fecal microbiota transplant for treatment of clostridium difficile infection in immunocompromised...
TRANSCRIPT
Fecal Microbiota Transplant for Treatment of Clostridium difficile Infection in Immunocompromised Patients
Colleen Kelly1, Chioma Ihunnah1,Monika Fischer2, Alexander Khoruts3,
Lawrence Brandt4, Anita Afzali5, Olga Aroniadis4, Amy Barto6, Thomas Borody7, Andrea Giovanelli8, Shelley Gordon9, Michael Gluck10, Elizabeth Hohmann11, Dina Kao12, John Y.
Kao13, Daniel McQuillen6, Mark Mellow14, Kevin Rank3, Krishna Rao13, Arnab Ray15, Margot Schwartz10, Namita Singh16, Neil Stollman8, Christina Surawicz5, David Suskind16, Stephen
Vindigni5, Ilan Youngster11
1 Brown Alpert Medical School, Providence, RI 2 Indiana University School of Medicine, Indianapolis, IN
3 University of Minnesota, Minneapolis, MN4Montefiore Medical Center, Bronx, New York
5University of Washington, Seattle, Washington6 Lahey Clinic Medical Center, Burlington, MA
7Centre for Digestive Diseases, Five Dock, New South Wales, Australia8 Northern California Gastroenterology Consultants, Inc. Oakland, CA
9California Pacific Medical Center, San Francisco, CA10Virginia Mason Medical Center, Seattle, WA.11Massachusetts General Hospital, Boston, MA
12University of Alberta, Edmonton, AB, Canada13University of Michigan, Ann Arbor, MI
14Integris Baptist Medical Center, Oklahoma City, Oklahoma15Ochsner Clinic Foundation, New Orleans, LA
16Seattle Children’s Hospital, Seattle, WA
Corresponding Author: Dr. Colleen Kelly
Brown Alpert Medical SchoolWomen’s Medicine Collaborative
Division of Gastroenterology146 West River StreetProvidence, RI 02904
T 401-793-7080F 401-793-7404

Guarantor of the article: Dr. Colleen Kelly
Specific author of contributions: Dr. Colleen Kelly - Involved in study design, planning, conducting, collecting and interpreting data for this study and drafting/editing the manuscriptDr. Chioma Ihunnah - Involved in planning, collecting and interpreting data for this study and drafting the manuscriptDr. Monika Fischer - Involved in data collection and drafting/editing of the manuscriptDr. Alexander Khoruts-Involved in data collection and drafting/editing of the manuscriptDr. Lawrence J. Brandt - Involved in data collection and editing the manuscriptDr. Anita Afzali - Involved in data collectionDr. Olga C. Aroniadis - Involved in data collectionDr. Amy Barto - Involved in data collectionDr. Thomas Borody - Involved in data collectionAndrea Giovanelli - Involved in data collectionDr. Shelley Gordon - Involved in data collectionDr. Michael Gluck –Involved in data collectionDr. Elizabeth Hohmann - Involved in data collectionDr. Daniel McQuillen - Involved in data collectionDr. Mark Mellow - Involved in data collectionDr. Dina Kao - Involved in data collectionDr. John Y. Kao - Involved in data collectionDr. Kevin Rank - Involved in data collectionDr. Krishna Rao- Involved in data collectionDr. Arnab Ray - Involved in data collectionDr. Margot Schwartz - Involved in data collectionDr. Namita Singh - Involved in data collectionDr. Neil Stollman - Involved in data collectionDr. Christina Surawicz - Involved in data collectionDr. David Suskind - Involved in data collection Dr. Stephen Vindigni – Involved in data collectionDr. Ilan Youngster - Involved in data collection
All above authors have approved the final draft submitted.
Financial Support: 1,4NIH 1R21DK093839-01A13NIH R21 AI091907
Potential Conflicts of Interest: Brandt L. Optimer Pharmaceuticals, Inc; Speaker’s Bureau and Research supportKhoruts A. CIPAC, Ltd Research SupportStollman N. Optimer Pharmaceuticals, Inc Speaker’s Bureau Kelly C. US endoscopy, Inc. Received consulting fees

Study Highlights: 1. WHAT IS CURRENT KNOWLEDGE C. difficile infection (CDI) is common in immunocompromised patients. Fecal Microbiota Transplantation (FMT) appears effective and is indicated for the treatment
of CDI not responding to standard therapies.2. WHAT IS NEW HERE FMT appears to be effective and safe in immunocompromised patients Immunocompromised patients do not appear to be at high risk of infection transmitted by
FMT Patients with IBD may experience disease flare following FMT, though whether this is
precipitated by the CDI, FMT itself or progression of the underlying disease state is not known.
ABSTRACT
Objectives: Patients who are immunocompromised (IC) are at increased risk of C. difficile
infection (CDI), which has increased to epidemic proportions over the past decade. Fecal
microbiota transplantation (FMT) appears effective for the treatment of CDI, though there is
concern IC pts may be at increased risk of having adverse events (AEs) related to FMT. This
study describes the multicenter experience of FMT in IC patients
Methods: A multicenter retrospective series was performed on the use of FMT in IC patients
with CDI that was recurrent, refractory or severe. We aimed to describe rates of CDI cure after
FMT as well as AEs experienced by IC patients after FMT. A 32-item questionnaire soliciting
demographic and pre- and post-FMT data was completed for 99 patients at 16 centers of which
80 were eligible for inclusion. Outcomes included (1) rates of CDI cure after FMT, (2) serious
adverse events (SAEs) such as death or hospitalization within 12 weeks of FMT, (3) infection
within 12 weeks of FMT and (4) AEs (related and unrelated) to FMT.
Results: Cases included adult (75) and pediatric (5) patients treated with FMT for recurrent
(54%), refractory (11%), and severe and/or overlap of recurrent/refractory & severe CDI (27%).
79% were outpatients at time of FMT. The mean follow-up period between FMT and data
collection was 11 months (range 3-46 months). Reasons for IC included: HIV/AIDS (3), solid
organ transplant (19), oncologic condition (7), immunosuppressive therapy for IBD (36), and
other IC due to medical condition/medication (15). The CDI cure rate after a single FMT was
78%, with 62 pts suffering no recurrence at least 12 weeks post-FMT. Eleven patients
underwent repeat FMT of which 8 had no further CDI. Thus, the overall cure rate was 89%.
Twelve (15%) had any SAE within 12 weeks post-FMT, of which 10 were hospitalizations. Two

deaths occurred within 12 weeks of FMT, one of which was the result of aspiration during
sedation for FMT administered via colonoscopy; the other was unrelated to FMT. None suffered
infections definitely related to FMT, but 1 patient developed an unrelated infection and 5 had
self-limited diarrheal illness which were probably unrelated, and no causal organism was
identified. Four (11% of IBD patients) experienced disease flare post-FMT. Three ulcerative
colitis (UC) patients underwent colectomy related to course of UC >100 days after FMT. One
patient had a superficial mucosal tear caused by the FMT colonoscopy and 3 patients reported
mild, self limited abdominal discomfort post-FMT.
Conclusions: This series demonstrates effective use of FMT for CDI in IC pts with few SAEs or
related AEs. Importantly, there were no infectious complications in these high-risk pts.

INTRODUCTION
Clostridium difficile infection (CDI) is responsible for 15-25% of nosocomial antibiotic-
associated diarrhea1 and has increased rapidly in the past decade2 to an incidence of 10.4 cases
per 1000 patient admissions.3 Immunocompromised (IC) patients are particularly at risk of CDI.
C. difficile is the most common cause of bacterial diarrhea in persons with HIV infection and has
its highest incidence in those with advanced HIV disease/AIDS.4 Organ transplant recipients are
also observed to suffer higher frequency of CDI. Retrospective case series of patients after solid
organ transplant (SOT) report an overall CDI incidence of 8% and incidence as high as 16% in
kidney transplant recipients.5 Furthermore, 40% of SOT patients who acquired CDI did not have
any recent antibiotic exposure, which suggests that IC status may be an independent risk factor
for CDI.5 Increased length of stays in hospitals and extended-care facilities in addition to
multiple exposures to broad-spectrum antibiotics increases the risk of CDI in this population of
patients.6,7 However disruptions of both the innate and adaptive immune responses are additional
factors, as signaling pathways involved with recruitment of neutrophils mitigate inflammation in
acute infection8 and patients with increased anti-toxin A and B IgG antibodies may be at
decreased risk of suffering recurrences of CDI compared with those who have reduced levels of
the antibody.9,10
Inflammatory bowel disease (IBD) patients develop CDI at a three-fold higher rate
compared to the general population and have an estimated 10% life time chance to contract C.
difficile.11,12 Recent increases in hospitalization, mortality, and colectomy rates in CDI IBD
patients are well demonstrated.13-16 Up to 19% of patients with an IBD flare test positive for C.
difficile.17 Immunosuppressive medications commonly used in this patient population multiply
the risk of CDI, above all, corticosteroids confer a threefold increase in CDI and twofold
increase in mortality.18,19 The strong association between IBD and CDI is hypothesized to be
based on disturbed mucosal barrier function and altered gut microbial flora.20
Recurrence is a common management problem and occurs in up to 20% of patients after
initial CDI treatment.21 Current guidelines recommend a tapering course of vancomycin after a
second recurrence, however up to 60% of patients do not respond to this treatment strategy or
develop further recurrence after the vancomycin is stopped.22 Initially described for treatment of
pseudomembranous enterocolitis in 1958,23 Fecal Microbiota Transplant (FMT) has proven to be
efficacious and safe in numerous case series24 and a recently published clinical trial.25 The use of
FMT among IC patients with CDI has been limited due to concerns about its safety in this
population. Published guidelines recommend avoidance of fecal transplant in SOT recipients
because of the theoretic potential for infection26 and caution even against the use of probiotics in
IC hosts because of the rare complication of superinfection (including bloodstream infections)
which has been reported from these “non pathogenic” organisms.27,28 A recent guidance issued
by the FMT working group specified that considerations for increased risk of adverse events
should be given to patients on major immunosuppressive agents and patients with
decompensated liver cirrhosis, advanced HIV/AIDS, recent bone marrow transplant, or other
cause of severe immunodeficiency.29 Furthermore, the FDA/Center for Biologics Evaluation and
Research recommended that patients who are immunocompromised for any reason be excluded
from the first randomized trial of FMT in this country.30 To date, no study has systematically
investigated the safety and efficacy of FMT in IC patients. We and colleagues at other medical
centers offering FMT have treated a number of IC patients with FMT. By this collective
experience we aim to describe rates of CDI cure in this population as well as adverse events
(AEs) experienced by IC patients after FMT.
METHODS
We performed a retrospective case series of IC patients with CDI who underwent FMT at
16 medical centers nationally and internationally. The study was approved by the Lifespan IRB
and the protocol was then made available to any center participating in the study for institution-
specific IRB approval. The methods used to administer FMT differed among sites, though most
(12 of 16) exclusively used an endoscopic lower GI route of administration. Informed consent
had been obtained from all patients prior to FMT. A 32-item data collection form was developed,
which elicited demographic data, CDI characteristics, and pre- and post-FMT data for each
patient. Patients were included if they were IC and had undergone FMT for recurrent, refractory,
severe or complicated CDI unresponsive to standard therapy. Definitions used to classify
recurrent, severe and complicated CDI for this study were based on recently published ACG
guidelines [Surawicz 2013].
1. Recurrent or relapsing CDI: At least three episodes of mild-to-moderate CDI and
failure of a 6-8 week taper with vancomycin with or without an alternative antibiotic (e.g.
fidaxomicin, rifaximin) or at least two episodes of severe CDI resulting in hospitalization
and associated with significant morbidity.
2. Refractory CDI: Moderate CDI not responding to standard therapy (vancomycin) for at
least a week
3. Severe CDI: WBC ≥ 15,000 cells/mm3, albumin < 3g/dl and abdominal tenderness
4. Complicated CDI defined by at least one of the following: admission to the ICU,
hypotension with or without the use of vasopressors, fever ≥ 38.5°C, ileus or significant
abdominal distention, mental status changes, WBC ≥ 35,000 cells/mm3, or < 2 cells/mm3,
serum lactate >2.2 mmol/L or any evidence of end-organ failure
At least 12 weeks of post FMT follow up data was required in order for the patient’s data to be
included in the analysis. We included patients who were immunocompromised at the time of
FMT as a result of or more of the following: HIV infection (any CD4 count), AIDS-defining
diagnosis or CD4<200/mm3, inherited or primary immune disorders, and immunodeficient or
immunosuppressed from a medical condition/medication including current or recent (<3 most)
treatment with anti-neoplastic agent or immunosuppressant medications (including but not
limited to monoclonal antibodies to B and T cells, anti-TNF agents, glucocorticoids,
antimetabolites (azathioprine, 6-mercaptopurine, methotrexate), calcineurin inhibitors
(tacrolimus, cyclosporine), mycophenolate mofetil).
Data collected included demographic information, reason for IC status, treatment with
immunosuppressant medication, other significant medical conditions, CDI treatments prior to
and around FMT, indication for FMT (recurrent, refractory or severe/complicated CDI), post
FMT mortality and hospitalizations, post FMT adverse events (AEs) and serious adverse events
(SAEs), and outcomes (CDI recurrence post-FMT, need for colectomy and response to second
FMT if required). Sixteen centers submitted data collection forms for 99 patients. Patients were
excluded from analysis if FMT was conducted for reasons other than CDI, if they did not meet
the criteria for IC or if they did not have a minimum of 12 weeks post-FMT follow-up,
The primary outcomes were CDI cure and any serious adverse events (SAEs) or adverse
events (AEs) within 12 weeks post-FMT. Cure was defined as absence of diarrhea, or marked
reduction in stooling frequency without need for further anti-CDI therapy. AEs were defined as
any untoward medical occurrence in a patient to whom FMT was administered. The AE did not

necessarily need to have a causal relationship with the treatment and thus we included
unfavorable signs or symptoms or disease temporally associated with the use of FMT, whether or
not related to the FMT. AEs could be clinically significant changes from baseline physical exam,
laboratory tests or other diagnostic investigations, complications related to the procedure used to
administer FMT, or new events or pre-existing conditions that became aggravated or worsened in
severity or frequency within 12 weeks post-FMT. SAEs were defined as any death, life
threatening experience, unplanned hospitalization, or important medical event within 12 weeks
after FMT. AEs and SAEs were determined to be related, probably or possibly related, or
unrelated to FMT. Secondary outcomes were CDI recurrence, need for colectomy, and response
to repeat FMT. Cure rates and percentages were calculated after one FMT and more than one
FMT for the population. Rates and percentages were also calculated for SAEs, AEs, and
inflammatory bowel disease (IBD) flares.
RESULTS
Study Patient Characteristics – Table 1a
Data collection forms were completed on 99 patients who had received FMT at one of the
study centers. Of these, 19 were excluded from analysis because they had undergone FMT for
indications other than CDI (15), did not meet criteria for IC (2), or were lost to follow-up prior to
having 12 weeks of post-FMT follow up (2). Eighty patients were included in the final analysis
(Table 1). The study population included similar numbers of men and women. The majority of
these patients were adults (75 of 80, 94%) and the mean age of the adults treated was 53 years
(range: 20-88 years). Reasons for IC included IBD patients treated with immunosuppressive
agents (37, 46.3 %), solid organ transplant recipients (19, 24%) and patients
immunocompromised because of severe or end-stage chronic medical conditions (17, 14%).
Additionally, there were 7 (8.9%) patients with cancer who were receiving antineoplastic agents
concurrently or within 3 months prior to FMT, and 3 (3.8%) patients had HIV/AIDs. Specific
immunosuppressant agents used, indications and numbers of patients exposed are listed in Table
1b. Recurrent CDI was the most common indication for FMT (44 of 80, 55%). Nine (11%) of
patients received FMT for refractory CDI and 27 (34%) met criteria for severe or complicated
CDI. FMT was conducted as a hospital inpatient in 17 (21.2%) patients and 63 (78.8%) received
FMT as outpatients.
Outcomes
Efficacy
Resolution of CDI occurred in 62 (78%) patients after a single FMT. Eleven patients who
either had recurrence or did not respond after one FMT underwent repeat FMT, of which 8 were
cured. Thus, overall cure (defined as resolution of CDI after one or more FMTs) within a
minimum of 12 weeks was observed in 70 (89%) patients.
Safety
SAEs were observed in 12 (15%) patients within 12 weeks post-FMT (Table 2a). Two
deaths occurred. One patient, whose diarrhea ceased after FMT, died secondary to progressive
pneumonia, for which he was being treated before FMT. The other died as a result of a
witnessed aspiration at the time of sedation for the colonoscopy used to administer the FMT.
There were 10 hospitalizations within 12 weeks of FMT. One patient was hospitalized with self-
limited abdominal pain, which occurred after the colonoscopy used to administer FMT and was
thus related to FMT. Three hospitalizations were unrelated to FMT and 1 case of influenza was
possibly related. Four patients were hospitalized with flares of IBD possibly related to FMT,
though more specific data regarding the course of their IBD prior to FMT was not obtained. One

catheter line infection requiring hospitalization occurred and was probably unrelated to FMT.
There were no infectious complications directly attributable to FMT. Three deaths were reported
outside of 12-weeks post-FMT and were not considered as SAEs. All occurred more than 6
months after FMT and were related to chronic progressive illnesses unrelated to CDI. Patients
with IBD did not have an increased rate of SAE (11%) compared to patients without IBD (18%).
We observed 13 patients with AEs (Table 2b). Of these, 4 were related, 6 were possibly related,
and 3 were unrelated to FMT. Three patients underwent colectomy, though none were for CDI.
One patient with ulcerative colitis (UC) had a colectomy less than 1 month post-FMT for
progressively worsening UC which had not improved after treatment of CDI. Another patient
with UC underwent colectomy 105 days post-FMT for indeterminate colitis and a third UC
patient had colectomy 293 days post-FMT for worsening UC.
Discussion and Limitations
This multicenter case series showed that 89% of IC patients achieved symptom resolution
after FMT for C. difficile infection and most CDI resolved after a single FMT. Rates of cure
were similar to those observed in previous studies.24,25 This population has previously been
excluded from FMT studies and possibly denied this effective therapy because of concern about
bacterial translocation and infection. In these 80 patients who underwent FMT at 16 centers,
there were no deaths or documented infections that occurred after FMT as result of the FMT
itself. One death occurred as a result of the procedure used to re-administer a second FMT in a
critically ill patient. We believe it is prudent to consider less invasive means of administering
FMT (such as enema or unsedated sigmoidoscopy) or delaying FMT in favor of traditional
medical management in unstable patients with severe or complicated CDI or significant
comorbidities. Administering vancomycin indefinitely to prevent further CDI recurrence is
another option when treating patients with a limited life expectancy in whom the risk of FMT
may outweigh benefits.
It is noteworthy that 14% of patients with IBD experienced complications post FMT in
the form of a disease exacerbation, one of which required a colectomy within 1 month of FMT.
No information about the course of IBD in these patients prior to FMT is known, and we cannot
say whether these flares were attributable to FMT, CDI or a progression of the underlying
disease. However, IBD flare after FMT to treat CDI in a patient with previously quiescent UC
has been reported31 and fevers along with temporary elevations of C reactive protein levels have
been described in small series of UC patients treated with FMT for IBD. 32,33 Certainly continued
studies regarding safety and efficacy of FMT in this population are warranted.
This study is the first to systematically report safety outcomes in FMT and the first to
address the question of efficacy and safety of FMT for CDI in IC patients. Physicians may be
reluctant to prescribe FMT in these patients in keeping with the presumption that they are “high
risk,” though there has not previously been evidence either for or against this belief in this
population. In fact, patients with recurrent CDI have been shown to have marked expansion of
members of the Enterobacteraceae family of Proteobacteria in their gut microbiota.34-36 which
are frequently relatively invasive pathobionts that may be responsible for other infectious
complications in these patients.37 In contrast, FMT leads to restoration of dominance of
Bacteroidetes and Firmicutes in the distal gut microbiota. It is reasonable to expect that
normalized gut microbial ecology should improve colonization resistance to potential pathogens
in IC patients.
IC patients have been excluded from clinical trials of FMT for concerns that seemed
reasonable yet were not supported by data. Prospective studies will enable real-time tracking of
patients and variables prior to and after FMT, which will help to eliminate biases, such as recall
or selection bias. In describing outcomes after FMT in this first series among IC hosts, many of
whom suffered from severe CDI, we hope to be an impetus for additional and prospective
studies. Furthermore, physicians may be encouraged to use FMT more frequently in this group
of patients. The multicenter design strengthened the study by increasing external validity,
minimizing any regional effects or skewing by individual clinician practices. There are no
standardized guidelines for the administration of FMT in terms of the amount of stool or routes
of administration. This study, performed at multiple sites, each with its own protocol for
administration, supports an overall curative effect seen among IC patients despite practice
variation. The FMT-performing clinicians closely followed each patient, enabling the collection
of good quality, complete data in this retrospective study.
Weaknesses of this study are related the retrospective design. The data points available
for the study were limited to data that was collected and available in the medical record at each
center. Patients were not solicited for adverse events which were only included in the study if
documented in the medical record at the study center. However, all centers provided sufficient
details to answer the 32-item survey tool required to analyze the primary outcomes. Additional
limits included potential selection and recall biases. More information on each patient’s
functional status and course of immunocompromising illnesses could be helpful in stratifying
patients as sickest to healthiest among this IC group. The multicenter design, while a strength,
also made standardization of data points challenging. Classification of CDI was based specific
criteria, though the data collection survey did not distinguish between severe and complicated
CDI or allow submitting centers to specify which criteria for severe or complicated disease were
fulfilled. Patients may have been classified as severe based on leukocytosis or low albumin (not
necessarily sepsis or organ failure). Furthermore, it is unknown at what time point FMT was
performed in these severe patients, such as after a course of vancomycin when they had
improved clinically but were at risk for further recurrence. The fact that the majority of these
FMTs were performed as outpatient procedures suggests that most patients in this series were not
acutely ill at the time of FMT. Ultimately, a prospective cohort study of patients with complex
CDI or a matched case-control series would be reasonable to further investigate the use of FMT
in CDI in IC patients, while minimizing some of these biases. In conclusion, this study showed
that FMT appears to be a safe and effective treatment for recurrent, refractory or severe CDI in
this high risk population of IC patients.

REFERENCES
1. Cohen SH, Gerding DN, Johnson S, et al. Clinical Practice Guidelines for Clostridium
difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of
America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control
Hosp Epidemiol 2010; 31(5):431–55.
2. McDonald LC, Owings M, Jernigan DB. Clostridium difficile Infection in Patients
Discharged from US Short Stay Hospitals, 1996-2003. Emerg Infect Dis 2006; 12(3):409-
15.
3. King RN, Lager SL. Incidence of Clostridium difficile infections in patients receiving
antimicrobial and acid-suppression therapy. Pharmacotherapy 2011; 31(7):642-8.
4. Sanchez TH, Brooks JT, Sullivan PS et al. Bacterial Diarrhea in Persons with HIV Infection,
United States, 1992-2002. Clin Infect Dis 2005; 41:1621-1627.
5. West M, Pirenne J, Chavers B et al. Clostridium difficile colitis after kidney and kidney-
pancreas transplantation. Clin Transplant 1999; 13:318–323.
6. Gorschluter M, Glasmacher A, Hahn C et al. Clostridium difficile infection in patients with
neurtropenia. Clin Infect Dis 2001; 33:786-791.

7. Anand A. Glatt AE. Clostridium difficile infection associated with antineoplastic
chemotherapy: a review. Clin Infect Dis 1993; 17:109-113.
8. Buffie CG, Pamer EG. Microbiota-mediated colonization resistance against intestinal
pathogens. Nat Rev Immunol 2013; 13(11):790-801.
9. Kyne L, Warny M, Qamar A et al. Association between antibody response to toxin A and
protection against recurrent Clostridium difficile diarrhea. Lancet 2001; 357:189–93.
10. Leav BA, Blair B, Leney M et al. Serum anti-toxin B antibody correlates with protection
from recurrent Clostridium difficile infection (CDI). Vaccine 2010; 28: 965–969.
11. Rodemann, J.F., et al., Incidence of Clostridium difficile infection in inflammatory bowel
disease. Clin Gastroenterol Hepatol, 2007. 5(3): p. 339-44.
12. Binion, D.G., Clostridium difficile Infection in Patients with Inflammatory Bowel Disease.
Gastroenterol Hepatol (N Y), 2012. 8(9): p. 615-7.
13. Ananthakrishnan, A.N., et al., A nationwide analysis of changes in severity and outcomes of
inflammatory bowel disease hospitalizations. J Gastrointest Surg, 2011. 15(2): p. 267-76.
14. Ananthakrishnan, A.N., et al., Temporal trends in disease outcomes related to Clostridium
difficile infection in patients with inflammatory bowel disease. Inflamm Bowel Dis, 2011.
17(4): p. 976-83.
15. Nguyen, G.C., et al., A national survey of the prevalence and impact of Clostridium difficile
infection among hospitalized inflammatory bowel disease patients. Am J Gastroenterol,
2008. 103(6): p. 1443-50.
16. Jen, M.H., et al., Increased health burden associated with Clostridium difficile diarrhoea in
patients with inflammatory bowel disease. Aliment Pharmacol Ther, 2011. 33(12): p. 1322-
31
17. Meyer, A.M., et al., The diagnostic yield of stool pathogen studies during relapses of
inflammatory bowel disease. J Clin Gastroenterol, 2004. 38(9): p. 772-5.
18. Schneeweiss, S., et al., Infliximab and other immunomodulating drugs in patients with
inflammatory bowel disease and the risk of serious bacterial infections. Aliment Pharmacol
Ther, 2009. 30(3): p. 253-64.
19. Das, R., P. Feuerstadt, and L.J. Brandt, Glucocorticoids are associated with increased risk of
short-term mortality in hospitalized patients with clostridium difficile-associated disease. Am
J Gastroenterol, 2010. 105(9): p. 2040-9.

20. Berg A, Kelly C, Farray F. Clostridium difficile Infection in the Inflammatory Bowel Disease
Patient. Inflamm Bowel Dis 2013; 19(1):194-204.
21. McFarland LV, Surawicz CM, Rubin M, et al. Recurrent Clostridium difficile disease:
Epidemiology and clinical characteristics. Infect Control Hosp Epidemiol 1999;20:43-50.
22. McFarland LV. Alternative treatments for Clostridium difficile disease: what really works?
Journal of Medical Microbiology 2005;54:101-11.
23. Eiseman B, Silen W, Bascom, GS, et al. Fecal enema as an adjunct in the treatment of
pseudomembranous enterocolitis. Surgery 1958;44:854.
24. Kassam Z, Lee CH, Yuan Y, et al. Fecal microbiota transplantation for Clostridium difficile
infection: systematic review and meta-analysis. Am J Gastroenterol 2013 Apr;108(4):500-8.
25. Van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal Infusion of Donor Feces for
Recurrent Clostridium difficile. N Engl J Med 2013; 368(5):407-15.
26. Dubberke ER, Burdette SE, et al. Clostridium difficile Infections in Solid Organ
Transplantation. Am J Transplant 2013; 13:42-49.
27. Munoz P, Bouza E, Cuenca-Estrella M et al. Saccharomyces cerevisiae fungemia: an
emerging infectious disease. Clin Infect Dis 2005; 40:1625–1634.
28. Surawicz CM, Brandt LJ, Binion DG et al. Guidelines for diagnosis, treatment, and
prevention of Clostridium difficile infections. Am J Gastroenterol. 2013; 108(4):478-98.
29. Bakken JS, Borody T, Brandt LJ, et al. Treating Clostridium difficile infection with fecal
microbiota transplantation. Clin Gastroenterol Hepatol 2011;9(12):1044-9.
30. Kelly C, Brandt L. Fecal Transplant for Relapsing C. difficile infection. Trial in progress.
Accessed December 27, 2013 at: http://clinicaltrials.gov/ct2/show/NCT01703494?
term=FMT+providence&rank=1
31. De Leon L, Watson J, Kelly C. Transient Flare of Ulcerative Colitis After Fecal Microbiota
Transplantation for Recurrent Clostridium difficile Infection. Clin Gastroenterol Hepatol
2013; 11(8):1036-8.
32. Angelberger S, Reinisch W, Makristathis A, et al. Temporal Bacterial Community Dynamics
Vary Among Ulcerative Colitis Patients After Fecal Microbiota Transplantation. Am J
Gastroenterol 2013; 108:1620-30.
33. Kump PK, Grochenig HP, Lackner S, et al. Alteration of intestinal dysbiosis by fecal
microbiota transplantation does not induce remission in patients with chronic active
ulcerative colitis. Inflmm Bowel Dis 2013; 19(10):2155-65.

34. Chang JY, Antonopoulos DA, Kalra A, et al. Decreased diversity of the fecal microbiome in
recurrent Clostridium difficile associated diarrhea. J Infect Dis 2008;197(3):435-6.
35. Hamilton MJ, Weingarden AR, et al. High-thoughput DNA sequence analysis reveals stable
engraftment of gut microbiota following transplantation of previously frozen fecal bacteria.
Gut Microbes 2013;4(2):125-35.
36. Weingarden AR, Chen C, Bobr A, et al. Microbiota Transplantation Restores Normal Fecal
Bile Acid Composition in Recurrent Clostridium difficile Infection. Am J Physiol
Gastrointest Liver Physiol 2013; Nov 27 [Epub ahead of print].
37. Chow J, Tang H, Mazmanian SK. Pathobionts of the gastrointestinal microbiota and
inflammatory disease. Curr Opin Immunol 2011; 23(4):473-80.
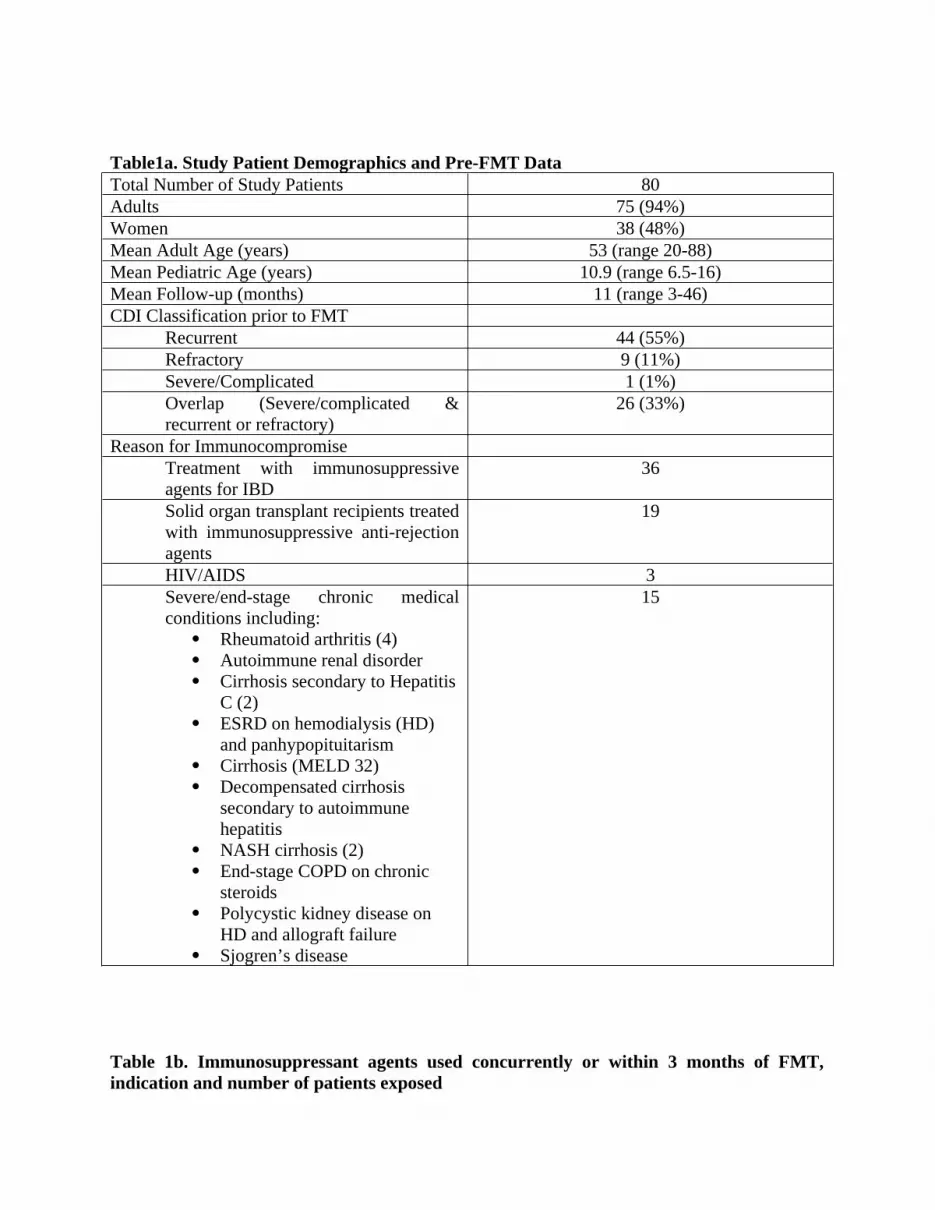
Table1a. Study Patient Demographics and Pre-FMT DataTotal Number of Study Patients 80Adults 75 (94%)Women 38 (48%)Mean Adult Age (years) 53 (range 20-88)Mean Pediatric Age (years) 10.9 (range 6.5-16)Mean Follow-up (months) 11 (range 3-46)CDI Classification prior to FMT
Recurrent 44 (55%)Refractory 9 (11%)Severe/Complicated 1 (1%)Overlap (Severe/complicated & recurrent or refractory)
26 (33%)
Reason for ImmunocompromiseTreatment with immunosuppressive agents for IBD
36
Solid organ transplant recipients treated with immunosuppressive anti-rejection agents
19
HIV/AIDS 3Severe/end-stage chronic medical conditions including:
Rheumatoid arthritis (4) Autoimmune renal disorder Cirrhosis secondary to Hepatitis
C (2) ESRD on hemodialysis (HD)
and panhypopituitarism Cirrhosis (MELD 32) Decompensated cirrhosis
secondary to autoimmune hepatitis
NASH cirrhosis (2) End-stage COPD on chronic
steroids Polycystic kidney disease on
HD and allograft failure Sjogren’s disease
15
Table 1b. Immunosuppressant agents used concurrently or within 3 months of FMT, indication and number of patients exposed

Agent Indication Number of patients exposedInfliximab IBD 12
Adalimumab IBD 3Natalizumab MS 1Nataluzimab IBD 1
Certolizumab pegol IBD 1Prednisone SOT 6Prednisone COPD 1Prednisone IBD 15Prednisone RA 3
Hydrocortisone Autoimmune kidney disease 1Hydrocortisone Panyhypopituitarism 1Hydrocortisone IBD 1
Solumedrol IBD 2Methotrexate IBD 3Methotrexate RA 2Azathioprine IBD 10Azathioprine SOT 3
6-mercaptopurine IBD 1Sirolimus IBD 1
Tacrolimus SOT 15Mycophenolate mofetil SOT 6
Cyclosporine SOT 3Bevacizumab Cancer 1Adriamycin Cancer 1Fludarabine Cancer 1
5-FU Cancer 1Cisplatin Cancer 1
Bleomycin Cancer 1Dasatanib Cancer 1
Lenalidomide Multiple Myeloma 1Leflunomide RA 1
Plaquenil Sjogrens 1Rituximab RA 1
Table 2a. Serious Adverse EventsSerious Adverse Event (Etiology) Number of days post-FMT event occurred

DeathsPneumonia complicated by effusions present pre-FMT
13
Aspiration during sedation for colonoscopy to administer FMT
0
HospitalizationsFever, cirrhosis-related encephalopathy and pancytopenia
4
Abdominal pain-self limited; no antibiotics or sequelae
0
Crohn’s flare *<84UC flare *<84Crohn’s flare *<84CVA; nausea & vomiting 21UC flare *<28Fall and sustained hip fracture 84Influenza B 3Catheter infection *<84
*exact number of days post-FMT but within 12 week follow up period at which event occurred unknown
Table 2b. Adverse EventsAdverse Event Number of patients sustaining this AE
Self-limited diarrheal illness (non-CDI, not requiring hospitalization)
5
Fever 1Bloating & abdominal discomfort immediately post- FMT (lasting <48 hours)
3
Hip pain 1Pertussis 1Nausea (one month post-FMT) 1Mucosal tear during colonoscopy used to administer FMT repaired with clip; no sequelae
1