rapid sequence intubation – et intubation student handoutpcairwaycourse.org/docs/rsi...
TRANSCRIPT
Paramedic Airway Management Course
Rapid Sequence Intubation – ET Intubation Student Handout
Just Getting’ a Tube…
Goal of the Paramedic Airway Management Course Rapid Sequence Intubation (RSI)/Medical Advanced Airway Management
Students will learn to:
• Determine the risks and benefits of RSI and Advanced Airway (ET) Management.
• Understand the pharmacology of sedation, pain management and neuromuscular blockage.
• Demonstrate knowledge of the “Seven Ps of RSI” and Medical Advanced Airway Management
per local protocols.
• Appropriately manage critical patients’ airway through case-based scenarios.
Cognitive Objectives
1. Identify advantages, disadvantages and dosage of anesthesia, analgesia, sedative agents
and neuromuscular blocking drugs and/or other agents used in medicated rapid-sequence
intubation according to pre-hospital protocol.
2. Define the time sequencing of the Rapid Sequence Intubation steps,
the “Seven P’s:” • Preparation: Zero minus 10 minutes
• Pre-oxygenate: Zero minus 5 minutes
• Pre-medicate: Zero minus 3 minutes
• Paralysis with induction: Zero
• Protection: Zero plus 20-30 seconds
• Placement: Zero plus 45 seconds
• Post Intubation Management: zero plus 1 minute 3. Define the equipment and steps necessary to insure a successful advanced airway by direct
visual endotracheal intubation.
Psychomotor Objectives
1. Utilizing available resources to manage a patient’s uncomplicated airway and ventilations
using both basic and advanced airway management skills.
2. Rapid Sequence Intubation procedure according the “Seven P’s.”
3. Direct endotracheal intubation using steps that include cricoid pressure/B.U.R.P. and other
methods that confirms proper placement.
4. Demonstrate rescue airway procedures following a failed airway.
Affective Objectives
Given a specific scenario to secure a patient’s airway involving an advanced airway method
emergency, students will use critical thinking skills, resources and equipment necessary to
manage the situation.
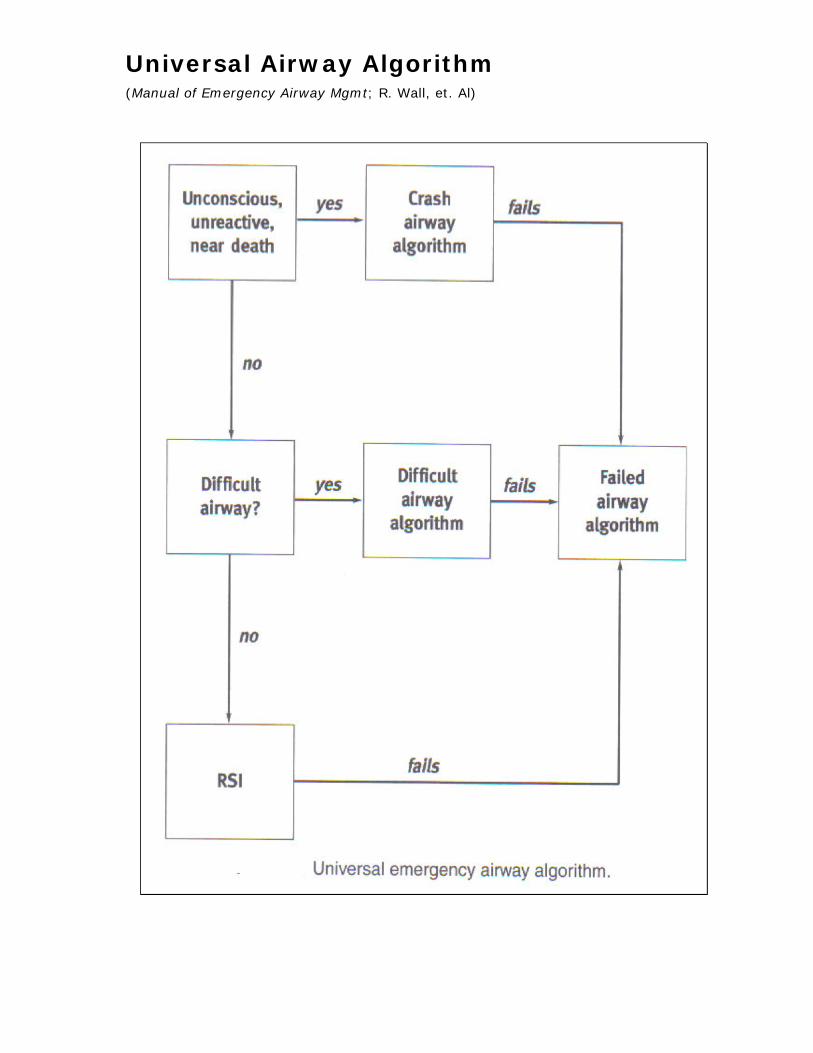
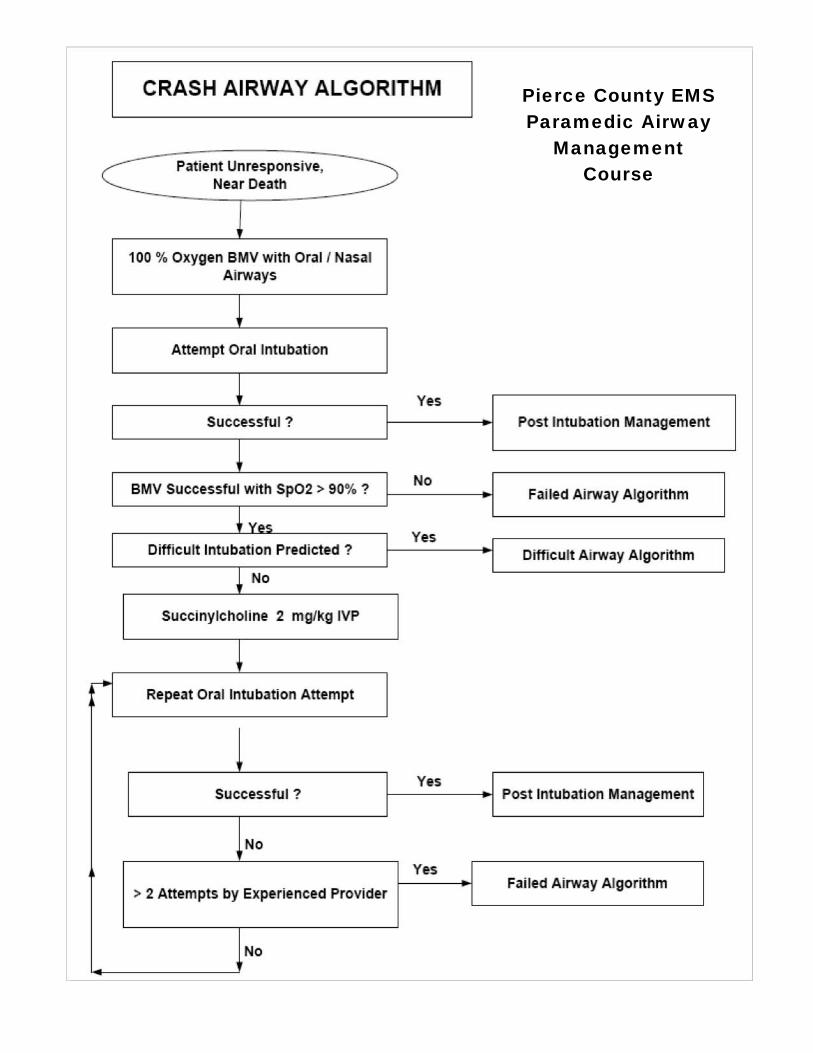
Universal Airway Algorithm (Manual of Emergency Airway Mgmt; R. Wall, et. Al)
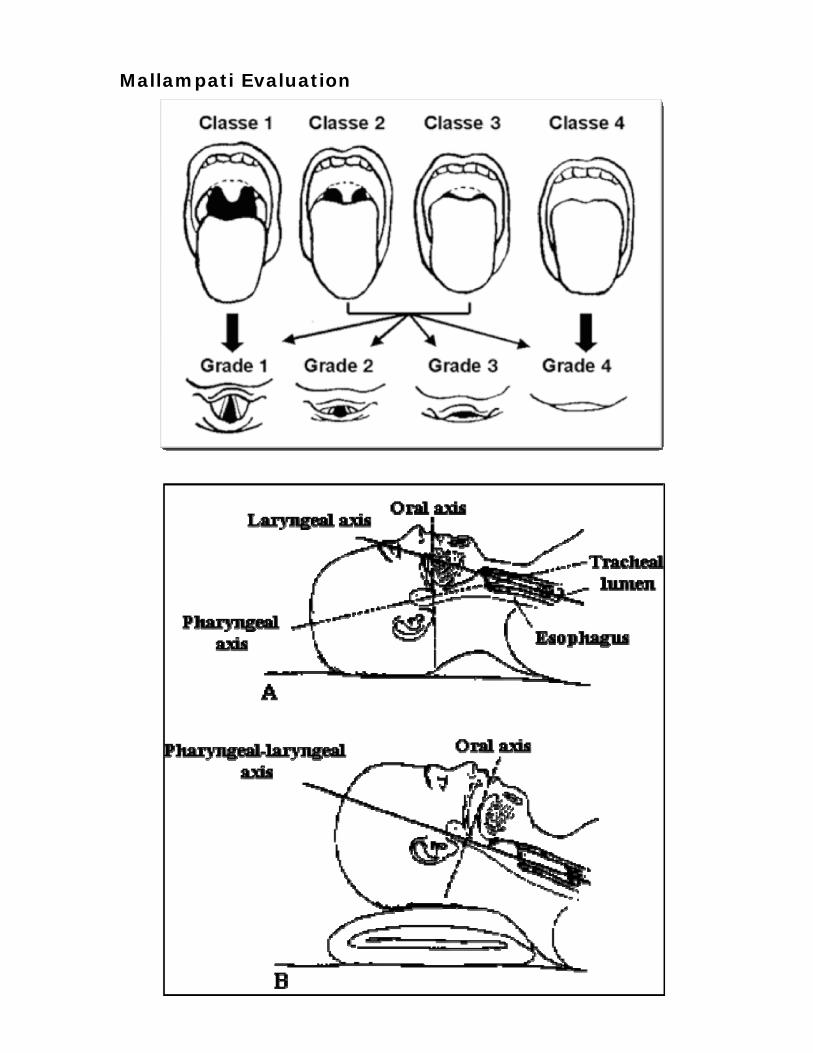
Mallampati Evaluation
Pierce County EMS Paramedic Airway
Management Course

LEMON Mnemonic airway assessment method
L Look externally (facial trauma, large incisors, beard or moustache, large
tongue)
E Evaluate the 3-3-2 rule (incisor distance-3 finger breadths, hyoid-mental
distance-3 finger breadths, thyroid-to-mouth distance-2 finger breadths)
M Mallampati (Mallampati score > 3).
O Obstruction (presence of any condition like epiglottitis, peritonsillar abscess,
trauma).
N Neck mobility (limited neck mobility)
3-3-2 Rule
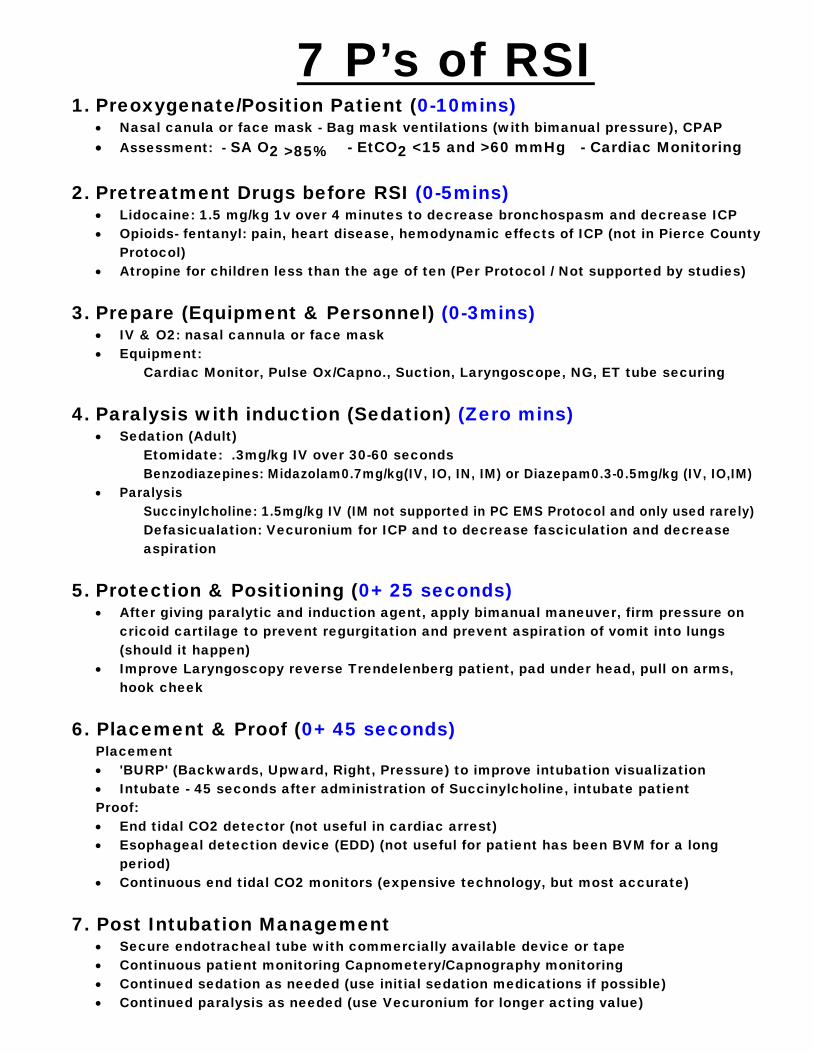
7 P’s of RSI 1. Preoxygenate/Position Patient (0-10mins)
• Nasal canula or face mask - Bag mask ventilations (with bimanual pressure), CPAP • Assessment: - SA O2 >85% - EtCO2 <15 and >60 mmHg - Cardiac Monitoring
2. Pretreatment Drugs before RSI (0-5mins) • Lidocaine: 1.5 mg/kg 1v over 4 minutes to decrease bronchospasm and decrease ICP • Opioids- fentanyl: pain, heart disease, hemodynamic effects of ICP (not in Pierce County
Protocol) • Atropine for children less than the age of ten (Per Protocol / Not supported by studies)
3. Prepare (Equipment & Personnel) (0-3mins) • IV & O2: nasal cannula or face mask • Equipment:
Cardiac Monitor, Pulse Ox/Capno., Suction, Laryngoscope, NG, ET tube securing
4. Paralysis with induction (Sedation) (Zero mins) • Sedation (Adult)
Etomidate: .3mg/kg IV over 30-60 seconds Benzodiazepines: Midazolam0.7mg/kg(IV, IO, IN, IM) or Diazepam0.3-0.5mg/kg (IV, IO,IM)
• Paralysis Succinylcholine: 1.5mg/kg IV (IM not supported in PC EMS Protocol and only used rarely) Defasicualation: Vecuronium for ICP and to decrease fasciculation and decrease aspiration
5. Protection & Positioning (0+ 25 seconds) • After giving paralytic and induction agent, apply bimanual maneuver, firm pressure on
cricoid cartilage to prevent regurgitation and prevent aspiration of vomit into lungs (should it happen)
• Improve Laryngoscopy reverse Trendelenberg patient, pad under head, pull on arms, hook cheek
6. Placement & Proof (0+ 45 seconds) Placement
• 'BURP' (Backwards, Upward, Right, Pressure) to improve intubation visualization • Intubate - 45 seconds after administration of Succinylcholine, intubate patient
Proof: • End tidal CO2 detector (not useful in cardiac arrest) • Esophageal detection device (EDD) (not useful for patient has been BVM for a long
period) • Continuous end tidal CO2 monitors (expensive technology, but most accurate)
7. Post Intubation Management • Secure endotracheal tube with commercially available device or tape • Continuous patient monitoring Capnometery/Capnography monitoring • Continued sedation as needed (use initial sedation medications if possible) • Continued paralysis as needed (use Vecuronium for longer acting value)

DIAZEPAM (VALIUM)
CLASSIFICATION 1. Anticonvulsant, anti-anxiety, sedative. ACTION 1. Depresses central nervous system. 2. Skeletal muscle relaxer. ONSET OF ACTION 1. 1 − 5 minute, peak actions at 5 − 10 minutes. DURATION OF ACTION 1. 15 − 60 minutes. INDICATION 1. Seizures secondary to head trauma, status epilepticus. 2. Prior to pacing, cardioversion, and Rapid Sequence Intubation for relief of anxiety, tension, and
diminish recall of procedures. 3. Envenomations resulting in muscle spasm. 4. Skeletal muscle relaxer. 5. Severe anxiety. CONTRAINDICATION 1. Known hypersensitivity. 2. Patients that have used other CNS depressants. USE WITH CAUTION 1. Elderly. 2. Patients with inadequate pulmonary function. 3. Patients with liver and/or kidney disease. 4. Patients with a history of drug addiction. DOSAGE AND ADMINISTRATION 1. Adult: 2.0 − 10.0 mg IV, IO or IM if unable to start IV or IO. For RSI: 0.2 mg/kg IV; 0.1 mg/kg IV if hypotensive. 2. Pediatric: 0.2 mg/kg IV or IO in increments no greater than 2.0 mg to a maximum dose of 10.0 mg. Wait 1 –
2 minutes between doses to observe effect. Rectal: 0.5 mg/kg in increments no greater than 2.0 mg to a maximum dose of 10.0 mg.
Wait at least 5 minutes between doses. Contact Mary Bridge for repeat dose. ADVERSE REACTION 1. Central nervous system depression, Ataxia, Drowsiness, Fatigue, Dizziness, Urticaria, Skin rash, Transient hypotension, Respiratory depression. 2. Venous thrombosis and phlebitis at the injection site. REFERENCE IN PROTOCOL 1. Traumatic Emergencies (seizures; burns − thermal). 2. Cardiac Emergencies (see AHA handbook). 3. Medical Emergencies (Altered level of consciousness − if actively seizing). 4. Environmental Emergencies (Envenomations). 5. Behavioral Emergencies (Violent patients). 6. Rapid Sequence Intubation (Appendix D).
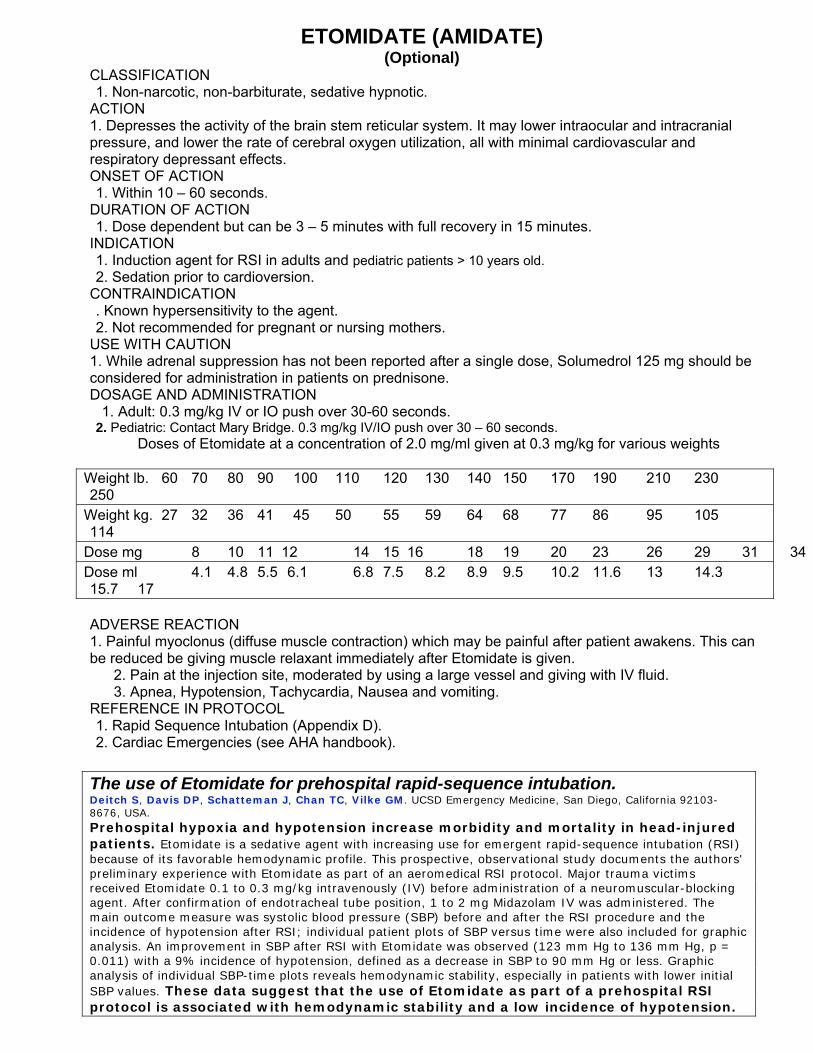
ETOMIDATE (AMIDATE) (Optional)
CLASSIFICATION 1. Non-narcotic, non-barbiturate, sedative hypnotic. ACTION 1. Depresses the activity of the brain stem reticular system. It may lower intraocular and intracranial pressure, and lower the rate of cerebral oxygen utilization, all with minimal cardiovascular and respiratory depressant effects. ONSET OF ACTION 1. Within 10 – 60 seconds. DURATION OF ACTION 1. Dose dependent but can be 3 – 5 minutes with full recovery in 15 minutes. INDICATION 1. Induction agent for RSI in adults and pediatric patients > 10 years old. 2. Sedation prior to cardioversion. CONTRAINDICATION . Known hypersensitivity to the agent. 2. Not recommended for pregnant or nursing mothers. USE WITH CAUTION 1. While adrenal suppression has not been reported after a single dose, Solumedrol 125 mg should be considered for administration in patients on prednisone. DOSAGE AND ADMINISTRATION 1. Adult: 0.3 mg/kg IV or IO push over 30-60 seconds. 2. Pediatric: Contact Mary Bridge. 0.3 mg/kg IV/IO push over 30 – 60 seconds.
Doses of Etomidate at a concentration of 2.0 mg/ml given at 0.3 mg/kg for various weights
Weight lb. 60 70 80 90 100 110 120 130 140 150 170 190 210 230 250 Weight kg. 27 32 36 41 45 50 55 59 64 68 77 86 95 105 114 Dose mg 8 10 11 12 14 15 16 18 19 20 23 26 29 31 34Dose ml 4.1 4.8 5.5 6.1 6.8 7.5 8.2 8.9 9.5 10.2 11.6 13 14.3 15.7 17
ADVERSE REACTION 1. Painful myoclonus (diffuse muscle contraction) which may be painful after patient awakens. This can be reduced be giving muscle relaxant immediately after Etomidate is given.
2. Pain at the injection site, moderated by using a large vessel and giving with IV fluid. 3. Apnea, Hypotension, Tachycardia, Nausea and vomiting.
REFERENCE IN PROTOCOL 1. Rapid Sequence Intubation (Appendix D). 2. Cardiac Emergencies (see AHA handbook). The use of Etomidate for prehospital rapid-sequence intubation. Deitch S, Davis DP, Schatteman J, Chan TC, Vilke GM. UCSD Emergency Medicine, San Diego, California 92103-8676, USA. Prehospital hypoxia and hypotension increase morbidity and mortality in head-injured patients. Etomidate is a sedative agent with increasing use for emergent rapid-sequence intubation (RSI) because of its favorable hemodynamic profile. This prospective, observational study documents the authors' preliminary experience with Etomidate as part of an aeromedical RSI protocol. Major trauma victims received Etomidate 0.1 to 0.3 mg/kg intravenously (IV) before administration of a neuromuscular-blocking agent. After confirmation of endotracheal tube position, 1 to 2 mg Midazolam IV was administered. The main outcome measure was systolic blood pressure (SBP) before and after the RSI procedure and the incidence of hypotension after RSI; individual patient plots of SBP versus time were also included for graphic analysis. An improvement in SBP after RSI with Etomidate was observed (123 mm Hg to 136 mm Hg, p = 0.011) with a 9% incidence of hypotension, defined as a decrease in SBP to 90 mm Hg or less. Graphic analysis of individual SBP-time plots reveals hemodynamic stability, especially in patients with lower initial SBP values. These data suggest that the use of Etomidate as part of a prehospital RSI protocol is associated with hemodynamic stability and a low incidence of hypotension.
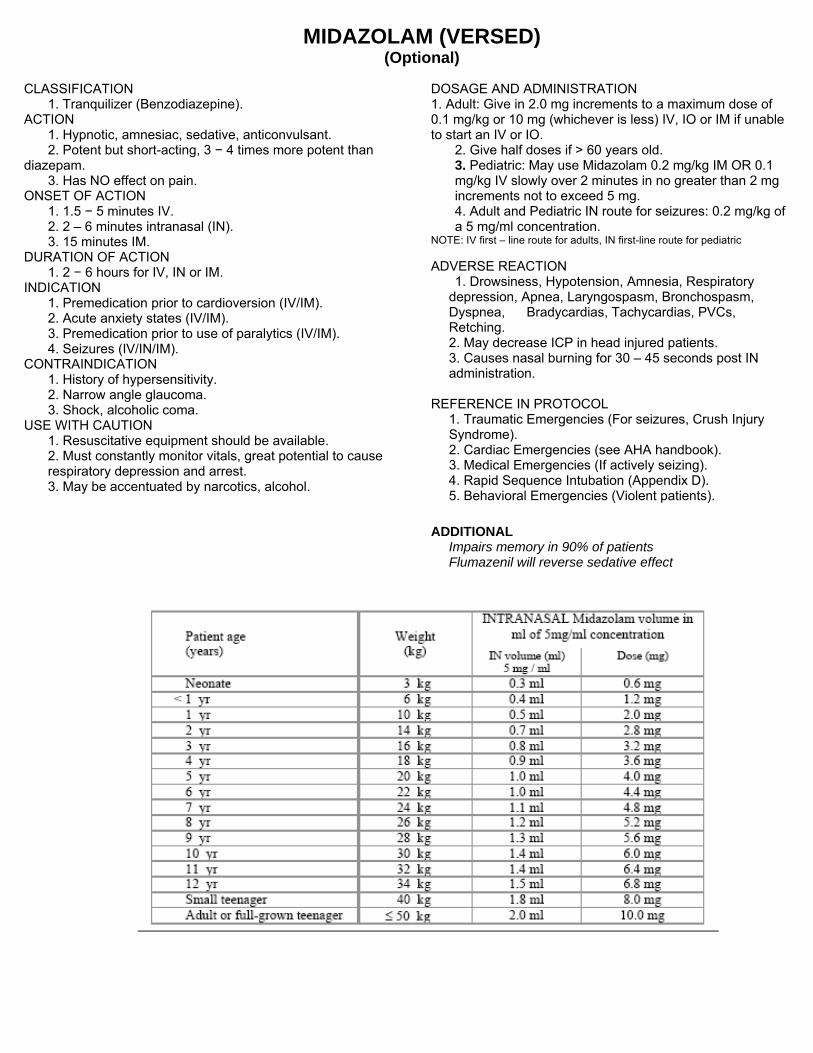
MIDAZOLAM (VERSED) (Optional)
DOSAGE AND ADMINISTRATION CLASSIFICATION 1. Adult: Give in 2.0 mg increments to a maximum dose of 0.1 mg/kg or 10 mg (whichever is less) IV, IO or IM if unable to start an IV or IO.
1. Tranquilizer (Benzodiazepine). ACTION 1. Hypnotic, amnesiac, sedative, anticonvulsant.
2. Give half doses if > 60 years old. 2. Potent but short-acting, 3 − 4 times more potent than diazepam. 3. Pediatric: May use Midazolam 0.2 mg/kg IM OR 0.1
mg/kg IV slowly over 2 minutes in no greater than 2 mg increments not to exceed 5 mg.
3. Has NO effect on pain. ONSET OF ACTION
4. Adult and Pediatric IN route for seizures: 0.2 mg/kg of a 5 mg/ml concentration.
1. 1.5 − 5 minutes IV. 2. 2 – 6 minutes intranasal (IN). 3. 15 minutes IM. NOTE: IV first – line route for adults, IN first-line route for pediatric
DURATION OF ACTION ADVERSE REACTION 1. 2 − 6 hours for IV, IN or IM. 1. Drowsiness, Hypotension, Amnesia, Respiratory
depression, Apnea, Laryngospasm, Bronchospasm, Dyspnea, Bradycardias, Tachycardias, PVCs, Retching.
INDICATION 1. Premedication prior to cardioversion (IV/IM). 2. Acute anxiety states (IV/IM). 3. Premedication prior to use of paralytics (IV/IM).
2. May decrease ICP in head injured patients. 4. Seizures (IV/IN/IM). 3. Causes nasal burning for 30 – 45 seconds post IN
administration. CONTRAINDICATION 1. History of hypersensitivity.
2. Narrow angle glaucoma. REFERENCE IN PROTOCOL 3. Shock, alcoholic coma. 1. Traumatic Emergencies (For seizures, Crush Injury
Syndrome). USE WITH CAUTION 1. Resuscitative equipment should be available.
2. Cardiac Emergencies (see AHA handbook). 2. Must constantly monitor vitals, great potential to cause respiratory depression and arrest. 3. Medical Emergencies (If actively seizing).
4. Rapid Sequence Intubation (Appendix D). 3. May be accentuated by narcotics, alcohol. 5. Behavioral Emergencies (Violent patients).
ADDITIONAL Impairs memory in 90% of patients Flumazenil will reverse sedative effect

VECURONIUM (NORCURON) (Optional)
CLASSIFICATION 1. Skeletal muscle relaxant. 2. Non-depolarizing neuromuscular blocker. ACTION 1. Provides skeletal muscle relaxation to facilitate endotracheal intubation. ONSET OF ACTION 1. 1 minute. DURATION OF ACTION 1. 25 − 30 minutes. INDICATION 1. Maintenance of paralysis AFTER intubation to assist ventilation during prolonged transport. 2. Initial means of paralysis with Crush Injury Syndrome. CONTRAINDICATION 1. Hypersensitivity. 2. Inability to intubate. USE WITH CAUTION 1. Elderly. 2. Patients with cardiovascular disease, hepatic disease, obesity, neuromuscular disease. 3. Do not mix with alkaline solutions. 4. Prior administration of Succinylcholine may enhance the neuromuscular blocking effect. 5. Monitor heart rate continuously. 6. Should be used ONLY by persons skilled at intubation. DOSAGE AND ADMINISTRATION 1. 0.1 mg/kg IV. ADVERSE REACTION 1. Prolonged dose related to respiratory insufficiency or apnea, Wheezing, Aspiration, Bradycardia, Sinus
arrest, Hyper or Hypotension, Increased intraocular pressure. REFERENCE IN PROTOCOL 1. Rapid Sequence Intubation (Appendix D).
2. Traumatic Emergencies (Crush Injury Syndrome).
SUCCINYLCHOLINE (ANECTINE) CLASSIFICATION 1. Ultra short acting skeletal muscle relaxant, depolarizing neuromuscular blocker. ACTION 1. Prolongs depolarization of the muscle end plate. 2. Induces skeletal muscle relaxation causing onset of flaccid paralysis in less than 1 minute. 3. Has no effect on consciousness, pain threshold or cerebration. ONSET OF ACTION 1. 30 − 60 seconds. DURATION OF ACTION 1. 4 − 10 minutes. INDICATION 1. To facilitate endotracheal intubation in
patients with an intact gag reflex. CONTRAINDICATION 1. Known hypersensitivity. 2. Acute glaucoma, penetrating eye injuries.
† CONTRAINDICATION /USE WITH CAUTION: 1) Suspected hyperkalemia ↓ renal failure and missed dialysis. 2) 24 hours or more post-burn. 3) 7 days or more post crush injury. 4) Penetrating eye injury. 5) Increased ICP.
3. Suspected hyperkalemia. 4. 24 hours or more post burn. 5. Post Crush Injury Syndrome. USE WITH CAUTION 1. Should be used ONLY by persons skilled in airway management. 2. Changes in cardiac rhythm may result from vagal stimulation. 3. In patients with possible increased ICP. DOSAGE AND ADMINISTRATION (*Based upon total body weight [Chap.35] -- Manual of Airway Mgmt; Wall, M.D., et Al.) 1. Adult: 1.5 mg/kg IV. 2. Pediatric: 1.0 mg/kg IV. ADVERSE REACTION 1. Prolonged muscle relaxation, Prolonged respiratory depression or apnea, Bradycardia, Tachycardia, Hypertension, Hypotension, Arrhythmias, Excessive salivation. 2. Potential increase in ICP with second and third doses. REFERENCE IN PROTOCOL 1. Rapid Sequence Intubation (Appendix D). 2. Traumatic Emergencies (Crush Injury Syndrome). Note: Must be replaced quarterly whether used or not!!
Succinylcholine: Can We Get By with Less? (No, we need more 1.5mg/kg) Ron M. Walls, MD, FRCPC, FACEP Anesth Analg 2004 Jun; 98:1680-5.
Studies have shown that critical oxyhemoglobin desaturation can occur before recovery of spontaneous ventilation in patients given 1 mg/kg of Succinylcholine (SCh), a matter of concern in cases of "can't intubate, can't ventilate" failed airways. This finding has prompted assessment of lower doses (JWEM Nov 26 2003). One minute after SCh administration, experienced anesthesiologists who were blinded to the dose graded intubation conditions as impossible, poor, good, or excellent. In true rapid sequence intubation (RSI), the induction agent and SCh are given simultaneously, so the burden of intubating conditions falls much more on SCh than it did in this study, where patients received full general anesthesia before they received SCh. Patients in this study were not obese and healthy with normal hemodynamic status, making them quite different from emergency department RSI patients. Third, we are notoriously poor at estimating weight (JWEM Aug 1 1999). The appropriate dose of SCh for ED RSI is 1.5 mg/kg, which avoids the potential for incomplete relaxation and has virtually no downside except for a slightly longer duration of action. The half-life of SCh in the body is about 1 minute, so doubling the dose should increase duration of action only by 60 seconds.
LIDOCAINE 2%
For Rapid Sequence Intubation CLASSIFICATION 1. Antiarrhythmic. ACTION 1. Suppresses ventricular arrhythmias. 2. Local anesthetic. ONSET OF ACTION 1. Immediate. DURATION OF ACTION 1. 10 – 20 minutes. INDICATION 1. Cardiac arrest from VF/VT. 2. Stable VT, wide-complex tachycardias of uncertain type, wide complex PSVT (Indeterminate). 3. Block development of increasing ICP secondary to intubation. 4. As anesthetic flush prior to IO infusion for patients that are awake. CONTRAINDICATION 1. Known hypersensitivity. 2. Heart blocks. USE WITH CAUTION 1. Liver disease. 2. Congestive heart failure. 3. Severe respiratory depression. 4. Hypovolemia. 5. Shock. 6. Any form of heart block. DOSAGE AND ADMINISTRATION 1. Cardiac Arrest from VF/VT, use as follows: a. IV or IO bolus 1.0 − 1.5 mg/kg. b. May give additional 0.5−0.75 mg/kg IV for refractory VF; repeat in 5–10 mins; max. total dose is
3mg/kg. c. A single dose of 1.5 mg/kg in cardiac arrest is acceptable. d. For IO anesthesia: give 20 – 50 mg IO prior to infusion. e. ET dose: 2 − 4 mg/kg. 2. Perfusing arrhythmia of stable VT, wide complex tachycardia of uncertain type, significant ectopy, use as
follows: a. IV bolus 0.5 − 0.75mg/kg up to 1.0 − 1.5 mg/kg. b. Repeat 0.5 − 0.75 mg/kg IV every 5 − 10 minutes, maximum total dose is 3.0 mg/kg. NOTE: In patients with liver disease or severe congestive heart failure, administer half of the above
recommended doses for maintenance dose (not initial). 4. Rapid Sequence Intubation for reactive airway or increased ICP prophylaxis: 1.5mg/kg IV. 5. Pediatric: 1.0 mg/kg.
Lidocaine Pearls: (Manual of Airway Mgmt; Wall, M.D., et Al.) - Lidocaine suppress coughing related intubation - Although Sux. increases the ICP sufficiently small
and variable; the use Lido. elevated ICP until further research suggests otherwise. Fentanyl can be use to combat increased ICP related insults.
- Severe interaction with MOI; can cause hypotension
ADVERSE REACTION 1. CNS: Dizziness, Somnolence, Confusion,
Paresthesias, Muscle twitching, Seizures, Slurred speech.
2. CV: Hypotension, Bradycardia. 3. EENT: Tinnitus, Blurred vision. REFERENCE IN PROTOCOL 1. Cardiac Emergencies (see AHA handbook). 2. Rapid Sequence Intubation (Appendix D). 3. Pediatric Cardiac Arrest Guide (Appendix I)

Malignant Hyperthermia
Malignant hyperthermia (MH) the mortality is high. The exact incidence of MH is unknown. The rate of occurrence has been estimated as one in 5,000 or as rare as one in 65,000 administrations of general anesthesia with triggering agents. Succinylcholine is one of the agents that “trigger” MH, a hypermetabolic response: • Fever (<105), • Tachycardia, * Vecuronium is considered safe for
patients with MH risk factors • Tachypnea, • Acidosis, • Hyperkalemia, • Ventricular dysrhythmias, • Rhabdomyolysis. Risk Factors Includes positive family history of MH History of same, Duchene’s Muscular Dystrophy, Guillain-Barre syndrome Certain myopathies. Increased intraocular pressure Rhabdomyolysis and myoglobinuria Muscle pain-reduced if a defasciculating dose of Pancuronium is used Increased intragastric pressure Increased intracranial pressure-blunted by pretreatment with adequate sedation and a defasciculating dose of Pancuronium. Treatment The MH crisis must be identified and treated immediately for a successful outcome. Dantrolene sodium for injection (Dantrium® I.V.) is the medication of choice. It is vital that all hospitals, ambulatory centers and offices where general anesthesia is administered have a full supply of Dantrolene immediately available. In addition, the provider must have facilities to rapidly lower body temperature, measure acid/base changes in the blood, measure coagulation changes, blood electrolytes and tests for muscle breakdown.
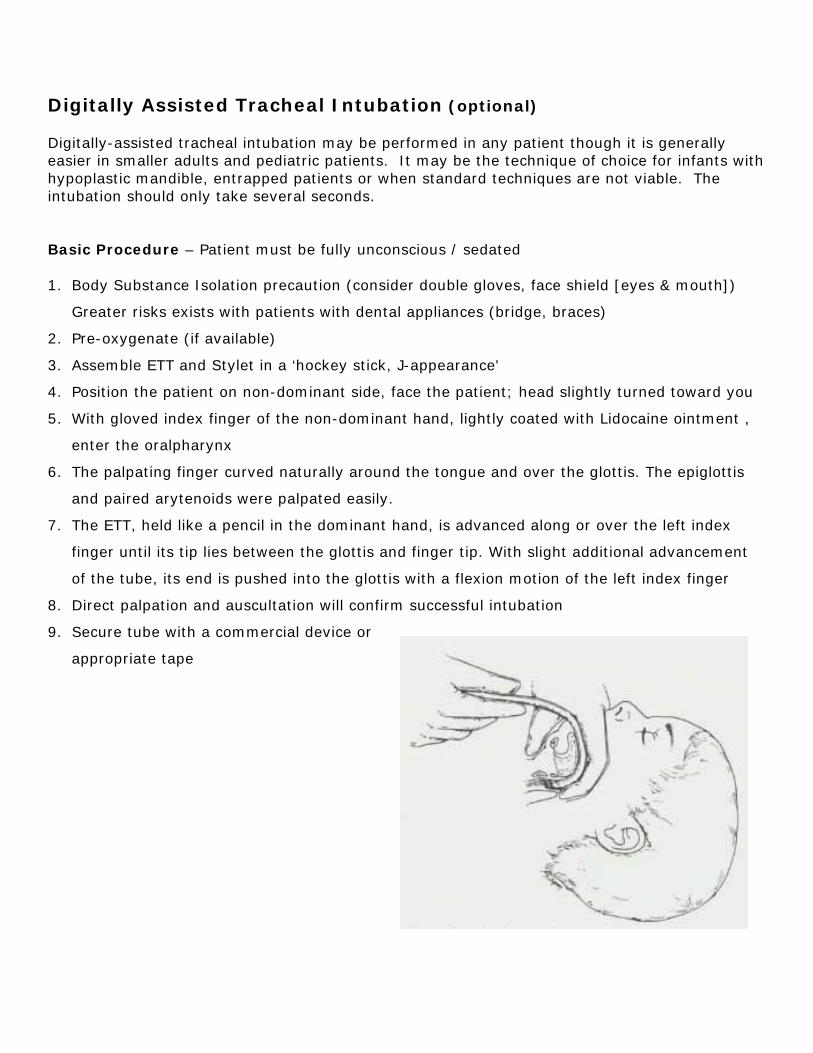
Digitally Assisted Tracheal Intubation (optional) Digitally-assisted tracheal intubation may be performed in any patient though it is generally easier in smaller adults and pediatric patients. It may be the technique of choice for infants with hypoplastic mandible, entrapped patients or when standard techniques are not viable. The intubation should only take several seconds. Basic Procedure – Patient must be fully unconscious / sedated 1. Body Substance Isolation precaution (consider double gloves, face shield [eyes & mouth])
Greater risks exists with patients with dental appliances (bridge, braces)
2. Pre-oxygenate (if available)
3. Assemble ETT and Stylet in a ‘hockey stick, J-appearance'
4. Position the patient on non-dominant side, face the patient; head slightly turned toward you
5. With gloved index finger of the non-dominant hand, lightly coated with Lidocaine ointment ,
enter the oralpharynx
6. The palpating finger curved naturally around the tongue and over the glottis. The epiglottis
and paired arytenoids were palpated easily.
7. The ETT, held like a pencil in the dominant hand, is advanced along or over the left index
finger until its tip lies between the glottis and finger tip. With slight additional advancement
of the tube, its end is pushed into the glottis with a flexion motion of the left index finger
8. Direct palpation and auscultation will confirm successful intubation
9. Secure tube with a commercial device or
appropriate tape
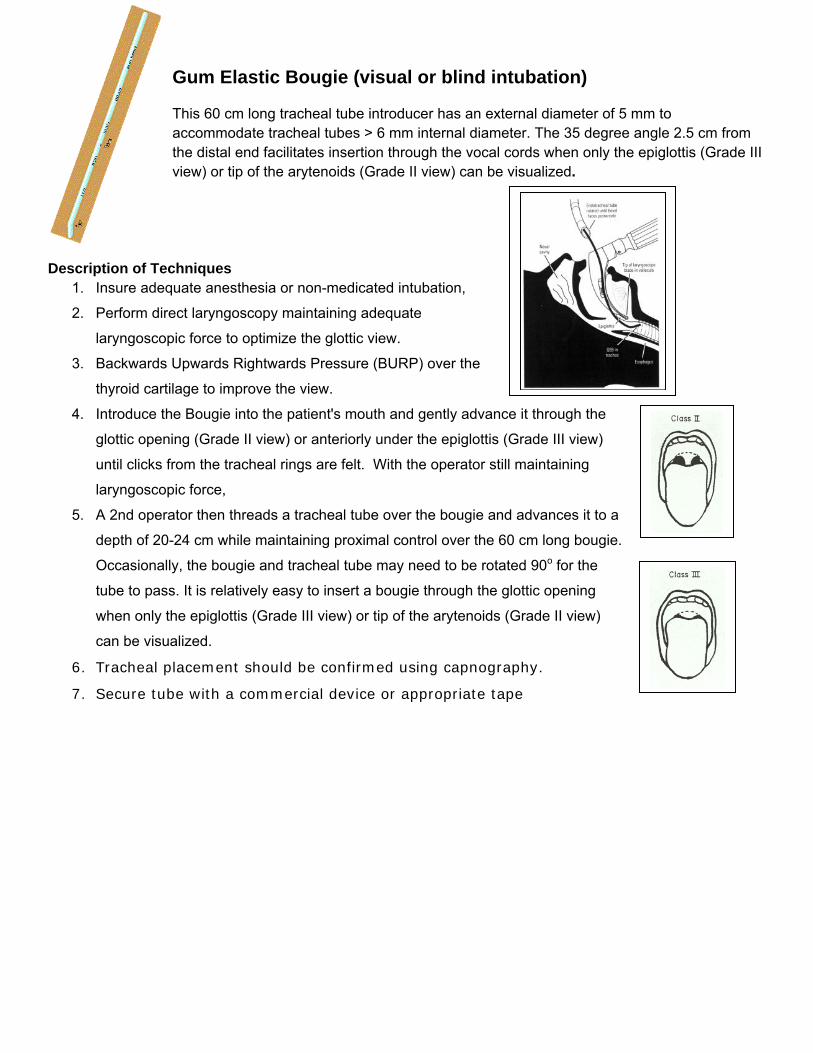
Gum Elastic Bougie (visual or blind intubation) This 60 cm long tracheal tube introducer has an external diameter of 5 mm to accommodate tracheal tubes > 6 mm internal diameter. The 35 degree angle 2.5 cm from the distal end facilitates insertion through the vocal cords when only the epiglottis (Grade III view) or tip of the arytenoids (Grade II view) can be visualized.
Description of Techniques 1. Insure adequate anesthesia or non-medicated intubation,
2. Perform direct laryngoscopy maintaining adequate
laryngoscopic force to optimize the glottic view.
3. Backwards Upwards Rightwards Pressure (BURP) over the
thyroid cartilage to improve the view.
4. Introduce the Bougie into the patient's mouth and gently advance it through the
glottic opening (Grade II view) or anteriorly under the epiglottis (Grade III view)
until clicks from the tracheal rings are felt. With the operator still maintaining
laryngoscopic force,
5. A 2nd operator then threads a tracheal tube over the bougie and advances it to a
depth of 20-24 cm while maintaining proximal control over the 60 cm long bougie.
Occasionally, the bougie and tracheal tube may need to be rotated 90o for the
tube to pass. It is relatively easy to insert a bougie through the glottic opening
when only the epiglottis (Grade III view) or tip of the arytenoids (Grade II view)
can be visualized.
6. Tracheal placement should be confirmed using capnography.
7. Secure tube with a commercial device or appropriate tape