aerosolized liposomal amphotericin b: a potential prophylaxis of invasive pulmonary aspergillosis in...
TRANSCRIPT

Pediatric Pulmonology 49:574–580 (2014)
Aerosolized Liposomal Amphotericin B:A Potential Prophylaxis of Invasive PulmonaryAspergillosis in Immunocompromised Patients
Harutai Kamalaporn, MD,1* Kitty Leung, BSc,2 Mark Nagel, BSc,3 Saranya Kittanakom, PhD,4
Battista Calvieri, PhD,5 Reinhart A.F. Reithmeier, PhD,4 and Allan L. Coates, MD6
Summary. Background: Aerosolized liposomal Amphotericin B may reduce the incidence of
invasive pulmonary Aspergillosis in adults with chemotherapy-induced prolonged neutropenia
with less nephrotoxicity. The breath-actuated AeroEclipse1 BAN nebulizer is very efficient and
minimizes environmental drug contamination since no aerosol is produced, unless the patient is
inspiring through the device. Our aim is to develop an appropriate delivery system suitable for
children that does not disrupt the liposomes due to the shear forces in nebulization. Methods: This
is an in vitro experimental study in vitro. Six ml of 4 mg/ml liposomal Amphotericin B solution
(AmBisome1; Astellas Pharma Inc., Markham, Ontario, CA) was nebulized with the breath-
actuated nebulizer (AeroEclipse1; Trudell Medical International, Canada) and captured by the
glass liquid impinger. Sodium dodecyl sulfate was used as detergent to disrupt the liposomes in
control samples. Gel filtration, electron microscopy, and high performance liquid chromatography
(HPLC) were used to compare the size and shape of the liposomes, and amount of the drug before
and after nebulization. The aerosol particle size was obtained by the laser diffraction. Results:
After nebulization, 97.5% of amphotericin B was captured by the liquid impinger and detected by
HPLC. Gel filtration and electron microscopy demonstrated that the drug remained in its liposomal
configuration after nebulization. The mass median diameter (MMD) was 3.7 mm and 66% of aerosol
particleswere less than 5 mm in diameter. Conclusions:Wedemonstrated that liposomal Amphotericin
B can be nebulized successfully without disrupting the liposomes andminimize drug loss by using the
breath-actuated nebulizer. Pediatr Pulmonol. 2014; 49:574–580. � 2013 Wiley Periodicals, Inc.
Key words: aerosolized liposomal amphotericin B; invasive pulmonary Aspergillosis;
breath-actuated nebulizer; AeroEclipse.
Funding source: none reported.
INTRODUCTION
Advances in transplantation medicine have led to anincrease in the number of immunocompromised patients.Invasive pulmonary Aspergillosis (IPA) usually causedby Aspergillus fumigatus is the most common fungal
pulmonary infection in patients undergoing intensivechemotherapy.1–5 The spores measuring 3–5 mm aredisseminated through the air and direct inhalation ornasopharyngeal colonization of spores that can descend tothe lowest regions of the lungs is the usual route of entry.The incidence of IPA in patients ranges from 4% to 13%
1Division of Pulmonology, Department of Pediatrics, Ramathibodi
Hospital, Mahidol University, Bangkok, Thailand.
2Physiology and Experimental Medicine, Research Institute, The Hospital
for Sick Children, Toronto, Ontario, Canada.
3Trudell Medical International, London, Ontario, Canada.
4Department of Biochemistry, University of Toronto, Toronto, Canada.
5Faculty of Medicine, Microscopy Imaging Laboratory, University of
Toronto, Toronto, Ontario, Canada.
6Physiology and Experimental Medicine, The Hospital for Sick Children-
Research Institute, University of Toronto, Toronto, Ontario, Canada.
Conflict of interest: None.
�Correspondence to: Harutai Kamalaporn, MD, Division of Pulmonology,
Department of Pediatrics, Ramathibodi Hospital, Mahidol University, 270
Rama VI Rd., Ratchatewi, Bangkok 10400, Thailand.
E-mail: [email protected]
Received 20 December 2012; Accepted 10 May 2013.
DOI 10.1002/ppul.22856
Published online 10 July 2013 in Wiley Online Library
(wileyonlinelibrary.com).
� 2013 Wiley Periodicals, Inc.

after hematopoietic stem cell transplantation. It remains adevastating disease with a mortality rate of approximately70–90% because of difficulties in early diagnosis andinsufficient and ineffective treatment options. Mortality isstrongly correlated with the underlying condition, thestage of the underlying disease, the extension of theAspergillosis, and is negatively correlated with earlyadministration of antifungal therapy, and the speed ofgranulocyte recovery. Standard treatment of IPAwith IVantifungal agents such as Amphotericin B is oftenunsuccessful and complicated by drug toxicity. Despitethe combination therapy of new intravenous antifungalagents such as Voriconazole plus Caspofungin, the rate ofpositive response was only 50–60%.1–7 Failure oftreatment with IV antifungal agents may derive fromthe inability to achieve high enough pulmonary tissuelevels without systemic toxicity. Aerosol delivery couldresult in high pulmonary tissue levels but produce bloodlevels below that of systemic toxicity. However, twochallenges remain before aerosol treatment can be safelyrecommended for the pediatric population. The first is thatjet nebulization subjects the liquid in the nebulizer toshear stress in order to break up the liquid droplet surfaceforces and generate an aerosol. Larger particles of theaerosol generated impact on the baffles of the nebulizerand then run back into the well to be nebulized again. It isestimated that roughly 99% of the volume ofdroplets generated undergo this fate,8 which means thatthe liposomes in the solution will be exposed tocumulative shear forces that may cause disruption ofthe liposome membrane and potential loss of theencapsulated drug. Secondly, nebulizers have a vastrange of efficiencies and knowing the likely pulmonarydeposition is key to the selection of the appropriate doseof human studies.There are some studies in a rat model using aerosolized
antifungal agents in order prevent or directly attackAspergillus spp. in the lungs.9,10 It has been shown thatliposomal Amphotericin B can deposit at bronchioleepithelium, alveolar sacs and ducts, and uptake intoalveolar macrophages right after nebulization.7 Regard-ing survival, combination of systemic and local adminis-tration of liposomal Amphotericin B was superior to thatof either treatment alone.7 When given as prophylaxis,aerosolized Amphotericin B can decrease the incidenceof IPA in a rat model2,11 There are four commerciallyavailable of Amphotericin B preparations includingAmphotericin B desoxycholate (AMB-DOC), LiposomalAmphotericin B (L-AMB), Amphotericin B lipid com-plex (ABLC), and Amphotericin B colloidal dispersion(ABCD). When delivered by nebulization6 in rats itappeared that AMB-DOC, had a detrimental effect onsurfactant size and integrity. Desoxycholate is a detergentand acts as a surfactant. The lipid formulations withoutadded detergentmay be safer for the surfactant function of
the respiratory tract.6 When given at 6 weeks beforefungal inoculation only nebulized L-AMB showed asignificantly prolonged survival. It is known thatamphotericin B tightly binds to cell membranes andsterol receptors and that the liposomal formulation mayact as a slow release pool, resulting in long-term efficacywith minimal systemic toxicity.There are encouraging human studies in adults, post
lung transplantation12–16 and there was a randomizedplacebo-controlled trial in adult neutropenic patientswhere a lower incidence of IPAwas found in patients withL-AMB prophylactic nebulization 2 days per week untilneutrophil recovery17 The dose was 12.5 mg of L-AMBusing the breath actuated Halolite nebulizer which wouldbe expected to delivery approximately 8 mg based ondevice performance.18
What is not known are the appropriate aerosol dose,especially in children and how to deliver the formulationwith minimal environmental contamination. A potentialdevice would be the breath-actuated AeroEclipse1 BAN(TrudellMedical International, London,Ontario, Canada)nebulizer, which is very efficient and minimizesenvironmental drug contamination since no aerosol isproduced unless the patient is actively inspiring throughthe device.18–20 The purpose of this in vitro study is todemonstrate that the liposomal formulation of amphoter-icin is not disrupted by the shear forces of nebulizationand to develop algorithms that will predict the appropriatedose of drug to place in the nebulizer in preparation for aclinical pilot study.
MATERIALS AND METHODS
The delivery system was characterized both in terms ofoutput and particle size distribution at the Physiology andExperimental Medicine Aerosol Laboratory at theHospital for Sick Children Research Institute, quantitativeamphotericin B assay was done at Trudell MedicalInternational and the integrity of the lipids was assayed inthe Department of Biochemistry, University of Toronto,Canada.
Particle Size Distribution and Rate of OutputStudies Using Laser Diffraction
The output of the AeroEclipse1 BANwhen nebulizing24 mg of Liposomal Amphotericin B (AmBisome1;Astellas Pharma Canada, Inc.) in 6 ml of solution wascharacterized in terms of particle size distribution and rateof output during steady state conditions as previouslydescribed.18,21,22 The nebulizer was driven with com-pressed dry air (hospital air, 50 psi source) at 8 L/min,which is recommended by the manufacturer. Flow fromthe hospital air line was measured by a flow calibrationinstrument, Mass flow meter TSI 4040E (TSI Inc., Shoreview, MN). The top button of the nebulizer was depressed
Aerosolized Liposomal Amphotericin B 575
Pediatric Pulmonology

to allow steady state output without active breathing. Thedevicewasmounted at right angles to the laser beam closeenough to the lens of a Malvern Mastersizer X (MalvernInstruments, Inc., Worcestershire, UK) to avoid vignett-ing but far enough to avoid contamination of the lens andthe calculations used the Mie theory for transparentdroplets.21 Measurements were made after 3.5 min ofnebulization, which allowed the nebulizer to attain asteady state temperature,22 after which particle sizedistribution and respirable fraction (RF) were calculated.The respirable fraction was defined as the fraction of themass of the aerosol in particles�5 mm, which, if inhaledthrough amouthpiece are likely to deposit below the vocalcords.23 Given that the device generates aerosol onlyduring inspiration, the expected pulmonary depositionwould be the output of the device multiplied by the RF.The output of the nebulizer was measured gravimetri-
cally using salbutamol which can be easily assayed byUVspectrophotometry as a proxy for amphotericin andcalculated taking both changes in weight and concentra-tion in well of the nebulizer into consideration. This hasbeen described in detail elsewhere.18,24 This calculatedoutput was then compared to that captured and assayed foramphotericin B with agreement within 5% consideredsatisfactory.
Nebulization
AmBisome1 was reconstituted with distilled water to4 mg/ml. A glass liquid impinger (Ace Glass Inc.,Vineland, NJ) immersed in ice to prevent evaporativeloss was used to capture the output from the Aero-Eclipse1 BAN driven by the hospital air and with asuction flow of 30 L/min (Gast Pump, Model # 10709,Anderson Instruments Inc., Atlanta, GA). Six milliliter ofAmBisome1 was nebulized until dryness for approxi-mately 20 min.The amount of amphotericin B recovered from the
glass liquid impinge was assayed by High PerformanceLiquid Chromatography (HPLC; Varian Prostar 410Autosampler; Spectralab Scientific Inc., Markham, Ontario,Canada) and compared to the output calculated above.Analytical grade (HPLC grade) acetonitrile, methanoland 1-heptanesulfonic acid sodium salt (Fisher Scientific,Oakville, Ontario, Canada) and HPLC-grade water wasused in the preparation of the mobile phase for HPLC.
Gel Filtration
Gel electrophoresis and UV spectrophotometer wereused to determine liposomal stability from the number ofconfigurations of molecules in the sample based on the“number of the peak.” Liposomal and free amphotericin Bwere separated by the gel electrophoresis and thenassayed with UV spectrophotometry. Amphotericin Bgives specific UV absorption peaks at 382 and
405 nm25,26 while liposomes give UV absorption peakat 254 nm.Prior to nebulization, with Amphotericin B enclosed in
the liposomes, only one peak was detected. Two separatepeaks will be detected if liposomes and Amphotericinare separated, either though deliberate destruction of theliposomes or through disruption by the shear forces fromnebulization. Hence, if after nebulization, only one peakis detected, then the liposomes had not been disrupted bythe shear forces of the nebulizer. The control solution wascreated by the disruption of the liposomes by a 10%sodium dodecyl sulphate (SDS), an anionic detergentfromSigma–AldrichCompany (Oakville, Ontario, Canada).Equal volumes of SDS and AmBisome1were mixed thenshaken vigorously until the yellow turbid AmBisome1
became a yellow clear solution. Gel filtration wasperformed by applying 500 ml of each sample (pre-neb,post-neb, and control sample with SDS), on a SephacrylS-1000 Superfine column (internal diameter 0.9 cm,height 60 cm) equilibrated with phosphate buffer saline(PBS) at 48C.After two bed volumes of eluent buffer, PBShad passed through the column, a flow adapter was set at aflow rate of 0.5 ml/min. The columnwas calibrated with aset of globular protein standards (Gel Filtration Calibra-tion Kit, Amersham Pharmacia Biotech Inc., Piscataway,NJ) with the same buffer. Each sample was collected as500 ml for 96 fractions. Subsequent UV spectrophotom-eter (DU 640B Spectrophotometer; Beckman CoulterInc., Brea, CA) readout verified the expected sample at254, 382, and 405 nm, respectively. Each process wasrepeated three times.
Electron Microscopy
Electron microscopy was used to illustrate the sizes andshapes of controlled, pre-, and post-nebulized solutions.Prior to staining, 400 mesh copper grids coated with a thincarbon film were positively charged in a glow dischargeapparatus. This made the grids hydrophilic. A sample dropof approximately 1 mg/ml was placed on the carbon-coated grid and plotted with filter paper to remove ofexcess sample. When the sample has almost dried a dropof 2% Phosphotungstic acid pH 6.5 was then place on thesample grid. The excess stain is also plotted. The driedsample/grid is then placed into the electronmicroscope forobservations. Images were taken with the Hitachi H-7000electron microscope using an AMT digital camera in theMicroscopy Imaging Laboratory (MIL) in the Faculty ofMedicine at the University of Toronto.
STATISTICS
All measurements were done in triplicate and resultsexpressed as a mean and standard deviation except theparticle size from electron microscopy which was shownas median and range.
576 Kamalaporn et al.
Pediatric Pulmonology
RESULTS
Output and Particle Size
After the nebulizer had achieved a steady stage at3.5 min, the mass median diameter (MMD) was foundto be 3.7 mm and the respirable fraction (RF) was 66%.Of the 24 mg charge, 15.9 � 1.3 mg were recovered,which would mean an expected pulmonary depositionof approximately 10.5 mg (output multiplied by RF).The residual volume was 1.29 � 0.38 ml when run todryness.
HPLC
The mass balance was determined by the calculatedoutput based on the UV spectrophotometric assay ofsalbutamol compared to the quantification of amphoteri-cin B. The HPLC was 97.5% of that calculated from theoutput assayed using salbutamol verifying that salbuta-mol could be used as a proxy for the output ofamphotericin B. HPLC could not detect the differencefrom intact or disrupted liposomes.
Gel Filtration Chromatography
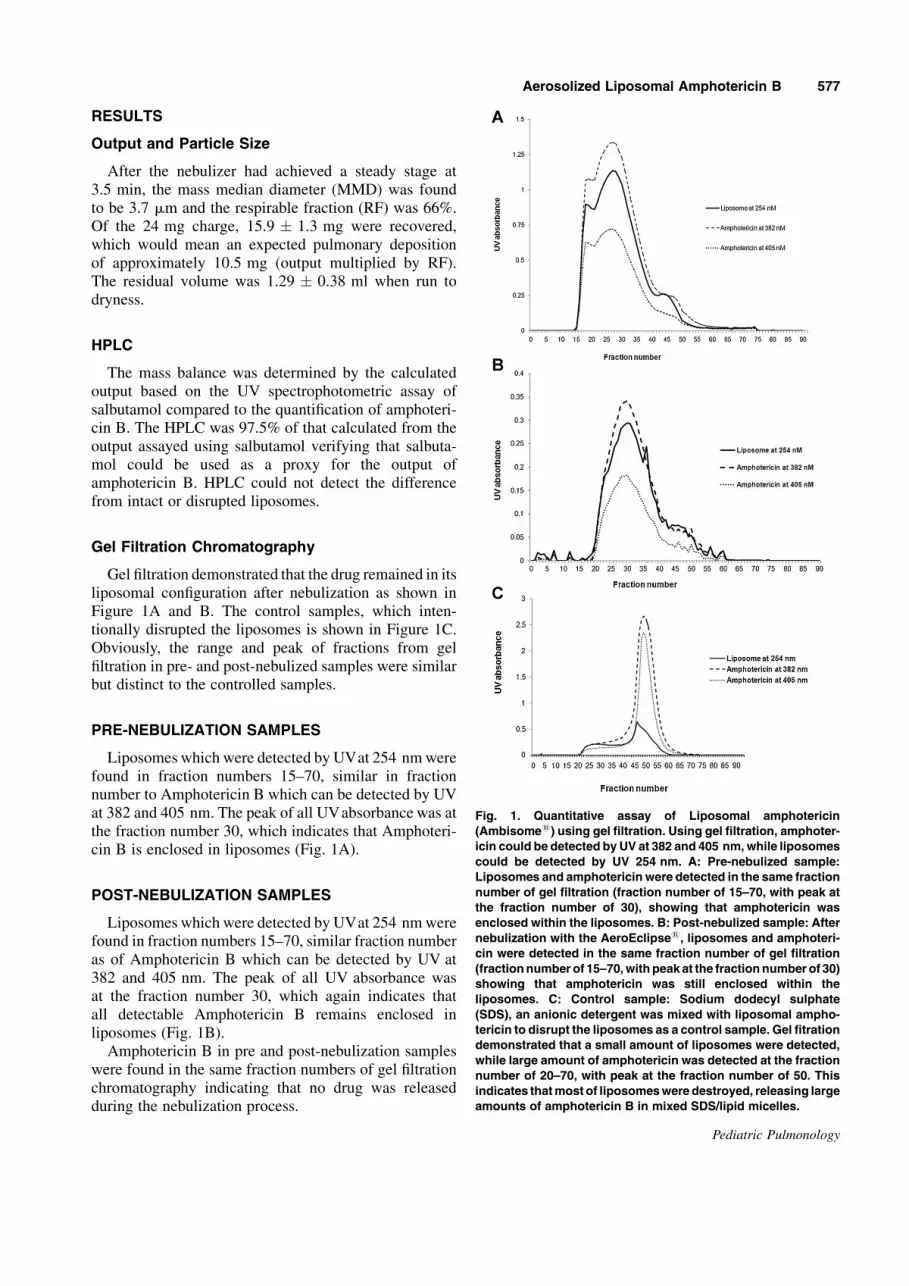
Gel filtration demonstrated that the drug remained in itsliposomal configuration after nebulization as shown inFigure 1A and B. The control samples, which inten-tionally disrupted the liposomes is shown in Figure 1C.Obviously, the range and peak of fractions from gelfiltration in pre- and post-nebulized samples were similarbut distinct to the controlled samples.
PRE-NEBULIZATION SAMPLES
Liposomes which were detected by UVat 254 nmwerefound in fraction numbers 15–70, similar in fractionnumber to Amphotericin B which can be detected by UVat 382 and 405 nm. The peak of all UVabsorbance was atthe fraction number 30, which indicates that Amphoteri-cin B is enclosed in liposomes (Fig. 1A).
POST-NEBULIZATION SAMPLES
Liposomes which were detected by UVat 254 nmwerefound in fraction numbers 15–70, similar fraction numberas of Amphotericin B which can be detected by UV at382 and 405 nm. The peak of all UV absorbance wasat the fraction number 30, which again indicates thatall detectable Amphotericin B remains enclosed inliposomes (Fig. 1B).Amphotericin B in pre and post-nebulization samples
were found in the same fraction numbers of gel filtrationchromatography indicating that no drug was releasedduring the nebulization process.
Fig. 1. Quantitative assay of Liposomal amphotericin
(Ambisome1) using gel filtration. Using gel filtration, amphoter-
icin could be detected by UV at 382 and 405 nm,while liposomes
could be detected by UV 254 nm. A: Pre-nebulized sample:
Liposomes and amphotericin were detected in the same fraction
number of gel filtration (fraction number of 15–70, with peak at
the fraction number of 30), showing that amphotericin was
enclosed within the liposomes. B: Post-nebulized sample: After
nebulization with the AeroEclipse1, liposomes and amphoteri-
cin were detected in the same fraction number of gel filtration
(fractionnumber of 15–70,withpeak at the fractionnumber of 30)
showing that amphotericin was still enclosed within the
liposomes. C: Control sample: Sodium dodecyl sulphate
(SDS), an anionic detergent was mixed with liposomal ampho-
tericin to disrupt the liposomes as a control sample. Gel fitration
demonstrated that a small amount of liposomes were detected,
while large amount of amphotericin was detected at the fraction
number of 20–70, with peak at the fraction number of 50. This
indicates thatmost of liposomesweredestroyed, releasing large
amounts of amphotericin B in mixed SDS/lipid micelles.
Aerosolized Liposomal Amphotericin B 577
Pediatric Pulmonology
CONTROL SAMPLES (10% SDS: AMBISOME1:1 v/v)
Only a small amount of liposomes was found,suggesting that liposome were disrupted by the detergentSDS.Large amounts of Amphoterin B were detected from
fraction number 20–75 with the peak at fraction number50 which were significantly different from the peak ofpre- and post-nebulization samples. These findings reflectAmphotericin B solubilized in mixed SDS/lipid micellesformed by detergent disruption of liposomes (Fig. 1C).
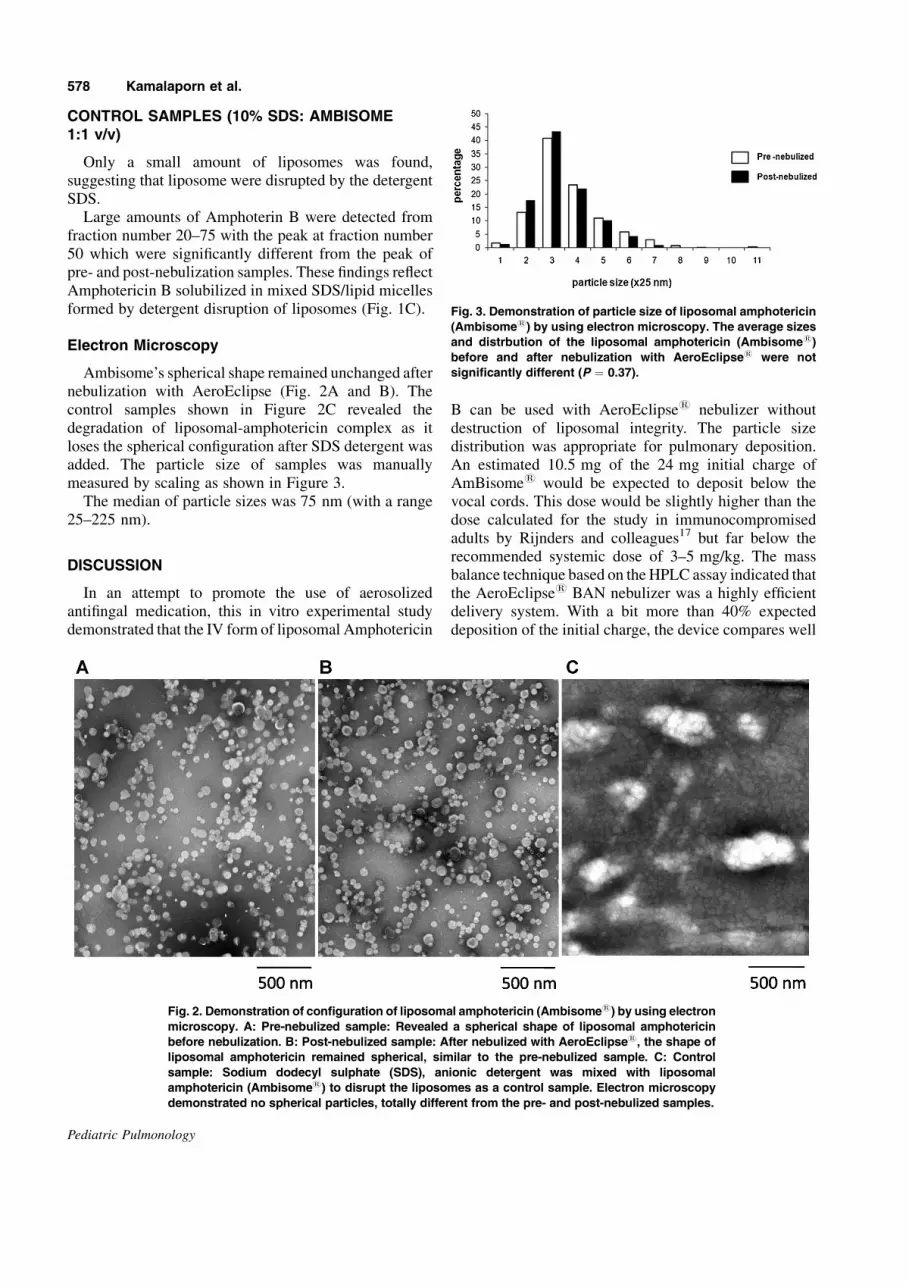
Electron Microscopy
Ambisome’s spherical shape remained unchanged afternebulization with AeroEclipse (Fig. 2A and B). Thecontrol samples shown in Figure 2C revealed thedegradation of liposomal-amphotericin complex as itloses the spherical configuration after SDS detergent wasadded. The particle size of samples was manuallymeasured by scaling as shown in Figure 3.The median of particle sizes was 75 nm (with a range
25–225 nm).
DISCUSSION
In an attempt to promote the use of aerosolizedantifingal medication, this in vitro experimental studydemonstrated that the IV form of liposomal Amphotericin
B can be used with AeroEclipse1 nebulizer withoutdestruction of liposomal integrity. The particle sizedistribution was appropriate for pulmonary deposition.An estimated 10.5 mg of the 24 mg initial charge ofAmBisome1 would be expected to deposit below thevocal cords. This dose would be slightly higher than thedose calculated for the study in immunocompromisedadults by Rijnders and colleagues17 but far below therecommended systemic dose of 3–5 mg/kg. The massbalance technique based on theHPLC assay indicated thatthe AeroEclipse1 BAN nebulizer was a highly efficientdelivery system. With a bit more than 40% expecteddeposition of the initial charge, the device compares well
Fig. 2. Demonstration of configuration of liposomal amphotericin (Ambisome1) by using electron
microscopy. A: Pre-nebulized sample: Revealed a spherical shape of liposomal amphotericin
before nebulization. B: Post-nebulized sample: After nebulized with AeroEclipse1, the shape of
liposomal amphotericin remained spherical, similar to the pre-nebulized sample. C: Control
sample: Sodium dodecyl sulphate (SDS), anionic detergent was mixed with liposomal
amphotericin (Ambisome1) to disrupt the liposomes as a control sample. Electron microscopy
demonstrated no spherical particles, totally different from the pre- and post-nebulized samples.
Fig. 3. Demonstration of particle size of liposomal amphotericin
(Ambisome1) by using electron microscopy. The average sizes
and distrbution of the liposomal amphotericin (Ambisome1)
before and after nebulization with AeroEclipse1 were not
significantly different (P ¼ 0.37).
578 Kamalaporn et al.
Pediatric Pulmonology

to the Pari LC Star1 jet nebulizer at approximately 25%and the Pari eFlow1 vibrating membrane nebulizer atapproximately 38%.27 Both gel filtration and by electronmicroscopy demonstrated the integrity of the liposomesduring nebulization indicating stability of the liposomesdespite being exposed to significant shear forces.One of the challenges with aerosol drug administration
to children is that they frequently take the nebulizer out oftheir mouths. If the device continues to produce aerosol,this goes into the environment which could have anadverse effect on care givers and it also makes theestimate of pulmonary deposition more unreliable. Amajor advantage of the AeroEclipse1 is that as long as thechild is old enough to make a tight seal with the mouthpiece and can generate inspiratory flows greater than13 L/m, aerosol will be produced and inhaled. Should thechild be distracted and remove the device from the lips, noaerosol will be generated. Hence, the device would beapplicable to most children 5 years of age and older aswell as adults and quite tolerant of distractions resulting inremoval of the nebulizer from the mouth.Another advantage of the AeroEclipse1 BAN nebuliz-
er compared to jet nebulizers is that since it nebulizes onlyduring inspiration, there is very little environmentalcontamination. This would minimize the likelihood ofcaregivers developing allergic reactions or other adverseeffects and also minimize the possibility of the fungusdeveloping resistance.While there may be significant advantages, especially in
terms of time saved, to administer drugs using vibratingmembrane systems, there can be problemswhen nebulizingdrugs that are not a relatively dilute aqueous solution. It hasbeen found that aerosolized antibiotic partially clogged themesh of hand-held adaptive aerosol delivery (AAD) device(I-neb) indicated by the prolonged treatment time.28
Aerosolized liposomes may be trapped in the vibrating-mesh nebulizer (VMN; Aeroneb1 Go) causing markeddrug loss.29 In contrast, Manunta et al.30 reported thatnebulization of receptor-targeted nanocomplxes for genedelivery inCF patients viaAeroEclipse II1 breath-actuatednebulizer preserved almost unchanged colloidal suspensionand was the most effective nebulizer in vivo, whereas theAeroneb1 Pro VMN tended to block and has less efficacy.To the best of our knowledge, this is the first in vitro
study to compare liposomal continuity pre- and post-nebulization. As an in vitro study it is impossible to knowif the local environment in the lung may degrade theliposomes, but there is nothing in the literature to suggestthat this will be the case. However, an in vivo study isneeded to prove its efficacy against invasive pulmonaryfungal infection. A further limitation is that the expectedpulmonary deposition was based on in vitro measure-ments rather than nuclear medicine deposition studies.However, a comparison of previous in vitro studies31 to invivo data27 would suggest fairly close agreement such that
the present data could be used for dosing decision in aclinical trial.
CONCLUSION
Liposomal Amphotericin B can be nebulized success-fully without disrupting the liposomes and minimizingdrug loss using the breath-actuated nebulizer. Inneutropenic patients who are at risk of invasive pulmo-nary fungal infection, nebulized liposomal AmphotericinB could be a potential prophylactic regimen. These datacan be used for the planning of a clinical trial based on thecontinued integrity of the liposome preparation afternebulization.
REFERENCES
1. Schwartz S, Behre G, Heinemann V,Wandt H, Schilling E, Arning
M, Trittin A, Kern WV, Boenisch O, Bosse D, Lenz K, Ludwig
WD,HiddemannW, SiegertW, Beyer J. Aerosolized amphotericin
B inhalations as prophylaxis of invasive aspergillus infections
during prolonged neutropenia: results of a prospective randomized
multicenter trial. Blood 1999;93:3654–3661.
2. Allen SD, Sorensen KN, Nejdl MJ, Durrant C, Proffit RT.
Prophylactic efficacy of aerosolized liposomal (AmBisome) and
non-liposomal (Fungizone) amphotericin B in murine pulmonary
aspergillosis. J Antimicrob Chemother 1994;34:1001–1013.
3. Olson JA, Adler-Moore JP, Schwartz J, Jensen GM, Proffitt RT.
Comparative efficacies, toxicities, and tissue concentrations of
amphotericin B lipid formulations in a murine pulmonary
aspergillosis model. Antimicrob Agents Chemother 2006;50:
2122–2131.
4. Gavalda J, Martin MT, Lopez P, Gomis X, Ramirez JL, Rodriguez
D, Len O, Puigfel Y, Ruiz I, Pahissa A. Efficacy of nebulized
liposomal amphotericin B in treatment of experimental pulmonary
aspergillosis. Antimicrob Agents Chemother 2005;49:3028–3030.
5. Ruijgrok EJ, Vulto AG, Van Etten EW. Efficacy of aerosolized
amphotericin B desoxycholate and liposomal amphotericin B in
the treatment of invasive pulmonary aspergillosis in severely
immunocompromised rats. J Antimicrob Chemother 2001;48:
89–95.
6. Ruijgrok EJ, Fens MH, Bakker-Woudenberg IA, van Etten EW,
Vulto AG. Nebulization of four commercially available ampho-
tericin B formulations in persistently granulocytopenic rats with
invasive pulmonary aspergillosis: evidence for long-term biologi-
cal activity. J Pharm Pharmacol 2005;57:1289–1295.
7. Ruijgrok EJ, Fens MH, Bakker-Woudenberg IA, van Etten EW,
Vulto AG. Nebulized amphotericin B combined with intravenous
amphotericin B in rats with severe invasive pulmonary aspergillo-
sis. Antimicrob Agents Chemother 2006;50:1852–1854.
8. Ruijgrok EJ, Vulto AG, Van Etten EW. Aerosol delivery of
amphotericin B desoxycholate (Fungizone) and liposomal
amphotericin B (AmBisome): aerosol characteristics and in-
vivo amphotericin B deposition in rats. J Pharm Pharmacol 2000;
52:619–627.
9. Dennis JH, Hendrick DJ. Design characteristics for drug
nebulizers. J Med Eng Technol 1992;16:63–68.
10. Lambros MP, Bourne DW, Abbas SA, Johnson DL. Disposition of
aerosolized liposomal amphotericin B. J Pharm Sci 1997;86:
1066–1069.
11. Diot P, Rivoire B, Le Pape A, Lemarie E, Dire D, Furet Y, Breteau
M, Smaldone GC. Deposition of amphotericin B aerosols in
pulmonary aspergilloma. Eur Respir J 1995;8:1263–1268.
Aerosolized Liposomal Amphotericin B 579
Pediatric Pulmonology

12. Monforte V, Roman A, Gavalda J, Bravo C, Tenorio L, Ferrer A,
Maestre J, Morell F. Nebulized amphotericin B prophylaxis for
Aspergillus infection in lung transplantation: study of risk factors.
J Heart Lung Transplant 2001;20:1274–1281.
13. Ruffini E, Baldi S, Libertucci D, Solidoro P, Di Marzio P, Cavallo
A, Mancuso M. Aerosolized liposomal amphotericin B: a novel
and effective treatment for Aspergillus infections in lung
transplant recipients. Proceedings of the 42nd ICAAC (Inter-
science Conferrence on Antimicrobial Agents and Chemotherapy)
Meeting, San Diego, CA. Sept 2002; Abstract#M-1237.
14. Monforte V, Roman A, Gavalda J, et al. Pharmacokinetic and
efficacy of nebulized AmBisome in lung transplantation.
Proceedings of the 44th ICAAC (Interscience Conferrence on
Antimicrobial Agents and Chemotherapy) Meeting, Washington
DC. Oct/Nov 2004; Abstract#M-1042.
15. Corcoran TE, Venkataramanan R,Mihelc KM,Marcinkowski AL,
Ou J, McCook BM, Weber L, Carey ME, Paterson DL, Pilewski
JM, Mccurry KR, Husain S. Aerosol deposition of lipid complex
amphotericin-B (Abelcet) in lung transplant recipients. Am J
Transplant 2006;6:2765–2773.
16. Monforte V, Roman A, Gavalda J, Lopez R, Pou L, Simo M,
Aguade S, Soriano B, Bravo C, Morell F. Nebulized amphotericin
B concentration and distribution in the respiratory tract of lung-
transplanted patients. Transplantation 2003;75:1571–1574.
17. Rijnders BJ, Cornelissen JJ, Slobbe L, Becker MJ, Doorduijn JK,
HopWC, Ruijgrok EJ, Lowenberg B, Vulto A, Lugtenburg PJ, De
Marie S. Aerosolized liposomal amphotericin B for the prevention
of invasive pulmonary aspergillosis during prolonged neutropenia:
a randomized, placebo-controlled trial. Clin Infect Dis. 2008;
46:1401–1408.
18. Leung K, Louca E, Coates AL. Comparison of breath-enhanced to
breath-actuated nebulizers for rate, consistency, and efficiency.
Chest 2004;126:1619–1627.
19. MacIntyre NR, Mitchell JP, Nagel MW, Coppolo D. Similar
delivery of amphotericin lipid complex is possible at one-half dose
via a breath-actuated nebulizer compared to a continuously
operating nebulizer. Poster presentation in ATS (American
Thoracic Society) Conferrence, San Diego. May 22–24, 2005.
20. Mitchell JP, Nagel MW, MacIntyre NR. A mechanically operated
breath-actuated nebulizer enables both improved control of dosing
and delivery efficiency. Accepted for Drug Delivery to the Lungs-
16, Edinburgh-December 7–9, 2005.
21. Mitchell JP, Nagel MW, Nichols S, Nerbrink O. Laser
diffractometry as a technique for the rapid assessment of aerosol
particle size from inhalers. J Aerosol Med 2006;19:409–433.
22. KwongWT, Ho SL, Coates AL. Comparison of nebulized particle
size distribution with Malvern laser diffraction analyzer versus
Andersen cascade impactor and low-flowMarple personal cascade
impactor. J Aerosol Med 2000;13:303–314.
23. Coates AL, DenkO, LeungK, Ribeiro N, Chan J, GreenM,Martin
S, Charron M, Edwardes M, Keller M. Higher tobramycin
concentration and vibrating mesh technology can shorten
antibiotic treatment time in cystic fibrosis. Pediatr Pulmonol
2011;46:401–408.
24. O’Callaghan C, Clark AR, Milner AD. Why nebulise for more
than five minutes? Arch Dis Child 1989;64:1270–1273.
25. Kawabata M, Onda M, Mita T. Effect of aggregation of
amphotericin B on lysophosphatidylcholine micelles as related
to its complex formation with cholesterol or ergosterol. J Biochem
2001;129:725–732.
26. Byrne B, Carmody M, Gibson E, Rawlings B, Caffrey P.
Biosynthesis of deoxyamphotericins and deoxyamphoteronolides
by engineered strains of Streptomyces nodosus. Chem Biol 2003;
10:1215–1224.
27. Coates AL, Green M, Leung K, Chan J, Ribeiro N, Ratjen F,
Charron M. A comparison of amount and speed of deposition
between the PARI LC STAR(R) jet nebulizer and an investiga-
tional eFlow(R) nebulizer. J Aerosol Med Pulm Drug Deliv 2011;
24:157–163.
28. McCormack P, Southern KW, McNamara PS. New nebulizer
technology to monitor adherence and nebulizer performance
in cystic fibrosis. J Aerosol Med Pulm Drug Deliv 2012;25:
307–309.
29. Elhissi A, Gill H, Ahmed W, Taylor K. Vibrating-mesh
nebulization of liposomes generated using an ethanol-based
proliposome technology. J Liposome Res 2011;21:173–180.
30. Manunta MD, McAnulty RJ, Tagalakis AD, Bottoms SE,
Campbell F, Hailes HC, Tabor AB, Laurent GJ, O’Callaghan C,
Hart SL. Nebulisation of receptor-targeted nanocomplexes for
gene delivery to the airway epithelium. PLoS ONE 2011;6:
e26768.
31. Katz SL, Adatia I, Louca E, Leung K, Humpl T, Reyes JT, Coates
AL. Nebulized therapies for childhood pulmonary hypertension:
an in vitro model. Pediatr Pulmonol 2006;41:666–673.
580 Kamalaporn et al.
Pediatric Pulmonology