the hillingdon hospitals nhs foundation trust … hillingdon hospitals nhs foundation trust ......
TRANSCRIPT

The Hillingdon Hospitals NHS Foundation Trust
Meeting of the Council of Governors
Tuesday 8 November 2016
Civic Centre, Uxbridge, UB8 1UW 6.30pm
Paper Pages
1. Welcome and apologies for absence -
2. Declarations of interest and any amendments to the Register of Governors’ Interests
-
3. Declarations of Any Other Business -
4. Minutes of the meeting of the Council of Governors held on11th July 2016 and Action Log and any matters arising
(There are no outstanding actions from previous meetings)
A 3
5. Chair’s report and strategic update including Governor questions on any matters not otherwise covered on the Agenda
B 11
6. Presentations from Non-Executive Directors -
7. Finance Report C 17
8. Integrated Quality and Performance Report D 19
9. ICT Strategy Update E 27
10. Membership Development and Engagement Update (Verbal update) -
11. Any Other Business -
12. Questions from the Public -
1
Dates of 2017 meetings: (all to start at 6.30pm and proceeded by a Governor only pre-meeting at 5pm). It has been agreed that the Council of Governor meetings in 2017 will be held in the Medical Education Centre at Hillingdon Hospital and one meeting will be held in the Medical Education Centre at Mount Vernon Hospital.
• Monday 6th February 2017 (Hillingdon) • Tuesday 9th May 2017 (Mount Vernon) • Monday 10th July 2017 (Hillingdon) • Tuesday 7 th November 2017(Hillingdon)
-
* NB timings and order are indicative only: the Chair may decide to vary the timings and order.
** It is expected that items 13-14 will be discussed in closed session given the confidential nature of the items.
Governors unable to attend the meeting are asked to submit any apologies in advance to the Trust Secretary on 01895 279976 or email
2
The Hillingdon Hospitals NHS Foundation Trust
Meeting of the Council of Governors Tuesday 11th July 2016
Committee Room 6, Civic Centre, Uxbridge, UB8 1UW 6.30pm
Members of the Council of Governors present: Richard Sumray (RS) Trust Chair Rekha Wadhwani (RWa) Lead Governor David Bishop (DB) Public Governor Donald Dakin (DD) Public Governor Doreen West (DW) Public Governor Graham Bartram (GB) Public Governor Harkishan Chander Public Governor Keith Saunders (KS) Public Governor Ray A Smith (RAS) Public Governor Roger Shipton (RSh) Public Governor Terry Thompson (TT) Public Governor Tony Ellis (TE) Public Governor Graham Coombs (GC) Staff Governor Alvan Pope (AP) Staff Governor Jack Creagh (JC) Staff Governor Shelia Kehoe (SK) Staff Governor Mary O’Connor (MOC) Appointed Governor Pauline Cranmer (PC) Appointed Governor Also present: Shane Degaris (SDG) Chief Executive Katey Adderley (KA) Non-Executive Director Lis Paice (LP) Non-Executive Director David Searle (DS) Director of Strategy and Business Development Joe Smyth (JS) Chief Operating Officer Matt Tattersall (MT) Director of Finance Craig Wisdom (CW) Partner, Deloitte Catherine Holly (CH) Patient & Public Engagement Steve Wedgwood (SW) Head of Facilities Ritu Sharma Information Governance Manager (minutes) 1 member of the public Apologies: Paul Cornford Staff Governor Sheila Bacon Staff Governor Richard Whittington Non-Executive Director Carol Bode Non-Executive Director Soraya Dhillon Non-Executive Director
3

Carl Powell Non-Executive Director Theresa Murphy Director of Nursing and Patient Experience Carolyn Cullen Trust Secretary
1. Welcome and apologies for absence
The Chair welcomed everyone to the meeting and introduced Ray Smith, Public Governor for the South. Apologies noted.
2. Declarations of interest None declared.
3. Declarations of Any Other Business PLACE matter - GB Skin Centre – TE
4. Minutes of the meeting of the Council of Governors held on 10th May 2016, action log and any matters arising not otherwise covered on the agenda The minutes of the meeting held on 10th May 2016 were agreed as an accurate record of the meeting. One minor amendment was noted, GB stated he did not ask the question about ventilation on Page 3, and asked that his name be removed. Action log: Action 23: CH stated that she had recently visited Kingston NHS Foundation Trust with the (Patient Advice and Liaison) PALs Manager. This was a helpful visit and provided further information which could be incorporated into the development of a volunteer strategy. Action 24: DS updated the meeting regarding the perception that there is more halal food provided in the Trust restaurants. He stated that halal food was introduced in 2012 when the need was identified from a customer survey. The restaurant only provides one halal meat dish, alongside two non halal dishes, on a daily basis. There are also thirteen different ranges of sandwiches and wraps available, of which only five contain halal meat. Halal products account for approximately 17% of total daily sales and11% of the local patient population is Muslim (2011 census). On the Electronic Staff Record (ESR) system 5.3% of permanent and fixed term staff is recorded as Muslim (although 30% of Trust staff have chosen not to express their religious beliefs). In summary, the Trust’s catering service clearly meets an identified specific customer need, but not to the detriment of the wider service and other catering requirements. Questions: HC enquired if any routine employment or security checks such as DBS were made before volunteers were allowed to work here.
4

RS stated that they are; however, this is dependent on the role being undertaken. GB commented that the issue regarding halal food in the restaurant is that it is not always clearly labelled as halal, not that it is being provided. GB also stated that it can be argued this is not pure halal; because it has been prepared in a kitchen with non halal food using the same equipment. GB suggested that staff and visitors could order halal food separately from a halal food supplier. DS confirmed no complaints or concerns had been raised about the halal food served in the restaurant to date.
5.
Chair’s report and strategic update including Governor questions on any matters not otherwise covered on the agenda RS highlighted three matters to the Council of Governors; firstly, the scale of the pressure that A&E is under; secondly, the growing importance of the Accountable Care Partnership (ACP) and a report on progress of the ACP will be presented to the Board on 21st July 2016; and lastly the increased financial pressure the Trust is facing. RS stated that it is good to see these matters in context; and our financial performance still compared well to some other London trusts. RS also informed the Council of Governors that the Stroke Service has recently been audited and has gone from being rated poorly performing to performing well. JS stated A&E has seen an increase in activity of 9% in the first quarter of 2016, with a month on month increase of attenders of between 8% and 10%. The current A&E department is built to support approximately 145 patients per day, however the department now sees on average 170 to 190 patients per day. To improve the flow from the daily build-up of queues, two new schemes have been introduced; firstly, two new triage rooms to support early triage are in place and secondly the CDU area has been expanded to provide an area where patients can wait for test results. Questions: GB enquired about Master Planning and what the Board’s decision was on this. RS replied that the Board’s preferred position would be to build on the Brunel site, if that were possible. MOC commented that initiatives in A&E were welcomed, however had additional staffing been considered. JS stated that it had, and a bid for extra staff has been made to Hillingdon CCG. This business case also includes a bid for additional doctors, nurses and Health Care Assistants (HCAs). TE requested an update on negotiations with North and East Herts NHS Trust. SDG stated an agreement had not been reached; however negotiations were still in progress although the slow pace of negotiation is frustrating. SDG stated that an alternative being considered is to seek outside resolution from NHS Improvement should negotiations not conclude satisfactorily. DB asked whether the value of services being transferred to the Accountable Care Partnership is £37 million.
5
SDG clarified that this is not money coming out of the system, but a pooling of resources where our Trust would be one of four partners delivering services. This partnership makes clinical sense and will lead ultimately to financial benefits. RS added that the ACP will support the aim of more people being treated in the community, although this will be a gradual process. HC asked if the Trust knew which patients attending A&E should have gone there and which patients should have been seen by primary care. JS stated it was difficult to identify if a patient should have come to A&E cases or not. KS informed the meeting that posters are currently being developed to explain the alternative places where patients can go to receive treatment.
6.
Non-Executive Director Presentation KA gave a short account of what it was like being a Non-Executive Director at the Trust. KA has been a Non-Executive for five and half years and will be stepping down at the end of November 2016. KA stated that when she became a Non-Executive Director the external environment was all about obtaining Foundation Trust status; and this had been a huge task for the Board. Conversely today integration of services is key. KA stated that making strategic change is difficult and the Trust needs to debate and proceed with caution; an open mind needs to be kept regarding integration and partnership work. KA stated that the Trust is a caring and friendly organisation and had conducted itself well through financial difficulties and done a decent job in reducing costs. KA commented that the Trust needs to embrace learning from mistakes; particularly the organisation needs to ensure that it is doing as much as it can to improve and embed changes following the CQC inspection which highlighted key concerns including poor care on Beaconsfield East Ward, non-compliance with the World Health Organisation (WHO) check list, ventilation problems in theatres and poor cleaning standards to name a few. The Trust needs to continue to working with its internal audit team to check compliance and progress. The Board needs to assure itself that it receives the correct amount of information and is mindful that it is not just about receiving data, but ensuring that the Trust has the right culture to pick up issues and act on them. Questions: MOC commented the presentation was thoughtful and it was good to hear that the patient care experience remains paramount. RWa asked what Governors should be worried about. KA said there was nothing to be worried about as the organisation is open and believes in transparency. RSh asked how we can unblock the lack of urgency to action things. KA stated it was hard to embed change; it may help to streamline some Committees which sit under the Board Committees.
7. External Auditors Report on 2015/16 Accounts and Quality Accounts
6
CW stated that the 2015/16 report on the accounts gave an unmodified audit option. This audit was undertaken to look at the strength of arrangements in place, rather than to comment as to whether outcomes had been achieved. CW drew attention to Page 4 of the report which highlighted the financial risks facing the Trust; but this should be seen in the context of how other Trusts have performed. Overall results are satisfactory and there is no evidence of management bias. Questions: TE commented that on Page 3 the surplus was shown in the middle of the table which is confusing to read. CW noted this comment. HC asked if the Trust is still sustainable as ongoing concern. CW stated that the Trust is rated as a going concern. TE asked if any patients suffered due to poor record keeping. CW stated that the audit tested process, but cannot answer this clinical question. JS replied the audit was helpful and the 18 week RTT performance was a complex area to review. The A&E system is not always aligned with manual systems used in A&E such as CAS cards; however work is ongoing to look at improving the accuracy of data recording. RS thanked CW for attending.
8. Quality and Operational Performance Update JS highlighted that as part of the A&E recovery plan the Band 7 nurse co-ordinators had been made supernumerary so that they could be targeted at where they could do the most good.
9.
Finance MT stated that the Trust financial performance year to date showed a deficit of £1.9 million, against a planned deficit of £1.3 million. MT stated that this is due to three factors: higher levels of activity in A&E that resulted in the need to open additional beds; the loss of income due to the junior doctor’s strike and increasing maintenance costs. NHS Improvement has confirmed that the Trust will be eligible for an additional £6.7 million through Sustainability and Transformation Funding (STF), but this funding will only move the Trust from a deficit to a surplus. Receipt of STF monies will be conditional on meeting financial targets as well as meeting the 62 day cancer target, RTT and A&E performance targets. Questions: TE enquired whether there was sufficient funding to combat legionella. DS stated that water hygiene is prioritised in the Capital Plan, however additional work is required to improve the water quality. This risk has been recorded on the risk register.
7

GB asked what the purpose of a £5 million surplus was. MT stated the use of this cash has not been determined; however it is good for liquidity and as a buffer against unforeseen events.
10.
Sustainability and Transformation Plan (STP) Update RS stated that he is attending a meeting of STP leads and Chief Executives on the 14th July 2016. Further information on implementation and guidance on governance procedures is expected in the Autumn. Questions: RWa asked who will be accountable for delivering STPs and what will the role of Governors be in the new process. DS stated that this question was raised at a NHS London meeting. More guidance is expected in the Autumn.
11.
Membership Engagement RWa informed the meeting that the Membership and Engagement Group met on the 9th June 2016. Discussions took place on how to recruit more members in the North of our area. Recruitment of younger members via social media, with possible support from students at Brunel, was also discussed. Proposals for future events in the North will be further discussed at the PIP meeting in January 2017.
12.
Any Other Business GB stated that he had attended the PLACE meeting last month and highlighted an incident regarding some spare bed parts had been thrown away by mistake; and due to delays in the invoicing further bed repairs had not being undertaken for three weeks. GB was concerned by the lack of urgency to resolve this issue whilst patients lay on dangerous beds. DS replied that it was a strong statement to make that patients were lying on dangerous beds and as an Executive he has not been made aware of this issue. The PLACE meeting is not the appropriate forum to raise this issue. However bed management and bed stock review is being conducted by the Director of Nursing and Patient Experience, the outcome of which it is hoped is to negotiate a better bed repair and leasing contract. JS stated that regarding the Skin Centre at Mount Vernon, a planning meeting is taking place this Friday to review progress. Following this meeting a formal planning application and detailed drawings will be prepared. The planning application is due to be submitted on the 15th August 2016.
8

13.
Questions from the Public None.
14 Review of the meeting Governors commented that having their pre-meeting prior to this meeting is helpful. The meeting closed at 20:45.
15. Date of Next Meeting: Tuesday 8th November 2016,CR 3A, Civic Centre, Uxbridge, 6:30 pm
9

10

Meeting of the Council of Governors
8 November 2016 Agenda Item 5
Paper B
Title: Chair’s report
Summary & reason for item: Monitor’s NHS Foundation Trust Code of Governance states that the Trust Chair is responsible for ensuring that the Council of Governors receives the information required to undertake its role. In line with this, the attached report updates the Council of Governors on developments at the Trust and relevant matters more widely. Recommended Governor action: 1. Review the report. 2. Ask questions and comment as appropriate.
Report from: Richard Sumray, Chair Equality Impact Assessment: N/A – there is no positive or negative impact from this report
11
Chair’s Report to the Council of Governors: November 2016
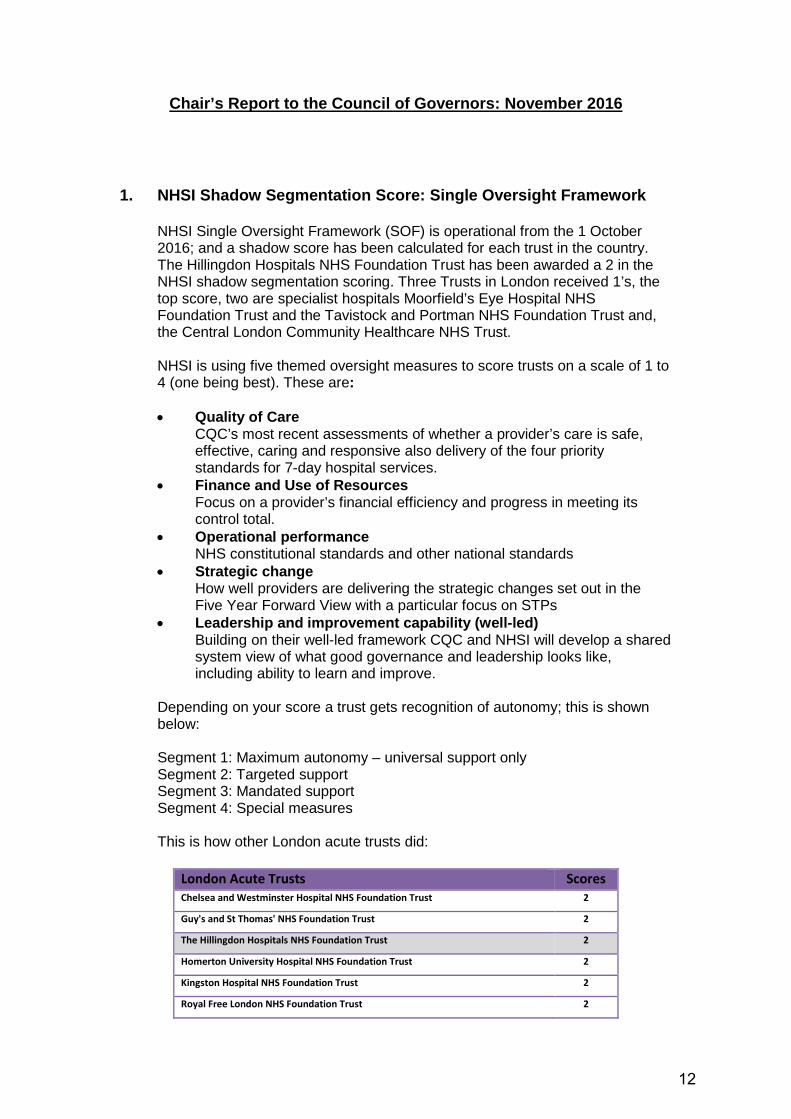
1. NHSI Shadow Segmentation Score: Single Oversight Framework
NHSI Single Oversight Framework (SOF) is operational from the 1 October 2016; and a shadow score has been calculated for each trust in the country. The Hillingdon Hospitals NHS Foundation Trust has been awarded a 2 in the NHSI shadow segmentation scoring. Three Trusts in London received 1’s, the top score, two are specialist hospitals Moorfield’s Eye Hospital NHS Foundation Trust and the Tavistock and Portman NHS Foundation Trust and, the Central London Community Healthcare NHS Trust. NHSI is using five themed oversight measures to score trusts on a scale of 1 to 4 (one being best). These are: • Quality of Care CQC’s most recent assessments of whether a provider’s care is safe,
effective, caring and responsive also delivery of the four priority standards for 7-day hospital services.
• Finance and Use of Resources Focus on a provider’s financial efficiency and progress in meeting its
control total. • Operational performance NHS constitutional standards and other national standards • Strategic change How well providers are delivering the strategic changes set out in the
Five Year Forward View with a particular focus on STPs • Leadership and improvement capability (well-led) Building on their well-led framework CQC and NHSI will develop a shared
system view of what good governance and leadership looks like, including ability to learn and improve.
Depending on your score a trust gets recognition of autonomy; this is shown below: Segment 1: Maximum autonomy – universal support only Segment 2: Targeted support Segment 3: Mandated support Segment 4: Special measures
This is how other London acute trusts did:
London Acute Trusts Scores Chelsea and Westminster Hospital NHS Foundation Trust 2
Guy's and St Thomas' NHS Foundation Trust 2
The Hillingdon Hospitals NHS Foundation Trust 2
Homerton University Hospital NHS Foundation Trust 2
Kingston Hospital NHS Foundation Trust 2
Royal Free London NHS Foundation Trust 2
12

Royal National Orthopaedic Hospital NHS Trust 2
University College London Hospitals NHS Foundation Trust 2
The Whittington Hospital NHS Trust 2
Epsom and St Helier University Hospitals NHS Trust 3
Imperial College Healthcare NHS Trust 3
King's College Hospital NHS Foundation Trust 3
Lewisham and Greenwich NHS Trust 3
London North West Healthcare NHS Trust 3
North Middlesex University Hospital NHS Trust 3
St George's University Hospitals NHS Foundation Trust 3
Barking, Havering and Redbridge University Hospitals NHS Trust 4
Barts Health NHS Trust 4
Croydon Health Services NHS Trust 4
2. Sustainability and Transformation Plans
Across England 44 Sustainability and Transformation Plans have been submitted. Ours, one of the bigger ones with a population base of over two million is North West London. National progress to date includes:
• Draft STPs being submitted in June reviewed with second iterations
being submitted by 21 October 2016 • Strategic planning guidance asked STP partners to set out plans to
engage key stakeholders. Once specific proposals have been developed this should be supported by local engagement, and consultation
• NHSI has reiterated the need to close the finance and efficiency gap through improved productivity, long-term sustainability and capital requirements; including implementation of the Carter review
• Guidance highlights the importance of local authorities and NHS commissioners pooling funds
• Local leadership must have sufficient support, including establishing effective governance, for STP partners working together as a system.
NW London Localities were directed to submit detailed plans in October 2016. The strategic plans for each footprint are the starting point for two-year, organisation-level operational plans for 2017/18 and 2018/19 which themselves need to be finalised at a local level before the end of the calendar year. NW London STP planning started from a strong base having had the Shaping a Healthier Future (SaHF) programme for some years. However agreement with some councils in NW London was slow to develop, despite good individual borough relationships with CCGs, but has now progressed to a better positon. Engagement events have happened to a varying degree across the NW London; and Hillingdon, to discuss just the Hillingdon segment, had a
13

successful local engagement event with its community organised by Hillingdon CCG at Brunel University in July 2016. The Trust is awaiting guidance on when the NW London will be published, and the local Hillingdon STP component. Governors views were sought via workshop in developing the plans and Governors will have the opportunity to discuss STPs when they are in the public domain.
3. Accountable Care Partnership Update
Since late 2013, Hillingdon has invested a significant amount of time and energy in developing a vision for integrated care that is centred on the needs of service users. A critical component of this has been the development of an Accountable Care Partnership (ACP). This is a collaboration of Hillingdon’s key healthcare providers coming together to develop new ways of delivering better, integrated services which are financially sustainable. The partners are Central and North West London NHS Foundation Trust, Hillingdon GP Federation and H4All – a collaboration of third sector providers. In January 2015, the ACP appointed a director to oversee and accelerate progress. The ACP is now testing its new arrangements under an alliance contract for the care of older people aged over 65 from April 2017. The clinical care model includes the Care Connection Team based in primary care and the ACP clinical team who are designing a frailty pathway which aims to improve care for elderly people with complex problems. The aim is to enable patients to avoid long stays in hospital by returning home with appropriate support. Working closely with legal advisors, a road map detailing next steps has been developed. This work includes beginning due diligence processes with partner providers and agreeing the contract for services in shadow form for 2017/18.
4. Peter Pan Ward Opening
There was an official opening of the extension to Peter Pan Ward on Friday 22 October 2016. The Trust was very pleased to welcome Boris Johnson, the Secretary of State for Foreign and Commonwealth Affairs and MP for Uxbridge and South Ruislip to the Trust to do the honours. John McDonnell, Shadow Chancellor of the Exchequer and MP for Hayes and Harlington has been asked to open the new outpatients’ pharmacy.
5. Declaring Independence
Sir Malcolm Grant, Chairman of NHS England has published proposals on managing conflicts of interest in the NHS. The scope of the regime proposed covers: Executive and Non-Executive Directors, Foundation Trust Governors, members of advisory groups, medical staff including NHS contractor professions such as pharmacists and dentists and NHS staff Agenda for Change Band 7 and above. All members of Boards and Sub-Committees and Council of Governors should review and update their interests at the start of each meeting. The Chair will then advise on the appropriate action to take which may include declaring and recording the interest and leaving the meeting for the item(s) concerned or declaring and recording the interest but being allowed to participate.
14
These rules also apply to advisory committees which bring together experts from a specific field of practice including patient and public voice representatives. These rules also apply to procurement panels or evaluation panels for a tender exercise. What must be declared are: specific direct or indirect financial or non-financial, loyalty interests or family interests. These are the classifications of interest: Direct Financial Interest includes: gifts, hospitality, outside employment, shareholdings and patents. This also includes financial gain to close family members, close friends and associates, and business partners (dependent on the circumstances and the nature of such relationships). Indirect Financial Interest includes: donations, sponsored events, sponsored research, sponsored posts. Non-financial interest includes: where there is or appears to be an opportunity for non-financial gain (e.g. status), or where an individual’s decision making is or could be compromised for example due to a conflict of loyalty. Detailed guidance, when published, will be sent to all Governors; but until then the moto is when in doubt declaring is the best way to go.
6. Update from the Constitution Working Party
It was hoped to bring a report on proposed revisions to the Trust’s Constitution to this meeting. Unfortunately our legal adviser has been unable to provide the Trust with the legal advice asked for due to family illness. Examples of some of the matters that the Trust is seeking clarification on include whether: • a Governor’s term of office starts from when they have taken over a
vacancy or when the vacancy is due for re-election • The external auditor is appointed at a Council of Governors meeting or at
the Annual Members’ Meeting • A resolution disputes protocol (required by external auditor Deloitte.
A report will now be presented to the Council of Governors in February 2017.
7. 2017 Board Meeting Dates
Please find the dates below for Trust Board Meetings in 2017. After discussion with the Lead Governor, and a review of attendance, it was decided to revert back to all Board meetings starting at 2 pm as it was found that no more members of the public or Governors attended at 5 pm than did at 2pm.
15
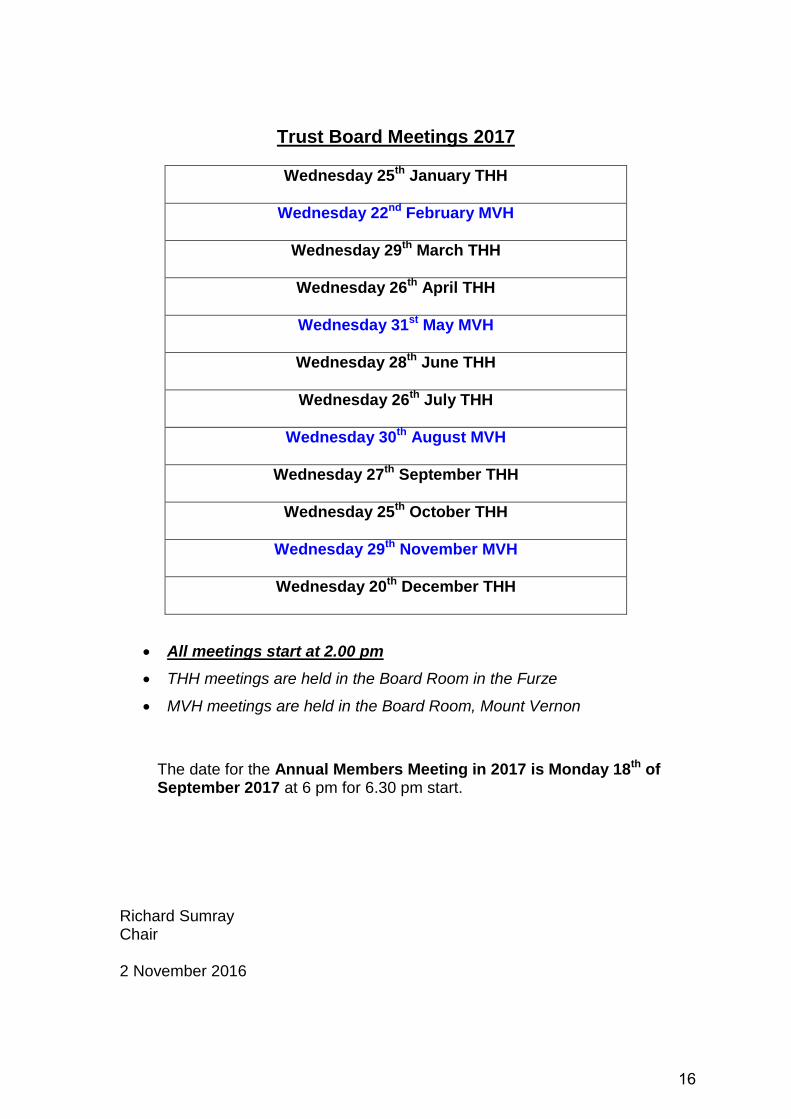
Trust Board Meetings 2017
Wednesday 25th January THH
Wednesday 22nd February MVH
Wednesday 29th March THH
Wednesday 26th April THH
Wednesday 31st May MVH
Wednesday 28th June THH
Wednesday 26th July THH
Wednesday 30th August MVH
Wednesday 27th September THH
Wednesday 25th October THH
Wednesday 29th November MVH
Wednesday 20th December THH
• All meetings start at 2.00 pm • THH meetings are held in the Board Room in the Furze
• MVH meetings are held in the Board Room, Mount Vernon
The date for the Annual Members Meeting in 2017 is Monday 18th of September 2017 at 6 pm for 6.30 pm start.
Richard Sumray Chair 2 November 2016
16

REPORT TO: Council of Governors 8 November 2016
REPORT FROM: Matt Tattersall, Director of Finance
SUBJECT: Finance Report for period end of September 2016
Key Issue Summary RAG
Rating
Financial Plan The Trust’s original plan for the year was to deliver a £1.9m deficit. Should the Trust achieve its financial and key operational performance targets, it will receive a further £6.7m funding from the Sustainability and Transformation Fund (STF). Therefore, the revised plan is to deliver a £4.8m surplus.
Financial Summary
Trust financial performance for the first half of the year was a £61k surplus. This is after receiving £3.1m from the STF. Delivery of the financial performance has only been possible due to a number of non-recurrent benefits including: receipt of capital monies through revenue funding; review of balance sheet liabilities; back dated rents. The underlying financial position is significantly overspent as a result of keeping additional beds open through the summer period and the additional staffing required in A&E.
A
Forecast Much of the underlying financial pressure is forecast to continue for the remainder of the year as it is linked to the additional patients we are treating. As there are no further non-recurrent benefits expected to offset the overspending in the second half of the year, it is unlikely the Trust will continue to achieve its financial control total. Discussions are underway with Hillingdon CCG and NHS Improvement as to what further actions the Trust can take to mitigate the financial pressure.
R
Activity Total A&E attendances are 7.7% higher than the same period in 2015/16. Non-elective admissions remain below plan due to the success of the development of ambulatory emergency care. Daycase activity is 11% above plan with elective activity 3% below plan. GP referrals were 3.8% higher than last year. Births were 198 higher year-on-year, 114 of which were as a result of the Ealing Hospital transfer.
A
Revenue Overall revenue was £2.6m above plan and 3.2% higher year-on-year.
Operating Expenses
Operating expenses were above plan by £4.3m, 7.2% higher year-on-year. The main area of overspend are the pay costs associated with meeting the increasing demand in A&E and staffing for the additional beds. As a consequence, agency costs have begun to increase again, reversing the reductions seen earlier in the year.
R
QIPP The QIPP programme is targeting delivery of £9m in 2016/17. Year to date, the Trust has delivered £4.1m against a plan of £3.3m (N.B. this includes a £2m non-recurrent benefit). The Trust is still forecasting a shortfall on QIPP.
R
Cash flow The cash balance at the end of September was £1.0m, this being £4.3m below plan. This position largely reflects the underlying financial deficit and the fact that many of the mitigating actions do not generate a cash benefit.
R
Capital Expenditure
Capital expenditure at the end of September was £1.5m below plan. This reflected the slippage on Estates schemes following the increased priority given to the Legionella project.
A
Financial Sustainability Risk Rating
The Financial Sustainability Risk Rating was a 2. NHS Improvement is introducing a new rating system for October reporting onwards. The Trust remains at the second best financial rating under the new framework.
A
17

Appendix 1
Annual Yr on Yr Actual Actual Var Actual Var
Plan Growth to to-date Yr on Yr to-date This Yr on Yr This
Outturn Growth Month Growth Month
£000s % £000s % £000s £000s % £000s
Operating Income
NHS Clinical Income * 212,256 3.2% 106,866 5.5% 2,156 18,278 7.4% 748Non-NHS Clinical Income 3,610 (2.0%) 1,907 2.7% 101 349 9.1% 48Other Operating Income * 26,774 (9.0%) 13,285 (8.7%) 386 2,333 (14.4%) 183Total Operating Income 242,640 1.6% 122,058 3.7% 2,643 20,960 4.5% 979
Operating Expenses
Employee Expenses (158,476) 1.2% (83,075) 6.7% (3,744) (14,143) 8.3% (964)Drugs (19,240) 6.7% (9,127) 6.4% 603 (1,416) (8.9%) 201Clinical Supplies and Services (23,758) (0.8%) (12,648) 7.6% (709) (2,066) 8.0% (85)Other Operating Expenses* (27,236) 2.3% (14,106) 10.6% (400) (2,376) 9.1% (101)Total Operating Expenses (228,710) 1.6% (118,956) 7.2% (4,250) (20,001) 11.4% (949)
EBITDA 13,930 3.3% 3,102 (42.2%) (1,607) 959 (18.9%) 30
PFI & Lease Depreciation (2,036) (0.1%) (1,026) 0.8% (6) (175) (9.3%) (5)Other Depreciation (7,838) 6.9% (3,730) (3.6%) 188 (627) (3.8%) 26Interest Income 24 26.3% 8 (33.3%) (4) 1 (50.0%) (1)Other Finance Costs (79) 1.3% (41) 5.1% 1 (6) 0.0% 1Interest Expense on Capital Investment Loans (240) 0.0% (114) (5.0%) 6 (19) (5.0%) 1Interest Expense on Working Capital Loans (168) 2.4% (75) (10.7%) 9 (12) (14.3%) 2Interest Expense on LIFT Contract (1,394) (0.5%) (705) 1.1% (9) (108) (5.3%) 8Interest Expense on Other Finance Leases (268) (2.9%) (117) (12.7%) 15 (22) (4.3%) 0PDC Dividend Expense (3,831) (3.2%) (1,916) 0.5% (2) (320) 0.6% (1)Surplus(Deficit) before Exceptionals (1,900) - (4,614) - (1,409) (329) - 61
Gains/(Loss) on Investment Properties 0 1,535 1,535 0 - 0Profit/(Loss) on the Disposal of Assets 0 0 0 0 0Impairments 0 0 0 0 - 0
Surplus(Deficit) after Exceptionals (1,900) - (3,079) - 126 (329) - 61
Sustainability & Transformation Fund 6,700 3,140 - (210) 488 - (71)
Surplus/Deficit with Sustainability Funding 4,800 - 61 - (84) 159 - (10)
EBITDA % without STF 5.7% 2.5% 4.6%EBITDA % with STF 8.5% 5.1% 6.9%Surplus/(Deficit) % 2.0% 0.0% 0.8%Normalised Surplus (Deficit) % (0.8%) (3.8%) (1.6%)FSRR Surplus/(Deficit) % 2.0% 0.0% (0.1%) 0.8% (0.0%)
* reclassified following submission of Annual Plan ( ) variance indicates it is adverse
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST
Statement of Comprehensive Income
Period Ending 30th September 2016 (Month 6)
18

Meeting of the Council of Governors
Agenda item 8
Integrated Quality & Performance Report
Reason for item:
To provide assurance to the Governors that the Trust's key quality, operational and experience objectives are being delivered. To direct the Board's attention to significant risks, issues and exceptions ensuring we remain focused on the delivery of our vision "To put compassionate care, safety and quality at the heart of everything we do."
Summary:
This report provides analysis of quality, experience and operational performance to the end of September 2016. The report covers performance against the Monitor Risk Assessment Framework as well as national and local key performance indicators.
Report Authors:
Melissa Mellett, Director of Operational Performance
Jacqueline Walker, Deputy Director of Nursing and Integrated Governance
Obi Maduako-Ezeanyika, Head of Workforce and OD
Report Sponsors:
Professor Theresa Murphy - Director of Patient Experience and Nursing
Dr Abbas Khakoo - Medical Director
Joe Smyth, Chief Operating Officer
Terry Roberts, Director of People
Links to Trust strategic priorities:
• To create a patient centred organisation to deliver improvements in patient experience and the quality of care we provide.
• To deliver high quality care in the most efficient way.
Previous consideration at Board or Committees: Reviewed monthly as standard
Equality and diversity considerations: There is no positive or negative impact from this report.
Financial implications: The financial implications of delivering the additional capacity to meet the non-elective demand over and above plan are detailed in the report.
19

Integrated Quality & Performance Report
1. Summary
This report reflects on achievements in performance standards for Month 6, September 2016, including the improvements made in delivery against all key standards. The format of the performance dashboard reflects the core principles of the five Domains set out in the Care Quality Commission's Intelligent Monitoring System (i.e. Caring, Well-led, Effective, Safe and Responsive).
1. Key Highlights 2.1 Safe Three cases of C.diff have been attributed to the Trust in September. Two cases were linked in time and place (Fleming Ward) and therefore a Period of Increased Incidence (PII) has been declared and enhanced cleaning and surveillance will continue until three weeks have passed with no further C.diff cases and all IPC audit results meet the required standard. The samples have been sent for typing and results are awaited. The threshold for 2016/17 is eight cases where a lapse in care has been identified. Two of the five cases reported for this year have been reviewed by the commissioners and no lapses in care identified. The three cases reported in September have had full root cause analysis investigation and will be reviewed with our commissioners by end of October. Confirmation has been received from Monitor that for cases where no lapse in care has been identified, these cases will not count against the Trust as part of the outcomes metric assessment on the Monitor scorecard or our quality governance rating. The rate of hospital acquired pressure ulcers in August was 0.8 1000 bed days (12 reported Category 2 ulcers). This is within target and the year-to-date figure remains on track at 0.9 against a target of 1.0. The rate of patient falls remained at 4.7 per 1000 bed days against the Trust’s internal target of 3.9. The year-to-date position is 4.4 which while not meeting our own challenge does continue to be lower than national averages published by NPSA in 2010 (5.6) and by the RCP in 2015 (6.6). 2.2 Caring Friends and Family Test Wards are engaging well with offering the survey, however the number of responses returned in September was reduced. Satisfaction scores though were improved, with inpatients, maternity and outpatients achieving scores over 96 percent. Complaints
20

Whilst there has been a reduction in complaints received year-to-date compared with the same period last year, volume received in recent months has led to a high number of responses being due in-month: 42 in September. This has been challenging to achieve within agreed timeframe, particularly for the medical division where volume is highest. The reply performance at 57.1 percent is significantly below target but is slightly improved compared to last month. The Director of Nursing has supported the medical division to source temporary additional resource to focus entirely on coordination of complaint responses. This is already delivering, with backlog complaints reduced. The full impact will be more apparent in coming months. 2.3 Responsive 18 weeks RTT – Incomplete The Trust incomplete submission remains compliant with the national standards of 92.2%. RTT improvement work continues and as planned and expected, as the longest waiting patients are treated the admitted performance will remain below the internally monitored targets and will remain so until December, when the specialty backlogs have been cleared. 4 Hour A&E Access Target All types performance for September is recorded at 84.8% -which is a small improvement against August performance. During September, there was a 8.5% increase in type 1 activity on 15/16 with a 17% increase in paediatrics. Overall LAS attendances are up by 3.5%, with blue light activity up by 22.9%. Despite the apparent increase in acuity the admission rate continues on a downward trend with a 25% reduction on 15/16. Type 1 attendances for the over 65s and the over 80s remains elevated and shows a reverse in the trend of reduced admissions for this patient cohort. Exit block remains a significant factor for increased dwell time in the ED. The trust continues in all escalation capacity. The discharge task force programme is due to culminate in a clinical summit which will identify key initiatives designed to reduce bed utilisation which will improve patient flow. Collaborative work continues with health and social care partners to refine plans for the winter period. Actions since last report: The new assessment area has been opened in the department to allow ambulant patients to be assessed earlier in their pathway, with a view to targeting short stay patients that can be discharged home or expediting the pathway for those who subsequently go on to require admission. This is having some improvement in reducing the dwell time in the ED. The bottle neck however has been in getting patients that need acute beds out of the ED department. Daily conference calls have occurred in September to help drive down the Delayed Transfers of Care (DTOC). While the number of DTOC remained high during September, there has been an improvement in the first two weeks of October 2016.
21
The new clinical Decision Unit (CDU) is completing sooner than planned, 24th
October – the original date was 15th December. ED are still working towards operationalising the unit in time for the 15th December deadline. In the meantime we are going to use the opportunity to utilise the space to pilot a Surgical Assessment Unit and discharge lounge. 2.4 Well-Led In September 2016, the year to date medical appraisal compliance was 33.94%, which is an improvement of 5.94% compared to August 2016. 94 out of 277 medical appraisals have been completed since April 2016. The Trust continues to exceed its Core Skills Training (CST) target of 80% and retains the highest CST compliance in North West London. In September 2016, the CST compliance was 91.02%, a 3.91% improvement compared to the same period last year. PDR completion rate was 98.01%, unchanged from the previous month. In September 2016, the sickness rate was 3.40% which is an increase of 0.03% compared to the previous month. Medicine Division has seen the highest increase by 0.27%, and will be provided targeted training and 1:1 sessions with key hot spots to encourage case conferences for long term sickness to review sustainability of impact of sickness cases. Surgery and Women's and Children Divisions have also been receiving targeted training and coaching from HR Business Partners on managing sickness cases and have both seen a reduction in the number of long term sickness cases. In September 2016, £58,740 was spent on Bank due to staff sickness. The overall Trust vacancy rate in September 2016 was 11.46%, which is a slight decrease of -0.14% on August 2016, where the vacancy rate was 11.60%. In comparison to the same period last year, the vacancy rate has increased by 0.47% from 10.99%. The Trust is working on improving the vacancy rate. In the medium term, the Trust is actively focussing on international recruitment and in the short term period, the Recruitment Team are actively holding Recruitment Days. The Surgery Division are exploring the possibility of overseas recruitment for junior doctors. The Trust has shown a significant improvement in the average time to recruit. It was at its highest in May 2016 at 67 days, however each month there has been continuous improvement and this month the time to recruit has been maintained at 55 days. The Trust's turnover rate has continued to remain the same since May 2016, at 16% in September 2016 against the newly agreed 13% target (agreed as part of the Recruitment and Retention Strategy approval at the September Board meeting). In order to develop effective action plans to reduce turnover, we are undertaking a series of face to face exit interviews with all our current leavers. The total spend on Bank and Agency staff was £2,164,215 in September 2016. This has decreased by - £20,539 compared to spend in August 2016, which was £2,184,754. The use of ‘off framework’ agency workers has increased in the month of September 2016, with the Trust at 1.13%, compared to 1.07% in August
22

2016. There continues to be an increase in the number of breaches of the price cap. In September 2016, there were 264 breaches, which is an increase of 41 compared to the previous month. The highest number of breaches was Medical Locums with 145. This is an increase of 74 breaches (51%), compared to the previous month. The Director of Nursing daily meetings have helped to identify where e-rostering can be improved and help reduce spend. The Trust had 2,975 FTE staff in post in September 2016, which is an increase of 3% compared to the same period last year in September 2015. Additional Professional Scientific and Technical Group has seen the biggest increase of 12% in September 2016, compared to the same period last year.
23

[1.06, 1.07 & 1.08] SAFE Medication, VTE & Pressure Ulcers
1.0.6 - Medication IncidentsWhere we want to be: targets and benchmarks: We want to increase incident reporting of no/low harm incidents for medication errors. This will support us to learn from near misses / low harm incidents to prevent more harmful incidents. Where we are: trends and patterns: Our reporting rate of medication errors was historically not in line with national average for acute (non-specialist) organisations (national average of 11%) as reported by NRLS, however we saw an improving picture in 2015/16. In 2016/17 we are now in line with the national average, which currenlty stands at 10.5%. Risks or opportunities for the Trust: The Trust is involved in a programme with the ICHP Patient Safety Collaborative to improve pharmacists’ provision of feedback to doctors on prescribing errors. The Medication Safety Officer and the Medication Safety Committee are taking a programme of work forward to improve practice based on the leanring from these incidents.1.07 - VTE - Target 95%Compliance YTD is above the 95 % target at 96.1%. Improved reporting in all previously low-reporting areas has contributed to an improved performance. N.B.There is a lag time for validation for the previous month and therefore September figures will change. The risk of VTE is now mitigated by the VTE risk information leaflet given to every inpatient explaining the risk of VTE and how individuals can reduce their own risk . There is also implementation of VTE risk assessment compliance as part of the WHO sign-out in operating theatres.
1.08 - Pressure Ulcers: (15% reduction by year end) Where we want to be: targets and benchmarks: We aimed to achieve a 15% reduction in hospital acquired pressure ulcers during 2015/16. This is in line with our Sign up to Safety campaign to reduce patient harms by 50% over three years. Where we are: trends and patterns: The hospital acquired pressure ulcer rate during 2013/14 was 1.34 per 1,000 bed-days and in 2014/15 this was 1.20. For 2015/16 we achieved a rate of 1.1, which although an improvement narrowly missed the target rate of 1.0 per 1000 beddays. For 2016/17 we are again aiming for a target rate of no more than 1.0 per 1000 beddays which are currently achieving (0.9 year to date). In September the rate for the month was within target at 0.8 and none were graded as category 3 or 4. Risks or opportunities for the Trust: This is a priority area of focus for the Sign up to Safety work and there are clear actions as part of the improvement plan including ward based and classroom based teaching , improved systems for referring to the Tissue Viability Nurse.
September-2016
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Medication Related Incidents as a Percentage of Total Incidents
2016/2017 2015/2016 Target
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
VTE Compliance
2016/2017 2015/2016 Target
0.0
1.0
2.0
3.0
4.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Pressure Ulcers per 1,000 Beddays
2016/2017 2015/2016 Target
24
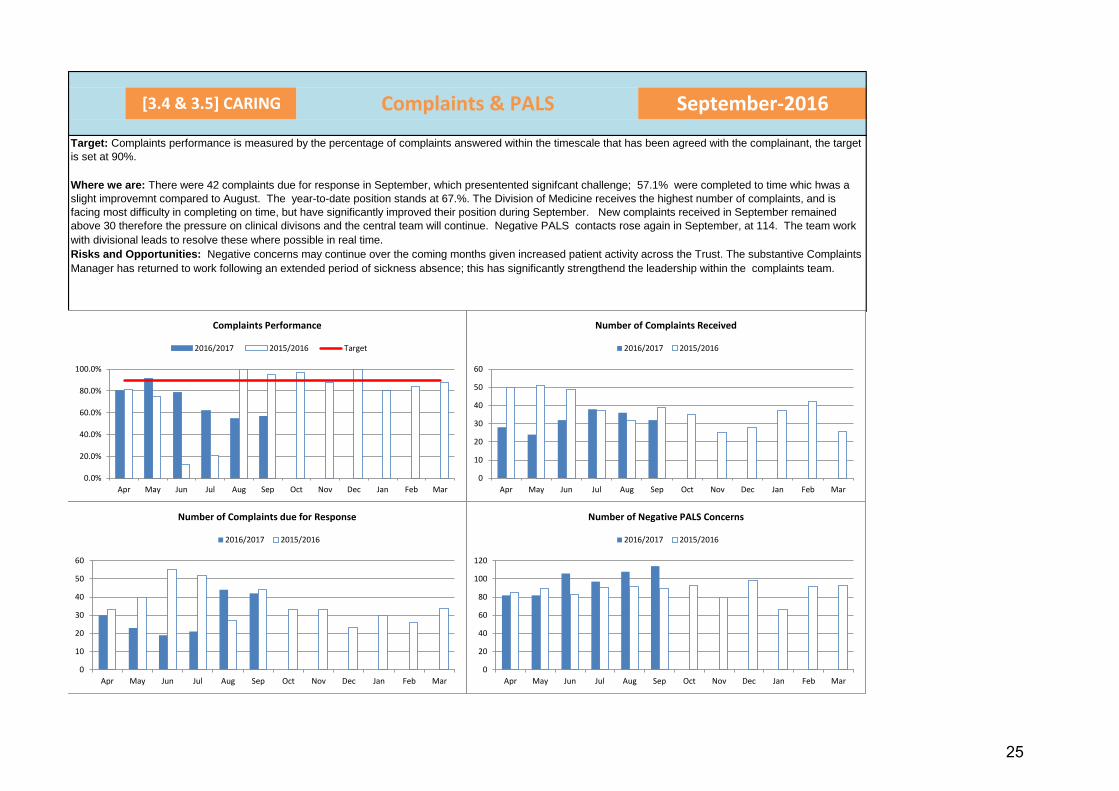
[3.4 & 3.5] CARING Complaints & PALS
Target: Complaints performance is measured by the percentage of complaints answered within the timescale that has been agreed with the complainant, the target is set at 90%.
Where we are: There were 42 complaints due for response in September, which presentented signifcant challenge; 57.1% were completed to time whic hwas a slight improvemnt compared to August. The year-to-date position stands at 67.%. The Division of Medicine receives the highest number of complaints, and is facing most difficulty in completing on time, but have significantly improved their position during September. New complaints received in September remained above 30 therefore the pressure on clinical divisons and the central team will continue. Negative PALS contacts rose again in September, at 114. The team work with divisional leads to resolve these where possible in real time. Risks and Opportunities: Negative concerns may continue over the coming months given increased patient activity across the Trust. The substantive Complaints Manager has returned to work following an extended period of sickness absence; this has significantly strengthend the leadership within the complaints team.
September-2016
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Complaints Performance
2016/2017 2015/2016 Target
0
20
40
60
80
100
120
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Negative PALS Concerns
2016/2017 2015/2016
0
10
20
30
40
50
60
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Complaints Received
2016/2017 2015/2016
0
10
20
30
40
50
60
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Complaints due for Response
2016/2017 2015/2016
25

[4.7] RESPONSIVE DEMAND AND CAPACITY September-2016
4.7 Demand and CapacityIndicators for A&E attendances and blue lights show an increase against last year. The impact of the ambulatory clinics can be seen in our reduction of our conversion from A&E attendances to admissions. What is evident is our length of stay and Delayed Transfers of Care (DTOCs) have increase against this time last year. The root causes to the length of stay are currently being worked through the Discharge Task Force and the outcomes of this will be reported regularly through this section of the Board report. The initial outcomes of the discharge task force are currently in the QIPP paper for this month.
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Average Length of Stay - Emergency
2016/2017 2015/2016 Target
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Average Length of Stay - Elective
2016/2017 2015/2016 Target
0
50
100
150
200
250
300
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Attendances - Blue Light
2016/2017 2015/2016 Target
0
500
1000
1500
2000
2500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Attendances - Paediatrics (ex UCC)
2016/2017 2015/2016 Target
0.0%2.0%4.0%6.0%8.0%
10.0%12.0%14.0%16.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Attendances - Inpatient Conversion
2016/2017 2015/2016 Target
0
5
10
15
20
25
30
35
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Delayed Transfers of Care - Patients
2016/2017 2015/2016 Target
0
100
200
300
400
500
600
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Delayed Transfers of Care - Days Delayed
2016/2017 2015/2016 Target
110001150012000125001300013500140001450015000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Attendances - Total Attendances (A&E, MIU & UCC)
2016/2017 2015/2016 Target
26

ICT Strategy Update Governors Meeting, November 2016
27

The Journey …
The Trust is on a journey towards paperless working
28
The ICT Strategy Strategy – 5-year : 2013-18 Choice:
– Single integrated solution or Integrate existing systems
Approach:
– build on its investments since 2013 – cultivate organisation and governance – invest in infrastructure – develop digital capabilities
29

The Hillingdon Care Record
Clinical Documents
GP Summary Record
Risk Notifications
Coordinate My Care
Child Protection
Integrated Care
Electronic Record Developments – Aug ‘15 on
I
Integrated Care Care Information Exchange (NW London) - Accountable Care Provider (ACP)
Social Care - Admission/Discharge notifications
Co-design - Referrals/Discharge - eRS : application and interface development
Acute-to-acute transfers - Developing standards with NHSE
Hillingdon Care Record:
Patient Demographics
Patient Activity
Documents
Diagnostics
- Pathology reports
- Radiology reports
30

Digital Roadmaps
• Government spending review (Nov ‘15) – £1.4bn NHS IT to support the local Sustainability
and Transformation Plan (STP) • Digital Maturity Assessments
– providers required to complete by 15th January ’16 • Digital Roadmaps
– CCGs produced roadmaps by June ‘16 – Single roadmap for North West London
31
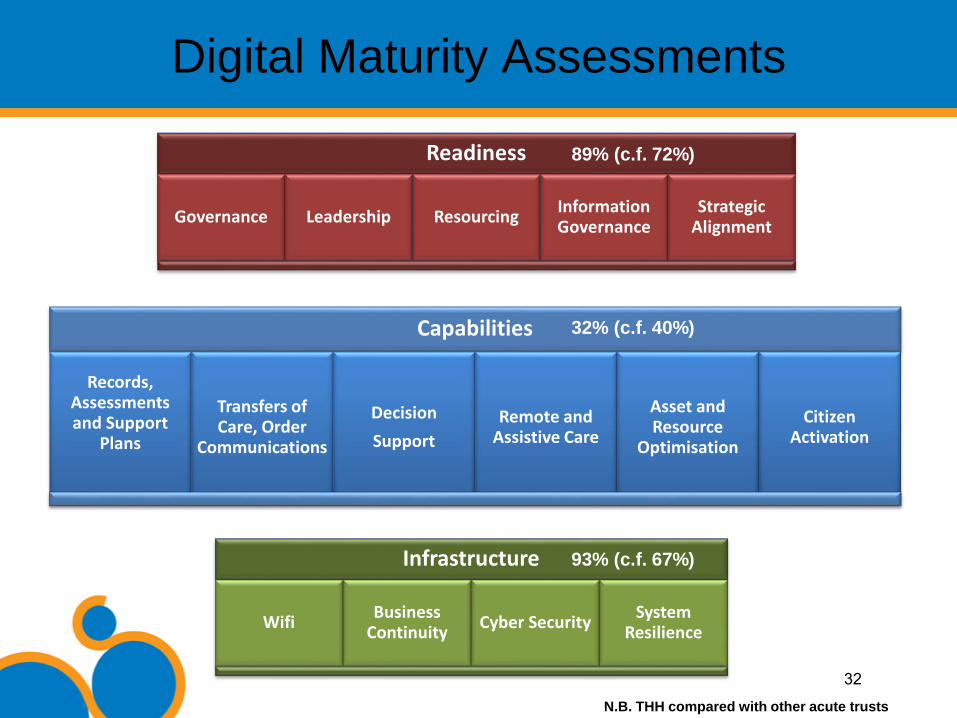
Readiness
Governance Leadership Resourcing Information Governance
Strategic Alignment
Capabilities
Records, Assessments and Support
Plans
Transfers of Care, Order
Communications
Decision Support
Remote and Assistive Care
Asset and Resource
Optimisation
Citizen Activation
Infrastructure
Wifi Business Continuity Cyber Security System
Resilience
Digital Maturity Assessments
89% (c.f. 72%)
32% (c.f. 40%)
93% (c.f. 67%)
N.B. THH compared with other acute trusts
32

Digital Capability – The Gaps • Hillingdon Care Record (HCR) development
– electronic forms (incl.VTE), vital signs monitoring/Early Warning Scores 2016-17
• Clinical Handover – pilot and roll-out, in 2016-17
• Electronic Document Management System (EDM) – includes the scanning/ digitisation of patient case notes, 2017-19
• Electronic Prescription and Medicines Administration (EPMA) – also referred to as e-Prescribing, 2017-19
• NHSmail 2 (incl. video-conferencing capability, 2016) • Clinical Decision Support (2018 - ) • Medical equipment integration (2018 -) • National systems (clinical portals, booking, electronic referrals) • Transfers of care (provider–to-provider)
33

ICT Strategy Refresh Informatics Strategy, July 2013 (5-year, 2013-18) Replaced with 3-year, rolling ICT Strategy (2016-19) • Aligned to NWL Digital Roadmap • Capital £11.699m (inclusive of £1.064m contingency, revenue£659k pa, rising to £1.183m pa - 0.49% of £239.3m income - by year 3)
• Funding for IT to support STP to be made available in ‘late autumn’, but not all of £1.4bn • Business cases developed for unfunded EDM and EPMA
‘big-ticket’ items • Funding requirements forwarded to NWL for inclusion in
investment plan
34