transposition of the great arteries in the developing world · transposition of the great arteries...
TRANSCRIPT

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y VO L . 6 9 , N O . 1 , 2 0 1 7
ª 2 0 1 7 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 1 0 . 0 5 1
Transposition of the Great Arteriesin the Developing WorldSurgery and Outcomes
David N. Schidlow, MD, MMUS,a Kathy J. Jenkins, MD, MPH,b Kimberlee Gauvreau, SCD,b
Ulisses A. Croti, MD, PHD,c Do Thi Cam Giang, MD,d Rama K. Konda, DCH,e William M. Novick, MD, MS,f
Nestor F. Sandoval, MD,g Aldo Castañeda, MD, PHDh
ABSTRACT
Fro
DC
Jos
Ind
Me
Gu
rep
Ma
BACKGROUND Little has been published regarding surgery for transposition of the great arteries (TGA) in the
developing world.
OBJECTIVES This study sought to identify patient characteristics, surgical interventions, institutional characteristics,
risk factors for mortality, and outcomes among patients undergoing surgery for TGA in this setting.
METHODS Developing world congenital heart surgical programs submitted de-identified data to a novel international
collaborative database as part of a quality improvement project.We conducted a retrospective cohort study that included all
cases of TGA with intact ventricular septum and TGA with ventricular septal defect performed from 2010 to 2013.
Demographic, surgical, and institutional characteristics and their associations with in-hospital mortality were identified.
RESULTS There were 778 TGA operations performed at 26 centers, 480 (62%) for TGA with intact ventricular septum
and 298 (38%) for TGA with ventricular septal defect. Most (80%) were single-stage arterial switch operations, but
20% were atrial baffling procedures (atrial switch operation) or 2-stage repairs (pulmonary artery band followed by
arterial switch operation). Age at operation was >30 days in one-half of the cases and did not vary significantly with
operation type. Survival was 85% and did not significantly vary with age at operation or operation type. Preceding
septostomy was infrequently reported (16%) and was not associated with surgical mortality. Mortality was associated
with lower World Health Organization weight/body mass index-for-age percentile and lower institutional volume of
TGA repair.
CONCLUSIONS Surgical repair of TGA performed in the developing world is associated with an early survival of 85%.
Type of surgical repair and age at operation varied considerably, but no associations with mortality were identified.
In contrast, poor nutrition and small surgical volume were most strongly associated with mortality. Multicenter
collaborative quality improvement efforts may benefit patients with TGA in the developing world.
(J Am Coll Cardiol 2017;69:43–51) © 2017 by the American College of Cardiology Foundation.
S urgical care for congenital heart disease (CHD)in the developing world is evolving rapidly,enhancing survival and improving quality of
life for children with previously lethal cardiac malfor-mations (1). This is important progress, but mortality
m the aChildren’s National Heart Institute, Children’s National Medical C
; bDepartment of Cardiology, Boston Children’s Hospital, Boston, Massac
é do Rio Preto, São José do Rio Preto, Brazil; dChildren’s Hospital 1, Ho
ia; fDepartment of Surgery, University of Tennessee Health Science C
mphis, Tennessee; gFundación Cardioinfantil IC, Bogotá, Colombia; a
atemala City, Guatemala. Dr. Schidlow is supported by the National Institu
orted that they have no relationships relevant to the contents of this pap
nuscript received June 2, 2016; revised manuscript received September 1
associated with CHD and its surgical care remainschallenging (2).
D-loop transposition of the great arteries (TGA) isthe second most common form of cyanotic congenitaldisease (3). Left untreated, TGA is associated with
enter, George Washington University, Washington,
husetts; cHospital da Criança e Maternidade de São
Chi Minh City, Vietnam; eCare Hospital, Hyderabad,
enter and William Novick Global Cardiac Alliance,
nd hUNICAR and the Fundación Aldo Castañeda,
tes of Health (T32-HL007572). All other authors have
er to disclose.
, 2016, accepted October 4, 2016.

ABBR EV I A T I ON S
AND ACRONYMS
ASO = arterial switch operation
ATS = atrial switch
BMI = body mass index
CHD = congenital heart disease
IQIC = International Quality
Improvement Collaborative for
Congenital Heart Surgery in
Developing World Countries
IVS = intact ventricular septum
STS = Society of Thoracic
Surgeons
TGA = transposition of the
great arteries
VSD = ventricular septal defect
WHO = World Health
Organization
Schidlow et al. J A C C V O L . 6 9 , N O . 1 , 2 0 1 7
TGA in the Developing World J A N U A R Y 3 / 1 0 , 2 0 1 7 : 4 3 – 5 1
44
mortality approaching 85% to 90% (4,5). Themedical and surgical management of TGA iswell established in many North American andEuropean countries, with the usual practicebeing single-stage anatomic repair witharterial switch operation (ASO) in the firstweek of life (3,6,7). Thirty-day mortalityis <3%, and 20-year survival approaches 90%(6,8–10). However, less is known about sur-gery for TGA in the developing world.
SEE PAGE 52
The purpose of this study was to identifypatient characteristics, surgical interven-tions, institutional characteristics, risk factorsfor mortality, and outcomes among patientswith TGA in the developing world, using datafrom the International Quality Improvement
Collaborative for Congenital Heart Surgery in Devel-oping World Countries (IQIC), a novel, multicentereffort aimed at reducingmortality in developing worldsettings (Figure 1) (11).
METHODS
Twenty-six IQIC sites in 15 countries contributeddata to this study (Table 1). All sites self-identified aspracticing in a resource-limited environment andparticipated voluntarily in IQIC. Sites submitted de-identified data pertaining to patients <18 years of ageundergoing operative repair for CHD that werecollected for quality improvement purposes. Datawereverified using a random 10% sample of cases from eachsite. Key variables audited included type of procedure,Risk Adjustment for Congenital Heart Surgery 1(RACHS-1) category, age, prematurity, post-operativeoutcomes, and 30-day follow-up outcomes. Approvalto conduct research using the IQIC database was ob-tained from the Boston Children’s Hospital Institu-tional Review Board. The IQIC database was searchedfor all instances of ASO, atrial switch (ATS), and TGAbetween January 2010 and December 2013. Associatedcardiac lesions were noted.
INCLUSION/EXCLUSION CRITERIA. Operations forTGA with intact ventricular septum (TGA/IVS) andTGA with ventricular septal defect (TGA/VSD) wereincluded. Patients entered into the database as hav-ing double-outlet right ventricle who underwent ASOwith VSD closure were included as TGA/VSD.
Operations in which the underlying anatomyincluded right- or left-sided obstructive lesions,including coarctation of the aorta, were excluded, aswere operations that involved complex intracardiaclesions, such as straddling atrioventricular valves.
Operations without data pertaining to mortality alsowere excluded.
STATISTICAL ANALYSIS. Demographic, surgical, andinstitutional characteristics were summarized withfrequencies and percentages. In order to account forthe correlation among patients within the sameinstitution, generalized estimating equation modelswere used to evaluate associations with in-hospitalmortality. Risk factors significant at the 0.10 level inunivariate analysis were considered for inclusion in amultivariable model; p < 0.05 was required forretention in the final model. Odds ratios and 95%confidence intervals were estimated.
RESULTS
There were 778 operations performed for TGA from2010 to 2013 (Table 2). Most surgeries (62%) werefor TGA/IVS; the remainder (38%) were for TGA/VSD.The majority of surgeries (70%) were performed inmales. Patients in a large proportion of cases (48%)were below the 5th percentile for World HealthOrganization (WHO) weight/body mass index (BMI)-for-age percentile. Surgeries in patients with identi-fied chromosomal abnormalities, major noncardiacstructural abnormalities, and prematurity were un-common. Preceding septostomy was reported in 16%of cases.
Most surgeries (80%) were single-stage ASO, butMustard or Senning ATS (13%) or 2-stage pulmonaryartery banding followed by ASO (7%) occurredfrequently. Only 11% of operations were performedduring the first week of life. The remaining 89% ofoperations were performed later, with a large pro-portion (51%) performed after 1 month of age. Amongthose in the latter group, 350 surgeries (45%) wereperformed between 1 month and 1 year of age, and 44(6%) were undertaken between 1 and 12 years of age.There was no significant association between patientage and choice of surgical repair.
The average annual institutional volume of TGAoperations varied. Most centers (62%) performedfewer than 10 TGA repairs annually. There was noassociation between surgical volume and choice ofsurgical repair.
Univariate associations with mortality are given inTable 3. The overall mortality rate was 15%. VSDclosure as part of the operation, male sex, lower WHOweight/BMI-for-age percentile, weight <3 kg, andprematurity were all factors associated with higherin-hospital mortality. Average annual volumes of TGArepair <10 cases and from 10 to 19 cases were alsoassociated with higher mortality relative to averageannual volume $20 cases.
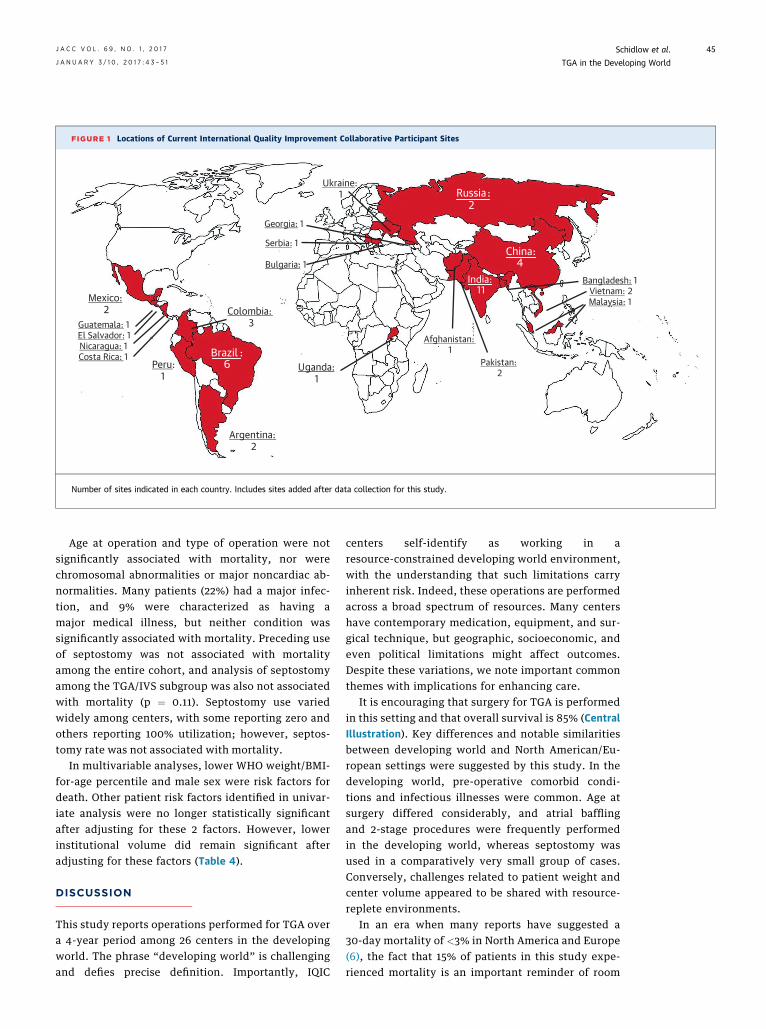
FIGURE 1 Locations of Current International Quality Improvement Collaborative Participant Sites
Russia:2
China:4
India:11
Brazil :6
Argentina:2
Peru:1
Colombia:3
Uganda:1
Mexico:2
Guatemala: 1El Salvador: 1Nicaragua: 1Costa Rica: 1
Georgia: 1
Serbia: 1
Bulgaria: 1
Ukraine:1
Afghanistan:1
Pakistan:2
Bangladesh: 1Vietnam: 2Malaysia: 1
Number of sites indicated in each country. Includes sites added after data collection for this study.
J A C C V O L . 6 9 , N O . 1 , 2 0 1 7 Schidlow et al.J A N U A R Y 3 / 1 0 , 2 0 1 7 : 4 3 – 5 1 TGA in the Developing World
45
Age at operation and type of operation were notsignificantly associated with mortality, nor werechromosomal abnormalities or major noncardiac ab-normalities. Many patients (22%) had a major infec-tion, and 9% were characterized as having amajor medical illness, but neither condition wassignificantly associated with mortality. Preceding useof septostomy was not associated with mortalityamong the entire cohort, and analysis of septostomyamong the TGA/IVS subgroup was also not associatedwith mortality (p ¼ 0.11). Septostomy use variedwidely among centers, with some reporting zero andothers reporting 100% utilization; however, septos-tomy rate was not associated with mortality.
In multivariable analyses, lower WHO weight/BMI-for-age percentile and male sex were risk factors fordeath. Other patient risk factors identified in univar-iate analysis were no longer statistically significantafter adjusting for these 2 factors. However, lowerinstitutional volume did remain significant afteradjusting for these factors (Table 4).
DISCUSSION
This study reports operations performed for TGA overa 4-year period among 26 centers in the developingworld. The phrase “developing world” is challengingand defies precise definition. Importantly, IQIC
centers self-identify as working in aresource-constrained developing world environment,with the understanding that such limitations carryinherent risk. Indeed, these operations are performedacross a broad spectrum of resources. Many centershave contemporary medication, equipment, and sur-gical technique, but geographic, socioeconomic, andeven political limitations might affect outcomes.Despite these variations, we note important commonthemes with implications for enhancing care.
It is encouraging that surgery for TGA is performedin this setting and that overall survival is 85% (CentralIllustration). Key differences and notable similaritiesbetween developing world and North American/Eu-ropean settings were suggested by this study. In thedeveloping world, pre-operative comorbid condi-tions and infectious illnesses were common. Age atsurgery differed considerably, and atrial bafflingand 2-stage procedures were frequently performedin the developing world, whereas septostomy wasused in a comparatively very small group of cases.Conversely, challenges related to patient weight andcenter volume appeared to be shared with resource-replete environments.
In an era when many reports have suggested a30-day mortality of <3% in North America and Europe(6), the fact that 15% of patients in this study expe-rienced mortality is an important reminder of room

TABLE 1 IQIC Sites Contributing Data
Institution City, Country
Aga Khan University Hospital Karachi, Pakistan
Amrita Institute of Medical Sciences Kochi, India
Armed Forces Institute of Cardiology, National Institute ofHeart Disease
Rawalpindi, Pakistan
Care Hospital Hyderabad, India
Research Institute for Complex Problems of CardiovascularDiseases, Siberian Branch of the Russian Academy ofMedical Sciences
Kemerovo, Russia
First Hospital of Lanzhou University Lanzhou, Gansu Province, China
Frontier Lifeline Hospital Chennai, India
Fundación Cardioinfantil de Bogotá Bogotá, Colombia
Fundación Cardiovascular Adulto-Pediátrica Clínica SanRafael
Bogotá, Colombia
Hospital da Criança e Maternidade de São José do RioPreto
São José do Rio Preto, Brazil
Hospital de Niños Córdoba, Argentina
Hospital Garrahan Buenos Aires, Argentina
Innova Children’s Heart Hospital Hyderabad, India
Institute of General & Urgent Surgery, Academy of MedicalSciences
Kharkiv, Ukraine
Instituto do Coração do Hospital das Clinicas deUniversidade de São Paulo
São Paulo, Brazil
Instituto Nacional de Pediatría México City, México
Instituto Nacional del Corazón Lima, Perú
Kokilaben Dhirubhai Ambani Hospital & Medical ResearchCenter
Mumbai, India
Mother and Child Health Institute Belgrade, Serbia
National Children’s Cardiac Medical Center Minsk, Belarus
Nhi Dong 1 (Children’s Hospital #1) Ho Chi Minh City, Vietnam
Shanghai Children’s Medical Center Shanghai, China
Star Hospital Hyderabad, India
Unidad de Cirugía Cardiovascular de Guatemala Guatemala City, Guatemala
United Hospital Dhaka, Bangladesh
West China Hospital, Sichuan University Chengdu, China
IQIC ¼ International Quality Improvement Collaborative for Congenital Heart Surgery in DevelopingWorld Countries.
Schidlow et al. J A C C V O L . 6 9 , N O . 1 , 2 0 1 7
TGA in the Developing World J A N U A R Y 3 / 1 0 , 2 0 1 7 : 4 3 – 5 1
46
for improvement in developing world settings. Thereasons for the relatively high mortality rate in thevaried groups described in this study are undoubtedlymultifactorial. However, this discrepancy is lessdisconcerting when one considers that mortality fromASO was similarly high in the early experience indeveloped countries (12). For example, in 1986,Quaegebeur et al. (13) reported an overall mortalityrate of 12% for ASO and 18% for ASO/VSD, similar tothe rates reported for surgeries in the current study. Alearning curve for the operative care of children withTGA is one historical certainty.
It must be noted, however, that many centers thatparticipated in this study have considerable experi-ence with TGA operations. The IQIC database does notcapture data regarding the number of years a centerhas been performing a specific surgery, nor does itcapture data regarding individual surgeon experience.Nevertheless, findings in this study regarding surgical
volume were similar to those identified using Societyof Thoracic Surgeons (STS) data in that a rate of <10ASO operations per year was associated with increasedmortality. Analysis of STS data also identified indi-vidual surgeon volume as an important factor associ-ated with increased mortality (14,15).
Operations in this study were clearly performed ata later patient age than in the developed world.Reasons were likely heterogenous on both regionaland patient levels. Differences in pre-natal diagnosis,cardiac anatomic details, pre-operative health, andcritical care and resuscitative expertise all likelycontributed to choices regarding age at operation.
Recent data from developed countries suggestedthat increasing numbers of infants with TGA arediagnosed prenatally, with rates ranging from 18% to50% (16–19). Sparse data from developing countriesexist, but our experience and that of other in-vestigators suggest that pre-natal diagnosis ofcongenital anomalies is rare, usually <5% (20).
Lack of pre-natal diagnosis is further complicatedby limited access to pulse oximetry in many regio-nal facilities and limited training in detection ofCHD, as pointed out by Mocumbi et al. (21). Local ge-ography might pose additional challenges to patientcare. In Vietnam, for example, only 5 centers have fa-cilities that perform CHD surgery. Long transportationtimes, often exceeding several hours, combinedwith limited or no access to prostaglandin maycontribute to patient deterioration (22). In addition,local customs might affect timing of patient care; forexample, some infants in Vietnam are deliberatelykept from light exposure, which may delay detectionof cyanosis (23).
This study identified major medical illnesses andmajor infections as common occurrences in this pa-tient group. The reasons are speculative, and specificdetails regarding the type and duration of illness orinfection are lacking. It is possible that some patientssuccessfully initiated on prostaglandin receivedexcessive doses, with resultant apnea that requiredassisted ventilation and hemodynamic support. Someinfants may require transport to treatment centerslocated high above sea level, which can result ininhibited pulmonary blood flow. Contributing tothese significant challenges is the inadequate numberof pediatric cardiologists in a number of countries (1).
Altogether, infants who present with such pre-operative challenges may require significant resusci-tation, which can delay surgery from several days toweeks. Other patients previously may have receivedcardiopulmonary resuscitation, and little or no in-formation about their neurological status may beavailable. Finally, many patients present with active

TABLE 2 Patient Characteristics, Operations, and Mortality
Surgeries Mortality
Total 778 (100) 119 (15)
TGA/IVS 480 (62) 67 (14)
TGA/VSD 298 (38) 52 (17)
Sex
Male 542 (70) 89 (16)
Female 236 (30) 30 (13)
Age at surgery
#7 days* 83 (11) 13 (16)
#30 days* 384 (49) 59 (15)
31 days to <1 yr 350 (45) 56 (16)
1–12 yrs 44 (6) 4 (9)
Nutrition status†
Overweight 3 (<1) 0 (0)
Normal 504 (65) 71 (14)
Malnourished 166 (21) 38 (23)
Emaciated 105 (13) 10 (10)
Weight <3 kg 225 (29) 46 (20)
WHO weight/BMI-for-age percentile
<5th 371 (48) 72 (19)
5th–14th 109 (14) 17 (16)
$15th 295 (38) 29 (10)
Prematurity 36 (5) 10 (28)
Major noncardiac structural anomaly 16 (2) 3 (19)
Major chromosomal abnormality 6 (1) 2 (33)
Major medical illness 68 (9) 14 (21)
Visiting surgical group present 30 (4) 4 (13)
Open chest post-surgery 284 (37) 58 (20)
Major infection 175 (22) 25 (14)
Operation
Arterial switch 382 (49) 53 (14)
Atrial switch 66 (8) 7 (11)
2-stage arterial switch 32 (4) 7 (22)
Arterial switch/VSD 240 (31) 44 (18)
Atrial switch/VSD 35 (5) 4 (11)
2-stage arterial switch/VSD 23 (3) 4 (17)
Annual volume TGA repair
<10 16 (122)‡ 36 (30)
10–19 5 (243)‡ 49 (20)
$20 5 (413)‡ 34 (8)
Values are n (%). *Age categories are not mutually exclusive. †Subjective assessment. ‡Number ofinstitutions (number of patients).
BMI ¼ body mass index; IVS ¼ intact ventricular septum; TGA ¼ transposition of the greatarteries; VSD ¼ ventricular septal defect; WHO ¼ World Health Organization.
J A C C V O L . 6 9 , N O . 1 , 2 0 1 7 Schidlow et al.J A N U A R Y 3 / 1 0 , 2 0 1 7 : 4 3 – 5 1 TGA in the Developing World
47
infection. One can infer that a later age at presentationand/or the degree of illness at presentation, ratherthan an intentional delay in surgical repair, are at leastpartly responsible for the timing of repairs (24).
It is interesting to note that few patients under-went preceding septostomy. Practices at institutionsin the United States and Europe vary, but many cen-ters frequently perform septostomy before surgicalrepair (6). In contrast, a preceding septostomy forpatients with TGA was rarely performed (16%) in thisstudy. Some centers reported ASO within the first24 h of life, possibly obviating the need for septos-tomy (25). This certainly does not reflect the low ratereported in this study, as most patients in this grouphad surgery after 1 month of life. This raises impor-tant questions about the pre-operative status of someof these patients. Some centers do not have readyaccess to catheterization equipment, facilities, orexpertise (26), suggesting that the patients who pre-sented for ASO in this study reflect a significant sur-vivorship bias. This is supported by the lack ofassociation between increased septostomy and sur-vival identified in this study. Simply put, those apriori lacking adequate atrial septal defects, a patentductus arteriosus, or other physiologically favorableattributes may not survive to operation.
Pediatric critical care in developing countries lagsbehind care in developed countries, as pointed out bySmith et al. (27). The finding of a 50% intensive careunit mortality rate in their study was ascribed todelayed presentation, poor access to health care re-sources, insufficient staffing, and limitations ofdiagnostic and interventional capabilities.
The types of repair reported in this study are ofinterest. The majority of patients underwent primaryASO, but 20% underwent ATS or 2-stage ASO. Ouranalysis did not reveal institutional preference, agedifference, or a survival benefit for a particular sur-gical approach, which raises important questions asto why the physiologically preferable ASO was notperformed. Perhaps this reflected inexperience withsurgical management of complex coronary patterns(e.g., intramural and single coronary) known to carrya higher mortality at repair in developed countries(28). Nonetheless, it seems unlikely that coronaryartery patterns alone could explain the high numberof ATS and 2-stage ASO.
Furthermore, previous experience with atrialbaffling procedures has revealed that the rightventricle is suboptimal as the systemic pumpingchamber in the long term (29), and with no differencein survival and no clear institutional preference, thisstudy closely resembled the early experience re-ported by the Congenital Heart Surgeons Society (12)
in that surgeon preference might be related to anat-omy. As experience is gained, ASO should be thepreferred approach, and recent studies suggest thattraining and uniform acquisition of surgical tech-nique in due course are feasible (14).
Among the types of surgical repair performed, thepatients who underwent 2-stage ASO for TGA/IVSexperienced the highest mortality. This difference didnot achieve statistical significance, possibly due tothe relatively low number of patients. This studycould not identify the reasons for this particular

TABLE 3 Univariate Associations With Mortality*
OR 95% CI p Value
Diagnosis
TGA/IVS 1.00 — —
TGA/VSD 1.30 1.00–1.69 0.05
Male 1.35 1.04–1.74 0.02
WHO weight/BMI-for-age percentile
<5th 2.20 1.48–3.29 <0.001
5th–15th 1.69 0.92–3.10 0.09
$15th 1.00 — —
Weight <3 kg 1.71 1.09–2.68 0.02
Prematurity 2.26 1.13–4.53 0.02
Open chest post-surgery 1.82 0.90–3.69 0.10
Average annual volume of TGA repair
<10 4.66 2.08–10.4 <0.001
10–19 2.82 1.12–7.09 0.03
$20 1.00 — —
*No statistically significant associations with age at surgery, major noncardiacstructural anomaly, major chromosomal abnormality, major medical illness,surgical procedure, whether a visiting surgical group was present, or presence of amajor infection.
CI ¼ confidence interval; OR ¼ odds ratio; other abbreviations as in Table 2.
Schidlow et al. J A C C V O L . 6 9 , N O . 1 , 2 0 1 7
TGA in the Developing World J A N U A R Y 3 / 1 0 , 2 0 1 7 : 4 3 – 5 1
48
approach; nonetheless, utilization of the 2-stage ASOstrategy raised interesting questions in light of re-ports, some recent, which suggested that primaryarterial switch can safely be performed at 1 month ofage and beyond, even in the presence of a decondi-tioned left ventricle (30). Given the high rate ofmortality among the 2-stage ASO patients, this mightbe a potential target for reducing mortality, particu-larly among patients younger than 1 month at thetime of planned surgery. Furthermore, as attention in
TABLE 4 Multivariable Associations With Mortality
OR 95% CI p Value
Patient characteristics
WHO weight/BMI-for-age percentile
<5th 2.23 1.48–3.33 <0.001
5th–15th 1.66 0.91–3.04 0.10
$15th 1.00 — —
Male 1.36 1.07–1.75 0.01
Adding annual TGA volume
WHO weight/BMI-for-age percentile
<5th 1.98 1.30–3.02 0.002
5th–15th 1.60 0.91–2.82 0.10
$15th 1.00 — —
Male 1.45 1.10–1.90 0.008
Average annual volume of TGA repair
<10 4.71 2.10–10.5 <0.001
10–19 2.41 0.91–6.41 0.08
$20 1.00 — —
Abbreviations as in Tables 2 and 3.
this setting inevitably gravitates from in-hospitalsurvival toward long-term neurodevelopmental out-comes, increasing focus will be placed on the timingand type of surgery.
Low WHO weight/BMI-for-age percentile wassignificantly associated with mortality. Associationsbetween weight at surgery and mortality have alsobeen identified using STS data. Curzon et al. (31)found that for a number of operations, includingASO, lower weight at surgery was a risk factor formortality. Although this was notably similar to thefindings in our study, the interplay among pre-operative condition, later age at surgery, nutritionalstatus, and mortality in developing world settingsis complex and merits additional investigation.Certainly, the importance of pre-operative nutritionalstatus in these settings cannot be overstated, andimproving nutrition for these particularly sensitivepatients is an important goal.STUDY LIMITATIONS. The IQIC database includesmany data elements regarding patients and out-comes; however, ensuring accurate data collection,despite annual data audits, is challenging. In addi-tion, data regarding patient characteristics haveintrinsic limitations. Major noncardiac abnormalitiesand prematurity probably were clinically evident, yetit is unlikely that genetic testing was performed for allpatients. Therefore, it is possible a larger patientproportion than that reported had 1 or more of thesepre-operative risk factors.
This study only collected data on TGA operativeoutcomes during a 4-year period. It is possible thatthese 4 years were not representative of the collabo-rative as a whole, especially as new centers joined theIQIC. Importantly, this study reflected data from 26centers from regions throughout the world, and thereare undoubtedly region-specific differences thatcannot be adequately delineated by this study.Furthermore, TGA surgery outcomes among IQICparticipating centers might not reflect all such sur-geries throughout the developing world. Importantly,although this study explored the effects of centervolume on outcomes, data regarding the extent ofcenter and surgeon experience were not obtained.
Details regarding the type and timing of infectiousillness, specific types of major medical illnesses, andimportant anatomic details (e.g., coronary artery andatrial septum anatomy) were not captured. Addi-tional details regarding pre-natal diagnosis, delay inpost-natal diagnosis, transport times, availability ofresuscitative medications (including prostaglandin),pre-operative status, availability and utilizationof extracorporeal membrane oxygenation, and sur-geon preferences might help shed light on choices

CENTRAL ILLUSTRATION Transposition of the Great Arteries in the Developing World:Patient Characteristics, Surgeries, and Outcomes
Schidlow, D.N. et al. J Am Coll Cardiol. 2017;69(1):43–51.
(A)WHOweight/BMI-for-age percentile. Results displayed as number and percentage of all operations. (B) Age at surgery. Results displayed as number and percentage
of all operations. (C) Operations performed and mortality. Results displayed as number and percentage of operations for each type of anatomy (TGA/IVS or TGA/VSD).
Mortality displayed as number and percentage of specific operations. 2S ¼ 2-stage; ASO ¼ arterial switch operation; ATS ¼ atrial switch operation; BMI ¼ body
mass index; IVS ¼ intact ventricular septum; TGA ¼ transposition of the great arteries; VSD ¼ ventricular septal defect; WHO ¼ World Health Organization.
J A C C V O L . 6 9 , N O . 1 , 2 0 1 7 Schidlow et al.J A N U A R Y 3 / 1 0 , 2 0 1 7 : 4 3 – 5 1 TGA in the Developing World
49

PERSPECTIVES
COMPETENCY IN SYSTEMS-BASED PRACTICE:
The pre-operative health status, use of antecedent
septostomy, age at operation, and surgical approach
for patients with TGA undergoing corrective surgery
in resource-limited developing world settings
differ from those in North America and Europe.
Overall in-hospital survival is encouraging at 85% in
this study comprising 26 centers in 15 countries.
Poor nutrition and lower surgical center volume are
associated with higher rates of in-hospital
mortality.
TRANSLATIONAL OUTLOOK: Quality
improvement initiatives such as the IQIC may identify
opportunities to improve outcomes for patients
undergoing surgical correction of TGA and other
forms of congenital heart disease in
resource-limited developing world settings.
Schidlow et al. J A C C V O L . 6 9 , N O . 1 , 2 0 1 7
TGA in the Developing World J A N U A R Y 3 / 1 0 , 2 0 1 7 : 4 3 – 5 1
50
regarding operations and outcomes. Importantly, thisstudy did not address patients with TGA who diedbefore receiving operative care.
CONCLUSIONS
Surgery for TGA is increasingly available in thedeveloping world. Survival is encouraging at 85%, butgains can be made. Important questions regardingpre-operative status, surgical strategy, timing of sur-gery, and post-operative care remain.
ACKNOWLEDGMENTS The authors thank the IQICcenters that contributed data for this study and theentire collaborative’s ongoing efforts towardimproving outcomes for children with congenitalheart disease.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.David N. Schidlow, Children’s National HeartInstitute, Children’s National Medical Center, 111Michigan Avenue, Northwest, Washington, DC 20010.E-mail: [email protected].
RE F E RENCE S
1. Bernier P-L, Stefanescu A, Samoukovic G,Tchervenkov CI. The challenge of congenital heartdisease worldwide: epidemiologic and de-mographic facts. Semin Thorac Cardiovasc SurgPediatr Card Surg Annu 2010;13:26–34.
2. Hoffman JI. The global burden of congenitalheart disease. Cardiovasc J Afr 2013;24:141–5.
3. Hoffman JI, Kaplan S. The incidence ofcongenital heart disease. J Am Coll Cardiol 2002;39:1890–900.
4. Mitchell SC, Korones SB, Berendes HW.Congenital heart disease in 56,109 births: inci-dence and natural history. Circulation 1971;43:323–32.
5. Campbell M. Incidence of cardiac malformationsat birth and later, and neonatal mortality. Br HeartJ 1973;35:189–200.
6. Villafañe J, Lantin-Hermoso MR, Bhatt AB, et al.D-Transposition of the great arteries. J Am CollCardiol 2014;64:498–511.
7. van der Linde D, Konings EEM, Slager MA, et al.Birth prevalence of congenital heart diseaseworldwide: a systematic review and meta-analysis.J Am Coll Cardiol 2011;58:2241–7.
8. Brown JW, Park HJ, Turrentine MW. Arterialswitch operation: factors impacting survival inthe current era. Ann Thorac Surg 2001;71:1978–84.
9. Sarris GE, Chatzis AC, Giannopoulos NM, et al.The arterial switch operation in Europe for trans-position of the great arteries: a multi-institutionalstudy from the European Congenital Heart Sur-geons Association. J Thorac Cardiovasc Surg2006;132:633–9.
10. Khairy P, Clair M, Fernandes SM, et al. Car-diovascular outcomes after the arterial switchoperation for D-transposition of the great arteries.Circulation 2013;127:331–9.
11. Jenkins KJ, Castaneda AR, Cherian KM, et al.Reducing mortality and infections after congenitalheart surgery in the developing world. Pediatrics2014;134:e1422–30.
12. Castaneda AR, Trusler GA, Paul MH,Blackstone EH, Kirklin JW. The early results oftreatment of simple transposition in the cur-rent era. J Thorac Cardiovasc Surg 1988;95:14–28.
13. Quaegebeur JM, Rohmer J, Ottenkamp J, et al.The arterial switch operation. An eight-yearexperience. J Thorac Cardiovasc Surg 1986;92:361–84.
14. Karamlou T, Jacobs ML, Pasquali S, et al.Surgeon and center volume influence on outcomesafter arterial switch operation: analysis of the STSCongenital Heart Surgery Database. Ann ThoracSurg 2014;98:904–11.
15. Jacobs JP, O’Brien SM, Pasquali SK, et al.Variation in outcomes for benchmark operations:an analysis of the Society of Thoracic SurgeonsCongenital Heart Surgery Database. Ann ThoracSurg 2011;92:2184–92.
16. Escobar-Diaz MC, Freud LR, Bueno A, et al.Prenatal diagnosis of transposition of the arteriesover a 20-year period: improved but imperfect.Ultrasound Obstet Gynecol 2015;45:678–82.
17. Bonnet D, Coltri A, Butera G, et al. Detection oftransposition of the great arteries in fetuses re-duces neonatal morbidity and mortality. Circula-tion 1999;99:916–8.
18. Bartlett JM, Wypij D, Bellinger DC, et al. Effectof prenatal diagnosis on outcomes in D-trans-position of the great arteries. Pediatrics 2004;113:e335–40.
19. Friedberg MK, Silverman NH, Moon-Grady AJ,et al. Prenatal detection of congenital heart dis-ease. J Pediatr 2009;155:26–31, 31.e1.
20. Kouame B, N0guetta-Brou I, Kouame GY, et al.Epidemiology of congenital abnormalities in WestAfrica: results of a descriptive study in teachinghospitals in Abidjan: Cote d0Ivoire. Afr J PaediatrSurg 2015;12:51.
21. Mocumbi AO, Lameira E, Yaksh A, Paul L,Ferreira MB, Sidi D. Challenges on the manage-ment of congenital heart disease in developingcountries. Int J Cardiol 2011;148:285–8.
22. Bartlett JM, Wypij D, Bellinger DC, et al.Challenges in the management of congenital heartdisease in Vietnam: a single center experience.Ann Pediatr Cardiol 2015;8:44–6.
23. Le LT, Partridge JC, Tran BH, et al. Carepractices and traditional beliefs related toneonatal jaundice in northern Vietnam: apopulation-based, cross-sectional descriptive study.BMC Pediatr 2014;14:264.
24. Bisoi AK, Ahmed T, Malankar DP, et al.Midterm outcome of primary arterial switchoperation beyond six weeks of life in children withtransposition of great arteries and intact ventric-ular septum. World J Pediatr Congenit Heart Surg2014;5:219–25.
25. Nevvazhay T, Chernogrivov A, Biryukov E,et al. Arterial switch in the first hours of life: noneed for Rashkind septostomy? Eur J CardiothoracSurg 2012;42:520–3.

J A C C V O L . 6 9 , N O . 1 , 2 0 1 7 Schidlow et al.J A N U A R Y 3 / 1 0 , 2 0 1 7 : 4 3 – 5 1 TGA in the Developing World
51
26. Kumar RK, Tynan MJ. Catheter in-terventions for congenital heart disease in thirdworld countries. Pediatr Cardiol 2005;26:241–9.
27. Smith ZA, Ayele Y, McDonald P. Outcomes incritical care delivery at Jimma University Speci-alised Hospital, Ethiopia. Anaesth Intensive Care2013;41:363–8.
28. Pasquali SK, Hasselblad V, Li JS, Kong DF,Sanders SP. Coronary artery pattern and outcomeof arterial switch operation for transposition of the
great arteries: a meta-analysis. Circulation 2002;106:2575–80.
29. Lange R, Hörer J, KostolnyM, et al. Presence of aventricular septal defect and the Mustard operationare risk factors for latemortalityafter theatrial switchoperation: thirty years of follow-up in 417 patients ata single center. Circulation 2006;114:1905–13.
30. Ma K, Hua Z, Yang K, et al. Arterial switch fortransposed great vessels with intact ventricularseptum beyond one month of age. Ann ThoracSurg 2014;97:189–95.
31. Curzon CL, Milford-Beland S, Li JS, et al. Car-diac surgery in infants with low birth weight isassociated with increased mortality: analysis ofthe Society of Thoracic Surgeons Congenital HeartDatabase. J Thorac Cardiovasc Surg 2008;135:546–51.
KEY WORDS arterial switch operation,congenital heart surgery, international,mortality, resource limited