“work empowerment as perceived by nurses and...
TRANSCRIPT

“Work Empowerment as Perceived by Nurses and Physicians Working
at National Heart Institute”
By
Dr. / Fatma Hamdy Hassan
Professor of Nursing Administration
Faculty of Nursing; Ain Shams University

2
The present study was derived from the M.Sc. thesis done by Mrs.
/Enayat Thabet Yakob under supervision of the author and Dr. Samia
Adam; Lecturer of Nursing Administration.
Introduction & Review of Literatures
Nowadays, many seek power but few possess it. Nurses are not
exception (Marquis and Huston, 2000). In health care settings, an unequal
power base exists among administrator, physicians, and nurses as a result
of the competing goals of administration and the coexistence of multiple
lines of authority (Sabiston and Laschinger, 1995). The rigidity of
hierarchical rule-bound structures has been specifically blamed for nurses’
inability to sufficiently control the content of their practice (Laschinger and
Havens, 1996).
Kanter (1993) proposed that an individual’s effectiveness on the job
is influenced largely by organizational aspects of the work environment.
This author identified power and access to opportunities to learn and grow,
as structural determinants affecting the behavior of the individual. This
power is derived from the ability to mobilize information, support, and
resources necessary for getting the job done.
Access to these empowering structures is influenced by the degree of
formal and informal power an employee has in the organization (Kanter,
1993). Formal power evolves from having a defined job that affords
flexibility, visibility and centrality to organizational purpose and goals.
Informal power is determined by the extent of employee’s networks and
alliances with sponsors, peers, and subordinates within the organization.

3
Access to these empowering structures has a positive impact on
employees, resulting in increasing their job satisfaction, level of
organizational commitment of and feelings of autonomy. Consequently,
employees are more productive and effective in meeting organizational
goals (Dutcher and Adams, 1994; Laschinger et. al., 1999).
Nurses’ autonomy or control over work was seriously limited by
unequal power relationships with medical staff, which enhanced physician
power and restricted the nurses’ freedom, and consequently hindered their
empowerment (Skelton, 1994; Fulton, 1997; McParland et al., 2000).
To achieve excellence in nursing requires empowered staff nurses in
order to be effective in their roles, and to be more autonomous (Marquis
and Huston, 2000). Nurses who perceive themselves to be empowered are
more likely to enhance client care through more effective work practice.
Thus by providing the sources of job-related empowerment and autonomy,
work methods and outcomes could be improved (Kanter, 1993; Sabiston
and Laschinger, 1995).
Empowerment
In the view of Hawks (1992), empowerment is the interpersonal
process of providing the proper information, support, resources and
environment to build, develop and increase the ability and effectiveness of
individuals to set and achieve organizational goals. It occurs between two
or more people, the person who empowers i.e. the manager, and the person
(s) who is (are) empowered, i.e. employee (s).
Baker and Young (1994) have claimed that empowerment occurs
when leaders communicate their vision, employees are given the

4
opportunity to make the most of their talents, and learning, creativity and
exploration are encouraged.
In simple terms, empowerment would appear to be the process of
enabling or imparting power transfer from one individual or group to
another. It includes the elements of power, authority, choice and
permission (Rodwell, 1996).
To feel empowered, in the context of new employment relationship,
means to understand the purpose and contribution of our work, and to
believe that we are ultimately responsible for the work we do, the service
we provide, and our own continual development and growth, personally
and professionally (Cassidy and Koroll, 1994).
Empowerment connotes sharing influence and power rather than
striving to enhance one’s power by taking it from others (Mason, et. al.,
1991). Empowerment focuses more on solutions than on problems. It
includes enabling people to recognize their strength, rights, abilities and
personal power (Rissel, 1994). In organizational settings, empowerment is
creating and sustaining a work environment that facilitates the employee’s
choice to invest in and own personal actions and behaviors resulting in
positive contributions to the organization’s mission (Cassidy and Koroll,
1994; Marquis and Huston, 2000).
Job Related Empowerment Factors
According to Kanter (1993), people are empowered to reach
organizational goals if their work environments are structural in ways that
provide access to information, support and resources necessary to getting
the job done, as well as opportunities to learn and grow. These
organizational structures are important determinants that affect behavior of

5
the individual. The author considers them as job related empowerment
factors.
Information
Information refers to the data, technical knowledge, and expertise
required to function effectively in one’s position (Laschinger and Havens,
1996). Information is defined as knowledge about work goals, plans,
organizational decisions, and changes in policies, environmental
relationships, and future decisions in an organization (Kanter, 1993;
Schermerhorn,1999).
Access to information is accomplished by providing staff members
with information beyond what is required to carry out specific patient care
on their unit, and becoming more familiar with the issues that affect them
and their jobs (Farley, 1989; Bruhn and Chesney, 1995). Access to
information represents an important source of power (Mintzberg, 1990). In
popular terms, “information is power”.
Support
Support is described by Kanter (1993) as the feedback and guidance
received from superiors, peers, and subordinates. Longest (1996) has
added that support is backing, acknowledgment of achievements,
endorsement, legitimacy, approval, advice, and problem solving of the
work environment.
According to Champan (1993), support can be divided into two
broad categories: material and psychosocial. Material support includes
money, equipment, supplies and the physical environment. Psychosocial
support is primarily in terms of expert cognitive advice from the manager.

6
Such structure helps the work group to do the job and share responsibilities
(Coffey and Coleman, 2001).
Interaction is necessary for support, and usually involves reciprocity
expectations (Stichler, 1995). For these reasons, support occurs with stable
or continuing relationships developed with co-workers. Although
managers are responsible for supporting employees, the strongest support
relationships may be among co-workers (Huddleston, 1999).
Resources
According to Carbonu and Soares (1997), the success of
empowerment is linked to resources. Access to resources is the most
critical empowerment factor (Marquis and Huston, 2000). Access to
resources refers to the ability to exert influence in the organization to bring
in needed materials. Examples of these are equipment, supplies, space, and
human resources necessary to do the job. They also include financial
resources such as funds, time, budget allocation, recognition for work, etc.,
and other supplies needed to do the job
efficiently and effectively in the organization (Chandler, 1991;
Sabiston and Laschinger, 1995).
Opportunities
The structure of opportunity is described by Kanter (1993) as the
chances for growth and mobility in the organization. It involves chances to
increase knowledge and skills, competencies of individuals, give them
recognition and rewards, provide possibilities for their growth and
advancement in their positions, and to participate on committees, task
forces, and interdepartmental work groups (Dibert and Goldenberg, 1995;
Soeren et al., 2000).

7
Managers empower subordinates when they delegate assignments to
provide learning opportunities and allow employees to share in the
satisfaction derived from achievement (Marsick and Watkins, 1996).
Managers are responsible for developing, upgrading employee’s
knowledge, skills and attitudes, to improve work methods and outcomes
that create productive work environments (Gillies, 1994). This can be
achieved through planning, development and implementation of
educational programs
(Lehmann, 1994). Provision of educational opportunities to expand
knowledge and skills has become a reward function that supports
motivation, and positively reinforces the employee’s autonomy, job
satisfaction and organizational commitment (Wiles et al., 2001).
Formal and Informal Power
Power is the ability to exert influence over others. Kanter (1993) has
stated that access to job-related empowerment factors, is facilitated by
formal and informal systems of power in the organization.
Formal Power
Formal power pertains to the authority inherent in the job position.
Formal power is the result of performance of job activities that are extra-
ordinary,
visible and relevant to the organizational problems and evolves from
positions that allow flexibility, creativity, and innovation (Kanter, 1993;
Stahl, 1995).

8
Extra-Ordinary Activities
Hoelzel (1989) and Gordon (1993) emphasize that if tasks are non-
routine and must be continually adjusted; those who make decisions
concerning these tasks have control over work and thereby acquire power.
Nursing administrators should examine the implications of task
routinaization in order to assign routine tasks to less skilled personnel
(Edward, 1994; Kreitner and Kinicki, 1998)
Visibility
For activities to enhance power, they have to be visible, and to attract
the notice of other people (Kanter, 1993; Smith, 1997). It is also possible
to gain visibility through increasing the relationships nurses have
throughout the organization by creating opportunities for staff nurses to
participate on interdepartmental committees and task forces. Furthermore,
recognition of employee achievements is an important component of
maintaining successful work teams that improves staff quality of work life
in current work environments, thus leading to improved productivity
(Sohier, 1992; Rocchiccioli and Tilbury, 1998).
Relevance
In the view of Rocchiccioli et al. (1998), relevance or centrality is
the degree to which activities are connected within a system. A subunit is
seen central if the activities performed are linked with the other activities of
the organization. Furthermore, Hoelzel (1989) emphasized that because
nursing participates in all aspects of patient care; the nursing department is
centrally linked with other hospital departments, and is critical to the
workflow of the organization.

9
Informal Power
Power is not automatic with the designation of authority, and is often
strengthened through the informal power (Kanter, 1993). The informal
social network plays a significant role in the exercise of power. It is almost
a necessity for power to come from social connections, especially those
outside of the immediate work group (Thompson, Melia and Boyd, 1995;
Catalano, 1996). Informal power results from alliances with sponsors,
peers and subordinates in the organization (Laschinger and Havens, 1996).
Sponsors
Sponsors have been found to be important in the careers of managers
and professionals in many settings. They are higher in the hierarchy than
those sponsored, and act as teachers or coaches whose functions are
enabling a young person to move effectively through the organizational
system (Gordon, 1993; Kanter, 1993).
Sponsors often provide the occasion for lower level organization
members to bypass the hierarchy; to get inside information, or to cut red
tapes. This could be very important to formal job success (Kelly and Joel,
1996; Hein, 1998).
Peers
According to Richard (1990) and Dutcher and Adams (1994) peer
alliances means the relationship between colleagues. This relationship can
be collaborative and supportive. Turning to colleagues for advice and
support empowers them, and expands one’s own power base at the same
time.

10
Beyers (1999) identified the components of collegial
communications as confidence, trust, mutual support, friendliness,
enjoyment, and team efforts toward goal achievement, creativity, open
communication, freedom from threat and the amount of interpersonal
contact in the job. Higher peer acceptance is necessary to any power base
or career success. Furthermore, it facilitates coordination among
interdependent units, and also can be used for joint problem solving
(Sullivan and Decker, 1997).
Subordinates
Alliances with subordinates are important when a supportive team is
required to carry out the mission of the organization or department (Kanter,
1993). The manager needs to provide subordinates with enough
information about organizational and unit goals, so that they understand
how their efforts and those of their manager are contributing to goal
attainment. This can be done by being a source and role model to
subordinates (Fitzpatrick, 1997; Marquis and Huston, 2000). These
alliances are effective method to coordinate activities among personnel,
and to use resources of time and abilities effectively (Sullivan and Decker,
1992; Griffin, 1994).
Autonomy
According to Stahl (1996) and Ellis and Hartely (2000), professional
employees indicate they want autonomy for practicing their profession, and
for making decisions about their work. They do not want their decisions
made for them by hospital administrators, physicians, or others.
Gillon (1995) has mentioned that autonomy is “the capacity to think,
decide, and act on the basis of such thought and decision freely and

11
independently and without hindrance”. Autonomy involves the right of the
individual to take independent action based upon his/her unique values and
desires. Additionally, it involves the right of self determination, and
freedom (Blegen et al., 1993; Aiken, 1994).
Autonomy does not mean the nurse will have total control, but the
autonomous nurse is free to choose when control should be abdicated or
retained. More simply stated, autonomy is the freedom to act on what one
knows (Kramer and Schmalenberg, 1993; Castledine, 1999). It means self-
directed clinical practice for individual nurses (Cassidy and Oddi 1991 and
Chitty, 1993). Professional nurse autonomy is the belief in the centrality of
the client when making responsible discretionary decisions. It reflects
advocacy for the client (Wade, 1999).
Kelly and Joel (1999) have emphasized that the keys to autonomy as
applied to nursing care are that no other profession or administrative force
can control nursing practice and that the nurse has latitude in making
judgment in patient care with the scope of nursing practice defined by the
profession.
Subjects and methods
Present study aims at investigating nurse’s and physicians’
perception of work empowerment available to nurses at work through: (1)
Identifying nurses and physicians perception of empowerment factors
available at work. (2) Describing nurses and physicians perceptions of
autonomy. (3) Examining the relationship between nurses’ perceptions of
job related empowerment and their perception of autonomy.

12
Setting
The study was conducted in different units at the National Heart
Institute, Imbaba-Giza, affiliated to the General Organization for Teaching
Hospitals and Institutes. The study units included open heart intensive care,
coronary care, medical/surgical, outpatient, emergency units and operating
theatres.
Subjects
Study subjects included two main groups; nurses and physicians.
They were all fulfilling the criteria of being fulltime employed in the
setting for a period of at least one year.
1. The Nurses Group
The nurses group included two different groups of nurses; staff
nurses and head nurses. Each represents a different level and category of
personnel in the nursing department organizational chart.
Staff Nurses Group
A consecutive sample of 117 staff nurses were selected from a total
number of 202 nurses working in the above mentioned study units. Their
work responsibilities included the provision of total nursing care to patients
in the study units.
Head Nurses Group
A total number of 17 head nurses were included. They represent all
available head nurses in charge of management of above mentioned study
units.

13
2. Physicians Group
Consecutive samples of 58 physicians were selected from a total
number of 82 physicians who have been working in the above mentioned
units as residents, assistant specialists and specialists.
Tools of Data Collection
The data for this study were colleted by using two types of
questionnaire sheets, one for nurses groups and the other for physicians
group. Both questionnaires aim to assess respondent’s perception of nurses’
empowerment. The questionnaire was divided into four main sections.
The first section is the condition of work effectiveness questionnaire
adopted from Chandler (1986). It contains 35 statements about job related
empowerment factors available to nurses at work. These were categorized
under the four subsections namely; opportunities (8 statements),
information (8 statements), support (10 statements) and resources (9
statements).
The second section was the job activities scale developed by
Laschinger et al. (1993). The scale includes 12 statements related to formal
power characteristics (jobs that provide recognition, relevance, and
discretion).
The third section was the organizational relationships scale
developed by Laschinger et al (1993). This instrument included 24
statements for assessing informal power or political and social alliances in
a job setting.
The fourth section was the job description questionnaire developed
by Sabiston and Lascginger (1995). This instrument includes “10”

14
statement about respondents perception of autonomy defined as control
over work.
Respondents were asked to indicate their opinion on a 5 points Likert
scale ranging from “1” (none) to “5” (a lot). The job related empowerment
score was obtained by adding the means for the four subsections with a
possible range from 4 to 20, denoting availability of evidence. Theses
scores were linearly converted into a percent score by dividing the obtained
score by the maximum attainable score, and multiplying by 100. These
percent scores were expressed in mean. The higher the mean score, the
more empowered the respondents perceived work empowerment. For
individual items of the scale, a score of <=3 on the Likert scale was
considered disagree with the item, while a score of >3 was considered
agree with the item.
Results & Discussion
Table (1) shows scores related to work empowerment factors, power
and autonomy as reported by nursing and physicians groups. According to
the table all the studied groups generally reported low level scores related
to nurses’ access to work empowerment, power or autonomy. Difference
between scores was statistically significant (p<0.05).
The lowest scores in relation to all empowerment factors were
reported by staff nurses. However, physicians had their highest scores in
the two variables; job-related empowerment and power. Meanwhile, head
nurses had the highest scores (59.3) of autonomy.
physicians point of view denoting that nurses have more access to
both the work empowerment factors and power, than do nurses themselves

15
might reflect a lack of familiarity and clarity on the part of medical staff
with the extend of having these factors available to nurses.
Study findings suggest that head nurses perceive themselves as
having greater access to empowering factors than do staff nurses. It is
known that higher level in the hierarchy which head nurses possess provide
them with more power as well as, better chances for access to available
work empowerment factors (Kanter, 1993).
It is evident that the nursing and physicians groups perceived certain
factors as more empowering than others. For access to support in nurse’s
current jobs, both nursing and physicians groups rated it as the highest
empowering factors, followed by access to opportunities, then availability
of resources, while access to information was rated as the least empowering
factor.
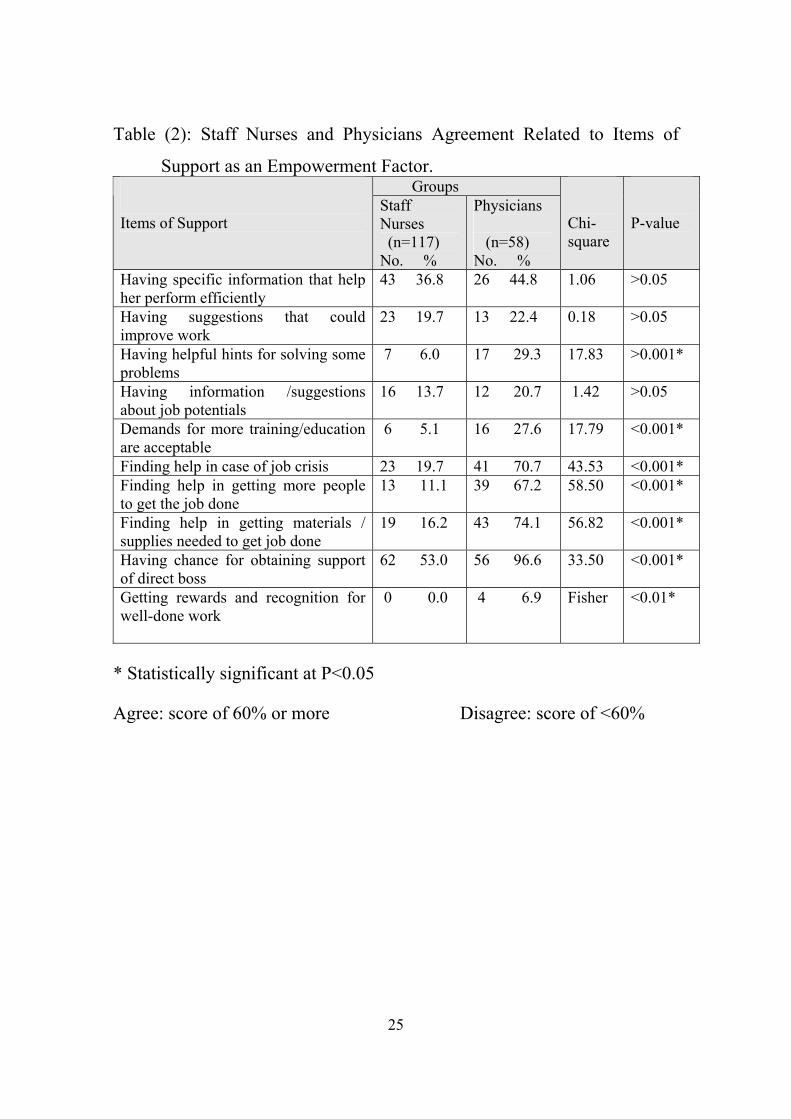
Among items denoting access to support (table 2), majority of the
studied physicians, (96.6%) compared to slightly more than one half (53%)
of the staff nurses, reported that nurses are having the chance to work
closely with their direct bosses. Conversely, none of the staff nurses and
6.9% of the studied physicians agreed that the nurse was getting rewards
and recognition for well-done work.
Table (3) was concerned with opportunities as an empowerment
factor in nurses’ work. Findings revealed that the highest percentage of the
staff nurses and physicians (62.4% and 91.4%; respectively) agreed that the
nurse was having the chance to work closely with her direct supervisor.
The aforementioned result could be expected because more than one
half of the nursing subjects in the present study were employed in the
critical care units. Traditionally, critical care areas have offered nurses

16
excellent opportunities challenging work either in their contact with patient
or with the health team members. Moreover, nurses working in these units
have opportunities to learn new skills and knowledge.
As regards to availability of resources as an empowerment factor
(table 4), the percentages of agreement of staff nurses on availability
resources for wok were very low, with a maximum of 21.4% and minimum
of 0%. Physicians reported a higher agreement level; that was significantly
or high significantly different. Agreement related to availability of time for
nurses to accomplish required tasks was reported by majority (93.1%) of
physicians compared to about one fifth of the staff nurses.
On the same line, Raatikainen (1994) has emphasized that
unavailability of resources limits nurses’ capacity to work properly.
Besides, it could create problems among nurses and between nurses and
other members of the health team. It could also negatively affect patients’
perception of nurses as competent professionals. Therefore nurses cannot
perform their work effectively and efficiently without resources.
The lower access to information (table, 5) reported by studied nurses
and physicians groups could be attributed to lack of communication. On the
same line, Wilson and Laschinger (1994) mentioned that the place of staff
nurses at the bottom of the hierarchy could result in limited opportunities to
access communication channels available within the organization.
Table (6) demonstrates agreement related to items of formal power
available to nurses at work. As shown in the table the percentages of
agreement reported by staff nurses and physicians were very low. On one
hand, the item with the highest rate of agreement among staff nurses (41%)
and physicians (93.1%) was that related to the current hospital problems

17
affecting nurse’s job functions. On the other hand, none of the staff nurses
agreed that the nurse was getting incentives for extraordinary work. The
lowest agreement in the physician group was in relation to the item of
clarity of activities related to the nurse work in the hospital (1.7%).
Table (7) clarifies the agreement related to items of informal power
as reported by the studied nurses and physicians. The figures in the table
indicate that staff nurses had very low percentages of agreement about all
items, with exception of that related to “collaborating with physicians in
patient care”. The later, had the highest percent of agreement both among
staff nurses (81.2%) and physicians (98.3%). Meanwhile, the item of
having opportunity to increase nurse’s efficiency outside her unit was the
item with lowest agreement in the two groups. Only 0.9% of the staff
nurses and none of the physicians have agreed upon it.
According to table (11) low level of perceived nurses’ autonomy was
reported by both nurses and physicians. The highest percent of staff nurses
agreement was related to having control over the pace of her work, whereas
the highest percentage of studied physicians (70.7%) agreed that the nurse
was having the freedom to perform her job functions independently of her
supervisor. Alternatively, it was noticed that only 4.3% of the staff nurses
and none of the studied physicians agreed that the nurses’ job allows her to
make decisions on her own.
Moreover, the results show that the studied physicians had
statistically significantly higher percentage of agreement (p<0.05) on the
statements such as: “the nurse left on her own to accomplish her work’,
“the nurse having the freedom to perform her job functions independent of
her supervisor”, and “the nurses’ job allows her to express her opinions at
work”.

18
Recommendations
• Nurse managers must provide staff nurses by sources of job-related
empowerment, namely access to opportunities, information,
support and resources.
• Nurses should be allowed to participate in decision making to
empower them, as well as increasing their feeling of autonomy.
• Committees should be established to allow nurses to form new
relationships, learn new skills, and gain recognition by having the
opportunity to demonstrate their abilities.
• Increasing the level of nursing education may be another key to
boosting the level of autonomy perceived nurses.

19
References
• Baker, A.M. and Young, C.E. (1994): Transformational
Leadership: The Feminist Connection in Postmodern
Organizations. Holistic Nursing Practice. 9 (1) 16-25.
• Bruhn , J.G. and Chesney, A.P. (1995): Organizational Moles,
Information Control and the Acquisition of Power. Health Care
Supervisor. 14 (1) 24-31.
• Carbonu, D.M. and Soares, J.M. (1997): Forensic Nursing in
Pakistan Bridging the Gap between Victimized Women and
Health Care Delivery System. Journal of Psychology in Nursing.
35 (6) 19-26.
• Cassidy, V.R. and Koroll, C.J. 91994): Ethical Aspects of
Transformal Leadership. Holistic Nursing Practice. 9 (1) 41-47.
• Champan, J. (1993): Collegial Support Linked to Reduction Job
Stress. Nursing Management. 24 (5) 52-55.
• Chandler, G. (1991): Creating an Environment to Empower
Nurses. Nursing Management. 22 (8) 20-23.
• Coffey, M., and Coleman, M. (2001): The Relationship between
Support and Stress in Forensic Community Mental Health
Nursing. Journal of Advanced Nursing. 34 (3) 397-407.
• Dibert, C. and Goldenberg, D. (1995): Preceptor’s Perceptions of
Benefits, Reward, Support and Commitment to the Preceptor
Role. Journal of Advanced Nursing. 7 (21) 1144-1151.

20
• Dutcher, L.A. and Adam, C.E. (1994): Work Environment
Perception of Staff Nurses and Aids in Home Health Agencies.
Journal of Nursing Administration. 24 (10) 24-30.
• Farley, M.J. (1989): Assessing Communication in Organization.
Journal of Nursing Administration. 19 (12) 27-31.
• Fulton, Y. (1997): Nurses’ View of Empowerment; a Critical
Social Theory Perceptive. Journal of Advanced Nursing. 26:
529-534.
• Gillies, D.A. (1994): Nursing Management; A System Approach.
2nd. ed. Philadelphia. W.B. Saunders Co. PP. 119, 407.
• Hawks, H.J. (1992): Empowerment in Nursing Education;
Concept Analysis and Application to Philosophy, Learning and
Instruction. Journal of Advanced Nursing. 17 (5) 609-618.
• Huddleston, D. (1999): Empowerment in Nursing Staff for
Optimal Job Performance. Journal of Nursing Administration.
29 (12) 5-16.
• Kanter, R.M. (1993): In: Sabiston, J.A. and Laschinger, H.k.
(1995): Staff Nurse Work Empowerment and Perceived
Autonomy; Testing Kanter’s Theory of Structural Power in
Organizations. Journal of Nursing Administration. 25 (9) 42-50.
• Kanter, R.M. (1993): Men and Women of the Corporation. 2nd.
ed., New York: Basic Books. PP. 166-174.
• Laschinger, H.K. and Havens, D.S. (1996): Staff Nurse Work
Empowerment and Perceived Control Over Nursing Practice;

21
Conditions for Work Effectiveness. Journal of Nursing
Administration. 26 (9) 27-35.
• Laschinger, H.K., Wong, C., Macmahon, L. and Kaufmann, C.
(1999): Leader Behavior Impact on Staff Nurse Empowerment,
Job Tension, and Work Effectiveness. Journal of Nursing
Administration. 29 (5) 28-39.
• Lehmann, R.S. (1994): Nursing Management Desk Reference
Concepts; Skills and Strategies. Philadelphia. W.B. Saunders Co.
PP. 198-210.
• Longst, B.B. (1996): Health Professionals in Managements.
Philadelphia. A Simon and Schuler Co., P. 40.
• Marquis, B.L. and Huston, C.J. (2000): Leadership Roles and
Management Functions in Nursing; Theory and Application. 3rd
ed., Philadelphia. Lippincott Co., PP. 34, 139.
• Marsick, V.J. and Watkins, K.E. (1996): Adult Educators and
The Challenge of The Learning Organization. Adult Learning. 7
(4) 18.
• Mason, D.J., Backer, B.A. and Georges, C.A. (1991): Toward a
Feminist Model for Political Empowerment of Nurses Image.
Journal of Nurses Scholarship. 23 (2) 72-77.
• McParland, J., Scott, P.A., Arndt, M., Dassen, T., Gasull, M. and
Lemonidou, C. (2000): Autonomy and Clinical Practice; 1;
Identifying Areas of Concern. British Journal of Nursing. 9 (8)
507.

22
• Mintzberg, H. (1990): The Power in and Around Organizations.
Journal of Nursing Administration. 20 (12) 15-22.
• Rissel, C. (1994): Empowerment: The Holy Grail of Health
Promotion? Health Promotion International. 9 (1) 39-47.
• Rodwell, C.M. (1996): An Analysis of the Concept of
Empowerment. Journal of Advanced Nursing. 23:305-313.
• Sabiston, J.A. and Laschinger, H.K. (1995): Staff Nurse Work
Empowerment and Perceived Autonomy; Testing Kanter’s
Theory of Structural Power in Organizations. Journal of Nursing
Administration. 25 (9) 42-50.
• Schermerhorn, J.R. (1999): Management. 6th ed. New York.,
John Wiley and Sons Co., PP. 262-267.
• Skelton, R. (1994): Nursing and Empowerment; Concepts and
Strategies. Journal of Advanced Nursing. 19:415-423.
• Soeren, V.M., Anderusyszyn, M.A., Laschinger, H.K.,
Goldenberg, D., and Dicenso, A. (2000): Consortium Approach
for Nurse Practioner Education. Journal of Advanced Nursing.
32 (4) 825.
• Stichler, J.F. (1995): In: Hojat, M; Nasca, T.J.; Cohen, M.J. and
Fields, S.K. (2001): Attitudes toward Physicians-Nurse
Collaboration; A Cross-Cultural Study of Male and Female
Physicians and Nurses in the United States and Mexico. Nursing
Research. 50 (2) 123.

23
• Wiles, R., Postle, K., Steiner, A., and Walsh, B. (2001): Nurse-
Led Intermediate Care; An Opportunity to Develop Enhanced
Roles for Nurses? Journal of Advanced Nursing. 34 (6) 818.

24
Table (1): Scores Related to Empowerment Factors, Power, and Autonomy
as Reported Nursing and Physicians Groups in the Study.
Study Subjects
Staff
Nurses
(n=117)
Head
nurses
(n=17)
Physicians
(n=58)
Study
Variables
X +-- X S.D. X S.D
ANOVA p-value
Job related empowerment factors
Opportunities
Information
Support
Resources Total
Empowerment
36.3+13.9
26.6+12.2
38.6+14.7
35.4+10.6
33.5+9.5
47.1+13.9
33.5+11.7
52.8+ 12.5
42.2+10.4
44.3+10.1
56.5+11.4
52.8+ 8.0
59.7+12.0
56.0+9.6
56.5+8.46
46.6
108.9
47.7
77.5
114.3
<0.001*
<0.001*
<0.001*
<0.001*
<0.001*
Power
- Formal
- Informal
23.6+9.3
37.0+11.6
35.7+12.6
48.7+12.1
53.1+11.4
55.3+8.5
160.1
58.2
<0.001*
<0.001*
Autonomy 39.2+18.5 59.3+16.9 52.9+11.5 20.0 <0.001*
* Statistically significant at P<0.05
25
Table (2): Staff Nurses and Physicians Agreement Related to Items of
Support as an Empowerment Factor. Groups
Items of Support
Staff Nurses (n=117) No. %
Physicians (n=58) No. %
Chi- square
P-value
Having specific information that help her perform efficiently
43 36.8 26 44.8 1.06 >0.05
Having suggestions that could improve work
23 19.7 13 22.4 0.18 >0.05
Having helpful hints for solving some problems
7 6.0 17 29.3 17.83 >0.001*
Having information /suggestions about job potentials
16 13.7 12 20.7 1.42 >0.05
Demands for more training/education are acceptable
6 5.1 16 27.6 17.79 <0.001*
Finding help in case of job crisis 23 19.7 41 70.7 43.53 <0.001* Finding help in getting more people to get the job done
13 11.1 39 67.2 58.50 <0.001*
Finding help in getting materials / supplies needed to get job done
19 16.2 43 74.1 56.82 <0.001*
Having chance for obtaining support of direct boss
62 53.0 56 96.6 33.50 <0.001*
Getting rewards and recognition for well-done work
0 0.0 4 6.9
Fisher <0.01*
* Statistically significant at P<0.05
Agree: score of 60% or more Disagree: score of <60%

26
Table (3): Staff Nurses and Physicians Agreement Related to Items of
Opportunities as an Empowerment Factor.
Groups
Items of Opportunities
Staff
Nurses
(n=117)
No. %
Physicians
(n=58)
No. %
Chi-
square
P-value
Good competition with peers 28 23.9 31 53.4 15.12 <0.001*
Chance to gain new skills and
knowledge at work
51 43.6 39 67.2 8.68 <0.005*
Access to training programs for
new learning
7 6.0 8 13.8 Fischer >0.05
Chance to work closely with
direct boss
37 62.4 53 91.4 16.16 <0.001*
Chance to learn how the hospital
works
2 1.7 4 6.9 Fisher >0.05
Tasks that need all of her skills
and knowledge
31 26.5 34 58.6 17.14 <0.001*
Chance of promotion at work 8 6.8 12 20.7 7.35 <0.01*
Getting incentive for tasks
achieved efficiently
0 0.0 5 8.6 Fisher <0.005*
* Statistically significant at P<0.05
Agree: score of 60% or more Disagree: score of <60%

27
Table (4): Staff Nurses and Physicians Agreement Related to Items of
Resources as an Empowerment Factor. Groups
Items of Resources
Staff Nurses (n=117) No. %
Physicians (n=58) No. %
Chi- square
P-value
Availability of supplies necessary for the job
23 19.7 35 60.3 28.97 <0.001*
Time available to do necessary paperwork
1o 8.5 19 32.8 16.44 <0.001*
Time available to accomplish required tasks
25 21.4 54 93.1 80.58 <0.001*
Acquiring temporary help when needed
21 17.9 25 43.1 12.66 <0.001*
Sharing in choosing rewards for her colleagues at work
0 0.0 2 3.4 Fisher >0.05
Getting rewards for a job well done
1 0.9 5 8.6 Fisher <0.05*
Unit decisions are influential in obtaining permanent manpower
12 10.3 24 41.4 22.99 <0.001*
Unit decisions are influential in obtaining supplies
17 14.5 40 69.0 52.32 <0.001*
Unit decisions are influential in obtaining special equipment
13 11.1 35 60.3 47.22 <0.001*
* Statistically significant at P<0.05
Agree: score of 60% or more Disagree: score of <60%

28
Table (5): Staff Nurses and Physicians Agreement Related to Items of
Nurses’ Information as an Empowerment Factor.
Groups
Items of Nurses’ Information
about
Staff
Nurses
(n=117)
No. %
Physicians
(n=58)
No. %
Chi-
square
P-value
The relation of the work of her
unit to the hospital
14 12.0 26 44.8 23.75 <0.001*
How nursing colleagues perform
their work
27 23.1 49 84.5 59.51 <0.001*
Goals of top management 3 2.6 0 0.0 Fisher >0.05
This year’s plan of her unit 5 4.3 1 1.7 Fisher >0.05
Salaries of work colleagues 16 13.7 41 70.7 57.39 <0.001*
Other departments’ opinions
about her unit
9 7.7 43 74.1 81.97 <0.001*
What patients think of the work
in her unit
36 30.8 51 87.9 50.68 <0.001*
Current hospital ambiance 1 0.9 12 20.7 Fischer <0.001*
* Statistically significant at P<0.05
Agree: score of 60% or more Disagree: score of <60%

29
Table (6): Staff Nurses and Physicians Agreement Related to Items of
Formal Power Available to Nurses at Work. Groups
Items of Formal Power
Staff Nurses (n=117) No. %
Physicians (n=58) No. %
Chi- square
P-value
Available bylaws regulating activities and job functions
5 4.3 30 51.7 54.57 <0.001*
Having a well-defined routine to accomplish her job
24 20.5 27 46.6 12.73 <0.001*
Having variability in the tasks related to her job
21 17.9 31 53.4 23.40 <0.001*
Getting incentives for extraordinary work
0 0.0 9 15.5 Fisher <0.001*
Getting incentives for outstanding work
2 1.7 9 15.5 Fisher <0.001*
Having flexibility in her job 13 11.1 15 25.9 6.28 <0.01* Availability of approvals for non-routine decisions
4 3.4 17 29.3 24.62 <0.001*
Declaring of nurses’ job activities 3 2.6 8 13.8 Fisher <0,01* Current hospital problems affect her job functions
48 41.0 54 93.1 43.25 <0.001*
Participation in educational programs in the hospital
1 0.9 11 19.0 Fisher <0.001*
Participation in solving problems 2 1.7 25 43.1 50.92 <0.001*Clarity of activities related her work in the hospital
2 1.7 1 1.7 Fisher 1.00
* Statistically significant at P<0.05
Agree: score of 60% or more Disagree: score of <60%

30
Table (7): Staff Nurses and Physicians Agreement Related to Items of
Informal Power Available to Nurses at Work.
Groups
Items of Support
Staff
Nurses
(n=117)
No. %
Physicians
(n=58)
No. %
Chi-
square
P-value
Collaborating with physicians on
patient care
95 81.2 57 98.3 9.91 <0.005*
Receiving positive feedback from
physicians about her work
55 47.0 50 86.2 24.83 <0.001*
Asking physicians for patients’
information
40 34.2 47 81.0 34.04 <0.001*
Having physicians appreciation 23 19.7 36 62.1 31.21 <0.001*
Physician use her opinions 11 9.4 11 19.0 3.23 >0.05
Giving opinions about
administrative aspects to her
supervisor
10 8.5 29 50.5 38.47 <0.001*
Direct supervisor makes use of
her opinions
14 12.0 33 56.9 39.85 <0.001*
Knows early about changes in
unit work from direct supervisor
22 18.8 33 56.9 26.11 <0.001*
Opportunity to increase her
efficiency outside her unit
1 0.9 0 0.0 Fisher 1.00
* Statistically significant at P<0.05
Agree: score of 60% or more Disagree: score of <60%

31
Table (8): Staff Nurses and Physicians Agreement Related to Items of
Nurses Autonomy.
Groups
Items of Support
Staff
Nurses
(n=117)
No. %
Physicians
(n=58)
No. %
Chi-
square
P-value
Left on her own to accomplish
her work
* Statistically significant at P<0.05
Agree: score of 60% or more Disagree: score of <60%