the next generation: new genes and panels at pgxl kristen k. reynolds, phd vp laboratory operations...
TRANSCRIPT
The Next Generation: New Genes and Panels at
PGXL
Kristen K. Reynolds, PhDVP Laboratory Operations
Copyright 2012 PGXL Laboratories, Louisville KYAll materials herein are the exclusive property of PGXL Laboratories

2012 Q4 New GenesCYP3A4/3A5: Statins, benzodiazepines, Ca++ channel blockers
CYP1A2: Antidepressants, antipsychotics
SLCO1B1: Statin-induced myopathy risk
SLC6A4 (Serotonin transporter): SSRI antidepressant sensitivity/resistance
SULT4A1: Olanzapine
OPRM1: Opioid sensitivity/resistance (expected December 2012)

CYP3A4 and CYP3A5

CYP3A4 and 3A5
• Together metabolize 50% of all medications• 80% redundancy of function• Genetic variants in each
– decrease enzyme function (clearance)– Increased risk of dose-dependent adverse events

CYP3A4/5 master drug
list
CYP3A4/CYP3A5 Substrates PSYCHIATRY OTHER Benzodiazepines Antimicrobials/antivirals Alprazolam Xanax Clarithromycin Biaxin Midazolam Versed Erythromycin E-Mycin Triazolam Halcion Telithromycin Ketek Antipsychotics Indinavir Crixivan Quetiapine Seroquel Nelfinavir Viracept Ziprasidone Geodon Ritonavir Norvir Buspirone Buspar Saquinavir Fortovase Lurasidone Latuda Carbamazepine Various brands Steroids Antidepressants Estradiol Various brands Desvenlafaxine Pristiq Hydrocortisone Various brands Vilazodone Viibryd Progesterone Various brands Trazadone Desyrel Testosterone Various brands Nefazadone Serzone Reboxetine Edronax Chemotherapeutics Nortriptyline Pamelor, Aventyl Vincristine Oncovin Docetaxel Taxotere CARDIOLOGY Quinidine Various brands Pain Management Ticareglor Brilinta Cyclobenzaprine Flexaril Rivaroxaban Xarelto Fentanyl Actiq, Duragesic Statins Alfentanil Alfenta Atorvastatin Lipitor Lovastatin Mevacor, Advicor Immunosuppressants Mevastatin Compactin Cyclosporine Gengraf Simvastatin Zocor, Vytorin, Caduet, Simcor Tacrolimus Prograf Ca Channel Blockers Amlodipine Norvasc Diltiazem Cardizem Felodipine Plendil Lercanidipine Zanidip Nifedipine Adalat Nisoldipine Sular Nitrendipine Various brands Verapamil Various brands

CYP3A4/5 significant variants
• CYP3A4*22– Decreased dose requirements for tacrolimus,
cyclosporin, simvastatin, atorvastatin, lovastatin, midazolam
– 4-8% frequency
• CYP3A5*3– Decreased dose requirements vincristine, tacrolimus,
cyclosporin– 90% freq Cauc, 50% AA, 60% Asians

3A4 InterpretationCYP3A4 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Extensive Metabolizer
Normal metabolic clearance expected. Common CYP3A4 medications below.
CYP3A4 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Partially Decreased Metabolizer
Decreased metabolic clearance expected with increased risk of dose-dependent side effects. Common CYP3A4 medications below.
CYP3A4 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Decreased Metabolizer
Decreased metabolic clearance expected with increased risk of dose-dependent side effects. Common CYP3A4 medications below.
CYP3A4 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
*22 Decreased Metabolizer
Decreased metabolic clearance expected with increased risk of dose-dependent side effects.
Adjust Dosage Adjustment
Simvastatinmax 10-20 mg, or consider alternative statin if also SLCO1B1 *5/*5 genotype
Atorvastatin max 10-20 mgLovastatin max 10-20 mgTacrolimus decrease by up to 40%

3A5 InterpretationCYP3A5 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Extensive Metabolizer
Genotype consistent with the highest baseline enzymatic activity for CYP3A5. Patients with this genotype represent only 1% of the population. Maintenance dosages for most CYP3A5 drugs may be at the higher end of the typical dose range. Common CYP3A5 medications below.
CYP3A5 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Partially Decreased Metabolizer
Genotype consistent with intermediate CYP3A5 enzymatic activity and represents approximately 20% of the population. For PDMs, maintenance dosages for most CYP3A5 drugs are lower than extensive metabolizers and are higher than decreased metabolizers.
CYP3A5 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Decreased Metabolizer
Genotype consistent with reduced CYP3A5 enzymatic activity and represents the majority (60-80%) of the population. For DMs, maintenance dosages for most CYP3A drugs are lower than extensive metabolizers. Common CYP3A5 medications below.

SLCO1B1statin myopathy risk
• Statin therapy reduces risk of CV events• Statin therapy can lead to muscle weakness
and ultimately muscle breakdown with rhabdomyolysis
• GWAS studies revealed a single genetic determinant of statin induced myopathy

N Engl J Med 2008;359:789-99.

• ~35% of population are carriers of the SLC01B1*5 allele– Myalgia/muscle cramps
• Myopathy on 40mg/day: – SLCO1B1 *1/*5, OR = 2.6– SLCO1B1 *5/*5, OR = 5.2
• Most frequently associated with simvastatin > atorvastatin > pravastatin
SLC01B1 OATP1B1
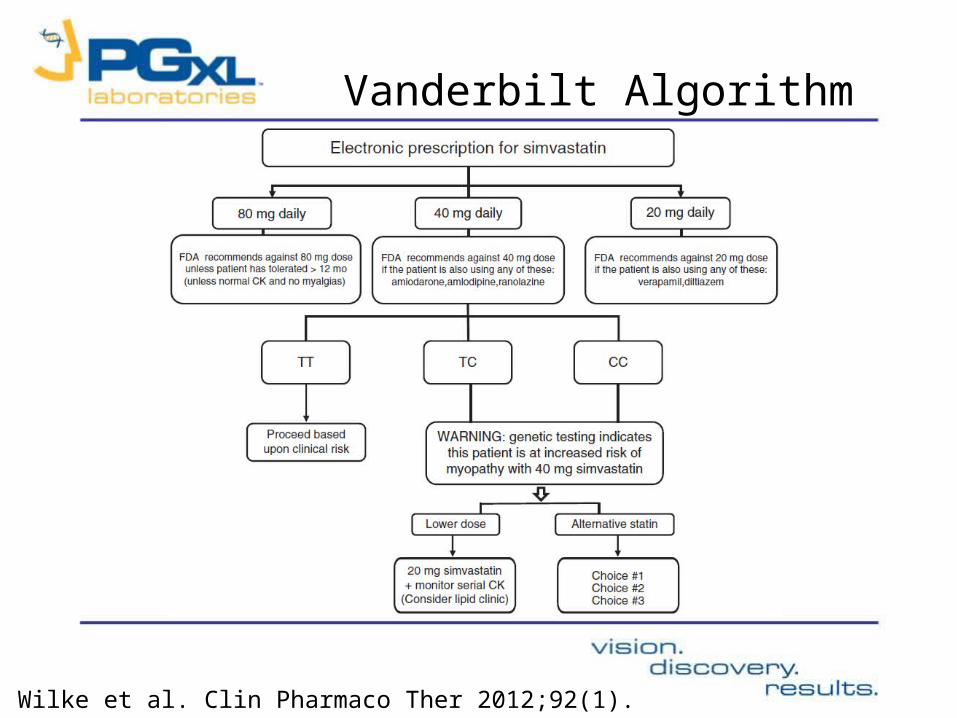
Vanderbilt Algorithm
Wilke et al. Clin Pharmaco Ther 2012;92(1).

SLCO1B1 InterpretationSLCO1B1 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
No Increased Risk
Normal OATP1B1 transporter function. No increased risk of statin-induced myopathy expected at low to moderate doses (10-40 mg). Consider 10-20 mg dose if also CYP3A4*22 carrier.
SLCO1B1 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
2.6 Fold Increased Myopathy Risk
Reduced OATP1B1 transporter function. Increased risk of statin-induced myopathy.
Adjust Dosage Adjustment
Simvastatin
max 10-20 mg and consider monitoring CK levels, or consider alternative statin if also taking verapamil or diltiazem. Consider low 10-20 mg dose of alternative statin if patient also CYP3A4*22 carrier.
Atorvastatin max 10-20 mg
SLCO1B1 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
>5 Fold Increased Myopathy Risk
Avoid Alternative Consideration Adjust Dosage Adjustment
Simvastatinpravastatin, lovastatin, fluvastatin, rosuvastatin, mevastatin
Atorvastatin max 10-20 mg

SLC6A4serotonin transporter

SLC6A4 Serotonin Transporter

SLC6A4
• 50-60% depressed patients have recurrence and 20% fail 1st line Rx (SSRIs)– TRD increased # of Rx, hospitalization risk, costs (19x higher)
• 75% people carry S or LG
• S/S, S/LG, or LG/LG should be considered for non-SSRI therapies

AntidepressantsSSRIs SNRIs
2C19 citalopram Celexa 2D6,1A2 duloxetine Cymbalta2C19 escitalopram Lexapro 2D6 venlafaxine Effexor2D6 fluoxetine Prozac 3A4/5 desvenlafaxine Pristiq2D6,1A2 fluvoxamine Luvox renal milnacipran Savella2D6 paroxetine Paxil 2D6,1A2,3A4/5 mirtazapine Remeron2C19 sertraline Zoloft3A4/5 vilazodone Viibryd
TCAs2D6,1A2,3A4/5 amitriptyline Elavil Atypicals (NRIs, NDRIs)2D6,1A2 clomipramine Anafranil 2B6,1A2 bupropion Wellbutrin2D6,2C19 desipramine Norpramin 3A4/5 trazadone Desyrel2D6 doxepin Sinequan 3A4/5 nefazadone Serzone2D6 imipramine Tofranil 2D6 maprotiline Ludiomil2D6,3A4/5 nortriptyline Pamelor, Aventyl 2D6,1A2 mianserin2D6,3A4/5,2C19 trimipramine Surmontil 3A4/5 reboxetine Edronax
MAOIsphenelzine Nardiltranylcyromine Parnateisocarboxazid Marplan
2C19 moclobemide
Black indicates major pathway; Gray indicates minor pathway
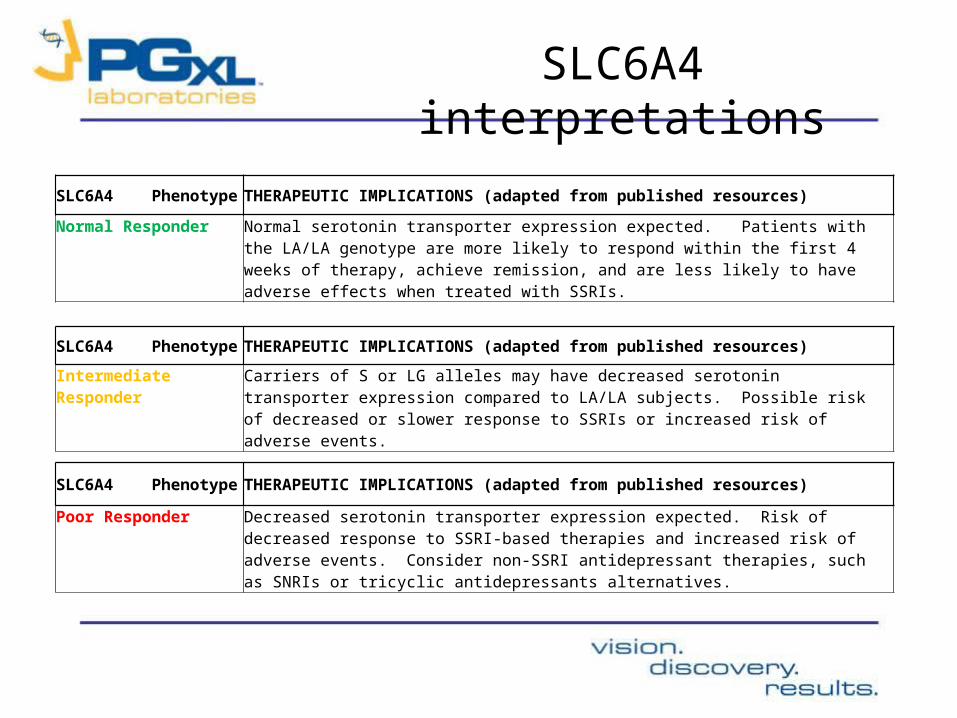
SLC6A4 interpretations
SLC6A4 Phenotype THERAPEUTIC IMPLICATIONS (adapted from published resources)
Normal ResponderNormal serotonin transporter expression expected. Patients with the LA/LA genotype are more likely to respond within the first 4 weeks of therapy, achieve remission, and are less likely to have adverse effects when treated with SSRIs.
SLC6A4 Phenotype THERAPEUTIC IMPLICATIONS (adapted from published resources)
Intermediate ResponderCarriers of S or LG alleles may have decreased serotonin transporter expression compared to LA/LA subjects. Possible risk of decreased or slower response to SSRIs or increased risk of adverse events.
SLC6A4 Phenotype THERAPEUTIC IMPLICATIONS (adapted from published resources)
Poor ResponderDecreased serotonin transporter expression expected. Risk of decreased response to SSRI-based therapies and increased risk of adverse events. Consider non-SSRI antidepressant therapies, such as SNRIs or tricyclic antidepressants alternatives.

CYP1A2

CYP1A2
• Metabolizes many antidepressants and antipsychotics
• Inducible by several medications and smoking• Variants cause altered enzymatic activity, particularly
in the presence of an inducer• Increased risk of having adverse drug reactions or
therapeutic failure to standard dosages of CYP1A2 medications

CYP1A2 master drug listCYP1A2
Other Psychiatry
Ropivicaine Various brands Olanzapine Zyprexa
Lidocaine Various brands Clozapine Clozaril
Theophylline Aerolate Imipramine Tofranil
Zolmipitran Zomig Clomipramine Anafranil
Triamterene Dyrenium Mirtazapine Remeron
Flutamide Eulexin Bupropion Wellbutrin
Tizanidine Zanaflex Duloxetine Cymbalta
Tacrine Cognex Promazine Sparine
Cyclobenzaprine Flexaril Asenapine Saphris
Caffeine
17-beta estradiol

1A2 InterpretationCYP1A2 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Normal Inducer Normal metabolic clearance expected. Common CYP1A2 medications below.
This patient’s genotype is consistent with normal CYP1A2 enzymatic activity and normal induction in the presence of an inducer, such as tobacco smoke. CYP1A2*1A/*1A patients with inducers have 30% lower plasma concentrations of CYP1A2 substrates such as olanzapine.CYP1A2*1A*1A patients without inducers have a 30% increased plasma concentration over those who have inducers present.
CYP1A2 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Hyperinducer Rapid metabolism expected, especially in smokers. Consider dose increases for medications inactivated by CYP1A2 particularly in smokers, or alternative medications not metabolized by CYP1A2. Common CYP1A2 medications below.
CYP1A2 Hyperinducer: Presence of the CYP1A2*1F allele results in the hyperinduction phenotype. Hyperinduction may yield 20-40% higher CYP1A2 activity compared to the normal *1A allele in the presence of an inducer, such as tobacco smoke. Patients who are homozygous for the CYP1A2*1F/*1F genotype may exhibit even higher rates of CYP1A2 enzymatic activity and have been described as ultra-rapid metabolizers for olanzapine. As an example, carriers of CY1A2*1F with the hyperinduction phenotype may exhibit as much as 50% lower than expected plasma levels of olanzapine, clozapine, and haloperidol, which could lead to sub-therapeutic response. Hyperinducers may require increased dosages of CYP1A2 substrates due to higher than normal rates of drug metabolism in the presence of an inducer.
CYP1A2 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Non-Inducer Normal metabolic clearance not affected by inducers. Consider dose decreases for medications inactivated by CYP1A2 or alternative medications not metabolized by CYP1A2. Common CYP1A2 medications below.
SULT4A1psychosis

• PGXL exclusive provider of SULT4A1 marker (schizophrenia, bipolar disorder)

SULT4A1• Brain enzyme that interacts with neurochemicals• Efficacy advantage with olanzapine
Efficacy Hospitalization

SULT4A1 Interpretations
Gene THERAPEUTIC IMPLICATIONS (adapted from published resources)
SULT4A1-1POSITIVE
Consider olanzapine. SULT4A1-1 positive patients have been shown to demonstrate enhanced treatment efficacy and reduced hospitalization risk when treated with olanzapine compared to both SULT4A1-1 negative patients treated with olanzapine and SULT4A1-1 positive patients treated with risperidone.
SULT4A1-1NEGATIVE
SULT4A1-1 negative patients treated with olanzapine do not display the expected efficacy advantage compared to other atypical antipsychotics.

How do we implement these new genes?
Panels and specialty-specific focus

Panels*
PGXL Core Panel:
CYP2D6CYP2C9CYP2C19CYP3A4CYP3A5CYP1A2
Thrombophilia Panel:
Factor V LeidenFactor IIMTHFR
Panel Add-Ons (build specialty-specific uses):
VKORC1 (warfarin)SLC6A4 (SSRIs)SLCO1B1 (statins)OPRM1 (opioids)
*All genes always orderable a la carte

Specialty Requisition Forms

General Practice - DRAFT

Cardiology - DRAFT
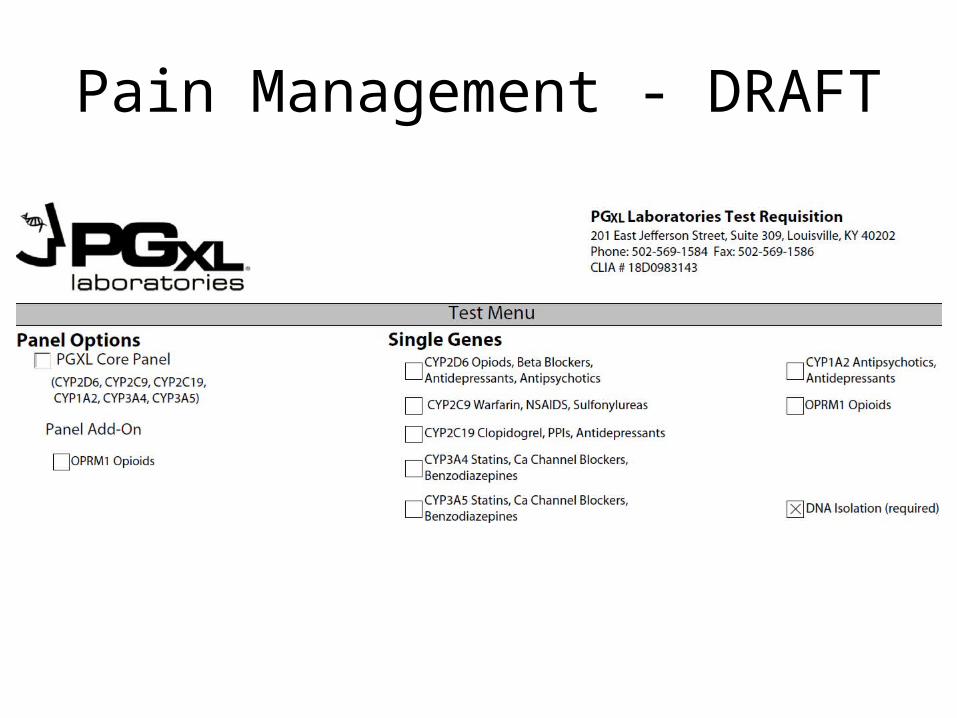
Pain Management - DRAFT

OB/GYN - DRAFT

Psychiatry - DRAFT
Depression
Psychosis

PGXL Depression
PanelDRAFT
(Panel + SLC6A4 add-on)
SLC6A4 S/S SLC6A4 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Poor Responder Decreased serotonin transporter expression expected. Risk of decreased response to SSRI-based therapies and increased risk of adverse events. Consider non-SSRI antidepressant therapies, such as SNRIs or tricyclic antidepressant alternatives.
CONFIDENTIAL COPYRIGHT PGXL LABORATORIES 2012

Is olanzapine likely to have increased efficacy? Yes See SULT4A1
Does consensus data suggest alternatives to risperidone? Yes See CYP2D6
Are SSRIs likely to have decreased efficacy and increased risk of side effects?
Yes See SLC6A4
See below for possible dosage considerations.
SULT4A1 rs763120 CC rs5764010 TT SULT4A1-1 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
POSITIVE Consider olanzapine. SULT4A1-1 positive patients have been shown to demonstrate enhanced treatment efficacy and reduced hospitalization risk when treated with olanzapine compared to both SULT4A1-1 negative patients treated with olanzapine and SULT4A1-1 positive patients treated with risperidone.
CYP2D6 *4/*4 CYP2D6 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Avoid Alternative Consideration Adjust Dosage Adjustment Poor Metabolizer Risperidone† Quetiapine, olanzapine, clozapine Aripiprazole† 10 mg/day maximum Venlafaxine† Citalopram, sertraline Clomipramine† Decrease 50% Amitriptyline† Citalopram, sertraline Doxepin† Decrease 60% Haloperidol† Decrease 50% Imipramine† Decrease 70% Nortriptyline† Decrease 60% Zuclopenthixol† Decrease 50%, or
flupenthixol, quetiapine, olanzapine, clozapine
SLC6A4 S/S SLC6A4 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Poor Responder Decreased serotonin transporter expression expected. Risk of decreased response to SSRI-based therapies and increased risk of adverse events. Consider non-SSRI antidepressant therapies, such as SNRIs or tricyclic antidepressant alternatives.
CYP2C19 *2/*2 CYP2C19 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Poor Metabolizer Decreased metabolic clearance expected. Adjust Dosage Imipramine†
Adjustment Decrease 30%
Sertraline† Decrease 50% CYP1A2 *1F/*1F CYP1A2 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
HYPERINDUCER Rapid metabolism expected, especially in smokers. Consider dose increases for medications inactivated by CYP1A2 particularly in smokers, or alternative medications. Common CYP1A2 medications next page.
*Lack of efficacy due to failure to produce active metabolite; †Increased risk of adverse events due to diminished drug clearance.
STA2R Panel Report

2D6 master drug ListCYP2D6
Pain Management Psychiatry
Codeine** Various brands Antidepressants Antipsychotics
Oxycodone** Oxycontin, various Fluoxetine Prozac Haloperidol Haldol
Hydrocodone** Various brands Fluvoxamine Luvox Risperidone Risperidol
Tramadol** Ultram, various Paroxetine Paxil Aripiprazole Abilify
Venlafaxine Effexor Zuclopenthixol Various brands
Cardiology Duloxetine Cymbalta Perphenazine Trilafon
Carvedilol Coreg Maprotiline Ludiomil Thioridazine Mellaril
Metoprolol Toprol-XL Mirtazapine Remeron Iloperidine Fanapt
Propanolol Inderal, various Amitriptyline Various brands
Chlorpromazine Thorazine
Timolol Blocadren Clomipramine Ananfranil Atomoxetine Strattera
Propafenone Rythmol Desipramine Norpramin Amphetamine Adderall
Flecainide Tambocor Doxepin Sinequan
Imipramine Tofranil
Other Nortriptyline Pamelor, Aventyl
Loratadine Claritin Trimipramine Surmontil
Donepezil Aricept
Dextromethorphan Various brands
Tamoxifen** Various brands
** indicates prodrug

2C19 and 2C9 master drug listsCYP2C19 CYP2C9
Clopidogrel** Plavix Warfarin Coumadin
Citalopram Celexa Celecoxib Celebrex
Escitalopram Lexapro, various Ibuprofen Advil, Motrin
Imipramine Tofranil Naproxen Aleve
Sertraline Zoloft Glyburide Diabeta
Diazepam Valium Glipizide Glucotrol
Omeprazole Prilosec Tolbutamide Orinase
Esomeprazole Nexium Glimepiride Amaryl
Pantoprazole Protonix Phenytoin Dilantin
Rabeprazole Aciphex Fluvastatin Lescol
Lansoprazole Prevacid Rosuvastatin Crestor
Nelfinavir Viracept Losartan Cozaar
Methadone Various brands
Carisoprodol** Soma
Voriconazole Vfend

Cliff Notes on the Portal
SLCO1B1
SLCO1B1 is the gene that makes a liver enzyme called OATP1B1, which helps transport statins medications into the liver more effectively. Roughly 15% of the population possesses the *5 variant, an inherited form of SLOC1B1 which increases risk of statin-induced muscle damage, or myopathy, by 3 to 5 fold. Risk of myopathy with the *5 variant is most closely associated with simvastatin and to a lesser extent, atorvastatin. Patients with the *5 variant may need the lowest doses of simvastatin or an alternative statin to reduce risk of myopathy.
SLC6A4
SLC6A4 is the gene that makes the serotonin transporter in the brain. The role of the serotonin transporter is to shuttle the potent brain chemical serotonin from one neuron to another. Inhibiting serotonin transport is associated with improved mood; thus the effectiveness of many antidepressant drugs (namely selective serotonin reuptake inhibitors, SSRIs) is thought to be due to their inhibition of the serotonin transporter. Nearly 75% of people have an inherited form of the SLC6A4 gene that can lead to decreased response to SSRI therapy. The Short (S) and Long G (LG) forms of the transporter are associated with delayed response to SSRI antidepressants and increased risk of adverse drug reactions (ADRs) during antidepressant therapy. Patients who possess two copies of the S or LG forms may be more likely to benefit from non-SSRI therapies.
CYP3A4
CYP3A4 is a liver enzyme that, in concert with CYP3A5, metabolizes approximately 50% of medications, including many of the statins, benzodiazepines, antibiotics, and antipsychotics. Detecting variants of the CYP3A4 gene that cause altered enzymatic activity can identify patients who may be at increased risk of having adverse drug reactions while taking standard dosages of 3A4 substrates. Roughly 4-10% of the general population possesses inherited differences in 3A4 that cause decreased metabolism. These Decreased Metabolizers may be at increased risk for dose-dependent side effects to drugs normally inactivated by 3A4.

Questions?


*Lack of efficacy due to failure to produce active metabolite; †Increased risk of adverse events due to diminished drug clearance.
CYP2D6 Poor Metabolizer (PM): This patient’s genotype is consistent with a lack of CYP2D6 enzymatic activity. PMs are at increased risk of drug-induced side effects due to diminished drug elimination of active drugs or lack of therapeutic effect resulting from failure to generate the active form of the drug, as is the case with pro-drugs.
CONFIDENTIAL COPYRIGHT PGXL LABORATORIES 2012
CYP2D6 *4/*4 CYP2D6 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Poor Metabolizer Avoid Alternative Consideration Adjust Dosage Adjustment Codeine** Morphine, non-opioid Aripiprazole† 10 mg/day maximum Hydrocodone** Hydromorphone, non-opioid Clomipramine† decrease 50% Oxycodone** Oxymorphone, non-opioid Doxepin† decrease 60% Tramadol** Consider active drug, non-opioid Flecainide† decrease 50% Tamoxifen** Anastrozole, exemestane, letrozole Haloperidol† decrease 50% Amitriptyline† Citalopram, sertraline Imipramine† decrease 70% Venlafaxine† Citalopram, sertraline Nortriptyline† decrease 60% Risperidone† Quetiapine, olanzapine, clozapine Propafenone† decrease 70% Metoprolol† decrease 75%, or
atenolol, bisoprolol, carvedilol
Zuclopenthixol† decrease 50%, or flupenthixol, quetiapine, olanzapine, clozapine

RESULTS THERAPEUTIC IMPLICATIONS (adapted from published resources1,4,6) Gene Phenotype Avoid Alternative Consideration Adjust Dosage Adjustment X CYP2D6 *4/*4
Poor Metabolizer
Codeine* Hydrocodone* Oxycodone* Tramadol* Tamoxifen* Amitriptyline† Venlafaxine† Risperidone†
Morphine, non-opioid Hydromorphone, non-opioid Oxymorphone, non-opioid Consider active drug, non-opioid Anastrozole, exemestane, letrozole Citalopram, sertraline Citalopram, sertraline Quetiapine, olanzapine, clozapine
Aripiprazole† Clomipramine† Doxepin† Flecainide† Haloperidol† Imipramine† Nortriptyline† Propafenone† Metoprolol† Zuclopenthixol†
10 mg/day maximum 50% 60% 50% 50% 70% 60% 70% 75%, or atenolol, bisoprolol, carvedilol 50%, or flupenthixol, quetiapine, olanzapine, clozapine
CYP2D6 *1/*1
Extensive Metabolizer
Normal metabolic clearance expected. Common CYP2D6 medications next page
! CYP2D6 *1/*4
Intermediate Metabolizer
Oxycodone* Hydrocodone* Propafenone† Risperidone† Velafaxine†
Oxymorphone, non-opioid Hydromorphone, non-opioid Sotalol, disopyramide, quinidine, amiodarone Quetiapine, olanzapine, clozapine Citalopram, sertraline
Codeine* Tramadol* Tamoxifen* Amitriptyline† Imipramine† Nortriptyline† Zuclopenthixol† Doxepin† Flecainide† Metoprolol†
15-60 mg/hr titrate to pain relief Avoid CYP2D6 inhibitors, e.g. paroxetine, or consider aromatase inhibitor in post-menopausal women 25% 30% 40% 25% 20% 25% 50%, or atenolol, bisoprolol, carvedilol
X CYP2D6 *1/*1xN
Ultra-Rapid Metabolizer
Codeine* Hydrocodone* Oxycodone* Amitriptyline† Clomipramine†
Paroxetine† Atomoxetine†
Risperidone† Zuclopenthixol† Propafenone†
Morphine, non-opioid Hydromorphone, non-opioid Oxymorphone, non-opioid Citalopram, sertraline Citalopram, sertraline Citalopram, sertraline Methylphenidate Quetiapine, olanzapine, clozapine Flupenthixol, quetiapine, olanzapine, clozapine Sotalol, disopyramide, quinidine, amiodarone
Tramadol* Imipramine† Nortriptyline†
Venlafaxine†
Haloperidol† Doxepin†
Metoprolol†
30% 70% 60% 150%, or citalopram, sertraline based on plasma measurement, or pimozide, flupenthixol, fluphenazine, quetiapine, olanzapine, clozapine 100% up to 250%, or atenolol, bisoprolol, carvedilol
CONFIDENTIAL COPYRIGHT PGXL LABORATORIES 2012
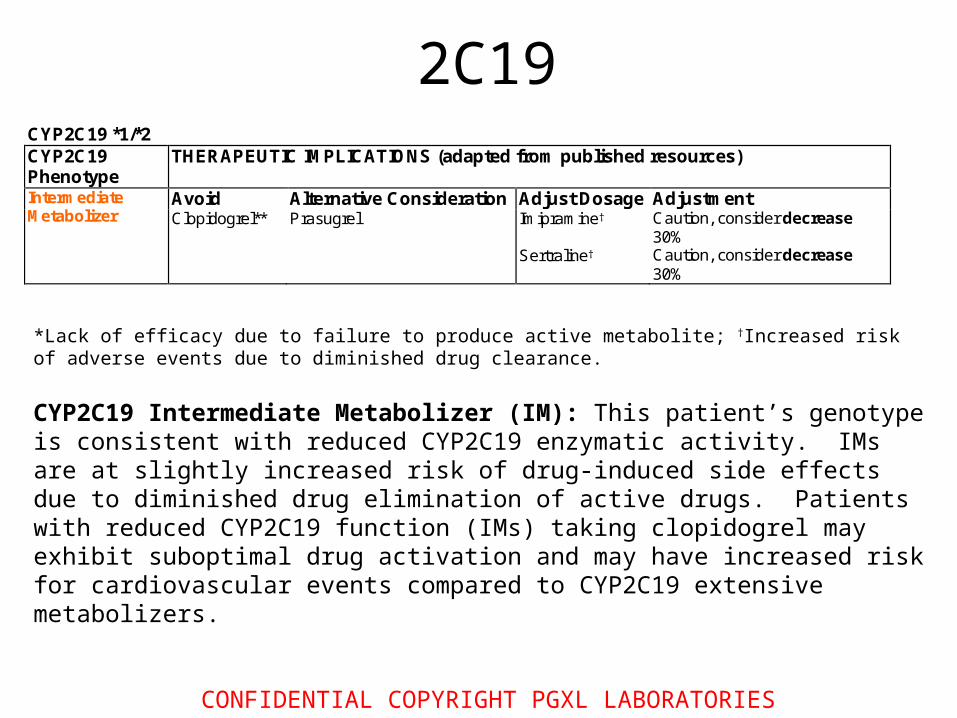
*Lack of efficacy due to failure to produce active metabolite; †Increased risk of adverse events due to diminished drug clearance. CYP2C19 Intermediate Metabolizer (IM): This patient’s genotype is consistent with reduced CYP2C19 enzymatic activity. IMs are at slightly increased risk of drug-induced side effects due to diminished drug elimination of active drugs. Patients with reduced CYP2C19 function (IMs) taking clopidogrel may exhibit suboptimal drug activation and may have increased risk for cardiovascular events compared to CYP2C19 extensive metabolizers.
CYP2C19 *1/*2 CYP2C19 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Intermediate Metabolizer
Avoid Alternative Consideration Adjust Dosage Adjustment Clopidogrel** Prasugrel Imipramine† Caution, consider decrease
30% Sertraline† Caution, consider decrease
30%
2C19

2C19 all
! CYP2C19 *1/*2
Intermediate Metabolizer
Clopidogrel* Prasugrel Imipramine† Sertraline†
Caution, consider 30% Caution, consider 50%
X CYP2C19 *2/*2
Poor Metabolizer
Clopidogrel*
Prasugrel Imipramine† Sertraline†
30% 50%
X CYP2C19 *17/*17
Ultra-Rapid Metabolizer
Increased metabolic clearance expected. Possible increased risk of bleeding events with clopidogrel7.
Citalopram† Escitalopram† Omeprazole† Esomeprazole† Lansoprazole† Pantoprazole†
up to 150% up to 150% 100-200% 50-100% 200% 400%
CYP2C19 *1/*1
Extensive Metabolizer
Normal metabolic clearance expected. Common CYP2C19 medications next page
! CYP2C19 *2/*17 Or *3/*17
Intermediate Metabolizer ∫
Decreased metabolic clearance expected based on presence of the inactive allele.
Imipramine† Sertraline†
Caution, consider 30% Caution, consider 50%

CONFIDENTIAL COPYRIGHT PGXL LABORATORIES 2012
CYP2C9 Intermediate Metabolizer (IM): This patient’s genotype is consistent with reduced CYP2C9 enzymatic activity. Reduced CYP2C9 activity leads to lower warfarin dose requirement due to decreased clearance, increased elimination half-life, and increased time to reach steady-state blood concentrations. The time to reach steady-state affects the timing of INR measurement for optimal interpretation. Time to reach steady-state is the time period required for the dosage to consistently yield reproducible blood concentrations of warfarin. INR measurements are most reliable when measured after steady-state has been achieved. INR measurements before steady-state blood concentrations have been achieved should be interpreted with caution, as they may not be indicative of stable therapy.
VKORC1 Low Warfarin Sensitivity: This patient’s genotype is consistent with higher VKORC1 enzyme expression and higher warfarin dose requirement. ‡The warfarin maintenance dose estimate was derived using a published formula that accounts for age, gender, weight, and CYP2C9 and VKORC1 genotypes. This estimate should be viewed as an example of how this information can be taken into consideration by the physician as part of the overall patient management strategy.
CYP2C9 *1/*2 CYP2C9 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Intermediate Metabolizer
Decreased metabolic clearance expected. Adjust Dosage Adjustment Phenytoin† decrease 25%
Warfarin† See below
VKORC1 GG VKORC1 Phenotype
THERAPEUTIC IMPLICATIONS (adapted from published resources)
Low warfarin sensitivity
Estimated warfarin maintenance dose requirement: 6.20 mg/day‡ Estimated time to steady-state: Delayed, 8-11 days INRs measured before steady state blood concentrations have been achieved should be interpreted with caution as they may not be indicative of stable therapy.
**Lack of efficacy due to failure to produce active metabolite; †Increased risk of adverse events due to diminished drug clearance.
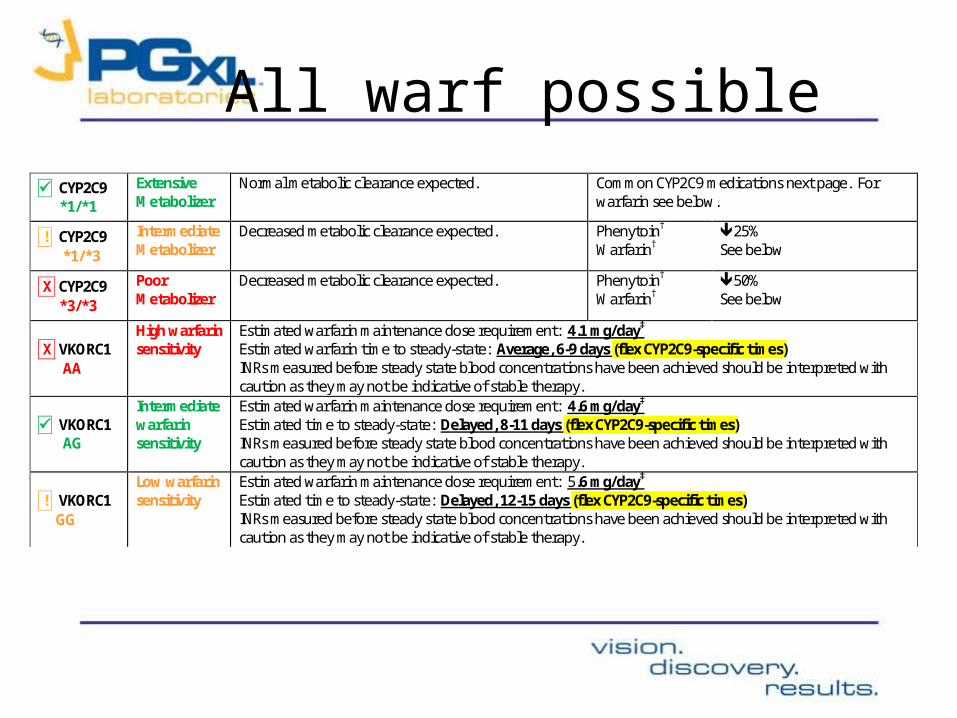
All warf possible
CYP2C9 *1/*1
Extensive Metabolizer
Normal metabolic clearance expected. Common CYP2C9 medications next page. For warfarin see below.
! CYP2C9 *1/*3
Intermediate Metabolizer
Decreased metabolic clearance expected. Phenytoin†
Warfarin† 25% See below
X CYP2C9 *3/*3
Poor Metabolizer
Decreased metabolic clearance expected. Phenytoin†
Warfarin† 50% See below
X VKORC1 AA
High warfarin sensitivity
Estimated warfarin maintenance dose requirement: 4.1 mg/day‡
Estimated warfarin time to steady-state: Average, 6-9 days (flex CYP2C9-specific times) INRs measured before steady state blood concentrations have been achieved should be interpreted with caution as they may not be indicative of stable therapy.
VKORC1 AG
Intermediate warfarin sensitivity
Estimated warfarin maintenance dose requirement: 4.6 mg/day‡
Estimated time to steady-state: Delayed, 8-11 days (flex CYP2C9-specific times) INRs measured before steady state blood concentrations have been achieved should be interpreted with caution as they may not be indicative of stable therapy.
! VKORC1 GG
Low warfarin sensitivity
Estimated warfarin maintenance dose requirement: 5.6 mg/day‡
Estimated time to steady-state: Delayed, 12-15 days (flex CYP2C9-specific times) INRs measured before steady state blood concentrations have been achieved should be interpreted with caution as they may not be indicative of stable therapy.

X Factor V Leiden AA
>9 fold Increased Thrombosis Risk
Positive family history of thrombotic events: avoid estrogen-containing oral contraceptives and consider alternative contraceptive (e.g., IUD or progestin-only contraceptive).
Negative family history of thrombotic events: avoid additional risk factors (e.g., obesity, smoking).
! Factor II GA
2-3 fold Increased Thrombosis Risk
X MTHFR 677 TT 1298 AA
Increased Risk
Increased risk of hyperhomocysteinemia, coronary artery disease, and thrombosis when folate deficiency is present. Consider folate supplementation.
Factor V Leiden High Thrombosis Risk: This genotype result revealed that the patient is homozygous for (has two copies of) the Factor V Leiden (1691 G>A) variant, which has been associated with an increased risk of thromboembolic events.This variant is found in approximately 4% of individuals in the U.S. Presence of the Factor V Leiden variant increases the risk of venous thromboembolism (VTE) by 3-8 fold in heterozygous carriers and >9 fold in homozygous carriers.
Factor II Moderate Thrombosis Risk: This genotype result revealed that the patient is heterozygous for (has one copy of) the Factor II (Prothrombin) 20210 G>A variant, which has been associated with an increased risk of thromboembolic events. This variant is found in approximately 2% of individuals in the U.S. Presence of the Factor II 20210G>A variant increases the risk of venous thromboembolism (VTE) by 2-3 fold in heterozygous carriers and >3 fold in homozygous carriers.
MTHFR Increased Risk: Presence of the 677 C>T polymorphism of MTHFR leads to decreased MTHFR enzymatic activity and elevated homocysteine. This patient’s genotype is consistent with an increased risk of hyperhomocysteinemia, atherosclerotic heart disease, myocardial infarction, cerebrovascular disease, and venous thrombosis. Additionally, associations between the 677 C>T polymorphism and increased risk for methotrexate toxicity, increased 5-fluorouracil chemosensitivity, and increased risk of fetal neural tube defects in pregnant women have also been reported in states of folate deficiency.

Factor V Leiden GG
No Increased Thrombosis Risk
! Factor V Leiden GA
3-8 fold Increased Thrombosis Risk
Female, Positive family history of thrombotic events: avoid estrogen-containing oral contraceptives and consider alternative contraceptive (e.g., IUD or progestin-only contraceptive).
Female, Negative family history of thrombotic events: avoid additional risk factors (e.g., obesity, smoking).
X Factor V Leiden AA
>9 fold Increased Thrombosis Risk
Positive family history of thrombotic events: avoid estrogen-containing oral contraceptives and consider alternative contraceptive (e.g., IUD or progestin-only contraceptive).
Negative family history of thrombotic events: avoid additional risk factors (e.g., obesity, smoking).
Factor II GG
No Increased Thrombosis Risk
! Factor II GA
2-3 fold Increased Thrombosis Risk
X Factor II AA
>3 fold Increased Thrombosis Risk
MTHFR 677 CC 1298 AA
No Increased Risk of hyperhomocysteinemia, coronary artery disease, or thrombosis
MTHFR 677 CC 1298 AC
No Increased Risk of hyperhomocysteinemia, coronary artery disease, or thrombosis
MTHFR 677 CC 1298 CC
No Increased Risk of hyperhomocysteinemia, coronary artery disease, or thrombosis
MTHFR 677 CT 1298 AA
No Increased Risk of hyperhomocysteinemia, coronary artery disease, or thrombosis
MTHFR 677 CT 1298 AC
No Increased Risk of hyperhomocysteinemia, coronary artery disease, or thrombosis
MTHFR 677 CT 1298 CC
No Increased Risk of hyperhomocysteinemia, coronary artery disease, or thrombosis
X MTHFR 677 TT 1298 CC
Increased Risk
Increased risk of hyperhomocysteinemia, coronary artery disease, and thrombosis when folate deficiency is present. Consider folate supplementation.
X MTHFR 677 TT 1298 AC
Increased Risk
Increased risk of hyperhomocysteinemia, coronary artery disease, and thrombosis when folate deficiency is present. Consider folate supplementation.
X MTHFR 677 TT 1298 AA
Increased Risk
Increased risk of hyperhomocysteinemia, coronary artery disease, and thrombosis when folate deficiency is present. Consider folate supplementation.