1 family drug court fundamentals and evidence based practices presented by william s. owens...
TRANSCRIPT

1
Family Drug Court Fundamentals and Evidence
Based PracticesPresented by
William S. OwensAssociate Juvenile Judge
Des Moines, IowaMarch 30, 2015

Treatment courts can be messy…

and it usually takes a team…

that knows how to work together…

to pick participants up when they fall...

and help them keep slogging along…

so in the end...it’s all worth it!









Defining the Key Components
• Participants are identified early and promptly placed in drug court program.– Eligibility based on written criteria– Candidates promptly advised of
expectations– Trained professionals screen participants– Appearance before Judge occurs
promptly– Participants promptly ordered into
treatment

Treatment courts where participants entered within 50-days of “incident” had a 63% greater reduction in
recidivist behavior
0%10%20%30%40%
39%24%
Percentage reduction in recidivist behavior

Defining the Key Components
• Using a non-adversarial approach agency counsel, GAL and parents’ counsel collaborate while still protecting client rights.– Prosecutors and defense counsel should
participate in design, screening and case-processing policies
– Consistency and stability require judges, prosecutors and defense counsel to be assigned for sufficient time to build sense of teamwork and collaboration


Judge’s role…Traditional Court Family Treatment Court
Judge calls “balls and strikes” Judge is educated on substance abuse;Engages all the parties; andLeads a multi-disciplinary team focusing on addressing parental substance abuse
Judge seeks evidence of compliance with services and orders of the Court
Judge actively engages parent participants in dialogue; andUses incentives and interventions to address parent behavior
Judge bases decisions on written reports and evidence presented by counsel
Judge inquires of parents, team, and others regarding parents’ compliance with program requirements
Judge relies on witness testimony offered by the parties
Judge relies on information from participant, the team, and others involved in providing parents a continuum of services

Parent’s attorney roleTraditional Court Family Treatment Court
Does the talking in Court and directs the client NOT to talk
Educates the parents regarding the court process, appropriate way to interact with the court and the team; andAssists the client when speaking to the judge
Focuses on protecting the parent’s rights and “winning” the case
Focuses not only on protecting parent’s rights, but also on advocating for services; Supports parent needs to achieve self-identified short and long-term goals
Cross-examines clinicians and social workers and challenges negative statements about client
Develops a working relationship with DHS staff and clinicians;Questioning geared to supporting parent’s goals and the coordinated treatment plan
Focuses on simply completing “tasks” in case plan
Advocates for quality, evidence based or informed services and interventions linked to sobriety and long-term stability

DHS caseworker roleTraditional Court Family Treatment Court
Requests report from substance abuse clinician;Develops case plan recommendations
Works with substance abuse clinician as a part of a multi-disciplinary team;Incorporates clinician recommendations into a comprehensive case plan for client
Provides a report to the court, but otherwise not an active participant in court proceeding
Works with the judge and treatment providers as a part of a team that develops comprehensive case plan for client;Takes active role in court review to address needs of client
Has limited familiarity with substance abuse treatment modalities and clinical needs of client suffering from substance abuse and/or mental health disorders
Is familiar with substance abuse treatment and treatment needs of clients; Works closely with team to develop and help assist client in working through comprehensive treatment/case plan

Substance Abuse Clinician RoleTraditional Court Family Treatment Court
Limited, if any, direct involvement in CINA case or proceedings
Provides clinical information during staffing process and treatment review hearings
Provides a report to be attached to the case plan, or admitted as an exhibit
Reports proactively submitted to team and parties; Reports are discussed during staffing and with client during court reviews
Keeps all information confidential;Unfamiliar with legal terms and the process in court
Discusses information with releases of information by the client;Understands the CINA process, familiar with legal terminology, and makes recommendations in the context of the legal proceedings
Defining the Key Components
• Abstinence is monitored by frequent alcohol and other drug testing– Random testing in accordance with
established principles– No less than twice weekly during the first
several months of participation– Procedures must be certain/reliable– Prompt reporting of results to Court – results
reported within 48-hours had 68% higher cost savings
– Prompt action by Court on positive test

Treatment courts where participants were tested at least 2x per week in Phase 1 had
61% higher cost savings
Participants tested 2x per week Participants tested LESS than 2x per week
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
29%
18%
Column1

Defining the Key Components
• A coordinated strategy governs responses to participant compliance.– Regular communication between Court and
treatment providers– Responses explained to participants– Responses to compliance vary in intensity– Sanctions for noncompliance – statistically
when sanctions imposed immediately after non-compliance it resulted in twice the cost savings.

Defining the Key Components
• Ongoing Judicial interaction with each participant is essential.– Regular status hearings used to monitor
performance– Time between hearings can be extended– Status meetings with a number of
participants together– Court uses incentives and sanctions to
address program compliance
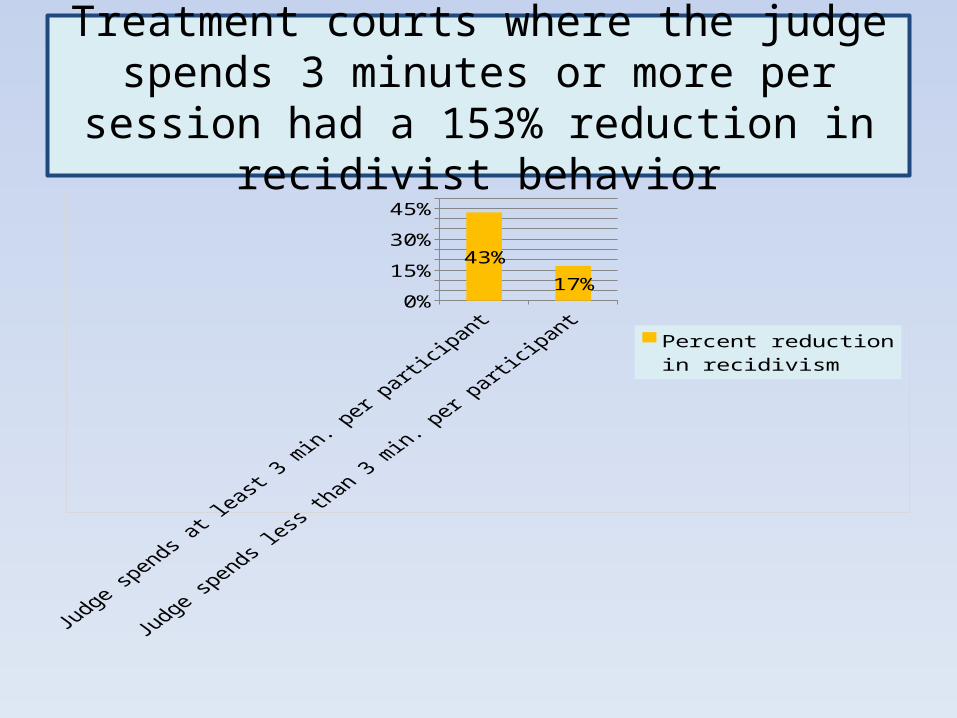
Treatment courts where the judge spends 3 minutes or more per session
had a 153% reduction in recidivist behavior
0%10%20%30%40%50%
43%
17%
Percent reduction in recidivism

Defining the Key Components
• Forging partnerships among drug courts, public agencies, and community based organizations generates local support and enhances drug court program effectiveness.– Frequent meetings between Court, lawyers,
treatment and community to provide direction– Drug court provides a critical role in forming links
between community and judicial system– Use of Steering Committee

Defining the Key Components
• Monitoring and evaluation measure the achievement of program goals and gauge effectiveness. – Goals clearly stated at outset to define
parameters of data collection– Ideally an automated system of data
collection is used to monitor and evaluate program

Use of evidence based and evidence informed practices
“Those who are enamored of practice without science are like a pilot who goes into a ship without a rudder or compass and never has any certainty where he is going”.
Leonardo da Vinci

What does it mean to be evidence-based?
• Evidence-based practice [EBP] is applying the best available research evidence in the provision of health, behavior, and education services to enhance outcomes (Child Trends, Research-to-Results Brief, June 2007).
• The American Psychological Association defines EBP as “the integration of the best available research with clinical expertise in the context of patient characteristics, culture, and preferences”.

What does evidence-based mean and why is it
important?• The evaluation research shows the
program produces positive results• The results can be attributed to the
program itself rather than other extraneous factors
• The evaluation is peer reviewed by experts in the field
• The program is “endorsed” by a federal agency or a respected research organization

More on why evidence is important…
• Improves quality of care and services• Increases likelihood of achieving desired
outcomes• Have carefully described service
components• Improve consistency in delivering services
–fidelity to model• More efficient use of available resources
What does it mean to be evidence-informed?
• The program articulates a theory of change and specifies identified outcomes through a detailed logic model.
• The practice has a book, manual or training that specifies the practice protocol.
• The practice is generally accepted in clinical practice.
• Requires less rigorous research to support its efficacy as a program or practice.

Parent Partner program
• Celebrates individuals how have overcome obstacles through change, recovery and accountability by using their skills to mentor families who are currently navigating through DHS system.
• Parent partners demonstrate advocacy and effective communication, while holding families accountable in meeting their case plan goals.
• Often the parent partner has personal experience with domestic violence, substance abuse and mental health and it is those experiences that make parent partners beneficial to the families currently receiving DHS services due to protective concerns.

Parent Partner program• Parent partners will:
– Work intensively with parents to promote engagement in case plan activities
– Maintain connections between parents and children– Share insight and understanding about personal
experiences that will assist parents to be successful– Assist in the goal of reunification, or in the
development of alternative permanency goals– Connect parents with resources needed to
complete the case plan– Provide encouragement, outreach and support – Act as a role model, mentor, a resource and
support.

24/7 Dad’s program• 24/7 Dad’s program is a 12-week evidence based
curriculum that empowers males to become more involved, responsible, and committed in their role as a father-figure.
• The program focuses on improving father’s self-awareness, caring for self, fathering skills, parenting skills and relationship skills.
• The program covers the universal aspects of fatherhood so that men of all cultures, races, religions and ethnic backgrounds can benefit.
• The program is designed to provide empowerment and support in a father friendly environment.

Strengthening Families
• An evidence based prevention program focusing on increasing family skills to support health child development.
• The program includes parenting skill sessions that address positive communication, family functioning, discipline and guidance.
• The children’s sessions focus on social-emotional development, communication skills, and healthy behavior.
• The family sessions include structured activities and the opportunity to practice new skills.
Celebrating Families!
• A 16-week evidence based program that addresses the needs of children and parents in families that have serious problems with alcohol and other drugs.
• Each session begins with a family meal. Afterwards family members break into age groups for developmentally appropriate activities led by group facilitators.
• The model is developed for children of alcoholics/ addicts and their parents.

Celebrating Families!
• Break cycles of drug use and violence/abuse by teaching healthy living skills.
• Decrease use of drug and alcohol use and reduce relapse by teaching all members of the family about the disease of chemical dependency and its impact on families.
• Positively influence family reunification by integrating recovery into daily family life and by teaching healthy parenting skills.
Iowa Family Treatment Court analysis

Adult Indicator Highlights – Access to Treatment
6 FDC Si
tes
Matc
hed Compariso
n
Referred Compari
son
0
20
40
60
80
100
120
3.1 27.017.9
96.9 73.082.1
Entered treatmentDid not enter treatmetn

Adult Indicator Highlights – Time from Assessment to Treatment
6 FDC SitesMatched
Comparison Referred Comparison
0
10
20
30
40
50
60
70
80
31.730.9
30.7
44.4
32.130.7
0 to 7 days8 to 30 days

Adult Indicator Highlights – Time from FTC entry to treatment
6 FDC SitesMatched
Comparison Referred Comparison
0
20
40
60
80
100
120
140
15.3
88.9
46.0
84.7
11.1
54.0 Entered treatment more than 7 days after FTC entryunknown

Adult Indicator Highlights – Care assessed matches level received
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
15.1 18.816.2
84.9 81.283.8 Level assessed matches
with level receivedLevel assessed differs from level received

Adult Indicator Highlights – Percentage successfully completing first treatment
episode
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
34.9 43.7 54.5
65.1 56.3 45.5
Successfully completed first episode of treatmentDid not complete first episode of treatment

Adult Indicator Highlights - Retention in Treatment
6 FDC SitesMatched
Comparison Referred Comparison
0
50
100
150
200
250
233
66 100
Average number of days in treatment for first episode

Adult Indicator Highlights - Methamphetamine use by parents
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
86.3 100
75.0
9.4
3.6
4.3
21.4
No change in Meth useIncrease in Meth UseDecrease in Meth Use

Adult Indicator Highlights -Alcohol use by parents
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
90.1
70.8 75.8
8.3
8.3 2.8
1.6
20.8 21.4
No change in Alcohol useIncrease in Alcohol useDecrease in Alcohol use

Adult Indicator Highlights - Marijuana use by parents
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
84.8 89.5
71.9
10.6
9.4
4.510.5
18.8
No change in Marijuana useIncrease in Marijuana useDecrease in Marijuana use

Adult Indicator Highlights - Criminal behavior by parents
6 FDC SitesMatched
Comparison Referred Comparison
75
80
85
90
95
100
85.084.8 84.3
13.112.1
13.4
0.5 3.0 2.2
Increase in arrests between intake and dischargeDecrease between intake and dischargeNo arrests at intake and discharge

Adult Indicator Highlights - Employment
6 Pilot Sites Matched Comparison
Referred Comparison
0
10
20
30
40
50
60
70
57.6
41.5
62.7
29.446.2
26.2
12.9 12.3 11.1
UnemployedFT EmployedPT Employed
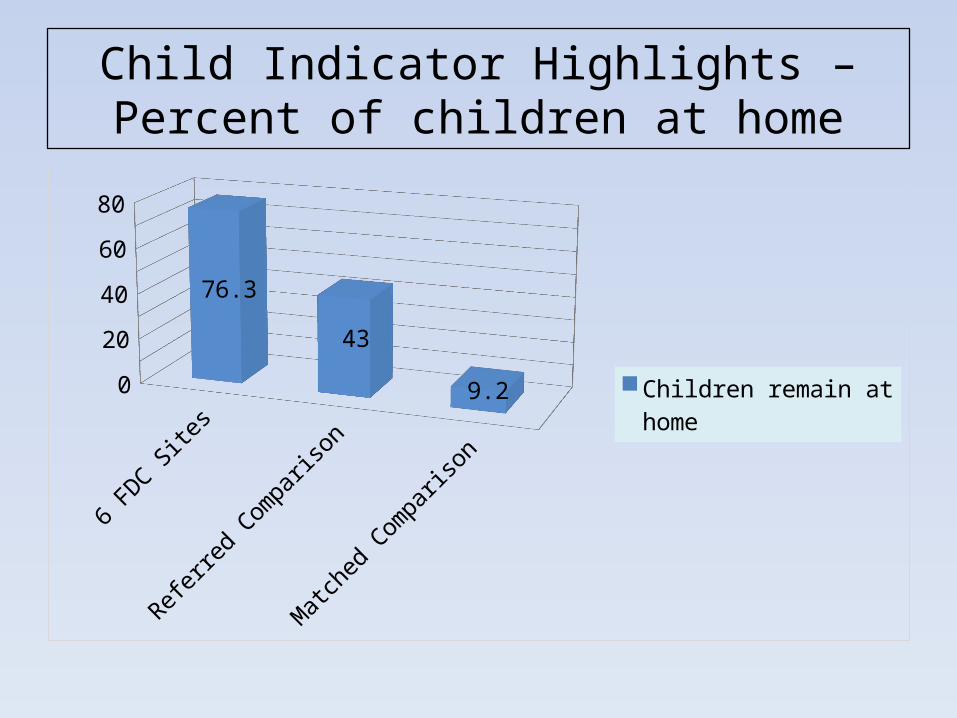
Child Indicator Highlights – Percent of children at home
6 FDC SitesReferred
Comparison Matched Comparison
0
10
20
30
40
50
60
70
80
76.3
43
9.2
Children remain at home

Child Indicator Highlights – Occurrence of maltreatment
6 FDC SitesMatched
Comparison Referred Comparison
9191.5
9292.5
9393.5
9494.5
9595.5
96
94.9
92.9
96Percent of childen who did not have a substanti-ated/indicated mal-treatment within 6-months of entry

Child Indicator Highlights – Occurrence of maltreatment
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
79.972.4 85.4
20.127.6 13.6
Substantiated or indicated maltreatmentNo substantiated or in-dicated maltreatment

Child Indicator Highlights – Average Length of Stay in Days
6 FDC SitesMatched
Comparison Referred Comparison
0
50
100
150
200
250
300
350
400
450
337 350445 Average length of stay in
foster care - days to reuni-fication

Child Indicator Highlights – Reunification Rates
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
72.7
52.451.4
27.3
47.648.6
Not Reunified Reunified

Child Indicator Highlights – Remained in Home
6 FDC SitesReferred Comparison
0102030405060708090
100
23.757
76.3
43
Remained in home through closureRemoved from home prior to case closure
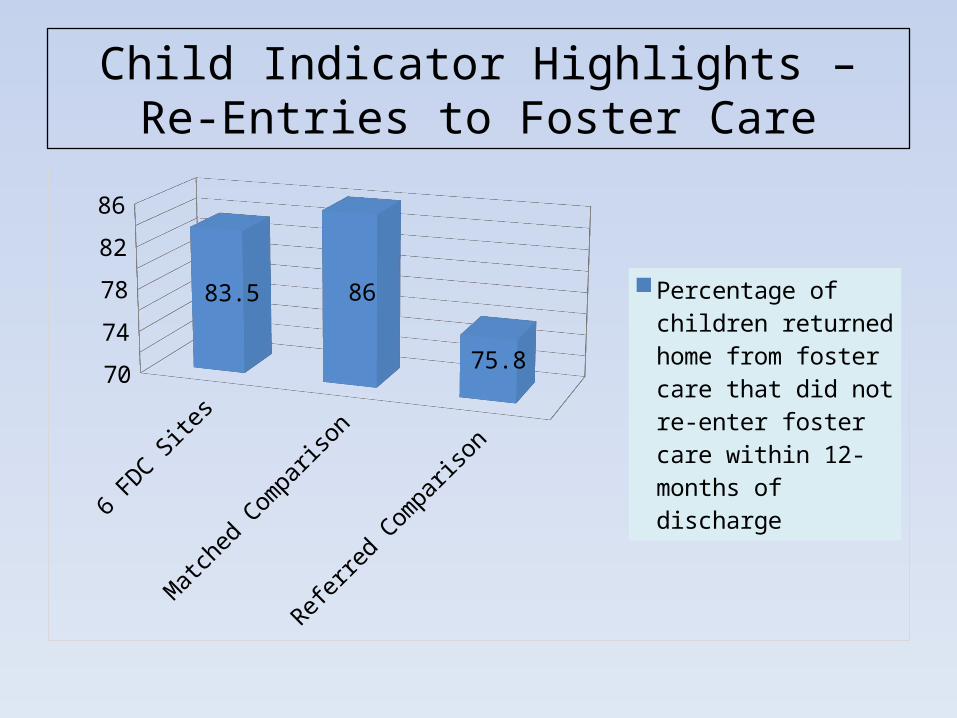
Child Indicator Highlights – Re-Entries to Foster Care
6 FDC SitesMatched
Comparison Referred Comparison
70
72
74
76
78
80
82
84
86
83.5 86
75.8
Percentage of children returned home from fos-ter care that did not re-enter foster care within 12-months of discharge

Child Indicator Highlights – Re-Entries to Foster Care
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
75.269.8
64.8
24.830.2
35.2
Re-entered foster careDid not re-enter foster care

Child Indicator Highlights – Timeliness of Reunification
6 FDC SitesMatched
Comparison Referred Comparison
0
10
20
30
40
50
60
70
80
90
77.6 81.4
61.5
Pecentage of children physically reunified in less than 12-months from date of first foster care entry

Child Indicator Highlights – Timeliness of Reunification
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
22.418.6
38.5
77.681.4
61.5
Legally reunified within 12-monthsLegally reunified greater than 12-months

Child Indicator Highlights – Timeliness of Permanency
6 FDC SitesMatched
Comparison Referred Comparison
62
64
66
68
70
72
74
76
75.974.4
67.1
Percent of children in foster care, who in less than 24-months from date of most recent fos-ter care placement, achieved adoption or guardianship

Child Indicator Highlights – Achieving Permanency within 24-mos.
6 FDC SitesMatched
Comparison Referred Comparison
0102030405060708090
100
75.974.4
65.2
24.1 25.634.8
Permanency greater than 24 mos.Permanency within 24-mos.




Cost avoidance summary…
• There is a relationship between greater resources spent on parent substance abuse treatment and current and future child welfare savings.
• Compared to non-program participants, FTC participants have:– Higher costs due to:
• A greater percentage of parents receiving substance abuse treatment and staying in treatment longer; and
• More children in out of home care at the start of the program (placement decisions were made prior to enrollment.
– Cost avoidance due to:• A higher reunification rate• More children being able to remain in custody of a
parent; and• Shorter foster care episode lengths of stay.
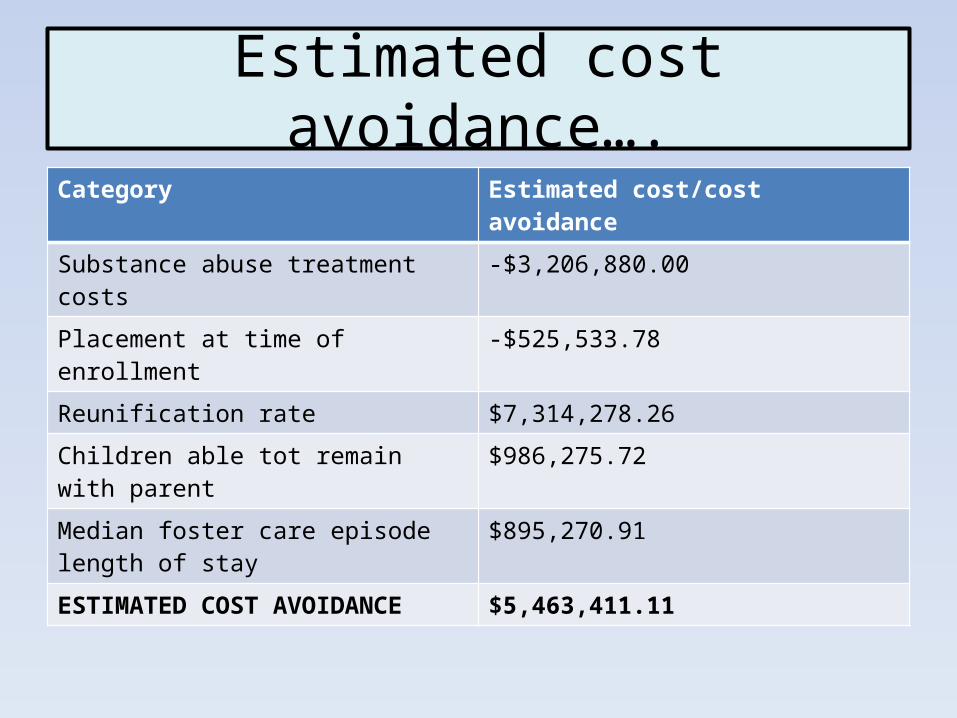
Estimated cost avoidance….Category Estimated cost/cost avoidance
Substance abuse treatment costs -$3,206,880.00
Placement at time of enrollment -$525,533.78
Reunification rate $7,314,278.26
Children able tot remain with parent $986,275.72
Median foster care episode length of stay $895,270.91
ESTIMATED COST AVOIDANCE $5,463,411.11
Why we do this work…

To Contact Me
Hon. William S. Owens
Associate Juvenile Judge
101 West Fourth Street, Suite 401
641-683-1791
A special thanks to: Doyle Evans, Kathy Thompson and Gail Barber – Iowa Children’s Justice – for the
Iowa Statistics for Family Treatment Court.
**National statistics courtesy of NADCP