louisville medicine medicine/lm... · louisville medicine is published monthly by the greater...
TRANSCRIPT

LouisviLLe MedicineGREATER LOUISVILLE MEDICAL SOCIETY VOL. 59 NO. 12 MAY 2012


I don’t justhave insurance.
I own the company.
Medical Professional Liability Insurance
Mutual Interests. Mutually Insured.
Contact Susan Decareaux or Jesse Lawler at [email protected] or call 1-800-342-2239. svmic.com
“Like me, you’ve probably noticed some professional liability insurance providers recently offeringphysicians what seem to be lower rates. But when I took a closer look at what they had to offer, I realizedthey simply couldn’t match SVMIC in terms of value and service. And SVMIC gives me the peace ofmind that comes when you’re covered by a company with more than 30 years of service and the financialstability of an “A” (Excellent) rating. At SVMIC, I know it’s not just one person I rely on… there are 165professionals who work for me. That’s because SVMIC is owned by you, me, and over 15,000 otherphysicians across the Southeast. So we know our best interests will always come first.”
PediatricianPEDIATRIC & ADOLESCENT
ASSOCIATES, LEXINGTON, KY
Katrina Hood, M.D., F.A.A.P.
5_SVMIC_KY_Hood_LouisMed_7.5x9.5_2009.qxd:Layout 1 9/15/09 9:07 AM Page 1

MAY 2012 3
Where Does the Money Go? Part VIII‘As Good As It Gets’ – The Federal Employees Health Benefits ProgramMichael B. Flynn, MD
Countdown to ICD-10GLMS to Hold Education Series This SummerRandy Schrodt Jr., MD
History of the University of Louisville School of MedicineIII. A River Runs Through ItGordon R. Tobin, MD
GLMS Annual Report 2012Ellen R. Hale
Have Beretta, Will TravelB. Gordon Carnes, MD, Diplomate ABFM
GLMS BoARD oF GoVERnoRSKimberly A. Alumbaugh, MD, board chairDavid E. Bybee, MD, presidentRussell A. Williams, MD, president-electRobert A. Zaring, MD, MMM, vice president and AMA alternate delegateHeather L. Harmon, MD, treasurerJames Patrick Murphy, MD, secretaryRobert H. Couch, MD, at-largeJohn M. Gormley, MD, at-largeJeffrey L. Reynolds, MD, at-largeWayne B. Tuckson, MD, at-largeDaniel W. Varga, MD, at-largeJonathan W. Wilding, MD, at-largeBruce A. Scott, MD, AMA delegateGordon R. Tobin, MD, KMA immediate past presidentFred A. Williams, Jr. MD, KMA vice presidentRandy Schrodt, Jr. MD, KMA 5th district trusteeDavid R. Watkins, MD, KMA 5th district alternate trusteeK. Thomas Reichard, MD, GLMS Foundation president Stephen S. Kirzinger, MD, Medical Society Professional Services presidentToni M. Ganzel, MD, MBA, interim dean, U of L School of MedicineJay P. Davidson, president and CEO, The Healing PlaceLaQuandra S. Nesbitt, MD, MPH, director, Louisville Metro Department of Public Health & WellnessRhonda Rhodes, GLMS Alliance president
LoUISVILLE MEDICInE EDIToRIAL BoARDEditor: Mary G. Barry, MDElizabeth A. Amin, MDDeborah Ann Ballard, MDR. Caleb BuegeArun K. Gadre, MDStanley A. Gall, MDLarry P. Griffin, MDKenneth C. Henderson, MDJonathan E. Hodes, MD, MSTom James, MDTeresita Bacani-Oropilla, MDTracy L. Ragland, MDCharles B. Ross, MDM. Saleem Seyal, MDDave Langdon, Louisville Metro Department of Public Health & WellnessKimberly A. Alumbaugh, MD, board chairDavid E. Bybee, MD, presidentRussell A. Williams, MD, president-electLelan K. Woodmansee, CAE, executive directorBert Guinn, MBA, chief communications officerEllen R. Hale, communications associateDonna Watts, communications designer
ADVERTISInG Cheri K. McGuire, director of marketing736.6336, [email protected]
Follow us on Linkedin, Facebook, Twitter and YouTube
LouisviLLe Medicine is published monthly by the Greater Louisville Medical Society, 101 W. Chestnut St. Louisville, Ky. 40202 (502) 589-2001, Fax 581-9022, www.glms.org. Articles to be submitted for publication in LM must be received on electronic file on the first day of the month, two months preceding publication. Opinions expressed herein are those of individual contributors and do not necessarily reflect the position of the Greater Louisville Medical Society. LM reminds readers this is not a peer reviewed scientific journal. LM reserves the right to make the final decision on all content and advertisements. Circulation: 4,000
on THE CoVER: A look back at the 2011-12 year at GLMS. Story on page 20. Design by Donna Watts.
LouisviLLe MedicineGREATER LoUISVILLE MEDICAL SoCIETY VoL. 59 no. 12 MAY 2012
f E A T U R E A R T I C L E S
D E p A R T M E N T SFrom the PresidentThis I Also BelieveDavid E. Bybee, MD, MACP, FACE
ReflectionsSnippets of World War II MemoriesTeresita Bacani-Oropilla, MD
In RemembranceMcHenry S. Brewer, MDCecy Norman Brewer
We Welcome You
Physicians in Print
Alliance newsRhonda Rhodes
Doctors’ LoungeBans from BozosMary G. Barry, MD The Social History (SH)David Seligson, MD
Letter to the EditorLarry P. Griffin, MD, FACOG
Letter to the EditorTracy L. Ragland, MD
Letter to the EditorGordon R. Tobin, MD
7
12
14
2026
5
32
35
36363739

4 LouisviLLe Medicine

MAY 2012 5
fROM ThE pRESIDENTDavid E. Bybee, MD, MACP, FACEGLMS President
ThIS I ALSO BELIEVE Over the last year we have been on a journey looking at our profession. I hope that you have enjoyed some of the thoughts and suggestions. I wish I could say that the journey has led to a happy ending, but I am very concerned.
obituaryThe Louisville Courier-Journal, January 1, 2020 Relationship, Patient-Physician. Our beloved Patient-Physician Relation- ship (P-PR) died of strangulation slowly and painfully at year’s end. Born in the cradle of human civilization, P-PR enjoyed a long and productive life. Many were touched by her caring nature and strong advocacy for the good in health care. She nurtured her offspring, the profession of medicine, to grow into service for mankind, creat- ing miracles and using them for the good of all. She was preceded in death by the medical profession, and, as all mothers would, she wept bitterly. She was also preceded in death by medi- cal collegiality, advocacy for the patient, patient autonomy and her beloved Art of Medicine. She is survived by myriad health care systems with widgets and throughput, ACOs, medical homes and neighbor- hoods, and the medical homeless. She is also survived by IPABs, shared savings, audit by “RACk,” PECOS billing and value purchasing. In lieu of flowers, she has requested the donation of your heart and soul to her resurrection and reinstatement as the centerpiece of medical care. I believe the patient-physician relation-ship is in real danger. A friend of mine told me the story of her mother’s recent experience. Her mother is 77 years old and lives in the Okolona neighborhood. She loves her primary care physician and has experienced excellent medical care through a two-way patient-physician relationship. Just before the end of April, she opened the community section of The
Courier-Journal and saw an advertisement for a new Norton medical facility that was coming soon in her neighborhood. Her doctor was in the picture. The patient’s mother realized, however, that her doctor had been working in a practiced owned by TPG at Jewish. She tried to find out details from that practice but was stonewalled by the (system-employed) office staff. She was told that, on May 1, new physi-cians would be in that practice space and that someone would take care of her. She became worried and felt somewhat aban-doned. My takehome lesson from this sto-ry is that health care systems are looking at doctors as plug-in modules. This is shift-ing the patient relationship to the system rather than to the physician. And doctors are reacting with acquiescence, looking at their relationship with the health care system only with the eye of self-interest for what is most profitable. In last month’s article, I observed: “We have all seen that patients become somewhat powerless in the various payment schemes for health care.” Earlier this year, I described two reasons for this attack on our profession. The first is that society is out of money, and the second is the changing nature of informa-tion. Dr. Urbach, in his comments about medical students today, noted that they are all wearing electronic information de-vices on their belts and that there was no reason for anyone to be dumb. This access to information also applies to mid-level practitioners. I do not disagree with this in-creased access to information. However, as I pointed out in the first article of this se-ries, Knowledge and Experience are valued less by the public. As a result, information, so easily obtained, is substituted for actual thinking. With respect to the financial dilemma, within the patient-physician re-lationship, attention to the patient’s needs and respect for the patient’s wants by the physician are the most cost-effective medicines available. However, our current health care plans substitute surrogate systems of care for humanized medicine. I hope that I have been able to help
you understand the urgent need for your action. I call upon you to always keep the patient-physician relationship as the foundation of your medical practice. Let no one or no thing intrude on it. I also ask you to place yourself, the physician, as the “Brand.” Do not allow the insurer, the health care system or any other health care-related entity claim to be the face of the profession of medicine. If you join a health care system, as many of us have done or will do, maintain control of your patient list and your relationships. And finally, I call upon you to continue or begin your support of GLMS by your member-ship to help us achieve our mission to: • Promote the science, art and profession of medicine • Protect the integrity of the patient-physician relationship • Advocate for the health and well-being of the community • Unite physicians to achieve these ends. We are a very unusual medical society. GLMS has a membership of approximately 84 percent of those eligible for member-ship in our service area. My first thanks for support during this last year goes to you, the membership, for your gifts of finances, expertise and, most important, your pre-cious time. I also am grateful and indebted to my fellow officers, Drs. Kimberly Alum-baugh, Russ Williams, Rob Zaring, Heather Harmon and J. Patrick Murphy along with the members of the Board of Governors and committee chairs and members. I am also thankful for the support and thought-ful guidance, delivered in a gentle and clear way, from Lelan Woodmansee, Bert Guinn, Glenda Klass and the great staff of GLMS. I pray that all of us will give Dr. Williams the same support and encour-agement to resurrect and reinstate the patient-physician relationship as the centerpiece of the profession of medicine.
Note: Dr. Bybee practices Endocrinology with Endocrine & Diabetes Associates.
LM

6 LouisviLLe Medicine

The Federal Employees Health Benefits Program is administered by the Office of Person-nel Management, which has oversight of the federal workforce.1 The FEHBP offers a choice of five government-
wide fee-for-service plans and another five plans available to employees of certain small federal agencies (e.g. the Foreign Service). In addition in 2010, enrollees had 235 different private health care plan choices, including all regionally available options, multiple plan choices includ-ing standard option, high option and high-deductible plans. All FEHBP plans cover a range of benefits, including hospital, surgical, physician, mental health, prescription drug, emergency care and “catastrophic” benefits. The federal government and enrollees jointly pay the cost of the FEHBP plans. The government share varies de-pending on the plan selected. Participants pay an average of 30 percent, no less than 25 percent of premium cost, and could pay more depending on the plan.1 The average premium amount for 2010 is shown in Table 1.
Table 1. Average FEHBP Premium Amount for 2010
Government Share Enrollee’s Share Total $6,287.84 $2,724.54 $9,012.38
Source: 2010 Press Release on FEHBP from the Office of Personnel Management
The FEHBP negotiates contracts annually with all insur-ance companies that wish to participate.2 The FEHBP is the largest employer-sponsored health plan in the U.S., with an estimated 2.15 million workers, so there is plenty of competition for the business.3 The FEHBP is a remark-ably well-administered plan that provides a wide range of options and prevents most of the exploitive practices of the for-profit health care industry. So, if Blue Cross Blue Shield, Humana, CIGNA, WellPoint and etc. want to play in the FEHBP sandbox, they must play by FEHBP rules, not the predatory standards of the industry. Members of Congress are eligible to participate in the FEHBP, as one of the benefits of having been elected to the political ruling class in this country. This is a pretty good deal especially when added to all of the other perks of elected office. According to the National Taxpayers Union, the salary for a rank-and-file member of Congress ($174,000) is 3.4 times higher than the average full-time employee in the U.S.4 Compared to a number of other industrialized nations, only Japan has a higher “pay gap” between legislators and average workers (3.7 to 1). The ra-tio of lawmakers’ salaries to average wages is much lower in the United Kingdom (2.2 to 1), France (2.0 to 1) and Germany (2.8 to 1). When all the goodies of total congressional compensa-tion are added up, this is a reasonably good package, not free but very comprehensive and at a modest cost. The sal-ary, the value of health and life insurance, a defined benefit pension, a defined contribution arrangement with a gener-ous “match” from taxpayers adds up to nearly $285,000 a year.4 This is meager compensation compared to the packages of the CEOs of the for-profit health care insur-ance companies, but one hopes that members of Congress are driven by higher goals. In addition to being eligible for the FEHBP, these legisla-tors have access to the Office of Attending Physician. This is a walk-in primary care office, located on the second floor of the U.S. Capitol, run by the U.S. Navy.5 This office pro-vides members of Congress and the nine Supreme Court justices with primary care medical services, physicals and routine examinations, on-site X-rays and lab work, physical therapy and referral to military hospitals and private prac-tices for an annual fee of $503.5 Members do not have to pay for individual services or submit claims. The Navy pays most of the cost, about $4 million yearly. On top of all this, members of Congress have privileged access to military hospitals whether or not they are veter-ans.3 Outpatient medical care at the Naval Medical Center, Bethesda, and at Walter Reed Army Medical Center (before it closed) is/was free.6 Other services at these institutions can be obtained using FEHBP benefits.
MAY 2012 7
Michael B. Flynn, MD
Where Does the Money Go? Part VIII
‘As GooD As It Gets’ – the FeDerAl eMPloyees heAlth BeneFIts ProGrAM
Continued on page 8

8 LouisviLLe Medicine
Many members of Congress have taken advantage of these privileges. In February 2003, Sen. Mitch McConnell underwent coronary artery bypass surgery at the National Naval Medical Center.7 At the same institution, Sen. John McCain had a skin lesion removed from his left temple in May 2000 and Sen. Kit Bond had a hip replacement in April 2003. Rep. Debbie Wasserman Schultz was treated for breast cancer both at the Naval Medical Center and Walter Reed.7,8 These are just a few examples of a long list of politi-cal leaders who have received health care at government-run facilities. In my opinion, it is entirely reasonable and appropri-ate for elected officials doing the country’s business to have these privileges and to have them available at a reasonable cost. Compensation for this important work is modest compared to business, entertainment and sports standards. The FEHBP is a model that should be the goal of health care for the rest of the country. Table 2 is a list of 14 important components of health care provided to mem-bers of Congress, with heavy subsidy at taxpayer expense.9 Interestingly, the Affordable Care Act provides the same protections and guarantees to the rest of the population of the country.9
Table 2. Health Care Protections and Guarantees Found in both the FEHBP and the ACA
1. Affordable health coverage2. Guaranteed coverage, regardless of preexisting conditions3. A right to appeal claims that are denied by insurers4. Protection against discriminatory premiums due to preexisting conditions5. A complete package of health insurance benefits6. Guaranteed coverage that can’t be taken away7. A prescription drug benefit with no coverage gap8. Protection against catastrophic health care costs9. A choice of easy-to-compare health insurance plans10. Protection against unreasonable premium increases11. Fair and equal premiums for women12. Coverage for early retirees13. Access to free or low-cost preventive services14. Access to affordable care at clinics
Continued from page 7
Continued on page 10
MAY 2012 9

10 LouisviLLe Medicine
The fate of the ACA, whether it is an end unto itself, the beginning of a process or destined for repeal, is unclear and will be determined by the judicial and political pro-cess in the next year. Whatever the outcome for the ACA, the components of heath care available to members of Congress at reasonable cost should be the foundation of health care available to the rest of the population. As well as can be determined, very few members of Con-gress have declined the opportunity for health care under FEHBP.3,5 An exact head count of members of Congress covered under government-sponsored health care is not possible without directly contacting each member. Good luck with that one! During the opening days of the 112th Congress, a measure was offered in the House of Represen-tatives that would have required members of Congress to disclose their health care coverage status.5 It was defeated 240-191.5 An interesting dichotomy is afoot in the legislative branch of our national government today. On the one hand, active and retired legislators enthusiastically participate in and benefit from an exceptionally well-administered and very inclusive FEHBP, which provides a wide range of options and services at modest cost and with heavy taxpayer subsidy. On the other hand, many members of Congress, including one active and two retired members who have been in the presidential race, are vehemently opposed to providing the same degree of health care security to the rest of the population. “Europe-an socialism, bankrupt the country, violation of individual
rights!” cry they. Clearly what is good for the goose (Con-gress) is not good for the gander (everybody else in the country). Hypocrisy thrives in the halls of Congress.
References1. Health Benefits for Members of Congress. Barbara English, Congressional Research Service. March 16, 2011.
2. Health Care for Members of Congress? Barbara English, Con-gressional Research Service. FactCheck.org. August 25, 2009.
3. GOP can Hate “Obamacare,” love congressional health perk. Bill Straub. Suntimes.com, August 4, 2011.
4. Piling on the Perks. Pete Sepp. National Taxpayers Union. August 6, 2011.
5. Health benefits for members of Congress generous. Bill Straub. Scrippsnews. January 27, 2011.
6. No debating Congress’ Lavish Health Care. Sharyl Attkisson. CBSnews.com. October 14, 2009.
7. GOPers Decrying “Socialized Medicine” Go to Govt. Hospital For Surgeries. The HuffingtonPost.com. October 18, 2009.
8. Lawmakers get “generous” health plans. John Fritze, USA TO-DAY. June 24, 2009.
9. H.R. 2: Guilty of a Double Standard. FamiliesUSA.org. 2011.
Note: Dr. Flynn is a professor at the University of Louisville School of Medicine, Department of Surgery, Division of Surgical Oncolo-gy. He practices with University Surgical Associates. Extensive and detailed background research has been conducted by Ms. Leslie Pancratz, the highly skilled and professional medical librarian of the Norton Hospital library. Her persistent pursuit of objective information is greatly appreciated.
Continued from page 8
LM

MAY 2012 11
© 2
012
Bap
tist
Hea
lthca
re S
yste
m, I
nc. /
Mem
ber
, Bap
tist
Hea
lthca
re S
yste
m
LOUISVILLE’SLEADING ORTHOPEDIC HOSPITAL.
NO BONESABOUT IT.
RANKED 8TH IN THE NATION IN TOTAL JOINT REPLACEMENT.
KENTUCKY’S LEADING ORTHOPEDIC PROGRAM.
baptisthealthky.comBAPTIST HOSPITAL EAST | BAPTIST HOSPITAL NORTHEAST | BAPTIST SPORTS MEDICINE | BAPTIST URGENT CARE | BAPTIST MEDICAL ASSOCIATES
Only one hospital in Kentucky is nationally ranked for total joint
replacement. Baptist Hospital East leads the state when it comes
to orthopedic procedures and offers some of the most advanced
procedures and skilled orthopedic surgeons and specialists.
To learn more, visit baptisthealthky.com, or call (502) 897-8131
to refer a patient.
BH 506 Ortho_stretch (8.5x11)_FNL.indd 1 3/6/12 4:45 PM

12 LouisviLLe Medicine
On February 16, the Department of Health and Human Services announced its intent to delay the ICD-10 compliance date. In April, it announced a proposed rule to set the new compliance date as October 1, 2014. There has been much debate on the merits of implementing ICD-10, with the American Medical Association being one of the most
vocal critics of the pending implementation and lobbying to stop it altogether. As with any delay, there have been both sighs of relief and anger at the delay announcement. Many organizations have already spent an extraordinary amount of money to enhance their IT systems and to train their staff and physicians.
What does this mean for physicians? It means that physicians can step back, realize that most of us were not ready for the original implementation date of October 1, 2013, and take a strategic step forward to plan for the impending implementation. We should take this delay as an opportunity to cre-ate our plans for education and training correctly and thoughtfully. Practices should take advantage of this delay to begin education and documentation review, which can only help a practice, regardless of the new implementation date. Costs associated with implementa-tion can also be spread out over time, reducing the financial impact to the practice. GLMS plans to host a summer educational series that will be free for GLMS members. Both seminars will take place from 7 to 8:30 a.m. in Baptist Hospital East Auditorium. On July 12, the business impact will be covered by Jessica Williams, GLMS physician education and practice support manager. On August 9, ICD-10 documentation will be discussed by Sherry Thomas, CCP, CCP-AS, CEO and director of education at the Professional Healthcare Institute of America. Let’s not waste the opportunity we have been given. The time to prepare is now. Note: Dr. Schrodt is chair of the GLMS Emerging Medical Con-cepts Committee. He practices Psychiatry with Integrative Psy-chiatry PLLC. The GLMS physician education and practice support staff of Dottie Hargett, Jessica Williams and Stephanie Woods and Sherry Thomas, CEO and director of education for the Profession-al Healthcare Institute of America, assisted with this article.
Randy Schrodt Jr., MD
GLMS TO hOLD EDUCATION SERIES ThIS SUMMER
LM
MEET OUR NEWEST SPINE CARE EXPERT.
Norton Healthcare offers some of the most highly
experienced specialists in the field of spine care.
Our newest spine care expert, Venu Vemuri, D.O.,
specializes in herniated discs, spinal stenosis,
degenerative disc disease, scoliosis, spondylolisthesis,
compression fractures, neck pain and back pain.
To learn more or to arrange a referral to Dr. Vemuri,
call Norton Spine Specialists – Johnson & Vemuri
at (502) 629-5225.
VENU VEMURI, D.O.
210 E. GRAy ST.SUITE 701LOUISVILLE, Ky

MAY 2012 13
NATIONALINSURANCEAGENCY INC.
Professional Association & Affinity Insurance Services
NATIONALINSURANCEAGENCY INC.
Professional Association & Affinity Insurance Services
NATIONALINSURANCEAGENCY INC.
Professional Association & Affinity Insurance Services
NATIONALINSURANCEAGENCY INC.
Is your family growing?
w w w . n i a i . c o m • P h o n e : 5 0 2 4 2 5 - 3 2 3 2 • w r l @ n i a i . c o m
level Term life insurance
individual own occupation Disability insurance
In person, In your maIlbox, onlIne, nIa.
Lab_Ad_fullPage_GLMS_GameChange.indd 1 7/6/11 2:36 PM

14 LouisviLLe Medicine
The University of Louisville School of Medicine was founded 175 years ago
with a faculty torn from the heart of Lexington’s Transyl-vania Medical Department (TMD). A fierce conflict over these educators erupted between the two cities, which was reflected in the flamboyant 19th century language of their city councils, public meetings and newspapers. However, these dramatic conflicts were visible elements of a much larger saga, like wind-whipped whitecaps on a stormy sur-face, blowing over silent deep currents that determined the true course of flow. Peering into these old waters reveals the currents that defined our destiny and shows that not only U of L, but the city of Louisville itself, owe their very existence to a river and its unique geography.
pIONEER pOpULATIONS fLOw wESTwARD As the flow of pioneer settlers followed Daniel Boone’s Wilderness Trail overland into central Kentucky’s fertile bluegrass region, a small trickle of adventurers and set-tlers were floating down the Ohio in hand-hewn flatboats and keel boats. They were soon joined by boatmen seeking profits in commercial downriver shipping. All had to deal with the notorious falls between the pioneer settlement on Corn Island and the bend in the river (Fig. 1). Portage was required, as the falls could be navigated only in very high
water. Good economic opportunity from provid-ing portage and supplies lured op-portunists to
the tiny south-bank village of Louisville. However, financial gain came at substantial risk to health, as this swampy, fever-ridden site fully earned the label “graveyard of the West.” Dr. Henry McMurtrie, an early historian, described early Louisville society as “gathered from every corner of the earth ... with one single object in view, that of acquiring money ... and devoting no time to literature or the acquire-ment of those graceful nothings ... of polished society.” This contrasted sharply with the civilized culture of urbane Lexington, Kentucky’s metropolis, with its university and medical school.
AN AwE-INSpIRING MAChINE COMES DOwNSTREAM (ThEN Up) The winter of 1811-12 brought an event that would forever change the fate of Louisville (and the entire Mis-sissippi Valley). Between 1803 and 1807, inventor/en-trepreneurs Robert Fulton, Robert Livingston (Louisiana Purchase negotiator) and Nicholas Roosevelt (relative of two future presidents) struggled to adapt steam propulsion to river navigation, with success in passenger transport on the Hudson in 1807 (Fulton’s famous Clermont) (Fig. 2). They then sought to expand onto Ohio and Mississippi waterways, with commerce-derived profits in mind. In 1809, Roosevelt floated the intended route by flatboat to chart waters and find coal sup-plies. In 1811 near Pittsburgh, the three designed and tested a large, side-wheeled steamboat christened the New Orleans, for its goal. The vessel embarked in October 1811 with Roosevelt as captain, his pregnant wife, young
Gordon R. Tobin, MD
hISTORY Of ThE UNIVERSITY Of LOUISVILLE SChOOL Of MEDICINE:III. A River Runs Through It
fig. 1 The falls of the Ohio at Louisville.
fig. 2A Steamboat pioneer Robert fulton.
Continued on page 16

MAY 2012 15
JEFFERSON MANOR HEALTH & REHABILITATION 1801 Lynn WayLouisville, KY 502.426.4513
JEFFERSON PLACE HEALTH & REHABILITATION 1705 Herr Lane Louisville, KY 502.426.5600
MEADOWVIEW HEALTH & REHABILITATION 9701 Whipps Mill Road Louisville, KY502.426.2778
OAKLAWN HEALTH & REHABILITATION 300 Shelby Station Drive Louisville, KY502.254.0009
ROCKFORD HEALTH & REHABILITATION 4700 Quinn Drive Louisville, KY502.448.5850
SUMMERFIELD HEALTH & REHABILITATION 1877 Farnsley Road Louisville, KY502.448.8622
Good therapy for thebody begins with asmile on the face.
Maybe you won’t enjoy the therapy part of your
recovery, but at least, at Elmcroft, you’ll enjoy the
therapists. They’ve been handpicked for their skill
as rehab experts and their compassionate spirits.
Call any of our six Louisville communities
to learn more. Elmcroft.com/skillednursing
ELSN-101 LMed 8.5x11.indd 5 1/9/12 2:29 PM
16 LouisviLLe Medicine
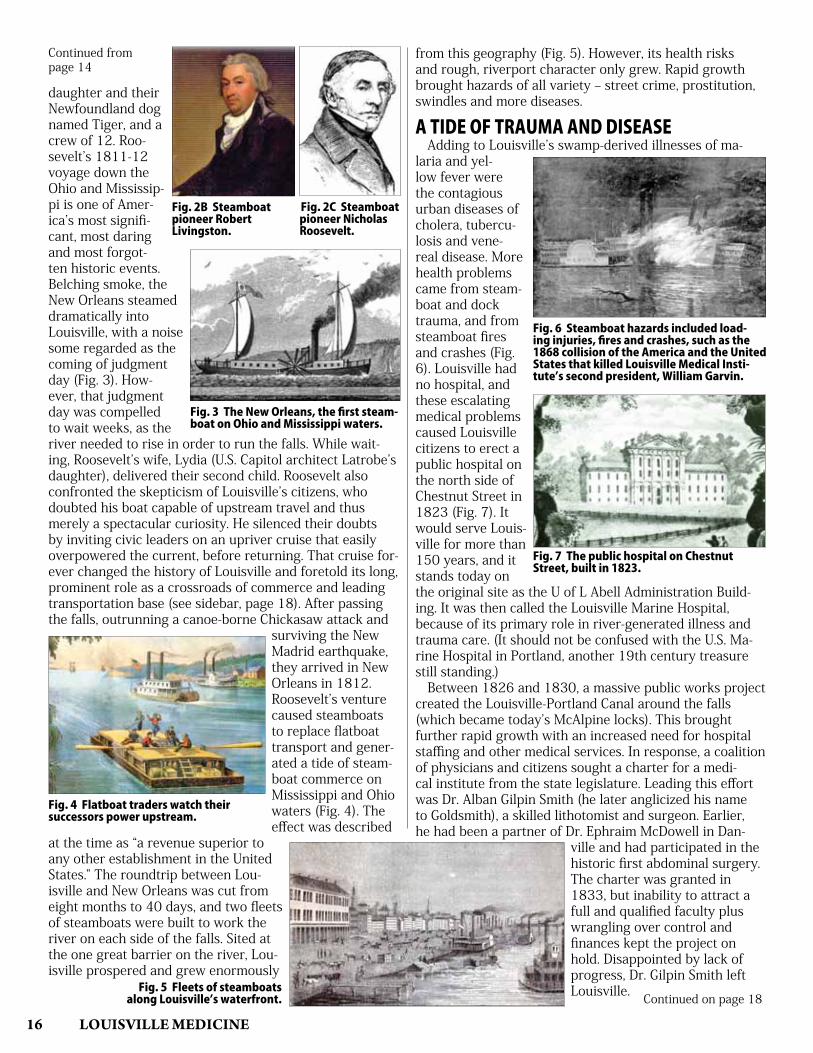
daughter and their Newfoundland dog named Tiger, and a crew of 12. Roo-sevelt’s 1811-12 voyage down the Ohio and Mississip-pi is one of Amer-ica’s most signifi-cant, most daring and most forgot-ten historic events. Belching smoke, the New Orleans steamed dramatically into Louisville, with a noise some regarded as the coming of judgment day (Fig. 3). How-ever, that judgment day was compelled to wait weeks, as the river needed to rise in order to run the falls. While wait-ing, Roosevelt’s wife, Lydia (U.S. Capitol architect Latrobe’s daughter), delivered their second child. Roosevelt also confronted the skepticism of Louisville’s citizens, who doubted his boat capable of upstream travel and thus merely a spectacular curiosity. He silenced their doubts by inviting civic leaders on an upriver cruise that easily overpowered the current, before returning. That cruise for-ever changed the history of Louisville and foretold its long, prominent role as a crossroads of commerce and leading transportation base (see sidebar, page 18). After passing the falls, outrunning a canoe-borne Chickasaw attack and
surviving the New Madrid earthquake, they arrived in New Orleans in 1812. Roosevelt’s venture caused steamboats to replace flatboat transport and gener-ated a tide of steam-boat commerce on Mississippi and Ohio waters (Fig. 4). The effect was described
at the time as “a revenue superior to any other establishment in the United States.” The roundtrip between Lou-isville and New Orleans was cut from eight months to 40 days, and two fleets of steamboats were built to work the river on each side of the falls. Sited at the one great barrier on the river, Lou-isville prospered and grew enormously
from this geography (Fig. 5). However, its health risks and rough, riverport character only grew. Rapid growth brought hazards of all variety – street crime, prostitution, swindles and more diseases.
A TIDE Of TRAUMA AND DISEASE Adding to Louisville’s swamp-derived illnesses of ma-laria and yel-low fever were the contagious urban diseases of cholera, tubercu-losis and vene-real disease. More health problems came from steam-boat and dock trauma, and from steamboat fires and crashes (Fig. 6). Louisville had no hospital, and these escalating medical problems caused Louisville citizens to erect a public hospital on the north side of Chestnut Street in 1823 (Fig. 7). It would serve Louis-ville for more than 150 years, and it stands today on the original site as the U of L Abell Administration Build-ing. It was then called the Louisville Marine Hospital, because of its primary role in river-generated illness and trauma care. (It should not be confused with the U.S. Ma-rine Hospital in Portland, another 19th century treasure still standing.) Between 1826 and 1830, a massive public works project created the Louisville-Portland Canal around the falls (which became today’s McAlpine locks). This brought further rapid growth with an increased need for hospital staffing and other medical services. In response, a coalition of physicians and citizens sought a charter for a medi-cal institute from the state legislature. Leading this effort was Dr. Alban Gilpin Smith (he later anglicized his name to Goldsmith), a skilled lithotomist and surgeon. Earlier, he had been a partner of Dr. Ephraim McDowell in Dan-
ville and had participated in the historic first abdominal surgery. The charter was granted in 1833, but inability to attract a full and qualified faculty plus wrangling over control and finances kept the project on hold. Disappointed by lack of progress, Dr. Gilpin Smith left Louisville.
fig. 4 flatboat traders watch their successors power upstream.
fig. 3 The New Orleans, the first steam-boat on Ohio and Mississippi waters.
fig. 5 fleets of steamboats along Louisville’s waterfront.
fig. 6 Steamboat hazards included load-ing injuries, fires and crashes, such as the 1868 collision of the America and the United States that killed Louisville Medical Insti-tute’s second president, william Garvin.
fig. 7 The public hospital on Chestnut Street, built in 1823.
fig. 2B Steamboat pioneer Robert Livingston.
fig. 2C Steamboat pioneer Nicholas Roosevelt.
Continued from page 14
Continued on page 18

MAY 2012 17
Kindred Healthcare understands that when people are discharged from a traditional hospital, they often need continued care in order to recover completely. That’s where we come in.
Kindred offers services including aggressive, medically complex care, intensive care and short-term rehabilitation.
Doctors, case managers, social workers and family members don’t stop caring simply because their loved one or patient has changed location.
Neither do we.
Come see how we care at continuethecare.com
Recovery doesn’t always happen overnight.Dedicated to Hope, Healing and Recovery
NATIONALLY, KINDRED CARES FOR PATIENTS IN: LONG-TERM ACUTE CARE HOSPITALS • NURSING AND REHABILITATION CENTERS • INPATIENT REHABILITATION HOSPITALS
TRANSITIONAL AND SUBACUTE CARE • ASSISTED LIVING • CONTRACT THERAPY SERVICES • HOME CARE • HOSPICE
CONTINUE THE CARE

ThE UNDERCURRENTS Of UphEAVAL The steamboat commerce that brought rapid growth to Louisville eroded the economy of inland cities, especially Lexington, which had poor access to the Ohio. Commerce and industry fled to the riverports, and Lexington’s popula-tion plummeted, falling below that of growing Louisville by 1830. All Lexington’s civic institutions were affected, including TMD. Moreover, Lexington lacked a hospital. The TMD faculty were acutely aware of the busy Louisville hospital and the enormous educational value of hospital experience, since many trained in Philadelphia, with its paired hospital and school. Moreover, bodies for anatomic studies were always scarce in Lexington, leading to much risky grave-robbing. In contrast, Louisville and Cincinnati had more abundant anatomic specimens from riverport trauma and unclaimed bodies of river passenger deaths. These undercurrents of change swept medical education in Kentucky to the brink of revolution.
A DARk pOOL Of CONSpIRACY Louisville’s hospital and growing population generated covert considerations of moving Transylvania’s medi-cal school to Louisville. Something was clearly brewing by 1834, when TMD’s spokesman, Dr. Charles Caldwell, publicly condemned multiplication of medical schools in Kentucky, especially at Louisville. After eloquently praising TMD, he rhetorically asked if “public interest called for an-other school of medicine in Kentucky?” He then answered himself, stating that it is “impossible to be a student in Louisville ... [because] numerous scenes of seduction and dissipation ... were eminently injurious to the youth who resorted to it for their education. While an emporium of commerce and trade is the best place in which to practice a profession ... it is among the worst in which to acquire a knowledge of it.” By late 1835, however, the TMD faculty members (including Dr. Caldwell) concluded that their medical school should be transferred. Clandestine discus-sions likely occurred between TMD faculty and Louisville leaders, for in late 1836 the Louisville city council openly offered Transylvania University $40,000, and a city square in Louisville to erect a building, for moving TMD.
A pOLITICAL TSUNAMI This offer created a tsunami of outrage in Lexington, with civic leaders and Transylvania trustees bitterly op-posing the concept and hurling a volley of charges against the TMD faculty, including “treason,” “fraud,” “treachery” and “moral cowardice.” When the Lexington Intelligencer reported discovery of a visit by Dr. Caldwell to Louisville, the newspaper accused him of “efforts ... not only to de-stroy our school, but to injure our city also.” The Louisville Public Advertiser caustically responded that “Lexington is now regarded as an inconsiderable inland town ... and must hereafter be viewed as a pastoral village or a declin-ing and decaying town, in the midst of hemp growing and stock raising country.” Proposals submitted before the 1837 state legislature to transfer TMD or to give Louisville a charter for a new school were rejected after a strong lob-bying effort by Lexington. Louisville responded by reviv-
ing Dr. Gilpin Smith’s unfulfilled 1833 charter to justify starting a new Louisville school. The Louisville Public Advertiser advocated a “medical institute established in Louisville capable of entering into effective and successful competition with the medical college in Lexington,” and sarcastically added, “we would not advocate a removal [from Lexington] of the lunatic asylum ... [as] her present race of statesmen will likely need an asylum in their old age.”
CROSSING ThE RUBICON In March 1837, a crisis erupted when Dr. Caldwell came to Louisville to meet city leaders, surely on behalf of his colleagues. Learning of this, the Transylvania trustees be-came enraged. Charges were leveled against Dr. Caldwell, and the trustees fired him without a hearing. They then dissolved the entire TMD faculty. Drs. Benjamin Dudley and William Richardson denied involvement in the conspir-acy and were reinstated. Drs. Lunsford Yandell and John Esten Cooke were offended by the acts of the trustees and the duplicity of their colleagues. Drs. Cooke and Yandell refused to be reinstated and set sail for Louisville. The Rubicon had been crossed. Under Drs. Dudley and Richardson, TMD would rebuild a faculty, but its vital wellspring was slowly running dry. Underlying population decline and the relentless religious strife afflicting Transylvania’s administration caused pro-gressive instability. TMD trickled to a close 20 years later, followed by its parent university.
ThE ExODUS Everything would increasingly flow to Louisville – pa-tients to the hospital, a fine faculty to Louisville Medical Institute and medical students to the city, but the waters never calmed. The founding of TMD in 1799 was the “Genesis” of medical education in Kentucky and the West; the 1837 faculty move thus became the “Exo-dus.” However, no sea would part to ease the journey, and the Promised Land of Louisville would offer great challenges for each promise fulfilled. The next chapter in this anniversary series describes a new well-spring of medical education amidst more stormy waters in the riverport city at the falls.Note: Dr. Tobin is a professor at the University of Louisville School of Medicine, Department of Surgery, Division of Plastic and Reconstruc-tive Surgery. He practices with University Surgical Associates.
18 LouisviLLe Medicine
Continued from page 16
LM

MAY 2012 19
Roneka L. RaveneLL, M.D., anD TRoy k. Takagishi, M.D.
NortoN HealtHcare welcomes
two rHeumatology specialists
we are pleased to announce that Roneka L. Ravenell, M.D., and
Troy k. Takagishi, M.D., have joined Norton rheumatology specialists.
Drs. ravenell and takagishi are board certified and fellowship trained
in rheumatology.
Norton rheumatology specialists provides care for patients with
rheumatoid arthritis, osteoarthritis, gout, lupus, osteoporosis,
fibromyalgia, bursitis and more.
to make an appointment with a Norton rheumatology specialists
physician, call (502) 629-1234. For more information about
Drs. takagishi and ravenell, visit nortonhealthcare.com/Rheumatology.
ORT-4986_LM_8.5x11_4c.indd 1 2/24/12 9:49 AM

20 LouisviLLe Medicine
he Greater LouisviLLe MedicaL society en-gaged nearly 50 leaders from business, education, government, media and nonprofit organizations in 2011-12 by giving them the opportu-nity to shadow a physician and to exchange ideas for improving the
health of the community. The launch of the Wear the White coat program was one of numerous GLMs efforts to increase the influence of physicians and the medical profession in society, a main strategic goal for the past year. “it was truly, honestly one of the greatest experiences of my life,” Wave 3 anchor dawne Gee said after shadowing Gordon r. tobin, Md, during the 2011 Wear the White coat program held in July. “i came out with an even greater ap-preciation for the physician and gratitude for what is able to be done.” under the leadership of President david e. Bybee, Md, GLMs advocated for physicians in various arenas as part of the organization’s mission to: promote the science, art and profession of medicine; protect the integrity of the physician-patient relationship; advocate for the health and well-being of the community; and unite physicians to achieve these ends.
Wear the White Coat Participants in Wear the White coat hailed from a variety of businesses and organizations including at&t, Business First, churchill downs, Ge, Louisville Metro council, Louisville Public Media, Pnc Bank, southeast christian church and yum! Brands. several individuals who serve on the boards of local hospitals joined the 2012 Wear the White coat program in February. each program began with a kickoff event at the Louisville science center that included viewing Pulse of surgery, the medical society’s educational program connecting middle and high school students to real-time heart operations at Jewish hospital. Participants then made arrangements to
shadow their physician precep-tor. each program ended with a dinner where participants shared their shadowing experiences and brainstormed ideas for improving the health of the community. Wear the White coat will be an annual event organized by the community connections com-mittee, which will maintain rela-tionships with program alumni through special events and other means. GLMs invited christine Johnson, the retired president and ceo of the Leadership Louisville center, to join the committee
GLMS AnnuAL RepoRt 2012
One Wear the White COat experienCe Kevin Lundy, a 2012 Wear the White Coat graduate and government affairs director at Yum! Brands, wrote the fol-lowing on the Leadership Louisville Center’s blog in March: My knowledge of the medical community is limited to my annual physicals and medical care of my family. Beyond that, I know little about what goes into the success of the medical profession. Was there really more than a check-up, prescribing medicine and chicken soup?! I have since learned that the answer is an unequivocal YES! Recently I had the honor of completing one of the community’s most humbling and rewarding programs, the Greater Louisville Medical Society’s “Wear the White Coat” program. This program allows community leaders to experi-ence the practice of medicine through a partnership with a Society physician member. This eye-opening experience helped me realize not only the tremendous contributions physicians make in the community, but also the challenges they face in trying to provide immediate care to their pa-tients. The heart surgery viewing was very impactful to me, be-ing the closest I had ever gotten to such a procedure. Visually seeing the operation on TV helped prepare me for my day observing in the operating room. My shadowing day was like nothing I have experienced before. I was fortunate to shadow a wonderful general surgeon who had a packed day of surgeries planned. I spent nearly six hours in the hospital operating room, viewing six different surgeries, all while not passing out! While it was ed-ucational to learn and see where various organs are located in the human body, the most impressive part of surgery was seeing the teamwork and interaction between the tending physicians. Each doctor depended on the others, ensuring the correct dosage of patient anesthesia, making each inci-sion correctly and accounting for each medical instrument post-surgery. Everyone needed to be one step ahead of the other in order to preserve the patient’s well-being. We owe a great deal of gratitude and appreciation to the medical community. Their dedication to patient health and ensuring a healthier community is vital to our collective success. I not only challenge others to take personal respon-sibility for their own health, but to participate in GLMS’ ongoing discussion on how to improve the well-being of the Louisville community.
President-Elect Russell A. Williams, MD, and Kevin Lundy during Wear the White Coat.t
President David E. Bybee, MD, (left) hosts Rick Howlett of Louisville Public Media during Wear the White Coat.
Lara O. Fakunle, MD, (left) was shadowed by Maria Hampton, senior branch executive for the Federal Reserve Bank.
ellen r. hale

MAY 2012 21
and offer her ideas in these efforts. seeing a need for educating GLMs developing leaders about the city of Louisville, GLMs in turn decided to select and send four GLMs members to the center’s Focus Louisville program in 2012. Focus Louisville is a 2 ½-day program
that gives participants exposure to local leaders, issues and opportuni-ties for community leadership. todd J. Purkiss, Phd, Md, was selected as the first representative and attended Focus Louisville in February. The Leadership and Program development committee will select future attendees in the interest of on-going leadership development. GLMs wel-comed the new director of the Louisville Metro department for Public health and Wellness, LaQuandra s. nesbitt, Md, MPh, to the Board of Gover-nors. dr. nesbitt and GLMs teamed up on a March event where phy-sicians and business leaders, including Wear the White coat gradu-ates, were surveyed about Louisville’s health care delivery system. The data was to be used for the community health needs assessment, a requirement of the affordable care act and tool for improving local health care services.
Pulse of surgery in its first full school year, Pulse of surgery held 15 programs at the Louisville science center, allowing GLMs to promote careers in medicine and healthy lifestyle choices among middle and high school students. The Jewish hospital team teaching the students through open heart surgeries shown in real time included the following GLMs physi-cians: aneeta r. Bhatia, Md, Michael Bouvette, Md, Jiapeng huang, Md, dana M. settles, Md, Mark s. slaughter, Md, david slater, Md, and Matthew L. Williams, Md. as of March, 1,376 students from nine Kentucky counties and one indiana county had attended a Pulse of surgery program this school year. another 585 students were scheduled to attend in april and May, including those from another three Kentucky counties. GLMs also provided a physician or medical student to speak to the students in person at the end of each program. during the summer, GLMs arranged for about 40 students from Kentucky state university’s upward
Bound program to attend a Pulse of surgery program. upward Bound prepares low-income and/or first-generation college students in Frankfort for success at the post-secondary level. Pulse of surgery captured national recognition by receiving a Profiles of excellence award from the american association of Medical society executives. Pulse of surgery won for the education category at the aaMse annual conference in Boston. The awards were open only to the 390 organizations that make up aaMse. GLMs also connected with Jefferson county Public schools’ professional career theme high schools in medicine, health and the environment. students at Moore traditional high school, valley tra-ditional high school and Waggener traditional high school are able to major in allied health, biomedical or nursing. one senior from each school was invited to participate in the 2012 Wear the White coat program. GLMs will continue to explore ways to support the students at Moore, valley and Waggener.
partners fOr hOpe The Board of Governors decided to have GLMs play a promi-nent role in The healing Place’s $5 million Partners for hope initia-tive, which is raising money from Louisville’s business community for the nationally recognized recovery program. The board commit-ted to collecting at least $75,000 from GLMs members and, by the end of 2011, physicians had exceeded that goal by giving more than $120,000 toward the special effort. The total included $10,000 from
Gill Holland (right), co-owner of The Green Building, shadows John M. Mandrola, MD.
LaQuandra S. Nesbitt, MD, MPH, director of Louis-ville Metro Public Health and Wellness, gets feedback on Louisville’s health care needs.
(Left to right) Executive Director Lelan K. Woodmansee, CAE, Dr. Bybee, Board Chair Kimberly A. Alumbaugh, MD, and Mark S. Slaughter, MD, celebrate a national award for Pulse of Surgery.
(Left to right) Peggy Williford, JCPS specialist for medicine, health and the environment career and technical education, Waggener senior Cintya Lara, Valley senior Shalaya Baber and Moore senior Labinot Prushi during Wear the White Coat.
continued on page 22

22 LouisviLLe Medicine
the GLMs Foundation. Because of GLMs leadership, Brown-Forman, the humana Foundation and texas roadhouse also signed on as “Partners for hope.” The support enabled The healing Place to secure an $800,000 matching grant from the Kresge Foundation and complete funding for its Women and children’s campus. The GLMs physicians who con-tributed will be recognized for their generosity in the lobby of the Will W. Ward Jr., Md, clinic at the campus, where thP clients receive free medical care from volunteer physicians.
PhysiCian eduCation and PraCtiCe suPPort The department of Physician education and Practice support, renamed in January from Professional relations, worked in a variety of ways to advocate for physicians with payers and to provide valuable education to both members and their office staff. Preparation for the transition to icd-10 was identified as a top priority by the emerging Medical concepts committee (eMcc) and Physician Practice ad-vocacy committee (PPac). Monthly articles about icd-10 appeared in Louisville Medicine and a two-part series of free workshops was developed for summer 2012. PPac held monthly educational meetings on topics such as health literacy, compliance plans and coding updates. a series of roundtable meetings with each of the five major payers in Louisville took place for the fourth straight year. The insurance issues resolu-tion committees chaired by GLMs physicians continued to meet with anthem, cGs (Medicare), humana, Passport and united-healthcare on a quarterly basis about hassles reported by members. The five annual roundtables served as a way for the membership to interact with representatives from the carriers. The PePs department also reintroduced Practice advocacy house calls to gather feedback during meetings at practices with physicians and their administrators and staff. eMcc also surveyed GLMs members about employment status, job satisfaction and GLMs member services. as expected, the survey documented an increase in employed physicians in the community. however, regardless of employment status, respondents ranked “advocating for the physician as the director of patient care” along with providing education and cMe opportunities as the top priorities for GLMs in the future. eMcc also held discussions on accountable care organization development and employer health coalitions.
The community transitions of care Workgroup, chaired by President-elect russell a. Williams, Md, brought together physicians, hospitals, nursing homes and home health agencies from across the community. The workgroup developed a universal form to provide timely, accurate and useful information at the time of transfer in an effort to ensure patient safety. a tiered, multi-phase pilot program was initiated. The Physicians take aiM at diabetes Program was active this year in performing diabetes recognition Program audits. The aiM program reached an all-time high of 118 GLMs physicians who have the national committee for Quality assurance recognition. The Quality improvement and Patient safety com-
mittee (QiPs) oversaw the aiM and transitions of care initiatives as well as exploring other topics such as falls prevention, quality reporting processes locally and
nationally, and the Metro Public health and Wellness department’s as-sessment on community health screening and disease reporting.
Leadership deveLOpment GLMs held its second Physician Leadership course in october for select university of Louisville residents, first-year and second-year practicing physicians and current GLMs leaders. Mark a. covaleski, Phd, cPa, from the american college of Physician executives taught approximately 60 GLMs members about health care finance. The annual course is a way to support young physicians and develop future leaders for both the medical society and the community. an annual tradition, GLMs provided the incoming students at the university of Louisville school of Medicine with their first white coats during a ceremony in august. Board chair Kimberly a. alum-baugh, Md, spoke at the ceremony. afterward, 124 of the medical students activated their free GLMs membership by having a compli-mentary professional portrait taken. The third annual specialty speed networking event in March linked medical students with GLMs physicians from eight different specialties. The Lead-ership and Program development com-mittee coordinated the event, designed to assist students with selecting a specialty, with u of L’s aMa Medical student section. tables rotated every several minutes so students could network with all the doctors on hand.
legislative advoCaCy GLMs took a leading role at the KMa annual Meeting in september by drafting 11 resolutions that were adopted by the house of delegates, as physicians began to
(Left to right) Gregg Carter from the Humana Foundation, Lelan Woodmansee, The Healing Place President and CEO Jay Davidson, THP Board Chair Dan Caudill and Texas Roadhouse President Scott Colosi represent the “Partners for Hope.”
Todd J. Purkiss, PhD, MD, and medical stu-dents at the Specialty Speed Networking event.
GLMS Treasurer Heather L. Harmon, MD, addresses the KMA House of Delegates.
continued from page 21
GLMS AnnuAL RepoRt 2012

MAY 2012 23
mobilize for the Kentucky General assembly’s 2012 session. KMa, supported by its GLMs members, focused during the session on lobbying lawmakers about proposed legisla-tion regarding Kentucky’s prescription drug monitor-ing program, KAsPer, and oversight of controlled substance prescribing by physicians. GLMs held a town hall meeting in early March to educate members about concerns with the bills giving too much authority to law enforcement and vio-lating the privacy rights of patients. on the federal level, dr. Williams and secretary James Patrick Murphy, Md, attended the american Medical association’s annual national advocacy conference in Feb-ruary and had meetings with Louisville’s elected officials.
MeMbershiP and CoMMuniCations GLMs membership reached an all-time high of 2,112 in sep-tember 2011. That represented 84 percent of physicians practicing in Jefferson county. Louisville Medicine awarded prizes in the fourth annual richard spear, Md, Memorial essay contest. The theme was “Why did you choose to be a doctor?” George John, Md, was the winner in the practicing/life member category for “The Price of Passion.” r. caleb Buege, a university of Louisville medical student, was the winner in the in-training/student member category for “The Janus Perspective.” trudi rash, Md, received an honorable mention for “a summer’s event, a Lifetime decision.” The essays were published in the July issue. GLMs published two issues of its patient magazine, vital signs, which is distributed to members for use in their practices. one issue focused on osteoporosis and the other focused on eye disease and sur-gery. GLMs continued its mobile extension of the publication called vitalsigns2Go on twitter, which reaches patients who subscribe with brief health and wellness messages. to stimulate further communication with the general public, GLMs formed a Medical Writing club under the direction of Louis-ville Medicine editor Mary G. Barry, Md. The club held three meet-ings at area restaurants for interested physicians to share their writing with each other. GLMs members continued to be served by centralized ap-plication Processing service, which handles hospital privileges, and Medical society employment services, which provides temporary, temp-to-hire and direct hire services for physicians’ staffing needs. Medical society Professional services linked GLMs members to the following quality vendors offering discounts on products and services: health care excel, health information technology consulting services; intelligent collections system, collection services; MedX12, electronic health records and practice management system; national insurance agency, specialty life and disability insurance; and national Processing company, credit card processing and other point-of-sale payment solutions.
glMs foundation The GLMs Foundation had an active year focused on its initia-tives of medical missions/indigent care, scholarships and preservation
of The old Medical school Building. The inaugural scholarship Golf tournament was held in september at hurstbourne country club to benefit medical student scholarships. Many physicians joined the 18 teams of golfers sponsored by businesses in the community. at the awards ceremony, five u of L medical students each received a $4,000 scholarship.
in January, a team of 13 volunteers organized by the GLMs Foundation traveled to nicaragua on a medical mission trip. The foundation made it possible for one u of L resident and one u of L medical student to join the trip. at the state level, the foundation was involved for the second year in recruiting volunteers for a medical, dental and vision clinic for the underserved in Pikeville in June. The GLMs Foundation awarded other grants to a variety of organizations including $10,000 to The healing Place’s Partners for hope initiative and $12,500 to supplies over seas for sponsorship of the overseas shipment of a 40-foot container with surplus medi-cal supplies and equipment. The sponsorship, made in honor of sos founder norton G. Waterman, Md, was announced during a Found-ers reception at The old Medical school Building in november.
glMs allianCe under the leadership of President rhonda rhodes, the GLMs alliance had a full year of activities for members’ spouses. From a Men’s night out at Westport village in the fall to the annual scholar-ships fundraiser on opening night at churchill downs in the spring, the GLMs alliance provided special events and opportunities for charitable work and volunteerism. in september, former GLMs alli-ance President Millicent evans was installed as KMa alliance presi-dent for the year. in March, the GLMs alliance recognized dr. Ward at its annual doctors’ day luncheon honoring retired physicians.
Note: Ellen R. Hale is the communications associate for the Greater Louisville Medical Society.
At the SOS Founders Reception, (left to right) Judy Waterman, Norton G. Waterman, MD, K. Thomas Reichard, MD, and Toni Linville, RN.
(Right) AMA Delegate Bruce A. Scott, MD, and Vice President/AMA Alternate Delegate Robert A. Zaring, MD, MMM, at the GLMS caucus dinner during the KMA Annual Meeting.
At the GLMS Foundation Scholarship Golf Tournament, (left to right) Linda H. Gleis, MD, Daniel Ontenient, Lacy Lashbrook, Kayla Lundsten, Ashley Blaske, Jonathan Feist, Toni M. Ganzel, MD, and David R. Watkins, MD.
LM
GLMS AnnuAL RepoRt 2012

24 LouisviLLe Medicine
greater louisville MediCal soCietystateMent of finanCial Position
deCeMber 31, 2011assets
current assets cash/cash equivalents $ 614,928 accounts receivable 165,199Prepaid expenses 18,671 798,798
investMents and other assetsinvestments at market value 1,906,250annuity contracts 70,569
ProPerty and eQuiPMentLeasehold improvements 113,739office equipment 188,497Less accumulated depreciation (270,025) 32,211
ToTAL AsseTs $2,807,828
LiaBiLities and net assets
current LiaBiLitiesaccounts payable $ 96,420accrued expenses 23,350unearned income 476,100 595,870
deFerred retireMent BeneFits 70,569
net assetsunrestricted 2,141,389
ToTAL LiABiLiTies And neT AsseTs $2,807,828
greater louisville MediCal soCietystateMent of aCtivities
January-deCeMber 2011changes in net assetsdues $ 745,622Louisville Medicine advertising 214,523GLMS News advertising 68,303roster sales & advertising 260,065centralized application Processing service 616,601society office services 6,659sponsorship revenue 8,615administrative fee from Medical society Professional services 54,996administrative fee from GLMs Foundation 45,000Vital Signs 72,930Website advertising 6,900other operating revenue 13,940Total operating revenue 2,114,154
investment income 72,030
Total revenues $ 2,186,184
Program service expensecommittee and general administration $ 865,830Louisville Medicine 206,200GLMS News 102,936roster 176,602centralized application Processing service 530,760society office services 4,271Vital Signs 70,860Website 26,788Total expenses 1,984,247
net increase in unrestricted net assets 201,937
Gain (loss) on sale of investments 24,673unrealized gain (loss) on marketable investments (85,760)
changes in net assets $ 140,851
GLMS AnnuAL RepoRt 2012
MAY 2012 25
the greater louisville MediCal soCietyreCognizes
the business and CoMMunity leadersWho Wore the White Coat in
2011 & 2012
PrecePtors:Mary G. Barry, Mdtimothy a. Bratton, Mddavid e. Bybee, Mdelizabeth doyle, MdPatricia Figert, Mdheather L. harmon, MdWilliam P. hoagland, Mdrobin G. Kindig, MdJohn d. Kolter, MdJohn M. Mandrola, MdJames Patrick Murphy, Mdstephen c. Payne, MdJeffrey L. reynolds, MdMatthew P. rogers, Mdregi varghese, Mdrussell a. Williams, Md
ParticiPants:shalaya Baber Jefferson county Public schools studentGary Best united Food and commercial Workers Local 227Jimmy Bornstein Bornstein Building co.vicki Buster Mountjoy chilton Medleyrusty ellison Walnut street Baptist churchscott haner yum! BrandsGill holland The Green Buildingcintya Lara JcPs studentKevin Lundy yum! BrandsJerry Miller Louisville Metro councilLabinot Prushi JcPs studentedmund roberts Jr. at&tdana shumate JcPsdave stone southeast christian churchGary ulmer Louisville BatsLouis Waterman Fore, Miller & schwartzPeggy Williford JcPs
PrecePtors:John W. arnett, MdMary G. Barry, Mdangela L. Bell, Mddavid e. Bybee, Mdalfonso cervera, Mdstephen h. church, MdLara o. Fakunle, MdJohn M. Gormley, MdKristi M. horlander, Mda. o’tayo Lalude, MdMichael W. Mccall, MdJames Patrick Murphy, Mdtracy L. ragland, Mdcharles B. ross, MdBruce a. scott, MdGordon r. tobin, Mdregi varghese, Mdrussell a. Williams, Md
* Special thanks to all GLMS physician precep-tors who volunteered their valuable time and made this program a huge success.
ParticiPants:John allen Pnc Bankashley anderson The voice-tribunerelia Bailey canaan community development corporationsteve Barger steve Barger consultingMarty Bonick Jewish hospitalteresa Bridgewaters The Mardrian GroupLarry caruso Geranda deaton uaW-Ford community healthcare initiativeKelly downard Louisville Metro councilKevin Flanery churchill downsJohn Fleming Louisville community initiativeKenneth Fleming Louisville Metro councildawne Gee Wave 3Maria hampton Federal reserve BankKaryn hascal The healing Placedevone holt JcPsrick howlett Louisville Public Mediatom hudson nth/worksGary hurt valley traditional high schoolsteve ivey Business Firststeve Jester second Presbyterian churchallen Montgomery supplies over seasKate ratliff Junior League of LouisvilleLacey smith Quick ThinkPenny smith Kentucky state universityLora tucker Girl scouts of Kentuckianatonya york-dees york Management
2012
2011

26 LouisviLLe Medicine
Dr. Wayne Tuckson asked me to appear on his “Kentucky
Health” on KET, and when it aired, Louisville Medicine asked me to share some of my experiences in the Army that were “different” compared to my civilian practice. Here are some thoughts. While seeing patients in the office, I don’t normally take phone call solicitations from salespeople and the like, but I know it was providential on a busy Monday af-ternoon, in 2007, that I took a call from an Army health professions recruiter. My first thought at the time was “Really Lord, now is the time, I am 52 years old?” My next words to the recruiter were that I bleed blue, having been the son of a career Air Force chaplain. I called the Air Force – they didn’t want me. The Army took me with no waivers. One of my motivations for saying “yes” to the Army was to fulfill a lifelong dream of serving in the Armed Forces. I had tried on three different occasions, and the door to those opportunities was always closed. One of my motivations for wanting to serve is that I come from a long line of servicemen. My great-grandfather fought for the Confederacy, my grandfather served in the Army in 1918 during the end of World War I, and my father served for 21 years in the Air Force. Dad had fought both during the Korean
B. Gordon Carnes, MD, Diplomate ABFM
hAVE BERETTA, wILL TRAVEL
Continued on page 28B. Gordon Carnes, MD, with the 12-year-old girl he treated in Afghanistan.
MAY 2012 27
IF IT’S HEALTH CARE,WE WILL BE THERE.
www.hallrender.com
THIS IS AN ADVERTISEMENT
614 West Main Street | Suite 4000 | Louisville, KY 40202 | 502.568.1890
• The largest health care focused law firm in the nation.
• Over 40 years in the health law business.
• More than 150 attorneys serving health care clients.
• Representing over 500 health care organizations nationwide.
HR_KY_GLMS2011.indd 1 5/20/2011 12:23:14 PM

28 LouisviLLe Medicine
Continued from page 26
War and in Vietnam. I wanted to serve on the battlefield as well. He had shown us some Kodachrome slides, telling of his humanitarian service in the orphanages of South Korea and the leper colonies around Bien Hoa, Vietnam. Naturally as a physician I am thinking I’ll have the opportunity to continue the Carnes tradition of altruistic service. As you may know, once you sign on the dotted line you’ll pretty much serve when and where the Army needs you at the time. I completed 29 days of the Officer Basic Leadership Course at Camp Bullis, San Antonio, to learn basic Army skills of camping out, land navigation day and night, convoy operations and weapons qualification. Then I took six weeks of Aviation Medicine at Fort Rucker to earn my Flight Surgeon wings. In 2009, I spent my first of four 90-day “Boots on Ground” obligations at Camp Eggers, Kabul, Afghanistan. I served as a General Medical Officer to a small camp of 1,400 soldiers and civilian contractors ranging in ages from 19-72. I was the only doctor for the camp and had nine medics (EMTs) working in the platoon. We had sick call for the military, followed by sick call for civilians. Afternoons were for consultations and health screening for Afghans desiring to work in the camp. For the most part it was traditional Family Medicine – just different location and different dress. I was a little nervous practicing in a somewhat austere medical environment. Camp Eggers TMC is a “Level 1-minus,” meaning we really only had the very basic capability of diagnosis and treatment. We did not qualify at that level to have an X-ray machine. One Saturday afternoon a civilian contractor, a 48-year-old man, came in with shortness of breath. He looked younger than his stated age and obviously worked out regularly, but said he hadn’t been able to the previous three days due to shortness of breath. He had also decided to quit his three-packs-a-day cigarette habit the same week. He was pale appearing, somewhat diaphoretic and tachycardic 114, and except for sinus tachycar-dia, had a normal EKG. My gut told me he was having angina. Oh by the way, his dad had an MI at age 48. The challenge was, in that location, I had no real way of confirming my diagnosis. So the new challenge involved getting him armored up, getting him and a medic into a Suburban with bulletproof glass and getting an escort in an up-armored HUMVEE to escort him five miles through Kabul traffic to a Level 2 facility to continue his care. (This sort of reminded me of the old days in Jessamine County where I practiced in the late ’80s, where the ambulance carried oxygen – and that was all – to transport people to more standard care in Fayette County.) My patient arrived at the Level 2 facility where he was diagnosed with having a non-STEMI, was med-evaced to Bagram, and then flown to Landstuhl, Germany. There he had a single vessel angioplasty and a stent placed. After the patient left, I started snooping around the supplies for the clinic and found reagent for a troponin that I could have checked on our Piccolo analyzer system. His was twice normal when he arrived at the Level 2. After that, I made it my mission, while I was there, to get an X-ray machine and Vertex reader for the clinic. The second most interesting patient I had came at the request of one of the naval officers who was an adviser to the Af-ghan National Police in the office of budget and finance. He had a translator whose daughter had been ill for eight years. He asked if
I could examine her and if so I would make him a god in the eyes of his Afghan colleagues, to have an American doctor take care of his daughter. Now the challenge was that, by AMEDD command, I was not allowed off the camp. However, with coverage by another Air Force physician doing consulting work and a special dispensation from the 30th Medical Command surgeon, we were able to steal me away in a Toyota Highlander with armored glass, improved outer tactical vest with 40 pounds of ceramic plates and our trusty 9mm Berettas. I also had the obligatory stethoscope and otolarygoscope tucked away in one of the cargo pockets of my fire-resistant ACU uniform. I was escorted into the Ministry of Defense building where my friend worked and was overwhelmed by the pungent smell of what smelled like a bunch of dirty feet – my friend thought it smelled like a urinal. Maybe we were both right. CDR Brown had described a sickly child and from what I could gather she was going to die if she didn’t get some good medical attention. I had spent the whole night before trying to remember some of the exotic pediatric conditions that I was only required to know for testing purposes. How I wished I had at least a Nelson’s “Textbook of Pediatrics” to refer to. After restless sleep I awakened at 0300, my mind still trying to conjure up conditions that I might encounter. Worse yet, I was not autho-rized to treat such in any way, shape or manner, without inciting a reprimand literally from the State Department. We got to the office, unloaded our ballistic vests and Kevlar helmets and waited for our patient. Eventually, in walked a well-dressed man who looked like he came from the Mongolian line of his Afghan heritage, with a beautiful young 12-year-old girl, impeccable in her traditional Afghan dress. She had the typical shy smile of a girl her age. So at first blush I felt a huge sigh of relief, seeing what appeared to be a completely healthy young girl with no obvious life-threatening illness. I wondered what this father feared so for his child. The father had two concerns. 1) He reported that around age 4 she had a fever and what I can best determine is she may have had a febrile seizure. Since that time she did not speak plainly. I gathered that she stuttered. 2) She was not as outgoing and gre-garious as her older sister. He had also related that he had taken her all the way to Pakistan to seek medical care for her condition. I did as much of an exam as would be culturally acceptable; it was as I suspected a normal exam. I didn’t understand the Dari language, but I really didn’t appreciate any stuttering. I spent the majority of my time after the exam reassuring the worried father that he had an absolutely beautiful normal daughter. I told him that the stuttering was a result of the seizure most likely. I advised him not to measure her according to her sister, that she clearly had her own personality. I spent my second 90-day tour with my Apache helicopter battalion in Camp Taji, Iraq, during the first four months of 2011. After I redeployed from Afghanistan, the Army implemented mandatory trauma training (Tactical Combat Medical Care) for all providers going into theater. They figured out that having IV access by a medic was wasting too much time and the mortality rate was not impacted by that sort of care. That week of trauma training was the best I had had in the Army and rated up there with my month on the Trauma service at U of L during my Family
Continued on page 30

MAY 2012 29

30 LouisviLLe Medicine
LM
Continued from page 28
Medicine internship. I was amazed at why our service members were dying on the battlefield. We have done an excellent job of providing protective gear for the thorax and abdomen, so the majority of wounds are of the extremities. The course focused on controlling the three most common causes of mortality: exsan-guinations, airway compromise, and, surprising to me, hypo-thermia. The week included classroom instruction, mannequin training, cadaver lab and live goat lab (well-protected under the watchful eye of PETA). By the end of the week, I felt confident that I could control hemorrhage from an amputation (60 per-cent of amputations were dying due to either improperly placed or inadequate tourniquet application), deal with the collapsed lung, manage the airway, get interosseous IV access, do initial assessment of eye injuries, control hypothermia and prepare the patient for transport to definitive care. We would have an op-portunity to apply our knowledge shortly after Osama bin Laden was killed, when professionals were brought in to attack our base with mortars: 51 rounds were walked through the housing area and our flight line in the course of a half hour. When the big voice announced the all clear I ran to the TMC in my PT uniform with my trusty 9mm (never leave home without it.) We had trained as a unit for mass casualty care, so the TMC was actively moving stretchers and preparing to triage all, any-one from the walking wounded to the expectant (dying). All was in place when the first up-armored ambulance showed up from the flight line. A single soldier with his shoulder all bandaged up walked himself off the ambulance. He had been on the flight line working on the helicopters when the attack started at 0430. He
did the right thing in lying on the ground behind a T-wall barrier; however, his shoulder and head were exposed. A round landed approximately 15 feet from his position and he took a piece of shrapnel in the left deltoid. Three inches more superior, and it would have been fatal. We bundled him up literally, put him on a helicopter to Baghdad, then to Landstuhl for surgery and pro-longed antibiotic treatment. This sort of wound was extremely contaminated. Miraculously, that day we had a ruptured ear drum and a leg laceration. The majority of wounded we saw for screen-ing, for anxiety and mild Traumatic Brain Injury (we only had one TBI that required brain rest and limited duty, with full recovery). What I learned that day and in the TCMC course was that to have a casualty is absolutely a random act. We were fortunate. Another base shortly thereafter had five casualties from a direct hit from a mortar. I don’t get to know how I affected these three patients’ lives in the grand scheme of things, but I’d like to think I helped the 48-year-old civil servant get proper care as fast as possible to save him from a massive MI; that I saved the social life of that little girl in a society that believes that imperfection physically or other-wise makes you unmarryable and therefore of no value; and that gratefully I had reassured the soldier that it was not his fault for getting wounded. It is my prayer that the father listened and took to heart my encouragement about his charming daughter.
Note: Dr. Carnes practices Family Medicine with Jewish Physician Group-Sun Valley Family Care. He is a lieutenant colonel, Medical Corps, flight surgeon in the U.S. Army Reserve’s 8-229th Aviation Regiment (Attack) at Fort Knox.
• ForGLMSmembersonly• DownloadtoEHRsystem• Oneyearlicenseagreement• AccessselectGLMSmember informationonline24/7• Reducesstafftime• Affordabletiered-pricingbasedon practicesize
Formoreinformationcontact:CheriK.McGuire,DirectorofMarketing

MAY 2012 31

32 LouisviLLe Medicine
Davao City, PhilippinesApril 1, 2012 It is April Fools’ Day in Louisville, Ken-tucky, where for nigh 40 years my late hus-band and I made our home. There we raised our son and daughter. Now Ric is gone, but
our six grandchildren still grace the place with their intermittent presence. The news of the hour, by cell phone, is that U of L lost to UK in the NCAA Final Four, but grandson Marc is staying for the championship game in New Orleans before heading for home. On the other hand, coming to Davao to spend the Easter holidays with my siblings and their families was a treat I had designed for this year. My journalist sister met me with a welcom-ing gift, a collaborative book written by 19 contemporaries titled The Davao We Knew. Each wrote of their recollections of this city where they, and incidentally, I too, grew up. In various ways, they touched on the history, prevailing customs and culture of those times including World War II and their relationship with the Japanese invaders and the American liberators, and the city of Davao’s transitions to what it is today. Fascinating, inspirational and personal, their stories marched the reader down the aisles of memory, challenging others to join them. Here is a snippet of mine. In 1936, my 29-year-old father, a government surveyor of the Philippine Commonwealth under the USA, was assigned to survey part of Davao Province in the large island of Mindanano to the south. Despite fears of the unknown and of the fierce Moros (Muslims, called that by the Spanish), Davao had become fabled as the land of opportunity. Davao Province had fertile lands to cultivate and abundant natural resources. As in the days of the Wild West, an exodus from the populated north headed down to form a melting pot of eager enterprising people in quest of a better life. Among these were Japanese laborers who manned the abaca plantations and brought their families with them. There were so many of these Japanese nationals that Davao was dubbed “Little Tokyo” by the time Japan joined WWII. I was 12 when Japan bombed Pearl Harbor on December 7, 1941. Because I was boarded with nuns in an exclusive Catholic high school, my parents could not retrieve me home in time. When the Japanese forces invaded Davao on December 20, the nuns and their charges fled to the adjoining farms. Anyone visible from the air was fired upon by Japanese planes. Anyone caught was herded back to the city. A “Juez de cutsillo” (judge by knife
or kill on sight) was imposed on all white peoples. That included our then-French Canadian missionaries. We heard of atrocities committed against women. That drove us deeper into unknown territory, the jungles. Thus, for the next three months, we walked away from the city and Japanese-occupied towns, surviving on abandoned root crops, edible palms and whatever the jungle had to offer. One day, our band of 13 came upon the fresh skin, feet and bones of a deer that a previous group had left behind. We boiled and feasted on these, the first meat we had had in weeks. Leeches and mosquitoes were a constant nuisance. We did not have salt. This was freshwater inland country. To get out of the jungle we had entered, we had to negotiate a currentless mass of marshes and swamps as far as the eye could see. Fortunately, floating on the marsh was an edible water plant called kangkong. Our dietary needs were taken care of for the next month. On a bamboo raft, with the aid of a native guide, we reached the big Agusan River where then we could follow the current to a mis-sionary post of two Belgian priests. They served us a real meal on real dishes on a table with tablecloths. What luxury! Many over-ate. To their chagrin, they spent the rest of the night visiting the smallest room in that small rectory. Once more we were able to travel freely. My family, in the meantime, continued to search for me via news carried by bands of evacuees. Having been found by my uncle, we left the nuns and teachers at a sister convent and took another route via the sea, taking a sailboat going south along the east coast of Davao. We made very slow progress. Sometimes, the wind died down and we would be dead in the water for a day. When the wind picked up but in the opposite direction of where we were headed for, we would tack back and forth, thus making little headway. In September of 1942, a year and three months after I was left at boarding school, my uncle and I reached my parents and sib-lings in the mountains of Manay. My father, sought by the Japa-nese because he was a government official, had made a slash-and-burn farm in the forest to feed the family. I had blossomed into a young adolescent and was introduced to a new baby sister, 9 months old, born in my absence. We sat out the war in the mountains, making friends with the native people and adopting their ways of survival. We learned to boil the bark of the chincona tree to cure malaria, roasted the best corn tamales in raw bamboo tubes, recognized a tree whose shaved bark worked like soap, sneaked out to the sea and re-duced seawater to make salt, making sure the smoke did not alert Japanese patrols, treated scabies by ferreting out the mites with a pin, made rice cakes for the roving guerrilla armies. My father taught me to play a bamboo flute whose dulcet sounds floated among the trees and carried on to the next hill at night. We oc-casionally rented the guitar of a tubercular person by paying him with chicken eggs and accompanied our songs with it. Our only reading material consisted of a set of volumes of the Classics that Papa’s friend had left on his farm. Thus my sister and I tried to figure out the tragic romance of Tolstoy’s Anna Karenina and the dreams of Dickens’ Scrooge at about that time. Soon we saw double-bodied American planes in the sky and knew liberation was near. We moved back to town when the Japanese left and resumed our peacetime lives. Thanks be to God! We had survived!
Note: Dr. Oropilla is a retired psychiatrist.
Teresita Bacani-Oropilla, MD
snippets of World War II Memories
LM

MAY 2012 33
✓ Business Accounts
✓ Commercial Loans
✓ Lines of Credit✓ Equipment Leasing
✓ Personal Checking
✓ Mortgage Loans✓ Special Mortgage Programs
for Medical Residents & New Physicians
Chairman and CEO - Republic Bank
Looking for a Bank That Understands
Your Special Needs?
We were here for you yesterday. We are here for you today.
We will be here for you tomorrow.®
JOHN MASONSenior Vice President, Private BankingUniversity of Louisville PhysiciansNMLS ID# 419162
P 588-1600F 498-1271E [email protected]
AMY BROWNVice President, Private BankingNorton HealthcareNMLS ID# 419158
P 560-8617E [email protected]
ASHLEY ROBERTSAssistant Vice President, Banking Center ManagerBaptist Hospital EastNMLS ID# 419157
P 394-4483E [email protected]
MISSY KAISERAssistant Vice President, Banking Center ManagerJewish HospitalNMLS ID# 419180
P 420-1847E [email protected]
We’ve Been Serving the Medical Community for Over 25 Years.
Steve Trager
34 LouisviLLe MedicineLOUISVILLE MEDICINE8
WeProvide:• Direct placement• Temporary placement• Temp to hire
WeGuarantee:• Criminal backgroundchecks
• Reference checks• Credit checks• Drug screening• Skills testing
Serving greater Louisvilleand southern Indiana witha 60-year track record ofquality and dedication.Call Ludmilla Plenty,employment director,at 502-736-6342 or visit usat www.glms.org.

MAY 2012 35
IN REMEMBRANCE
Mchenry s. BreWer, MD(1922-2012)
McHenry Brewer, who died on February 19, was a general sur-geon in Louisville from 1955 until his retirement 40 years later. He received his surgical training in New York City at Columbia Pres-byterian Hospital and Cornell New York Hospital, where he became chief resident. He practiced alone at first and then together with Dr. Hart Hagan for some years, and worked at the old Baptist Hospital, the Method-ist Hospital, the Norton Infirmary, Children’s Hospital and St. Antho-ny’s Hospital. This was in the old days before cell phones and radios, so keeping up with him was quite a trick. In later years, he worked mostly at Baptist Hospital East. He was pleased to welcome his son, Dr. Judson Brewer, into his practice in 1988 and delighted in teaching him and the other surgical interns who spent time in rotation with him on his daily rounds. He was known for his kindly ways and irreverent sense of hu-mor, and was loved by his patients and fellow doctors and nurses. He was always on call for many years and seemed to have boundless
energy. He was the loving hus-band of the former Cecy Norman and was the proud father of Jud, Charles and Mary. He loved games of all kinds, from backgammon and bridge to tennis, golf and croquet, and was the kind of competitor that people loved to beat. He was the president of the Jefferson County Medical Society in 1972-73 and was president of the staff at the Baptist Hospital and the Methodist Hospital in the ’70s. He also was the president of the Southern Society of Clinical Sur-geons in 1974. As he neared retirement, he could spend more time in the mountains of North Carolina where he had a summer home and could play endless rounds of golf and croquet and did some hiking. He had a knack for friendship and fun but also was serious and studious and believed in honesty and the Golden Rule. In the last five years, he was seriously impaired by a series of strokes and proved he could be a brave patient as well as a doctor.
–Cecy Norman Brewer
LM

36 LouisviLLe Medicine
w E w E L C O M E Y O U
P H Y S I C I A n S I n P R I n T
GLMS would like to welcome and con-gratulate the follow-ing physicians who have been elected by Judicial Council as provisional members. During the next 30 days, GLMS members have the right to sub-mit written comments pertinent to these new members. All com-ments received will be forwarded to Judicial Council for review. Provisional member-ship shall last for a period of two years or until the member’s first hospital reap-pointment. Provisional members shall be-come full members upon completion of this time period and favorable review by Judicial Council. LM
Ali, Jermaine Ash-Shahid (31026)Marlyce Hill Ali, MDBingham Child Guidance Clinic 200 E Chestnut St 40202852-1034Psychiatry U of Louisville 08
Eads, Emily Dawn (30918)222 S 1st St Ste 501 40202583-2731Diagnostic Radiology 11 Duke U 06
CAnDIDATES ELECTED To PRoVISIonAL ACTIVE MEMBERSHIPChugh, Atul R (30992)401 E Chestnut St Unit 310 40202584-8563Internal Medicine 06 U of Pune 01
Kad, Surinder Kumar (30891)400 S 6th St 40202574-2080Internal Medicine Nephrology Punjabi U 74
Kenagy, David Neil (30948)RobinUniversity Children’s Kidney Specialists LLC Pediatrics 86,95,04 Pediatric Nephrology 08 Jefferson Medical Coll 81
Koenig, Heidi M (17067)Wm. W. Holt, MD, PhDUL Anesthesia 530 S Jackson St 40202852-1735Anesthesiology 93,09 U of Nebraska 85
CAnDIDATES ELECTED To In TRAInInG
Walker, Rebecca Paige (12138)Norbert J. Burzynski, Jr601 S Floyd St Ste 350 40202 629-2030Obstetrics Gynecology 01,06-11 Mercer U 95
Yunker, Jacob J (17048)Tosha4121 Dutchmans Ln Ste 410 40207897-9881Internal Medicine 08 U of Louisville 03
Aqil F, Gupta A, Munagala R, Jeyabalan J, Kausar H, Sharma RJ, Singh IP, Gupta RC. Antioxidant and Antiproliferative Activities of Anthocyanin/Ellagitannin-Enriched Extracts From Syzygium cumini L. (Jamun, the Indian Blackberry). Nutr Cancer. 2012 Apr;64(3):428-38. PubMed PMID: 22420901.
Billeter AT, Polk HC Jr, Hohmann SF, Qadan M, Fry DE, Jorden JR, McCafferty MH, Galandiuk S. Mortality after Elective Colon Resection: The Search for Outcomes that Define Qual-ity in Surgical Practice. J Am Coll Surg. 2012 Apr;214(4):436-43. PubMed PMID: 22397975.
Bozeman MC, Ross CB. Intra-abdominal hypertension and abdominal compart-ment syndrome in association with ruptured
abdominal aortic aneurysm in the endovas-cular era: vigilance remains critical. Crit Care Res Pract.2012;2012:151650. PubMed PMID: 22454763.
Byrnes KR, Ross CB. The current role of carotid duplex ultrasonography in the management of carotid atherosclerosis: foundations and advances. Int J Vasc Med. 2012;2012:187872. PubMed PMID: 22489269.
Cannon RM, Smith JW, Franklin GA, Harbrecht BG, Miller FB, Richardson JD. Flail chest injury: are we making any progress? Am Surg. 2012 Apr;78(4):398-402. PubMed PMID: 22472394.
Cannon RM, Legrand R, Chagpar RB, Ahmad SA, McClaine R, Kim HJ, Rupp C, Cho CS, Brinkman A, Weber S, Winslow ER, Kooby DA, Chu CK,
Staley CA, Glenn I, Hawkins WG, Parikh AA, Mer-chant NB, McMasters KM, Martin RC, Callender GG, Scoggins CR. Multi-institutional analysis of pancreatic Adenocarcinoma demonstrating the effect of diabetes status on survival after resection. HPB (Oxford). 2012 Apr;14(4):228-35. PubMed PMID: 22404260.
NOTE: GLMS members’ names appear in boldface type. Most of the references have been obtained through the use of a MEDLINE computer search which is provided by Norton healthcare Medical Library. If you have a recent reference that did not appear and would like to have it published in our next issue, please send it to Alecia Miller by fax (736-6363) or e-mail ([email protected]). LM

MAY 2012 37
We fight frivolous claims. We smash shady litigants. We over-prepare, and our lawyers do, too. We defend your good name. We face every claim like it’s the heavyweight championship. We don’t give up. We are not just your insurer. We are your legal defense army. We are The Doctors Company.The Doctors Company built its reputation on the aggressive defense of our member physicians’ good names and livelihoods. And we do it well: Over 82 percent of all malpractice cases against our members are won without a settlement or trial, and we win 87 percent of the cases that do go to court. So what do you get for your money? More than a fighting chance, for starters. Our medical professional liability program is exclusively endorsed by the Kentucky Medical Association. To learn more about our benefits for KMA members, call Frank Buster or Gary Noel at (800) 338-7148 or e-mail [email protected].
Exclusively Endorsed by
www.thedoctors.com
A3743_KY_LouisvilleMed._Defend_May2012_12.indd 1 3/7/12 2:17 PM
Wow, how time flies when you are having fun. I can’t believe how quickly my year as president has gone. I have truly felt hon-
ored to be the GLMS Alliance president for 2011-12. I look forward to continuing my relationship with the GLMS Alliance and hope our future is bright. On February 7, 2012, my oldest son, Travis, was diagnosed with leukemia. He is 32 years old with a wife and three beautiful children. He is continuing to do well with his chemo, and his prognosis is good. But the reason I am sharing this sto-ry with you is because of the many GLMS Alliance friends and family who have been here to support me during all of this. Our GLMS Alliance members all rally around when one of us is in need. Travis lives in northern Kentucky, and the out-pouring of support from my KMA Alliance members as well as the former Southern Medical Association Alliance president, Dr. Nancy Swikert, was a true blessing. If you ever want to know what the
GLMS Alliance does for you, it is easy to see. I have developed many friendships during my time with the Alliance on all three levels. If I had not taken that step to get involved and become a member, I would never have had the opportunity to meet such amazing people. I feel the GLMS Alliance does great things and gives us an opportunity to give back to our community through education. We have had the ability to support the Pulse of Surgery program through volunteering as well as the School Choice program. Our legislation chair, Dean Furman, has kept us abreast of the many changes in health care. We need to be the advocates for our medical community. It may be a phone call or a letter, but it does make a difference. I hope in some way the work I have been able to do this past year through the GLMS Alliance has made a difference. I have truly enjoyed working with each and every one of the people on my board and members of our organization. Their love and support have
been priceless. We attended opening night at Churchill Downs on April 28. We had more than 150 GLMS Alliance members and friends enjoy night racing at its best. If you have not ever had the opportunity to attend this event, it is lots of fun and a great way to kick off the Derby week. We will have our Annual Meeting on May 8. Adele Murphy, wife of Dr. Pat Murphy, will become the new GLMSA president for 2012-13. I hope you all will consider supporting her in the year ahead. Note: Email Rhonda Rhodes at [email protected].
Rhonda RhodesGLMSA President
LM
At the Doctors’ Day luncheon on March 30, (left to right) President Rhonda Rhodes, honoree Will W. Ward Jr., MD, GLMS Executive Director Lelan K. Woodmansee, CAE, and President-Elect Adele Murphy.
A L L I A N C E N E w S

38 LouisviLLe Medicine
There’s a guiding philosophy To Mag MuTual’s efforTs to defend your reputation: Whatever it takes. Claims committees staffed 100% by physicians. An exhaustive review and medical opinion for every claim filed. Outside help, when needed, to prepare a physician for deposition. Deep exploration of the best available expert witnesses. A detailed game plan weeks before trial. Testing the defense with focus groups. Mock trials. Continuous involvement of MAG Mutual’s claims specialists.
Much of the above represents an “expense” to other carriers – an expense they often don’t want to pay. So, they’re often inclined to settle. But settling just to avoid cost isn’t in the best interest of the physician, whose reputation, life and livelihood are at stake.
We defend.
Mag Mutual
Rusty Wells 1-888-642-3074
neace lukens
Chuck Durant 270-393-6218
hayes, utley & hedgspeth
Todd Sorrell 502-493-7974
for more information contact one of the agents below:
MAG Mutual... a clear advantage.A.M. Best A (Excellent) rating
Insurance Products and Services are issued and underwritten by MAG Mutual Insurance Company and its affiliates.

Bans from Bozos In March the New York City Board of Education released a list of 50 words it
would henceforth ban from appearing in new test materials written for NYC stu-dents. Four days later, after an onslaught of criticism, the board backed down. “After reconsidering our message to test publishers and the reaction from parents, we will revise our guidance and eliminate the list of words to avoid on tests. We will continue to advise companies to be sensi-tive to student backgrounds and to avoid unnecessary distractions ...” In a word, only a bozo would believe that banning specific words is either realistic or right. Hurtful or obscene words are all over the Net. They’re everywhere in music, in print, and in everyday speech. They are broadcast across the nation on talk radio and on TV shows. Movie ratings do little to protect young ears; parents are supposed to do that. But a child who can read, or tune a radio, or download a song, a tweet, a post or an article has access to the words of the world. The very notion that a board of education can censor a test, and that censoring a test might keep a child from feeling unpleasantly distracted, is idiotic. As for test design, no principled writer for schoolchildren would ever choose words that are outright ugly – racist slurs, etc. – out of sheer good manners and good judgment. So which dangerous words were, at least for a while, banned? (You highly sensitive hothouse flowers should cover your ears, or flee from the room in tears now.) May I have a drumroll?
“Birthdays.” Horrors! One might have to produce a non-Kenyan birth certificate. “Bodily functions.” I’d prefer you didn’t say wee-wee, but I can see how a 5-year-old might. “Alcohol, tobacco or drugs.” As if kids didn’t already, sadly, know firsthand. “Cigarettes.” Smokers pay more taxes than I do – ha ha. “Computers in the home.” Feeling underprivileged? Some kid never realized she was dirt-poor till she read this on a test, because the lack of food and shelter hadn’t clued her in? Jeez. “Crime.” CSI, thy name is legion. “Death and disease.” Dickens is not just rolling, he’s somersaulting in that grave. “Divorce.” Shh! Don’t tell Tammy Wyn-ette. “Evolution.” Ah – the creationists try to put their oar in here. Notify Steve Beshear; we don’t want the Ark business to fall off any. “Homelessness.” A New York City kid who isn’t homeless sure can’t hide his eyes from those who are. “Hunting.” No Harry Potter? No Hunger Games? No Daniel Boone? No SEALs Team Six?? “Junk food.” The real motto of McDon-ald’s: “Resistance is futile.” “Nuclear weapons.” You mean they don’t have civil defense drills where you sit in the hallways with your head down in NYC? After 9/11? Hell, they have evacua-tion drills, anthrax drills, even mass casu-alty drills there – in kindergarten. “Politics.” One must discuss politics, or how else could lying be explained to little ones? “Poverty.” Chapter 72: “Dick and Jane Go to the Unemployment Office and Wait in Line for Three Days.” Chapter 73: “Dick and
Jane Beat Up a Homeless Guy and Steal His Tarp.” “Religion.” Have you heard about the guy who strapped his dog Seamus to the roof of his car? Is that some new religion? “Rock and roll music.” I miss Jumpin’ Jack Flash. “Running away.” The cherished dream of every child at some point, immortalized in Peter Pan, but far too suggestive for the Bronx? Maybe it would play better on Broadway … “Sex.” Have they heard of Rush Lim-baugh? No? Thank God. “Slavery.” Yeah, let’s hide our nation’s past from its present, and call it education. “Terrorism.” In a city where Ground Zero is a shrine: Let’s just call them the Board of Buttheads. “Vermin.” Have they seen the cock-roaches in Chinatown? Maybe they have bedbugs on the brain. “War and bloodshed.” Hard to study history that way – do we call it the Civil Conflict then? Did everybody get a trophy at the end? “Weapons.” Make My Day. “Witchcraft.” Inevitably, uppity women are the villain. Let’s ship the Board of Bozos to Salem with little charms around their necks and see what happens. Censorship doesn’t pay. The power of Twitter fueled the Arab Spring, and even though totalitarian regimes will always find a way to harness their words against them, people under the boot of dictators will always speak out, as bravely as they can. That’s what we should be teaching children: Speak truth to power. Do the right thing, even when no one is watch-ing. Stand on principle and mean it. Even if
MAY 2012 39
Mary G. Barry, MDLouisville Medicine [email protected]
SpEAk YOUR MIND
Continued on page 40
The views expressed in Doctors’ Lounge or any other article in this publication are not those of the Greater Louisville Medical Society or Louisville Medicine. If you would like to respond to an article in this issue, please submit an article or letter to the editor. Contributions may be sent to [email protected] or may be submitted online at www.glms.org. The GLMS Editorial Board reserves the right to choose what will be published.

The Social history (Sh) “PSH: 1pkg cigs/d.” With the habit of young doctors writing always in abbrevia-
tions, my medical records are filled with house staff gibberish worthy of Molière’s “Médicin malgré lui.” Indeed the Cur-rent Procedural Terminology (CPT2012) considers that a history of “tobacco” use qualifies for a billable bullet point as social history. As we move into the computer environment, checking the box “smokes cigarettes” will produce a sentence in the narrative medical record, “The patient admits to smoking cigarettes.” If I use the drop-down menu to document a frequency of one package per day, the narrative will instantly change to, “The patient states he smokes one package of cigarettes a day.” In the final reconciliation for charges, a point of social history could increase the CPT code for reimbursement. Such is the progress of the degradation of our profession and the English language as mandated by government. I find it much more interesting to ask where the patient smokes and with whom. I know that my clinic workers take off together to smoke a few paces outside the medical center non-smoking zone. It is not so much the smoking as being together with windbreakers in the cold – they prob-ably do not inhale much. My young high school senior with the distant affect, and dissociation from the consequences of his injury, told me he smokes “alone.” Today’s youngsters smoke in groups and often pass the cigarettes one to the next. My fellow’s “alone” is the real social history. Of course the computer record is not language-specific. In the future, it is theoretically practical to produce an entire medical record in, for example, Chinese, by ticking the appropriate boxes in the computer and creating a narrative in a language other than the language used
for the data entry side of the program. We tried an English-to-German computer translator for some letters to a colleague in Frankfurt a few years back. It generally works, but the result when automatically transposing the English “vice chairman” into computer German was amusing. The computer rendering was “director for crime prevention.” Returning to the business of the billable record, CPT allows one bullet for “Marital status and/or living arrangement.” Since CPT is not state-specific, the question would have varying implications depend-ing on the law, as it varies in the defini-tion of marriage from state to state. I was operating on the elbow of a young lad who had two adult men, one older and one younger at the bedside. Oh hello, I said. And stepping awkwardly into the situation, I then said to the younger of the two, “You must be the father and is this the grandfather.” The immediate and unembarrassed response from the boy was, “This is my Dad, and this is my Daddy.” I retreated: This was a situation probably not easily documented in a drop-down menu. I am not sure that asking generically, “Are you married?” is the best way to go about this part of the social history. Most people in the United States are not married, and the term marriage can have political and also religious implications, to which we have alluded. Asking about marriage without having the subject brought up by the patient subtly places the examiner in a judgmental or perhaps politically incorrect position. The question, “To whom are you married?” is theoreti-cally not allowed in a job interview. So I usually ask, “With whom do you live?” This question works. In one case the patient re-sponded, “I live alone.” So I opined looking at the nice lady of about the same middle age who brought the patient to the office, “This must be your sister then.” No, I had stepped into it again. “No,” he replied, “this is my wife.” When
sorted, it turned out that they live in houses near each other, often eat together and walk their dogs together. But as for “living arrangement,” they do not actually live together. This is really social history. My single best question for social history is, “Do you have any pets?” One patient was affronted and demanded to know, why are you asking, what is it to you? I answered that the social history was now required by our president in order to com-plete the medical record and get paid. This is not entirely true. Remember that billable events are generated automatically by the computer from checking boxes in the data entry system. Free texting, no matter how detailed, in medical records generated at the beginning of the 21st century pro-duces an entry that indeed is in the final record but is one which will not be used in the tally of checked boxes that creates the charge for level of service. One old couple shared with me the loss of their beloved cocker spaniel, Checkers. With encourage-ment they acquired Winston, and the new brightness this little dog introduced into their lives was evident. This aspect of doc-toring comes only from taking the social history in its richest sense. The breed of dog tells a lot about its owner. The cocky young man with the tattoos sports a rottweiler. The gruff farmer drives around on his tractor with his Chihuahua. I still do not know what to make of the family with the three Jack Rus-sell terriers, the German shepherd and the ferret, but I did find out that the ferret is in charge. Has medicine made progress? We have moved from the Latin gibberish of Molière’s “Sganarelle ou Le Cocu” (the Imaginary Cuckold) to my resident’s “pkg cigs/day.” The next step in this process apparently is the introduction of the computer, in the form of the EMR, which promises further to suck the life out of our profession by putting the emphasis on “bullet points.” These, of course, can be counted up to prove the value of the
you have to say words that are upsetting, like “Violence.” Learn something about the past, so that your future has meaning, even if you never win “Expensive gifts, vacations, and prizes.”
There’s just one category that would never fly in Louisville, ever: “In-depth discussions of sports that require prior knowledge.” You want the kid to secede from his state? I rest my case.
Note: Dr. Barry practices Internal Medicine with Norton Community Medical Associ-ates-Barret. She is a clinical associate pro-fessor at the University of Louisville School of Medicine, Department of Medicine.
40 LouisviLLe Medicine
Continued from page 39
LM
David Seligson, MD

MAY 2012 41
service provided. Remember, as you treat patients, to look up from the computer screen, meet the patient as a human fel-low traveler and preserve the true value
and esteem in providing compassionate medical care.
Note: Dr. Seligson is professor and vice
chair of the University of Louisville School of Medicine, Department of Orthopaedic Surgery, and practices with Orthopaedic Trauma Associates.
Letter to the Editor I read with interest the letter from Dr. Timir Banerjee re-sponding to Dr. Tracy Ragland’s article on
nurse practitioners and the proposed leg-islation that would eliminate the need for consultation and collaboration with physi-cians in practice. I think that Dr. Banerjee has missed the point completely. No one is questioning the value of nurse practi-tioners, their capabilities or their goals of serving patients. I, too, as I am certain does Dr. Ragland, consider them my colleagues in practice. It is simply a fact, however, that the practice of medicine requires a certain minimum level of education, training and experience to be able to effectively provide the diagnostic and therapeutic armamentarium that patients require and deserve in their encounters with providers of health care. If it were not so, we would be stepping backward into the pre-Flexner days of preparing physicians. Even though I am quite confident that he is respectful of such a person, I am certain Dr. Banerjee would not have a less than fully educated and trained practitioner performing neurosurgery, even if such a practitioner claimed his education as an optometrist should permit it. This minimal level of education, train-ing and experience is obtained through a four-year medical school curriculum,
followed by graduated responsibilities for independent patient care during post-graduate residency training, for another four or more years. The idea that a master degree-trained nurse practitioner, or even a DNP “doctor nurse,” could without the benefit of such education and experience replace a physician is without any realistic basis. For those who say they can diag-nose wellness or disease and then simply refer for care anyone with a disease, I would respond that the diagnosis of well-ness is the diagnosis of absence of disease and that referrals require some basic knowledge of the wide range of disorders from which the human population could suffer. Without that wide range of knowl-edge, patients are ill-served, unneces-sary testing is performed, inappropriate referrals are made and delays in diagnosis and treatment put patients at risk. No one places blame on all nurses for one nurse’s misdiagnosis, but a system that fosters such mismanagement of patient condi-tions is to be condemned, not written into law. Once again, those who have not taken the time or effort to become physicians through legitimate routes are attempt-ing to become physicians by legislation, regardless of what they are called. You can call an elephant a bird to confuse and distract, but it will never fly, no matter how much it may want to. For those who think that the training and education of nurses permits them to be replacements for physicians, it is good to remember the ancient philosopher
who said that to a bird who has known no world outside his cage, the world IS his cage. The same is true when it comes to limitations of knowledge in medicine. A limited knowledge base can only be rec-ognized by those who have a wider and more in-depth fund of knowledge. The current and seasoned system of collaboration between physicians and advanced practice nurses has proved beneficial. It permits an expanded pool of health care providers with the necessary safeguards of physician oversight and professional collaboration. To take a step backward by legislative fiat would be a terrible mistake. I trust that my physician colleagues will not further mistake actions and opinions that are intended to safeguard the public from unprepared practitioners of the art and science of medicine as attacks on the nursing profession or those nurses who have worked hard to prepare themselves for collaborative practice with physicians. By all of us working together, utilizing our unique skills and knowledge, a team of professionals providing health care in a collaborative system ensures patient safety, practice efficiency and an expand-ed pool of qualified health care providers all practicing within a scope of practice for which they have been appropriately educated, trained and mentored.
Note: Dr. Griffin practices Obstetrics and Gynecology with Women’s Care Physicians of Louisville.
Larry P. Griffin, MD, FACOG
LM
LM
Letter to the Editor After reading Dr. Timir Banerjee’s as-sessment of my article regarding nursing leaders’ efforts to win
the right for APRNs to practice medicine as independent physician substitutes without oversight by or collaboration with physicians, I felt that I needed to
clearly state my reason for writing it. My sincere intent was to help educate GLMS readers about the issue, in the interest of patient health and safety. Specifically, I have no interest in “self-aggrandizement” and would never attempt to elevate my medical practice to something it is not. As a general internist and pediatrician, I respect nurse practitioners and appreciate their contributions to primary care and other specialties. However, given the great responsibility for patient care that comes
with the practice of medicine, I hope that nurse practitioners will continue to work in office settings, urgent care clinics, com-munity health centers and hospitals as in-tegral members of teams led by physicians so that all patients in Kentucky will have better access to high-quality, affordable health care.
Note: Dr. Ragland practices Internal Medi-cine and Pediatrics with Internal Medicine & Pediatrics Associates.
Tracy L. Ragland, MD
LM

42 LouisviLLe Medicine
Letter to the Editor In preparing the series on the history of the University of Louisville School of Medicine, I find many
errors in previous accounts. I know my ar-ticles will also have errors, in spite of best efforts otherwise. Dr. Morris Weiss is a leading Louisville medical historian and the only Louisville physician to have interned at the Philadel-phia Hospital. He has supplied the follow-ing corrections to my March article: “On page 16 of the article you write about Dr. Thomas Bond in America’s first public hospital, Philadelphia Hospital. Let me make a correction
please. In 1731 the City of Philadelphia established the Alms House and House of Employment for the care of the aged and infirm, but it was not until 1769 that a physician was appointed to care for the inmates. One of these two physicians was Thomas Bond. In 1836 the Alms House was officially designated Philadelphia Hospital and Alms House. In 1902 the name Philadelphia General Hospital was given to the institution. Pennsylvania Hospital is dated to 1751 and is the first true hospital in America with a physician on staff. The managers of Philadelphia Alms House for many years sent their sick inmates to Pennsylvania Hospital for treatment and paid for their maintenance of the wards. In Benjamin Franklin’s autobiography
he disclaimed the credit for first suggesting the project and ascribed to Dr. Thomas Bond the idea of Pennsyl- vania House. However, Franklin made it happen and raised the funds.” Louisville has many fine historians, like Dr. Weiss. I ask that you bring any errors I make to my attention at [email protected] or (502) 852-6880, and I will endeavor to correct the record. Also, I wel-come any additional information, insights or comments on this remarkable story. Let’s keep alive the exceptional medical history of this community. Note: Dr. Tobin is a professor at the Uni-versity of Louisville School of Medicine, Department of Surgery, Division of Plastic and Reconstructive Surgery. He practices with University Surgical Associates.
Gordon R. Tobin, MD
LM
Board Certified Family Practice Physician NeededHealthstat Inc will be opening an on-site employee health clinic in
Louisville, KY for GE (General Electric)Theon-siteclinicprovidestheopportunitytoperformafull-arrayofmedi-calservices.Thegoaloftheclinicistoalleviatetherisingcostofhealthcarebyimprovingthehealthofemployees.Partofyourrolewillinclude: Educating,explaining,andmonitoringhighhealthriskintervention, diseasemanagementandprimarycare Developinganindividualhealthcareplanforeachemployeetolower healthrisks Diagnosingandtreatingchronicdiseasesandacute/episodic occurrencesthroughtheuseoflabsandprescriptionmedication Servingasanextensionoftheirsupervisingprimarycarephysician Referringpatientswithcomplexmedicalproblemstoaprimary physicianorspecialist Implementingwellnessprogramsforweightmanagement,diabetes management,andothertopics
Send resume to:RandyMack
704-529-6161(office)704-323-7931(fax)

MAY 2012 43
PHYSICIAN OPPORTUNITYMD/DO Part-time position available in Lexington and Florence, KY. Please visit our website at chambersmedical.com.
No call required. All specialties considered. We are willing to train.
Please email current CV [email protected].
B U S I n E S S C A R D G A L L E R Y
"We specialize in medical office cleaning"
Contact us today for a free estimate:(502) 587-7675 (800) [email protected] www.divisionone.us
MEDClean
Condo for rentCondowithtwobedrooms(fourpersons)atHarrisonHotSprings-Fraziervalleywithfunctionalkitchen—VancouverBCavailableforrentonlargelake.Facilitiesforboating,hiking,golfing,fishingforsalmonandviewingeagles.Excellentviewofmountainsandwaterfromtwodiffer-entbalconies.EasydrivetoferryforVancouverIsland,328Esplanade.Internetavailable.$2200.00for8days.IfinterestedemailTimirb@aol.comorcallTimirBanerjeeat502-386-4466.
COnDOFORREnTTwo bed room condo atKaanapali Beach—Maui
available from December 15-December 22, 2012for $2200.00. If interested please
contact Timir Banerjee 502-386-4466 or email [email protected].
MEDICAL OFFICEAVAILABLE IN NORTON COMMONS,
TIME SHARE, FULLY EQUIPPED, READY TO START NOW,
CLOSE TO NORTON BROWNSBORO HOSPITAL.CALL ENESA AT 502.523.3348.
Prime East End Office SpaceDupont Circle area, 1400 sq. ft. 3 offices+ Conf. room (may be converted to add’l space if need-ed). Reception area, bathroom, small kitchen with access to appliances, storage/supply room. Phone/Internet access. Furniture included in rent if desired. Free parking. Space available immediately. Call Sherry at 291.1309 or [email protected].
YOUR REFERRALS ARE ALWAYS APPRECIATEDLynnhurst Office Center, 8009 New LaGrange Rd., Suite 4,
Louisville, KY 40222
WALKER COUNSELING SERVICES, INC.MAUREEN A. WALKER, M.A.
KY Board Licensed Clinical Marriage and Family TherapistFamily Systems Psychotherapist
YOUR THERAPIST AND COACH FOR LIFE• Individual • Couple
• Marital and Divorce • Family • Group• Effective • Strategic • Healthy
Office (502) 425-5482Direct (502) 553-5482
LMMarch2012:August 07 4/30/2012 11:23 AM Page 139

44 LouisviLLe Medicine
A D V E R T I S E R S ’ I n D E XAthena Health 9www.athenahealth.com
Baptist Hospital East 11www.baptisthealthky.com
Baptist Hospital East IBCwww.baptisthealthky.com
Chambers Medical Group 43www.chambersmedical.com
Division One Commercial Cleaning Inc 43www.divisionone.us
Elmcroft Senior Living 15www.elmcroftseniorliving.com
Hall Render Killian Heath & Lyman 27www.hallrender.com
Healthcare Underwriters 42www.hugroupky.com
HealthStat Inc 42www.healthstatinc.com
John Kenyon Eye Center 8www.johnkenyon.com
Kentuckiana Pain Specialists 31www.painstopshere.org
Kindred 17www.kindredhealthcare.org
MAG Mutual Insurance Co 38www.magmutual.com
Medical Society Employment Services 34www.glms.org
Murphy Pain Center 1www.murphypaincenter.com
National Insurance Agency 13www.niai.com
Norton Healthcare Physicians 19www.nortonhealthcare.com
Norton Leatherman Spine Center 12www.nortonhealthcare.com
Physicians’ Medical Center 4www.pmcindiana.com
Physicians’ Medical Center 6www.pmcindiana.com
PNC 29www.pnc.com
Professionals’ Purchasing Group 30www.ppginc.net
Republic Bank & Trust Co 33www.republicbank.com
State Volunteer Mutual Insurance Co 2www.svmic.com
The Doctors Company 37www.thedoctors.com
The Pain Institute OBCwww.thepaininstitute.com
The Physicians Billing Group 43www.thephysiciansbilling.com
VanZandt Emrich & Cary 10www.vzecins.com
VNA Nazareth IFCwww.vnanazareth.org
Walker Counseling Services 43
Through the use of Twitter, GLMS has the ability to reach patients with health and wellness reminders. Please ask your patients to sign up! They can become a follower of @VitalSigns2Go on Twitter or text “follow VitalSigns2Go” to 40404 and receive the brief messages on their phone. The tweets are a free service connecting patients to reliable medical information.
Standard message rates from their carrier may apply.

Feel better.
© 2
012
Bap
tist
Hea
lthc
are
Syst
em, I
nc. /
Mem
ber,
Bap
tist
Hea
lthc
are
Syst
em
know someone facing a weighty decision?
If you have a patient whose health is dramatically
affected by excess weight, here’s a way to make the
bariatric surgery decision a little lighter. The Baptist
East Bariatric Center is offering a series of free patient
seminars discussing laparoscopic surgical weight loss
procedures which include adjustable gastric banding,
gastric bypass, sleeve gastrectomy, as well as revisional
incision-less procedures.
To refer a patient, visit baptisteast.com/weightloss or
phone (502) 897-8131 for more info.
• Thursday, May 3 (6:30 p.m.)
• Saturday, May 19 (10 a.m.)
• Thursday, June 7 (6:30 p.m.)
• Saturday, June 16 (10 a.m.)
baptisteast.com/weightlossfacebook.com/baptisteastweightloss
A free info session on bariatric surgery answers patients’ questions and could change their lives.
BHB-105-PhysicianRef(8.5X11)_4.5.12.indd 1 4/5/12 11:05 AM

PRSRT STDU.S. POSTAGE
PAIDLOUISVILLE, KYPERMIT NO. 6
Greater Louisville Medical Society101 WEST CHESTNUT STREETLOUISVILLE, KY 40202