fluid and electrolyte requirements of newborn infants...
TRANSCRIPT
Arch. Dis. Childh., 1963, 38, 231.
FLUID AND ELECTROLYTE REQUIREMENTS OFNEWBORN INFANTS WITH INTESTINAL OBSTRUCTION
BY
ALEXANDER PEONIDES, WINIFRED F. YOUNG and VALENTINE A. J. SWAINFrom the Queen Elizabeth Hospitalfor Children, London
(RECEIVED FOR PUBLICATION OCTOBER 30, 1962)
The findings in a consecutive series of 120 childrenof all ages treated with parenteral fluid therapy insupport of major abdominal surgery have beenreported (Young, McIntosh, Swain and Levin, 1959).The series included 23 newborn infants with intes-tinal obstruction. The plan of fluid therapy usedwas designed to replace initial deficits of water andelectrolytes, to provide water, electrolytes andcalories for maintenance, and to replace furtherabnormal losses after operation. This plan is nowsupported by the findings from balance studies onthree older children with ileal obstruction in thatseries and by similar observations reported pre-viously (Lowe, Rourke, MacLachlan and Butler,1950; Holliday, Wallace and Stapleton, 1958).However, the newborn infants' requirements offluid and electrolytes remain controversial, and somesurgeons (Gross, 1953; Santulli, 1954; Rickham,1957; Wilkinson, 1960) have advised less waterand electrolytes than are recommended in the plan,preferring to keep such infants 'on the dry side'.On the other hand, Swenson (1958) and Grob (1960)include infants 1-2 days old in emphasizing thatdehydration should be corrected before operation,and Colle and Paulsen (1959) consider that theassessment of volumes required for maintenanceshould be based upon the average normal oralintake from day to day during the first week of life,which is also recommended in this plan (Fig. 1).These authors were unable to demonstrate a fall inurine flow even in the early phase after surgery innewborns, Calcagno, Rubin and Singh (1955) ininfants a few weeks old, and Young et al. (1959) inolder children, although adults usually pass verylittle urine on the first day after operation (LeQuesne and Lewis, 1953; Le Quesne, 1957; Black,1957).
WaterIt is especially important to give newborn infants
enough water to promote a free flow of urine, since
their kidneys function less efficiently and withgreater deterioration under stress than those ofolder subjects (McCance, 1948). When the intakeof water is restricted, the glomerular filtration ratefalls with the urine volume (McCance and Widdow-son, 1954), so that infants becoming dehydratedare unable to excrete nitrogen and other meta-bolites from protein breakdown, including potas-sium. Stress at birth, or after birth, from respira-tory distress or progressive dehydration acceleratesthis breakdown, and either acidosis or hyper-kalaemia may then be lethal. Thus, fluid therapywhich restores and maintains the glomerular filtra-tion rate (gauged by a high urine flow) is particularlyneeded at times of stress in order to improve andmaintain the excretion of nitrogen, potassium and
ml./24hrs8001
700
600
500-
400-
300-
200'
100-
0-
ml./hr.301
25
20
15.
10'
5.-
Ia23 4
Day of lifes 6 7
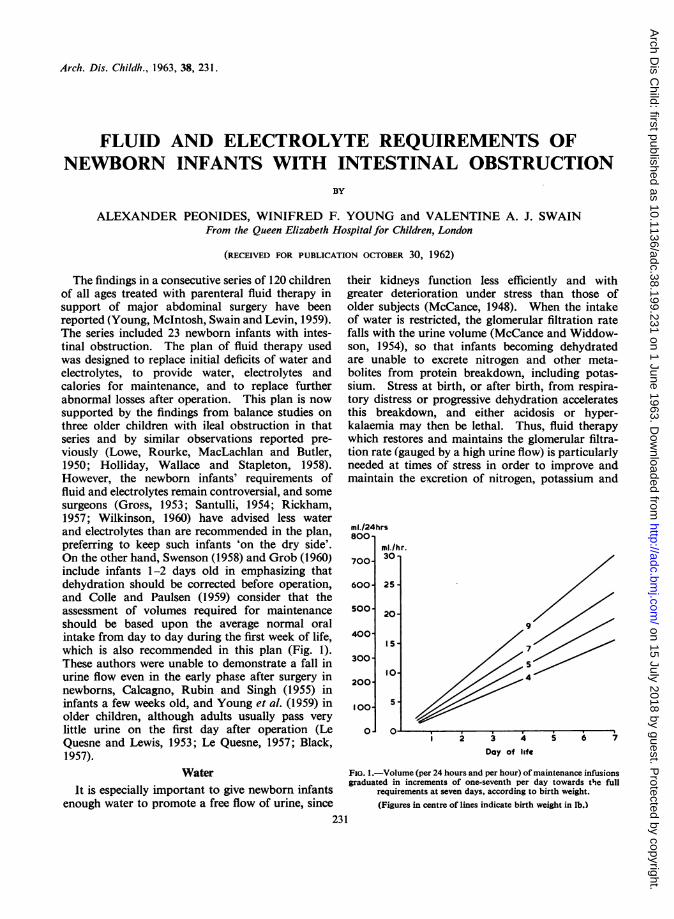
FIG. 1.-Volume (per 24 hours and per hour) of maintenance infusionsgraduated in increments of one-seventh per day towards the full
requirements at seven days, according to birth weight.(Figures in centre of lines indicate birth weight in lb.)
231
0 1I
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from
ARCHIVES OF DISEASE IN CHILDHOOD
acid metabolites. Furthermore, calories for meta-bolism from the glucose in the solutions used willdiminish protein katabolism and therefore themetabolic products demanding excretion. At thesame time great care must be taken to avoid givingexcessive amounts of fluid to newborn infants whoare unable to dilute their urine in response to awater load as efficiently as adults (Heller, 1951).
ElectrolytesPreviously, Young et al. (1959) discussed the reasons
for early adequate treatment of electrolyte depletionin patients undergoing abdominal surgery. The riskof oedema in newborns from over-retention of salt,which may only be partly renal in origin (Dean andMcCance, 1949; McCance and Widdowson, 1957),and also the liability of premature infants to oedemaand sclerema beginning before any significantaddition of water and salt, are often taken too muchinto consideration in prescribing for patients atthis age. The management of cases with the lattertendency needs separate consideration, for theycannot be treated successfully unless the distributionof their body fluids improves spontaneously. Infact, restoration of electrolyte losses in newborns iseven more important than in older patients sincetheir renal excretory capacity is lower and thereforeepisodes of salt depletion are more hazardous.Solutions of sodium chloride for replacement areneeded by infants with a history of vomiting, andsince such losses cannot be assessed accurately, anexcess must usually be prescribed to ensure completerepair. Over-retention of sodium promotes potas-sium loss and augments any potassium deficit dueinitially to vomiting, dehydration or perhaps thestress of surgery. Administration of potassiumpromotes excretion of sodium and is also neededto restore any deficit of itself. It should be givenas early in treatment as is consistent with safety,and this can be gauged by restoration of the urineflow, or often before this by finding a normalconcentration of potassium in the plasma. Rick-ham (1957) considers that potassium is not usuallyneeded for repair, since the losses from the stress ofsurgery appeared to be absent or negligible in hispatients, the amount of potassium relative tonitrogen in their urine not exceeding that derivedfrom protein breakdown. However, his patientswere passing little urine, which would have dimin-ished the output ofpotassium in this phase (McCanceand Widdowson, 1954), and therefore this obser-vation does not exclude losses at higher rates ofurine flow. In either case, potassium should be givenin order to avoid the retention of sodium and
potassium depletion resulting from administrationof excess sodium salts, since sodium over-retention,as already discussed, is a special hazard in the earlydays of life.The management of fluid therapy is acknowledged
to be difficult in newborn infants, but restorationof the body fluids may greatly improve the prognosisafter surgery for intestinal obstruction. It wastherefore decided to make further detailed obser-vations in this group of patients including balancestudies whenever possible, in order to evaluate thetreatment and modify it if necessary for futurecases. The most useful results have been obtainedfrom balance studies in a few cases, but relevantinformation has also been obtained from measuring(a) the composition of aspirated gastro-intestinalfluid and (b) the daily output of electrolytes in theurine in some further cases and from observingthe progress of all the patients in a consecutiveseries.
Methods
The plan for intravenous fluid therapy which has beenused at the Queen Elizabeth Hospital for Children since1953 is summarized in Table 1 and Fig. 1. It is adaptedto the needs of the individual case from hour to houraccording to clinical condition and laboratory findings.Antibiotics (usually penicillin or streptomycin) andvitamins are given intramuscularly or intravenouslyduring the period of infusion.
Collection and measurement of the output, as urineand aspirated gastro-intestinal fluid, were arranged asbefore (Young et al., 1959). The solutions used forintravenous infusions were prepared by the hospitalpharmacist and checked by analysis from time to time.At first the reconstituted dried plasma used was assumedto contain Na 140, K 5, and Cl 100 mEq/litre, but analysisduring later experiments showed higher concentrationsof sodium and potassium. Thus, in cases where analysisof the intake was omitted, the retention of electrolytescalculated by subtracting the output is likely to havebeen slightly underestimated. Small amounts of glucoseand electrolyte solutions given orally towards the endof the balance periods were carefully measured andincluded in the intake.The balance periods were usually continued until bowel
function was restored with return of bowel sounds andpassage of faeces, plugs of meconium being disregarded.Balance studies were sometimes terminated before bowelfunction had been restored, for example, in one caseowing to loss of urine and, in another, when proteindigest solutions had been given. Since a fraction ofthese amino acids would have been excreted directlyinto the urine, the ratio of potassium to nitrogen in theurine could not then be used to calculate potassiumderived from endogenous metabolism.The laboratory techniques were the same as those used
previously (Young et al., 1959).
232
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from

233PARENTERAL FLUID THERAPY IN INTESTINAL OBSTRUCTIONTABLE 1
INTRAVENOUS FLUID THERAPY FOR NEWBORN INFANTS WITH INTESTINAL OBSTRUCTION
Infusion
Initial
During surgery
Maintenance at age7 days* .. ..
Replacement
Volume (ml.)
Per kg. Per lb.Birth BirthWeight Weight
66 30or less or less
Duration(hrs.)
Four or less if(1) urine ispassed freely;(2) emergencysurgery
As indicated
165-198 75-90
Equals that ofaspirated gas-tro-intestinalfluids includ-ing 'pool' atsurgery
I Composition ofElectrolyte Solutions
in 5% Dextrose
Electrolytes(mEa oer ki1.)
Na K Cl- I I--
Half isotonic saline77 mEq/l.
Plasma (diluted orfull strength)
Blood only to replaceblood losses
4-8
I-
24One-fifth isotonic
saline 31 mEq/l.K salts (KCI or Kacetate) 20 mEq/l.
150-6 1333-40
I. --
Varies
Isotonic saline + Ksalts as for main-tenance
48
8 -3-10 1if KCIadded;50-6 1
if Kacetateadded
Remarks
Isotonic saline if Na level inplasma is low
If oral feeding delayed morethan 2 days after surgery,plasma (diluted to one-quarter in 5% dextrosesolution) or protein digestsin 5% dextrose and appro-priate electrolyte solutions
K salts omitted if oliguric
* Graduation of amounts of infusions for infants of 1-7 days old is shown in Fig. 1.
MaterialBetween 1957 and 1960, a consecutive series of 24
newborn infants with intestinal obstruction treatedaccording to the plan has been studied, but materialfor balance data was collected successfully from onlyfive male infants, all of whom had duodenal obstruction.An infant with dehydration associated with oesophagealatresia was similarly investigated in order to comparethe findings from a patient without previous loss ofgastro-intestinal secretions with those from the casesof intestinal obstruction.Each patient was given intravenous infusions before
surgery, which was performed within 24 hours of admis-sion, except in one patient with incomplete obstructionof the ileum due to bands, in whom operation was delayedfor three days.
ResultsClinical Course. Of the 24 infants, 21 survived
and three died, each of whom had obstruction to thesmall bowel. Table 2 shows the site and cause ofobstruction, associated abnormalities and theoutcome in these 24 patients. Their birth weightsranged from 3 lb. 3 oz. (1-45 kg.) to 8 lb. 10 oz.(3 -9 kg.), and age on admission from 2 hours to11 days. Hydration was assessed clinically, theincidence of dehydration at presentation (Table 3)being much greater among those where diagnosiswas delayed beyond two days. The dehydratedpatients had lost between 9 and 22% of their birthweight, but since different scales were used, the
recorded amount of weight lost was of little valuein assessing subsequent requirements for rehydra-tion, which was judged mainly by the clinical andlaboratory findings.Of the 21 cases who survived, 11 recovered
uneventfully; seven showed complications possiblyrelated to parenteral fluid therapy and three due toalimentary dysfunction. Among the former, local-ized twitching occurred within 24 hours of operationin three, but this was attributed to anoxia frompulmonary collapse after inhalation of vomit in one,and in another, to hypocalcaemia which respondedto calcium gluconate intravenously. In the third,twitching of longer duration was thought to be dueeither to water intoxication (serum sodium 125mEq/l.) or hypocalcaemia (serum calcium 6- 3mg./100 ml.). One infant had signs of cerebralirritation (opisthotonus and hypertonia) withoutobvious cause, which regressed without specialtreatment. Three infants had sequelae due toinfection from the intravenous infusions, despiteprophylactic penicillin and streptomycin givenintramuscularly. Phlebitis at the site of the infusionoccurred in one (due to a Staph. pyogenes resistantto penicillin and streptomycin) and osteomyelitis intwo infants. One of these whose right elbow andcervical vertebrae were affected had had an umbilicalstump infected with a Staph. pyogenes as well as amild thrombophlebitis; in the other case the right
4
-I ~ ~
-1,
k....
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from
ARCHIVES OF DISEASE IN CHILDHOODTABLE 2
SITE AND CAUSE OF OBSTRUCTION AND RECOVERY RATE IN 24 CASES
Site Cause Number Recovered Died
Intrinsic-complete 6 6-incomplete 1 1
Duodenum Extrinsic (one with volvulus) 2 2 -
Total 9 9 0
f Single 2 2 -
Atresia I Multiple 1 1t Z+Volvulus 1 1 -
Hirschsprung 1 including jejunum 1 - 1A including ileum 1 - I
Jejunum and ileum Volvulus with cystic fibrosis of pancreas 1 1 -
Torsion of mesentery 1 1 -
Bands (incomplete obstruction) 1 1 -
Exomphalos + gangrenous bowel 1 - 1Inguinal hernia (strangulated) 1 1 -
Total 11 8 3
Rectal atresia 3 3 -
Colon Hirschsprung 1 1 -
Total 4 4 -
Total .24 21 3
femur was involved. Large doses of antibioticsother than penicillin and streptomycin were givento both of these patients, and their bones havehealed without serious residual deformity.Two of the infants with alimentary dysfunction
had diarrhoea from intestinal hurry, in one per-sisting for three months and in the other for onlytwo weeks, but followed by chronic malabsorptionwith persistent steatorrhoea; the third had symptomsfrom a segment of dilated bowel, shown radio-logically to be above the anastomosis, for two anda half months. The later course of these threepatients is described elsewhere (Swain, Peonides andYoung, 1963).
Three infants died, two while still receiving intra-venous fluid therapy, and one at a later stage. Oneof two with Hirschsprung's disease had aganglionicbowel reaching the jejunum and died six days aftersurgery, two laparotomies having showed noobvious cause for the obstruction. The ileum wasinvolved in the other who died aged 2 months,following a diagnostic laparotomy and then a highileostomy. Tetany, occurring immediately after
TABLE 3INCIDENCE OF DEHYDRATION IN RELATION TO AGE
Age on AdmissionNumber
2 days or less More than 2 days
Dehydrated 9 2 7
Not dehydrated .. 15 9 6
both operations, was treated successfully withcalcium given intravenously and inhalations ofcarbon dioxide and the patient was sustained byoral feeding from the fifth post-operative day. Theileostomy worked satisfactorily for two to threeweeks, but malabsorption led to progressivedeterioration in nutrition and he died from aterminal pneumonia.A premature baby (birth weight 3 lb. 3 oz.
(1*45 kg.)) with exomphalos complicated bygangrene of the ileum, died five days after 53 cm. ofbowel had been resected and an end-to-end anas-tomosis performed. Ileus had persisted with pool-ing of intestinal fluids followed by oliguria withwater retention. Renal function may have deterior-ated from incomplete replacement of salt duringthe 'pooling' phase. The sodium level in the plasmawas low, 124 mEq/l., and the potassium high,7 8 mEq/l., on the day of death. Oedema had beenpresent for 24 hours.
Plasma Electrolyte Levels. The concentration ofelectrolytes in plasma was usually estimated daily,levels having been obtained initially and as soonafter the operation as possible in the more severelydehydrated cases. A few low levels, for sodium,below 130 mEq/l., chloride, below 95 mEq/l.,and potassium, below 3-8 mEq/l., were recordedboth in the early and later phases of treatment,indicating either electrolyte depletion due to insuffi-cient salt replacement, or haemodilution. In eithercase the correct treatment is administration of moreconcentrated saline solutions at a slow rate guided
234
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from
PARENTERAL FLUID THERAPY IN INTESTINAL OBSTRUCTION
e 0._A. J lst. 5 hrs Day I Day 2 Day 3 Day 4 Day S1 C22 hrs) _ j C12 hrs3
W.ibAft' I OAR v om0 I .!2 I % %la Is*'af%4. I 4
137
67
22
and measured output
LI
137
4-6
24
O
Li
Asratlons
Urine
Dailyaintenane
requirements
Cudmative
43a
Na CI
+6 +106
K+6'7+33 K:N+ I.O0Total
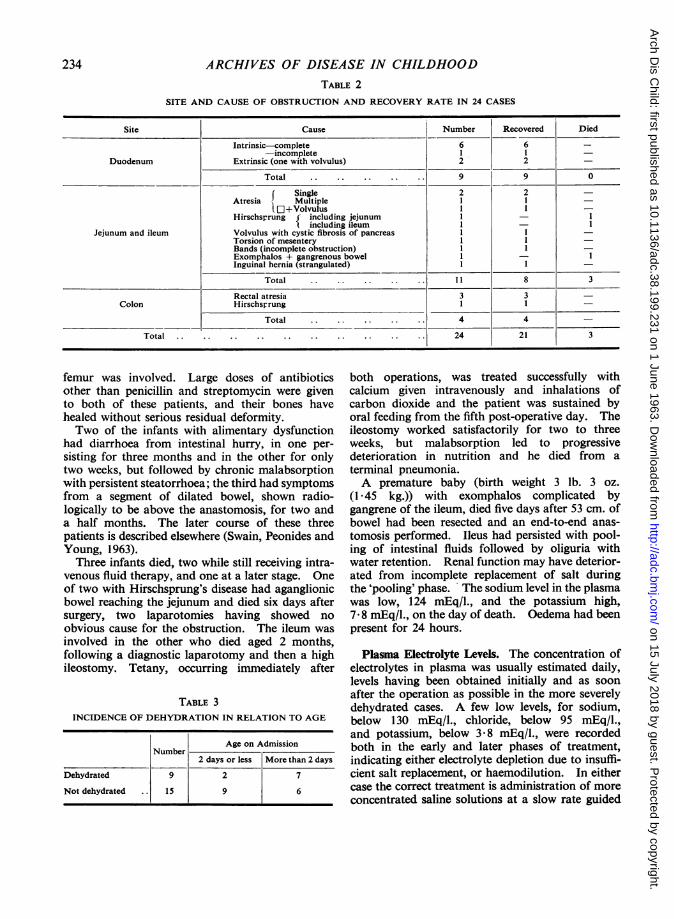
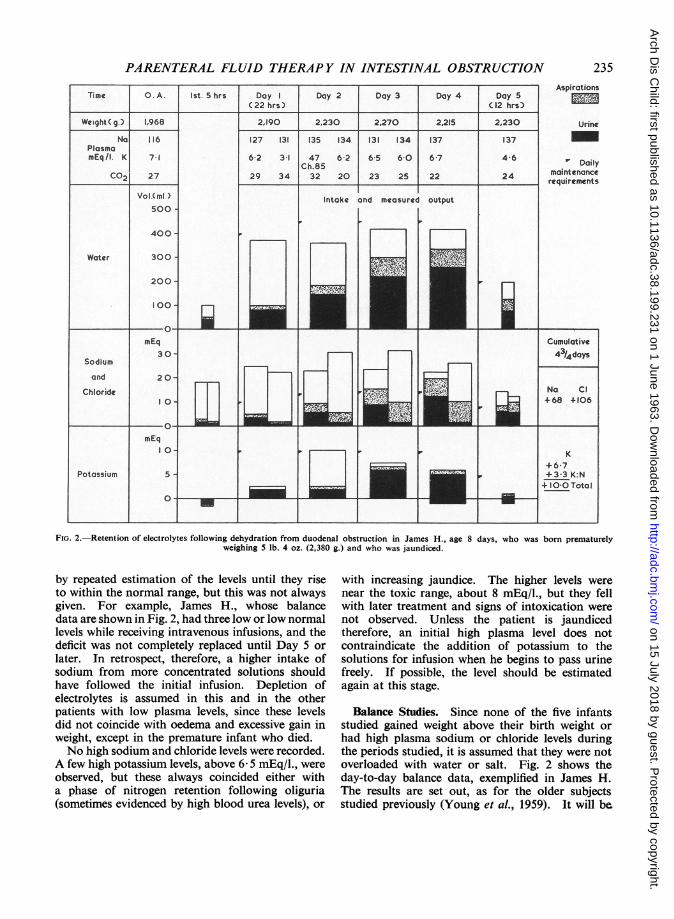
FIG. 2.-Retention of electrolytes following dehydration from duodenal obstruction in James H., age 8 days, who was born prematurelyweighing 5 lb. 4 oz. (2,380 g.) and who was jaundiced.
by repeated estimation of the levels until they riseto within the normal range, but this was not alwaysgiven. For example, James H., whose balancedata are shown in Fig. 2, had three low or low normallevels while receiving intravenous infusions, and thedeficit was not completely replaced until Day 5 orlater. In retrospect, therefore, a higher intake ofsodium from more concentrated solutions shouldhave followed the initial infusion. Depletion ofelectrolytes is assumed in this and in the otherpatients with low plasma levels, since these levelsdid not coincide with oedema and excessive gain inweight, except in the premature infant who died.No high sodium and chloride levels were recorded.
A few high potassium levels, above 6- 5 mEq/l., wereobserved, but these always coincided either witha phase of nitrogen retention following oliguria(sometimes evidenced by high blood urea levels), or
with increasing jaundice. The higher levels werenear the toxic range, about 8 mEq/l., but they fellwith later treatment and signs of intoxication werenot observed. Unless the patient is jaundicedtherefore, an initial high plasma level does notcontraindicate the addition of potassium to thesolutions for infusion when he begins to pass urinefreely. If possible, the level should be estimatedagain at this stage.
Balance Studies. Since none of the five infantsstudied gained weight above their birth weight orhad high plasma sodium or chloride levels duringthe periods studied, it is assumed that they were notoverloaded with water or salt. Fig. 2 shows theday-to-day balance data, exemplified in James H.The results are set out, as for the older subjectsstudied previously (Young et al., 1959). It will be
5 I
I
4
235
C|tVv iaidlZ ,m
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from
ARCHIVES OF DISEASE IN CHILDHOODTABLE 4
INITIAL DEFICIT OF ELECTROLYTES IN SIX CASES ESTIMATEDFROM POSITIVE BALANCES DURING TREATMENT
Age on Birth Weight Loss Positive Balances* Duration ofSite Subject Arrival Weight (approx.) (mEq/kg. birth weight) Investigation
(days) (kg.) - (days)kg. % Na K Cl
Oesophagus P.B. 5 3-32 0 520 16 5 4 Not done Pre-operative(16) (13)Inc. 7
M.J. 2 3*35 0-360 11 12 1-3 10 Pre- and post-operative(40) (4- 3)tInc. (35) 44
tFor K 6gl)D.D. 3 3-27 0-410 12 13 1-5 13 21
(44) (5)tnc. (42) (For K 37a)Duodenum B.P. 4 156 0-212 14 11 3-5 12 32
(I 7)Inc. (5 * 4)Inc. (18)Inc.M.D. 6 2-15 0-475 22 17 6 22 312
(36)Inc. (13)Inc. (47)Inc.J.H. 8 2-38 0-425 18 29 4-2 44 4'i
(68)Inc. (10) (106)Inc.
Average . . 16 3 - 3 20
* Figures in parentheses are totals. Inc. = Incomplete, due to discontinuation before balance was negative.tlnc. = Incomplete, due to lack of data for K: N. If K deriving from protein katabolism is omitted, the apparent total cumulative
positive K balances would diminish to: P.B.: 7-4, D.D.: 1-8, B.P.: 3 0, M.D.: 11-7, and J.H.: 6-7.
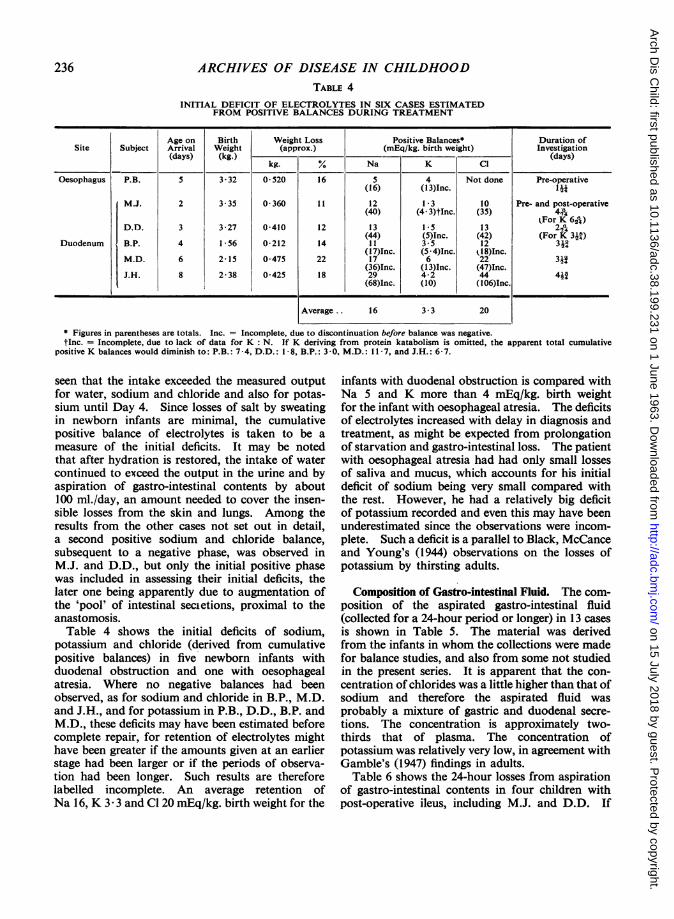
seen that the intake exceeded the measured outputfor water, sodium and chloride and also for potas-sium until Day 4. Since losses of salt by sweatingin newborn infants are minimal, the cumulativepositive balance of electrolytes is taken to be ameasure of the initial deficits. It may be notedthat after hydration is restored, the intake of watercontinued to exceed the output in the urine and byaspiration of gastro-intestinal contents by about100 ml./day, an amount needed to cover the insen-sible losses from the skin and lungs. Among theresults from the other cases not set out in detail,a second positive sodium and chloride balance,subsequent to a negative phase, was observed inM.J. and D.D., but only the initial positive phasewas included in assessing their initial deficits, thelater one being apparently due to augmentation ofthe 'pool' of intestinal secietions, proximal to theanastomosis.Table 4 shows the initial deficits of sodium,
potassium and chloride (derived from cumulativepositive balances) in five newborn infants withduodenal obstruction and one with oesophagealatresia. Where no negative balances had beenobserved, as for sodium and chloride in B.P., M.D.and J.H., and for potassium in P.B., D.D., B.P. andM.D., these deficits may have been estimated beforecomplete repair, for retention of electrolytes mighthave been greater if the amounts given at an earlierstage had been larger or if the periods of observa-tion had been longer. Such results are thereforelabelled incomplete. An average retention ofNa 16, K 3- 3 and Cl 20 mEq/kg. birth weight for the
infants with duodenal obstruction is compared withNa 5 and K more than 4 mEq/kg. birth weightfor the infant with oesophageal atresia. The deficitsof electrolytes increased with delay in diagnosis andtreatment, as might be expected from prolongationof starvation and gastro-intestinal loss. The patientwith oesophageal atresia had had only small lossesof saliva and mucus, which accounts for his initialdeficit of sodium being very small compared withthe rest. However, he had a relatively big deficitof potassium recorded and even this may have beenunderestimated since the observations were incom-plete. Such a deficit is a parallel to Black, McCanceand Young's (1944) observations on the losses ofpotassium by thirsting adults.
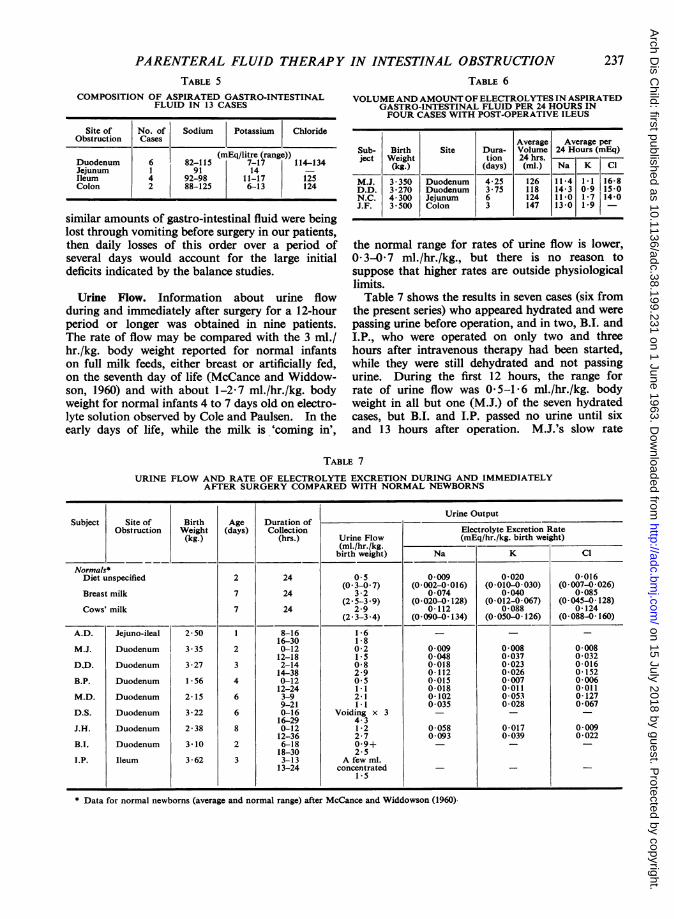
Composition of Gastro-intestinal Fluid. The com-position of the aspirated gastro-intestinal fluid(collected for a 24-hour period or longer) in 13 casesis shown in Table 5. The material was derivedfrom the infants in whom the collections were madefor balance studies, and also from some not studiedin the present series. It is apparent that the con-centration of chlorides was a little higher than that ofsodium and therefore the aspirated fluid wasprobably a mixture of gastric and duodenal secre-tions. The concentration is approximately two-thirds that of plasma. The concentration ofpotassium was relatively very low, in agreement withGamble's (1947) findings in adults.
Table 6 shows the 24-hour losses from aspirationof gastro-intestinal contents in four children withpost-operative ileus, including M.J. and D.D. If
236
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from
PARENTERAL FLUID THERAPY IN INTESTINAL OBSTRUCTIONTABLE 5
COMPOSITION OF ASPIRATED GASTRO-INTESTINALFLUID IN 13 CASES
Site of No. of Sodium Potassium ChlorideObstruction Cases
DuodenumJejunumIleumColon
6
4
2
(mEq/litre (range)) Seub-82-115 7-17 114-134
91 1492-98 11-17 125 M.J.88-125 6-13 124 D.D.
similar amounts of gastro-intestinal fluid were beinglost through vomiting before surgery in our patients,then daily losses of this order over a period ofseveral days would account for the large initialdeficits indicated by the balance studies.
Urine Flow. Information about urine flowduring and immediately after surgery for a 12-hourperiod or longer was obtained in nine patients.The rate of flow may be compared with the 3 ml./hr./kg. body weight reported for normal infantson full milk feeds, either breast or artificially fed,on the seventh day of life (McCance and Widdow-son, 1960) and with about 1-2-7 ml./hr./kg. bodyweight for normal infants 4 to 7 days old on electro-lyte solution observed by Cole and Paulsen. In theearly days of life, while the milk is 'coming in',
TABLE 6
VOLUME AND AMOUNT OF ELECTROLYTES IN ASPIRATEDGASTRO-INTESTINAL FLUID PER 24 HOURS INFOUR CASES WITH POST-OPERATIVE ILEUS
Average Average perBirth Site Dura- Volume 24 Hours (mEq)Weight tion 24 hrs.(kg.) (days) (ml.) Na K Cl
3 350 Duodenum 4-25 126 11*4 11 16-83*270 Duodenum 3 75 118 14-3 0 9 15-04- 300 Jejunum 6 124 1101* 7 14-03*500 Colon 3 147 1301* 9 -
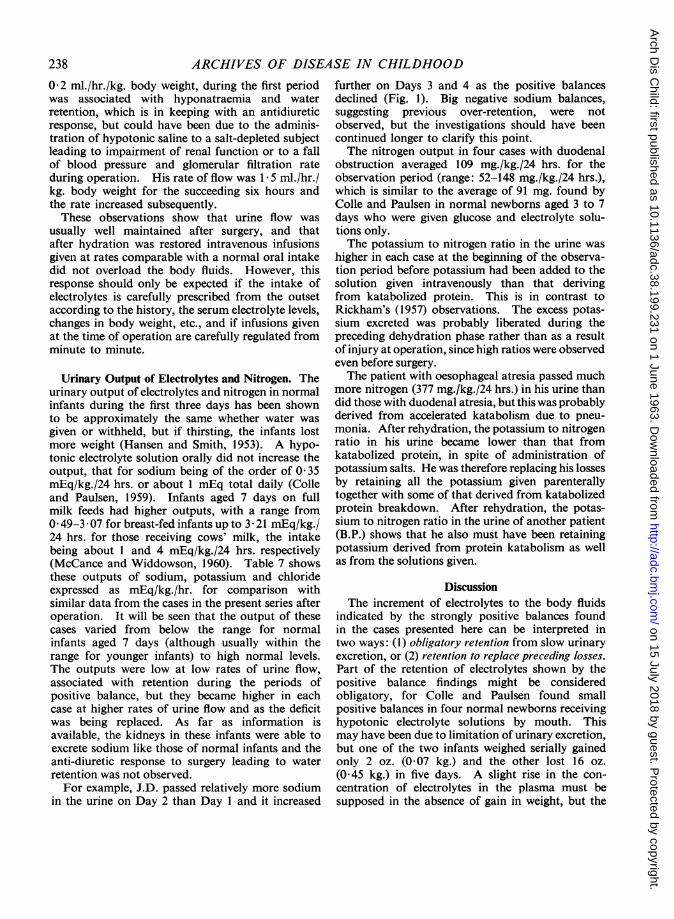
the normal range for rates of urine flow is lower,03-0-7 ml./hr./kg., but there is no reason tosuppose that higher rates are outside physiologicallimits.Table 7 shows the results in seven cases (six from
the present series) who appeared hydrated and were
passing urine before operation, and in two, B.I. andI.P., who were operated on only two and threehours after intravenous therapy had been started,while they were still dehydrated and not passingurine. During the first 12 hours, the range forrate of urine flow was 0-5-1 6 ml./hr./kg. bodyweight in all but one (M.J.) of the seven hydratedcases, but B.I. and I.P. passed no urine until sixand 13 hours after operation. M.J.'s slow rate
TABLE 7
URINE FLOW AND RATE OF ELECTROLYTE EXCRETION DURING AND IMMEDIATELYAFTER SURGERY COMPARED WITH NORMAL NEWBORNS
Urine OutputSubject Site of Birth Age Duration of
Obstruction Weight (days) Collection Electrolyte Excretion Rate(kg.) (hrs.) Urine Flow (mEq/hr./kg. birth weight)
(ml./hr./kg. _ _
birth weight) Na K Cl
Normals*Diet unspecified 2 24 05 0009 0020 0016
(03-0*7) (0 002-0016) (0 010-0*030) (0*007-0026)Breast milk 7 24 3*2 0074 0040 0085
(2 5-3 9) (0-020-0 128) (0-012-0-067) (0-045-0-128)Cows' milk 7 24 2 9 0*112 0*088 0*124
(2 3-3 4) (0-090-0 134) (0-050-0 126) (0-088-0 160)
A.D. Jejuno-ileal 2-50 1 8-16 1i 6 - - -
16-30 1-8M.J. Duodenum 3*35 2 0-12 0-2 0 009 0008 0 008
12-18 1 5 0 048 0 037 0-032DD. Duodenum 3*27 3 2-14 0*8 0*018 0 023 0 016
14-38 2-9 0-112 0-026 0 152B.P. Duodenum 156 4 0-12 0 5 0015 0007 0006
12-24 1 1 0-018 0-011 0 011M.D. Duodenum 2-15 6 3-9 2 1 0-102 0 053 0-127
9-21 1*1 0 035 0 028 0-067D.S. Duodenum 3-22 6 0-16 Voiding x 3 - - -
16-29 4-3J.H. Duodenum 2-38 8 0-12 1-2 0-058 0-017 0 009
12-36 2-7 0 093 0 039 0-022B.I. Duodenum 3-10 2 6-18 0*9+ - - -
18-30 2- 5I.P. Ileum 3-62 3 3-13 A few ml.
13-24 concentrated - -
- .Data 15n*Data for normal newborns (average and normal range) after McCance and Widdowson (1960)-
1..
237
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from
ARCHIVES OF DISEASE IN CHILDHOOD
0-2 ml./hr./kg. body weight, during the first periodwas associated with hyponatraemia and waterretention, which is in keeping with an antidiureticresponse, but could have been due to the adminis-tration of hypotonic saline to a salt-depleted subjectleading to impairment of renal function or to a fallof blood pressure and glomerular filtration rateduring operation. His rate of flow was 15 ml./hr./kg. body weight for the succeeding six hours andthe rate increased subsequently.These observations show that urine flow was
usually well maintained after surgery, and thatafter hydration was restored intravenous infusionsgiven at rates comparable with a normal oral intakedid not overload the body fluids. However, thisresponse should only be expected if the intake ofelectrolytes is carefully prescribed from the outsetaccording to the history, the serum electrolyte levels,changes in body weight, etc., and if infusions givenat the time of operation are carefully regulated fromminute to minute.
Urinary Output of Electrolytes and Nitrogen. Theurinary output of electrolytes and nitrogen in normalinfants during the first three days has been shownto be approximately the same whether water wasgiven or withheld, but if thirsting, the infants lostmore weight (Hansen and Smith, 1953). A hypo-tonic electrolyte solution orally did not increase theoutput, that for sodium being of the order of 0 35mEq/kg./24 hrs. or about 1 mEq total daily (Colleand Paulsen, 1959). Infants aged 7 days on fullmilk feeds had higher outputs, with a range from0 49-3 07 for breast-fed infants up to 3 21 mEq/kg./24 hrs. for those receiving cows' milk, the intakebeing about 1 and 4 mEq/kg./24 hrs. respectively(McCance and Widdowson, 1960). Table 7 showsthese outputs of sodium, potassium and chlorideexpressed as mEq/kg./hr. for comparison withsimilar data from the cases in the present series afteroperation. It will be seen that the output of thesecases varied from below the range for normalinfants aged 7 days (although usually within therange for younger infants) to high normal levels.The outputs were low at low rates of urine flow,associated with retention during the periods ofpositive balance, but they became higher in eachcase at higher rates of urine flow and as the deficitwas being replaced. As far as information isavailable, the kidneys in these infants were able toexcrete sodium like those of normal infants and theanti-diuretic response to surgery leading to waterretention was not observed.For example, J.D. passed relatively more sodium
in the urine on Day 2 than Day 1 and it increased
further on Days 3 and 4 as the positive balancesdeclined (Fig. 1). Big negative sodium balances,suggesting previous over-retention, were notobserved, but the investigations should have beencontinued longer to clarify this point.The nitrogen output in four cases with duodenal
obstruction averaged 109 mg./kg./24 hrs. for theobservation period (range: 52-148 mg./kg./24 hrs.),which is similar to the average of 91 mg. found byColle and Paulsen in normal newborns aged 3 to 7days who were given glucose and electrolyte solu-tions only.The potassium to nitrogen ratio in the urine was
higher in each case at the beginning of the observa-tion period before potassium had been added to thesolution given intravenously than that derivingfrom katabolized protein. This is in contrast toRickham's (1957) observations. The excess potas-sium excreted was probably liberated during thepreceding dehydration phase rather than as a resultof injury at operation, since high ratios were observedeven before surgery.The patient with oesophageal atresia passed much
more nitrogen (377 mg./kg./24 hrs.) in his urine thandid those with duodenal atresia, but this was probablyderived from accelerated katabolism due to pneu-monia. After rehydration, the potassium to nitrogenratio in his urine became lower than that fromkatabolized protein, in spite of administration ofpotassium salts. He was therefore replacing his lossesby retaining all the potassium given parenterallytogether with some of that derived from katabolizedprotein breakdown. After rehydration, the potas-sium to nitrogen ratio in the urine of another patient(B.P.) shows that he also must have been retainingpotassium derived from protein katabolism as wellas from the solutions given.
DiscussionThe increment of electrolytes to the body fluids
indicated by the strongly positive balances foundin the cases presented here can be interpreted intwo ways: (1) obligatory retention from slow urinaryexcretion, or (2) retention to replace preceding losses.Part of the retention of electrolytes shown by thepositive balance findings might be consideredobligatory, for Colle and Paulsen found smallpositive balances in four normal newborns receivinghypotonic electrolyte solutions by mouth. Thismay have been due to limitation of urinary excretion,but one of the two infants weighed serially gainedonly 2 oz. (0 07 kg.) and the other lost 16 oz.(0 45 kg.) in five days. A slight rise in the con-centration of electrolytes in the plasma must besupposed in the absence of gain in weight, but the
238
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from
PARENTERAL FLUID THERAPY IN INTESTINAL OBSTRUCTIONplasma was not examined. In McCance andWiddowson's (1957) experiments, where much largeramounts of salt were fed to three premature infantsand to newborn piglets, the subjects gained weight,developed oedema and, at the same time, increasedthe concentration of sodium and chloride in theplasma.
Retention for replacement as the main cause ofthe positive balances in our series of cases is sug-gested by the following evidence.
1. The body weight was no higher than the birthweight in any case at the end of the balance period,and subsequent loss of weight did not exceed3-4 ounces. High concentrations of extracellularelectrolytes in plasma were not recorded. Reten-tion in excess of the body's needs for replacementcausing expansion of the extracellular fluid thereforeseems improbable.
2. When a negative followed a positive balanceit was never large or sustained for long enoughto suggest that much of the previously retainedelectrolyte was being excreted, but the duration ofthe observations in some cases was too short toexclude this trend.
3. During positive balance periods the highrates of urine flow, with lower concentrations ofelectrolytes than newborn kidneys can achieve,suggest that the retention was not due to inadequaterenal excretion.
4. The measurement of large electrolyte lossesin the aspirated gastro-intestinal fluids after opera-tion demonstrates that had similar losses fromvomiting occurred before operation, initial deficitsof the order of the positive balances here recordedmight well have been sustained. The higher positivebalances of the older newborns supports this con-tention, for the deficits would have been increasingeach day until diagnosis and treatment.The urinary output of potassium at first exceeded
amounts liberated by katabolism of protein (accor-ding to the ratio of potassium to nitrogen) in thefour cases where data are available. After rehydra-tion, when potassium salts were being given, thepotassium derived from katabolized protein couldhave contributed by being available for repair,but the amount was only a small fraction of thatretained. High levels of potassium in the plasmaat the outset should not therefore be considereda contraindication to the addition of potassium tothe solutions for repair, for this is needed as soonas a free flow of urine is established.
In the light of the results of the present investiga-tions, the prospective plan (Table 1) for intravenousfluid therapy for newborn infants with intestinalobstruction requires some modification.
Initial infusions of 60 ml./kg. (30 ml./lb.) bodyweight consisting of half isotonic saline, whichsupply only 4 5 mEq of Na/kg. body weight, areunlikely to replace the initial deficits, especiallyof the more severely depleted cases whose treatmenthas been delayed until the age of 5 days or longer.Even if this infusion is changed to contain in partisotonic saline (as recommended if low plasma Naand Cl levels have been determined) it will some-times contain insufficient salt for replacement. Inyounger, less depleted patients, replacement may becompleted satisfactorily by the amount of sodiumchloride in maintenance infusions of one-fifthisotonic saline, together with increments from theisotonic saline solution usually given in equalvolume to that of aspirated gastro-duodenal fluid,for it has been shown that the aspirate containsabout 100 mEq/l. sodium and chloride comparedwith the 150 mEq/l. in isotonic saline. The largerdeficits which must be assumed in older newbornsindicate that initial infusions of greater volumeshould be given, e.g. 90-120 ml./kg. body weightover six to eight hours. It may be wise to delaysurgery for this, or if not, an infusion of half isotonicsaline for repair and maintenance should be con-tinued at a slower rate after surgery, e.g. to supply120 ml./kg. (60 ml./lb. body weight) in 24 hours,which is about the volume used for maintenanceinfusions in a 5-day-old baby. Isotonic in place ofthe hypotonic saline should be given if low plasmasodium and chloride levels are found and the levelsrepeated at six- to 12-hour intervals to guide theconcentration of the solution used. After a freeurine flow is established, potassium salts should beadded in the same way as for the weaker solutionsof saline used for maintenance. The guidance ofrepeated estimations of the plasma electrolyte levelsis extremely valuable at this stage and should beobtained whenever possible, and in any case wherediuresis is delayed.
It should always be supposed that the deficits ofinfants with low intestinal, as compared with duo-denal, obstruction will be greater at an earlier stageand that they may be partially masked becauseintestinal pooling occurs rather than the copiousvomiting of high intestinal obstruction. Also, thatthese deficits are best replaced by a mixture ofsodium salts both in the isotonic and the halfisotonic solutions, e.g. two parts sodium chlorideand one part Na lactate instead of the saline solutionalone.
Maintenance Infusions. Glucose in hypotonicsalt solutions must be prescribed cautiously fornewborn infants (especially if premature) whose
239
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from
240 ARCHIVES OF DISEASE IN CHILDHOOD
urine flow is poor. Oliguria may be due to incom-plete repair of depletion, or to capillary damage witha tendency to oedema, associated with stress atbirth, infection or hypothermia. In either case,hypotonic solutions will precipitate a fall in theplasma sodium level and consequent deteriorationin renal function. Judgement based upon repeatedclinical examination and assessment of urine flowand plasma electrolyte levels must then guidetreatment from hour to hour. The criteria warrant-ing safe use of hypotonic (one-fifth isotonic) salineor salt lactate with added K salts to supply 20 mEq/litre as a maintenance infusion in newborn infantsare as follows.
1. Restoration of body weight to near the birthweight and clinical evidence of rehydration.
2. Return of good urine flow as judged bypassage of a good volume of pale urine withoutdeposit.
3. Normal concentrations of sodium and potas-sium in the plasma. If the plasma sodium levelfalls below 130 mEq/l., isotonic saline solutionshould be given at a slow rate until it rises. Unlessthe plasma potassium level is raised, potassiummay be added to this solution and will help tomaintain the urine flow.
Careful selection of the concentration of sodiumchloride in the solutions to be used, together withthe judicious use of potassium salts, will usuallyavoid the complications from either over-retentionof sodium or water intoxication.
Prevention and treatment of hyponatraemia isemphasized because of the associated risk of con-vulsions which are difficult to control. Twitchingmay also be due to hypocalcaemia, examples ofwhich were recorded in the earlier part of thispaper. Twitching due to neonatal hypoglycaemiais avoided by the recommended use of 5 % glucosewith the electrolyte solutions.
Summary and ConclusionsA consecutive series of 24 newborn infants with
intestinal obstruction has been given parenteralfluids during the pre- and post-operation periodaccording to a plan devised for older infants andchildren, adapted for the first week of life. Thetreatment aims to replace abnormal losses, bothpreceding and following the operation and to main-tain the volume and composition of the body fluidswith emphasis on the importance of maintaininga free flow of urine.
Assessment of the results is based upon (i) theclinical course of all the 24 patients in the series,of whom 21 survived and three died, but in onlyone was the cause of death associated with electro-
lyte imbalance; (ii) balance studies in five infantswith duodenal obstruction; and (iii) analysis of(a) aspirated gastro-intestinal fluid and (b) the urineoutput in these and further cases.The average initial deficits deduced from the
balance data were Na 16, K 3- 3, and Cl 20 mEq/kg.body weight in the cases of duodenal obstruction,compared with much smaller deficits of sodium andchloride in an infant with oesophageal atresiainvestigated for comparison. The volume andcomposition of the aspirated gastro-intestinal fluidshow that daily losses from vomiting could have ledto these deficits.
Neither an immediate antidiuretic response, norretention of sodium following surgery were apparentfrom observations of urinary volume and of electro-lyte output, except perhaps in one premature infant.The amounts of sodium chloride in the solutions
recommended in the plan for the early phase of treat-ment are insufficient to replace the average deficits.Since the cumulative losses increase with delay intreatment and probably also with obstruction at lowerlevels of the small bowel, the amounts of sodiumsalts given for replacement should be judgedaccordingly. The treatment, especially in prematureinfants with a tendency to oedema, must be guidedby frequent reappraisal (clinical examination, serialweight, urine output and estimate of plasma electro-lyte levels) to avoid the risks of inadequate replace-ment on the one hand and of overloading on theother.
In conclusion, since the sodium and chloridedeficits of infants with severe dehydration asso-ciated with intestinal obstruction is likely to behigher than previously supposed, the need forreplacement of larger deficits should be assumedat the outset of treatment. As the extent of thedeficits cannot be closely predicted, frequentreappraisal is essential so that the initial plan can bemodified where necessary.
The authors are grateful to the consultant medical staffof the Queen Elizabeth Hospital for Children for per-mission to study cases under their care, and to the juniorstaff for their help. They also wish to thank the nursingstaff for their willing co-operation and skilled assistancethroughout the investigation. They are greatly indebtedto Dr. B. Levin, pathologist-in-charge, and Mr. V. G.Oberholzer, senior biochemist to the hospital, for thelaboratory investigations. The British Council andMessrs. Cow and Gate Ltd., generously supported thiswork by providing A.P. with a full-time research grantfor three and four months respectively.
REFERENCESBlack, D. A. K. (1957). The breakdown of the water equilibrium in
disease. Proc. Nutr. Soc., 16, 123.-, McCance, R. A. and Young, W. F. (1944). A study of dehydra-
tion by means of balance experiments. J. Physiol. (Lond.),102, 406.
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from

PARENTERAL FLUID THERAPY IN INTESTINAL OBSTRUCTION 241Calcagno, P. L., Rubin, M. 1. and Singh, W. S. A. (1955). The
influence of surgery on renal function in infancy. I. The effectof surgery on the postoperative renal excretion of water-Theinfluence of dehydration. Pediatrics, 16, 619.
Colle, E. and Paulsen, E. P. (1959). Response of the newborn infantto major surgery. I. Effects on water, electrolyte and nitrogenbalances. ibid., 23, 1063.
Dean, R. F. A. and McCance, R. A. (1949). The renal responsesof infants and adults to the administration of hypertonic solu-tions sodium chloride and urea. J. Physiol. (Lond.), 109, 81.
Gamble, J. L. (1947). Chemical Anatomy, Physiology and Pathologyof Extra-cellular Fluid. Harvard University Press, Cambridge,Massachusetts.
Grob, M. (1960). Intestinal obstruction in the newborn infant.Arch. Dis. Childh., 35, 40.
Gross, R. E. (1953). The Surgery of Infancy and Childhood, p. 21.Saunders, Philadelphia.
Hansen, J. D. L. and Smith, C. A. (1953). Effects of withholdingfluid in the immediate postnatal period. Pediatrics, 12, 99.
Heller, H. (1951). The water metabolism in newborn infants andanimals. Arch. Dis. Childh., 26, 195.
Holliday, M. A., Wallace, W. M. and Stapleton, T. Unpublisheddata quoted by Stapleton, T. (1958). In Modern Trends inPaediatrics (2nd series), p. 285, ed. A. Holzel and J. P. M.Tizard. Butterworth, London.
Le Quesne, L. P. (1957). Fluid Balance in Surgical Practice.Lloyd-Luke, London.and Lewis, A. A. G. (1953). Postoperative water and sodiumretention. Lancet, 1, 153.
Lowe, C. U., Rourke, M., MacLachlan, E. and Butler, A. M. (1950).Use of parenteral potassium therapy in surgical patients.Pediatrics, 6, 183.
McCance, R. A. (1948). Renal function in early life. Physiol. Rev.,28, 331.and Widdowson, E. M. (1954). The influence of events duringthe last few days in utero on tissue destruction and renal functionin the first two days of independent life. Arch. Dis. Childh.,29, 495.
-- (1957). Hypertonic expansion of the extra-cellularfluids, Acta paediat. (Uppsala), 46, 337.
- (1960). Renal aspects of acid base control in the newlyborn. 1. Natural development. ibid., 49, 409.
Rickham, P. P. (1957). The Metabolic Response to Neonatal Surgery.Harvard University Press, Cambridge, Massachusetts.
Santulli, T. V. (1954). Intestinal obstruction in the newborn infant.J. Pediat., 44, 317.
Swain, V. A. J., Peonides, A. and Young, W. F. (1963). Prognosisafter resection ofsmall bowel in the newborn. Arch. Dis. Childh.,38, 103.
Swenson, 0. (1958). Pediatric Surgery, p. 310. Appleton-Century-Crofts, New York.
Wilkinson, A. W. (1960). Body Fluids in Surgery, 2nd ed. Living-stone, Edinburgh and London.
Young, W. F., McIntosh, J., Swain, V. and Levin, B. (1959). Paren-teral fluid therapy for children undergoing major abdominalsurgery. Brit. J. Surg., 47, 261.
on 15 July 2018 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.38.199.231 on 1 June 1963. Dow
nloaded from