trieste april 12, 2012 gonadal non-germ cell tumorschped.it/gico/trieste/tumori gonadici - virgone -...
TRANSCRIPT
Gonadal non-Germ Cell
Tumors
C. Virgone – G. Cecchetto
TREP project (January 2000-March 2012)
TREP Meeting Trieste
April 12, 2012

Gonadal non-Germ Cell Tumors
Various and different histotypes including:
– Sex Cord-Stromal tumors (Ovary and Testis) 45 (13
t) » Juvenile Granulosa Cell tumors 24 (5
testic.)
» Sertoli-Leydig Cell tumors 14 (8
testic.)
» Others (fibrothecoma, GCT,…) 7
– Epithelial tumors 15 » Mucinous/Serous Cystadenoma (benign) 12
» Mucinous/Serous Cystadenoma (border-line) 3
» Mucinous/Serous Cystadenocarcinoma -
– Gonadoblastomas 2
• 23 girls (5-176 mo; median 110)
• Precocious puberty in 9/23 (8 JGCT)
• Ovarian torsion in 2, spontaneous tumor
rupture in 1
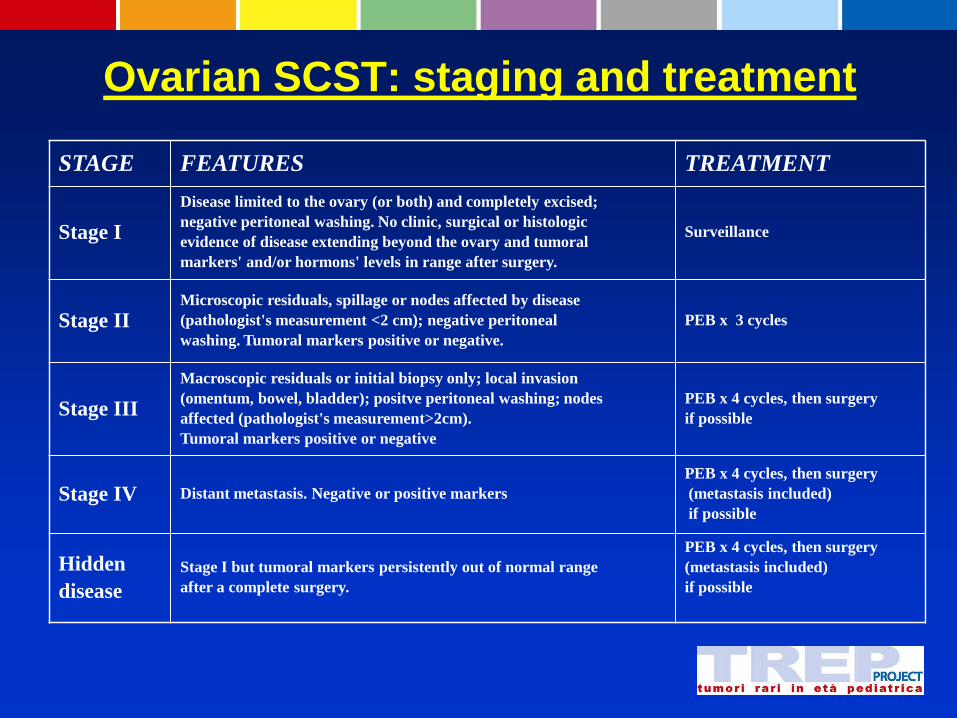
Ovarian SCST: staging and treatment
STAGE FEATURES TREATMENT
Stage I
Disease limited to the ovary (or both) and completely excised;
negative peritoneal washing. No clinic, surgical or histologic
evidence of disease extending beyond the ovary and tumoral
markers' and/or hormons' levels in range after surgery.
Surveillance
Stage II Microscopic residuals, spillage or nodes affected by disease
(pathologist's measurement <2 cm); negative peritoneal
washing. Tumoral markers positive or negative.
PEB x 3 cycles
Stage III
Macroscopic residuals or initial biopsy only; local invasion
(omentum, bowel, bladder); positve peritoneal washing; nodes
affected (pathologist's measurement>2cm).
Tumoral markers positive or negative
PEB x 4 cycles, then surgery
if possible
Stage IV Distant metastasis. Negative or positive markers
PEB x 4 cycles, then surgery
(metastasis included)
if possible
Hidden
disease
Stage I but tumoral markers persistently out of normal range
after a complete surgery.
PEB x 4 cycles, then surgery
(metastasis included)
if possible


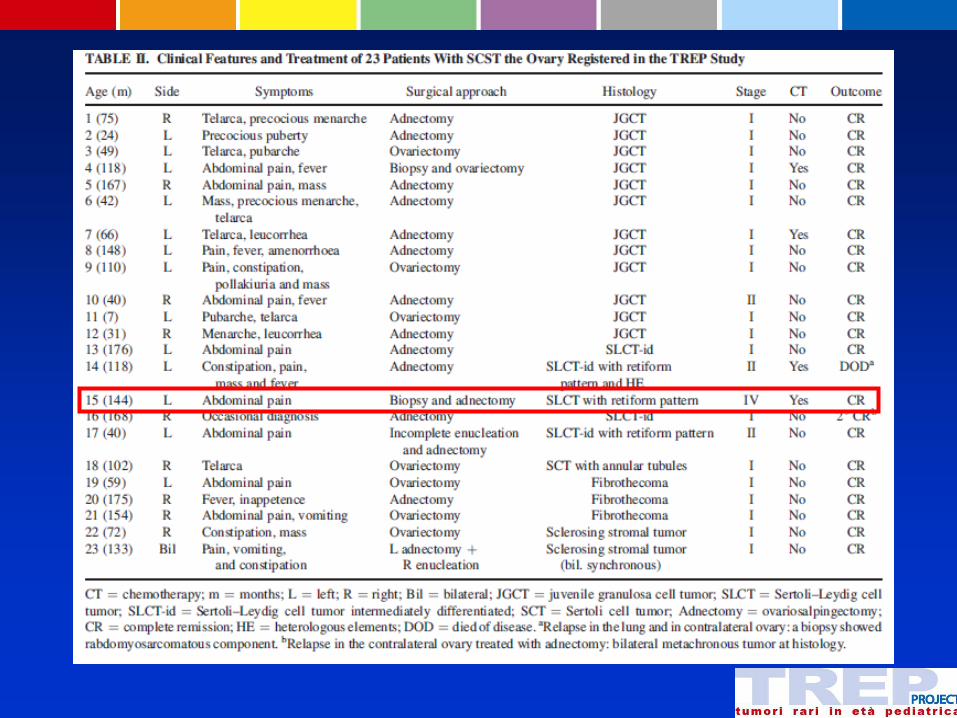
Treatment
• 16/25 adnectomy, 8/25 ovarectomy; 1 enucleation
• 2 bilateral tumors
» 1 SST: adnectomy and contralateral enucleation
» 1 SLCT: bilateral adnectomy (metachronous)
• 19 St I, 3 St II and 1 St IV: CT in 4/23 (2 St I, 1 St II
and St IV)
• 21 CR, 1 2° CR and 1 DOD
New cases
• 9 new patients registered from 2010 » 7 JGCT
» 1 GCT cistico, variante adulto
» 1 Fibroma/Thecoma
• 7 St I, 1 St II e 1 St III
• PEB in 2 cases
• CR in 9/9 cases

Series’ update (March 31, 2012)
Pts Age Endocrine
Symptoms Side Surgery CT Stage and Outcome (FU)
JGCT 19 70 mo
(4-172)
14 (prec.
puberty)
11 left
8 right
6 ovariectomy
13 adnectomy 4
16 st. I 19 CR
2 st. II (29 mo; 3-86)
1 st. III
SLCT 6 128 mo
(40-176) 0
4 left
1 bil
5 adnectomy
1 adnectomy 2
1 st. I 2nd CR 3 st. II 1 CR, 1 DOD*
1 st. IV CR*
(14; 3-32)
Thecoma 4 125 mo
(59- 175) 0
2 left
2 right
2 ovariectomy
2 adnectomy
0 4 st. I 4 CR
Sclerosing
Stromal
Tumor
2
172 and
133 mo
0 1 right
1 bil
1 ovariectomy
1 adnectomy +
contralateral
enucleation
0 1 st. I 2 CR
1 st. II (12, unk.)
GCT adult 1 144 mo 1 left adnectomy - St I CR (59 mo)

Ovary: conclusive results (follow-up 24 months – range 3-86)
32 cases:
first CR 30
second CR 1
DOD 1
- JGCT: 19/19 first CR
- SLCT: 4/6 first CR
1 second CR
1 DOD
- Other: 7/7 first CR
Remarks General compliance to guidelines
JGCT was the most frequent histotype: early stage at
diagnosis and excellent prognosis
SLCT affected older patients: major aggressiveness in
tumors with heterologous elements and/or retiform
pattern
Fibroma/Thecoma tumors and sclerosing stromal
tumors are uncommon in children and have a benign
behaviour
Remarks
Ovariectomy with sparing of adnexa when feasible
Minimally invasive procedures only in small tumors
Chemotherapy (as for MGCT) seems useful, but larger series are needed

• 11 patients
• 5/11 < 1 year (median 23 mo; 1-171)
• 1/11 with hormonal signs, 9/11 testicular enlargement

Testis SCST: staging and treatment
STAGE FEATURES TREATMENT
Stage I
Disease limited to the testis and completely excised via
inguinotomy. Tumoral markers' and/or hormons' levels in range
after surgery. Negative histological examination after
hemyscrotectomy (performed because of transscrotal approach
at first surg.)
Surveillance
Stage II
Microscopic residuals, nodes affected by disease (pathologist's
measurement <2 cm) or transcrotal orchiectomy with spillage.
Tumoral markers positive or negative. Positive histological
examination after hemyscrotectomy
PEB x 3 cycles
Stage III Nodes affected (pathologist's measurement>2cm). Tumoral
markers positive or negative
PEB x 4 cycles, then surgery
if possible
Stage IV Distant metastasis. Negative or positive markers
PEB x 4 cycles, then surgery
(metastasis included)
if possible
Hidden
disease
Stage I but tumoral markers persistently out of normal range
after a complete surgery.
PEB x 4 cycles, then surgery
(metastasis included)
if possible

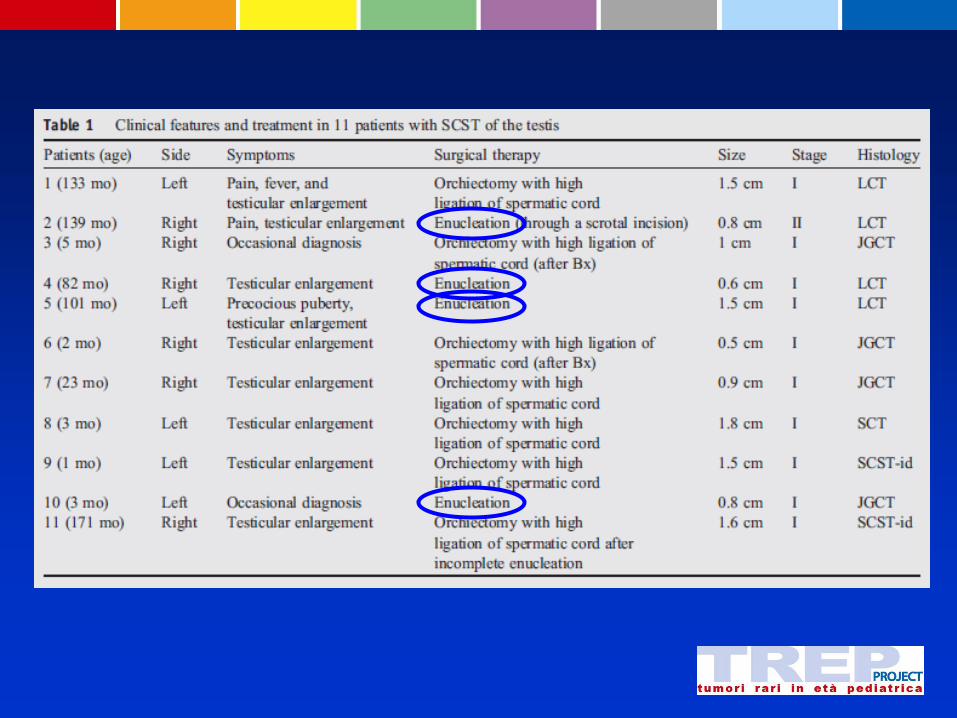
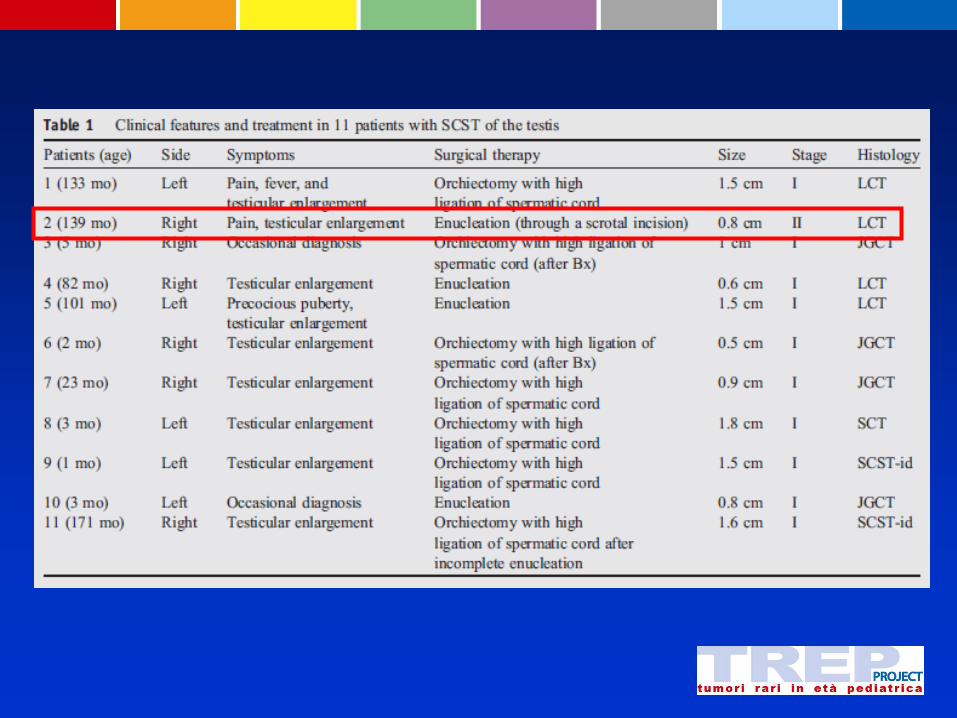

Treatment
4 enucleations
1 scrotal approach (St. II)-> no CT
10/11 St I; 11/11 CR

New cases
2 new cases registered from 2010:
1 JGCT: 20 days, testicular
enlargement, left orchifunicolectomy
1 Sertoli Cell tumor (only registration
form)
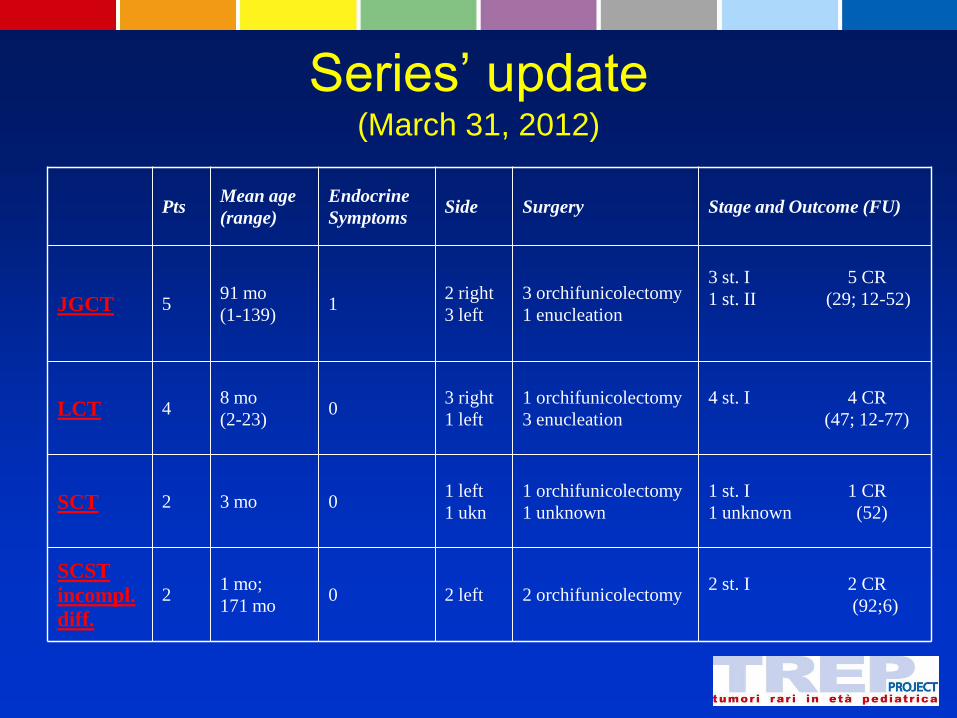
Series’ update (March 31, 2012)
Pts Mean age
(range)
Endocrine
Symptoms Side Surgery Stage and Outcome (FU)
JGCT 5 91 mo
(1-139) 1
2 right
3 left
3 orchifunicolectomy
1 enucleation
3 st. I 5 CR
1 st. II (29; 12-52)
LCT 4 8 mo
(2-23) 0
3 right
1 left
1 orchifunicolectomy
3 enucleation
4 st. I 4 CR
(47; 12-77)
SCT 2 3 mo 0 1 left
1 ukn
1 orchifunicolectomy
1 unknown
1 st. I 1 CR
1 unknown (52)
SCST
incompl.
diff.
2 1 mo;
171 mo 0 2 left 2 orchifunicolectomy
2 st. I 2 CR
(92;6)

Testis: conclusive results (follow-up 44 months-range 12-92)
13 cases first CR 12 (1 case missing data)
- JGCT: 6/6 first CR (3 enucl.)
- LCT: 4/4 “ (1 enucl.)
- SCT: 1/2 “
- other: 2/2 “
Remarks
General compliance to guidelines
LCT the most common histotype
Clinical benign behaviour (early diagnosis?)

Remarks
Enucleation accepted (if α-FP negative)
Intraoperative frozen section to allow testis-sparing
surgery
Scrotal access doesn’t need emiscrotectomy (if no
micro residuals)?
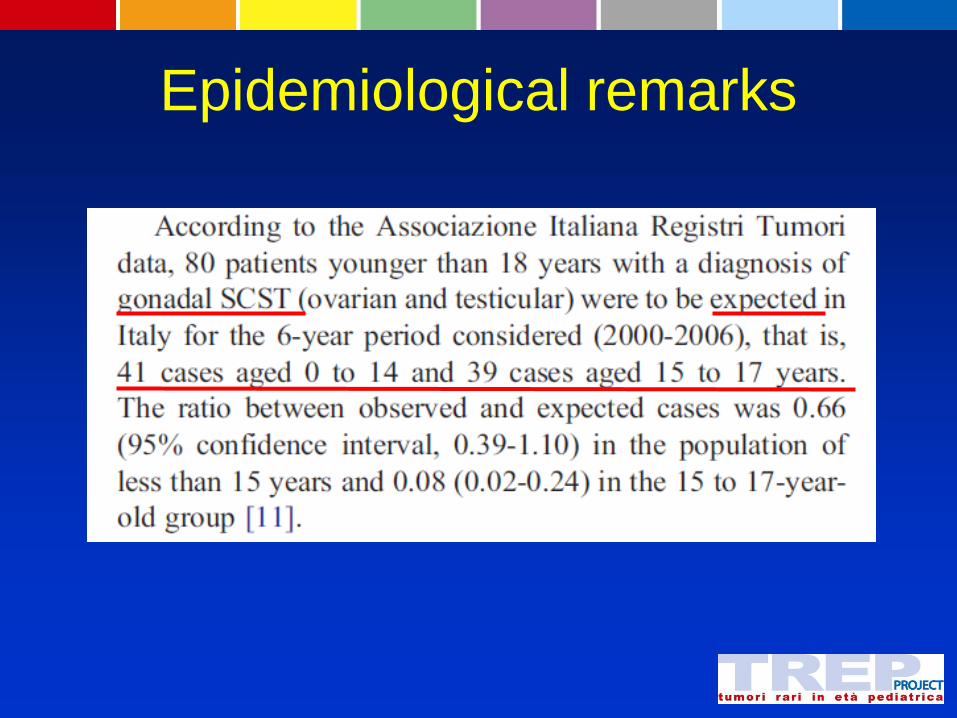
Epidemiological remarks

Epidemiological remarks
Epidemiological remarks
No children > 15 years in our testis SCST series
» 2 patients > 10 ys
No girls > 15 years in our ovarian SCST series » 11 patients > 10 ys
Girls > 15 ys affected by epithelial tumors
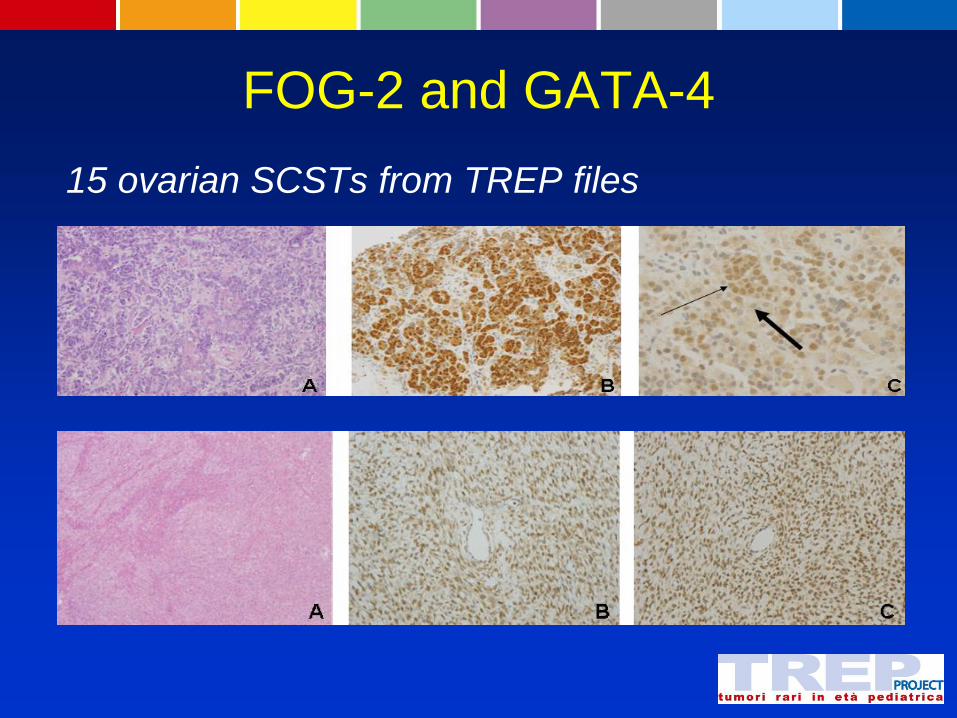
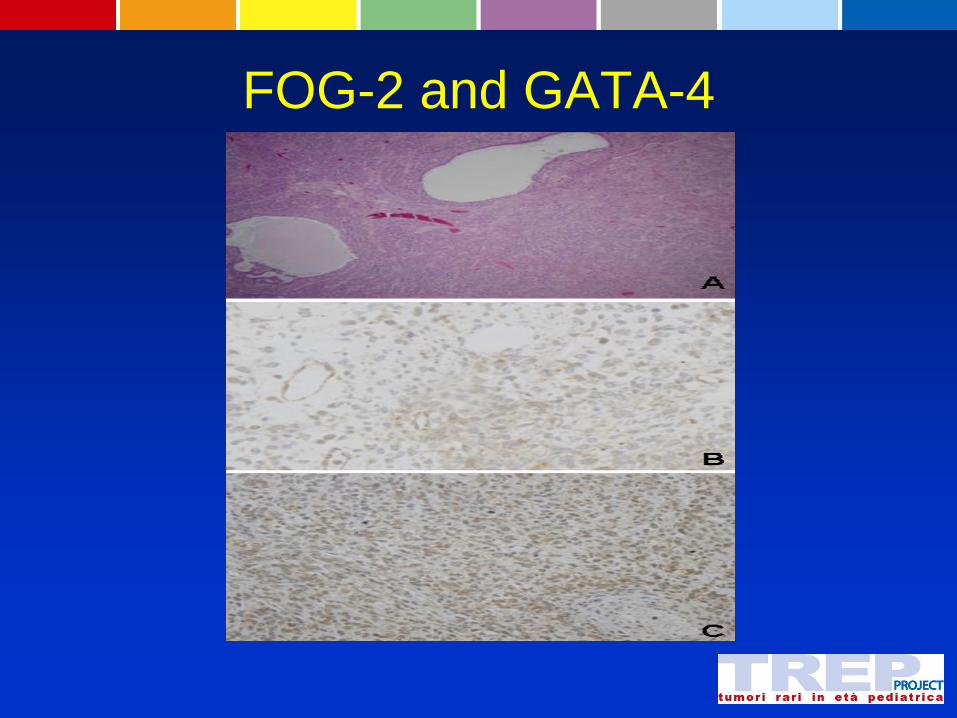
FOG-2 and GATA-4
15 ovarian SCSTs from TREP files
FOG-2 and GATA-4
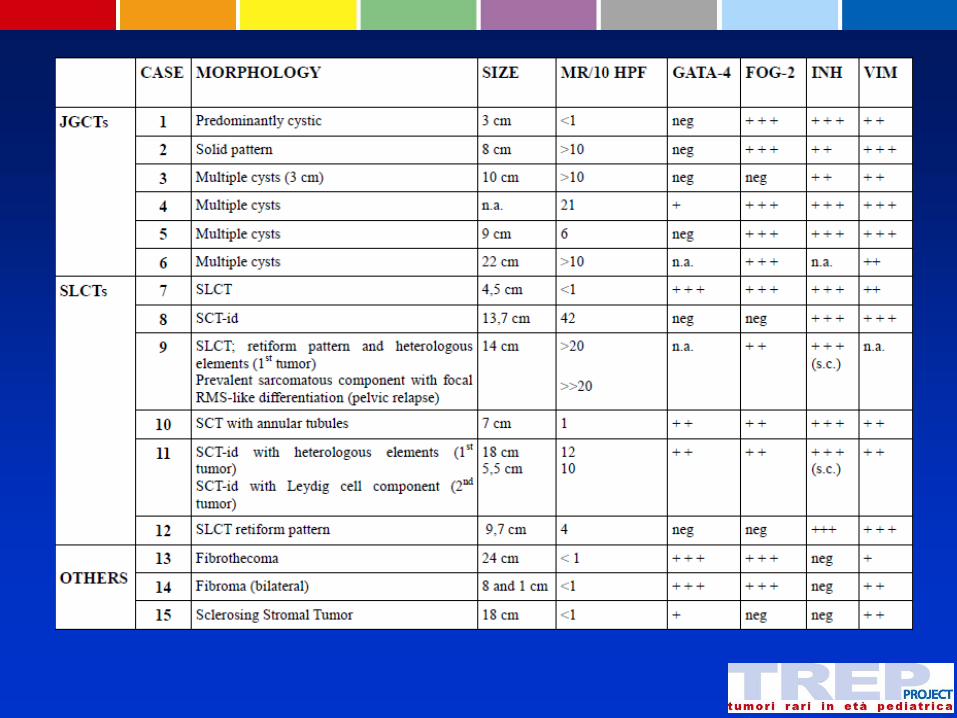

FOG-2 and GATA-4:
FOG/GATA expression replicates embryonal gonadal phenotype:
» JGCTs replicates primordial ovarian follicles
» SLCTs embryonal testis
In fibroma/thecoma group GATA-4 and FOG-2 indicate abnormal activation of GATA pathway and might be involved in the onset of these tumors

FOG-2 and GATA-4:
No correlation between GATA-4 and prognosis
and/or clinical behaviour both in JGCT and SLCT
GATA-4 expression in JGCTs may be contrasted
by strong FOG-2 expression (inhibiting role)
FOG-2 expression in SLCTs may have a
prognostic value? (lacking in advanced stage
tumors)