mindfulness, health symptoms and healthcare utilization: active facets and possible affective...
TRANSCRIPT
For Peer Review O
nly
Mindfulness, health symptoms, and healthcare utilization:
active facets and possible affective pathways
Journal: AIDS Care - Psychology, Health & Medicine - Vulnerable Children and Youth
Studies
Manuscript ID: PHM-2013-02-0131.R2
Journal Selection: Psychology, Health & Medicine
Keywords: symptoms, health utilization, mindfulness, emotion, mindfulness facets
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences

For Peer Review O
nly
Mindfulness facets and health 1
Mindfulness, health symptoms, and healthcare utilization: active facets and possible affective
mediators
RUNNING HEAD: MINDFULNESS FACETS AND HEALTH
Page 1 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 2
Abstract
Prior work has linked mindfulness with superior physical and psychological health
outcomes. However, studies to date have infrequently tested the unique contributions of individual
mindfulness facets, inadequately tested links between facets and healthcare utilization, and have not
tested whether depression or anxiety may influence these links. In the current report, 40 young,
middle aged and older adults (N = 121) completed measures of dispositional mindfulness, health,
healthcare utilization and depression/anxiety. As expected, global trait mindfulness did not predict
outcomes while individual mindfulness facets predicted both objective and subjective health as well
as healthcare utilization. Across models, observe scores – the tendency to attend to thoughts,
sensations and feelings – predicted poorer, and non-reactivity scores better, outcomes even when
controlling for demographic and health confounds. Depressed and anxious emotion reduced some
but not all mindfulness-health links. Results are discussed in terms of the mechanisms by which
greater mindfulness may facilitate better health and health behaviour.
Key words: mindfulness; mindfulness facets; health; symptom reporting; healthcare utilization;
anxiety; depression
Page 2 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 3
Mindfulness – the ability or tendency towards bringing attention to present experiences in a
nonjudgmental or accepting way (Baer, Smith, Hopkins, Krietemeyer, & Toney, 2006) – predicts
better health. Trait mindfulness predicts better health and health behaviour (Greeson, 2009), fewer
symptoms (Brown & Ryan, 2003), better perceived health (Zvolensky et al., 2006) and lower
healthcare utilization (Brown & Ryan, 2003). Mindfulness also predicts fewer psychological
symptoms, lower anxiety and less depression (McCracken, Gauntlett-Gilbert, & Vowles, 2007).
However, aspects of these links remain unclear. First, the most relevant facets of
mindfulness are unknown (Schneider, Hough, & Dunnette, 1996). Describing, awareness, non-
judging, and non-reactivity facets predict fewer, but observe greater, symptoms (Baer et al., 2008).
Specifically relevant to physical health, observe scores index the tendency to attend to internal
stimuli such as thoughts, sensations and feelings, while non-reactivity reflects a considered approach
to these phenomena and responding with purposeful behaviour (Reynolds, Consedine, &
McCambridge, 2013).
Second, data have primarily linked mindfulness facets to subjective rather than objective
metrics. We contrast the ability of mindfulness facets to predict objective versus subjective
outcomes. Three, while total mindfulness predicts health behaviour (Brown & Ryan, 2003), how
specific facets predict utilization is unclear. This report evaluates which facets predict utilization for
chronic and psychological issues.
Finally, the mechanisms by which mindfulness predicts health remain unclear (Coffey,
Hartman, & Fredrickson, 2010). Although mindfulness may bolster disease resistance (Davidson et
al., 2003) or reduce symptom sensitivity (Zeidan et al., 2011), it may also predict better health
indirectly by lowering anxiety and depression (Zvolensky et al., 2006). Mindfulness predicts lower
anxiety and depression (Williams, Ciarrochi, & Deane, 2010) and negative affect (Giluk, 2009).
Commensurately, depressed affects predict greater symptoms (Consedine, 2008) and utilization
(Callahan, Kesterson, & Tierney, 1997), while anxiety has weaker links to symptoms but predicts
greater utilization (Consedine & Moskowitz, 2007). Effects on subjective outcomes persist even
Page 3 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 4
when controlling objective disease metrics (Cohen et al., 1995), implying affect may be more
heavily implicated in subjective symptomology.
Overall, we expected mindfulness facets would better predict outcomes than a global
mindfulness score. We expected the observe facet to predict greater symptomology and other facets
to predict less; neither facet nor total scores should predict objective health (number of diagnosed
conditions). Finally, depression and anxiety should weaken links between mindfulness and
subjective outcomes but leave the objective outcome models essentially unchanged.
Methods
Participants
40 community-dwelling adults aged 18+ years in each of 18-34, 35-59, and 60+ year
brackets (Total N = 121) were recruited. Two thirds were female, 54.5% married/living with
partner, and 86% of majority ethnicity; 16 years education was average.
Procedures
Recruitment used advertisements and flyers, with electronic advertisements sent via e-mail
and Facebook. Interested participants contacted the coordinator who posted paper questionnaires
and return envelopes. No exclusions or incentives were used and no drop outs were recorded.
Measures
Demographics and confounds. Self-reported gender, age (years), weight (kg), height (cm)
smoking history (ever/never), and current exercise frequency (using a 0 “never” to 7 “daily”) scale.
Dispositional mindfulness. Five Facet Mindfulness Questionnaire (FFMQ) (Baer et al.,
2006). The FFMQ assesses five facets and has good psychometric properties (Baer et al., 2008). In
this report reliabilities were .78 (observe), .91 (describe), .88 (awareness), .87 (non-judge), and .83
(non-react).
Objective health conditions. Participants reported formal diagnoses of physical or mental
health conditions. Condition counts were aggregated.
Page 4 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 5
Subjective symptomology. The 42-item Wahler Physical Symptom Inventory (WPSI)
(Wahler, 1968) has respondents indicate how often they are bothered by symptoms including
backaches, difficulty breathing, pain, and bowel trouble (Frezza, Wachtel, & Gordhamer, 2008).
The WPSI has good internal consistency and is widely used (Consedine et al., 2006). Reliability
was .87.
Healthcare utilisation. Participants reported the frequency of doctor/health professional
visits for chronic conditions and psychological issues in the past year.
Anxious and depressed affect. Hospital Anxiety and Depression Scale (HADS) (Zigmond &
Snaith, 1983). The scale excludes somatic symptoms (Bjelland, Dahl, Haug, & Neckelmann, 2002)
and has good internal consistency (Bjelland et al., 2002), convergent validity, and test retest
reliability. Reliabilities were .77 (anxiety) and .65 (depression).
Analytic strategy
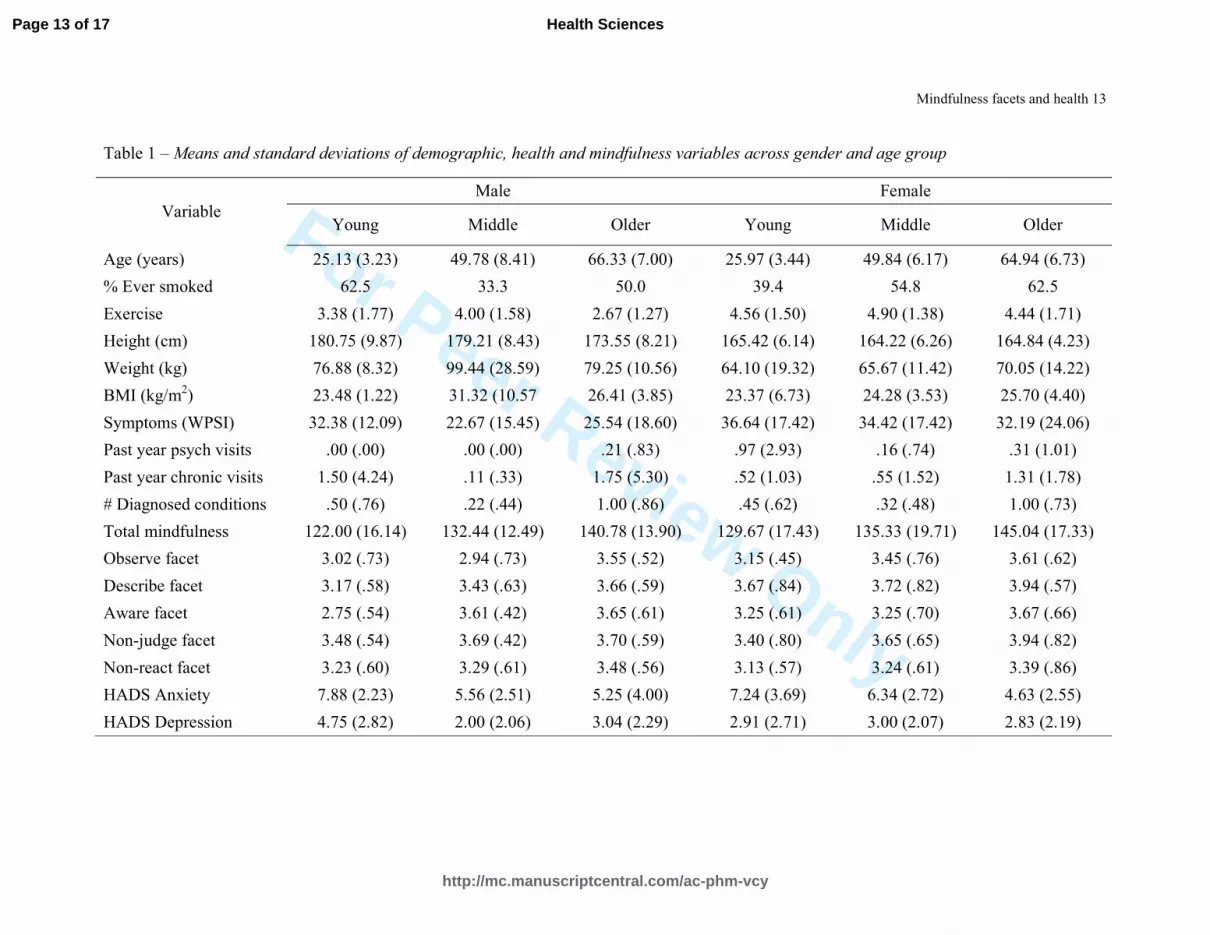
Data were analyzed in two phases. First, we characterized our sample (Table 1). Second,
step-wise linear regressions regressed outcomes on demographics/confounds, mindfulness facets,
and possible affect. Confounds and mindfulness were entered in Step 1 and depression/anxiety at
Step 2.
Results
Characteristics of the sample are displayed in Table 1. Health problems afflicted 57% of the
sample and 47% had been diagnosed with a condition (ranging from hayfever to CHD); 10.7% had
been diagnosed with a mental condition.
Multivariate prediction of objective and subjective health
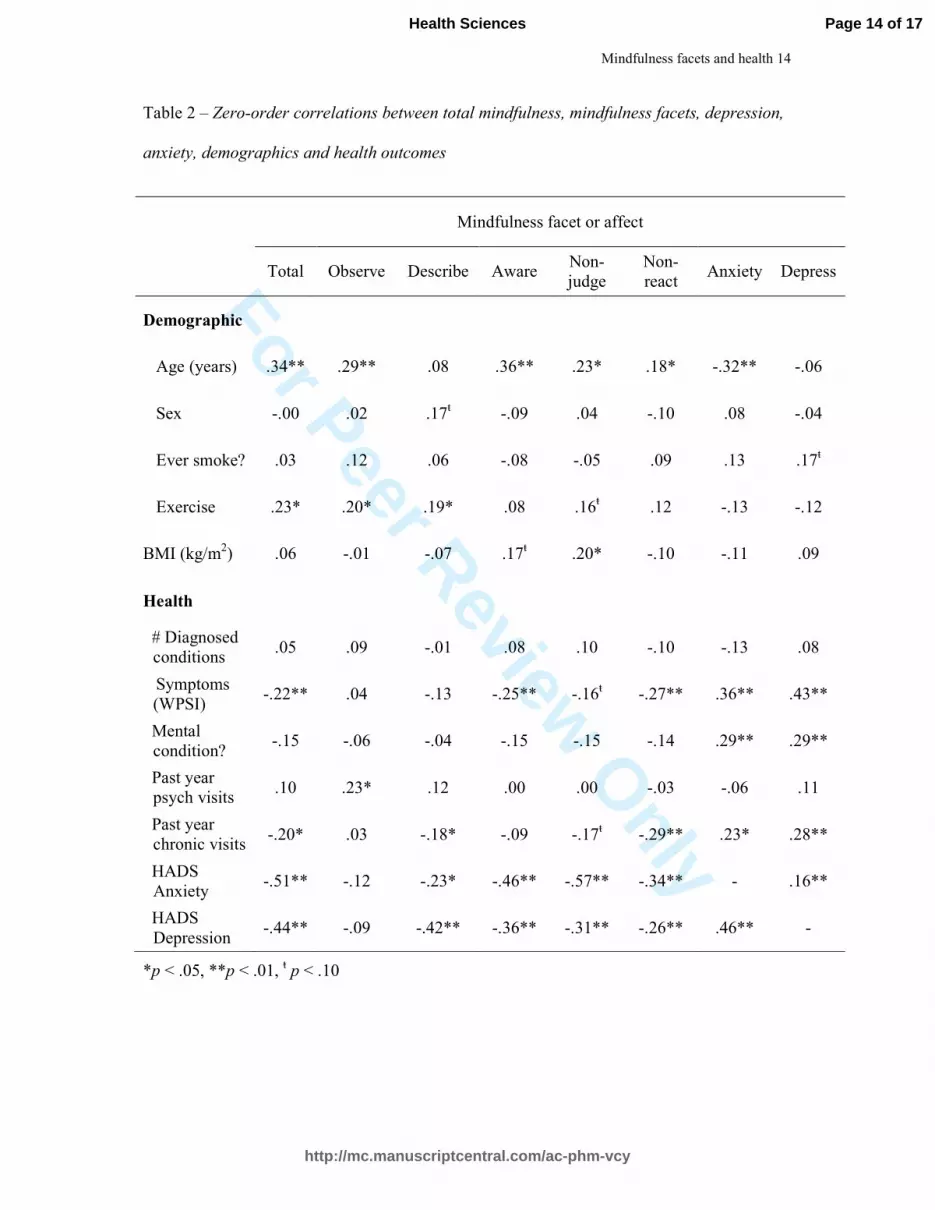
After checking univariate correlations (Table 2), we assessed whether facets versus total
mindfulness better predicted objective conditions. Total mindfulness was a poor predictor (Table 3);
the initial model was marginal, F (6, 114) = 1.90, p = .09, with no mindfulness effect. Adding
depression and anxiety in Step 2 did not improve fit, F∆ (2, 112) = 1.27, n. s. The model using
Page 5 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 6
facets was slightly better. Although neither Step 1 nor Step 2 models were significant, non-
reactivity predicted fewer conditions (see Table 3).
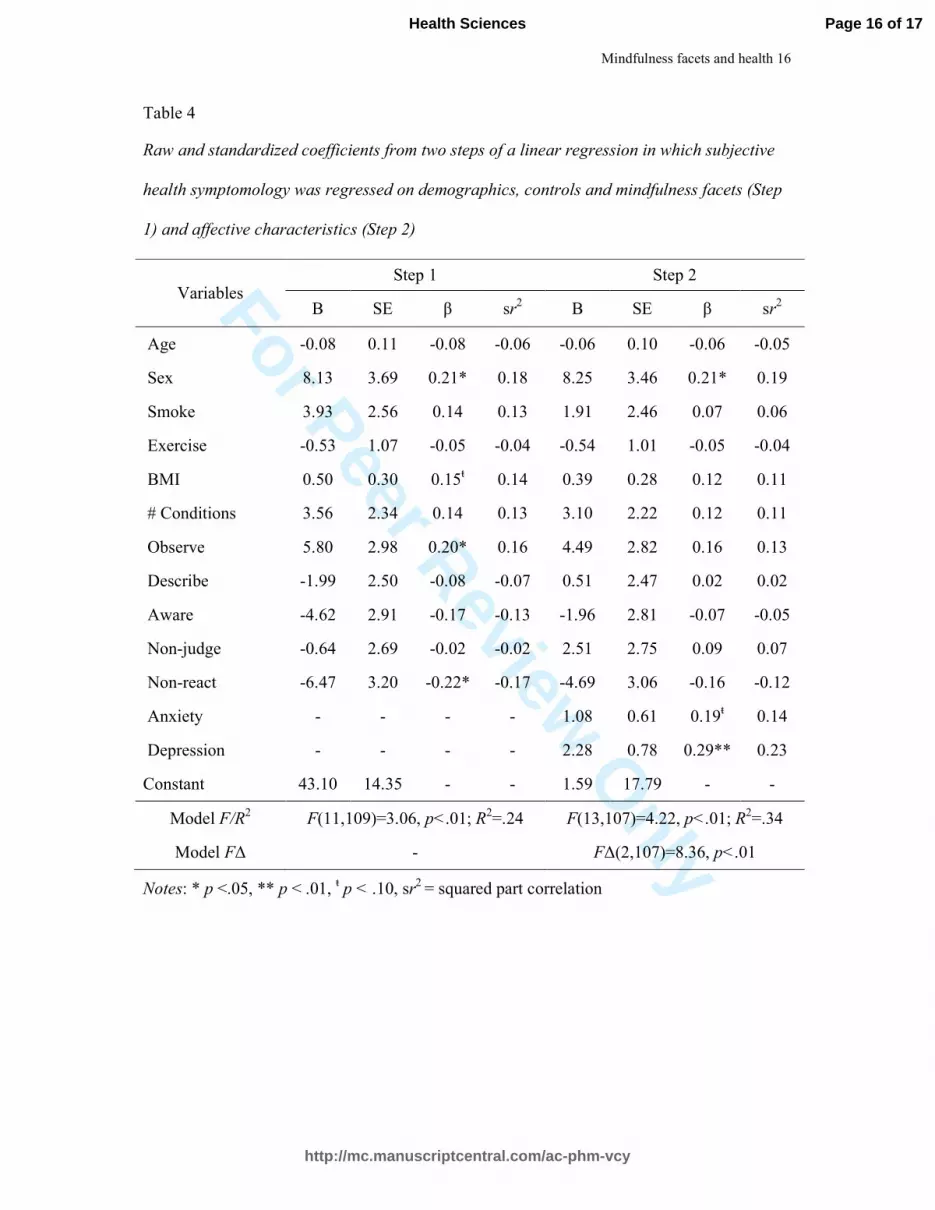
Given this pattern, hypotheses regarding subjective symptoms were tested using facets
alone. Symptomology was predicted at Step 1 by being female, greater observe, and lower non-
reactivity scores. After adding depression and anxiety at Step 2 symptomology remained greater
among females but observe and non-reactivity effects were eliminated while greater depression and,
marginally, anxiety were now predictors (Table 4).
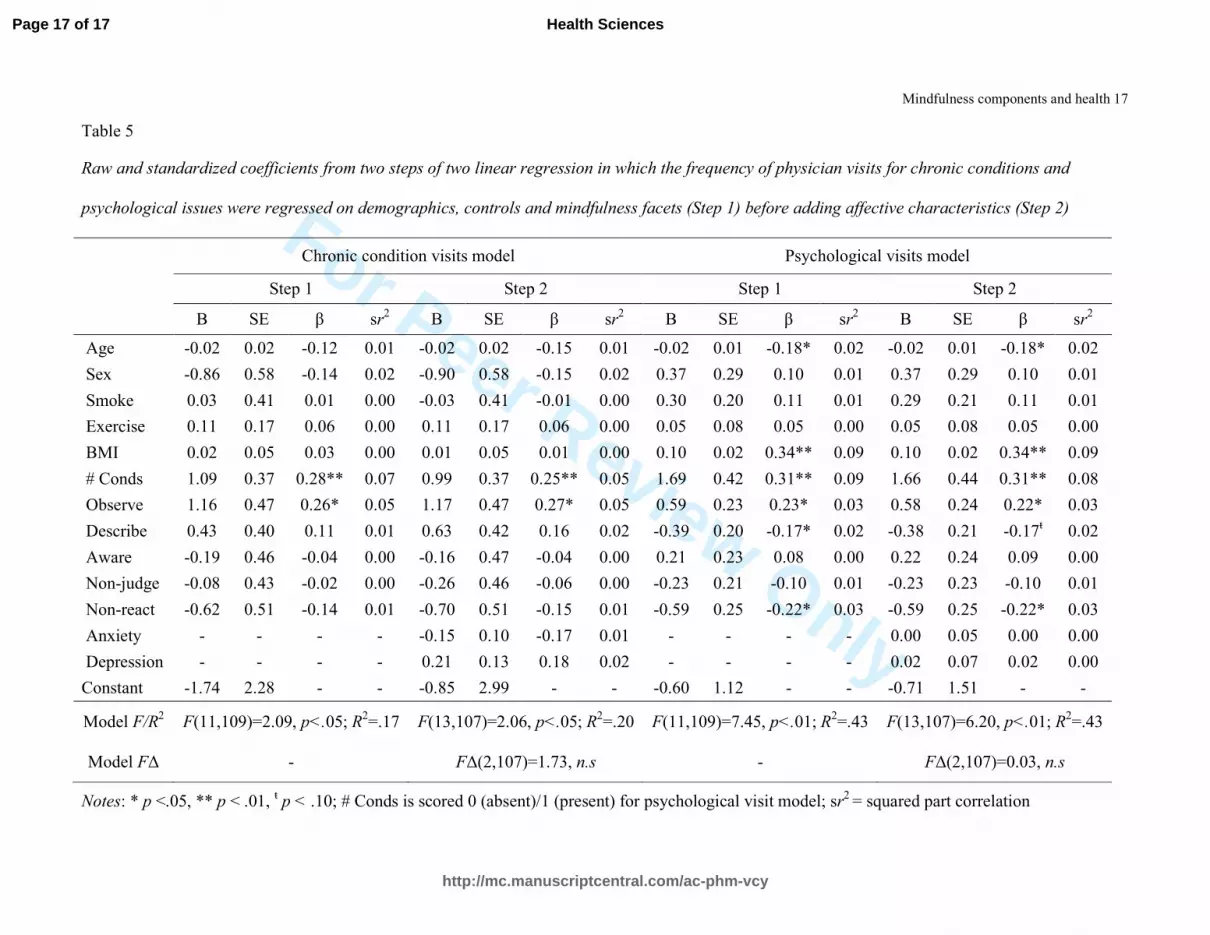
Multivariate prediction of chronic condition and psychological visit frequency
The initial model predicting chronic visit frequency was significant (Table 5). Visits were
predicted by health conditions and greater observe scores. Adding depression and anxiety changed
nothing in this model. The initial model predicting psychological visits explained 43% variance;
having a psychological diagnosis, greater BMI, lower age, greater observe, lower non-reactivity,
and, marginally, lower describe scores predicted more visits. Adding depression and anxiety did not
alter these effects; the model remained significant but was not improved.
Discussion
The current report makes several contributions. First, relative to mindfulness facets, total
mindfulness failed to predict outcome; effects held even when controlling for confounds. Second,
mindfulness facets were better predicts of subjective versus objective health indices. Finally,
depressed or anxious affect may influence some but not all mindfulness-health links.
Operationalizing mindfulness in health and health behaviour research
Specific mindfulness facets appear more useful than global scores in predicting health. As
expected, observe scores predicted greater symptomology but non-reactivity scores predicted less.
Similarly, higher observe scores predicted more frequent chronic conditions and psychological
visits while non-reactivity scores predicted less frequent psychological visits. High observe
individuals may not have objectively worse health but experience health as poorer while non-
reactivity may index the ability to manage health issues without responding with anxiety or
Page 6 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 7
impulsiveness (Baer, 2009). Overall, notwithstanding whether symptoms, conditions, or behaviours
were considered, modelling mindfulness facets was consistently more informative. Importantly, it
was not just that mindfulness predicted more conditions (Table 3). Even when condition counts
(and other confounds) were covaried, persons with greater observe scores consumed more
healthcare while those with greater non-react scores consumed less (see Tables 4-5).
The mechanism question – depression and anxiety as possible mediators
As expected, the link between non-reactivity and objective conditions did not change (Table
4), but effects for observe and non-react facets in predicting subjective symptoms were eliminated
after controlling for HADS scores (Table 5). Although low reliability in the HADS-D in this
healthy sample is important (see Mykletun, Stordal, & Dahl, 2001), negative affect mediates
mindfulness-sleep links (Caldwell, Harrison, Adams, Quin, & Greeson, 2010). Because
mindfulness predicts less depression/anxiety and negative affects predict greater symptoms and
utilization, adding such variables might weaken mindfulness-health links. In our study, however,
observe scores (associated with an internal focus) did not predict depressive symptoms (Table 2),
but predicted greater utilization even when controlling for depression. This pattern suggests the link
between mindfulness facets and utilization is not merely a function of a depressogenic internal
focus or affect more broadly (Table 5). Indeed, the role of negative affect in mindfulness-health
links may be most prominent when assessing subjective symptoms. Behaviourally, persons with
greater non-reactivity have more flexible cognitive control (Anicha, Ode, Moeller, & Robinson,
2012) and persons who are less reactive may be less prone to reflexively seek care when confronted
with symptoms or health anxiety.
Obviously, interpretations are constrained by design. Although using distinct metrics to
assess mindfulness, symptoms, and behaviour should ameliorate method bias (Podsakoff,
MacKenzie, & Podsakoff, 2012), only the diagnosis count is objective and our sample relatively
young and healthy. Objective measures of disease are obvious next steps as are designs among older
groups or those in poorer health; links between mindfulness and outcome might vary in less healthy
Page 7 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences

For Peer Review O
nly
Mindfulness facets and health 8
groups. We assessed trait mindfulness not meditation experience; measurement may vary with
experience (Veehof, ten Klooster, Taal, Westerhof, & Bohlmeijer, 2011). Most interventions
include formal training/practice that is supplemented by informal use. In theory, living mindfully
rather than training should produce benefits (Dimidjian & Linehan, 2006). Our data do not enable
commentary on this issue.
Despite such limitations, the present work extends data linking mindful functioning to
health. Tendencies to observe and/or react predicted outcomes, for both objective and subjective
symptomology, as well as for utilization. While depressed and anxious affect reduced the effects on
subjective symptomology, objective health and healthcare utilization models remained unchanged.
Providing participants are prepared for initial increases in symptomatic awareness, mindfulness
interventions aimed at health might thus profitably target non-reactivity.
Page 8 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 9
References
Anicha, C. L., Ode, S., Moeller, S. K., & Robinson, M. D. (2012). Toward a cognitive view of trait
mindfulness: distinct cognitive skills predict its observing and nonreactivity facets. Journal
of Personality, 80(2), 255-285.
Baer, R. A. (2009). Self-Focused Attention and Mechanisms of Change in Mindfulness-Based
Treatment. Cognitive Behaviour Therapy, 38(sup1), 15-20.
Baer, R. A., Smith, G. T., Hopkins, J., Krietemeyer, J., & Toney, L. (2006). Using self-report
assessment methods to explore facets of mindfulness. Assessment, 13(1), 27-45.
Baer, R. A., Smith, G. T., Lykins, E., Button, D., Krietemeyer, J., Sauer, S., et al. (2008). Construct
validity of the Five Facet Mindfulness Questionnaire in meditating and non-meditating
samples. Assessment, 15(3), 329-342.
Bjelland, I., Dahl, A. A., Haug, T. T., & Neckelmann, D. (2002). The validity of the Hospital
Anxiety and Depression Scale: An updated literature review. Journal of Psychosomatic
Research, 52(2), 69-77.
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in
psychological well-being. Journal of Personality and Social Psychology, 84(4), 822-848.
Caldwell, K., Harrison, M., Adams, M., Quin, R. H., & Greeson, J. (2010). Developing mindfulness
in college students through movement-based courses: Effects on self-regulatory self-
efficacy, mood, stress, and sleep quality. Journal of American College Health, 58(5), 433-
442.
Callahan, C. M., Kesterson, J. G., & Tierney, W. M. (1997). Association of symptoms of depression
with diagnostic test charges among older adults. Annals of Internal Medicine, 126, 426-432.
Coffey, K. A., Hartman, M., & Fredrickson, B. L. (2010). Deconstructing mindfulness and
constructing mental health: Understanding mindfulness and its mechanisms of action.
Mindfulness, 1(4), 235-253.
Page 9 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 10
Cohen, S., Doyle, W. J., Skoner, D. P., Fireman, P., Gwaltney, J. M., & Newsom, J. T. (1995). State
and trait negative affect as predictors of objective and subjective symptoms of respiratory
viral infections. Journal of Personality & Social Psychology, 68(1), 159-169.
Consedine, N. S. (2008). The health-promoting and health-damaging effects of emotions: the view
from developmental functionalism. In M. Lewis, J. Haviland-Jones & L. F. Barrett (Eds.),
Handbook of emotions (3rd ed., pp. 676 - 690). New York: Guilford.
Consedine, N. S., Magai, C., Kudadjie-Gyamfi, E. K., Kaluk Longfellow, J., Ungar, T. M., & King,
A. R. (2006). Stress versus discrete negative emotion in the prediction of physical
complaints: Does predictive utility vary across groups. Cultural Diversity and Ethnic
Minority Psychology, 12(3), 541-557.
Consedine, N. S., & Moskowitz, J. T. (2007). The role of discrete emotions in health outcomes: a
critical review. Journal of Applied and Preventive Psychology, 12(2), 59-75.
Davidson, R. J., Kabat-Zinn, J., Schumacher, J., Rosenkranz, M., Muller, D., Santorelli, S. F., et al.
(2003). Alterations in brain and immune function produced by mindfulness meditation.
Psychosomatic Medicine, 65(4), 564-570.
Dimidjian, S., & Linehan, M. M. (2006). Defining an agenda for future research on the clinical
application of mindfulness practice. Clinical Psychology: Science and Practice, 10(2), 166-
171.
Frezza, E. E., Wachtel, M. S., & Gordhamer, R. (2008). Psychological Assessment. In N. T.
Nguyen, E. J. Maria, S. Ikramuddin & M. M. Hutter (Eds.), The SAGES Manual (pp. 43-50):
Springer New York.
Giluk, T. L. (2009). Mindfulness, Big Five personality, and affect: A meta-analysis. Personality
and Individual Differences, 47(8), 805-811.
Greeson, J. M. (2009). Mindfulness Research Update: 2008. Complementary Health Practice
Review, 14(1), 10-18.
Page 10 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 11
McCracken, L. M., Gauntlett-Gilbert, J., & Vowles, K. E. (2007). The role of mindfulness in a
contextual cognitive-behavioral analysis of chronic pain-related suffering and disability.
PAIN, 131(1-2), 63-69.
Mykletun, A., Stordal, E., & Dahl, A. A. (2001). Hospital Anxiety and Depression (HAD) Scale:
factor structure, item analyses and internal consistency in a large population. British Journal
of Psychiatry, 179(540-544).
Podsakoff, P. M., MacKenzie, S. B., & Podsakoff, N. P. (2012). Sources of method bias in social
science research and recommendations on how to control it. Annual Review of Psychology,
63, 539-569.
Reynolds, L. M., Consedine, N. S., & McCambridge, S. M. (2013). Experimentally induced disgust
and avoidance in colorectal cancer scenarios: The role of non-judging and non-reacting
mindfulness. Mindfulness.
Schneider, R. J., Hough, L. M., & Dunnette, M. D. (1996). Broadsided by broad traits: How to sink
science in five dimensions or less. Journal of Organizational Behavior, 17(6), 639-655.
Veehof, M., ten Klooster, P., Taal, E., Westerhof, G., & Bohlmeijer, E. (2011). Psychometric
properties of the Dutch Five Facet Mindfulness Questionnaire (FFMQ) in patients with
fibromyalgia. Clinical Rheumatology, 30(8), 1045-1054.
Wahler, H. J. (1968). The physical symptoms inventory: Measuring levels of somatic complaining
behavior. Journal of Clinical Psychology, 24(2), 207-211.
Williams, V., Ciarrochi, J., & Deane, F. P. (2010). On being mindful, emotionally aware, and more
resilient: Longitudinal pilot study of police recruits. Australian Psychologist, 45(4), 274-
282.
Zeidan, F., Martucci, K. T., Kraft, R. A., Gordon, N. S., McHaffie, J. G., & Coghill, R. C. (2011).
Brain mechanisms supporting the modulation of pain by mindfulness meditation. The
Journal of Neuroscience, 31(14), 5540-5548.
Page 11 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences

For Peer Review O
nly
Mindfulness facets and health 12
Zigmond, A. S., & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta
Psychiatrica Scandinavica, 67(6), 361-370.
Zvolensky, M. J., Solomon, S. E., McLeish, A. C., Cassidy, D., Bernstein, A., Bowman, C. J., et al.
(2006). Incremental validity of mindfulness-based attention in relation to the concurrent
prediction of anxiety and depressive symptomology and perceptions of health. Cognitive
Behaviour Therapy, 35(3), 148-158.
Page 12 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review Only
Mindfulness facets and health 13
Table 1 – Means and standard deviations of demographic, health and mindfulness variables across gender and age group
Variable
Male Female
Young Middle Older Young Middle Older
Age (years) 25.13 (3.23) 49.78 (8.41) 66.33 (7.00) 25.97 (3.44) 49.84 (6.17) 64.94 (6.73)
% Ever smoked 62.5 33.3 50.0 39.4 54.8 62.5
Exercise 3.38 (1.77) 4.00 (1.58) 2.67 (1.27) 4.56 (1.50) 4.90 (1.38) 4.44 (1.71)
Height (cm) 180.75 (9.87) 179.21 (8.43) 173.55 (8.21) 165.42 (6.14) 164.22 (6.26) 164.84 (4.23)
Weight (kg) 76.88 (8.32) 99.44 (28.59) 79.25 (10.56) 64.10 (19.32) 65.67 (11.42) 70.05 (14.22)
BMI (kg/m2) 23.48 (1.22) 31.32 (10.57 26.41 (3.85) 23.37 (6.73) 24.28 (3.53) 25.70 (4.40)
Symptoms (WPSI) 32.38 (12.09) 22.67 (15.45) 25.54 (18.60) 36.64 (17.42) 34.42 (17.42) 32.19 (24.06)
Past year psych visits .00 (.00) .00 (.00) .21 (.83) .97 (2.93) .16 (.74) .31 (1.01)
Past year chronic visits 1.50 (4.24) .11 (.33) 1.75 (5.30) .52 (1.03) .55 (1.52) 1.31 (1.78)
# Diagnosed conditions .50 (.76) .22 (.44) 1.00 (.86) .45 (.62) .32 (.48) 1.00 (.73)
Total mindfulness 122.00 (16.14) 132.44 (12.49) 140.78 (13.90) 129.67 (17.43) 135.33 (19.71) 145.04 (17.33)
Observe facet 3.02 (.73) 2.94 (.73) 3.55 (.52) 3.15 (.45) 3.45 (.76) 3.61 (.62)
Describe facet 3.17 (.58) 3.43 (.63) 3.66 (.59) 3.67 (.84) 3.72 (.82) 3.94 (.57)
Aware facet 2.75 (.54) 3.61 (.42) 3.65 (.61) 3.25 (.61) 3.25 (.70) 3.67 (.66)
Non-judge facet 3.48 (.54) 3.69 (.42) 3.70 (.59) 3.40 (.80) 3.65 (.65) 3.94 (.82)
Non-react facet 3.23 (.60) 3.29 (.61) 3.48 (.56) 3.13 (.57) 3.24 (.61) 3.39 (.86)
HADS Anxiety 7.88 (2.23) 5.56 (2.51) 5.25 (4.00) 7.24 (3.69) 6.34 (2.72) 4.63 (2.55)
HADS Depression 4.75 (2.82) 2.00 (2.06) 3.04 (2.29) 2.91 (2.71) 3.00 (2.07) 2.83 (2.19)
Page 13 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 14
Table 2 – Zero-order correlations between total mindfulness, mindfulness facets, depression,
anxiety, demographics and health outcomes
Mindfulness facet or affect
Total Observe Describe Aware Non-
judge
Non-
react Anxiety Depress
Demographic
Age (years) .34** .29** .08 .36** .23* .18* -.32** -.06
Sex -.00 .02 .17ŧ -.09 .04 -.10 .08 -.04
Ever smoke? .03 .12 .06 -.08 -.05 .09 .13 .17ŧ
Exercise .23* .20* .19* .08 .16ŧ .12 -.13 -.12
BMI (kg/m2) .06 -.01 -.07 .17
ŧ .20* -.10 -.11 .09
Health
# Diagnosed
conditions .05 .09 -.01 .08 .10 -.10 -.13 .08
Symptoms
(WPSI) -.22** .04 -.13 -.25** -.16
ŧ -.27** .36** .43**
Mental
condition? -.15 -.06 -.04 -.15 -.15 -.14 .29** .29**
Past year
psych visits .10 .23* .12 .00 .00 -.03 -.06 .11
Past year
chronic visits -.20* .03 -.18* -.09 -.17
ŧ -.29** .23* .28**
HADS
Anxiety -.51** -.12 -.23* -.46** -.57** -.34** - .16**
HADS
Depression -.44** -.09 -.42** -.36** -.31** -.26** .46** -
*p < .05, **p < .01, ŧ p < .10
Page 14 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences

For Peer Review Only
Mindfulness facets and health 15
Table 3:
Raw and standardized coefficients from two steps of two linear regressions in which objective health condition frequency was regressed on
demographics, controls and either global mindfulness or mindfulness facets (Step 1) before adding affective characteristics (Step 2)
Global mindfulness model Mindfulness facets model
Step 1 Step 2 Step 1 Step 2
B SE β sr2 B SE β sr
2 B SE β sr
2 B SE β sr
2
Age .01 .00 .28** .06 .01 .00 .25* .05 .01 .00 .25* .04 .01 .00 .22* .03
Sex -.09 .14 -.06 .00 -.09 .14 -.06 .00 -.18 .15 -.12 .01 -.18 .15 -.12 .01
Smoke -.08 .10 -.07 .00 -.09 .11 -.08 .01 -.06 .10 -.05 .00 -.07 .11 -.07 .00
Exercise -.03 .04 -.06 .00 -.02 .04 -.05 .00 -.03 .04 -.08 .00 -.03 .04 -.07 .00
BMI .00 .01 -.01 .00 .00 .01 -.03 .00 -.01 .01 -.06 .00 -.01 .01 -.08 .01
Global MF .00 .00 -.02 .00 .00 .00 .00 .00 - - - - - - - -
Observe - - - - - - - - .15 .12 .14 .01 .15 .12 .13 .01
Describe - - - - - - - - .00 .10 .00 .00 .05 .11 .05 .00
Aware - - - - - - - - -.03 .12 -.02 .00 -.01 .12 -.01 .00
Non-judge - - - - - - - - .14 .11 .14 .01 .11 .12 .11 .01
Non-react - - - - - - - - -.29 .13 -.25* .04 -.30 .13 -.26* .04
Anxiety - - - - -.03 .02 -.12 .01 - - - - -.03 .03 -.14 .01
Depression - - - - .05 .03 .16 .02 - - - - .05 .03 .16 .02
Constant .43 .58 - - .46 .75 - - 0.61 0.58 - - .73 .77 - -
Model F/R2 F(6,114)=1.90, n.s.; R
2=.09 F(8,112)=1.75, n.s; R
2=.11 F(10,110)=1.76, n.s.; R
2=.14 F(12,108)=1.68, p=.08; R
2=.16
Model F∆ - F∆(2,112)=1.27, n.s F∆(2,108)=1.25, n.s
Notes: * p <.05, ** p < .01, ŧ p < .10, sr
2 = squared part correlation
Page 15 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review O
nly
Mindfulness facets and health 16
Table 4
Raw and standardized coefficients from two steps of a linear regression in which subjective
health symptomology was regressed on demographics, controls and mindfulness facets (Step
1) and affective characteristics (Step 2)
Variables Step 1 Step 2
B SE β sr2 B SE β sr
2
Age -0.08 0.11 -0.08 -0.06 -0.06 0.10 -0.06 -0.05
Sex 8.13 3.69 0.21* 0.18 8.25 3.46 0.21* 0.19
Smoke 3.93 2.56 0.14 0.13 1.91 2.46 0.07 0.06
Exercise -0.53 1.07 -0.05 -0.04 -0.54 1.01 -0.05 -0.04
BMI 0.50 0.30 0.15ŧ 0.14 0.39 0.28 0.12 0.11
# Conditions 3.56 2.34 0.14 0.13 3.10 2.22 0.12 0.11
Observe 5.80 2.98 0.20* 0.16 4.49 2.82 0.16 0.13
Describe -1.99 2.50 -0.08 -0.07 0.51 2.47 0.02 0.02
Aware -4.62 2.91 -0.17 -0.13 -1.96 2.81 -0.07 -0.05
Non-judge -0.64 2.69 -0.02 -0.02 2.51 2.75 0.09 0.07
Non-react -6.47 3.20 -0.22* -0.17 -4.69 3.06 -0.16 -0.12
Anxiety - - - - 1.08 0.61 0.19ŧ 0.14
Depression - - - - 2.28 0.78 0.29** 0.23
Constant 43.10 14.35 - - 1.59 17.79 - -
Model F/R2 F(11,109)=3.06, p<.01; R
2=.24 F(13,107)=4.22, p<.01; R
2=.34
Model F∆ - F∆(2,107)=8.36, p<.01
Notes: * p <.05, ** p < .01, ŧ p < .10, sr
2 = squared part correlation
Page 16 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences
For Peer Review Only
Mindfulness components and health 17
Table 5
Raw and standardized coefficients from two steps of two linear regression in which the frequency of physician visits for chronic conditions and
psychological issues were regressed on demographics, controls and mindfulness facets (Step 1) before adding affective characteristics (Step 2)
Chronic condition visits model Psychological visits model
Step 1 Step 2 Step 1 Step 2
B SE β sr2 B SE β sr
2 B SE β sr
2 B SE β sr
2
Age -0.02 0.02 -0.12 0.01 -0.02 0.02 -0.15 0.01 -0.02 0.01 -0.18* 0.02 -0.02 0.01 -0.18* 0.02
Sex -0.86 0.58 -0.14 0.02 -0.90 0.58 -0.15 0.02 0.37 0.29 0.10 0.01 0.37 0.29 0.10 0.01
Smoke 0.03 0.41 0.01 0.00 -0.03 0.41 -0.01 0.00 0.30 0.20 0.11 0.01 0.29 0.21 0.11 0.01
Exercise 0.11 0.17 0.06 0.00 0.11 0.17 0.06 0.00 0.05 0.08 0.05 0.00 0.05 0.08 0.05 0.00
BMI 0.02 0.05 0.03 0.00 0.01 0.05 0.01 0.00 0.10 0.02 0.34** 0.09 0.10 0.02 0.34** 0.09
# Conds 1.09 0.37 0.28** 0.07 0.99 0.37 0.25** 0.05 1.69 0.42 0.31** 0.09 1.66 0.44 0.31** 0.08
Observe 1.16 0.47 0.26* 0.05 1.17 0.47 0.27* 0.05 0.59 0.23 0.23* 0.03 0.58 0.24 0.22* 0.03
Describe 0.43 0.40 0.11 0.01 0.63 0.42 0.16 0.02 -0.39 0.20 -0.17* 0.02 -0.38 0.21 -0.17ŧ 0.02
Aware -0.19 0.46 -0.04 0.00 -0.16 0.47 -0.04 0.00 0.21 0.23 0.08 0.00 0.22 0.24 0.09 0.00
Non-judge -0.08 0.43 -0.02 0.00 -0.26 0.46 -0.06 0.00 -0.23 0.21 -0.10 0.01 -0.23 0.23 -0.10 0.01
Non-react -0.62 0.51 -0.14 0.01 -0.70 0.51 -0.15 0.01 -0.59 0.25 -0.22* 0.03 -0.59 0.25 -0.22* 0.03
Anxiety - - - - -0.15 0.10 -0.17 0.01 - - - - 0.00 0.05 0.00 0.00
Depression - - - - 0.21 0.13 0.18 0.02 - - - - 0.02 0.07 0.02 0.00
Constant -1.74 2.28 - - -0.85 2.99 - - -0.60 1.12 - - -0.71 1.51 - -
Model F/R2 F(11,109)=2.09, p<.05; R
2=.17 F(13,107)=2.06, p<.05; R
2=.20 F(11,109)=7.45, p<.01; R
2=.43 F(13,107)=6.20, p<.01; R
2=.43
Model F∆ - F∆(2,107)=1.73, n.s - F∆(2,107)=0.03, n.s
Notes: * p <.05, ** p < .01, ŧ p < .10; # Conds is scored 0 (absent)/1 (present) for psychological visit model; sr
2 = squared part correlation
Page 17 of 17
http://mc.manuscriptcentral.com/ac-phm-vcy
Health Sciences