in patients with advanced limb isch-emia. J. Cardiovasc. Surg. 49:51–58; 2008.Van Tongeren, R. B.; Hamming, J. F.; le Cessie, S.; van 33. Erkel, A. R.; van Bockel, J. H. Limited value of digital sub-traction angiography in the evaluation of cell-based therapy in patients with limb ischemia. Int. J. Cardiovasc. Imaging 26:19–25; 2010. Verma, 34. S.; Kuliszewski, M. A.; Li, S. H.; Szmitko, P. E.; Zucco, L.; Wang, C. H.; Badiwala, M. V.; Mickle, D. A.; Weisel, R. D.; Fedak, P. W.; Stewart, D. J.; Kutryk, M. J. C-reactive protein attenuates endothelial progenitor cell survival, differentiation, and function: Further evidence of a mechanistic link between C-reactive protein and cardio-vascular disease. Circulation 109:2058–2067; 2004.Walter, D. 35. H.; Krankenberg, H.; Balzer, J. O.; Kalka, C.; Baumgartner, I.; Schlüter, M.; Tonn, T.; Seeger, F.; Dimmeler, S.; Lindhoff-Last, E.; Zeiher, A. M. for the PROVASA Investigators. Intra-arterial administration of bone marrow mononuclear cells in patients with critical limb ischemia: A randomized-start, placebo-controlled pilot trial (PROVASA). Circ. Cardiovasc. Interv. 4:26–37; 2011.Yoshida, 36. M.; Horimoto, H.; Mieno, S.; Nomura, Y.; Okawa, H.; Nakahara, K.; Sasaki, S. Intra-arterial bone marrow cell transplantation induces angiogenesis in rat hindlimb isch-emia. Eur. Surg. Res. 35:86–91; 2003.Zafarghandi, M. 37. R.; Ravari, H.; Aghdami, N.; Namiri, M.; Moazzami, K.; Taghiabadi, E.; Fazel, A.; Pournasr, B.; Farrokhi, A.; Sharifian, R. A.; Salimi, J.; Moini, M.; Baharvand, H. Safety and efficacy of granulocyte- colony-stimulating factor administration following autologous intramuscular implantation of bone marrow mono nuclear cells: A randomized controlled trial in patients with advanced lower limb ischemia. Cytotherapy 12:783–791; 2010.