case report posterior cortical atrophy presenting with...
TRANSCRIPT
Case ReportPosterior Cortical Atrophy Presenting withSuperior Arcuate Field Defect
Sue Ling Wan,1,2 Danuta M. Bukowska,1 Stephen Ford,3 and Fred K. Chen1,2
1Centre for Ophthalmology and Visual Science (Incorporating Lions Eye Institute), The University of Western Australia,Nedlands, WA 6009, Australia2Department of Ophthalmology, Royal Perth Hospital, Perth, WA 6000, Australia3Department of Psychiatry, Sir Charles Gairdner Hospital, North Metropolitan Mental Health Service, Older Adult Program,Nedlands, WA 6009, Australia
Correspondence should be addressed to Fred K. Chen; [email protected]
Received 17 March 2015; Revised 28 July 2015; Accepted 13 August 2015
Academic Editor: Cristiano Giusti
Copyright © 2015 Sue Ling Wan et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
An 80-year-old female with reading difficulty presented with progressive arcuate field defect despite low intraocular pressure. Overa 5-year period, the field defect evolved into an incongruous homonymous hemianopia and the repeated neuroimaging revealedprogressive posterior cortical atrophy. Further neuropsychiatric assessment demonstrated symptoms and signs consistent withBenson’s syndrome.
1. Introduction
Posterior cortical atrophy (PCA) is a neurodegenerativesyndrome characterised by atrophy of the posterior cere-bral cortex and disruption of higher visual functions. Herewe describe a unique case of posterior cortical atrophypresenting with superior arcuate defect simulating earlyglaucoma.
2. Case Presentation
A right-handed 80-year-old Caucasian female was referredfor further evaluation of reading difficulty. She initiallypresented at age of 72 years with reduced vision and glare. Shehad no history of stroke or head injury. Following bilateralsequential phacoemulsification and insertion of intraocularlenses, she was diagnosed by a general ophthalmologistwith low tension glaucoma in the left eye on the basis ofunilateral superior arcuate field defect, temporal neuroretinalrim thinning, and a maximum intraocular pressure (IOP)of 17mmHg at several clinic visits over an 18-month period(Figures 1(a)-1(b)). Timolol and then subsequently combinedtimolol-latanoprost eye drops were prescribed and IOP was
reduced to around 12–15mmHg. Despite good control over4 years, the left visual field defect progressed and left sidedhomonymous hemianopia developed in the right visualfield without significant change in the optic nerve heads(Figure 1(a)). Since she was also experiencing difficulty inreversing her car due to poor vision on the left-hand side, herantiglaucoma medication was ceased and ocular diagnosisreevaluated. Brain and orbital computer tomography (CT)scan showed no compressive lesion in the posterior visualpathway.Magnetic resonance imaging (MRI) of the brain andorbits (without contrast) demonstrated nomass or infiltrativelesion in the optic tracts or nerves that could explain thehemianopia. Although technically difficult, visual electro-physiology demonstrated delayed P50 and N95 implicittimes with only mild reduction in amplitude on patternelectroretinography (PERG) whilst small and large checkpattern visual evoked potentials (PVEP) were significantlyreduced (Figure 2). At this point, further opinion was soughtto exclude a retinal cause for her progressive visual fieldloss.
Examination showed visual acuity of 6/9 in both eyeswithIOPs of 10 and 11mmHg in right and left eyes. Pupil reactionswere slow and a definite afferent pupillary defect could not
Hindawi Publishing CorporationCase Reports in Ophthalmological MedicineVolume 2015, Article ID 796381, 6 pageshttp://dx.doi.org/10.1155/2015/796381
2 Case Reports in Ophthalmological Medicine
T1 coronal scan T2 axial scan
2013
2014
Left eyeRight eye
(b)
(c)
Left eyeD
ecem
ber 2
012
Right eyeAp
ril 2
009
April
201
3N
ovem
ber 2
014
30
30
30
30 30
30
30
30
(a)
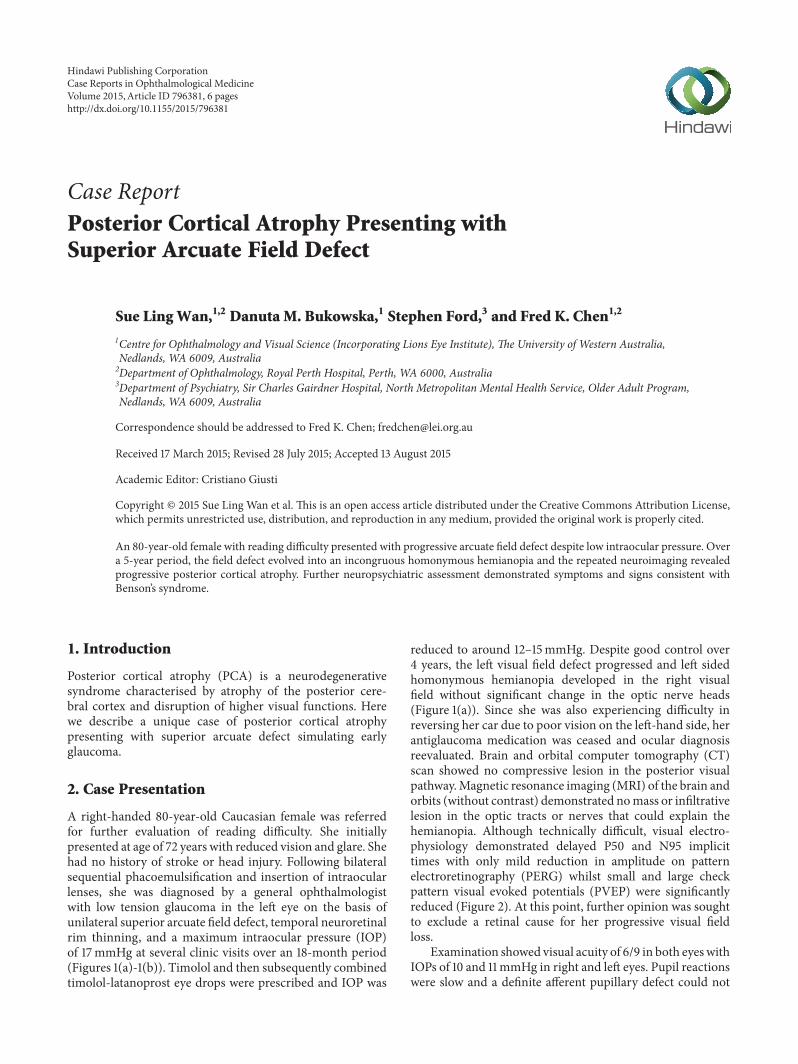
Figure 1: (a) Serial Humphrey visual fields fromApril 2009 toNovember 2014 showing progression of superior arcuate defect in the left eye toleft-sided incongruous homonymous hemianopia. (b) Optic nerve head imaging in 2014 using theHeidelberg retinal tomography showing nosignificant disc cupping. (c) Coronal and axial magnetic resonance imaging (without contrast) in 2013 and 2014 showed progressive parietaland occipital cortical atrophy. Posterior cortical atrophy was suspected only in the 2014 scan.
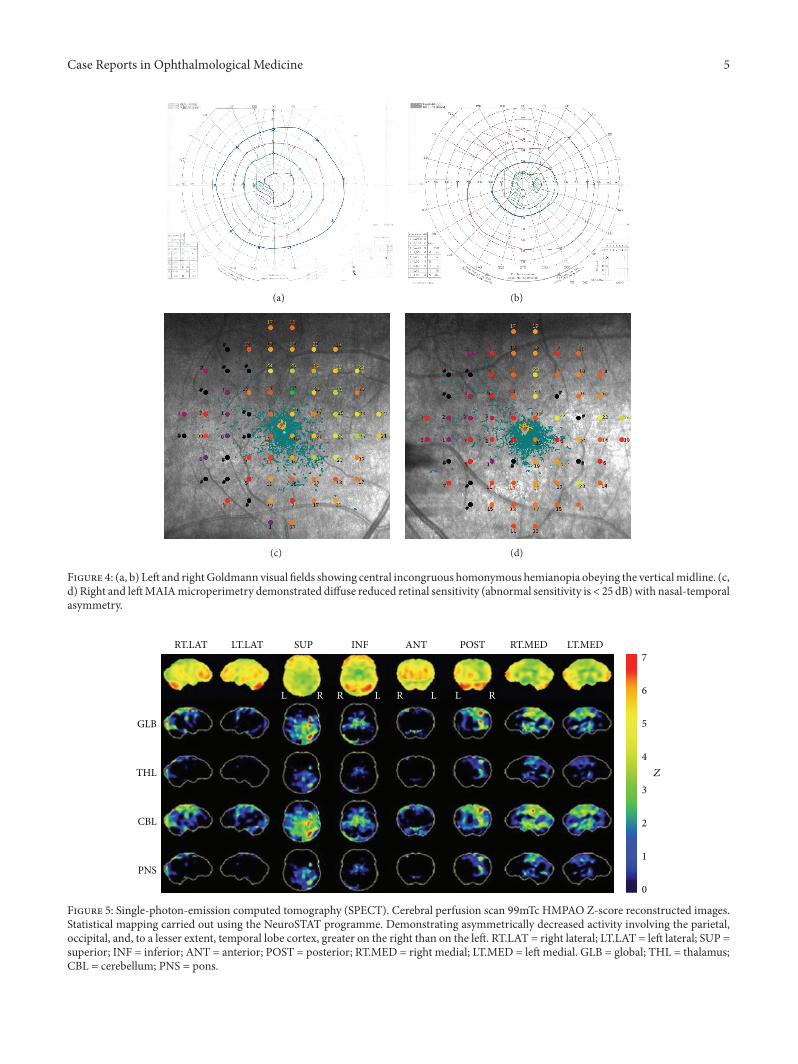
be elicited. Range of ocular motility was full but saccadeswere hypometric. She was unable to recognise any numberson the Ishihara pseudoisochromatic charts despite being ableto discriminate hues of colours by tracing out the numberscorrectly from each eye separately using her dominant indexfinger. Slight temporal pallor of the discs was noted inboth eyes and there was no glaucomatous disc cupping(Figures 3(a)-3(b)). Drusen were noted in the peripheralretina and retinal vessels and maculae were normal. Nervefibre layer thickness on optical coherence tomography waswithin normal limits in each eye (Figures 3(c)-3(d)). RepeatHumphrey visual field testing consistently demonstratedan incomplete incongruous hemianopia (Figure 1(a)). Gold-mann field showed hemianopic defect obeying the verticalmidline whilst microperimetry (MAIA, CentreVue, Padova,Italy) demonstrated diffuse reduction in macular sensitivitywith nasal-temporal asymmetry (Figure 4).
The combination of number agnosia and statokineticdissociation of the incongruous homonymous hemianopiaredirected our attention to the occipital cortex. A repeat MRIscan confirmed parietal, occipital, and posterior temporalatrophy, more severe on the right side involving the rightoccipital lobe, suggesting a diagnosis of posterior corticalatrophy (PCA or Benson’s syndrome). Comparison to previ-ousMRI scan in 2013 showeddeterioration in cortical atrophy(Figure 1(c)). Detailed psychogeriatric assessment revealedsimultanagnosia, left visual neglect, constructional apraxia,number and image agnosia, altered colour perception, andmild memory and language deficits. She scored 78/100 onAddenbrooke’s Cognitive Examination (version 3, normal >82)with prominent deficits on the visuospatial (10/16) and thememory (23/26) subscales. On the Informant Questionnaireon Cognitive Decline in the Elderly (IQCODE, score =3.75), her husband rated her as having deteriorated memory
Case Reports in Ophthalmological Medicine 3
Pattern-ERG transient Pattern-ERG steady-stateRight eye Left eye Right eye Left eye5𝜇V/div
20ms/div
5𝜇V/div
20ms/div
(a)
Pattern-VEP60minPattern-VEP15min
Right eye Left eye Right eye Left eye10𝜇V/div
50ms/div
10𝜇V/div
50ms/div
(b)
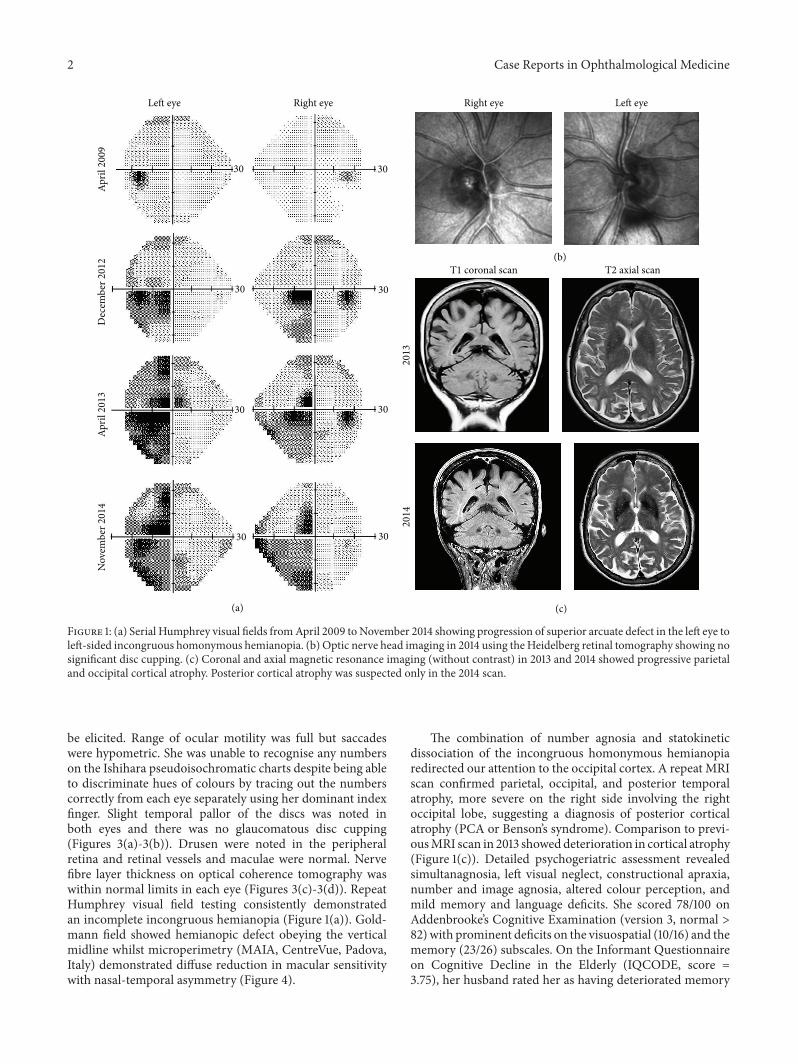
Figure 2: (a) Pattern electroretinography showing delayed P50 and N95 implicit times and only mild reduction in amplitude. (b) Patternvisual evoked potential showing significant reduction in amplitude.
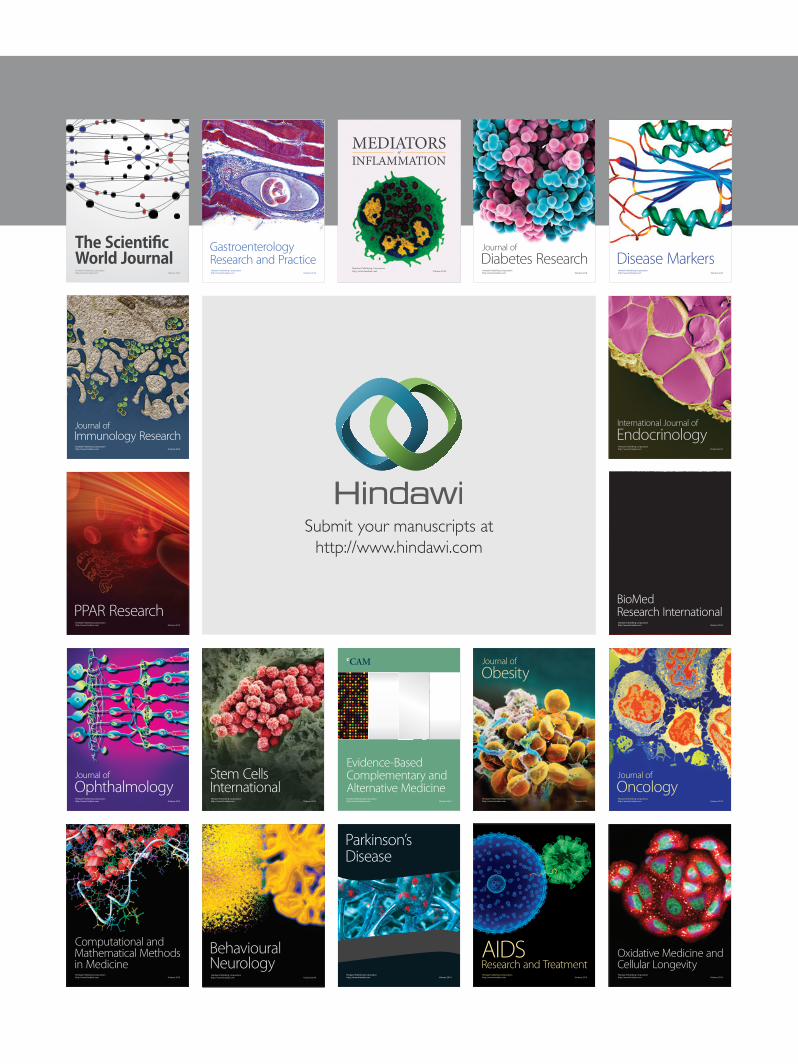
about family and friends and much worse for recent events.Functionally the main impairment was difficulty in judgingdistances and visual search. Cerebral perfusion scan demon-strated cognitive and perfusion deficits that were consistentwith this diagnosis (Figure 5) and not consistent with typicalAlzheimer’s disease or Lewy body dementia.
3. Discussions
This case illustrates the evolution of PCA and the diagnosticdilemma faced by three ophthalmologists whenPCApresentswith nonspecific symptoms such as difficulty in readingand subtle visual field defect. The differential diagnosis forthis patient’s presentation includes low tension glaucoma,ischaemic optic neuropathy, and postchiasmal visual pathwaydiseases. The lack of neuroretinal rim thinning despite pro-gressive field defect makes glaucoma unlikely. The abnormalIshihara chart test result could be due to number agnosia asthe patient was able to discriminate hues of colour by tracing
out the numbers correctly using each eye separately. Furtherneuropsychiatric assessment showed that she was unable toname or distinguish colours placed adjacent to each other andthis may be secondary to colour agnosia or cerebral achro-matopsia. Although nonarteritic ischaemic optic neuropathy(NAION) can present with pallor of the optic nerve head,paracentral scotoma, and reduced colour vision, progressionof incongruous homonymous hemianopia, hemifield visualneglect, and the development of simultanagnosia, construc-tional apraxia, and deficit of a variety of other corticalfunctions despite preservation of nerve fibre layer thicknesssuggests that PCA is a more likely diagnosis than NAION.The possibility of PCA was also supported by features onMRI and functional brain imaging. Although it took threeneuroimaging sessions to confirm PCA, a comparison withprior scans showed that cortical atrophy was already present,but, to a lesser extent, in the occipital lobe. This highlightsthe importance of the treating physician in communicatingwith the radiologist to evaluate cortical atrophy as well as
4 Case Reports in Ophthalmological Medicine
(a) (b)
RNFL layer thickness
Position (∘)
Within normal limits (p > 0.05)Borderline (p < 0.05)Outside normal limits (p < 0.01)
0 45 90 135 180 225 270 315 360
TMP SUP NAS INF TMP
0
60
120
180
240
300
RNFL
thic
knes
s (𝜇
m)
SD-OCT B-scan
200𝜇m
(c)
RNFL layer thickness
0
60
120
180
240
300
RNFL
thic
knes
s (𝜇
m)
Position (∘)
Within normal limits (p > 0.05)Borderline (p < 0.05)Outside normal limits (p < 0.01)
0 45 90 135 180 225 270 315 360
TMP SUP NAS INF TMP
SD-OCT B-scan
200𝜇m
(d)
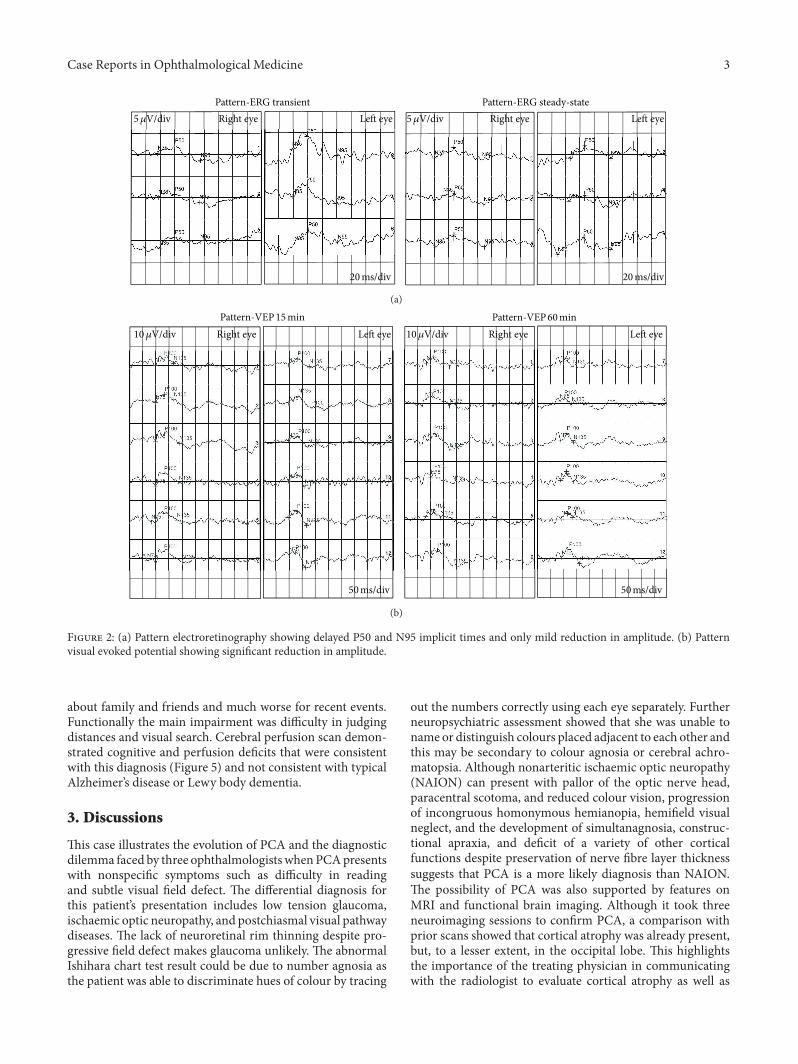
Figure 3: (a, b) Optic nerve head and (c, d) nerve fibre layer thickness imaging showing mild temporal pallor but no glaucomatous disccupping and normal peripapillary nerve fibre thickness profile.
ruling out compressive lesionwithin the visual pathwaywhencentral visual loss is investigated by neuroimaging. However,diagnosing early stage PCA with structural neuroimaging byMRI is often difficult, and examination by a neurologist orpsychologist ismore important. Another unique aspect in ourcase study is the illustration of incongruous hemianopia usingmicroperimetry. Furthermore, combining microperimetrywith kinetic perimetry, we have also demonstrated statoki-netic dissociation, a common feature of cortical visual loss.
PCA was first described in 1988 by Benson et al. [1].Recent literature reviews have summarised the visual clinical
features, neuroimaging, possible pathology, biology, andgenetics of PCA [2–4]. Alzheimer’s disease is the mostcommon underlying cause of PCA in pathological studiesalthough there is continuing debate on whether these are twoseparate conditions. PCA is a relatively rare condition andthe visual manifestations are outlined in Table 1. Our casedemonstrated that patients may not have obvious corticalatrophy on clinical imaging in the early stages. Greaterawareness of the syndrome will improve identification ofearly symptoms of PCA and prevent unnecessary medicalinterventions.
Case Reports in Ophthalmological Medicine 5
(a) (b)
(c) (d)
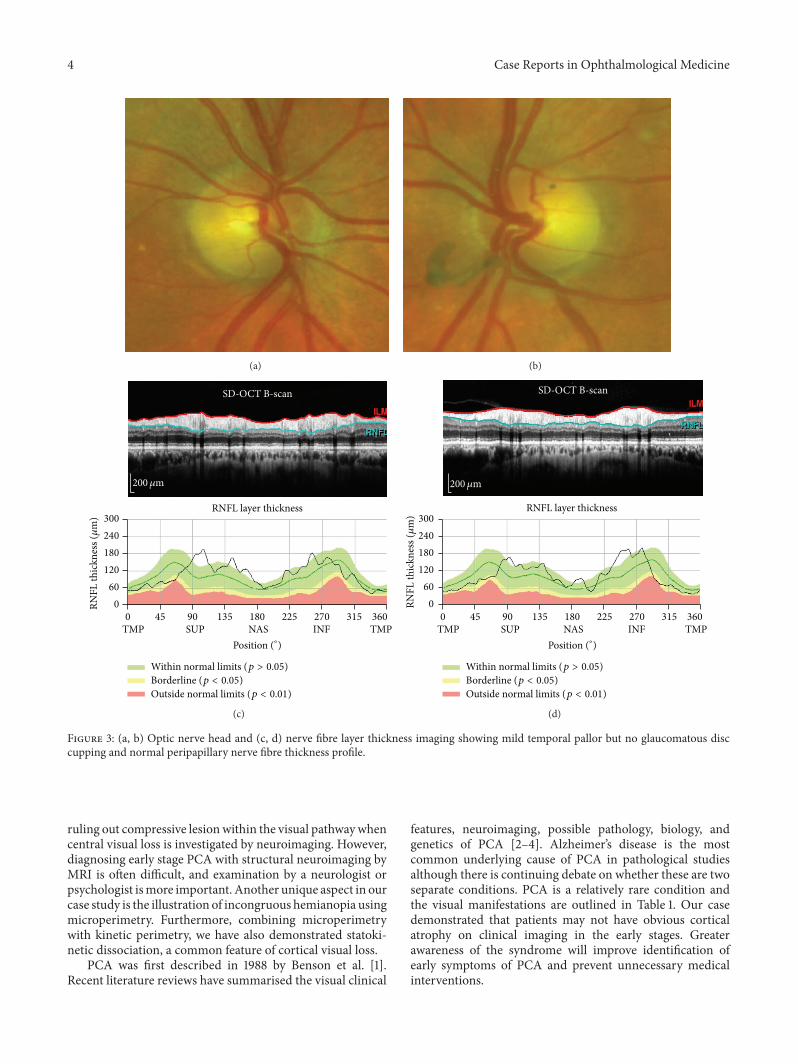
Figure 4: (a, b) Left and rightGoldmann visual fields showing central incongruous homonymous hemianopia obeying the verticalmidline. (c,d) Right and leftMAIAmicroperimetry demonstrated diffuse reduced retinal sensitivity (abnormal sensitivity is< 25 dB) with nasal-temporalasymmetry.
GLB
THL
CBL
PNS
RT.LAT LT.LAT SUP INF ANT POST RT.MED LT.MED
L LR R LR L R
Z
7
6
5
4
3
2
1
0
Figure 5: Single-photon-emission computed tomography (SPECT). Cerebral perfusion scan 99mTc HMPAO Z-score reconstructed images.Statistical mapping carried out using the NeuroSTAT programme. Demonstrating asymmetrically decreased activity involving the parietal,occipital, and, to a lesser extent, temporal lobe cortex, greater on the right than on the left. RT.LAT = right lateral; LT.LAT = left lateral; SUP =superior; INF = inferior; ANT = anterior; POST = posterior; RT.MED = right medial; LT.MED = left medial. GLB = global; THL = thalamus;CBL = cerebellum; PNS = pons.

6 Case Reports in Ophthalmological Medicine
Table 1: Visual manifestations of posterior cortical atrophy [3].
Glare sensitivity Impaired contrastsensitivity Visual disorientation
Simultanagnosia Alexia Reverse-sizephenomena
Optic ataxia Visual crowding Mirror sign
Optic apraxia Prosopagnosia Illusions of movementof static objects
Visual field deficits Palinopsia AkinetopsiaComplex visualhallucinations Achromatopsia 180-degree upside
down room tilt illusionImpaired depthperception
Prolonged colourafter images
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
Acknowledgments
This work was supported by the NH&MRC Early CareerFellowship (Fred K. Chen) and Novartis Medical RetinaFellowship (Sue Ling Wan).
References
[1] D. F. Benson, R. J. Davis, and B. D. Snyder, “Posterior corticalatrophy,” Archives of Neurology, vol. 45, no. 7, pp. 789–793, 1988.
[2] S. J. Crutch, M. Lehmann, J. M. Schott, G. D. Rabinovici, M. N.Rossor, and N. C. Fox, “Posterior cortical atrophy,” The LancetNeurology, vol. 11, no. 2, pp. 170–178, 2012.
[3] S. C. Beh, T. C. Frohman, and E. M. Frohman, “Neuro-ophthalmic manifestations of cerebellar disease,” NeurologicClinics, vol. 32, no. 4, pp. 1009–1080, 2014.
[4] F.-X. Borruat, “Posterior cortical atrophy: review of the recentliterature,” Current Neurology and Neuroscience Reports, vol. 13,no. 12, article 406, 2013.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com