2009 annual report - bhsala.com · the comprehensive cancer committee at princeton baptist medical...
TRANSCRIPT

Breast CanCer Data
2009 AnnuAl RepoRt

The Comprehensive Cancer Committee at Princeton Baptist Medical Center is pleased to present the 2009 Annual Report. Our cancer program draws expertise from a multi-disciplinary team of medical and radiation oncologists, surgeons, radiologists, pathologists, other oncology professionals, allied health workers and other support personnel. This team approach enables us to provide the best exemplary services and care to each individual patient and family while continuing to provide a caring and personalized environment. The Annual Report outlines the activities of the Princeton Baptist Cancer program during 2008. Nine hundred and thirty four (934) cancer patients were evaluated and/or treated at Princeton. Included in the database are over 625 patients from Jefferson County, 142 patients from Walker County, as well as representatives from 32 other Alabama counties. The five most common cancers were lung, colorectal, prostate, breast and Non-Hodgkin’s lymphoma representing 63% of all new cancer patients diagnosed and/or treated at Princeton in 2008. The Comprehensive Cancer Committee works intensely to make every aspect of the cancer program excellent in the scope of prevention, early detection, diagnosis, treatment and rehabilitation of cancer patient’s. Our goal for quality care and compliance to the standards of the Commission on Cancer of the American College of Surgeons (COC/ACoS), the College of American Pathology (CAP), American College of Surgeons Stereotactic Accreditation and the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has kept our program dedicated to our patients since the cancer program began in 1979. Our Cancer Program is committed to the highest quality of cancer care to our patients. In order to provide patients with state-of-the-art care, we continue to invest in new, innovative medical technology, such as the da Vinci S HD Robot to perform minimally invasive prostate surgery, mammography equipment at the Princeton Hoover location, and the latest generation of hybrid imaging with a new nuclear camera, the GE Infinia Hawkeye 4 in our premier diagnostic imaging center. In October, Princeton also sponsored a special free mammogram awareness day for underserved women between the ages of 40 -64 who have insufficient or no insurance. The Cancer Committee implemented quality studies which included the Colorectal Cancer Study with the National Cancer Data Base benchmark, catheter related hospital acquired urinary tract infection, impact of neoadjuvant therapy, staging of breast and rectal cancer cases. Patient data from 1992, 1997, 2002, and 2007 were submitted to the National Cancer Data Base for inclusion in national statistics. In 2008, Princeton provided cancer screenings for ten industrial companies with prostate specific antigen (PSA), mammography, hemocult and skin screening. Free public cancer related seminars with printed materials on cancers, clinical trials, prevention and early detection were provided to several community churches, health fairs, and the Hispanic community. Interdisciplinary conferences such as weekly Tumor Boards, monthly Stereotactic Breast Concordance Conferences and other specialty conferences were held for ongoing educational opportunities. Princeton also offered
Symposiums on “Thrombocytopenia” and “Multiple Myeloma/Monoclonal Gammopathy” including National Treatment Guidelines to all physicians, nurses and other allied health professionals to continually provide and draw upon expertise for patient care. This year’s Annual Report contains a detailed analysis of Lung Cancers diagnosed and /or treated from 1990 to 2008 at Princeton Baptist Medical Center with National Cancer Data Base (NCDB) comparison. Information on stage, treatment, and survival is presented.
Our medical, professional, and administrative staff is dedicated in their continual pur-suit of excellence in patient care. The Comprehensive Cancer Committee invites you
to review our 2009 Annual Report.
James C. lasker, MD Chairman, Comprehensive Cancer Committee
Comprehensive CanCer Commmittee C h a i r m a n ’ s r e p o r t
3
ChAiRMAnJames C. Lasker, M.D., Medical Oncology/Hematology
physiCiAn liAisonThomas A. Gaskin, III, M.D., General Surgery/Surgical
Oncology
suB-CoMMittee ChAiRMAnJohn Pinkston, M.D., Radiation Oncology
BReAst CARe CenteR steeRinG CoMMittee ChAiRMAnThomas A. Gaskin, M.D., General Surgery/Director,
Breast Care Center
CooRDinAtoRsCancer Conference
Belinda Limbaugh, RHIT, CTR, Oncology Data Specialist
Cancer RegistryJudy Lang, CTR, Coordinator, Cancer Registry
Quality improvementLynn Morgan, BS, RT, (R), (T), Director,
Cancer Center
Community outreachLaTonya Hall, RN, Coordinator, Breast Cancer Center
Rehabilitation services outpatientCarol Stephens, PT, CLT, Director, Rehabilitation Services
Outpatient
Clinical ResearchVonda Ellis, RN, BSN, OCN, Radiation Oncology
Comprehensive CanCer Committee
The Cancer Committee at Princeton Baptist is a standing committee of the hospital’s medical staff to provide high-quality, multidisciplinary cancer care. The Committee is dedicated to providing cancer prevention, education and support programs for patients and to ensure those diagnosed with a malignancy have access to the most effective treatment available. The Cancer Committee meets quarterly and includes multidisciplinary physician members from the diagnostic and therapeu-tic specialties, as well as allied health professionals involved in the care of cancer patients. The program’s goals and success depends on the Committee’s leadership to plan, implement and evaluate cancer patient care and other cancer-related activi-ties at Princeton.
R. Cem Cezayirli, M.D., Neurosurgery
Scott Day, M.D., Pathology
Michael Garcia, M.D., Medical Oncology/Hematology/Palliative Care Physician
David Russakoff, M.D., Medical Staff Affairs
Yahya Sabri, M.D., Obstetrics/Gynecology
Jay Smith, M.D., Thoracic Surgery
Gregory Thomas, M.D., Thoracic Surgery
James C. Walker, M.D., Radiology
Debbie Cox, RN, BSN, CRNH, Manager, Hospice-Patient Care
Suzanne Daniel, RHIA, MA, Director, Health Information Management
Sharon Day, R.D., Dietician
Len Gavin, Chaplain, Pastoral Care
Dan Gillis Pharm D., Clinical Pharmacy Specialist
Donna Green, RN, OCN, Manager, Oncology Unit
Jacqueline Kelley, Chaplain, Pastoral Care
Terri Lamons, BS, Director, Radiology
Laura Catherine Mason, Employer Relations Specialist
Terri Milazzo, RHIA, CPAQ, Director, Quality Management
Hillary Parmer, MA, RA, American Cancer Society Representative
Betsy Postlethwait, Chief Operating Officer
Shirley Reed, RN, American Cancer Society Representative
Andy Simulia, RN, BA, OCN, Case Management
Lisa Seal, LCSW, Case Management, Social Worker
4
CoMMittee MeMBeRs
otheR MeMBeRs

CliniCal Goalsprovide screening mammography at hoover princeton Clinic. • January 2008 equipment was purchased and installed. A technologist is onsite every Wednesday to perform mammograms.
Quality improvement GoalsAchieve excellence in patient satisfaction • Patient satisfaction excellence was achieved by consistently conducting walking rounds, identify-ing caregivers and promptly addressing any patient concerns.
Renovate oncology unit • Oncology unit remolding with new beds, art work, window treatment and furnishing. • A patient family suite has been added to the unit so the family can stay with the patient. It has a shower and sofa in the room and glass doors in between the patient’s room and the family room.
Monthly documentation audits • Documentation for patient care was monitored through monthly audits and focused on patient plan of care and review medication sheet.
provide quality patient care by consistently following guidelines related to infection control, medication/che-motherapy and blood product administration. • Monthly reports from infection control, medica-tion audit, and blood bank. • Quality of care increased due to the decrease in nosocominal infections incompliance with the blood bank quality guidelines.
Community outreaCh Goalsestablish 2 additional industrial screenings a year and screening at Relay for life.• New screenings were established and provided at Hanna Steele and Sloss Furnace Industries pro-viding Prostate Exam, Hemocult, Dermascan and Educational Material.
• Screenings continue at Drummond Coal Mines Provide Hemocult, Bone Density, Eye Vision, Mammograms and Lab including PSA• Screening provided for Relay for Live including Bone Density and Teaching on Breast and Prostate Exams using models with mass.
proGrammatiC GoalsDevelop and implement a process to set the required accuracy rate for the collaborative stage derived through the collection of the Cs data items and physician quality check for accuracy of the collabora-tive staging.• Accuracy rate 90%• Quality checks added to the monthly physician data audit.• Reviewed by Committee quarterly• Policy and Procedure developed
Develop and implement a process to promote and document physician use of AJCC staging in treatment planning and AJCC staging recorded in a standardized location in the medical record for 90% or more of eligible annual analytic cases.• AJCC staging form will remain on the medical records as a chart deficiency.• AJCC staging implemented in the discussed at Tumor Board for each case.• Staging on the medical records included in physi-cian review monthly and reported quarterly to the Comprehensive Cancer Committee.• Maintained 90% accuracy rate.• The staging policy and procedure revised to include the new guidelines.
Develop and implement a process to receive the CoC outstanding Achievement Award.• The subcommittee will review the standards quarterly and make recommendation to cancer committee if needed.
CanCer program goals 2008
5
The Comprehensive Cancer Committee sets goals each year to improve care of the cancer patient at Princeton. Below are the 2008 goals and accomplishments.
2008 Quality improvements
patient Care improvements
6
• Process implemented to offer mammography at the Princeton Hoover location one day a week.
• Process developed to make Tip TV educational material available to all nursing and technical staff with CEU’s available.
• Dr. Katisha Vance, Medical Oncologist, has joined the Princeton medical staff.
• DVD’s on general generic clinical trials are available to physicians and patients.
• The stereotactic breast biopsy imaging services of Princeton received accreditation for Mammog-raphy testing through January 2011.
• Princeton and New Beacon Hospice jointly implemented an annual teleconference “Living with Grief-Children and Adolescences” held in April.
• Prayer room on 5 West was refurnished and decorated for the comfort and enjoyment of patients and families.
• The Congregational Health Program imple-mented a process to provide churches with the ability to have lectures on “Alabama Faith United Against Tobacco” presented by Clarice Davis of the Jefferson County Department of Health.
• Princeton Baptist now has the daVinci® S HD robot, a state-of-the-art robotic surgical system which arrived at the hospital on June 12, 2008.
• Referral Clinic made physical changes to the chemo room to make it more comfortable and moved it away from the medical and surgical activities.
• American Cancer Society provided education to the residents on the services they provide.
• Renovations on the Inpatient Oncology Unit include a family suite adjoining a patient room which will have a sleeper sofa; patient room’s renovation included new furniture and window treatment.
• The Employee Benevolent Fund assisted pa-tients from the Lymphedema Clinic with funds for parking as needed and requested.
• Video for mastectomy education was produced and distributed to patients in Preadmission Testing; Surgical Nursing Units, and Breast Care Center.
CanCer support groups
ameriCan CanCer soCiety support Groups on prinCeton’s Campus
look GooD…. Feel BetteRA free program that teaches beauty techniques to women with cancer that is on active treatment to help them combat the appearance-related side effects of cancer treatment. Look Good…feel Better is offered the second Monday, quarterly.
ReACh to ReCoveRy - Reach to Recovery program provides information and support to anyone facing breast cancer through one-on-one contact with an American Cancer Soci-ety volunteers. Reach to Recovery is by Physician referral.
touCh—toDAy ouR unDeRstAnDinG oF CAnCeR is hope Touch is a program for cancer patients, their families and friends to help them better understand and cope with can-cer. Touch is offered the fourth Tuesday, monthly.
stRetCh - Exercise class for cancer survivors. STRETCH is offered every Wednesday, weekly.
BosoM BuDDies - BReAst CAnCeR suppoRt GRoupProvide women who have had breast cancer with the knowledge and understanding they need to make informed decisions and regain a sense of control over their lives.Bosom Buddies is offered the third Wednesday, monthly.
A plACe oF hope - Hope Lodge is a unique “home away from home” for people who need temporary, warm, comfortable, supportive, non-cost accommodations during cancer treat-ment. Hope Lodge is offered by referral.
prinCeton’s support GroupBReAst CAnCeR suppoRt GRoup - Interactive presentations and discussions among Breast cancer survivors and profes-sionals. Offered the third Wednesday of each month.
sMokinG CessAtion pRoGRAM - Program offered to smok-ers who need assistance in trying to quit smoking. Offered quarterly. Referral offered to Alabama Quit Line (State Program).
nAtionAl suRvivoRs DAySurvivor’s celebration with reception, speaker, door prizes and prize to longest survivor. Offered June of every year.
STRETCH Support Group – Back: Janice Jackson, Violette Ford, Dinia Jo Chapman,
Mary Turner and Doris Rodgers. Front: Crystalyn Johnson, and Ola Nora.
7
Dinia Chapman, Cancer Survivor
STRETCH Leader

outreaCh aCtivities
Princeton has a long history of serving the community by offering cancer education, information, awareness and screening. We also participated in community fund raising events and other organizations for cancer research, treat-ment, education and support. Below are a few examples of our activities in 2008.
Birmingham and Bessemer housing Authority health Awareness – February 20 – 60 Participants – Presentation on Breast Health Education, Breast Cancer and provided cancer educational material.
Robins and Morton health Fair – March 10 – 63 Participants - Screenings - PSA Screenings, Cancer Education, Blood Pressure, Body Composition, Glu-cose, and Cholesterol.
sloss industries health Fair – March 28 - 67 Participants - Screenings - PSA Screenings, Cancer Education, Blood Pressure, Body Composition, Glu-cose, and Cholesterol.
Miles Memorial AMe Church – March 29 – 70 Participants – Screenings – Dermascan and provided Breast Health Information.
Drummond Coal health Fair – April – 467 Partici-pants - Screenings - Mammograms, PSA, Bone Den-sity, Blood Pressure, and Complete Blood Counts.
Relay for life – May – 150 Participants - Princ-eton sponsored Urban Relay for Life and provided Bone Density and teaching on Breast and Prostate exams using models with simulated mass.
hanna steel health Fair – May 20 – 70 Partici-pants - Screening - PSA, DermaScan, Blood Pres-sure, Bone Density, Cholesterol, Glucose, and Body Composition.
First Baptist Church kingston – August 2 – 60 Partici-pants – Provided prostate and breast cancer infor-mation.
Family life Center Church health Fair – August 30 – 25 Participants – Screenings – Bone Density, provide breast cancer education material and Alabama Breast and Cervical Program information.
susan G. komen – Race for the Cure – October 11 – Princeton participated in the 5K run and provided cancer educational material.
City Wholesale health Fair – October 16th and 17th – 93 Participants - Screenings - DermaScan, Breast Health Education, Bone Density, Blood Pressure, Cholesterol, Glucose, Body Composition, and Vision.
nCp solutions health Awareness Day – October 22 – 80 Participants - Screenings - Bone Density, DermaScan, Blood Pressure, Body Composition, Breast Health Education, Cholesterol, Glucose.
Colonial properties health Fair – October 24 – 33 Participants - Screenings - Bone Density
8
Laura Catherine MasonEmployer Relations Specialist

researCh anD CanCer ConferenCe
researCh Princeton’s Comprehensive Cancer Committee recognizes that clinical research advances science and ensures that care for the cancer patient approaches the highest possible level of quality. Clinical trial information is readily avail-able in all cancer care areas as well as our patient library and treating physicians’ offices. The percentage of Princeton patients entered into cancer related clinical trials for 2008 was 7% of total cancer patients, and for the last five years ranged from 5% to 10%.
yeAR ACCRuAls CAseloAD peRCentAGe
2007 81 825 10
2008 29 859 7
2004 39 761 5
2005 59 786 8
2006 72 789 9
Princeton’s cancer conferences are
multidisciplinary conferences consisting
of weekly Tumor Board, monthly Stereot-
actic Breast Conferences and periodic
Hematology/Oncology/ Medicine Confer-
ence. The conferences include individual
patient presentation, and are open to the
entire facility and medical staff. Cancer
conferences are integral to improving the
care of cancer patients by contributing to
the patient management process, monitor-
ing outcomes, and providing education to
physicians and other staff.
Didactic Lectures 5sites Digestive System 22Respiratory System 14Lymphatic System 11Breast 18Male Genital 4Blood/Bone Marrow 3Urinary System 1Brain/CNS 3Endocrine System 3Female Genital 3Skin/Melanoma 0Oral Cavity 3Other/Ill-Defined 4totAl CAses 94 steReotAtiC 94heMAtoloGy/ onColoGy/MeDiCine 14physiCiAn CAnCeR upDAte 2
tuMoR BoARD
9
ConFeRenCe CAse pResentAtion
ConFeRenCes
CanCer registry
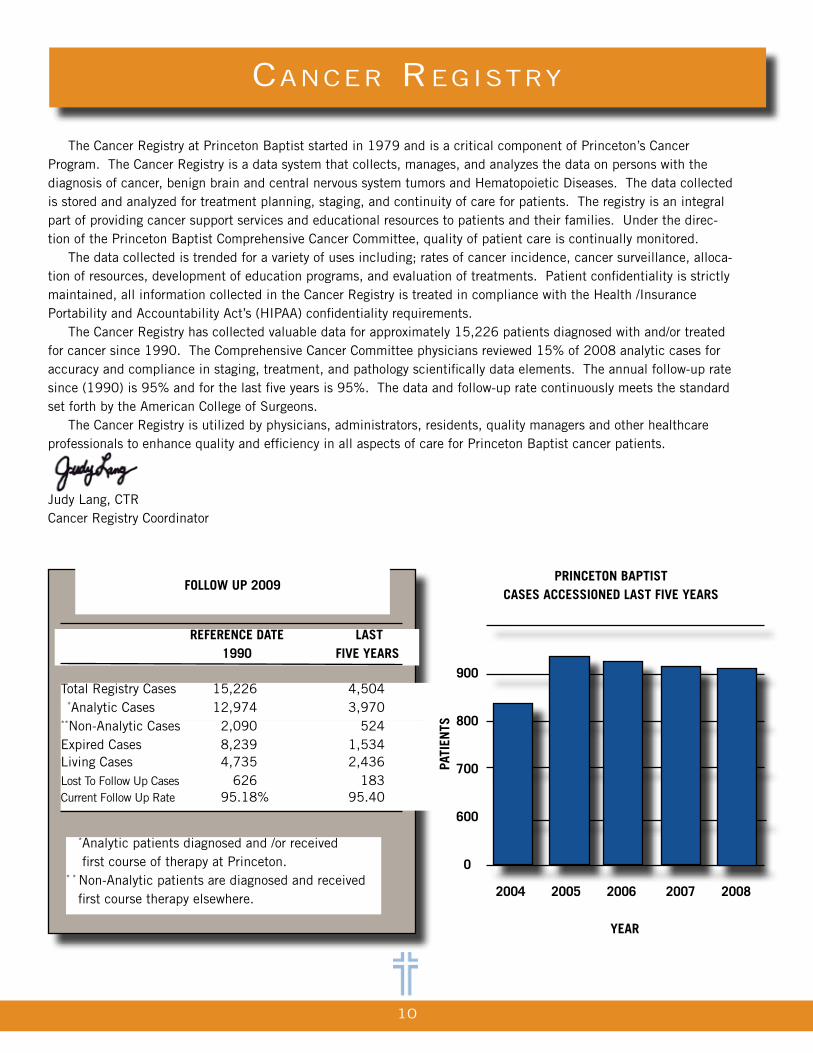
The Cancer Registry at Princeton Baptist started in 1979 and is a critical component of Princeton’s Cancer Program. The Cancer Registry is a data system that collects, manages, and analyzes the data on persons with the diagnosis of cancer, benign brain and central nervous system tumors and Hematopoietic Diseases. The data collected is stored and analyzed for treatment planning, staging, and continuity of care for patients. The registry is an integral part of providing cancer support services and educational resources to patients and their families. Under the direc-tion of the Princeton Baptist Comprehensive Cancer Committee, quality of patient care is continually monitored. The data collected is trended for a variety of uses including; rates of cancer incidence, cancer surveillance, alloca-tion of resources, development of education programs, and evaluation of treatments. Patient confidentiality is strictly maintained, all information collected in the Cancer Registry is treated in compliance with the Health /Insurance Portability and Accountability Act’s (HIPAA) confidentiality requirements. The Cancer Registry has collected valuable data for approximately 15,226 patients diagnosed with and/or treated for cancer since 1990. The Comprehensive Cancer Committee physicians reviewed 15% of 2008 analytic cases for accuracy and compliance in staging, treatment, and pathology scientifically data elements. The annual follow-up rate since (1990) is 95% and for the last five years is 95%. The data and follow-up rate continuously meets the standard set forth by the American College of Surgeons. The Cancer Registry is utilized by physicians, administrators, residents, quality managers and other healthcare professionals to enhance quality and efficiency in all aspects of care for Princeton Baptist cancer patients.
Judy Lang, CTRCancer Registry Coordinator
FolloW up 2009
ReFeRenCe DAte 1990
lAst Five yeARs
Total Registry Cases 15,226 4,504 *Analytic Cases 12,974 3,970**Non-Analytic Cases 2,090 524 Expired Cases 8,239 1,534Living Cases 4,735 2,436 Lost To Follow Up Cases 626 183Current Follow Up Rate 95.18% 95.40
*Analytic patients diagnosed and /or received first course of therapy at Princeton.* * Non-Analytic patients are diagnosed and received first course therapy elsewhere. 2004 2005 2006 2007 2008
yeAR
1,000
900
800
700
600
0
pRinCeton BAptist CAses ACCessioneD lAst Five yeARs
pAti
ents
10
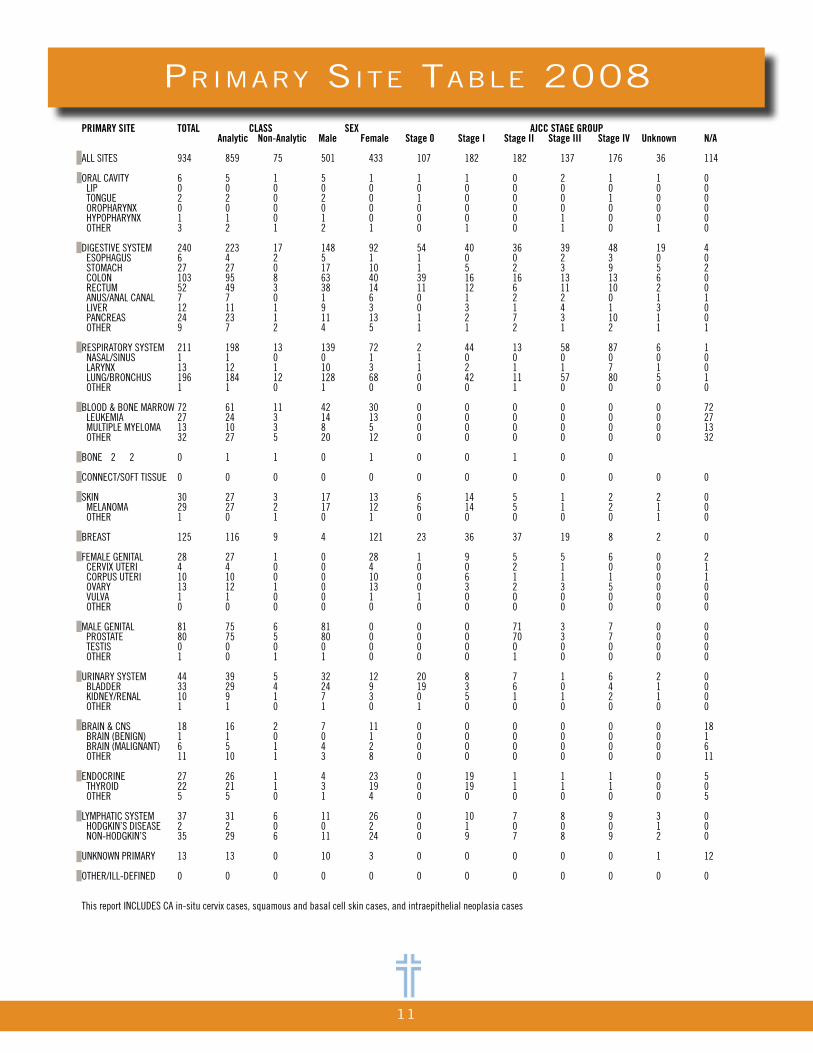
primary site taBle 2008PRIMARY SITE TOTAL CLASS SEX AJCC STAGE GROUP Analytic Non-Analytic Male Female Stage 0 Stage I Stage II Stage III Stage IV Unknown N/A ALL SITES 934 859 75 501 433 107 182 182 137 176 36 114 ORAL CAVITY 6 5 1 5 1 1 1 0 2 1 1 0 LIP 0 0 0 0 0 0 0 0 0 0 0 0 TONGUE 2 2 0 2 0 1 0 0 0 1 0 0 OROPHARYNX 0 0 0 0 0 0 0 0 0 0 0 0 HYPOPHARYNX 1 1 0 1 0 0 0 0 1 0 0 0 OTHER 3 2 1 2 1 0 1 0 1 0 1 0 DIGESTIVE SYSTEM 240 223 17 148 92 54 40 36 39 48 19 4 ESOPHAGUS 6 4 2 5 1 1 0 0 2 3 0 0 STOMACH 27 27 0 17 10 1 5 2 3 9 5 2 COLON 103 95 8 63 40 39 16 16 13 13 6 0 RECTUM 52 49 3 38 14 11 12 6 11 10 2 0 ANUS/ANAL CANAL 7 7 0 1 6 0 1 2 2 0 1 1 LIVER 12 11 1 9 3 0 3 1 4 1 3 0 PANCREAS 24 23 1 11 13 1 2 7 3 10 1 0 OTHER 9 7 2 4 5 1 1 2 1 2 1 1 RESPIRATORY SYSTEM 211 198 13 139 72 2 44 13 58 87 6 1 NASAL/SINUS 1 1 0 0 1 1 0 0 0 0 0 0 LARYNX 13 12 1 10 3 1 2 1 1 7 1 0 LUNG/BRONCHUS 196 184 12 128 68 0 42 11 57 80 5 1 OTHER 1 1 0 1 0 0 0 1 0 0 0 0 BLOOD & BONE MARROW 72 61 11 42 30 0 0 0 0 0 0 72 LEUKEMIA 27 24 3 14 13 0 0 0 0 0 0 27 MULTIPLE MYELOMA 13 10 3 8 5 0 0 0 0 0 0 13 OTHER 32 27 5 20 12 0 0 0 0 0 0 32 BONE 2 2 0 1 1 0 1 0 0 1 0 0 CONNECT/SOFT TISSUE 0 0 0 0 0 0 0 0 0 0 0 0 SKIN 30 27 3 17 13 6 14 5 1 2 2 0 MELANOMA 29 27 2 17 12 6 14 5 1 2 1 0 OTHER 1 0 1 0 1 0 0 0 0 0 1 0 BREAST 125 116 9 4 121 23 36 37 19 8 2 0 FEMALE GENITAL 28 27 1 0 28 1 9 5 5 6 0 2 CERVIX UTERI 4 4 0 0 4 0 0 2 1 0 0 1 CORPUS UTERI 10 10 0 0 10 0 6 1 1 1 0 1 OVARY 13 12 1 0 13 0 3 2 3 5 0 0 VULVA 1 1 0 0 1 1 0 0 0 0 0 0 OTHER 0 0 0 0 0 0 0 0 0 0 0 0 MALE GENITAL 81 75 6 81 0 0 0 71 3 7 0 0 PROSTATE 80 75 5 80 0 0 0 70 3 7 0 0 TESTIS 0 0 0 0 0 0 0 0 0 0 0 0 OTHER 1 0 1 1 0 0 0 1 0 0 0 0 URINARY SYSTEM 44 39 5 32 12 20 8 7 1 6 2 0 BLADDER 33 29 4 24 9 19 3 6 0 4 1 0 KIDNEY/RENAL 10 9 1 7 3 0 5 1 1 2 1 0 OTHER 1 1 0 1 0 1 0 0 0 0 0 0 BRAIN & CNS 18 16 2 7 11 0 0 0 0 0 0 18 BRAIN (BENIGN) 1 1 0 0 1 0 0 0 0 0 0 1 BRAIN (MALIGNANT) 6 5 1 4 2 0 0 0 0 0 0 6 OTHER 11 10 1 3 8 0 0 0 0 0 0 11 ENDOCRINE 27 26 1 4 23 0 19 1 1 1 0 5 THYROID 22 21 1 3 19 0 19 1 1 1 0 0 OTHER 5 5 0 1 4 0 0 0 0 0 0 5 LYMPHATIC SYSTEM 37 31 6 11 26 0 10 7 8 9 3 0 HODGKIN’S DISEASE 2 2 0 0 2 0 1 0 0 0 1 0 NON-HODGKIN’S 35 29 6 11 24 0 9 7 8 9 2 0 UNKNOWN PRIMARY 13 13 0 10 3 0 0 0 0 0 1 12 OTHER/ILL-DEFINED 0 0 0 0 0 0 0 0 0 0 0 0 This report INCLUDES CA in-situ cervix cases, squamous and basal cell skin cases, and intraepithelial neoplasia cases
11
top ten sites Comparison 2008
prinCeton Baptist
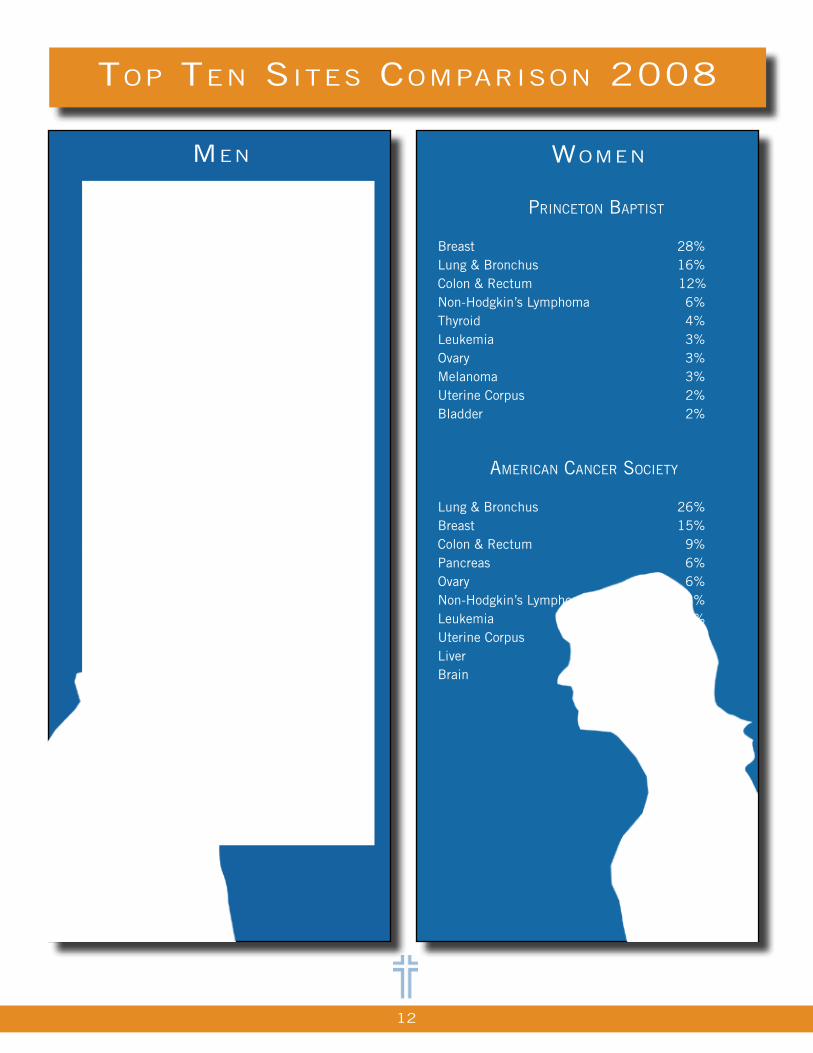
Lung & Bronchus 26%Colon & Rectum 20%Prostate 16 %Bladder 5% Melanoma 3%Stomach 3%Leukemia 3%Pancreas 3%Non-Hodgkin’s Lymphoma 3%Liver 2%
ameriCan CanCer soCiety
Lung & Bronchus 31%Prostate 10%Colon & Rectum 8% Pancreas 6%Liver 4%Leukemia 4%Esophagus 4%Urinary Bladder 3%Non-Hodgkin’s Lymphoma 3%Kidney & Renal Pelvis 3%
Womenmen
prinCeton Baptist Breast 28%Lung & Bronchus 16%Colon & Rectum 12%Non-Hodgkin’s Lymphoma 6%Thyroid 4%Leukemia 3%Ovary 3%Melanoma 3%Uterine Corpus 2%Bladder 2%
ameriCan CanCer soCiety Lung & Bronchus 26%Breast 15%Colon & Rectum 9%Pancreas 6%Ovary 6%Non-Hodgkin’s Lymphoma 3%Leukemia 3%Uterine Corpus 3%Liver 2%Brain 2%
12
geographiC DistriBution 2008
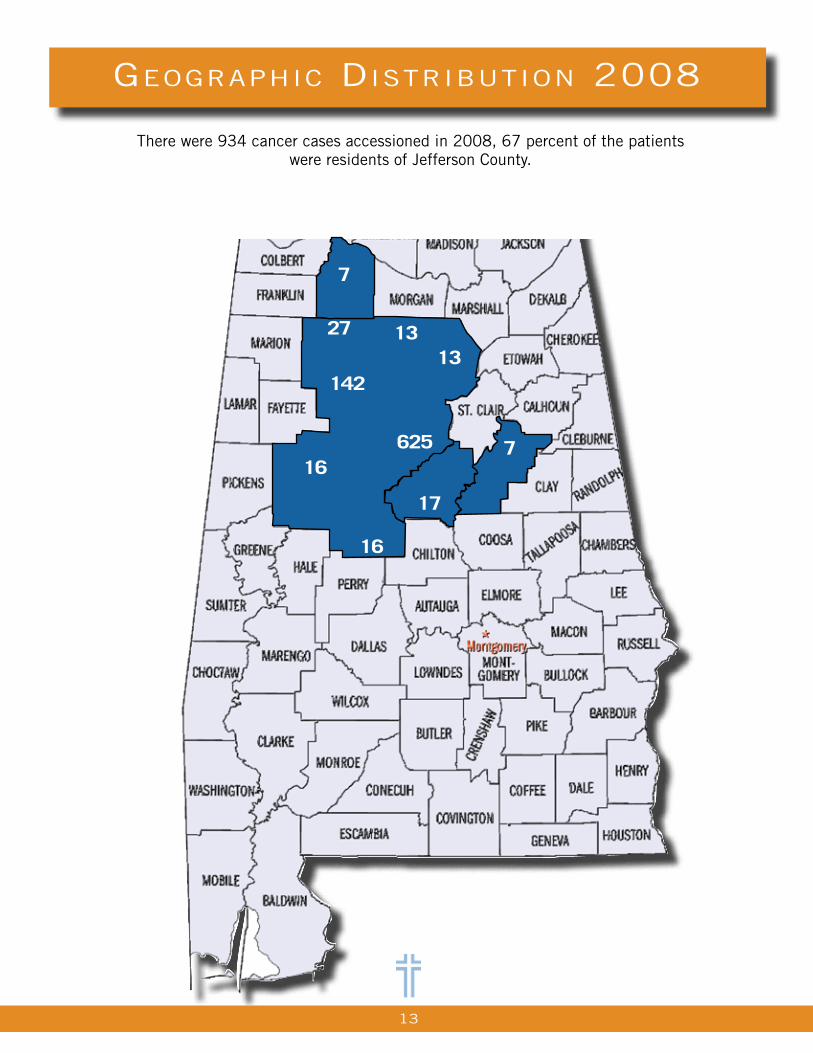
There were 934 cancer cases accessioned in 2008, 67 percent of the patients were residents of Jefferson County.
13
625
142
1313
16
16
27
7
17
7
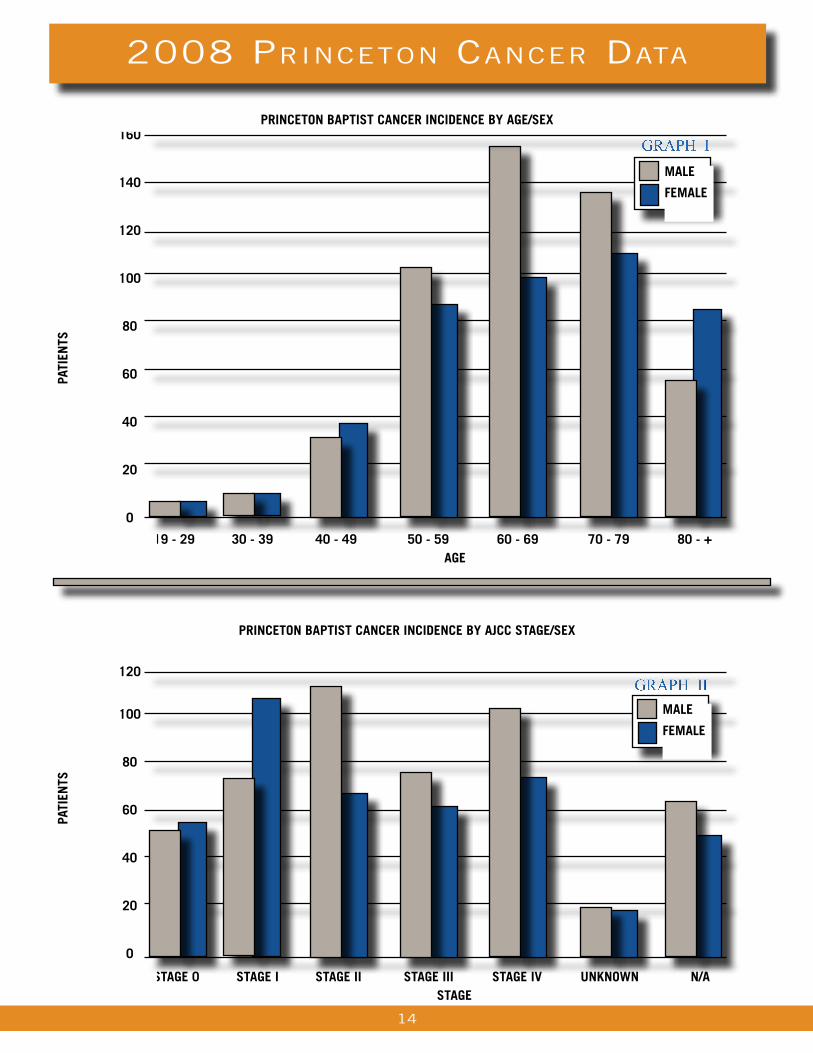
2008 prinCeton CanCer Data
19 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 79 80 - + AGe
160
140
120
100
80
60
40
20
0
pRinCeton BAptist CAnCeR inCiDenCe By AGe/seX
pAti
ents
stAGe 0 stAGe i stAGe ii stAGe iii stAGe iv unknoWn n/A stAGe
120
100
80
60
40
20
0
pRinCeton BAptist CAnCeR inCiDenCe By AJCC stAGe/seX
pAti
ents
MAle
FeMAle
MAle
FeMAle
14
graph i
graph ii
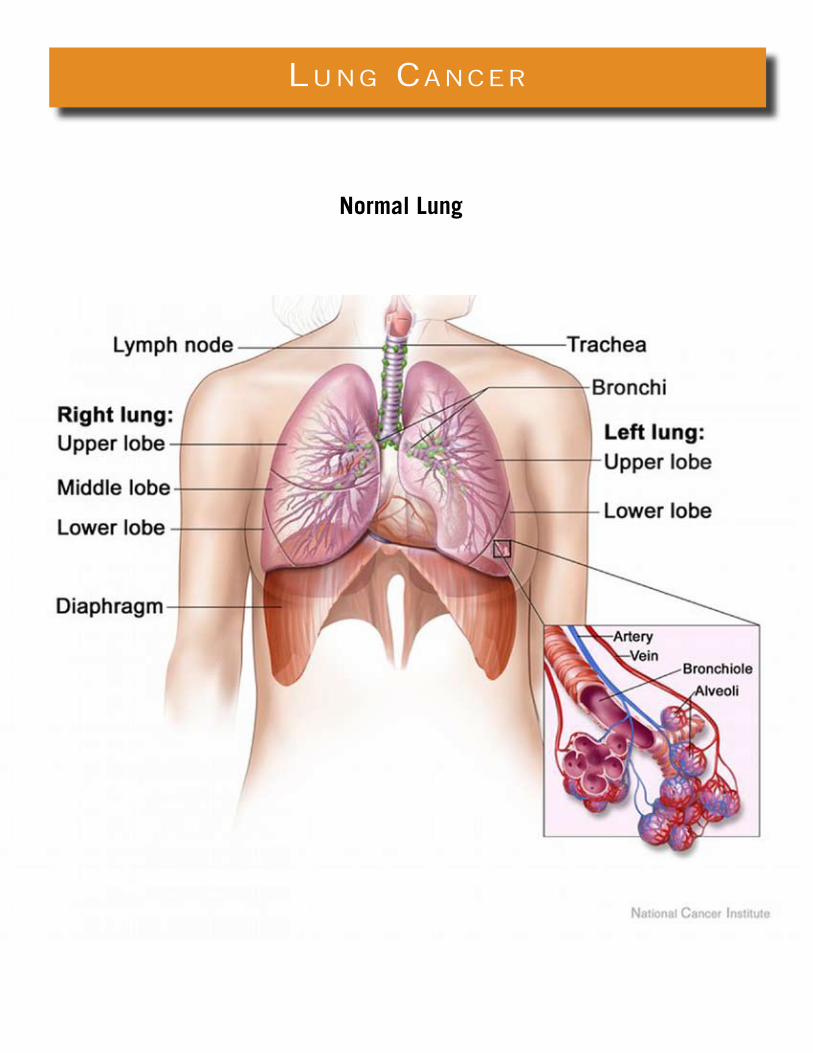
lung CanCer
Normal Lung

lung CanCer summary
Lung cancer is the second most common cancer diagnosis in both males and females in the United States, excluding
non-melanoma skin cancers. It is the most commonly diagnosed cancer in men and the second most commonly diagnosed
cancer in women in the population served by Princeton Baptist Medical Center. An estimated 215,000 new diagnoses of
lung cancer were anticipated in 2008 in the United States, accounting for about 15% of all cancer diagnoses. The
incidence in males is declining significantly, from a high of 102 cases per 100,000 in 1984 to 73.6 per 100,000 in
2004. The incidence in females is approaching a plateau after a long period of increase. Lung cancer is classified
clinically as non-small cell (87%) or small cell (13%) for treatment purposes.
Symptoms for lung cancer may include but are not limited to persistent cough, bloody sputum, chest pain, dyspnea,
change in voice, and recurrent pneumonia or bronchitis.
Tobacco uses, particularly cigarette smoking, is the most important risk factor for lung cancer. Risk increases
proportionally with quantity and duration of use. Other risk factors include history of tuberculosis, and occupational or
environmental exposure to second hand smoke, radon, asbestos (particularly among smokers), certain metals (chromium,
cadmium, and arsenic), some organic chemicals, radiation, and air pollution. Genetic susceptibility plays an important
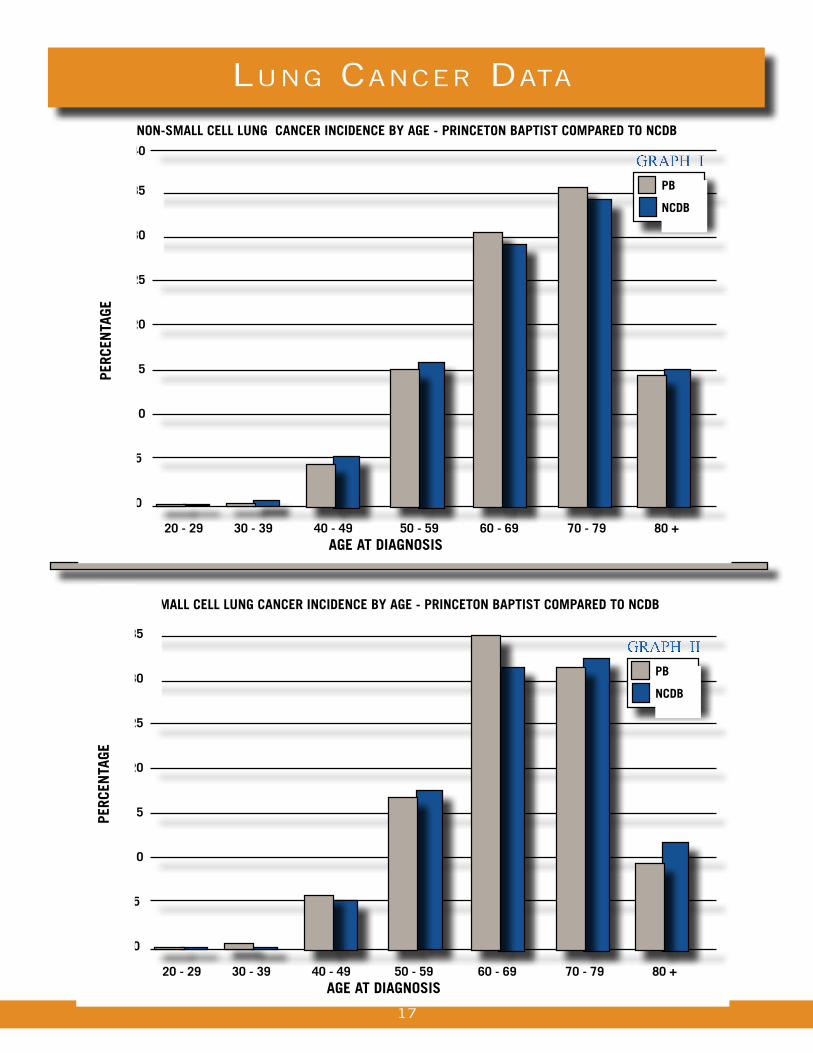
role in development of lung cancer, especially in those who develop the disease at a younger age. Age is not a primary
risk factor for lung cancer. Both subtypes of lung cancer are rare in those below the age of 40, both nationally and in
the Princeton population. As Graphs 1 and 2 indicate, the disease is most commonly diagnosed between the ages
of 60 and 79.
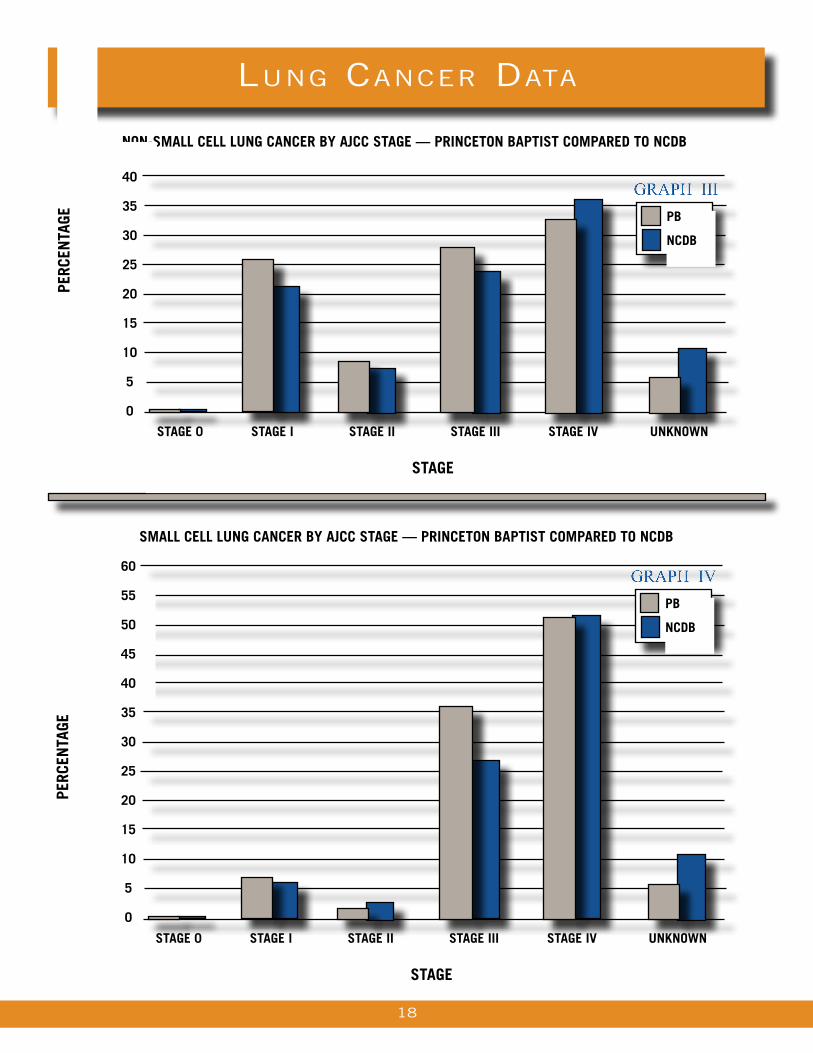
Staging of lung cancer indicates the degree of spread within the lung, nearby tissues, and distant organs. The stage
is one of the most important decisive factors in treatment planning and the most important prognostic factor. Graph 3
and 4 demonstrate that more than 60% of non-small cell lung cancers and more than 80% of small cell lung cancers
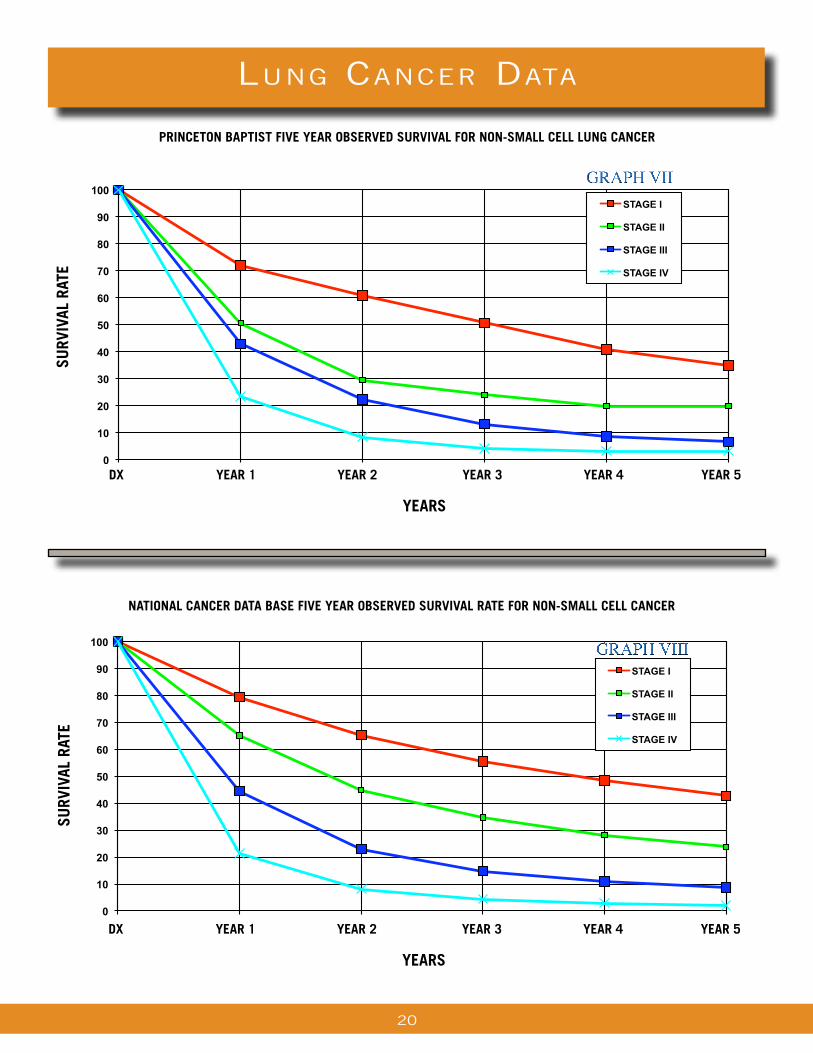
are stage III to IV at diagnosis, both at Princeton and nationally. The five year survival rate for non-small cell lesions
diagnosed in Stage I to II is 55 to 60%, and in Stage III to IV is 10%, both at Princeton and nationally, as indicated in
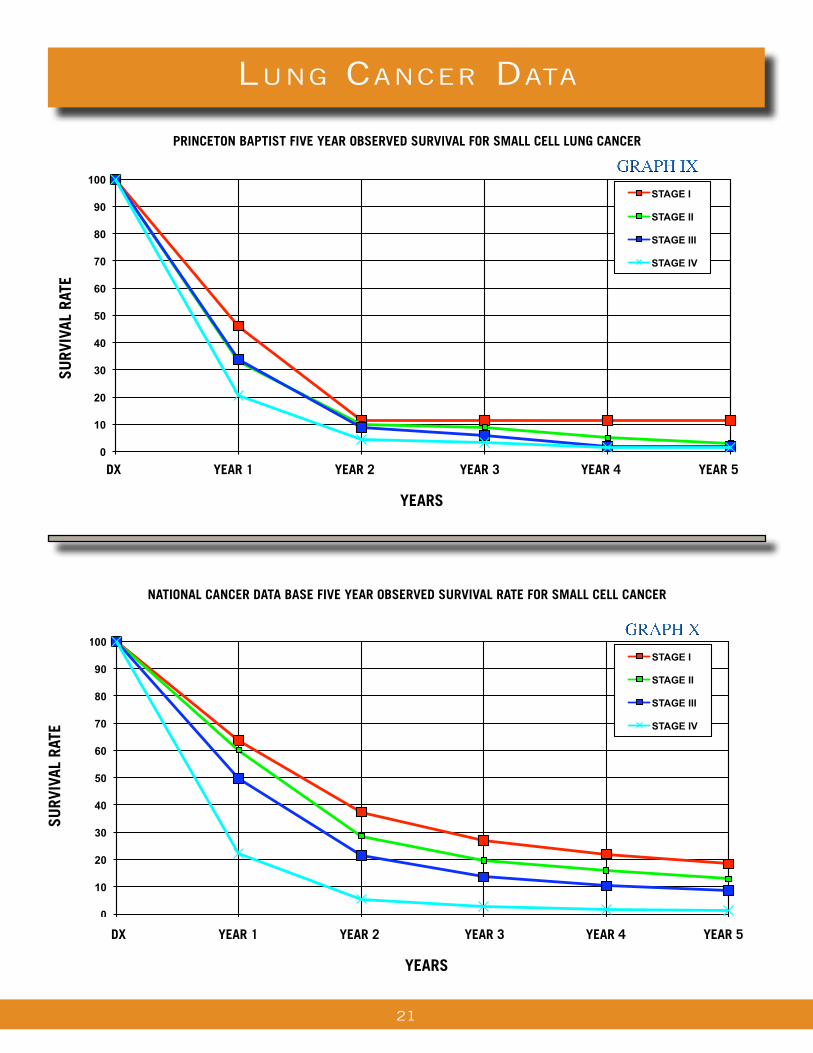
Graphs 7 and 8. The five year survival rate for small cell lung cancers diagnosed at Stage I to II is 15 to 30%, and
Stage III to IV is 4 to 10%, as shown in Graphs 9 and 10. These findings underline the dramatic reduction in survival
rates for both non-small cell and small cell lung cancers diagnosed in Stages III to IV.
Treatment options are determined by the subtype and stage of the cancer, and include surgery, radiation therapy,
chemotherapy, and targeted biological therapies. Surgery is usually the treatment of choice for localized lesions.
Chemotherapy, either alone or in combination with radiation, is gold standard for small
cell lesions. Radiation therapy and chemotherapy, sometimes in combination with
surgery, are utilized in advanced non-small cell lung cancers.
Clint Holladay, M.D.
16
lung CanCer Data
17
non-sMAll Cell lunG CAnCeR inCiDenCe By AGe - pRinCeton BAptist CoMpAReD to nCDB
20 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 79 80 + AGe At DiAGnosis
40
35
30
25
20
15
10
5
0
peRC
entA
Ge
pB
nCDB
graph i
sMAll Cell lunG CAnCeR inCiDenCe By AGe - pRinCeton BAptist CoMpAReD to nCDB
20 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 79 80 + AGe At DiAGnosis
35
30
25
20
15
10
5
0
peRC
entA
Ge
pB
nCDB
graph ii
lung CanCer Data
non-sMAll Cell lunG CAnCeR By AJCC stAGe — pRinCeton BAptist CoMpAReD to nCDB
stAGe 0 stAGe i stAGe ii stAGe iii stAGe iv unknoWn stAGe
40
35
30
25
20
15
10
5
0
peRC
entA
Ge pB
nCDB
graph III
18
sMAll Cell lunG CAnCeR By AJCC stAGe — pRinCeton BAptist CoMpAReD to nCDB
stAGe 0 stAGe i stAGe ii stAGe iii stAGe iv unknoWn stAGe
60
55
50
45
40
35
30
25
20
15
10
5
0
peRC
entA
Ge
pB
nCDB
graph IV
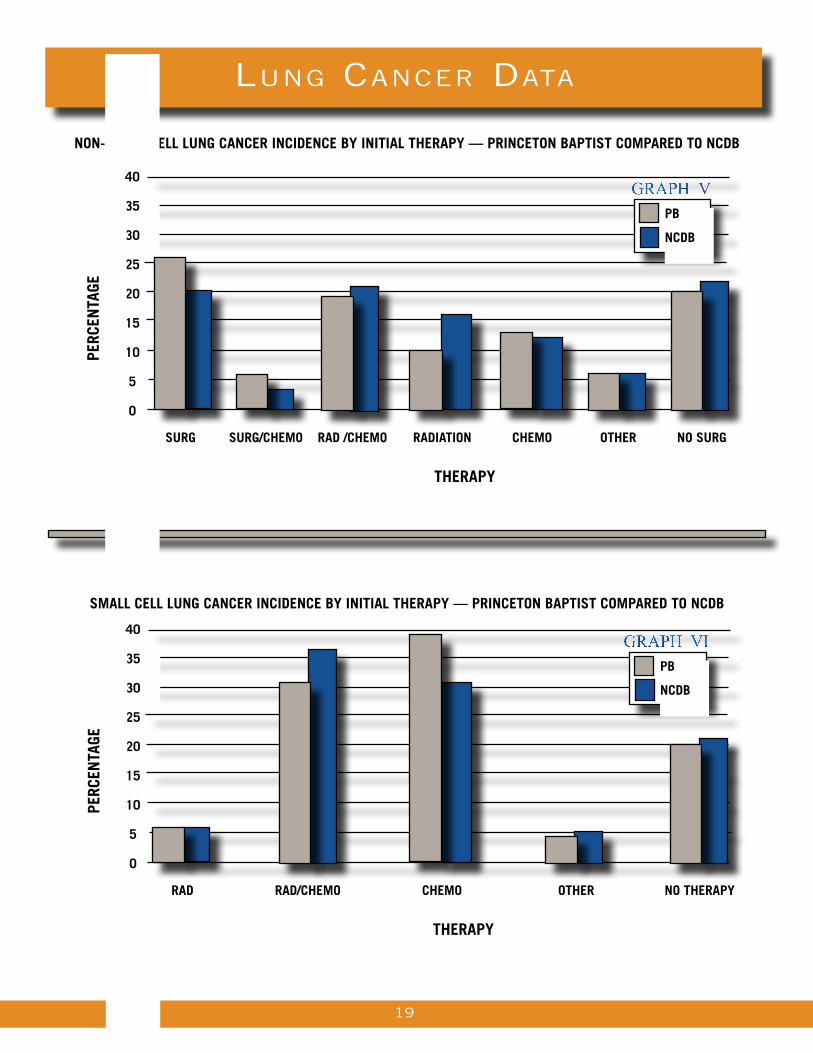
non-sMAll Cell lunG CAnCeR inCiDenCe By initiAl theRApy — pRinCeton BAptist CoMpAReD to nCDB
lung CanCer Data
19
RAD RAD/CheMo CheMo otheR no theRApy
theRApy
40
35
30
25
20
15
10
5
0
sMAll Cell lunG CAnCeR inCiDenCe By initiAl theRApy — pRinCeton BAptist CoMpAReD to nCDB
peRC
entA
Ge
pB
nCDB
graph VI
40
35
30
25
20
15
10
5
0
peRC
entA
Ge
pB
nCDB
graph V
suRG suRG/CheMo RAD /CheMo RADiAtion CheMo otheR no suRG
theRApy
lung CanCer Data
DX yeAR 1 yeAR 2 yeAR 3 yeAR 4 yeAR 5 yeARs
pRinCeton BAptist Five yeAR oBseRveD suRvivAl FoR non-sMAll Cell lunG CAnCeR
suRv
ivAl
RAt
e
nAtionAl CAnCeR DAtA BAse Five yeAR oBseRveD suRvivAl RAte FoR non-sMAll Cell CAnCeR
suRv
ivAl
RAt
e
20
DX yeAR 1 yeAR 2 yeAR 3 yeAR 4 yeAR 5 yeARs
0
10
20
30
40
50
60
70
80
90
100
DX YEAR 1 YEAR 2 YEAR 3 YEAR 4 YEAR 5
SU
RV
IVA
L R
AT
E
PRINCETON BAPTIST FIVE YEAR OBSERVED SURVIVAL
FOR NON-SMALL CELL LUNG CANCER
STAGE I
STAGE II
STAGE III
STAGE IV
graph VII
0
10
20
30
40
50
60
70
80
90
100
DX YEAR 1 YEAR 2 YEAR 3 YEAR 4 YEAR 5
SU
RV
IVA
L R
AT
E
NATIONAL CANCER DATA BASE FIVE YEAR OBSERVED SURVIVAL
FOR NON-SMALL CELL LUNG CANCER
STAGE I
STAGE II
STAGE III
STAGE IV
graph VIII
lung CanCer Data
DX yeAR 1 yeAR 2 yeAR 3 yeAR 4 yeAR 5 yeARs
pRinCeton BAptist Five yeAR oBseRveD suRvivAl FoR sMAll Cell lunG CAnCeR
suRv
ivAl
RAt
e
nAtionAl CAnCeR DAtA BAse Five yeAR oBseRveD suRvivAl RAte FoR sMAll Cell CAnCeR
suRv
ivAl
RAt
e
DX yeAR 1 yeAR 2 yeAR 3 yeAR 4 yeAR 5 yeARs
21
graph IX
0
10
20
30
40
50
60
70
80
90
100
DX YEAR 1 YEAR 2 YEAR 3 YEAR 4 YEAR 5
SU
RV
IVA
L R
AT
E
PRINCETON BAPTIST FIVE YEAR OBSERVED SURVIVAL
FOR SMALL CELL LUNG CANCER
STAGE I
STAGE II
STAGE III
STAGE IV
0
10
20
30
40
50
60
70
80
90
100
DX YEAR 1 YEAR 2 YEAR 3 YEAR 4 YEAR 5
SU
RV
IVA
L R
AT
E
NATIONAL CANCER DATA BASE FIVE YEAR OBSERVED SURVIVAL
FOR SMALL CELL LUNG CANCER
STAGE I
STAGE II
STAGE III
STAGE IV
graph X
BiBliography
glossary
aCknoWleDgements
NCDB – National Cancer Data Base Benchmarks
AJCC - American Joint Committee on Cancer, Manual for Staging of Cancer, J.B. Lippincott Company Sixth
Edition
Cancer Facts and Figures, American Cancer Society, 2008
Commission on Cancer, Cancer Program Standards
Lung Cancer, Treatment Guidelines for Patients, ACS, NCCN, Version 5/Febuary 2008
ACoS American College of Surgeons
COC Commission on Cancer
AJCC American Joint Commission Cancer
ACS American Cancer Society
ASCR Alabama Statewide Cancer Registry
NCDB National Cancer Date Base
Analytic Patients initial diagnosis and or treat for cancer at Princeton Baptist Medical Center
Non-analytic Patients diagnosed and treated at Princeton Baptist Medical Center prior to reference date or
Cases diagnosed and initially treated elsewhere.
PB Princeton Baptist
CNS Central Nervous System
TOUCH Today Our Understanding of Cancer is Hope
The Princeton Baptist Cancer Program is proud to present the 2009 Annual Report produced by Judy Lang,
CTR, Cancer Registry Coordinator. Special appreciation goes to Belinda Limbaugh, RHIT, CTR, Oncology Data
Specialist, Lynn Morgan, BS, RT, (R), (T) Cancer Center Director, Stella Seagle, CTR, Cancer Registrar and the
Cancer Registry volunteers who have helped make this annual report possible. We would also like to recognize the
following contributions: James Lasker, M.D., Chairman, Clint Holladay, M.D., John Pinkston, M.D. and Princeton
Baptist Comprehensive Cancer Committee for sharing their expertise and critiquing of this report. Special thanks
to Keith Dunn for his design and editing contributions. Appreciation is also extended to the administrative staff at
Princeton for their continued support of the cancer program.
22

our mission
as a Witness to the love of goD,
revealeD through Jesus Christ,
the Baptist health system
is CommitteD to ministries that
enhanCe the health, Dignity,
anD Wholeness of those We serve,
through integrity, Compassion,
aDvoCaCy, resourCefulness,
anD exCellenCe.