ane intubationpub.qxp 1/24/08 10:45 am page i new advances ... article_new... · new advances in...
TRANSCRIPT

Distinguished Panelists
Gavin F. Fine, MBBCh – Program Chair
Lynne G. Maxwell, MD, FAAP
Andreas C. Gerber, MD
New Advances in Pediatric Ventilation: Revolutionizing the Management of Pediatric Intubation with Cuffed Tubes
Sponsored by
Pediatric MicrocuffEndotracheal Tube2006
Kühn Tube with Stylet1899–1911
ANE IntubationPub.qxp 1/24/08 10:45 AM Page i

Foreword
It is my pleasure to present you with this special publication regarding thenew advances that have been made in pediatric ventilation.
Traditionally, it has been taught that only uncuffed endotracheal tubes (ETTs)should be used for intubation in children under 8 years of age. Recentadvances to the design of ETTs have fostered a debate on the use of uncuffedversus cuffed ETTs. This educational supplement features a history ofpediatric intubation, issues and “work arounds”to current practices, andclinical experiences using a new cuffed endotracheal tube.
Increased knowledge about the advances discussed in this supplement willhopefully help us to improve patient management in the future.
Gavin F. Fine, MBBChDepartment of AnesthesiologyCook Children’s Health CareFort Worth, Texas
ANE IntubationPub.qxp 1/24/08 10:45 AM Page ii

Table of ContentsEndotracheal Tube Use in Children: History as Pretext for Current Teaching . . . 1Lynne G. Maxwell, MD, FAAPDepartment of Anesthesiology and Critical Care MedicineChildren’s Hospital of PhiladelphiaPhiladelphia, Pennsylvania
Problems with Endotracheal Tubes, Cuffed vs. Uncuffed. . . . . . . . . . . . . . . . . . 6Gavin F. Fine, MBBChDepartment of AnesthesiologyCook Children’s Health CareFort Worth, Texas
Microcuff Pediatric Tube: Now Anesthesiologists Can Use Cuffed Endotracheal Tubes in Children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Andreas C. Gerber, MDDepartment of AnesthesiaUniversity Childrens’ Hospital Zürich, Switzerland
This Supplement is funded through an educational grant from Kimberly-Clark Health Care
© 2008 Kimberly-Clark Healthcare, Adair Greene McCann
ANE IntubationPub.qxp 1/24/08 10:45 AM Page iii
1
INTRODUCTION
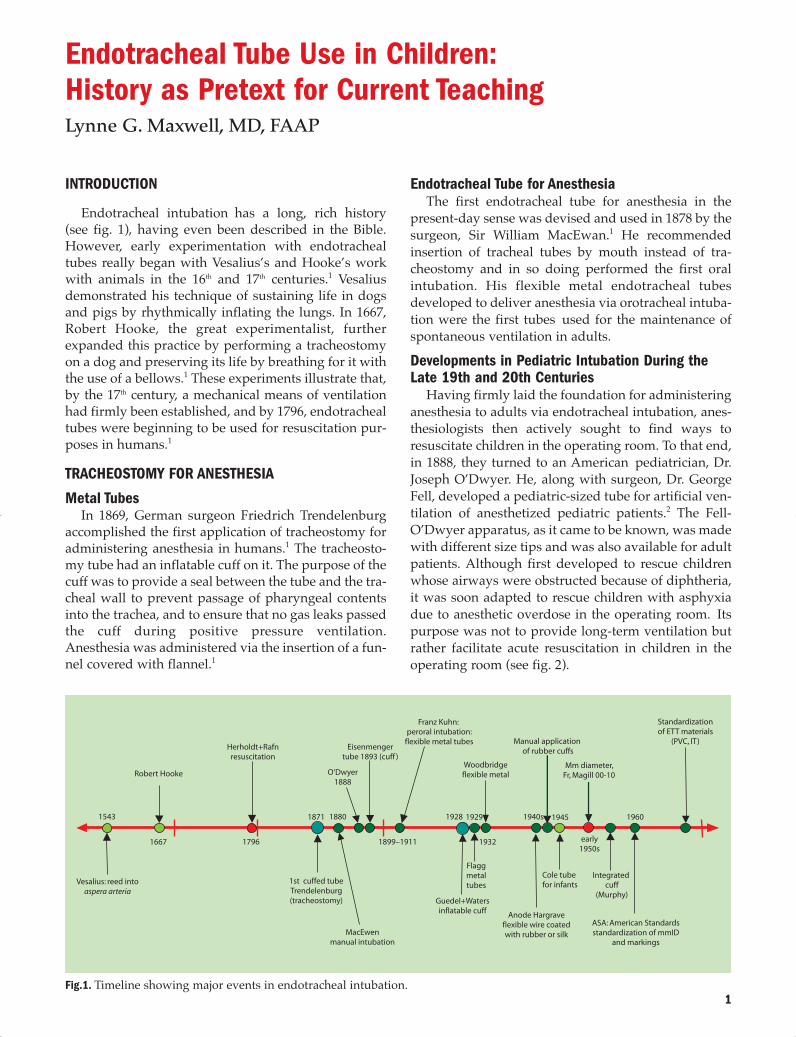
Endotracheal intubation has a long, rich history(see fig. 1), having even been described in the Bible.However, early experimentation with endotrachealtubes really began with Vesalius’s and Hooke’s workwith animals in the 16th and 17th centuries.1 Vesaliusdemonstrated his technique of sustaining life in dogsand pigs by rhythmically inflating the lungs. In 1667,Robert Hooke, the great experimentalist, furtherexpanded this practice by performing a tracheostomyon a dog and preserving its life by breathing for it withthe use of a bellows.1 These experiments illustrate that,by the 17th century, a mechanical means of ventilationhad firmly been established, and by 1796, endotrachealtubes were beginning to be used for resuscitation pur-poses in humans.1
TRACHEOSTOMY FOR ANESTHESIA
Metal TubesIn 1869, German surgeon Friedrich Trendelenburg
accomplished the first application of tracheostomy foradministering anesthesia in humans.1 The tracheosto-my tube had an inflatable cuff on it. The purpose of thecuff was to provide a seal between the tube and the tra-cheal wall to prevent passage of pharyngeal contentsinto the trachea, and to ensure that no gas leaks passedthe cuff during positive pressure ventilation.Anesthesia was administered via the insertion of a fun-nel covered with flannel.1
Endotracheal Tube for AnesthesiaThe first endotracheal tube for anesthesia in the
present-day sense was devised and used in 1878 by thesurgeon, Sir William MacEwan.1 He recommendedinsertion of tracheal tubes by mouth instead of tra-cheostomy and in so doing performed the first oralintubation. His flexible metal endotracheal tubesdeveloped to deliver anesthesia via orotracheal intuba-tion were the first tubes used for the maintenance ofspontaneous ventilation in adults. Developments in Pediatric Intubation During theLate 19th and 20th Centuries
Having firmly laid the foundation for administeringanesthesia to adults via endotracheal intubation, anes-thesiologists then actively sought to find ways toresuscitate children in the operating room. To that end,in 1888, they turned to an American pediatrician, Dr.Joseph O’Dwyer. He, along with surgeon, Dr. GeorgeFell, developed a pediatric-sized tube for artificial ven-tilation of anesthetized pediatric patients.2 The Fell-O’Dwyer apparatus, as it came to be known, was madewith different size tips and was also available for adultpatients. Although first developed to rescue childrenwhose airways were obstructed because of diphtheria,it was soon adapted to rescue children with asphyxiadue to anesthetic overdose in the operating room. Itspurpose was not to provide long-term ventilation butrather facilitate acute resuscitation in children in theoperating room (see fig. 2).
Vesalius: reed intoaspera arteria
1st cuffed tubeTrendelenburg(tracheostomy)
MacEwenmanual intubation
Guedel+Watersinflatable cuff
Flaggmetaltubes
Anode Hargraveflexible wire coatedwith rubber or silk
Cole tube for infants
Integratedcuff
(Murphy)
ASA: American Standardsstandardization of mmID
and markings
Woodbridgeflexible metal
Manual applicationof rubber cuffs
Mm diameter,Fr, Magill 00-10
Standardizationof ETT materials
(PVC, IT)
Robert Hooke
Herholdt+Rafnresuscitation
Eisenmengertube 1893 (cuff )
O’Dwyer1888
Franz Kuhn: peroral intubation:
flexible metal tubes
1543
1667
1871 1880
1899–1911
1928 1929
1932
1940s 1945
early1950s
1960
1796
Fig.1. Timeline showing major events in endotracheal intubation.
Endotracheal Tube Use in Children: History as Pretext for Current TeachingLynne G. Maxwell, MD, FAAP
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 1

2
Dr. Eisenmenger’s endotracheal tube soon followed.His device, developed in 1893, consisted of a metaltube that had a cuff applied to it and had all the fea-tures of a modern cuffed endotracheal tube.1 It had apilot balloon as well as an additional balloon to inflatethe cuff to seal the lower airways against air leakageand aspiration of secretions (see fig. 3).
Early in the 20th century, Franz Kühn, a German sur-geon, modified endotracheal tubes for easier intuba-tion.1 His patient-oriented studies led to vast improve-ments in patient safety.1 Kühn’s device was a flexiblemetal tube used to keep the respiratory tract clear dur-ing narcosis and featured 3 important benefits. Thefirst was an oral airway to prevent the patient from bit-ing the tube, the second was a small attachment on theside of the tube that helped hold the tube to thepatient’s face, and the third was a stylet to help thetube maintain its rigidity during placement.1 Kühn’stubes were inserted via manual intubation (see fig. 4.)Rubber Tubes
Rubber tubes were first developed in the 1940s and1950s. The Cole tracheal tube, developed in 1945, wasinitially designed for emergency use in pediatric anes-thesia (see fig. 5).1 The Cole tube was made of rubberand had no connectors on it. This form of endotrachealtube had a wide proximal portion with a slopingshoulder leading to a narrow distal tip to prevent thetube from being advanced too far in the trachea.1 Otheruncuffed endotracheal tubes at the time were of uni-form diameter along the entire axis.1 The tube wasthought to be an improvement over the uniform diam-eter tubes, due to lower resistance to airflow in thewider lumen. However, there were several adverseoutcomes that directly resulted from the tube’s shoul-der, such as impingement on the vocal cords whichcould cause laryngeal dilation and postoperative
Fig.2. The Fell-O’Dwyer apparatus for artificial ventilation of anesthetized patients. Adapted from Brandt L. IllustrierteGeschichte der Anästhesie. Wissenschaftliche Verlagsgesellschaft mbH. 1997.
Fig.3. The Eisenmenger tube with pilot balloons. Adaptedfrom Gillespie NA. Endotracheal Anaesthesia, Third Edition.University of Wisconsin Press. 1963.
Fig.4. Kühn tube with stylet. Adapted from Brandt L.Illustrierte Geschichte der Anästhesie. WissenschaftlicheVerlagsgesellschaft mbH. 1997.
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 2

3
croup.3 Interestingly, the modern Cole tube with thesame configuration is still popular for intubation ofveterinary patients and still has the narrowing.
Connectors Come Into PracticeIn the 1950s, a wide range of uncuffed and cuffed
tubes was available, but all lacked metal connectorsthat required attachments.1 Connectors, either straightor curved, had to be attached, depending on theirintended use. There were two types of connectors, theAyres Y-piece and the Ayres T-piece, which used con-nectors with rubber tubes. They were connected to asource of oxygen flow and allowed expiratory gas toescape. There were numerous problems with the con-nectors, however, such as frequent kinking at the jointbetween the connector and the tube, resulting inobstruction of the tube. As a solution, various deviceswere invented to join the connector to the tube withoutnarrowing the orifice of the tube.
By the 1940s and 1950s, anesthesiologists finallybegan to realize the advantages of cuffed tubes andattempted to add cuffs to existing tubes by hand.Manual devices with large clamps and other acces-sories that were inserted into the cuffs to stretch themwere developed. See figure 6 for the Waters cuff appa-ratus, an extremely complicated example of thedevices of this period.1
The Murphy TubeTo address the difficulty of manually adding cuffs to
existing tubes, the Murphy tube was developed in the1940s by FJ Murphy.1 His tube came complete with itsown manufactured cuff, a pilot balloon and the infa-mous Murphy eye. The eye was a side vent betweenthe cuff and the tip of the endotracheal tube to preventtube obstruction if the beveled end of the tube becameblocked by mucus or sealed by contact with the tra-cheal wall.1 Often, the bevel of the tube was in line withthe curve of the tube and could abut the tracheal wall.The eye on the tube surface opposite the end holeallowed ventilation to occur despite occlusion of theend of the tube. It was also believed that if there wasinadvertent mainstem intubation, the Murphy eyewould allow ventilation of the other side, or in situa-tions of deliberate intubation of the right mainstembronchus, allow ventilation of the right upper lobe.1
Manufactured cuffed rubber tubes were developedin the 1950s and are still in existence.1 They are current-ly used primarily in laser surgery after wrapping withmetal foil or other non-flammable materials, althoughtheir use has declined in the last decade because ofincreasing concern about the prevalence of latex aller-gy.4,5 These very small tubes came with exceptionallylong cuffs, which made it impossible for them to beused in infants, in whom it was unlikely to get theentire cuff below the vocal cords without having amainstem intubation.Plastic Tubes
In 1962, Dr. Brandstater wrote the first description ofthe use of plastic polyvinyl chloride (PVC) endotra-cheal tubes in the routine intubation of small children.6Dr. Brandstater felt there needed to be a satisfactoryalternative to the hazards of tracheostomy, which wasthe standard of care of patients of that time, but whichwas also unfortunately associated with significantmorbidity and mortality in small children. These plas-tic tubes were developed in 1959 through the work ofDavid Sheridan, an engineer, and their introductionhelped advance pediatric anesthesiology and criticalcare.7 This technique allowed prolonged mechanicalventilation in children, since the tubes softened at bodytemperature and were much less likely to cause sub-glottic stenosis than their metal or rubber counterparts.
With the development of so many tubes, standardi-zation was imperative. As such, guidelines for endo-tracheal tube selection in children were published bySmith in 1959 in Anesthesia for Infants and Children.3The guidelines recommended using plain Magilltubes, which lacked the Murphy eye, for children up to6 years of age. An uncuffed tube was thought to bemore suitable for children ages 8 and younger, becausethe narrowest part of the airway of children of that agewas thought to be the subglottic area at the level of thecricoid ring.
Prior to standardization, there were major discrep-ancies in tube measurements with tube dimensionsbeing expressed in either French sizes or inner diame-ter in millimeters. Finally, in 1960, the AmericanSociety of Anesthesiologists (ASA) advocated thatthere should be standards for endotracheal tube sizes,making millimeters the universal unit for internal
Fig.5. The Cole tube. Theoretically, ithad a lower resistance to airflow thanuniform diameter tubes. Adaptedfrom Gillespie NA. EndotrachealAnaesthesia, Third Edition. Universityof Wisconsin Press. 1963.
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 3
4
diameter. This was codified with the development ofthe American Standards Specifications for AnestheticEquipment: Endotracheal Tubes in collaboration withthe American Standards Association.1 Further ASAguidelines stipulated that the tubes should have grad-uation markings placed from the tip to indicate thedepth of intubation, radiopaque lines throughout thelength of the tube to allow radiographic assessment ofthe exact location of the tube, and a standard 15-mil-limeter connector added to ensure compatibility withcircuit connectors.1
ADULT LARYNX VS CHILD LARYNXAnatomical dissection of cadavers of children, initi-
ated with Bayeux in 1897 and subsequently spread byothers in the 1950s and 1960s, concluded that the adultlarynx resembles a cylinder with equal dimensions atthe cords and the cricoid.8 They found that childrenunder the age of 8, however, had a cone-shaped larynxwith the narrowest portion at the cricoid ring. This dif-fers from adults, in whom the vocal cords form the nar-
rowest portion of the larynx and trachea, and are thelimiting dimension for determination of appropriatetube size.9
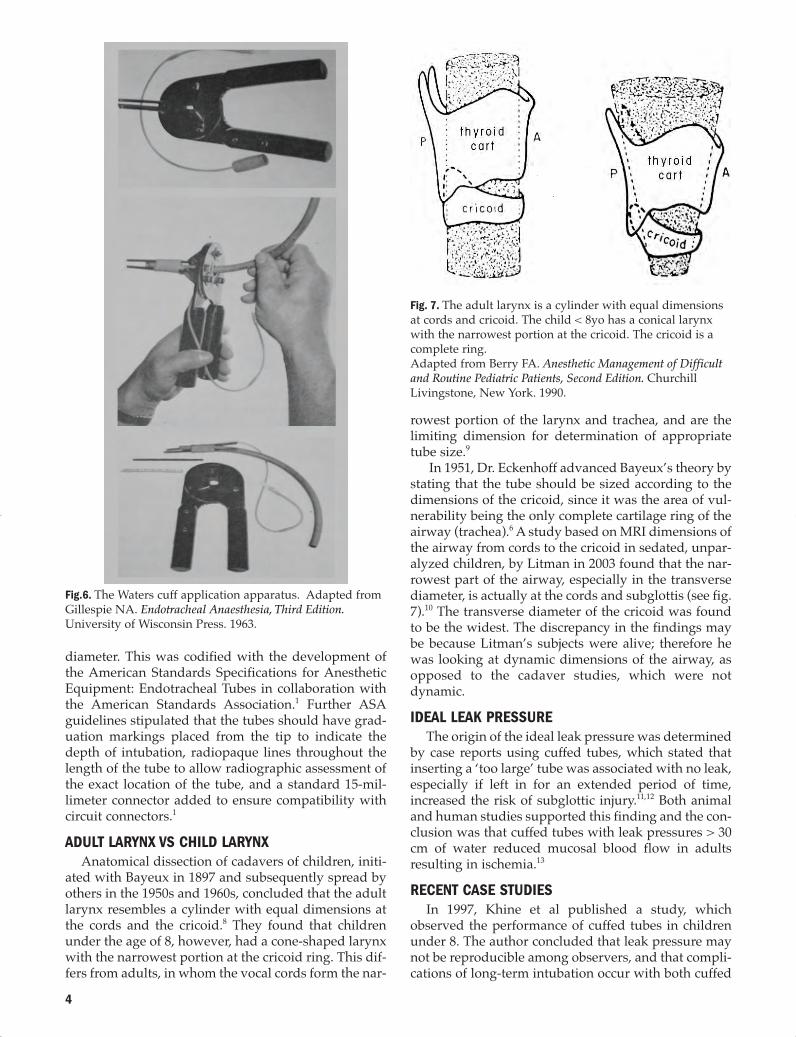
In 1951, Dr. Eckenhoff advanced Bayeux’s theory bystating that the tube should be sized according to thedimensions of the cricoid, since it was the area of vul-nerability being the only complete cartilage ring of theairway (trachea).6 A study based on MRI dimensions ofthe airway from cords to the cricoid in sedated, unpar-alyzed children, by Litman in 2003 found that the nar-rowest part of the airway, especially in the transversediameter, is actually at the cords and subglottis (see fig.7).10 The transverse diameter of the cricoid was foundto be the widest. The discrepancy in the findings maybe because Litman’s subjects were alive; therefore hewas looking at dynamic dimensions of the airway, asopposed to the cadaver studies, which were notdynamic.IDEAL LEAK PRESSURE
The origin of the ideal leak pressure was determinedby case reports using cuffed tubes, which stated thatinserting a ‘too large’ tube was associated with no leak,especially if left in for an extended period of time,increased the risk of subglottic injury.11,12 Both animaland human studies supported this finding and the con-clusion was that cuffed tubes with leak pressures > 30cm of water reduced mucosal blood flow in adultsresulting in ischemia.13
RECENT CASE STUDIESIn 1997, Khine et al published a study, which
observed the performance of cuffed tubes in childrenunder 8. The author concluded that leak pressure maynot be reproducible among observers, and that compli-cations of long-term intubation occur with both cuffed
Fig.6. The Waters cuff application apparatus. Adapted fromGillespie NA. Endotracheal Anaesthesia, Third Edition.University of Wisconsin Press. 1963.
Fig. 7. The adult larynx is a cylinder with equal dimensionsat cords and cricoid. The child < 8yo has a conical larynxwith the narrowest portion at the cricoid. The cricoid is acomplete ring.Adapted from Berry FA. Anesthetic Management of Difficultand Routine Pediatric Patients, Second Edition. ChurchillLivingstone, New York. 1990.
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 4

5
and uncuffed tubes.14 Koka found that postintubationcroup in children was associated with higher leak pres-sure.15 A recent study found that leak pressure greaterthan 25 cm of water was associated with increased inci-dence of postoperative stridor.16 These, as well as earli-er studies identifying complications of intubation inchildren were all done with uncuffed tubes, or withrubber tubes. On the contrary, recent studies and caseseries have yet to find increased adverse events withmodern cuffed tubes.11
References 1. Gillespie NA. Endotracheal Anaesthesia. 3rd ed.
Madison: Univ. of Wisconsin Press;1963.2. Brandt L. The history of endotracheal anesthesia, with
special regard to the development of the endotrachealtube. Anaesthetist. 1986;35:523–530.
3. Smith’s Anesthesia for Infants and Children. 1st ed. 1959.4. Sosis MB, Braverman B. Advantage of rubber over plas-
tic endotracheal tubes for rapid extubation in a laser fire.J Clin Laser Med Surg. 1996;14:93–95.
5. Kashima ML, Tunkel DE, Cummings CW. Latex allergy:an update for the otolaryngologist. Arch OtolaryngolHead Neck Surg. 2001;127:442–446.
6. Brandstater B. Prolonged intubation: an alternative totracheostomy in infants. Proceedings of the FirstEuropean Congress of Anesthesiology. Vienna; 1962.Paper 106.
7. Berry FA, ed. Anesthetic Management of Difficult andRoutine Pediatric Patients. 2nd ed. New York, NY;Churchill Livingstone:1990.
8. Bayeux. Tubage de larynx dans le croup. Presse Med.1897;20:1.
9. Eckenhoff JE. Some anatomic considerations of the infantlarynx influencing endotracheal anesthesia.Anesthesiology. 1951;12:401–410.
10.Litman RS, Weissend EE, Shibata D, Westesson PL.Developmental changes of laryngeal dimensions inunparalyzed, sedated children. Anesthesiology.2003;98:41–45.
11. Hedden M, Ersoz CJ, Donnelly WH, Safar P.Laryngotracheal damage after prolonged use of orotra-cheal tubes in adults. JAMA. 1969;207:703–708.
12.Bishop MJ, Weymuller EA, Fink BR. Laryngeal effects ofprolonged intubation. Anesth Analg. 1984;63:335–342.
13.Seegobin RD, van Hasselt GL. Endotracheal cuff pressureand tracheal mucosal blood flow: endoscopic study ofeffects of four large volume cuffs. Br Med J (Clin Res Ed).1984;288:965–968.
14.Khine HH, Corddry DH, Kettrick RG, et al. Comparisonof cuffed and uncuffed endotracheal tubes in young chil-dren during general anesthesia. Anesthesiology.1997;86:627–631.
15.Koka BV, Jeon IS, Andre JM, Smith RM. Postintubationcroup in children. Anesth Analg. 1977;56:501–505.
16.Suominen P, Taivainen T, Tuominen N, et al. Optimallyfitted tracheal tubes decrease the probability of postextu-bation adverse events in children undergoing generalanesthesia. Pediatr Anesth. 2006;16:641–647.
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 5

6
Prior to the 1960s, most children who required pro-longed intubation were given tracheotomies, whichwas associated with significant morbidity and mortal-ity. However, prolonged endotracheal intubation wasnot without its own risks, and the first reports of ETTblockage and subglottic stenosis started to appear inthe literature.1,2 Since 1966 it has been known thatthere are a number of factors to consider when trachealintubation is needed in children. The first is the size ofthe tube. According to Stocks’ important article pub-lished in the British Medical Journal in 1966, “Selectionof an appropriate size of tracheal tube is fundamentalto the success of prolonged nasal intubation in chil-dren.”3 This can not be overstated. Stocks knew that anendotracheal tube (ETT) that was too small wouldmake intermittent positive pressure ventilation diffi-cult because of gas leaks through the larynx, and onethat was too large could possibly cause subglotticstenosis.
There are many indications for tracheal intubationsuch as airway protection, maintenance of airwaypatency, pulmonary toilet, application of positive-pres-sure ventilation, maintenance of adequate oxygena-tion, predictable FiO2 and positive end-expiratorypressure.4 However, endotracheal intubation is notwithout its risks.
RISKS OF INTUBATIONAs with many things in medicine, there are risks
associated with endotracheal intubation: Dentalinjuries, which vary between 1 in 150 to 1 in 1000 cases,are the most common; cervical or neck problems;laryngotracheal trauma; corneal abrasion; uvular dam-age, vocal cord paralysis; or esophageal or bronchialintubation. The most serious complication is subglotticinjury, which takes the form of stenosis or dilatation,and is manifested through stridor. Studies have shownthat between 2–18% of patients will exhibit signs ofstridor post-anesthesia.5,6
SIZE OF THE TUBEIn order to prevent injury and to obtain appropriate
ventilation in an intubated child, a correctly sized ETT isneeded. Multiple age-based formulas have been used topredict the appropriate size of the uncuffed ETT in thepediatric population.7-9 For children less than 6 years ofage, Slater et al, recommended using the sum of 3.75 +age divided by 4; and for children 6 and up, the sum of4.5 + age divided by 4.7,8 These formulae have sincebeen simplified into: 4 + age divided by 4. It has beensuggested that for a tighter-fitting tube the base num-ber should be 4.5 + age divided by 4 (see fig. 1).FORMULAS FOR ENDOTRACHEAL TUBE SELECTION
Formulas are not perfect. One problem is that ETTshave different external diameters. Even a fraction of amillimeter variation in external diameter size may beconsequential in smaller children with smaller diame-ter airways. A study conducted by King et al in 1993concluded that in about 97.5% of patients, the age-based formula accurately predicted the correctly sizedETT. However, the study also determined that the for-mulas do not take into account the natural variationsbetween patients and tend to be very inaccurate if theage of the patient is unknown.9
LEAK AROUND TUBEThe “appropriate” size of ETT has been defined as
that size of ETT which allowed an audible air leakaround the ETT occurring between 15 and 25 cm H2Opressure. In a large retrospective study in 2953 pedi-atric patients over a 4 year period, Black et al foundthat a slight leak around the tube with the applicationof 25 cm of pressure to the airway resulted in a lessthan 1% incidence of stridor requiring re-intubation.10
We now know that a leak at a pressure greater than 30cm of water probably predisposes patients to subglot-tic injury, especially in prolonged intubation. A pres-sure of less than 15 cm H2O may result in inadequateventilation in patients with poor pulmonary compli-ance from intrinsic lung disease or to changes in chestwall or abdominal compliance.
Problems with Endotracheal Tubes,Cuffed vs. UncuffedGavin F. Fine, MBBCh
Formulas for Endotracheal Tube Selection
Under 6 years of age
3.75 + age / 4
Over 6 years of age OR for atighter-fitting tube
4.5 + age / 4
Simplified Formula
4 + age / 4
Fig.1. Formulas for Endotracheal Tube Selection
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 6
7
RELIABILITY OF LEAK TESTIn any case, the leak test is unreliable. In 1993,
Schwartz et al conducted a study of 242 patients usingstandard conditions for the leak test, defined as 5 litersof fresh gas flow in neutral head position and neuro-muscular blockade. Thirty patients were excludedbecause they did not have leaks at a pressure greaterthan 50 cm of water. Among the results, a 38% variancebetween observers was seen, especially at levels above30 cm H2O.11
In 2000, Pettignano et al repeated the study to deter-mine reproducibility of the leak test.12 Thirteen patientswere enrolled, personnel were trained for at least anhour, and standard conditions for the leak test wereused. The study concluded that neither interobservernor intraobserver variability was statistically signifi-cant when a standardized method was used to deter-mine the leak.12 However, because of the small popula-tion studied, the results seem to contradict other stud-ies showing significant intraobserver variance in theleak test.CHANGES IN ENDOTRACHEAL TUBE LEAK
In addition to variance between observers, the leakis not a constant and changes depending on patientpositioning and degree of paralysis or sedation.Finholt’s study conducted in 1985 with 80 patientsbetween 2 weeks and 11 years of age, intubated withuncuffed ETTs, found that a patient whose head was ina neutral position had a smaller leak than if their headwas turned sideways. He also noted that the degree ofparalysis or sedation significantly affected the leak.However, the leak was not affected by fresh gas flow orendotracheal tube depth.5
IMPORTANCE OF AIR LEAKIn 2006, Suominen et al, conducted a study in 234
pediatric patients ranging in age from newborn to 9years, requiring tracheal intubation for elective oremergency surgery. The tube size was calculated usinga modified Cole formula (age/4 + 4.5). An audible airleak at 25 cm H2O or below was associated with a sig-nificantly lower incidence of stridor (9%) comparedwith an absent air leak at the same pressure (19%). Thisstudy concluded that 25 cm H2O is the thresholdwhere complications begin to arise.13 A separate studyby Mhanna et al, however, concluded that the air leaktest was age dependent as a predictor of stridor in chil-dren. The authors found that the test has a low sensi-tivity when used in children younger than 7, whereasin children older than 7, the test may predict postextu-bation stridor.14
COMPLICATIONS OF A LARGE LEAKMultiple complications may arise if there is a large
leak. Inaccurate measurements of ventilation function,calorimetry and indirect cardiac output are just a few.Limiting patients’ and healthcare workers’ exposure toenvironmental pollution is a consideration. Lower
fresh gas flow results in less agent being used, which inturn decreases the cost of drug used for the anesthetic.It is known that the leak changes with regards to posi-tion, sedation and use of neuromuscular blockade andthis may affect the ability to ventilate.4,7
CUFFED OR UNCUFFED ENDOTRACHEAL TUBESThe next logical question is whether the complica-
tions can be altered by use of a cuff or uncuffed tra-cheal tube. It has been widely accepted that uncuffedendotracheal tubes be used for the intubation of chil-dren younger than 8 to 10 years of age.4 The primaryreasoning being that uncuffed endotracheal tubesallow for use of a tube of larger internal diameter,which minimizes resistance to airflow and the work ofbreathing in the spontaneous-breathing patient. Thisadvantage is not as valid for maintenance of anesthesiain the 21st century, when very few patients are allowedto breathe spontaneously under anesthesia for pro-longed periods of time. In the intensive care, patientsoften do breathe spontaneously, but with modern ven-tilators and modern ventilation techniques, the workof breathing from smaller diameter ETTs can regularlybe overcome. As far back as 1977, a study by Battersbyet al concluded that there was no subglottic stenosisfrom proper use of uncuffed endotracheal tubes forlong term intubation.15 Black et al confirmed this think-ing in a 1990 study published in the British Journal ofAnaesthesia.10
Black et al’s study included 2953 pediatric intensivecare admissions over a 4-year period. The overall com-plication rate was 8%. Endotracheal tube blockageoccurred in about 2.6 % of the patients. Of note, 80% ofthese occurred in patients who had an internal diame-ter less than 3.5. A study by Newth et al in 2004showed that the incidence of ETT blockage is greater inpatients that go to the operating room when the inter-nal diameter of the tube is less than 4 mm than in thosethat stay in a unit with proper humidification of gases.Stridor occurred in less than 1% of the patients, with 14having had preexisting laryngeal pathology (leak testless than 25 cm H20).16
Deakers et al studied 243 patients in a pediatricintensive care unit during a 7-month period to com-pare cuffed and uncuffed endotracheal tube utilizationand outcome.17 Patients who were less than 1 year ofage, or who had tubes in place for less than 72 hourswere more likely to have had insertion of an uncuffedendotracheal tube. Patients who were more than 5years of age or for whom long term intubation wasexpected, were more likely to have an insertion of acuffed ETT. Inflation pressures were kept to less than25 cm of water. The overall incidence of postextubationstridor was 14.9%, with no significant differencebetween the 2 ETT groups even after controlling forpatient age, duration of intubation, trauma, leakaround ETT before extubation, and pediatric risk ofmortality score.
Newth et al studied 597 patients (210, cuffed; 387
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 7

8
uncuffed) in the first 5 years of life using an age-basedformula. They found no difference in clinically detect-ed subglottic edema between the 2 groups. The authorseven went as far to state that cuffed tubes should be thefirst-line choice in critically ill patients. In the anesthe-sia literature, there are no reports of subglottic stenosisfrom short-term intubation irrespective of tube size orcuff pressure, and the incidence of stridor seems to besimilar among cuff and uncuffed tubes.16
ADVANTAGES OF CUFFED TUBESThere have been several studies done to determine
the need for changing from an uncuffed endotrachealtube to a cuffed one in the pediatric population. Moststudies seem to conclude that there are more advan-tages associated with the use of cuffed tubes asopposed to uncuffed ones. In a 488-patient study con-ducted by Khine et al, they determined that cuffedtubes provided both an environmental benefit—decreasing operating room contamination, as well asan economic one—requiring lower fresh gas flow overuncuffed endotracheal tubes in children between theages of 2 weeks to 8 years.18 In addition, Murat’s studysupports this significant drop in operating room pollu-tion with the simple change to cuffed endotrachealtubes.19
Fine et al studied 20 patients in 3 age groups andfound there was less chance at reintubation and laryn-goscopy with cuffed tubes. By decreasing the numberof laryngoscopies, one directly decreases the chance ofcausing trauma to the upper airway. It was also con-cluded that there was less incidence of hypoventilationif 200 mL per minute per kilo of fresh gas flow wasused.20
Silver et al conducted a multicenter study in burnunits and determined that in these large pediatric burncenters there was a preference for cuffed endotrachealtubes. With significant burns, more patients were like-ly to be changed from uncuffed to cuffed ETT especial-ly if there was lung injury.21
In an aspiration study, Browning and Graves com-pared cuffed to uncuffed tubes in 22 children (9 cuffed;13 uncuffed). Their study showed that 11% of cuffedpatients exhibited dye positive tracheal aspirates notaffected by PEEP, compared to 70% of uncuffedpatients.22 Goitein et al with 50 infants using uncuffedendotracheal tubes found an 8% incidence of clinicallysignificant aspirations.23
There are several case reports of retrograde leak ofventilating gases, especially oxygen, during electro-cautery in tonsillectomies where the polyvinyl tubeshave caught fire. All of these case reports were inuncuffed endotracheal tubes.24-26
In conclusion, the literature suggests that the bene-fits of cuffed tubes include: decreased attempts at intu-bation; less OR contamination anesthetic gases; lessICU contamination (from droplet spread ofpathogens); less chance of hypoventilation; betterpatient ventilatory management with more accurate
end tidal CO2 monitoring especially in patients withchanges in pulmonary compliance; decreased risk ofaspiration and decreased incidence of airway fires (seefig. 2). These factors speak for themselves as to theadvantages of cuffed over uncuffed ETTs.ENDOTRACHEAL DEPTH PLACEMENT
Endotracheal tube length, like size, is dependent onthe age and size of the individual child. There are for-mulas that confirm successful placement, but mostlythis applies to children older than 2 years of age.Auscultation is always a method for correct endotra-cheal depth placement. However, in a study conductedby Verghese et al, where they did 153 intubations in thecardiac catheterization lab, auscultation did not detectproper placement in 11.8% of the patients who had aright mainstem intubation. In 19% of the patients, theywere within one centimeter of the carina. All of thesepatients were less than 5 years of age, and they attrib-uted this to the Murphy’s eye, which reduces the relia-bility of chest auscultation in detecting endobronchialintubation.27
To establish correct depth, the only 100% certainmethod is via radiologic confirmation, but that wouldexpose children to unnecessary radiation. Similarly,Hsieh et al showed that the Murphy’s eye could causeconfusion during ultrasounds of the diaphragm.28
Palpitation of the endotracheal tip above the sternalnotch was advocated in 1975 by Bednarek et al,29 but Ifind that most children have thick necks, making pal-pitation difficult. WORK OF BREATHING
As anesthesiologists, we very rarely let childrenbreathe under anesthesia spontaneously for prolongedperiods of time. In fact, a study by Bock et al in Chest,showed that new mechanical ventilators are so goodthey can overcome the work of resistance irrespectiveof endotracheal tube internal diameter.30
THE FUTURE OF ENDOTRACHEAL TUBESThere are exciting product developments currently
being studied that will facilitate endotracheal intuba-tion. These include an ultrathin-walled endotracheal
Fig.2. Advantages of cuffed endotracheal tubes
Advantages of Cuffed Tubes• Decreased attempts at intubation• Less OR and ICU contamination• Less risk of hypoventilation• Better patient management and changes in
pulmonary compliance• Decreased incidence of aspiration• Less risk of airway fires• More accurate ETCO2 monitoring
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 8
9
tube as described by Okhuysen, a no-pressure sealdesign used by Reali-Forster, and the thinner, moredistensible cuffed tube, Microcuff, which was specifi-cally designed for the pediatric anatomy.31,32 This tubeemploys a short cylindrical microthin polyurethanecuff that helps secure placement in the lower trachea(not the pressure-sensitive larynx), depth markings toensure a cuff-free subglottic zone, and four pre-glotticplacement markings. Having been developed andthoroughly studied by Dullenkopf, Gerber, and Weiss,this tube may very well represent a new standard forpediatric airway management.References1. McDonald IH, Stocks JG. Prolonged endotracheal intu-
bation: a review of its development in a paediatric hospi-tal. Br J Anaesth. 1965;37:161–173.
2. Allen TH, Steven IM. Prolonged endotracheal intubationin infants and children. Br J Anaesth. 1965;37:566–573.
3. Stocks JG. Prolonged intubation and subglottic stenosis.BMJ. 1996;2:1199–1200.
4. Fine GF, Borland LM. The future of the cuffed endotra-cheal tube. Paediatr Anaesth. 2004;14:38–42.
5. Finholt DA, Henry DB, Raphaely RC. Factors affectingleak around tracheal tubes in children. Can Aneasth SocJ. 1985;32:326–329.
6. Wiel E, Vilette B, Darras JA, Scherpereel P, Leclerc F.Laryngotracheal stenosis in children after intubation.Report of five cases. Paediatr Anaesth. 1997;7:415-419.
7. Slater HM, Sheridan CA, Ferguson RH. Endotrachealtube sizes for infants and children. Anesthesiology.1955;16:950–952.
8. Cole F. Pediatric formulas for the anaesthesiologists. AmJ Dis Child. 1957;94: 672–673.
9. King BR, Baker MD, Braitman LE, Seidl-Friedman J,Schreiner MS. Endotracheal tube selection in children: acomparison of four methods. Ann Emerg Med.1993;22:530–534.
10.Black AE, Hatch DJ, Nauth-Misir N. Complications ofnasotracheal intubation in neonates, infants and children:a review of 4 years’ experience in a children’s hospital.Br J Anaesth. 1990;65:461–467.
11. Schwartz RE, Stayer SA, Pasquariello CA. Tracheal tubeleak test-is there inter-observer agreement? Can JAnaesth. 1993;40:1049–1052.
12.Pettignano R, Holloway SE, Hyman D, Labuz M. Is theleak test reproducible? South Med J. 2000;93:683–685.
13.Suominen P, Taivainen T, Tuominen N et al. Optimallyfitted endotracheal tubes decrease the probability of pos-textubation adverse events in children undergoing gen-eral anesthesia. Pediatr Anesth. 2006;16:641–647.
14.Mhanna MJ, Zamel YB, Tichy CM, Super DM. The airleak test around the endotracheal tube, as a predictor ofpostextubation stridor, is age dependent in children. CritCare Med. 2002;30:2639–2643.
15.Battersby EF, Hatch DJ, Towey RM. The effects of pro-longed naso-endotracheal intubation in children. A studyin infants and young children after cardiopulmonarybypass. Anaesthesia. 1977;32:154–157.
16.Newth CJ, Rachman B, Patel N, Hammer J. The use ofcuffed versus uncuffed endotracheal tubes in pediatricintensive care. J Pediatr. 2004;144:333–337.
17.Deakers TW, Reynolds G, Stretton M, Newth CJ. Cuffedendotracheal tubes in pediatric intensive care. J Pediatr.1994;125:57–62.
18.Khine HH, Corddry DH, Kettrick RG et al. Comparisonof cuffed and uncuffed endotracheal tubes in young chil-dren during general anesthesia. Anesthesiology.1997;86:627–631.
19.Murat I. Cuffed tubes in children: a 3-year experience ina single institution. Paediatr Anaesth. 2001;11:748–749.
20.Fine GF, Fertal K, Motoyama EK. The effectiveness ofcontrolled ventilation using cuffed versus uncuffed ETTin infants. Anesthesiology. 2000;A-1251.
21.Silver GM, Freiburg C, Halerz M, Tojong J, Supple K,Gamelli RL. A survey of airway and ventilator manage-ment strategies in north American pediatric burn units. JBurn Care Rehabil. 2004;25:435-440.
22.Browning DH, Graves SA. Incidence of aspiration withendotracheal tubes in children. J Pediatr.1983;102:582–584.
23.Goitein KJ, Rein AJ, Gornstein A. Incidence of aspirationin endotracheally intubated infants and children. CritCare Med. 1984;12:19–21.
24.Kaddoum RN, Chidiac EJ, Zestos MM, Ahnmed Z.Electrocautery-induced fire during adenotonsillectomy:report of two cases. J Clin Anesth. 2006;18:129-131.
25.Keller C, Elliott W, Hubbell RN. Endotracheal tube safetyduring electrodissection tonsillectomy. Arch OtolaryngolHead Neck Surg. 1992;118:643-645.
26.Aly A, McIlwain M, Duncavage JA. Electrosurgery-induced endotracheal tube ignition during tracheotomy.Ann Otol Rhinol Laryngol. 1991;100:31-33.
27.Verghese ST, Raafat SH, Slack MC, Cross RR, Patel KM.Auscultation of bilateral breath sounds does not rule outendobronchial intubation in children. Anesth Analg.2004;99:56–58.
28.Hsieh KS, Lee CL, Lin CC et al. Secondary confirmationof endotracheal tube position by ultrasound image. CritCare Med. 2004;32:S374–S377.
29.Bednarek FJ, Kuhns LR. Endotracheal tube placement ininfants determined by suprasternal palpation: a newtechnique. Pediatrics. 1975;56:224–229.
30.Bock KR, Silver P, Rom M, Sagy M. Reduction in tracheallumen due to endotracheal intubation and its calculatedclinical significance. Chest. 2000;118:468–472.
31.Okhuysen RS, Bristow F, Burkhead S, Kolobow T, LallyKP. Evaluation of a new thin-walled endotracheal tubefor use in children. Chest. 1996;109:1335–1338.
32.Reali-Forster C, Kolobow T, Giacomini M, Hayashi T,Horiba K, Ferrans VJ. New ultrathin-walled endotrachealtube with a novel laryngeal seal design. Long-term eval-uation in sheep. Anesthesiology. 1996;84:162–172.
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 9
10
Uncuffed endotracheal tubes have been the norm inthe pediatric population for 50 years and are still wide-ly used today.1 As a result pediatric anesthesiologistsare accustomed to this means of intubating and venti-lating children.2 Switching to cuffed endotrachealtubes may not seem like a necessary choice consideringthe success and widespread use of uncuffed ones,however, as this article will point out, there’s much tobe gained from using cuffed endotracheal tubes. VITAL LINK
The endotracheal tube is the link between our mostexpensive and our most sophisticated object, our anes-thesia machine, and our most delicate and most precioussubject, our pediatric patients. This vital link shouldfulfill 2 requirements: 1) it should be precise, consistentand reliable, and 2) it should be leak proof and neverdamage the airway.1 The leak proof aspect of the endo-tracheal tube is necessary in order to efficientlyexchange gases and vapors, to transmit precise pres-sures, to monitor respiratory and anesthetic gases, andto protect against the aspiration of fluids.2 Whileachieving these things, the tube must simultaneouslynot obstruct mucosal perfusion or cause direct mechani-cal trauma to the airway. The traditional method ofobtaining such acceptable leak tightness in uncuffedendotracheal tubes is through cricoidal sealing.1
CRICOIDAL SEALING WITH UNCUFFED TUBESThe key to securing acceptable sealing with
uncuffed tubes is by matching the diameter of theendotracheal tube to the diameter of the cricoid ring.1Getting this right, of course, is the challenge. If a tubeis too small, unreliable ventilation, unreliable monitor-ing, and risk of aspiration are high. If a tube is toolarge, mucosal compression and mechanical traumawill occur.1 Having a very small, mandatory leak thatdoes not interfere with precise ventilation may, to acertain extent, guarantee that the tube is not too big. Asis evident, selection of the right tube size is paramount,but it is not an easy task in cricoidal sealing. Despiteformulas that help calculate the size of uncuffed endo-tracheal tubes, up to 30% of the tubes have to beexchanged due to incorrect size.3-5
TRACHEAL SEALING WITH CUFFED TUBESThe lack of success in calculating the size of the
uncuffed endotracheal tube is directly attributed toanatomy. A study in 2003, by Ronald Litman, based on
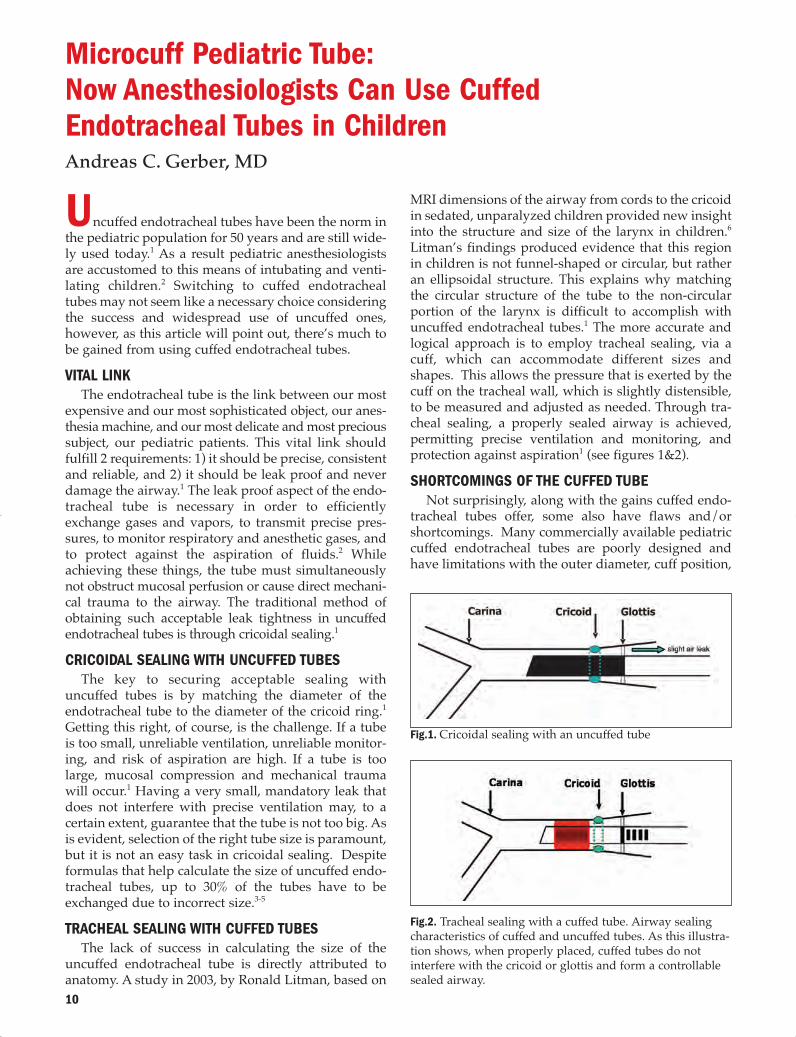
MRI dimensions of the airway from cords to the cricoidin sedated, unparalyzed children provided new insightinto the structure and size of the larynx in children.6Litman’s findings produced evidence that this regionin children is not funnel-shaped or circular, but ratheran ellipsoidal structure. This explains why matchingthe circular structure of the tube to the non-circularportion of the larynx is difficult to accomplish withuncuffed endotracheal tubes.1 The more accurate andlogical approach is to employ tracheal sealing, via acuff, which can accommodate different sizes andshapes. This allows the pressure that is exerted by thecuff on the tracheal wall, which is slightly distensible,to be measured and adjusted as needed. Through tra-cheal sealing, a properly sealed airway is achieved,permitting precise ventilation and monitoring, andprotection against aspiration1 (see figures 1&2).SHORTCOMINGS OF THE CUFFED TUBE
Not surprisingly, along with the gains cuffed endo-tracheal tubes offer, some also have flaws and/orshortcomings. Many commercially available pediatriccuffed endotracheal tubes are poorly designed andhave limitations with the outer diameter, cuff position,
Microcuff Pediatric Tube: Now Anesthesiologists Can Use Cuffed Endotracheal Tubes in Children Andreas C. Gerber, MD
Fig.2. Tracheal sealing with a cuffed tube. Airway sealingcharacteristics of cuffed and uncuffed tubes. As this illustra-tion shows, when properly placed, cuffed tubes do notinterfere with the cricoid or glottis and form a controllablesealed airway.
Fig.1. Cricoidal sealing with an uncuffed tube
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 10
11
cuff diameter and depth markings.7 Since endotrachealtubes are chosen according to internal diameter, thedifferences in outer tube diameters, more often thannot, go unnoticed. This may lead to the use of over-sized, ill-fitting tubes, which can cause damage to thesubglottis.7 In addition many endotracheal tube cuffsrequire inflation to a high pressure for sealing.Presently, there is no data about cuff pressure limits inchildren; in adults acceptable cuff pressure is 25–30 cmH2O.8 Accordingly cuff pressures in children should be≤ 20 cm H2O In many cuffed tubes, the upper borderof the cuff corresponds to the upper border of thedepth marking of the next larger sized uncuffed endo-tracheal tube. The reduced margin of safety withregard to endobronchial intubation of cuffed endotra-cheal tubes, even with the cuff placed within the lar-ynx, is a serious problem with current cuffed tubes.Not all cuffed tubes have depth markings, and in theones that do have them, the distances from depthmarkings to tube tip are greater than the age-relatedminimal tracheal length9 (see fig. 3). A satisfactorycuffed tube size in children depends on the size of boththe outer tube and cuff diameter with sealing pressureat less than 20 cm H2O.10
IDEAL PEDIATRIC CUFFED TRACHEAL TUBESIdeally a cuffed pediatric tracheal tube should be
designed to accommodate a high-volume low-pressurecuff with a short cuff length. It should have the follow-ing attributes:• The cuff should be located below the cricoid ring,
at the level of the tracheal cartilages, which are ableto expand.7
• The tube must not be intra-laryngeal, which cancause vocal cord palsy; the length of the cuff andthe presence of a Murphy eye are important deter-minants of final upper cuff position in cuffed pedi-atric tracheal tubes.7
• Adequate depth markings are needed to guaranteea cuff position below the cricoid and a tip farenough above the tracheal carina.7
• Importantly, a good tube has correct depth marking.• Verified recommendations for using the correct tube.
Reliable depth markings are a must to position atube correctly.9 If it is placed according to the depthmark, then the tip of this tube must lie somewhere inthe middle part of the trachea, such that there is a wideenough margin of safety. For example, if the head isextended, the tip of the tube will move cranially, butthe cuff should still be below the larynx. The tube willtravel caudally when the head is flexed, but nonethelessthe tip should not reach the carina.
Recently, our group assisted the development of anew cuffed pediatric tube, the Microcuff pediatric tube.This tube employs a patented cuff capable of sealing atvery low pressures.10
A CORRECTLY SIZED TUBE ELIMINATES THE NEEDFOR FORMULAS
In our institution our goals were to have a sealedairway at low cuff pressures, a low tube exchange rate,and to move away from the various sizing formulas,which really only represent a best guess.9 In reviewingthe literature, my colleague, Markus Weiss consideredthe available radiological and anatomical data aboutthe pediatric airway and carefully calculated the agespecific dimensions for an ideal cuffed pediatric tube.We used a modified version of the Cole formula as ourbasis for the tube size selection.7 In our experience, the3.5 mm tube can fit children as young as eight months.7(See figure 4).
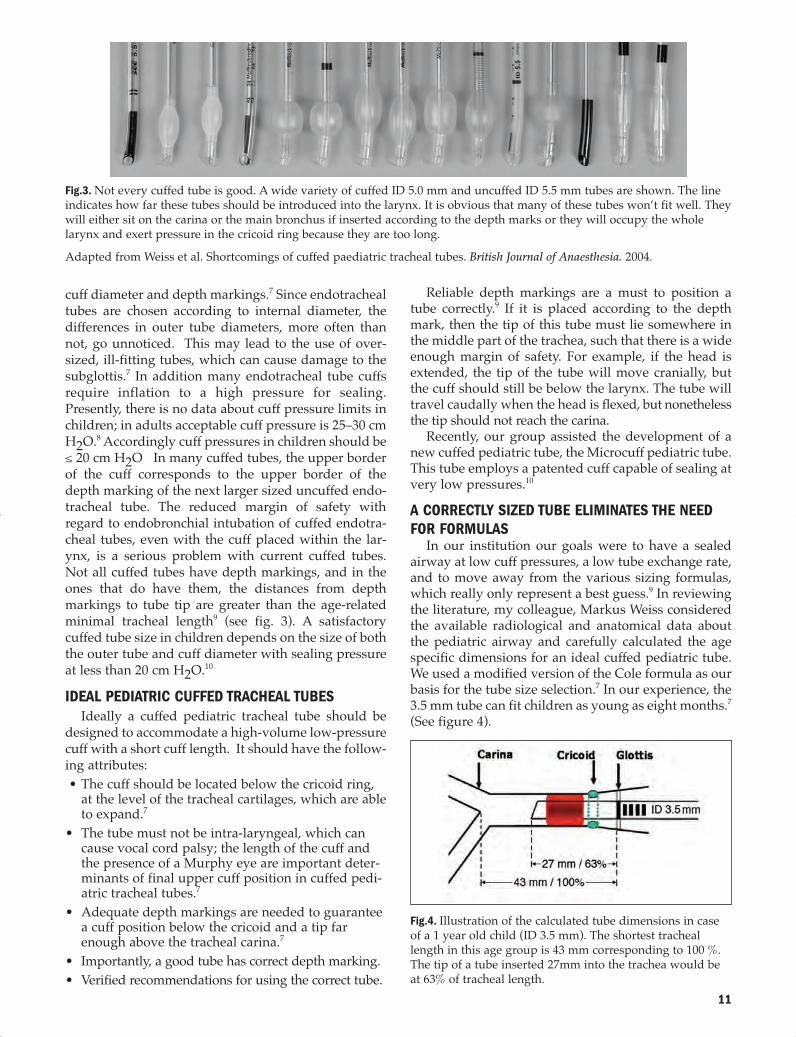
Fig.3. Not every cuffed tube is good. A wide variety of cuffed ID 5.0 mm and uncuffed ID 5.5 mm tubes are shown. The lineindicates how far these tubes should be introduced into the larynx. It is obvious that many of these tubes won’t fit well. Theywill either sit on the carina or the main bronchus if inserted according to the depth marks or they will occupy the wholelarynx and exert pressure in the cricoid ring because they are too long. Adapted from Weiss et al. Shortcomings of cuffed paediatric tracheal tubes. British Journal of Anaesthesia. 2004.
Fig.4. Illustration of the calculated tube dimensions in caseof a 1 year old child (ID 3.5 mm). The shortest tracheallength in this age group is 43 mm corresponding to 100 %.The tip of a tube inserted 27mm into the trachea would beat 63% of tracheal length.
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 11

12
We feel strongly that there is no need for a Murphyeye, as it makes the tracheal part of the tube unneces-sarily long. Using a correct depth mark will ensure thatthe tube will not encroach on the carina.10 That is betterthan hoping that a Murphy eye will still allow bilater-al ventilation if the tube is too deep.9
MICROCUFF DEPTH AND SIZE RECOMMENDATIONS Correct insertion depth is critical for cuffed tubes, so
we ensured that Microcuff employ a clear mark. Thismark must be situated between the vocal cords and the4 “alerting bars”, helps ensure correct positioningwhen a perfect view of the glottis cannot be obtained,or when a tube is initially inserted too deep.9
Instead of various formulas for tube selection, wedecided on explicate size recommendations. This siz-ing chart is provided with all Microcuff packages.
STUDIES WITH MICROCUFF PEDIATRIC TUBETo ensure that the Microcuff tube fulfills our expec-
tations, we have so far conducted 7 studies with over1000 patients and have confirmed that Microcuff fitsand performs well.
The most important study was published in ActaAnaesthesiologica Scandinavica and included 500patients from neonates up to 16 years of age. In almostall patients (98.4 %), Microcuff fit well.10 We also foundthat the depth marks and dimensions were correct. Thetube was too large in only 8 out of 500 patients and wasnever found to be too small.10 This was expected sincea cuffed tube can accommodate various sizes andshapes of the airway. When the tubes were insertedaccording to the depths markings on the tube, all thetubes were within a safe tracheal range, and the cuffwas situated safely below the cricoid with flexion andextension of the head.9 This was confirmed with endo-scopic and radiological studies. We found the tube tips
Fig.4 continued: In all age groups, there must be a cuff-freesubglottic zone (blue bars). The burgundy bars representthe region of the cuff. The end of the yellow bar is the tip ofthe tube in neutral head position. The tip will move down-ward towards the carina with flexion of the head, butshould not go further than the green bars. The dark upper-most columns represent the margin of safety so the tube isnever situated on the carina or in the main bronchus.
Fig.5. Photograph depicting the clear depth marks on thePediatric Microcuff Endotracheal Tube to ensure correctpositioning.
Fig.6. Microcuff Sizing Chart
Recommended Size Selecton
Tube Size Age/WeightI.D. Years/kg
3.0 mm term/≥ 3kg – 8 months3.5 mm 8 months – 2 years4.0 mm 2 – 4 years4.5 mm 4 – 6 years5.0 mm 6 – 8 years5.5 mm 8 –10 years6.0 mm 10 – 12 years6.5 mm 12 – 14 years7.0 mm 14 – 16 years
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 12

13
were correctly placed in the middle ofthe trachea, between the vocal cords andthe carina and that there was an ade-quate margin of safety when the head isflexed or extended. No tube becamelocated endobronchially and there wasno accidental extubation with headextension.THE MICROCUFF SEAL
The Microcuff seal is clearly excep-tional. Made of ultra thin polyurethane,the cuff fills the gap between tube andtracheal wall without folds and chan-nels.10 It virtually drapes and clings tothe wet mucosa similar to the way house-hold plastic wrap clings to meat. Thisattribute results in better sealing at lowerpressures compared to PVC.10 In addi-tion, leaking does not occur between thecuff and the wall, as one would imagine,but through the cuff itself, as illustrated when thecuffed tube is inserted into a glass tube (see fig. 7).
We also confirmed this excellent sealing in vivo. Infigure 8 we see the cuff pressures required in our 500-patient study. The mean pressure was around 10 cm ofwater.10
In figure 9 we have in vivo cuff pressures of variouswell-known endotracheal tubes. Again the Microcuffsealed at a mean pressure of 10 cm of water, whereasthe other tubes required mean cuff pressures of 20 and35 cm of water.11
WITH MICROCUFF PEDIATRIC TUBE THERE IS A LOWINCIDENCE OF STRIDOR
The main concern is for the cuffed tube not to causeairway damage, and we found that Microcuff had alow incidence of stridor.10 We know that severe sub-glottic swelling results either from inadequate perfu-sion or mechanical trauma by tubes that are too large.
Another cause is multiple intubations. Comparing theincidence of postintubation croup is difficult becauseof variable definitions. As such, we measured postintu-bation stridor, a clinical surrogate symptom for earlyairway damage.
In our studies, we have found postintubation stri-dor in 1.8% of patients, with 2 patients needing epi-nephrine inhalation.10 This incidence is comparable tothe work of Khine, who in 1997 found an incidence of2.4% with cuffed tubes and 2.9% for uncuffed tubes.3 Inan older, large retrospective study (n=7875) from Kokaconducted in 1977, the overall incidence of postintuba-tion croup was 1%; the incidence in patients 1 to 4years of age was 5%.12 And in a separate study byNewth in 2004 on intensive care patients with longerduration of intubation, an incidence of 4.8 % withcuffed and 6.9% with uncuffed tubes was found.13
Fig.7. As these CT scans illustrate, contrast dye leaks through the unnamed cuff through foldsand cracks. There is no leaking through the Microcuff because there are no such folds.
Fig.8. Adapted from Dullenkopf A, Gerber AC, Weiss M. Fit and seal charac-teristics of a new paediatric tracheal tube with high volume-low pressurepolyurethane cuff. Acta Anaesthesiol Scand. 2005.
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 13

14
In our department, we’ve been using cuffed tubes inchildren regularly for 5 years, which comes to over15,000 patients. We have not seen any long term mor-bidity in our patients. This was confirmed by Prof.Isabelle Murat from Paris who has even more experi-ence with cuffed tubes.14
MONITORING CUFF PRESSURE MUST BECOME ROUTINEThe results we have obtained with cuffed tubes are
very reassuring, but there is one very important point.Cuffed tubes should only be used in children if thecommitment is made to control cuff pressure. As anes-thesiologists, we spend more time than we care tothink about measuring. We measure blood pressure,central venous pressure, atrial and pulmonary pres-sure, gas pressure, and cerebral perfusion pressure.Now, we just have to include cuff pressure into ourpressure routine. Cuff pressure can be measured andcontrolled with a simple manometer or with an elec-tronic cuff regulator, which is what we use on all ouranesthesia machines.10
MICROCUFF — A NEW ERA IN PEDIATRIC AIRWAYMANAGEMENT
For more definitive proof, Microcuff pediatric endo-tracheal tube is currently undergoing a large, prospec-tive, randomized, controlled study in 24 European cen-ters. The goal is to enroll 5000 pediatric patients, fromneonates up to 5 years of age, corresponding to tubesfrom ID 3.0 to 4.5 mm. The study should be complet-ed in 2007. However, for cuffed tubes to be routinelyused not only is a large prospective study needed, clin-ical standards and textbook recommendations mustalso change. Such a change has already begun.
The American Heart Association (AHA) and theInternational Liaison Committee on Resuscitation(ILCOR) state in their guidelines for pediatric resusci-tations that the use of cuffed tubes in infants and chil-dren is now an accepted alternative to uncuffed tubes
in infants and children. Likewise, Dr.Golden of the Society for PediatricAnesthesia (SPA) has also stated in anSPA newsletter that cuffed tubes aresuitable as an alternative from size 4.0mm on, and that they are actuallypreferred in patients at risk forpulmonary aspiration, those with lowlung compliance (including laparos-copy, thoracoscopy, cardio-pulmonarybypass) and in whom precise ventila-tion and CO2 control is important. CONCLUSION
Using uncuffed tubes in childrenup to 8 years of age has been the para-digm for the last 50 years. Withuncuffed tubes a sealed airway canonly be obtained with an oversizedtube. The recommendation to use atube which fits snugly through the
cricoid ring with a slight air leak at 20 cm of inflationpressure allows acceptable ventilation and monitoring.However, a high tube exchange rate is unavoidabledue to variations of size and shape of the airway anddue to the fact that a circular tube does not fit ideallyinto the ellipsoidal cricoid cartilage. Tracheal sealingwith a cuffed tube is a much more logical way ofobtaining a leak proof link between the anesthesiamachine and the patient. The gap between a deliber-ately smaller tube and the trachea is filled by a cuffinflated to a cuff pressure ≤ 20 cm H2O. The newMicrocuff pediatric tube has been designed and testedto fit the dimensions of the pediatric airway, to seal atcuff pressures below 20 cm H2O and to allow precisepositioning due to clear and correct depth markings.With such an endotracheal tube pediatric anesthesiolo-gists can safely switch to cuffed tubes in infants andsmall children. References1. Weiss M, Gerber AC. Cuffed tracheal tubes in children –
things have changed. Pediatr Anesth. 2006;16:1005–1007.2. Fine GF, Borland LM. The future of the cuffed endotra-
cheal tube. Pediatr Anesth. 2004;14:38–42.3. Khine HH, Corddry DH, Kettrick RG, et al. Comparison
of cuffed and uncuffed endotracheal tubes in young chil-dren during general anesthesia. Anesthesiology.1997;86:627-631.
4. Mukubo Y, Iwai S, Suzuki G. Practical method for theselection of optimal endotracheal tube size in pediatricanesthesia. Kobe J Med Sci. 1978;24:77-85.
5. Mostafa SM. Variation in subglottic size in children. ProcR Soc Med. 1976;69:793-795.
6. Litman RS, Weissend EE, Shibata D, Westesson PL.Developmental changes of laryngeal dimensions inunparalyzed, sedated children. Anesthesiology.2003;98:41-45.
7. Weiss M, Dullenkopf C, Gysin C, Dillier CM, Gerber AC.Shortcomings of cuffed paediatric tracheal tubes. Br JAnaesth. 2004;92:78-88.
Fig.9. Adapted from Dullenkopf A, Schmitz A, Gerber AC, Weiss M. Trachealsealing characteristics of pediatric cuffed tracheal tube. Pediatr Anesth. 2004.
Sealing Characteristics
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 14

15
8. Seegobin RD, van Hasselt GL. Endotracheal cuff pressureand tracheal mucosal blood flow: endoscopic study ofeffects of four large volume cuffs. Brit Med J.1984;288:965-968.
9. Weiss M, Balmer C, Dullenkopf A et al. Intubation depthmarkings allow an improved positioning of endotrachealtubes in children. Can J Anesth. 2005;52:721-726.
10.Dullenkopf A, Gerber AC, Weiss M. Fit and seal charac-teristics of a new paediatric tracheal tube with high volume-low pressure polyurethane cuff. ACTA.2005;49:232-237.
11. Dullenkopf A, Schmitz A, Gerber AC, Weiss M. Trachealsealing characteristics of pediatric cuffed tracheal tubes.Pediatr Anesth. 2004;14:825-830.
12.Koka BV, Jeon IS, Andre JM, MacKay I, Smith RM.Postintubation croup in children. Anesth Analg.1977;56:501-505.
13.Newth CJ, Rachman B, Patel N, Hammer J. The use ofcuffed versus uncuffed endotracheal tubes in pediatricintensive care. J Pediatr. 2004;144:333-337.
14. Murat I. Cuffed tubes in children: A 3-year experience ina single institution. Paediatr Anaesth. 2001;11:748-749.
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 15

H0726-07-01
ANE IntubationPub.qxp 1/24/08 10:45 AM Page 16