vitamin k prophylaxis contents in newborn infants
TRANSCRIPT
VITAMIN K PROPHYLAXISIN NEWBORN INFANTS
VITAMIN K AND HAEMORRHAGIC DISEASE OF THE NEWBORN
In NSW the practice of giving vitamin K to neonates to preventhaemorrhagic disease of the newborn (HDN) began in the 1950s. Initiallyit was given only to neonates considered to be at increased risk ofintracranial haemorrhage (ag. after difficult instrumental deliveries). In1971 the NSW Maternal and Perinatal Committee recommended that all
newborn infants receive vitamin Ki prophylaxis, and in subsequent years theintramuscular (IM) administration of 1mg of vitamin Ki (phytomenadione) atbirth became the universal regimen.
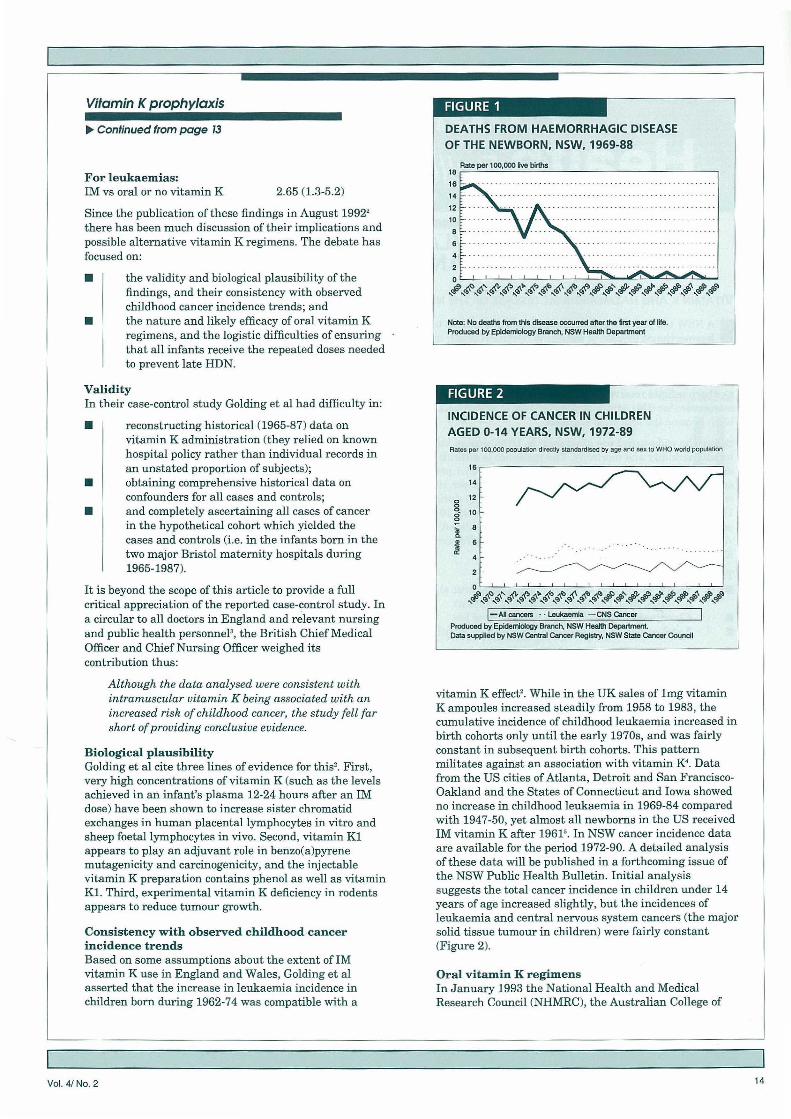
Before the widespread use of vitamin K, HDN was an important cause ofinfant morbidity and mortality. The incidence is difficult to assess, but 13deaths were attributed to HDN in NSW in 1969 (15.1 per 100,000 live births),and 14 deaths each year in 1970-71 (15.8 and 14.2 per 100,000 live birthsrespectively). Mortality from HDN declined sharply during the 1970s (Figure1), and a total of only four deaths was recorded in the 10 years 1980-89 (0.5per 100,000 live births). The incidence has also declined. That the condition isvirtually unknown in NSW today testifies to the effectivenesa of IM vitaminKin prevention.
Three types of HDN are recognised:•Early, in the first 48 hours of life, and almost always related to
maternal drug therapy (especially phenytoin)• Classical, in the second to seventh day of life• Late, occurring between one week and six months of age.
All three types present with a spectrum of severity ranging from slightbleeding to severe haemorrhage, and with a variety of possible bleeding sitesincluding the skin, umbilicus, gastrointestinal tract, circumcision site, orintracranial. Late HDN is the most likely to be severe and to present withintracranial haemorrhage.
VITAMIN K AND CHILDHOOD CANCERIn 1990 Golding et al published the results of a 10-year follow-up of arepresentative sample of 16,193 infants delivered in Great Britain in oneweek during 1970'. A case-control study of the 33 children identified ashaving cancer, with controls selected from the same cohort, suggested anassociation between cancer and prophylactic vitamin K given at birth toprevent HUN.
This unexpected finding led to a separate case-control study of childrendiagnosed with cancer between 1971 and 1991 and born in the two majorBristol maternity hospitals between 1965 and 1987. Exposure factors in thisstudy were vitamin K administration at birth (oral or IM) and pethidinegiven to the mother in labour. The main findings, expressed as odds ratiosand 95 per cent confidence intervals, were as follow&:
For all cancers:Oral vs no vitamin K 1.15 (0.5-2.7)IM vs oral or no vitamin K 1.97 (1.3-3.0)Pethidine vs no pethidine 1.05 (0.7-1.5)
Contents
[] Articles
13 Vitamin Kprophylaxisin newborn infants
16 Strategy aims to 4ftorgan donations
Infectious diseases
Public HealthAbstracts
[] Reader survey
Correspondence
Please address allcorrespondence and potentialcontributions to:
The Edito;NSW Public Health Bulletin,Public Health Divison,IVSW Health DepartmentLocked Bag No 961,North Sydney NSW 2059Telephone.' (02) 391 9218Facsimile.' (02) 391 9232
VoI.4/No.2 13
Vitamin K prophylaxis
Continued from page 13
For leukaemias:IM vs oral or no vitamin K 2.65 (1.3-5.2)
Since the publication of these findings in August 19922there has been much discussion of their implications andpossible alternative vitamin K regimens. The debate hasfocused on:
• the validity and biological plausibility of thefindings, and their consistency with observedchildhood cancer incidence trends; and
• the nature and likely efficacy of oral vitamin Kregimens, and the logistic difficulties of ensuringthat all infants receive the repeated doses neededto prevent late HDN.
ValidityIn their case-control study Golding et al had difficulty in:
• reconstructing historical (1965-87) data onvitamin K administration (they relied on knownhospital policy rather than individual records inan unstated proportion of subjects);
• obtaining comprehensive historical data onconfounders for all cases and controls;
• and completely ascertaining all cases of cancerin the hypothetical cohort which yielded thecases and controls (i.e. in the infants born in thetwo major Bristol maternity hospitals during1965-1987).
It is beyond the scope of this article to provide a fullcritical appreciation of the reported case-control study. Ina circular to all doctors in England and relevant nursingand public health personnel3, the British Chief MedicalOfficer and Chief Nursing Officer weighed itscontribution thus:
Although the data analysed were consistent withintramuscular vitamin K being associated with anincreased risk of childhood cancer, the study fell farshort of providing conclusive evidence.
Biological plausibilityGolding et al cite three lines of evidence for this2. First,very high concentrations of vitamin K (such as the levelsachieved in an infant's plasma 12-24 hours after an IMdose) have been shown to increase sister chromatidexchanges in human placental lymphocytes in vitro andsheep foetal lymphocytes in vivo. Second, vitamin Kiappears to play an adjuvant role in benzo(a)pyrenemutagenicity and carcinogenicity, and the injectablevitamin K preparation contains phenol as well as vitaminKi. Third, experimental vitamin K deficiency in rodentsappears to reduce tumour growth.
Consistency with observed childhood cancerincidence trendsBased on some assumptions about the extent of IMvitamin K use in England and Wales, Golding et alasserted that the increase in leukaemia incidence inchildren born during 1962-74 was compatible with a
DEATHS FROM HAEMORRHAGIC DISEASE
OF THE NEWBORN, NSW, 1969-88
I.I_I__r.jII__Ij______________________________
? rØ c #rlia.' \ . , \ \
Note: No deaths trots this disease occurred after the Itrot year at •Produced by Epidemiology Branch, NSW Health Department
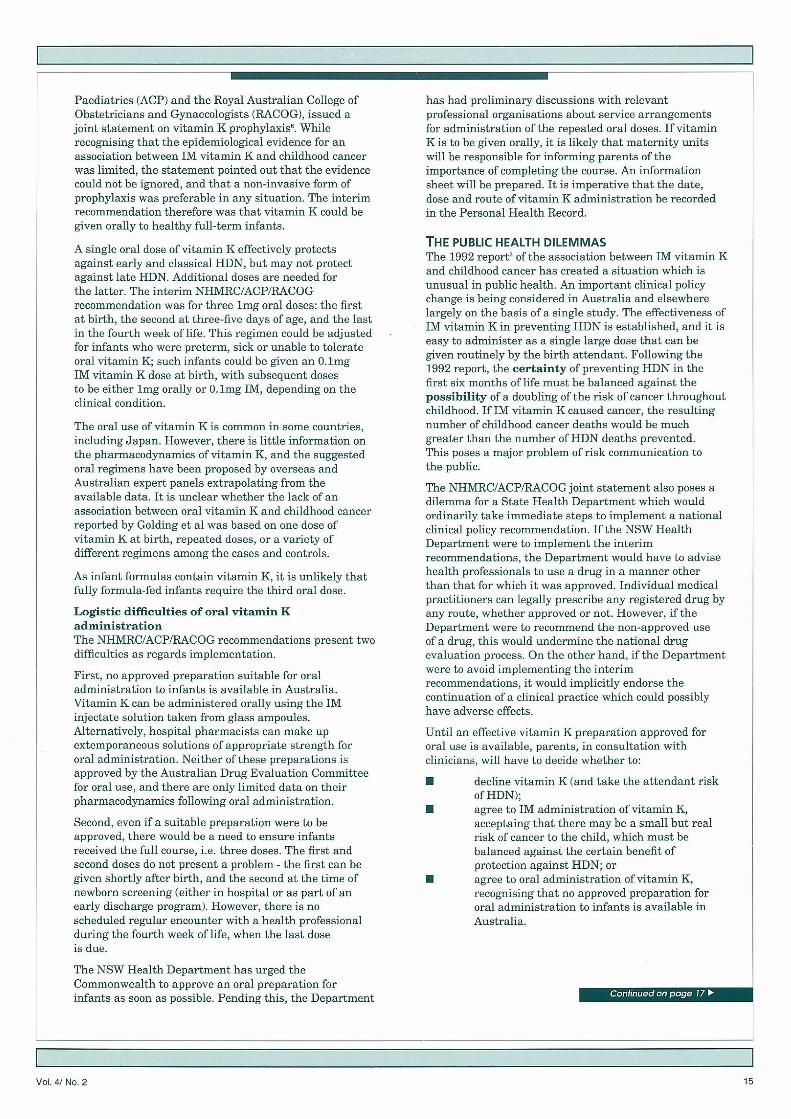
INCIDENCE OF CANCER iN CHILDRENAGED 0-14 YEARS, NSW, 1972-89Rates pn 100000 populat:or doecily standardised by age and sax to WHO world population
§Saaat 6
0 lL 11111 11111!
I-Allcancers - Leukeerria -CNS Cancer
Produced by Epidemiology Branch, NSW Health Department
L Data supplied by NSW CerWal Cancer RegisEy, NSW State Cancer Courtcfl
vitamin K effect2. While in the UK sales of 1mg vitaminK ampoules increased steadily from 1958 to 1983, thecumulative incidence of childhood leukaemia increased inbirth cohorts only until the early 1970s, and was fairlyconstant in subsequent birth cohorts. This patternmilitates against an association with vitamin K'. Datafrom the US cities of Atlanta, Detroit and San Francisco-Oakland and the States of Connecticut and Iowa showedno increase in childhood leukaemia in 1969-84 comparedwith 1947-50, yet almost all newborns in the US receivedIM vitamin K after 196 lb. In NSW cancer incidence dataare available for the period 1972-90. A detailed analysisof these data will be published in a forthcoming issue ofthe NSW Public Health Bulletin. Initial analysissuggests the total cancer incidence in children under 14years of age increased slightly, but the incidences ofleukaemia and central nervous system cancers (the majorsolid tissue tumour in children) were fairly constant(Figure 2).
Oral vitamin K regimensIn January 1993 the National Health and MedicalResearch Council (NHMRC), the Australian College of
VoI.4/No.2 14
Paediatrics (ACP) and the Royal Australian College ofObstetricians and Gynaecologists (RACOG), issued ajoint statement on vitamin K prophylaxis. Whilerecognising that the epidemiological evidence for anassociation between IM vitamin K and childhood cancerwas limited, the statement pointed out that the evidencecould not be ignored, and that a non-invasive form ofprophylaxis was preferable in any situation. The interimrecommendation therefore was that vitamin K could begiven orally to healthy full-term infants.
A single oral dose of vitamin K effectively protectsagainst early and classical HDN, but may not protectagainst late HDN. Additional doses are needed forthe latter. The interim NHMRC/ACP/RACOGrecommendation was for three 1mg oral doses: the firstat birth, the second at three-five days of age, and the lastin the fourth week of life. This regimen could be adjustedfor infants who were preterm, sick or unable to tolerateoral vitamin K; such infants could be given an 0.1mgIM vitamin K dose at birth, with subsequent dosesto be either 1mg orally or 0.1mg IM, depending on theclinical condition.
The oral use of vitamin K is common in some countries,including Japan. However, there is little information onthe pharmacodynamics of vitamin K, and the suggestedoral regimens have been proposed by overseas andAustralian expert panels extrapolating from theavailable data. It is unclear whether the lack of anassociation between oral vitamin K and childhood cancerreported by Golding et al was based on one dose ofvitamin K at birth, repeated doses, or a variety ofdifferent regimens among the cases and controls.
As infant formulas contain vitamin K, it is unlikely thatfully formula-fed infants require the third oral dose.
Logistic difficulties of oral vitamin KadministrationThe NHMRC/ACP/RACOG recommendations present twodifficulties as regards implementation.
First, no approved preparation suitable for oraladministration to infants is available in Australia.Vitamin K can be administered orally using the IMinjectate solution taken from glass ampoules.Alternatively, hospital pharmacists can make upextemporaneous solutions of appropriate strength fororal administration. Neither of these preparations isapproved by the Australian Drug Evaluation Committeefor oral use, and there are only limited data on theirpharmacodynamics following oral administration.
Second, even if a suitable preparation were to beapproved, there would be a need to ensure infantsreceived the full course, i.e. three doses. The first andsecond doses do not present a problem - the first can begiven shortly after birth, and the second at the time ofnewborn screening (either in hospital or as part of anearly discharge program). However, there is noscheduled regular encounter with a health professionalduring the fourth week of life, when the last doseis due.
The NSW Health Department has urged theCommonwealth to approve an oral preparation forinfants as soon as possible. Pending this, the Department
has had preliminary discussions with relevantprofessional organisations about service arrangementsfor administration of the repeated oral doses. If vitaminK is to be given orally, it is likely that maternity unitswill be responsible for informing parents of theimportance of completing the course. An informationsheet will be prepared. It is imperative that the date,dose and route of vitamin K administration be recordedin the Personal Health Record.
THE PUBLIC HEALTH DILEMMASThe 1992 report2 of the association between IM vitamin Kand childhood cancer has created a situation which isunusual in public health. An important clinical policychange is being considered in Australia and elsewherelargely on the basis of a single study. The effectiveness ofIM vitamin K in preventing HDN is established, and it iseasy to administer as a single large dose that can begiven routinely by the birth attendant. Following the1992 report, the certainty of preventing HDN in thefirst six months of life must be balanced against thepossibility of a doubling of the risk of cancer throughoutchildhood. If IM vitamin K caused cancer, the resultingnumber of childhood cancer deaths would be muchgreater than the number of HDN deaths prevented.This poses a major problem of risk communication tothe public.
The NHMRCJ'ACP/RACOG joint statement also poses adilemma for a State Health Department which wouldordinarily take immediate steps to implement a nationalclinical policy recommendation. If the NSW HealthDepartment were to implement the interimrecommendations, the Department would have to advisehealth professionals to use a drug in a manner otherthan that for which it was approved. Individual medicalpractitioners can legally prescribe any registered drug byany route, whether approved or not. However, if theDepartment were to recommend the non-approved useof a drug, this would undermine the national drugevaluation process. On the other hand, if the Departmentwere to avoid implementing the interimrecommendations, it would implicitly endorse thecontinuation of a clinical practice which could possiblyhave adverse effects.
Until an effective vitamin K preparation approved fororal use is available, parents, in consultation withclinicians, will have to decide whether to:
• decline vitamin K (and take the attendant riskof HDN);
• agree to IM administration of vitamin K,acceptaing that there may be a small but realrisk of cancer to the child, which must bebalanced against the certain benefit ofprotection against HDN; or
• agree to oral administration of vitamin K,recognising that no approved preparation fororal administration to infants is available inAustralia.
VOI.4/No.2 15
Vitamin K prophy! axis
Continued from page 15
The dilemma confronting the Department also facesclinicians and parents of newborn infants. There is noclear immediate solution. The NHMRC/ACP/RACOGstatement acknowledges the need for more information.It recommends that epidemiological surveillance of HDNand childhood cancer be enhanced and that research beundertaken into the pharmacology and potentialcarcinogenicity of vitamin K preparations. TheEpidemiology and Health Services Evaluation Branchhas a major role in the former.
INFECTIOUS DISEASES
TIMELINESS AND COMPLETENESS OF REPORTiNG
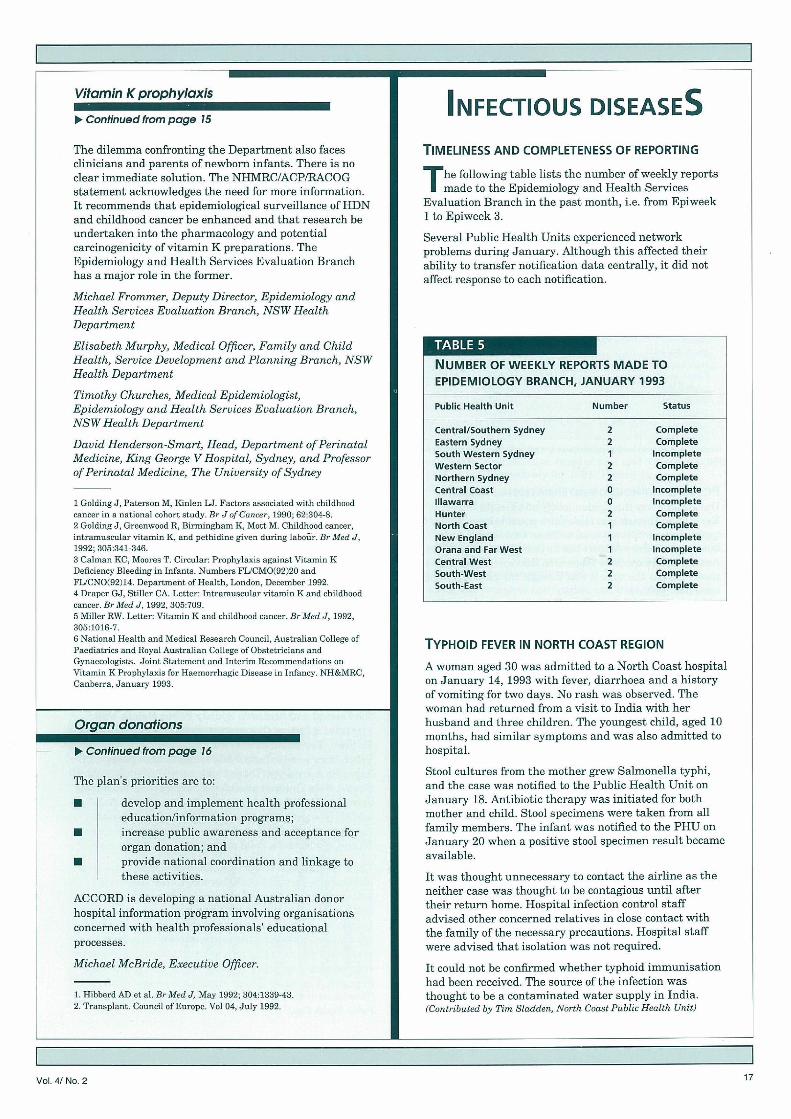
The following table lists the number of weekly reportsmade to the Epidemiology and Health Services
Evaluation Branch in the past month, i.e. from Epiweek1 to Epiweek 3.
Several Public Health Units experienced networkproblems during January. Alihough this affected theirability to transfer notification data centrally, it did notaffect response to each notification.
Michael Frommer, Deputy Director, Epidemiology andHealth Services Evaluation Branch, NSW HealthDepartment
Elisabeth Murphy, Medical Officer, Family and ChildHealth, Service Development and Planning Branch, NSWHealth Department
Timothy Churches, Medical Epidemiologist,Epidemiology and Health Services Evaluation Branch,NSW Health Department
David Henderson-Smart, Head, Department of PerinatalMedicine, King George V Hospital, Sydney, and Professorof Perinatal Medicine, The University of Sydney
1 GcldingJ, Paterson H, Kiii]en LI. Factors associated with childhoodcancer in a national cohort study. Br J of Cancer, 1990; 62:504.8.2 GcldingJ, Greenwood K, Birmingham K, Mott M. Childhood cancer,intramuscular vitamin K, and pethidine given during Iabdir, Br Med J,1992; 305:341-346.3 Cahnan KC, Moore T. Circular: Prophylaxis against Vitamin KDeficiency Bleeding in Infants. Numbers FLICMO(92)20 andFLJCNOI92)14. Department of Health, London, December 1992.4 Draper G,J, Stiller CA. Letter: Intramusrular vitamin K and childhoodcancer. Br Med J, 1992, 305:709.5 Miller RW. Letter: Vitamin K and childhood cancer. llrMed J, 1992,305:1016-7.6 National Health and Medical Research Council, Australian College ofPaedistric and Royal Acsstra]iari College of Obstetricians andGynaccologists. Joint Statement and Interim Recommendations onVitamin K Prophylaxis for Haeinorrhagic Disease in Infancy. NH&MRC,Canberra, January 1903.
donations
) Con hnued from page 16
The plan's priorities are to:
• develop and implement health professionaleducationlinformation programs;
• increase public awareness and acceptance fororgan donation; and
• provide national coordination and linkage tothese activities.
ACCORD is developing a national Australian donorhospital information program involving organisationsconcerned with health professionals' educationalprocesses.
Michael McBride, Executive Officer.
1. Hibberd AD et al. Br Med J May 1992; 304:1339-43.2. Transplant. Council of Europe. Vol 04, July 1992.
NUMBER OF WEEKLY REPORTS MADE TOEPIDEMIOLOGY BRANCH, JANUARY 1993
Public Health Unit Number Status
Central/Southern Sydney 2 CompleteEastern Sydney 2 CompleteSouth Western Sydney I IncompleteWestern Sector 2 CompleteNorthern Sydney 2 CompleteCentral Coast 0 IncompLetelllawarra 0 IncompleteHunter 2 CompleteNorth Coast 1 CompleteNew England 1 IncompleteOrana and Far West 1 IncompleteCentral West 2 CompleteSouth-West 2 CompleteSouth-East 2 Complete
TYPHOiD FEVER IN NORTH COAST REGION
A woman aged 30 was admitted to a North Coast hospitalon January 14, 1993 with fever, diarrhoea and a historyof vomiting for two days. No rash was observed. Thewoman had returned from a visit to India with herhusband and three children. The youngest child, aged 10months, had similar symptoms and was also admitted tohospital.
Stool cultures from the mother grew Salmonella typhi,and the case was notified to the Public Health Unit onJanuary 18. Antibiotic therapy was initiated for bothmother and child. Stool specimens were taken from allfamily members. The infant was notified to the PHU onJanuary 20 when a positive stool specimen result becameavailable.
It was thought unnecessary to contact the airline as theneither case was thought to be contagious until aftertheir return home. Hospital infection control staffadvised other concerned relatives in close contact withthe family of the necessary precautions. Hospital staffwere advised that isolation was not required.
It could not be confirmed whether typhoid immunisationhad been received. The source of the infection wasthought to be a contaminated water supply in India.(Gout rib ated by Tim S/ac/den, North Coast Public Health Unit)
V0L4/No,2 17