an overview of oral cancer in indian subcontinent and ... overview of oral cancer in indian...
TRANSCRIPT

Article ID: WMC003626 ISSN 2046-1690
An Overview of Oral Cancer in Indian Subcontinentand Recommendations to Decrease its Incidence.Corresponding Author:Dr. Zahid Ullah Khan,Assistant professor, Community Medicine Department, NIMS Medical College, Abbottabad., House No: 01,Opposite Police Colony Gate No: 02, Kalapul, Mansehra Road, Abbottabad., 22010 - Pakistan
Submitting Author:Dr. Zahid U Khan,Assistant professor, Community Medicine Department, NIMS Medical College, Abbottabad., House No: 01,Opposite Police Colony Gate No: 02, Kalapul, Mansehra Road, Abbottabad., 22010 - Pakistan
Article ID: WMC003626
Article Type: Research articles
Submitted on:05-Aug-2012, 04:46:02 PM GMT Published on: 06-Aug-2012, 05:07:32 PM GMT
Article URL: http://www.webmedcentral.com/article_view/3626
Subject Categories:CANCER
Keywords:Oral Cancer in Indian Subcontinent and Preventive Recommendations
How to cite the article:Khan Z. An Overview of Oral Cancer in Indian Subcontinent and Recommendations toDecrease its Incidence. . WebmedCentral CANCER 2012;3(8):WMC003626
Copyright: This is an open-access article distributed under the terms of the Creative Commons AttributionLicense(CC-BY), which permits unrestricted use, distribution, and reproduction in any medium, provided theoriginal author and source are credited.
Source(s) of Funding:
I have not taken any funding for this article from any other party and its only my work and have not been fundedby any third party.
Competing Interests:
No
WebmedCentral > Research articles Page 1 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
An Overview of Oral Cancer in Indian Subcontinentand Recommendations to Decrease its Incidence.Author(s): Khan Z
Abstract.
The Objective of this article is to review the currentprevalence and risk factors for oral carcinoma acrossthe Indian subcontinent. Oral cancer is increasing inIndian subcontinent mainly due to lack of hygiene,tobacco use, chewing tobacco leaves, smoking andmany other factors which are discussed in detail in thisarticle. Cancer is the second most common cause ofmortality and morbidity today after cardiovascularproblems. Oral cancer is the eleventh most commoncancer in the world and two third deaths due to oralcancer occurs in developing world, out of which onethird occurs in Indian Subcontinent. Human papillomavirus is a known risk factor oral cancer specially type16 and 18. This is causing not only huge impact onthe health of the community but also the economy ofthe Indian subcontinent countries. We havesummarized few recommendations in this article, bywhich oral cancer can be tackled in Indiansubcontinent. We have recommended differentapproaches from primary prevention to secondary andtertiary prevention methods. These include betterhygiene, health education, and proper screeningmethods to detect those at risk, earlier treatment andsmoking cessation clinics, proper legislation atgovernment level and global approach as well.
Table of Contents
1. Introduction---- 41.1 Indian Subcontinent---- 41.2 Oralcancer------ 41.2.1 The international scenario for oral cancer--- 4
2. The scenario for oral cancer in the IndianSubcontinent--- 52.1 Cancer registration in the Subcontinent------- 5
3. The plan of action for oral cancer in theSubcontinent---- 63.1 The vision3.2 The mission-- 14 3.3 Core values-- 143.3.1 Science --- 14 3.3.2 Trust ----- 14 3 . 3 . 3 S o c i e t y - - -
15 3 . 4 O v e r v i e w - - -15 3 . 5 C u r i n g o r a l c a n c e r - -15 3 .6 Fac ing the cha l l enge o f t obacco - -16 3.7 Building capacity through co-ordination --16 3 . 8 S u s t a i n i n g t h e u n i q u e n e s s - -16 3 . 9 O t h e r c h a l l e n g e s - -17 3 . 9 . 1 P s y c h o l o g i c a l a s p e c t s - -17 3 . 9 . 2 E c o n o m i c a s p e c t - -17
4. SAOCF’s efforts in addressing the challenges--17 4 . 1 Add ress i ng t he va r i ous aspec t s - -17 4 . 2 B u i l d i n g c o m p e t e n c i e s - -18 4.3 Bridging research and practical efforts --18 4 . 4 F a c i n g t h e b u r d e n o f d i s e a s e - -18 4 . 5 A d d r e s s i n g d i s p a r i t i e s - -19 4.6 Professional workforce -- 19 4 .7 St rengthen ing the research base - -19 4.8 Creation of a platform for united efforts --20 4.9 Creating media and public awareness --20 4.10 Establishing and developing collaborations --20 4.11 Creating and upgrading tangible evidence based -- 21
5. Experience with technical and policy solutions --21 5 . 1 S o l u t i o n s - -21 5 . 1 . 1 P r i m a r y p r e v e n t i o n - -22
WebmedCentral > Research articles Page 2 of 29
WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
5.1.2 Cost effectiveness of primary prevention --22 5 . 1 . 3 C o m m u n i t y i n t e r v e n t i o n s - -23 5 . 1 . 4 M a s s m e d i a i n t e r v e n t i o n - -23 5.1.5 Sufficient evidence for long term oral cancer riskReduction for the South Asian region -- 23 5 . 1 . 6 S e c o n d a r y p r e v e n t i o n - -24 5.1.7 Cost effectiveness of secondary prevention --24 5 . 1 . 8 M e d i c a l i n t e r v e n t i o n s - -24 5.2 Programmatic approach and structural challenges-- 24 5 . 3 T o b a c c o c e s s a t i o n c l i n i c s - -25 5 . 4 E c o n o m i c i n t e r v e n t i o n s - -25 5.5 Political approaches and structural challenges --25 5 . 6 L e g i s l a t i o n - -26 5 . 7 G l o b a l s t r a t e g y - -27 5.8 Reasons for current lack of activity or ineffectivelegislation and Implementation in South Asiancountries -- 27 6. Conclusion -- 27 7. References -- 28
1. Introduction 1.1 IndianSubcontinent
The Indian Subcontinent is a region of the Asiancontinent on the Indian tectonic plate south of theHimalayas, forming a land mass which extendssouthward into the Indian Ocean. It is also calledSouth-Asian subcontinent, Indo-Pak subcontinent orsimply South-Asia or the Subcontinent. Geographically,the Indian subcontinent is a peninsular region insouth-central Asia, rather resembling a diamond whichis delineated by the Himalayas on the north, the HinduKush in the west and Arakanese in the east; andwhich extends southward into the Indian Ocean withthe Arabian Sea to the southwest and the Bay ofBengal to the south-east. With all seven countriesincluded, the area covers about 4.4 million squarekilometres, which is 10% of the Asian continent or2.4% of the world's surface area. Some academicshold, that the term South Asia is more common in
Europe and America as compared to subcontinent orIndian subcontinent. A booklet published by the UnitedStates Department of State in 1959 includesAfghanistan, Ceylon (Sri Lanka), India, Nepal andPakistan as part of subcontinent region, “Indiansubcontinent”: Geology and Geography. The ColumbiaElectronic Encyclopaedia, 6th edition, ColumbiaUniversity Press, 2003”. Central Asia comprising ofPakistan, India, Bangladesh, Nepal , Bhutan, SriLanka and an island off the south eastern tip of theIndian peninsula is also, often considered as part ofthe subcontinent”.)
Historically forming the Greater Indian subcontinent orpart of British Empire were Pakistan, India,Bangladesh, Nepal, Offshore of Sri Lanka, Maldivesand Bhutan. The region also includes the disputedTerritory of Aksai Chin and Jammu and Kashmir whichare now controlled by Xinjiang province of China.Overall, it accounts for about 34% of world'spopulation. Here we consider only Afghanistan, India,Pakistan, Nepal, Bangladesh and Sri Lanka along withJammu and Kashmir as part of subcontinent. (AfterPartition: India, Pakistan, and Bangladesh. (BBC,2007-08-08).
1.2 Oral cancer
The term oral cavity refers to lips, buccal mucosa,alveolar ridges, retro molar trigone, hard palate, floorof the mouth and anterior two-thirds of the tongue.Oral cancer or oral cavity cancer, a subtype of headand neck cancer, is any cancerous tissue growthlocated in the oral cavity [3]. There are several typesof oral cancers, some being squamous cellcarcinomas, basal cell carcinomas, veraciouscarcinomas, nasopharyngeal carcinomas, malignantmelanoma, ameloblastoma, mucoepidermoidcarcinoma, and so on; around 90% are squamous cellcarcinomas, originating in the tissues that line themouth and lips. Many other different types ofcarcinomas of oral cavity can finally become malignantand result in a squamous cell carcinoma. Oral ormouth cancer most commonly involves the tongue. Itmay also occur on the floor of the mouth, cheek lining,gingiva (gums), lips, palate (roof of the mouth), maxillaor mandible. Most oral cancers look very similar underthe microscope and are called squamous cellcarcinoma. These are malignant and tend to spreadrapidly. These oral cancers are heterogeneous andarise from different parts of the oral cavity, withdifferent predisposing factors, prevalence, andtreatment outcomes. It is the sixth most commoncancer reported globally with an annual incidence of
WebmedCentral > Research articles Page 3 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
over 300,000 cases, of which 62% arise in developingcountries. There is a significant difference in theincidence of oral cancer in different regions of theworld. The age-adjusted rates of oral cancer vary fromover 20 per 100,000 populations in India, to 10 per100,000 in the United States, and less than 2 per100,000 in the Middle East [4]. In comparison with theU.S. population, where oral cavity cancer representsonly about 3% of malignancies, it accounts for over30% of all cancers in India. The variation in incidenceand pattern of oral cancer is due to regionaldifferences in the prevalence of risk factors. But sinceoral cancer has well-defined risk factors; these may bemodified giving real hope for primary prevention.Despite the fact that the oral cavity is accessible forvisual examination and that oral cancer andpremalignant lesions have well-defined clinicaldiagnostic features, oral cancers are typically detectedin their advanced stages. In fact, in India, 60-80% ofpatients present with advanced disease as comparedto 40% in developed countries. Consistent withpatients presenting for medical care with moreadvanced disease in India compared with developedcountries, overall survival is also reduced. Earlydetection would not only improve the cure rate, but itwould also lower the cost and morbidity associatedwith treatment. The precancerous lesions andconditions of oral cancer are a ray of hope inprevention.
The precancerous lesions are:1. Leukoplakia2. Erythroplakia3. Palatal changes amongst reverse smokers(smoker's palate)
The precancerous conditions are:1. Oral submucous fibrosis2. Oral lichen planus
The above mentioned conditions and lesions providean opportunity for early detection and thus helpprevent the malignant changes that may occur in themand then thus proceed to oral cancer. If diagnosed inthe early phase, stopping the tobacco habit canreverse the condition. Thus, if appropriate measuresfor early detection and with good public educationcarried out, nipping the problem in the bud would bepossible.
Classification of oral cancer is as follows:
Oral cancerClassification and external sources
ICD-10 C00.-C006.ICD-9 140-146DiseasesDB 9288MeSH D009959
International classification of oral tumors by Americansociety of cancer.
1.2.1 The internationalscenario for oral cancer
Cancer is the second most common cause ofmorbidity and mortality in the world today aftercardiovascular problems. Six million people die due tocancer every year. It is estimated that by 2020 therewill be 15 million new cases every year. Oral cancer isthe eleventh most common cancer in the world with anestimated 267,000 cases and 128,000 deaths inaround 2000, two-third of which occurs in developingcountries. The Indian subcontinent accounts forone-third of the world burden. The incidence from oralcancer is increasing in several parts of the worldparticularly in Australia, Japan and parts of Europe.Oro-pharyngeal cancer is a significant part of theglobal burden of cancer. Oral cancer occurrence isparticularly high in males. Incidence rates for oralcancer vary in men from 1 to 10 cases per 100,000populations in many countries. Tobacco and alcoholare regarded as the major causes for oral cancer.There are strong synergistic effects on oral cancer riskwhen a person is both a smoker and drinker. This riskis generally increased as compared to being smokeror drinker alone. The population-attributable risks ofsmoking and alcohol consumption have beenestimated to 80% for males, 61% for females, and74% overall. The evidence that smokeless tobaccocauses oral cancer was confirmed recently by theInternational Agency for Research on Cancer.Tobacco use, including smokeless tobacco, andexcessive alcohol intake estimated to account forabou t 90% o f o ra l cance rs . (Na i r MK,Sankaranarayanan R. Epidemiologic leads to cancercontrol in India. Cancer Causes Control. 1991 July,2(4):263-5). The 58th World Health AssemblyResolution on Cancer Prevention and Control(WHA58.22, 25 May 2005) urged member states todevelop and reinforce national cancer controlprogrammes, prioritizing preventable tumours and riskfactors intervention (http://screening.iarc.fr). Focus ison cancers amenable to early detection and treatment,such as oral cancer.
2. The scenario for oral cancer
WebmedCentral > Research articles Page 4 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
in Indian Subcontinent
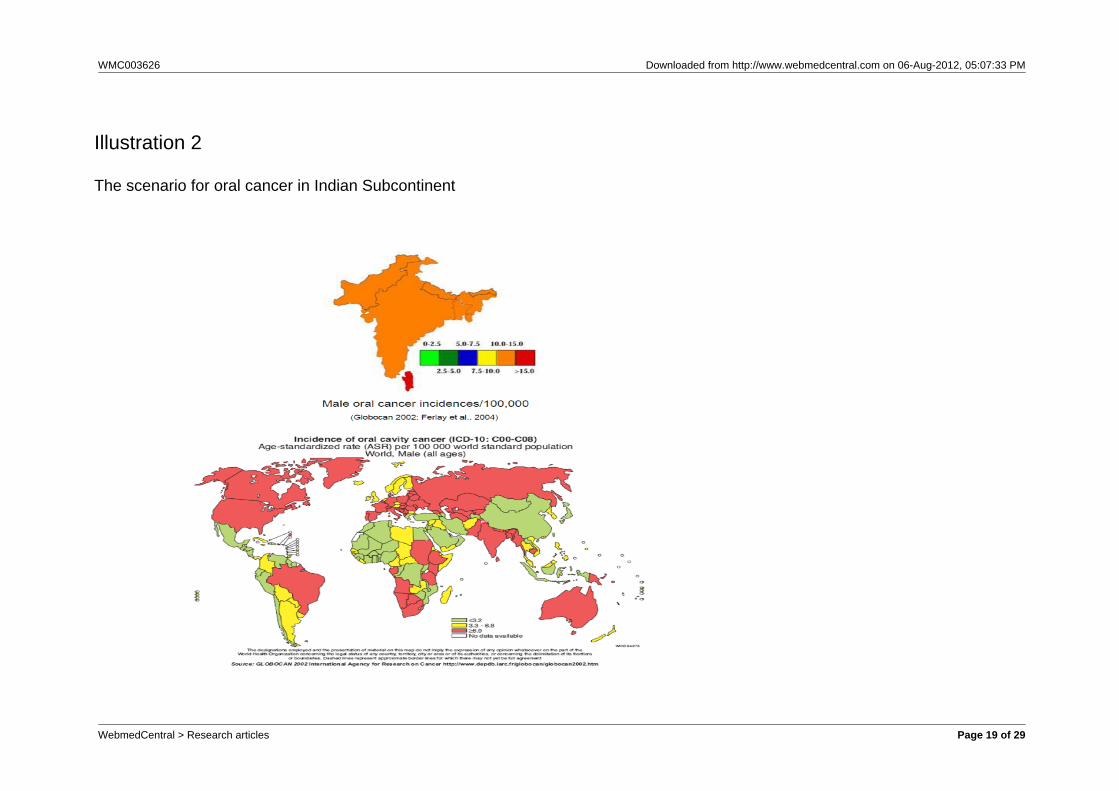
The problem of cancer is universal; the only variationoccurs in types, site or other clinicoepidemiologicparameters. Tobacco chewing was identified as itscause about century ago but continued practice andresearch proved it as the most important avoidablefactor of oral cancer. Head and neck cancers accountfor one of the fourth of all cancers in Indian males. Insouth Asia oral cancers account for about up to 40%of all cancers. In India the incidence of oral cancer isabout 3-7 times more common as compared toresource rich countries. India tops in the prevalence oforal cancer in the world and remains the commonestcancer amongst the male population. Oral cancer isthe third most common cancer in India after cervicaland breast cancer amongst women. In India, the agestandardized incidence rate of oral cancer is reportedat 12.6 per 100,000 people. The increased prevalenceof the oral cancer in the Indian subcontinent seems tobe due to the high exposure to sunlight due to farming,smoking and other smokeless tobacco habits, alcohol,spicy food, and neglect of overall oral health. It is saidthat one third of all oral cancers are preventable andone third of them occur due to risk factors. The highestage-adjusted incidence for oral cancer is highest inIndia, i.e. 15.7 per100, 000 and lowest in Japan whichis 0.2 per 100,000 and the difference is predominantlydue to use of tobacco between the two nations. In theWest, the cancer of tongue and floor of mouth iscommon whereas in Indian subcontinent the cancersof gingival and buccal mucosa are common due toplacement of tobacco quid in the oral cavity. Thiscancer of gingivobuccal complex is termed as Indianoral cancer (Oral Cancer Prevention and ResearchFoundation, India).
Human Papilloma Virus (HPV) especially types 16 and18 are known risk factors (there are over 100 variables)and independent causative factor for oral cancer(Gilsion et.al. John Hopkins).
Symptoms associated with oral cancer are asfollows:Skin lesions, lump or ulcer:1. On tongue, lips or other mouth area2. Usually small3. Most often pale colored, rarely dark or discoloured4. Early signs include white patch (Leukoplakia) or ared patch (Erythroplakia) on soft tissues of the mouth5. Usually painless initially but may develop withburning sensation as the tumour advances
Additional problems and symptoms associated withoral cancers maybe1. Tongue problems2. Swallowing difficulty3. Mouth sores that do not resolve in 14 days
Signs and tests for oral cancer: An examination ofthe mouth by a physician or dentist or other healthcare provider shows a visible and /or palpable mass orlesion on the lip, tongue or mouth. A tissue biopsy ofthe lip or tongue or other oral tissues and microscopicexamination of the lesion confirms the diagnosis oforal cancer. The person may develop difficulty inspeaking and swallowing with oral cancer.
The information emerging from Vietnam and Chinaindicate that oral cancer incidence have tripled since1980, partly due to chewing of betel quid althoughtobacco is generally not added to betel quid in theseregions. In some parts of Pakistan, Afghanistan andIndia it is the leading cancer in men and third mostcommon cancer in females in these areas. Culturaland hereditary factors are considered as risk factors inthese parts and along with that, a lack of awareness,poor oral hygiene and fruit and vegetable lacking dietsare also important risk factors in this connection. Oralcancer is common form of cancer and accounts formuch of cancer related deaths in Indian males. (SujhaSubramanian et.al, Bulletin of the World HealthO r g a n i z a t i o n ; R e s e a r c h A r t i c l e D O I :10.2471/BLT.08.053231).
In case of oral cancer the greatest risk factor istobacco. It is important to mention here that tobacco isalso one of the largest causes of preventable deaths inthe world.1. The relation of oral cancer with tobacco is wellestablished and documented. Since 1985, eight casecontrol studies conducted in India have given evidenceof the role of tobacco smoking and chewing in oralcancer causation. Five of these studies reportedsignificant estimated relative risks (as odds ratios) tocurrent chewers of paan with tobacco compared tonon-chewers, in men the relative risk varied from 1.8(95% CI: 1.2-2.7) to 5.8 (95% CI: 3.6-9.5) ( Rao andDesai ,1998; Rao et al., 1994; Nandakumar et al.,1990; Balaram et al., 2002; Dikshit and Kanhere, 2000)and the values for women ranged from 30.4 (95% CI:12.6-73.4) for current chewers to 42.4 (95% CI:23.8-75.6), chewers in the two studies that includedwomen (Nandakumar et al., 2000 and Balaram et al.,2002).2. The risk of developing oral cancer is high in casesof chewable tobacco. The incidence of oral cancer is
WebmedCentral > Research articles Page 5 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
highest of all cancer amongst men (12%) as comparedto women (8%).3. Smoking may also lead to development of oralcancer; however the chances of laryngeal cancers aremore in case of smoking rather than oral cancer.4. Paan (chewable leaf tobacco mainly in Pakistan,India and Bangladesh) is said to be the most potentrisk factor for the development of oral cancer. Thecombination of Areca nut, lime and tobacco is thepossible reason behind the increased risk.5. A case control study conducted in India revealedthat the chances of development of oral canceramongst men who were tobacco chewers were six foldhigher than non-chewers. As far as the femalepopulation was concerned the risk was as high as 46times more in females who had never chewed tobacco.6. Other than life style factors, there are physicalfactors like radiations which have also beenassociated with oral cancer and exposure to x-rays.7. Since risk factor is so profound and well established,undoubtedly curbing the use of tobacco is one of themajor steps to prevent oral cancer occurrence(http://www.xomba.com/user/rawnak).8. The increasing use of tobacco amongst the youngerpopulations and children along with lack of oralhygiene has largely contributed to the sharp increasei n t h e o c c u r r e n c e o f o r a l c a n c e r(http://www.xomba.com/user/rawnak).9. Nutritional factors like diet that is deficient in fruitsand vegetables could further increase the risk.10. Biological factors include viral and fungal infections.HPV type 16 is mostly associated with the oralcancers which occur on the back of the tongue(http://www.xomba.com/user/rawnak).11. One of the prominent factors associated with it isage (usually above 40 years).
Recently, a study from India demonstrated that oralcancer screening by trained health workers can lowermortality of the disease especially in individuals with ahistory of tobacco use [6]. In this randomized,controlled trial of almost 192,000 people, carried outover an eight-year period, there was a significantreduction in mortality in the intervention arm (29.9cases per 100,000) versus the control arm (45.4 casesper 100,000), due to detection of oral cancer at anearly stage. A cost-effectiveness analysis revealedthat an oral cancer visual inspection by trained healthworkers can be carried out for under U.S. $6 perperson. The incremental cost per life-year saved wasU.S. $835 for the all-screened population and U.S.$156 in the high-risk population – namely, individualswith a tobacco habit (Zeb et al, 2006; 2008). Currentusers of nasal snuff a product which is relatively
uncommon now faced a relative risk of 3.9 (p<0.05) forcancer o f g ing iva (gums) in one s tudy(Sankaranarayanan et al., 1989a,) and elevated butnot significant in another study on buccal mucosa, i.e.cheeks and lips (Sankaranarayanan et al., 1990b).The use of tobacco with lime was associated with oraland oropharyngeal cancer in a study conducted inPakistan with a relative risk of 10.4 for women and13.7 for men compared to those who neither chewednor smoked (Jafarey et al., 1977).
2.1 Cancer registration in theSubcontinent
Cancer registries have been active in the region formany years, with Mumbai being listed in the CancerIncidence in Five Continents from volume II in 1972(see Table 1) and there were a total of eight registriesincluded in the International Agency for Research onCancer compilation in 2002. However, all but theSouth Karachi registry are in India, and thereforerecourse has been made in the present report toGlobocan 2002 for comparison across countries. Theactual registries now in operation are illustrated inFigure 1. The overall mortality, incidence andprevalence of all cancers (not only oral cancers) canbe seen in the different regions in Figure 2.
The available population based data has beenpresented in Tables 2 and 3 and the most prevalentcancers have been shown in terms of percentage forwhole region in Figure 3. Besides Globocan and CIV,partial data has also been available for city or regionbased on registries in Quetta (Bhurgri et al., 2005) and (Bhurgri et al., 2000) for Karachi in Pakistan ,Allahabad (Mehrotra et al., 2008) and Kolkata (Sen etal., 2006) in India and multiple institutes in Nepal (Pradhananga et al., 2009).
High rates of oral cancers have been reported inNepal (Baskota et al., 2005) and in Indian tea estatelabourers in Sri Lanka (Ariyawardana et al., 2007).This in turn reflects the type of exposure to known riskfactors such as betal quid, Areca nut with or withoutAspergillus contamination and chewing or other formsof tobacco (Bhurgri et al., 2003b; Patel et al., 2007;Basu et al., 2008). In some situations alcohol mightplay a role rather than tobacco (Thomas et al., 2003).A history of diabetes mellitus may also predispose(Dikshit et al., 2006) while high socioeconomic statusis protective (Hashibe et al., 2003). The incidence ofboth tongue and oral cancers are decreasing in Indiaalthough they are both independent of each other asshown in Figure 4 & 5.
WebmedCentral > Research articles Page 6 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
3.1 The vision
To create a South Asian Oral Cancer Foundation(SAOCF) and to become a regional authority incombating the burden of oral cancer throughprevention, early diagnosis, treatment andrehabilitation and set an example of dedicated servicethrough futuristic science, to the internationalcommunity.
3.2 The mission
To create a region, free from oral cancer:1. The mission of SAOCF is to l iberate theSubcontinent from the deadly claws of oral cancer,especially in view of the fact that our region tops theFigures of oral cancer sufferers
We aim to accomplish our mission by:1. Establishing a chain of centres across the regionand making the service for oral cancer prevention andearly detection, accessible to all the citizens of theSubcontinent.2. Prevention, in view of the fact that it is the only curefor oral cancer, would remain the mainstay.3. Bringing about development of dental professionalsby training them in the latest oral cancer detectiontechniques, thus making it possible for them to preventoral cancer through early detection.4. Aiding development and providing support tomultidisciplinary approach in scientific and researchrelated activities in the field of oral cancer detectionand prevention.5. Providing necessary support for conducting oralcancer research and to make provisions for timelytransfer of the research outcomes for practicalapplication.6. A coordination of various agencies and relatedorganizations for establishing a multidisciplinaryapproach to face the challenge of oral cancer.
3.3 Core values
In our efforts to provide service for oral cancer, we willgive priority to improvement of scientific technologiesand making them available to the people via dentalprofessionals, based on the following core values.
3.3.1 Science
Our programmes and activities to support oral cancertraining for the dental professionals, and informationdissemination will be carried out on scientific basis
3.3.2 Trust
Our resources and programmes will be managed,conducted, and evaluated in a manner that upholdsthe trust placed in us by the people.
3.3.3 Society
Our programmes and actions will aim to improvehealth, especially oral health, of all people through aservice that provides both prevention and treatment oforal cancer.
3.4 Overview
The SAOCF's Strategic Plan is to make theSubcontinent, a region free from oral cancer. Thedriving forces behind our plan are to adopt neededchange and to respond to the needs of the people weserve. Just as we initiate this programme, we embarkon the strategic plan mindful of the momentum withwhich the epidemic of oral cancer is spreading, thetrends that are involved and the means by which wecan encourage people to consider health as theirpriority and ensure that they have the access to thebest services, which can benefit the region. Thisstrategic plan is drafted in a way that addresses themultitude of challenges that tobacco intervention canoffer. The goals and objectives of this plan are centredon:1. Knowledge that will help us in understandingdisease processes, their underlying causes as well asthe concepts that determine population dynamicsrelated to those diseases.2. Advances in oral cancer detection techniques thatprovide means for early diagnosis of pre-cancerousand cancerous lesions, with ease and precision. Alsoensuring dissemination of the advanced science forprofessional development.3. Innovation and development of excellentcommunication infrastructure that would enable us topropagate the message of prevention and earlydetection and simultaneously help dental professionalsto get connected to the community directly and provide
WebmedCentral > Research articles Page 7 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
them education as well as service.4. The plan is to set forth an aggressive agenda toenhance training and development of members. TheDental Associations and Dental Councils of memberstates recognizes the need to translate advances andprogress for bringing excellence in service through thecommunication of the information to healthprofessionals, professional organizations, and to thepublic, through organized efforts.
3.5 Curing oral cancer
1. Putting a stop to the soaring statistics of oral cancerin the region and considering the face that India ranksfirst in the prevalence of oral cancer, has raised theneed to curb the disease.2. Curing oral cancer is an ambitious goal of SAOCF,which is sought to be achieved through early detectionand prevention. SAOCF also recognizes theimportance of partnerships in mobilizing an integratedhealth promotion enterprise comprising healthprofessionals, voluntary health organizations, industryand government.3. To combat the rapid growth of oral cancer statisticswill require a greater ability to learn and absorb newtechniques and create a sound infrastructure forservice through the centres.
3.6 Facing the challenge oftobacco
1. The functions of taste, expression of feelings,speech and its contribution to aesthetics, to a largeextent, make the oral cavity a unique organ.2. Dental professionals are closely associated with thehealth of this complex environment. The challenge oralcancer poses is increased threat not only to the healthof oral cavity, but to overall health. The increasingmorbidity and mortality associated with this oraldisease has made the health of oral cavity a cause ofgreat concern.3. In the context of increasing threat of oral cancer andthe importance of dental professionals in its preventionand early detection, SAOCF will take a step forward ina unique way.4. Also, to strengthen the stand of the tobaccointervention initiative, we seek to bridge the gapsbetween various professionals and their organizations,by establishing active communication with them andusing various media for the same.5. With the efforts to strengthen the foothold of thedentists and the summation of the ongoing efforts of
the various professionals and organizations we aim toreach the summit of our mission. It won't be difficult toimagine a day, when oral cancer and the associatedmorbidity and mortality will become non-existent,resulting in humanity living healthier and moreproductive life.
3.7 Building capacity throughco-ordination
1. The unique role of the SAOCF in oral cancerprevention and early detection, attributing to its targetprofessionals and the mode of function, is its greatestprospect for its leadership role.2. The combination of oral cancer prevention, earlydetection, cure and promotion of oral health,consequently overall health, enables the SAOCF todiversify its goal. Enrooting the goal in variousprofessions and disciplines would help us materialize it.3. Providing the necessary training to strengthen oralhealth professionals in oral cancer will help us in thedevelopment of an effective task force against oralcancer. It is equally essential to communicate theinitiative to the people so as to make them realize thepotential health benefit that such a step would have.This further strengthens the role of the dentalprofessionals against cancer.
3.8 Sustaining the uniqueness
To achieve our vision and attaining the ultimate goal ofmaking the Subcontinent a cancer free region, ourdiverse investments and coordination with variousdisciplines need to be carefully balanced.1. Although we seek to undertake multidisciplinaryaction through a multidisciplinary task force, the visionand strategies, adopted and executed through thediverse professional groups, with the dental professionassuming the central role, is what makes our effortsunique.2. It is through this uniqueness that we aim to assumeleadership and set an example for all professionalorganizations to cooperate and coordinate with themin their efforts.
3.9 Other challenges
Oral cancer is not a disease that affects the healthalone. It also affects the socio-economic life of thepatient. Similarly, the burden of prevention, treatmentand rehabilitation of the disease is also felt on the
WebmedCentral > Research articles Page 8 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
national economy.
3.9.1 Psychological aspects
1. The very sound and the idea of the word "cancer" isenough to put the strongest person in despair. Theeffect of the word on the personality of the personstarts right from the time a biopsy is demanded for thediagnosis; with heightened anxiety till the reportsarrive.2. Once the patient is confirmed to have oral cancer oreven for that matter pre-malignant lesion, the role ofthe doctors/dentists is very crucial.3. The deleterious effect of oral cancer on thepsychosocial well being of the patient is one of themajor challenges faced by doctors. Also, if the canceris treated once, the fear of recurrence or relapsecurtails the person's happiness and confidence.4. The effect of cancer surgery that leads to thedisfigurement of face, changes the complete insigniaof the person. SAOCF aims to address theseproblems by training dental professionals to deal withthese aspects of cancer.
3.9.2 Economic aspect
1. The effect of oral cancer treatment takes a heavytoll on the financial condition of the person. Thetreatment is expensive, apart from its side effects.2. Oral cancer is now shifted from the high incomecountries to middle and low income countries, whichalready suffer from dearth of resources. India has themaximum number of oral cancer sufferers and theresources to serve such a huge number remain limited.3. The most pragmatic answer to such a situation isPREVENTION. The SAOCF aims at prevention andearly detection. Before the disease reaches the stateof higher morbidity and mortality, it has to beprevented or identified early and treated effectively.4. Prevention and early detection is the SAOCF'sanswer for the economic impact of the disease.
4.1 Addressing the variousaspects:
1. We will continue this battle against cancer and itswidespread ill effects on health and its other aspectsas well.2. Enabling the people to lead a healthy life in ahealthy environment needs a multilateral andmultidisciplinary approach.
3. Efforts to enable people to combat oral cancer willbe carried out in a way that educates them and makesthem aware of the pre-malignant lesions andconditions so that they can approach healthprofessionals at the right time and can get the righttreatment.4. Lack of awareness, misconceptions that culminateinto late detection of the disease will be addressedwith all our might, through our well reached serviceand extensive awareness programmes.5. To extend our network to every citizen through aninfrastructure of centre chain and the awarenessprogrammes is our noble and prime goal. Through thiswe seek an enhanced interaction and support from themasses, so that the SAOCF becomes strong and rockstable on which we would build a healthy geographicregion.
4.2 Building competencies:
1. With significant research and advancement in oralcancer detection and treatment techniques, there is anincreased responsibility to get them reaching to all theprofessionals and oral health professionals in specific.2. To bring about an improvement in every dentalclinic and skills of every dental professional needs avariety of flexible and innovative training programmesfor early detection and diagnosis of oral cancer so thata competent task force, for addressing every aspect oftobacco can be set-up.3. Carrying out research and development and gettinginto the mainstream poses an array of challenges thatneed to be dealt with, if the outcomes of the researchare to be adapted to benefit the common people.
4.3 Bridging research andpractical efforts:
1. Despite the fact that oral cancer and itsconsequences can be totally prevented, treated andcontrolled, there exists a significant gap in the public'sknowledge, attitudes and behaviours. Variouspreventive measures that can significantly reduce theoral cancer burden, contribute to bridging the gapbetween research and development and publicawareness.2. To get knowledge disseminated in a way that willhelp people adopt behaviour patterns, which willimprove their health and of those associated with them,and help them make appropriate decisions. Anenhanced and sound system of communication, whichutilizes all the measures and methods for timely
WebmedCentral > Research articles Page 9 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
knowledge and information sharing, will be set-up.3. SAOCF will take efforts, not only to equip theprofessionals with knowledge and skill, but also to getthem connected with the population in an effectivemanner, which can educate and make them aware.
4.4 Facing the burden of thedisease:
The far reaching efforts of oral cancer on the physical,social, psychological and economic well being of aperson and the increasing number of affected people,pose a huge challenge.1. The increasing number of people affected by thedisease, most of who belong to the weakersocio-economic section, has made it difficult to reachthe affected people.2. The increase in the prevalence of risk factor andsusceptible behaviour in the society has turned thedemographics to a greater number of younger andpoorer sufferers. An intensified approach for theprevention of risk factors and behaviour is the need ofthe day. The younger population especially needs tobe protected.
4.5 Addressing disparities:
Oral cancer has now become a greater threat becauseit is affecting people who belong to the lowersocio-economic strata. They have very limited accessto education, prevention and treatment. This segmentof the population is more vulnerable to oral cancerbecause of higher exposure to the risk factor (tobacco)which complicates the situation further. This shows theglaring disparities that would result in oral cancerstatistics. In order to bridge these disparities, SAOCFwill direct its action towards:1. Provision of easy and accessible, detection andtreatment services.2. Awareness and education programmes.3. Prevention through action against risk factors,especially tobacco.4. Provision of educational resources to both theprofessionals and public.
4.6 Professional workforce:
1. Adequately trained professionals are the lifeblood ofeducation, practice and research. Researchers,educators, and practitioners should reflect the diversityof the oral cancer challenge in the region and thus
have a broad mix of skills.2. There is a variation in the oral cancer distributionacross the region and its diverse communities.However, the research and professional dentalworkforce does not adequately represent thecomposition and the diversity of the country.3. Data show that under-represented minority dentistsplay a large role in increasing access to underserveand minority populations. They can influence otherhealth professionals to be more culturally sensitive,and serve as role models to other minorities and towould-be educators or researchers.4. To achieve proper coverage in the rural areas, alltrained dental health professionals after completion oftheir course have to do a 1 year compulsory workposting in rural areas, which will be paid according tothe government regulations.5. In terms of diversity, the magnitude of the challengeis perhaps best expressed by looking at the "pipeline",or the number of under-represented minority dentistsand students in the dental schools.6. Sustained efforts, new partnerships, and innovativeand flexible programmes are needed to ensure acompetent, diverse and robust research workforce.7. There is thus a need for a diverse and equaldistribution of personnel to face the challenge.
4.7 Strengthening theresearch base:
1. Strong research-oriented academic environmentsare needed to develop the intellectual talent forresearch, and to enable existing investigators toacquire and expand their skills in new areas of science.2. Oral health research can be carried out in a numberof settings including dental schools, differentcomponents of academic health centres, hospitals andindependent research institutions.3. The capacity of dental schools to conduct researchand to serve as training grounds for future researchersis important for the future of clinical and applied oralhealth research.4. However, major barriers must be overcome. Theseinclude a critical shortage of faculty, a lack ofintegration between the basic and clinical sciences inpre-doctoral programs, inadequate incorporation ofresearch into the dental curriculum, and financialshortfalls.5. Efforts to bolster the research infrastructure toensure a workforce that is adequate both in numbersand ability, is needed to meet the demands of thechanging oral health needs of the community.
WebmedCentral > Research articles Page 10 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
4.8 Creation of a platform forunited efforts:
1. Creation of a platform that allows activities andinputs from professionals from diverse backgrounds isessential for compilation and maximization of effortsand outcomes.2. It is vital to set-up a dynamic platform andundertake multilateral and inclusive research forcompiling a tangible evidence base, which canultimately benefit the common man.3. Utilizing the different modes of media andcommunication to translate research into practicalbenefit.4. Thus such a dynamic and inclusive platform wouldprovide for activities as well as resultant benefits.
4.9 Creating media and publicawareness:
1. As defined in Healthy People 2010, healthcommunication "encompasses the study and use ofcommunication strategies to inform and influenceindividual and community decisions to enhancehealth."2. Based on the above definition, communicationefforts are meant to ensure that target audiencesbecome informed, change behaviour, and makedecisions that will improve clinical care and healthoutcomes.3. Target audiences include health care providers,consumers, the research community, and other groupssuch as educators, policymakers, industry, and themedia.4. One of the main challenges of our healthcommunication efforts is to find the most effectiveways to communicate and disseminate healthinformation, clinical information and research findings,to target audiences.
4.10 Establishing anddeveloping collaborations:
1. The changing needs of the region, have unfoldedmany challenges and possibilities that need to betaken into consideration. Thanks to this fact, thenecessity to collaborate with the various channels oftechnical expertise cannot be overlooked orunderest imated. Thus for developing thecollaborations network SAOCF has set up the
following Goals2. Establishing communications with key stake holdersand informing them at the right time about our variousinitiatives and developments. Communication of thisnature will not get SAOCF the recognition of being oneamong various professional bodies. The recognitionand acknowledgement of our work is the key to thediversification of our vision and goal.3. In course of our efforts for establishing our identityand gaining recognition as one among variousprofessional and scientific bodies, SAOCF will do itslevel best to contribute to various disciplines throughour knowledge base and built capacity.4. The association that we seek with the variousprofessional and scientific bodies would be bilateral.Through our activities and investments in variousdisciplines, we will also attract interest andinvestments from these disciplines in SAOCF.5. This nature of association will result in multi-lateralbenefits and development.
4.11 Creating and upgradingtangible evidence base:
1. The provisions that are made on the SAOCFwebsite provide an excellent resource for creation of atangible data base. To make the facility more effective,we have set the following goals.2. The provisions available through the website shouldbe made suitable for use; this will be the first target ofthe preliminary stage. To achieve this task, we willprovide training to professionals for using the provision.Also, we aim to make the modules for the people easyand self explanatory.3. Unless these two are not implemented together, theutilization will be restricted to net savvy people inmetros and large cities.4. A thorough training of importance and utilization ofthe SAOCF provisions is vital. It should be done at theright time and in the right way.5. There have been efforts right from the time ofpreliminary development of the website that provisionsof the initial questionnaires that are asked to thepatients record accurate data; similarly, throughout thepatient dentist interaction, the data quality ismaintained.6. Once the initial modules are implemented, qualityimprovement of the questionnaire will begin, based onresponse to the first stage.7. Creation of a large evidence base needs a gooddeal of documentation. The process will not becomplete, unless the data collected is sorted andanalyzed.
WebmedCentral > Research articles Page 11 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
8. Efforts will be made to put the data in the correctpockets. The data base thus generated will be morepractical and helpful.9. A well managed and tangible evidence basecreation needs efforts from the preliminary stagesitself.
5. Experience with technicaland policy solutions
Non communicable diseases such as cancer areemerging as the main challenge and major publichealth problems in India. These diseases are mostlylife style related and have a long latent period andneed special infrastructure and personals and humanresources for managing it. Population based registrieswithin the National Cancer Registry programme andoutside the network has provided a picture of thepatterns of cancer in India, though it does notrepresent all areas in India but only some parts of it asshown in the Figure 6. The number of new cancers inIndia annually is presented in table 5.
Following are the different type of interventions whichcan be applied in reduction and cure of oral cancer inSouth Asia.
5.1.1 Primary prevention
Primary prevention eliminates exposure to the riskfactors or cancer causing agents. Primary preventionsfor the type of cancers that are of greatest concern indeveloping countries are immunization against thecausative agents and treating infectious agents,implementing dietary interventions , introducingtobacco control programmers, reducing excessivealcohol consumption and using chemoprophylaxis.Oral Submucous Fibrosis (OSF) is a condition which isdebilitating and potentially cancerous is causedprimarily by chewing areca nuts and its mixtures asdemonstrated by numerous studies and otherevidences (Murti et al., 1995). The condition mayextend sometimes beyond mouth to oesophagus(Misra et al., 1998). The high malignant potential ofOSF is well established (Murti et al., 1985). Assmoking is one of the main causes of oral cancer soprimary prevention is one of the best interventions toreduce the risk of oral cancers by minimizing the useof tobacco.
5.1.2 Cost effectiveness of
primary prevention
The cost effectiveness studies of primary preventiveintervention are relatively rare and are mostly availablein high income countries. For example studies in theUnited Kingdom (UK) and United States of America(USA) shows that the costs of treating and screeningof an individual for helicobacter pylori infection toreduce the risk of stomach cancer ranges from US$25,000 to US$ 50,000 per life year saved but anotherstudy showed that the cost effectiveness of theintervention would be more in Columbia where thecost of health care interventions are less and stomachcancers are common. In a study on costs of tobaccorelated cancers for the ICMR (Tata Memorial center,Mumbai, India), the direct and medical and nonmedical costs like travelling and indirect costs , likeloss of income during treatment and premature deathwere assessed in a cohort of 195 oral cancer patientsfor three years from 1990. The average total costs percancer patient, discounted at the 1999 level amountedto be about 350,000 Indian rupees with direct costsamounting to 13% of total costs. The costs of 163 500total tobacco related cancers diagnosed in India in1999 as estimated for this study amounted to beabout Rs. 57,225 billion (ICMR,2001). Apart fromfinancial costs tobacco users have a higher risk ofpremature death as compared to nonusers. In aretrospective study conducted in Chennai (India), therelative risk of death in men who were smokers was2.1 (Gajalakshmi and Peto, 2002). Thus anti-tobaccointervention is one of the most cost-effective andbeneficial intervention to prevent cancer and cancerrelated deaths besides many other diseases. In factmany longitudinal studies have shown that the risk oflung cancer decreases slowly after quitting smoking tillit reaches to the level of nonsmokers after 10 years ofquitting (IARC, 1986).
5.1.3 Community interventions
A large controlled educational intervention trial in threestates of India with ten years of annual follow up wasconducted during 1967-88. Messages impartedthrough personnel communication were reinforced bydocumentaries, slides, posters, exhibitions, folkdramas, radio messages and newspapers articles(Gupta et al. 1986a). The educational intervention wassignificantly effective in decreasing the use of tobaccoand increased the quitting rate of smoking in two areas(Ernakulum, Kerala and Srikakulam, Andhra Pradesh),assessed after five and ten years of follow up (9% and
WebmedCentral > Research articles Page 12 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
14.3% in Ernakulum and 17% and 18.3 in Srikakulam).This resulted in the substantial reduction in theincidence of Leukoplakia, a precancerous lesion toonly 40- 60% of the incidence rate in the interventionarea with smoking having higher level of reductionthan the chewing group (Gupta et al, 1992). Within theintervention area the incidence of oral lesions was lessin those who gave up smoking habit (Gupta et al,1995). These results underscore the great potential forprimary prevention of oral lesions and cancers throughanti-tobacco interventions and cessation of tobaccouse. In a similar intervention study conducted in SriLanka, the quit rates after 5 years of intervention inmen and women respectively were 26.5% and 36.7%compared to 1.1% and 1.5% in a control cohort(Anantha et al, 1995).
5.1.4 Mass media intervention
Media plays a very important role now adays so ifeffectively used it can be of significant use to mobilizethe mass and create awareness among the generalpublic about the risks of smoking and its hazards.Newspapers, Television, radio and internet all can beused for this purpose for conveying the message tothe general public. In 1990, information about thehazards of tobacco were broadcasted on All IndiaRadio (the only radio medium at that time), through 30Sunday morning episodes in 16 languages from 84stations. Community surveys in two states showedabout 30% listenership among the potential audiencein both states where in Karnataka about 6% of thelisteners reported to have quitted smoking and 4.3% inGoa. In addition about one third of tobacco usersintended to quit and another third had reduced theirconsumption and intended to quit as well (Chaudhary,1994). This clearly states that radio communicationhad potential benefits even during 1990,s where theway of communication was less and media was not asdeveloped as today as most of the people today haveaccess to some sort of communicatory media eitherinternet or radio or Television or newspapers. Besidesradio and television, newspapers can also be used toconvey anti-tobacco message through articles onsmoking hazards and different cartoons to reflect itshazards and to encourage the public to avoid tobaccouse.
5.1.5 Sufficient evidence forlong term oral cancer riskreduction for the South Asian
region
All the above efforts points to the utility of scaling upsimilar educational efforts through incorporating theminto routine regional government’s health programmesand mass communication and to add anti-tobaccoeducation in schools curriculum. Besides this thereshould be made voluntary organizations and theseorganizations can also play a role in educating thepeople about smoking and tobacco hazards and thusthey can make a difference as well.
5.1.6 Secondary prevention
Secondary prevention consists of screeningprogrammes to detect and treat precursors of oralcancer thus preventing or reducing the incidence ofhighly invasive cancers. Effective screening can detectinvasive cancers very early and thus improve thelikelihood that treatment will be successful. The costeffectiveness of secondary prevention depends onmany factors including the costs of diagnostic tests,the prevalence of disease and the availability ofeffective treatments.
5.1.7 Cost effectiveness ofsecondary prevention
The cost effectiveness of secondary prevention fororal cancer ranges from US$ 1300 to US$ 6,200 peryear of life saved. (Jamison DT, Breman JG, et al,editors. Washington (DC), World Bank, NCBI, 2006).
5.1.8 Medical interventions
Medical interventions include surgical removal of thetumors, chemotherapy and radiation. As compared tooral cancer treatment cost effectiveness, the costeffectiveness of treatment for stomach andesophageal cancers are worse and ranges from US$53,000 to US$ 163,000 per year of life saved. Ingeneral the standard of treatment in developingcountries is less well organized and not available toeverybody due to its costs as compared to developedcountries. The preventive interventions are alsodifferent in developing and developed countries withbetter preventive interventions in developed countries.The availability of cost effective methods of preventionand treatment for cancers in low and middle incomecountries varies significantly depending on the type of
WebmedCentral > Research articles Page 13 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
cancer, with a substantial effects on the equity of theoutcomes.
5.2 Programmatic approachand structural challenges
As smoking is one of the major causes and risk factorsfor oral cancer in South Asia so the South Asiangovernments i.e. Pakistan, India, Bangladesh, SriLanka, Nepal, Maldives and Jammu and Kashmir haveall launched different awareness programmers atdifferent levels to discourage smoking and createawareness among people to avoid smoking anddevelop clean habits. These programmes range fromadvertisements on Television, Radios and newspapersto work shops and posters preparation and organizingrallies and seminars in different places andinstitutions about smoking and its adverse effects onhealth and as a possible risk factor not only for oralcancer but also lung cancer,oesophygeal cancer andother cancers. In few Indian and few states of Nepalshopkeepers are informed not to sell cigarettes toyoungsters below 16 years of age but these is nolegislation passed about it yet in any of these countries.The basic problem in this part of the world is that mostpeople are illiterate and they do not have access toTelevision and radios so they don’t get the properawareness about it. The problem in the educatedpopulation is that they are although aware of theeffects of it but they either use it as a fashion or torelive stress. Both in India and Pakistan, there is banon smoking in public places but rarely seen to befollowed or obeyed by people and there is less actionfrom the government or legislative authorities againstthose who disobey or violate the roles. There areprogrammes about adverse effects of smoking onTelevision but as most of these cigarette companiesare international companies so they get the statetelevision and other private channels easily hired forpublicity of their cigarettes and other tobaccos. Thereneeds to be strict legislation against smoking fromthese regional governments and those who do notabide by the law should be punished. Smokingadvertisements should be banned on television andradios and strong anti smoking campaigns should belaunched. More awareness needs to be createdamongst the public about smoking hazards andsmoking should be strictly banned in all public placesand those found guilty of disobeying the law should befined. Besides antismoking campaign more is neededto be done in creating awareness among the generalpopulation about regular use of brush and tooth paste,use of less Paans (chewable form of tobacco in the
subcontinent) and discourage the use of Alcohol.
5.3 Tobacco cessation clinics
Although informal tobacco cessation clinics have beenin use in Pakistan, India, Sri Lanka and Bangladeshfor longtime but no evaluation reports are availablefrom any of these countries. The recent of availabilityof nicotine replacement therapy in the shape ofnicotine patches and Buproprion has prompted severalhealth facilities to set up tobacco cessation clinics forpeople who want to quit smoking but cannot do it ontheir own. These clinics are mostly funded by theregional governments and some of them are alsoworking in private sector and these clinics employpharmacologic therapy in addition to behaviouraltherapy which may include different strategies rangingfrom telephone calls, individual counselling, rationalemotive therapy and yoga with pranayam which hasshown encouraging results (Shastri, et al, 2003).
5.4 Economic interventions
Economic analysis by several agencies has shownthat tobacco is a net drain on an economy. Demandside interventions such as advertising and promotionbans, smoking restrictions as well as increase in pricethrough taxation are all effective at reducing tobaccorelated oral cancers, mortality and morbidity.Measures to reduce the supply of tobacco in thesecountries have been met with less success except incontrol of smuggling to some extent but neverthelessaids given to farmers in some parts of these countrieshave seen a shift amongst the farmers from tobaccocultivation to other crops cultivation and thus furthersteps must be taken to encourage the farmers tocultivate other crops instead of tobacco. The farmersshould be given special aid for this as once suggestedby World Bank as well in 1999 (World Bank, 1999).Research carried out in Indian state of Karnataka hasshown the willingness of framers to shift from tobaccocultivation to other crops like dairying and cotton cropsif given some aid and assistance by the government(Panchamukhi, 2002). Additionally phasing outgovernment support to tobacco production and findingsubstitute crops for revenue generation and export willaid in the transition to a tobacco free society.
5.5 Political approaches andstructural challenges
WebmedCentral > Research articles Page 14 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
The South Asian governments are taking steps onindividual levels to counter the risk of oral cancer andsmoking but not much on regional level and together.These include more taxes on tobaccos imports,decreasing the subsidies for tobaccos and increasingthe cost of cigarettes so that people can bediscouraged from smoking. As south Asia and Pacificaccounts for the highest smoking related deaths in theworld about 40%. Men are common smokers in thispart of the world and females are rare smokers in thisregion whereas this gap is narrow in high incomecountries mainly Europe and America. About 1.1billion people smoke currently and about four- fifths ofthese are residing in the low and middle incomecountries. Nearly all the South Asian governments areimplementing more taxes on cigarettes and tobacco toraise the cost of the habit and discourage smoking thisway. Only educating consumers that tobacco orsmoking is injurious to health is not sufficient as mostlythe people underestimate the future risk to their healthand young people are more prone to develop andadopt to risky behaviors and life styles. Although mostof these countries have done some sort of legislationto ban smoking in public places, implement high taxeson tobacco but more efforts are needed and moresteps should be taken be these regional governments.Intervention proven effects can be to increase thetaxes on tobacco, disseminating information abouthealth risks in the general public, restricting smoking inpublic places, banning advertising and increasingaccess to therapies. Some governments in thedeveloping countries are using the tobacco tax evenfor health care purposes.
Government interventions that could affect people’sattitudes towards smoking and knowledge about thehazards of smoking can also be very helpful. Ascigarettes are the most widely publicized products inthe world so strong anti smoking campaign in thepublic alongwith education and information campaignscan counter this hazardous effect of smoking. Thesegovernments can also publicize reports about smokinghazards through health ministry and directing all thesmoking manufacturer companies to put warninglabels on packages, broadcasting antismokingmessages in the media.
The governments can also provide nicotinereplacement tablets at low costs to smokers so thatthey can quit the habit of smoking. The challenge hereis that most of these governments take money fromthese companies while issuing licenses beforelaunching their products and also take financial aidfrom these companies during their election campaigns.
These tobacco manufacturers also provide money tomedia to promote their products and advertise theirtobacco products. Fortunately most demand sideinterventions are cost effective and even cost savingas well. A 70 % increase in the price of tobacco couldavert 10- 26 % of all smoking related deaths worldwide.Successful interventions in Poland and South Africawent well even with the modest increase in price,almost doubling the prices over short time (DCP2,Chapter 8; Levine and others 2004). Despite the priceincrease being the most cost effective measure tocounter tobacco consumption, this public healthmeasure is grossly underutilized. Indeed whenadjusted for purchasing power, the price of tobaccoproducts actually fell in the South Asian regionbetween 1990 and 2000.
There should be fewer taxes on the daily use materialfor hygiene. More awareness should be createdamong the general public about daily brushing theteeth twice, less alcohol consumption, in case of anyoral trauma inspection of the wound in oral region by asurgeon or physician and to avoid use of hot food ordrinks for longer time.
5.6 Legislation
In the South Asian region, Pakistan, India and Nepalalongwith Sri Lanka, health researchers, lawyers, NGO,s, health care providers alongwith others havejointly proposed more stringent actions to curb the useof tobacco and have called on the governments oftheir countries to make more comprehensivelegislation on advertisement, sale and use of tobacco.India also passed a bill through Lok Sabha on 30th
April, 2003 addressing all types of tobacco productsknown as Bill, 2001.The bill prohibits advertising andsport sponsorship by tobacco companies althoughsuch legislation is not in place in Pakistan, Bangladesh,Nepal and Afghanistan. Afghanistan is the worldleading opium producer currently and efforts are underway by the international community to halt the opiumtrade somehow. The bill also prohibits smoking inpublic places to protect nonsmokers especiallychildren from environmental smoke. It has put a banon selling of tobacco to persons below 18 years of ageand within 100 meters of educational institutions,government and semi-government offices. Clearhealth warnings are made mandatory on all packagesin local languages and in English, alongwith tar andnicotine content, to inform the public about the risk ofthe using the product (Gupta, 2001). This bill isawaiting presidential approval in India and the next
WebmedCentral > Research articles Page 15 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
step will be to tackle the issues of enforcement once itbecomes law and the law enforcement agencies haveto play a really active and honest role in implementingit to tackle the tobacco problem. It will need thesupport of all professionals and especially healthcareprofessionals have to support this idea andimplementation of the law besides all the citizens andinfluential Figures in this country.
5.7 Global strategy
In May, 1999, the World Health Assembly which isgoverning body of the World Health Organizationpassed a legislation called Framework Convention onTobacco Control (FCTC) that could address crosscountry issues like advertising and promotion,agricultural diversification, smuggling, taxes andsubsidies (WHO, 2000, Chaudhary, 2000). About 160members of the United Nation have participated inthese negotiations and this convention was adoptedby World Health Assembly in 2003. This treaty hasbeen ratified by most members of the United Nationand it has paved the way for strong and effectivecontrol of tobacco use and advertisement at nation aswell as international level.
5.8 Reasons for current lack ofactivity or ineffectivelegislation and implementationin South Asian countries
There are multiple factors which are causing obstaclesin the effective tobacco control policy implementationat both national and regional level. At regional levelthere is lack of trust between the member states ofSouth Asian region and their border disputes. Atnational levels, corruption in politics involvingpoliticians accepting money as bribes from thetobacco companies so they are not sincere in tacklingthis problem in most of these countries. Anotherproblem at the public level is lack of awareness andsocial support for those people who want to quitsmoking but can’t do it due to lack of tobaccocessation clinics and other facilities.
6. Conclusion
Indian Subcontinent is a region which is highly
affected with lots of diseases including oral cancer.Many of steps have to be taken to improve the currentsituation. This is just an initiative in that direction.Much is still needed to be done at both the regionallevel and national level in all these countries. There isalso a greater need for more efficient steps to be takenby all these countries to create awareness among thegeneral public, provide aid to farmers to cultivate othercrops and to provide health care access and facilitiesto the general public, effective screening programmesto detect cancers at early stages and thus making thetreatment possible and cheaper. There is also a greatneed at the regional level between these countries towork with one another to counter this problem andthus decrease the incidence of oral cancer as itsincidence is one of the highest in this region ascompared to the rest of the world.
References:
1. "Indian subcontinent". New Oxford Dictionary ofEnglish New York: Oxford UniversityPress, 2001; p. 929.2. "Indian subcontinent". Geology and Geography. TheColumbia Electronic Encyclopaedia, 6th ed. ColumbiaUniversity Press, 2003.3. Werning, John W (May 16, 2007). Oral cancer:diagnosis, management, and rehabilitation. pp. 1.4. Sankaranarayanan, R., et al., Head and neckcancer: a global perspective on Epidemiology andprognosis. Anticancer Res, 1998. 18(6B): p. 4779-86.5. Sankaranarayanan, R., et al., Aetiology of oralcancer in patients less than or equal to 30 years ofage. Br J Cancer, 1989. 59(3): p. 439-40.6. Sankaranarayanan, R., et al., Effect of screening onora l cancer morta l i ty in Kera la, Ind ia: acluster-randomized controlled trial. Lancet, 2005.365(9475): p. 1927-33.7. Subramanian, S., et al., Cost-effectiveness of oralcancer screening: results from a Cluster randomizedcontrolled trial in India. Bull World Health Organ, 2009.87(3): p. 200-6.8. Phukan Rk, Zomawia E, Narain K, Hazarika NC,Mahanta J(2005). Tobacco use and stomach cancer inMizoram, India. Cancer Epidemiol Biomarkers Prev,14, 1892-6.9. Nair MK, Nambi KS, Amma NS etal ( 1999).Population study in the high natural backgroundradiation area in Kerala, India. Radiate Res, 152(Supply), S145-8.10. Siddiquee BH, Alauddin MH, Choudhurry AA,Akhtar N (2006). Head & Neck Squamous CellCarcinoma (HNSCC) 5 years study at BSMMU.
WebmedCentral > Research articles Page 16 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Bangladesh Med Res Counc Bull, 32, 43-8.11. Tyagi BB, Verma K, Singh RP (2001). Is incidenceof cancer on decline in Delhi, capital of India? Indian JCancer, 38, 8-16.12. Thomas G, Hashibe M, Jacob BJ et al (2003). Riskfactors for multiple oral premalignant lesions. Int JCancer, 107, 285-91.13. Zeb A, Rasool A, Nasreen S (2008). Cancerincidence in the district of Dir (North West FrontierProvince), Pakistan: a preliminary study. J Chin MedAssoc, 71, 62-5.14. Shanta V, Gajalakshmi CK, Swaminathan R,Ravichandran K, Vasanthi L, (2002).Cancerregistration in Madras, Metropolitan Tumor Registry,India. Eur J Cancer, 30A, 974-8.15. Yeole BB (2007). Trends in the incidence of Headand Neck Cancers in India. Asian Pacific J cancerPrev, 8, 607-12.16. Khan H, Khwaja MI, Khwaja MR. Dilemma ofcancer screening in Pakistan. Asian Pacific J CancerPrev, 7, 340-117. Gajalakshmi, C K & Shanta, V. Lifestyle and riskof stomach cancer: a hospital based case controlstudy. Int J Epidemiol.1996; 25 (6): 1146- 1153.18. Chaudhary, K. Control or Promotion – the Paradox.Tobacco Control SAARC Edition 1994; 1:4.19. Gupta, P.C, Sinor, P.N, Bhonsle, R.B, Pawar, V.Sand Mehta, H.C. Oral Submucous Fibrosis in India: Anew epidemic? The National Medical Journal ofIndia1998; 11: 113- 116.20. Jafarey, N.A, Mahmood, Z & Zaidi, S.H.M. Habitsand dietary patterns of cases of carcinoma of oralcavity and oropharynx. J. Pakistan med. Assoc. 1977;27:340- 434.
WebmedCentral > Research articles Page 17 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Illustrations
Illustration 1
Front Page Of the article
WebmedCentral > Research articles Page 18 of 29
WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Illustration 2
The scenario for oral cancer in Indian Subcontinent
WebmedCentral > Research articles Page 19 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Table 1-Numbers of South Asian Registries in the series of nine volumes of CIV
Illustration 3
Table 01
WebmedCentral > Research articles Page 20 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Figure 2- A Cancer Journal for Clinician (http://caonline.amcancersoc.org/misc/about.shtml).
Illustration 4
Figure 01
WebmedCentral > Research articles Page 21 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Figure 2- A Cancer Journal for Clinician (http://caonline.amcancersoc.org/misc/about.shtml).
Illustration 5
Figure 02
WebmedCentral > Research articles Page 22 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Illustration 6
Table
WebmedCentral > Research articles Page 23 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Table 5. Number of new cases of Cancer per Annum in India. (National Center RegistryProgramme in India, ICMR & National Cancer Institute(http://www.cancer.gov/cancertopics/types/head-and-neck).
Illustration 7
Table 5
WebmedCentral > Research articles Page 24 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Figure 3- Percentage data for the five most prevalent cancers in countries of South Asia(Globocan 2002) (Asian Pacific Journal of Cancer Prevention, Vol 10, AsianEpidemiology Supplement, 2009).
Illustration 8
Figure 03
WebmedCentral > Research articles Page 25 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Figure 6. Commonest Cancers in Indian males and females in different regions of India.
Illustration 9
Figure 06
WebmedCentral > Research articles Page 26 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Figure 4. Male Mouth Cancer Incidence /100,000 over time (Waterhouse etal., 1982; Muir et al., 1987; Parkin et al., 1992, 1997, 2002, Curado et al.,2007).
Illustration 10
Figure 4
WebmedCentral > Research articles Page 27 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
Figure 5. Male Tongue Cancer Incidence /100,000 over time (Waterhouse et al., 1982;Muir et al., 1987; Parkin et al., 1992, 1997, 2002, Curado et al., 2007).
Illustration 11
Figure 05
WebmedCentral > Research articles Page 28 of 29

WMC003626 Downloaded from http://www.webmedcentral.com on 06-Aug-2012, 05:07:33 PM
DisclaimerThis article has been downloaded from WebmedCentral. With our unique author driven post publication peerreview, contents posted on this web portal do not undergo any prepublication peer or editorial review. It iscompletely the responsibility of the authors to ensure not only scientific and ethical standards of the manuscriptbut also its grammatical accuracy. Authors must ensure that they obtain all the necessary permissions beforesubmitting any information that requires obtaining a consent or approval from a third party. Authors should alsoensure not to submit any information which they do not have the copyright of or of which they have transferredthe copyrights to a third party.
Contents on WebmedCentral are purely for biomedical researchers and scientists. They are not meant to cater tothe needs of an individual patient. The web portal or any content(s) therein is neither designed to support, norreplace, the relationship that exists between a patient/site visitor and his/her physician. Your use of theWebmedCentral site and its contents is entirely at your own risk. We do not take any responsibility for any harmthat you may suffer or inflict on a third person by following the contents of this website.
WebmedCentral > Research articles Page 29 of 29