the relationship between wealth and use of health services ... · ... a literature review and...
TRANSCRIPT

Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/320384259
Therelationshipbetweenwealthanduseofhealthservicesintheprivatesector:Aliteraturereviewandsecondarydataanaly....
TechnicalReport·July2016
DOI:10.13140/RG.2.2.28547.20008
CITATIONS
0
READS
33
2authors,including:
Someoftheauthorsofthispublicationarealsoworkingontheserelatedprojects:
EquityandPrivateSectorViewproject
HealthSystemsStrengtheningViewproject
NiraliMChakraborty
MetricsforManagement
26PUBLICATIONS398CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyNiraliMChakrabortyon13October2017.
Theuserhasrequestedenhancementofthedownloadedfile.

Therelationshipbetweenwealthanduseofhealthservicesintheprivatesector:Aliteraturereviewandsecondarydataanalysisfocusingonfamily
planningandcommonchildhoodillness
NiraliM.ChakrabortyAndreaSprockett
PreparedbyMetricsforManagement(M4M)forPopulationServicesInternational(PSI)
July,2016
ThisreportismadepossiblebythesupportoftheAmericanpeoplethroughtheUnitedStatesAgencyforInternationalDevelopment(USAID),underthetermsofCooperativeAgreementNo.AID-OAA-A-14-00037.ThePSI‘SupportforInternationalFamilyPlanningandHealthOrganizations(SIFPO)2:SustainableNetworks’Projectisafive-yearcommitmentfundedbyUSAID,thepurposeofwhichistoincreaseaccesstoanduseofhighquality,affordableFPandotherhealthinformation,productsandservicesglobally.

2
ExecutiveSummary....................................................................................................................3
Introduction...............................................................................................................................5
Section1:Publicversusprivatecare...........................................................................................6Familyplanningservices.............................................................................................................................................................7IMCIservices.....................................................................................................................................................................................8
Section2:Data.........................................................................................................................10
Section3:Results.....................................................................................................................11FamilyPlanning............................................................................................................................................................................12Diarrhea...........................................................................................................................................................................................16Fever/ARI........................................................................................................................................................................................22Limitationsofdata......................................................................................................................................................................27
Summary..................................................................................................................................27
References...............................................................................................................................30
Annex.......................................................................................................................................33

3
ExecutiveSummaryInordertounderstandifandhowwellthepoorarebeingservedathealthfacilities,socialfranchisesandotherserviceprovidershavebeguntosystematicallyassessthewealthoftheirclients.Understandingwhetherornottherelativelypoorareseekinghealthservicesataparticulartypeoffacilityisonlymoderatelyhelpfulwithoutassociatedcontext.Ifthepoorarenotcomingtoonetypeoffacility,aretheyinsteadseekingcareatanotherfacilitytype?Doesthewealthprofileofclientsdifferbaseduponthetypeofservicebeingsought?Whilethisanalysisfoundsomeinformationinthepublishedliteraturetodescribethisrelationship,analysesdidnotdifferentiatebetweenthevarietyofnon-publicsectorfacilities,oraggregatedresultsfromindividualcountriesintoregions.Studiesmadeclearthatthereisvariationintheuseoftheprivatesectorbytherelativelypoor–regionally,andbyreasonforseekingcare.Afterinvestigatingtheavailableliterature,thisanalysisfocusedonFamilyPlanningandIntegratedManagementofChildhoodIllness(IMCI)services,andlookedatpatternsofneedanduseofhealthservicesacross44low-andmiddle-incomecountries.Wefoundthatmoderncontraceptiveprevalencerates(mCPR)varywidely,from4.6%intheGuineato72.9%inColombiawithoutanobviousrelationshipbetweenmoderncontraceptiveprevalenceratesanduseoftheprivatesector.Forthechildhoodillnessesofdiarrhea,feverandacuterespiratoryinfection(ARI),prevalencewasremarkablysimilaracrosscountries,andcouldnotexplainthevariationinproportionofsickchildrenforwhomformaltreatmentwassought.Forexample,31%ofchildrenwithself-reportedARIsymptomssoughttreatmentinTanzania,comparedto65%ofchildreninneighboringKenya.ThelackofadiscernablepatternacrosscountriesforprivatesectoruseofFPandchildhealthservicesledtoamorein-depthanalysisof12countries.DatafromBangladesh,Cambodia,DemocraticRepublicofCongo,DominicanRepublic,Ghana,Haiti,Kenya,Liberia,Mali,Nigeria,SenegalandZambiawasexaminedtounderstandtheuseofFPandchildhealthservicesacrossdifferentpublicandprivatesectorfacilitytypes,andbywealth.Theresultsarerepresentedinaseriesofgraphs,andindicatethattherearedistinctregionalandcountrydifferencesintheuseofclinicsversuspharmacies,care-seekingforasickchild,anduseofthepublicversusprivatesector,acrosswealthquintiles.WesawfromthesecondaryanalysisofDHSdatathatinsomecountries,thepublicsectorisfavoredfortreatmentforchildren,whileinothers,theprivatesectorholdsalargeadvantage.Thesamecountrieswhichfavorthepublicsectorforchildhoodillnessdonotnecessarilyfavoritforfamilyplanningservices.Thereisalsonotaclearrelationshipbetweenuseofservicesinonesector,anddesirableoutcomes.Forexample,greateruseofservicesinonesector(publicorprivate)doesnotcorrelatewithhighercontraceptiveprevalenceratesincountries.Consequently,generalizationscannotbemadeacrosscountrieswithregardtouseofprivatesectorservices.Rather,countryandhealthareaspecificinformationiswarranted.Therewerealsocleardifferencesinwhereindividualsfromdifferentwealthquintilessoughtfamilyplanningservicesandcareforchildrenwithdiarrhea,fever,andARI.InWestAfricancountries,familyplanningusersareconcentratedamongthewealthy,andfavortheprivate

4
sector,ascomparedtopoorwomen.ThesamedifferentialisnotseenintheAsianorCaribbeancountries,withsimilarproportionsofwomenusingfamilyplanninginallwealthquintiles.Forchildrensufferingfromdiarrhea,treatmentintheprivatesectorisfavoredamongallwealthquintilesinBangladesh,CambodiaandNigeria,whereasthepublicsectorisalmostexclusivelyusedforthosewhosoughttreatmentinSenegalandZambia.Thesedifferencesareexaminedfurther,andareeasilyseeninthegraphspresented.Inexaminingthecontributionofsocialfranchises,additionalinformationisrequired.NoneoftheDHSdataisabletodisaggregateresultstodemonstratethecontributionsocialfranchisesmaketoprovidingcriticalservices.Countrylevelassessmentsofcareseekingbysectorandwealth,furtheranalysisofwhythesamehouseholdmakesdifferentchoicesincare-seeking,andcomparingthewealthprofileoffranchisedclientswithotherswillfurtherourunderstandingoftheroleoffranchisesinprivatesectorhealthcare,andcountryhealthsystemsmoregenerally.Forsocialfranchisesseekingtoplacetheirclientsinabroadercontext,theseresultssuggestthatatminimum,nationalanalysesofsecondarydatashouldbeconductedinordertounderstandwheretherelativelypoorandwealthyclientsseekhealthservices.Morein-depthstudies,suchasproposedbyMetricsforManagementinKenyafollowingthisreviewandanalysis,canprovideanswerstowhyclientschooseparticularserviceproviders.Thisinturnwillhelpimplementersandpolicyorfinancingdecisionmakerstomakemorestrategicdecisionsonpoliciesandresourceallocation.
5
IntroductionManyhealthprogramsindevelopingcountriesaimtoservethepoor,oftendefinedasthepoorest40%ofthetotalpopulationorasthoselivingbelow$1.90/day.Equityintheutilizationofhealthcareservices,aswellasthedifferencesinhealthoutcomesbasedonsocioeconomicstatus,isofinteresttodonororganizations,programleaders,researchers,andgovernments.Researchshowsusthatpoorerpatientsaremorelikelytogowithouthealthcarethanwealthierpatients,andtospendproportionatelymoreoftheirincomesonhealthcare(1,2).Policymakersandprogramleadersneedtounderstanddifferencesinwhoisservedbyvarioushealthserviceoutletsinthepublicandprivatesectors,includingwithinsocialfranchisingservices.Therearetrade-offsbetweenaccesstocare,qualityofcareprovided,andcoststhatmustbebalanced(3),makingitimportanttoputprogramperformanceincontextinordertomakeinformedpolicyandprogramdecisions.Whilemanysocialfranchisesaimtoservethepoorestwealthquintiles,asystematicreviewbyBeyeleretal.foundthatsocialfranchisesserverelativelyhigherincomepatients.BothhouseholdsurveysandexitinterviewsinPakistanshowedthatwealthierwomenweremorelikelytovisitasocialfranchiseclinic,whilepoorerwomenweremorelikelytousenon-franchisedservices.WhilethesameresultswereshowninEthiopia,asinglestudyinMyanmarshowedthatfranchisedclinicsinurbanareasservedahigherproportionofpoorerclients,althoughtherewasnodifferenceinruralornationalsamples(4).AstudyonaNepalesefranchisereportedpro-poorresults,whileworkinBihardidnotdemonstrateanystatisticallysignificantassociationbetweenhouseholdincomeanduseoffranchisedservices(5).Thesemixedresultspointtotheneedforadditionalresearchtounderstandtherelationshipbetweenaclient’swealthandtheiruseofhealthservices.Someofthedifferencesmaybedrivenbytheservicesbeingsought.Associalfranchiseorganizationsandothernot-for-profitandfor-profitserviceprovidershavebeguntosystematicallyassessequitybycapturingthewealthprofileoftheirclients,questionsareemergingregardingwhatanoptimalclientwealthdistributionshouldbe,andhowclientsatonefacilitytypecomparetoanotherfacilitytypeincludingpublic,privateforprofit,andnot-for-profitinstitutions.Thispaperpresentsareviewofthepublishedliteraturewithregardtouseofprimaryhealthservicesbysourceofcareandclientprofile.ItissupplementedwithdescriptiveresultsfromanarrayofrecentDemographicandHealthSurveys(DHS).Thefirstsectionreviewstheliterature.Thesecondsectiondescribesthedataandmethodsusedforthesecondaryanalysis.Thethirdsectionpresentstheresultsoftheseanalyses,followedbyaconclusion.TheseanalysessupporttheplannedresearchstudyinKenyatosystematicallyassessclientwealthacrossmultipletypesofhealthfacilities.

6
Section1:PublicversusprivatecarePrivateprovidersdeliverasignificantportionofhealthcareservicesinlow-andmiddle-incomecountries(LMICs)inbothruralandurbanareas,forlowsocioeconomicgroupsandforthewealthy(1).Mostliteratureuseslarge-scalesurveyssuchastheDemographicandHealthSurveysasthesourceofdata,andconsequentlyuseswealthquintileasthemeasureofsocio-economicstatus.ThewealthquintileisconstructedfromDHSdatausinganindexofassets,anddividesthepopulationintofiveequalgroups.Whilethepreciselevelsofprivateproviderprovision,especiallyfordifferingwealthquintilesandservicetypes,isnotwellunderstood,importantdifferencesinprivatesectorusebyindividualsofdifferentsocioeconomicstatushavebeenrecorded.Forexample,thereishighuseandhighvariationinuseoftheprivatesectorfortreatmentoffever,diarrhea,andforfamilyplanningservices(estimatesrangingfrom5-90%ofservicesdeliveredbytheprivatesector).Thereislessvariationinantenatalcareanddeliveryservices,whereglobally,anaverageof40%ofwomenusetheprivatesectorfortheseservices.Useoftheprivatesectorvariesbyregionandservicetype,highlightingtheneedtobetterunderstandwhereindividualsfromdifferentwealthquintilesseekhealthcare(6).Weseelargeregionalvarianceinuseoftheprivatesector.Insub-SaharanAfrica,healthcareservicedeliveryisnearlyevenlydividedbetweenthepublicandprivatesectorforallwealthquintiles.InSoutheastAsia,approximately65%ofthelowestwealthquintileseekscarefromtheprivatesector,comparedtoapproximately80%ofthehighestwealthquintile,whiletheprivatesectorprovidesnearly80%ofcareacrossallquintilesinSouthAsia.AndinLatinAmericanandtheCaribbean,thelowestwealthquintilereceivesapproximately22%ofcarefromtheprivatesector,whilethehighestwealthquintilereceives61%fromtheprivatesector(7).However,researchontheequityofprivateprovisionofhealthcareisinconclusive(8).Inhighincomecountries,nationalsurveysusingincomeandhealthserviceutilizationdatahaveshownthataccesscanbecomelessequitablewhenaprivatesectoroptionisavailable(9,10).Someanalyseshaveshownthatprovisionofcareintheprivatesectorisinherentlyinequitable,withsignificantlygreaterservicesaccessedbythewealthy(2).Othershaveshownthatstrategiessuchascontractingoutservicestotheprivatesectorcanimproveequity,orminimally,thatagrowingprivatesectordoesnotharmservicedeliveryequity(11,12).Whilepolicymakershaveofteninvestedmoreinpublicsectorservicedelivery,thereisgrowinginterestinhowtheprivatesectorcancomplementthepublicsector(3).Studiesassessingtheequityofsocialfranchisingasaservicedeliverystrategyarelimited,butindicatethatfranchisescanservepoorerclients(3,4,13).Forexample,inMyanmar,astudyoftheSunQualityHealthfranchisesprovidingtreatmentfortuberculosisfoundthattheseclinicsaretreatingpatientswhoarepoorerthanthegeneralpopulationinurbanareas(14).A2011studyfoundthatinPakistanthecostsperclientandtheproportionofclientsinthelowestwealthquintiledidnotdifferbetweenfranchisedandnon-franchisedprivateclinics.However,inEthiopia,franchisedclinicshadhighercostsandsawasmallerproportionofclientsinthelowestwealthquintile(3).Itisimportanttolookmorecloselyatthevarietyofprivateproviders,alongsidepublicproviders,andthepopulationstheyserveinlow-andmiddle-incomecountries.Large-scalehouseholdsurveyssuchastheDHSoffer
7
somedetailsonthetypeofprivatesectorcaresought,butnotwhetherornotitwasafranchise.Itisalsoimportanttoexaminedifferentpatternsofusebythetypeofhealthserviceneeded,astheprivatesectorisnotusedtothesameextentforallserviceneeds.Thisreviewexaminesservicesforfamilyplanningandchildhoodillness,specificallydiarrhea,feverandARI,inmoredetail.TheseserviceswerechosenbecausetheyareincludedinDHSsurveys,andareprovidedbysocialfranchises.
FamilyplanningservicesWhilepublicprovidersaretheprimarysourceoffamilyplanningservices,for-profitprivatesectorprovidersareresponsibleforalargeportionoffamilyplanningservicesinAsiaandAfrica,andnongovernmentalorganizations(NGOs)providealargeportionoffamilyplanningservicesinLatinAmerica(6).TherecentreinvigorationoffamilyplanningfundingthroughtheFP2020movementhasledtoanincreaseinresearchontheeffectivenessofprivatesectorfamilyplanningprograms.Forexample,onecomprehensivemeta-analysisofDHSdatafrom57LMICssystematicallylooksatuseoffamilyplanningbysector,bytypeofprivatesectorsource,andbycharacteristicsoftherespondents,includingwealth,education,andmethodchosen(15).Theseinterestingresults,summarizedbelow,aresupplementedbyothersmallerstudiesthatinvestigatewhywomenchooseonesectoroveranotherinvariouscountries.Campbellandcolleagues(2015)findthatwhileoverallcontraceptiveprevalenceismuchlowerinSub-SaharanAfricaascomparedtootherregions,theprivatesectorshareoffamilyplanningisremarkablysimilar(37-39%acrossallregions)(15).Additionally,useoftheprivatesectorforfamilyplanningincreasesbywealthandisgreaterinurbanascomparedtoruralareas.Thereare,again,limiteddifferencesbetweenregionsamongusersoffamilyplanning.Between15%and25%offamilyplanningusersinthepoorestquintileusetheprivatesectoracrossallregions(Sub-SaharanAfrica,MiddleEast/Europe,Asia,LatinAmerica),andbetween45%and50%ofthoseinthewealthiestquintileusetheprivatesector.Theprivatesectorisnotahomogeneousentity.Itcontainsdifferenttypesofproviders,rangingfromformalmedicalclinics,toregisteredpharmacies,drugsellers,generalretailers,faithbasedandnon-governmentalorganizations,andcanbeforprofitornon-profit.Thestudyisbasedonself-reporteddata,withitsinherentproblemsofrecallbias,poorrespondentknowledgeoffacilitytypes,andawkwardandinconsistentcategorizationsofsourceofcareintheDHSstudies(16).Yet,asauthorsnote,anin-depthlookatwhousestheprivatesectorforfamilyplanningisasignificantadditiontoourknowledgebase(15).Privateretailers,oftensellingcondomsandOCs,areamoresignificantsourceofcareinSub-SaharanAfrica(>10%oftheprivatesector)ascomparedtotheotherregions(<5%oftheprivatesector).SourcesclassifiedasaprivateNGOaremoreimportantinLatinAmerica,althoughitcompriseslessthan5%ofprivatesectorprovisionoffamilyplanning.Themajorityofprivatesectorsourcesareeithermedical,orspecializeddrugsellers(pharmacies,chemists).Privatemedicalsourcesaccountfor30%(Sub-SaharanAfrica)to60%(Asia)ofprivateFPprovision,andprovidemorecareinruralareasascomparedtourbanones,acrossallregions.Interestingly,theproportionofwomenwithnoorprimaryonlyeducationseekingcarefrom

8
theprivatemedicalsectorisgreaterthanthosewithhighereducation,amongthoseusingtheprivatesector(15).Onecanexaminespecificcountriesinmoredetail,tounderstanddifferencesbetweenthepublicandprivatesectors.ResearchinKenya,GhanaandTanzaniafindsthatclientsatisfactionisgreaterintheprivatesectorforfamilyplanningservices,howeverdifferencesinqualityweresmall,orfavoredthepublicsector(17,18).InEthiopiaandPakistan,publicsectorFPqualitywasfoundtobesignificantlyhigherthantheprivatefor-profitsector,butnotgreaterthansocialfranchises(3).InastudyinIndia,consultationtimeintheprivatesectorwassignificantlygreater,aswasprivacyandcleanliness(19).Thecostofcareisalsoasignificantconsiderationinprivatesectorprovision.ItisnotedthatprivatesectorFPuseincreaseswithwealth(15).Thepublicsectormaybenefitfromdonationsoffamilyplanningcommodities,allowingforprovisionoflowercostfamilyplanningservices.InNicaragua,thepublicsectorprovidesfree,3-monthinjectablessopoorerwomenandwomenchoosingthismethodweremorelikelytoseekcarefromthepublicsector(20).However,inLatinAmerica,theprivatesectorislosingdominanceinmanycountries(21).Thisisproblematicatatimewhendonorsupportforcommoditiesisdecreasing,andgovernmentsarenotsufficientlyfundingcontraceptiveservices(21).Overall,theliteratureindicatesthattheprivatesectorisanimportantsourceoffamilyplanningworldwide,withdifferencesinusebywealth,aswellasbymethodofchoice.EvidenceonimprovedqualityintheprivatesectorforFPismixed,howeverclientperceptionofqualityissuperior.
IMCIservicesAcuteRespiratoryInfections(ARIs)anddiarrheaarethemostcommonchildhoodillnesses,bothofwhichstronglycontributetochildmortality(22).IntegratedManagementofChildhoodIllnesses(IMCI)combinespreventionwithtreatmenttoimprovechildhealthoutcomes.Healthseekingbehaviorandoutcomesdifferbetweenthewealthquintiles,withwealthierhouseholdsbeingmorelikelytoseekcarethanpoorerhouseholds(23).Inastudyofcountriesthatshowedimprovementsinchildsurvival,andhadcompletedatleasttworecentDHS,morethanhalfofthecountriesshowedanincreasinggapinchildmortalitybetweenthehighestandlowestwealthquintiles(24).Basedonaggregatedatafromsub-SaharanAfricanDHS,althoughtheincidenceoffeverishighinallquintiles,incidenceishigherinthepoorestquintile(41%)ascomparedtothewealthiestquintile(32%).Controllingforothercharacteristics,thisdifferencedisappears,indicatingthatfeverisnotmorecommonamongonewealthgroup(23).Iftherateofillnessissimilar,anequitableoutcomewouldimplythatthepoorandwealthyseekcaresimilarlyalso.Globally,morethanhalfofallcareforchildrenseekingtreatmentfordiarrhea,fever,andcoughisprovidedbyprivateproviders(6).InananalysisofDHSdata,morethanone-quarterofmothersofsickchildrensoughtcarefrommultiplesectors,usingacombinationofpublicandprivateproviders,althoughtheprivatesectoristheprimarysourceofcarefor

9
fever/coughanddiarrhea(6,25).Inananalysisof38countries,Bustreo(2003)andcolleaguesfoundthatbetween37%-99%ofchildrenfromthepoorestwealthquintilewhosoughtcarefordiarrheaorARIwentoutsidethepublicsector(26).InSouthAsia,approximatelythreequartersofchildrenwithacuterespiratoryinfectionsfromthepoorestwealthquintileseekcarefromprivateproviders(25).Forexample,inBangladesh,nearly90%ofhouseholdsvisitedaprivateproviderforcommonchildhoodillnessesandmorethan80%ofchildrenwithdysenterysoughtcarefromprivateprovidersinIndia(6).Nevertheless,manyparentsdonotseektreatmentoutsidethehomefortheirchildren(27).InIndia,privateproviderswerepreferredfortreatmentofcommonchildhoodillnesses,suchasacuterespiratoryinfectionsandacutediarrhealdiseases.Althoughnearlyone-thirdofchildrenwithdiarrheaorfever/coughdidnotreceiveanytreatment,two-thirdsofthechildrenwhodidreceivetreatmentsoughtcarefromtheprivatesector.Althoughprivateprovidersarepreferredacrossallwealthquintiles,womenfromthehighestwealthquintilesweremorelikelytotaketheirsickchildrentoaprivateproviderthanwomenfromthepoorestquintiles(22).Inastudyinsub-SaharanAfricancountries,useoftheprivatesectorfortreatmentofchildhoodillnessesincreasedwithwealth.In60%offevercases,childrenweretakentoamodernmedicalprovidersuchasahospital,lower-levelfacility,privateprovider,pharmacyorshop,oratraditionalhealer.Only6%ofcasesoffeverinthelowestquintilesoughtcarefromapublichospital,while18%ofcasesvisitedapublichospitalinthehighestwealthquintile.Thehighestwealthquintilewasalsomorelikelytouseanysourceofcare,publicorprivate(23).Across26Africancountries45%ofsickchildrenseekcarefromeitheraformalorinformalprivateprovider(25).InLatinAmerica,37%ofchildrenwithdiarrheasoughtcareintheprivatesector(6).AnotherstudythatanalyzedDHSdatafrom26sub-SaharanAfricancountriesfoundthat28%ofparentsofchildrenwithdiarrheaoracuterespiratorytractinfectionsoughtcareatapublicfacility,22%ataprivateprovider,andtheremainingpercentdidnotseekcareoutsidethehome.Ofchildreninthelowestwealthquintilewhosoughtcareoutsidetheirhomes,51%wenttothepublicsectorand45%wenttotheprivatesector(24).Aswithfamilyplanning,theliteraturerevealsthattheprivatesectoriswellutilizedforcare-seekingforchildhoodillness,evenamongthoseinthepoorestquintiles.However,manychildhoodillnessesarenottreatedintheformalmedicalsector,revealingan‘unmetneed’forcare.Thereviewofliteratureonuseofprivatesectorhealthservicesbywealthlendsitselftoanumberoffollow-upinquiries.AlthoughtheCampbelletalanalysis(2015)findsuseofprivatesectorFPissimilaracrossregions,arethereimportantwithinregiondifferences?Docountriesfollowsimilarpatternsofprivatesectoruseforbothwomen’sandchildren’shealthneeds?Inexploringtherelationshipbetweenhouseholdwealthandhealthsectorused,thispaperexaminesthedataindifferentwaystodrawmeaningfulconclusionsforsocialfranchises.Insection2,wedescribethedatausedfortheseanalyses.
10
Section2:Data
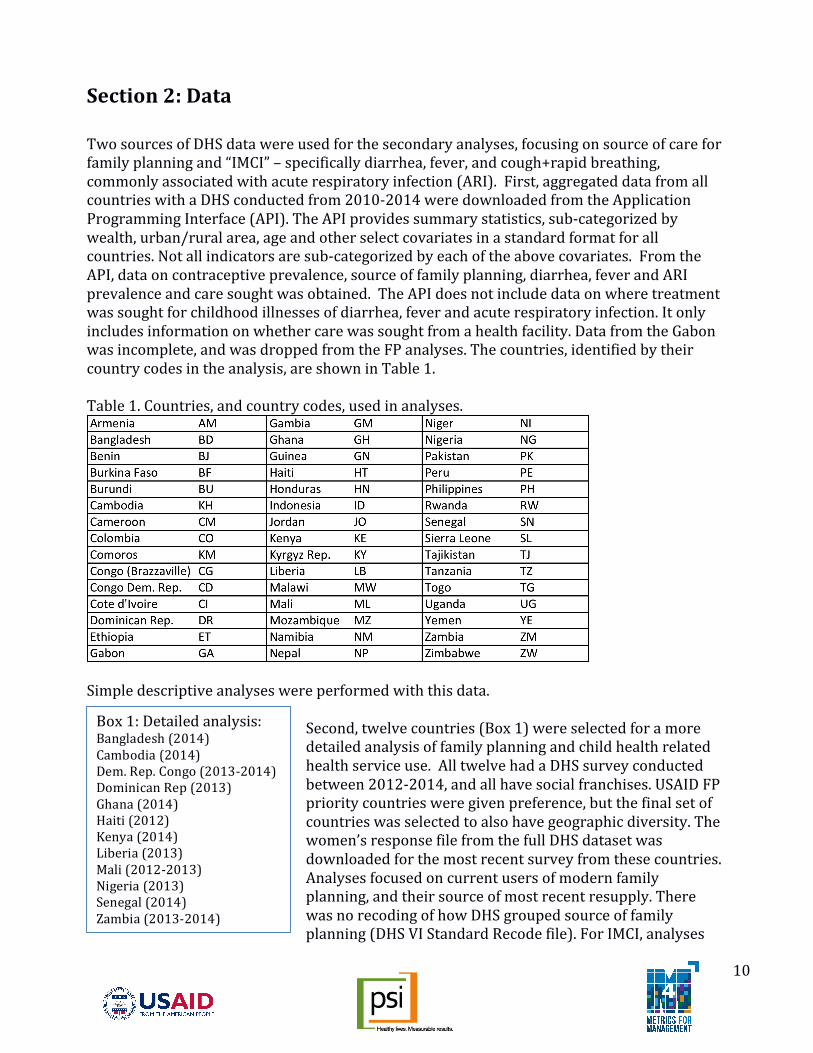
TwosourcesofDHSdatawereusedforthesecondaryanalyses,focusingonsourceofcareforfamilyplanningand“IMCI”–specificallydiarrhea,fever,andcough+rapidbreathing,commonlyassociatedwithacuterespiratoryinfection(ARI).First,aggregateddatafromallcountrieswithaDHSconductedfrom2010-2014weredownloadedfromtheApplicationProgrammingInterface(API).TheAPIprovidessummarystatistics,sub-categorizedbywealth,urban/ruralarea,ageandotherselectcovariatesinastandardformatforallcountries.Notallindicatorsaresub-categorizedbyeachoftheabovecovariates.FromtheAPI,dataoncontraceptiveprevalence,sourceoffamilyplanning,diarrhea,feverandARIprevalenceandcaresoughtwasobtained.TheAPIdoesnotincludedataonwheretreatmentwassoughtforchildhoodillnessesofdiarrhea,feverandacuterespiratoryinfection.Itonlyincludesinformationonwhethercarewassoughtfromahealthfacility.DatafromtheGabonwasincomplete,andwasdroppedfromtheFPanalyses.Thecountries,identifiedbytheircountrycodesintheanalysis,areshowninTable1.Table1.Countries,andcountrycodes,usedinanalyses.
Simpledescriptiveanalyseswereperformedwiththisdata.
Second,twelvecountries(Box1)wereselectedforamoredetailedanalysisoffamilyplanningandchildhealthrelatedhealthserviceuse.AlltwelvehadaDHSsurveyconductedbetween2012-2014,andallhavesocialfranchises.USAIDFPprioritycountriesweregivenpreference,butthefinalsetofcountrieswasselectedtoalsohavegeographicdiversity.Thewomen’sresponsefilefromthefullDHSdatasetwasdownloadedforthemostrecentsurveyfromthesecountries.Analysesfocusedoncurrentusersofmodernfamilyplanning,andtheirsourceofmostrecentresupply.TherewasnorecodingofhowDHSgroupedsourceoffamilyplanning(DHSVIStandardRecodefile).ForIMCI,analyses
Box1:Detailedanalysis:Bangladesh(2014)Cambodia(2014)Dem.Rep.Congo(2013-2014)DominicanRep(2013)Ghana(2014)Haiti(2012)Kenya(2014)Liberia(2013)Mali(2012-2013)Nigeria(2013)Senegal(2014)Zambia(2013-2014)

11
focusedontheyoungestchildunderaged5(thefirstchildlisted).Respondentsareaskedifthechildhadanepisodeofdiarrheaintheprevioustwoweeks,andthesourceofcare,ifany,forthechild.Respondentsarealsoaskedifthechildhadafeverintheprevioustwoweeks,andifthechildhasacough.Childrenwhosecoughisaccompaniedbyrapidbreathing,andthosewithfever,areaskedaboutsourceofcare,ifany.Thesourceofcareforthesetwoillnessesisgroupedtogether.Sourcesofcarefordiarrheaandfever/ARIarecategorizedinupto24countryspecificcategories.Thesecategorieswererecodedinto8groupsforall12countries,andarepresentedintheanalysesassuch.Childrenmayseekcareatmorethanoneplaceforthesameepisode,soanalysespresentedallowformultipleresponses.Weighteddescriptiveanalyseswereconductedforfamilyplanning,andunweightedcountry-specificanalyseswereconductedfordiarrheaandfever/ARI.Covariatesofinterestwerewealthquintile,urban/ruralresidenceandrespondentage(woman’sage).
Section3:ResultsAnalysesfocusonpatterns,inordertoidentifyifthereareanytrendsinuseofprivatesectorservices,whichservicesorproviderswithintheprivatesectoraremorefavored,andifitispossibletoassessthesedatabywealthquintile.Table2liststhemoderncontraceptiveprevalenceforeachofthe12countriesassessedindepth,aswellasthesamplesizesforwomenandchildren.Columns4and5listtheincidenceofdiarrheaandfeverorARIreportedfortheyoungestchild.Samplesizesvarygreatlyamongcountries,indicativeofvaryingillnessprevalence,aswellasdifferentsurveyrequirements.Forexample,inNigeriaandKenya,largesampleswerecollectedinordertohaveregionanddistrictspecificestimatesforkeyindicators.Analysesbymultiplesub-categoriesarelimitedbysmallsamplesizesinsomeinstances.Inotherwords,itisnotfeasibletoassessuseofpharmaciesfordiarrheabywealthquintile,assamplesizeswouldbetoosmall.Table2.Summarystatistics.

12
Foreachofthethreehealthneeds(familyplanning,diarrhea,ARI/Fever),wefirstexaminecountrylevelpatternsofuseandneed,andwhereorifcareissought.Second,welookat12countriesindepth,andexaminepatternsofusebytypeoffacility.Finally,weseeifthesepatternsdifferbywealthquintile.Databywealthquintileisnotasnuancedduetosamplesizelimitations.
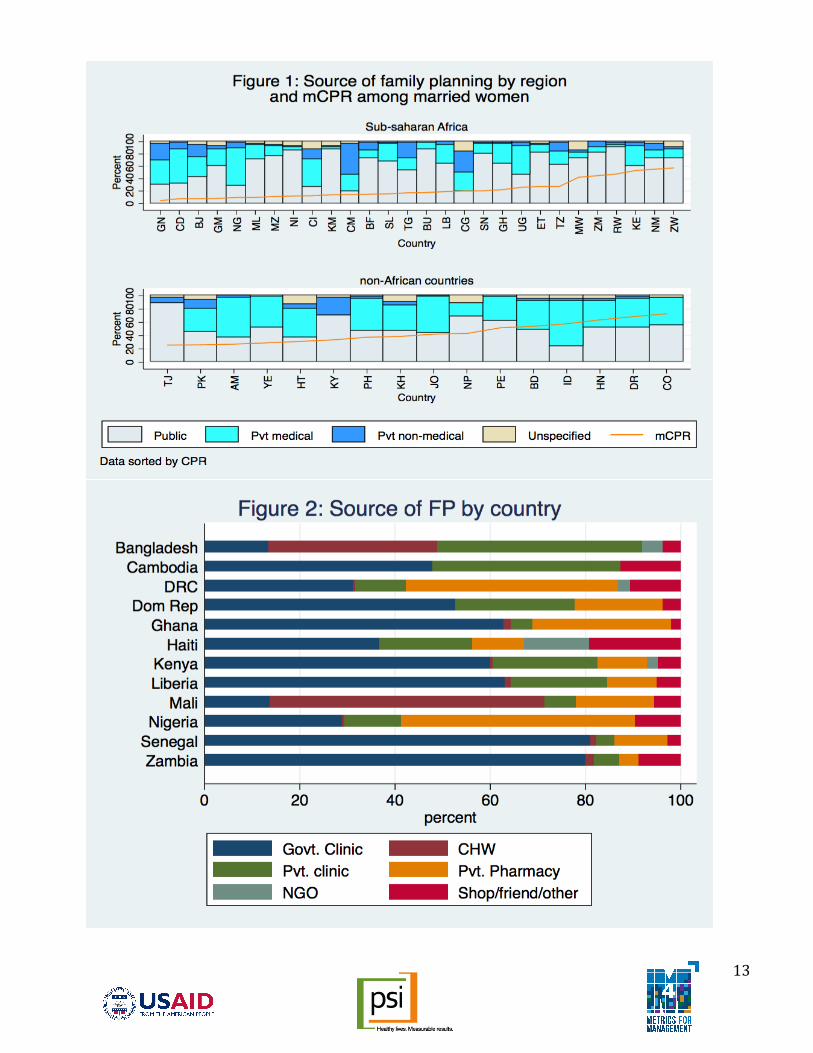
FamilyPlanningLookingacross44low-andmiddle-incomecountries,wefindthatmoderncontraceptiveprevalencerates(mCPR)varywidely,from4.6%intheGuineato72.9%inColombia(seeappendix1).Asseeninthisgraph,thereisnotanobviousrelationshipbetweenmoderncontraceptiveprevalenceratesanduseoftheprivatesector(figures1).IncreasedmCPRdoesnotcorrespondtoincreaseduseoftheprivatesectoracrossregions.Forexample,Mozambique(MZ)andZimbabwe(ZW)havesimilaruseoftheprivatemedicalsectorat16.1%and14.1%respectively.YettheCPRamongmarriedwomenis11.3%inMozambiqueand57.3%inZimbabwe.WedotendtoseeanoverallhighermCPRininnon-Africancountriesthaninsub-SaharanAfricancountries(withnotableexceptionsofKenya,Zimbabwe,andNamibiawheretheratesareabove50%).Theprivatemedicalsectorinthesegraphsreferstoclinics,hospitalsandpharmacies,whiletheprivatenon-medicalsectorreferstoshops,churches,friendsandrelatives.Useofboththeprivatemedicalandprivatenon-medicalsectorsvarywidelyinsub-SaharanAfrica,from5.5%inComoros(KM)to77%inCameroon(CM),yetthesecountrieshaveremarkablysimilarmCPRratesamongmarriedwomenat14.2%and14.4%,respectively.Wealsoseeamoderatelyhigheruseoftheprivatesectorinmiddle-incomecountriesthaninlow-incomecountries,yetmCPRratesdonotvaryinaccordancewithuseoftheprivatesector.Privatesectoruseisapproximately40%inthemiddle-incomecountriesofKenya,Ghana,Peru,Colombia,andHonduras,yetmCPRratesrangefrom22.2%inGhanaupto72.9%inColombiaamongmarriedwomen,despitesimilarprofilesofprivatesectoruse(Seeannex).Lookingmorein-depthat12comparisoncountries,weareabletofurtherdifferentiateinthetypeofpublicandprivatesectorsourcesused.Sourceoffamilyplanningservicesvarieswidelyacrosscountries,withthegreatestuseofprivateclinicsinBangladeshandCambodia,highuseofprivatepharmaciesintheDRCandNigeria(over40%)andthepublicsectordominatinginSenegalandZambia(figure2).Haitiisnotableforitshighuseofshop/friend/otherforservices,aswellaslargerNGOuseforFP,ascomparedtotheothercountriesanalyzed.BangladeshandMalibothhaveaveryhighproportionofservicesprovidedbycommunityhealthworkersinthepublicsector,at35%and58%,respectively.Approximatelytwo-thirdsofservicesinKenyaareprovidedbygovernmentclinics,withnearly30%providedbyprivateclinics,pharmacies,orNGOs.
13

14
Patternsinthetypesoffacilitiesusedforfamilyplanningservicesremainsimilaracrossurbanandruraldivides,althoughprivateclinicsaremoreoftenusedinurbansettingsthaninrural(seeannex).WealsoseeincreaseduseofgovernmentclinicsinruralKenyathaninurban,pairedwithdecreaseduseofprivateclinicsandprivatepharmacies.Unlikeotherhealthneeds,FPdatacanalsobeanalyzedbythetypeofmethodsought.AlthoughpublicsectorclinicsarenothighlyusedbywomeninBangladesh,womeninBangladeshweremorelikelytousethepublicsectorforpermanentandlong-actingreversiblecontraceptives(LARCs),andaprivatesectorclinicforshort-termmethods.InSenegal,womenusedapublicsectorclinicorpharmacyforalltypesoffamilyplanningmethods(91%ofpermanentmethods,76%ofshort-termmethods,and93%ofLARCs).Zambiawassimilarwith68%ofwomenreceivingpermanentmethodsfromapublicsectorclinicorpharmacy,78%receivingshort-termmethods,and95%receivingLARCsinthepublicsector.Acrossall12countries,womenweremorelikelytousethepublicsectorforpermanentandLARCmethods(seeannex).Acrossthe12in-depthcomparisoncountries,mCPRgenerallyincreasesfromthelowesttothehighestwealthquintiles,withtheinterestingexceptionsoftheDominicRepublicandGhanawherethereversetrendisseenwithhigheruseofmoderncontraceptivemethodsinthelowesttwowealthquintiles(Table3).Kenya’swealthquintilesallfallaround40%use,withtheexceptionofthelowestwealthquintilewithonly23.5%ofallwomenusingmoderncontraceptivemethods.Table3.PercentageuseofmoderncontraceptivemethodsamongmWRAbywealthquintile.
Asseeninfigure3,theprivatesectorisamoresignificantsourceoffamilyplanningforwomeninquintiles4and5,ascomparedtopoorerwealthquintiles.Whiletable3showsthecontraceptiveprevalenceineachquintile,figure3showswhatproportionofFPusersareineachquintile,andwheretheywentthelasttimetheyneededFP.Ingeneral,useoftheprivatesectorincreasesbywealthquintile.EvenincountrieswhereasimilarpercentageofwomenineachwealthquintileuseFP,wealthierwomenseektheirservicesfromtheprivatesectormorefrequently.Acountrylevelanalysisshowsthatregionalcategorizations,asprovidedbyCampbell,maskdifferences(15).

15

16
DiarrheaWorldwide,treatmentpatternsfordiarrheavary,despitelimitedvariationintheprevalenceratefordiarrhea.Similarproportionsofchildrenunderfivereporteddiarrheainthetwoweeksprecedingthesurvey,howeverchildrenaretwiceaslikelytobetakentoafacilityinGambia,Malawi,Namibia,SierraLeoneorZambiathantheyareinCameroon,Coted’Ivoire,NigeriaorTogo.Figure4showsthisvariationbycountry,aswellasvariationintheproportionofchildrenwhoreceivenotreatmentatall,acrudemeasureof‘unmetneed’.ThedatausedforFigure4cannotdifferentiatebyfacilitytype(i.e.hospitalorpharmacy),sector(publicorprivate),orseverityofdiarrhea.Childrenseekingtreatmentat“other”havegonetoashoporunqualifiedprovider.
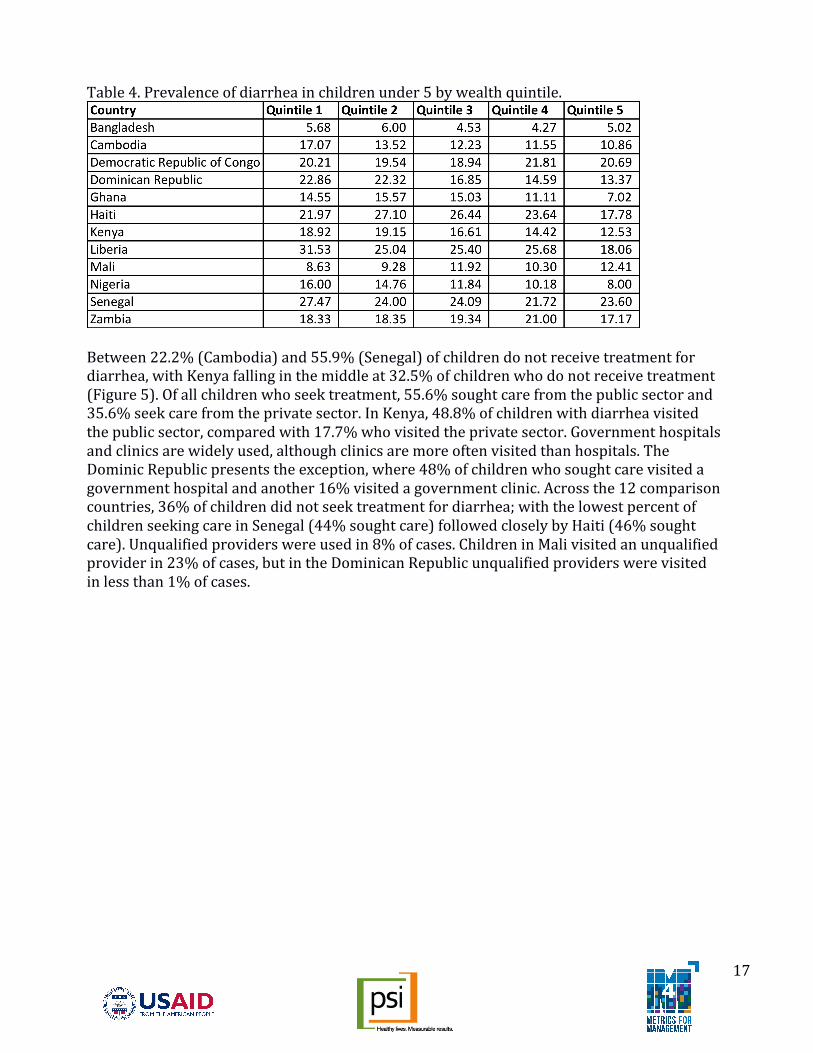
Focusingonthe12comparisoncountries,wefindthatprevalenceofdiarrheaintheprevioustwoweeksvariesfrom5.1%inBangladeshto26.8%inLiberia(seeTable4).Acrossthecomparisoncountries,overhalfofallcasesofdiarrheaoccurredinthelowesttwoquintilesversusjustoverone-quarterofcasesinthehighesttwowealthquintiles,andtwo-thirdsofcasesoccurredinrurallocations(datanotshown).
17
Table4.Prevalenceofdiarrheainchildrenunder5bywealthquintile.
Between22.2%(Cambodia)and55.9%(Senegal)ofchildrendonotreceivetreatmentfordiarrhea,withKenyafallinginthemiddleat32.5%ofchildrenwhodonotreceivetreatment(Figure5).Ofallchildrenwhoseektreatment,55.6%soughtcarefromthepublicsectorand35.6%seekcarefromtheprivatesector.InKenya,48.8%ofchildrenwithdiarrheavisitedthepublicsector,comparedwith17.7%whovisitedtheprivatesector.Governmenthospitalsandclinicsarewidelyused,althoughclinicsaremoreoftenvisitedthanhospitals.TheDominicRepublicpresentstheexception,where48%ofchildrenwhosoughtcarevisitedagovernmenthospitalandanother16%visitedagovernmentclinic.Acrossthe12comparisoncountries,36%ofchildrendidnotseektreatmentfordiarrhea;withthelowestpercentofchildrenseekingcareinSenegal(44%soughtcare)followedcloselybyHaiti(46%soughtcare).Unqualifiedproviderswereusedin8%ofcases.ChildreninMalivisitedanunqualifiedproviderin23%ofcases,butintheDominicanRepublicunqualifiedproviderswerevisitedinlessthan1%ofcases.

18
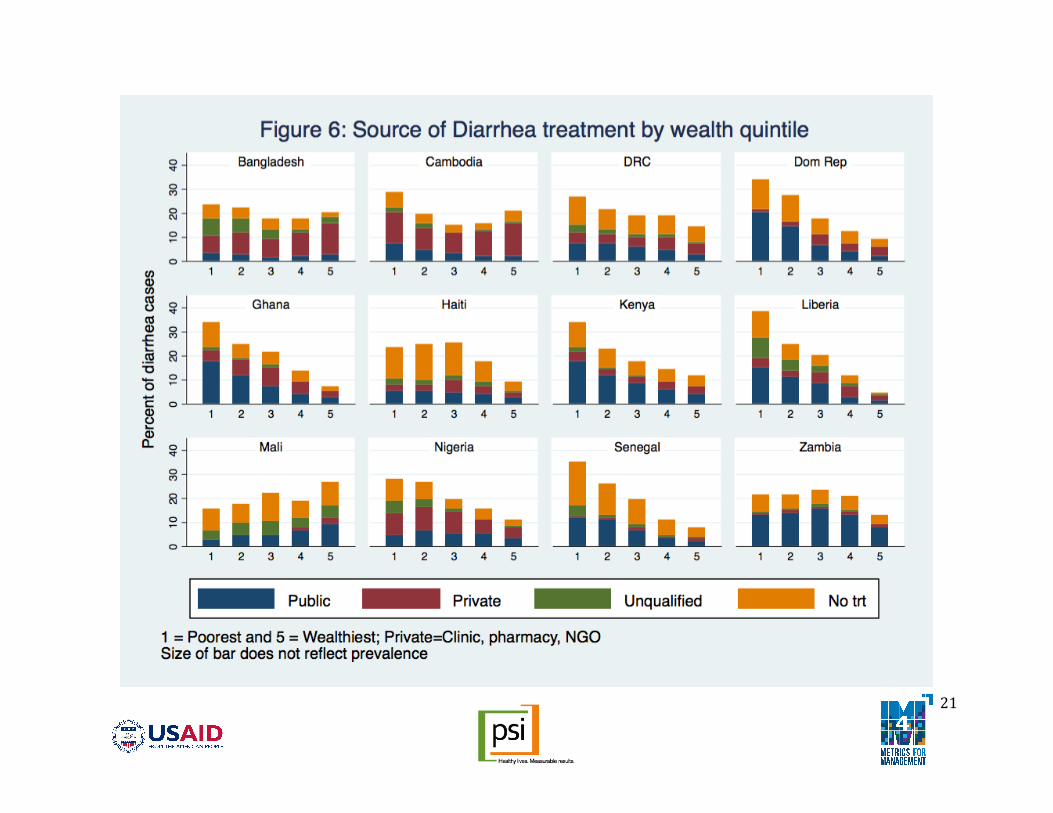
Lookingatdifferencesbywealth,thereissignificantvariationacrosscountries.ThelowestwealthquintileinKenyawasmorelikelytousepublicservicesthanprivate(57%versus10%,respectively),with29%ofchildrenwhodidnotseektreatment(seefigure6).Thehighestwealthquintilewasalsomorelikelytousepublicservices,butthedifferencewassmaller(35%usedpublicservices,26%private),with39%ofchildrenwhodidnotseektreatment.InCambodia,wherenearly80%ofchildrenacrossallwealthquintilesseektreatmentfordiarrhea,thistrendforuseofpublicorprivateservicesisreversed.Allwealthquintilesweremorelikelytouseprivateratherthanpublicservices(56%versus22%,respectively),althoughthehighestwealthquintileismorelikelytouseprivateservices(65%)thanthelowestwealthquintile(51%).InSenegal,56%ofchildrendidnotseekcarefordiarrhea,andboththelowestandhighestwealthquintilesusedpublicservicesinaboutone-thirdofcases,whileonly2%ofcasesinthelowestwealthquintilesvisitedaprivateprovidercomparedto12%inthehighestwealthquintile.
21

22
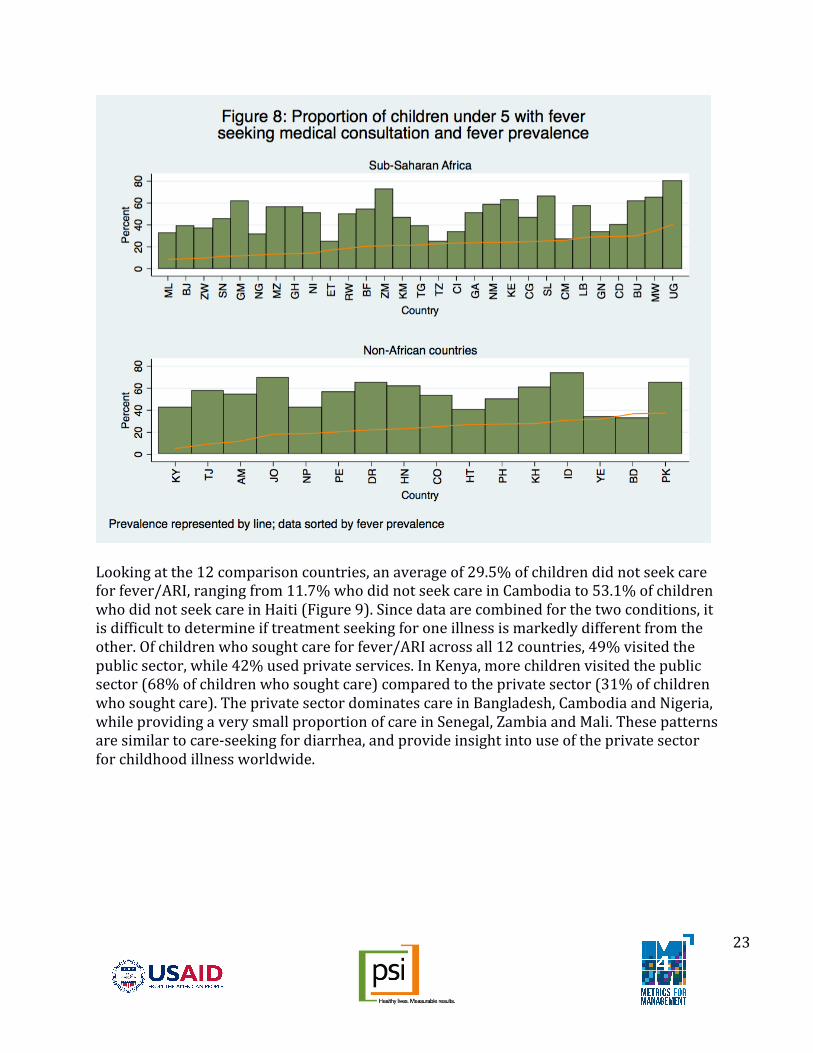
Fever/ARIForbothARIandfever,thereisnoclearrelationshipbetweenprevalenceoftheconditionandtreatmentseekingbehavior.OverallprevalenceofARIissignificantlylowerthanfeverinallcountriesforwhichdataisshowninfigures7and8.Uganda(UG)andZambia(ZM)displayaconsistentlyhighuseoftreatmentseekingforallthreechildhoodillnesses,whileEthiopia(ET)andCameroon(CM)havelowlevelsoftreatmentseeking.OutsideofAfrica,thedifferencesbetweenYemenandPakistanforARItreatmentseeking,orYemen,BangladeshandPakistanforfevercases,isparticularlystriking.Inbothinstances,prevalenceofARIorfeverissimilar,buttheproportionofchildrenforwhomformaltreatmentissoughtisnearlydoubleinPakistanascomparedtoYemenandBangladesh.WhileYemenmayhaveahealthfacilityshortage,thesameexplanationcannotbeconsideredforBangladesh,andfurthercontextualfactorswouldneedtobeexplored.
23
Lookingatthe12comparisoncountries,anaverageof29.5%ofchildrendidnotseekcareforfever/ARI,rangingfrom11.7%whodidnotseekcareinCambodiato53.1%ofchildrenwhodidnotseekcareinHaiti(Figure9).Sincedataarecombinedforthetwoconditions,itisdifficulttodetermineiftreatmentseekingforoneillnessismarkedlydifferentfromtheother.Ofchildrenwhosoughtcareforfever/ARIacrossall12countries,49%visitedthepublicsector,while42%usedprivateservices.InKenya,morechildrenvisitedthepublicsector(68%ofchildrenwhosoughtcare)comparedtotheprivatesector(31%ofchildrenwhosoughtcare).TheprivatesectordominatescareinBangladesh,CambodiaandNigeria,whileprovidingaverysmallproportionofcareinSenegal,ZambiaandMali.Thesepatternsaresimilartocare-seekingfordiarrhea,andprovideinsightintouseoftheprivatesectorforchildhoodillnessworldwide.

24
Differencesinillnessprevalenceandcare-seekingbywealthisalsoaconsideration.NearlyhalfofallfeverorARIcasesoccurinthelowesttwowealthquintiles,withlessthanone-thirdofcasesoccurringinthehighesttwowealthquintiles.Forexample,inKenya,53%offever/ARIcasesoccurinthelowesttwowealthquintilesand29%inthehighesttwowealthquintiles(table5).Theproportionofchildrenwhoreceivenotreatmentforfever/ARIisstronglycorrelatedwithwealthstatusinDRC,Haiti,Liberia,MaliandSenegal.Forexample,45%ofchildrenwithARI/feverinthepoorestquintileinDRCreceivednotreatment,ascomparedto31%intherichestquintile.Useofprivatesectorclinicsisalsocorrelatedwithwealth,withonly6%ofsickchildreninthepoorestquintilevisitingaprivateclinicinKenya,HaitiandLiberia,comparedwith25%-37%ofthoseintherichestquintileinthosesamecountries.Useofprivatesectorpharmacies,bycontrast,ismuchmoreequitable,especiallyintheDominicanRepublic,Ghana,KenyaandNigeria.Figure10indicateshowcasesofARIorfeveraredistributedacrosswealthquintiles.OfallcasesofARIorfeverinSenegal,36%arefoundinhouseholdsinthepoorestquintile,while7%areinthewealthiesthouseholds.Alargeproportionofthoseinthepoorestquintilereceivenotreatment,andthosewhodoseektheirtreatmentinthepublicsector.Incontrast,inNigeria,casesofARIarefairlyevenlydistributedacrosswealthquintiles,asisseekingprivatesectorcare.

25
Table5.Prevalenceoffever/ARIinchildrenunder5bywealthquintile.
27
LimitationsofdataItisimportanttonotethefollowinglimitationswhenusingDHSorotherhouseholddata.Alldataisself-report,andinthecaseoffamilyplanningservices,therecalltimemaybequitelong.Womenmaymis-specifythesourceofcareforthemselvesortheirchildren.Second,forchildhoodillnessepisodes,researchindicatesthatcaremaybesoughtatmorethanonelocation,andthatthereasonforseekingcareatmultiplelocationsisimportant(24).TheDHSdoesnotcapturetheorderofcare-seeking,northereasonforseekingcareataparticularsite.Nevertheless,datashownindicatesthattheprivatesectorcanbeanimportantsourceofcareforbothfamilyplanningandIMCIservices.Inparticular,childrenwhodonotreceivetreatmentfromaqualifiedprovider,likewomenwithanunmetneedforfamilyplanning,canbeconsideredintherealmofpotentialdemand.Additionalinformationontheseverityofillnessmayberequiredtounderstandifallcaseswheretreatmentwasnotsoughtareinneedofmedicaladvice.
SummaryAreviewoftheliteratureregardinguseofhealthservicesbysectorandwealthrevealsthatservicesmustbelookedatseparately.Althoughacountrymaybelabeledashavingastrongprivatesector,reflectiveofthenumberofqualifiedprivatesectorprovidersavailableandthedispersionofthefacilitiesbeyondurbancenters,thisdoesnotimmediatelycorrelatetohigherprivatesectoruseforallhealthneeds.ThisreviewandanalysislookedfirstatthepublishedliteratureondifferencesinuseofpublicversusprivatesectorcareinLMIC.Thesedifferencesmaybeattributedtowealth,geographiclocation,orhealthservicesought.Thereissubstantialvariationincareseekingthroughtheprivatesectoracrosscountries(7,15,24).Forthetreatmentofchildhoodillnesses,weoftenseehigheruseoftheprivatesectorinAsiathaninAfrica.Similarly,forfamilyplanningservices,publicclinicsarehighlyfavoredinAfricancountries.Nevertheless,MalireliesheavilyoncommunityhealthworkersandNigeriahashighutilizationofprivatepharmacies.DespitetherelativelysimilaraggregateresultsfoundbyCampbelletal,sourceofcareforfamilyplanningvariessignificantlyacrosscountrieswhenlookingindepth(15).Governmentfacilitiesareusedbylessthan20%ofwomeninBangladesh,andmorethan80%ofwomeninSenegalandZambia.InBangladeshandCambodia,privateclinicsprovideover40%ofFPservices,andmorethan50%ofservicesinNigeriaarereportedasprovidedthroughprivatepharmacies.NGOservicesaccountforalimitedamountoffamilyplanningservicedeliveryacrossthesixtypesofcaresourcesprovidinglessthan4%ofcareinmostcountries,withtheexceptionofnearly20%ofruralcareinHaiti.NGOsgenerallyprovidedsmallpercentage(lessthan15%inallcountries)ofshort-termfamily
28
planningmethodsor,inBangladesh,DemocraticRepublicofCongo,Haiti,andKenya,asmallpercentage(lessthan4%)ofLARCs(seeannex).SomeofthelowreporteduseofNGOsasasourceofcarelikelyhastodowithalimitationofself-reporteddata.Womenmaynotknowhowtoclassifythefacilitytheyvisit,andfacilitiessuchaswhollyownedMarieStopesInternational(MSI)clinicsmaynotbeconsideredan“NGOfacility”byaclient.Whenconsideringhowtheresultsfromthisreviewcanbeappliedtosocialfranchises,itisimportanttoconsiderhowfranchisesare‘classified’bythetargetpopulation,versushowtheymaybeclassifiedinhealthfacilitysurveys(16).Althoughsignificantliteratureonthissubjectdoesnotexist,itisconceivablethatafranchisedprovidermayself-identifyasamemberofalargerNGOentity,orthatvisiblebrandingmayleadthefranchisetobeclassifiedassuch.Futureresearchshouldunderstandhowclientsofdifferenthealthserviceprovidersclassifythem,andifthisaffectsconclusionsdrawnfromsectorbasedanalysesofDHSdata.Whiletheideaofunmetneedforfamilyplanningiswellestablishedandstudied,thesameconceptdoesnothaveasmuchtractionforchildhoodillness.Yet,acrossthe12comparisoncountries,morethanone-thirdofallchildrendidnotreceivetreatmentfordiarrhea.Over50%ofchildreninHaitiandMalireceivenotreatment,ortreatmentfromanunqualifiedsource,forfever/ARI.Investigatingcare-seekingpatternsanduseoftheprivatesectorbysocio-economicstatusprovidesinsightintowhethertheprivatesectorisaviablesourceofcareforthosenotcurrentlyseekingtreatment.Inmostcountries,prevalenceofdiarrhea,ARIandfeverisgreaterinpoorerwealthquintiles,orinruralareas.Yetneedinurbanareas,wheremoreprivatesectorprovidersarelocated,persists.Between16%(Bangladesh)and58%(Senegal)ofchildrenwithdiarrheainurbanareasreceivednotreatmentinouranalysis(datanotshown).Interestingly,parentsappeartochoosetheprivatesectormoreforARI/Feverthanfordiarrhea.Forexample,inCambodia,DRC,DominicanRepublic,Ghana,Haiti,Kenya,MaliandNigeria,useofbothprivateclinicsandpharmaciesisgreaterinurbanareasforARI/feverthanfordiarrhea.Reasonswouldhavetobeexplored,butpresentopportunityforincreasinguseofthesamefacilitiesfordiarrheatreatment,aswellasamongthoseseekingnotreatment.Incomparingpatternsofusebyquintileandsector,thereareclearsimilaritiesbetweentreatmentseekingfordiarrheaandARI/feverbycountry(figures6and10,orfigures4,7and8).Bangladesh,CambodiaandNigeriahaverelativelyhighuseoftheprivatesectoracrossallquintiles,aswellaslimiteddifferentiationinthenumberofcasesbyquintile.HigherratesofnotreatmentinSenegalandHaitiareconsistentforbothdiarrheaandARI.AcrossallLMICwithdataavailable,countrieswithhigherproportionsofcareseekingaresimilarforfever,ARIanddiarrhea.Agreaterunderstandingofwhyhouseholdsinsomecountriesseekmedicaladviceatamuchhigherratethanothers,evenamongregional

29
neighbors,wouldimprovecare-seekinginsight.Forexample,care-seekingforsickZambianchildrenisconsistentlyhigherthanforTanzanianones,fordiarrhea,ARIandfever.Finally,therewaslittlecorrelationbetweenuseoftheprivatesectorforchildhoodillness,anduseoftheprivatesectorforfamilyplanninginthesamehousehold(betweenawomanandherchild).Thisispartlybecausethepopulationdoesnotoverlapwell–alargepercentageoffamilyplanningusersdidnothaveasickchildintheprecedingtwoweeks.Nevertheless,patternsofuseoftheprivatesectorarenotalwayssimilaracrosswealthquintilesforfamilyplanningversusARIordiarrhea(figure3,6and10).Forexample,womeninHaitiandtheDominicanRepublicusetheprivatesectoracrossallquintilesforFP,butnotforARI.InBangladeshandCambodia,thepublicsectorisrarelyusedforchildhoodillnesstreatment,butprovidesabouthalfofservicesforFP.Understandingtheiruseofcaremorebroadlyspeakingwouldprovidegreaterinsightintohouseholdchoices.AsDavidsonGwatkinwroteina2006reviewofIMCI,“aninterventioncannothelpthepoorunlessitgetstothem”(1).WeseefromthesecondaryanalysisofDHSdatathattherearecleardifferencesinwhereindividualsfromdifferentwealthquintilesseekfamilyplanningservicesandcareforchildrenwithdiarrhea,fever,andARI.Insomecountries,thepublicsectorisfavoredfortreatmentforchildren,whileinothers,theprivatesectorholdsalargeadvantage.Thesamecountrieswhichfavorthepublicsectorforchildhoodillnessdonotnecessarilyfavoritforfamilyplanningservices.Thereisalsonotaclearrelationshipbetweenuseofservicesinonesector,anddesirableoutcomes.Forexample,greateruseofservicesinonesector(publicorprivate)doesnotcorrelatewithhighercontraceptiveprevalenceratesincountries.Consequently,generalizationscannotbemadeacrosscountrieswithregardtouseofprivatesectorservices.Rather,countryandhealthareaspecificinformationiswarranted.Inexaminingthecontributionofsocialfranchises,additionalinformationisrequired.NoneoftheDHSdataisabletodisaggregateresultstodemonstratethecontributionsocialfranchisesmaketoprovidingcriticalservices.Countrylevelassessmentsofcareseekingbysectorandwealth,furtheranalysisofwhythesamehouseholdmakesdifferentchoicesincare-seeking,andcomparingthewealthprofileoffranchisedclientswithotherswillfurtherourunderstandingoftheroleoffranchisesinprivatesectorhealthcare,andcountryhealthsystemsmoregenerally.

30
References1. MontaguD,AnglemyerA,TiwariM,DrasserK,RutherfordG,HorvathT,etal.Private
versuspublicstrategiesforhealthserviceprovisionforimprovinghealthoutcomesinresource-limitedsettings.2011Aug9;1–80.
2. GwatkinDR,BhuiyaA,VictoraCG.Makinghealthsystemsmoreequitable.TheLancet.Elsevier;2004Oct2;364(9441):1273–80.
3. ShahN,WangW,BishaiDM.ComparingprivatesectorfamilyplanningservicestogovernmentandNGOservicesinEthiopiaandPakistan:howdosocialfranchisescompareacrossquality,equityandcost?HealthPolicyandPlanning.2011Jul5;26(Suppl.1):i63–i71.
4. BeyelerN,YorkDeLaCruzA,MontaguD.TheImpactofClinicalSocialFranchisingonHealthServicesinLow-andMiddle-IncomeCountries:ASystematicReview.PLoSONE.PublicLibraryofScience;2013Apr23;8(4):e60669.
5. PatouillardE,GoodmanCA,HansonKG,MillsAJ.Canworkingwiththeprivatefor-profitsectorimproveutilizationofqualityhealthservicesbythepoor?Asystematicreviewoftheliterature.IntJEquityHealth.BioMedCentral;2007;6(1):17.
6. GrepinK.WhatistheroleoftheprivatesectorinachieveingUniversalHealthCoverage?Estimatesoftrendsandlevelsfrom205DemographicandHealthSurveys(1990-2013).
7. MontaguD,ViscontiA.ImportanceoftheprivatesectorforoutpatienthealthcareinLMICs.Toronto,Canada;2011.
8. MakinenM,WatersH,RauchM,AlmagambetovaN,BitranR,GilsonL,etal.Inequalitiesinhealthcareuseandexpenditures:empiricaldatafromeightdevelopingcountriesandcountriesintransition.BullWorldHealthOrgan.WorldHealthOrganization;2000;78(1):55–65.
9. VanDoorslaerE.Inequalitiesinaccesstomedicalcarebyincomeindevelopedcountries.CanadianMedicalAssociationJournal.2006Jan17;174(2):177–83.
10. RegidorE,MartínezD,CalleME,AstasioP,OrtegaP,DomínguezV.Socioeconomicpatternsintheuseofpublicandprivatehealthservicesandequityinhealthcare.BMCHealthServRes.2008;8(1):183–9.
11. LiuX,HotchkissDR,BoseS.Theeffectivenessofcontracting-outprimaryhealthcareservicesindevelopingcountries:areviewoftheevidence.HealthPolicyandPlanning.2008Jan;23(1):1–13.

31
12. HotchkissDR,GodhaD,DoM.Effectofanexpansioninprivatesectorprovisionofcontraceptivesuppliesonhorizontalinequityinmoderncontraceptiveuse:evidencefromAfricaandAsia.IntJEquityHealth.2011;10:33.
13. LönnrothK,AungT,MaungW,KlugeH,UplekarM.SocialfranchisingofTBcarethroughprivateGPsinMyanmar:anassessmentoftreatmentresults,access,equityandfinancialprotection.HealthPolicyandPlanning.2007May1;22(3):156–66.
14. MontaguD,SudhinarasetM,LwinT,OnozakiI,WinZ,AungT.EquityandtheSunQualityHealthPrivateProviderSocialFranchise:comparativeanalysisofpatientsurveydataandanationallyrepresentativeTBprevalencesurvey.IntJEquityHealth.BioMedCentral;2013;12:5–5.
15. CampbellOMR,BenovaL,MacleodD,GoodmanC,FootmanK,PereiraAL,etal.Who,What,Where:ananalysisofprivatesectorfamilyplanningprovisionin57low-andmiddle-incomecountries.TropMedIntHealth.2015Dec;20(12):1639–56.
16. FootmanK,BenovaL,GoodmanC,MacleodD,LynchCA,Penn-KekanaL,etal.Usingmulti-countryhouseholdsurveystounderstandwhoprovidesreproductiveandmaternalhealthservicesinlow-andmiddle-incomecountries:acriticalappraisaloftheDemographicandHealthSurveys.TropMedIntHealth.2015Mar5;20(5):589–606.
17. HutchinsonPL,DoM,AghaS.Measuringclientsatisfactionandthequalityoffamilyplanningservices:acomparativeanalysisofpublicandprivatehealthfacilitiesinTanzania,KenyaandGhana.BMCHealthServRes.2011;11:203.
18. AghaS,DoM.ThequalityoffamilyplanningservicesandclientsatisfactioninthepublicandprivatesectorsinKenya.IntJQualHealthCare.TheOxfordUniversityPress;2009Apr;21(2):87–96.
19. BhatiaJ,ClelandJ.Healthcareoffemaleoutpatientsinsouth-centralIndia:comparingpublicandprivatesectorprovision.HealthPolicyandPlanning.OxfordUniversityPress;2004Nov1;19(6):402–9.
20. WinfreyW,LacayoY.NicaraguaFamilyPlanningMarketSegmentationAnalysis[Internet].Seattle:PATH;2013.Availablefrom:https://www.path.org/publications/files/RH_nica_fp_segment_rpt.pdf
21. SharmaS,GribbleJN,MenottiEP.CreatingoptionsinfamilyplanningfortheprivatesectorinLatinAmerica.RevPanamSaludPublica.2005Jul;18(1):37–44.
22. SreeramareddyCT,SathyanarayanaTN,KumarHNH.UtilizationofHealthCareServicesforChildhoodMorbidityandAssociatedFactorsinIndia:ANationalCross-SectionalHouseholdSurvey.PLoSONE.SanFrancisco,USA:PublicLibraryofScience;2012;7(12):e51904.

32
23. FilmerD.Feveranditstreatmentamongthemoreandlesspoorinsub-SaharanAfrica.HealthPolicyandPlanning.OxfordUniversityPress;2005Nov;20(6):337–46.
24. LimwattananonS.Private-PublicMixinWomanandChildHealthinLow-IncomeCountries:AnAnalysisofDemographicandHealthSurveys[Internet].1sted.ResultsforDevelopmentInstituteandtheRockefellerFoundation;2008Oct.Availablefrom:http://resultsfordevelopment.org/sites/resultsfordevelopment.org/files/resources/Private-public%20mix%20in%20woman%20and%20child%20health%20in%20low-income%20countries.pdf
25. BerendesS,HeywoodP,OliverS,GarnerP.Qualityofprivateandpublicambulatoryhealthcareinlowandmiddleincomecountries:systematicreviewofcomparativestudies.JenkinsR,editor.PLoSMed[Internet].2011Apr;8(4):e1000433.Availablefrom:http://dx.plos.org/10.1371/journal.pmed.1000433
26. BustreoF,HardingA,AxelssonH.Candevelopingcountriesachieveadequateimprovementsinchildhealthoutcomeswithoutengagingtheprivatesector?BullWorldHealthOrgan.WorldHealthOrganization;2003;81(12):886–95.
27. MuhuriPK,AnkerM,BryceJ.Treatmentpatternsforchildhooddiarrhoea:evidencefromdemographicandhealthsurveys.BullWorldHealthOrgan.WorldHealthOrganization;1996;74(2):135–46.

33
AnnexAdditionaldataforfamilyplanningisshownhere.Familyplanningdataismorerich,allowingforalargernumberofsub-analyseswhicharerelevantforsocialfranchises.Thefirstgraphusesthesamedataseeninfigure1,butarrangedinadifferentway.Countriesaresortedbyincomestatusanduseoftheprivatesector,toseeifthereisanyrelationshipbetweenacountry’sincomelevel,privatesectoruseofFPandcontraceptiveprevalence.MiddleincomecountriestendtohaveahigherCPRthanlow-incomecountries,butthereisnoapparentrelationshipbetweenincomestatusanduseoftheprivatesectorforFP,orbetweenCPRanduseoftheprivatesector.

34
Thenexttwographslookatthe12countriesindepthtoseeiftherearedifferencesinsectorsusedforFPbyregion(urbanversusrural)andbymethod.Inmanycountries,privateclinicsandpharmaciesareusedmoreinurbanareas.
Finally,thepublicsectorprovidesthemajorityofpermanentmethodsinall12countries,andprivatepharmaciesareamoreimportantsourceofshorttermmethodsinDRCandNigeriathanothercountries.ThehighreporteduseofCHWsinMaliandBangladeshmay

35
requirefurtherinvestigation,especiallysincetheyarereportedtoprovideLARCsandpermanentmethods.
View publication statsView publication stats