affective symptoms and cognitive functions in the acute phase of graves’ thyrotoxicosis
TRANSCRIPT

ARTICLE IN PRESS
Available at www.sciencedirect.com
Psychoneuroendocrinology (2007) 32, 36–43
0306-4530/$ - see frdoi:10.1016/j.psyne
�Corresponding au
E-mail address: a
journal homepage: www.elsevier.com/locate/psyneuen
Affective symptoms and cognitive functions in theacute phase of Graves’ thyrotoxicosis
Asmus Vogela,�, Tina. V. Elberlinga, Merete Hørdinga, Jytte Docka,Åse K. Rasmussenb, Ulla Feldt-Rasmussenb, Hans Perrildc, Gunhild Waldemara
aMemory Disorders Research Group, Department of Neurology, Neuroscience Centre, Copenhagen University Hospital,Rigshospitalet, N6702 9, Blegdamsvej 2100 Copenhagen, DenmarkbDepartment of Medical Endocrinology, Copenhagen University Hospital, Rigshospitalet, DenmarkcDepartment of Endocrinology, Bispebjerg Hospital, Denmark
Received 3 May 2006; received in revised form 26 September 2006; accepted 29 September 2006
KEYWORDSGraves’thyrotoxicosis;Hyperthyroidism;Cognition;Neuropsychology;Affective symptoms
ont matter & 2006uen.2006.09.012
thor. Tel.: +45 354
SummaryIn the acute phase of Graves’ thyrotoxicosis patients often have subjective cognitivecomplaints. Continuing controversy exists about the nature of these symptoms andwhether they persist after treatment. This prospective study included 31 consecutivelyreferred, newly diagnosed, and untreated patients with Graves’ thyrotoxicosis. A controlgroup of 34 individuals matched for age, education and premorbid intelligence was alsoincluded. At baseline all patients and control subjects were examined with psychiatricrating scales and a comprehensive neuropsychological battery. The effect of treatment onaffective symptomatology was examined in the patient group after reaching euthyroidismand 1 year after treatment initiation. At initial examination patients had significantlyhigher scores on psychiatric rating scales as compared with controls, and the majorityreported memory and concentration problems. No significant differences between thepatient and the control group on neuropsychological test performances were found.Thyroid levels did not correlate with the neuropsychological test performances orpsychiatric ratings. After reaching euthyroidism the level of affective symptoms (includingreports of cognitive deficits) had decreased significantly, with further normalisation 1-yearafter treatment initiation. In conclusion, patients had subjective reports of cognitivedeficits in the toxic phase of Graves’ thyrotoxicosis but comprehensive neuropsychologicaltesting revealed no cognitive impairment. Reports of cognitive dysfunction may reflectaffective and somatic manifestations of thyrotoxicosis and in most patients thesesymptoms disappear after treatment of Graves’ thyrotoxicosis.& 2006 Elsevier Ltd. All rights reserved.
Elsevier Ltd. All rights reserved.
5 2982; fax: +45 3545 2446.
sp.dk (A. Vogel).

ARTICLE IN PRESS
Affective and cognitive symptoms in Graves’ thyrotoxicosis 37
1. Introduction
Graves’ disease is an autoimmune disease of the thyroidgland and one of the most common causes of hyperthyroid-ism worldwide. Graves’ disease best fits a polygenic,multifactorial model of disease in which genetically suscep-tible individuals are exposed to a constitutional or environ-mental insult resulting in immune system activation(McLachlan and Rapoport, 2000).
The clinical presentation depends on the severity ofthyrotoxicosis, the duration of the disease, individualsusceptibility to excess thyroid hormone and the age ofthe patient. The clinical picture in a young woman typicallyincludes hyperactivity, sweating, heat intolerance, tremor,fatigue, weight loss, weakness (especially of the legs),palpitations, tachycardia, and dyspnoea on exertion.
In the acute phase of Graves’ thyrotoxicosis the patientsoften complain of memory and concentration deficits. Somestudies have demonstrated cognitive deficits in the acutephase of thyrotoxicosis compared to the level aftertreatment (Whybrow et al., 1969; Trzepacz et al., 1988a).Others have found cognitive dysfunction in the acute phasecompared to a control group (Alvarez et al., 1983; Zeitlhoferet al., 1984; Schlote et al., 1992) or compared to normativedata (Trzepacz et al., 1988b). Correlations between thyroidhormone levels and cognitive functions have been found insome studies (MacCrimmon et al., 1979), whereas others didnot find such correlations (Trzepacz et al., 1988a; Paschkeet al., 1990). Two studies did not find any cognitiveimpairment in hyperthyroid groups (Wallace et al., 1980;Paschke et al., 1990). Many of the previous studies did nothave examination of cognitive impairment as their pre-dominant focus, and some of these studies were associatedwith (one or more) methodological problems. Few studieshave combined assessment of cognitive and affectivesymptomatology in Graves’ thyrotoxicosis. Therefore, theimpact of Graves’ thyrotoxicosis on cognitive functioningremains unresolved.
In the acute phase of Graves’ thyrotoxicosis manypatients have also been found to have affective symptoms,including emotional lability, irritability, insomnia, restless-ness, agitation, depression and anxiety (Whybrow et al.,1969; MacCrimmon et al., 1979; Wallace et al., 1980;Zeitlhofer et al., 1984; Kathol et al., 1986; Trzepacz et al.1988a,b, 1989; Paschke et al., 1990; Schlote et al., 1992;Demet et al., 2002). Some prospective studies investigatinglong-term affective symptoms in treated patients havegenerally shown that affective symptoms improve afterthe patients were rendered euthyroid (Whybrow et al.,1969; MacCrimmon et al., 1979; Wallace et al., 1980;Zeitlhofer et al., 1984; Kathol et al., 1986; Paschke et al.,1990; Harsch et al., 1992), in fact one study has shown thataffective symptoms decreased after beta-adrenergic antag-onistic treatment alone (Trzepacz et al., 1988b). However,other studies showed residual affective symptoms despitesuccessful treatment of thyrotoxicosis (Bommer et al., 1990;Sonino et al., 1993; Stern et al., 1996; Fahrenfort et al.,2000; Placidi et al., 1998; Engum et al., 2002).
The objective of this study was to investigate affectivesymptoms and cognitive deficits in a group of consecutivelyreferred, newly diagnosed and untreated patients withGraves’ thyrotoxicosis as compared to healthy control
subjects. We also wanted to investigate if patients withmany complaints of cognitive dysfunction had more cogni-tive deficits than patients with no (or little) subjectivecognitive dysfunction. Our second aim was to investigate thecorrelation between thyroid function and neuropsychologi-cal test performances and psychiatric ratings in patientswith Graves’ disease. Finally, we wanted to investigate theeffect of treatment on affective symptoms and cognitivecomplaints.
2. Methods
2.1. Subjects
This study included consecutively referred, newly diag-nosed, and untreated patients with Graves’ thyrotoxicosis,18–60 years of age, from two endocrinological departmentsat hospitals in the Copenhagen area. Results from thesepatients concerning health-related quality of life havepreviously been published (Elberling et al., 2004). Thediagnosis of Graves’ disease was based on increased serumconcentration of thyroid hormones, suppressed thyrotropin(TSH), positive TSH-receptor antibodies (TRAb), and diffuseuptake on a Tc-99m pertechnetate scintigraphy of thethyroid gland. The laboratory variables were measured bystandard methods. Patients with prior thyroid disease oraffective disorders were excluded from the study. Likewise,patients with prior neurological disorders known to influ-ence neuropsychiatric functions were also excluded. Finally,patients unable to speak or read Danish were excludedbecause they were unable to participate in neuropsycholo-gical testing.
Out of 53 consecutively referred patients with newlydiagnosed and untreated Graves’ disease 31 were includedin the study. The causes of exclusion were: previousaffective disease ðN ¼ 5Þ, ongoing drug abuse ðN ¼ 1Þ,foreign primary language ðN ¼ 6Þ, cerebral metastasesðN ¼ 1Þ, multiple sclerosis ðN ¼ 1Þ, familial relation to theinvestigator ðN ¼ 1Þ, vacation of the investigator ðN ¼ 1Þ, noinformed consent ðN ¼ 5Þ, and in one ðN ¼ 1Þ patientGraves’ disease was never confirmed since the patientnever showed up for further investigations.
From advertising we included 34 healthy volunteersmatched for age, gender, education and premorbid intelli-gence. Similar exclusion criteria were applied to the groupof healthy volunteers with addition of exclusion upon familyhistory of thyroid disease. The local Ethical Committeeapproved the study and all participants gave informedconsent.
2.2. Psychiatric rating scales andneuropsychological testing
The Hamilton depression rating scale (HDRS), a 17-itemrating scale, was used to quantify depressive symptoms(Hamilton, 1967). Most items on the HDRS are ratedbetween ‘0’ and ‘4’ (‘0’ ¼ no symptoms present); someitems are rated between ‘0’ and ‘2’. A total scale scorebelow 8 is considered normal. The Hamilton anxiety scale(HAS), a 14-item rating scale, was used to quantify anxietysymptoms (Hamilton, 1969). Items on the HAS are rated

ARTICLE IN PRESS
A. Vogel et al.38
similarly to the HDRS and a total score below 8 is considerednormal.
An experienced neuropsychologist administered neurop-sychological tests. Premorbid intellectual level was assessedby Danish adult reading test (DART), a Danish equivalent tothe National adult reading test (Nelson and O’Connell,1978). Attention and concentration were assessed by Digitspan, sentence repetition (Spreen and Benton, 1969) andthe Stroop test (Stroop, 1935). Memory was assessed withselective reminding test (Buschke, 1973) (measuring freerecall), Category Cued Recall (Buschke et al., 1997)(measuring cued recall), and forced choice word/facerecognition (Warrington, 1974) (measuring recognition).Psychomotor speed and executive functions were assessedby Trail Making Test A and B (Reitan, 1958), Symbol digitmodalities test (Smith, 1973), WAIS picture arrangement,WAIS similarities, Wisconsin card sorting test (Nelson, 1976),and the abbreviated version of The California computerizedassessment package (CALCAP). Visuospatial functions wereassessed with block design test (WAIS Block Design, modifiedby Bruhn) (Mortensen and Gade, 1993).
2.3. Follow-up assessments
The effect of treatment on affective and cognitivesymptomatology (evaluated by psychiatric rating scalesand neuropsychological testing) was examined in the patientgroup after the patients had reached euthyroidism (approxi-mately 3 months after the baseline visit) and again 1 yearafter initiation of treatment. The healthy controls were onlyexamined once.
2.4. Treatment
After the diagnosis of Graves’ disease had been confirmed,all patients received methimazole therapy (supressingelevated thyroid hormone level). Due to adverse events(itching), three patients were changed to propylthiouracil.One year after initiation of treatment all patients were stilltreated with anti-thyroid medication.
Table 1 Demographic characteristics and thyroid status in pat
Gender (female/male)Age (years)Education yearsPremorbid intelligence (Danish adult reading test)Thyrotropin (0.4–4.0miU/L)a
Total thyroxine (60–160 nmol/L)a
Free thyroxine (9.1–23.8 pmol/L)a
Total triiodothyronine (0.9–2.7 nmol/L)a
TRAb (pos/neg)
Note: All values are presented as mean� SD, except thyrotropin preFor all thyroid values 95% reference limits are presented in parentheTRAb positive is above 1 IU/l.
aIndication of the reference interval.
2.5. Statistical analyses
For continuous variables independent samples t-tests wereapplied to test the significance of differences betweengroups (patients versus healthy controls). Chi-square testwas used to analyse group differences in gender. Someneuropsychological variables, neuropsychiatric rating scalesand measures of thyroid function had skewed distributions(floor or ceiling effects) in either the patient or the controlgroup. Thus, to investigate differences between thesegroups Mann–Whitney U test was used. For neuropsycholo-gical variables where normal distributions were foundindependent samples t-tests were also applied to test thesignificance of differences between groups (patients versushealthy controls). Wilcoxon signed ranks test was used toinvestigate differences in affective symptoms at baselineand at follow-up examinations. Due to the skewed distribu-tion of data on psychiatric rating scales and measures ofthyroid functioning, Spearman’s rank order correlationswere used to analyse bivariate associations betweenvariables (neuropsychological test results, psychiatric rat-ings and thyroid levels). A p-value of less than 0.05 wasconsidered significant.
3. Results
3.1. Demographic characteristics
In Table 1 demographic characteristics and thyroid level forpatients and healthy controls are shown. No significantdifferences between the patient and the healthy subjects inage, education years, premorbid intelligence or genderdistribution were found.
3.2. Psychiatric ratings and subjective reports ofcognitive dysfunctions: patients versus controlsubjects
Baseline performances on the psychiatric scales by patientsand controls are displayed in Table 2. None of the healthyvolunteers had signs of depression or anxiety. Patients had
ients with Graves’ disease and healthy controls
Graves’ patients Control subjects
30/1 30/435:2� 9:8 35:8� 11:114:7� 2:1 15:2� 1:827:1� 7:7 28:1� 4:90.01 (o0:01–0.07) 1.5 (0.7–2.5)254� 62 95� 1645:1� 12:0 12:5� 1:35:4� 1:5 1:5� 0:331/0 2/32
sented as median (range).sis.

ARTICLE IN PRESS
Table 2 Performances on psychiatric scales and neuropsychological tests in patients with newly diagnosed and untreatedGraves’ disease as compared to control subjects
Graves’ patients Control subjects p-ValueN ¼ 31 N ¼ 34
Psychiatric scalesHamilton depression rating scale 8 (2–14) 0 (0–4) o0.001Hamilton anxiety scale 11 (2–20) 0 (0–5) o0.001
Neuropsychological testsMemorySelective Reminding Test 8 (0–28) 8 (1–21) 0.74Category cued recall, immediate recall 41 (29–58) 43 (31–62) 0.36Category cued recall, delayed recall 41 (29–61) 42 (28–64) 0.40Forced choice word recognition 49 (43–50) 49 (44–50) 0.58Forced choice face recognition 45 (33–50) 47 (40–50) 0.031
Attention and concentrationDigit span forwards 11 (7–14) 11 (8–15) 0.92Digit span reverse orders 8 (5–13) 9 (4–12) 0.078Sentence repetition 17 (12–21) 19 (14–21) 0.021Stroop test, congruent 50 (34–75) 47 (37–76) 0.56Stroop test, incongruent 99 (65–167) 95 (69–200) 0.62
Psychomotor speed/executive functionsTrail making A 23 (12–44) 22 (14–44) 0.97Trail making B 60 (32–98) 50 (33–128) 0.35Symbol digit modalities test 58 (33–73) 58 (38–77) 0.59CALCAPSimple reaction 315 (244–462) 331 (256–450) 0.26Choice reaction (‘7’) 394 (342–467) 414 (347–623) 0.16Sequential no. (1-back, identical) 525 (379–709) 527 (381–678) 0.92Sequential no. (1-back, ascending) 593 (367–815) 582 (375–774) 0.42WAIS, picture arrangement 24 (14–34) 25 (14–34) 0.49WAIS, similarities 20 (14–26) 22 (15–25) 0.07Wisconsin card sorting test 5 (1–25) 5 (1–12) 0.99
Visuospatial functionBlock design test 14 (6–44) 11 (6–40) 0.08
Values are represented as median (range).Statistical comparisons were performed with Mann–Whitney U Test.
Affective and cognitive symptoms in Graves’ thyrotoxicosis 39
significantly higher HDRS scores as compared to controls.One patient was diagnosed with moderate/severe depres-sion according to ICD-10 and anti-depressive treatment wasinitiated. Seventeen of the patients had mild to moderatedepressive symptoms (HDRS 8–17) and the remaining ðN ¼14Þ had no depressive symptoms (HDRS below 8). Likewise,Graves’ patients had significantly higher scores on HAS ascompared to healthy controls. Most patients ðN ¼ 27Þ hadmild to moderate anxiety symptoms (HAS 8–28). Fourpatients had no anxiety (HAS below 8).
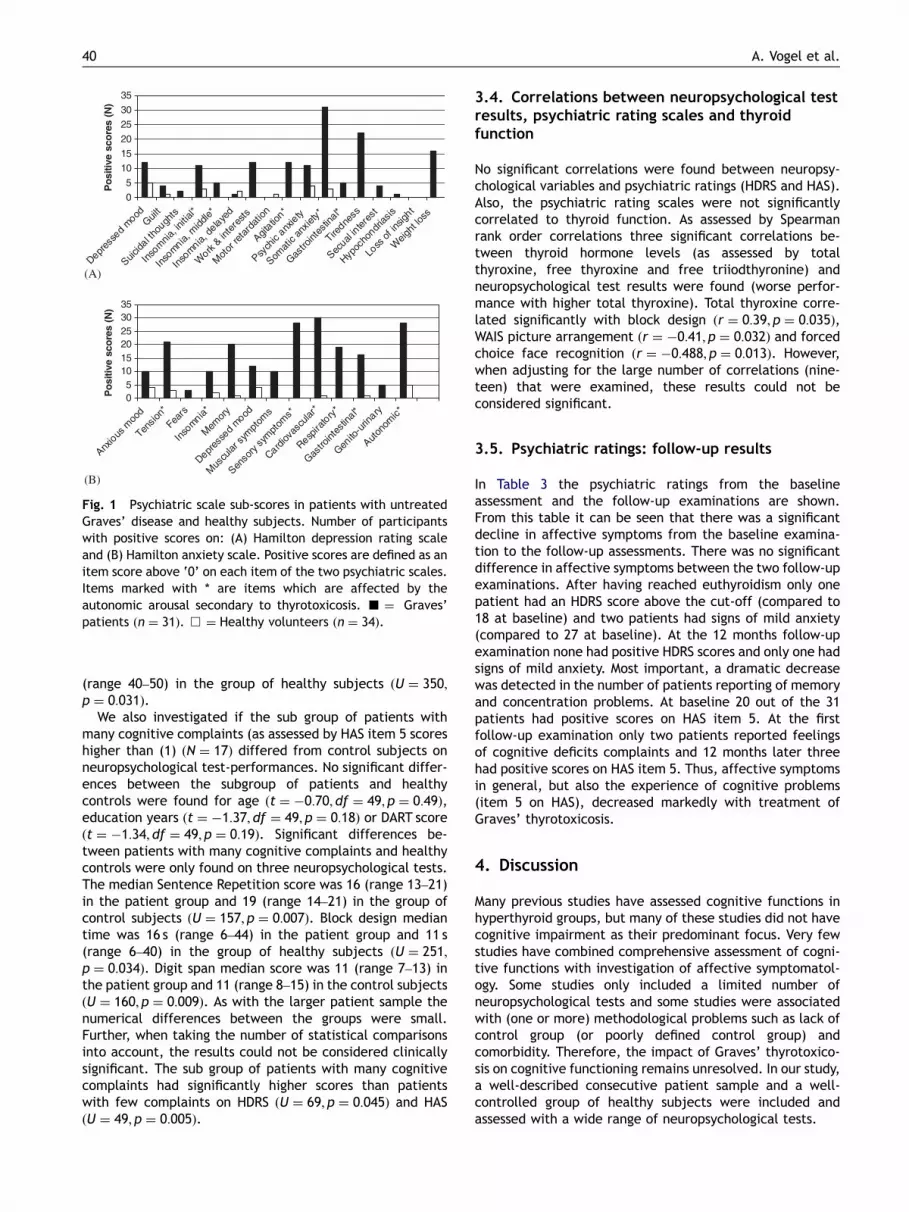
Fig. 1 present all item scores in HDRS and HAS for patientsand control subjects at baseline. Forty percent of thepatients complained of depressed mood as based on HDRSitem 1 (15% of the healthy volunteers) and 35% describedpsychic anxiety in the acute phase of Graves’ disease asbased on HDRS item 10 (12% of the healthy volunteers). Item5 on HAS assesses whether patients experience problems ofmemory and concentration and to which degree theseproblems interfere with everyday functioning. On this item
65% of the patients had positive scores, as compared to 3% incontrol subjects.
3.3. Neuropsychological test-performances:patients versus control subjects
Results from neuropsychological tests are given in Table 2.Since some of the tests had ceiling effect in the controlgroup, all results are presented as median scores. Nodifferences were found in statistical significance when bothparametric and non-parametric statistical methods wereapplied where normal distribution was found. Only two ofthe neuropsychological tests were found to differ signifi-cantly between the two groups. The median sentencerepetition score was 17 (range 12–21) in the patient groupand 19 (range 14–21) in the group of control subjectsðU ¼ 353; p ¼ 0:021Þ. Forced choice face recognition medianscore was 45 (range 33–50) in the patient group and 47
ARTICLE IN PRESS
(B)
(A)
Fig. 1 Psychiatric scale sub-scores in patients with untreatedGraves’ disease and healthy subjects. Number of participantswith positive scores on: (A) Hamilton depression rating scaleand (B) Hamilton anxiety scale. Positive scores are defined as anitem score above ‘0’ on each item of the two psychiatric scales.Items marked with * are items which are affected by theautonomic arousal secondary to thyrotoxicosis. ’ ¼ Graves’patients ðn ¼ 31Þ. & ¼ Healthy volunteers ðn ¼ 34Þ.
A. Vogel et al.40
(range 40–50) in the group of healthy subjects ðU ¼ 350;p ¼ 0:031Þ.
We also investigated if the sub group of patients withmany cognitive complaints (as assessed by HAS item 5 scoreshigher than (1) ðN ¼ 17Þ differed from control subjects onneuropsychological test-performances. No significant differ-ences between the subgroup of patients and healthycontrols were found for age ðt ¼ �0:70; df ¼ 49; p ¼ 0:49Þ,education years ðt ¼ �1:37; df ¼ 49; p ¼ 0:18Þ or DART scoreðt ¼ �1:34; df ¼ 49; p ¼ 0:19Þ. Significant differences be-tween patients with many cognitive complaints and healthycontrols were only found on three neuropsychological tests.The median Sentence Repetition score was 16 (range 13–21)in the patient group and 19 (range 14–21) in the group ofcontrol subjects ðU ¼ 157; p ¼ 0:007Þ. Block design mediantime was 16 s (range 6–44) in the patient group and 11 s(range 6–40) in the group of healthy subjects ðU ¼ 251;p ¼ 0:034Þ. Digit span median score was 11 (range 7–13) inthe patient group and 11 (range 8–15) in the control subjectsðU ¼ 160; p ¼ 0:009Þ. As with the larger patient sample thenumerical differences between the groups were small.Further, when taking the number of statistical comparisonsinto account, the results could not be considered clinicallysignificant. The sub group of patients with many cognitivecomplaints had significantly higher scores than patientswith few complaints on HDRS ðU ¼ 69; p ¼ 0:045Þ and HASðU ¼ 49; p ¼ 0:005Þ.
3.4. Correlations between neuropsychological testresults, psychiatric rating scales and thyroidfunction
No significant correlations were found between neuropsy-chological variables and psychiatric ratings (HDRS and HAS).Also, the psychiatric rating scales were not significantlycorrelated to thyroid function. As assessed by Spearmanrank order correlations three significant correlations be-tween thyroid hormone levels (as assessed by totalthyroxine, free thyroxine and free triiodthyronine) andneuropsychological test results were found (worse perfor-mance with higher total thyroxine). Total thyroxine corre-lated significantly with block design ðr ¼ 0:39; p ¼ 0:035Þ,WAIS picture arrangement ðr ¼ �0:41; p ¼ 0:032Þ and forcedchoice face recognition ðr ¼ �0:488; p ¼ 0:013Þ. However,when adjusting for the large number of correlations (nine-teen) that were examined, these results could not beconsidered significant.
3.5. Psychiatric ratings: follow-up results
In Table 3 the psychiatric ratings from the baselineassessment and the follow-up examinations are shown.From this table it can be seen that there was a significantdecline in affective symptoms from the baseline examina-tion to the follow-up assessments. There was no significantdifference in affective symptoms between the two follow-upexaminations. After having reached euthyroidism only onepatient had an HDRS score above the cut-off (compared to18 at baseline) and two patients had signs of mild anxiety(compared to 27 at baseline). At the 12 months follow-upexamination none had positive HDRS scores and only one hadsigns of mild anxiety. Most important, a dramatic decreasewas detected in the number of patients reporting of memoryand concentration problems. At baseline 20 out of the 31patients had positive scores on HAS item 5. At the firstfollow-up examination only two patients reported feelingsof cognitive deficits complaints and 12 months later threehad positive scores on HAS item 5. Thus, affective symptomsin general, but also the experience of cognitive problems(item 5 on HAS), decreased markedly with treatment ofGraves’ thyrotoxicosis.
4. Discussion
Many previous studies have assessed cognitive functions inhyperthyroid groups, but many of these studies did not havecognitive impairment as their predominant focus. Very fewstudies have combined comprehensive assessment of cogni-tive functions with investigation of affective symptomatol-ogy. Some studies only included a limited number ofneuropsychological tests and some studies were associatedwith (one or more) methodological problems such as lack ofcontrol group (or poorly defined control group) andcomorbidity. Therefore, the impact of Graves’ thyrotoxico-sis on cognitive functioning remains unresolved. In our study,a well-described consecutive patient sample and a well-controlled group of healthy subjects were included andassessed with a wide range of neuropsychological tests.

ARTICLE IN PRESS
Table 3 Affective symptoms for patients ðN ¼ 31Þ at baseline, 3 months after treatment initiation and one year aftertreatment initiation
Baseline Post treatment 3 months Post treatment 1 year
Hamilton depression rating scale 8 (2–14) 1 (0–9)* 0 (0–7)*
Hamilton anxiety scale 11 (2–20) 1 (0–11)* 0 (0–9)*
*Significant difference from baseline po0:001.Values are represented as median (range).Statistical comparisons were performed with Wilcoxon signed ranks tests.
Affective and cognitive symptoms in Graves’ thyrotoxicosis 41
This study showed that the majority of patients in theacute phase of Graves’ thyrotoxicosis reported memory andconcentration problems, which they experienced as inhibit-ing for everyday functioning. However, the patients wereonly significantly impaired on two out of 18 neuropsycholo-gical tests as compared to control subjects and thenumerical differences were clinically insignificant. Thus, ingeneral patients were not cognitively impaired. Not evenpatients with severe cognitive complaints differed signifi-cantly from healthy control subjects on cognitive tests.Further, we did not find any significant correlations betweenthyroid levels and performances on neuropsychologicaltests. Thus, according to our results patients in the acutephase of Graves’ thyrotoxicosis are not cognitively impaireddespite the fact that the patients experience cognitivedeficits.
Our results are in accordance with other studies whoneither could find cognitive impairment in hyperthyroidgroups (Wallace et al., 1980; Paschke et al., 1990) andstudies that did not find significant correlations betweenthyroid function and neuropsychological performances(Trzepacz et al., 1988a; Paschke et al., 1990). However,our results differ from other studies of cognitive functions inhyperthyroid patients. Some studies have demonstratedcorrelations between thyroid hormone levels and tests formemory, attention, psychomotor speed and executivefunctions (MacCrimmon et al., 1979; Wallace et al., 1980).Studies that compared neuropsychological test perfor-mances of patients with Graves’ disease and results fromcontrol subjects found impaired performances for patientsof tests measuring attention and psychomotor speed(Alvarez et al., 1983; Zeitlhofer et al., 1984; Schloteet al., 1992). Impaired performances in test of immediatememory, attention and problem solving compared tocontrols (Zeitlhofer et al., 1984; Paschke et al., 1990;Schlote et al., 1992), and normative data have also beenreported (Trzepacz et al., 1988b). Further, some studieshave demonstrated that performances on tests of memory,attention and psychomotor speed were lower in the acutephase of thyrotoxicosis compared to the level aftertreatment (Whybrow et al., 1969; Trzepacz et al., 1988a).
Differences in previous findings may be due to methodo-logical differences such as different criteria for patientinclusion, different cognitive tests administered, differentcriteria for definition of abnormality and different degreesof affective disorders in different patient samples. In ourstudy, very small differences were found between patientsand control subjects on neuropsychological testing. How-ever, these differences were so small that they were
clinically insignificant. We cannot exclude the possibilitythat the cognitive battery was not sufficiently sensitive toreveal cognitive impairments. However, we used manyneuropsychological tests that in clinical practice aresensitive to cognitive impairments, and most tests arewidely used in both clinical practice and in scientificinvestigations (including some of the previous studies).The discrepancy between our and previous studies may beexplained by methodological differences, and based on theexisting literature and our results we hypothesize, that ifcognitive deficits do occur they are only very mild in degree.A clinical implication of our study may be that referral toneuropsychological examination of patients in the acutephase of Graves’ thyrotoxicosis is very likely not to revealany deficits even if patients complain of memory orconcentration problems. However, it is important toacknowledge the reports of cognitive impairment andinform the patient that these symptoms will disappear withtreatment.
The results from the psychiatric rating scales clearlydemonstrated that the majority of patients in the acutephase of Graves’ thyrotoxicosis had symptoms both ofdepression and anxiety compared to control subjects.However, although these symptoms were bothersome forpatients few met the diagnostic criteria for major depres-sion or anxiety. Many previous studies have found affectivesymptoms including emotional lability, irritability, insomnia,restlessness, agitation, depression and anxiety in the acutephase of Graves’ disease (Whybrow et al., 1969; MacCrim-mon et al., 1979; Kathol et al., 1986; Wallace et al., 1980;Zeitlhofer et al., 1984; Trzepacz et al. 1988a,b, 1989;Paschke et al., 1990; Demet et al., 2002). In one studyelevated anxiety was found as a constant personality trait(Harsch et al., 1992) although personality changes assessedin the acute thyrotoxic phase are considered to be transient(Jadresic, 1990; Freedman et al., 1993). Case reports havedescribed psychotic states associated with thyrotoxicosis(Greer and Parsons, 1968; Steinberg, 1994). Rarely, thyr-otoxicosis may present itself as ‘‘apathetic thyrotoxicosis’’which usually occurs in elderly patients, in which classicalthyrotoxic symptoms are lacking and the presentationmimics depression or pseudo-dementia (Brenner, 1978;Sonino et al., 1993; Ghobrial and Ruby, 2002). Our resultsare in line with previous research documenting thataffective symptoms are very common in the acute phaseof Graves’ disease. Further, the results clearly show thattreatment of the thyrotoxicosis markedly decreased theaffective symptomatology. However, a few retrospectivestudies suggest that some patients have long-term neurop-

ARTICLE IN PRESS
A. Vogel et al.42
sychiatric symptoms despite successful antithyroid treat-ment (Perrild et al., 1986; Bommer et al., 1990), and health-related quality of life impairments may also exist in the longterm (Elberling et al., 2004; Watt et al., 2006). Futurestudies with focus upon previous affective disease, actualthyroid hormone status, number of relapses, and duration ofremission are needed.
Trzepacz et al. (1988a) found that propranolol treatmentalone had positive effect on affective symptoms but thatimprovements in cognitive functioning was first registeredwhen antithyroid medication was administered. In accor-dance with our results Kathol et al. (1986) describedsuccessful treatment of affective symptoms in hyperthyroidpatients with antithyroid therapy alone. Paschke et al.(1990) found a significant decrease in affective symptomsafter euthyroidism was reached but the mode of therapy(antithyroid drugs versus subtotal thyroid resection) had noinfluence on the test result. In hypothyroid patientscognitive functions may not be completely restored despiteT4 treatment (Wekking et al., 2005), and in a recent studyreplacement therapy with T4 plus T3 did not improve moodor cognitive performance as compared to T4 monotherapy(Siegmund et al., 2004). In our study we treated thehyperthyroid patients with methimazole according to titra-tion regime, and it may be interesting to compare withpatients treated with block-replacement regime, where theratio between T3 and T4 may be higher. Future studies areneeded to investigate the effectiveness of different treat-ments for affective (and cognitive) symptoms in the acutephase of Graves’ disease (and in hypothyroidism).
A limitation of the study was that reports of cognitivedysfunction were only assessed with one item from HAS.Results from this single item can only demonstrate theexistence of subjective cognitive deficits, but the degree orcharacter of the subjective cognitive dysfunction cannot beinvestigated. Another limitation is that scores on psychiatricrating scales may be confounded by autonomic arousalsecondary to thyrotoxicosis (e.g. tachycardia, tremor andsweating). To which degree the elevated psychiatric ratingsin patients with Graves’ thyrotoxicosis reflected suchsecondary effects of thyrotoxicosis cannot be investigatedwith our data.
To summarize, we generally found no cognitive impair-ments in a group of consecutively referred, newly diagnosedand untreated patients with Graves’ thyrotoxicosis com-pared to healthy control subjects. Not even patients withmany cognitive complaints differed in cognitive perfor-mance from control subjects. The majority of patients hadsymptoms of depression and anxiety. Follow-up data showeda marked decrease of affective symptoms and subjectivecognitive complaints after treatment of hyperthyroidism.Graves’ disease may lead to experiences of cognitive deficitsbut our results indicate that subjective cognitive symptomsreflect affective and somatic manifestations of thyrotox-icosis and in most patients these symptoms disappear aftertreatment of Graves’ thyrotoxicosis.
Acknowledgements
We wish to thank ‘The Danish Medical Research Council’,‘The 1991 Pharmacy Foundation’, ‘‘Danish Alzheimer Re-
search Foundation’’, and ‘The Health Insurance Foundation’for financial support to the Memory Disorders ResearchGroup. An additional grant was given from the ‘DanishHospital Foundation for Medical Research, Region ofCopenhagen, The Faroe Islands and Greenland’. We aregrateful for the work of technician Betty Fischer.
References
Alvarez, M.A., Gomez, A., Alavez, E., Navarro, D., 1983. Attentiondisturbance in Graves’ disease. Psychoneuroendocrinology 8,451–454.
Bommer, M., Eversmann, T., Pickardt, R., Leonhardt, A., Naber, D.,1990. Psychopathological and neuropsychological symptoms inpatients with subclinical and remitted hyperthyroidism. KlinWochenschr. 68, 552–558.
Brenner, I., 1978. Apathetic hyperthyroidism. J. Clin. Psychiatry 39,479–480.
Buschke, H., 1973. Selective reminding for analysis of memory andlearning. J. Verb. Learn. Verb. Behav. 12, 543–550.
Buschke, H., Sliwinski, M.J., Kuslansky, G., Lipton, R.B., 1997.Diagnosis of early dementia by the double memory test:encoding specificity improves diagnostic sensitivity and specifi-city. Neurology. 48, 989–997.
Demet, M.M., Ozmen, B., Deveci, A., Boyvada, S., Adiguzel, H.,Aydemir, O., 2002. Depression and anxiety in hyperthyroidism.Arch. Med. Res. 33, 552–556.
Elberling, T.V., Rasmussen, A.K., Feldt-Rasmussen, U., Hording, M.,Perrild, H., Waldemar, G., 2004. Impaired health-related qualityof life in Graves’ disease. A prospective study. Eur. J. Endocrinol.151, 549–552.
Engum, A., Bjoro, T., Mykletun, A., Dahl, A.A., 2002. An associationbetween depression, anxiety and thyroid function—a clinicalfact or an artefact? Acta. Psychiatr. Scand. 106, 27–34.
Fahrenfort, J.J., Wilterdink, A.M., van der Veen, E.A., 2000. Long-term residual complaints and psychosocial sequelae afterremission of hyperthyroidism. Psychoneuroendocrinology 25,201–211.
Freedman, M., Sala, M., Faraj, G., Niepomniszcze, H., 1993.Psychological changes during thyrotoxicosis. Thyroidology 5,25–28.
Ghobrial, M.W., Ruby, E.B., 2002. Coma and thyroid storm inapathetic thyrotoxicosis. South. Med. J. 95, 552–554.
Greer, S., Parsons, V., 1968. Schizophrenia-like psychosis in thyroidcrisis. Br. J. Psychiatry 114, 1357–1362.
Hamilton, M., 1967. Development of a rating scale for primarydepressive illness. Br. J. Soc. Clin. Psychol. 6, 278–296.
Hamilton, M., 1969. Diagnosis and rating of anxiety. Br. J. Psychiat.Special Publication 3, 76–79.
Harsch, I., Paschke, R., Usadel, K.H., 1992. The possible etiologicalrole of psychological disturbances in Graves’ disease. Acta. Med.Austriaca. 19 (Suppl. 1:62–5), 62–65.
Jadresic, D.P., 1990. Psychiatric aspects of hyperthyroidism. J.Psychosom. Res. 34, 603–615.
Kathol, R.G., Turner, R., Delahunt, J., 1986. Depression and anxietyassociated with hyperthyroidism: response to antithyroid ther-apy. Psychosomatics 27, 501–505.
MacCrimmon, D.J., Wallace, J.E., MGoldberg, W., Streiner, D.L.,1979. Emotional disturbance and cognitive deficits in hyperthyr-oidism. Psychosom. Med. 41, 331–340.
McLachlan, S.M., Rapoport, B., 2000. Genetic factors in thyroiddisease. In: Braverman, L., Utiger, R. (Eds.), Werner & Ingbar’sThe Thyroid: A Fundamental and Clinical Text. LippincottWilliams & Wilkins, Philadelphia, pp. 474–487.

ARTICLE IN PRESS
Affective and cognitive symptoms in Graves’ thyrotoxicosis 43
Mortensen, E.L., Gade, A., 1993. On the relation betweendemographic variables and neuropsychological test perfor-mance. Scand. J. Psychol. 34, 305–317.
Nelson, H.E., 1976. A modified card sorting test sensitive to frontallobe defects. Cortex 12, 313–324.
Nelson, H.E., O’Connell, A., 1978. Dementia: the estimation ofpremorbid intelligence levels using the new adult reading test.Cortex 14, 234–244.
Paschke, R., Harsch, I., Schlote, B., Vardarli, I., Schaaf, L.,Kaumeier, S., Teuber, J., Usadel, K.H., 1990. Sequentialpsychological testing during the course of autoimmune hy-perthyroidism. Klin Wochenschr. 68, 942–950.
Perrild, H., Hansen, J.M., Arnung, K., Olsen, P.Z., Danielsen, U.,1986. Intellectual impairment after hyperthyroidism. Acta.Endocrinol. (Copenhagen) 112, 185–191.
Placidi, G.P., Boldrini, M., Patronelli, A., Fiore, E., Chiovato, L.,Perugi, G., Marazziti, D., 1998. Prevalence of psychiatricdisorders in thyroid diseased patients. Neuropsychobiology 38,222–225.
Reitan, R.M., 1958. Validity of the trail making test as an indicatorof organic brain damage. Percept. Mot. Skills 8, 271–276.
Schlote, B., Nowotny, B., Schaaf, L., Kleinbohl, D., Schmidt, R.,Teuber, J., Paschke, R., Vardarli, I., Kaumeier, S., Usadel, K.H.,1992. Subclinical hyperthyroidism: physical and mental state ofpatients. Eur. Arch. Psychiatry Clin. Neurosci. 241, 357–364.
Siegmund, W., Spieker, K., Weike, A.I., Giessmann, T., Modess, C.,Dabers, T., Kirsch, G., Sanger, E., Engel, G., Hamm, A.O., Nauck,M., Meng, W., 2004. Replacement therapy with levothyroxineplus triiodotryronine (bioavailable molar ratio 14:1) is notsuperior to thyroxine alone to improve well-being and cognitiveperformance in hypothyroidism. Clinical Endocrinology 60,750–757.
Smith, A., 1973. Symbol digit modalities test. Manual, Los Angeles.Sonino, N., Fava, G.A., Belluardo, P., Girelli, M.E., Boscaro, M.,
1993. Course of depression in cushing’s syndrome: response totreatment and comparison with Graves’ disease. Hormone Res.Basel 39, 202–206.
Spreen, O., Benton, L., 1969. Neurosensory Center Comprehen-sive Examination for Aphasia. University of Victoria Press,Victoria, BC.
Steinberg, P.I., 1994. A case of paranoid disorder associated withhyperthyroidism. Can. J. Psychiatry 39, 153–156.
Stern, R.A., Robinson, B., Thorner, A.R., Arruda, J.E., Prohaska,M.L., Prange Jr., A.J., 1996. A survey study of neuropsychiatriccomplaints in patients with Graves’ disease. J. NeuropsychiatryClin. Neurosci. 8, 181–185.
Stroop, J.R., 1935. Studies of interference in serial verbal reactions.J. Exp. Psychol. 18, 643–662.
Trzepacz, P.T., Klein, I., Roberts, M., Greenhouse, J., Levey, G.S.,1989. Graves’ disease: an analysis of thyroid hormone levels andhyperthyroid signs and symptoms. Am. J. Med. 87, 558–561.
Trzepacz, P.T., McCue, M., Klein, I., Greenhouse, J., Levey, G.S.,1988a. Psychiatric and neuropsychological response to propra-nolol in Graves’ disease. Biol. Psychiatry 23, 678–688.
Trzepacz, P.T., McCue, M., Klein, I., Levey, G.S., Greenhouse, J.,1988b. A psychiatric and neuropsychological study of patientswith untreated Graves’ disease. Gen. Hosp. Psychiatry 10,49–55.
Wallace, J.E., MacCrimmon, D.J., Goldberg, W.M., 1980. Acutehyperthyroidism: cognitive and emotional correlates. J. Abnorm.Psychol. 89, 519–527.
Warrington, E.K., 1974. Deficient recognition memory in organicamnesia. Cortex 10, 289–291.
Watt, T., Groenvold, M., Rasmussen, Å.K., Bonnema, S.J., Hegedus,L., Bjorner, J.B., Feldt-Rasmussen, U., 2006. Quality of life inpatients with benign thyroid disorders. A Review. Eur. J.Endocrinology 154, 501–510.
Wekking, E.M., Appelhof, B.C., Fliers, E., Schene, A.H., Huyser, J.,Tijssen, J.G.P., Wiersinga, W.M., 2005. Cognitive functioning andwell-being in euthyroid patients on thyroxine replacementtherapy for primary hypothyroidism. Eur. J. Endocrinology 153,747–753.
Whybrow, P.C., Prange Jr., A.J., Treadway, C.R., 1969. Mentalchanges accompanying thyroid gland dysfunction. A reappraisalusing objective psychological measurement. Arch. Gen. Psychia-try 20, 48–63.
Zeitlhofer, J., Saletu, B., Stary, J., Ahmadi, R., 1984. Cerebralfunction in hyperthyroid patients. Psychopathology, psycho-metric variables, central arousal and time perception beforeand after thyreostatic therapy. Neuropsychobiology 11, 89–93.