dilated cardiomyopathy 09.20.2013
TRANSCRIPT
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 1/19
MORNING REPORTCaitlin Kaeppler
9/20/2013
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 2/19
You’re on the wards and it’s the last day of
Intern year… • 6-month-old male who is directly admitted from an outside
hospital for respiratory distress.
• More sleepy and has decreased appetite for the past fewdays. No fevers or URI symptoms.
• Day prior to admission, the family was camping and had been
swinging the infant in a tire swing and picked him up and hesubsequently had NBNB emesis that was projectile.
• After this, he seemed very sleepy and developed perioralcyanosis. There was no choking or respiratory distress. Hewas responding to parents but would fall asleep very easily.
• Parents drove him to Hospital (about 20 minutes away.) Theyhad to poke him several times to keep him awake during thecar ride because he was so sleepy.
• At the OSH, parents say that his color was much better but hewas still acting very sleepy. In the ED, he had de-sats requiring1 LPM NC O2 and he was admitted.
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 3/19
At the OSH…
• Parents say that during his admission (~36h), he became
less sleepy but more irritable. He had eaten well
overnight, waking up almost every hour to eat. He
continued to have emesis. No diarrhea.
• He remained on supplemental 1L NC O2 overnight but
due to lack of improvement in respiratory status the next
morning, he was transferred to Primary Children’s
Hospital inpatient service for further management.
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 4/19
HPI continued…
• PMH: Born full term via NSVD without complications. He hadcongenital cataracts. No other medical problems.
• PSH: Cataract surgery 1 month prior to admission
• Immunizations: Has not yet received his 6 month vaccines but
is otherwise up to date.• Meds: None
• Allergies: NKDA
• Diet: Formula fed and assorted table foods
• Development: Appropriate for age
• FH: No history of significant medical problems in childhood.
• SH: Lives in UT with his parents, no other siblings. There is acat in the home. No one has been sick at home. The familywas camping when his symptoms began.

7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 5/19
Review of SystemsGENERAL/CONSTITUTIONAL: Increased in fatigue over the past few days. Nofever, change in appetite, change in weight.
HEENT: Denies eye redness or irritation. No problems with hearing or ear pain. No epistaxis, runny nose, congestion, sneezing. No mouth sores, sorethroat, or problems swallowing.CARDIOVASCULAR: Shortness of breath since admission to OSH. Nosweating with feeds, color change with feeds, history of murmur, or fainting.
RESPIRATORY: Respiratory distress with desats requiring supplementaloxygen. Perioral cyanosis prior to ED presentation. Denies chronic cough,hemoptysis, history of pneumonia, wheezing, or night sweats.GASTROINTESTINAL: NBNB vomiting. Denies diarrhea, pain with urination, or blood in urine.MUSCULOSKELETAL: Denies joint or muscle pain, neck pain, or recent injuries.HEME: Denies easy bruising or bleeding tendency.
SKIN: Denies rashes or new lesions.NEUROLOGIC: Irritability over the past day. Prior to that, he had beenlethergic. Denies trauma, LOC, seizure activity, or developmental delays.
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 6/19
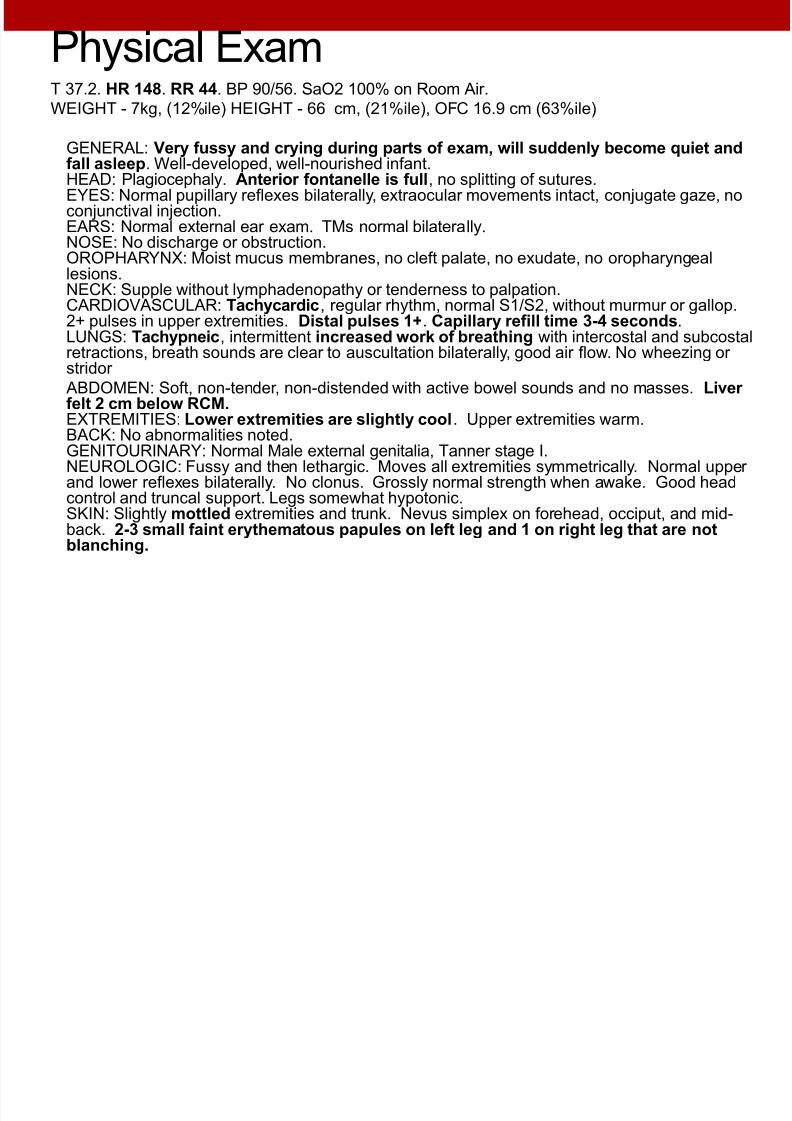
Physical ExamT 37.2. HR 148. RR 44. BP 90/56. SaO2 100% on Room Air.
WEIGHT - 7kg, (12%ile) HEIGHT - 66 cm, (21%ile), OFC 16.9 cm (63%ile)
GENERAL: Very fussy and crying during parts of exam, will suddenly become quiet andfall asleep. Well-developed, well-nourished infant.HEAD: Plagiocephaly. Anterior fontanelle is full, no splitting of sutures.EYES: Normal pupillary reflexes bilaterally, extraocular movements intact, conjugate gaze, noconjunctival injection.EARS: Normal external ear exam. TMs normal bilaterally.NOSE: No discharge or obstruction.OROPHARYNX: Moist mucus membranes, no cleft palate, no exudate, no oropharyngeal
lesions.NECK: Supple without lymphadenopathy or tenderness to palpation.CARDIOVASCULAR: Tachycardic, regular rhythm, normal S1/S2, without murmur or gallop.2+ pulses in upper extremities. Distal pulses 1+. Capillary refill time 3-4 seconds.LUNGS: Tachypneic, intermittent increased work of breathing with intercostal and subcostalretractions, breath sounds are clear to auscultation bilaterally, good air flow. No wheezing or stridor
ABDOMEN: Soft, non-tender, non-distended with active bowel sounds and no masses. Liver felt 2 cm below RCM. EXTREMITIES: Lower extremities are slightly cool. Upper extremities warm.BACK: No abnormalities noted.GENITOURINARY: Normal Male external genitalia, Tanner stage I.NEUROLOGIC: Fussy and then lethargic. Moves all extremities symmetrically. Normal upper and lower reflexes bilaterally. No clonus. Grossly normal strength when awake. Good headcontrol and truncal support. Legs somewhat hypotonic.SKIN: Slightly mottled extremities and trunk. Nevus simplex on forehead, occiput, and mid-back. 2-3 small faint erythematous papules on left leg and 1 on right leg that are not
blanching.
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 7/19
Differential diagnosis for a 6-month-old male
with two days of respiratory distress, altered
mental status, emesis, and poor perfusion on
exam…
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 8/19
Differential Diagnosis:Respiratory:
-Bronchiolitis-Asthma or reactive airway disease
-Bacterial pneumonia
-Aspiration
-Foreign body
-Pneumothorax
-Pulmonary edema
-HAPE
CV:
-Congenital heart defect
-Cardiomyopathy
-Myocarditis
-Cardiogenic shock
-Arrythmia-Pericardial effusion
-Pericarditis
FEN/GI:
-GERD
-Dehydration
-Gastroenteritis-Ulcers
NEURO:
-Space-occupying lesion-HACE
HEME/ID
-Septic shock
-Meningitis- bacterial or viral
-Viral encephalitis
-TORCH infection-Anemia
Metabolic
-Inborn error of metabolism
Other:
-Trauma-NAT
-Ingestion
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 9/19
Labs and Tests
• OSH labs: Tox screen was negative, VRP negative,
electrolytes normal, CXR reportedly normal
• Initial labs: Blood gas showed pH 7.36, mild metabolic
acidosis. Lactate 5.
• 10 cc/kg NS bolus was started
• Patient was sent to radiology for a stat head CT, CXR,
and KUB
• Head CT: Unexplained ventricular and extraventricular fluid prominence.
• KUB normal
• CXR…

7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 10/19
Radiology

7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 11/19
Radiology
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 12/19
Radiology
• Kerley B lines represent interstitial edema in the
pulmonary septa from back-up of flow from left ventricular
failure.
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 13/19
Treatment Course
• Cardiology was called and the fellow performed a statecho at bedside, which showed marked left ventricular dilation and estimated EF 16%
• Transferred to PICU
• Approximately 15 minutes after arrival to the PICU, thepatient had a PEA arrest. Due to potential reversibility of this process, ECMO was activated. He received 17 dosesof epinephrine and 50 minutes of CPR without consistentreturn of pulses
• Emergent decompressive atrial septostomy
• Studies sent: EBV, HSV, CMV, HIV, mycroplasma, toxo, Adenovirus, respiratory viral panel
• Acyclovir started and IVIG for myocarditis
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 14/19
Dilated Cardiomyopathy
• Most common reason for heart transplantation in children
worldwide and the most common cardiomyopathy in
children
• Ventricular dilation may help compensate and maintain
cardiac output, so children may remain asymptomatic for
many years
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 15/19

7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 16/19
Presentation
• Predominantly left-sided
• Cough, dyspnea on exertion, orthopnea
• Predominantly right-sided
• Abdominal pain, emesis, anorexia, peripheral edema
• All patients
• Nausea, chest pain, diaphoresis, palpitations
• Physical exam shows tachypnea, rales, increased JVP,
hepatomegaly, peripheral edema
7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 17/19
Circulatory shock
• In children, CO is more dependent on heart rate than on
stroke volume due to lack of ventricular muscle mass
• Children maximize SVR to maintain a normal BP, even
with significant decreases in CO
• Therefore, pay most attention to HR and perfusion (cap
refill, pulses, UOP, mentation)

7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 18/19
Shock
Heart rate Pulses/Perfusion Blood Pressure
Hypovolemic
Septic
Distributive
Cardiogenic

7/27/2019 Dilated Cardiomyopathy 09.20.2013
http://slidepdf.com/reader/full/dilated-cardiomyopathy-09202013 19/19
References
• Pediatrics in Review: Index of Suspicion. Vol 25, No. 3.
March 2004.
• Madriago, Erin and Michael Silberbach. Heart Failure in
Infants and Children. Pediatrics in Review 2010;31;4
• McKiernan, Christine A. and Stephen A. Lieberman.
Circulatory Shock in Children: An Overview. Pediatrics in
Review. 2005;26;451