the hillingdon hospitals nhs foundation trust meeting … · the hillingdon hospitals nhs...
TRANSCRIPT
The Hillingdon Hospitals NHS Foundation Trust
Meeting of the Board of Directors
Wednesday 27th May 2015, 2.00pm Board Room, Mount Vernon Hospital
Paper
a) Introductory business
1. Welcome and apologies for absence -
2. Declaration of hospitality or amendments to the Register of Interests -
3. Minutes of the Board meeting held in Public on 29th April 2015
4. Actions Log
5. Declaration of Any Other Business -
6. Patient Story (TM) – for information -
7. Chair’s Oral Report (RS) – for information -
8. Chief Executive’s Report (SDG) – for information
b) Strategy
9. Shaping a Healthier Future Maternity Transition Readiness Assurance (JS) – for review
10. ICT Strategy: Delivery Update (PW) – for review
11. Trust Response to the Mid Staffordshire Public Inquiry (TM) – for information
c) Quality, Operational & Financial Performance
12. National Survey of Adult Inpatients 2014 (TM) – for review
13. Safer Staffing: Planned and Actual Staffing Levels (TM) – for review
14. Integrated Quality & Performance Report (JS / TM) – for review
15. Financial Report (PW) – for review
16. Transformation and QIPP Report (JS) – for review
17. Complaints PALS Annual Report (TM) – for review
d) Risk
18. Safeguarding (TM) – for information
19. Health & Safety Policy (PW) – for decision
e) Regulatory
20. Care Quality Commission Inspection Action Plan: Progress Update (TM) – for review
21. Annual Report and Accounts 2014/15 (PW / SDG / TM) – for decision
22. Annual Monitor Board Statements (TM) – for decision
f) Other
23. Report on Actions in Response to Kate Lampard Report on Themes and Lessons Learnt from NHS Investigations into Matters Relating to Jimmy Savile (TM) – for review
24. Emergency Preparedness Resilience and Response (JS) – for information
25. Appointment of the Senior Independent Director (RS) – for decision
26. Issues arising from the Board Committees – for information -
27. Use of Trust Seal – for information
28. Any Other Business -
29. Questions from the Public
This item is an opportunity for members of the public to ask questions to the Board on matters that relate to the Board agenda. Where possible, questions should be sent to David Coombs, Trust Secretary, by Monday 25th May 2015 in order that the Board can ensure the information is available to answer the question raised.
-
Date of next meeting:
• Wednesday 24th June 2015, Board Room, Hillingdon Hospital – 5.30pm
ITEM 3
Board Meeting in Public 27th May 2015
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST
MINUTES OF THE MEETING OF THE BOARD OF DIRECTORS HELD ON WEDNESDAY 29th APRIL 2015
IN THE BOARD ROOM, HILLINGDON HOSPITAL
Meeting held in public
Present:
Richard Sumray (RS) Chair Katey Adderley (KA) Non-Executive Director Carol Bode (CB) Non-Executive Director Shane DeGaris (SDG) Chief Executive Soraya Dhillon (SDh) Non-Executive Director
Abbas Khakoo (AK) Medical Director Lis Paice (LP) Non-Executive Director Pradip Patel (PP) Deputy Chair and Non-Executive Director Joe Smyth (JS) Chief Operating Officer Theresa Murphy (TM) Director of the Patient Experience &
Nursing David Searle (DS) Director of Strategy & Business Development
Richard Whittington (RW) Non-Executive Director Paul Wratten (PW) Finance Director
In Attendance:
Claire Gore (CG) Director of People David Coombs (DC) Trust Secretary (minutes)
Apologies:
None
Also Present: Helen Cobb (HC)* Assistant Director, Governance & Quality Standards Helen Hardy (HH)** Assistant Director of Nursing Catherine Holly (CH)*** Head of Patient & Public Engagement Nick Jenkins (NJ)**** Programme Director Rekha Wadhwani Public Governor Four members of public
* for items 18/04/2015 to 20/04/2015 ** for item 05/04/2015 *** for item 09/04/2015 **** for item 08/04/2015 ACTION 01/04/2015
Declaration of Hospitality or Amendments to Register of Interests
1
ACTION
None declared.
02/04/2015 Minutes of the last Meeting The draft minutes of the Board meeting held in public on 25th March 2015 were approved as an accurate record.
03/04/2015 Actions Log The Board reviewed the update on the actions arising from the Board meeting held in public on 25th March 2015 and those outstanding from previous meetings. DC updated the Board on action 20 and stated that the report on safeguarding is now scheduled for the May Board. The Board noted the update and agreed to remove those marked ‘complete’.
04/04/2015 Declaration of Any Other Business None declared.
05/04/2015 Patient Story TM welcomed HH to the meeting who provided feedback from the family of a patient with dementia who had been an inpatient as a result of urosepsis. HH stated that the patient’s family did not live locally and were unable to regularly visit. It was therefore important for the nursing staff to build up a strong personal relationship with the patient and her family. As part of this, the ward staff would ring the patient’s family to provide updates on her condition. The care provided had a profound effect on the family who wrote to thank the hospital. The Board welcomed the positive feedback and noted the positive impact of the dementia training. RS asked that the Trust’s annual report includes information on dementia training.
TM
06/04/2015 Chair’s Oral Report RS thanked CG and her team for organising the staff awards that were held last week. RS congratulated the winners of the awards, all those who were nominated, and also the staff who organised the event.
07/04/2015 Chief Executive’s Report SDG presented the report that updated the Board on a range of local, regional and national publications and developments. RS welcomed the announcement that the Trust will lead the
2
ACTION
development of the National Skills Academy for Health’s North West London Excellence Centre and asked that an update is provided to the Board at an appropriate time in the future. SDh referred to Monitor’s updated guidance on the integrated care licence condition and asked how the principles and behaviours will be taken forward in the divisions. SDG stated that these will need to be taken forward by the divisions in how they relate to each other. In terms of external working, SDG stated that the integrated care principles and behaviours are being picked up through the current work with the Shadow Provider Board. The Board noted the report.
CG
08/04/2015 Physician Associates CG presented the report that asked the Board to support the hosting of the National Physician Associate Expansion Programme (NPAEP) at the Trust. CG stated that the Programme Director has been appointed, and approval is now sought for the recruitment of the Physician Associates (PAs). RS asked about the implications of the second tranche of PAs being recruited through two northern consortia without Local Education and Training Board (LETB) input, in particular whether this increases the risk exposure to the Trust. NJ and SDG confirmed that there would be no additional financial risk as the funding would be provided prior to the PAs being recruited. Also, this second tranche would be recruited after the initial LETB coordinated PAs, which provides the opportunity to take stock and learn from the first recruitment. SDG advised the Board that the Trust has been successful in its bid for seven PAs out of the requested eight. The Board: 1. Noted the further development of the NPAEP. 2. Agreed that the Trust should continue to host the NPAEP
and that the programme should progress to begin the recruitment of the Physician Associates.
3. Agreed that there should be a further report back to the Board once there has been significant further progress with the programme (i.e. in at least six months time).
CG
09/04/2015 Equality, Diversity & Human Rights CG presented the report that updated the Board on key developments and progress in the area of equality and diversity. AK highlighted the low level of promotions amongst Black and
3
ACTION
Minority Ethnic (BME) staff. CG stated that the Trust has appointed an organisation to review the Trust’s policies and deliver training on ‘unconscious bias’. Also, the Trust is increasing the training and development programmes for junior staff groups, which have higher BME representation. KA asked whether there are any statutory or compliance issues in relation to equality, diversity and human rights. CG stated that there were not. CB noted the extensive action plan and asked which areas are the greatest priority. CG stated that these are ensuring recruitment, selection and promotion processes are fair; and addressing bullying and harassment. PW asked where the action plan will be tracked. CG stated that the Head of Workforce and Organisational Development will be establishing a working group to oversee progress. SDh asked whether the Trust is an outlier compared to other Trusts. CG stated that limited comparative information is available, however from the data that is available the Trust is broadly in line with other Trusts. The Trust will be looking to improve the information that is captured through the Electronic Staff Record (ESR). RS stated that he had a number of queries and comments on the action plan. For example, the reduction in turnover to 3% seemed overly ambitious, whilst a 1% improvement in an aspect of the staff survey did not seem ambitious enough. RS stated that he would meet with CG to pick up these issues and also discuss further the appropriate governance mechanism for overseeing progress with the action plan. The Board: 1. Noted the Trust’s workforce profile between November 2013
and October 2014 and the progress on the January 2014 report.
2. Noted the update on Trust equality objectives in relation to service delivery.
3. Agreed that RS would meet with CG to refine the action plan for implementation of a strategic equality and diversity plan informed by the new Workforce Race Equality Plan, and consider the most appropriate governance mechanism for overseeing progress.
4. Agreed that the updated action plan in light of point 3 would be circulated to the Board for information.
CG
10/04/2015 Delivering the Strategy 2014/15 DS presented the report that summarised the completion of the Board agreed objectives for 2014/15.
4
ACTION
KA referred to objective seven and asked whether there are any further service developments planned than pathology, dermatology and neuro-rehabilitation. JS stated that he would be meeting with the new Divisional Directors to discuss the service developments that the clinicians would like to take forward. RS stated that it would be helpful to bring the outcomes of these discussions back to a Board Seminar, unless this is covered at the Transformation Committee. PP confirmed that that the Transformation Committee receives a standing update on proposed service developments. PP suggested that the year is reviewed to reflect on the successes and those objectives that were not achieved, in order that the lessons that can be learnt. PP stated that this would enable the strategic ‘SWOT’ analysis to be updated. DS stated that this look-back has not been undertaken but agreed it could be helpful and suggested it could be overseen by the Trust Management Executive. RS referred to objective three and the stated next steps of focusing on the areas where the scores are consistently low. RS stated that it would be helpful to reference in future reports which areas are being focused on. The Board noted the report.
DS
11/04/2015 Safer Staffing: Planned & Actual Staffing Levels and Acuity & Dependency Review for A&E and Women’s and Children’s Wards RS asked that the paper on the acuity and dependency review is withdrawn from this meeting given that it was not clear what is being recommended to the Board. RS stated that the paper does not include a financial analysis of whether the investment referenced in the paper is possible, the impact of this investment, or whether this investment is supported by the Executives. RS stated that reports of this nature that refer to proposed expenditure must be supported by the Executive Team or Trust Management Executive prior to presentation to the Board. TM therefore presented the aspect of the item that outlined the planned and actual staffing levels for each inpatient ward in February. Fill-rates overall have increased, however the Acute Medical Unit (AMU) remains a concern with substantive staffing in place for 32 of the 46 beds. Fleming ward is also under pressure in terms of the senior nursing leadership. Whilst for Lister and Churchill wards, which are escalation wards, the substantive leadership is in place however the challenge is around the band five nursing.
5
ACTION
RS asked about the nursing vacancy rate. CG stated that this is approximately 15% which does not include those who have not yet started. CG stated that this is a transparent figure based on all beds, including the escalation beds. SDG highlighted the importance of having a clearly understood figure that can be tracked month on month. RS asked that this is included in the report on an ongoing basis. LP asked whether the Trust is an outlier in terms of the number of escalation beds open. JS stated that it is difficult to benchmark this issue, however anecdotally it is known that other Trusts have found it difficult to close escalation beds. CB stated that the discussion at the Quality & Risk Committee (QRC) highlighted the importance of transparency in how risk is balanced across the demands of finance and quality. SDG stated that the priority is ensuring sufficient staffing, which is demonstrated in the unprecedented agency spend and deterioration in the financial position. SDG stated that there is no block on booking agency staff when clinically required. SDh recommended that the issues around agency spend are subject to further re-examination. SDh asked whether the Trust has considered restricting those agencies for which there have been concerns about the quality of staff provided; whether the Trust is seeking regularity amongst agency nurses; and also whether enough is being done to develop the Trust’s temporary staffing bank. JS stated that the Trust has approached the most used agencies to seek regular lines of nurses for the next three to six months. There has been limited success as the nursing staff have sought to retain flexibility in their working patterns. TM stated that the key action remains to reduce the number of beds open. CG stated that work is underway with the Trust’s procurement team and the London Procurement Partnership to reduce costs. Analysis indicates that a key cost pressure is the use of ‘specials’ to provide one on one care and therefore a range of options are being explored as to how this support can be provided. CG stated that the Trust is constantly seeking to recruit staff to the bank. PP asked whether it would be sensible to over recruit Health Care Assistants (HCAs) to help provide cover for nursing vacancies. TM stated that the Trust is over subscribed with high quality applicants for HCAs and is therefore looking at over-recruiting to these roles in order to assist when patients require one to one supervision (‘specialling’). PW highlighted that the Trust is using more agency staff than there are vacancies and therefore it is important to be clear on why these staff are being used. JS stated that the processes around ‘specials’ are being tightened, and cover for sickness or other absence must be booked through the e-roster system and
CG
6
ACTION
therefore controlled. CG stated that there is also a focus on agency spend for medical staffing and stated that the Trust is looking to centralise the booking of locums which will have financial and quality benefits. RS welcomed the action being taken and asked for further information back to the Board on actions being taken in relation to the controls around the booking of specials and medical locums, and also the action being taken to recruit nursing graduates as they near the end of their training. The Board noted the report.
CG
12/04/2015 Quality and Operational Performance Report JS presented the report that covered the month of March, and which also included the first phase of the new integrated Board performance report. RS welcomed the new format of the report and stated that the next stage is to develop the analysis and information on the actions being taken to address areas of underperformance. CB advised the Board that the Quality & Risk Committee spent considerable time reviewing the quality indicators in detail and sought to identify the underlying issues. RS highlighted that a number of indicators still did not have a target at the end of the year. This prompted a wider discussion amongst Board members on the targets that are being set. It was agreed that it is important to be clear when setting targets on the level of aspiration within the target and whether these are realistic to achieve. SDh stated that she would be looking to see the analysis of the patient impact when a target is not met – for example, how long these patients are waiting for treatment. RS stated that this links to the next stage of the development of the integrated report, which is to develop the analysis on areas of concern. AK highlighted that in December 2014 the number of deaths was the highest in his time whilst Medical Director; however it is positive to note that the Standardised Hospital Mortality Ratio (SMR) for both weekday and weekend admissions was lower than the expected level. AK stated that this also reinforces the point that the acuity of the patients being seen has increased. The Board: 1. Noted the report and welcomed the generally strong year-
end performance. 2. Noted the actions in place to address areas of under-
7
ACTION
performance. 3. Supported the new integrated performance report.
13/04/2015 Financial Report PW presented the finance report for the end of the 2014/15 financial year and stated that the Trust ended the year with a deficit before exceptional items of £2.5m. This was £2.6m behind plan for the year. However, including exceptional items the deficit was £5.6m, which was £2.5m better than plan. The Trust’s Continuity of Services Risk Rating (CoSRR) remained a 3 (2.5). PW highlighted benchmarking information collected by NHS Providers which reported that for the 97 Foundation Trusts for which information was available, the average deficit was £2.7m; whilst for general hospitals this rose to £7.6m. KA asked why employee benefits and other expenditure increased in March and were out of line with the rest of the year. PW stated that underlying pay costs continued to increase month on month in the last quarter, and agency pay costs almost tripled over the year. PW stated that there were a number of cost pressures in March, including annual leave cover, CQC compliance costs, plus one-off liabilities around off-payroll engagements and partially completed spells. KA stated that when reviewing the 2015/16 financial position it will be important to remain mindful that the quarter four position in 2014/15 did not reflect the preceding part of the year. The Board noted the report.
14/04/2015 2014/15 Month 12 Transformation and QIPP Update JS presented the report that provided the year end position against the 2014/15 QIPP plan and provided an update on the development of the 2015/16 QIPP plan and multi-year transformation programme. JS updated the Board on the development of the 2015/16 QIPP programme and stated that since the report was written £8.4m of schemes have been identified against the target of £9.5m. JS stated that he is confident a further £0.5m of schemes have been identified, and additional schemes are being scoped to close the remaining gap. RS highlighted the importance of looking at clinical pathways and new roles. Whilst this may not be possible for the 2015/16 programme, such schemes should be developed for future years’ programmes. JS agreed and stated that the aim is for a QIPP programme that looks two to three years ahead.
8
ACTION
AK stated that the Clinical Assurance Panel (CAP) remains active and will become increasingly important as the QIPP programme becomes ever more challenging and the potential risks to quality increase. CG referred to RS’ comments and highlighted that workforce transformation is a key workstream in the transformation programme. PP agreed on the importance of multi-year planning for workforce transformation and stated that this coming year is likely to be one for planning the multi-year scheme, rather than delivering savings. The Board: 1. Noted the report. 2. Supported the 2015/16 QIPP programme to date.
15/04/2015 Freedom to Speak Up Review
CG presented the report that updated the Board on the review of whistle-blowing processes in the NHS overseen by Sir Robert Francis QC, and outlined the proposed actions at the Trust in response. KA asked how many cases had been raised under the formal whistle-blowing / raising concerns process in the last year. CG stated that there had been two cases. KA stated that given this low number, the informal processes for raising and resolving concerns are important. CG stated that the new confidential reporting line will help with the information gathering and analysis in this area. PP stated that the new Divisional Directors will have an important role in supporting these processes and suggested that they could be the independent champions for raising concerns. SDG stated that this requires further thought given the Divisional Directors’ role in the line management structure. RS agreed, and stated the champion role will be extremely challenging given the need to be seen as independent and available to staff. The Board: 1. Noted the report. 2. Supported the proposed actions by the Trust in response to
the review. 3. Requested feedback at a suitable point in the future on the
progress with the delivery of the actions.
CG
16/04/2015 Safer Staffing: Medical Template AK presented the report that set out medical staffing levels in the Women’s and Children Division. AK stated that the report had been requested given the imbalance in information
9
ACTION
reported on medical staffing levels compared to that for nursing staffing. AK highlighted that this has not been straightforward given there are few national and local standards to benchmark the data against; also that the doctors are not usually based in one particular ward. In terms of the risks identified in the report, AK stated that the single tier rota in obstetrics and paediatrics will be addressed by the Shaping a Healthier Future (SaHF) reforms. RS asked AK about the next steps in terms of future reporting. AK suggested that the junior doctor staffing could be addressed through the six monthly medical education reports, whilst Consultant staffing could be picked up through the reports on seven days services and SaHF. KA stated that the Board require an understanding of the gaps across the divisions and where the Divisional Directors have concerns about the staffing levels. AK proposed that this is addressed through the medical education report as this relates to the trainees and the positions filled. SDh suggested that further consideration is given to the reporting outside of the meeting and stated that this should link to the information on the divisional dashboards around weekend cover and medical staffing. RS asked about the level of risk arising from the single tier rotas. AK stated that the position in paediatrics has been addressed with the expansion of Consultant cover until 10pm in A&E six days a week. The move of gynaecological services to Fleming ward will address the issues in gynaecology, and the Director of Medical Education will also be acting on the feedback regarding the induction in gynaecology. RS asked whether this will alleviate the issue of the Trust being the only Trust in North West London with a single tier middle grade rota in obstetrics and gynaecology. AK stated that mitigations are in place and he did not feel there is a patient safety issue. SDG stated that whilst there are risks, these are being mitigated. The Trust has though made it clear that it can only receive the increased activity under SaHF if the second tier rota is in place. SDh recommended that the data is triangulated with other information such as complaints and incidents. The Board: 1. Noted the report and the key issues highlighted. 2. Agreed that a sub-group of NEDs (SDh, LP and KA) should
meet with AK to develop proposals for future reporting.
AK
17/04/2015 Response to the Morecambe Bay Investigation Report TM presented the report that outlined the Trust’s position against the issues identified in the investigation into maternity services at Furness General hospital. TM highlighted that the Care Quality Commission (CQC) inspection praised the
10
ACTION
governance and multidisciplinary working in the Trust’s maternity service, however it is important not to be complacent. RS proposed that a further report is brought to the Quality & Risk Committee (QRC) with greater information on the actions that are being taken in response to the report. CB stated that the QRC reviewed the governance in the Women’s & Children’s Division and were assured on the processes in place and that the gaps for further improvement had been identified. CB stated that she did not feel the Committee should monitor an action plan, but rather should continue to maintain a general oversight of governance in the division. The Board noted the report.
18/04/2015 Integrated Risk Register TM welcomed HC to the meeting who presented the high level risks on the integrated risk register following review by the Quality & Risk Committee (QRC) on 22nd April 2015. HC highlighted the changes to the high level risks since the last quarterly review by the Board and QRC. CB stated that the QRC reviewed the high and medium risks in detail. CB stated that whilst it is positive that the risk register is now reviewed by the Trust Management Executive (TME), the QRC is not though receiving the output of these discussions. CB stated that the QRC need to undertake a different role to other meetings and stated that this could be hindered by the fact the same format of information is reported to the Board, QRC and TME. CB stated that some risks have been graded red for some time, notably the risk around the high dependency care for children. A Board discussion is therefore required on whether this is an accepted position. CB advised the Board that the Committee were assured that the Trust is doing everything possible to ensure these services are safe; the issue is whether anything more could be done to address this risk. KA stated that it is also important to ensure there is sufficient time for the TME and QRC to review the amber risks. RS stated that there should be a pyramidal structure in which the Board only reviews the high risks. SDG endorsed this comment and stated that AK and TM should review and clarify the roles of the various governance groups in relation to the risk register, in conjunction with the chairs of these meetings. JS advised the Board that paediatric high dependency care has been again raised formally with the commissioners in the contract negotiations.
TM / AK
11
ACTION
RS stated that he would discuss with the relevant Executives outside of the meeting why the safeguarding risk had been upgraded given the focus on this area. The Board noted the report and the actions in place, and those planned, to mitigate the high risks.
19/04/2015 Health & Safety Report (Including Annual Report) PW presented the standard quarterly report on the Trust’s management of health and safety issues in the period January to March 2015. PW stated that the report also included annual information on 2014/15. The Board noted the report.
20/04/2015 Risk Management Strategy & Policy TM presented the updated Risk Management Strategy & Policy for the Board’s approval. HC highlighted that the three yearly review of the document was brought forward in light of the CQC inspection findings. The Board approved the updated Risk Management Strategy & Policy.
21/04/2015 Care Quality Commission (CQC) Inspection Report Action Plan Progress Update TM presented the report that provided an update on progress with the action plan developed in response to the CQC inspection. RS noted that the Trust has not received a reinspection from the CQC. SDG stated the mock inspection programme has though continued and the Trust also complied with the statutory requirements regarding the display of ratings. A number of Executives also met with Monitor last week to provide an update on progress with the action plan. RS asked why the venous thromboembolism (VTE) assessments are not being completed. AK stated that given the paper recording processes, the current performance underreports the current position. Compliance in the medicine division is now over 95%; compliance is however lower in surgery and is therefore being closely monitored by the Specialty Leads and Matron in the division. RS emphasised the importance of sustaining and embedding the actions and stated that this message must be fed back to the divisions from the Board. CB stated that this issue was reviewed in depth at the QRC where it was noted that the introduction of electronic
12
ACTION
recording would be a key factor in sustaining performance in the long-term. SDG stated that the terms of reference for the Root Case Analysis (RCA) of the CQC non-compliance are currently being finalised and will be circulated to the Board for comment. The Board noted the progress of the action plan.
22/04/2015 Research and Development Operational Capacity Statement The Board approved the updated Research and Development Operational Capacity Statement (RDOCS).
23/04/2015 Foundation Trust Membership TM presented the report that provided an annual update on membership recruitment and engagement during 2014/15. RS noted that the membership had reduced over the year. The Board: 1. Reviewed the report on the development and engagement of
the Foundation Trust membership. 2. Agreed a target of 7200 public members for 2015/16,
focusing on improving representation, engagement and replacing “lost members”.
24/04/2015 Issues Arising from the Board Committees Charitable Funds Committee (CFC) RS presented the report from the meeting of the Charitable Funds Committee on 9th March 2015. RS stated that the key recommendation is to increase the focus on fundraising through the recruitment of a fundraiser using the charitable funds already held. DS asked at what point the effectiveness of the fundraiser post will be reviewed. PW stated that he would expect this to be reviewed at the Charitable Funds Committee. DS asked whether the impact on the Trust’s communications and marketing functions had been considered. PW stated that the independent scoping report made clear the significant potential for fundraising at the Trust. The Board: 1. Noted the report and the issues highlighted. 2. Supported the recommendations from the Committee about
fundraising. 3. Agreed that the following should commence:
13
ACTION
• Improving the communication around the charity. • Identifying a suitable scheme at each of the Trust’s two
sites. • Recruiting a fundraiser using the existing funds held by
the charity. Audit & Assurance Committee (AAC) KA presented the report from the Audit & Assurance Committee meeting on 21st April 2015. KA stated that the Committee recommended that Board members undertake refresher training on fraud and bribery which could be undertaken online. KA stated that the Committee had a very productive discussion on estates compliance and agreed that the monitoring proposals should be refined and brought back to the Board for approval. KA reiterated the importance of management appropriately responding to internal audit reviews. KA stated that if management agree to the timescales for implementing the audit action plans then these must be complied with and staff held accountable. The Board noted the report and the issues highlighted.
25/04/2015 Use of the Trust Seal None to report.
26/04/2015 Any Other Business There was no further business to discuss.
27/04/2015 Questions from the Public Mrs Thomas asked whether the Trust is discussing the vacancy rate in the AMU with other Trusts. Mrs Thomas praised the Trust for allowing carers of patients with dementia to stay beyond visiting hours and asked whether this will be extended to carers of other patients. Mrs Thomas stated that this can relieve the pressure on staff as relatives can help at mealtimes and with personal care. Mrs Thomas also strongly recommended against moving to an online only system for seeking patient feedback. TM stated that the AMU is a challenging area to work given the significant patient throughput. Currently there are no courses to train nurses to work in an acute medical unit, but she has an aspiration to create this. Rekha Wadhwani welcomed the report on fundraising and stated that she will be interested to see how this progresses.
14
ACTION
RS stated that he would be looking for Governor and public involvement in this area.
Date of Next Meeting The next meeting is scheduled to take place on Wednesday 27th May 2015, at 2.00pm in the Board Room, Mount Vernon Hospital.
Richard Sumray Date Chair ……………………………………… ……………………………….
15
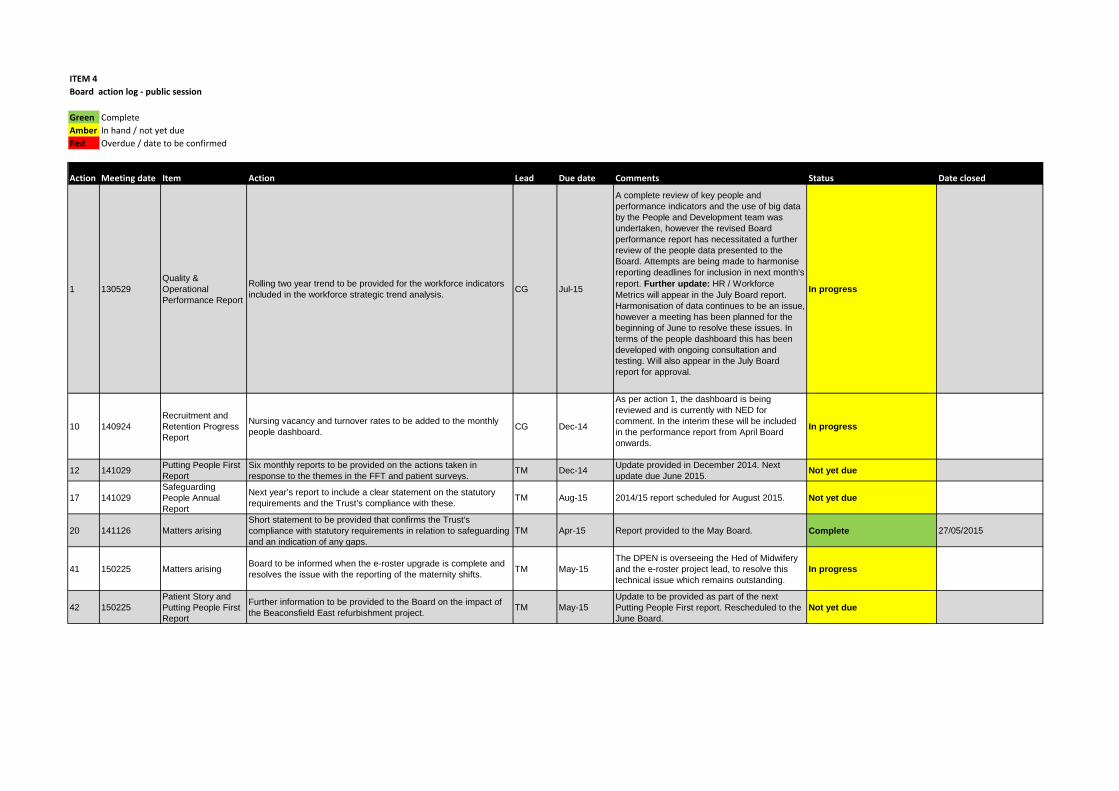
ITEM 4 Board action log - public session
Green CompleteAmber In hand / not yet dueRed Overdue / date to be confirmed
Action nMeeting date Item Action Lead Due date Comments Status Date closed
1 130529Quality & Operational Performance Report
Rolling two year trend to be provided for the workforce indicators included in the workforce strategic trend analysis. CG Jul-15
A complete review of key people and performance indicators and the use of big data by the People and Development team was undertaken, however the revised Board performance report has necessitated a further review of the people data presented to the Board. Attempts are being made to harmonise reporting deadlines for inclusion in next month's report. Further update: HR / Workforce Metrics will appear in the July Board report. Harmonisation of data continues to be an issue, however a meeting has been planned for the beginning of June to resolve these issues. In terms of the people dashboard this has been developed with ongoing consultation and testing. Will also appear in the July Board report for approval.
In progress
10 140924Recruitment and Retention Progress Report
Nursing vacancy and turnover rates to be added to the monthly people dashboard. CG Dec-14
As per action 1, the dashboard is being reviewed and is currently with NED for comment. In the interim these will be included in the performance report from April Board onwards.
In progress
12 141029 Putting People First Report
Six monthly reports to be provided on the actions taken in response to the themes in the FFT and patient surveys. TM Dec-14 Update provided in December 2014. Next
update due June 2015. Not yet due
17 141029Safeguarding People Annual Report
Next year’s report to include a clear statement on the statutory requirements and the Trust’s compliance with these. TM Aug-15 2014/15 report scheduled for August 2015. Not yet due
20 141126 Matters arisingShort statement to be provided that confirms the Trust's compliance with statutory requirements in relation to safeguarding and an indication of any gaps.
TM Apr-15 Report provided to the May Board. Complete 27/05/2015
41 150225 Matters arising Board to be informed when the e-roster upgrade is complete and resolves the issue with the reporting of the maternity shifts. TM May-15
The DPEN is overseeing the Hed of Midwifery and the e-roster project lead, to resolve this technical issue which remains outstanding.
In progress
42 150225Patient Story and Putting People First Report
Further information to be provided to the Board on the impact of the Beaconsfield East refurbishment project. TM May-15
Update to be provided as part of the next Putting People First report. Rescheduled to the June Board.
Not yet due
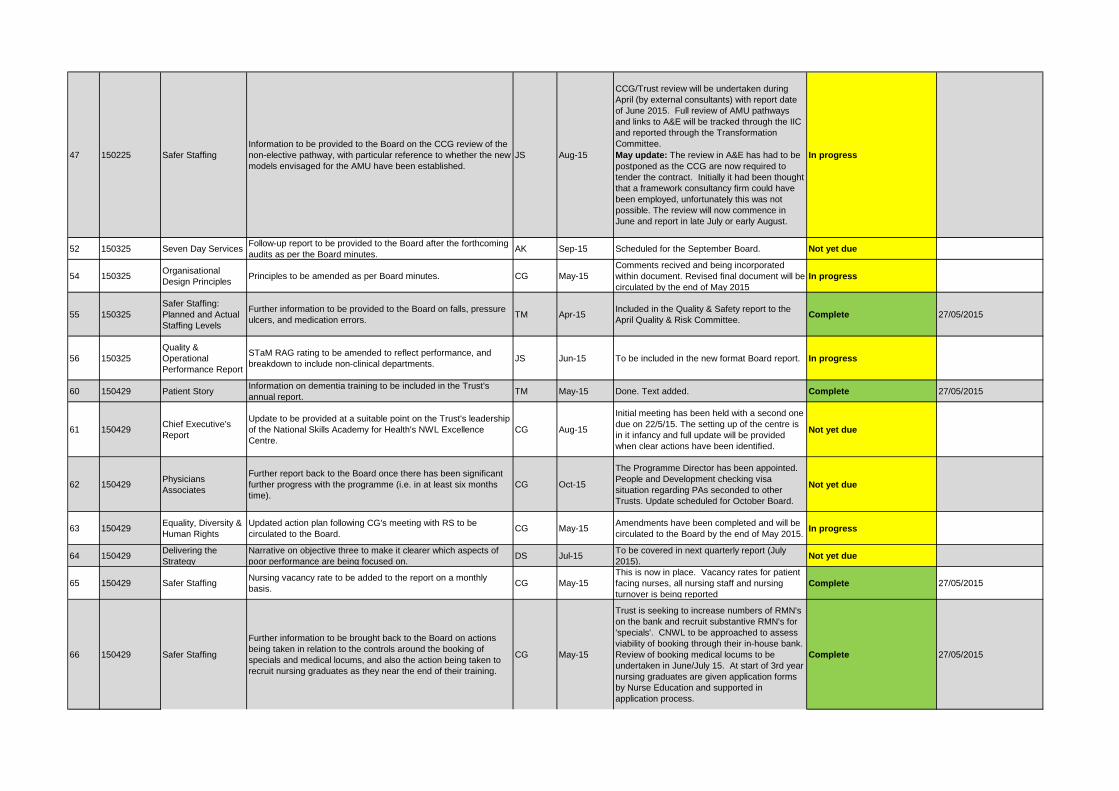
47 150225 Safer StaffingInformation to be provided to the Board on the CCG review of the non-elective pathway, with particular reference to whether the new models envisaged for the AMU have been established.
JS Aug-15
CCG/Trust review will be undertaken during April (by external consultants) with report date of June 2015. Full review of AMU pathways and links to A&E will be tracked through the IIC and reported through the Transformation Committee. May update: The review in A&E has had to be postponed as the CCG are now required to tender the contract. Initially it had been thought that a framework consultancy firm could have been employed, unfortunately this was not possible. The review will now commence in June and report in late July or early August.
In progress
52 150325 Seven Day Services Follow-up report to be provided to the Board after the forthcoming audits as per the Board minutes. AK Sep-15 Scheduled for the September Board. Not yet due
54 150325 Organisational Design Principles Principles to be amended as per Board minutes. CG May-15
Comments recived and being incorporated within document. Revised final document will be circulated by the end of May 2015
In progress
55 150325Safer Staffing: Planned and Actual Staffing Levels
Further information to be provided to the Board on falls, pressure ulcers, and medication errors. TM Apr-15 Included in the Quality & Safety report to the
April Quality & Risk Committee. Complete 27/05/2015
56 150325Quality & Operational Performance Report
STaM RAG rating to be amended to reflect performance, and breakdown to include non-clinical departments. JS Jun-15 To be included in the new format Board report. In progress
60 150429 Patient Story Information on dementia training to be included in the Trust's annual report. TM May-15 Done. Text added. Complete 27/05/2015
61 150429 Chief Executive's Report
Update to be provided at a suitable point on the Trust's leadership of the National Skills Academy for Health's NWL Excellence Centre.
CG Aug-15
Initial meeting has been held with a second one due on 22/5/15. The setting up of the centre is in it infancy and full update will be provided when clear actions have been identified.
Not yet due
62 150429 Physicians Associates
Further report back to the Board once there has been significant further progress with the programme (i.e. in at least six months time).
CG Oct-15
The Programme Director has been appointed. People and Development checking visa situation regarding PAs seconded to other Trusts. Update scheduled for October Board.
Not yet due
63 150429 Equality, Diversity & Human Rights
Updated action plan following CG's meeting with RS to be circulated to the Board. CG May-15 Amendments have been completed and will be
circulated to the Board by the end of May 2015. In progress
64 150429 Delivering the Strategy
Narrative on objective three to make it clearer which aspects of poor performance are being focused on. DS Jul-15 To be covered in next quarterly report (July
2015). Not yet due
65 150429 Safer Staffing Nursing vacancy rate to be added to the report on a monthly basis. CG May-15
This is now in place. Vacancy rates for patient facing nurses, all nursing staff and nursing turnover is being reported
Complete 27/05/2015
66 150429 Safer Staffing
Further information to be brought back to the Board on actions being taken in relation to the controls around the booking of specials and medical locums, and also the action being taken to recruit nursing graduates as they near the end of their training.
CG May-15
Trust is seeking to increase numbers of RMN's on the bank and recruit substantive RMN's for 'specials'. CNWL to be approached to assess viability of booking through their in-house bank. Review of booking medical locums to be undertaken in June/July 15. At start of 3rd year nursing graduates are given application forms by Nurse Education and supported in application process.
Complete 27/05/2015
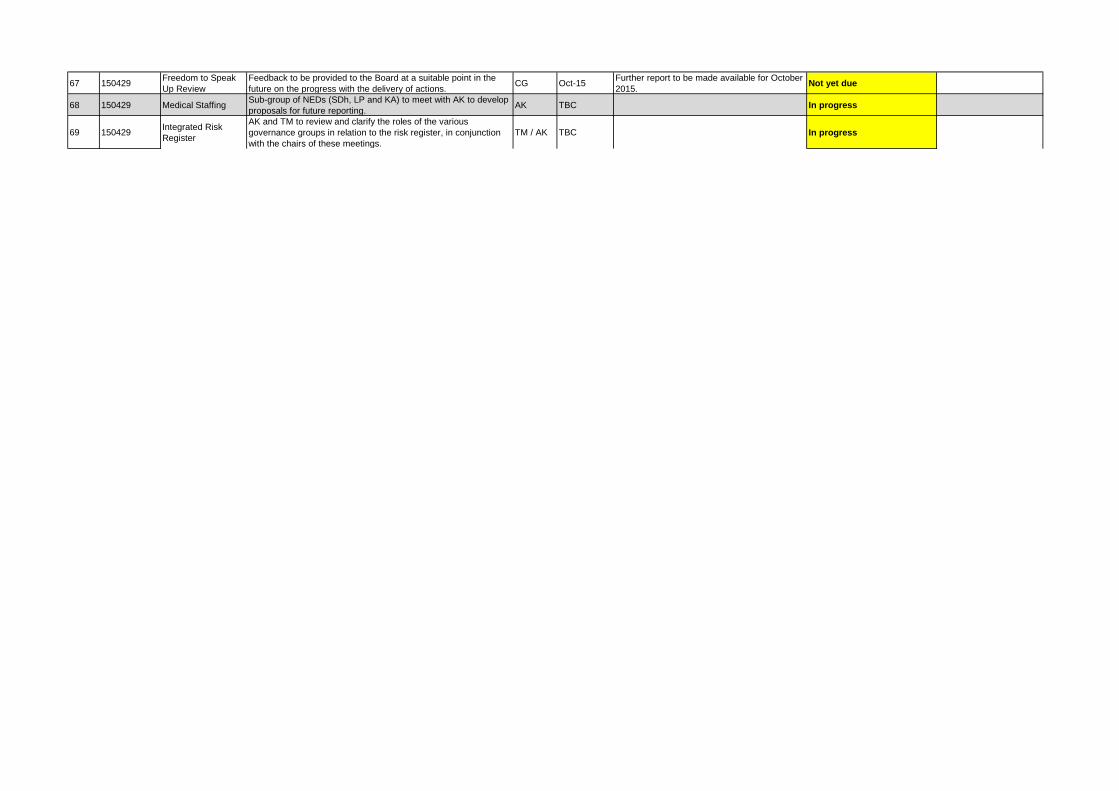
67 150429 Freedom to Speak Up Review
Feedback to be provided to the Board at a suitable point in the future on the progress with the delivery of actions. CG Oct-15 Further report to be made available for October
2015. Not yet due
68 150429 Medical Staffing Sub-group of NEDs (SDh, LP and KA) to meet with AK to develop proposals for future reporting. AK TBC In progress
69 150429 Integrated Risk Register
AK and TM to review and clarify the roles of the various governance groups in relation to the risk register, in conjunction with the chairs of these meetings.
TM / AK TBC In progress
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 8
Chief Executive’s Report Reason for item: This is a standard monthly report to the Board that seeks to ensure the Board is informed of key issues not otherwise covered in the agenda papers. Summary: The report updates the Board on a range of issues including local, regional and national strategic developments, recent publications, and developments at the Trust not otherwise covered in the Board reports. As such, it seeks to provide context to the Board’s discussions. This month’s report includes information on the Care Quality Commission’s (CQC) re-inspection of the Trust, the Trust’s nomination for a national award, and the general election outcome. Board Action required: The Board is asked to: 1. Review the report and agree any further actions as required. Report from: Shane DeGaris, Chief Executive Links to Trust strategic priorities: • The report is relevant to all of the strategic priorities. Previous consideration at Board or Committees: n/a. Equality and diversity considerations: none. Financial implications: There are no direct financial implications arising from this information report.
1
Chief Executive’s Report 1. Care Quality Commission (CQC) re-inspection CQC inspectors undertook a re-inspection of the Trust on 5th and 7th May, in which a small team visited a number of areas including A&E, Theatres, Peter Pan and Bevan Wards. They also interviewed a number of staff to find out how well we have addressed the issues they identified in their comprehensive inspection in October 2014. The inspectors’ key areas of focus were infection control, cleanliness and child safeguarding. They were also keen to establish the Trust’s compliance with staff training and understanding on the Mental Capacity Act (MCA) and DoLS (deprivation of liberty safeguards). Initial verbal feedback was positive, but the Trust awaits formal feedback on the outcome. 2. HSJ awards The Trust has been shortlisted in the Health Service Journal (HSJ) top 100 places to work in healthcare. The list includes mental health and community trusts, acute trusts and clinical commissioning groups. The HSJ and Best Companies Group (BCG) used the NHS staff survey findings to analyse each organisation across seven core areas: • Leadership and planning • Corporate culture and communications • Role satisfaction • Work environment • Relationship with supervisor • Training and development • Employee engagement and employee satisfaction.
An awards lunch is being held on 7th July at the Patient Safety Congress in Birmingham. This is a great achievement and recognition of the extensive work to engage our staff in the significant challenges facing the Trust. 3. General Election Nick Hurd and John McDonnell and were re-elected for further terms for their respective constituencies (Ruislip, Northwood & Pinner and Hayes & Harlington), whilst Boris Johnson is the new MP for Uxbridge & South Ruislip. We hope to continue our close working with the three Hillingdon MPs over the coming years, in particular on the key strategic issues such as integrating care in Hillingdon and looking at how to develop our estate.
2
In terms of Government appointments, the Rt Hon Jeremy Hunt MP continues as Secretary of State for Health, whilst David Prior has stepped down as chair of the Care Quality Commission to become a health minister. The Prime Minister used his first major post-election speech on 18th May to commit to a pre-election pledge to increase budgets by at least £8bn a year by 2020. The speech also included a vow to create a ‘seven-day’ health service. Shane DeGaris Chief Executive 18th May 2015
3
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 9
Shaping a Healthier Future (SaHF) Maternity Transition Readiness Assurance Reason for item: This report forms part of the assurance process for Shaping a Healthier Future (SaHF). Summary: • Plans to transfer maternity, neonatal and gynecology services from Ealing Hospital
are well under way. • Transitional funding has been requested and is agreed. • Recruitment is underway and good progress has been made on increasing the
midwifery and neonatal nurse establishment. • The Trust is required to issue official confirmation on its preparedness at the May
public Board meeting. Action required: The Board is asked to discuss and confirm the Trust’s readiness to proceed with a safe transition of maternity and neonatal services in line with the planned timescale. Report from: Liz Weller, SaHF Programme Manager Report sponsor: Joe Smyth, Chief Operating Officer Links to Trust strategic priorities: • To develop sufficient sustainable scale to enable us to improve and grow healthcare
services for our communities Previous consideration at Board or Committees: February and April Private Board meetings. Equality and diversity considerations: None Financial implications: There are no direct financial consequences arising from this report. A final revenue and capital budget has been prepared and is undergoing refinement and sensitivity analysis.
1
Operational Readiness for Maternity Transition 1. Background The decision on the date to close Ealing Maternity services has been postponed until at least 20th May as Ealing Clinical Commissioning Group (CCG) required further clarification on the state of operational readiness. Comprehensive action plans to ensure the safe transition of services are being developed within the Trust and across the sector. 2. Maternity The division is undertaking an extensive recruitment campaign to increase the number of midwives and midwifery support workers. Good progress has been made to date with further interviews scheduled for mid-May. A number of midwives will transfer from Ealing once services cease there, and the Trust will use bank and agency staff to fill any temporary vacancies whilst substantive posts are being filled. Health Education North West London (HENWL) have agreed further funding for a band 7 Practice Development midwife to support an increased number of preceptees. The division are currently establishing ambulatory pathways for Day Assessment and Triage services to reduce antenatal admissions. Antenatal and community services will be provided in the Ealing area from Children’s Centres and three Health Centres. 3. Neonatal Recruitment is also ongoing for additional neonatal nurses to provide transitional care alongside midwifery support. This service is for low-risk babies requiring further support (e.g. IV antibiotics, phototherapy) but not requiring NNU/SCBU level care. Temporary staff will be used as necessary to fill gaps whilst substantive posts are being filled, dependent on the number of women booked to deliver post-transition. 4. Obs & Gynae medical staff The Trust requires four additional medical registrars to fill the essential second tier rota. The Trust has been informed by HENWL that 2.8 posts will transfer, and the Trust has advertised for additional Trust Grade locums to cover the gap. The Trust has received confirmation that SaHF funding will be provided to underwrite the costs of over recruitment in the event that transition in June does not go ahead. 5. Capital requirements The estate is being reconfigured and remedial work will be undertaken, to include
• Building work on Fleming to allow the transfer of Early Pregnancy Assessment Unit (EPAU) from Marina
• Works on Marina to install security access controls beyond existing EPAU
2

• Minor works on the ground floor of maternity in offices and existing triage to provide additional antenatal consulting rooms.
Post reconfiguration, Marina will consist of an expanded triage area, four day-care beds, six transitional care plus two postnatal beds. A new Midwifery led unit will operate on Katherine ward in the space vacated by day-care (trialled successfully during the labour ward refurbishment). Additional equipment will be required, most significantly an ultrasound scanner to enable the relocation of EPAU to Fleming, which has been ordered and will be delivered on time to ensure a safe and timely transfer of service. 6. Next Steps The Board is asked to confirm the Trust’s readiness to proceed with a safe transition of maternity and neonatal services in line with the planned timescale.
3
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 10
ICT Strategy Delivery Update Reason for item This is an item the Board requested for periodic update. Summary New IT infrastructure is now being utilised with a Guest WiFi available for use by patients, the public and staff, and the trials of mobile devices with staff and patients (for the Friends and Family Test) are in progress. The application development tools for developing the Clinical Viewer for the electronic Hillingdon Care Record were procured and the first release of the viewer is expected to be trialled by clinicians on mobile devices during May 2015. Access to the electronic record is essential to introducing new ways of working in the Trust and integration across the wide care economy for the delivery of safer and more cost-effective care. In undertaking the integration work with GP systems the Trust met 100% of its £1.2m CQUINs in 2014/15. Board Action required The Board is asked to note: 1. The successful delivery of the ICT programme during 2014/15. 2. Progress with the Hillingdon Care Record (HCR), and to review the risks
associated with the development approach.
Report from: Charles Yeomanson, Director of ICT Report sponsor: Paul Wratten, Finance Director Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient
experience and the quality of care we provide.
• To deliver high quality care in the most efficient way. Previous consideration at Board or Committees: n/a Equality and diversity considerations: none. Financial implications: Use of resources to achieve service improvement, innovation and efficiency, especially for IT, is a key issue for the Board. Delivery of the benefits of the Board approved informatics strategy is therefore an important matter for the Board to monitor.
ICT Strategy Delivery Update
1. Introduction In July 2013 the Board approved a new 5-year ICT strategy with the aim of achieving an integrated digital care record by 2018 by bringing together best of breed systems. This report provides an update on progress against the strategy in the 2014/15 financial year and summarises next steps in 2015/16. 2. Infrastructure In order to provide the means of access to information systems both internal and external to the Trust, significant investment was made in 2014/15 in a wireless network, new internet connections with firewall security and a mobile device management solution. These technologies were deployed within the overall budget and to schedule. Since April 2015 the new connectivity has enabled the provision of a Guest WiFi service for use by patients, the public and staff on the Hillingdon site and from May 2015 at Mount Vernon Hospital. Authorised Trust laptops were trialled on the new Wireless Network in March 2015 and connectivity is since being rolled out to all such devices. Configuration of the Mobile Management system is now progressing alongside trials of mobile devices. A pilot of the ‘RaTE’ system for undertaking Friends and Family Test surveys and audits electronically, using mobile devices, also started in March 2015 and is due to complete in May 2015. Improvements in access to information services have been achieved by configuring multiple logins on selected PCs across the Trust in the first months of 2015. Upgrades to email services completed in April 2015 and mailboxes have been expanded significantly to avoid considerable time being spent by staff in managing their mailbox space. Work is now progressing on the configuration of the new firewall and Mobile Management security systems that will permit wider remote access to Trust email and support synchronisation with mobile phones other than the current Trust BlackBerry devices. 3. Integration Over 30 system interfaces have now been implemented with the Trust Integration Engine (TIE) permitting patient demographics on information systems to be kept in step with the Trust’s Patient Information System (PAS) and electronic documents from both PAS and departmental systems to be shared. Following the ‘Docman’ system going live in August 2014 84% of outpatient attendance letters and A&E discharge letters were being sent electronically via the TIE with significantly reduced manual intervention. This was over and above the target set by our commissioners of 60% for the period and amounted to 40,000 letters sent via the system in Q3 for Hillingdon GPs alone. The Trust has since gone on to achieve its Q4 target of 90%. This has improved patient safety by ensuring that key patient information is available to patients’ GPs in a timely and secure manner. Access to patient records in Hillingdon GP systems was also provided in December 2014 for staff working primarily in A&E, Pharmacy and Paediatrics. Further, the national Summary Care Record was deployed in the Trust in March 2015. This is proving very useful for out-of-area patients with between 200 and 300 records being viewed per week.
Page 1 of 5
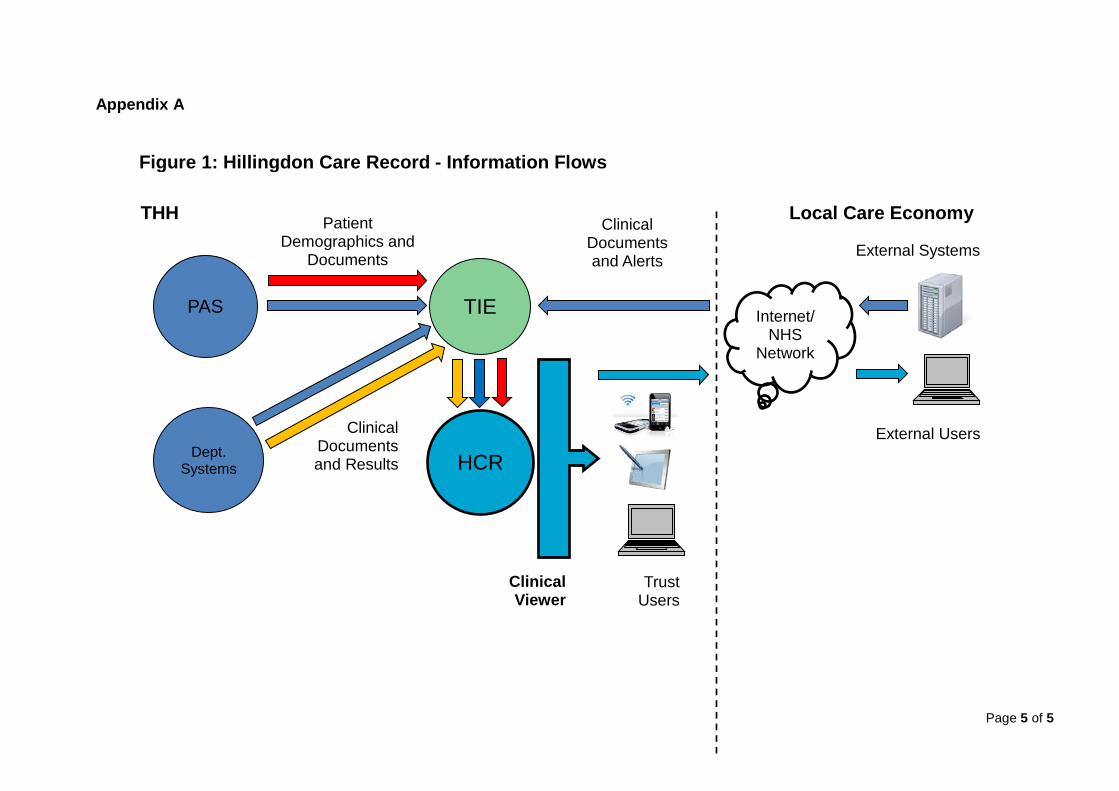
As a result of successfully delivering these initiatives ICT has enabled the Trust to achieve 100% of its IT data sharing Commissioning for Quality and Innovation targets (CQUINS) worth £1.2m in 2014/15. Having achieved the two year CQUINS in the first year the data-sharing CQUINS for 2015-16 will provide alerts and improved patient data flows necessary to build the Trust’s own electronic patient record; the Hillingdon Care Record (HCR). 4. Clinical Systems Since the business case for the Hillingdon Care Record (HCR) was approved by the Trust Board in November 2014 the core patient record system is being built from information passed through the TIE from Trust systems. The architecture of the initial HCR with the information flows is shown in Figure 1 in Appendix A. The initial system is to include patient demographics, activity and letters. The software tools for developing the Clinical Viewer have also been procured and installed and the first release has been built and is being tested. Trials by clinicians on mobile devices are expected to commence during May 2015. Developments in 2015/16 During 2015/16 the HCR and Clinical Viewer will be developed further to incorporate Pathology and Radiology results and made available across the Trust. In A&E the HCR will provide a single portal for accessing patient records that will address an issue raised in the CQC full inspection. To support the transformation agenda in 2015/16 a project to provide electronic clinical handover, integrated with patient flow, is to be delivered. This should enable significant efficiency benefits and improve the quality of information and patient care. HCR Development Risks Some concern was expressed by the Board in November 2014 at the risk associated with an in-house development. The risk can be mainly attributed to the small number of staff involved in the development of the HCR and associated with staff leaving or not having the capacity to develop the system in a timely manner. The risk is being mitigated by developing the HCR predominantly with an open, Web-standard language (HTML5) for the clinical viewer and using a Microsoft SQL database for the patient record. There is a great deal of skills in the marketplace for both technologies and the system is well-documented. Both the TIE and the clinical viewer of the HCR can be regarded as a part of the ‘glue’ in the architecture that allows access to the patient record from the various information systems. As there is constant change to these systems the Trust needs the capability and flexibility to continually create and update the HCR. Further, the software toolset will permit other ‘app’ development and avoid costs in the future. The initial HCR development has been fast-tracked using the software supplier’s professional services and working with the supplier there has been knowledge transfer to Trust staff; three currently have the expertise to develop both in the TIE and HCR environments to provide resilience and capacity. In summary, the risks with the integration and development approach have been addressed and the mitigations in place are felt to be sufficient at this time to reduce the risk to an acceptable level.
Page 2 of 5
PACS Following the replacement of the PACS system in July 2014 the Trust completed the localisation of its imaging data out of the London data centre in January 2015 well ahead of the July 2015 deadline. Financial benefits in excess of £113k pa over the lifetime of the contract are being realised. The replacement system also provides new functionality such as 3D reconstructions and the separate management of teaching files. The system was upgraded in April 2015 to the latest version of Sectra PACS that will enable voice recognition to be introduced for reporting in this multi-phased project. Further efficiencies and timeliness of radiology reporting should be achieved and this will help the Trust to reduce its reporting backlog. 5. Informatics The Informatics function within ICT has continued to support the Trust throughout 2014/15, ensuring;
• timely operational information is available via the Trust’s business intelligence solution, iReporter;
• submission of external reports for secondary uses and contracting; • audits of data quality; and • coding of patient episodes. During the year use of the Trust’s Business Intelligence system, iReporter, had got to the point where a hardware upgrade was required. This will be undertaken during 2015/16. In the longer-term new tools will be required to support the future analytical requirements of the organisation and an option appraisal is to be undertaken during the year. The information transacted with Hillingdon CCG for contractual purposes has changed year-on-year and has required regular changes to iReporter. For 2015/16 the contractual data set changes are significant and major changes are required to iReporter. The Trust is working closely with Hillingdon CCG to ensure that the new system is effective and efficient and doesn't unduly affect payments. 6. ICT Services As the Trust’s business becomes even more reliant on ICT and moves towards 24x7 working it is essential the ICT service is robust, responsive and is delivered cost-effectively. Further, there are requirements that new healthcare systems comply with the NHS Information Standards Board (ISB) standards (ISB-0160 for clinical risk management in the implementation of health systems) and the Information Governance Toolkit (for the management of ICT system security). To meet these objectives it is important further controls are established for the procurement, implementation and maintenance of ICT systems. These will also serve to reduce the Trust’s risk exposure. A programme of work has been put together to develop the ICT service from what is mostly a reactive towards a proactive service. The initial key changes are: • Centralisation of service management (in line with ITIL industry best practice) • ICT Service Desk move from Mount Vernon Hospital to Hillingdon Hospital • Introduction of monitoring of ICT systems and alerting. The main ICT Service Desk has already moved from the Mount Vernon Hospital to the Hillingdon Hospital site providing a more resilient and responsive service and extended hours for new user account creation. Further, the Trust’s ICT maintenance costs have been identified and centralised.
Page 3 of 5
7. Strategy Review An initial review of the Informatics Strategy in July 2014 identified a re-sequencing of developments to provide Hillingdon Hospitals with an integrated digital care record and the need to develop the ICT service to support the investments most effectively. Subsequently a review of the finances for the programme was undertaken in December 2014 to inform the capital plans for 2015/16. Some of the larger developments scheduled from 2016 are: • Electronic Document Management System (EDM, for digitisation of patient
case notes) • Electronic prescribing (e-Prescribing) • Replacement of the main Hillingdon telephone switch. A formal review of the ICT Strategy has begun that will take into account the following: • NHS Five Year Forward View (October 2014); • Personalised Health and Care 2020 (NHS Informatics Board, November 2014);
and • Shaping a Healthier Future, SaHF (including NWL Whole Systems Integrated
Care developments). The refreshed Strategy will be brought back to the Board for approval in 2015. Charles Yeomanson Director of ICT
Page 4 of 5
Appendix A
HCR
TIE
Dept. Systems
PAS
Clinical Viewer
Clinical Documents and Results
THH Local Care Economy Clinical Documents and Alerts
Internet/NHS
Network
External Users
Patient Demographics and
Documents
Figure 1: Hillingdon Care Record - Information Flows
External Systems
Trust Users
Page 5 of 5
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 11
Trust Response to the Mid Staffordshire NHS Foundation Trust Public Inquiry (Francis) Report Reason for item: To provide an update to the Board on the action taken by the Trust in response to the Public Inquiry report. Summary: This report sets out the Trust’s progress with implementation of the recommendations in the Mid Staffordshire NHS Foundation Trust Public Inquiry chaired by Robert Francis QC (Francis Report) and the Government’s response in Hard Truths-The Journey to Putting People First. It demonstrates that there has been significant progress towards implementing the recommendations and identifies a number of actions that should be considered or implemented. Board Action required: The Board is asked to: 1. Review the response overview. 2. Discuss and agree the further actions identified. Report from: Bev Hall, Deputy Director of Nursing and Patient Experience Report sponsor: Theresa Murphy, Director of the Patient Experience and Nursing Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience
and the quality of care we provide. Previous consideration at Board or Committees: None Equality and diversity considerations: None Financial implications: none directly arising from the report.
1
Trust Response to the Mid Staffordshire NHS Foundation Trust Public Inquiry (Francis) Report
1. Introduction This report sets out the Trust’s progress with implementation of the recommendations in the Mid Staffordshire NHS Foundation Trust Public Inquiry chaired by Robert Francis QC (Francis Report) and the Government’s response in Hard Truths-The Journey to Putting People First. 2. The Francis report 290 recommendations The recommendations can be grouped into five key themes:
• Clearly understood fundamental standards and measures of compliance • Openness, transparency and candour throughout they system • Improved support for compassionate and committed nursing • Strong and patient centred healthcare leadership • Accurate, useful and relevant information.
Approximately 120 recommendations apply to the acute hospital setting, or will impact in terms of reforms and changes, which as a result, we may be required to undertake. 3. Hard Truths- The Journey to Putting Patients First This report provided the Government’s detailed response to the 290 recommendations made in the Francis report. All the recommendations are accepted either in part, in full or in principle. It outlined a five point plan to revolutionise the care that people receive from the NHS and put an end to failure:
• Preventing problems • Detecting problems quickly • Taking actions promptly • Ensuring robust accountability • Ensuring staff are trained and motivated.
4. Overview of Trust Actions In relation to understanding and responding to the Francis report the Trust had a wide ranging approach, an overview is provided in the graphic below.
2
5. Update on THH progress: The next section provides an overview of our progress under key theme headings 5.1 Staffing: • Nursing establishment reviews are undertaken twice yearly and presented to
Board. Staffing is benchmarked against national guidance, for example NICE or best practice where they are available, evidence based tools are used to inform the review and decision making.
• Safe staffing policy in place, this contains a clear escalation procedure for staff to use if they believe that staffing levels are insufficient to provide safe care. Staff have access to and can also report any concerns via the datix system. Sub- optimal staffing levels reported by staff are shown on the Safer Staffing monthly Board report
• Staffing levels are displayed in a visible place on each ward • To strengthen the identification of healthcare support workers and nurses, a
poster is displayed on each ward that includes a photograph showing the different uniforms of nurses who may be seen alongside an overview of their role. Similar information is available in the Bedside Guides. The ‘Hello, my name is…’ campaign discussed at induction also encourages all staff to introduce themselves by name and role.
• In relation to public disclosure, the Trust has a Raising Concerns at Work Policy (formerly known as the Whistleblowing Policy) in place that is available to all staff. The Trust Policy adheres to the principles contained within the Public Interest Disclosure Act (PIDA), which came into force in 1988, and gives employees protection under the law by stating that employers should not victimise any employee who raised a concern internally or to a prescribed regulator.
• To engage with staff and gain staff feedback the Trust participates in the annual staff survey and has fully implemented the Staff Friends and Family Test with results available and accessible on the Trust intranet.
• Exit interviews are in place for all leavers although the uptake is low. • All levels of nursing forum are structured to enable nursing staff to give feedback
about working life and experiences ‘from the frontline’ • Doctors’ revalidation requires doctors to obtain feedback every five years- the
Trust has invested in an external system called Equiniti 360 to help facilitate this process.
• Clarity about roles and responsibilities, team structures, team working are provided through job descriptions (JDs). Although JDs include accountability they do not all provide a description of the team structure. Staff receive a Trust and a local induction.
• Appraisals have been strengthened and include an assessment of attitude and behaviour against the Trust values. Appraisal training is available to managers and appraisal awareness is available to all staff to help them to get the best out of the appraisal process .Appraisal rates are monitored.
• Following on from the Cavendish review, the Induction Care Certificate has been successfully piloted within the Trust for both new starters and current healthcare assistants. It is due to be rolled out nationally in spring 2015. We are continuing to implement the Induction Care Certificate throughout the Trust. In 2015 there
3
will be a pathway for healthcare assistants who would like to develop themselves within their role.
Further action: • Organise forums for new starters to give them the opportunity to provide
feedback from a ‘fresh eyes’ perspective. • Consider implementing a method to capture feedback from staff following their
appraisals- ‘how was it for you?’. • Incorporate team structure graphic into job descriptions. • Reconsider supervisory ward sister/charge nurse role and include the appraisal in
the twice yearly establishment review. Information gained from the care contact work will help to identify how ward sisters currently spend their time.
5.2 The Board /Leadership • The Trust Board has a Medical Director and Director of Patient Experience &
Nursing. • Currently there are no former nurses as Non-Executive Directors (NEDs),
although our present NEDs bring experience and knowledge from different walks of life including clinical backgrounds.
• All Public and Staff Governors have been through an induction process and a Governor Development Programme delivered by NHS Providers.
• A Governor questioning and challenging session is also planned, delivered by NHS Providers.
• There is a membership engagement strategy in place to support communication with membership. Quarterly People in Partnership (PiP) sessions are scheduled and held on Trust premises and in the community, all sessions include time for Q&A, these are also published on the Trust website
• The Trust has a Leadership Strategy in place that sets out a structured approach to developing leadership capability at all levels across the Trust. There are Leadership development programmes such Leadership 100, available to staff
• Divisions are clinically led with Clinical Directors and Assistant Directors of Nursing leading clinical care alongside Assistant Director of Operations.
• Speciality Leads are now in place within each division, with time allocated within their job plans to lead the service
• The Trust does not necessarily seek to only recruit leaders from the NHS. • Listening sessions with the Medical Director and Director of Patient Experience &
Nursing are open to junior doctors and nurses and scheduled at regular intervals. • The CEO also hosts briefing sessions to share information, these sessions
include time for questions and answers. • The Director of Patient Experience & Nursing has an open door policy and is
highly visible in all areas of the Trust receiving staff feedback in a more informal way.
5.3 Listening to Patients • Friends and Family Test rolled out to all services in line with national timescales,
the Trust has good response rates for inpatients and A&E at or above the London and national average.
4
• There are also a number of local surveys in place. There is an established mechanism for reviewing and responding to feedback left on NHS Choices. Patients and the public can also leave feedback via Twitter, whilst the PiP sessions provide an opportunity to receive feedback.
• We have a good relationship with our local Healthwatch and have quarterly scheduled meetings where patient feedback is shared; patient concerns are also shared reactively as they occur.
• Patient stories are now heard at the beginning of each monthly Board Meeting. • A Being Open Policy is in place, and in line with national implementation
timescales a system has been implemented to respond Duty of Candour. • Serious incident procedure includes a requirement to be open with patients,
sharing investigation reports. The CEO or a member of the Executive Board meets with patients/families involved in Serious Incident (SI) investigations (should they wish to take up this opportunity).
• There is a complaints procedure in place that meets the requirements of the Local Authority Social Services and National Health Service Complaints (England) Regulations 2009.
• A procedure in place to ensure that every effort is made to contact complainants to discuss their complaint to ensure that we understand the issues that require investigation and response, and how the complainant would like their complaint handled.
• The CEO or nominated director review and sign off each complaint response. • The complaint investigation report template is structured to encourage
investigating teams to include learning and actions to prevent re-occurrence. • Complaints are screened and may trigger an incident or Serious Incident level
investigation. • We have implemented a number of changes to ensure that patients are
encouraged to raise any worries or concerns and know how they can do this, this includes: o New complaints and PALS posters and leaflets o Posters outside each ward with the name of the sister/charge nurse and
matron and a message to encourage concerns to be raised with these individuals as they arise
o ‘Working Together’ booklet that sets out an escalation procedure for patients to raise any worries or concerns, alongside this matrons now carry mobile phones so that they can be contacted by patients
o Patient bedside boards include a message encouraging concerns to be raised at a local level as they arise
o PALS proactively visiting wards • Complainant satisfaction survey implemented, response rate is low but it provides
a helpful insight to where improvements may be required. • Learning from complaints is included in the quarterly Quality and Safety Report to
the Quality & Risk Committee. • Triangulation from all sources of feedback is undertaken to identify where Trust-
wide improvement initiatives should be focused. • In relation to hearing from people whose voice can sometimes be harder to hear,
we have a dementia carers survey and also visit dementia cafes which provide an opportunity for feedback. Interpreting and translation services are available,
5
and robust safeguarding processes are in place. Representatives from the Trust also attend the local disabled residents association.
Further action: • Consider communication training to enhance communication with patients
especially associated with difficult conversations where concerns are raised about care.
5.4 External Relationships • Healthwatch representatives are currently involved with a number of Trust groups
or workstreams including the Experience and Engagement Group, PLACE, Transforming Inpatient Care.
• The Deputy Director of Nursing & Integrated Governance and other Trust staff have scheduled quarterly meetings Healthwatch.
5.5 Information • Work is currently underway to review the quality and performance report • The Trust quality dashboard has a greater focus on outcomes rather than
processes. • Clinical Quality Strategy in place. • Each division has a divisional dashboard. • The Heatmap – Nursing Dashboard includes a number of measures by ward, the
majority of the indicators are outcome related. The dashboard forms part of the Trust Quality and Safety Report.
• Each ward displays quality information in an area accessible to the public including: Friends and Family Test results, and hospital acquired harms such as pressure ulcers.
• Root Cause Analysis investigations in place for harms such as hospital acquired pressures ulcers of grade 3 or 4 and falls resulting in a fracture or someone who has fallen three or more times.
• The Trust has signed up to the national ‘Sign up to Safety’ campaign, established a steering group to support the development of an implementation plan to reduce patient harm by 50% over three years.
• The Safer Staffing report includes staffing fill rates and temporary staffing levels alongside a range of nurse sensitive outcome indicators. This enables senior nurses and divisional management teams to gain insight into the differences between wards.
• All eligible wards complete the national Safety Thermometer tool and submit information to the national data set.
• The Trust has an information team and a workforce information team. • Electronic information technology to enable staff to spend more time caring for
patients includes PASplus, e-procurement, Epro electronic discharge summaries, and Anglia-Ice.
• Wifi is now available across the Trust. • We have recently introduced the Rate system, initially this is being trialled in
outpatient and care settings capturing FFT data, it is also being trialled by the audit department.
6
Further Action: • Following the evaluation of Rate we will be able to use the system to collect the
monthly safety thermometer information, patient acuity and dependency and ward level assessment associated with nursing key performance indicators.
• Implementation of the Hillingdon Care Record project (Five Year Forward View) will provide electronic access to patient letters, pathology results.
5.6 Fundamental Standards of Care • We have introduced ‘Safe, Comfortable, Informed and Involved’ as a key
message to staff and patients. It provides a helpful foundation to support our standards and also delivers a clear message about the fundamental of care. It is linked to the Trust’s CARES values and brought to life in a number of different ways, including: • As a header on our new bedside patient information boards. • Within the Working Together patient leaflet that sets out what inpatients can
expect and is laid out under the safe, comfortable, informed and involved headings.
• On staff jigsaw posters that graphically illustrate how the standards, procedures, interventions and assessments that have been introduced ‘fit together’ to help us keep patients safe, comfortable informed and involved.
• Our Essential Nursing Standards linked to the Trust CARES values set out explicit standards and expectations for every nurse and care assistant also providing a framework for proactive care (the Trust approach to intentional rounding).
• Proactive care charts have been introduced to provide prompts for what is required when rounding and a method to record care delivery.
• Dementia training is now mandatory and a Dementia Specialist Nurse who provides ward based advice and expertise is now in post.
• The Trust has a Dementia Strategy, implementation of which is overseen by the Dementia Steering Group.
• Core nursing care plans have been implemented; these include dementia, hygiene, hydration and fluid balance, nutrition.
• The care plans show the key interventions that should be implemented for all patients with scope to include individualised actions that are specific for each patient’s unique needs.
• Call bell and Comfort at Night standards have been implemented; these are discussed at the nurse induction.
• Bedside Information Boards are magnetic and include a visual alerts section. Magnets are used, with the patient’s consent to identify any risks or key information that support nurses to deliver fundamental care to patients.
• Unannounced mealtime observation visits are conducted with support from Age UK.
• An audit of fluid charts was undertaken in May 2015. • The name of the key nurse with responsibility for the patients care for each shift
and the lead consultant is included on the bedside information board.
7
• A consent policy is in place but feedback from the national inpatient survey and FFT feedback suggests that opportunity for improvement in the information that patients receive about how they will feel after surgery.
• The Trust has recruited a number of Patient Companion Volunteers and has an ongoing commitment to continue with this.
• Shift handover standard operating procedure includes an element of handover at the bedside to encourage involvement and information sharing with the patient.
• Nurses now record evaluations of care in the medical record alongside doctors and other allied health professionals to facilitate information sharing.
• Full implementation of the National Early Warning System and associated vital signs observations charts.
• Following on from the Cavendish review, the Induction Care Certificate has been successfully piloted within the Trust for both new starters and current healthcare assistants. We are continuing to implement the Induction Care Certificate throughout the Trust. In 2015 there will be a pathway for healthcare assistants who would like to develop themselves within their role.
• A Medications Safety Committee is driving forward security and safety of medicines to reduce potential harm to patients.
• Monthly medicines audit. • Sign up to Safety Campaign includes reducing harm related to medicine errors,
malnutrition, pressure ulcers and falls. Further Action: • Following specific feedback received post the ‘Perfect Week’ initiative, review the
possibility of releasing Trust staff who have expressed an interest in volunteering to support patients at mealtimes.
• Using the Rate electronic system reintroduce a schedule of regular assessments of fundamental care by ward.
• The Trust does not have a specialist nurse dedicated to continence, we will review the relevant expertise of our current specialist nurses such as Tissue Viability Nurse and Urology Specialist Nurse and identify potential interventions that could improve care.
5.7 Cleanliness The Board approved a Cleaning Strategy in February 2015. The strategy sets out a professional and effective approach for the Trust to deliver a safe and clean environment for everyone using its healthcare facilities that meets the requirements and guidance set out in the National Specifications for Cleanliness in the NHS 2007. The strategy: • Provides clarity on cleaning roles and responsibilities across the Trust. • Sets out clear governance and reporting arrangements on cleaning standards
against the targets agreed by the Board. • Sets out the need to ensure cleaning services are sufficiently resourced to meet
the requirements of the NSC and achieve a clean and safe environment. • Details the processes for monitoring performance.
8
6. Recommendations This overview demonstrates that the Trust has made significant progress in responding to the Francis recommendations. A plan setting out the agreed actions will be developed and monitored through the Quality and Risk Committee.
9
Meeting of the Board of Directors – public session Wednesday 27th May 2015
Agenda item 12 National Survey of Adult Inpatients 2014 Reason for item: The purpose of this report is to update the Board on the results from the 2014 survey of adult inpatients. Summary: The results of the survey are based on responses from 312 patients who completed the survey, giving a response rate of 38%. The average response rate of all Trusts was 47%. This is a lower Trust response rate in comparison to the 2013 survey (42%). There are two out of ten sections where the Trust appears in the worst performing Trust category; the Trust was in the ‘about the same’ category in all ten sections in last year’s survey. The Trust has been rated as worse than most other Trusts in six questions; this is an increase in comparison to two questions in the 2013 survey. An analysis of comments has been provided this year which highlights some key areas for focus. Areas for improvement during 2015/16 will be aligned with the Quality Report priorities and Transformation Programmes where robust governance arrangements are already in place to monitor progress and outcomes. Any specific initiatives outside of these will be discussed at the Experience and Engagement Group. Board Action required: The Board is asked to: 1. To discuss and comment on the update. 2. Agree or recommend any further actions.
Report from: Bev Hall, Deputy Director of Nursing and Patient Experience Report sponsor: Theresa Murphy, Director of Nursing and Patient Experience Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience and the
quality of care we provide. Previous consideration at Board or Committees: none. Equality and diversity considerations: There is no positive or negative impact from this report. Financial implications: None.
1
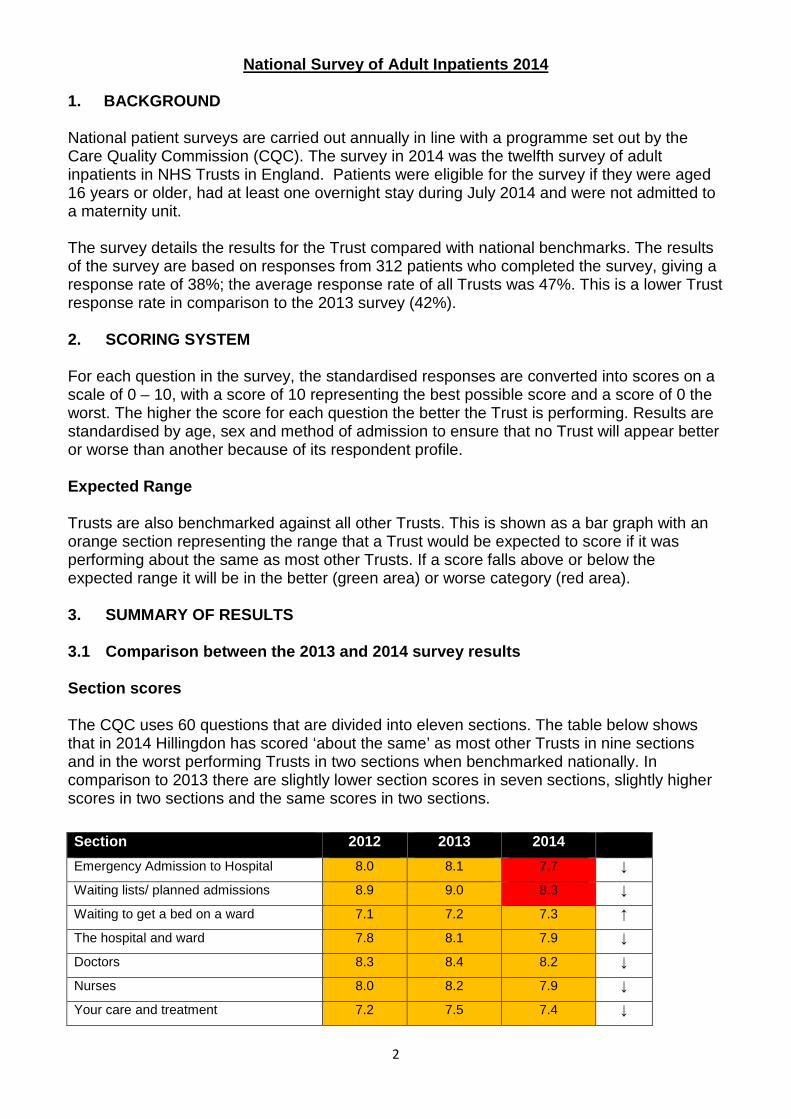
National Survey of Adult Inpatients 2014
1. BACKGROUND National patient surveys are carried out annually in line with a programme set out by the Care Quality Commission (CQC). The survey in 2014 was the twelfth survey of adult inpatients in NHS Trusts in England. Patients were eligible for the survey if they were aged 16 years or older, had at least one overnight stay during July 2014 and were not admitted to a maternity unit. The survey details the results for the Trust compared with national benchmarks. The results of the survey are based on responses from 312 patients who completed the survey, giving a response rate of 38%; the average response rate of all Trusts was 47%. This is a lower Trust response rate in comparison to the 2013 survey (42%). 2. SCORING SYSTEM For each question in the survey, the standardised responses are converted into scores on a scale of 0 – 10, with a score of 10 representing the best possible score and a score of 0 the worst. The higher the score for each question the better the Trust is performing. Results are standardised by age, sex and method of admission to ensure that no Trust will appear better or worse than another because of its respondent profile. Expected Range Trusts are also benchmarked against all other Trusts. This is shown as a bar graph with an orange section representing the range that a Trust would be expected to score if it was performing about the same as most other Trusts. If a score falls above or below the expected range it will be in the better (green area) or worse category (red area). 3. SUMMARY OF RESULTS
3.1 Comparison between the 2013 and 2014 survey results Section scores The CQC uses 60 questions that are divided into eleven sections. The table below shows that in 2014 Hillingdon has scored ‘about the same’ as most other Trusts in nine sections and in the worst performing Trusts in two sections when benchmarked nationally. In comparison to 2013 there are slightly lower section scores in seven sections, slightly higher scores in two sections and the same scores in two sections.
Section 2012 2013 2014 Emergency Admission to Hospital 8.0 8.1 7.7 ↓
Waiting lists/ planned admissions 8.9 9.0 8.3 ↓
Waiting to get a bed on a ward 7.1 7.2 7.3 ↑
The hospital and ward 7.8 8.1 7.9 ↓
Doctors 8.3 8.4 8.2 ↓
Nurses 8.0 8.2 7.9 ↓
Your care and treatment 7.2 7.5 7.4 ↓
2
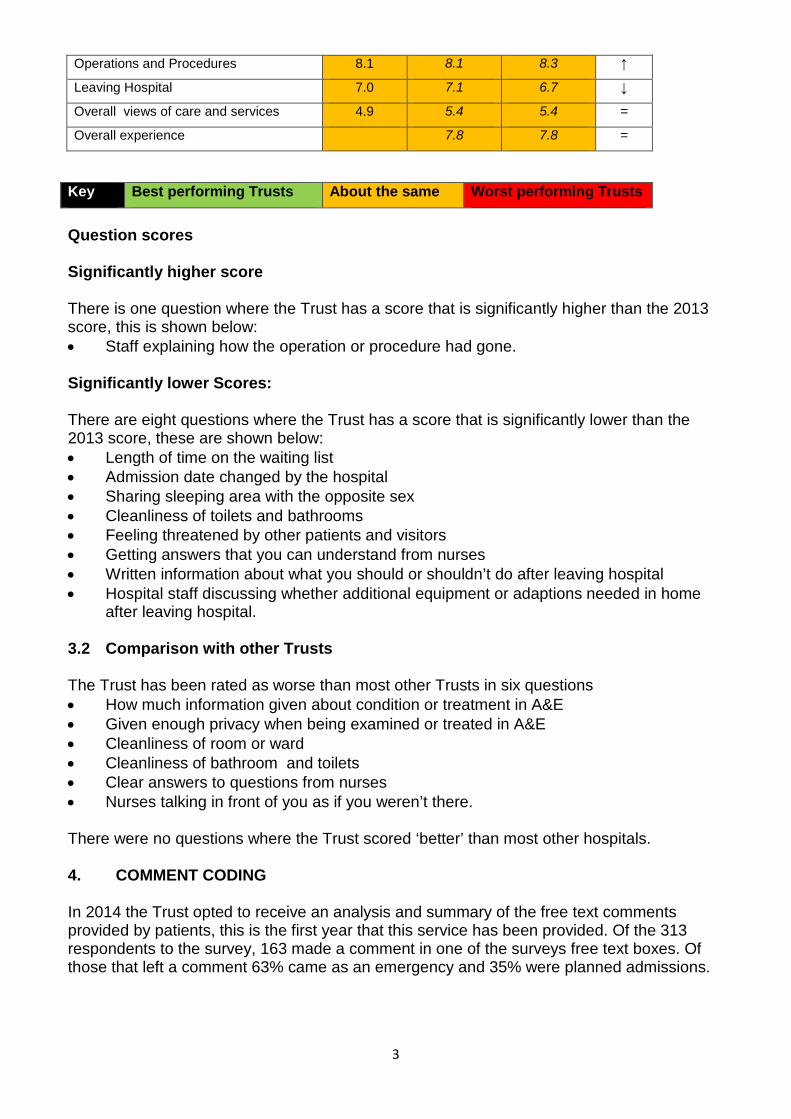
Operations and Procedures 8.1 8.1 8.3 ↑
Leaving Hospital 7.0 7.1 6.7 ↓
Overall views of care and services 4.9 5.4 5.4 =
Overall experience 7.8 7.8 =
Question scores Significantly higher score There is one question where the Trust has a score that is significantly higher than the 2013 score, this is shown below: • Staff explaining how the operation or procedure had gone.
Significantly lower Scores: There are eight questions where the Trust has a score that is significantly lower than the 2013 score, these are shown below: • Length of time on the waiting list • Admission date changed by the hospital • Sharing sleeping area with the opposite sex • Cleanliness of toilets and bathrooms • Feeling threatened by other patients and visitors • Getting answers that you can understand from nurses • Written information about what you should or shouldn’t do after leaving hospital • Hospital staff discussing whether additional equipment or adaptions needed in home
after leaving hospital. 3.2 Comparison with other Trusts The Trust has been rated as worse than most other Trusts in six questions • How much information given about condition or treatment in A&E • Given enough privacy when being examined or treated in A&E • Cleanliness of room or ward • Cleanliness of bathroom and toilets • Clear answers to questions from nurses • Nurses talking in front of you as if you weren’t there. There were no questions where the Trust scored ‘better’ than most other hospitals. 4. COMMENT CODING In 2014 the Trust opted to receive an analysis and summary of the free text comments provided by patients, this is the first year that this service has been provided. Of the 313 respondents to the survey, 163 made a comment in one of the surveys free text boxes. Of those that left a comment 63% came as an emergency and 35% were planned admissions.
Key Best performing Trusts About the same Worst performing Trusts
3
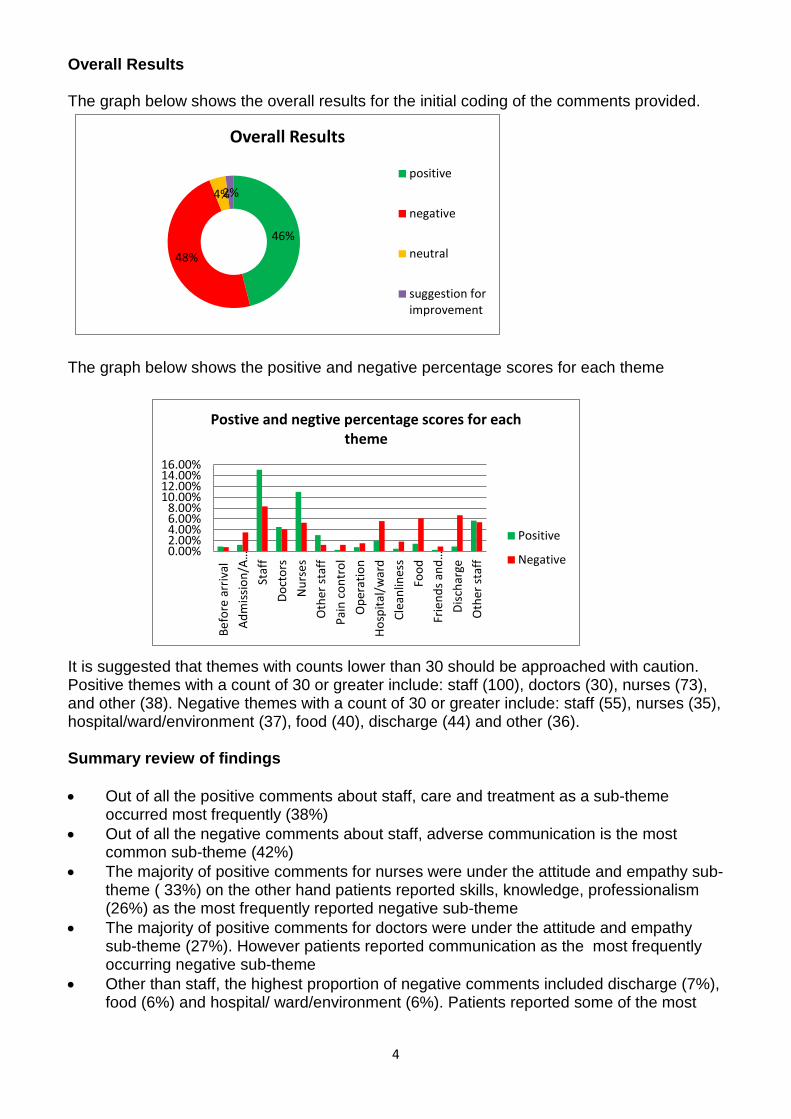
Overall Results The graph below shows the overall results for the initial coding of the comments provided.
The graph below shows the positive and negative percentage scores for each theme
It is suggested that themes with counts lower than 30 should be approached with caution. Positive themes with a count of 30 or greater include: staff (100), doctors (30), nurses (73), and other (38). Negative themes with a count of 30 or greater include: staff (55), nurses (35), hospital/ward/environment (37), food (40), discharge (44) and other (36). Summary review of findings • Out of all the positive comments about staff, care and treatment as a sub-theme
occurred most frequently (38%) • Out of all the negative comments about staff, adverse communication is the most
common sub-theme (42%) • The majority of positive comments for nurses were under the attitude and empathy sub-
theme ( 33%) on the other hand patients reported skills, knowledge, professionalism (26%) as the most frequently reported negative sub-theme
• The majority of positive comments for doctors were under the attitude and empathy sub-theme (27%). However patients reported communication as the most frequently occurring negative sub-theme
• Other than staff, the highest proportion of negative comments included discharge (7%), food (6%) and hospital/ ward/environment (6%). Patients reported some of the most
4
46%
48%
4% 2%
Overall Results
positive
negative
neutral
suggestion forimprovement
0.00%2.00%4.00%6.00%8.00%
10.00%12.00%14.00%16.00%
Befo
re a
rriv
alAd
miss
ion/
A…St
aff
Doct
ors
Nur
ses
Oth
er st
aff
Pain
con
trol
Ope
ratio
nHo
spita
l/war
dCl
eanl
ines
sFo
odFr
iend
s and
…Di
scha
rge
Oth
er st
aff
Postive and negtive percentage scores for each theme
Positive
Negative
negative experiences with information and involvement and after care following discharge (each 27%) quality of food (58%) and comfort in the ward (32%)
• Over a quarter of all positive comments under the other non-medical staff theme were about attitude and empathy.
• The majority of positive comments under the other theme included a favourable overall outcome (40%) and thanks to staff (47%).
5. DISCUSSION There are a number of factors that may have had an impact on the results for 2014, these include: • Additional bed capacity opened without substantive staffing in place • Medical staff managing care across an increased spread of wards • Nursing vacancies • Proportion of temporary nursing staff. The analysis of the free text comments left by patients provides further insight and helps to identify where the Trust is performing well and where improvement is required. Although the many comments received through the Friends and Family Test are not coded formally, they are all screened every month by the Deputy Director of Nursing. It would be fair to say that there are many similarities between the positive and negative themes emerging from these comments and those from the 2014 survey of adult inpatients. It is pleasing to see that the majority of positive comments across doctors, nurses and other non-medical staff groups relate to attitude and empathy; key elements of compassion. This finding appears to be aligned with the recent CQC inspection, where ‘caring’ was rated as good. In a report about enabling compassionate care in hospitalsi it is suggested that the attention that senior managers and the Board give to meeting financial targets and achieving national targets deeply affects the behaviour and priorities of staff. In a difficult financial climate and the need for NHS organisations to be as cost efficient as they can be, this needs be balanced with a continued focus on creating the right conditions to enable our staff to deliver it. In relation to the cleanliness results some of this resonates with the CQC assessment covering the cleaning responsibilities undertaken by domestics, nurses and estates staff. Work has already been undertaken to review the resources that we have for cleaning and since February 2015 the Trust has been working to the National Specifications for Cleanliness in the NHS (NSC) which sets out quality standards to be achieved and audit processes. The Trust's regular technical audits of cleanliness undertaken in each patient area on a weekly and monthly basis, since adopting the NSC, show that the Trust is meeting the required standards. Feedback from our Friends and Family Test show that there is good satisfaction with cleanliness. The Facilities team also directly survey 5,400 in-patients on average each year across both hospital sites to assess patient satisfaction with cleaning and this also consistently shows good satisfaction and highlights any areas where improvements are needed and action can be taken. When the comments and the sections/questions where the Trust has lower results are reviewed alongside the top ten subject codes from complaints it is apparent that there are clear links. The graphic below outlines the subject areas that appear frequently across a
5
number of sources of feedback suggesting that these themes should be our focus for improvement during 2015/16. There are a number of transformational programmes underway that have links to some of the themes set out above including Transforming Inpatient Care and Workforce transformation. Improving patient experience is identified as a positive outcome from these programmes. Survey results will be shared with the Programme Leads to ensure that the interventions and planned actions included in the programme take account of what patients have reported. This will enable specific patient experience outcome measures linked to the national patient survey to be set to monitor improvements. Improving communication and involvement with patients is embedded in priority four of the 2015/16 Quality Report, with a focus on improving in some fundamental elements; for example: Always: • Taking time to explain what is happening and what is planned • Checking the patient/families understanding of information given • Keeping patients informed if there are delays • Involving patients in decisions about care and treatment and offering choice • Providing more information about what to expect following surgery. Going forward, we will scope out specific initiatives and actions that will make a difference to these areas and ensure that other programmes of work as outlined above integrate these simple ‘habits’. The local survey programme will enable the Trust to monitor improvements in these elements. 6. CONCLUSION
The CQC adult inpatient survey provides a helpful annual check of our inpatients’ experience and enables the Trust to compare our performance with that of other Trusts. Overall the 2014 survey results appear to show that there are a number of areas where patients have reported a worse experience compared to the previous year. There are two sections where the Trust appears in the worst performing Trust category, the Trust was in the about the
6
Complaints, 2014 survey of
adult inpatients, Friends and Family Test
Communication, involvement and
information
Waiting lists and planned admissions
( complaints and 2014 survey only)
Leaving Hospital
Comfort & responding to need
same category in all sections the previous year. There has also been an increase to six in the number of questions where the Trust has been rated as worse than most other Trusts, compared to two in 2013. Areas for improvement during 2015/16 will be aligned with the Quality Report priorities and Transformation Programmes where robust governance arrangements are already in place to monitor progress and outcomes. Any specific initiatives outside of these will be discussed and monitored through the Experience and Engagement Group.
i Point of Care , Enabling Compassionate Care in Hospital ( Kings Fund 2009) http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/poc-enabling-compassionate-care-hospital-settings-apr09.pdf
7
Meeting of the Board of Directors – public session Wednesday 27th May 2015
Agenda item 13 Safer Staffing – Planned and actual staffing levels Reason for item: This is a standard monthly report on the planned and actual nursing staffing levels. It includes the data that is submitted nationally to NHS England. Summary: The report presents the planned and actual staffing levels for April on all inpatient wards. The average fill rate for each ward together with Nurse Sensitive Outcome Indicators is provided in Appendix 1. This enables the Board to triangulate staffing levels with quality indicators. The Board should note that: • Achieving high fill rates for night shifts continues to be prioritised. • Vacancy levels and the additional beds opened in 2014/15 continue to be the biggest
challenge. • Divisional Senior Nurses review staffing levels on each shift and take action to ensure
that patient care remains safe and effective. Board Action required: The Board is asked to: 1. Review the information provided and the actions in place to achieve and maintain
staffing levels that will enable safe and compassionate care to be delivered to our patients.
2. Agree any further actions that are required. Report from: Vanessa Saunders, Assistant Director of Nursing Report sponsor: Theresa Murphy, Director of the Patient Experience & Nursing Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience
and the quality of care we provide. Previous consideration at Board or Committees: n/a. Equality and diversity considerations: none. Financial implications: There are no direct financial implications arising from this monitoring report; however the ongoing drive to recruit substantive staff outlined in the report will have a positive financial impact by reducing reliance on agency staff.
1
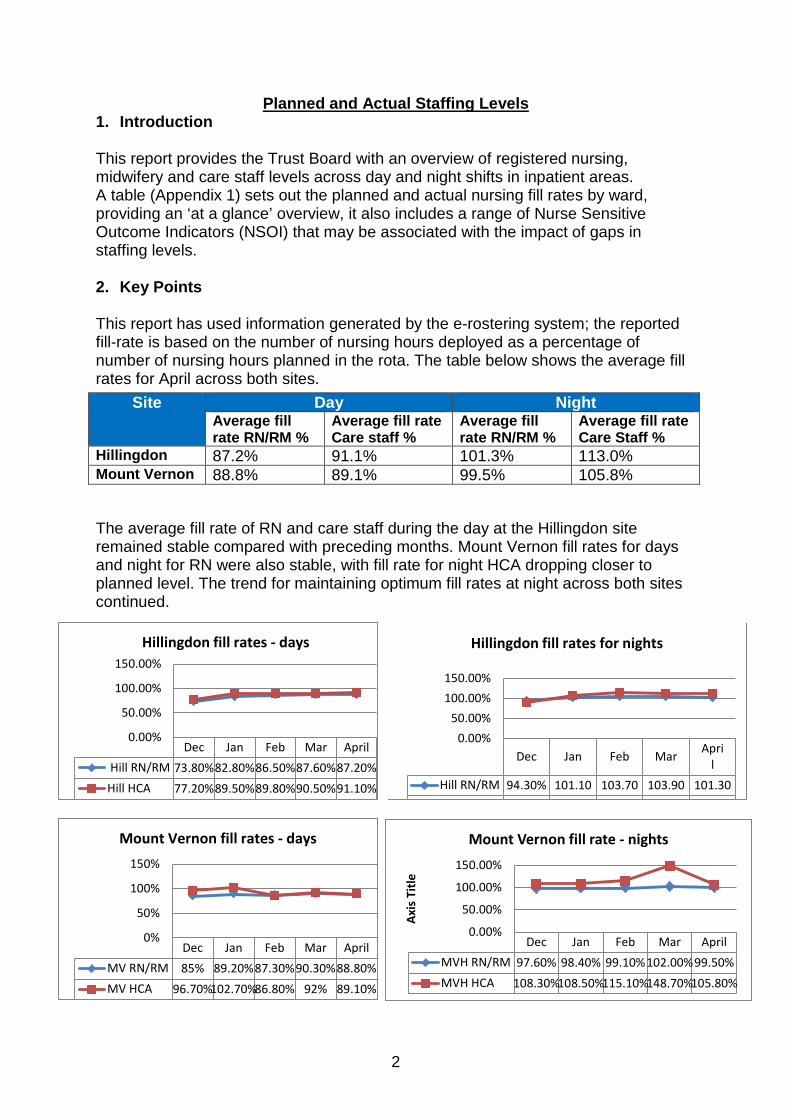
Planned and Actual Staffing Levels 1. Introduction This report provides the Trust Board with an overview of registered nursing, midwifery and care staff levels across day and night shifts in inpatient areas. A table (Appendix 1) sets out the planned and actual nursing fill rates by ward, providing an ‘at a glance’ overview, it also includes a range of Nurse Sensitive Outcome Indicators (NSOI) that may be associated with the impact of gaps in staffing levels. 2. Key Points
This report has used information generated by the e-rostering system; the reported fill-rate is based on the number of nursing hours deployed as a percentage of number of nursing hours planned in the rota. The table below shows the average fill rates for April across both sites.
The average fill rate of RN and care staff during the day at the Hillingdon site remained stable compared with preceding months. Mount Vernon fill rates for days and night for RN were also stable, with fill rate for night HCA dropping closer to planned level. The trend for maintaining optimum fill rates at night across both sites continued.
Dec Jan Feb Mar April
Hill RN/RM 94.30% 101.10 103.70 103.90 101.30
0.00%50.00%
100.00%150.00%
Hillingdon fill rates for nights
Site Day Night Average fill rate RN/RM %
Average fill rate Care staff %
Average fill rate RN/RM %
Average fill rate Care Staff %
Hillingdon 87.2% 91.1% 101.3% 113.0% Mount Vernon 88.8% 89.1% 99.5% 105.8%
2
Dec Jan Feb Mar AprilMV RN/RM 85% 89.20%87.30%90.30%88.80%MV HCA 96.70%102.70%86.80% 92% 89.10%
0%
50%
100%
150%
Mount Vernon fill rates - days
Dec Jan Feb Mar April Hill RN/RM 73.80%82.80%86.50%87.60%87.20%Hill HCA 77.20%89.50%89.80%90.50%91.10%
0.00%
50.00%
100.00%
150.00%Hillingdon fill rates - days
Dec Jan Feb Mar AprilMVH RN/RM 97.60% 98.40% 99.10%102.00%99.50%MVH HCA 108.30%108.50%115.10%148.70%105.80%
0.00%
50.00%
100.00%
150.00%
Axis
Titl
e
Mount Vernon fill rate - nights

Achieving planned staffing levels and skill mix during April remained challenging, contributory factors remain unchanged and include:
• The impact of AMU opening in place of EAU, with an additional 16 beds • The impact of Marina moving to Fleming, with a net gain of 15 beds • The continuing volume of three extra capacity wards open • Vacancy levels above planned • Acuity and Dependency of patients, resulting in the need to increase staff
above the planned levels on some shifts to provide the care or additional supervision required.
3. Actions to address gaps Planned and actual staffing levels are reviewed on a shift by shift basis by the ward sister and matron and discussed at the daily capacity meetings. Plans to ensure safe staffing are formulated and agreed at the daily capacity meetings in conjunction with the Director of Patient Experience & Nursing. Where a shift is running below the planned level of staffing other elements will be reviewed, such as the activity on the ward, the acuity and dependency of the patients and the experience and skills of the actual staff on duty. In some circumstances it may be safe and appropriate to provide care with the actual staff on duty. In this situation staff will be especially vigilant to any aspects of care that is at risk of being missed and escalate their concerns to Senior Nurses for further action. If the actual level or experience and skills of staff is assessed as insufficient for the needs of the patients further action will be taken with the aim of maintaining safe and effective nursing care for our patients. Examples of actions taken to address any gaps in planned staffing levels include:
• Reallocation of staff from within the division or other divisions in the Trust • Support from non-ward based nursing/midwifery or care staff • Matron working clinically providing ‘hands on care ’ • Requests for bank or agency staff.
3.1 Recruitment Update – Paul Corn ford, Interim Head of Employee Services The table below shows the current Registered Nurse vacancy position. Percentage Nurses (Patient facing areas) 15.49%
Nurses (Trust wide) 8.12%
Nursing Labour Turnover (year to date):
All nursing 12.59%
3
Recruitment of UK based nurses continues to be a challenge and will remain so for the immediate future. In this respect the Trust is continuing with monthly weekend recruitment days for nurses and HCAs which prove a positive source of recruitment. HCA recruitment has proved especially effective and vacancies for this staff group remain within an acceptable level of turnover. Specific areas are targeted for standalone campaigns where recruitment is proving especially difficult, such as AMU. The Trust has commenced recruiting nurses from the EU and overseas, and 11 nurses from Italy arrived to start work with the Trust in May. They will undergo an in-depth induction before taking up their posts. Other nurses have been recruited from Spain, start date to be confirmed, and additional trips to Europe and the Philippines are planned. Sohan Bissoonauth, previously from ITU, has taken up the post of Lead Nurse for Overseas Recruitment to co-ordinate and take forward this strand of work across the Trust. 4. Divisional Overview and Assurance 4.1 Medical Division – Russell Wernham, Assistant Director of Nursing Alderbourne Whilst the ward is not an acute area, some rehabilitating acute patients are admitted requiring ‘specials’. This is especially reflected in the night fill rates for HCAs. The ward currently has a band 6 vacancy. The ward is currently scoring 86% of patients being extremely likely or likely to recommend the ward in the Friends and Family test. Beaconsfield East (B’East) Beaconsfield East staffing has remained consistent to previous months. Three pressure ulcers were reported in the month and there were five falls in the month, none with harm. The senior team are reviewing these and will implement measures to reduce occurrence. The Friends and Family test score shows 91% of Friends and Family would be extremely likely or likely to recommend the ward. Bevan We have had two sub-optimal staffing datix reports completed to show the areas of shortfall, however these reports were acted on and staffing was increased to support the ward. The number of falls on Bevan has been recorded as six, although none of which was with harm. The ward is currently scoring 100% of patients being extremely likely or likely to recommend the ward.
4
CCU We have had one staffing datix report for sub optimal levels in April. This was addressed and support given by the matron. The unit has a band 6 vacancy and two band 5 vacancies. All vacancies have been advertised. One fall and one pressure ulcer were reported. The Unit has a score of 100% for friends and family extremely likely or likely to recommend rating which demonstrates the hard work and focus of the team, with some very complex patients. Daniels There have been five falls in April, none with harm. The ward is now open to 16 beds. The relatives and friends of patients on Daniels give a 100% return on being extremely likely or likely to recommend to others. Drayton The staffing on the ward remains challenged with high maternity leave numbers. There is one band 6 vacancy which has been advertised. There has been a fall with harm; a Root Cause Analysis has been commenced. The ward has seen an extremely likely or likely return of 86% in April for the Friends and Family test. The ward team are working to improve on this for May. AMU Staffing on AMU remains challenged and we have been recruiting to the vacancies on the Unit. The division continues to work with People and Development on targeted recruitment for these posts. We are still witnessing high agency use with 45% use in April. There have been seven falls. The medication errors have been addressed and we are working to retrain the staff involved in safe administration of medication. There were 81% of friends and family who were extremely likely or likely to recommend the Unit to others in April. This has been noted and the new matron is working to improve this rate in May. The high number of agency staff also accounts for some of the reduction in recommendation. Grange Staffing within the RN group has improved with more recruitment ongoing as we are still experiencing multiple vacancies. The band 7 has been actively recruiting to band 5 positions. The Division has plans in place to limit the number of high acuity patients needing NIV being placed on that ward. There have also been issues with sickness which are being addressed. The falls on the ward have increased and it should be noted that the ward still has had multiple acutely confused patients. These patients are being provided with ‘specials’ where assessment indicates these are required to improve safety. There has been one fall with harm in April. Medication errors have been reviewed and staff involved have been retrained in medication safety. Friends and Family test returns indicate that 88% of friends and family would recommend the ward to others.
5
Hayes There remains a high incidence of confused patients on the ward; ‘specials’ are being provided on top of the extra staffing to support these patients. There has been a decrease in falls on the ward with four in April; one fall resulted in harm and a Root Cause Analysis (RCA) has been commenced. There has also been a pressure ulcer recorded. The ward manager and matron are working to maintain standards and support patient care. The current percentage of friends and family extremely likely or likely to recommend Hayes ward stands at 100%. Stroke The Stroke Unit is outstanding a band 6 which has been advertised with support from a recruitment agency. At this time unfortunately no suitable applicants have applied. The ward bed capacity continues to fluctuate between 20 – 26 beds with additional bank/agency being used as necessary. However the falls on the ward have decreased despite an increase in confused patients. The current percentage of friends and family extremely likely or likely to recommend the Stroke Unit stands at 100%. Edmunds Staffing on Edmunds remains constant with long lines of agency still working on the ward. There were five falls on the ward and while this is reflective of the patient group the matron and senior sister are reviewing preventative measures in place. The current percentage of friends and family extremely likely or likely to recommend Edmunds ward stands at 86% and the matron is working with the ward manager to ensure appropriate action is taken to address this. Pinewood The ward leadership team is now fully established. We are now continuing to build the junior team and moving from bank to substantive on junior lines. We have a high care staff fill-rate overnight due to the need for ‘specials’ to prevent patient falls. The current percentage of friends and family extremely likely or likely to recommend Pinewood ward stands at 100%. Churchill Churchill staffing is being addressed by the band 7, the two band 6 posts are now filled. The ward manager is ensuring staff get a timely local induction and assessment of competencies. Medication errors have decreased. There have been three falls, one with harm and an RCA has been commenced. The current percentage of friends and family extremely likely or likely to recommend Churchill ward stands at 88%. The ward manager is working to address this in May. Lister The band 7 ward manager started at the beginning of March and two band 6 sisters have now been appointed. The high staff fill rate is needed to compensate for the
6
lack of continuity due to vacancy rate and also the need for ‘specials’ to provide enhanced care for confused patients. We are still seeing some sub optimal staffing datix reports mainly based on staff being relocated to ensure safety at night. There have been three patient falls, one with harm. Medication errors have been reviewed and staff involved have reflected on the errors and actions and learning agreed. The current percentage of friends and family extremely likely or likely to recommend Lister ward stands at 100%. General Overview There has been increased scrutiny on datix responses in terms of staffing and a focus on ensuring root cause analyses are undertaken for falls and pressure ulcers. The Division is now re-focusing on the friends and family test, with the aim to see the Division increase its responses in both inpatient and emergency medicine with positive results. 4.2 Surgical Division – Sinead Fagan, Assistant Director of Nursing Jersey Staffing fill rates on the ward continue to increase month on month it is now currently at 83% for April (due to vacant posts) and 110 % at night. Recruitment of a Band 6 nurse has taken place to ensure safer staffing and leadership within the ward. Recruitment has been ongoing on a monthly basis, however temporary staffing solutions are still required to cover vacant shifts.
• 1.7 staff nurse vacancies - Band 5. • 3 HCA vacancies (actively been recruited into)
88% of responses from Friends and Family test stated they would be likely or extremely likely to recommend the ward. 2% responded with an extremely unlikely comment. This was due to staff attitude with the staff members named. The ward manager and matron are addressing this directly with the staff concerned. We have seen an improvement this month in our nurse sensitive indicators within the ward. Kennedy Staffing fill rates are 89%. This is a significant improvement on the last couple of months with recruitment that has taken place and the new staff in position. The opening of Fleming ward has also had an impact on the safe staffing of Kennedy ward due to the ward sister temporarily redeployed to work as matron and take on this role. Positions have been filled by bank and agency members of staff where possible. The clinical need of the patients and staffing levels are continually being reviewed by the sister and matron with provisions made to cover where possible by reallocating staff from other surgical areas or matron assisting in clinical practice. We had one datix incident stating that the ward was understaffed. Substantive registered Nurse fill rates at night were prioritised to ensure safe care, with additional one to one specials in place when required for specific patient conditions. The fill rate for March
7
on Kennedy Ward was 108% at night shift due to a requirement for 1:1 nurse to patient ratio for some patients for some nights. Substantive nursing positions continue to be recruited to and sickness management has been undertaken for those staff requiring it.
• 1.78 staff nurse vacancies. • 1 HCA vacancies (2 of these staff were new members starting in May)
94% of received FFT responses stated they would likely or extremely likely recommend the area. Most of the commentary was very positive with compliments for the nursing staff and care delivery. We continue to strive in getting more feedback from the Friends & Family Test. There was one fall with no harm recorded and two hospital acquired pressure ulcers. We now have an agreement to keep three pressure relieving mattresses on the ward for all patients requiring one on admission. The dependency on the ward has been extremely high over the last two months. We have many patients who are bed bound and require one to one nursing care both at night and day time. This has been provided where possible by increasing the nursing establishment during the day and night time. Trinity Ward Trinity has a fill rate of 79%; this is an increase from last month. All night shifts were covered appropriately; there was also an increase in bank & agency. This is due to the introduction of weekend lists in the centre. The vacancy rate on Trinity has been reduced after successful recruitment to meet the funded establishment. The ward has one RN currently on long term sickness. Temporary staffing has been used for backfill. Trinity Ward staffing fill rate reflects the activity associated with the ward. Staffing levels were increased in line with the number of patients on the ward as activity fluctuates but the planned numbers are based on an assumption of full occupancy. Saturday and Sunday operating lists have been the norm for the last few months due to the transition of activity to Mount Vernon whilst the Hillingdon theatre project has got under way. This shall be the case until at least September. There were two falls, and one medication error. These incidents have been investigated by the ward sister and matron. ITU Staffing in ITU fluctuates depending on the patient acuity. ITU patients require a ratio of 1:1 (RN:Patient) where as some HDU patients can be nursed on a ratio of 1:2 (RN:Patients). This is monitored on a daily basis by the ITU senior nurse manager, with staffing levels adjusted accordingly in line with acuity and actual patient present on the unit during the month. For April 75.5% of shifts were filled in line with patient activity. Bank and agency staff were utilised as required, however the unit was able to redeploy their staff elsewhere in the Trust when the unit had fewer or lower acuity
8
patients. There were no required shifts that were unfilled meaning the staffing hours met the needs of the patients on ITU/HDU during April. ITU has had one medication incident reported. The unit also reported zero hospital acquired pressure ulcers. One fall was reported also during safety thermometer check. ITU has now a Band 7 position recruited into. Fleming Ward Fleming Ward opened as a ward in the surgical directorate in January 2015. The ward has 15 beds that are utilised for gynaecological inpatients and there are 14 beds on the surgical assessment unit. 87% of day shifts were filled throughout the month and nearly all night shifts. There is a substantive and experienced band 7 senior sister and there will be a band six junior sister vacant post from May due to promotion. The ward shall have strong presence of matron on the ward during this time. There is an active recruitment for the ward but in the interim suitable bank and agency staff are being given permanent lines of off duty to maintain greater continuity for the patients and the substantive ward team. Recruitment to Fleming Ward has been a priority for the division. This month we have seen our nurses from Italy start. Three of these nurses have joined the team this month. Fleming Ward scored 88% in FFT in April, with 2% of patients stating that they are extremely unlikely or unlikely to recommend the ward. Over the next few months close scrutiny shall be on Fleming regarding patient experience as we shall be carrying out some essential work to upgrade rooms to accommodate EPAU from Marina ward. No harms have been reported through the Safety Thermometer. Greater vigilance and scrutiny will support the team through the transition and implementation of new pathways and team working. 4.3 Women and Children’s Division - Anita Hutchins, Head of Midwifery Labour Ward Six midwives are absent through long term sickness, maternity leave and non-clinical duties. Short term sickness was high for all levels of staff. All sickness absence is proactively managed. Shift activity/acuity was assessed throughout the day, bank and agency was requested. However staffing numbers were 'flexed down' where it was deemed safe i.e. activity was low. Staff who were working non-clinical shifts were pulled to cover the shifts when necessary and staff were reassigned from other wards depending on the acuity. Night shifts were covered with bank and agency as required. Alexandra Ward There was one vacancy and midway through the month, two further midwives were rotated off the ward. This is due to the Unit monthly preceptor rotation and six monthly general rotation. There were six shifts of short term sickness and one full-time midwife on long term sickness who has now returned to work. These shifts were put out to bank and most were filled. The night and weekend shifts were filled as a priority over the day shifts as managers are available if the activity demands midwifery support.
9
This is also compounded with the majority of shifts being filled with staff members working Long Days when an Early and Late shift was on the roster. Katherine Ward Although the ward was over staffed by 0.8 WTE the staff were allocated to other areas to support their shortfalls - Community midwives and Labour Ward. During April there was 97 hours of sickness from the midwifery roster and one long term sickness HCA who is going through a redeployment process and another HCA on maternity leave. These shifts were put out to bank but not all were filled. The night and weekend shifts were filled as a priority over the day shifts as managers are available if the activity demands midwifery support. There is one midwife on a career break who will return in November. This is also compounded with the majority of shifts being filled with staff members working Long Days when an Early and Late shift was on the roster. Peter Pan – Chris Mann, Nursing Services Manager, Paediatric Unit The figures for paediatrics reflect a change from our winter numbers to our summer staffing, it identifies where vacancies have not been covered when the ward had less high acuity. There is some skewing though as two staff who were awaiting their PIN numbers were working as HCAs which led to HCA numbers being higher than expected and RN numbers lower. This is compounded by one RN being on long term sick leave. The higher numbers of RNs at night can generally be attributed to RMN specials, with children being discharged the following day. The HCA on nights reflects the staff working as HCAs whilst awaiting PIN at night this would have been supported by additional RNs as less cover around also accounting for higher numbers.
10
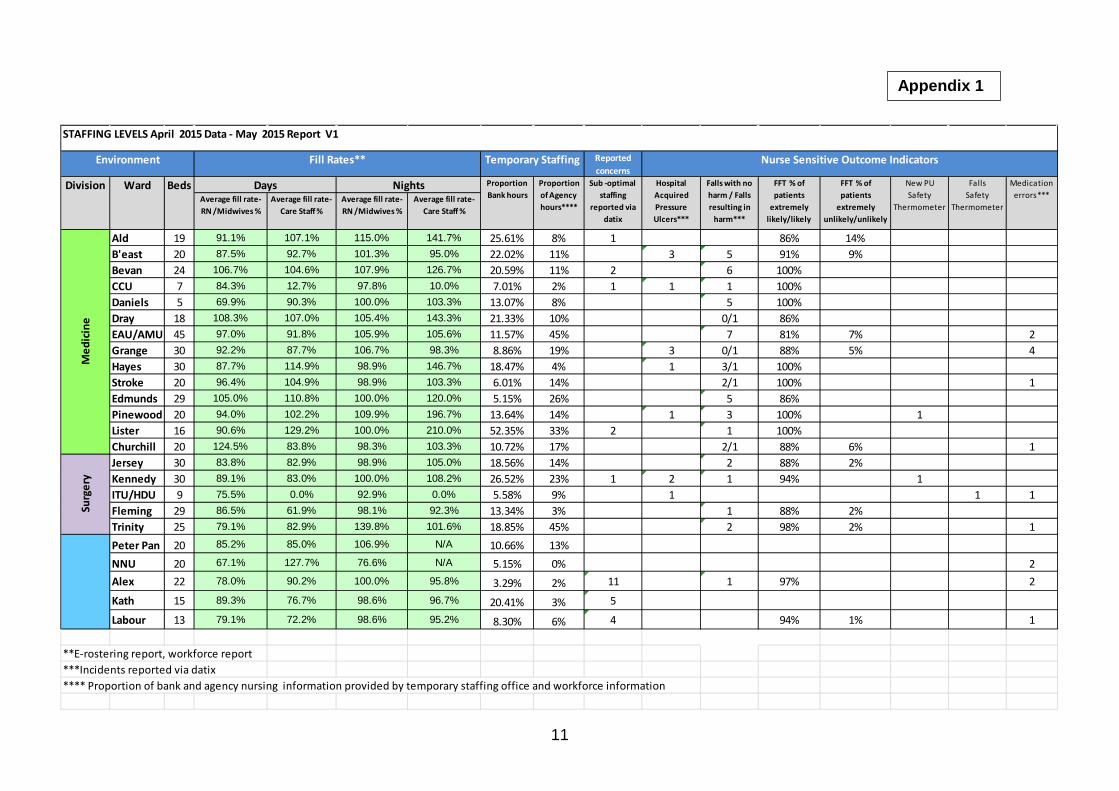
Appendix 1
11
Reported concerns
Average fill rate- RN /Midwives %
Average fill rate- Care Staff %
Average fill rate- RN /Midwives %
Average fill rate- Care Staff %
Ald 19 91.1% 107.1% 115.0% 141.7% 25.61% 8% 1 86% 14%B'east 20 87.5% 92.7% 101.3% 95.0% 22.02% 11% 3 5 91% 9%Bevan 24 106.7% 104.6% 107.9% 126.7% 20.59% 11% 2 6 100%CCU 7 84.3% 12.7% 97.8% 10.0% 7.01% 2% 1 1 1 100%Daniels 5 69.9% 90.3% 100.0% 103.3% 13.07% 8% 5 100%Dray 18 108.3% 107.0% 105.4% 143.3% 21.33% 10% 0/1 86%EAU/AMU 45 97.0% 91.8% 105.9% 105.6% 11.57% 45% 7 81% 7% 2Grange 30 92.2% 87.7% 106.7% 98.3% 8.86% 19% 3 0/1 88% 5% 4Hayes 30 87.7% 114.9% 98.9% 146.7% 18.47% 4% 1 3/1 100%Stroke 20 96.4% 104.9% 98.9% 103.3% 6.01% 14% 2/1 100% 1Edmunds 29 105.0% 110.8% 100.0% 120.0% 5.15% 26% 5 86%Pinewood 20 94.0% 102.2% 109.9% 196.7% 13.64% 14% 1 3 100% 1Lister 16 90.6% 129.2% 100.0% 210.0% 52.35% 33% 2 1 100%Churchill 20 124.5% 83.8% 98.3% 103.3% 10.72% 17% 2/1 88% 6% 1Jersey 30 83.8% 82.9% 98.9% 105.0% 18.56% 14% 2 88% 2%Kennedy 30 89.1% 83.0% 100.0% 108.2% 26.52% 23% 1 2 1 94% 1ITU/HDU 9 75.5% 0.0% 92.9% 0.0% 5.58% 9% 1 1 1Fleming 29 86.5% 61.9% 98.1% 92.3% 13.34% 3% 1 88% 2%Trinity 25 79.1% 82.9% 139.8% 101.6% 18.85% 45% 2 98% 2% 1Peter Pan 20 85.2% 85.0% 106.9% N/A 10.66% 13%NNU 20 67.1% 127.7% 76.6% N/A 5.15% 0% 2Alex 22 78.0% 90.2% 100.0% 95.8% 3.29% 2% 11 1 97% 2
Kath 15 89.3% 76.7% 98.6% 96.7% 20.41% 3% 5
Labour 13 79.1% 72.2% 98.6% 95.2% 8.30% 6% 4 94% 1% 1
**E-rostering report, workforce report ***Incidents reported via datix**** Proportion of bank and agency nursing information provided by temporary staffing office and workforce information
Days NightsDivision Ward
Med
icin
eSu
rger
y
Falls Safety
Thermometer
Medication errors***
Nurse Sensitive Outcome Indicators
STAFFING LEVELS April 2015 Data - May 2015 Report V1
Beds New PU Safety
Thermometer
Hospital Acquired Pressure Ulcers***
Falls with no harm / Falls resulting in
harm***
FFT % of patients
extremely likely/likely
Fill Rates**Environment
Sub -optimal staffing
reported via datix
Proportion of Agency hours****
Proportion Bank hours
Temporary Staffing
FFT % of patients
extremely unlikely/unlikely
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 14
Integrated Quality & Performance Report
Reason for item:
This report provides the Board with an analysis of quality and operational performance to the end of April 2015. The report covers performance against the Monitor Risk Assessment Framework as well as national and local key performance indicators.
Summary:
This is the second phase of the integrated board report. This report now includes the quality performance and the operational performance in the new style format. The workforce metrics continue to be in the previous format due to the timeless of the data available. Work remains underway on the data collection processes with the aim to resolving this for the June Board. Changes have been made from the first version following feedback from Board members. The Board is asked to consider both the format and contents of the performance report to improve subsequent versions.
Board Action required:
The Board is asked to: 1. Agree any changes to the format and contents of future Reports;2. To agree any actions arising from the contents of this Report
Report from: Melissa Mellett, Interim Director of Operational Performance and Jacqueline Walker, Deputy Director of Nursing and Integrated Governance
Report sponsor: Joe Smyth, Chief Operating Officer
Links to Trust strategic priorities:
• To create a patient centred organisation to deliver improvements in patient experienceand the quality of care we provide.
• To deliver high quality care in the most efficient way.
Previous consideration at Board or Committees: Reviewed monthly as standard
Equality and diversity considerations: There is no positive or negative impact from this report.
Financial implications: The financial implications of delivering the additional capacity to meet the non-elective demand over and above plan are detailed in the report.
1
Integrated performance report 1. Summary This is the second phase of moving to an Integrated Board Report which will set out progress against our vision “To put compassionate care, safety and quality at the heart of everything we do”, and against our key objective of a patient centred organisation and delivering high quality care in the most efficient way. 2. Timing Data on the workforce indicators in the Dashboard are not yet available through automated processes. Workforce data requires significant manual input to compile and is therefore always presented a month in arrears. This process is being reviewed, with a view to automating the collection method which will bring the timing of the workforce data in line with the other standards. The Quality indicators have now been added to provide a more comprehensive overview. Further work is required to streamline the reporting and to provide more comprehensive analysis. 3. Contents and items of note
3.1 Safe The range of information available gives assurance that Hillingdon Hospital services continue to be safe and of good quality, with lower mortality than the expected case mix. There is a risk associated with the Clostridium Difficile objective as two cases have been reported in April and a further case in May; detailed root cause analysis (RCA) investigations have been completed for the April cases and there was no evidence of lapse of care. The third RCA is currently underway. 3.2 Effective 30 day readmission position has deteriorated slightly a robust action plan is in place following the root cause analysis. DNA rates remain within a good threshold. Extensive work is being undertaken to improve the availability of Choose and Book slots for GPs and patients. Work continues within the Divisions on recovery plans, the main problems relating to capacity within certain specialties. 3.3 Caring Patients’ feedback on their experience of services is very positive. However further work is required to improve response rates particularly in A&E.
2
3.4 Responsive The Trust achieved 94.9% against the 95% A&E four hour target. Extensive work is being undertaken with the CCG to implemented schemes to prevent patients presenting at A&E or to support admission avoidance. The Transforming Patient Care (TPC) programme chaired by the Divisional Director for Medicine has commenced work on making the significant changes required to improve patient pathways to reduce lengths of stay and help reduce the number of beds in the Trust. The planned closure of escalation beds will provide additional permanent nursing staff for the remaining established wards. The Trust continues to sustain excellent performance in both the admitted and non-admitted RTT treatment pathways. 3.5 Well-Led
The data contained in the workforce dashboards remains a month in arrears. Work is continuing to automate the collection of data which will bring reporting in line with the other indicators. 4. Summary This is a new style report to the Board which integrates reporting on quality and performance. The report remains under development and comments are invited to the Director of Operational Performance. The purpose of the report is to ensure the Board is sighted on areas of concern and provided with a high level analysis on actions being taken to improve performance. This is achieved by presenting a balanced set of key performance indicators (KPIs) giving a more comprehensive view of the quality and performance standards. The Board is asked to agree the changes to the format and note the content of this report.
3
Appendix 1 Extreme and high level corporate risk review at the monthly Trust Management
Executive (TME) meeting, 6th May 2015
Before the corporate risk register was discussed A.D. Governance & Quality Standards (ADGQS) reminded TME of the changes to the risk evaluation matrix and that this is the first report received under the revised Board approved risk management strategy & policy. Corporate Risk Register 5 extreme level risks and 27 high level risks were presented to TME. The following risk discussions took place:
• 350 – Suboptimal maternity staffing levels within Midwifery, Obstetrics and Anaesthetics – Chief Executive (CE) asked for clarification whether the controls in place are adequate. For obstetric cover, there is a clear escalation process and a clear remit for suspension of services. The 2nd tier and cover at night will be resolved with SaHF. These controls will reduce the risk and mitigate. Risk level for review as gaps close.
• 452 - Estates records of compliance with Health Technical Memoranda and statutory standards – Director of Strategic Estate Development & Asset Management (DoE) stated there is reporting to the Board Audit & Assurance Committee. There will be mitigation once the tenders are sorted. We are moving in the right direction. There was discussion regarding clarity of what were the controls and what were the actions. Controls and actions to be reviewed and tidied up.
• 461 – Theatre Ventilation Compliance with Health Technical Memorandum – One theatre is now finished and two are nearly finished. Again gaps and actions need tidying.
• 480 – Healthcare Contract Penalties – Finance Director explained that it is an extremely high risk that we will not achieve the targets and incur financial penalties. He said although the contract control mitigates the full impact of the penalties, there will still be an impact. Controls to be updated and be more specific regarding CDiff and VTE and the actions being taken to mitigate the risks.
• 279 – Repeated problems with critical monitoring alarm system – DoE stated that UPS is now fitted. DoE to check on work that has been completed and gaps to be updated, risk level reviewed.
• Other risks were discussed: • 190 – Electrical single point of failure –clarification was sought that this was
an accepted risk. This was agreed at this point in time but would be due for review in a year as with all accepted risks.
• 194 – Environmental Controls in Therapies, Minor Injuries, X-Ray, Trinity Ward and Day Care in Princess Christian section of Mount Vernon Treatment
4
Centre - Executive Lead update. Chief Operating Officer is Executive Lead for operations and Director of Strategy & Business Developments for Estates. Risks are to be updated with this information. ADO Mount Vernon stated that the area is mainly too hot, it is a worry for patients and they have threatened not to come in. Estates are completing a survey regarding this. Discussion was had about the batteries being removed and because of this CE said that the TME is not for discussion around detail and resolution is to be done outside of the meeting. Detail to be discussed at the Estates Governance Group. The operational risk needs addressing.
5
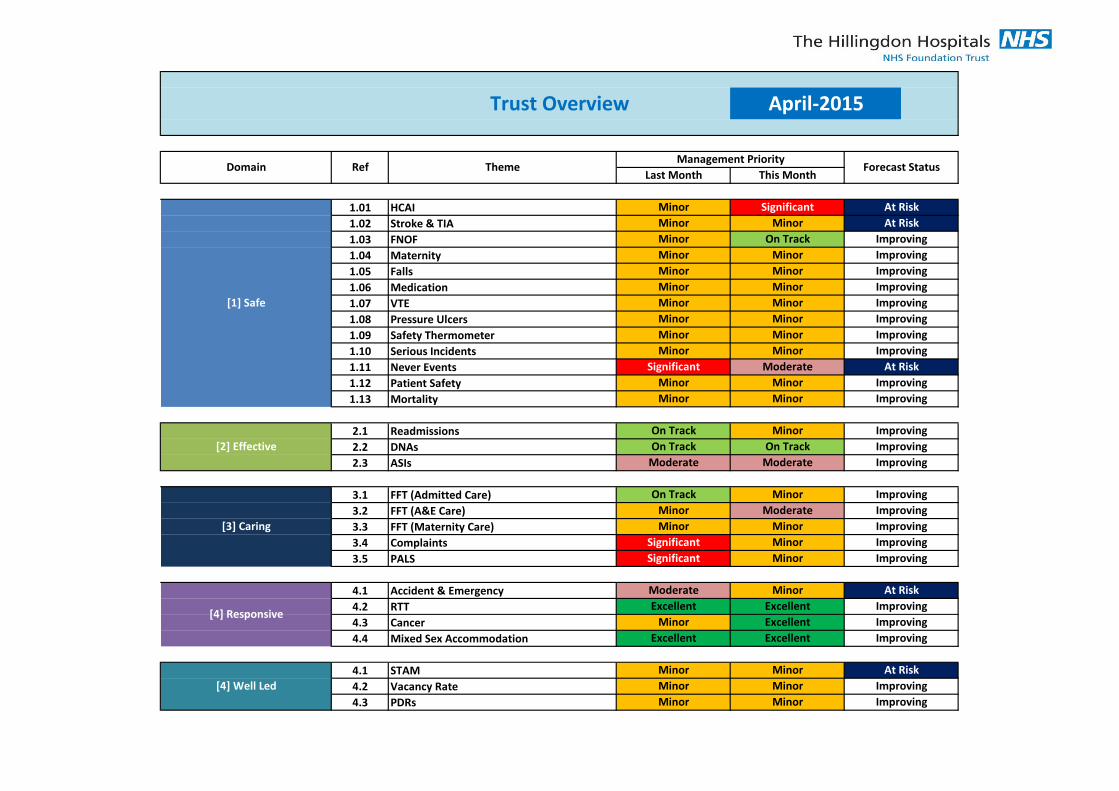
1.01
1.02
1.03
1.04
1.05
1.06
1.07
1.08
1.09
1.10
1.11
1.12
1.13
2.1
2.2
2.3
3.1
3.2
3.3
3.4
3.5
4.1
4.2
4.3
4.4
4.1
4.2
4.3
[4] Responsive
Mixed Sex Accommodation Excellent Excellent Improving
Improving
[3] Caring
Complaints Significant Minor Improving
PALS Significant Minor Improving
[1] Safe
Medication Minor Minor Improving
VTE Minor Minor Improving
FFT (Admitted Care) On Track Minor Improving
At Risk
Patient Safety Minor Minor Improving
FFT (A&E Care) Minor Moderate Improving
FFT (Maternity Care) Minor Minor Improving
ImprovingCancer Minor
Trust Overview April-2015
Domain Ref
Accident & Emergency Moderate Minor At Risk
RTT Excellent Excellent Improving
Improving
Minor Minor
Minor On Track
Minor
Minor Minor Improving
Forecast StatusManagement Priority
Last Month This Month
Minor Significant At Risk
Theme
HCAI
Stroke & TIA
FNOF
Excellent
Maternity
MinorFalls
Never Events Significant Moderate
Mortality Minor Minor
Improving
Improving
DNAs On Track On Track Improving[2] Effective
Readmissions On Track Minor
ASIs Moderate Moderate
At Risk
Improving
Pressure Ulcers Minor Minor Improving
Safety Thermometer Minor Minor Improving
Serious Incidents Minor Minor Improving
[4] Well Led
STAM Minor Minor At Risk
Vacancy Rate Minor Minor Improving
PDRs Minor Minor Improving
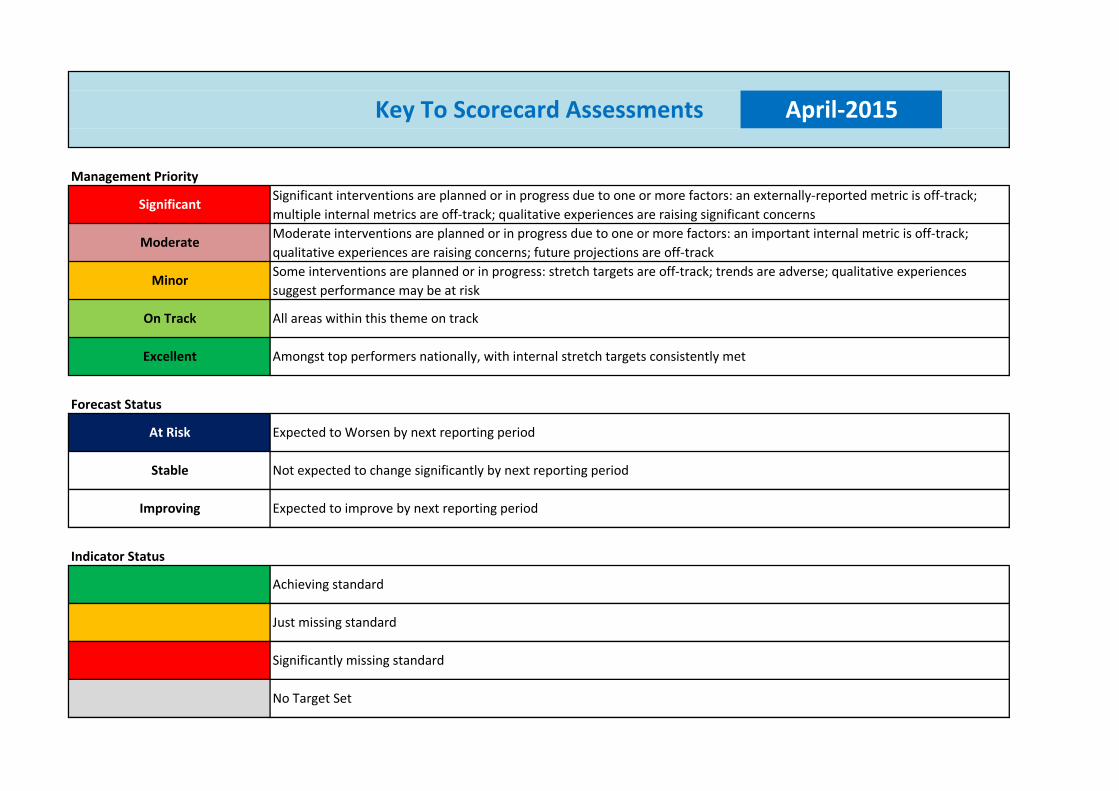
Forecast Status
Indicator Status
Significant interventions are planned or in progress due to one or more factors: an externally-reported metric is off-track;
multiple internal metrics are off-track; qualitative experiences are raising significant concerns
Moderate interventions are planned or in progress due to one or more factors: an important internal metric is off-track;
qualitative experiences are raising concerns; future projections are off-track
Some interventions are planned or in progress: stretch targets are off-track; trends are adverse; qualitative experiences
suggest performance may be at risk
Key To Scorecard Assessments April-2015
Management Priority
Significant
Moderate
Minor
On Track All areas within this theme on track
Amongst top performers nationally, with internal stretch targets consistently met
At Risk Expected to Worsen by next reporting period
Stable Not expected to change significantly by next reporting period
Excellent
Significantly missing standard
No Target Set
Improving Expected to improve by next reporting period
Achieving standard
Just missing standard
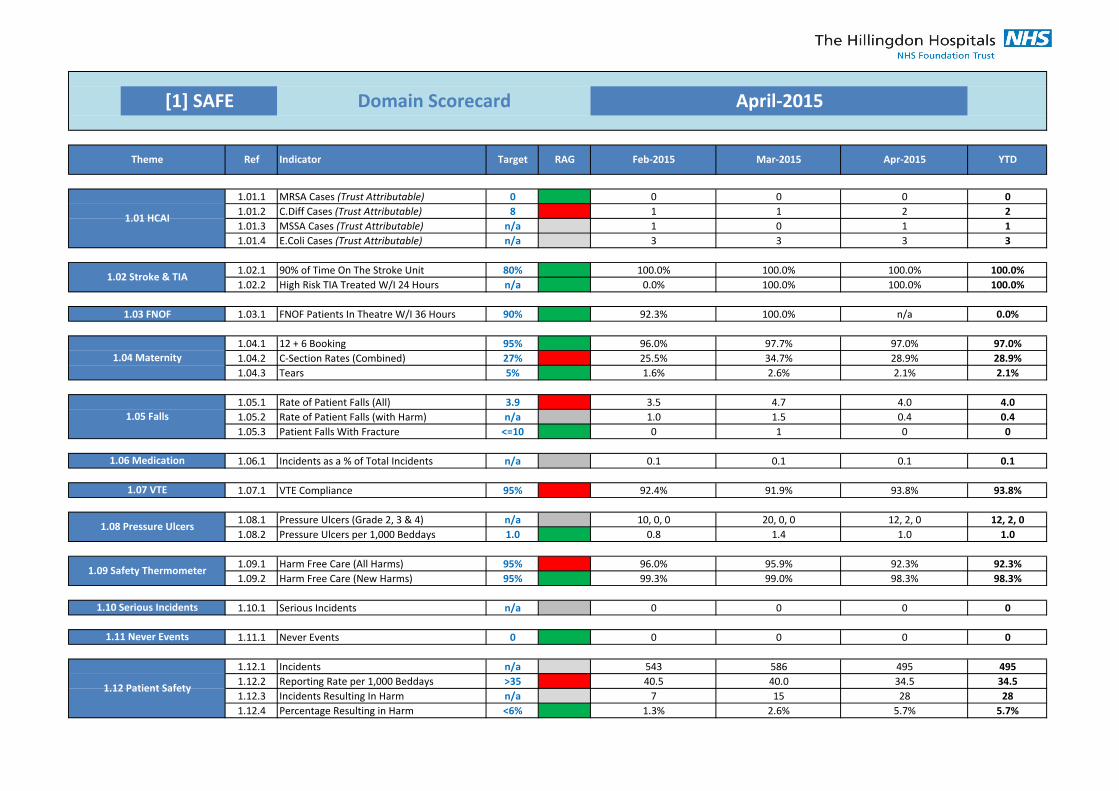
1.01.1 0 0 0 0 0
1.01.2 8 1 1 2 2
1.01.3 n/a 1 0 1 1
1.01.4 n/a 3 3 3 3
1.02.1 80% 100.0% 100.0% 100.0% 100.0%
1.02.2 n/a 0.0% 100.0% 100.0% 100.0%
1.03.1 90% 92.3% 100.0% n/a 0.0%
1.04.1 95% 96.0% 97.7% 97.0% 97.0%
1.04.2 27% 25.5% 34.7% 28.9% 28.9%
1.04.3 5% 1.6% 2.6% 2.1% 2.1%
1.05.1 3.9 3.5 4.7 4.0 4.0
1.05.2 n/a 1.0 1.5 0.4 0.4
1.05.3 <=10 0 1 0 0
1.06.1 n/a 0.1 0.1 0.1 0.1
1.07.1 95% 92.4% 91.9% 93.8% 93.8%
1.08.1 n/a 10, 0, 0 20, 0, 0 12, 2, 0 12, 2, 0
1.08.2 1.0 0.8 1.4 1.0 1.0
1.09.1 95% 96.0% 95.9% 92.3% 92.3%
1.09.2 95% 99.3% 99.0% 98.3% 98.3%
1.10.1 n/a 0 0 0 0
1.11.1 0 0 0 0 0
1.12.1 n/a 543 586 495 495
1.12.2 >35 40.5 40.0 34.5 34.5
1.12.3 n/a 7 15 28 28
1.12.4 <6% 1.3% 2.6% 5.7% 5.7%
[1] SAFE Domain Scorecard April-2015
Theme Ref Target RAG Feb-2015 Mar-2015 Apr-2015 YTDIndicator
MRSA Cases (Trust Attributable)
C.Diff Cases (Trust Attributable)
1.05 Falls
Rate of Patient Falls (All)
Rate of Patient Falls (with Harm)
Patient Falls With Fracture
E.Coli Cases (Trust Attributable)
1.01 HCAIMSSA Cases (Trust Attributable)
1.04 Maternity
12 + 6 Booking
C-Section Rates (Combined)
Tears
1.02 Stroke & TIA90% of Time On The Stroke Unit
High Risk TIA Treated W/I 24 Hours
1.03 FNOF FNOF Patients In Theatre W/I 36 Hours
1.09 Safety ThermometerHarm Free Care (All Harms)
Harm Free Care (New Harms)
1.06 Medication Incidents as a % of Total Incidents
1.07 VTE VTE Compliance
1.08 Pressure UlcersPressure Ulcers (Grade 2, 3 & 4)
Pressure Ulcers per 1,000 Beddays
1.10 Serious Incidents Serious Incidents
1.11 Never Events Never Events
1.12 Patient Safety
Incidents
Reporting Rate per 1,000 Beddays
Incidents Resulting In Harm
Percentage Resulting in Harm
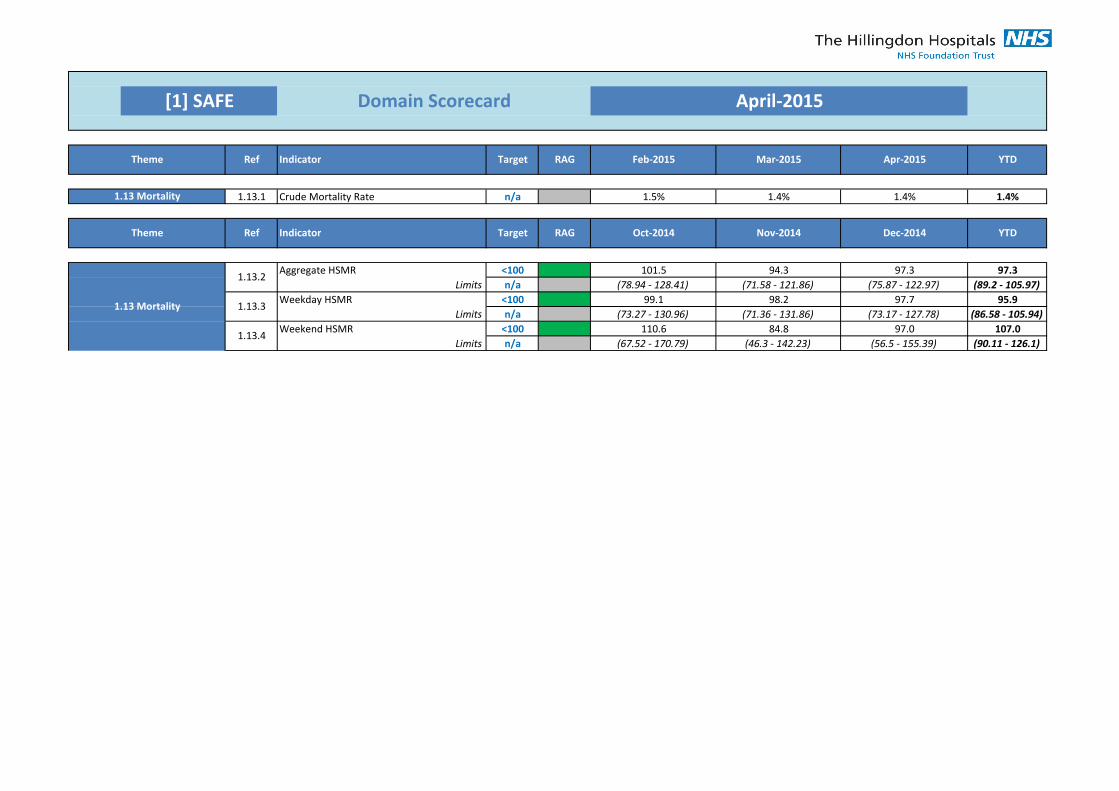
[1] SAFE Domain Scorecard April-2015
1.13.1 n/a 1.5% 1.4% 1.4% 1.4%
<100 101.5 94.3 97.3 97.3
n/a (78.94 - 128.41) (71.58 - 121.86) (75.87 - 122.97) (89.2 - 105.97)
<100 99.1 98.2 97.7 95.9
n/a (73.27 - 130.96) (71.36 - 131.86) (73.17 - 127.78) (86.58 - 105.94)
<100 110.6 84.8 97.0 107.0
n/a (67.52 - 170.79) (46.3 - 142.23) (56.5 - 155.39) (90.11 - 126.1)
RAG Oct-2014 Nov-2014 Dec-2014 YTDTheme Ref Indicator Target
1.13 Mortality
Aggregate HSMR
Limits
Weekday HSMR
Limits
Weekend HSMR
Limits
1.13.2
1.13.3
1.13.4
1.13 Mortality Crude Mortality Rate
Theme Ref Indicator YTDTarget RAG Feb-2015 Mar-2015 Apr-2015
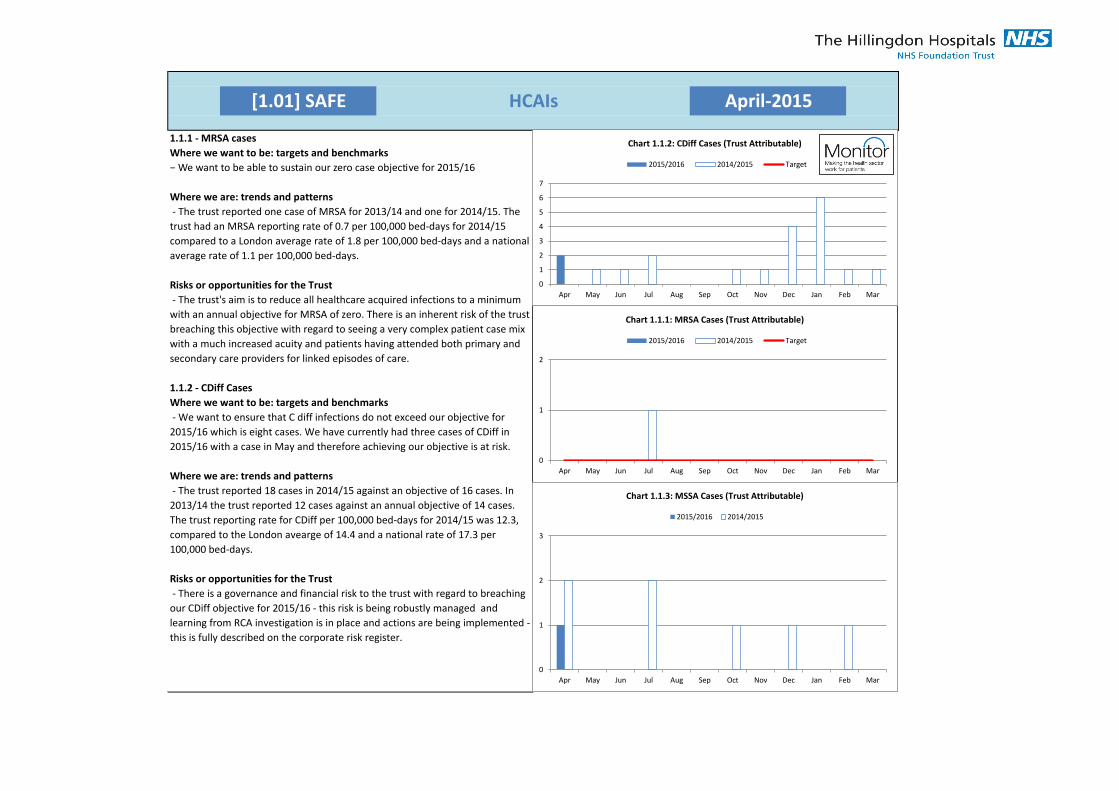
[1.01] SAFE April-2015HCAIs
1.1.1 - MRSA cases
Where we want to be: targets and benchmarks
− We want to be able to sustain our zero case objective for 2015/16
Where we are: trends and patterns
- The trust reported one case of MRSA for 2013/14 and one for 2014/15. The
trust had an MRSA reporting rate of 0.7 per 100,000 bed-days for 2014/15
compared to a London average rate of 1.8 per 100,000 bed-days and a national
average rate of 1.1 per 100,000 bed-days.
Risks or opportunities for the Trust
- The trust's aim is to reduce all healthcare acquired infections to a minimum
with an annual objective for MRSA of zero. There is an inherent risk of the trust
breaching this objective with regard to seeing a very complex patient case mix
with a much increased acuity and patients having attended both primary and
secondary care providers for linked episodes of care.
1.1.2 - CDiff Cases
Where we want to be: targets and benchmarks
- We want to ensure that C diff infections do not exceed our objective for
2015/16 which is eight cases. We have currently had three cases of CDiff in
2015/16 with a case in May and therefore achieving our objective is at risk.
Where we are: trends and patterns
- The trust reported 18 cases in 2014/15 against an objective of 16 cases. In
2013/14 the trust reported 12 cases against an annual objective of 14 cases.
The trust reporting rate for CDiff per 100,000 bed-days for 2014/15 was 12.3,
compared to the London avearge of 14.4 and a national rate of 17.3 per
100,000 bed-days.
Risks or opportunities for the Trust
- There is a governance and financial risk to the trust with regard to breaching
our CDiff objective for 2015/16 - this risk is being robustly managed and
learning from RCA investigation is in place and actions are being implemented -
this is fully described on the corporate risk register.
0
1
2
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Chart 1.1.1: MRSA Cases (Trust Attributable)
2015/2016 2014/2015 Target
0
1
2
3
4
5
6
7
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Chart 1.1.2: CDiff Cases (Trust Attributable)
2015/2016 2014/2015 Target
0
1
2
3
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Chart 1.1.3: MSSA Cases (Trust Attributable)
2015/2016 2014/2015
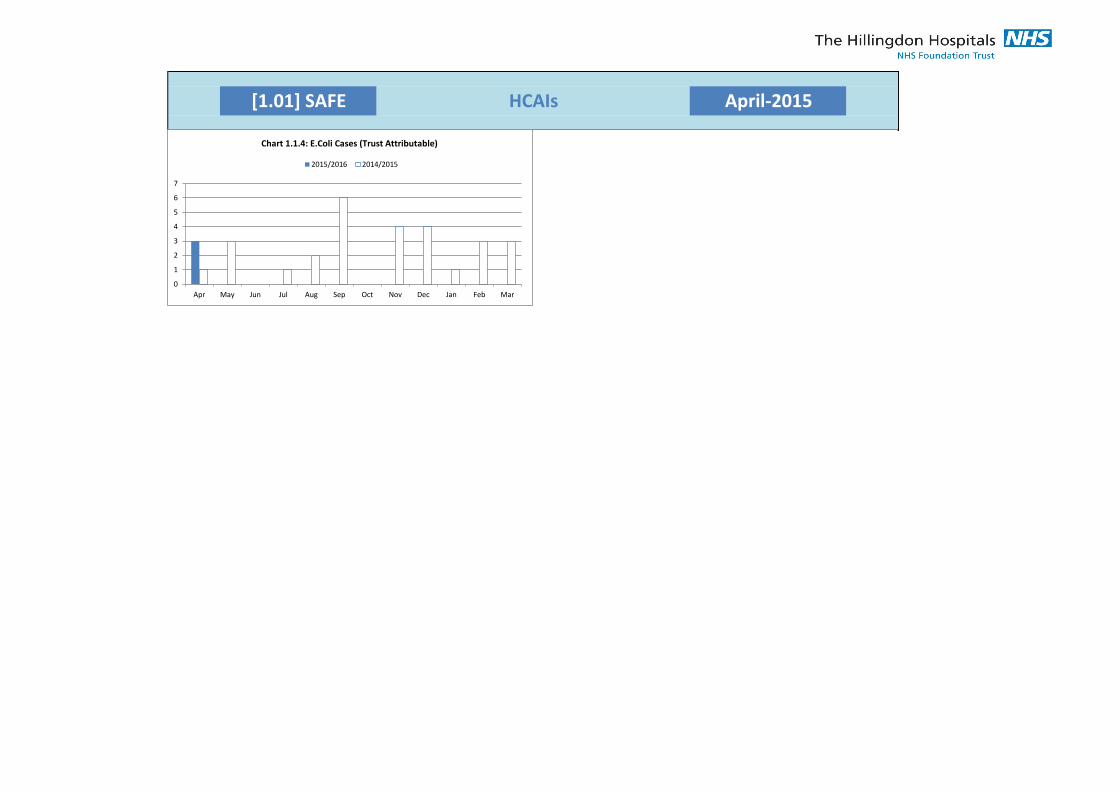
[1.01] SAFE April-2015HCAIs
0
1
2
3
4
5
6
7
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Chart 1.1.4: E.Coli Cases (Trust Attributable)
2015/2016 2014/2015
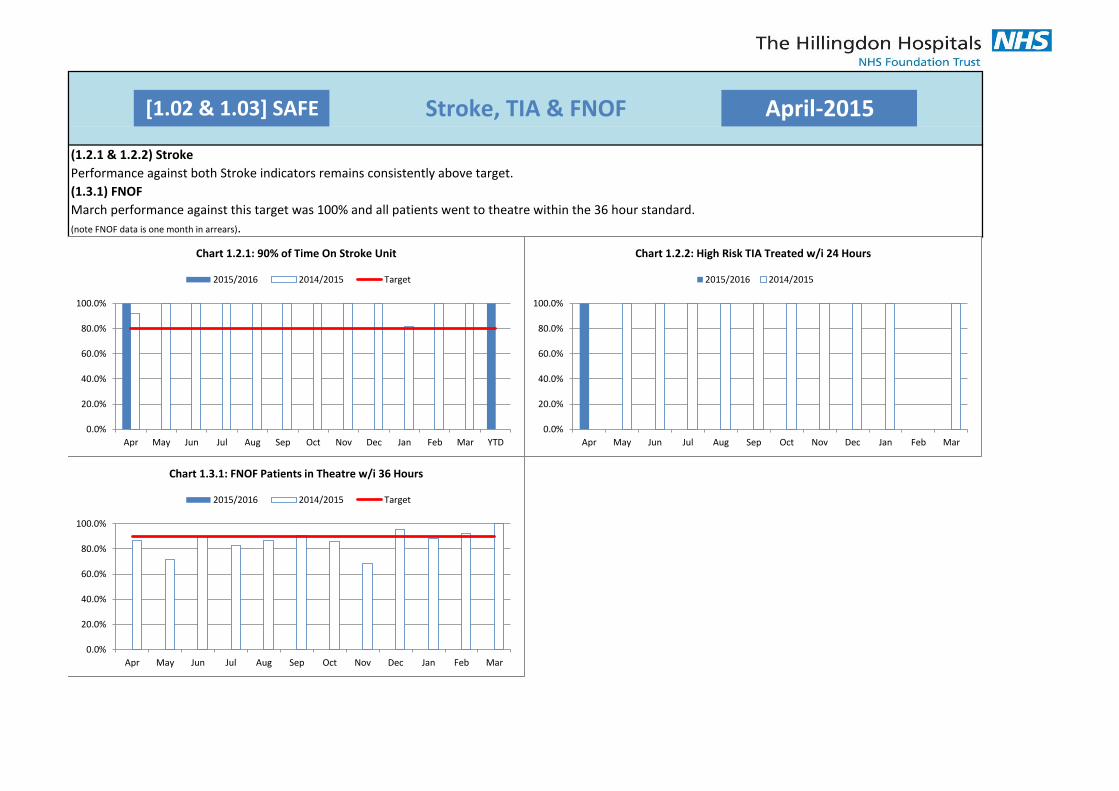
[1.02 & 1.03] SAFE Stroke, TIA & FNOF April-2015
(1.2.1 & 1.2.2) Stroke
Performance against both Stroke indicators remains consistently above target.
(1.3.1) FNOF
March performance against this target was 100% and all patients went to theatre within the 36 hour standard.
(note FNOF data is one month in arrears).
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
Chart 1.2.1: 90% of Time On Stroke Unit
2015/2016 2014/2015 Target
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Chart 1.2.2: High Risk TIA Treated w/i 24 Hours
2015/2016 2014/2015
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Chart 1.3.1: FNOF Patients in Theatre w/i 36 Hours
2015/2016 2014/2015 Target
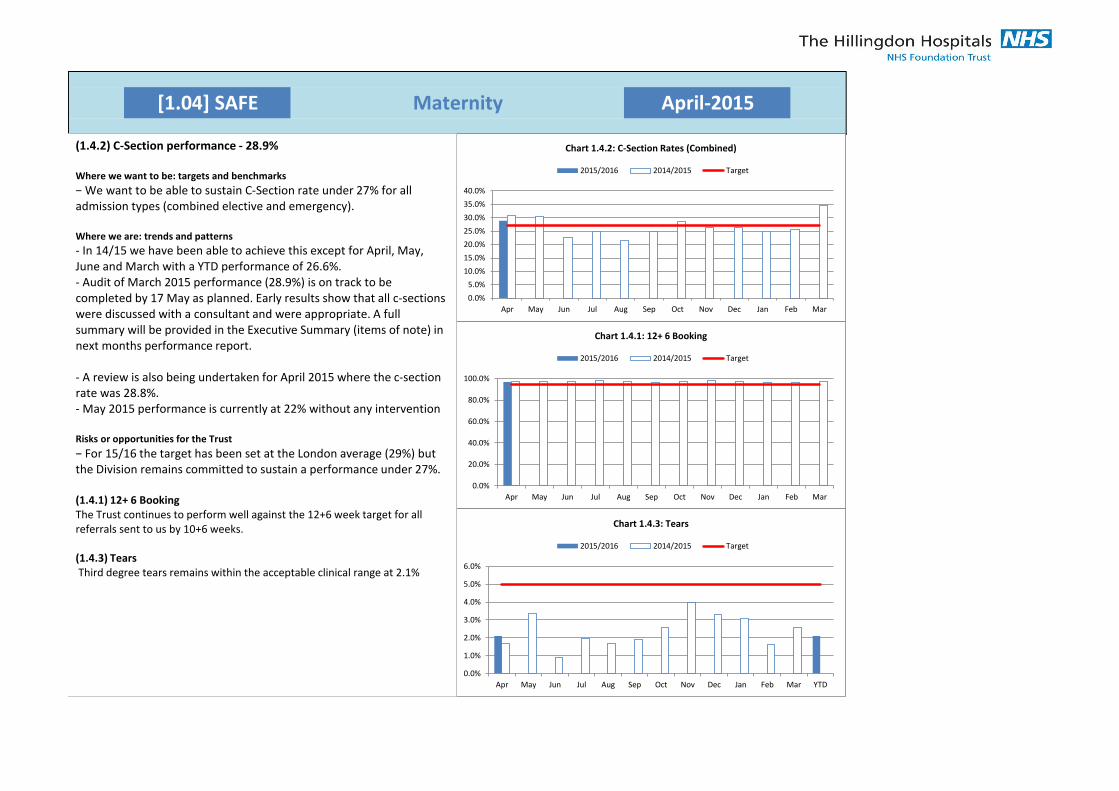
[1.04] SAFE Maternity April-2015
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Chart 1.4.1: 12+ 6 Booking
2015/2016 2014/2015 Target
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
35.0%
40.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Chart 1.4.2: C-Section Rates (Combined)
2015/2016 2014/2015 Target
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar YTD
Chart 1.4.3: Tears
2015/2016 2014/2015 Target
(1.4.2) C-Section performance - 28.9%
Where we want to be: targets and benchmarks
− We want to be able to sustain C-Section rate under 27% for all admission types (combined elective and emergency).
Where we are: trends and patterns
- In 14/15 we have been able to achieve this except for April, May, June and March with a YTD performance of 26.6%. - Audit of March 2015 performance (28.9%) is on track to be completed by 17 May as planned. Early results show that all c-sections were discussed with a consultant and were appropriate. A full summary will be provided in the Executive Summary (items of note) in next months performance report.
- A review is also being undertaken for April 2015 where the c-section rate was 28.8%. - May 2015 performance is currently at 22% without any intervention
Risks or opportunities for the Trust
− For 15/16 the target has been set at the London average (29%) but the Division remains committed to sustain a performance under 27%.
(1.4.1) 12+ 6 Booking The Trust continues to perform well against the 12+6 week target for all referrals sent to us by 10+6 weeks.
(1.4.3) Tears Third degree tears remains within the acceptable clinical range at 2.1%
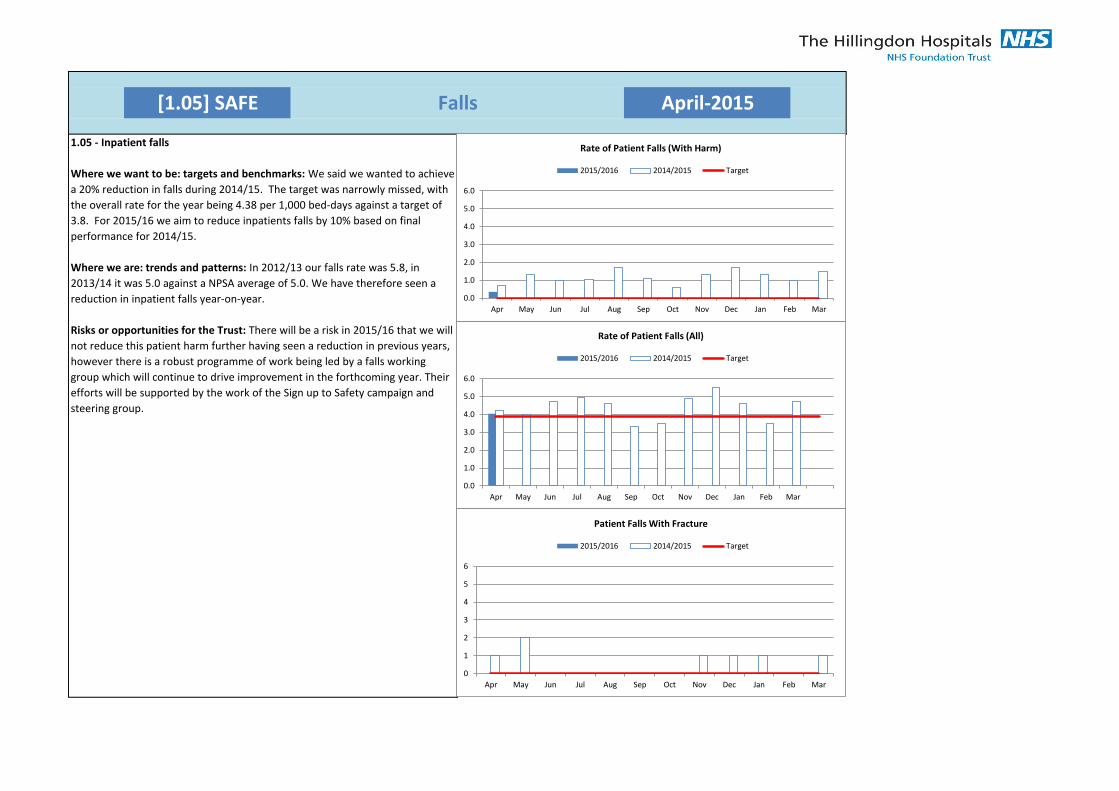
[1.05] SAFE Falls April-2015
1.05 - Inpatient falls
Where we want to be: targets and benchmarks: We said we wanted to achieve
a 20% reduction in falls during 2014/15. The target was narrowly missed, with
the overall rate for the year being 4.38 per 1,000 bed-days against a target of
3.8. For 2015/16 we aim to reduce inpatients falls by 10% based on final
performance for 2014/15.
Where we are: trends and patterns: In 2012/13 our falls rate was 5.8, in
2013/14 it was 5.0 against a NPSA average of 5.0. We have therefore seen a
reduction in inpatient falls year-on-year.
Risks or opportunities for the Trust: There will be a risk in 2015/16 that we will
not reduce this patient harm further having seen a reduction in previous years,
however there is a robust programme of work being led by a falls working
group which will continue to drive improvement in the forthcoming year. Their
efforts will be supported by the work of the Sign up to Safety campaign and
steering group.
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Rate of Patient Falls (All)
2015/2016 2014/2015 Target
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Rate of Patient Falls (With Harm)
2015/2016 2014/2015 Target
0
1
2
3
4
5
6
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Patient Falls With Fracture
2015/2016 2014/2015 Target
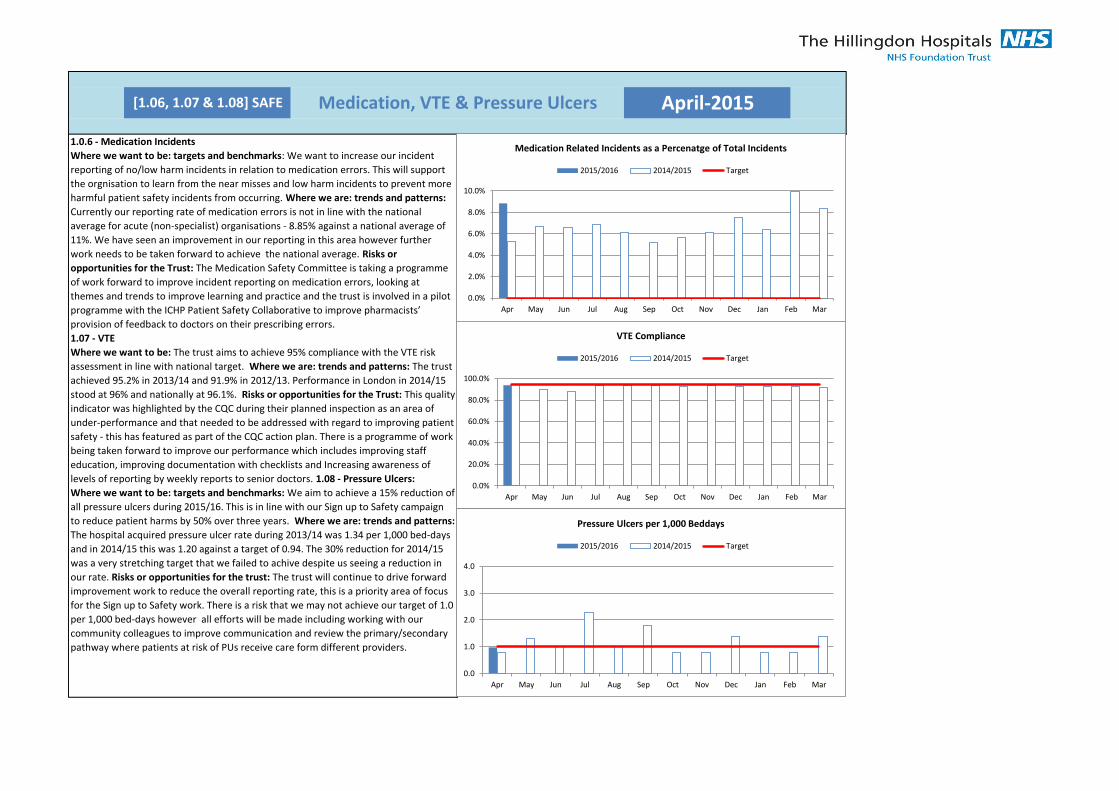
[1.06, 1.07 & 1.08] SAFE Medication, VTE & Pressure Ulcers April-2015
1.0.6 - Medication Incidents
Where we want to be: targets and benchmarks: We want to increase our incident
reporting of no/low harm incidents in relation to medication errors. This will support
the orgnisation to learn from the near misses and low harm incidents to prevent more
harmful patient safety incidents from occurring. Where we are: trends and patterns:
Currently our reporting rate of medication errors is not in line with the national
average for acute (non-specialist) organisations - 8.85% against a national average of
11%. We have seen an improvement in our reporting in this area however further
work needs to be taken forward to achieve the national average. Risks or
opportunities for the Trust: The Medication Safety Committee is taking a programme
of work forward to improve incident reporting on medication errors, looking at
themes and trends to improve learning and practice and the trust is involved in a pilot
programme with the ICHP Patient Safety Collaborative to improve pharmacists’
provision of feedback to doctors on their prescribing errors.
1.07 - VTE
Where we want to be: The trust aims to achieve 95% compliance with the VTE risk
assessment in line with national target. Where we are: trends and patterns: The trust
achieved 95.2% in 2013/14 and 91.9% in 2012/13. Performance in London in 2014/15
stood at 96% and nationally at 96.1%. Risks or opportunities for the Trust: This quality
indicator was highlighted by the CQC during their planned inspection as an area of
under-performance and that needed to be addressed with regard to improving patient
safety - this has featured as part of the CQC action plan. There is a programme of work
being taken forward to improve our performance which includes improving staff
education, improving documentation with checklists and Increasing awareness of
levels of reporting by weekly reports to senior doctors. 1.08 - Pressure Ulcers:
Where we want to be: targets and benchmarks: We aim to achieve a 15% reduction of
all pressure ulcers during 2015/16. This is in line with our Sign up to Safety campaign
to reduce patient harms by 50% over three years. Where we are: trends and patterns:
The hospital acquired pressure ulcer rate during 2013/14 was 1.34 per 1,000 bed-days
and in 2014/15 this was 1.20 against a target of 0.94. The 30% reduction for 2014/15
was a very stretching target that we failed to achive despite us seeing a reduction in
our rate. Risks or opportunities for the trust: The trust will continue to drive forward
improvement work to reduce the overall reporting rate, this is a priority area of focus
for the Sign up to Safety work. There is a risk that we may not achieve our target of 1.0
per 1,000 bed-days however all efforts will be made including working with our
community colleagues to improve communication and review the primary/secondary
pathway where patients at risk of PUs receive care form different providers.
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Medication Related Incidents as a Percenatge of Total Incidents
2015/2016 2014/2015 Target
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
VTE Compliance
2015/2016 2014/2015 Target
0.0
1.0
2.0
3.0
4.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Pressure Ulcers per 1,000 Beddays
2015/2016 2014/2015 Target
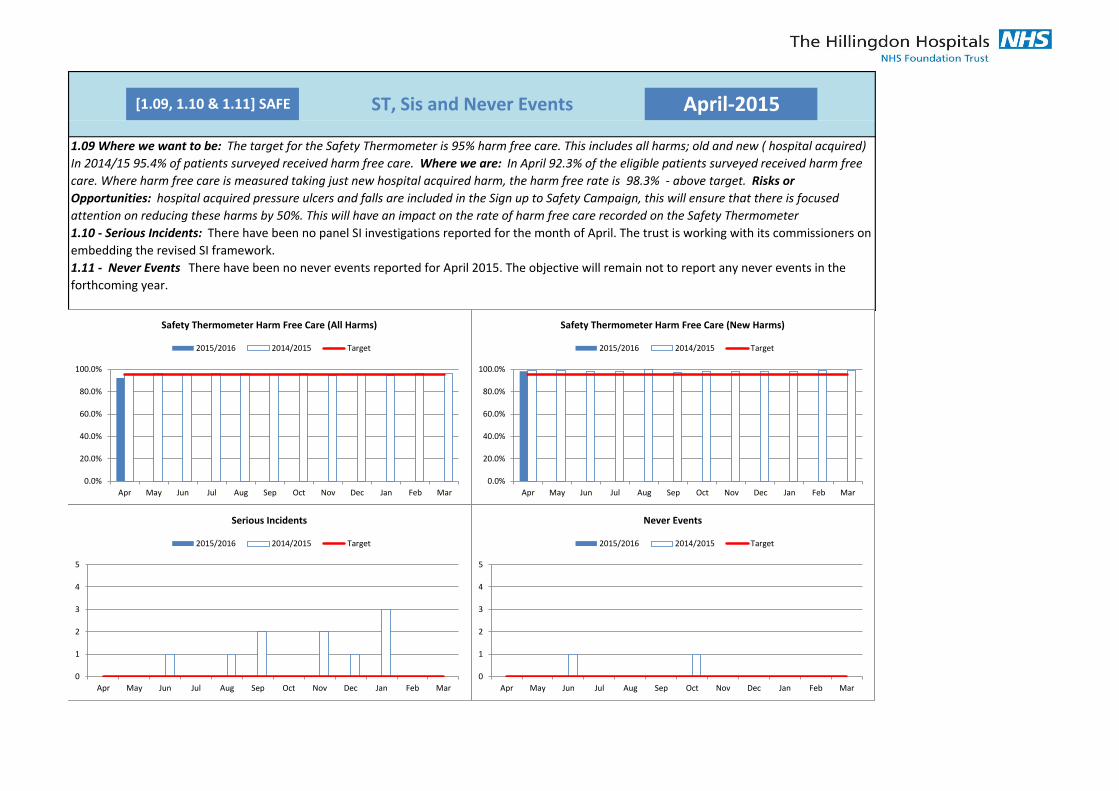
[1.09, 1.10 & 1.11] SAFE ST, Sis and Never Events April-2015
1.09 Where we want to be: The target for the Safety Thermometer is 95% harm free care. This includes all harms; old and new ( hospital acquired)
In 2014/15 95.4% of patients surveyed received harm free care. Where we are: In April 92.3% of the eligible patients surveyed received harm free
care. Where harm free care is measured taking just new hospital acquired harm, the harm free rate is 98.3% - above target. Risks or
Opportunities: hospital acquired pressure ulcers and falls are included in the Sign up to Safety Campaign, this will ensure that there is focused
attention on reducing these harms by 50%. This will have an impact on the rate of harm free care recorded on the Safety Thermometer
1.10 - Serious Incidents: There have been no panel SI investigations reported for the month of April. The trust is working with its commissioners on
embedding the revised SI framework.
1.11 - Never Events There have been no never events reported for April 2015. The objective will remain not to report any never events in the
forthcoming year.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Safety Thermometer Harm Free Care (All Harms)
2015/2016 2014/2015 Target
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Safety Thermometer Harm Free Care (New Harms)
2015/2016 2014/2015 Target
0
1
2
3
4
5
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Serious Incidents
2015/2016 2014/2015 Target
0
1
2
3
4
5
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Never Events
2015/2016 2014/2015 Target
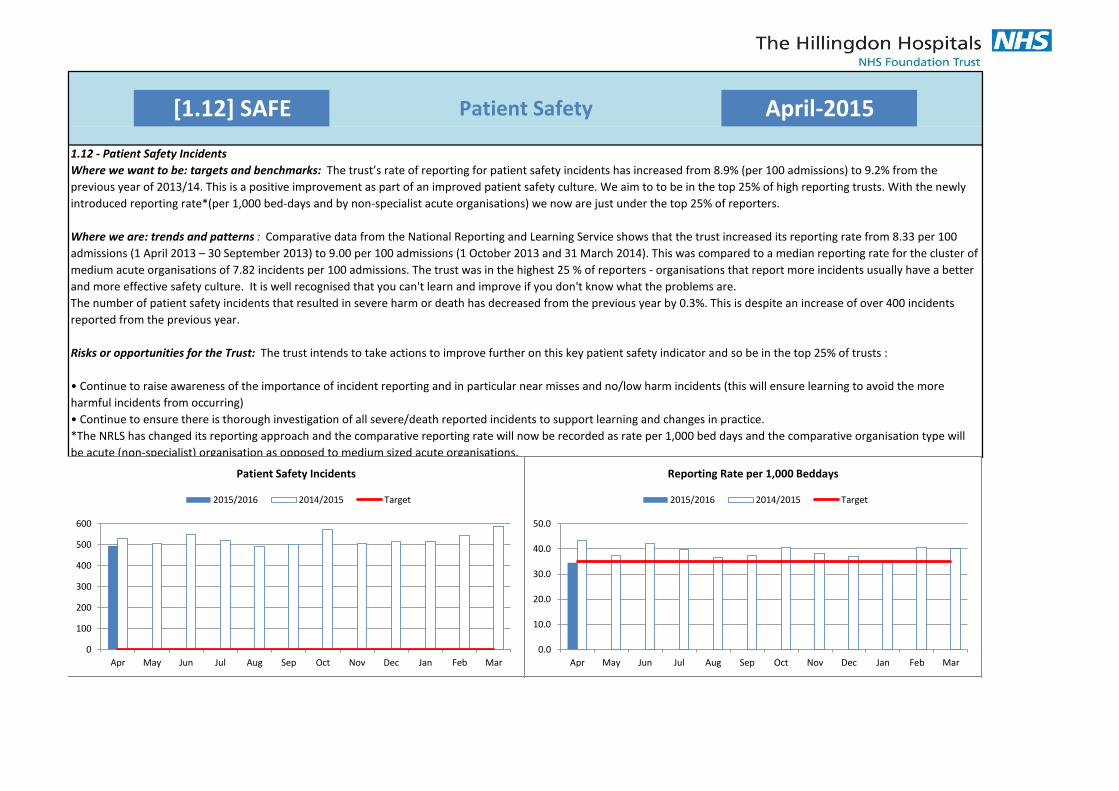
[1.12] SAFE Patient Safety April-2015
1.12 - Patient Safety Incidents
Where we want to be: targets and benchmarks: The trust’s rate of reporting for patient safety incidents has increased from 8.9% (per 100 admissions) to 9.2% from the
previous year of 2013/14. This is a positive improvement as part of an improved patient safety culture. We aim to to be in the top 25% of high reporting trusts. With the newly
introduced reporting rate*(per 1,000 bed-days and by non-specialist acute organisations) we now are just under the top 25% of reporters.
Where we are: trends and patterns : Comparative data from the National Reporting and Learning Service shows that the trust increased its reporting rate from 8.33 per 100
admissions (1 April 2013 – 30 September 2013) to 9.00 per 100 admissions (1 October 2013 and 31 March 2014). This was compared to a median reporting rate for the cluster of
medium acute organisations of 7.82 incidents per 100 admissions. The trust was in the highest 25 % of reporters - organisations that report more incidents usually have a better
and more effective safety culture. It is well recognised that you can't learn and improve if you don't know what the problems are.
The number of patient safety incidents that resulted in severe harm or death has decreased from the previous year by 0.3%. This is despite an increase of over 400 incidents
reported from the previous year.
Risks or opportunities for the Trust: The trust intends to take actions to improve further on this key patient safety indicator and so be in the top 25% of trusts :
• Continue to raise awareness of the importance of incident reporting and in particular near misses and no/low harm incidents (this will ensure learning to avoid the more
harmful incidents from occurring)
• Continue to ensure there is thorough investigation of all severe/death reported incidents to support learning and changes in practice.
*The NRLS has changed its reporting approach and the comparative reporting rate will now be recorded as rate per 1,000 bed days and the comparative organisation type will
be acute (non-specialist) organisation as opposed to medium sized acute organisations.
0
100
200
300
400
500
600
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Patient Safety Incidents
2015/2016 2014/2015 Target
0.0
10.0
20.0
30.0
40.0
50.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Reporting Rate per 1,000 Beddays
2015/2016 2014/2015 Target

[1.12] SAFE Patient Safety April-2015
0
10
20
30
40
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Incidents Resulting In Harm
2015/2016 2014/2015 Target
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Percentage Resulting In Harm
2015/2016 2014/2015 Target
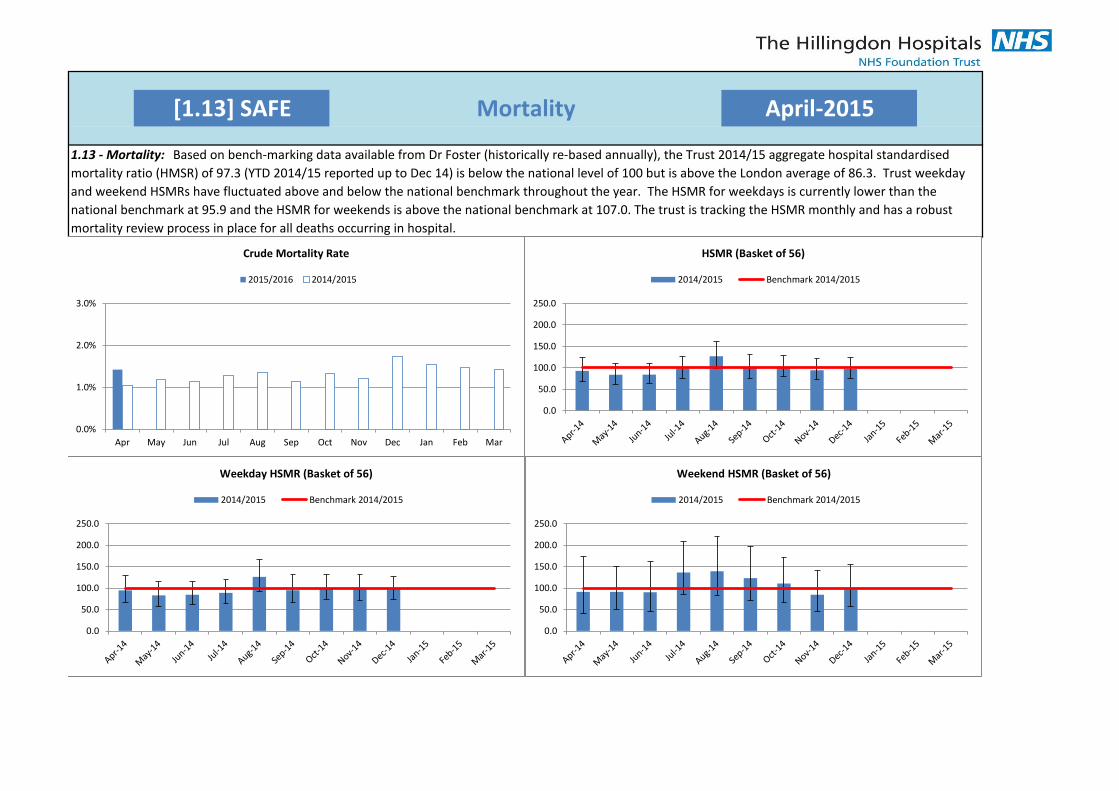
[1.13] SAFE Mortality April-2015
1.13 - Mortality: Based on bench-marking data available from Dr Foster (historically re-based annually), the Trust 2014/15 aggregate hospital standardised
mortality ratio (HMSR) of 97.3 (YTD 2014/15 reported up to Dec 14) is below the national level of 100 but is above the London average of 86.3. Trust weekday
and weekend HSMRs have fluctuated above and below the national benchmark throughout the year. The HSMR for weekdays is currently lower than the
national benchmark at 95.9 and the HSMR for weekends is above the national benchmark at 107.0. The trust is tracking the HSMR monthly and has a robust
mortality review process in place for all deaths occurring in hospital.
0.0%
1.0%
2.0%
3.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Crude Mortality Rate
2015/2016 2014/2015
0.0
50.0
100.0
150.0
200.0
250.0
HSMR (Basket of 56)
2014/2015 Benchmark 2014/2015
0.0
50.0
100.0
150.0
200.0
250.0
Weekday HSMR (Basket of 56)
2014/2015 Benchmark 2014/2015
0.0
50.0
100.0
150.0
200.0
250.0
Weekend HSMR (Basket of 56)
2014/2015 Benchmark 2014/2015
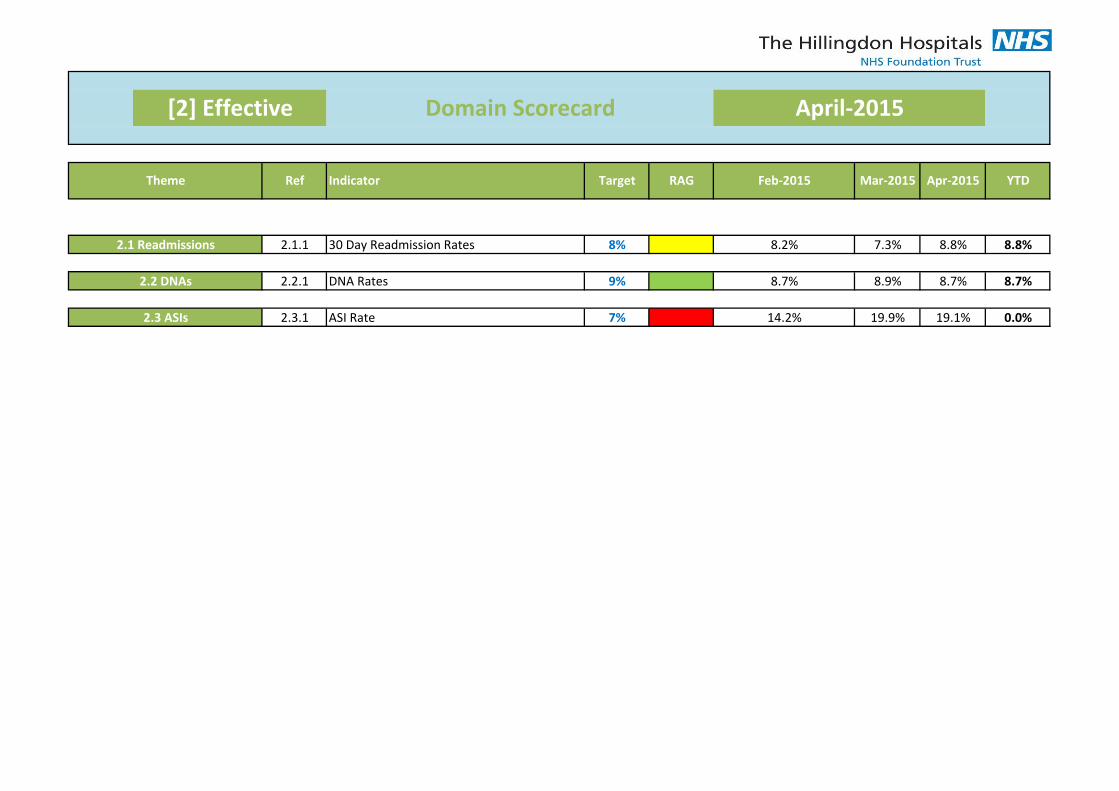
2.1.1 8% 8.2% 7.3% 8.8% 8.8%
2.2.1 9% 8.7% 8.9% 8.7% 8.7%
2.3.1 7% 14.2% 19.9% 19.1% 0.0%
YTDIndicator
2.2 DNAs
April-2015
Theme Ref Target RAG Feb-2015 Mar-2015 Apr-2015
ASI Rate
2.1 Readmissions 30 Day Readmission Rates
2.3 ASIs
[2] Effective Domain Scorecard
DNA Rates
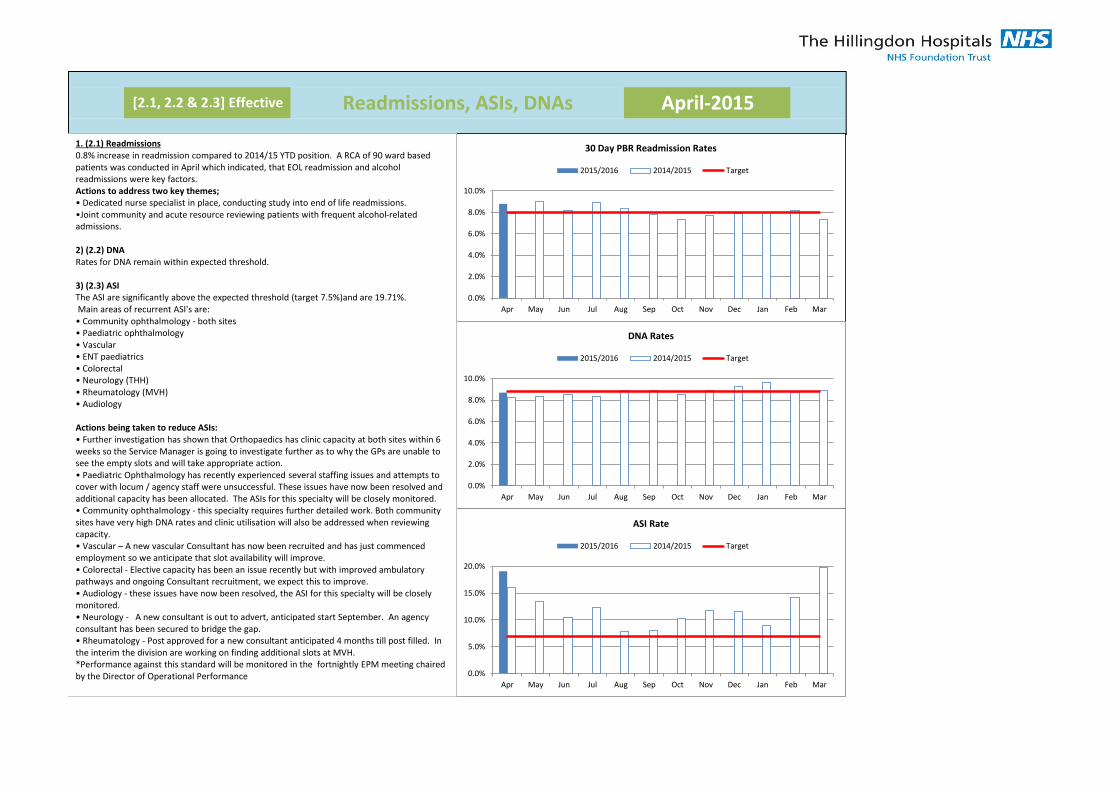
[2.1, 2.2 & 2.3] Effective April-2015Readmissions, ASIs, DNAs
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
30 Day PBR Readmission Rates
2015/2016 2014/2015 Target
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
DNA Rates
2015/2016 2014/2015 Target
0.0%
5.0%
10.0%
15.0%
20.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ASI Rate
2015/2016 2014/2015 Target
1. (2.1) Readmissions 0.8% increase in readmission compared to 2014/15 YTD position. A RCA of 90 ward based patients was conducted in April which indicated, that EOL readmission and alcohol readmissions were key factors. Actions to address two key themes; • Dedicated nurse specialist in place, conducting study into end of life readmissions. •Joint community and acute resource reviewing patients with frequent alcohol-related admissions. 2) (2.2) DNA Rates for DNA remain within expected threshold. 3) (2.3) ASI The ASI are significantly above the expected threshold (target 7.5%)and are 19.71%. Main areas of recurrent ASI's are: • Community ophthalmology - both sites • Paediatric ophthalmology • Vascular • ENT paediatrics • Colorectal • Neurology (THH) • Rheumatology (MVH) • Audiology Actions being taken to reduce ASIs: • Further investigation has shown that Orthopaedics has clinic capacity at both sites within 6 weeks so the Service Manager is going to investigate further as to why the GPs are unable to see the empty slots and will take appropriate action. • Paediatric Ophthalmology has recently experienced several staffing issues and attempts to cover with locum / agency staff were unsuccessful. These issues have now been resolved and additional capacity has been allocated. The ASIs for this specialty will be closely monitored. • Community ophthalmology - this specialty requires further detailed work. Both community sites have very high DNA rates and clinic utilisation will also be addressed when reviewing capacity. • Vascular – A new vascular Consultant has now been recruited and has just commenced employment so we anticipate that slot availability will improve. • Colorectal - Elective capacity has been an issue recently but with improved ambulatory pathways and ongoing Consultant recruitment, we expect this to improve. • Audiology - these issues have now been resolved, the ASI for this specialty will be closely monitored. • Neurology - A new consultant is out to advert, anticipated start September. An agency consultant has been secured to bridge the gap. • Rheumatology - Post approved for a new consultant anticipated 4 months till post filled. In the interim the division are working on finding additional slots at MVH. *Performance against this standard will be monitored in the fortnightly EPM meeting chaired by the Director of Operational Performance
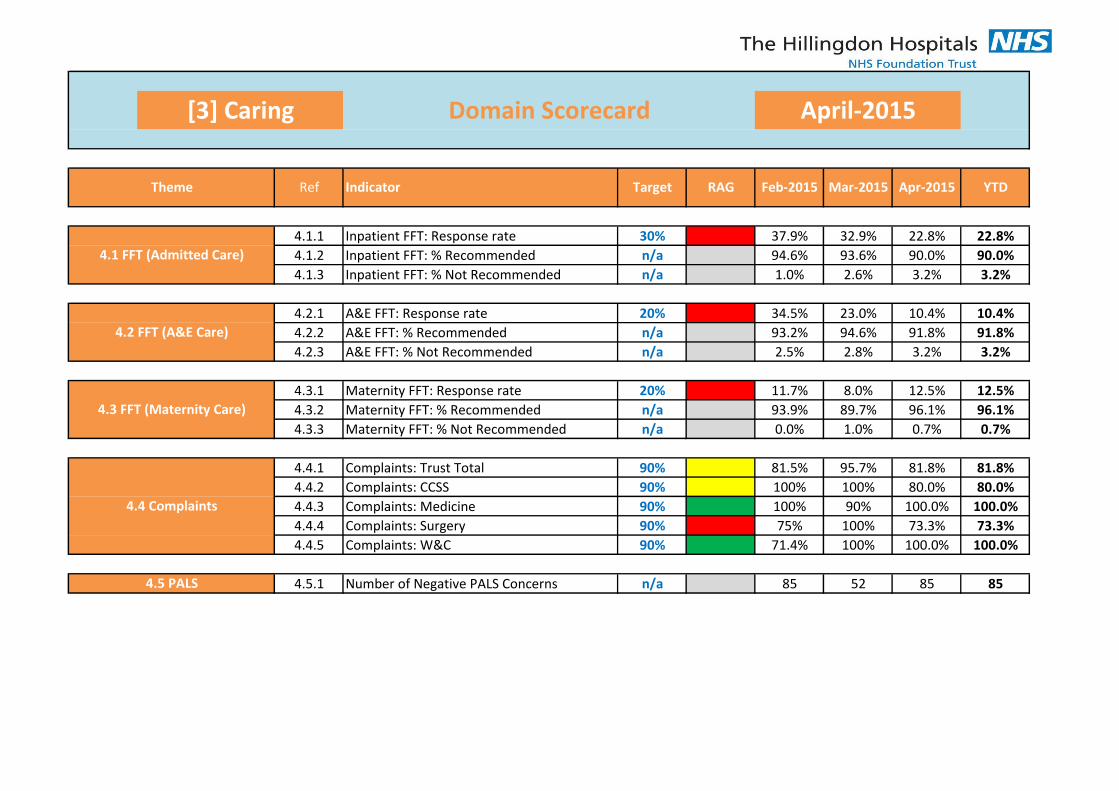
4.1.1 30% 37.9% 32.9% 22.8% 22.8%
4.1.2 n/a 94.6% 93.6% 90.0% 90.0%
4.1.3 n/a 1.0% 2.6% 3.2% 3.2%
4.2.1 20% 34.5% 23.0% 10.4% 10.4%
4.2.2 n/a 93.2% 94.6% 91.8% 91.8%
4.2.3 n/a 2.5% 2.8% 3.2% 3.2%
4.3.1 20% 11.7% 8.0% 12.5% 12.5%
4.3.2 n/a 93.9% 89.7% 96.1% 96.1%
4.3.3 n/a 0.0% 1.0% 0.7% 0.7%
4.4.1 90% 81.5% 95.7% 81.8% 81.8%
4.4.2 90% 100% 100% 80.0% 80.0%
4.4.3 90% 100% 90% 100.0% 100.0%
4.4.4 90% 75% 100% 73.3% 73.3%
4.4.5 90% 71.4% 100% 100.0% 100.0%
4.5.1 n/a 85 52 85 854.5 PALS Number of Negative PALS Concerns
4.4 Complaints
Complaints: Trust Total
Complaints: CCSS
Complaints: Medicine
Complaints: Surgery
Complaints: W&C
Inpatient FFT: Response rate
4.1 FFT (Admitted Care) Inpatient FFT: % Recommended
Inpatient FFT: % Not Recommended
4.2 FFT (A&E Care)
A&E FFT: Response rate
4.3 FFT (Maternity Care) Maternity FFT: % Recommended
A&E FFT: % Recommended
A&E FFT: % Not Recommended
Maternity FFT: Response rate
Maternity FFT: % Not Recommended
YTDIndicator Apr-2015
[3] Caring Domain Scorecard April-2015
Theme Ref Target RAG Feb-2015 Mar-2015
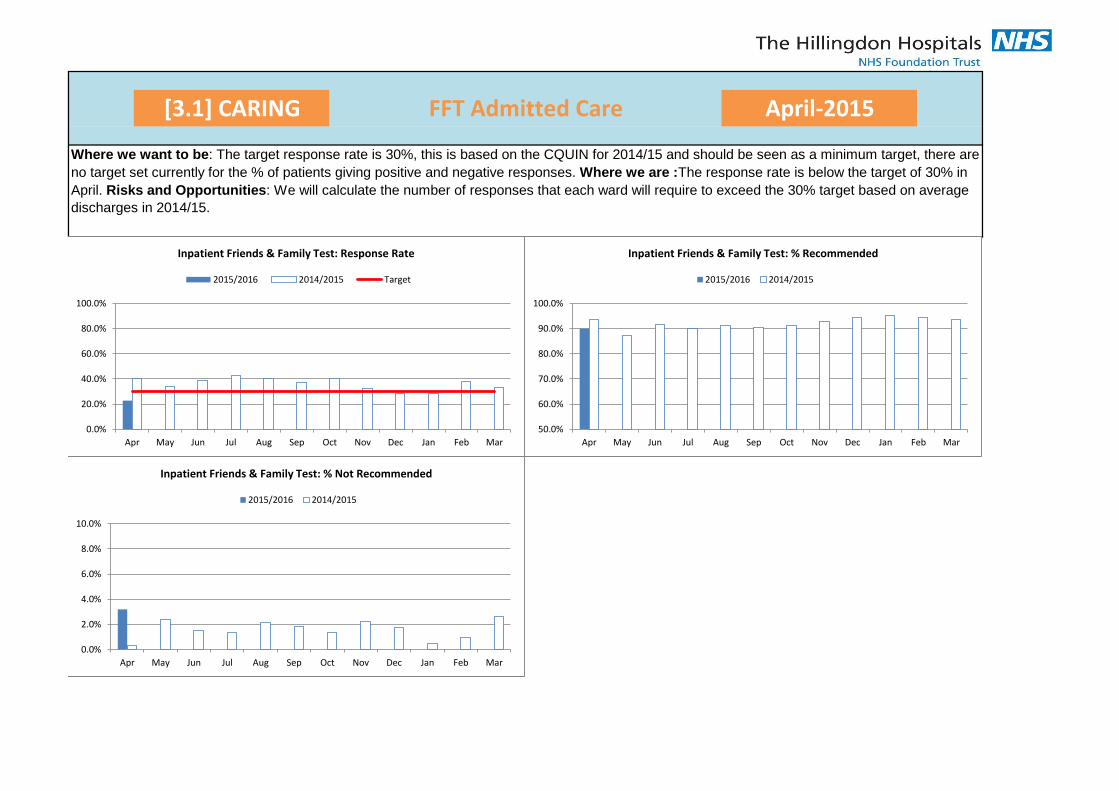
[3.1] CARING April-2015FFT Admitted Care
Where we want to be: The target response rate is 30%, this is based on the CQUIN for 2014/15 and should be seen as a minimum target, there are
no target set currently for the % of patients giving positive and negative responses. Where we are :The response rate is below the target of 30% in
April. Risks and Opportunities: We will calculate the number of responses that each ward will require to exceed the 30% target based on average
discharges in 2014/15.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Inpatient Friends & Family Test: Response Rate
2015/2016 2014/2015 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Inpatient Friends & Family Test: % Recommended
2015/2016 2014/2015
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Inpatient Friends & Family Test: % Not Recommended
2015/2016 2014/2015
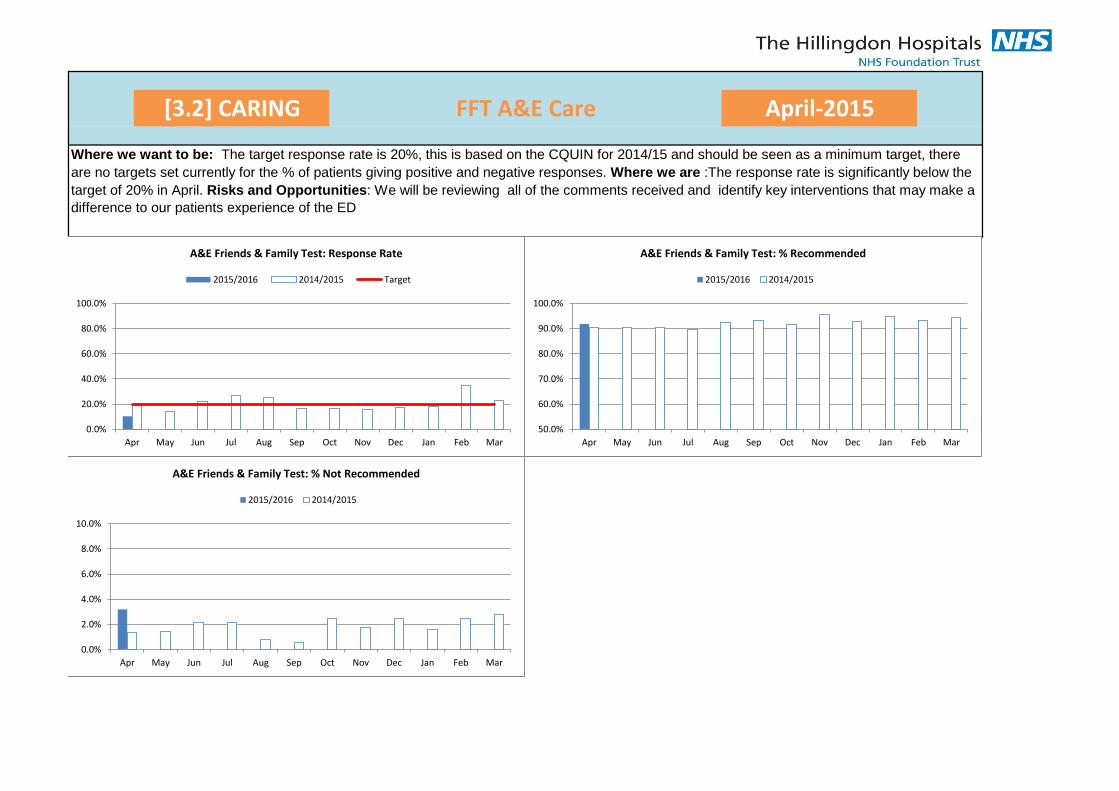
[3.2] CARING FFT A&E Care April-2015
Where we want to be: The target response rate is 20%, this is based on the CQUIN for 2014/15 and should be seen as a minimum target, there
are no targets set currently for the % of patients giving positive and negative responses. Where we are :The response rate is significantly below the
target of 20% in April. Risks and Opportunities: We will be reviewing all of the comments received and identify key interventions that may make a
difference to our patients experience of the ED
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Friends & Family Test: Response Rate
2015/2016 2014/2015 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Friends & Family Test: % Recommended
2015/2016 2014/2015
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Friends & Family Test: % Not Recommended
2015/2016 2014/2015
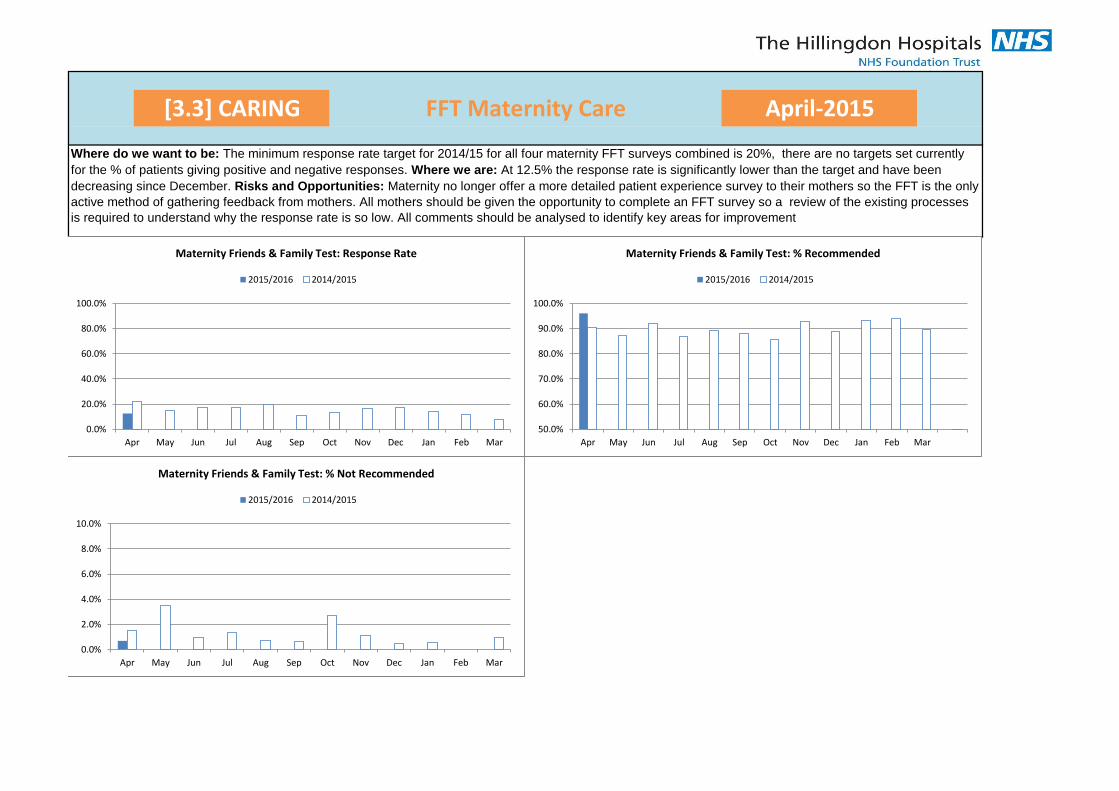
[3.3] CARING FFT Maternity Care April-2015
Where do we want to be: The minimum response rate target for 2014/15 for all four maternity FFT surveys combined is 20%, there are no targets set currently
for the % of patients giving positive and negative responses. Where we are: At 12.5% the response rate is significantly lower than the target and have been
decreasing since December. Risks and Opportunities: Maternity no longer offer a more detailed patient experience survey to their mothers so the FFT is the only
active method of gathering feedback from mothers. All mothers should be given the opportunity to complete an FFT survey so a review of the existing processes
is required to understand why the response rate is so low. All comments should be analysed to identify key areas for improvement
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Maternity Friends & Family Test: Response Rate
2015/2016 2014/2015
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Maternity Friends & Family Test: % Recommended
2015/2016 2014/2015
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Maternity Friends & Family Test: % Not Recommended
2015/2016 2014/2015
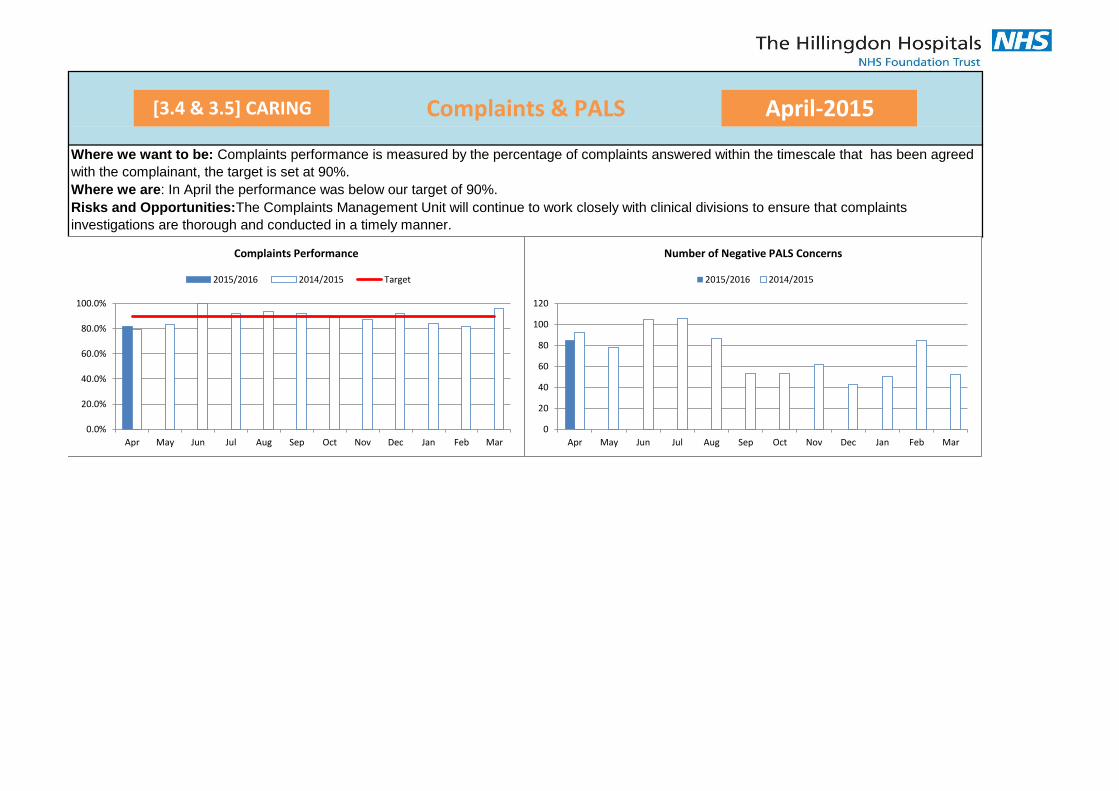
[3.4 & 3.5] CARING Complaints & PALS April-2015
Where we want to be: Complaints performance is measured by the percentage of complaints answered within the timescale that has been agreed
with the complainant, the target is set at 90%.
Where we are: In April the performance was below our target of 90%.
Risks and Opportunities:The Complaints Management Unit will continue to work closely with clinical divisions to ensure that complaints
investigations are thorough and conducted in a timely manner.
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Complaints Performance
2015/2016 2014/2015 Target
0
20
40
60
80
100
120
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Negative PALS Concerns
2015/2016 2014/2015
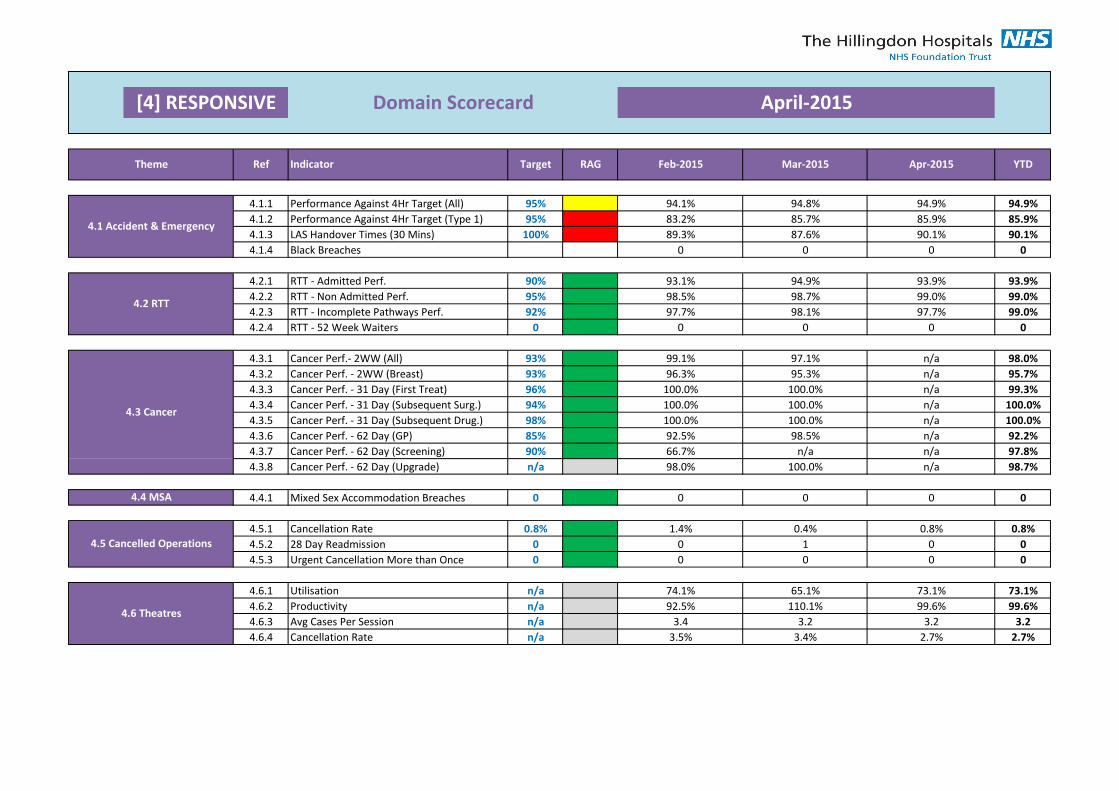
4.1.1 95% 94.1% 94.8% 94.9% 94.9%
4.1.2 95% 83.2% 85.7% 85.9% 85.9%
4.1.3 100% 89.3% 87.6% 90.1% 90.1%
4.1.4 0 0 0 0
4.2.1 90% 93.1% 94.9% 93.9% 93.9%
4.2.2 95% 98.5% 98.7% 99.0% 99.0%
4.2.3 92% 97.7% 98.1% 97.7% 99.0%
4.2.4 0 0 0 0 0
4.3.1 93% 99.1% 97.1% n/a 98.0%
4.3.2 93% 96.3% 95.3% n/a 95.7%
4.3.3 96% 100.0% 100.0% n/a 99.3%
4.3.4 94% 100.0% 100.0% n/a 100.0%
4.3.5 98% 100.0% 100.0% n/a 100.0%
4.3.6 85% 92.5% 98.5% n/a 92.2%
4.3.7 90% 66.7% n/a n/a 97.8%
4.3.8 n/a 98.0% 100.0% n/a 98.7%
4.4.1 0 0 0 0 0
4.5.1 0.8% 1.4% 0.4% 0.8% 0.8%
4.5.2 0 0 1 0 0
4.5.3 0 0 0 0 0
4.6.1 n/a 74.1% 65.1% 73.1% 73.1%
4.6.2 n/a 92.5% 110.1% 99.6% 99.6%
4.6.3 n/a 3.4 3.2 3.2 3.2
4.6.4 n/a 3.5% 3.4% 2.7% 2.7%
4.6 Theatres
Utilisation
Productivity
Avg Cases Per Session
Cancellation Rate
4.5 Cancelled Operations
Cancellation Rate
28 Day Readmission
Urgent Cancellation More than Once
Cancer Perf. - 31 Day (First Treat)
4.4 MSA Mixed Sex Accommodation Breaches
Cancer Perf. - 62 Day (Screening)
4.3 Cancer
Cancer Perf. - 62 Day (Upgrade)
Cancer Perf. - 31 Day (Subsequent Surg.)
Cancer Perf. - 31 Day (Subsequent Drug.)
Cancer Perf. - 62 Day (GP)
YTDIndicator
Performance Against 4Hr Target (All)
Performance Against 4Hr Target (Type 1)
LAS Handover Times (30 Mins)
Apr-2015
April-2015
Theme Ref Target RAG Feb-2015 Mar-2015
[4] RESPONSIVE Domain Scorecard
4.1 Accident & Emergency
Cancer Perf.- 2WW (All)
Cancer Perf. - 2WW (Breast)
4.2 RTTRTT - Incomplete Pathways Perf.
RTT - Admitted Perf.
RTT - Non Admitted Perf.
RTT - 52 Week Waiters
Black Breaches
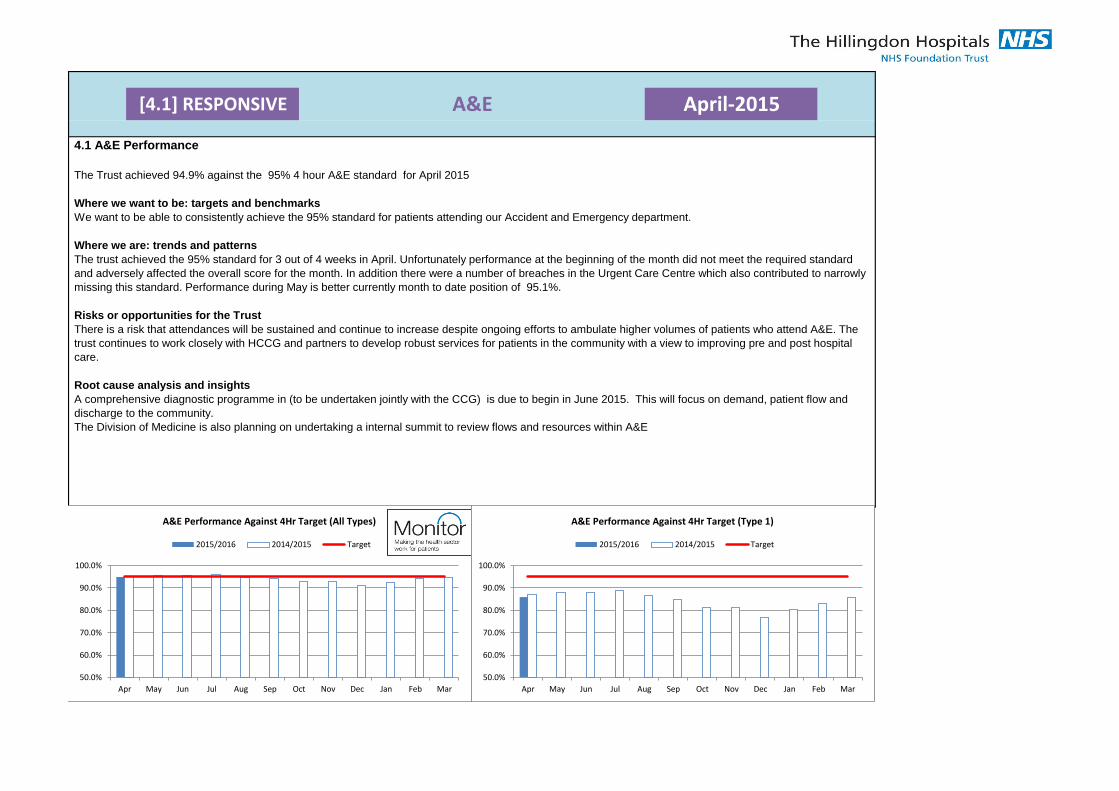
[4.1] RESPONSIVE April-2015A&E
4.1 A&E Performance
The Trust achieved 94.9% against the 95% 4 hour A&E standard for April 2015
Where we want to be: targets and benchmarks
We want to be able to consistently achieve the 95% standard for patients attending our Accident and Emergency department.
Where we are: trends and patterns
The trust achieved the 95% standard for 3 out of 4 weeks in April. Unfortunately performance at the beginning of the month did not meet the required standard
and adversely affected the overall score for the month. In addition there were a number of breaches in the Urgent Care Centre which also contributed to narrowly
missing this standard. Performance during May is better currently month to date position of 95.1%.
Risks or opportunities for the Trust
There is a risk that attendances will be sustained and continue to increase despite ongoing efforts to ambulate higher volumes of patients who attend A&E. The
trust continues to work closely with HCCG and partners to develop robust services for patients in the community with a view to improving pre and post hospital
care.
Root cause analysis and insights
A comprehensive diagnostic programme in (to be undertaken jointly with the CCG) is due to begin in June 2015. This will focus on demand, patient flow and
discharge to the community.
The Division of Medicine is also planning on undertaking a internal summit to review flows and resources within A&E
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Performance Against 4Hr Target (All Types)
2015/2016 2014/2015 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E Performance Against 4Hr Target (Type 1)
2015/2016 2014/2015 Target
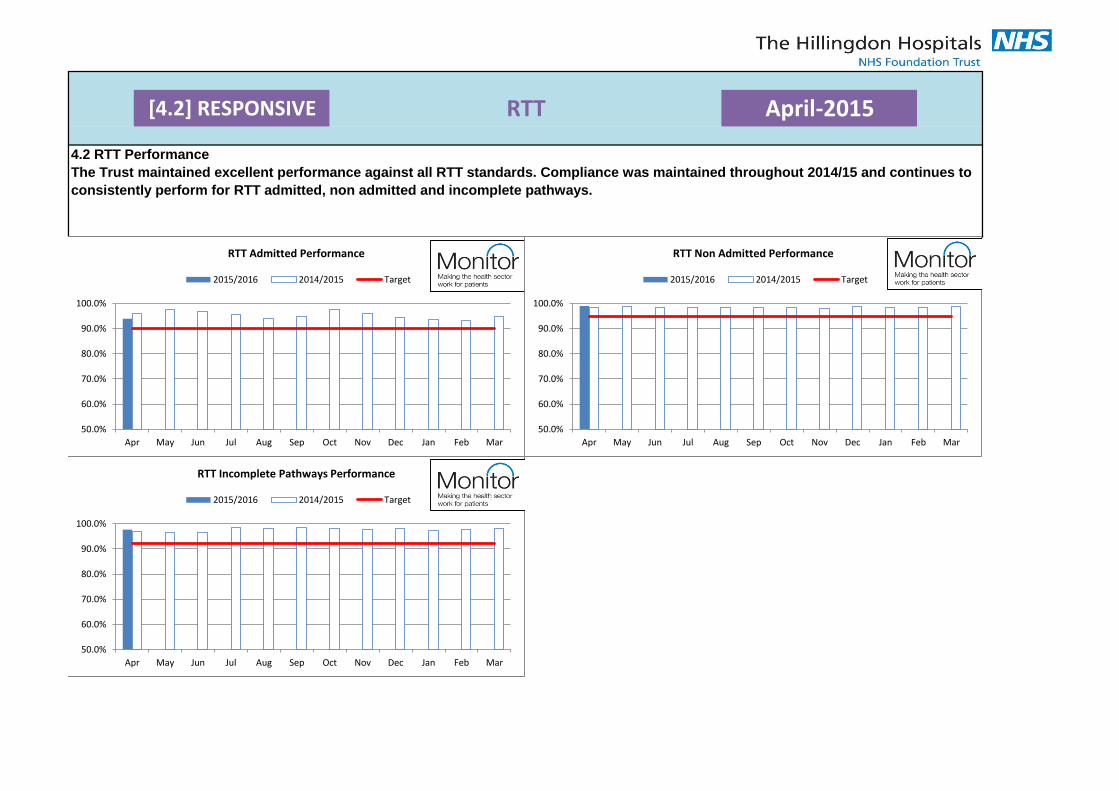
[4.2] RESPONSIVE RTT April-2015
4.2 RTT Performance
The Trust maintained excellent performance against all RTT standards. Compliance was maintained throughout 2014/15 and continues to
consistently perform for RTT admitted, non admitted and incomplete pathways.
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
RTT Admitted Performance
2015/2016 2014/2015 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
RTT Non Admitted Performance
2015/2016 2014/2015 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
RTT Incomplete Pathways Performance
2015/2016 2014/2015 Target
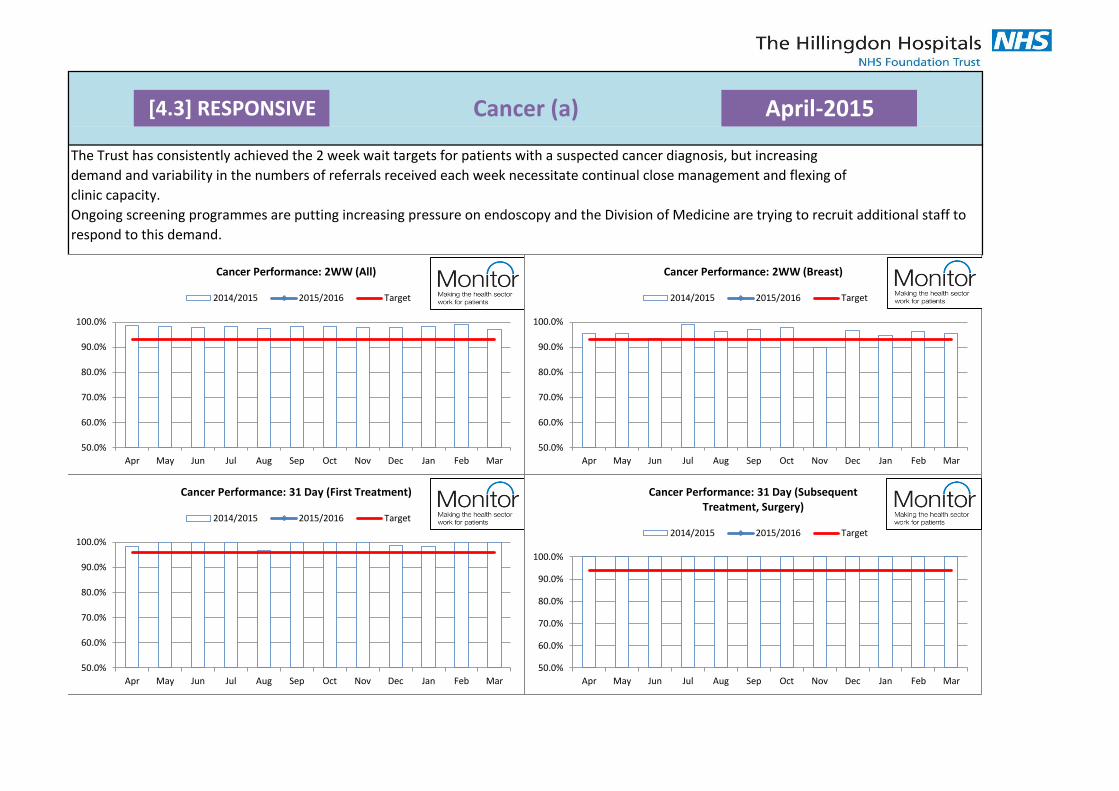
[4.3] RESPONSIVE Cancer (a) April-2015
The Trust has consistently achieved the 2 week wait targets for patients with a suspected cancer diagnosis, but increasing
demand and variability in the numbers of referrals received each week necessitate continual close management and flexing of
clinic capacity.
Ongoing screening programmes are putting increasing pressure on endoscopy and the Division of Medicine are trying to recruit additional staff to
respond to this demand.
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer Performance: 2WW (All)
2014/2015 2015/2016 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer Performance: 2WW (Breast)
2014/2015 2015/2016 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer Performance: 31 Day (First Treatment)
2014/2015 2015/2016 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer Performance: 31 Day (Subsequent Treatment, Surgery)
2014/2015 2015/2016 Target
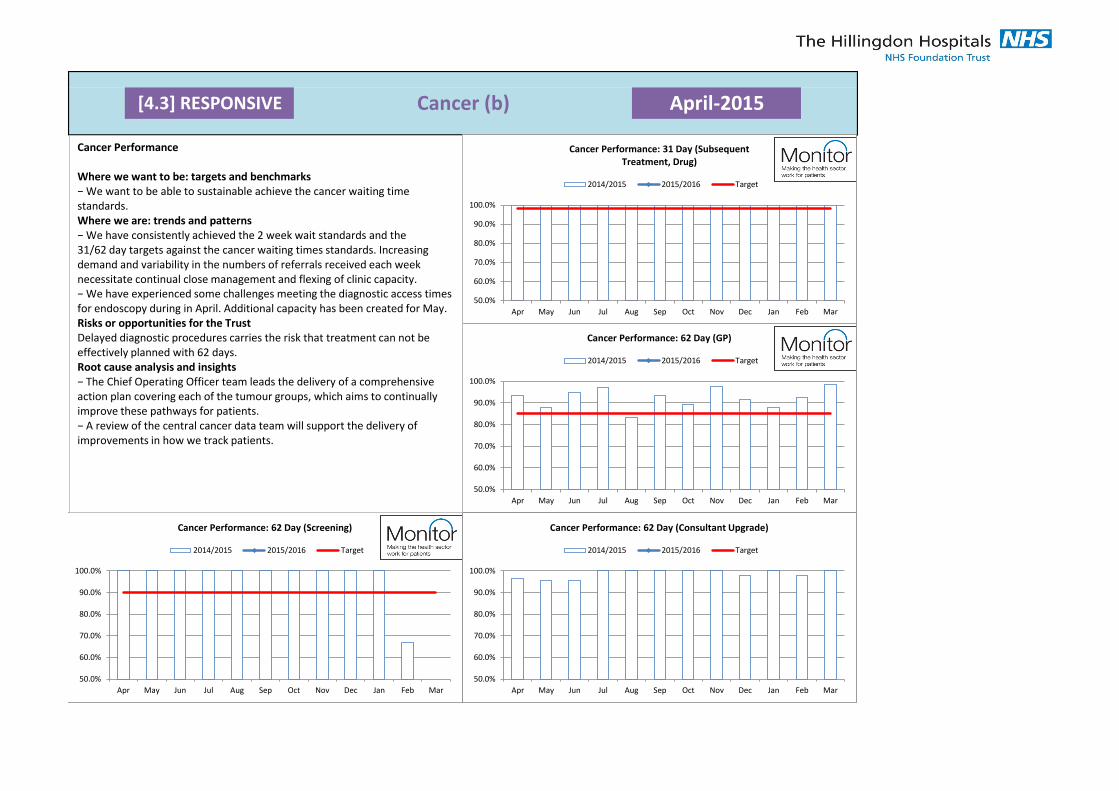
[4.3] RESPONSIVE Cancer (b) April-2015
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer Performance: 31 Day (Subsequent Treatment, Drug)
2014/2015 2015/2016 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer Performance: 62 Day (GP)
2014/2015 2015/2016 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer Performance: 62 Day (Screening)
2014/2015 2015/2016 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancer Performance: 62 Day (Consultant Upgrade)
2014/2015 2015/2016 Target
Cancer Performance
Where we want to be: targets and benchmarks − We want to be able to sustainable achieve the cancer waiting time standards. Where we are: trends and patterns − We have consistently achieved the 2 week wait standards and the 31/62 day targets against the cancer waiting times standards. Increasing demand and variability in the numbers of referrals received each week necessitate continual close management and flexing of clinic capacity. − We have experienced some challenges meeting the diagnostic access times for endoscopy during in April. Additional capacity has been created for May. Risks or opportunities for the Trust Delayed diagnostic procedures carries the risk that treatment can not be effectively planned with 62 days. Root cause analysis and insights − The Chief Operating Officer team leads the delivery of a comprehensive action plan covering each of the tumour groups, which aims to continually improve these pathways for patients. − A review of the central cancer data team will support the delivery of improvements in how we track patients.
[4.4] RESPONSIVE MSA April-2015
0
1
2
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Mixed Sex Accommodation Breaches
2015/2016 2014/2015 Target
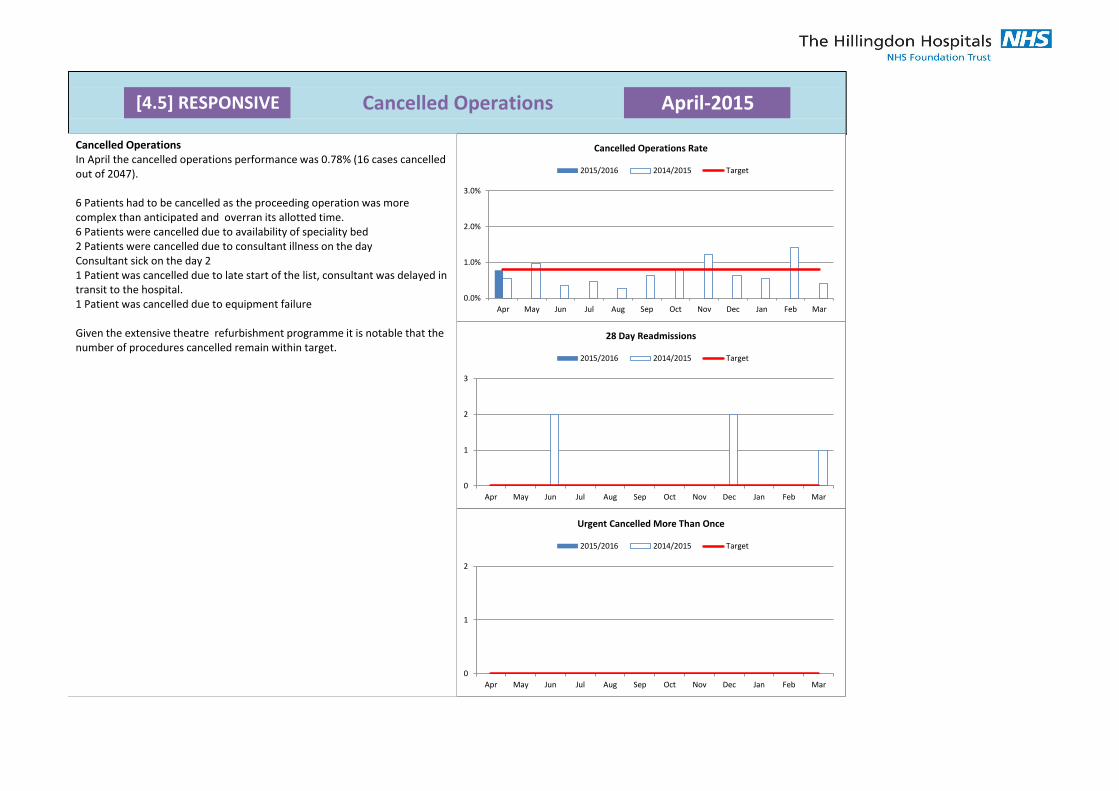
[4.5] RESPONSIVE Cancelled Operations April-2015
0.0%
1.0%
2.0%
3.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancelled Operations Rate
2015/2016 2014/2015 Target
0
1
2
3
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
28 Day Readmissions
2015/2016 2014/2015 Target
0
1
2
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Urgent Cancelled More Than Once
2015/2016 2014/2015 Target
Cancelled Operations In April the cancelled operations performance was 0.78% (16 cases cancelled out of 2047).
6 Patients had to be cancelled as the proceeding operation was more complex than anticipated and overran its allotted time. 6 Patients were cancelled due to availability of speciality bed 2 Patients were cancelled due to consultant illness on the day Consultant sick on the day 2 1 Patient was cancelled due to late start of the list, consultant was delayed in transit to the hospital. 1 Patient was cancelled due to equipment failure
Given the extensive theatre refurbishment programme it is notable that the number of procedures cancelled remain within target.
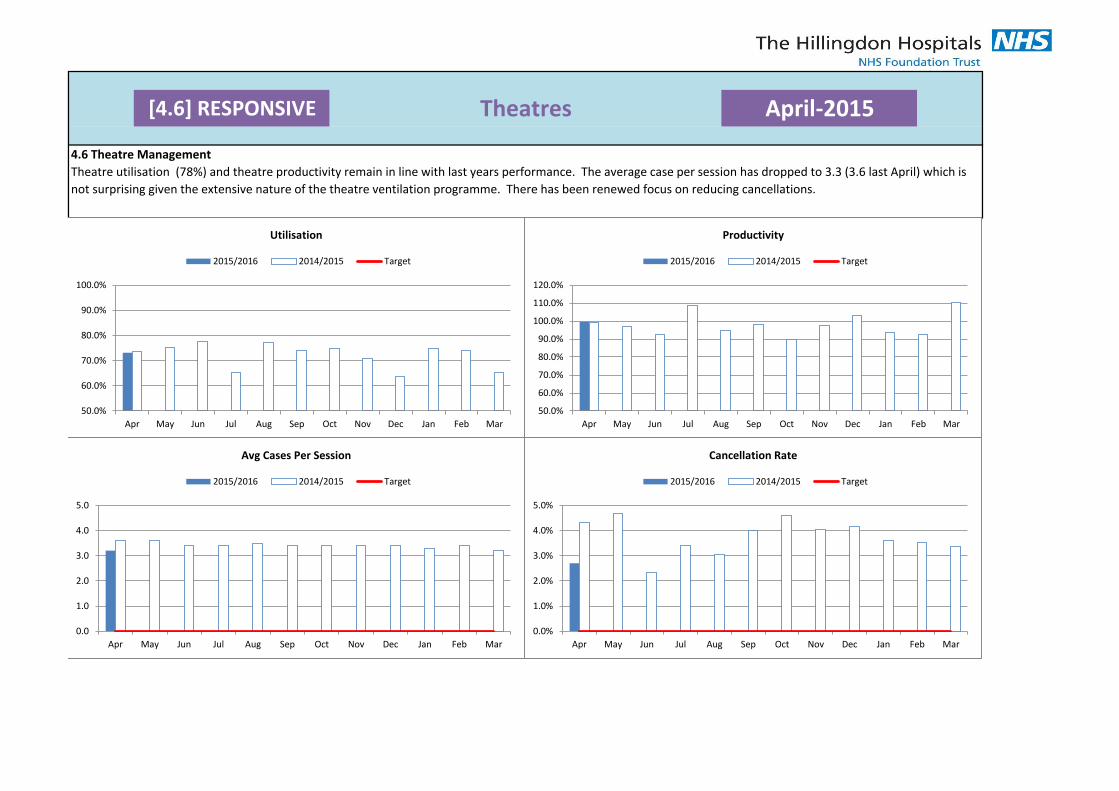
[4.6] RESPONSIVE Theatres April-2015
4.6 Theatre Management
Theatre utilisation (78%) and theatre productivity remain in line with last years performance. The average case per session has dropped to 3.3 (3.6 last April) which is
not surprising given the extensive nature of the theatre ventilation programme. There has been renewed focus on reducing cancellations.
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Utilisation
2015/2016 2014/2015 Target
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
110.0%
120.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Productivity
2015/2016 2014/2015 Target
0.0
1.0
2.0
3.0
4.0
5.0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Avg Cases Per Session
2015/2016 2014/2015 Target
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Cancellation Rate
2015/2016 2014/2015 Target
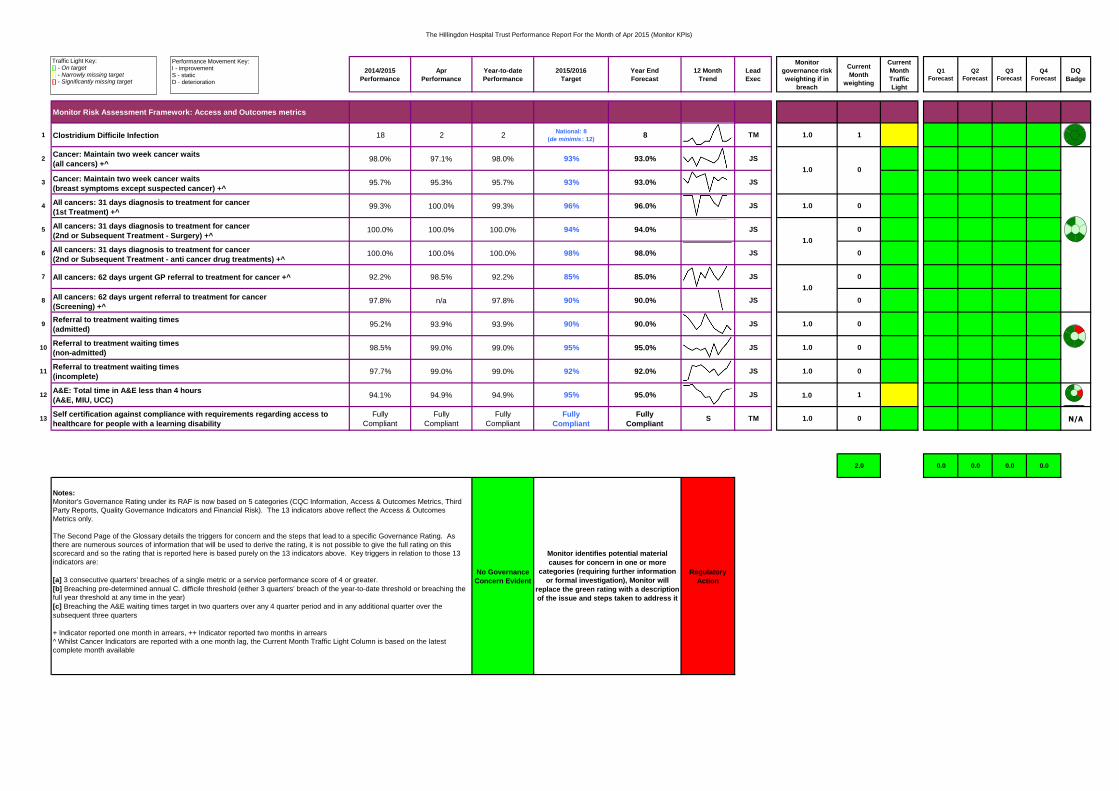
The Hillingdon Hospital Trust Performance Report For the Month of Apr 2015 (Monitor KPIs)
2014/2015
Performance
Apr
Performance
Year-to-date
Performance
2015/2016
Target
Year End
Forecast
12 Month
Trend
Lead
Exec
Monitor
governance risk
weighting if in
breach
Current
Month
weighting
Current
Month
Traffic
Light
Q1
Forecast
Q2
Forecast
Q3
Forecast
Q4
Forecast
DQ
Badge
Monitor Risk Assessment Framework: Access and Outcomes metrics
1 Clostridium Difficile Infection 18 2 2National: 8
(de minimis : 12)8 TM 1.0 1
2Cancer: Maintain two week cancer waits
(all cancers) +^98.0% 97.1% 98.0% 93% 93.0% JS
3 Cancer: Maintain two week cancer waits
(breast symptoms except suspected cancer) +^95.7% 95.3% 95.7% 93% 93.0% JS
4 All cancers: 31 days diagnosis to treatment for cancer
(1st Treatment) +^99.3% 100.0% 99.3% 96% 96.0% JS 1.0 0
5 All cancers: 31 days diagnosis to treatment for cancer
(2nd or Subsequent Treatment - Surgery) +^100.0% 100.0% 100.0% 94% 94.0% JS 0
6 All cancers: 31 days diagnosis to treatment for cancer
(2nd or Subsequent Treatment - anti cancer drug treatments) +^100.0% 100.0% 100.0% 98% 98.0% JS 0
7 All cancers: 62 days urgent GP referral to treatment for cancer +^ 92.2% 98.5% 92.2% 85% 85.0% JS 0
8 All cancers: 62 days urgent referral to treatment for cancer
(Screening) +^97.8% n/a 97.8% 90% 90.0% JS 0
9Referral to treatment waiting times
(admitted)95.2% 93.9% 93.9% 90% 90.0% JS 1.0 0
10Referral to treatment waiting times
(non-admitted)98.5% 99.0% 99.0% 95% 95.0% JS 1.0 0
11Referral to treatment waiting times
(incomplete)97.7% 99.0% 99.0% 92% 92.0% JS 1.0 0
12A&E: Total time in A&E less than 4 hours
(A&E, MIU, UCC)94.1% 94.9% 94.9% 95% 95.0% JS 1.0 1
13Self certification against compliance with requirements regarding access to
healthcare for people with a learning disability
Fully
Compliant
Fully
Compliant
Fully
Compliant
Fully
Compliant
Fully
CompliantS TM 1.0 0 N/A
2.0 0.0 0.0 0.0 0.0
No Governance
Concern Evident
Regulatory
Action
Notes:
Monitor's Governance Rating under its RAF is now based on 5 categories (CQC Information, Access & Outcomes Metrics, Third
Party Reports, Quality Governance Indicators and Financial Risk). The 13 indicators above reflect the Access & Outcomes
Metrics only.
The Second Page of the Glossary details the triggers for concern and the steps that lead to a specific Governance Rating. As
there are numerous sources of information that will be used to derive the rating, it is not possible to give the full rating on this
scorecard and so the rating that is reported here is based purely on the 13 indicators above. Key triggers in relation to those 13
indicators are:
[a] 3 consecutive quarters' breaches of a single metric or a service performance score of 4 or greater.
[b] Breaching pre-determined annual C. difficile threshold (either 3 quarters' breach of the year-to-date threshold or breaching the
full year threshold at any time in the year)
[c] Breaching the A&E waiting times target in two quarters over any 4 quarter period and in any additional quarter over the
subsequent three quarters
+ Indicator reported one month in arrears, ++ Indicator reported two months in arrears
Whilst Cancer Indicators are reported with a one month lag, the Current Month Traffic Light Column is based on the latest
complete month available
Monitor identifies potential material
causes for concern in one or more
categories (requiring further information
or formal investigation), Monitor will
replace the green rating with a description
of the issue and steps taken to address it
1.0
1.0 0
1.0
Traffic Light Key: [] - On target [] - Narrowly missing target [] - Significantly missing target
Performance Movement Key: I - improvement S - static D - deterioration
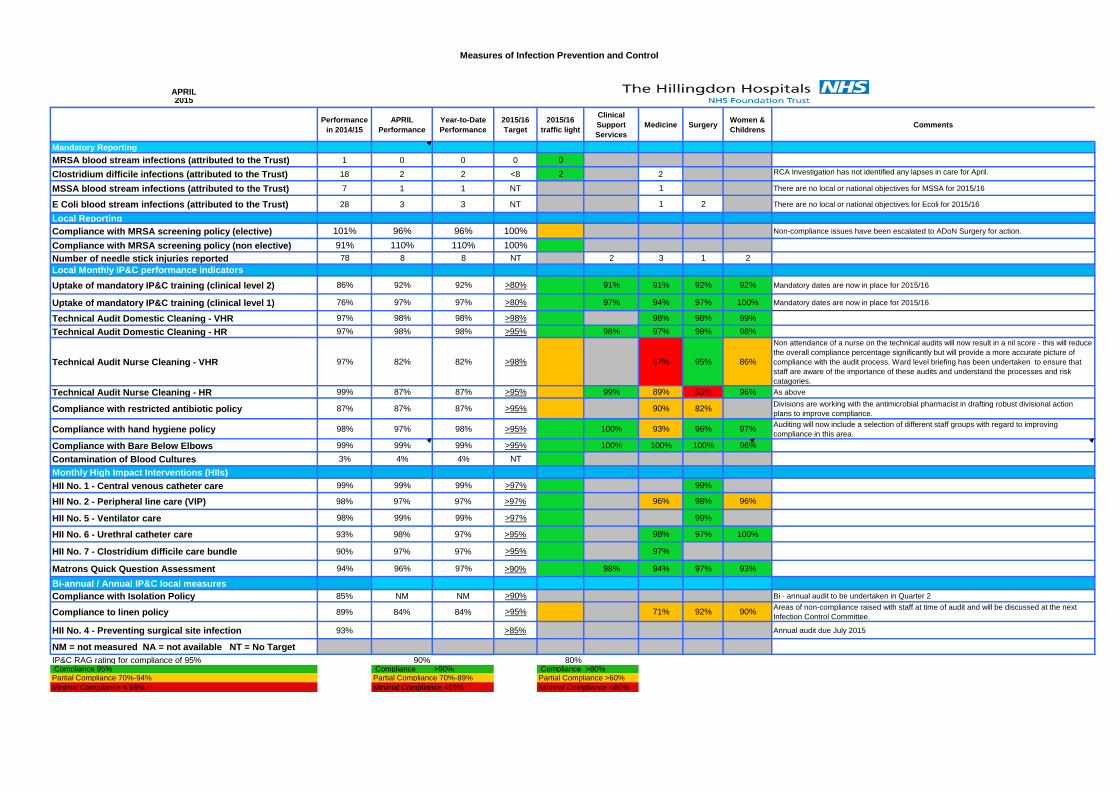
Measures of Infection Prevention and Control
APRIL2015
Performance in 2014/15
APRIL Performance
Year-to-Date Performance
2015/16Target
2015/16 traffic light
Clinical Support Services
Medicine Surgery Women & Childrens Comments
Mandatory ReportingMRSA blood stream infections (attributed to the Trust) 1 0 0 0 0
Clostridium difficile infections (attributed to the Trust) 18 2 2 <8 2 2 RCA Investigation has not identified any lapses in care for April.
MSSA blood stream infections (attributed to the Trust) 7 1 1 NT 1 There are no local or national objectives for MSSA for 2015/16
E Coli blood stream infections (attributed to the Trust) 28 3 3 NT 1 2 There are no local or national objectives for Ecoli for 2015/16
Local ReportingCompliance with MRSA screening policy (elective) 101% 96% 96% 100% Non-compliance issues have been escalated to ADoN Surgery for action.
Compliance with MRSA screening policy (non elective) 91% 110% 110% 100%Number of needle stick injuries reported 78 8 8 NT 2 3 1 2Local Monthly IP&C performance indicatorsUptake of mandatory IP&C training (clinical level 2) 86% 92% 92% >80% 91% 91% 92% 92% Mandatory dates are now in place for 2015/16
Uptake of mandatory IP&C training (clinical level 1) 76% 97% 97% >80% 97% 94% 97% 100% Mandatory dates are now in place for 2015/16
Technical Audit Domestic Cleaning - VHR 97% 98% 98% >98% 98% 98% 99%
Technical Audit Domestic Cleaning - HR 97% 98% 98% >95% 98% 97% 98% 98%
Technical Audit Nurse Cleaning - VHR 97% 82% 82% >98% 67% 95% 86%
Non attendance of a nurse on the technical audits will now result in a nil score - this will reduce the overall compliance percentage significantly but will provide a more accurate picture of compliance with the audit process. Ward level briefing has been undertaken to ensure that staff are aware of the importance of these audits and understand the processes and risk catagories.
Technical Audit Nurse Cleaning - HR 99% 87% 87% >95% 99% 89% 63% 96% As above
Compliance with restricted antibiotic policy 87% 87% 87% >95% 90% 82% Divisions are working with the antimicrobial pharmacist in drafting robust divisional action plans to improve compliance.
Compliance with hand hygiene policy 98% 97% 98% >95% 100% 93% 96% 97% Auditing will now include a selection of different staff groups with regard to improving compliance in this area.
Compliance with Bare Below Elbows 99% 99% 99% >95% 100% 100% 100% 96%
Contamination of Blood Cultures 3% 4% 4% NTMonthly High Impact Interventions (HIIs)HII No. 1 - Central venous catheter care 99% 99% 99% >97% 99%
HII No. 2 - Peripheral line care (VIP) 98% 97% 97% >97% 96% 98% 96%
HII No. 5 - Ventilator care 98% 99% 99% >97% 99%
HII No. 6 - Urethral catheter care 93% 98% 97% >95% 98% 97% 100%
HII No. 7 - Clostridium difficile care bundle 90% 97% 97% >95% 97%
Matrons Quick Question Assessment 94% 96% 97% >90% 98% 94% 97% 93%
Bi-annual / Annual IP&C local measuresCompliance with Isolation Policy 85% NM NM >90% Bi - annual audit to be undertaken in Quarter 2
Compliance to linen policy 89% 84% 84% >95% 71% 92% 90% Areas of non-compliance raised with staff at time of audit and will be discussed at the next Infection Control Committee.
HII No. 4 - Preventing surgical site infection 93% >85% Annual audit due July 2015
NM = not measured NA = not available NT = No Target IP&C RAG rating for compliance of 95% 90% 80% Compliance 95% Compliance >90% Compliance >80%Partial Compliance 70%-94% Partial Compliance 70%-89%Minimal Compliance < 69% Minimal Compliance <69%
Partial Compliance >60%Minimal Compliance <60%
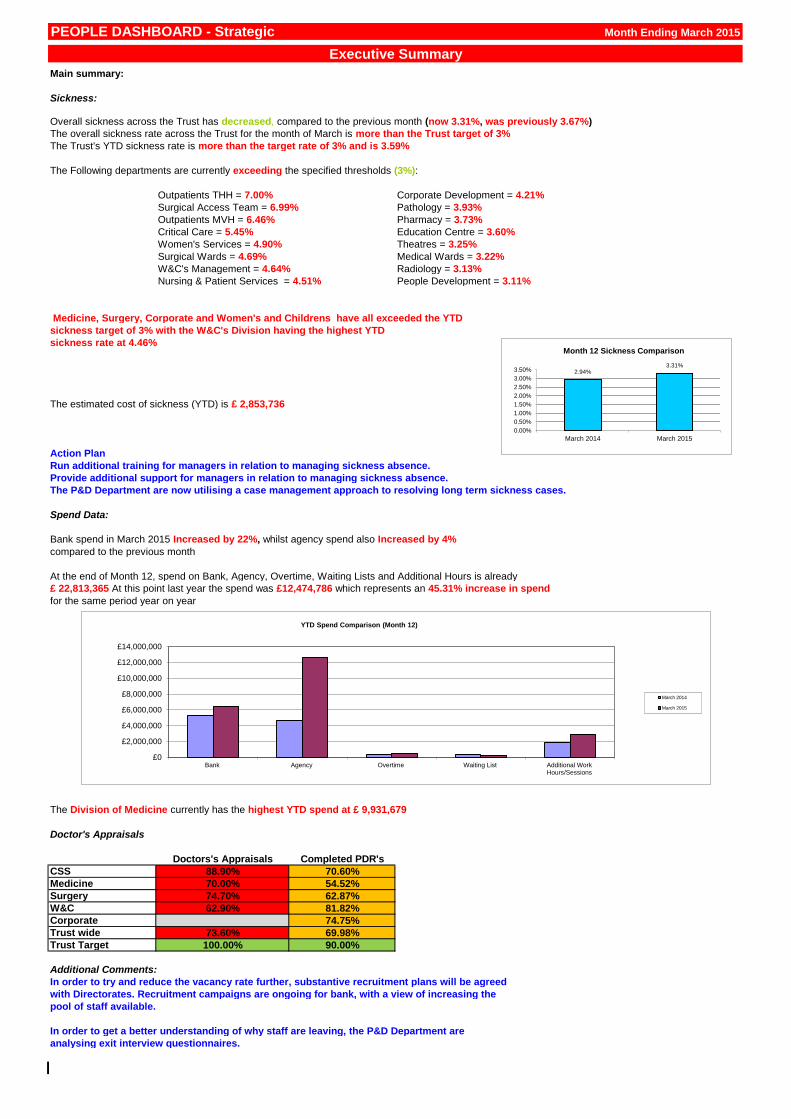
PEOPLE DASHBOARD - Strategic
Main summary:
Sickness:
The overall sickness rate across the Trust for the month of March is more than the Trust target of 3%
The Trust's YTD sickness rate is more than the target rate of 3% and is 3.59%
The Following departments are currently exceeding the specified thresholds (3%):
Outpatients THH = 7.00% Corporate Development = 4.21%
Surgical Access Team = 6.99% Pathology = 3.93%
Outpatients MVH = 6.46% Pharmacy = 3.73%
Critical Care = 5.45% Education Centre = 3.60%
Women's Services = 4.90% Theatres = 3.25%
Surgical Wards = 4.69% Medical Wards = 3.22%
W&C's Management = 4.64% Radiology = 3.13%
Nursing & Patient Services = 4.51% People Development = 3.11%
Medicine, Surgery, Corporate and Women's and Childrens have all exceeded the YTD
sickness target of 3% with the W&C's Division having the highest YTD
sickness rate at 4.46%
The estimated cost of sickness (YTD) is £ 2,853,736
Action Plan
Run additional training for managers in relation to managing sickness absence.
Provide additional support for managers in relation to managing sickness absence.
Spend Data:
Bank spend in March 2015 Increased by 22%, whilst agency spend also Increased by 4%
compared to the previous month
At the end of Month 12, spend on Bank, Agency, Overtime, Waiting Lists and Additional Hours is already
£ 22,813,365 At this point last year the spend was £12,474,786 which represents an 45.31% increase in spend
for the same period year on year
The Division of Medicine currently has the highest YTD spend at £ 9,931,679
Doctor's Appraisals
Doctors's Appraisals Completed PDR's
CSS 88.90% 70.60%
Medicine 70.00% 54.52%
Surgery 74.70% 62.87%
W&C 62.90% 81.82%
Corporate 74.75%
Trust wide 73.60% 69.98%
Trust Target 100.00% 90.00%
Additional Comments:
In order to try and reduce the vacancy rate further, substantive recruitment plans will be agreed
with Directorates. Recruitment campaigns are ongoing for bank, with a view of increasing the
pool of staff available.
In order to get a better understanding of why staff are leaving, the P&D Department are
analysing exit interview questionnaires.
Month Ending March 2015
Executive Summary
The P&D Department are now utilising a case management approach to resolving long term sickness cases.
Overall sickness across the Trust has decreased, compared to the previous month (now 3.31%, was previously 3.67%)
2.94% 3.31%
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
March 2014 March 2015
Month 12 Sickness Comparison
£0
£2,000,000
£4,000,000
£6,000,000
£8,000,000
£10,000,000
£12,000,000
£14,000,000
Bank Agency Overtime Waiting List Additional WorkHours/Sessions
YTD Spend Comparison (Month 12)
March 2014
March 2015
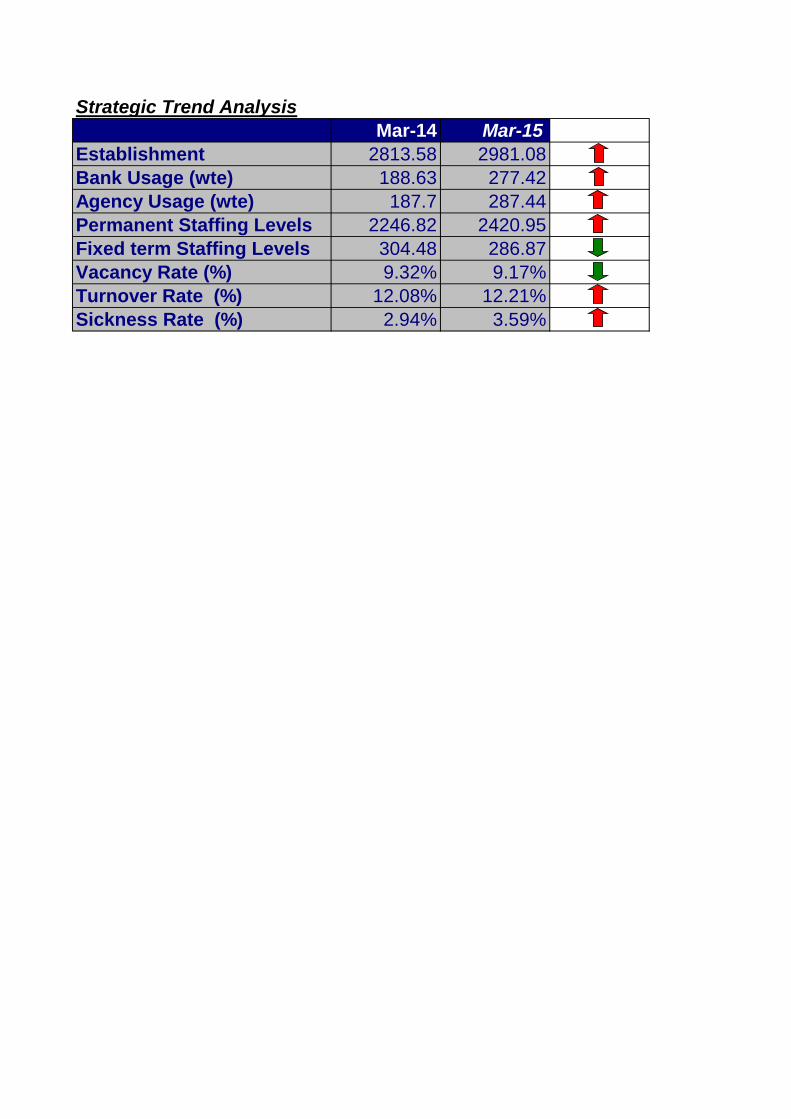
Strategic Trend Analysis
Mar-14 Mar-15
Establishment 2813.58 2981.08
Bank Usage (wte) 188.63 277.42
Agency Usage (wte) 187.7 287.44
Permanent Staffing Levels 2246.82 2420.95
Fixed term Staffing Levels 304.48 286.87
Vacancy Rate (%) 9.32% 9.17%
Turnover Rate (%) 12.08% 12.21%
Sickness Rate (%) 2.94% 3.59%
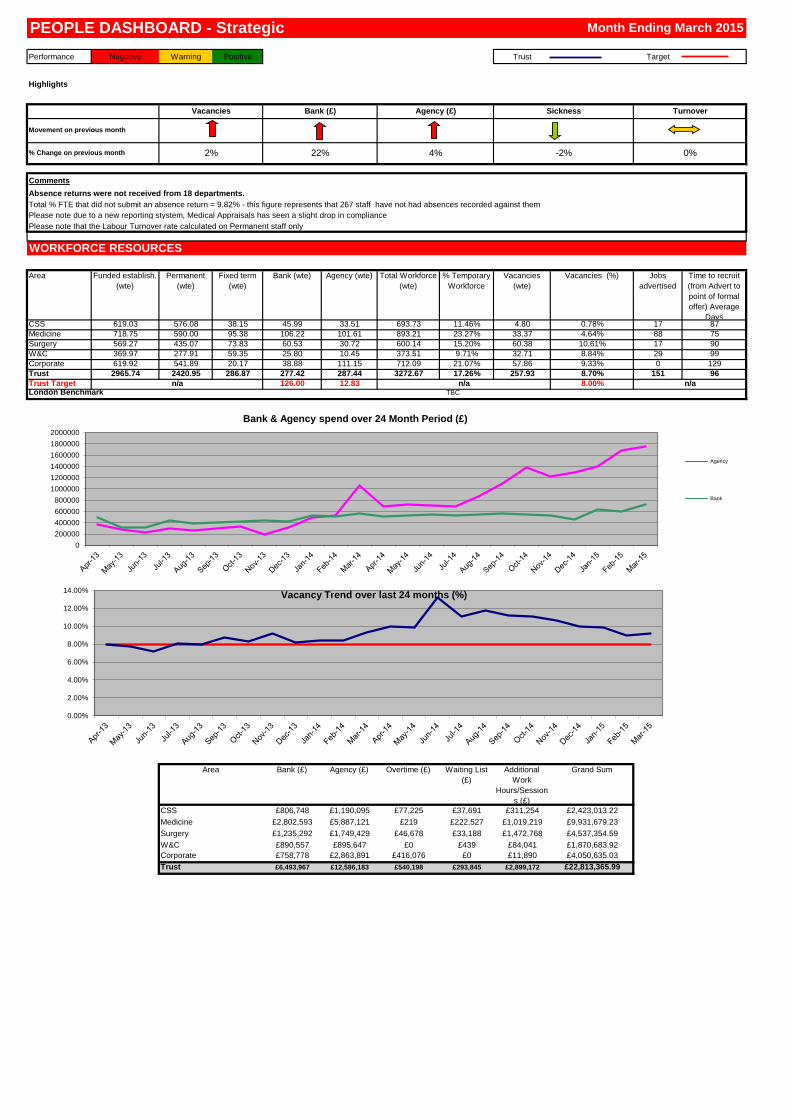
Performance Negative Warning Positive Trust Target
Highlights
Comments
Absence returns were not received from 18 departments.
Total % FTE that did not submit an absence return = 9.82% - this figure represents that 267 staff have not had absences recorded against them
Please note due to a new reporting stystem, Medical Appraisals has seen a slight drop in compliance
Please note that the Labour Turnover rate calculated on Permanent staff only
Area Funded establish.
(wte)
Permanent
(wte)
Fixed term
(wte)
Bank (wte) Agency (wte) Total Workforce
(wte)
% Temporary
Workforce
Vacancies
(wte)
Vacancies (%) Jobs
advertised
Time to recruit
(from Advert to
point of formal
offer) Average
DaysCSS 619.03 576.08 38.15 45.99 33.51 693.73 11.46% 4.80 0.78% 17 87
Medicine 718.75 590.00 95.38 106.22 101.61 893.21 23.27% 33.37 4.64% 88 75
Surgery 569.27 435.07 73.83 60.53 30.72 600.14 15.20% 60.38 10.61% 17 90
W&C 369.97 277.91 59.35 25.80 10.45 373.51 9.71% 32.71 8.84% 29 99
Corporate 619.92 541.89 20.17 38.88 111.15 712.09 21.07% 57.86 9.33% 0 129
Trust 2965.74 2420.95 286.87 277.42 287.44 3272.67 17.26% 257.93 8.70% 151 96
Trust Target 126.00 12.83 8.00%
Bank (£) Agency (£) Overtime (£) Waiting List
(£)
Additional
Work
Hours/Session
s (£)
Grand Sum
£806,748 £1,190,095 £77,225 £37,691 £311,254 £2,423,013.22
£2,802,593 £5,887,121 £219 £222,527 £1,019,219 £9,931,679.23
£1,235,292 £1,749,429 £46,678 £33,188 £1,472,768 £4,537,354.59
£890,557 £895,647 £0 £439 £84,041 £1,870,683.92
£758,778 £2,863,891 £416,076 £0 £11,890 £4,050,635.03
£6,493,967 £12,586,183 £540,198 £293,845 £2,899,172 £22,813,365.99
Area
London Benchmarkn/a n/a
% Change on previous month
n/a
22% -2%2%
W&C
CSS
TBC
Trust
Corporate
PEOPLE DASHBOARD - Strategic Month Ending March 2015
Vacancies Bank (£) Agency (£)
Movement on previous month
TurnoverSickness
4% 0%
WORKFORCE RESOURCES
Medicine
Surgery
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%Vacancy Trend over last 24 months (%)
0
200000
400000
600000
800000
1000000
1200000
1400000
1600000
1800000
2000000
Bank & Agency spend over 24 Month Period (£)
Agency
Bank
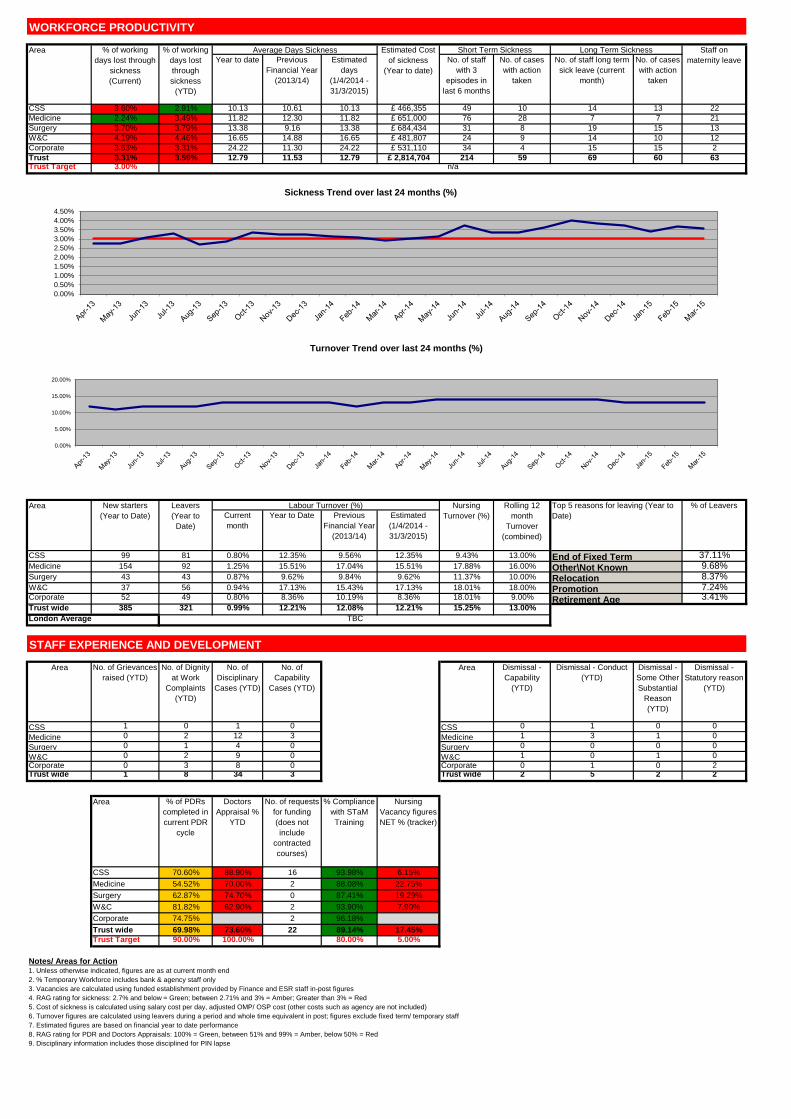
Year to date Previous
Financial Year
(2013/14)
Estimated
days
(1/4/2014 -
31/3/2015)
No. of staff
with 3
episodes in
last 6 months
No. of cases
with action
taken
No. of staff long term
sick leave (current
month)
No. of cases
with action
taken
CSS 3.60% 2.91% 10.13 10.61 10.13 £ 466,355 49 10 14 13 22
Medicine 2.24% 3.49% 11.82 12.30 11.82 £ 651,000 76 28 7 7 21
Surgery 3.70% 3.79% 13.38 9.16 13.38 £ 684,434 31 8 19 15 13
W&C 4.19% 4.46% 16.65 14.88 16.65 £ 481,807 24 9 14 10 12
Corporate 3.63% 3.31% 24.22 11.30 24.22 £ 531,110 34 4 15 15 2
Trust 3.31% 3.59% 12.79 11.53 12.79 £ 2,814,704 214 59 69 60 63Trust Target 3.00%
Current
month
Year to Date Previous
Financial Year
(2013/14)
Estimated
(1/4/2014 -
31/3/2015)
CSS 99 81 0.80% 12.35% 9.56% 12.35% 9.43% 13.00% 37.11%Medicine 154 92 1.25% 15.51% 17.04% 15.51% 17.88% 16.00% 9.68%Surgery 43 43 0.87% 9.62% 9.84% 9.62% 11.37% 10.00% 8.37%W&C 37 56 0.94% 17.13% 15.43% 17.13% 18.01% 18.00% 7.24%Corporate 52 49 0.80% 8.36% 10.19% 8.36% 18.01% 9.00% 3.41%Trust wide 385 321 0.99% 12.21% 12.08% 12.21% 15.25% 13.00%
Area No. of Grievances
raised (YTD)
No. of Dignity
at Work
Complaints
(YTD)
No. of
Disciplinary
Cases (YTD)
No. of
Capability
Cases (YTD)
Area Dismissal -
Capability
(YTD)
Dismissal - Conduct
(YTD)
Dismissal -
Some Other
Substantial
Reason
(YTD)
Dismissal -
Statutory reason
(YTD)
CSS 1 0 1 0 CSS 0 1 0 0
Medicine 0 2 12 3 Medicine 1 3 1 0
Surgery 0 1 4 0 Surgery 0 0 0 0
W&C 0 2 9 0 W&C 1 0 1 0
Corporate 0 3 8 0 Corporate 0 1 0 2Trust wide 1 8 34 3 Trust wide 2 5 2 2
Area % of PDRs
completed in
current PDR
cycle
Doctors
Appraisal %
YTD
No. of requests
for funding
(does not
include
contracted
courses)
% Compliance
with STaM
Training
Nursing
Vacancy figures
NET % (tracker)
CSS 70.60% 88.90% 16 93.98% 6.15%
Medicine 54.52% 70.00% 2 88.08% 22.75%
Surgery 62.87% 74.70% 0 87.41% 19.29%
W&C 81.82% 62.90% 2 93.90% 7.90%
Corporate 74.75% 2 96.18%
Trust wide 69.98% 73.60% 22 89.14% 17.45%
Trust Target 90.00% 100.00% 80.00% 5.00%
Notes/ Areas for Action1. Unless otherwise indicated, figures are as at current month end
2. % Temporary Workforce includes bank & agency staff only
3. Vacancies are calculated using funded establishment provided by Finance and ESR staff in-post figures
4. RAG rating for sickness: 2.7% and below = Green; between 2.71% and 3% = Amber; Greater than 3% = Red
5. Cost of sickness is calculated using salary cost per day, adjusted OMP/ OSP cost (other costs such as agency are not included)
6. Turnover figures are calculated using leavers during a period and whole time equivalent in post; figures exclude fixed term/ temporary staff
7. Estimated figures are based on financial year to date performance
8. RAG rating for PDR and Doctors Appraisals: 100% = Green, between 51% and 99% = Amber, below 50% = Red
9. Disciplinary information includes those disciplined for PIN lapse
WORKFORCE PRODUCTIVITY
End of Fixed Term
% of working
days lost through
sickness
(Current)
Estimated Cost
of sickness
(Year to date)
New starters
(Year to Date)
n/a
Staff on
maternity leave
Short Term SicknessAverage Days Sickness% of working
days lost
through
sickness
(YTD)
Long Term SicknessArea
Area Top 5 reasons for leaving (Year to
Date)
% of LeaversRolling 12
month
Turnover
(combined)
Leavers
(Year to
Date)
Labour Turnover (%) Nursing
Turnover (%)
Relocation
STAFF EXPERIENCE AND DEVELOPMENT
TBCLondon Average
Other\Not Known
Retirement AgePromotion
0.00%
0.50%
1.00%
1.50%
2.00%
2.50%
3.00%
3.50%
4.00%
4.50%
Sickness Trend over last 24 months (%)
0.00%
5.00%
10.00%
15.00%
20.00%
Turnover Trend over last 24 months (%)
Meeting of the Board of Directors – public session Wednesday 27th May 2015
Agenda item 15 Financial Report Reason for item: This is a standing monthly report to the Board in respect of its key regulatory financial responsibilities in compliance to the terms of its provider licence. Summary: This is the full financial report and commentary to the end of April 2015, month 1 of the 2015/16 financial year. The Trust ended the month with a deficit of £358k, £250k behind plan the month. The Trust’s Continuity of Services Risk Rating (CoSRR) was 2 (2.0) in line with the Annual Plan submitted to Monitor. Efficiency savings achieved were £427k, 2.3% of operating expenses and £236k behind the profile built into the approved Annual Plan. Cash ended the month at £9.0m with payables at 30 days. Capital expenditure was £438k, £207k below plan. The Board should note that as the Trust’s healthcare commissioning contract with its lead Commissioner Hillingdon CCG had not been signed it has not been possible to produce the two contract activity reports this month. The Board should also note that although the Trust-wide budget has been agreed and is reflected in the report, detailed budget setting to agree final Divisional and Directorate budgets will not be completed until next month’s report. Therefore, variances reported in Appendix C reflect rollover budgets, 2014/15 outturn funding, inflation pressures, QIPP and funding for agreed Quality Investments. At this stage there has been no assumption of funding for the additional cost pressures over and above 2014/15 outturn assumed within the Annual Plan. Board Action required: The Board is asked to:
1. Note the current financial performance of the Trust. 2. Discuss any actions required for the Trust to achieve its planned CoSRR. Report from: Paul Wratten, Finance Director Links to Trust strategic priorities:
• To deliver high quality care in the most efficient way.
Previous consideration at Board or Committees: n/a Equality and diversity considerations: none. Financial implications: The Trust’s ability to comply with the terms of its provider licence in respect of financial sustainability is critical to the organisation being able to continue to provide the fullest range of high quality health services.
FINANCIAL REPORT APRIL 2015 (MONTH 1)
QUARTER 1, 2015/16
EXECUTIVE SUMMARY The April financial position was a deficit of £358k, £250k worse than plan. EBITDA was £989k; 5.1% of revenue and £137k worse than plan. Overall Operating Expenses were on plan despite an over spend of £208k on pay and significantly on agency pay, generated by the slower delivery of divisional QIPP schemes. Operating revenue was behind plan by £136k, which was very similar to last April. There was a £111k over-spend on depreciation in April. The budget for depreciation was based on outturn 2014/15 but as part of the recent estate revaluation exercise the asset lives of some buildings were reviewed resulting in higher depreciation. Prior to closing the 2014/15 accounts in May an asset by asset review will be completed to determine whether the Trust will incur a significant over-spend against plan on depreciation in this financial year. The Board should note however, the level of depreciation has absolutely no impact on either of the Continuity of Services Risk Rating metrics. At the end of the month the Trust’s Continuity of Services Risk Rating was 2 (2.0). Efficiency savings achieved were £427k, 2.3% of operating expenses and £236k behind the £663k plan profile built into the approved Annual Plan. The Board should note the savings profile generated between the Divisions and the Project Management Office assumed a lower level of savings during quarter 1 than the overall annual plan with planned QIPP delivery of £478k for April generating a monthly shortfall of £51k. KEY MESSAGES • NHS Clinical Revenue under-performed by £62k in April. At the time of
producing this report the Trust had not signed any of its Commissioning Contracts but for all Commissioners, including Hillingdon CCG and NHS England, a financial envelope and key terms had been agreed.
• Non-NHS Clinical Revenue under-recovered in April by £16k.
• Other Operating Revenue under-recovered in April by £58k. The plan for Other
Operating Revenue, like all other elements of the Annual Plan, was based upon the outturn for 2014/15. It is expected additional revenue flows will be secured during the financial year, as has been the case in previous financial years.
• Pay was above plan by £208k in April, with expenditure consistent with
February and March. The Board should note agency expenditure across clinical divisions showed no evidence of reduction at all.
• Agency expenditure for April was £1.58m, compared to a monthly average of
£1.62m for quarter 4 2014/15 and an average of £1.13m per month for the whole of the last financial year.
Page 2 of 3
• Drugs costs were below plan for the month by £89k, which was partly explained by excluded drugs income and expenditure both being below plan.
• Clinical Supplies was below plan for the month by £83k.
• Other operating expenses were below plan for the month by £35k
• Efficiency savings of £427k were delivered in April 2015, £236k (35.6%) below the profile in the Annual plan. This compares with £413k of savings identified in the same month last year.
DIVISIONAL FINANCES • As previously stated the Divisional variances were only indicative though it was
certain that Medicine, Surgery and Women & Children were all significantly over spent in April even allowing for an assumption of funding outturn expenditure for 2014/15
• Divisions will not be allocated a share of contract over-performance revenue until month 2 but as overall NHS Clinical Revenue was below plan it was not anticipated this would significantly alter the financial position of any division.
CASH AND BALANCES • The Trust ended the month with a £9.0m cash balance as the whole year’s
SaHF general transitional support of £3.0m and Paediatric transition support of £3.2m was paid up front.
• The balance sheet reported a negative £1.6m net current liability worsening in-
year due to the net negative cash impact of the capital under spend and revenue statement deficit reported in month.
• Capital expenditure was £438k in-month, £207k below plan.
OTHER KEY STRATEGIC POINTS • Births at 350 for the month were 48 higher than April last year and 6 higher than
the monthly average for the last financial year.
• New GP outpatient referrals were 91 (1.4%) lower than April last year.
• Emergency Department attendances in April 2015 were 225 (3.4%) higher than April 2014 and 70 (1.0%) higher than the monthly average for the last financial year.
• Emergency inpatient spells increased by 248 (10.1%) compared to April last year and 189 (7.5%) compared to the monthly average for last year.
• Elective inpatient and day cases increased by 47, 2.3% compared to last April.
Paul Wratten Finance Director May 2015
Page 3 of 3
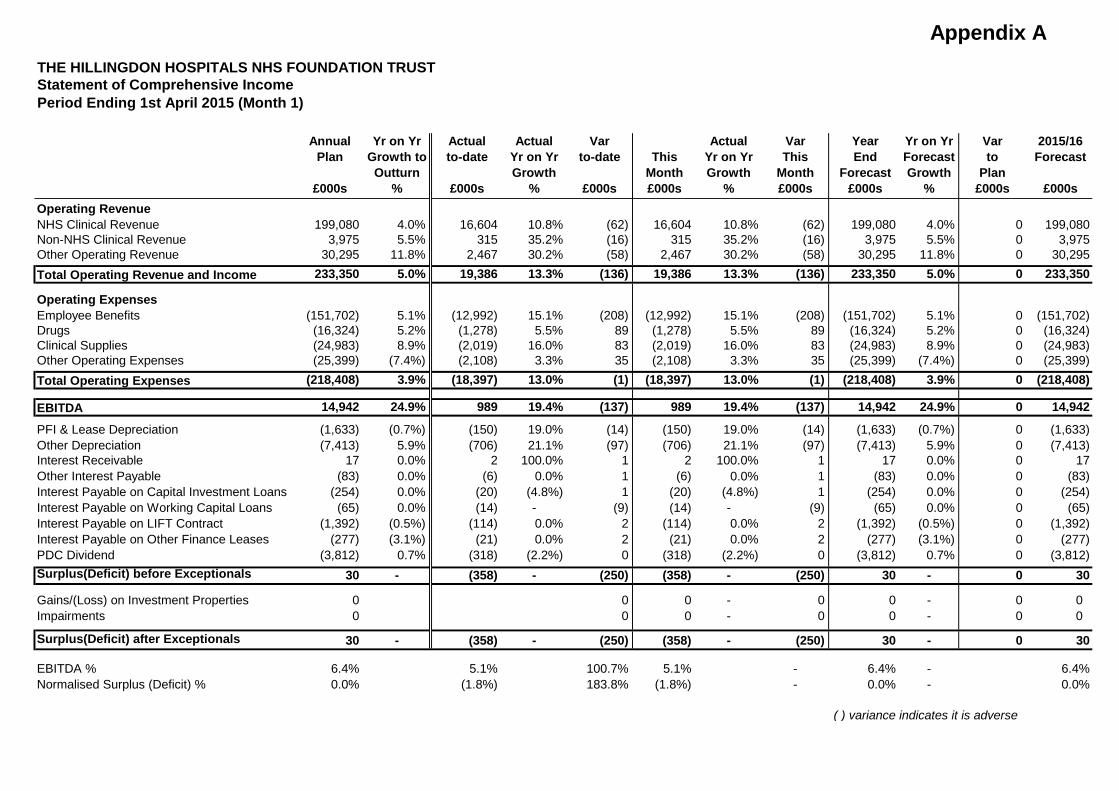
Appendix A
Annual Yr on Yr Actual Actual Var Actual Var Year Yr on Yr Var 2015/16Plan Growth to to-date Yr on Yr to-date This Yr on Yr This End Forecast to Forecast
Outturn Growth Month Growth Month Forecast Growth Plan£000s % £000s % £000s £000s % £000s £000s % £000s £000s
Operating RevenueNHS Clinical Revenue 199,080 4.0% 16,604 10.8% (62) 16,604 10.8% (62) 199,080 4.0% 0 199,080Non-NHS Clinical Revenue 3,975 5.5% 315 35.2% (16) 315 35.2% (16) 3,975 5.5% 0 3,975Other Operating Revenue 30,295 11.8% 2,467 30.2% (58) 2,467 30.2% (58) 30,295 11.8% 0 30,295Total Operating Revenue and Income 233,350 5.0% 19,386 13.3% (136) 19,386 13.3% (136) 233,350 5.0% 0 233,350
Operating ExpensesEmployee Benefits (151,702) 5.1% (12,992) 15.1% (208) (12,992) 15.1% (208) (151,702) 5.1% 0 (151,702)Drugs (16,324) 5.2% (1,278) 5.5% 89 (1,278) 5.5% 89 (16,324) 5.2% 0 (16,324)Clinical Supplies (24,983) 8.9% (2,019) 16.0% 83 (2,019) 16.0% 83 (24,983) 8.9% 0 (24,983)Other Operating Expenses (25,399) (7.4%) (2,108) 3.3% 35 (2,108) 3.3% 35 (25,399) (7.4%) 0 (25,399)Total Operating Expenses (218,408) 3.9% (18,397) 13.0% (1) (18,397) 13.0% (1) (218,408) 3.9% 0 (218,408)
EBITDA 14,942 24.9% 989 19.4% (137) 989 19.4% (137) 14,942 24.9% 0 14,942
PFI & Lease Depreciation (1,633) (0.7%) (150) 19.0% (14) (150) 19.0% (14) (1,633) (0.7%) 0 (1,633)Other Depreciation (7,413) 5.9% (706) 21.1% (97) (706) 21.1% (97) (7,413) 5.9% 0 (7,413)Interest Receivable 17 0.0% 2 100.0% 1 2 100.0% 1 17 0.0% 0 17Other Interest Payable (83) 0.0% (6) 0.0% 1 (6) 0.0% 1 (83) 0.0% 0 (83)Interest Payable on Capital Investment Loans (254) 0.0% (20) (4.8%) 1 (20) (4.8%) 1 (254) 0.0% 0 (254)Interest Payable on Working Capital Loans (65) 0.0% (14) - (9) (14) - (9) (65) 0.0% 0 (65)Interest Payable on LIFT Contract (1,392) (0.5%) (114) 0.0% 2 (114) 0.0% 2 (1,392) (0.5%) 0 (1,392)Interest Payable on Other Finance Leases (277) (3.1%) (21) 0.0% 2 (21) 0.0% 2 (277) (3.1%) 0 (277)PDC Dividend (3,812) 0.7% (318) (2.2%) 0 (318) (2.2%) 0 (3,812) 0.7% 0 (3,812)Surplus(Deficit) before Exceptionals 30 - (358) - (250) (358) - (250) 30 - 0 30
Gains/(Loss) on Investment Properties 0 0 0 - 0 0 - 0 0 Impairments 0 0 0 - 0 0 - 0 0
Surplus(Deficit) after Exceptionals 30 - (358) - (250) (358) - (250) 30 - 0 30
EBITDA % 6.4% 5.1% 100.7% 5.1% - 6.4% - 6.4%Normalised Surplus (Deficit) % 0.0% (1.8%) 183.8% (1.8%) - 0.0% - 0.0%
( ) variance indicates it is adverse
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTStatement of Comprehensive IncomePeriod Ending 1st April 2015 (Month 1)
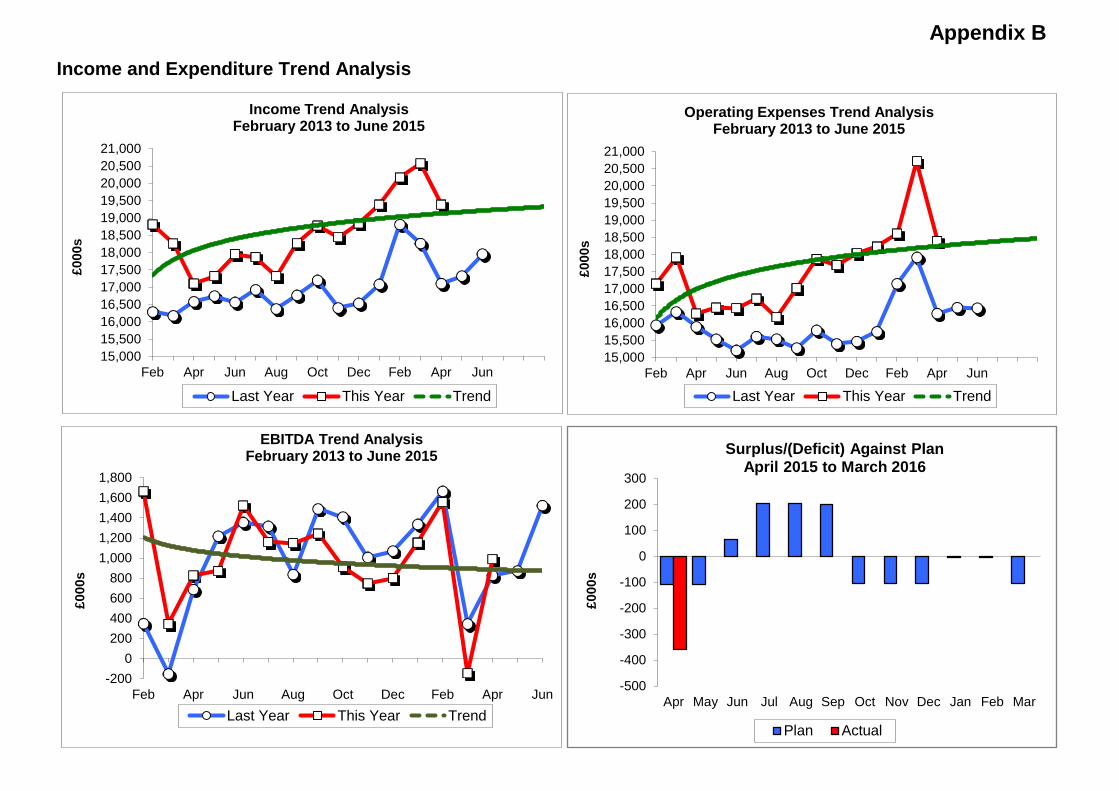
Appendix BIncome and Expenditure Trend Analysis
15,00015,50016,00016,50017,00017,50018,00018,50019,00019,50020,00020,50021,000
Feb Apr Jun Aug Oct Dec Feb Apr Jun
£000
s
Income Trend Analysis February 2013 to June 2015
Last Year This Year Trend
15,00015,50016,00016,50017,00017,50018,00018,50019,00019,50020,00020,50021,000
Feb Apr Jun Aug Oct Dec Feb Apr Jun
£000
s
Operating Expenses Trend Analysis February 2013 to June 2015
Last Year This Year Trend
-2000
200400600800
1,0001,2001,4001,6001,800
Feb Apr Jun Aug Oct Dec Feb Apr Jun
£000
s
EBITDA Trend Analysis February 2013 to June 2015
Last Year This Year Trend
-500
-400
-300
-200
-100
0
100
200
300
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
£000
s
Surplus/(Deficit) Against Plan April 2015 to March 2016
Plan Actual
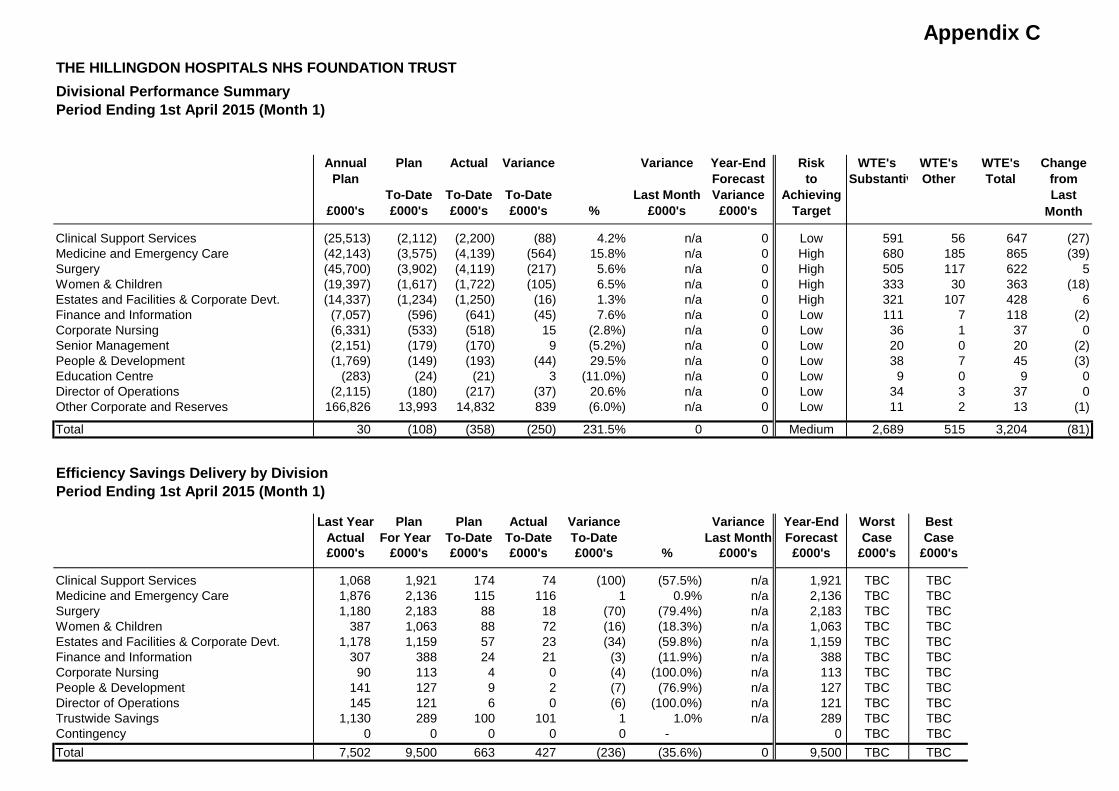
Appendix C THE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTDivisional Performance Summary Period Ending 1st April 2015 (Month 1)
Annual Plan Actual Variance Variance Year-End Risk WTE's WTE's WTE's ChangePlan Forecast to Substantiv Other Total from
To-Date To-Date To-Date Last Month Variance Achieving Last£000's £000's £000's £000's % £000's £000's Target Month
Clinical Support Services (25,513) (2,112) (2,200) (88) 4.2% n/a 0 Low 591 56 647 (27)Medicine and Emergency Care (42,143) (3,575) (4,139) (564) 15.8% n/a 0 High 680 185 865 (39)Surgery (45,700) (3,902) (4,119) (217) 5.6% n/a 0 High 505 117 622 5Women & Children (19,397) (1,617) (1,722) (105) 6.5% n/a 0 High 333 30 363 (18)Estates and Facilities & Corporate Devt. (14,337) (1,234) (1,250) (16) 1.3% n/a 0 High 321 107 428 6Finance and Information (7,057) (596) (641) (45) 7.6% n/a 0 Low 111 7 118 (2)Corporate Nursing (6,331) (533) (518) 15 (2.8%) n/a 0 Low 36 1 37 0Senior Management (2,151) (179) (170) 9 (5.2%) n/a 0 Low 20 0 20 (2)People & Development (1,769) (149) (193) (44) 29.5% n/a 0 Low 38 7 45 (3)Education Centre (283) (24) (21) 3 (11.0%) n/a 0 Low 9 0 9 0Director of Operations (2,115) (180) (217) (37) 20.6% n/a 0 Low 34 3 37 0Other Corporate and Reserves 166,826 13,993 14,832 839 (6.0%) n/a 0 Low 11 2 13 (1)
Total 30 (108) (358) (250) 231.5% 0 0 Medium 2,689 515 3,204 (81)
Efficiency Savings Delivery by DivisionPeriod Ending 1st April 2015 (Month 1)
Last Year Plan Plan Actual Variance Variance Year-End Worst BestActual For Year To-Date To-Date To-Date Last Month Forecast Case Case£000's £000's £000's £000's £000's % £000's £000's £000's £000's
Clinical Support Services 1,068 1,921 174 74 (100) (57.5%) n/a 1,921 TBC TBCMedicine and Emergency Care 1,876 2,136 115 116 1 0.9% n/a 2,136 TBC TBCSurgery 1,180 2,183 88 18 (70) (79.4%) n/a 2,183 TBC TBCWomen & Children 387 1,063 88 72 (16) (18.3%) n/a 1,063 TBC TBCEstates and Facilities & Corporate Devt. 1,178 1,159 57 23 (34) (59.8%) n/a 1,159 TBC TBCFinance and Information 307 388 24 21 (3) (11.9%) n/a 388 TBC TBCCorporate Nursing 90 113 4 0 (4) (100.0%) n/a 113 TBC TBCPeople & Development 141 127 9 2 (7) (76.9%) n/a 127 TBC TBCDirector of Operations 145 121 6 0 (6) (100.0%) n/a 121 TBC TBCTrustwide Savings 1,130 289 100 101 1 1.0% n/a 289 TBC TBCContingency 0 0 0 0 0 - 0 TBC TBCTotal 7,502 9,500 663 427 (236) (35.6%) 0 9,500 TBC TBC
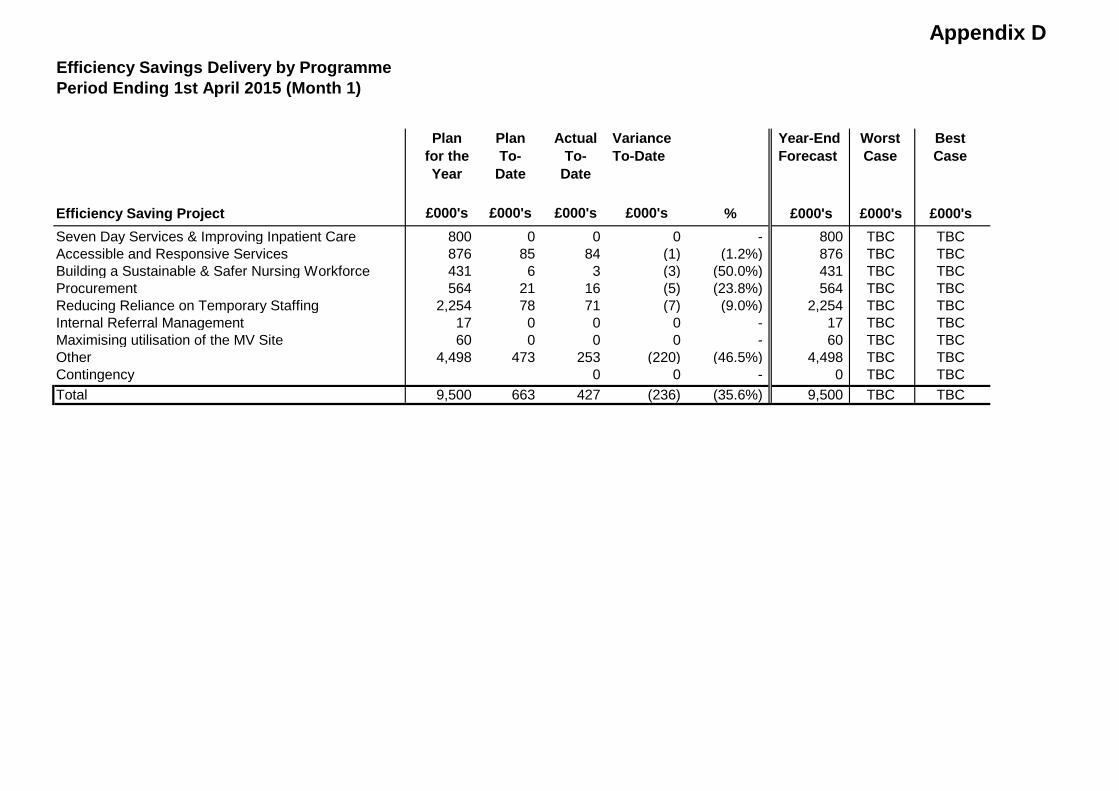
Appendix DEfficiency Savings Delivery by ProgrammePeriod Ending 1st April 2015 (Month 1)
Plan for the Year
Plan To-
Date
Actual To-
Date
Variance To-Date
Year-End Forecast
Worst Case
Best Case
Efficiency Saving Project £000's £000's £000's £000's % £000's £000's £000'sSeven Day Services & Improving Inpatient Care 800 0 0 0 - 800 TBC TBCAccessible and Responsive Services 876 85 84 (1) (1.2%) 876 TBC TBCBuilding a Sustainable & Safer Nursing Workforce 431 6 3 (3) (50.0%) 431 TBC TBCProcurement 564 21 16 (5) (23.8%) 564 TBC TBCReducing Reliance on Temporary Staffing 2,254 78 71 (7) (9.0%) 2,254 TBC TBCInternal Referral Management 17 0 0 0 - 17 TBC TBCMaximising utilisation of the MV Site 60 0 0 0 - 60 TBC TBCOther 4,498 473 253 (220) (46.5%) 4,498 TBC TBCContingency 0 0 - 0 TBC TBCTotal 9,500 663 427 (236) (35.6%) 9,500 TBC TBC
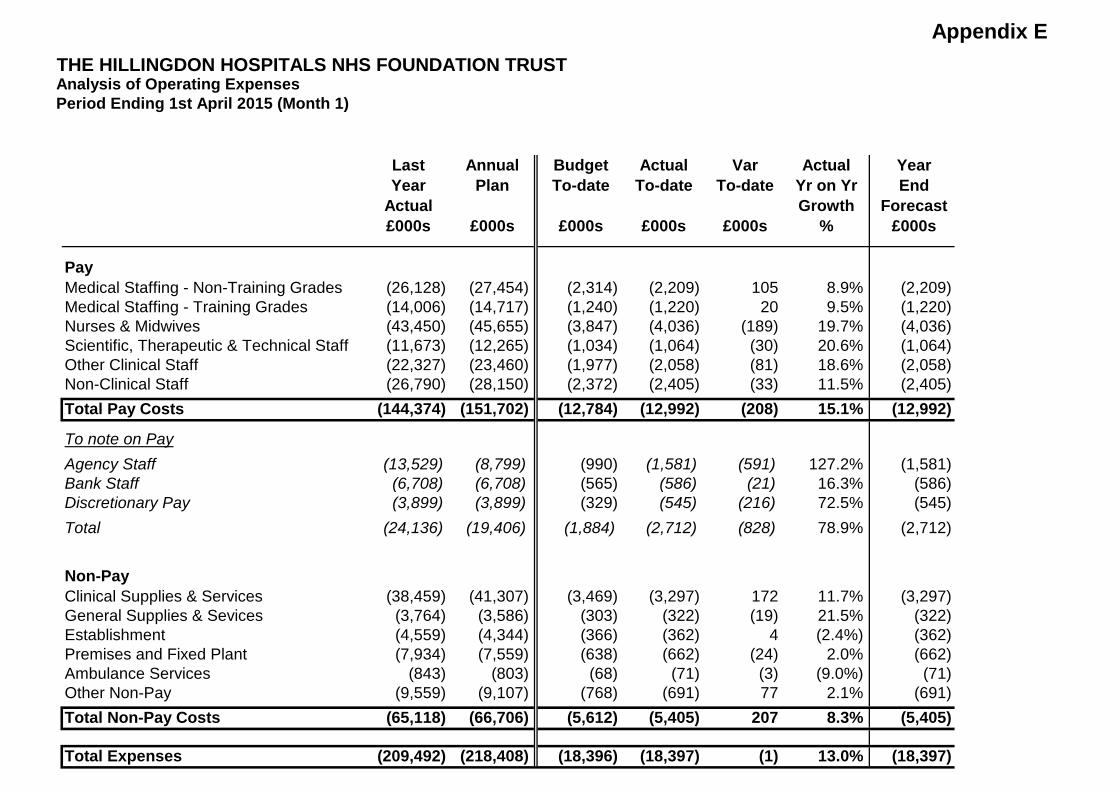
Appendix E THE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTAnalysis of Operating ExpensesPeriod Ending 1st April 2015 (Month 1)
Last Annual Budget Actual Var Actual YearYear Plan To-date To-date To-date Yr on Yr End
Actual Growth Forecast£000s £000s £000s £000s £000s % £000s
PayMedical Staffing - Non-Training Grades (26,128) (27,454) (2,314) (2,209) 105 8.9% (2,209)Medical Staffing - Training Grades (14,006) (14,717) (1,240) (1,220) 20 9.5% (1,220)Nurses & Midwives (43,450) (45,655) (3,847) (4,036) (189) 19.7% (4,036)Scientific, Therapeutic & Technical Staff (11,673) (12,265) (1,034) (1,064) (30) 20.6% (1,064)Other Clinical Staff (22,327) (23,460) (1,977) (2,058) (81) 18.6% (2,058)Non-Clinical Staff (26,790) (28,150) (2,372) (2,405) (33) 11.5% (2,405)Total Pay Costs (144,374) (151,702) (12,784) (12,992) (208) 15.1% (12,992)
To note on PayAgency Staff (13,529) (8,799) (990) (1,581) (591) 127.2% (1,581)Bank Staff (6,708) (6,708) (565) (586) (21) 16.3% (586)Discretionary Pay (3,899) (3,899) (329) (545) (216) 72.5% (545)Total (24,136) (19,406) (1,884) (2,712) (828) 78.9% (2,712)
Non-PayClinical Supplies & Services (38,459) (41,307) (3,469) (3,297) 172 11.7% (3,297)General Supplies & Sevices (3,764) (3,586) (303) (322) (19) 21.5% (322)Establishment (4,559) (4,344) (366) (362) 4 (2.4%) (362)Premises and Fixed Plant (7,934) (7,559) (638) (662) (24) 2.0% (662)Ambulance Services (843) (803) (68) (71) (3) (9.0%) (71)Other Non-Pay (9,559) (9,107) (768) (691) 77 2.1% (691)Total Non-Pay Costs (65,118) (66,706) (5,612) (5,405) 207 8.3% (5,405)
Total Expenses (209,492) (218,408) (18,396) (18,397) (1) 13.0% (18,397)
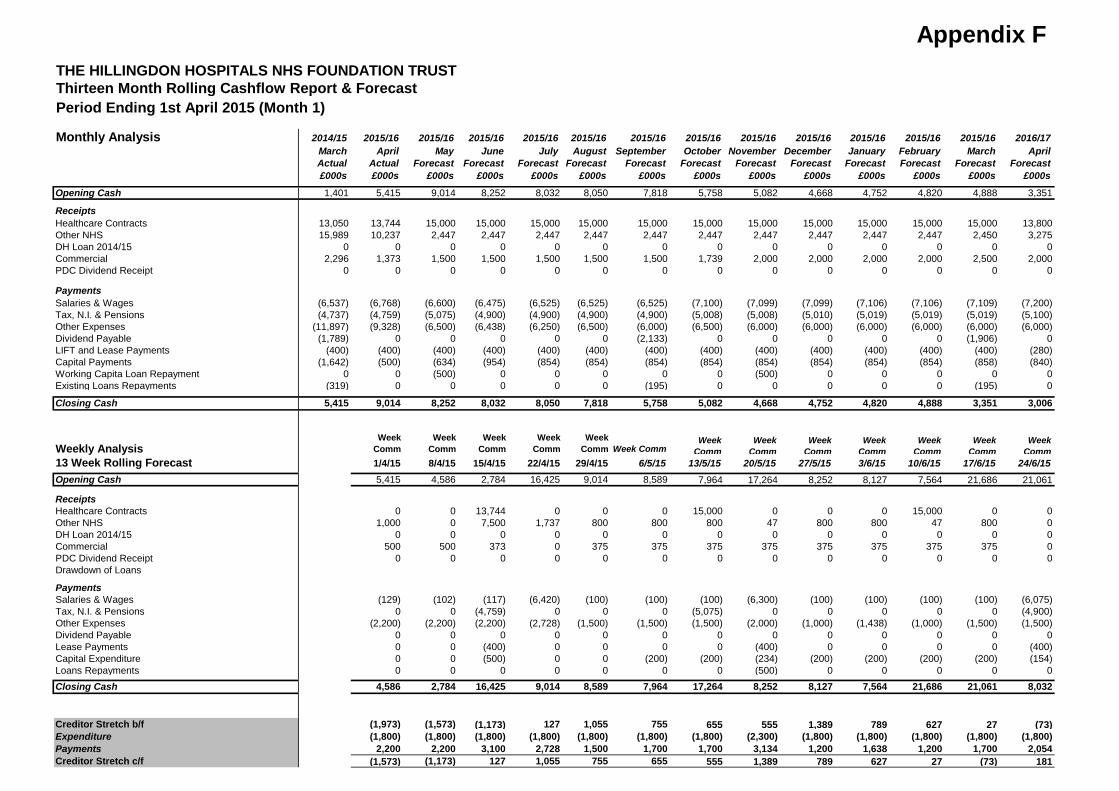
Appendix FTHE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTThirteen Month Rolling Cashflow Report & Forecast Period Ending 1st April 2015 (Month 1)
Monthly Analysis 2014/15 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2016/17March April May June July August September October November December January February March AprilActual Actual Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast£000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s
Opening Cash 1,401 5,415 9,014 8,252 8,032 8,050 7,818 5,758 5,082 4,668 4,752 4,820 4,888 3,351
ReceiptsHealthcare Contracts 13,050 13,744 15,000 15,000 15,000 15,000 15,000 15,000 15,000 15,000 15,000 15,000 15,000 13,800Other NHS 15,989 10,237 2,447 2,447 2,447 2,447 2,447 2,447 2,447 2,447 2,447 2,447 2,450 3,275DH Loan 2014/15 0 0 0 0 0 0 0 0 0 0 0 0 0 0Commercial 2,296 1,373 1,500 1,500 1,500 1,500 1,500 1,739 2,000 2,000 2,000 2,000 2,500 2,000PDC Dividend Receipt 0 0 0 0 0 0 0 0 0 0 0 0 0 0
PaymentsSalaries & Wages (6,537) (6,768) (6,600) (6,475) (6,525) (6,525) (6,525) (7,100) (7,099) (7,099) (7,106) (7,106) (7,109) (7,200)Tax, N.I. & Pensions (4,737) (4,759) (5,075) (4,900) (4,900) (4,900) (4,900) (5,008) (5,008) (5,010) (5,019) (5,019) (5,019) (5,100)Other Expenses (11,897) (9,328) (6,500) (6,438) (6,250) (6,500) (6,000) (6,500) (6,000) (6,000) (6,000) (6,000) (6,000) (6,000)Dividend Payable (1,789) 0 0 0 0 0 (2,133) 0 0 0 0 0 (1,906) 0LIFT and Lease Payments (400) (400) (400) (400) (400) (400) (400) (400) (400) (400) (400) (400) (400) (280)Capital Payments (1,642) (500) (634) (954) (854) (854) (854) (854) (854) (854) (854) (854) (858) (840)Working Capita Loan Repayment 0 0 (500) 0 0 0 0 0 (500) 0 0 0 0 0Existing Loans Repayments (319) 0 0 0 0 0 (195) 0 0 0 0 0 (195) 0
Closing Cash 5,415 9,014 8,252 8,032 8,050 7,818 5,758 5,082 4,668 4,752 4,820 4,888 3,351 3,006
Weekly AnalysisWeek
CommWeek
CommWeek
CommWeek
CommWeek
Comm Week CommWeek
CommWeek
CommWeek
CommWeek
CommWeek
CommWeek
CommWeek
Comm13 Week Rolling Forecast 1/4/15 8/4/15 15/4/15 22/4/15 29/4/15 6/5/15 13/5/15 20/5/15 27/5/15 3/6/15 10/6/15 17/6/15 24/6/15Opening Cash 5,415 4,586 2,784 16,425 9,014 8,589 7,964 17,264 8,252 8,127 7,564 21,686 21,061
ReceiptsHealthcare Contracts 0 0 13,744 0 0 0 15,000 0 0 0 15,000 0 0Other NHS 1,000 0 7,500 1,737 800 800 800 47 800 800 47 800 0DH Loan 2014/15 0 0 0 0 0 0 0 0 0 0 0 0 0Commercial 500 500 373 0 375 375 375 375 375 375 375 375 0PDC Dividend Receipt 0 0 0 0 0 0 0 0 0 0 0 0 0Drawdown of Loans
PaymentsSalaries & Wages (129) (102) (117) (6,420) (100) (100) (100) (6,300) (100) (100) (100) (100) (6,075)Tax, N.I. & Pensions 0 0 (4,759) 0 0 0 (5,075) 0 0 0 0 0 (4,900)Other Expenses (2,200) (2,200) (2,200) (2,728) (1,500) (1,500) (1,500) (2,000) (1,000) (1,438) (1,000) (1,500) (1,500)Dividend Payable 0 0 0 0 0 0 0 0 0 0 0 0 0Lease Payments 0 0 (400) 0 0 0 0 (400) 0 0 0 0 (400)Capital Expenditure 0 0 (500) 0 0 (200) (200) (234) (200) (200) (200) (200) (154)Loans Repayments 0 0 0 0 0 0 0 (500) 0 0 0 0 0Closing Cash 4,586 2,784 16,425 9,014 8,589 7,964 17,264 8,252 8,127 7,564 21,686 21,061 8,032
Creditor Stretch b/f (1,973) (1,573) (1,173) 127 1,055 755 655 555 1,389 789 627 27 (73)Expenditure (1,800) (1,800) (1,800) (1,800) (1,800) (1,800) (1,800) (2,300) (1,800) (1,800) (1,800) (1,800) (1,800)Payments 2,200 2,200 3,100 2,728 1,500 1,700 1,700 3,134 1,200 1,638 1,200 1,700 2,054Creditor Stretch c/f (1,573) (1,173) 127 1,055 755 655 555 1,389 789 627 27 (73) 181
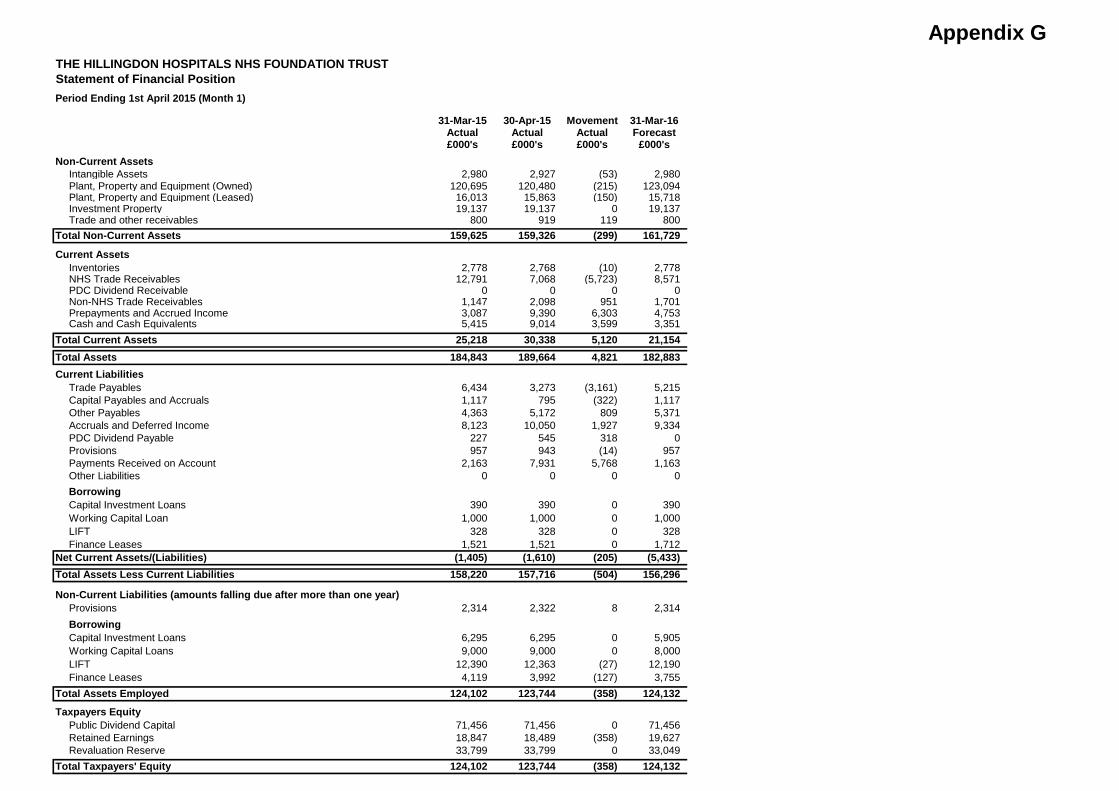
Appendix GTHE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTStatement of Financial Position Period Ending 1st April 2015 (Month 1)
31-Mar-15 30-Apr-15 Movement 31-Mar-16Actual Actual Actual Forecast£000's £000's £000's £000's
Non-Current AssetsIntangible Assets 2,980 2,927 (53) 2,980Plant, Property and Equipment (Owned) 120,695 120,480 (215) 123,094Plant, Property and Equipment (Leased) 16,013 15,863 (150) 15,718Investment Property 19,137 19,137 0 19,137Trade and other receivables 800 919 119 800
Total Non-Current Assets 159,625 159,326 (299) 161,729
Current AssetsInventories 2,778 2,768 (10) 2,778NHS Trade Receivables 12,791 7,068 (5,723) 8,571PDC Dividend Receivable 0 0 0 0Non-NHS Trade Receivables 1,147 2,098 951 1,701Prepayments and Accrued Income 3,087 9,390 6,303 4,753Cash and Cash Equivalents 5,415 9,014 3,599 3,351
Total Current Assets 25,218 30,338 5,120 21,154Total Assets 184,843 189,664 4,821 182,883Current Liabilities
Trade Payables 6,434 3,273 (3,161) 5,215Capital Payables and Accruals 1,117 795 (322) 1,117Other Payables 4,363 5,172 809 5,371Accruals and Deferred Income 8,123 10,050 1,927 9,334PDC Dividend Payable 227 545 318 0Provisions 957 943 (14) 957Payments Received on Account 2,163 7,931 5,768 1,163Other Liabilities 0 0 0 0BorrowingCapital Investment Loans 390 390 0 390Working Capital Loan 1,000 1,000 0 1,000LIFT 328 328 0 328Finance Leases 1,521 1,521 0 1,712
Net Current Assets/(Liabilities) (1,405) (1,610) (205) (5,433)Total Assets Less Current Liabilities 158,220 157,716 (504) 156,296
Non-Current Liabilities (amounts falling due after more than one year)Provisions 2,314 2,322 8 2,314BorrowingCapital Investment Loans 6,295 6,295 0 5,905Working Capital Loans 9,000 9,000 0 8,000LIFT 12,390 12,363 (27) 12,190Finance Leases 4,119 3,992 (127) 3,755
Total Assets Employed 124,102 123,744 (358) 124,132
Taxpayers EquityPublic Dividend Capital 71,456 71,456 0 71,456Retained Earnings 18,847 18,489 (358) 19,627Revaluation Reserve 33,799 33,799 0 33,049
Total Taxpayers' Equity 124,102 123,744 (358) 124,132
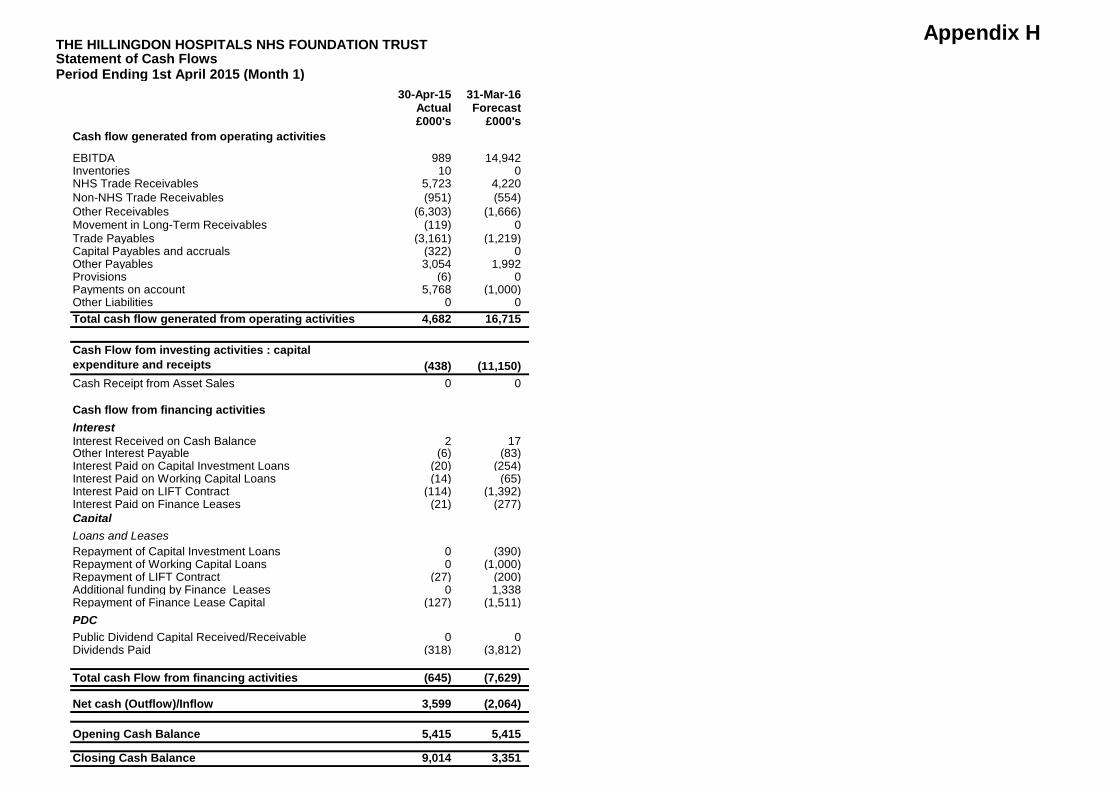
Appendix H THE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTStatement of Cash Flows Period Ending 1st April 2015 (Month 1)
30-Apr-15 31-Mar-16Actual Forecast£000's £000's
Cash flow generated from operating activities
EBITDA 989 14,942Inventories 10 0NHS Trade Receivables 5,723 4,220Non-NHS Trade Receivables (951) (554)Other Receivables (6,303) (1,666)Movement in Long-Term Receivables (119) 0Trade Payables (3,161) (1,219)Capital Payables and accruals (322) 0Other Payables 3,054 1,992Provisions (6) 0Payments on account 5,768 (1,000)Other Liabilities 0 0Total cash flow generated from operating activities 4,682 16,715
Cash Flow fom investing activities : capital expenditure and receipts (438) (11,150)Cash Receipt from Asset Sales 0 0
Cash flow from financing activitiesInterestInterest Received on Cash Balance 2 17Other Interest Payable (6) (83)Interest Paid on Capital Investment Loans (20) (254)Interest Paid on Working Capital Loans (14) (65)Interest Paid on LIFT Contract (114) (1,392)Interest Paid on Finance Leases (21) (277)CapitalLoans and LeasesRepayment of Capital Investment Loans 0 (390)Repayment of Working Capital Loans 0 (1,000)Repayment of LIFT Contract (27) (200)Additional funding by Finance Leases 0 1,338Repayment of Finance Lease Capital (127) (1,511)PDCPublic Dividend Capital Received/Receivable 0 0Dividends Paid (318) (3,812)
Total cash Flow from financing activities (645) (7,629)
Net cash (Outflow)/Inflow 3,599 (2,064)
Opening Cash Balance 5,415 5,415
Closing Cash Balance 9,014 3,351
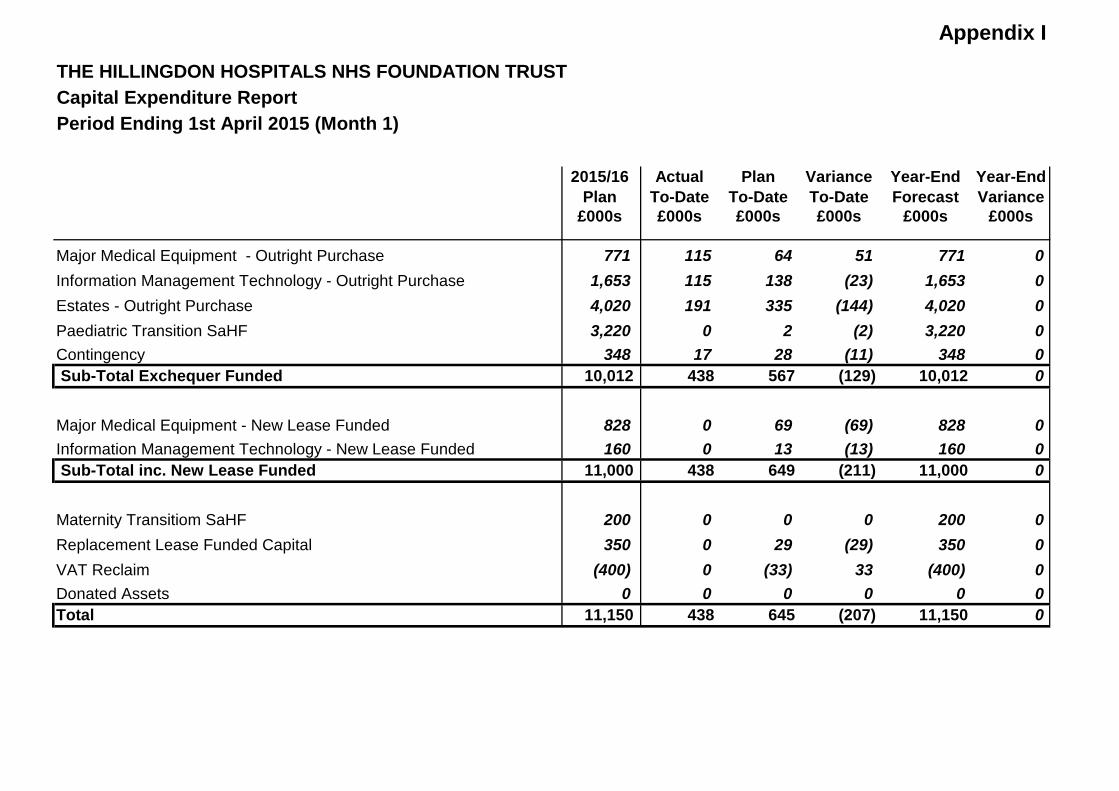
Appendix I
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTCapital Expenditure ReportPeriod Ending 1st April 2015 (Month 1)
2015/16 Actual Plan Variance Year-End Year-EndPlan To-Date To-Date To-Date Forecast Variance
£000s £000s £000s £000s £000s £000s
Major Medical Equipment - Outright Purchase 771 115 64 51 771 0Information Management Technology - Outright Purchase 1,653 115 138 (23) 1,653 0Estates - Outright Purchase 4,020 191 335 (144) 4,020 0Paediatric Transition SaHF 3,220 0 2 (2) 3,220 0Contingency 348 17 28 (11) 348 0 Sub-Total Exchequer Funded 10,012 438 567 (129) 10,012 0
Major Medical Equipment - New Lease Funded 828 0 69 (69) 828 0Information Management Technology - New Lease Funded 160 0 13 (13) 160 0 Sub-Total inc. New Lease Funded 11,000 438 649 (211) 11,000 0
Maternity Transitiom SaHF 200 0 0 0 200 0Replacement Lease Funded Capital 350 0 29 (29) 350 0VAT Reclaim (400) 0 (33) 33 (400) 0Donated Assets 0 0 0 0 0 0Total 11,150 438 645 (207) 11,150 0
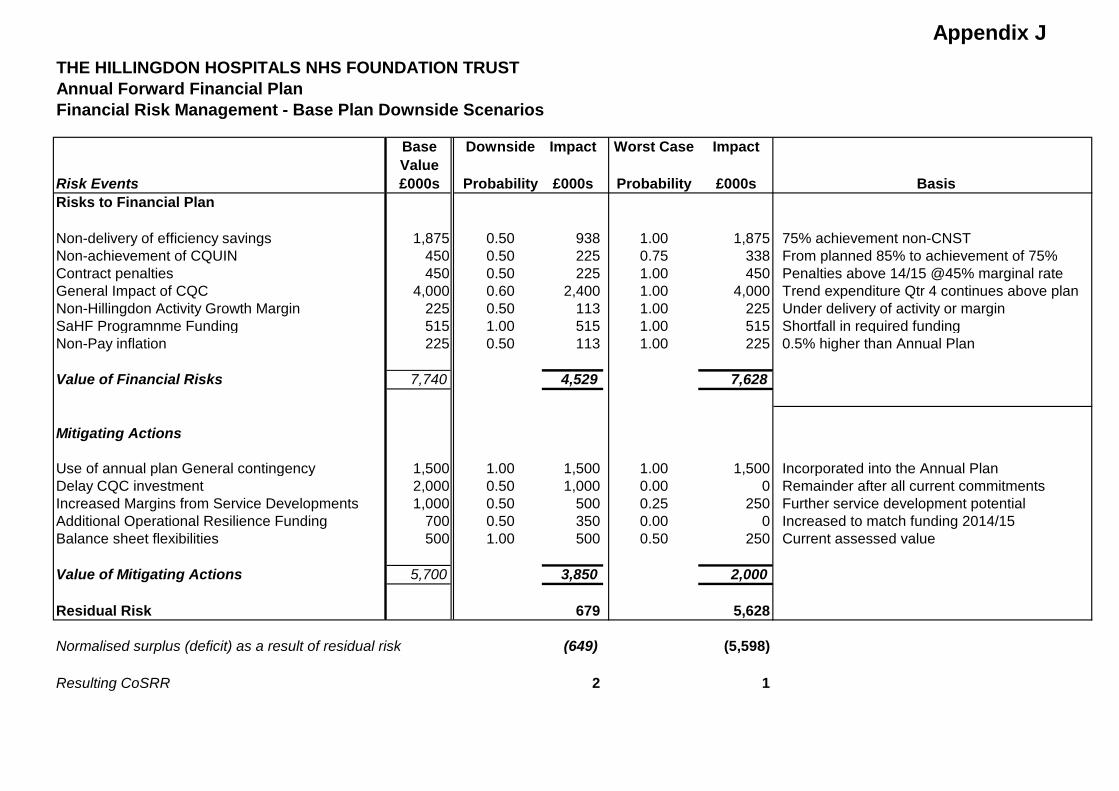
Appendix JTHE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTAnnual Forward Financial PlanFinancial Risk Management - Base Plan Downside Scenarios
Base Downside Impact Worst Case ImpactValue
Risk Events £000s Probability £000s Probability £000s BasisRisks to Financial Plan
Non-delivery of efficiency savings 1,875 0.50 938 1.00 1,875 75% achievement non-CNSTNon-achievement of CQUIN 450 0.50 225 0.75 338 From planned 85% to achievement of 75%Contract penalties 450 0.50 225 1.00 450 Penalties above 14/15 @45% marginal rateGeneral Impact of CQC 4,000 0.60 2,400 1.00 4,000 Trend expenditure Qtr 4 continues above planNon-Hillingdon Activity Growth Margin 225 0.50 113 1.00 225 Under delivery of activity or marginSaHF Programnme Funding 515 1.00 515 1.00 515 Shortfall in required fundingNon-Pay inflation 225 0.50 113 1.00 225 0.5% higher than Annual Plan
Value of Financial Risks 7,740 4,529 7,628
Mitigating Actions
Use of annual plan General contingency 1,500 1.00 1,500 1.00 1,500 Incorporated into the Annual PlanDelay CQC investment 2,000 0.50 1,000 0.00 0 Remainder after all current commitmentsIncreased Margins from Service Developments 1,000 0.50 500 0.25 250 Further service development potentialAdditional Operational Resilience Funding 700 0.50 350 0.00 0 Increased to match funding 2014/15Balance sheet flexibilities 500 1.00 500 0.50 250 Current assessed value
Value of Mitigating Actions 5,700 3,850 2,000
Residual Risk 679 5,628
Normalised surplus (deficit) as a result of residual risk (649) (5,598)
Resulting CoSRR 2 1
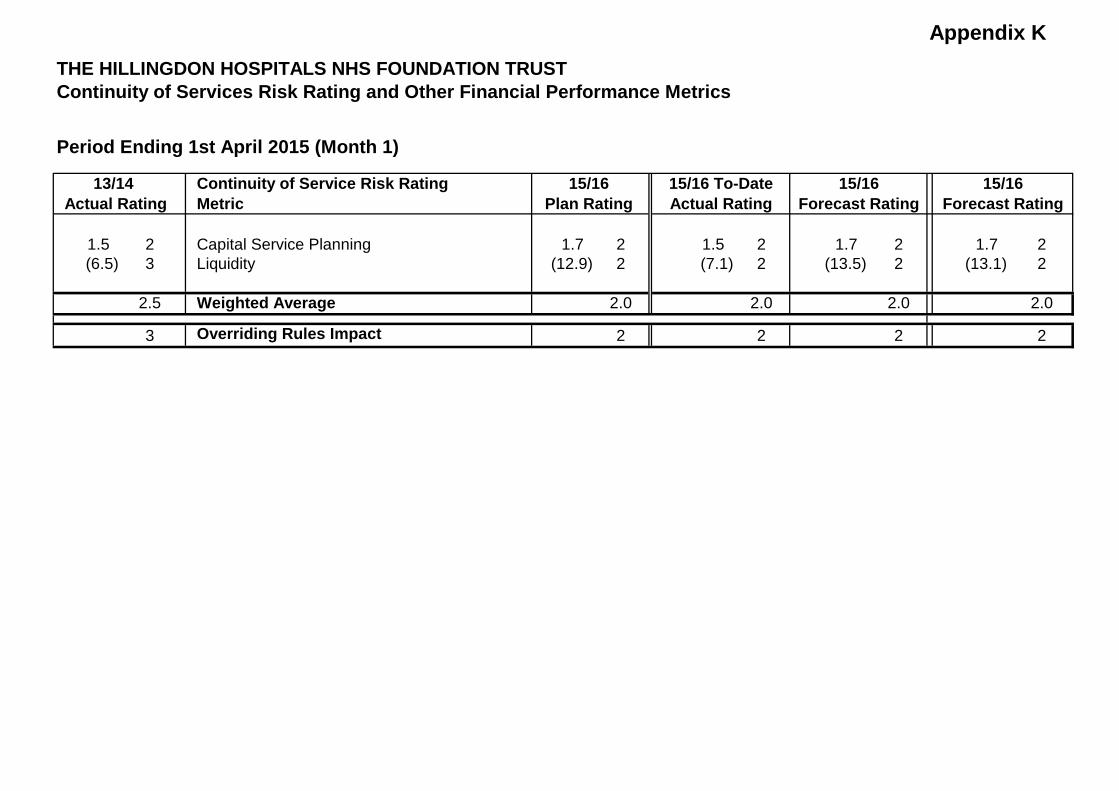
Appendix K
Continuity of Services Risk Rating and Other Financial Performance Metrics
Period Ending 1st April 2015 (Month 1)
Continuity of Service Risk RatingMetric
1.5 2 Capital Service Planning 1.7 2 1.5 2 1.7 2 1.7 2(6.5) 3 Liquidity (12.9) 2 (7.1) 2 (13.5) 2 (13.1) 2
2.5 Weighted Average 2.0 2.0 2.0 2.0
3 Overriding Rules Impact 2 2 2 2
Forecast Rating Forecast Rating
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST
13/14 15/16 15/16 To-Date 15/16 15/16Actual Rating Plan Rating Actual Rating
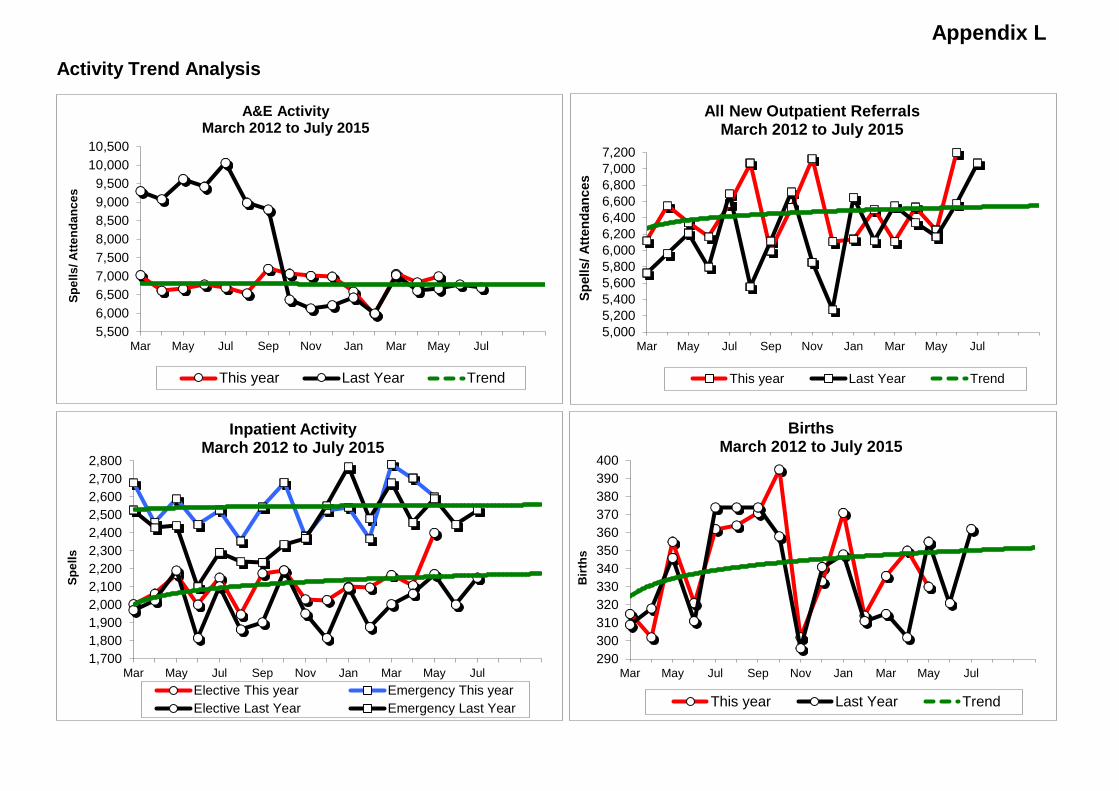
Appendix LActivity Trend Analysis
5,5006,0006,5007,0007,5008,0008,5009,0009,500
10,00010,500
Mar May Jul Sep Nov Jan Mar May Jul
Spel
ls/ A
ttend
ance
s
A&E Activity March 2012 to July 2015
This year Last Year Trend
5,0005,2005,4005,6005,8006,0006,2006,4006,6006,8007,0007,200
Mar May Jul Sep Nov Jan Mar May Jul
Spel
ls/ A
ttend
ance
s
All New Outpatient Referrals March 2012 to July 2015
This year Last Year Trend
1,7001,8001,9002,0002,1002,2002,3002,4002,5002,6002,7002,800
Mar May Jul Sep Nov Jan Mar May Jul
Spel
ls
Inpatient Activity March 2012 to July 2015
Elective This year Emergency This yearElective Last Year Emergency Last Year
290300310320330340350360370380390400
Mar May Jul Sep Nov Jan Mar May Jul
Birt
hs
Births March 2012 to July 2015
This year Last Year Trend
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 16
2015/16 Month 1 Transformation and QIPP update Reason for item: This monthly report provides an update on the 2015/16 QIPP programme as well as Month 1 performance against plan and the monthly phasing for the programme. The report also includes a review of the lessons learned in 2014/15 and how these have been incorporated in the planning for the current programme. Summary: Lessons from the 2014/15 programme have been incorporated into the planning for the 2015/16 QIPP programme. The approach this year is to identify more than the requirement to offset potential slippage of the schemes. To date the Trust has identified a QIPP programme of £9.57 million and work is ongoing to exceed this value. Delivery in Month 1 was £427k against a plan of £475k which equates to 90% of the value. Recognising that any shortfall has to be mitigated, the divisions and corporate areas are developing actions to offset this shortfall and ensure delivery of the identified schemes. The report includes an update on progress to date and next steps for the Trust-wide Transforming Patient Care and Workforce Transformation programmes. The focus for 2015/16 for Hillingdon CCG (HCCG) continues to be on reducing non-elective demand in the wider sense through their Long Term Conditions Schemes, improvements to the Practice Commissioning Initiative and Integrated Care Programme and other related schemes. The Trust will be analysing in detail the HCCG assumptions that relate to the Trust to ensure alignment of the two programmes. Board Action required: The Board is asked to: 1. Note the lessons that were learned from the 2014/15 QIPP programme and delivery in
Month 1 of 2015/16. 2. Review the overall position of the 2015/16 programme and agree any further actions that
need to be undertaken
Report from: Tendai Chikasha, Associate Director of Transformation Report sponsor: Joe Smyth, Chief Operating Officer (COO) Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience
and the quality of care we provide.
Page 1

• To deliver high quality care in the most efficient way. Previous consideration at Board or Committees: N/A Equality and diversity considerations: N/A Financial implications: There may be financial implications for some of the changes. These will be worked through with regards to their impact/benefit and prioritised for consideration within the governance framework.
Page 2
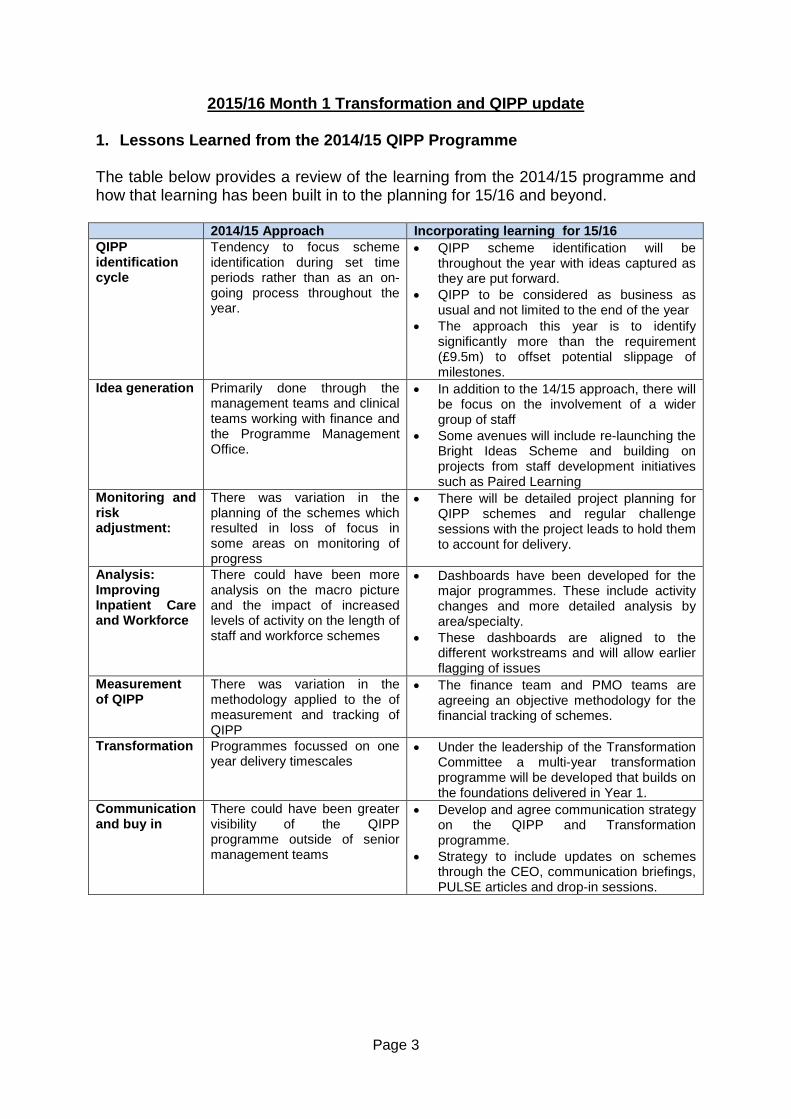
2015/16 Month 1 Transformation and QIPP update
1. Lessons Learned from the 2014/15 QIPP Programme The table below provides a review of the learning from the 2014/15 programme and how that learning has been built in to the planning for 15/16 and beyond. 2014/15 Approach Incorporating learning for 15/16 QIPP identification cycle
Tendency to focus scheme identification during set time periods rather than as an on-going process throughout the year.
• QIPP scheme identification will be throughout the year with ideas captured as they are put forward.
• QIPP to be considered as business as usual and not limited to the end of the year
• The approach this year is to identify significantly more than the requirement (£9.5m) to offset potential slippage of milestones.
Idea generation Primarily done through the management teams and clinical teams working with finance and the Programme Management Office.
• In addition to the 14/15 approach, there will be focus on the involvement of a wider group of staff
• Some avenues will include re-launching the Bright Ideas Scheme and building on projects from staff development initiatives such as Paired Learning
Monitoring and risk adjustment:
There was variation in the planning of the schemes which resulted in loss of focus in some areas on monitoring of progress
• There will be detailed project planning for QIPP schemes and regular challenge sessions with the project leads to hold them to account for delivery.
Analysis: Improving Inpatient Care and Workforce
There could have been more analysis on the macro picture and the impact of increased levels of activity on the length of staff and workforce schemes
• Dashboards have been developed for the major programmes. These include activity changes and more detailed analysis by area/specialty.
• These dashboards are aligned to the different workstreams and will allow earlier flagging of issues
Measurement of QIPP
There was variation in the methodology applied to the of measurement and tracking of QIPP
• The finance team and PMO teams are agreeing an objective methodology for the financial tracking of schemes.
Transformation Programmes focussed on one year delivery timescales
• Under the leadership of the Transformation Committee a multi-year transformation programme will be developed that builds on the foundations delivered in Year 1.
Communication and buy in
There could have been greater visibility of the QIPP programme outside of senior management teams
• Develop and agree communication strategy on the QIPP and Transformation programme.
• Strategy to include updates on schemes through the CEO, communication briefings, PULSE articles and drop-in sessions.
Page 3
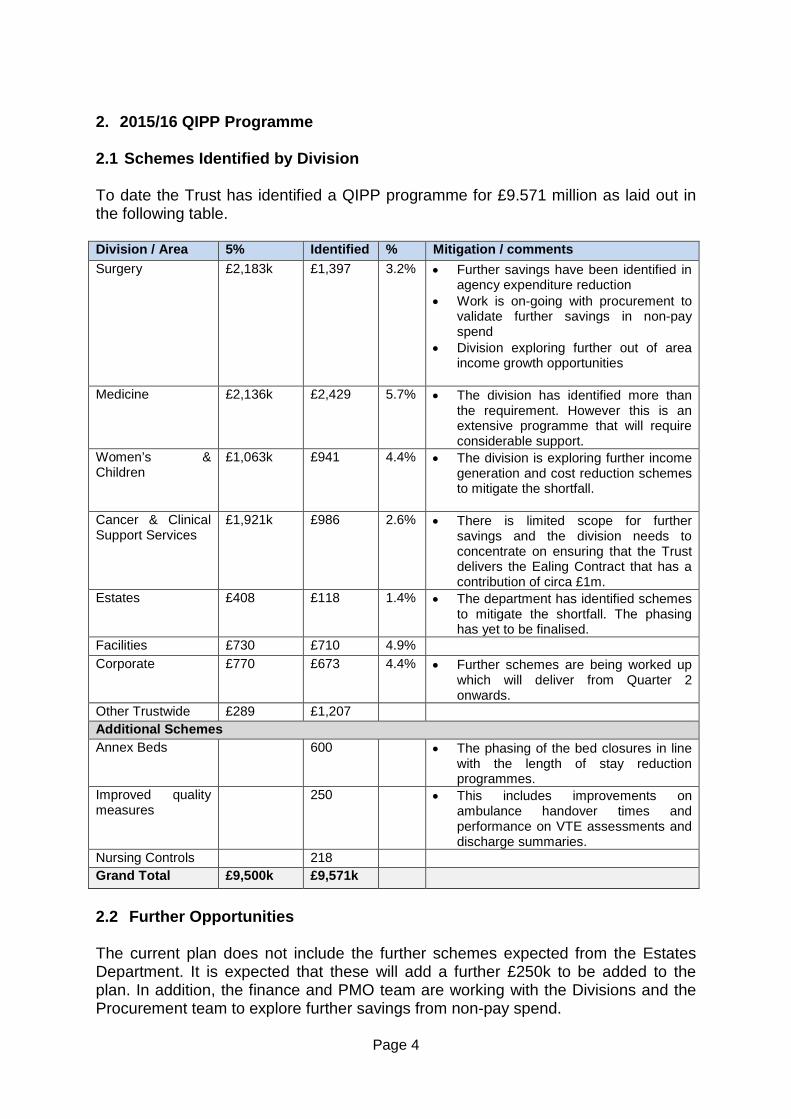
2. 2015/16 QIPP Programme 2.1 Schemes Identified by Division To date the Trust has identified a QIPP programme for £9.571 million as laid out in the following table. Division / Area 5% Identified % Mitigation / comments Surgery £2,183k £1,397 3.2% • Further savings have been identified in
agency expenditure reduction • Work is on-going with procurement to
validate further savings in non-pay spend
• Division exploring further out of area income growth opportunities
Medicine £2,136k £2,429 5.7% • The division has identified more than
the requirement. However this is an extensive programme that will require considerable support.
Women’s & Children
£1,063k £941 4.4% • The division is exploring further income generation and cost reduction schemes to mitigate the shortfall.
Cancer & Clinical Support Services
£1,921k £986 2.6% • There is limited scope for further savings and the division needs to concentrate on ensuring that the Trust delivers the Ealing Contract that has a contribution of circa £1m.
Estates £408 £118 1.4% • The department has identified schemes to mitigate the shortfall. The phasing has yet to be finalised.
Facilities £730 £710 4.9% Corporate £770 £673 4.4% • Further schemes are being worked up
which will deliver from Quarter 2 onwards.
Other Trustwide £289 £1,207 Additional Schemes Annex Beds 600 • The phasing of the bed closures in line
with the length of stay reduction programmes.
Improved quality measures
250 • This includes improvements on ambulance handover times and performance on VTE assessments and discharge summaries.
Nursing Controls 218 Grand Total £9,500k £9,571k
2.2 Further Opportunities The current plan does not include the further schemes expected from the Estates Department. It is expected that these will add a further £250k to be added to the plan. In addition, the finance and PMO team are working with the Divisions and the Procurement team to explore further savings from non-pay spend.
Page 4
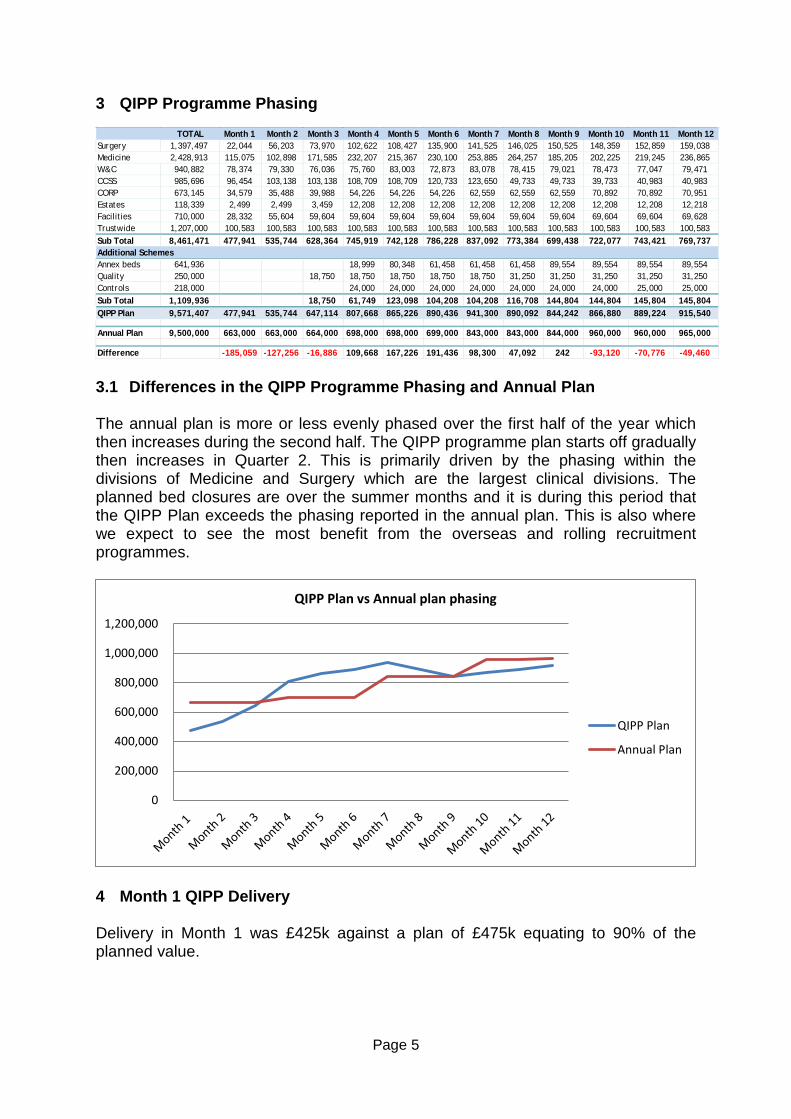
3 QIPP Programme Phasing
3.1 Differences in the QIPP Programme Phasing and Annual Plan The annual plan is more or less evenly phased over the first half of the year which then increases during the second half. The QIPP programme plan starts off gradually then increases in Quarter 2. This is primarily driven by the phasing within the divisions of Medicine and Surgery which are the largest clinical divisions. The planned bed closures are over the summer months and it is during this period that the QIPP Plan exceeds the phasing reported in the annual plan. This is also where we expect to see the most benefit from the overseas and rolling recruitment programmes.
4 Month 1 QIPP Delivery Delivery in Month 1 was £425k against a plan of £475k equating to 90% of the planned value.
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
QIPP Plan vs Annual plan phasing
QIPP Plan
Annual Plan
TOTAL Month 1 Month 2 Month 3 Month 4 Month 5 Month 6 Month 7 Month 8 Month 9 Month 10 Month 11 Month 12Surgery 1,397,497 22,044 56,203 73,970 102,622 108,427 135,900 141,525 146,025 150,525 148,359 152,859 159,038Medicine 2,428,913 115,075 102,898 171,585 232,207 215,367 230,100 253,885 264,257 185,205 202,225 219,245 236,865W&C 940,882 78,374 79,330 76,036 75,760 83,003 72,873 83,078 78,415 79,021 78,473 77,047 79,471CCSS 985,696 96,454 103,138 103,138 108,709 108,709 120,733 123,650 49,733 49,733 39,733 40,983 40,983CORP 673,145 34,579 35,488 39,988 54,226 54,226 54,226 62,559 62,559 62,559 70,892 70,892 70,951Estates 118,339 2,499 2,499 3,459 12,208 12,208 12,208 12,208 12,208 12,208 12,208 12,208 12,218Facilities 710,000 28,332 55,604 59,604 59,604 59,604 59,604 59,604 59,604 59,604 69,604 69,604 69,628Trustwide 1,207,000 100,583 100,583 100,583 100,583 100,583 100,583 100,583 100,583 100,583 100,583 100,583 100,583Sub Total 8,461,471 477,941 535,744 628,364 745,919 742,128 786,228 837,092 773,384 699,438 722,077 743,421 769,737Additional SchemesAnnex beds 641,936 18,999 80,348 61,458 61,458 61,458 89,554 89,554 89,554 89,554Quality 250,000 18,750 18,750 18,750 18,750 18,750 31,250 31,250 31,250 31,250 31,250Controls 218,000 24,000 24,000 24,000 24,000 24,000 24,000 24,000 25,000 25,000Sub Total 1,109,936 18,750 61,749 123,098 104,208 104,208 116,708 144,804 144,804 145,804 145,804QIPP Plan 9,571,407 477,941 535,744 647,114 807,668 865,226 890,436 941,300 890,092 844,242 866,880 889,224 915,540
Annual Plan 9,500,000 663,000 663,000 664,000 698,000 698,000 699,000 843,000 843,000 844,000 960,000 960,000 965,000
Difference -185,059 -127,256 -16,886 109,668 167,226 191,436 98,300 47,092 242 -93,120 -70,776 -49,460
Page 5
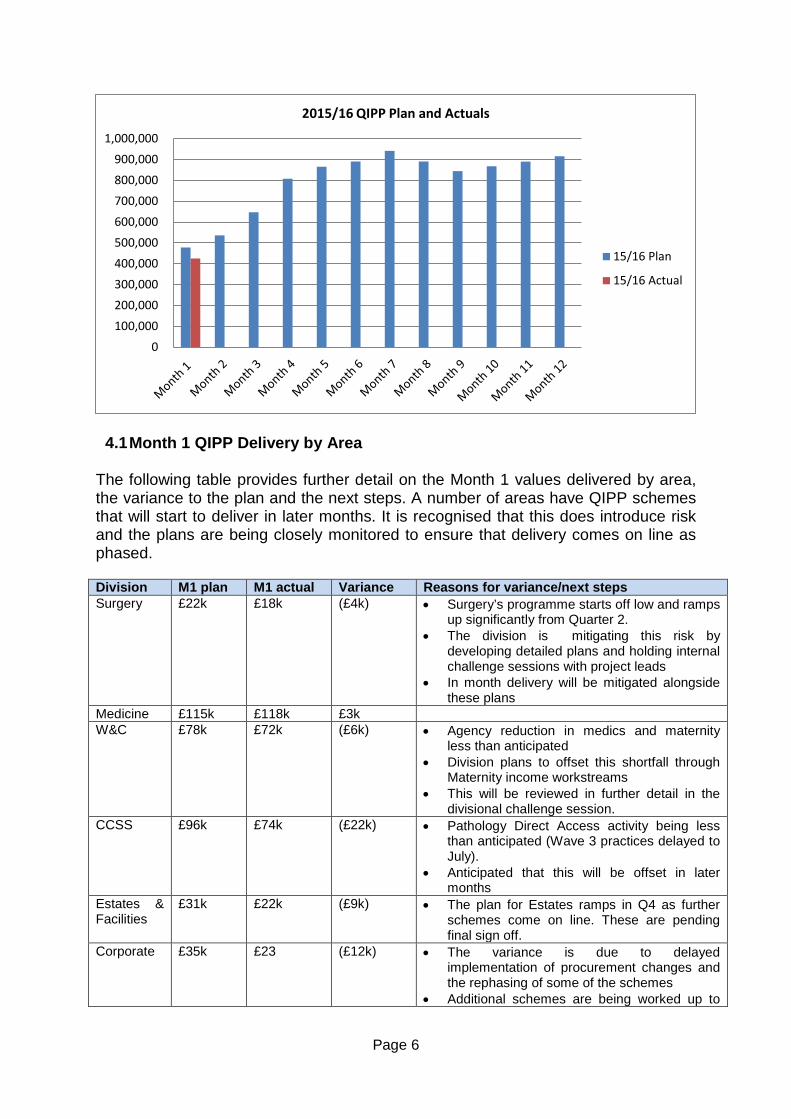
4.1 Month 1 QIPP Delivery by Area The following table provides further detail on the Month 1 values delivered by area, the variance to the plan and the next steps. A number of areas have QIPP schemes that will start to deliver in later months. It is recognised that this does introduce risk and the plans are being closely monitored to ensure that delivery comes on line as phased. Division M1 plan M1 actual Variance Reasons for variance/next steps Surgery £22k £18k (£4k) • Surgery’s programme starts off low and ramps
up significantly from Quarter 2. • The division is mitigating this risk by
developing detailed plans and holding internal challenge sessions with project leads
• In month delivery will be mitigated alongside these plans
Medicine £115k £118k £3k W&C £78k £72k (£6k) • Agency reduction in medics and maternity
less than anticipated • Division plans to offset this shortfall through
Maternity income workstreams • This will be reviewed in further detail in the
divisional challenge session. CCSS £96k £74k (£22k) • Pathology Direct Access activity being less
than anticipated (Wave 3 practices delayed to July).
• Anticipated that this will be offset in later months
Estates & Facilities
£31k £22k (£9k) • The plan for Estates ramps in Q4 as further schemes come on line. These are pending final sign off.
Corporate £35k £23 (£12k) • The variance is due to delayed implementation of procurement changes and the rephasing of some of the schemes
• Additional schemes are being worked up to
0100,000200,000300,000400,000500,000600,000700,000800,000900,000
1,000,000
2015/16 QIPP Plan and Actuals
15/16 Plan
15/16 Actual
Page 6
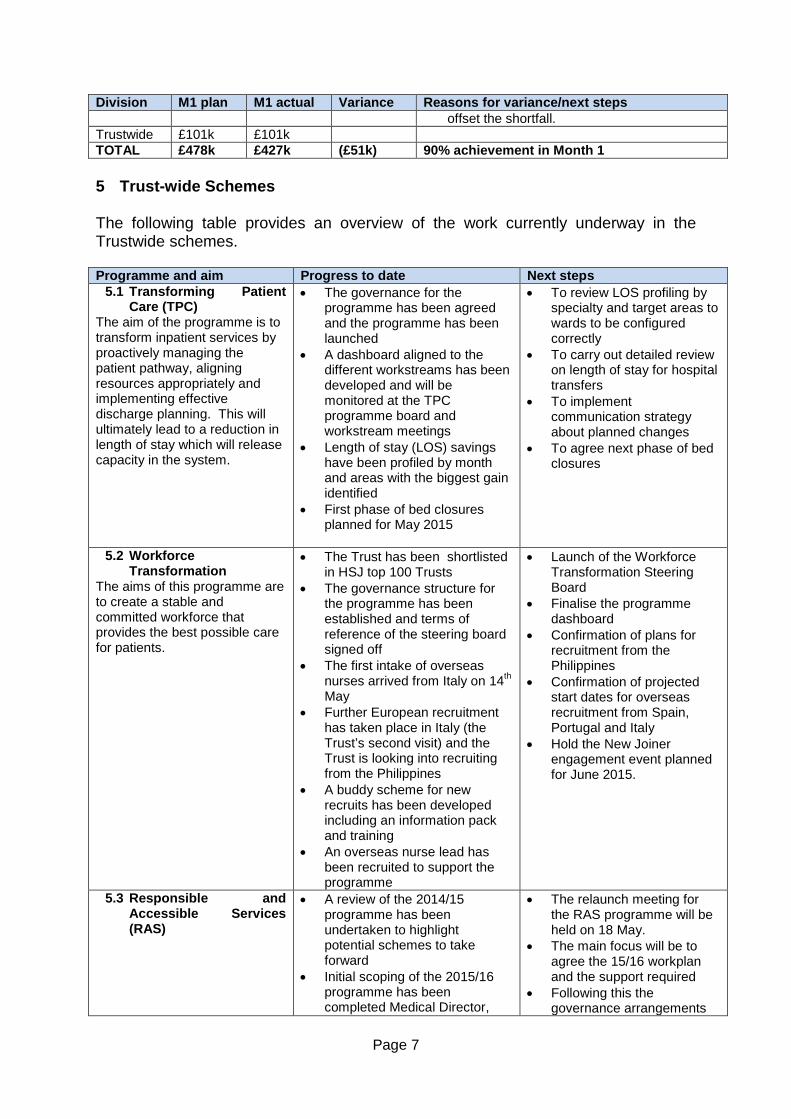
Division M1 plan M1 actual Variance Reasons for variance/next steps offset the shortfall.
Trustwide £101k £101k TOTAL £478k £427k (£51k) 90% achievement in Month 1
5 Trust-wide Schemes The following table provides an overview of the work currently underway in the Trustwide schemes. Programme and aim Progress to date Next steps
5.1 Transforming Patient Care (TPC)
The aim of the programme is to transform inpatient services by proactively managing the patient pathway, aligning resources appropriately and implementing effective discharge planning. This will ultimately lead to a reduction in length of stay which will release capacity in the system.
• The governance for the programme has been agreed and the programme has been launched
• A dashboard aligned to the different workstreams has been developed and will be monitored at the TPC programme board and workstream meetings
• Length of stay (LOS) savings have been profiled by month and areas with the biggest gain identified
• First phase of bed closures planned for May 2015
• To review LOS profiling by specialty and target areas to wards to be configured correctly
• To carry out detailed review on length of stay for hospital transfers
• To implement communication strategy about planned changes
• To agree next phase of bed closures
5.2 Workforce Transformation
The aims of this programme are to create a stable and committed workforce that provides the best possible care for patients.
• The Trust has been shortlisted in HSJ top 100 Trusts
• The governance structure for the programme has been established and terms of reference of the steering board signed off
• The first intake of overseas nurses arrived from Italy on 14th May
• Further European recruitment has taken place in Italy (the Trust’s second visit) and the Trust is looking into recruiting from the Philippines
• A buddy scheme for new recruits has been developed including an information pack and training
• An overseas nurse lead has been recruited to support the programme
• Launch of the Workforce Transformation Steering Board
• Finalise the programme dashboard
• Confirmation of plans for recruitment from the Philippines
• Confirmation of projected start dates for overseas recruitment from Spain, Portugal and Italy
• Hold the New Joiner engagement event planned for June 2015.
5.3 Responsible and Accessible Services (RAS)
• A review of the 2014/15 programme has been undertaken to highlight potential schemes to take forward
• Initial scoping of the 2015/16 programme has been completed Medical Director,
• The relaunch meeting for the RAS programme will be held on 18 May.
• The main focus will be to agree the 15/16 workplan and the support required
• Following this the governance arrangements
Page 7

Programme and aim Progress to date Next steps operational lead and PMO
will be finalised and workstream leads confirmed.
6. Hillingdon CCG (HCCG) QIPP The focus for 2015/16 for the HCCG continues to be on reducing non-elective demand in the wider sense through their Long Term Conditions Schemes, improvements to the Practice Commissioning Initiative and Integrated Care Programme and other related schemes. The Trust will be analysing in detail the HCCG assumptions that relate to the Trust to ensure alignment of the two programmes.
7. Summary There are several lessons from the 2014/15 programme that have been built into the 2015/16 programme. These include the need to identify more than the financial requirement and ensuring that QIPP planning is an on-going process. The Trust has identified a plan of £9.57m and work is ongoing to identify further schemes. Month 1 delivered £427k against a plan £475k. The divisions and corporate areas are developing actions and mitigate this shortfall and ensure delivery of the identified programme. Work is underway in the Transforming Patient Care and Workforce Transformation programmes and focus will be on ensuring that robust plans are developed that will deliver Trustwide benefits as laid out in the programme objectives.
Page 8
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 17
Complaints and PALS Annual Report Reason for item: The Local Authority Social Services and National Health Services Complaints (England) Regulations 2009, require NHS organisations to publish an annual report on complaints received by the Trust. Summary: This annual report presents information on informal concerns and formal complaints received by the Trust though the Patient Advice and Liaison Service (PALS) or via the formal complaints process between 1st April 2014 and 31st March 2015. Board Action required: The Board is asked to formally receive and comment on the Annual Complaints and PALS Report for 2014/15. Report from: Catherine Holly, Head of Patient and Public Engagement Bev Hall, Deputy Director of Nursing and Patient Experience Report sponsor: Theresa Murphy, Director of the Patient Experience & Nursing Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience and
the quality of care we provide. Previous consideration at Board or Committees: none. Equality and diversity considerations: There is no positive or negative impact from this report. Financial implications: There are no direct financial implications arising from this report.
1
Complaints and PALS Annual Report
1. INTRODUCTION The purpose of this report is to provide information on informal concerns and formal complaints received by the Trust through the Patient Advice and Liaison Service (PALS) or via the formal complaints process between 1 April 2014 and 31 March 2015. The Complaints Annual Report is produced in line with the requirements of section 18 of the NHS Complaints (England) Regulations 2009. 2. PALS
The PALS team continues to offer an on the spot open door service for patients, relatives and carers. PALS is a recognised service that users visit when seeking advice, information or wishing to raise a concern. PALS aim to be as accessible as possible to all users of the Trust’s services and can be contacted by attending the office, making a phone call or by written communication, using fax, email or letter. If an inpatient is unable to visit the office in person PALS are more than happy to visit a ward. A PALS online form is also easily accessible on the Hillingdon Hospital website inviting feedback from patients and relatives. PALS have become more proactive in visiting wards on a weekly basis, talking to carers of dementia patients to capture their feedback within the carers’ survey and ensuring that patients have had the opportunity to complete the inpatient survey during their stay and assisting those patients that have required help in doing so. A new PALS poster and leaflet have been designed and distributed around the whole of the Trust to promote the PALS and ensure that patients and relatives are aware of the support and advice that is available to them should they wish to discuss any worries or concerns. The opportunity for service users to have their compliments recorded and assurance that these are given to relevant teams has also been highlighted within the new poster. A key PALS role is to help people talk through their concerns enabling identification of the problem the patient/user is experiencing so that they may work out the various options available to resolve the issue. Those contacting PALS may initially frame their concern in the form of a complaint but the PALS staff will, with their experience, identify if the concern as a whole, or even partially, can be dealt with informally through PALS. In all cases, the choice of action should be taken by the person raising the issue. Although PALS and the Complaints Management Unit are two separate departments, there is the opportunity for dialogue between the two areas to ensure easy flow of information between the two functions and we work closely to offer a seamless service. 1,052 contacts have been recorded for the year 2014/15 compared to 1,157 contacts recorded for 2013/14.
2
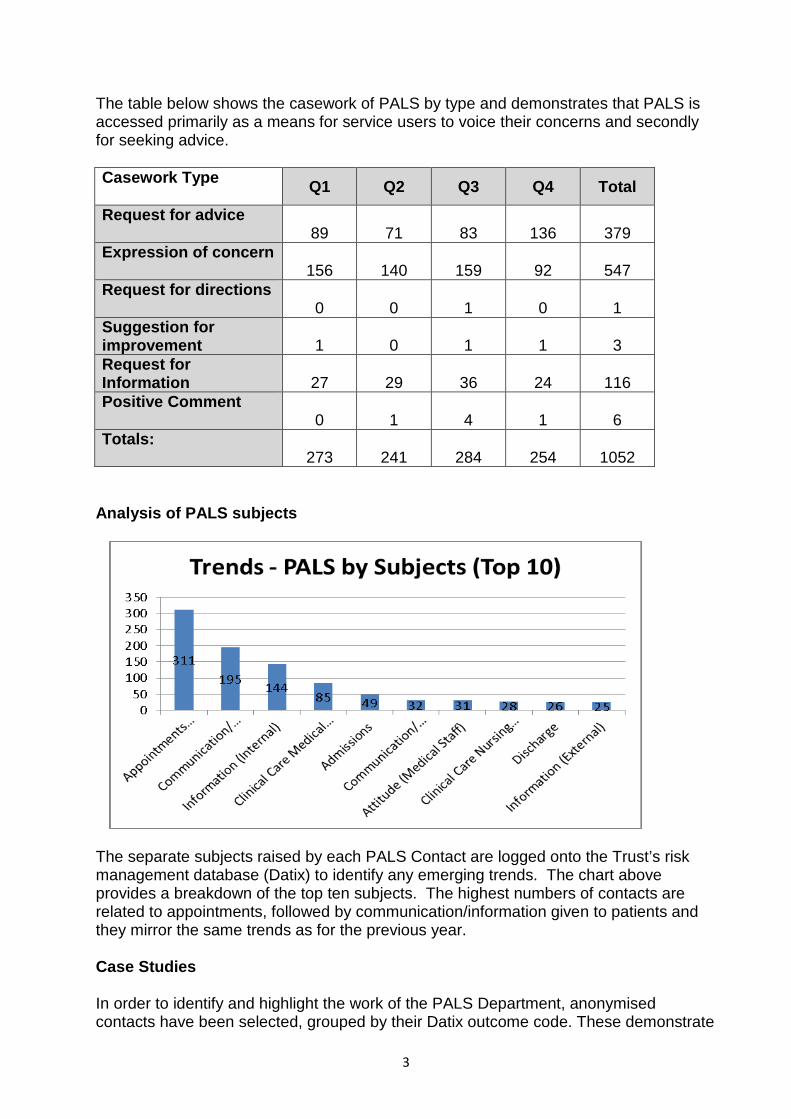
The table below shows the casework of PALS by type and demonstrates that PALS is accessed primarily as a means for service users to voice their concerns and secondly for seeking advice. Casework Type Q1 Q2 Q3 Q4 Total
Request for advice 89 71 83 136 379 Expression of concern 156 140 159 92 547 Request for directions 0 0 1 0 1 Suggestion for improvement 1 0 1 1 3 Request for Information 27 29 36 24 116 Positive Comment 0 1 4 1 6 Totals: 273 241 284 254 1052
Analysis of PALS subjects
The separate subjects raised by each PALS Contact are logged onto the Trust’s risk management database (Datix) to identify any emerging trends. The chart above provides a breakdown of the top ten subjects. The highest numbers of contacts are related to appointments, followed by communication/information given to patients and they mirror the same trends as for the previous year. Case Studies In order to identify and highlight the work of the PALS Department, anonymised contacts have been selected, grouped by their Datix outcome code. These demonstrate
3
PALS role in formal complaints avoidance where possible and their close working relationship all Trust staff. Information Given / Resolved by PALS • A patient had passed away and the carer made contact with PALS to ask if it was
possible to check the dates that bloods had been taken by the patient’s GP and sent to hospital as he had a complaint against the GP as they were disputing dates. PALS liaised with Pathology and the dates of the last four bloods taken were given, which matched those dates given to the carer by GP.
• Patient was unhappy that the consultant had said he wanted to see her in three
months for a follow up when the hospital had no availability to offer an appointment for nine months. The patient was in a great deal of pain and required steroid injections. PALS spoke with the Service Manager who explained that a specialist nurse was being trained to conduct flare up clinics. Extra clinics were being introduced and this particular patient would be added to one of those clinics.
• Son of a patient on a ward came to PALS as he had been waiting to speak with
his father’s consultant but the consultant had left the ward and the only doctor on the ward was an SHO whom the son had little confidence in. PALS phoned the consultant who explained her schedule and gave an update on the patient for PALS to relay to her son. She offered to speak with the family on her regular ward round for which the son was grateful.
Working with Trust staff to avoid a formal complaint • Patient had made contact with Watford PALS who in turn contacted THH PALS to
voice patient’s concerns that patient had anxieties regarding her neurology appointment the following day. Patient felt that she was never listened to despite the fact that she had never actually been a Hillingdon patient before. PALS had a lengthy conversation with the patient and took details from her in order to make contact with the Sister at Mount Vernon, explaining the patient’s needs and asking for their support in clinic. PALS offered reassurance to the patient and emphasised that she should call PALS again following her appointment if she needed any further support in taking her treatment forward.
• A patient’s family came to PALS to raise a number of concerns in relation to their
relative’s care which included failed monitoring and nursing standards. They raised the question of why the patient had been moved from ITU to a general ward as they did not believe the patient was well enough. PALS facilitated a meeting with the consultant who was happy to come to the PALS office and he spent a long time in discussion with the family who were happy with the explanations and reassurance given.
• Patient came to PALS asking for support in making a formal complaint as her
procedure date had been cancelled. The patient had made arrangements at work and with her family and was very angry. PALS asked for permission to discuss her case with the Surgical Manager before lodging a formal complaint. The Surgical Manager explained how the cancellation was due to an emergency and the patient was understanding and happy to accept explanation.
4
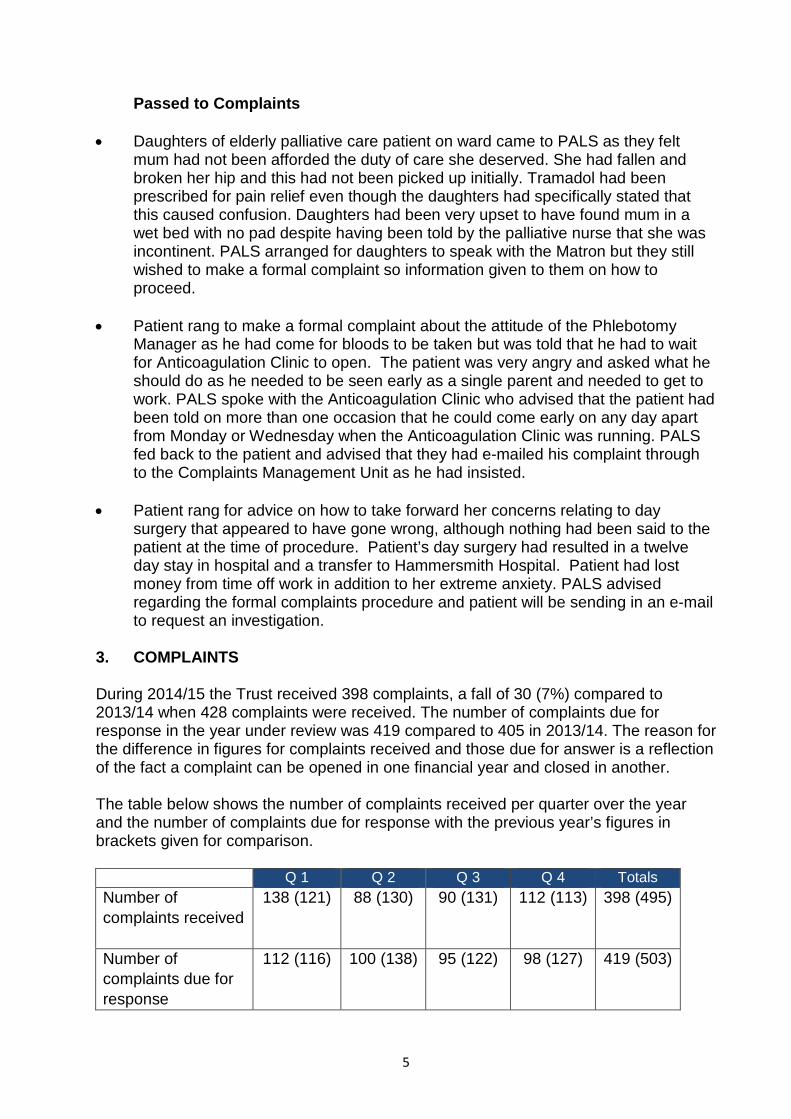
Passed to Complaints • Daughters of elderly palliative care patient on ward came to PALS as they felt
mum had not been afforded the duty of care she deserved. She had fallen and broken her hip and this had not been picked up initially. Tramadol had been prescribed for pain relief even though the daughters had specifically stated that this caused confusion. Daughters had been very upset to have found mum in a wet bed with no pad despite having been told by the palliative nurse that she was incontinent. PALS arranged for daughters to speak with the Matron but they still wished to make a formal complaint so information given to them on how to proceed.
• Patient rang to make a formal complaint about the attitude of the Phlebotomy Manager as he had come for bloods to be taken but was told that he had to wait for Anticoagulation Clinic to open. The patient was very angry and asked what he should do as he needed to be seen early as a single parent and needed to get to work. PALS spoke with the Anticoagulation Clinic who advised that the patient had been told on more than one occasion that he could come early on any day apart from Monday or Wednesday when the Anticoagulation Clinic was running. PALS fed back to the patient and advised that they had e-mailed his complaint through to the Complaints Management Unit as he had insisted.
• Patient rang for advice on how to take forward her concerns relating to day
surgery that appeared to have gone wrong, although nothing had been said to the patient at the time of procedure. Patient’s day surgery had resulted in a twelve day stay in hospital and a transfer to Hammersmith Hospital. Patient had lost money from time off work in addition to her extreme anxiety. PALS advised regarding the formal complaints procedure and patient will be sending in an e-mail to request an investigation.
3. COMPLAINTS During 2014/15 the Trust received 398 complaints, a fall of 30 (7%) compared to 2013/14 when 428 complaints were received. The number of complaints due for response in the year under review was 419 compared to 405 in 2013/14. The reason for the difference in figures for complaints received and those due for answer is a reflection of the fact a complaint can be opened in one financial year and closed in another. The table below shows the number of complaints received per quarter over the year and the number of complaints due for response with the previous year’s figures in brackets given for comparison.
Q 1 Q 2 Q 3 Q 4 Totals Number of complaints received
138 (121) 88 (130) 90 (131) 112 (113) 398 (495)
Number of complaints due for response
112 (116) 100 (138) 95 (122) 98 (127) 419 (503)
5
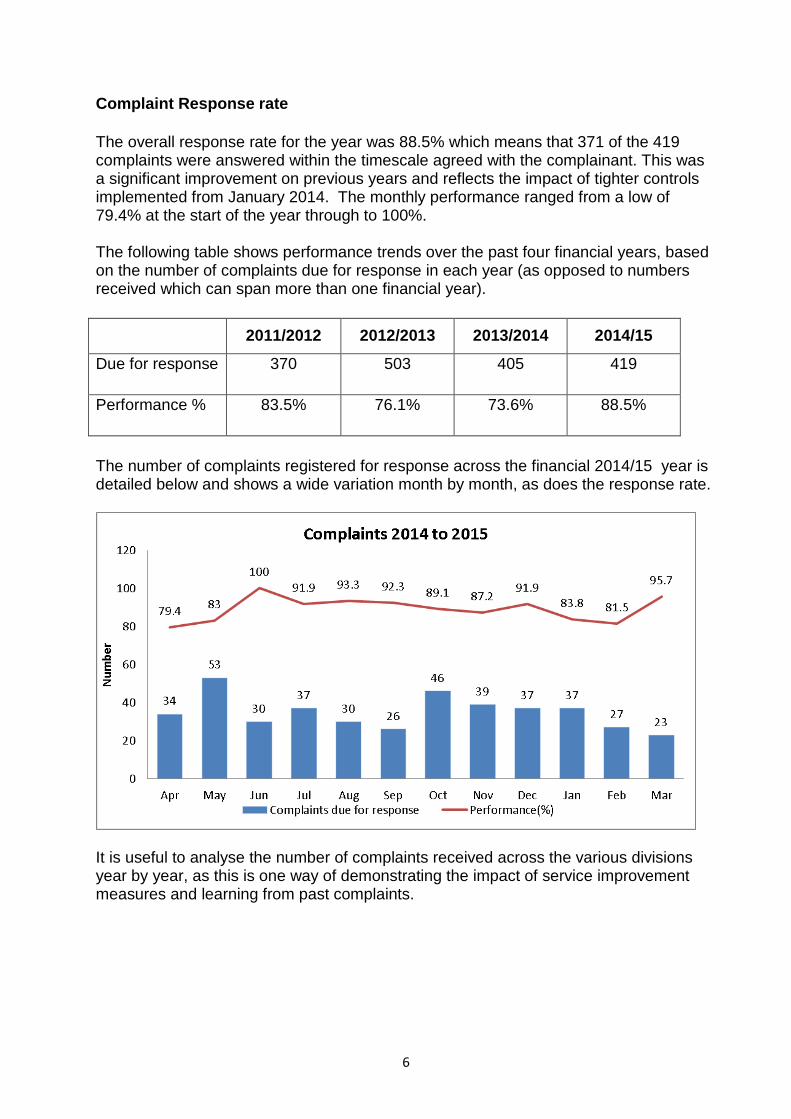
Complaint Response rate The overall response rate for the year was 88.5% which means that 371 of the 419 complaints were answered within the timescale agreed with the complainant. This was a significant improvement on previous years and reflects the impact of tighter controls implemented from January 2014. The monthly performance ranged from a low of 79.4% at the start of the year through to 100%. The following table shows performance trends over the past four financial years, based on the number of complaints due for response in each year (as opposed to numbers received which can span more than one financial year).
2011/2012 2012/2013 2013/2014 2014/15
Due for response 370 503 405 419
Performance %
83.5% 76.1% 73.6% 88.5%
The number of complaints registered for response across the financial 2014/15 year is detailed below and shows a wide variation month by month, as does the response rate.
It is useful to analyse the number of complaints received across the various divisions year by year, as this is one way of demonstrating the impact of service improvement measures and learning from past complaints.
6
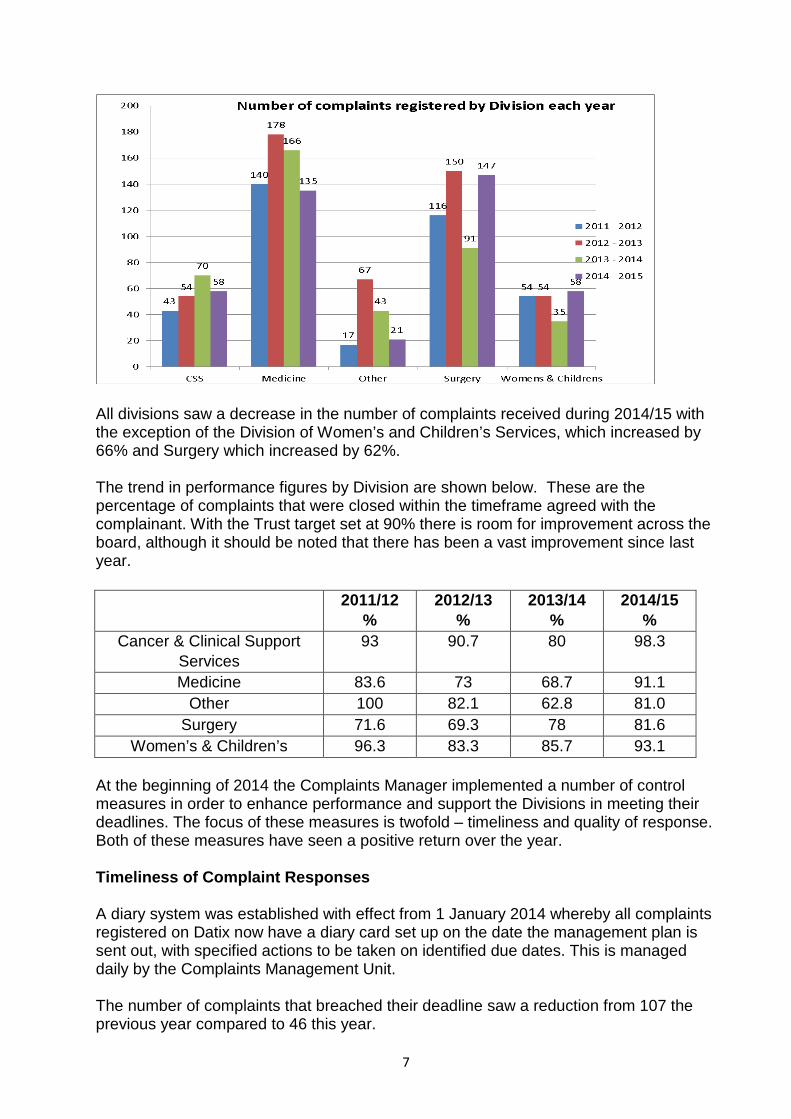
All divisions saw a decrease in the number of complaints received during 2014/15 with the exception of the Division of Women’s and Children’s Services, which increased by 66% and Surgery which increased by 62%. The trend in performance figures by Division are shown below. These are the percentage of complaints that were closed within the timeframe agreed with the complainant. With the Trust target set at 90% there is room for improvement across the board, although it should be noted that there has been a vast improvement since last year.
2011/12 %
2012/13 %
2013/14 %
2014/15 %
Cancer & Clinical Support Services
93 90.7 80 98.3
Medicine 83.6 73 68.7 91.1 Other 100 82.1 62.8 81.0
Surgery 71.6 69.3 78 81.6 Women’s & Children’s 96.3 83.3 85.7 93.1
At the beginning of 2014 the Complaints Manager implemented a number of control measures in order to enhance performance and support the Divisions in meeting their deadlines. The focus of these measures is twofold – timeliness and quality of response. Both of these measures have seen a positive return over the year. Timeliness of Complaint Responses A diary system was established with effect from 1 January 2014 whereby all complaints registered on Datix now have a diary card set up on the date the management plan is sent out, with specified actions to be taken on identified due dates. This is managed daily by the Complaints Management Unit. The number of complaints that breached their deadline saw a reduction from 107 the previous year compared to 46 this year.
7
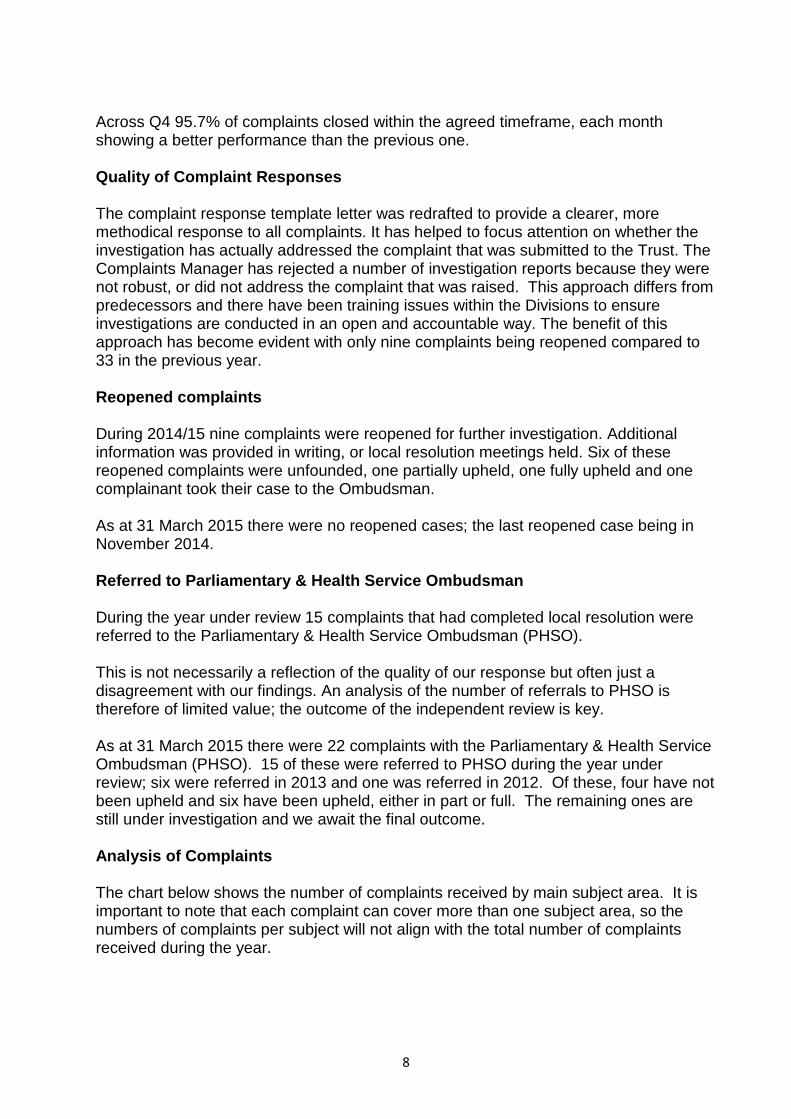
Across Q4 95.7% of complaints closed within the agreed timeframe, each month showing a better performance than the previous one. Quality of Complaint Responses The complaint response template letter was redrafted to provide a clearer, more methodical response to all complaints. It has helped to focus attention on whether the investigation has actually addressed the complaint that was submitted to the Trust. The Complaints Manager has rejected a number of investigation reports because they were not robust, or did not address the complaint that was raised. This approach differs from predecessors and there have been training issues within the Divisions to ensure investigations are conducted in an open and accountable way. The benefit of this approach has become evident with only nine complaints being reopened compared to 33 in the previous year. Reopened complaints During 2014/15 nine complaints were reopened for further investigation. Additional information was provided in writing, or local resolution meetings held. Six of these reopened complaints were unfounded, one partially upheld, one fully upheld and one complainant took their case to the Ombudsman. As at 31 March 2015 there were no reopened cases; the last reopened case being in November 2014. Referred to Parliamentary & Health Service Ombudsman During the year under review 15 complaints that had completed local resolution were referred to the Parliamentary & Health Service Ombudsman (PHSO). This is not necessarily a reflection of the quality of our response but often just a disagreement with our findings. An analysis of the number of referrals to PHSO is therefore of limited value; the outcome of the independent review is key. As at 31 March 2015 there were 22 complaints with the Parliamentary & Health Service Ombudsman (PHSO). 15 of these were referred to PHSO during the year under review; six were referred in 2013 and one was referred in 2012. Of these, four have not been upheld and six have been upheld, either in part or full. The remaining ones are still under investigation and we await the final outcome. Analysis of Complaints The chart below shows the number of complaints received by main subject area. It is important to note that each complaint can cover more than one subject area, so the numbers of complaints per subject will not align with the total number of complaints received during the year.
8
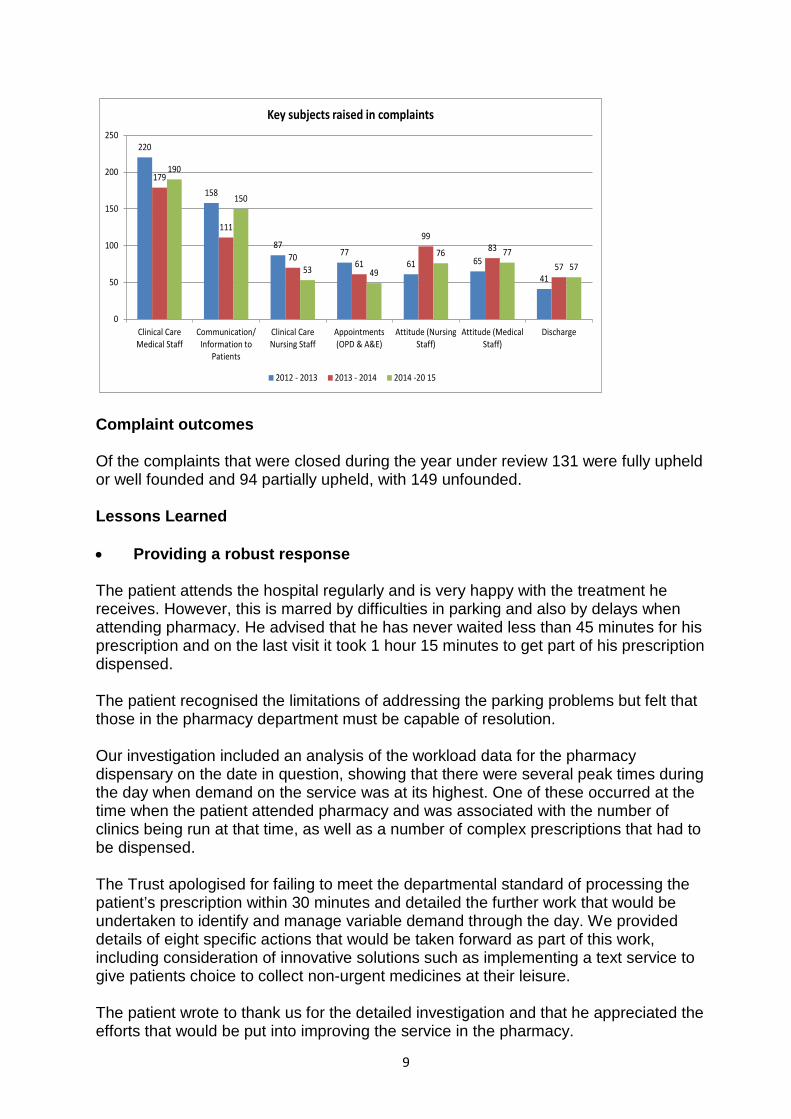
220
158
8777
61 65
41
179
111
7061
9983
57
190
150
53 49
76 7757
0
50
100
150
200
250
Clinical CareMedical Staff
Communication/Information to
Patients
Clinical CareNursing Staff
Appointments(OPD & A&E)
Attitude (NursingStaff)
Attitude (MedicalStaff)
Discharge
Key subjects raised in complaints
2012 - 2013 2013 - 2014 2014 -20 15
Complaint outcomes Of the complaints that were closed during the year under review 131 were fully upheld or well founded and 94 partially upheld, with 149 unfounded. Lessons Learned
• Providing a robust response The patient attends the hospital regularly and is very happy with the treatment he receives. However, this is marred by difficulties in parking and also by delays when attending pharmacy. He advised that he has never waited less than 45 minutes for his prescription and on the last visit it took 1 hour 15 minutes to get part of his prescription dispensed. The patient recognised the limitations of addressing the parking problems but felt that those in the pharmacy department must be capable of resolution. Our investigation included an analysis of the workload data for the pharmacy dispensary on the date in question, showing that there were several peak times during the day when demand on the service was at its highest. One of these occurred at the time when the patient attended pharmacy and was associated with the number of clinics being run at that time, as well as a number of complex prescriptions that had to be dispensed. The Trust apologised for failing to meet the departmental standard of processing the patient’s prescription within 30 minutes and detailed the further work that would be undertaken to identify and manage variable demand through the day. We provided details of eight specific actions that would be taken forward as part of this work, including consideration of innovative solutions such as implementing a text service to give patients choice to collect non-urgent medicines at their leisure. The patient wrote to thank us for the detailed investigation and that he appreciated the efforts that would be put into improving the service in the pharmacy.
9
• Improvements arising from Complaints A complaint about delays to appointment in the podiatry service prompted a review of the patient pathway through the podiatry service in Diabeticare. The root cause of delays was identified as inflexibility in how plaster casts were managed; the patient was not being put at the centre of service delivery. To avoid these patients being transported around the hospital, some diabeticare staff are being trained to remove plaster casts or a Plaster Technician attends the Diabeticare clinic. User Satisfaction Survey During 2014/15 the Complaints Management Unit introduced a user satisfaction survey which is sent to all complainants once their complaint has closed. Complainants are asked how they made contact with the Complaints department and then asked about their experience of using the service. The following graph demonstrates that over half of all complaints are in writing by letter.
The following results of the user satisfaction survey demonstrate that complainants are generally happy at receiving a phone call to discuss their complaint and to agree a timescale for the investigation. Complainants appear less satisfied with other areas of the complaints process relating to helpfulness of staff when raising a complaint, having confidence that staff have understood the complainant and being reassured that a thorough investigation has been undertaken or that corrective action would be taken following the investigation. Less than half of all complainants felt confidence that raising concerns would not lead to discrimination. Although the response rate so far has been low, the results help to us to understand the complainants’ experience and support continuous learning and improvement with the service. Question
Satisfaction
Received a call to discuss complaint and timescales
97%
Happy with timeframe
86%
Helpfulness of staff when raising a complaint
73%
Confidence that staff spoken to understood the complaint 68%
10
Reassured that corrective action would be taken
60%
Reassured that a thorough investigation had been undertaken
56%
Confidence that raising concerns would not lead to discrimination
49%
Future Plans • Provide reassurance that future health care will not be affected as a result of raising
a complaint; this can be carried out during the initial acknowledgement phone call and in writing when responding to the complainant.
• Amend user satisfaction survey to include a box for free text comments. • Schedule regular meetings between the Complaints Manager and the divisional
management teams to agree how they can best work together to improve the complaint handling process.
• Review and amend the Complaint Investigation Report and Plan to include the new risk matrix.
• Undertake a review of training requirements and consider developing an e- learning training package.
4. CONCLUSION This report has provided the Trust Board with an update on the Complaints and the Patient Advice and Liaison Service (PALS). The report outlines a reduction in PALS contacts, an increase in formal complaints and an increase in the number of complaints referred to the Ombudsman. The report provides examples of actions taken/learning following patient/user feedback. Complaints handling and learning from feedback remains high profile. Going forward the Trust will work towards providing a seamless responsive service that demonstrates the Trust’s commitment to listen and to learn and to ‘put people first’ in order to improve the quality of care and the patient experience.
11
Meeting of the Board of Directors – public session
Wednesday 29th May 2015 Agenda item 18
Safeguarding Adults and Children Reason for item: This report brings together information requested by the Board and Audit & Assurance Committee to highlight the Care Act 2014, revisions to Working Together to Safeguard Children (2015) and the new guidance related to Female Genital Mutilation (FGM). Summary: This paper outlines three main areas, demonstrating the Trust’s current position and the next steps. The report outlines: 1. An overview of statutory requirements for adult and children safeguarding. 2. Key actions taken in response to the CQC and TIAA internal audit. 3. New guidance relating to Female Genital Mutilation (FGM) and the Trust’s actions to
implement this. The report highlights the extensive range of actions taken since the CQC inspection and internal audit into safeguarding, including increased training uptake and strengthening of safeguarding processes. Board Action required: The Board is asked to: 1. Review the information provided and the actions in place to safeguard adults and
children 2. Agree any further actions that are required. Report from: Bev Hall, Deputy Director of Nursing Report sponsor: Theresa Murphy, Director of the Patient Experience Nursing Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience
and the quality of care we provide. Previous consideration at Board or Committees: none Equality and diversity considerations: None Financial implications: Business cases are being written to support the creation of a Child Safeguarding Advisor role and to extend the Safeguarding Administrator position beyond the current six months non-recurrent funding.
1
Safeguarding Adults and Children 1. Introduction This report provides an update to the Board on changes in requirements relating to safeguarding – The Care Act 2014, Revisions to Working Together to Safeguard Children 2015, and Female Genital Mutilation advanced data set reporting – setting out the Trust’s current position and next steps. The paper also outlines progress on actions following the TIAA internal audit on safeguarding children and the recent CQC inspection report, including the Mental Capacity Act and Deprivation of Liberty Safeguards. 2. Overview of Statutory Requirements adult and children safeguarding 2.1 Adult Safeguarding Under The Care Act 2014, which replaces ‘No Secrets’ and puts adult safeguarding on a legal footing, from April 2015 each Local Authority (LA) must:
• Make enquiries, or ensure others do so, if it believes an adult is subject to, or at risk of, abuse or neglect. An enquiry should establish whether any action needs to be taken to stop or prevent abuse or neglect, and if so, by whom.
• Safeguarding Adults Board (SAB) should be in in place, with core membership from the local authority, the Police and the NHS (specifically the local Clinical Commissioning Group/s) and the power to include other relevant bodies.
• Arrange, where appropriate, for an independent advocate to represent and
support an adult who is the subject of a safeguarding enquiry or Safeguarding Adult Review (SAR) where the adult has ‘substantial difficulty’ in being involved in the process and where there is no other appropriate adult to help them co-operate with each of its relevant partners in order to protect adults experiencing or at risk of abuse or neglect.
• The statutory guidance also introduces Designated Adult Safeguarding
Managers (DASMs) in organisations concerned with adult safeguarding. The Care Act (2014) extends the scope of adult safeguarding. The LA duty now applies whether or not the adult is ordinarily resident in the LA, and whether or not the LA is meeting any of the adult’s care and support needs. Local Authorities must follow up any concerns about actual or suspected adult abuse. SABs will have more powers than under current arrangements, but will also be more transparent and subject to greater scrutiny. All organisations who are involved in adult safeguarding training will need to reflect the Act’s statutory guidance and good practice guidance when developing and implementing their staff training programmes.
2
The Care Act (2014) also recognises three additional categories of abuse in relation to safeguarding:
• Domestic Violence/abuse • Modern slavery • Self-neglect: • Organisational Abuse (formerly referred to institutional abuse).
There have been a number of high profile hospital scandals that have highlighted the need for vigilance and action among staff and managers. The Act therefore sets out that CQC registration requirements would introduce a duty of candour which would place a duty on providers to be open with patients and their families about failings in their care. The NHS has particular duties for patients less able to protect themselves from harm, neglect or abuse. All commissioners and contractors have a responsibility to ensure that service specifications, invitations to tender, service contracts and service level agreements promote dignity in care and adhere to local multi-agency safeguarding policies and procedures. Commissioners must also assure themselves that care providers know about and adhere to relevant CQC standards. Contract monitoring must have a clear focus on safeguarding and robustly follow up any shortfalls in standards or other concerns about patient safety. NHS managers, commissioners and regulators will want assurance that when abuse or neglect occurs, responses are in line with local multi-agency safeguarding procedures, national frameworks for Clinical Governance and investigating patient safety incidents. Therefore these services must produce clear guidance to managers and staff that sets out the processes for initiating action and who is responsible for any decision making. To prevent cases falling through the net, the NHS and the local authority should have an agreement on what constitutes a ‘serious incident’ and what is a safeguarding concern and appropriate responses to both. Current Position at THH: • THH is well represented on the Hillingdon Safeguarding Adults Board • Mandatory safeguarding adults training and materials are being reviewed and
updated to ensure that they are compliant with the Act • The Designated Safeguarding Adults Manager role is likely to be the
Safeguarding Lead Nurse.
Next Steps: • A multi-agency Care Act (2014) workshop is being arranged by LBH, this will
ascertain how the Act will be implemented in an integrated way • The Safeguarding Lead Nurse will need to work closely with the LA and the CCG
to inform their agreement about definitions of a serious incident and a safeguarding concern
• Work with Communications team to develop a campaign for early in quarter 2 to
3
inform our staff of the key changes and their duties under the Act • Our local policy and procedures is being reviewed and updated to take account of
this new legislation 2.2 Revisions to Working Together to Safeguard Children March 2015 Following consultation the Government has updated and replaced the current statutory guidance Working Together to Safeguard Children revised and published in 2013. The revisions include changes to: 2.2.1 The referral of allegations against those who work with children; The proposal was that allegations against people who work with children should be routed through children’s social care, so that they are dealt with alongside child welfare concerns in a coordinated manner, e.g. MASH (Multi-Agency Safeguarding Hub). New guidance no longer refers to ‘Local Authority Designated Officer (LADO)’ but says ‘Local authorities should have designated a particular officer, or team of officers (either as part of multi-agency arrangements or otherwise)’. All new appointees to LADO should be qualified social workers, unless an existing LADO is moving between authorities. From March 2015, local authorities should have designated a particular officer, or team of officers (either as part of multi-agency arrangements or otherwise), to be involved in the management and oversight of allegations against people that work with children. Current Position at THH: • Trust flow chart for managing allegations against staff members is in place • Head of Safeguarding and Named Nurse have had an initial meeting with
Safeguarding HR manager, and local authority interim LADO, with a further meeting planned at the end of May to review process in line with revised guidance
• Level 1 and 2, Safeguarding Children Training by Named Nurse for Safeguarding Children incorporates information about allegations against people working with children and families
• The Named Nurse for Safeguarding Children has given a presentation to the Divisional Assistant Directors of Operations to raise awareness about allegations against staff working with children and families and their responsibilities in the management of such an allegation.
Next Steps: • The Trust flow chart will be reviewed and revised to clearly indicate roles and
responsibilities • Head of Safeguarding and Named Nurse will consider the value of writing a
concise policy to support flow chart or integrate this information into the existing policy
4
• Training will be updated after the flow chart has been reviewed and revised to include clear roles and responsibilities
2.2.2 Notifiable Incidents A notifiable incident is an incident involving the care of a child which meets any of the following criteria:
• A child has died (including cases of suspected suicide), and abuse or neglect is known or suspected;
• A child has been seriously harmed and abuse or neglect is known or suspected
• A looked after child has died (including cases where abuse or neglect is not known or suspected); or
• A child in a regulated setting or service has died (including cases where abuse or neglect is not known or suspected)
For the avoidance of doubt, if an incident meets the criteria for a Serious Case Review then it will also meet the criteria for a notifiable incident. There will, however, be notifiable incidents that do not proceed through to Serious Case Review. 2.2.3 Definition of serious harm for the purposes of serious case reviews Working Together 2015 now provides a definition of ‘seriously harmed’. There were concerns that some Local Safeguarding Children Boards (LSCBs) were failing to make appropriate decisions on what constituted serious harm. It is also hoped the new wording will help support local authority decision-making when determining whether to notify an incident. Next Steps:
• Trust policy will be amended to reflect the notifiable incidents and the definition of seriously harmed
3. Key actions taken in response to the CQC Inspection and TIAA internal
audit TIAA produced their report following a Review of Safeguarding children in December 2014. The scope of the audit was to review arrangements in place for safeguarding children, with a focus on Paediatric A&E and staff training. The overall assurance statement assessment was one of reasonable assurance, with five important action points and two routine action points. The recent CQC Inspection Report, published in February 2015 also identified some areas of practice related to safeguarding where the Trust needed to make improvements, including four ‘must do’ actions. Some of the areas highlighted in the TIAA audit also featured in the CQC report. Key actions/outcomes are highlighted below:
• The UCC data sharing agreement has been in place since 30th April, and data has been flowing from the UCC onto the i-reporter web page from 5th May. A section for adults has also been included. MIU will also have access. This will
5
ensure that information on previous UCC attendances is available shared with A&E staff.
• Safeguarding training compliance: o Adults: 94% o Children level 1: 94% o Children level 2: 90% o Children level 3: 93.5%
• All staff working directly with children should be able to receive Safeguarding Children Supervision. Safeguarding Children Supervision Training will be delivered in June. Staff attending will be able to give both planned and adhoc supervision to their colleagues.
• The trained supervisor will also be Safeguarding Children Champions for their department.
• Monitoring of the supervision will be done through a database managed by the safeguarding children team.
• Electronic minutes with action log had already been planned and were commenced in early October 2014.
• Notes and actions from Safety Net meetings are recorded electronically and all meetings start with a review of the action log and progress made. New actions are recorded with a responsible member of staff and expected date of completion.
• Named Nurse has a detailed overview of safeguarding children datix incident reports, ensuring that they are acted upon as required, closed in a timely manner and that learning is shared and minimises reoccurrence.
• Daily procedure of note checking for all children under 18 presenting to A&E lead by Consultants and senior nurses has been introduced.
• Colour coding of under 18 A&E notes and revision of child safeguarding checklist to ensure all staff receives safeguarding prompts for under 18s.
• Learning from incidents is incorporated into training. • Child sex exploitation and female genital mutilation have been included in the
policy. • Learning from the Daniel Pelka Serious Case Review has been shared at the
March Safeguarding Committee. • Safeguarding Administrator in post , funding secured for six months.
New robust procedures are highlighting that there is a need for expansion of the child safeguarding team. Business cases are being written to support the creation of a Child Safeguarding Advisor role and to extend the Safeguarding Administrator position beyond the current six months non recurrent funding. 4. Mental Capacity Act & Deprivation of Liberty Safeguards The CQC Inspection report also identified concerns related to staff’s understanding and application in practice of the Mental Capacity Act and Deprivation of Liberty Safeguards (MCA & DoLS). Current Position:
• Enhanced MCA and DoLS training programme established for 2015.
6
• Training Needs analysis (TNA) undertaken, this will be reviewed regularly. • Awareness of MCA and DoLS at a level appropriate to role has been
integrated into existing training programmes including mandatory safeguarding and nurse induction.
• Training monitored via WIRED. • MCA and DoLS policy ratified in February 2015. • Development of a DoLS database to monitor and report on DoLS applications
and outcomes. • Clinical areas have undertaken a risk assessment where there is a controlled
exit keypad. • Clear signage is positioned next to controlled exit keypads. • Revised Restraint policy for clinical staff ratified in February. • The Social Care Institute for Excellence framework for arrangements to put
DoLS into practice has been adopted. A gap analysis on current Trust arrangements against these standards has helped to identify where additional requirements are required. Actions with timescales are planned
5. Female Genital Mutilation (FGM) The Trust reported 57 new cases of FGM in 4 months; as such were the tenth highest reporting Trust in London. Mandatory requirements It is required that all acute Trusts to record and submit data via the Clinical Audit Platform (CAP) on FGM using the FGM Enhanced Dataset from 1st June 2015.
• All clinicians, regardless of organisation type, to record in clinical notes when FGM is identified, and what type it is following clinical examination.
• All Maternity Discharges, must include relevant FGM information identified, prior to and post-delivery of baby, informing the GP and Health Visitor of the FGM identified during the provision of care.
• All babies born to a mother with FGM must have the relevant FGM information recorded in the baby’s patient healthcare record (GP records and parent child health record (red book)) to help identify the potential risk of FGM facing the girl. A risk assessment has been developed to identify the level of risk.
• DH is issuing an information leaflet for women on FGM. • Safeguarding issues, requirement to report all cases of FGM in girls/women
under the age of 18 to the police by the clinician within 1 month. Submitting FGM Information The FGM Enhanced Dataset collection will specifically require the stated organisations to return detailed FGM information for each patient. The dataset is extremely extensive, including demographic data, history of where/ when FGM was performed, number of daughters, details of FGM type and reversal etc. Data is currently being entered onto the system however the information is being reported by maternity and gynaecology. Currently the data is being entered once but
7
a new attendance record is meant to be generated for each contact with a clinician. However this is resource intensive. Training requirements All clinicians throughout the organisation will require training in FGM; this could be a CQUIN for the organisation in 2016. This is because every woman with FGM needs to be risk assessed and informed of the health and legal implications of FGM by the clinician. Resources There is no extra funding from NHS England to support the implementation of the FGM enhanced dataset. The resources required are:
• Training clinicians across the organisation (e-learning package is available). Learning and development have been asked to have an additional section under safeguarding adults for FGM so that the Trust can capture the training data.
• Inputting data from every section of the Trust. • An IT solution for capturing information across the Trust so that women with
FGM are not repeatedly asked the same questions. Other Trusts have used the pathology system ICE or a modified form of the datix incident reporting system to capture this data.
• Changes in current systems to include information in discharges for general practitioners, health visitors and other health professionals.
• Consideration whether a clinic is required for women with FGM.
Current position in Maternity Procedures have been modified over the last eight weeks in order to improve compliance with national guidance; Maternity uses the “Euroking” software package to record data at all stages of pregnancy and in some cases to communicate with allied professionals.
• “FGM Yes/No” now appears as a standalone question at the ante-natal booking visit. If answered yes, further questions regarding type of FGM, reversal etc appear.
• The booking midwife is expected to complete the enhanced dataset FGM pro-forma for each woman with an identified FGM. This data is then inputted centrally.
• The booking midwife is expected to provide information on the health and legal aspects of FGM (via website/ leaflet).
• Post-natally midwives are recording “family history of FGM” in parent child health record (red book).
• They are also writing in the comments section of the postnatal discharge that the mother has FGM, in order to communicate with GP and health visitor as per national guidelines
• Education on FGM being provided to all midwives at monthly risk study day
8
Ongoing Work in Maternity
• FGM history to be included on printed ante-natal booking summary, to be sent to GP and health visitor.
• Aim for an automated letter to be produced via Euroking at time of post-natal discharge, detailing history of FGM, sex of the child and documenting that information has been provided on the health and legal implications.
• Safeguarding processes and documentation being improved (work in tandem with project to go “paperless” at maternity booking and use Euroking to full potential)- including advice to refer all women under the age of 18 with identified FGM to be referred to safeguarding midwives.
• Departmental FGM guideline to be updated by end of July. • Move towards online DH FGM training becoming part of mandatory
departmental requirements. Further Work Monthly meetings are occurring within maternity, with regards to the above processes. A Trust representative will be attending a meeting at Hillingdon Council on 20th May to work towards setting standards and procedures regarding FGM across multi-agencies within the Local Authority. This information will be shared with the Trust working group. A Trust-wide working group has also been set up involving relevant specialities, safeguarding and nursing leads, with a next meeting due 27th May. The focus for this meeting will be to learn from Maternity who are trail blazing in relation to reporting the enhanced dataset and plan for full implementation of reporting across all specialities.
9
Meeting of the Board of Directors – public session
Wednesday 27th May 2015
Agenda item 19 Health and Safety Policy Reason for item: This policy is coming to the Board as the Trust’s Health and Safety Policy has to be approved by the Board of Directors. This is because the Board should set the direction for effective health and safety management in the Trust. Summary: Health and safety law places duties on organisations and employers. Directors can be personally liable when these duties are breached. Members of the Board have both collective and individual responsibility for health and safety in the Trust. Board members need to establish a health and safety policy that is an integral part of the Trust’s culture, values and performance standards. All Board members should take the lead in ensuring the communication of health and safety duties and responsibilities throughout the Trust. The revised policy (attached) sets out the Board’s own role and that of individual Board members in leading health and safety in the Trust (Health and Safety Executive INDG417). The policy has been amended to reflect the recent Executive portfolio restructuring. Board Action required: The Board is asked to approve the attached policy. Report from: Sue Manthorpe, Assistant Director Health and Safety Report sponsor: Paul Wratten, Finance Director Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience
and the quality of care the Trust provides. • To deliver high quality care in the most efficient way. Equality and diversity considerations: None. Financial implications: Failure to comply with health and safety legislation can lead to litigation, financial penalties and significant cost to restore compliance.
The Health and Safety Management Policy
Policy Number: 62 Version: 7.0 Category Health and Safety Authorisation Committee/Group Health and Safety Committee Date of Authorisation: April 2015 Ratification Committee: Trust Board Date of Ratification Author name and Job Title : Sue Manthorpe, Assistant Director,
Health and Safety Sponsor Name and Job Title Paul Wratten, Executive Director of
Finance Date issued: Next version date: Review period: 3 years Scope Trust-wide This policy has been Equality Impact Assessed
Yes
Uncontrolled once printed. It is your responsibility to check against the intranet that this printout is the most recent version of this document. Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 1 of 34
Record of changes to this document
Version & Section Number
Amendment Date of Change
Change/ Addition
Reason
V5 section 3
Responsibilities June 2011
Updated to reflect Foundation Trust status
V6 Policy statement
Updated with current CEO
March 2013
Removal of previous CEO name and insertion of current CEO name
Change of CEO
V6 section 3
Responsibilities March 2013
Clarified roles Following recent H&S audit clarification of senior management roles
V6 section 3.8
Co-operation of shared sites
March 2013
Shared site health & safety arrangements
Clarification of process
V6 section 4
Monitoring of the policy
March 2013
Update of monitoring table
Continue to meet NHSLA/CNST requirements
V6.1 section 5.1
Audits and Inspections
Sept 2014
Insertion of the inspection checklist
Updated following health and safety internal audit recommendations
V6.1 App 2 Terms of Reference (TOR)
Sept 2014
Updated TOR Following QRC recommendations
V6.1 Front Sheet Sept 2014
Executive Director Name and Title
Due to change of Executive Director
V6.1 Section 5.1
Inspection Checklist
Sept 2014
Inspection checklist and H&S
References needed to be made to its use and monitoring
V7.0 Complete review March 2015
Updates to legislation e.g. CDM
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 2 of 34
Dissemination and Consultation with Stakeholders
Disseminated to (either directly or via meetings, etc.)
Position of Stakeholder or Name of Endorsing
Committee
Format (paper or
electronic)
Date
Sue Manthorpe Chair of Health & Safety Committee
Electronic June 2011
Clinical Governance Committee
Electronic June 2011
Health & Safety Committee Electronic April 2013 Health & Safety Committee Electronic April 2015
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 3 of 34
Contents
Section Page Operational Summary 5 Policy Statement 6
1 Purpose 7 2 Explanation of Terms 7 3 Duties 7 4 Practical Arrangements 17
4.1 Equipment, Materials and Substances 17 4.2 Accident/Incident reporting & Investigations 17 4.3 Risk Assessment 18 4.4 Provision of Information to Employees 18 4.5 First Aid Provision 19 4.6 Emergency Procedures and Business Continuity Plans 19 4.7 COSHH 19 4.8 Co-Operation of Shared Sites 20 4.9 Training 20
4.10 Selection of Contractors 20 5 Monitoring, Auditing and Review 21
5.1 Audits 21 5.2 Review of this Policy 21 5.3 Archiving Arrangements 22 5.4 Equality Impact Assessment 22 5.5 NHS Constitution 22 5.6 Monitoring 23
Appendices Appendix 1: Equality Impact Assessment 24 Appendix 2: Health and Safety Committee Terms of Reference 25 Appendix 3: General Safety Rules 28 Appendix 4: Policy Checklist 32
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 4 of 34
Operational Summary Policy Aim The policy supports the Trust’s Health and Safety Strategy and its aims are:
• To describe the Trusts beliefs, values and responsibilities for ensuring a safe and healthy workplace for all persons on Trust premises, increasing staff wellbeing and reducing risks through the provision of it services.
• To ensure that everyone is aware of the Trust’s and their own responsibilities under the Health and Safety at Work etc. Act 1974. And all associated legislation
Policy Summary The Policy consists of three sections: 1 Policy General Statement of Intent. The Policy Statement of intent is the written declaration by the Chief Executive on behalf of the Trust’s Board, as to the Trust’s intentions with regard to the health, safety and welfare of Trust employees and others who may be affected by the Trust’s operations. This Statement of Intent is produced in accordance with section 2(3) of the Health and Safety at Work (etc) Act 1974 and shall be bought to the attention of all employees. 2 General Responsibilities This section deals with personal responsibility for health and safety and welfare at work. Everyone from the Chief Executive to each and every employee will have responsibilities in implementing this policy 3 Practical Arrangements This section covers the policies and/or procedures which have been or will be introduced to make sure that the policy is implemented. It includes procedures for the recognition of hazards, investigating accidents and incidents and arrangements for dealing with emergencies. What it means for staff Everyone employed by the Trust has a legal duty to cooperate in matters of health and safety which includes complying with the requirements of this policy. It is therefore essential that all staff familiarise themselves with this policy and the promotion of its implementation. Assistant Directors of Operations /Dept Heads/Ward and Department Managers – are responsible for ensuring adequate dissemination and implementation of policies. In the event of an infection outbreak, flu pandemic or major incident, the Trust recognises that it may not be possible to adhere to all aspects of this document. In such circumstances, staff should take advice from their manager and all possible action must be taken to maintain patient and staff safety. Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 5 of 34
Health and Safety Policy General Statement of Intent It is the policy of The Hillingdon Hospitals NHS Foundation Trust to comply with the requirements of the ‘Health and Safety at Work (etc.) Act 1974’ and any other health and safety legislation that may from time to time be introduced and be relevant.
The Trust recognises that high standards of health, safety and welfare are an integral element of efficient management objectives and contribute to the overall operational success of the Trust. It is committed to the continuous improvement in occupational health and safety and environmental matters that may affect staff, patients, volunteers, contractors and members of the public. Health and Safety is a management responsibility of equal importance to all other objectives therefore Executive Directors and all managers will ensure that risks are reduced and improvements in health and safety performance are established by maintaining and communicating the necessary health and safety and risk information, providing appropriate training and encouraging co-operation between individuals and groups to ensure that a positive health and safety culture is promoted and developed. It is also recognised that all staff have duty to take care of themselves and others who may be affected by their individual acts or omissions, or by the way the Trust undertakes its business. This includes avoiding hazards, preventing accidents and cooperating with the Trust by complying with all instructions and recommendations on health and safety. So far as is reasonably practicable, the Trust will ensure that:
i. Safe and healthy work methods and conditions are provided and adopted to control the risks arising from work activities.
ii. Staff are consulted and made aware of potential hazards and the precautions to be adopted, by providing information, instruction, training, supervision and appropriate safety equipment.
iii. Steps are taken to identify the immediate and underlying causes of work related injuries, accidents and ill health and implement preventative action necessary.
iv. Statutory requirements are complied with and accepted as the minimum standards in all work areas and activities.
v. Employees are actively encouraged to participate in health and safety arrangements and submit ideas and suggestions for improving standards.
Employees who wilfully disregard Trust Health and Safety Policies and Procedures may be subject to Trust performance and conduct procedures. Shane DeGaris Chief Executive
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 6 of 34
1. Purpose The purpose of the policy is:
• To provide a healthy and safe environment in which to carry out the activities of the Trust.
• To ensure employees are aware of the Trust’s, and their own, responsibilities under the Health and Safety at Work etc. Act 1974.
• To ensure that any processes undertaken by the Trust do not adversely affect the public or the environment.
• To promote a positive safety culture for all day to day working practices taking into account any risks that may occur.
1.1 Scope All staff and other persons working on Trust premises. In the event of an infection outbreak, flu pandemic or major incident, the Trust recognises that it may not be possible to adhere to all aspects of this document. In such circumstances, staff should take advice from their manager and all possible action must be taken to maintain patient and staff safety. 2. Explanation of Terms HSE - Health and Safety Executive. Uk’s national regulator and enforcement body for workplace health and safety. 3. Duties This section of the policy sets out who is responsible for implementing the Statement of Intent, by identifying the responsibilities of different levels of management and specific functional roles.. 3.1 The Trust Board The Trust Board have a legal duty to ensure the health, safety and welfare at work of all who work at the Trust and those connected to its undertaking’s. Although the legal duty remains theirs, they delegate their duty to the Chief Executive, the Accounting Officer. The Trust Board set the direction for effective health and safety management. The Trust Board has responsibility for ensuring that all Board decisions reflect effective health and safety risk management. It will provide leadership through written and oral communications and by its actions. In carrying out these responsibilities, the members of the Trust Board will be aware of, and keep abreast of, appropriate health and safety legislation. The Trust Board will ensure that the Chief Executive is provided with all the necessary resources and assistance that is needed in order for the legal duty to be performed and will, through quarterly reports on health and safety performance, assure themselves that the performance of the legal duty, which has been delegated to the Chief Executive, is implemented.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 7 of 34
3. 2 Chief Executive The Chief Executive (CEO), as Accounting Officer, has ultimate responsibility and is accountable for health and safety within the Trust, and will ensure that:
3.2.1 The Executive Team understands and accepts its responsibilities and accountabilities for the implementation and monitoring of the Health and Safety Management Policy
3.2.2 The requirements of health and safety legislation and best practice guidance
are applied 3.2.3 The Trust’s policies and codes of practice are observed and that the
appropriate resources are made available to meet these requirements. In the execution of the duties placed upon him by health and safety legislation and this policy, the Chief Executive will delegate the performance of those duties to the Executive Director of Finance.
3.3 Executive Director of Finance The Executive Director of Finance will have the overall responsibility for the health, safety and welfare of the Trust. He will:
3.3.1 Ensure that the Health and Safety Policy is communicated to everyone who works at the Trust.
3.3.2 Ensure that the Health and Safety Policy is implemented by everyone who
works at the Trust. 3.3.3 Consult with Executives, Assistant Directors of Operations and other Senior
Managers, at budget review, to ensure adequate resources and facilities are made available to achieve stated health and safety objectives.
3.3.4 Report to the Trust Board and Chief Executive the effectiveness of the Health
and Safety Policy by presenting quarterly Health and Safety Reports to the Trust Board that details incident trends, levels of performance and matters of concern.
3.3.5 Ensure that annually health and safety objectives are defined with key
indicators and success criteria established to monitor performance.
The Executive Director will delegate the performance of some of the duties placed upon him by Health and Safety Legislation and this policy to the Assistant Director of Health and Safety. 3.4 Assistant Director of Health and Safety To assist the Executive Director in discharging his responsibilities, the Assistant Director will be responsible for the development and delivery of a Safety Advisory Service, which facilitates compliance with health, safety and environmental legislation by promoting safety risk management through senior management and divisional teams. In practical terms, this will involve: Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 8 of 34
3.4.1 The Assistant Director of Health and Safety is the designated competent person who provides health and safety assistance to the Trust Board and the Corporate Management Team. The Assistant Director has the authority to order the cessation of any process or activity which they consider to be unsafe or in breach of the Health and Safety at Work (etc) Act 1974 or any of the Health and Safety Regulations.
3.4.2 Coordinating and monitoring the effectiveness of safety arrangements within
the Trust, and advising the Executive Director of Finance, the Chief Executive and the Board of serious adverse incidents, unacceptable risks and associated Treatment Plans.
3.4.3 Ensuring that arrangements exist for the development and review of
appropriate policies, procedures and guidance on health, safety and welfare issues.
3.4.4 Assisting the Executive Director in developing strategic health and safety
objectives, key indicators and success criteria for monitoring overall performance
3.4.5 Ensuring that all staff training needs are identified, and that effective
arrangements exist for the delivery of training. 3.4.6 The provision of quarterly Health and Safety Report for the Health and Safety
Committee and Trust Board that advises on the implications of new legislation, details incident trends, levels of performance and matters of concern.
3.4.7 The development of appropriate policies and procedures that will provide the
Trust with necessary guidance for achieving compliance with legislative requirements and the provision of a safe, secure health environment. This will include the review of policies and revisions to take account of changes in legislation, standards and working practices.
3.4.8 The development of compliance testing and auditing on a regular basis to
ensure that the Trust is achieving compliance with legislative requirements and the implementation of agreed programs.
3.4.9 Ensure that adherence to this policy is incorporated in all contracts with
external agencies. 3.4.10 Ensure that effective health and safety communication exists between all
clinical, operational and functional disciplines, including third parties. 3.5 Executive Directors, Directors and Divisional Senior Managers Executive Directors, Divisional Senior Managers and Heads of Departments will be responsible to the Trust for health, safety and welfare on a day to day basis. Specifically they are responsible for implementing this policy by operating a safety culture and ensuring Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 9 of 34
adequate communication, training and the assessment and monitoring of risks. In particular this will include:
3.5.1 Ensuring that health and safety objectives defined by the Trust are incorporated in to the key indicators and success criteria established to monitor performance. Ensuring that at annual budget reviews adequate resources and facilities are available to ensure achievement of these objectives.
3.5.2 Ensuring health and safety is managed effectively in their services by
encouraging them to foster health and safety best practice. 3.5.3 Prioritising identified unacceptable health and safety risks and developing Risk
Treatment Plans to eliminate or minimise exposure. 3.5.4 Ensuring that all incidents and near misses, whether injury is sustained or not,
are reported and fully investigated in accordance with Trust policies. 3.5.5 Support participation in regular inspections and audits to ensure that the health
and safety management system is working effectively, and that any shortcomings are identified and dealt with.
3.5.6 Attending the Health and Safety Committee or identify a deputy to perform this
duty in their absence.
3.6 Head of Department, all Line Managers and Supervisors. Each Head of Department, all Managers and Supervisors is responsible for implementing this policy and for the health safety and welfare within their own departments. Specifically they will:
3.6.1 Ensure that the Trust policy is communicated to everyone in the work place. 3.6.2 Monitor the work place under their control to ensure that it remains safe and
ensure that health and safety performance is reviewed; risks are assessed, and subsequently, adequately controlled.
3.6.3 Ensure periodic work place inspections are carried out and any unsafe
conditions found are subsequently controlled or removed. 3.6.4 Participate in health and safety inspections and audits to ensure that the health
and safety management system is working effectively, and that any shortcomings are identified and dealt with.
3.6.5 Ensure any accident, incidents, ‘near misses’ and complaints are investigated,
taking appropriate timely remedial action to ensure any unsafe conditions found are either removed or controlled so that they do not become a subsequent cause of injury.
3.6.6 Ensure all work equipment is suitable for its intended purpose, appropriately
maintained and that all staff are trained in its use. Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 10 of 34
3.6.7 Ensure all staff receives information, instruction supervision and training which
will protect their health and safety and that of others. 3.6.8 Ensure that specific duties and responsibilities, with respect to implementing
and observing this policy, are described clearly in job descriptions and Trust contract specifications and included in the staff appraisal system and contract monitoring processes.
3.6.9 Consult, as appropriate, with Trade Union Safety Representatives and
employees on health and safety issues. 3.6.10 Act as (or, If necessary appoint an individual to assist them), the Safety Link
Person with regard to work place inspections and assisting with audits.
3.7 Ward and Departmental Safety Link Persons (SLPs) - work in partnership with their manager, colleagues and the Health and Safety Team and are a vital role in increasing levels of health & safety awareness, and establishing a positive and proactive approach to managing risk. Key aspects of the role are:
3.7.1 Working with their Manager with regard to undertaking risk assessments, inspections and audits the implementation of health and safety practice;
3.7.2 Acting as the liaison between their ward or department and the Health and Safety
Team, and assist with their safety audits and inspections 3.7.3 Ensuring that health and safety information received from the Health and Safety
Team is acted upon and brought to the attention of their colleagues; 3.7.4 Assisting with initiatives designed to promote a safe environment and working
practices. 3.7.5 Undertaking regular and routine inspections of the workplace under their control
and assisting in the annual risk assessment process.
3.8 All Employees (including Seconded Staff) All employees have a duty to themselves, colleagues, and any person who might be affected by their actions, to work in a safe manner. In particular, this will include:
3.8.1 Taking reasonable care for the health and safety of themselves and any other person who may be affected by their acts or omissions.
3.8.2 Co-operating with managerial and supervisory staff to ensure that all relevant
statutory regulations, policies and procedures are followed. 3.8.3 Attending as requested, health and safety training sessions designed to further
the cause of health and safety, and increase individual awareness. Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 11 of 34
3.8.4 Ensuring that where required, safety equipment and devices are used as
directed and appropriate protective clothing worn. 3.8.5 Reporting to their Manager or Supervisor all faults, hazards, unsafe practices,
accidents, adverse incidents, dangerous occurrences and near misses whether injury is sustained or not.
3.8.6 Ensuring that any ill health or medical condition, which may affect their ability to
work safely, is reported immediately to their manager and/or the Occupational Health Service.
3.9 Health and Safety Team The Health and Safety team are designated competent persons who provide health and safety assistance to the Trust managers and employees at all levels. The Health and Safety Team has the authority to order the cessation of any process or activity which they consider to be unsafe or in breach of the Health and Safety at Work Act or any of the Health and Safety Regulations.
The Health and Safety Team will:
3.9.1 Provide Health and Safety advice and assistance to all levels of staff. 3.9.2 Provide competent and professional advice and assistance with regard to
formulation and revision of the safety policy. 3.9.3 Assist in the devising of health and safety procedural documents. 3.9.4 Keep Heads of departments and Managers advised with regard to actual or
anticipated changes in health and safety legislation and accepted best practices.
3.9.5 Undertake workplace audits and provide reports to management on such
audits advising on actions to be taken to remedy hazards and risks. 3.9.6 Provide Managers regular reports on accident and incidents identifying any
trends and advising on mitigation and treatment plans to prevent as far as is reasonably practicable a reoccurrence.
3.9.7 Co-ordinate and oversee a programme of Health and Safety risk assessments
and annual audits throughout the whole of the workplace on a departmental basis.
3.9.8 Undertake accident and dangerous occurrence investigations and provide
management and, when required by law, the Health and Safety Executive, with reports of such incidents and dangerous occurrences.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 12 of 34
3.9.9 In conjunction with the Occupational Health Department undertake investigations in to cases of work related ill health and provide management and, where required by law, the Health and Safety Executive, with reports on such cases.
3.9.10 Undertake health and safety audits in order to determine the effectiveness of
the health and safety management procedures and, where appropriate, make recommendations as to the measures necessary to rectify failings in the procedures. Monitor the completion of the Health and Safety Management of Risk Inspection Forms on an annual basis, auditing a sample for data quality.
3.9.11 Provide support and assistance to those who are required to implement the
requirements of the safety policy and any of the safety management procedures.
3.9.12 Assist in the identification of health and safety training needs and, where
appropriate, deliver or arrange to be delivered, such training as may be necessary for the health and safety of employees.
3.9.13 Submit reports of all incidents which are reportable under the Reporting of
Injuries, Diseases and Dangerous Occurrences Regulations (RIDDOR) 2013 to the Enforcing authority.
3.10 Fire Safety Adviser The Fire Safety Adviser is designated by the Trust as a specialist officer responsible for the implementation and administration of fire precautions/procedures/prevention. Managers within the Trust should consult the Fire Safety Adviser when necessary, or refer to him any matters relating to fire precautions/prevention. In addition his responsibilities are:
3.10.1 To assist the Trust in carrying out its fire precautions responsibilities. 3.10.2 To advise the Fire Safety Manager and all other managers on fire precautions. 3.10.3 To survey and report on the standards of fire safety in the Trust premises. 3.10.4 To prepare staff training programmes and liaise with the learning and
development team and relevant manager in the organisation of fire drills and training exercises.
3.11 Local Security Management Specialist (LSMS) The LSMS is designated by the Trust as a specialist manager responsible for the implementation of all security matters including the prevention and detection of crime. Managers within the Trust should consult the LSMS when necessary, or refer to them any matters relating to security. In addition his responsibilities are:
3.11.1 To assist the Trust in carrying out its security responsibilities.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 13 of 34
3.11.2 To advise the Chief Executive, the Security Management Director and all other managers on security, and act as an adviser of various committees.
3.11.3 To recommend, where necessary, the order of priorities. 3.11.4 To survey and report on the standards of security within Trust premises and to
carry out security risk assessments liaising with the Health and Safety team as appropriate.
3.11.5 To investigate all cases of theft and any other security related incidents
3.12 Manual Handling Adviser The Manual Handling Adviser is designated by the Trust as a specialist person responsible for ensuring that all risk emanating from manual handling activities is controlled to an acceptable level. The Manual Handling Adviser responsibilities will include:
3.12.1 Implementation and the monitoring of the Trust Manual Handling Policy and
procedures. 3.12.2 Assessing and advising on the ergonomics of the working environment and
specific manual handling tasks, advising on areas of risk regarding manual handling operations.
3.12.3 Developing and providing training in safe handling techniques. 3.12.4. Following up any accident/incident or near miss report involving manual
handling. 3.12.5 Auditing the need for manual handling equipment and advising on the
purchase of manual handling equipment.
3.13 Occupational Health Department The responsibilities of the Occupational Health Department will be to provide health surveillance to particular staff exposed to occupational hazards in accordance with the Trust’s Policy and current legislation. The department will also be responsible for Pre-employment Medical Screening for every prospective employee as part of the selection and recruitment procedure. Furthermore they will be responsible for:
1) Health education 2) Rehabilitation and resettlement 3) To assist and advise where a risk to health exists
3.13.1 Health Surveillance
In order to monitor the effectiveness of the measures introduced to reduce risks to the health of employees, a programme of health surveillance will be undertaken which will be co-ordinated by the Occupational Health Department. Examples of the circumstances which may be selected for a programme of health surveillance will include:
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 14 of 34
1) Exposure to respiratory irritants. 2) Cytotoxic drug handling 3) Exposure to excessive noise. 4) Asbestos. 5) Ionising Radiation.
3.14 Infection Control Team The infection control team is responsible for undertaking surveillance of infection for the prevention and management of infection outbreaks, and reports to the Infection Control Committee. The infection control team will provide education in all aspects of infection control and prepare policies for and give advice on infection control issues. 3.15 Radiation Protection Advisers and Supervisors The Radiation Protection Advisers are appointed in accordance with the ‘Ionising Radiation Regulations 1999’ to provide advice on all aspects of the safe use of ionising and non-ionising radiation, to ensure risks to employees, patients and the general public are adequately controlled and in accordance with the relevant legislation. Radiation Protection Advisers will work with Radiation Protection Supervisors and managers in developing ‘local rules’ for each activity involving Ionising Radiation, and for ensuring compliance. In relevant departments, the Radiation Protection Supervisors are appointed to ensure that any obligations are met under the relevant regulations, and that safe practices and standards are adhered to. The Radiation Protection Advisers will hold a register of Radiation Protection Supervisors and administer the arrangements for assessing staff exposure levels to ionising radiation. 3.16 Estates Department The Director of Strategic Estate Development & Asset Management will have overall responsibility for ensuring that all buildings, premises, plant and equipment are maintained in a safe condition, good repair and in efficient working order. They will also devise and maintain procedures which are designed to ensure that reported defects are prioritised according to the risks to health and safety and attended to promptly. In addition they will:
3.16.1 Implement the requirements of the CDM Construction (Design and Management) Regulations 2015, and all other relevant legislation.
3.16.2 Ensure that all maintenance work (including that undertaken by contractors) is
carried out strictly in accordance with a safe procedure of work, legislation and best practice
3.16.3 Ensure that all contractors are aware of the safety procedures which are
currently in force and that such procedures are adhered to. 3.16.4 Prior to the commencement of any extraordinary or new works, liaise with the
Health and Safety Team. Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 15 of 34
3.17 Health and Safety Representatives The principal responsibility for Health and Safety lies with management. Therefore, management have the duty to make decisions on all matters affecting Health and Safety. However, the Trust believes that safe working is best brought about by the participation of all employees. The Trust therefore, supports the appointment of Trade Union and Professional Organisation nominated Health and Safety Representatives as in accordance with the ‘Health & Safety at Work Act 1974’ and ‘Safety Representatives and Safety Committee Regulations 1977’.
3.18 Agency and Locum Staff Managers must be assured that staff employed via NHS Professionals and other Agencies, have received basic health and safety training within the last 12 months. Minimum health and safety competency requirements shall be identified in all contractual agreements between the Trust and Agency providers, to ensure safe working practices for all employees and patients.
3.18.1 Agency or locum staff must have a local induction to the area they are working in. this must include an explanation of health and safety and fire procedures
3.18.2 Before Agency or Locum staff use any equipment, Trust Employees must
ensure that they are shown the correct operation, use and decontamination of the equipment.
3.19 Volunteers With regard to health, safety and welfare issues, the Trust affords the same rights to Volunteers as they do employed staff. Therefore, Volunteers have the same responsibilities as employed staff detailed in 3.8 above. 3.20 Contractors All contractors who work for the Trust will act in accordance with the Trusts’ contract procedures with respect to the management of their health and safety.
3.21 Health and Safety Committee The Trust maintains a Health and Safety Committee. Its objectives are to be a proactive force in promoting the highest standards of health and safety. The Health and Safety Committee will meet at least four times per year.
The Trust Health and Safety Committee is the main forum for consultation between the Trust and its employees. In addition, this committee will assist in ensuring a consistent, coordinated approach to health and safety management is taken across the Trust.
3.21.1 The Committee discusses matter of topical and strategic interest which have
corporate health and safety consequences. 3.21.2 To receive reports on matters of Health and Safety from:
a) Management b) Health and Safety Team
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 16 of 34
c) Occupational Health d) Security e) Risk Management f) The Fire Safety Adviser g) Safety Representatives h) Infection Control i) Radiation Protection j) Health and Safety Executive (H.S.E.) k) Manual Handling Adviser
See Appendix 2 For the Terms of Reference and Membership for the Trust Health and Safety Committee.
Local Health and Safety Meetings The Mount Vernon Hospital site holds a health and safety group meeting to provide opportunities for the routine communication and consultation between the Trust and others on the shared site.
4. Practical Arrangements 4.1 Equipment, Materials and Substances The Trust will ensure that the use, handling, storage and transport of equipment, materials and substances is safe and without risk in accordance with section 2 of the Health and Safety at Work etc 1974.
Any item of equipment or any materials or substances which are purchased for use at the place of work will only be purchased through NHS Supplies. Such purchases will specify the characteristics of anything purchased in terms of compliance with health and safety standards which may be defined in:
a) Any European Standard. b) Any British Standard. c) Any Industry Standard. d) Any standard specified in any appendices to any Health and Safety Regulations made under the Health and Safety Work Act 1974
4.2 Accident/Incident reporting and investigation Incident and accident records are vital to the effective monitoring of health and safety performance. They provide an opportunity for:
• Reactive assessment of the Trust arrangements for managing health and safety
risk • an opportunity for local learning and for the trust to develop new risk controls.
Managers will ensure their staff are aware of, and use, the Trust incident reporting procedures.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 17 of 34
Managers will review all reported incidents (including accidents) which occur in their service or ward area and investigate certain incidents further e.g. those incidents which are actually or potentially more serious or those which are frequent. The main purpose of the investigation is to identify and implement suitable measures which reduce the likelihood of a similar incident or accident occurring.
Managers will review periodically e.g. monthly all reported incidents (including accidents) in their service area or ward to identify trends e.g. the frequent occurrence of the same type of accident (such as a slip, trip or fall) or increasing numbers of accidents overall. Suitable action must be taken where the review reveals worsening health and safety performance e.g. review of risk assessments.
All incidents and accidents reportable under the Reporting of Injuries Diseases and Dangerous Occurrences Regulations 2013 (RIDDOR) will be subject to an investigation, the level of which will be commensurate with the severity of the incident (see Trusts policy on the management of Incidents).
The health and safety team will report to the Health and Safety Executive incidents that are notifiable under RIDDOR.
4.3 Risk Assessment In accordance with the Management of Health and Safety at Work Regulations 1999, risk assessments will be carried out in line with the Trust’s Risk Management Strategy. The method of risk assessment will be applied uniformly and consistently across the whole range of activities carried out at the Trust and the significant findings of such risk assessments will be recorded in the format laid out in the Risk Management Strategy.
4.4 Provision of Information to Employees In accordance with the requirements of Regulation 8 of the Management of Health and Safety at Work Regulations 1999 the Trust will ensure that Managers receive and disseminate suitable and relevant information relating to health, safety and welfare at the workplace to staff, volunteers, contractors and other users of Trust premises. This to include information on the hazards and risks associated with their work, and the systems in place to minimise exposure to these risks.
4.4.1 The statutory notice – ‘Health & Safety Law (what you should know)’ will be prominently displayed at all building entrances and other identified locations within the Trust. Other statutory notices will be displayed as appropriate.
4.4.2. Each Ward and Department will have a Health and Safety Notice Board, to
post all relevant information. As a minimum, the following need to be displayed:
• Copy of the Trust’s Health and Safety General Statement of Intent, (page 4 of this document).
• Copy of the Ward or Department Emergency Evacuation Plan. • Copy of the General Safety Rules, (see Appendix 3).
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 18 of 34
4.5 First Aid Provision The Trust will maintain a suitable number of qualified/appointed First Aiders in accordance with the Health and Safety (First Aid) Regulations 1981 in order that First Aid may be administered at any time when employees are at work.
A list of qualified first aiders and their contact details should be displayed in each department as appropriate.
Further information and advice is available in the Trust policy on First Aid. 4.6 Emergency Procedures and Business Continuity Plans In order to ensure the safety of employees, patients, visitors and members of the public and to comply with the requirements of Regulation 7 of the Management of Health and Safety at Work Regulations, procedures will be devised which will be implemented in the event of emergency or imminent danger. Each department or work area will have a plan for the purposes of the safe evacuation of persons in the event of emergency or imminent danger.
These include for example:
1. Major Incident and Internal Disaster Plans. 2. Fire Evacuation Plans. 3. Estates continuity plans, e.g. for loss of utilities and services. 4. Floods. 5. Bomb threats. 6. Radiation and chemical release. 7. Structural damage.
4.7 COSHH (Control of Substances Hazardous to Health) The COSHH Regulations 2002 requires the Trust to evaluate and control the risks to health for all employees from the exposure to hazardous substances at work. This includes exposure to microbiological agents, dusts of any kind in substantial quantities and all chemicals hazardous to health. Cytotoxic drugs come under the requirements of COSHH as there is a duty to protect the giver of these drugs not the patient.
The Trust is required to ensure the availability of up-to-date information upon the hazards associated with all substances used and establish that suitable controls and procedures are in place to minimise risk to the workforce. Each Hazardous substance identified will require a formal COSHH assessment which must identify:-
1. risk posed to the health of those exposed 2. steps necessary to control exposure to those hazards 3. prevention or adequate control of exposure 4. that the control measures are used and maintained 5. monitoring of the exposure 6. health surveillance where required 7. employees are properly informed and trained and supervised
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 19 of 34
4.8 Co-operation of Shared Sites The Trust has a shared site with other NHS and non-healthcare employers. The Trust will ensure its staff cooperates with these organisations in matters of health and safety in a timely manner of any activities which may affect the health and safety of their staff. Such cooperation includes:
4.8.1 Exchange of information on risks within the working environment and safe
systems of work. 4.8.2 Co-operating on matters such as implementing evacuation procedures, first aid,
and waste disposal. 4.8.3 Safety monitoring procedures, including routine inspections of common parts of
the facility
4.9 Training Training is regarded as an essential element of an effective health and safety management system and it is essential that all grades and disciplines of staff are trained to perform their job effectively and safely. The Director of People will ensure that general aspects of health and safety are incorporated into the Trust’s Training Policy and management training programmes. It shall be a responsibility of all Managers to identify the health and safety training needs of their staff as part of the personal development planning process.
General health and safety awareness will be included in the Trust Induction Programme, reinforced with more specific training as part of Departmental induction. Additional training will be provided when employees are exposed to new or increased risks because of a change in responsibilities, equipment or place of work. The Learning and Development Department will maintain a training database of attendance, and Managers will ensure that inadequate attendances are rectified
4.9.1 Induction Training The Trust recognises the importance of induction training for all full and part time employees, trainees, volunteers, and those on work experience programmes. Also included are those on temporary contracts.
4.10 Selection of Contractors Every employer or self-employed person, who expresses an interest in tendering for contracted out work on behalf of line management at the Trust will be subjected to an appraisal and selection procedure. Such procedures will require them to submit the following:
1) A properly prepared Health and Safety Policy. 2) A systematic programme of risk assessment. 3) Safe procedures and methods of work.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 20 of 34
All contractors engaged by the Trust have a responsibility, as specified in all contract documents, to carry out their work in a safe manner in respect of their own staff, sub-contractors, Trust employees and premises, patients and members of the public.
The Estates Department will use ‘Construction Line’ as part of their pre-qualification process as well as checking the HSE enforcement website. Contractors will be advised of any required standards, codes of practice, procedures, rules or other guidance applicable to the work to be undertaken. 5. Monitoring, Auditing and Review This policy and the safety management procedures which stem from it will be monitored in order to confirm their effectiveness in ensuring the health, safety and welfare at work of employees and others who might be affected by the work activities at the Trust. 5.1 Audits and Inspections Managers will ensure that the Health and Safety Management of Risk Inspection template is completed and reviewed on an annual basis. This will be sent to the health and safety department for review and monitoring of the action plan to manage any identified issues. Where appropriate, gaps highlighted by the inspection may be placed on the relevant risk registers. The inspection checklist action plan will be monitored by the relevant divisional governance committee and, by exception, the Health and Safety Committee.
A sample of the Health and Safety Management of Risk Inspection forms returned to the health and safety department will be audited annually to ensure the data quality is accurate.
The health and safety team will audit and inspect services across the Trust (the number and location of which will be stated in their annual audit and inspection plan) to determine both the level of compliance with the Trust’s health and safety policy and the degree to which risks are being adequately controlled. A number of inspection checklists will be audited for quality and compliance on an annual basis.
The audit or inspection findings will be reported to the service, departmental or ward manager and, if serious or Trust-wide matters have been found, the Health and Safety Committee.
The Health and Safety Executive may inspect the Trust at any time and provide recommendations for improvements. The Chief Executive will ensure any recommendations are implemented as appropriate.
5.2 Review of this Policy This policy will be reviewed as circumstances dictate, and if such reviews determine that the policy should be revised, then such revisions will take place after due consultation with the Health and Safety Committee.
Formally, the Trust Board and Health and Safety Committee will assess and approve this policy every three years, to determine its effectiveness and appropriateness.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 21 of 34

All revisions to this policy document will be brought to the attention of every employee. This policy has been assessed and is complaint with the Trust policy system, see Appendix 4.
5.3 Archiving Arrangements Responsibility for archiving trust-wide policies lies with the Corporate Services Department, where electronic folders have been set up to hold master copies.
Requests for retrieval of documents can be made to the Corporate Services Department. 5.4 Equality Impact Assessment The Trust is committed to promoting an environment that values diversity. The Trust aims to design and implement services, policies and measures that meet the diverse needs of our service, population and workforce, ensuring that none are placed at a disadvantage over others. This document has been equality impact assessed and this can be found in Appendix 1. 5.5 NHS Constitution The Trust is committed to the principles and values of the NHS constitution and this document takes in to account these principles and values.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 22 of 34
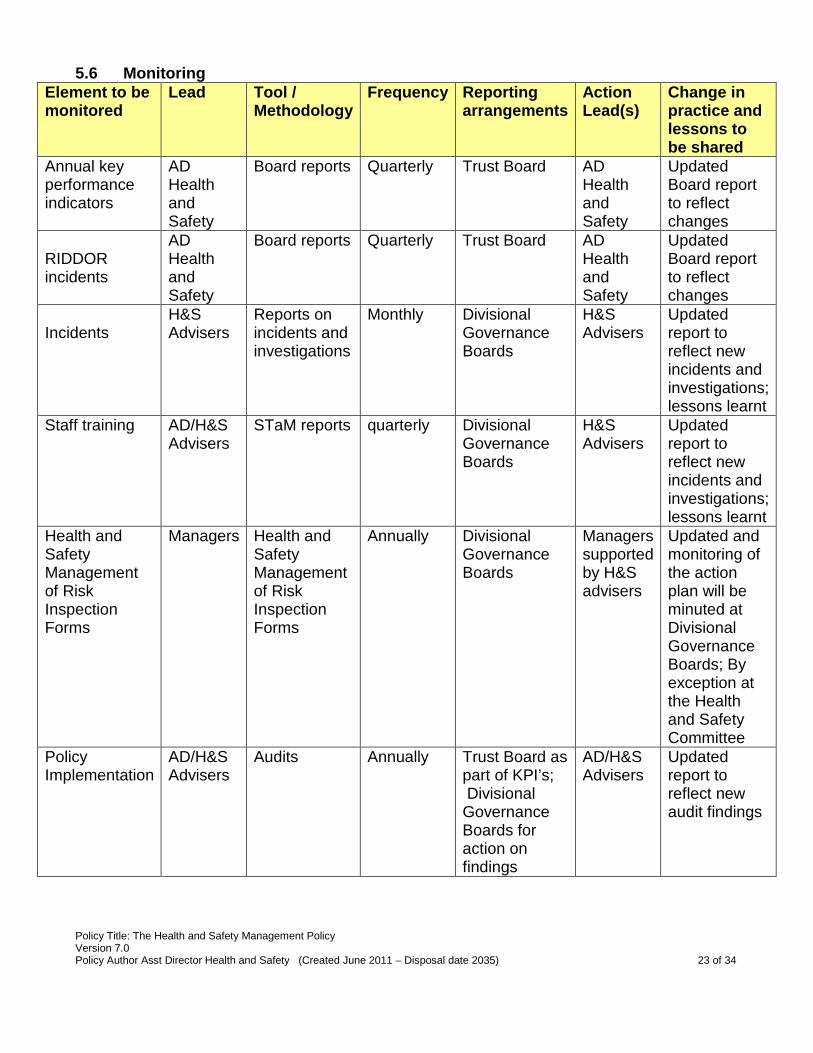
5.6 Monitoring Element to be monitored
Lead Tool / Methodology
Frequency Reporting arrangements
Action Lead(s)
Change in practice and lessons to be shared
Annual key performance indicators
AD Health and Safety
Board reports Quarterly Trust Board AD Health and Safety
Updated Board report to reflect changes
RIDDOR incidents
AD Health and Safety
Board reports Quarterly Trust Board AD Health and Safety
Updated Board report to reflect changes
Incidents
H&S Advisers
Reports on incidents and investigations
Monthly Divisional Governance Boards
H&S Advisers
Updated report to reflect new incidents and investigations; lessons learnt
Staff training
AD/H&S Advisers
STaM reports quarterly Divisional Governance Boards
H&S Advisers
Updated report to reflect new incidents and investigations; lessons learnt
Health and Safety Management of Risk Inspection Forms
Managers Health and Safety Management of Risk Inspection Forms
Annually Divisional Governance Boards
Managers supported by H&S advisers
Updated and monitoring of the action plan will be minuted at Divisional Governance Boards; By exception at the Health and Safety Committee
Policy Implementation
AD/H&S Advisers
Audits Annually Trust Board as part of KPI’s; Divisional Governance Boards for action on findings
AD/H&S Advisers
Updated report to reflect new audit findings
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 23 of 34
Appendix 1 Standard Equality Impact Assessment Tool
Name of Policy or Document The Management of Health and Safety Policy Name of Author Sue Manthorpe Who is this policy or service aimed at: (Employees, Patients/Carers, Visitors/General Public
All Employees
Description and aims of the policy/service change
This strategy supports the implementation of the Trust Health and Safety Policy and provides the direction for improvement of health and safety performance across all areas of Trust activities.
Date EIA Completed Nature of the Change Yes/No Details of adverse impact identified Does the policy/Service change affect one group less or more favourably than another on the basis of:
NO If yes to any of the following a full EIA must be completed
Race or Ethnicity No Nationality No Gender, Marital Status, Pregnancy and maternity
No
Culture or Heritage No Religion, Faith or belief No Sexual orientation, transgender Gender Reassignment
No
Age No Mental Health No Physical, sensory or Learning Disabilities
No
Homelessness, Gypsy/Travellers, Refugees/Asylum Seekers
No
I declare that in assessing the proposed documentation/change I have identified that a) There is unlikely to be an adverse impact on different minority groups Name Sue Manthorpe
Post: Assistant Director of Health and Safety
Date April 2015
Contact Number Ext 3829
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 24 of 34
Appendix 2 Health and Safety Committee Terms of Reference.
1. Introduction
All NHS Trusts are required to establish a Health and Safety Committee in accordance with the requirements of Section 2(7) of the Health and Safety at Work etc Act 1974 and the Safety Representative and Safety Committees Regulations 1997.
The Health and Safety Committee (HSC) is concerned with the development and implementation of a health and safety policy and safety management systems to facilitate the safe environment for staff, patients and visitors and all others affected by the activities of the Trust. It will seek clarification and investigate any health and safety related activity within its terms of reference and to monitor all aspects of health, safety and fire performance to comply with current regulations, legislation and best practice guidance. On occasions this may also include monitoring hazards and risks in partnership with the Clinical Governance Committee. The Committee Minutes will be presented to the Quality and Risk Committee on a quarterly basis.
2. Membership The Committee will be chaired initially by an Executive Director. This will be reviewed once Committee functions have become sufficiently established and embedded.
Assistant Director of Health and Safety Director of Operations Assistant Director of Operations (ADO) Representative (ADO Mount Vernon) Deputy ADO Surgery. Deputy Director of Nursing Interim Head of Employee Services Assistant Director of Clinical Governance Director of Estates and Facilities or Deputy Head of Facilities Trade Union x 3 representatives Fire Safety Adviser Health & Safety Adviser Manual Handling Adviser Occupational Health Manager Security Manager (LSMS)
Health and Safety Administrator – meeting support and minute taker 2.1 A quorum shall be 4 members, one of whom must be the Director or Assistant Director
of Operations together with the Director of Estates and Facilities, Trade Union Chair, Fire Safety Adviser or Health and Safety Adviser or, exceptionally, a nominated representative.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 25 of 34
3. Attendance
It is expected that members should make every effort to attend Committee meetings and will attend every meeting unless there are good reasons preventing attendance. The Chair may invite other persons as necessary to cover specific agenda items and attain the objectives of the Committee.
4. Frequency
Meetings shall be held not less than four times a year and will normally take place every three months. Meeting dates will be published annually although the Chair of the Committee can call a meeting at any time.
5. Authority
The Committee is authorised by the Trust Board to; Investigate any activity within its terms of reference; seek any information it requires from any employee; employees are directed to cooperate with any request made by the Committee; to initiate and monitor any action necessary for compliance with legislation.
6. Duties
1. To report on health, safety and fire issues to the Chief Executive and Trust Board.
2. To develop, approve, implement and review health, safety and fire related strategy, policy and procedures. On behalf of the Trust Board ratify such documents.
3. To review all identified health and safety risks within the Trust as contained in the
Corporate and Local Risk Registers, ensuring that the effectiveness of implemented risk management processes is monitored, reviewed and managed to address areas of concern.
4. Review and challenge health and safety key performance indicators, incidents, complaints, claims and ensure action plans are developed and implemented to address any concerns, as well as ensuring lessons have been learnt.
5. To consider and review health and safety related issues that arise out of risk assessments, audits and inspections, including those made by enforcing authority inspectors and other external agencies.
6. To receive and act upon information from; the Health & Safety Executive; NHS SAB
system and other relevant bodies or internal working groups.
7. Monitor the Trusts compliance with the Care Quality Commission registration requirements where these relate to health and safety and ensure action plans are implemented to improve practice where required.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 26 of 34
8. To monitor the effectiveness of health & safety and fire controls through the study of incident and accident statistics, trends, complaints and claims, identifying high risk areas recommending actions where appropriate.
9. The Committee reserves the right to establish time limited working groups. The
findings of these meetings will be referred to the Committee for ratification or progress and necessary actions. The membership of each working group will be agreed by the Health and Safety Committee and may not necessarily reflect the quorum identified in this document
10. Review the quarterly Board Health and Safety report and Annual report
11. Review and monitor the health and safety and fire safety work programme. 7. Reporting Groups
Oversee health and safety and receive regular reports from key groups (including but not limited to): Water Quality Group Security/Police liaison Waste management Ionising Radiation group Estates Governance group Laser Group
8. Reporting Arrangements
Agenda and papers of the Committee meetings will be circulated no less than five working days prior to the meeting. The minutes of the Committee meetings shall be formally recorded and presented to the Quality and Risk Committee. The Chair of the Committee shall draw to the attention of the Board any issues that require the attention of the full Board in the quarterly Health and Safety Board report.
9. Effectiveness The Health and Safety Committee will review its own effectiveness and TOR on an annual basis and report the outcomes of this review to the Trust Board.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 27 of 34
General Safety Rules Appendix 3
General 1. All employees should respect and be aware of the contents of this policy and all
other health & safety policies and procedures.
2. All employees shall immediately report any unsafe practices or conditions via the
Trust’s Incident Reporting Procedures and to their Manager or supervisor.
3. Any person under the influence of alcohol or any other intoxicating drug, which might
impair motor skills or judgements, whether prescribed or otherwise, will not be allowed to
undertake the task.
4. Unprofessional, careless, reckless and unsafe behaviour that might jeopardise the health
and safety of any other person, are forbidden.
5. Any person whose levels of alertness and/or ability are reduced due to illness or fatigue
will not be allowed to undertake an activity if this might jeopardise the health and safety of
that person or any other person.
6. Employees shall not adjust, move or otherwise tamper with any electrical equipment,
machinery or air or water lines in a manner not within the scope of their duties, unless
instructed to do so by a senior member of staff.
7. All waste materials must be disposed of carefully in accordance with Trust procedures,
and such a way that does not constitute a hazard to other workers.
8. No Employee shall undertake a task, which appears to be unsafe.
9. No Employee shall undertake a task unless they have received adequate safety
instruction and are authorised to carry out the task.
10. All work related injuries, ill health, incidents and near misses shall be reported in
accordance with the Trust’s Incident Reporting Procedures and to their manager or
supervisor.
11. Employees suffering from an injury at work should report to the Occupational Health
Service at the earliest opportunity.
12. Employees shall ensure that equipment/machinery is not used unless all protective
guards and other safety devices are properly fitted/provided and in good working order.
They shall immediately report any deficiencies to their manager or supervisor.
13. Work shall be well planned and supervised to avoid injuries in the handling of heavy Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 28 of 34
materials and while using equipment.
14. No employees shall use chemicals without the knowledge required to work with those
chemicals safely.
15. Suitable clothing and footwear will be worn at all times and in accordance with the Trust
Uniform Policy. . Personal protective equipment e.g. gloves, shall be worn wherever
appropriate, and in accordance with written safe systems of work.
16. All employees are expected to raise health and safety concerns
Working Environment 17. Work areas shall be kept clean and tidy.
18. Any spillage will be cleaned up immediately.
19. Waste materials and rubbish shall be removed routinely.
20. All combustible waste materials must be discarded in metal waste containers.
21. All fire exit routes must be kept clear from obstructions at all times.
22. All pits and holes must be covered when not in use and clearly marked with warning signs
when in use.
Walkways 23. Walkways and passageways must be kept clear from obstructions at all times.
24. If a walkway or passageway becomes wet, it must be clearly marked with warning signs
and/or covered with slip-resistant material.
25. Trailing cables are a trip hazard and must not be left in any passageway.
26. Any change in the floor elevation of any walkway or passageway must be clearly marked.
27. Where objects are stored in or around a passageway, care must be taken to ensure that
no long or sharp edges jut out into the passageway in such a way as to constitute a safety
hazard.
28. Where vehicles or other moving machinery is using a pedestrian area, pedestrians should
use an alternative route wherever possible. If no alternative route is possible, the area
must be clearly marked with warning signs.
Tools and Equipment Maintenance 29. Trust machinery and tools are only to be used by qualified and authorised personnel. It is
the responsibility of the manager to determine who is authorised to use specific tools and
equipment.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 29 of 34
30. It is the responsibility of all employees to ensure that any tools or equipment they use are
in a good and safe condition. Any tools or equipment, which is in any way defective, must
be repaired or replaced.
31. All tools must be properly and safely stored when not in use.
32. No tool and machinery shall be used without the manufacturer’s recommended shields,
guards or attachments.
33. Approved personal protective equipment shall be properly used, where appropriate.
34. Persons using machine tools must not wear clothing, jewellery or long hair in such a way
as might pose a risk to their own or anyone else’s safety.
35. Employees are prohibited from using any tools or piece of equipment for any purpose
other than its intended purpose.
Personal Protective Equipment 36. Employees shall use all personal protective equipment provided to them in accordance
with the training and instruction given to them regarding its use.
37. Employees who have been provided with personal protective equipment shall immediately
report any loss of or obvious defect in any equipment provided to the manager or
supervisor
Manual Handling 38. Wherever reasonably practicable, the moving and handling of objects will be undertaken
by mechanical devices, rather than manual handling. The equipment used shall be
appropriate for the task.
39. The load to be moved shall be inspected for sharp edges, slivers and wet or greasy
patches.
40. When moving or handling a load with sharp or splintered edges gloves will be worn.
Gloves shall be free from oil, grease or other agents, which might impair grip.
41. The route over which the load is to be moved or handled shall be inspected to ensure that
it is free of obstructions or spillage, which could cause tripping, or spillage.
42. Employees will not attempt to move or handle a load, which is too heavy to manage
comfortably.
43. Where team handling and moving is necessary, one person shall act as co-ordinator,
giving commands to move the load.
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 30 of 34
44. All manual handling must be undertaken in accordance with techniques, etc. covered at
Manual Handling training courses.
45. Any member of staff who believes that they may be suffering a back or musculoskeletal
injury, which may affect their ability to participate fully in manual handling work, shall
declare this to their manager immediately, and thereafter at the start of each shift.
46. In the case of accident or injury staff will either self-refer or be referred by their manager
to the Occupational Health Service, who will see them as soon as possible to discuss
the management of the injury
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 31 of 34
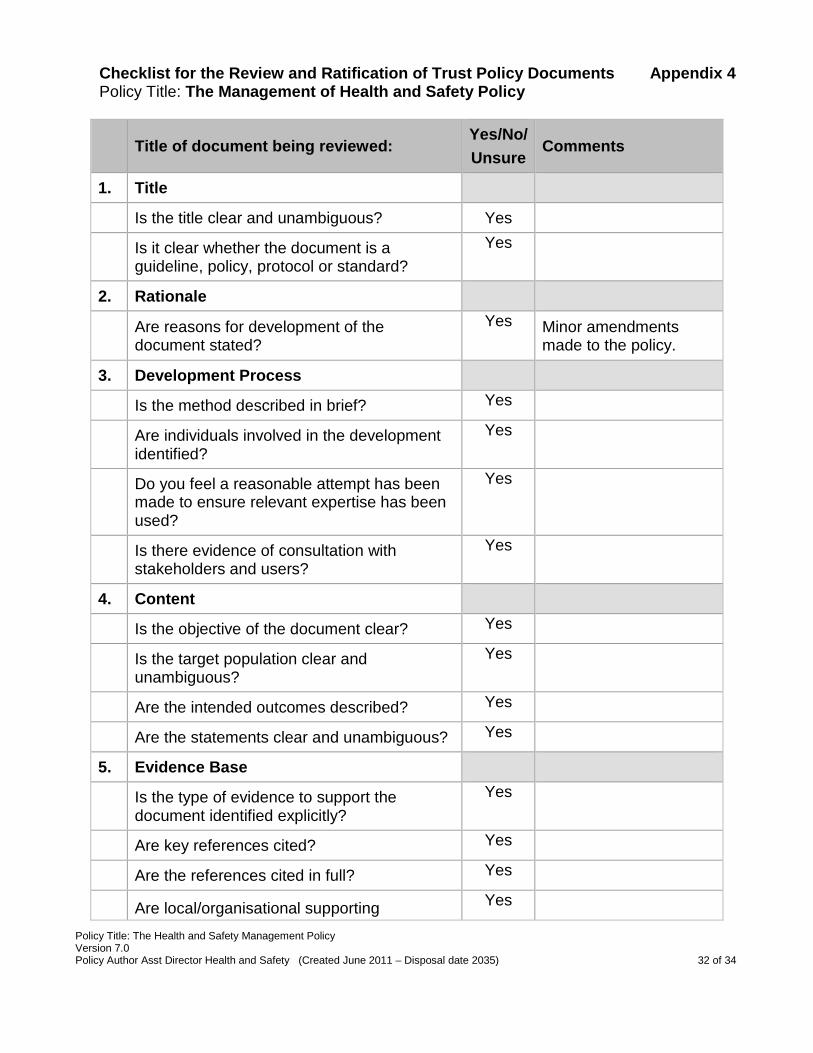
Checklist for the Review and Ratification of Trust Policy Documents Appendix 4 Policy Title: The Management of Health and Safety Policy
Title of document being reviewed: Yes/No/ Unsure
Comments
1. Title
Is the title clear and unambiguous? Yes
Is it clear whether the document is a guideline, policy, protocol or standard?
Yes
2. Rationale
Are reasons for development of the document stated?
Yes Minor amendments made to the policy.
3. Development Process
Is the method described in brief? Yes
Are individuals involved in the development identified?
Yes
Do you feel a reasonable attempt has been made to ensure relevant expertise has been used?
Yes
Is there evidence of consultation with stakeholders and users?
Yes
4. Content
Is the objective of the document clear? Yes
Is the target population clear and unambiguous?
Yes
Are the intended outcomes described? Yes
Are the statements clear and unambiguous? Yes
5. Evidence Base
Is the type of evidence to support the document identified explicitly?
Yes
Are key references cited? Yes
Are the references cited in full? Yes
Are local/organisational supporting Yes
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 32 of 34
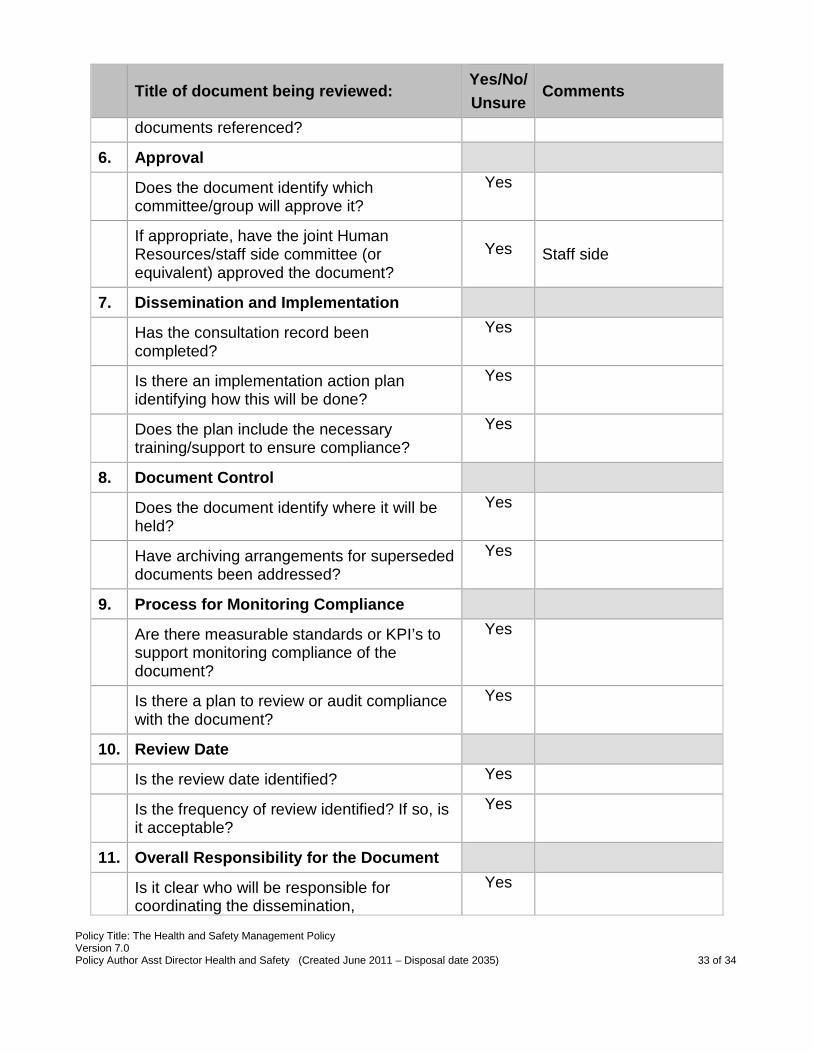
Title of document being reviewed: Yes/No/ Unsure
Comments
documents referenced?
6. Approval
Does the document identify which committee/group will approve it?
Yes
If appropriate, have the joint Human Resources/staff side committee (or equivalent) approved the document?
Yes Staff side
7. Dissemination and Implementation
Has the consultation record been completed?
Yes
Is there an implementation action plan identifying how this will be done?
Yes
Does the plan include the necessary training/support to ensure compliance?
Yes
8. Document Control
Does the document identify where it will be held?
Yes
Have archiving arrangements for superseded documents been addressed?
Yes
9. Process for Monitoring Compliance
Are there measurable standards or KPI’s to support monitoring compliance of the document?
Yes
Is there a plan to review or audit compliance with the document?
Yes
10. Review Date
Is the review date identified? Yes
Is the frequency of review identified? If so, is it acceptable?
Yes
11. Overall Responsibility for the Document
Is it clear who will be responsible for coordinating the dissemination,
Yes
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 33 of 34
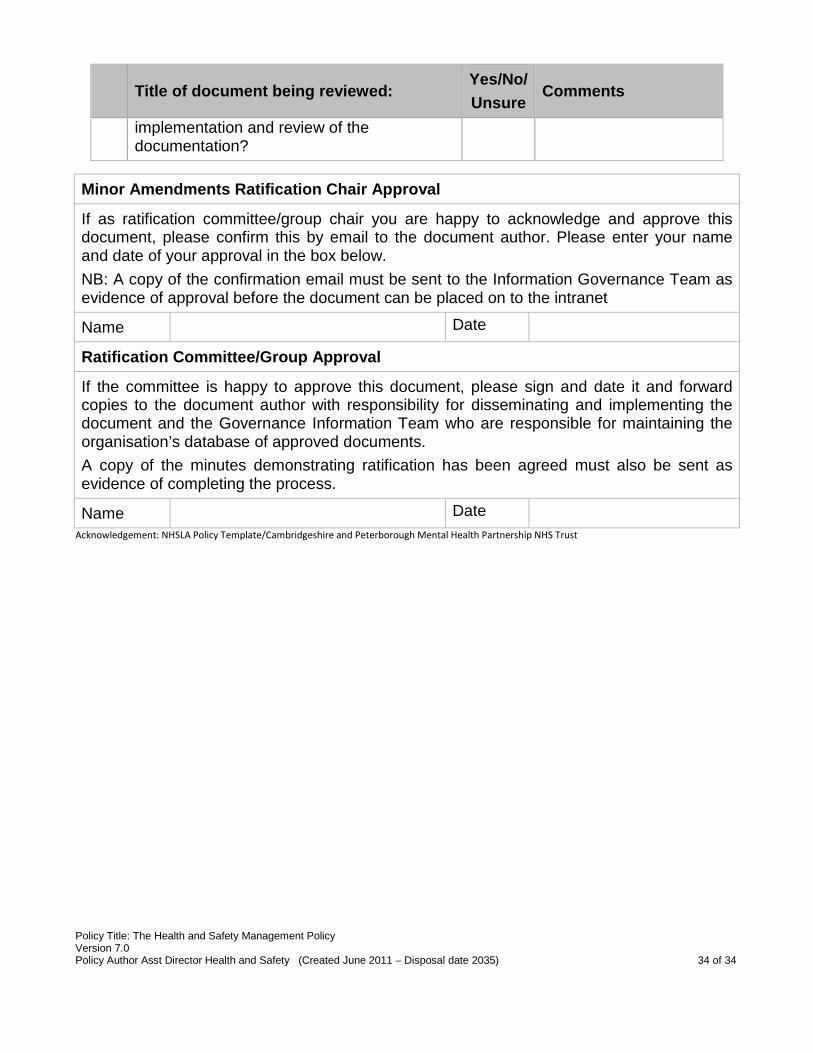
Title of document being reviewed: Yes/No/ Unsure
Comments
implementation and review of the documentation?
Minor Amendments Ratification Chair Approval
If as ratification committee/group chair you are happy to acknowledge and approve this document, please confirm this by email to the document author. Please enter your name and date of your approval in the box below. NB: A copy of the confirmation email must be sent to the Information Governance Team as evidence of approval before the document can be placed on to the intranet
Name Date
Ratification Committee/Group Approval
If the committee is happy to approve this document, please sign and date it and forward copies to the document author with responsibility for disseminating and implementing the document and the Governance Information Team who are responsible for maintaining the organisation’s database of approved documents. A copy of the minutes demonstrating ratification has been agreed must also be sent as evidence of completing the process.
Name Date Acknowledgement: NHSLA Policy Template/Cambridgeshire and Peterborough Mental Health Partnership NHS Trust
Policy Title: The Health and Safety Management Policy Version 7.0 Policy Author Asst Director Health and Safety (Created June 2011 – Disposal date 2035) 34 of 34
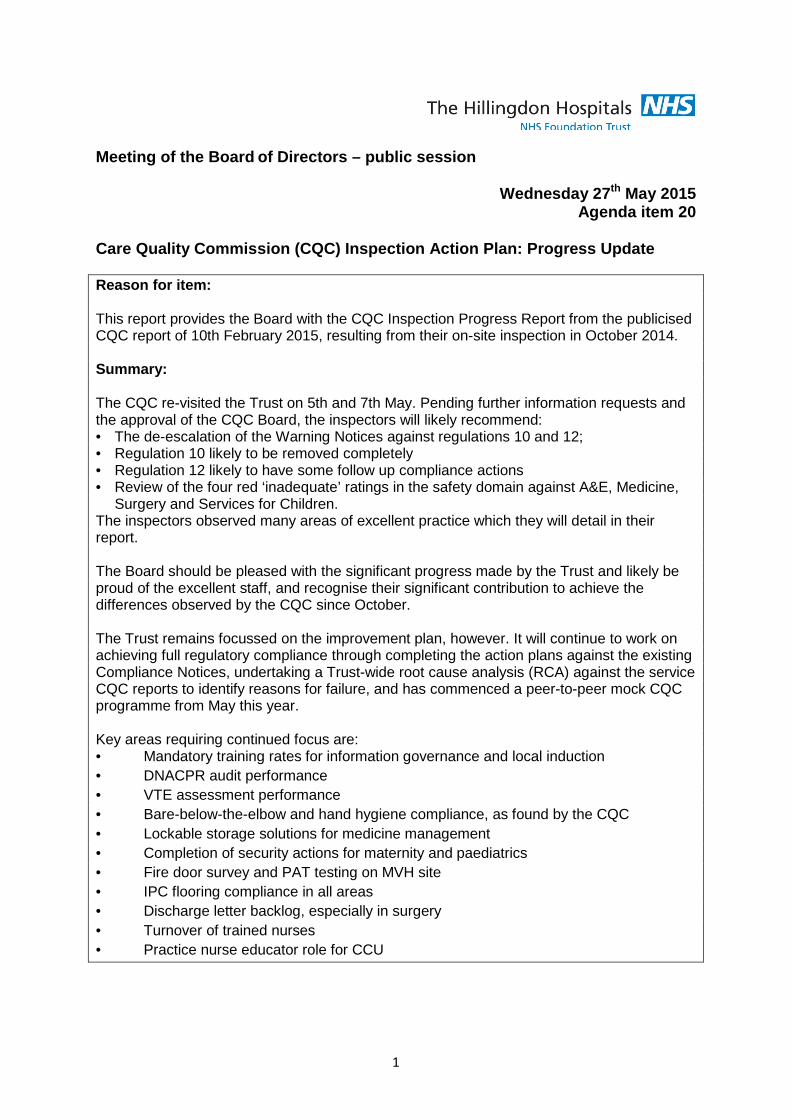
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 20
Care Quality Commission (CQC) Inspection Action Plan: Progress Update Reason for item: This report provides the Board with the CQC Inspection Progress Report from the publicised CQC report of 10th February 2015, resulting from their on-site inspection in October 2014. Summary: The CQC re-visited the Trust on 5th and 7th May. Pending further information requests and the approval of the CQC Board, the inspectors will likely recommend: • The de-escalation of the Warning Notices against regulations 10 and 12; • Regulation 10 likely to be removed completely • Regulation 12 likely to have some follow up compliance actions • Review of the four red ‘inadequate’ ratings in the safety domain against A&E, Medicine,
Surgery and Services for Children. The inspectors observed many areas of excellent practice which they will detail in their report. The Board should be pleased with the significant progress made by the Trust and likely be proud of the excellent staff, and recognise their significant contribution to achieve the differences observed by the CQC since October. The Trust remains focussed on the improvement plan, however. It will continue to work on achieving full regulatory compliance through completing the action plans against the existing Compliance Notices, undertaking a Trust-wide root cause analysis (RCA) against the service CQC reports to identify reasons for failure, and has commenced a peer-to-peer mock CQC programme from May this year. Key areas requiring continued focus are: • Mandatory training rates for information governance and local induction • DNACPR audit performance • VTE assessment performance • Bare-below-the-elbow and hand hygiene compliance, as found by the CQC • Lockable storage solutions for medicine management • Completion of security actions for maternity and paediatrics • Fire door survey and PAT testing on MVH site • IPC flooring compliance in all areas • Discharge letter backlog, especially in surgery • Turnover of trained nurses • Practice nurse educator role for CCU
1
Board Action required: The Board is asked to: 1. Review and comment on the CQC progress report. 2. The Board is asked to note and agree the governance arrangements comments. Report from: Wendy Cookson, Interim Director Compliance Report sponsor: Theresa Murphy, Director of Patient Experience & Nursing Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience
and the quality of care we provide. • A clinically led service strategy that responds to the needs of patients and other health
and social care partners • To deliver high quality care in the most efficient way Previous consideration at Board or Committees: Currently reviewed monthly by the Board. Equality and diversity considerations: Yes. Financial implications: nil
2
Care Quality Commission (CQC) Inspection Action Plan: Progress Update 1. Introduction
This report provides the Board with the CQC Inspection Progress Report from the publicised CQC report of 10th February 2015, resulting from their on-site inspection in October 2014.
2. CQC Inspection Progress Report
2.1 The CQC re-visited the Trust on 5th and 7th May. Pending further information requests and the approval of the CQC Board, the inspectors will likely recommend: • The de-escalation of the Warning Notices against regulations 10 and 12; • Regulation 10 likely to be removed completely • Regulation 12 likely to have some follow-up compliance actions • The review of the 4 red ‘inadequate’ ratings in the safety domain against
A&E, Medicine, Surgery and Services for Children; The inspectors observed many areas of excellent practice which they will detail in their report. The Board should be pleased with the significant progress made by the Trust and likely be proud of the excellent staff, and recognise their significant contribution to achieve the differences observed by the CQC since October. The Trust remains focussed on the improvement plan, however. It will continue to work on achieving full regulatory compliance through completing the action plans against the existing Compliance Notices, undertaking a Trust-wide RCA against the service CQC reports to identify reasons for failure, and has commenced a peer-to-peer mock CQC programme from May this year.
2.2 The compliance notices and all outstanding actions remain in place and will be assessed by the CQC through further data requests. The governance arrangements for compliance against the regulations will remain in place and will include the peer-to-peer mock CQC inspections and outcomes of the RCA exercise.
2.3 It is important to note the GREEN actions are complete/progressing as
planned but not assessed. A key to the Monitor BRAG (Blue, Green, Amber, Red) rating is on the front cover of the report. See appendix 1.
3. Updates for 17th April to 13th May
3.1 The attached report is the 12th May position against the action plan. Key areas
of change to note – by exception, ambers and reds in the report. Some completed actions previously seen at the last two Board meetings have been removed to enable clear focus on outstanding actions
3
• Warning Notice - Assessing and monitoring the quality of service provision.
o A Social Worker regularly attends A&E and maternity Safety-net meetings as agreed at MASH
o Mandatory training compliance rates, especially for key subjects of safeguarding and infection prevention and control, continue above the level of 80 %.
• There are 2 exceptions: Information Governance (where the target is 95%) – 89.74% and local induction – 67.68. Action to mitigate include:
• Individual staff members still requiring training all have training dates assigned
• New Bank Staff – timesheets must be accompanied by a local induction checklist
• Payment for STAM training will only be made when Bank staff are signed off as having completed ALL their training for the year
o Latest audit 10th May results: of 66 patients with DNACPR orders three were incomplete (96% completion rate). The CQC comments on the DNACPR forms they reviewed during their revisit are awaited and will be added to the action plan.
o The UCC data sharing agreement has been in place since 30th April and data has been flowing from the UCC onto the i-reporter web page from 5th May. Adults have been added as an option to search. All patients will be able to be reviewed by the number of attendances over any time period, reason for admission and any ‘flags’ currently on the PAS system. The MIU will also have access to the system thus providing complete cross-site visibility.
• Warning Notice - Cleanliness and infection control
o Since the introduction of the new NSC processes and targets the monthly data has shown consistently that the technical cleaning audit scores have been meeting the required targets. The combined site domestic cleaning scores have been 98% in Very High Risk areas (target 98%) and 97% in High Risk areas (target 95%).
o There have been refinements to the audit forms and processes as staff become more familiar with the audit, and additional training has also been undertaken to ensure that roles and responsibilities are clear particularly in relation to the nurse cleaning of equipment.
o The independent cleaning assessor’s review of cleaning has also shown that the technical cleaning audit scores for areas and standards is consistent with their own findings.
o For April local IPC audits, there was a full return with no areas outstanding. The audit tool has been revised for BBE/hand hygiene to be inclusive of all staff groups and disciplines.
o CQC verbal feedback re compliance with BBE and hand hygiene will be incorporated into revised training, observation and audit from w/c 18th May.
4
• Compliance Notice – Medicine Management
o All related policies are now up-to-date. o The PGD group has completed all PGD updates and have commenced
quarterly meetings from 9th April. o Estates work completed. Clinical areas have commenced ordering
cupboards where required. o NHS Protect audit actions being completed by Divisions and monitored
through Sit-rep and Divisional governance meetings. • Compliance Notice - Safety and suitability of premises
o Camera installation complete to monitor garden. CCTV system failures
have been identified and being rectified. Order placed for security swipe system.
o Fire door survey complete for THH site; MVH survey currently underway. o Flooring programme funding approved – lesser amount than requested
so works are being re-prioritised according to Infection Control risk assessment.
o Master Planning project scope of external advisers being finalised following Capital Investment Group review. Next step will be to invite tenders.
o Complete high-level list of assets has been assembled and being uploaded into Planet. PPMs will be developed according to HTM and HSE standards
• Compliance Notice - Safety, availability and suitability of equipment. o 12,411 items PAT tested by 30th April on THH site. MVH site PAT testing
has commenced. o All patient exercise/treatment equipment risk-assessed in five areas
across both sites and replacement programme created. o The paediatric resuscitation trolleys are delayed in transit from America
and will be with the Trust mid-July. o The review of the maintenance contracts for all the Trust equipment has
shown there are multiple, individual contracts requiring centralising. Business case created for sign-off in June for additional specialist resource to undertake this work.
o Replacement programme to be agreed for physiotherapy gym equipment.
• Compliance Notice - Records
o Regular six monthly reminders as sent on 13th February, planned to capture new staff and as a reminder to remaining staff.
o Medicine and Surgery & Anaesthetics are using name stamps to good effect. Paediatrics have placed an order. Delivery TBC. Discussions with A&E, considering the high locum numbers, are ongoing.
o Pharmacy are keen to implement stamps for their staff and are designing drug charts to accommodate.
o TIAA audit scope agreed for quality of medical records.
5
o Trust compliance against a target of 95% for VTE assessment performance for April 2015 was 93.8% and of 13th May, 91.7%.
o Latest DNACPR audit 10th May results: of 66 patients with DNACPR orders three were incomplete = 96% completion rate
o UCC the data sharing agreement was in place 30th April.
• Compliance Notice –Staffing
o Current update: • Italy: 9th to 13th February – 11 nurses commenced in post 15th May • Portugal: 3rd – 5th March; 19th - 21st May – 1 nurse • Spain: 25th – 27th March – 11 nurses – due to start 6th July • Italy - Rome: 14th – 16th April; - 6 nurses • Greece - Athens: 5th – 7th May – 0 nurses • Philippines and South Africa: dates TBC 2015.
o April turnover rate was 1.13% for nurses o Lead Nurse for overseas/EU recruitment commences Monday 18th May
with the explicit role for organising the Philippines and South African recruitment programme
o Mandatory training compliance rates, especially for key subjects of safeguarding and infection prevention and control, continue above the level of 80%.
o There are two exceptions: Information Governance (where the target is 95%) – 89.74% and local induction – 67.68%. Actions to mitigate are included in the main report
4. Governance arrangements
4.1 As recommended in last month’s Board paper, the completed and assured
actions (as per Monitor BRAG ratings) in this report have been closed in this version of the report. The aim of this is to facilitate a more focussed report and move towards one that covers full regulatory compliance monitoring beyond immediate CQC concerns outlined in the Notices. The actions for this will be created by the RCA process and mock CQC’s planned from May.
6
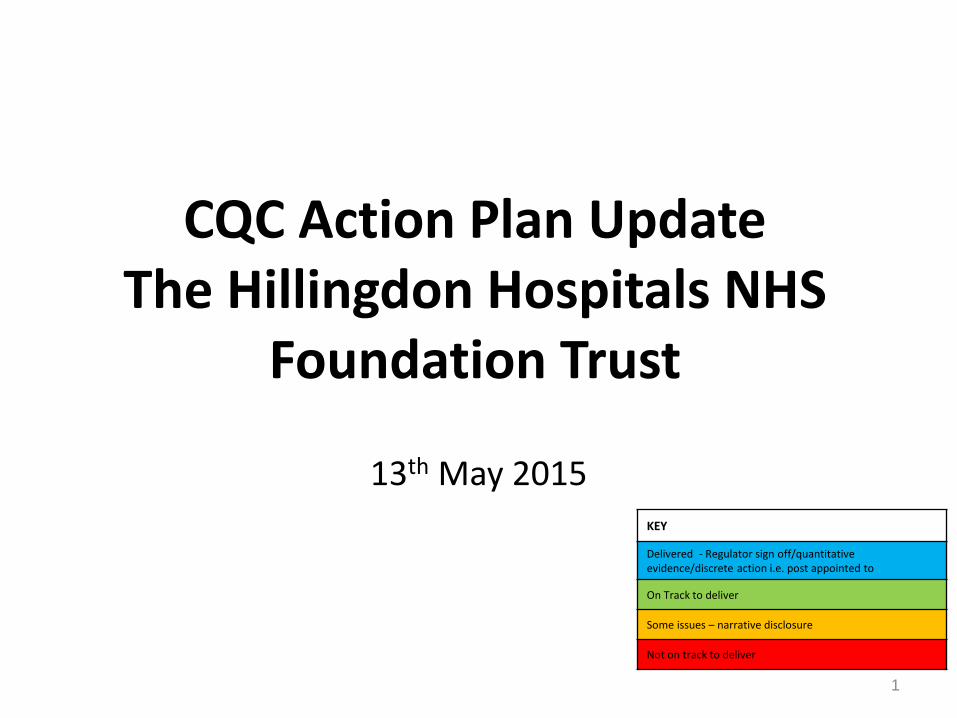
CQC Action Plan Update The Hillingdon Hospitals NHS
Foundation Trust
13th May 2015
KEY
Delivered - Regulator sign off/quantitative evidence/discrete action i.e. post appointed to
On Track to deliver
Some issues – narrative disclosure
Not on track to deliver
1
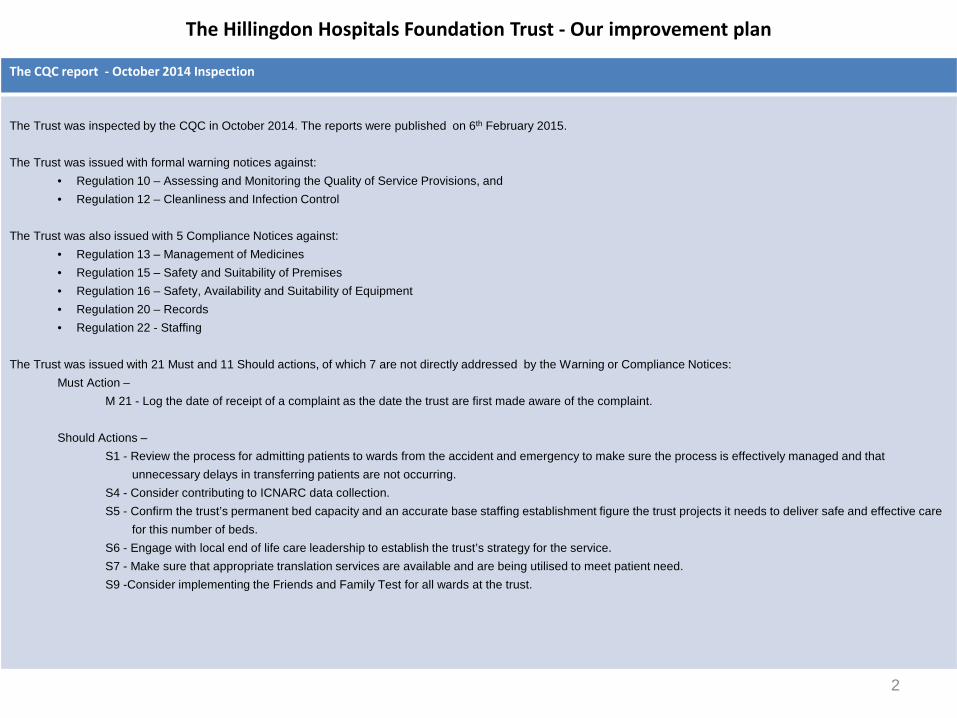
The Hillingdon Hospitals Foundation Trust - Our improvement plan
2
The CQC report - October 2014 Inspection
The Trust was inspected by the CQC in October 2014. The reports were published on 6th February 2015.
The Trust was issued with formal warning notices against:
• Regulation 10 – Assessing and Monitoring the Quality of Service Provisions, and • Regulation 12 – Cleanliness and Infection Control
The Trust was also issued with 5 Compliance Notices against:
• Regulation 13 – Management of Medicines • Regulation 15 – Safety and Suitability of Premises • Regulation 16 – Safety, Availability and Suitability of Equipment • Regulation 20 – Records • Regulation 22 - Staffing
The Trust was issued with 21 Must and 11 Should actions, of which 7 are not directly addressed by the Warning or Compliance Notices:
Must Action – M 21 - Log the date of receipt of a complaint as the date the trust are first made aware of the complaint.
Should Actions – S1 - Review the process for admitting patients to wards from the accident and emergency to make sure the process is effectively managed and that unnecessary delays in transferring patients are not occurring. S4 - Consider contributing to ICNARC data collection. S5 - Confirm the trust’s permanent bed capacity and an accurate base staffing establishment figure the trust projects it needs to deliver safe and effective care for this number of beds. S6 - Engage with local end of life care leadership to establish the trust’s strategy for the service. S7 - Make sure that appropriate translation services are available and are being utilised to meet patient need. S9 -Consider implementing the Friends and Family Test for all wards at the trust.
The Hillingdon Hospitals Foundation Trust - Our improvement plan
3
Governance, Accountabilities and Responsibilities
• We have accepted all the recommendations. An Interim Director of Compliance has been appointed and the improvements are managed through the governance structure outlined below, with Executive Directors as accountable leads for each Regulation:
• Improvements are monitored every week at twice-weekly Sit-Rep meetings, a weekly Steering Group and Executive Briefings • This document shows a plan for making these improvements and demonstrates our progress against the plan • The Trust will set out longer-term plans to maintain progress and ensure the actions lead to measurable improvements in the quality and safety of care for patients
How we will communicate our progress
• We will update this progress report every month
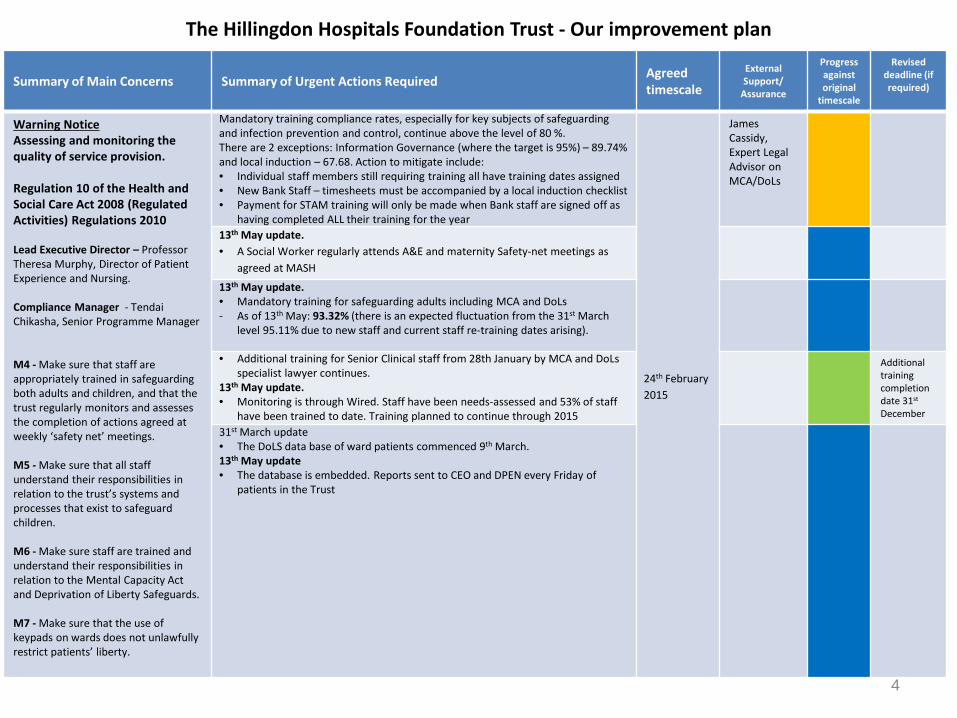
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Warning Notice Assessing and monitoring the quality of service provision. Regulation 10 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 Lead Executive Director – Professor Theresa Murphy, Director of Patient Experience and Nursing. Compliance Manager - Tendai Chikasha, Senior Programme Manager M4 - Make sure that staff are appropriately trained in safeguarding both adults and children, and that the trust regularly monitors and assesses the completion of actions agreed at weekly ‘safety net’ meetings. M5 - Make sure that all staff understand their responsibilities in relation to the trust’s systems and processes that exist to safeguard children. M6 - Make sure staff are trained and understand their responsibilities in relation to the Mental Capacity Act and Deprivation of Liberty Safeguards. M7 - Make sure that the use of keypads on wards does not unlawfully restrict patients’ liberty.
Mandatory training compliance rates, especially for key subjects of safeguarding and infection prevention and control, continue above the level of 80 %. There are 2 exceptions: Information Governance (where the target is 95%) – 89.74% and local induction – 67.68. Action to mitigate include: • Individual staff members still requiring training all have training dates assigned • New Bank Staff – timesheets must be accompanied by a local induction checklist • Payment for STAM training will only be made when Bank staff are signed off as
having completed ALL their training for the year
24th February 2015
James Cassidy, Expert Legal Advisor on MCA/DoLs
13th May update. • A Social Worker regularly attends A&E and maternity Safety-net meetings as
agreed at MASH
13th May update. • Mandatory training for safeguarding adults including MCA and DoLs - As of 13th May: 93.32% (there is an expected fluctuation from the 31st March
level 95.11% due to new staff and current staff re-training dates arising).
• Additional training for Senior Clinical staff from 28th January by MCA and DoLs specialist lawyer continues.
13th May update. • Monitoring is through Wired. Staff have been needs-assessed and 53% of staff
have been trained to date. Training planned to continue through 2015
Additional training completion date 31st December
31st March update • The DoLS data base of ward patients commenced 9th March. 13th May update • The database is embedded. Reports sent to CEO and DPEN every Friday of
patients in the Trust
4
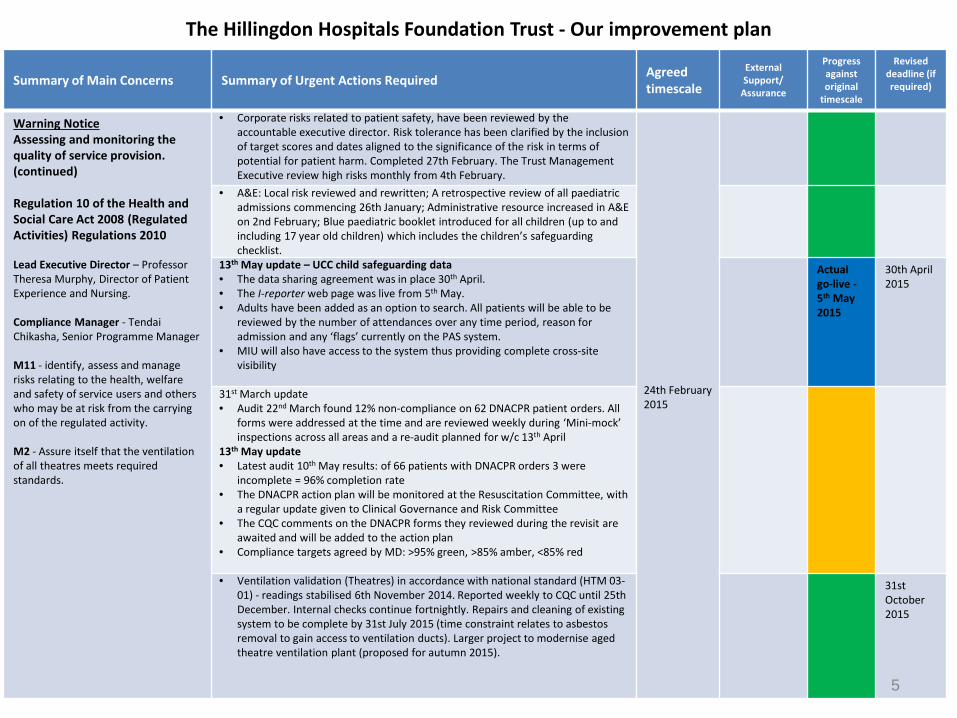
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Warning Notice Assessing and monitoring the quality of service provision. (continued) Regulation 10 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 Lead Executive Director – Professor Theresa Murphy, Director of Patient Experience and Nursing. Compliance Manager - Tendai Chikasha, Senior Programme Manager M11 - identify, assess and manage risks relating to the health, welfare and safety of service users and others who may be at risk from the carrying on of the regulated activity. M2 - Assure itself that the ventilation of all theatres meets required standards.
• Corporate risks related to patient safety, have been reviewed by the accountable executive director. Risk tolerance has been clarified by the inclusion of target scores and dates aligned to the significance of the risk in terms of potential for patient harm. Completed 27th February. The Trust Management Executive review high risks monthly from 4th February.
24th February 2015
• A&E: Local risk reviewed and rewritten; A retrospective review of all paediatric admissions commencing 26th January; Administrative resource increased in A&E on 2nd February; Blue paediatric booklet introduced for all children (up to and including 17 year old children) which includes the children’s safeguarding checklist.
13th May update – UCC child safeguarding data • The data sharing agreement was in place 30th April. • The I-reporter web page was live from 5th May. • Adults have been added as an option to search. All patients will be able to be
reviewed by the number of attendances over any time period, reason for admission and any ‘flags’ currently on the PAS system.
• MIU will also have access to the system thus providing complete cross-site visibility
Actual go-live -5th May 2015
30th April 2015
31st March update • Audit 22nd March found 12% non-compliance on 62 DNACPR patient orders. All
forms were addressed at the time and are reviewed weekly during ‘Mini-mock’ inspections across all areas and a re-audit planned for w/c 13th April
13th May update • Latest audit 10th May results: of 66 patients with DNACPR orders 3 were
incomplete = 96% completion rate • The DNACPR action plan will be monitored at the Resuscitation Committee, with
a regular update given to Clinical Governance and Risk Committee • The CQC comments on the DNACPR forms they reviewed during the revisit are
awaited and will be added to the action plan • Compliance targets agreed by MD: >95% green, >85% amber, <85% red
• Ventilation validation (Theatres) in accordance with national standard (HTM 03-
01) - readings stabilised 6th November 2014. Reported weekly to CQC until 25th December. Internal checks continue fortnightly. Repairs and cleaning of existing system to be complete by 31st July 2015 (time constraint relates to asbestos removal to gain access to ventilation ducts). Larger project to modernise aged theatre ventilation plant (proposed for autumn 2015).
31st October 2015
5
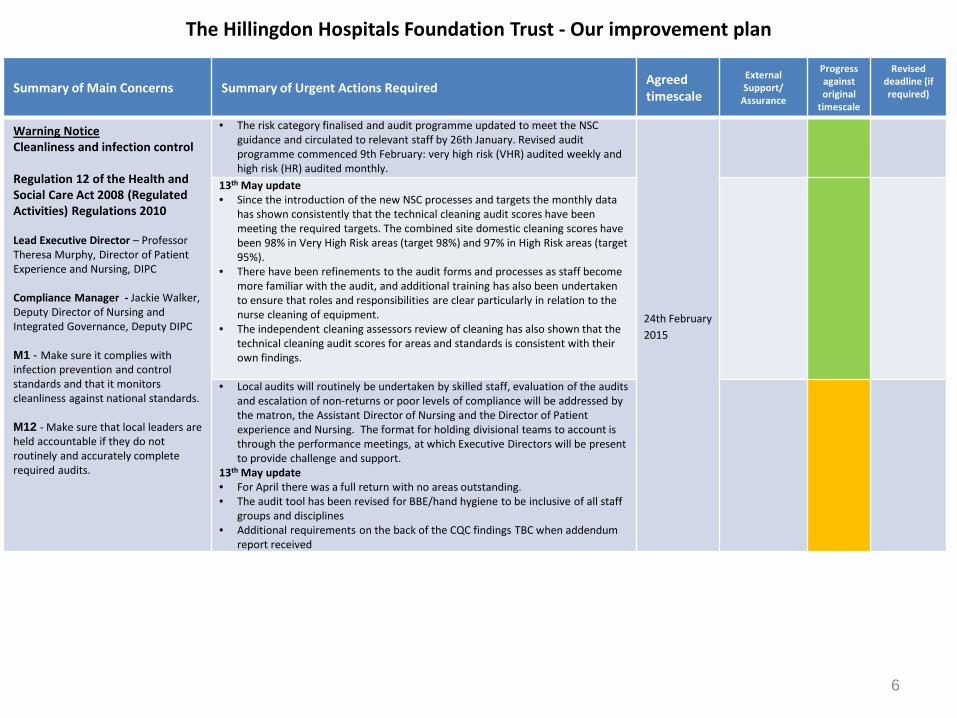
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Warning Notice Cleanliness and infection control Regulation 12 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 Lead Executive Director – Professor Theresa Murphy, Director of Patient Experience and Nursing, DIPC Compliance Manager - Jackie Walker, Deputy Director of Nursing and Integrated Governance, Deputy DIPC M1 - Make sure it complies with infection prevention and control standards and that it monitors cleanliness against national standards. M12 - Make sure that local leaders are held accountable if they do not routinely and accurately complete required audits.
• The risk category finalised and audit programme updated to meet the NSC guidance and circulated to relevant staff by 26th January. Revised audit programme commenced 9th February: very high risk (VHR) audited weekly and high risk (HR) audited monthly.
24th February 2015
13th May update • Since the introduction of the new NSC processes and targets the monthly data
has shown consistently that the technical cleaning audit scores have been meeting the required targets. The combined site domestic cleaning scores have been 98% in Very High Risk areas (target 98%) and 97% in High Risk areas (target 95%).
• There have been refinements to the audit forms and processes as staff become more familiar with the audit, and additional training has also been undertaken to ensure that roles and responsibilities are clear particularly in relation to the nurse cleaning of equipment.
• The independent cleaning assessors review of cleaning has also shown that the technical cleaning audit scores for areas and standards is consistent with their own findings.
• Local audits will routinely be undertaken by skilled staff, evaluation of the audits
and escalation of non-returns or poor levels of compliance will be addressed by the matron, the Assistant Director of Nursing and the Director of Patient experience and Nursing. The format for holding divisional teams to account is through the performance meetings, at which Executive Directors will be present to provide challenge and support.
13th May update • For April there was a full return with no areas outstanding. • The audit tool has been revised for BBE/hand hygiene to be inclusive of all staff
groups and disciplines • Additional requirements on the back of the CQC findings TBC when addendum
report received
6
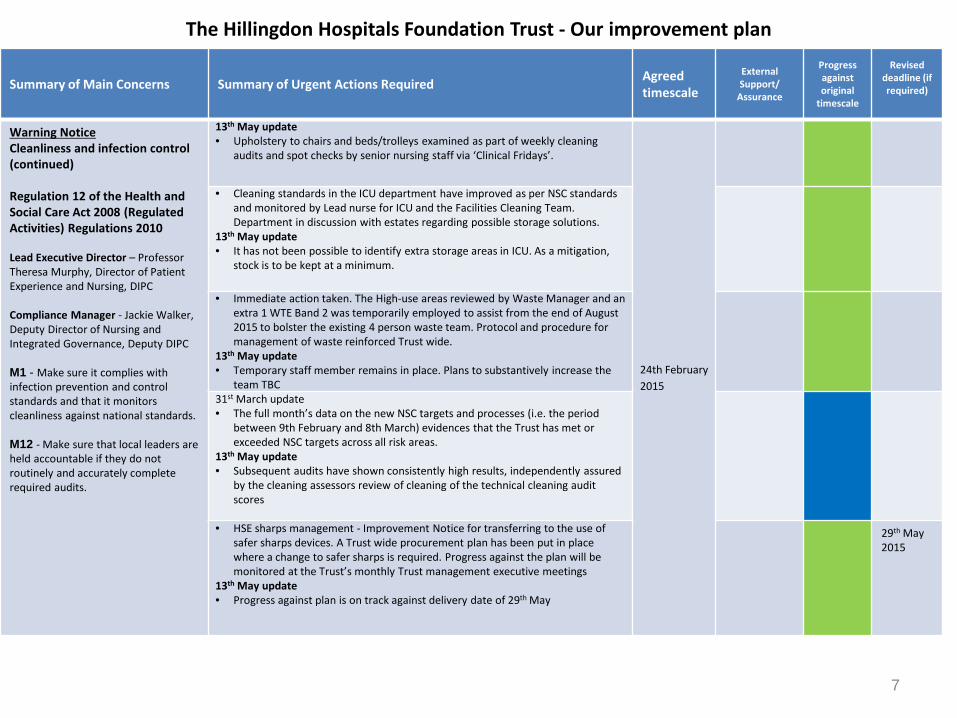
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Warning Notice Cleanliness and infection control (continued) Regulation 12 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 Lead Executive Director – Professor Theresa Murphy, Director of Patient Experience and Nursing, DIPC Compliance Manager - Jackie Walker, Deputy Director of Nursing and Integrated Governance, Deputy DIPC M1 - Make sure it complies with infection prevention and control standards and that it monitors cleanliness against national standards. M12 - Make sure that local leaders are held accountable if they do not routinely and accurately complete required audits.
13th May update • Upholstery to chairs and beds/trolleys examined as part of weekly cleaning
audits and spot checks by senior nursing staff via ‘Clinical Fridays’.
24th February 2015
• Cleaning standards in the ICU department have improved as per NSC standards and monitored by Lead nurse for ICU and the Facilities Cleaning Team. Department in discussion with estates regarding possible storage solutions.
13th May update • It has not been possible to identify extra storage areas in ICU. As a mitigation,
stock is to be kept at a minimum.
• Immediate action taken. The High-use areas reviewed by Waste Manager and an extra 1 WTE Band 2 was temporarily employed to assist from the end of August 2015 to bolster the existing 4 person waste team. Protocol and procedure for management of waste reinforced Trust wide.
13th May update • Temporary staff member remains in place. Plans to substantively increase the
team TBC 31st March update • The full month’s data on the new NSC targets and processes (i.e. the period
between 9th February and 8th March) evidences that the Trust has met or exceeded NSC targets across all risk areas.
13th May update • Subsequent audits have shown consistently high results, independently assured
by the cleaning assessors review of cleaning of the technical cleaning audit scores
• HSE sharps management - Improvement Notice for transferring to the use of safer sharps devices. A Trust wide procurement plan has been put in place where a change to safer sharps is required. Progress against the plan will be monitored at the Trust’s monthly Trust management executive meetings
13th May update • Progress against plan is on track against delivery date of 29th May
29th May 2015
7
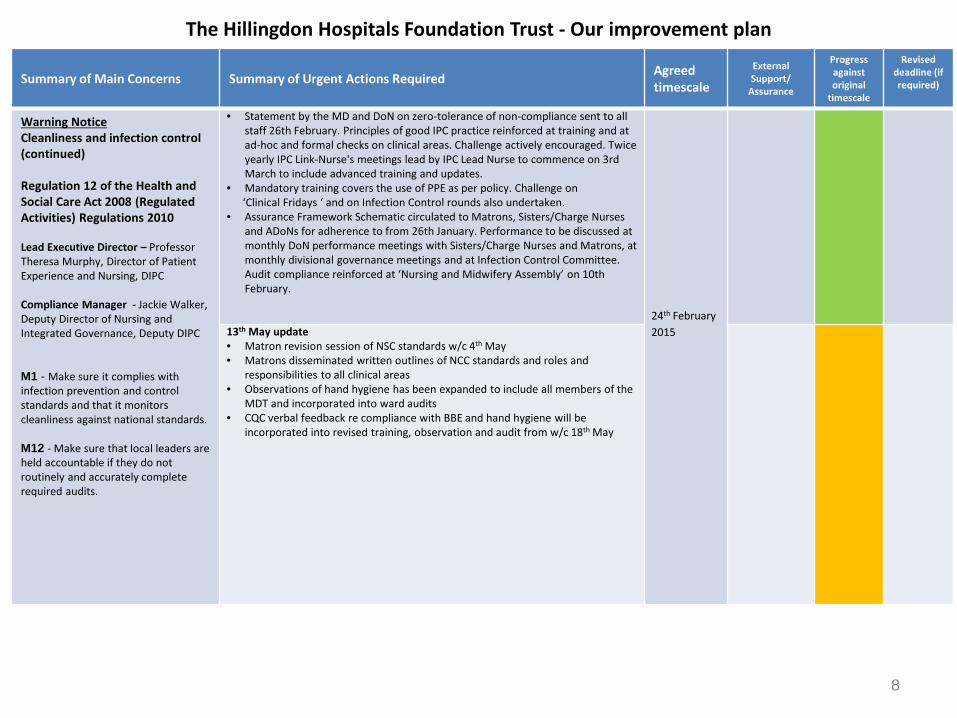
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Warning Notice Cleanliness and infection control (continued) Regulation 12 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 Lead Executive Director – Professor Theresa Murphy, Director of Patient Experience and Nursing, DIPC Compliance Manager - Jackie Walker, Deputy Director of Nursing and Integrated Governance, Deputy DIPC M1 - Make sure it complies with infection prevention and control standards and that it monitors cleanliness against national standards. M12 - Make sure that local leaders are held accountable if they do not routinely and accurately complete required audits.
• Statement by the MD and DoN on zero-tolerance of non-compliance sent to all staff 26th February. Principles of good IPC practice reinforced at training and at ad-hoc and formal checks on clinical areas. Challenge actively encouraged. Twice yearly IPC Link-Nurse's meetings lead by IPC Lead Nurse to commence on 3rd March to include advanced training and updates.
• Mandatory training covers the use of PPE as per policy. Challenge on ‘Clinical Fridays ‘ and on Infection Control rounds also undertaken. • Assurance Framework Schematic circulated to Matrons, Sisters/Charge Nurses
and ADoNs for adherence to from 26th January. Performance to be discussed at monthly DoN performance meetings with Sisters/Charge Nurses and Matrons, at monthly divisional governance meetings and at Infection Control Committee. Audit compliance reinforced at ‘Nursing and Midwifery Assembly’ on 10th February.
24th February 2015
13th May update • Matron revision session of NSC standards w/c 4th May • Matrons disseminated written outlines of NCC standards and roles and
responsibilities to all clinical areas • Observations of hand hygiene has been expanded to include all members of the
MDT and incorporated into ward audits • CQC verbal feedback re compliance with BBE and hand hygiene will be
incorporated into revised training, observation and audit from w/c 18th May
8
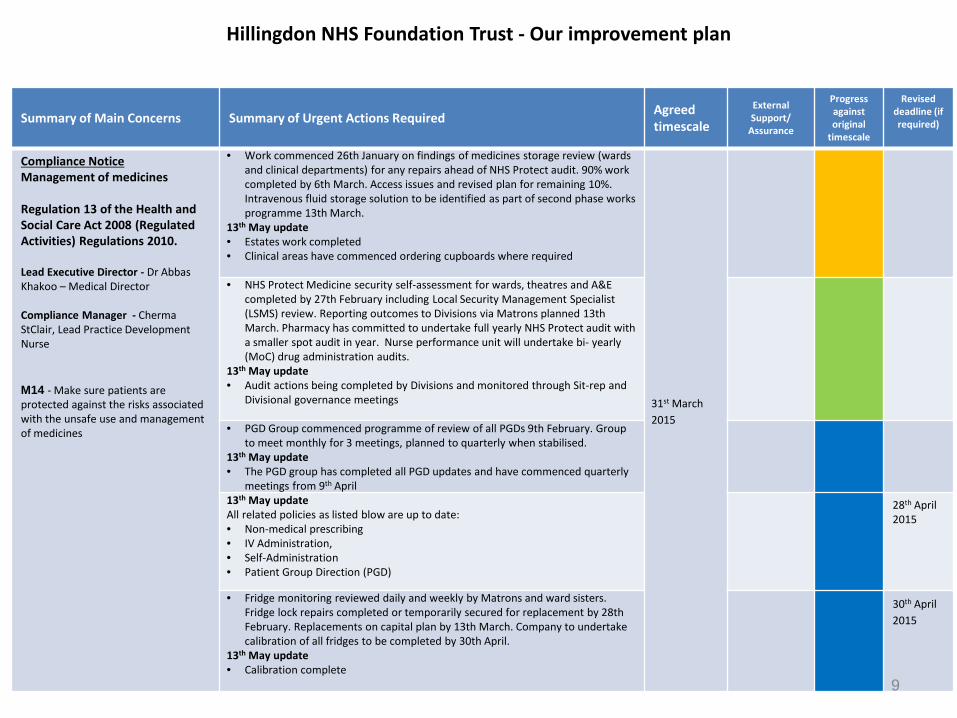
Hillingdon NHS Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Compliance Notice Management of medicines Regulation 13 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010. Lead Executive Director - Dr Abbas Khakoo – Medical Director Compliance Manager - Cherma StClair, Lead Practice Development Nurse M14 - Make sure patients are protected against the risks associated with the unsafe use and management of medicines
• Work commenced 26th January on findings of medicines storage review (wards and clinical departments) for any repairs ahead of NHS Protect audit. 90% work completed by 6th March. Access issues and revised plan for remaining 10%. Intravenous fluid storage solution to be identified as part of second phase works programme 13th March.
13th May update • Estates work completed • Clinical areas have commenced ordering cupboards where required
31st March 2015
• NHS Protect Medicine security self-assessment for wards, theatres and A&E completed by 27th February including Local Security Management Specialist (LSMS) review. Reporting outcomes to Divisions via Matrons planned 13th March. Pharmacy has committed to undertake full yearly NHS Protect audit with a smaller spot audit in year. Nurse performance unit will undertake bi- yearly (MoC) drug administration audits.
13th May update • Audit actions being completed by Divisions and monitored through Sit-rep and
Divisional governance meetings • PGD Group commenced programme of review of all PGDs 9th February. Group
to meet monthly for 3 meetings, planned to quarterly when stabilised. 13th May update • The PGD group has completed all PGD updates and have commenced quarterly
meetings from 9th April 13th May update All related policies as listed blow are up to date: • Non-medical prescribing • IV Administration, • Self-Administration • Patient Group Direction (PGD)
28th April 2015
• Fridge monitoring reviewed daily and weekly by Matrons and ward sisters. Fridge lock repairs completed or temporarily secured for replacement by 28th February. Replacements on capital plan by 13th March. Company to undertake calibration of all fridges to be completed by 30th April.
13th May update • Calibration complete
30th April 2015
9
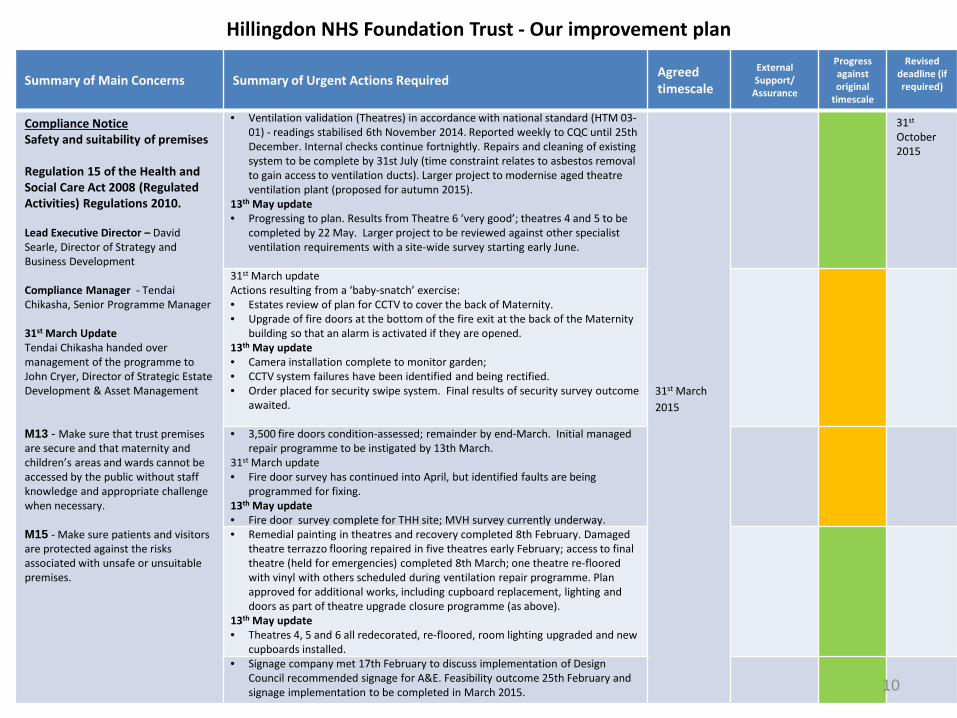
Hillingdon NHS Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Compliance Notice Safety and suitability of premises Regulation 15 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010. Lead Executive Director – David Searle, Director of Strategy and Business Development Compliance Manager - Tendai Chikasha, Senior Programme Manager 31st March Update Tendai Chikasha handed over management of the programme to John Cryer, Director of Strategic Estate Development & Asset Management M13 - Make sure that trust premises are secure and that maternity and children’s areas and wards cannot be accessed by the public without staff knowledge and appropriate challenge when necessary. M15 - Make sure patients and visitors are protected against the risks associated with unsafe or unsuitable premises.
• Ventilation validation (Theatres) in accordance with national standard (HTM 03-01) - readings stabilised 6th November 2014. Reported weekly to CQC until 25th December. Internal checks continue fortnightly. Repairs and cleaning of existing system to be complete by 31st July (time constraint relates to asbestos removal to gain access to ventilation ducts). Larger project to modernise aged theatre ventilation plant (proposed for autumn 2015).
13th May update • Progressing to plan. Results from Theatre 6 ‘very good’; theatres 4 and 5 to be
completed by 22 May. Larger project to be reviewed against other specialist ventilation requirements with a site-wide survey starting early June.
31st March 2015
31st October 2015
31st March update Actions resulting from a ‘baby-snatch’ exercise: • Estates review of plan for CCTV to cover the back of Maternity. • Upgrade of fire doors at the bottom of the fire exit at the back of the Maternity
building so that an alarm is activated if they are opened. 13th May update • Camera installation complete to monitor garden; • CCTV system failures have been identified and being rectified. • Order placed for security swipe system. Final results of security survey outcome
awaited. • 3,500 fire doors condition-assessed; remainder by end-March. Initial managed
repair programme to be instigated by 13th March. 31st March update • Fire door survey has continued into April, but identified faults are being
programmed for fixing. 13th May update • Fire door survey complete for THH site; MVH survey currently underway. • Remedial painting in theatres and recovery completed 8th February. Damaged
theatre terrazzo flooring repaired in five theatres early February; access to final theatre (held for emergencies) completed 8th March; one theatre re-floored with vinyl with others scheduled during ventilation repair programme. Plan approved for additional works, including cupboard replacement, lighting and doors as part of theatre upgrade closure programme (as above).
13th May update • Theatres 4, 5 and 6 all redecorated, re-floored, room lighting upgraded and new
cupboards installed. • Signage company met 17th February to discuss implementation of Design
Council recommended signage for A&E. Feasibility outcome 25th February and signage implementation to be completed in March 2015. 10
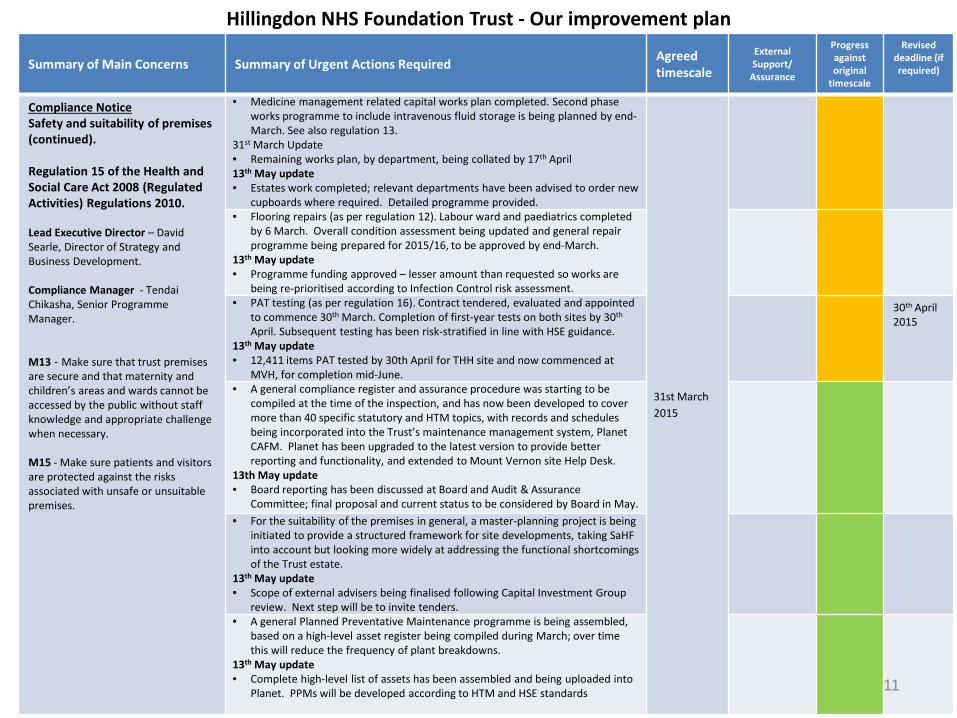
Hillingdon NHS Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Compliance Notice Safety and suitability of premises (continued). Regulation 15 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010. Lead Executive Director – David Searle, Director of Strategy and Business Development. Compliance Manager - Tendai Chikasha, Senior Programme Manager. M13 - Make sure that trust premises are secure and that maternity and children’s areas and wards cannot be accessed by the public without staff knowledge and appropriate challenge when necessary. M15 - Make sure patients and visitors are protected against the risks associated with unsafe or unsuitable premises.
• Medicine management related capital works plan completed. Second phase works programme to include intravenous fluid storage is being planned by end-March. See also regulation 13.
31st March Update • Remaining works plan, by department, being collated by 17th April 13th May update • Estates work completed; relevant departments have been advised to order new
cupboards where required. Detailed programme provided.
31st March 2015
• Flooring repairs (as per regulation 12). Labour ward and paediatrics completed by 6 March. Overall condition assessment being updated and general repair programme being prepared for 2015/16, to be approved by end-March.
13th May update • Programme funding approved – lesser amount than requested so works are
being re-prioritised according to Infection Control risk assessment. • PAT testing (as per regulation 16). Contract tendered, evaluated and appointed
to commence 30th March. Completion of first-year tests on both sites by 30th April. Subsequent testing has been risk-stratified in line with HSE guidance.
13th May update • 12,411 items PAT tested by 30th April for THH site and now commenced at
MVH, for completion mid-June.
30th April 2015
• A general compliance register and assurance procedure was starting to be compiled at the time of the inspection, and has now been developed to cover more than 40 specific statutory and HTM topics, with records and schedules being incorporated into the Trust’s maintenance management system, Planet CAFM. Planet has been upgraded to the latest version to provide better reporting and functionality, and extended to Mount Vernon site Help Desk.
13th May update • Board reporting has been discussed at Board and Audit & Assurance
Committee; final proposal and current status to be considered by Board in May. • For the suitability of the premises in general, a master-planning project is being
initiated to provide a structured framework for site developments, taking SaHF into account but looking more widely at addressing the functional shortcomings of the Trust estate.
13th May update • Scope of external advisers being finalised following Capital Investment Group
review. Next step will be to invite tenders. • A general Planned Preventative Maintenance programme is being assembled,
based on a high-level asset register being compiled during March; over time this will reduce the frequency of plant breakdowns.
13th May update • Complete high-level list of assets has been assembled and being uploaded into
Planet. PPMs will be developed according to HTM and HSE standards
11
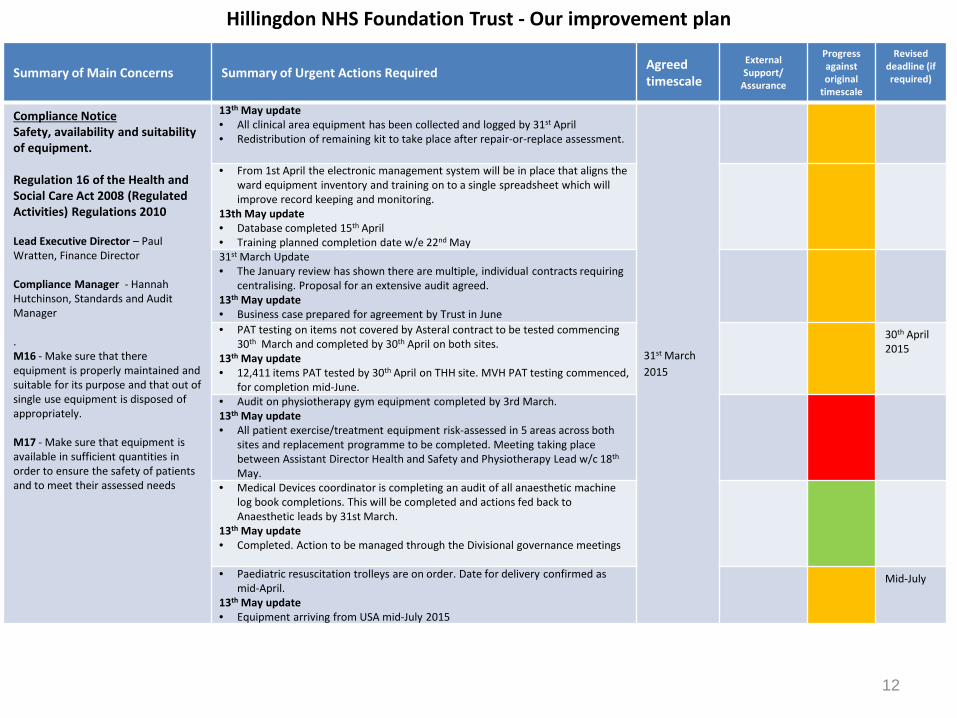
Hillingdon NHS Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Compliance Notice Safety, availability and suitability of equipment. Regulation 16 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 Lead Executive Director – Paul Wratten, Finance Director Compliance Manager - Hannah Hutchinson, Standards and Audit Manager . M16 - Make sure that there equipment is properly maintained and suitable for its purpose and that out of single use equipment is disposed of appropriately. M17 - Make sure that equipment is available in sufficient quantities in order to ensure the safety of patients and to meet their assessed needs
13th May update • All clinical area equipment has been collected and logged by 31st April • Redistribution of remaining kit to take place after repair-or-replace assessment.
31st March 2015
• From 1st April the electronic management system will be in place that aligns the ward equipment inventory and training on to a single spreadsheet which will improve record keeping and monitoring.
13th May update • Database completed 15th April • Training planned completion date w/e 22nd May 31st March Update • The January review has shown there are multiple, individual contracts requiring
centralising. Proposal for an extensive audit agreed. 13th May update • Business case prepared for agreement by Trust in June • PAT testing on items not covered by Asteral contract to be tested commencing
30th March and completed by 30th April on both sites. 13th May update • 12,411 items PAT tested by 30th April on THH site. MVH PAT testing commenced,
for completion mid-June.
30th April 2015
• Audit on physiotherapy gym equipment completed by 3rd March. 13th May update • All patient exercise/treatment equipment risk-assessed in 5 areas across both
sites and replacement programme to be completed. Meeting taking place between Assistant Director Health and Safety and Physiotherapy Lead w/c 18th May.
• Medical Devices coordinator is completing an audit of all anaesthetic machine log book completions. This will be completed and actions fed back to Anaesthetic leads by 31st March.
13th May update • Completed. Action to be managed through the Divisional governance meetings
• Paediatric resuscitation trolleys are on order. Date for delivery confirmed as
mid-April. 13th May update • Equipment arriving from USA mid-July 2015
Mid-July
12
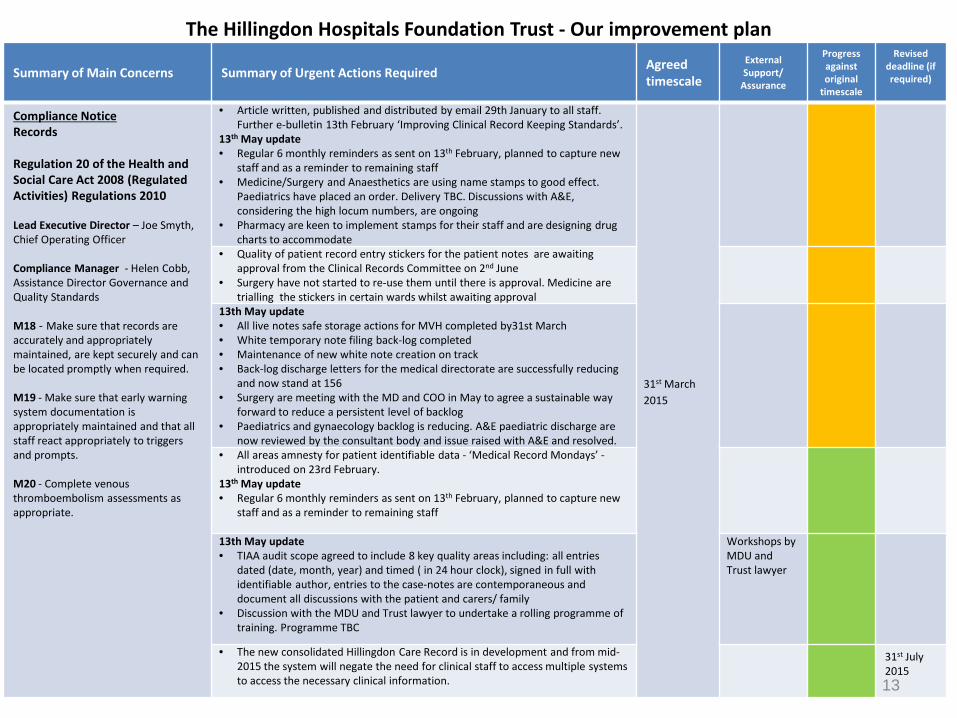
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Compliance Notice Records Regulation 20 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 Lead Executive Director – Joe Smyth, Chief Operating Officer Compliance Manager - Helen Cobb, Assistance Director Governance and Quality Standards M18 - Make sure that records are accurately and appropriately maintained, are kept securely and can be located promptly when required. M19 - Make sure that early warning system documentation is appropriately maintained and that all staff react appropriately to triggers and prompts. M20 - Complete venous thromboembolism assessments as appropriate.
• Article written, published and distributed by email 29th January to all staff. Further e-bulletin 13th February ‘Improving Clinical Record Keeping Standards’.
13th May update • Regular 6 monthly reminders as sent on 13th February, planned to capture new
staff and as a reminder to remaining staff • Medicine/Surgery and Anaesthetics are using name stamps to good effect.
Paediatrics have placed an order. Delivery TBC. Discussions with A&E, considering the high locum numbers, are ongoing
• Pharmacy are keen to implement stamps for their staff and are designing drug charts to accommodate
31st March 2015
• Quality of patient record entry stickers for the patient notes are awaiting approval from the Clinical Records Committee on 2nd June
• Surgery have not started to re-use them until there is approval. Medicine are trialling the stickers in certain wards whilst awaiting approval
13th May update • All live notes safe storage actions for MVH completed by31st March • White temporary note filing back-log completed • Maintenance of new white note creation on track • Back-log discharge letters for the medical directorate are successfully reducing
and now stand at 156 • Surgery are meeting with the MD and COO in May to agree a sustainable way
forward to reduce a persistent level of backlog • Paediatrics and gynaecology backlog is reducing. A&E paediatric discharge are
now reviewed by the consultant body and issue raised with A&E and resolved. • All areas amnesty for patient identifiable data - ‘Medical Record Mondays’ -
introduced on 23rd February. 13th May update • Regular 6 monthly reminders as sent on 13th February, planned to capture new
staff and as a reminder to remaining staff 13th May update • TIAA audit scope agreed to include 8 key quality areas including: all entries
dated (date, month, year) and timed ( in 24 hour clock), signed in full with identifiable author, entries to the case-notes are contemporaneous and document all discussions with the patient and carers/ family
• Discussion with the MDU and Trust lawyer to undertake a rolling programme of training. Programme TBC
Workshops by MDU and Trust lawyer
• The new consolidated Hillingdon Care Record is in development and from mid-2015 the system will negate the need for clinical staff to access multiple systems to access the necessary clinical information.
31st July 2015 13
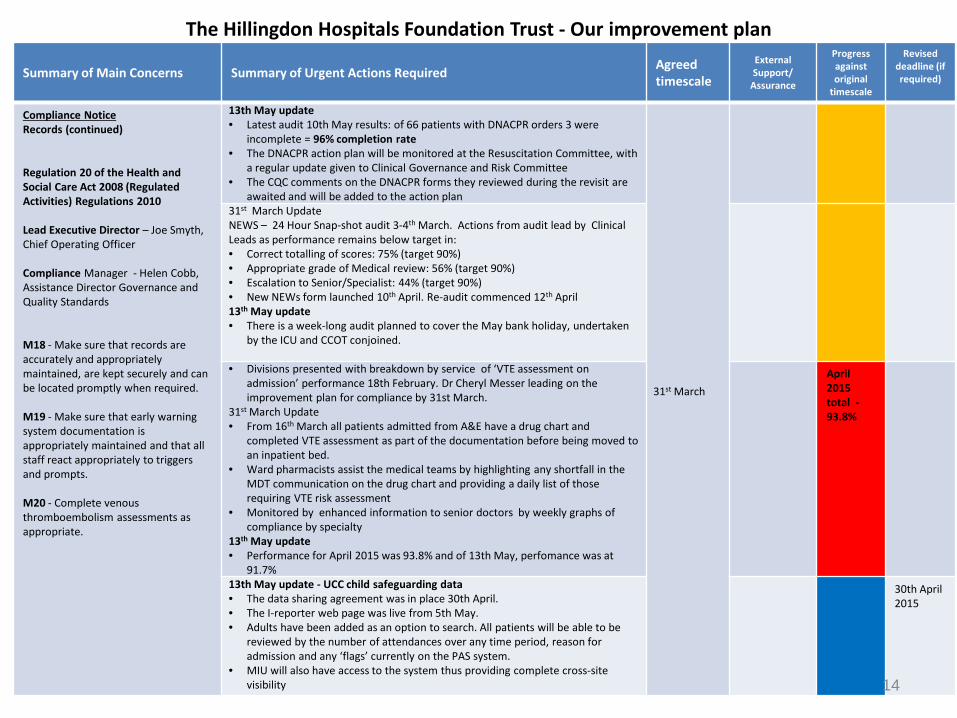
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Compliance Notice Records (continued) Regulation 20 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010 Lead Executive Director – Joe Smyth, Chief Operating Officer Compliance Manager - Helen Cobb, Assistance Director Governance and Quality Standards M18 - Make sure that records are accurately and appropriately maintained, are kept securely and can be located promptly when required. M19 - Make sure that early warning system documentation is appropriately maintained and that all staff react appropriately to triggers and prompts. M20 - Complete venous thromboembolism assessments as appropriate.
13th May update • Latest audit 10th May results: of 66 patients with DNACPR orders 3 were
incomplete = 96% completion rate • The DNACPR action plan will be monitored at the Resuscitation Committee, with
a regular update given to Clinical Governance and Risk Committee • The CQC comments on the DNACPR forms they reviewed during the revisit are
awaited and will be added to the action plan
31st March
31st March Update NEWS – 24 Hour Snap-shot audit 3-4th March. Actions from audit lead by Clinical Leads as performance remains below target in: • Correct totalling of scores: 75% (target 90%) • Appropriate grade of Medical review: 56% (target 90%) • Escalation to Senior/Specialist: 44% (target 90%) • New NEWs form launched 10th April. Re-audit commenced 12th April 13th May update • There is a week-long audit planned to cover the May bank holiday, undertaken
by the ICU and CCOT conjoined. • Divisions presented with breakdown by service of ‘VTE assessment on
admission’ performance 18th February. Dr Cheryl Messer leading on the improvement plan for compliance by 31st March.
31st March Update • From 16th March all patients admitted from A&E have a drug chart and
completed VTE assessment as part of the documentation before being moved to an inpatient bed.
• Ward pharmacists assist the medical teams by highlighting any shortfall in the MDT communication on the drug chart and providing a daily list of those requiring VTE risk assessment
• Monitored by enhanced information to senior doctors by weekly graphs of compliance by specialty
13th May update • Performance for April 2015 was 93.8% and of 13th May, perfomance was at
91.7%
April 2015 total - 93.8%
13th May update - UCC child safeguarding data • The data sharing agreement was in place 30th April. • The I-reporter web page was live from 5th May. • Adults have been added as an option to search. All patients will be able to be
reviewed by the number of attendances over any time period, reason for admission and any ‘flags’ currently on the PAS system.
• MIU will also have access to the system thus providing complete cross-site visibility
30th April 2015
14
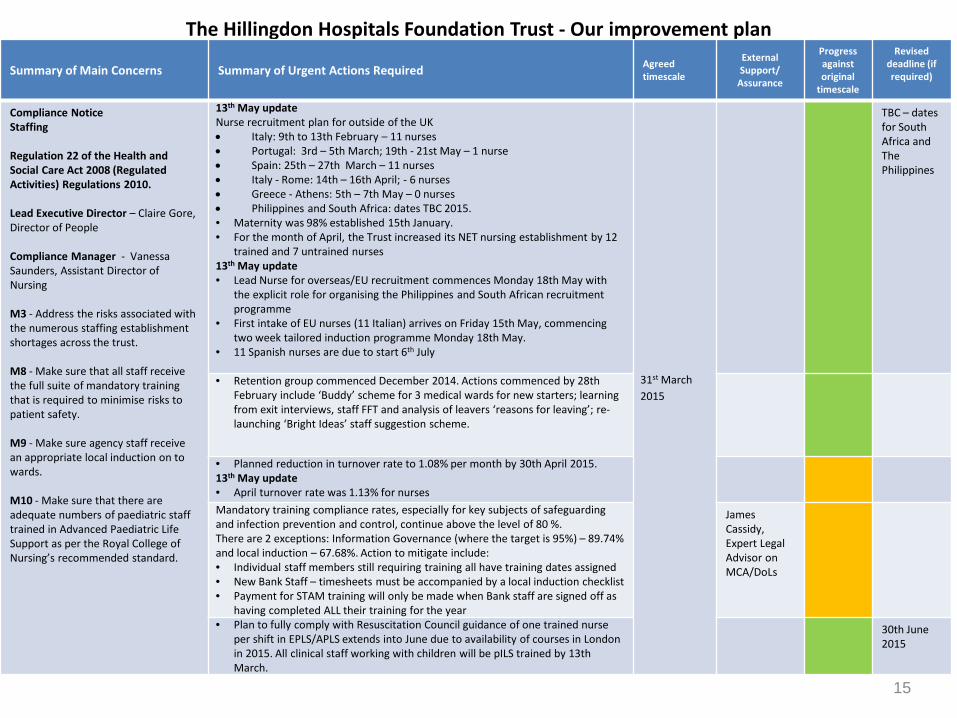
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Compliance Notice Staffing Regulation 22 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010. Lead Executive Director – Claire Gore, Director of People Compliance Manager - Vanessa Saunders, Assistant Director of Nursing M3 - Address the risks associated with the numerous staffing establishment shortages across the trust. M8 - Make sure that all staff receive the full suite of mandatory training that is required to minimise risks to patient safety. M9 - Make sure agency staff receive an appropriate local induction on to wards. M10 - Make sure that there are adequate numbers of paediatric staff trained in Advanced Paediatric Life Support as per the Royal College of Nursing’s recommended standard.
13th May update Nurse recruitment plan for outside of the UK • Italy: 9th to 13th February – 11 nurses • Portugal: 3rd – 5th March; 19th - 21st May – 1 nurse • Spain: 25th – 27th March – 11 nurses • Italy - Rome: 14th – 16th April; - 6 nurses • Greece - Athens: 5th – 7th May – 0 nurses • Philippines and South Africa: dates TBC 2015. • Maternity was 98% established 15th January. • For the month of April, the Trust increased its NET nursing establishment by 12
trained and 7 untrained nurses 13th May update • Lead Nurse for overseas/EU recruitment commences Monday 18th May with
the explicit role for organising the Philippines and South African recruitment programme
• First intake of EU nurses (11 Italian) arrives on Friday 15th May, commencing two week tailored induction programme Monday 18th May.
• 11 Spanish nurses are due to start 6th July
31st March 2015
TBC – dates for South Africa and The Philippines
• Retention group commenced December 2014. Actions commenced by 28th February include ‘Buddy’ scheme for 3 medical wards for new starters; learning from exit interviews, staff FFT and analysis of leavers ‘reasons for leaving’; re-launching ‘Bright Ideas’ staff suggestion scheme.
• Planned reduction in turnover rate to 1.08% per month by 30th April 2015. 13th May update • April turnover rate was 1.13% for nurses Mandatory training compliance rates, especially for key subjects of safeguarding and infection prevention and control, continue above the level of 80 %. There are 2 exceptions: Information Governance (where the target is 95%) – 89.74% and local induction – 67.68%. Action to mitigate include: • Individual staff members still requiring training all have training dates assigned • New Bank Staff – timesheets must be accompanied by a local induction checklist • Payment for STAM training will only be made when Bank staff are signed off as
having completed ALL their training for the year
James Cassidy, Expert Legal Advisor on MCA/DoLs
• Plan to fully comply with Resuscitation Council guidance of one trained nurse per shift in EPLS/APLS extends into June due to availability of courses in London in 2015. All clinical staff working with children will be pILS trained by 13th March.
30th June 2015
15
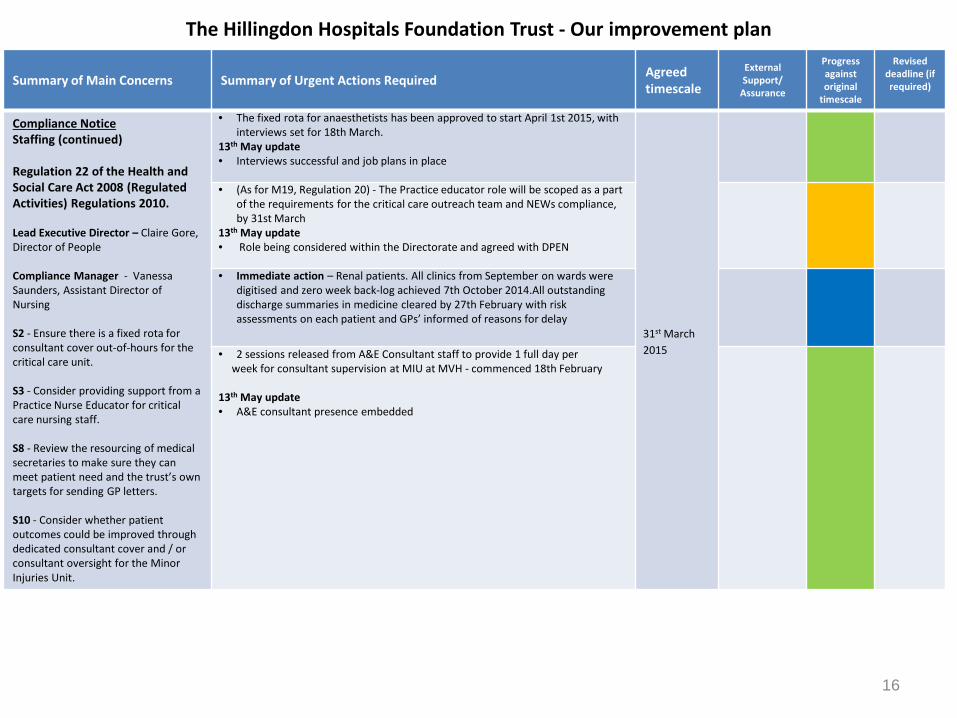
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Compliance Notice Staffing (continued) Regulation 22 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010. Lead Executive Director – Claire Gore, Director of People Compliance Manager - Vanessa Saunders, Assistant Director of Nursing S2 - Ensure there is a fixed rota for consultant cover out-of-hours for the critical care unit. S3 - Consider providing support from a Practice Nurse Educator for critical care nursing staff. S8 - Review the resourcing of medical secretaries to make sure they can meet patient need and the trust’s own targets for sending GP letters. S10 - Consider whether patient outcomes could be improved through dedicated consultant cover and / or consultant oversight for the Minor Injuries Unit.
• The fixed rota for anaesthetists has been approved to start April 1st 2015, with interviews set for 18th March.
13th May update • Interviews successful and job plans in place
31st March 2015
• (As for M19, Regulation 20) - The Practice educator role will be scoped as a part of the requirements for the critical care outreach team and NEWs compliance, by 31st March
13th May update • Role being considered within the Directorate and agreed with DPEN
• Immediate action – Renal patients. All clinics from September on wards were
digitised and zero week back-log achieved 7th October 2014.All outstanding discharge summaries in medicine cleared by 27th February with risk assessments on each patient and GPs’ informed of reasons for delay
• 2 sessions released from A&E Consultant staff to provide 1 full day per week for consultant supervision at MIU at MVH - commenced 18th February 13th May update • A&E consultant presence embedded
16
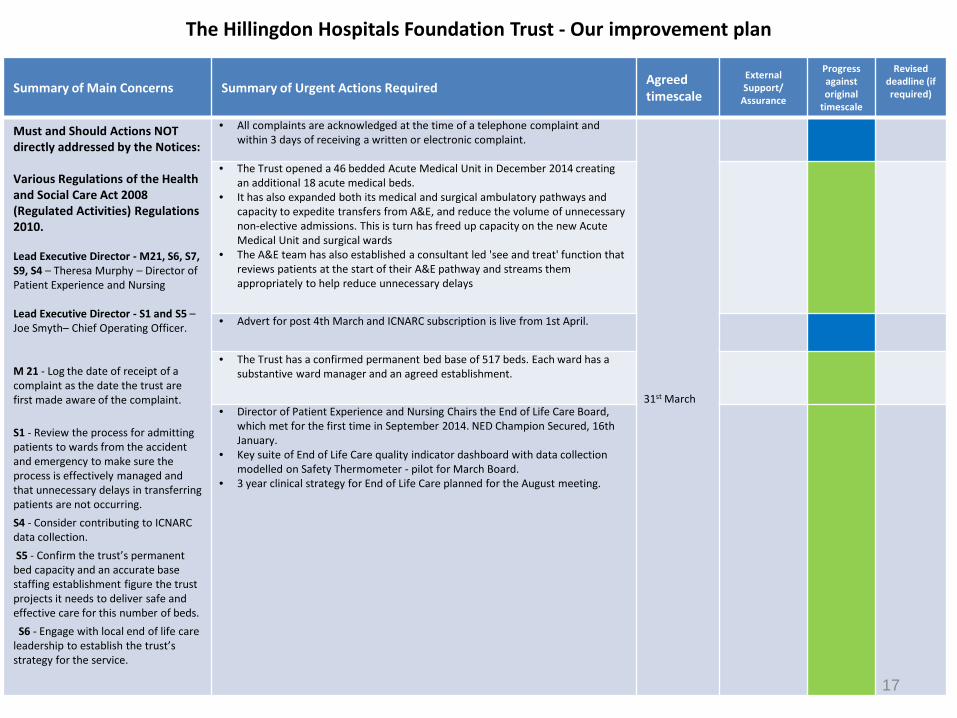
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Must and Should Actions NOT directly addressed by the Notices: Various Regulations of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010. Lead Executive Director - M21, S6, S7, S9, S4 – Theresa Murphy – Director of Patient Experience and Nursing Lead Executive Director - S1 and S5 – Joe Smyth– Chief Operating Officer. M 21 - Log the date of receipt of a complaint as the date the trust are first made aware of the complaint. S1 - Review the process for admitting patients to wards from the accident and emergency to make sure the process is effectively managed and that unnecessary delays in transferring patients are not occurring. S4 - Consider contributing to ICNARC data collection. S5 - Confirm the trust’s permanent bed capacity and an accurate base staffing establishment figure the trust projects it needs to deliver safe and effective care for this number of beds. S6 - Engage with local end of life care leadership to establish the trust’s strategy for the service.
• All complaints are acknowledged at the time of a telephone complaint and within 3 days of receiving a written or electronic complaint.
31st March
• The Trust opened a 46 bedded Acute Medical Unit in December 2014 creating an additional 18 acute medical beds.
• It has also expanded both its medical and surgical ambulatory pathways and capacity to expedite transfers from A&E, and reduce the volume of unnecessary non-elective admissions. This is turn has freed up capacity on the new Acute Medical Unit and surgical wards
• The A&E team has also established a consultant led 'see and treat' function that reviews patients at the start of their A&E pathway and streams them appropriately to help reduce unnecessary delays
• Advert for post 4th March and ICNARC subscription is live from 1st April.
• The Trust has a confirmed permanent bed base of 517 beds. Each ward has a substantive ward manager and an agreed establishment.
• Director of Patient Experience and Nursing Chairs the End of Life Care Board, which met for the first time in September 2014. NED Champion Secured, 16th January.
• Key suite of End of Life Care quality indicator dashboard with data collection modelled on Safety Thermometer - pilot for March Board.
• 3 year clinical strategy for End of Life Care planned for the August meeting.
17
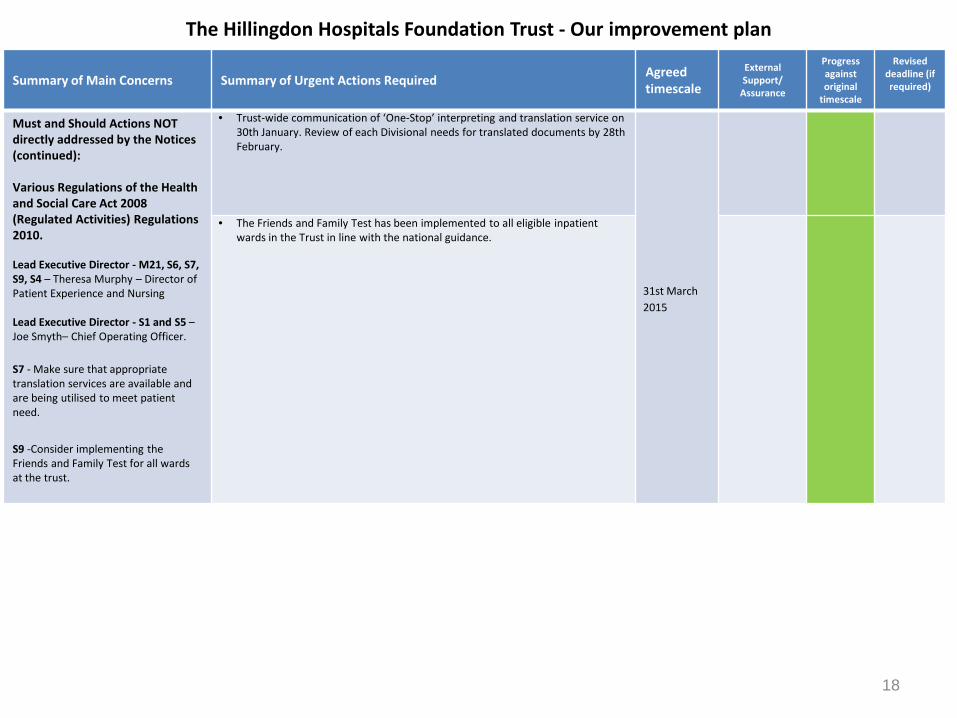
The Hillingdon Hospitals Foundation Trust - Our improvement plan
Summary of Main Concerns Summary of Urgent Actions Required Agreed timescale
External Support/
Assurance
Progress against original
timescale
Revised deadline (if required)
Must and Should Actions NOT directly addressed by the Notices (continued): Various Regulations of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2010.
Lead Executive Director - M21, S6, S7, S9, S4 – Theresa Murphy – Director of Patient Experience and Nursing
Lead Executive Director - S1 and S5 – Joe Smyth– Chief Operating Officer.
S7 - Make sure that appropriate translation services are available and are being utilised to meet patient need. S9 -Consider implementing the Friends and Family Test for all wards at the trust.
• Trust-wide communication of ‘One-Stop’ interpreting and translation service on 30th January. Review of each Divisional needs for translated documents by 28th February.
31st March 2015
• The Friends and Family Test has been implemented to all eligible inpatient wards in the Trust in line with the national guidance.
18
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 21
Annual Report and Accounts 2014/15 Reason for item: To enable the Board to approve the annual report and accounts. Summary: This paper presents the audited annual report and accounts for 2014/15 for the Board’s formal approval, prior to submission to Monitor on 29th May 2015 and subsequent laying before Parliament. The quality report will also separately be published as the Trust’s Quality Account on the NHS Choices website as per Department of Health requirements. The audited annual report and accounts will be circulated separately to the main agenda pack for the Board meeting as the audit remains underway at the time of the publication of the Board papers. Board action required: The Board is asked to:
1. Review the updated report outlining the basis for the audited accounts being prepared on a going concern basis.
2. Confirm whether there have been any post-balance sheet events that should be disclosed in the annual report.
3. Confirm the position agreed at the April Board meeting that:
• As far as each Director is aware, there is no relevant audit information of which the Trust’s auditors are unaware, and all Directors have taken all the steps that they ought to have taken as a Director to make themselves aware of any relevant audit information and to establish that the Trust’s auditors are aware of that information; and
• The annual report and accounts taken as a whole, is fair, balanced, and understandable and provides the information necessary for patients, regulators and stakeholders to assess the Trust’s performance, business model and strategy.
4. Review and approve the audited annual report and accounts 2014/15.
5. Authorise the Chief Executive to sign the strategic report, statement of financial position, annual report, foreword to the accounts, the annual governance statement, and the remuneration report.
6. Authorise the Chair and Chief Executive to sign the statement of Directors’ responsibilities in respect of the quality report.
7. Authorise the Chief Executive to sign the management representations letter to the external auditors.
1

Report from: David Coombs, Trust Secretary (annual report); Helen Cobb (annual governance statement); Wendy Cookson, Interim Director of Compliance (quality report); Jacob Manashe, Head of Financial Accounting (annual accounts) Report sponsor: Paul Wratten, Finance Director, Theresa Murphy, Director of Patient Experience & Nursing, Shane DeGaris, Chief Executive Links to Trust strategic priorities: n/a Previous consideration at Board or Committees: Audit & Assurance and Quality & Risk Committees in April and May; Board in April. Equality and diversity considerations: none. Financial implications: none.
2
Annual Report and Accounts 2014/15
Background and process
1. In line with the NHS Act 2006, the Foundation Trust Constitution requires the Trust to prepare an annual report and submit it to Monitor. The required content for the annual report is laid out in the Annual Reporting Manual (ARM) which is published by Monitor. The ARM states that the annual report and accounts must consist of: • The annual report which includes the strategic report, directors’ report, quality
report and remuneration report • The accounting officer’s statement of responsibilities • The auditor’s opinion and certificate • The annual governance statement • The foreword to the accounts which should state that the accounts are prepared
in accordance with paragraphs 24 and 25 of Schedule 7 to the 2006 Act • Four primary financial statements (Statement of Comprehensive Income,
Statement of Financial Position, Statement of Changes in Taxpayers’ Equity and a Statement of Cash Flows)
• The notes to the accounts. 2. A report to the April Board outlined the arrangements for the submission of the
audited annual report and accounts, and the timescale for this submission and subsequent circulation. In summary, the key remaining deadlines and dates are:
• Submission of audited annual report and accounts, and external audit reports to Monitor
29th May
• Laying of annual report and accounts before Parliament
Posted to arrive before 25th June
• Copy of the annual report and accounts that was laid before Parliament to be submitted to Monitor
10th July
• Annual report, accounts and auditor’s report presented to the Council of Governors
27th July
3. After adoption by the Board, the Chief Executive, as the Accounting Officer, must
sign and date the Statement of Financial Position and annual report as evidence of this. As Accounting Officer, the Chief Executive must also sign the foreword to the accounts, the annual governance statement and the remuneration report. The signed documents will then be sent to the external auditor for signature, and then returned back to the Trust for submission on 29th May.
4. The annual report submitted on 29th May must include all of the text which will be included in the final publication submitted to Parliament. This is because the auditors need to see the form of the annual report prior to signing their opinions. The period
3
between 29th May and submission to Parliament is to allow FTs time to format the document to the standards required for publication. Until the annual report and accounts have been laid before Parliament nothing can be published by the FT for the wider public. Once laid before Parliament the annual report and accounts cannot be changed.
Annual report
5. A draft of the annual report was reviewed at the April Board and Audit & Assurance Committee (AAC) meetings. The remaining gaps have been closed and the amendments requested by Board members made. The document has also been reviewed by the external auditor as required by the ARM. Quality report
6. The draft quality report has previously been reviewed by the AAC, Quality & Risk
Committee (QRC), and the Board. The quality report includes the comments from the consulted stakeholders: the Overview & Scrutiny Committee, Hillingdon Healthwatch, and the host commissioner. The Council of Governors also reviewed the draft at their meeting on 5th May 2015.
Annual accounts
7. The draft annual accounts were submitted to Monitor and external audit in line with
the 23rd April deadline. 8. The draft annual accounts are consistent with the monthly reporting to the Board.
They show a revenue statement deficit of £5.604m for the year. The cash balance ended the year at £5.4 above plan by £1.9m. The accounts also show the Foundation Trust ended the year with a continuity of services risk rating of 3.
9. A going concern report has been written for consideration by Trust Directors. It has
taken account of the points raised at the last AAC meeting. In particular, it reflects the impact of the current main financial risks facing the Trust and how they could be mitigated. It also clarifies the cash headroom available for the year and confirms plans are set to achieve positive cash balances for each month in 2015/16 and 2016/17. Post balance sheet events
10. The annual report and accounts should also include any important events since the
end of the 2014/15 financial year affecting the Foundation Trust. At the Board meeting in April, Board members agreed that no disclosures were required at that time. The Board is asked to confirm that there have subsequently been no events that require disclosure. Disclosures to the external auditors
11. The Directors’ report must contain a statement to the effect that for each individual who was a Director at the time that this report was approved:
4
• so far as the Director is aware, there is no relevant audit information of which the NHS Foundation Trust’s auditor is unaware; and
• the Director has taken all the steps that they ought to have taken as a Director in order to make themselves aware of any relevant audit information and to establish that the NHS Foundation Trust’s auditor is aware of that information.
12. The Annual Reporting Manual states that ‘relevant audit information’ means information needed by the auditor in connection with preparing their report, and that a director is regarded as having taken all the steps that they ought to have taken as a director in order to do the things mentioned above, and: • ‘made such enquiries of his/her fellow directors and of the company’s auditors for
that purpose; and • taken such other steps (if any) for that purpose, as are required by his/her duty as
a director of the company to exercise reasonable care, skill and diligence.’
13. Board members confirmed this position at the April Board and are asked to confirm that this remains valid. Balanced and comprehensive picture
14. The Board must also confirm that the Directors consider that the annual report and accounts taken as a whole, is fair, balanced, and understandable and provides the information necessary for patients, regulators and stakeholders to assess the Trust’s performance, business model and strategy. Board members agreed at the April Board meeting that this statement could be made, drawing on the recommendation of the AAC. In signing off the annual report and accounts at this meeting the Board is asked to formally note this requirement and confirm this statement.
5
The Hillingdon Hospitals NHS Foundation Trust (‘THH’) Going Concern 2014/15 Draft The Hillingdon Hospitals Foundation Trust (‘the Trust’) Accounts for the year ended 31 March 2015 Confirming the going concern basis and related disclosures 1. Opinion of the Executive Directors 1.1 Having considered the Trust’s circumstances, including the factors noted in this paper, the Executive Directors of the Trust are of the opinion that: (a) there are no significant doubts about the Trust’s ability to continue as a
going concern; (b) it is appropriate to prepare the accounts for the year ended 31 March 2015
on the going concern basis; (c) there are no significant uncertainties affecting the Trust’s ability to continue
as a going concern that should be disclosed in the accounts to ensure that those accounts give a true and fair view other than the uncertainties, if any, noted in section 4; and
(d) They have complied with relevant accounting requirements in forming their opinion.
2. Action requested of the Board of Directors (‘BoD’) 2.1 The Executive Directors invite the BoD to concur with that opinion, taking account of: (a) the matters noted in this paper; (b) the views of the Audit and Assurance Committee; (c) any other relevant factors of which they are aware. 3. Key factors considered by the executive directors 3.1 In forming their opinion the Executive Directors have considered the Trust’s circumstances that may give rise to significant business risks. The Executive Directors consider the Trust’s system of risk detection and management together with committee reporting identifies and adequately addresses any such material risks. The Executive Directors have also considered the Trust’s historical record of financial management and performance and other financial and non-financial factors including those noted below; including any risk analysis prepared by the Trust relating to the factors considered. The Executive Directors consider the BoD has been appropriately involved with all these factors. Annual accounts 3.2 The Trust’s audited accounts for 2013/14 reported an operating surplus of £5.7m and a surplus for the year of £0.3m excluding impairments. The draft accounts for 2014/15 report an operating surplus of £2.9m and a deficit for the year of £3.0m; 1.4% of turnover excluding impairments and gains on investment property. In both years the Trust ended with a closing cash surplus of £5.7m in 2013/14 and £5.4m in 2014/15 and with similar levels of trade payables of around 30 days. The external auditors expressed an unqualified (‘clean’) opinion on the 2013/14 accounts and it is expected they will similarly propose to express a clean opinion on the 2014/15 accounts. As required by the BoD, the Audit and Assurance Committee (AAC) have reviewed the draft 2014/15 accounts and confirmed they are consistent with the financial statements submitted to the Board throughout the reporting year.
Page 1 of 6
The Hillingdon Hospitals NHS Foundation Trust (‘THH’) Going Concern 2014/15 The BoD reviewed the final audited accounts on 27 May 2015 following presentation of the external audit report at the AAC on 26 May 2015. Assurance Framework 3.3 The Trust’s Assurance Framework is reviewed by the BoD bi-annually, and quarterly by the AAC and Quality and Risk Committee (‘QRC’) following appropriate review and update by senior executive management having regard to the risk registers maintained around the Trust. The Assurance Framework identified key risks and threats to achievement of the Trust’s key objectives and showed how the Trust was controlling these or planning taking action to do so. Annual Operating Plan and Strategic Plan 3.4 The Trust’s Operational Plan 2014/15 to 2015/16 outlines the Trust’s past performance; future business plans and risk analysis thereof. The Strategic Plan 2014 to 2019 is aims to describe the Trust’s future intentions over the coming years. Both documents are approved at BoD level. Financial Plan (appendix A) 3.5 The Trust has produced and approved at BoD level a detailed Financial Plan forecasting the following on a month by month basis for the period 1 April 2015 to 31 March 2016 containing;
- Income and expenditure; - Statement of Financial Position; - Cash flow; - Capital investment plan; - Continuity of Service (‘CoSRR’) risk ratings.
3.6 The Financial Plan shows: a) Agreed contracts with healthcare commissioners; b) Operating income based on contracts and activity plans materially
aligned with the Trust’s lead and other main commissioners but that fall short of the amount of income the Trust requires to meet its operational costs;
c) A ‘technical’ planned break-even for the year due to SaHF implementation funding but a cash pressure of £4.4m;
d) In-quarter deficits that can be financed however, from available working capital headroom so positive cash and bank balances each month (appendix B);
e) A requirement to achieve a total of £9.5m of savings; f) Specific revenue of £2m and capital investment of £3.4m to enable the
Trust to meet Care Quality Commission regulations and statutory estate compliance standards;
g) 14/15 outturn operating costs plus an additional £2m to reflect an increase in quarter 4 expenditure has been used as the starting basis for financial plans and means the significant bed capacity increase and extremely high agency pay costs have been incorporated;
h) As the Trust reached the physical limit of its bed capacity in 14/15 it is not expected this level of increase can be continued in 15/16 and as the main driver for agency staff use the rate this can increase further is also expected to reduce
i) Positive monthly cash balances in 15/16 and 16/17 staying above £3m with upfront payments in April 2015 (£4.1m) and April 2016 (£3m).
Page 2 of 6
The Hillingdon Hospitals NHS Foundation Trust (‘THH’) Going Concern 2014/15 3.7 Financial Plan Uncertainty and Sensitivities (appendix C) The Board are aware the 2015/6 financial plan is subject to a number of key financial uncertainties that will need to be successfully managed. These are as follows;
- The amount of savings that can be achieved; - Commissioners funding contract over performance and if required
further in-year support as was the case in 13/14 and 14/15; - Emergency resilience funding matching the 14/15 level; - Funding for the SaHF Programme Team.
These and a number of further identified risks most notably in relation to staff recruitment and its resultant impact on agency staff; contract performance penalties; CQUIN delivery and CQC compliance have been appraised in a ‘reasonable’ downside scenario quantified as a £3.90m financial risk and ‘worst case’ scenario quantified as a £6.30m financial risk. Based on current known financial contingencies and reasonable mitigating actions, £3.85m of combined measures should be available to offset the ‘reasonable’ downside scenario maintaining the Trust’s CoSRR at 2. In the ‘worst case’ scenario only £2.45m of measures could be relied upon resulting in residual adverse financial risks of £3.80m. This would result in the Trust’s CoSRR reducing to a 1 but working capital could still be reasonably stretched further to create the headroom to cover the full cash impact of this scenario. This is based on there being £3m of cash headroom identified in the Trust’s 24-month cash flow forecast and a further £2m working capital stretch possible. 3.8 Risk Rating The Trust is required, in line with all other NHS providers, to report to Monitor its CoSRR quarterly. CoSRR is based on two key financial operational metrics; the ability to service debt requirements, or “capital servicing capacity”; and “liquidity days”; the number of days for which the Trust’s liquid assets could cover its cash obligations excluding any working capital facilities. As at 31st March 2015 the Trust’s CoSRR was 3 (2014 CoSRR Rating was 3) Where a score of 1 means ‘highest risk’ and score 4 ‘lowest risk. The Forecast for 2015/16 is a planned CoSRR of 2 that indicates material financial risk at a level that could trigger an investigation of the circumstances by Monitor. It would not however, be considered by Monitor a significant financial risk that could lead to the appointment of the contingency planning team. These risk ratings support the Trust as a going concern under International Accounting Standard 1. 3.9 The Trust has to date met its day to day operational working capital and investment capital requirements and without ever having to access an overdraft or working capital facility. The Trust agreed a £10m working capital loan, repayable over 10 years at a fixed interest rate of 1.71%, with DH on 17 November 2014. The contractual purpose of the loan was for the Trust to utilise the cash to significantly reduce its level of payables. Loan repayments have been factored into cash projections and financial plans.
Page 3 of 6
The Hillingdon Hospitals NHS Foundation Trust (‘THH’) Going Concern 2014/15 Up to November 2014 the Trust had been operating on a 60 day credit terms policy. The additional funding enabled the Trust to operate on a 30 day policy in line with the Public Sector Payment Policy. This was the position at year-end. However, to manage the consequences of the 2015/16 planned cash deficit in-year payables (trade, other and capital) will be stretched by a total of £4m. Health Economy Context 3.10 Prior to the 2014 Autumn Statement that allocated £2bn of additional funding to the NHS in England, Hillingdon CCG (HCCG), the Trust’s lead and main commissioner was already expecting an increased allocation of 4% against a floor of 1.7%. This was in recognition of their position below their weighted capitation target. However, subsequent to the new resources being allocated their 2015/16 allocation was increased to 7.63%; a total increase of £22.5m and £10.9m above what they had originally planned. 3.11 This significant level of additional resource will allow HCCG to restore its historic deficit financial position to break-even in 15/16; much faster than originally planned. It will also allow it to set lower QIPP targets in relation to acute provider activity going forward and build in financial headroom in the health economy from 2016/17. 3.12 The 2015/16 contract signed with the lead commissioner confirms its intention to purchase a full range of healthcare services from the Trust. Revenue and activity plans are fully aligned with contracts, including the QIPP impact in full, which will significantly reduce the risk of contract dispute and delay in payment during the 15/16 financial year. The Trust has also agreed in principle cash payment terms in 15/16 that will greatly assist with in-year cash flow management. 3.13 The Trust’s contract with HCCG in 15/16 is a ‘guaranteed minimum’ sum with a 45% marginal rate built in for any over performance. It also makes recurrent £1.6m of emergency resilience funding. Above this however, further revenue can be agreed as was the case in 14/15 where a significant additional payment was agreed to reimburse the Trust for the premium cost of it opening substantial additional unplanned emergency bed capacity. 3.14 The Trust has successfully managed its healthcare contracts with all its main commissioners during 2014/15 with only non-material disputed contractual items outstanding at the year-end. These have been provided for. 3.15 The Trust has also agreed with HCCG that £5.3m of funding relating to Shaping a Healthier Future implementation and transition will be paid as a lump sum in April/ May 2015. In addition, elements outside the main contract guaranteed minimum such as CQUINs, excluded drugs and additional services will be paid monthly in 2015/16. Both of these developments will help the Trust manage in-year cash flow. Financial Report 3.16 The Financial Report for April 2015 produced by the Finance Director was reviewed by the BoD on 29 April 2015. The report notes that a revenue deficit of £2.5m was achieved for the financial year ending 31 March 2015. This is a greater deficit than the revised forecast position reported to the
Page 4 of 6
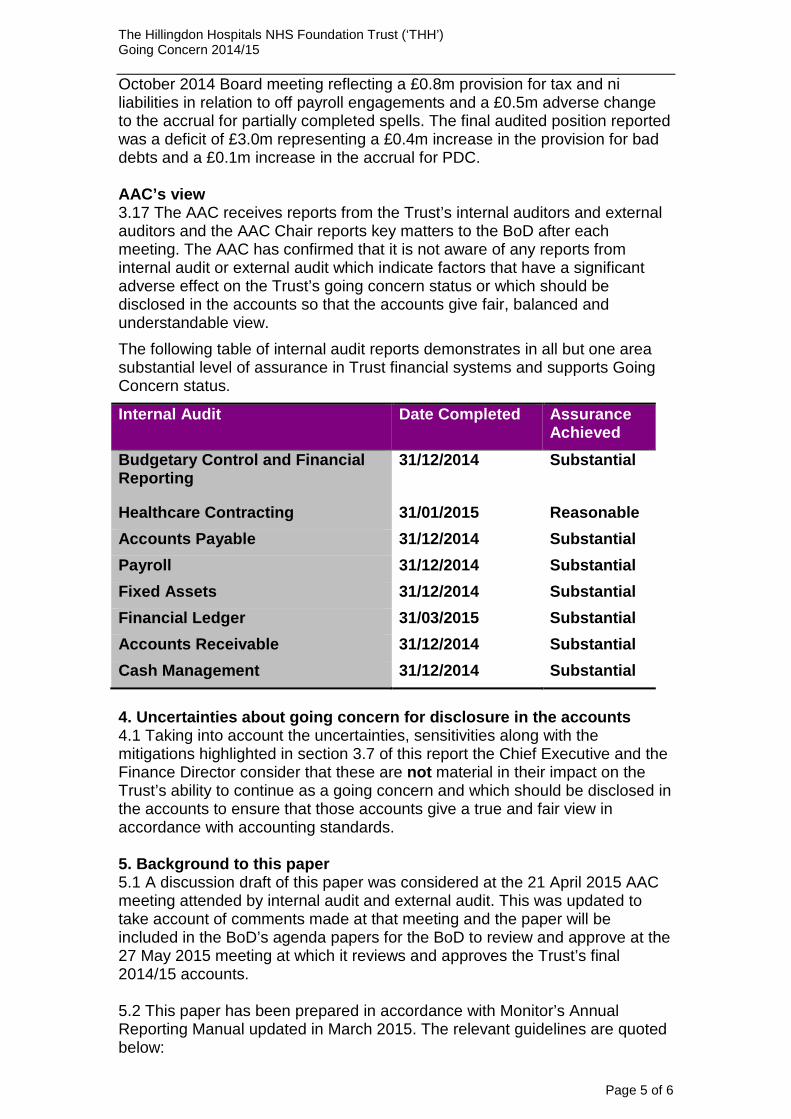
The Hillingdon Hospitals NHS Foundation Trust (‘THH’) Going Concern 2014/15 October 2014 Board meeting reflecting a £0.8m provision for tax and ni liabilities in relation to off payroll engagements and a £0.5m adverse change to the accrual for partially completed spells. The final audited position reported was a deficit of £3.0m representing a £0.4m increase in the provision for bad debts and a £0.1m increase in the accrual for PDC. AAC’s view 3.17 The AAC receives reports from the Trust’s internal auditors and external auditors and the AAC Chair reports key matters to the BoD after each meeting. The AAC has confirmed that it is not aware of any reports from internal audit or external audit which indicate factors that have a significant adverse effect on the Trust’s going concern status or which should be disclosed in the accounts so that the accounts give fair, balanced and understandable view. The following table of internal audit reports demonstrates in all but one area substantial level of assurance in Trust financial systems and supports Going Concern status.
Internal Audit Date Completed Assurance Achieved
Budgetary Control and Financial Reporting
31/12/2014
Substantial
Healthcare Contracting 31/01/2015 Reasonable Accounts Payable 31/12/2014 Substantial Payroll 31/12/2014 Substantial Fixed Assets 31/12/2014 Substantial Financial Ledger 31/03/2015 Substantial Accounts Receivable 31/12/2014 Substantial Cash Management 31/12/2014 Substantial
4. Uncertainties about going concern for disclosure in the accounts 4.1 Taking into account the uncertainties, sensitivities along with the mitigations highlighted in section 3.7 of this report the Chief Executive and the Finance Director consider that these are not material in their impact on the Trust’s ability to continue as a going concern and which should be disclosed in the accounts to ensure that those accounts give a true and fair view in accordance with accounting standards. 5. Background to this paper 5.1 A discussion draft of this paper was considered at the 21 April 2015 AAC meeting attended by internal audit and external audit. This was updated to take account of comments made at that meeting and the paper will be included in the BoD’s agenda papers for the BoD to review and approve at the 27 May 2015 meeting at which it reviews and approves the Trust’s final 2014/15 accounts. 5.2 This paper has been prepared in accordance with Monitor’s Annual Reporting Manual updated in March 2015. The relevant guidelines are quoted below:
Page 5 of 6
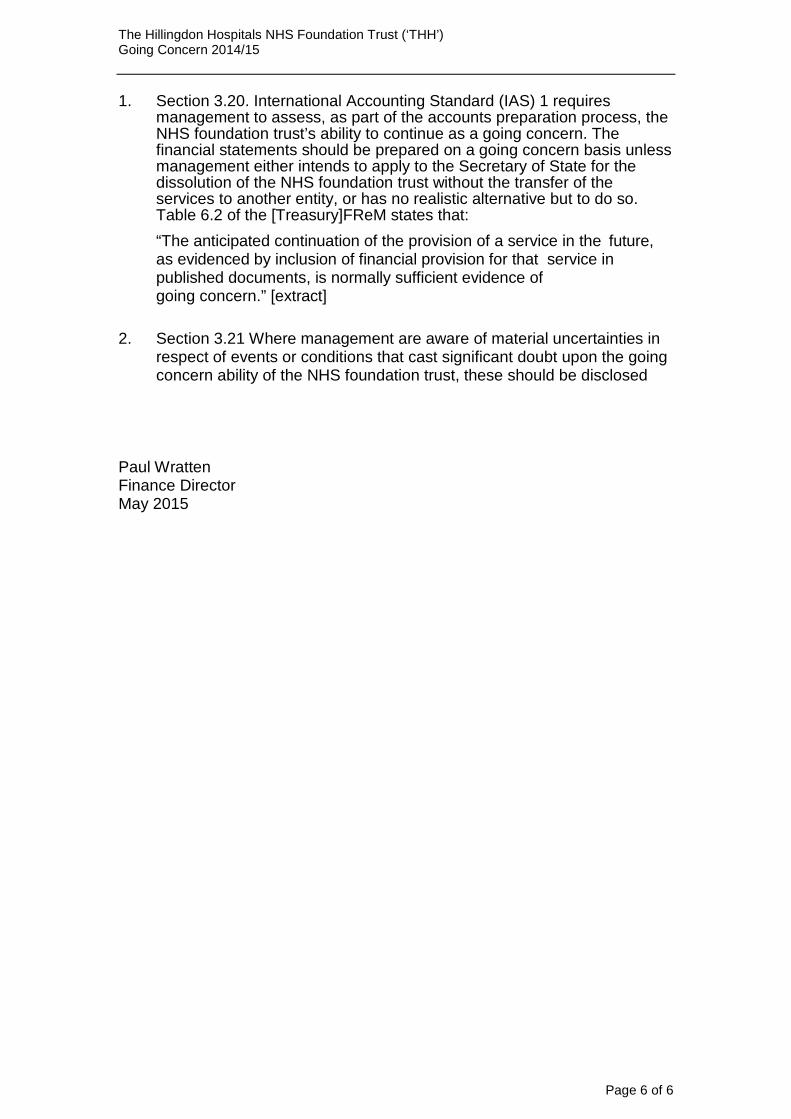
The Hillingdon Hospitals NHS Foundation Trust (‘THH’) Going Concern 2014/15 1. Section 3.20. International Accounting Standard (IAS) 1 requires
management to assess, as part of the accounts preparation process, the NHS foundation trust’s ability to continue as a going concern. The financial statements should be prepared on a going concern basis unless management either intends to apply to the Secretary of State for the dissolution of the NHS foundation trust without the transfer of the services to another entity, or has no realistic alternative but to do so. Table 6.2 of the [Treasury]FReM states that: “The anticipated continuation of the provision of a service in the future, as evidenced by inclusion of financial provision for that service in published documents, is normally sufficient evidence of going concern.” [extract]
2. Section 3.21 Where management are aware of material uncertainties in
respect of events or conditions that cast significant doubt upon the going concern ability of the NHS foundation trust, these should be disclosed
Paul Wratten Finance Director May 2015
Page 6 of 6
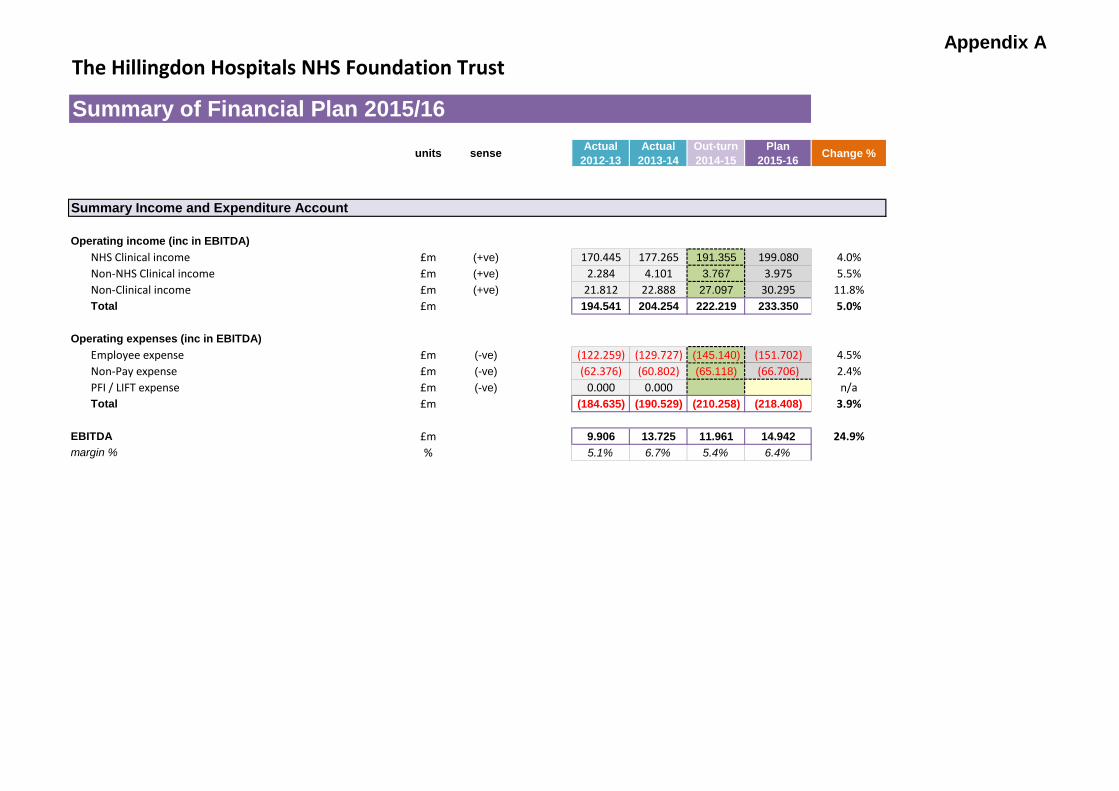
Appendix AThe Hillingdon Hospitals NHS Foundation Trust
units sense Actual 2012-13
Actual 2013-14
Out-turn 2014-15
Plan 2015-16 Change %
Operating income (inc in EBITDA)NHS Clinical income £m (+ve) 170.445 177.265 191.355 199.080 4.0%Non-NHS Clinical income £m (+ve) 2.284 4.101 3.767 3.975 5.5%Non-Clinical income £m (+ve) 21.812 22.888 27.097 30.295 11.8%Total £m 194.541 204.254 222.219 233.350 5.0%
Operating expenses (inc in EBITDA)Employee expense £m (-ve) (122.259) (129.727) (145.140) (151.702) 4.5%Non-Pay expense £m (-ve) (62.376) (60.802) (65.118) (66.706) 2.4%PFI / LIFT expense £m (-ve) 0.000 0.000 n/aTotal £m (184.635) (190.529) (210.258) (218.408) 3.9%
EBITDA £m 9.906 13.725 11.961 14.942 24.9%margin % % 5.1% 6.7% 5.4% 6.4%
Summary of Financial Plan 2015/16
Summary Income and Expenditure Account
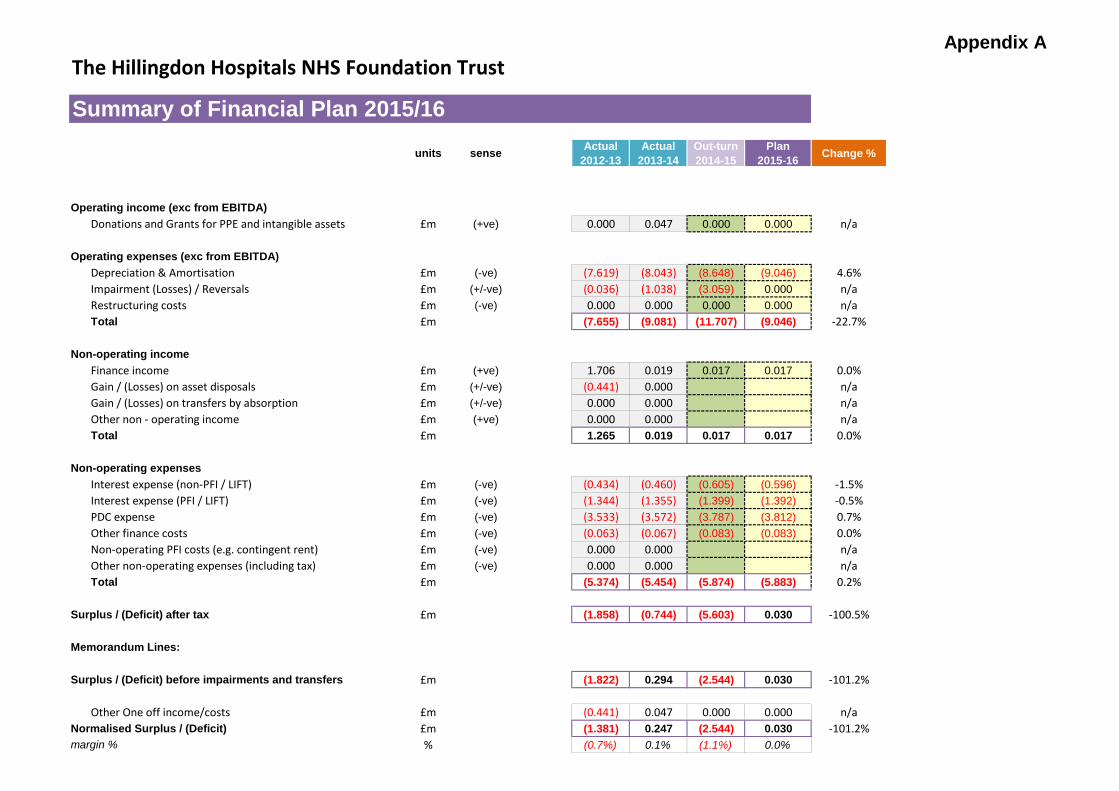
Appendix AThe Hillingdon Hospitals NHS Foundation Trust
units sense Actual 2012-13
Actual 2013-14
Out-turn 2014-15
Plan 2015-16 Change %
Summary of Financial Plan 2015/16
Operating income (exc from EBITDA)Donations and Grants for PPE and intangible assets £m (+ve) 0.000 0.047 0.000 0.000 n/a
Operating expenses (exc from EBITDA)Depreciation & Amortisation £m (-ve) (7.619) (8.043) (8.648) (9.046) 4.6%Impairment (Losses) / Reversals £m (+/-ve) (0.036) (1.038) (3.059) 0.000 n/aRestructuring costs £m (-ve) 0.000 0.000 0.000 0.000 n/aTotal £m (7.655) (9.081) (11.707) (9.046) -22.7%
Non-operating incomeFinance income £m (+ve) 1.706 0.019 0.017 0.017 0.0%Gain / (Losses) on asset disposals £m (+/-ve) (0.441) 0.000 n/aGain / (Losses) on transfers by absorption £m (+/-ve) 0.000 0.000 n/aOther non - operating income £m (+ve) 0.000 0.000 n/aTotal £m 1.265 0.019 0.017 0.017 0.0%
Non-operating expensesInterest expense (non-PFI / LIFT) £m (-ve) (0.434) (0.460) (0.605) (0.596) -1.5%Interest expense (PFI / LIFT) £m (-ve) (1.344) (1.355) (1.399) (1.392) -0.5%PDC expense £m (-ve) (3.533) (3.572) (3.787) (3.812) 0.7%Other finance costs £m (-ve) (0.063) (0.067) (0.083) (0.083) 0.0%Non-operating PFI costs (e.g. contingent rent) £m (-ve) 0.000 0.000 n/aOther non-operating expenses (including tax) £m (-ve) 0.000 0.000 n/aTotal £m (5.374) (5.454) (5.874) (5.883) 0.2%
Surplus / (Deficit) after tax £m (1.858) (0.744) (5.603) 0.030 -100.5%
Memorandum Lines:
Surplus / (Deficit) before impairments and transfers £m (1.822) 0.294 (2.544) 0.030 -101.2%
Other One off income/costs £m (0.441) 0.047 0.000 0.000 n/aNormalised Surplus / (Deficit) £m (1.381) 0.247 (2.544) 0.030 -101.2%margin % % (0.7%) 0.1% (1.1%) 0.0%
Appendix AThe Hillingdon Hospitals NHS Foundation Trust
units sense Actual 2012-13
Actual 2013-14
Out-turn 2014-15
Plan 2015-16 Change %
Summary of Financial Plan 2015/16
Summary Statement of Financial PositionDownside
Non-current Assets StretchIntangible assets £m (+ve) 1.948 2.141 2.980 2.980 0.0% 2.980Property, Plant & Equipment £m (+ve) 104.129 108.979 120.695 123.094 2.0% 123.094On-balance sheet PFI £m (+ve) 10.783 15.658 16.013 15.718 -1.8% 15.718Other £m (+ve) 16.289 16.251 20.578 20.578 0.0% 20.578Total £m 133.149 143.029 160.266 162.370 1.3% 162.370
Current AssetsCash and cash equivalents £m (+ve) 3.906 5.733 5.415 3.461 -36.1% 0.461Other current assets £m (+ve) 16.705 17.305 19.551 17.551 -10.2% 16.551Total £m 20.611 23.038 24.966 21.012 -15.8% 17.012
Current LiabilitiesPFI / LIFT leases £m (-ve) (0.236) (0.181) (0.328) (0.328) 0.0% (0.328)Other borrowings £m (-ve) (1.232) (1.499) (2.911) (3.102) 6.6% (3.102)Other current liabilities £m (-ve) (20.950) (20.730) (22.884) (22.767) -0.5% (23.767)Total £m (22.418) (22.410) (26.123) (26.197) 0.3% (27.197)
Non-current LiabilitiesPFI / LIFT leases £m (-ve) (12.900) (12.718) (12.390) (11.826) -4.6% (11.826)Other borrowings £m (-ve) (8.931) (10.641) (19.414) (18.024) -7.2% (18.024)Other non-current liabilities £m (-ve) (1.949) (2.272) (2.704) (2.704) 0.0% (2.704)Total £m (23.780) (25.631) (34.508) (32.554) -5.7% (32.554)
Reserves £m (+ve) 107.562 118.026 124.601 124.631 0.0% 119.6315.000
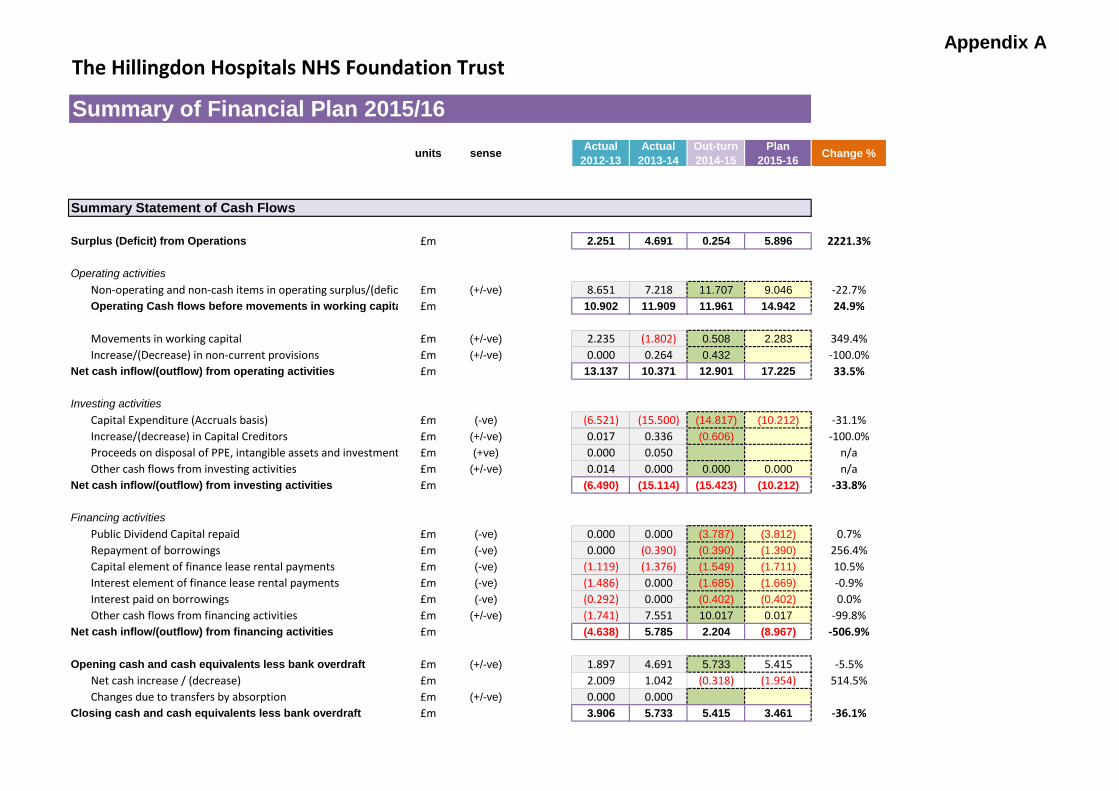
Appendix AThe Hillingdon Hospitals NHS Foundation Trust
units sense Actual 2012-13
Actual 2013-14
Out-turn 2014-15
Plan 2015-16 Change %
Summary of Financial Plan 2015/16
Summary Statement of Cash Flows
Surplus (Deficit) from Operations £m 2.251 4.691 0.254 5.896 2221.3%
Operating activitiesNon-operating and non-cash items in operating surplus/(defic £m (+/-ve) 8.651 7.218 11.707 9.046 -22.7%Operating Cash flows before movements in working capita £m 10.902 11.909 11.961 14.942 24.9%
Movements in working capital £m (+/-ve) 2.235 (1.802) 0.508 2.283 349.4%Increase/(Decrease) in non-current provisions £m (+/-ve) 0.000 0.264 0.432 -100.0%
Net cash inflow/(outflow) from operating activities £m 13.137 10.371 12.901 17.225 33.5%
Investing activitiesCapital Expenditure (Accruals basis) £m (-ve) (6.521) (15.500) (14.817) (10.212) -31.1%Increase/(decrease) in Capital Creditors £m (+/-ve) 0.017 0.336 (0.606) -100.0%Proceeds on disposal of PPE, intangible assets and investment £m (+ve) 0.000 0.050 n/aOther cash flows from investing activities £m (+/-ve) 0.014 0.000 0.000 0.000 n/a
Net cash inflow/(outflow) from investing activities £m (6.490) (15.114) (15.423) (10.212) -33.8%
Financing activitiesPublic Dividend Capital repaid £m (-ve) 0.000 0.000 (3.787) (3.812) 0.7%Repayment of borrowings £m (-ve) 0.000 (0.390) (0.390) (1.390) 256.4%Capital element of finance lease rental payments £m (-ve) (1.119) (1.376) (1.549) (1.711) 10.5%Interest element of finance lease rental payments £m (-ve) (1.486) 0.000 (1.685) (1.669) -0.9%Interest paid on borrowings £m (-ve) (0.292) 0.000 (0.402) (0.402) 0.0%Other cash flows from financing activities £m (+/-ve) (1.741) 7.551 10.017 0.017 -99.8%
Net cash inflow/(outflow) from financing activities £m (4.638) 5.785 2.204 (8.967) -506.9%
Opening cash and cash equivalents less bank overdraft £m (+/-ve) 1.897 4.691 5.733 5.415 -5.5%Net cash increase / (decrease) £m 2.009 1.042 (0.318) (1.954) 514.5%Changes due to transfers by absorption £m (+/-ve) 0.000 0.000
Closing cash and cash equivalents less bank overdraft £m 3.906 5.733 5.415 3.461 -36.1%
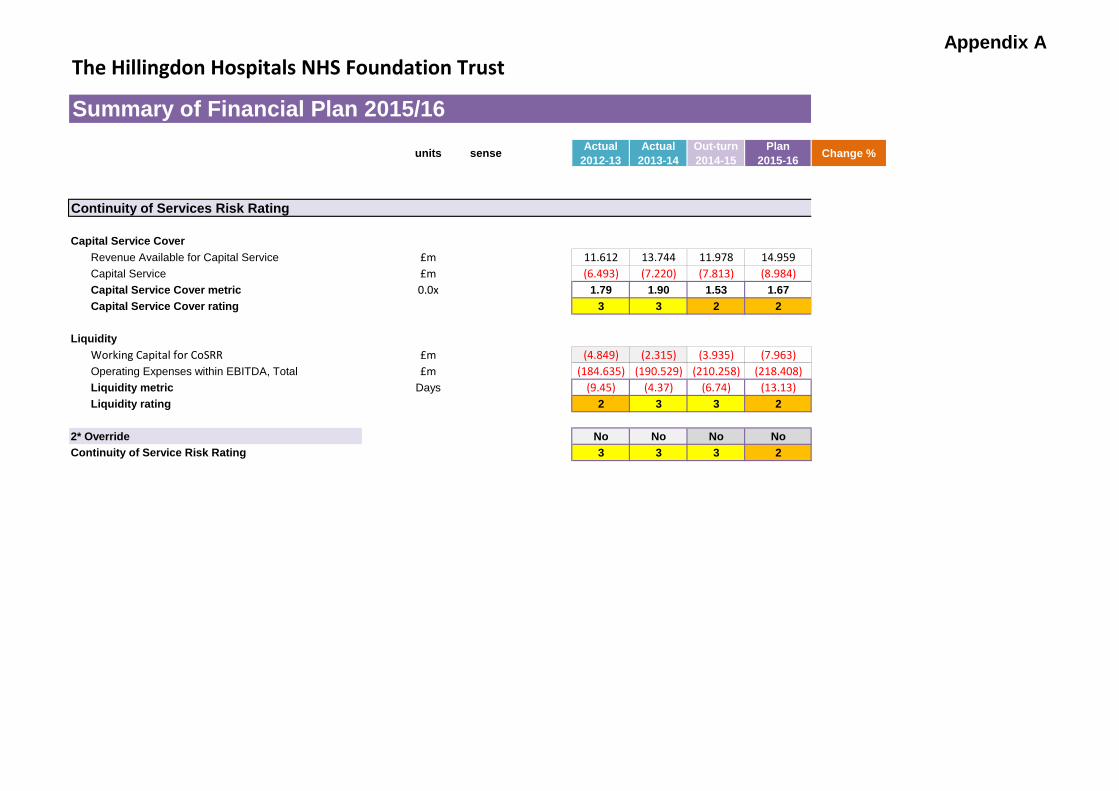
Appendix AThe Hillingdon Hospitals NHS Foundation Trust
units sense Actual 2012-13
Actual 2013-14
Out-turn 2014-15
Plan 2015-16 Change %
Summary of Financial Plan 2015/16
Continuity of Services Risk Rating
Capital Service CoverRevenue Available for Capital Service £m 11.612 13.744 11.978 14.959Capital Service £m (6.493) (7.220) (7.813) (8.984)Capital Service Cover metric 0.0x 1.79 1.90 1.53 1.67Capital Service Cover rating 3 3 2 2
LiquidityWorking Capital for CoSRR £m (4.849) (2.315) (3.935) (7.963)Operating Expenses within EBITDA, Total £m (184.635) (190.529) (210.258) (218.408)Liquidity metric Days (9.45) (4.37) (6.74) (13.13)Liquidity rating 2 3 3 2
2* Override No No No NoContinuity of Service Risk Rating 3 3 3 2
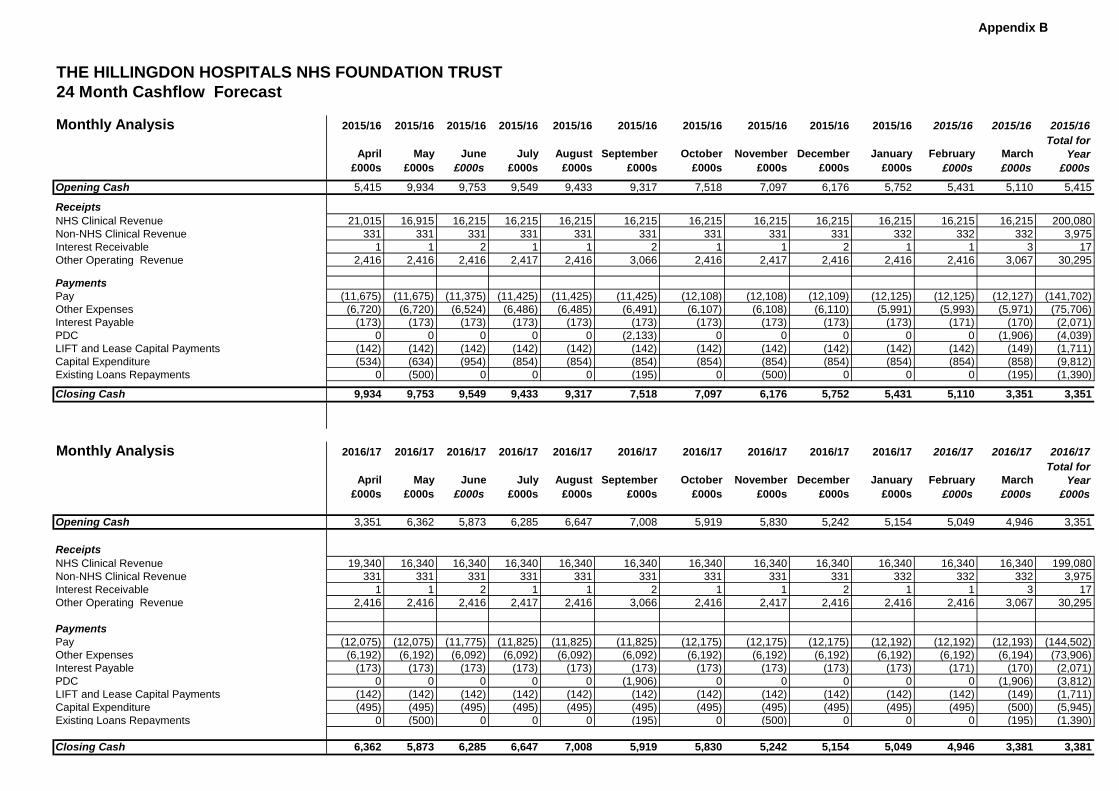
Appendix B
THE HILLINGDON HOSPITALS NHS FOUNDATION TRUST24 Month Cashflow Forecast
Monthly Analysis 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16 2015/16
April May June July August September October November December January February MarchTotal for
Year£000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s
Opening Cash 5,415 9,934 9,753 9,549 9,433 9,317 7,518 7,097 6,176 5,752 5,431 5,110 5,415
ReceiptsNHS Clinical Revenue 21,015 16,915 16,215 16,215 16,215 16,215 16,215 16,215 16,215 16,215 16,215 16,215 200,080Non-NHS Clinical Revenue 331 331 331 331 331 331 331 331 331 332 332 332 3,975Interest Receivable 1 1 2 1 1 2 1 1 2 1 1 3 17Other Operating Revenue 2,416 2,416 2,416 2,417 2,416 3,066 2,416 2,417 2,416 2,416 2,416 3,067 30,295
PaymentsPay (11,675) (11,675) (11,375) (11,425) (11,425) (11,425) (12,108) (12,108) (12,109) (12,125) (12,125) (12,127) (141,702)Other Expenses (6,720) (6,720) (6,524) (6,486) (6,485) (6,491) (6,107) (6,108) (6,110) (5,991) (5,993) (5,971) (75,706)Interest Payable (173) (173) (173) (173) (173) (173) (173) (173) (173) (173) (171) (170) (2,071)PDC 0 0 0 0 0 (2,133) 0 0 0 0 0 (1,906) (4,039)LIFT and Lease Capital Payments (142) (142) (142) (142) (142) (142) (142) (142) (142) (142) (142) (149) (1,711)Capital Expenditure (534) (634) (954) (854) (854) (854) (854) (854) (854) (854) (854) (858) (9,812)Existing Loans Repayments 0 (500) 0 0 0 (195) 0 (500) 0 0 0 (195) (1,390)
Closing Cash 9,934 9,753 9,549 9,433 9,317 7,518 7,097 6,176 5,752 5,431 5,110 3,351 3,351
Monthly Analysis 2016/17 2016/17 2016/17 2016/17 2016/17 2016/17 2016/17 2016/17 2016/17 2016/17 2016/17 2016/17 2016/17
April May June July August September October November December January February MarchTotal for
Year£000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s £000s
Opening Cash 3,351 6,362 5,873 6,285 6,647 7,008 5,919 5,830 5,242 5,154 5,049 4,946 3,351
ReceiptsNHS Clinical Revenue 19,340 16,340 16,340 16,340 16,340 16,340 16,340 16,340 16,340 16,340 16,340 16,340 199,080Non-NHS Clinical Revenue 331 331 331 331 331 331 331 331 331 332 332 332 3,975Interest Receivable 1 1 2 1 1 2 1 1 2 1 1 3 17Other Operating Revenue 2,416 2,416 2,416 2,417 2,416 3,066 2,416 2,417 2,416 2,416 2,416 3,067 30,295
PaymentsPay (12,075) (12,075) (11,775) (11,825) (11,825) (11,825) (12,175) (12,175) (12,175) (12,192) (12,192) (12,193) (144,502)Other Expenses (6,192) (6,192) (6,092) (6,092) (6,092) (6,092) (6,192) (6,192) (6,192) (6,192) (6,192) (6,194) (73,906)Interest Payable (173) (173) (173) (173) (173) (173) (173) (173) (173) (173) (171) (170) (2,071)PDC 0 0 0 0 0 (1,906) 0 0 0 0 0 (1,906) (3,812)LIFT and Lease Capital Payments (142) (142) (142) (142) (142) (142) (142) (142) (142) (142) (142) (149) (1,711)Capital Expenditure (495) (495) (495) (495) (495) (495) (495) (495) (495) (495) (495) (500) (5,945)Existing Loans Repayments 0 (500) 0 0 0 (195) 0 (500) 0 0 0 (195) (1,390)
Closing Cash 6,362 5,873 6,285 6,647 7,008 5,919 5,830 5,242 5,154 5,049 4,946 3,381 3,381
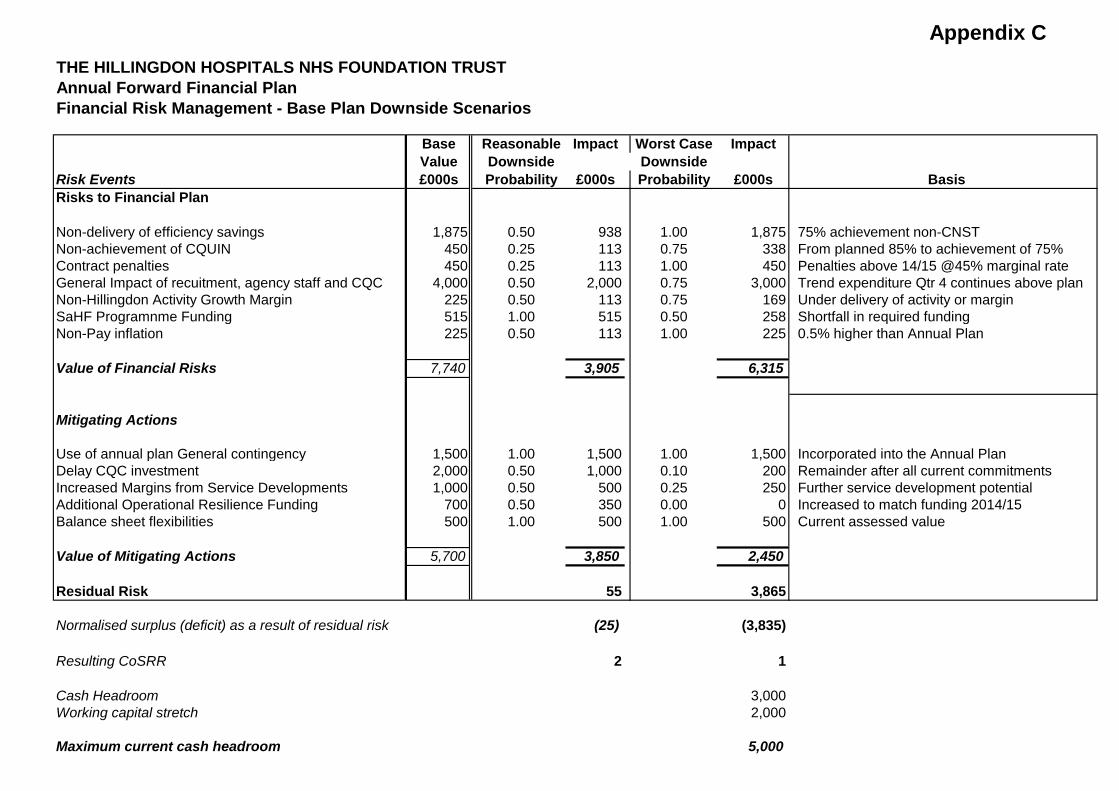
Appendix CTHE HILLINGDON HOSPITALS NHS FOUNDATION TRUSTAnnual Forward Financial PlanFinancial Risk Management - Base Plan Downside Scenarios
Base Reasonable Impact Worst Case ImpactValue Downside Downside
Risk Events £000s Probability £000s Probability £000s BasisRisks to Financial Plan
Non-delivery of efficiency savings 1,875 0.50 938 1.00 1,875 75% achievement non-CNSTNon-achievement of CQUIN 450 0.25 113 0.75 338 From planned 85% to achievement of 75%Contract penalties 450 0.25 113 1.00 450 Penalties above 14/15 @45% marginal rateGeneral Impact of recuitment, agency staff and CQC 4,000 0.50 2,000 0.75 3,000 Trend expenditure Qtr 4 continues above planNon-Hillingdon Activity Growth Margin 225 0.50 113 0.75 169 Under delivery of activity or marginSaHF Programnme Funding 515 1.00 515 0.50 258 Shortfall in required fundingNon-Pay inflation 225 0.50 113 1.00 225 0.5% higher than Annual Plan
Value of Financial Risks 7,740 3,905 6,315
Mitigating Actions
Use of annual plan General contingency 1,500 1.00 1,500 1.00 1,500 Incorporated into the Annual PlanDelay CQC investment 2,000 0.50 1,000 0.10 200 Remainder after all current commitmentsIncreased Margins from Service Developments 1,000 0.50 500 0.25 250 Further service development potentialAdditional Operational Resilience Funding 700 0.50 350 0.00 0 Increased to match funding 2014/15Balance sheet flexibilities 500 1.00 500 1.00 500 Current assessed value
Value of Mitigating Actions 5,700 3,850 2,450
Residual Risk 55 3,865
Normalised surplus (deficit) as a result of residual risk (25) (3,835)
Resulting CoSRR 2 1
Cash Headroom 3,000Working capital stretch 2,000
Maximum current cash headroom 5,000
Meeting of the Board of Directors – public session Wednesday 27th May 2015
Agenda item 22 Annual Monitor Board Statements
Reason for item: The Annual Monitor Board Statements relating to the financial year 2014/15 are presented to the Board for approval and sign off in preparation for submission to Monitor. Summary: The Monitor Risk Assessment Framework (RAF) (March 2015) requires the Trust to submit: • Annual Corporate Governance Statements (appendices 1 and 3) • Annual declarations required by General condition 6 (appendices 2 and 4) • Other Certifications (training of Governors) (appendix 3) • Continuity of services (CoS) condition 7 - Availability of Resources (appendix 5) The Corporate Governance Statements have been reviewed in-year by the Audit and Assurance Committee (AAC) in October 2014 and April 2015. The Executive Team formally considered both declaration returns on 18th March 2015 and recommend that the Board statements can be signed as specified in this paper. The Trust Secretary has provided information to recommend that the training of Governors can be confirmed. The CoS condition 7 was reviewed in-year by the Executive team and AAC (October 2014) and more recently by the Finance Director. Board Action required: The Board is asked to: 1. Approve the annual Corporate Governance Statements return (appendix 1 and 3). 2. Approve the declarations required by General condition 6 and Continuity of services
(CoS) condition 7 of the NHS provider licence (appendices 2 and 4). Report from: Helen Cobb, Assistant Director Governance & Quality Standards Report sponsor: Theresa Murphy, Director of the Patient Experience & Nursing Links to Trust strategic priorities: The Annual Monitor Board Statements impacts across all Trust strategic priorities Previous consideration at Board or Committees: AAC, April 2015 Equality and diversity considerations: None Financial implications: No direct implications
1
Annual Monitor Board Statements Annual Corporate Governance Statements & General Condition 6 These statements were reviewed in-year by the Audit & Assurance Committee (AAC) and recently by the Executive Team to see if there are any current risks to the delivery of the statements and if so what the mitigating actions have been. The risks and mitigating actions will be submitted to Monitor. The tables in appendices 1 and 2 have been amended following comments made at the October AAC and also to take account of wording changes to the statements by Monitor in its revised Risk Assessment Framework (RAF), March 2015. After further consideration following April AAC some amendments have been made and these are shown in the table as strike through or additions highlighted in yellow. For information appendices 3 and 4 are the Monitor spreadsheets populated with the information from appendices 1 and 2. Following this review two statements are ‘not confirmed’. Other Certifications - training of Governors The Trust has undertaken a range of initiatives to support Governors develop their effectiveness in their role. Induction was provided to Governors on taking office in April 2015, plus briefing sessions were held on a number of key issues affecting the Trust (including on clinical quality, Shaping a Healthier Future, and finance and the Monitor Licence). The Trust commissioned the Foundation Trust Network (now known as NHS Providers) to deliver a development day in June 2014 based on their ‘Governwell’ programme. This led to the identification of a number of actions to develop the Governors’ effectiveness including refocused Governor meeting agendas and reports, and Governor only pre-meets prior to the main Council of Governors meetings which have helped build relationships amongst Governors. Following on from this, NHS Providers will be delivering a session on questioning and challenge in June 2015 to further support Governors in their role. It is therefore recommended that the Board ‘confirm’ this training of Governors statement. Other Certifications - Academic Health Science Centre (AHSC) This certification is not relevant to this Trust Continuity of services (CoS) condition 7 - Availability of Resources This financial statement was reviewed in-year by the Executive team and AAC. The recommendation to the Board is to sign statement 2a on the basis that there is 'reasonable expectation' that the Licensee will have the Required Resources available to it…’ linked to the fact our CoS risk rating plan is 2 and not 1 and the Trust has not requested planned support (appendix 5).
2
The Board will note that:
• For the Board Corporate Governance Statements - where a statement has been proposed as ‘not confirmed’; the Board need to accordingly declare the reasoning.
• For the General condition 6 – Systems for compliance with license conditions an explanatory note is required if a statement is ‘not confirmed’.
• These explanations have been provided in bold in the tables in appendices 1 and 2 against the relevant statements. These explanations will be used to populate the Monitor return (appendices 3 and 4).
• The RAF states that: "Where the corporate governance statement indicates risks to compliance with the governance condition, Monitor will consider whether any actions or other assurance are required at the time of the statement or whether it is more appropriate to maintain a watching brief."
• Other Certifications covers: - where a statement has been proposed as ‘not confirmed’; the Board need to accordingly declare the reasoning.
3
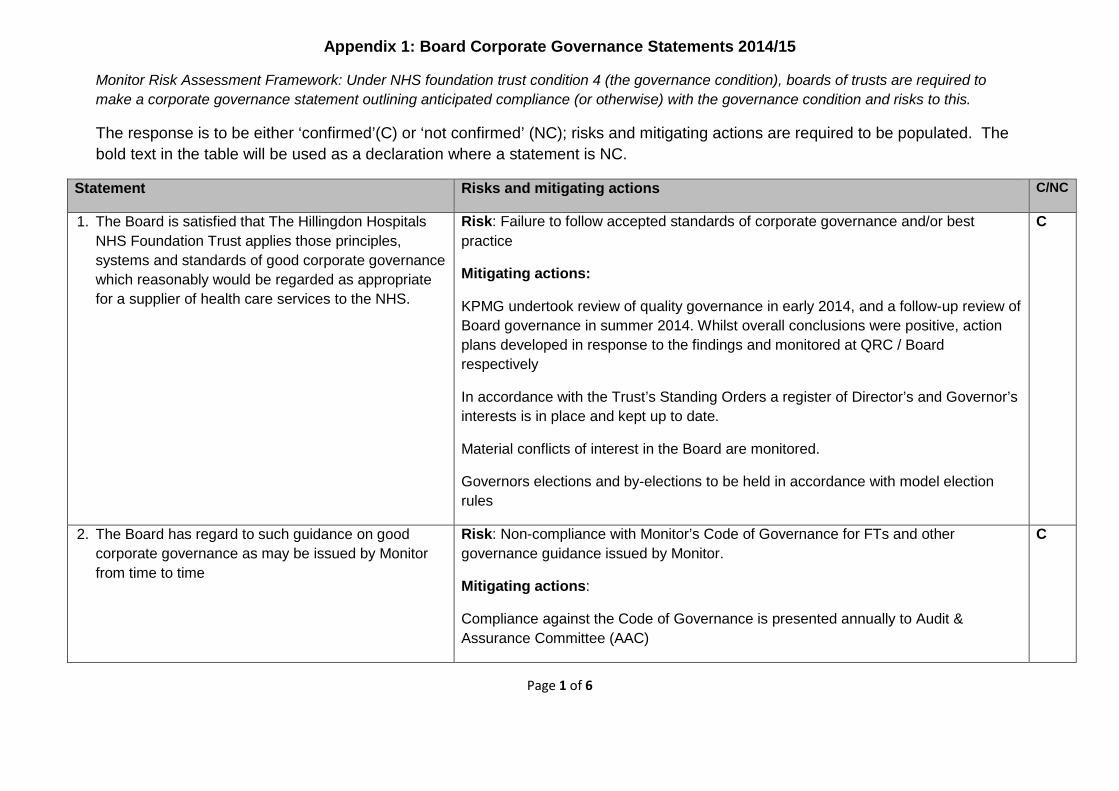
Appendix 1: Board Corporate Governance Statements 2014/15
Monitor Risk Assessment Framework: Under NHS foundation trust condition 4 (the governance condition), boards of trusts are required to make a corporate governance statement outlining anticipated compliance (or otherwise) with the governance condition and risks to this.
The response is to be either ‘confirmed’(C) or ‘not confirmed’ (NC); risks and mitigating actions are required to be populated. The bold text in the table will be used as a declaration where a statement is NC.
Statement Risks and mitigating actions C/NC
1. The Board is satisfied that The Hillingdon Hospitals NHS Foundation Trust applies those principles, systems and standards of good corporate governance which reasonably would be regarded as appropriate for a supplier of health care services to the NHS.
Risk: Failure to follow accepted standards of corporate governance and/or best practice
Mitigating actions:
KPMG undertook review of quality governance in early 2014, and a follow-up review of Board governance in summer 2014. Whilst overall conclusions were positive, action plans developed in response to the findings and monitored at QRC / Board respectively
In accordance with the Trust’s Standing Orders a register of Director’s and Governor’s interests is in place and kept up to date.
Material conflicts of interest in the Board are monitored.
Governors elections and by-elections to be held in accordance with model election rules
C
2. The Board has regard to such guidance on good corporate governance as may be issued by Monitor from time to time
Risk: Non-compliance with Monitor’s Code of Governance for FTs and other governance guidance issued by Monitor.
Mitigating actions:
Compliance against the Code of Governance is presented annually to Audit & Assurance Committee (AAC)
C
Page 1 of 6
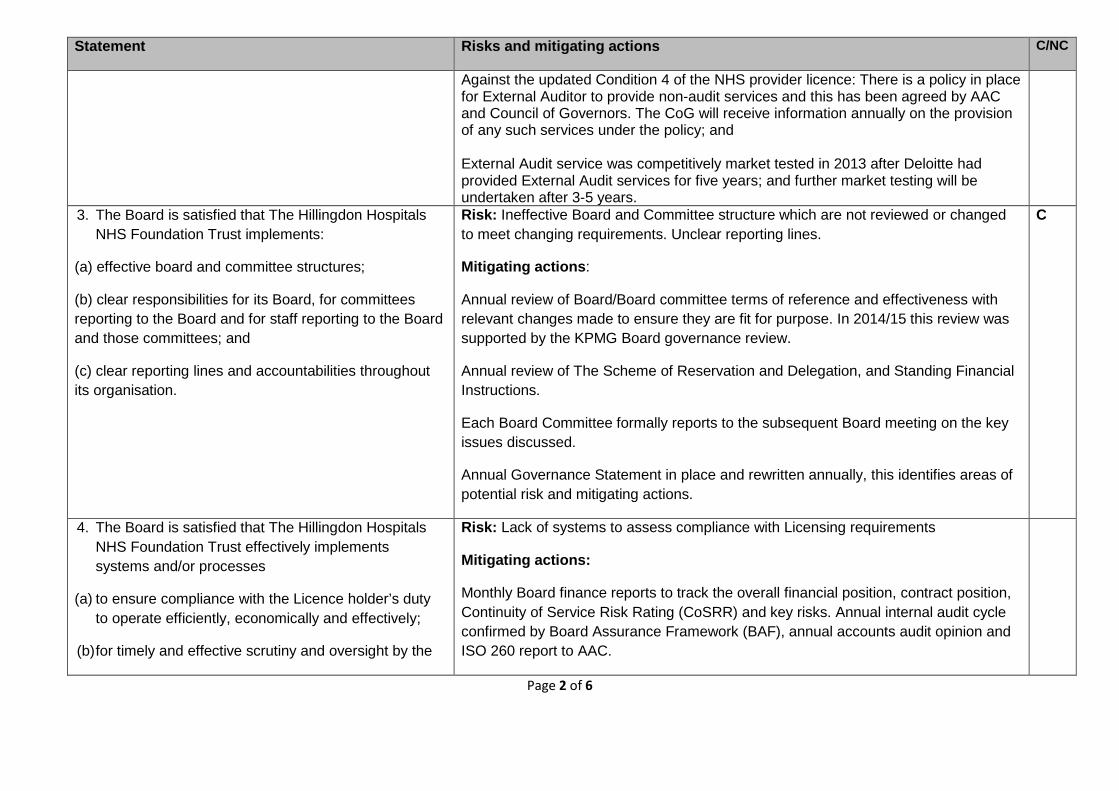
Statement Risks and mitigating actions C/NC
Against the updated Condition 4 of the NHS provider licence: There is a policy in place for External Auditor to provide non-audit services and this has been agreed by AAC and Council of Governors. The CoG will receive information annually on the provision of any such services under the policy; and External Audit service was competitively market tested in 2013 after Deloitte had provided External Audit services for five years; and further market testing will be undertaken after 3-5 years.
3. The Board is satisfied that The Hillingdon Hospitals NHS Foundation Trust implements:
(a) effective board and committee structures;
(b) clear responsibilities for its Board, for committees reporting to the Board and for staff reporting to the Board and those committees; and
(c) clear reporting lines and accountabilities throughout its organisation.
Risk: Ineffective Board and Committee structure which are not reviewed or changed to meet changing requirements. Unclear reporting lines.
Mitigating actions:
Annual review of Board/Board committee terms of reference and effectiveness with relevant changes made to ensure they are fit for purpose. In 2014/15 this review was supported by the KPMG Board governance review.
Annual review of The Scheme of Reservation and Delegation, and Standing Financial Instructions.
Each Board Committee formally reports to the subsequent Board meeting on the key issues discussed.
Annual Governance Statement in place and rewritten annually, this identifies areas of potential risk and mitigating actions.
C
4. The Board is satisfied that The Hillingdon Hospitals NHS Foundation Trust effectively implements systems and/or processes
(a) to ensure compliance with the Licence holder’s duty to operate efficiently, economically and effectively;
(b) for timely and effective scrutiny and oversight by the
Risk: Lack of systems to assess compliance with Licensing requirements
Mitigating actions:
Monthly Board finance reports to track the overall financial position, contract position, Continuity of Service Risk Rating (CoSRR) and key risks. Annual internal audit cycle confirmed by Board Assurance Framework (BAF), annual accounts audit opinion and ISO 260 report to AAC.
Page 2 of 6
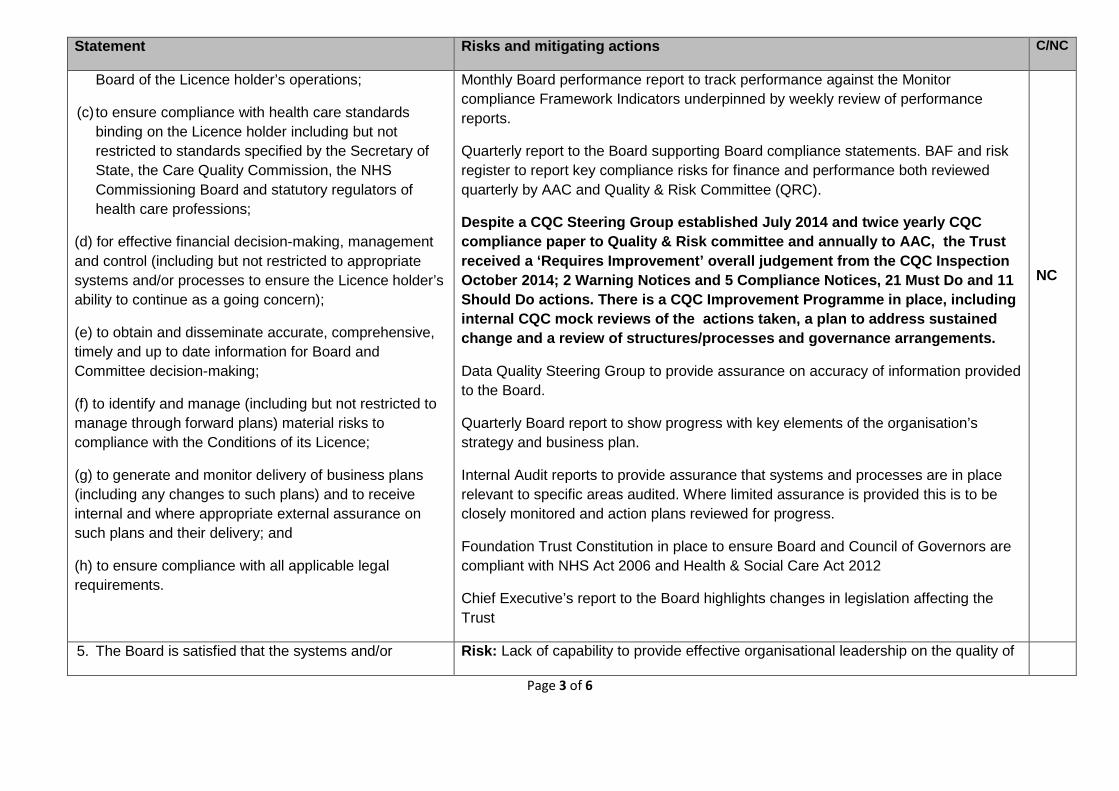
Statement Risks and mitigating actions C/NC
Board of the Licence holder’s operations;
(c) to ensure compliance with health care standards binding on the Licence holder including but not restricted to standards specified by the Secretary of State, the Care Quality Commission, the NHS Commissioning Board and statutory regulators of health care professions;
(d) for effective financial decision-making, management and control (including but not restricted to appropriate systems and/or processes to ensure the Licence holder’s ability to continue as a going concern);
(e) to obtain and disseminate accurate, comprehensive, timely and up to date information for Board and Committee decision-making;
(f) to identify and manage (including but not restricted to manage through forward plans) material risks to compliance with the Conditions of its Licence;
(g) to generate and monitor delivery of business plans (including any changes to such plans) and to receive internal and where appropriate external assurance on such plans and their delivery; and
(h) to ensure compliance with all applicable legal requirements.
Monthly Board performance report to track performance against the Monitor compliance Framework Indicators underpinned by weekly review of performance reports.
Quarterly report to the Board supporting Board compliance statements. BAF and risk register to report key compliance risks for finance and performance both reviewed quarterly by AAC and Quality & Risk Committee (QRC).
Despite a CQC Steering Group established July 2014 and twice yearly CQC compliance paper to Quality & Risk committee and annually to AAC, the Trust received a ‘Requires Improvement’ overall judgement from the CQC Inspection October 2014; 2 Warning Notices and 5 Compliance Notices, 21 Must Do and 11 Should Do actions. There is a CQC Improvement Programme in place, including internal CQC mock reviews of the actions taken, a plan to address sustained change and a review of structures/processes and governance arrangements.
Data Quality Steering Group to provide assurance on accuracy of information provided to the Board.
Quarterly Board report to show progress with key elements of the organisation’s strategy and business plan.
Internal Audit reports to provide assurance that systems and processes are in place relevant to specific areas audited. Where limited assurance is provided this is to be closely monitored and action plans reviewed for progress.
Foundation Trust Constitution in place to ensure Board and Council of Governors are compliant with NHS Act 2006 and Health & Social Care Act 2012
Chief Executive’s report to the Board highlights changes in legislation affecting the Trust
NC
5. The Board is satisfied that the systems and/or Risk: Lack of capability to provide effective organisational leadership on the quality of
Page 3 of 6
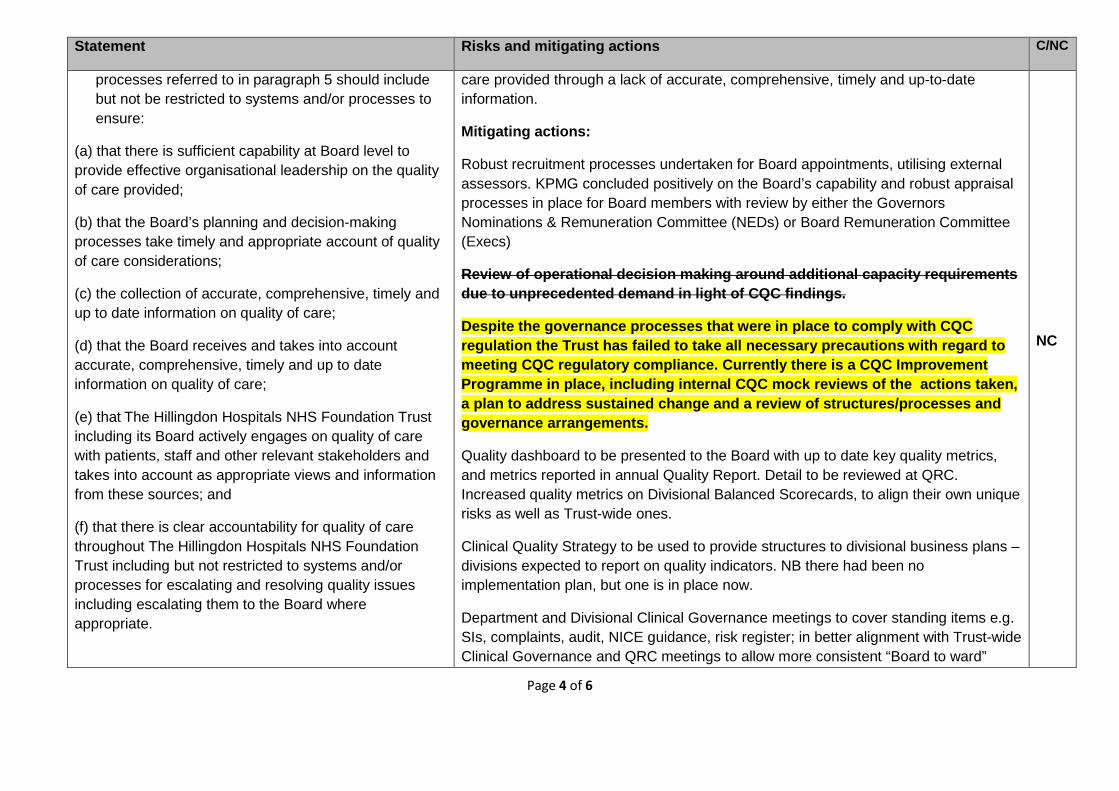
Statement Risks and mitigating actions C/NC
processes referred to in paragraph 5 should include but not be restricted to systems and/or processes to ensure:
(a) that there is sufficient capability at Board level to provide effective organisational leadership on the quality of care provided;
(b) that the Board’s planning and decision-making processes take timely and appropriate account of quality of care considerations;
(c) the collection of accurate, comprehensive, timely and up to date information on quality of care;
(d) that the Board receives and takes into account accurate, comprehensive, timely and up to date information on quality of care;
(e) that The Hillingdon Hospitals NHS Foundation Trust including its Board actively engages on quality of care with patients, staff and other relevant stakeholders and takes into account as appropriate views and information from these sources; and
(f) that there is clear accountability for quality of care throughout The Hillingdon Hospitals NHS Foundation Trust including but not restricted to systems and/or processes for escalating and resolving quality issues including escalating them to the Board where appropriate.
care provided through a lack of accurate, comprehensive, timely and up-to-date information.
Mitigating actions:
Robust recruitment processes undertaken for Board appointments, utilising external assessors. KPMG concluded positively on the Board’s capability and robust appraisal processes in place for Board members with review by either the Governors Nominations & Remuneration Committee (NEDs) or Board Remuneration Committee (Execs)
Review of operational decision making around additional capacity requirements due to unprecedented demand in light of CQC findings.
Despite the governance processes that were in place to comply with CQC regulation the Trust has failed to take all necessary precautions with regard to meeting CQC regulatory compliance. Currently there is a CQC Improvement Programme in place, including internal CQC mock reviews of the actions taken, a plan to address sustained change and a review of structures/processes and governance arrangements.
Quality dashboard to be presented to the Board with up to date key quality metrics, and metrics reported in annual Quality Report. Detail to be reviewed at QRC. Increased quality metrics on Divisional Balanced Scorecards, to align their own unique risks as well as Trust-wide ones.
Clinical Quality Strategy to be used to provide structures to divisional business plans – divisions expected to report on quality indicators. NB there had been no implementation plan, but one is in place now.
Department and Divisional Clinical Governance meetings to cover standing items e.g. SIs, complaints, audit, NICE guidance, risk register; in better alignment with Trust-wide Clinical Governance and QRC meetings to allow more consistent “Board to ward”
NC
Page 4 of 6
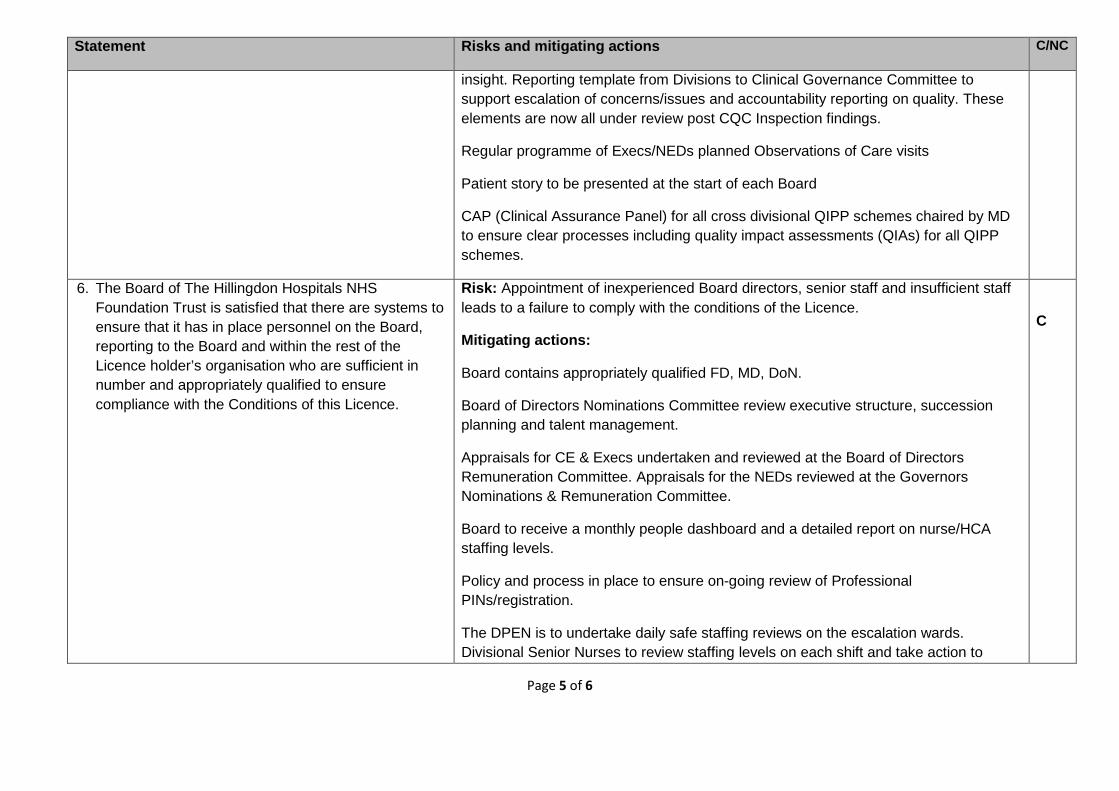
Statement Risks and mitigating actions C/NC
insight. Reporting template from Divisions to Clinical Governance Committee to support escalation of concerns/issues and accountability reporting on quality. These elements are now all under review post CQC Inspection findings.
Regular programme of Execs/NEDs planned Observations of Care visits
Patient story to be presented at the start of each Board
CAP (Clinical Assurance Panel) for all cross divisional QIPP schemes chaired by MD to ensure clear processes including quality impact assessments (QIAs) for all QIPP schemes.
6. The Board of The Hillingdon Hospitals NHS Foundation Trust is satisfied that there are systems to ensure that it has in place personnel on the Board, reporting to the Board and within the rest of the Licence holder’s organisation who are sufficient in number and appropriately qualified to ensure compliance with the Conditions of this Licence.
Risk: Appointment of inexperienced Board directors, senior staff and insufficient staff leads to a failure to comply with the conditions of the Licence.
Mitigating actions:
Board contains appropriately qualified FD, MD, DoN.
Board of Directors Nominations Committee review executive structure, succession planning and talent management.
Appraisals for CE & Execs undertaken and reviewed at the Board of Directors Remuneration Committee. Appraisals for the NEDs reviewed at the Governors Nominations & Remuneration Committee.
Board to receive a monthly people dashboard and a detailed report on nurse/HCA staffing levels.
Policy and process in place to ensure on-going review of Professional PINs/registration.
The DPEN is to undertake daily safe staffing reviews on the escalation wards. Divisional Senior Nurses to review staffing levels on each shift and take action to
C
Page 5 of 6
Statement Risks and mitigating actions C/NC
ensure that patient care remains safe and effective. Clear escalation plans in place and weekend monitoring of staffing is overseen by the DPEN and the corporate nursing team.
Page 6 of 6
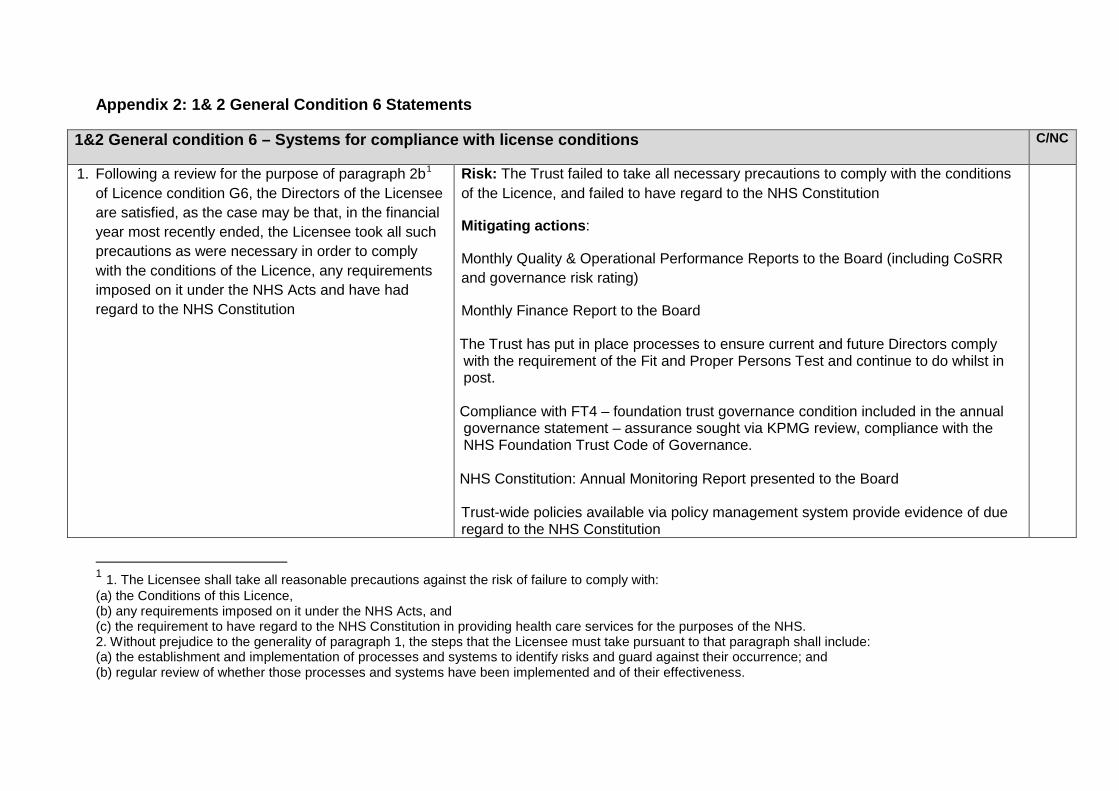
Appendix 2: 1& 2 General Condition 6 Statements
1&2 General condition 6 – Systems for compliance with license conditions C/NC
1. Following a review for the purpose of paragraph 2b1 of Licence condition G6, the Directors of the Licensee are satisfied, as the case may be that, in the financial year most recently ended, the Licensee took all such precautions as were necessary in order to comply with the conditions of the Licence, any requirements imposed on it under the NHS Acts and have had regard to the NHS Constitution
Risk: The Trust failed to take all necessary precautions to comply with the conditions of the Licence, and failed to have regard to the NHS Constitution
Mitigating actions:
Monthly Quality & Operational Performance Reports to the Board (including CoSRR and governance risk rating)
Monthly Finance Report to the Board The Trust has put in place processes to ensure current and future Directors comply with the requirement of the Fit and Proper Persons Test and continue to do whilst in post. Compliance with FT4 – foundation trust governance condition included in the annual governance statement – assurance sought via KPMG review, compliance with the NHS Foundation Trust Code of Governance. NHS Constitution: Annual Monitoring Report presented to the Board Trust-wide policies available via policy management system provide evidence of due regard to the NHS Constitution
1 1. The Licensee shall take all reasonable precautions against the risk of failure to comply with: (a) the Conditions of this Licence, (b) any requirements imposed on it under the NHS Acts, and (c) the requirement to have regard to the NHS Constitution in providing health care services for the purposes of the NHS. 2. Without prejudice to the generality of paragraph 1, the steps that the Licensee must take pursuant to that paragraph shall include: (a) the establishment and implementation of processes and systems to identify risks and guard against their occurrence; and (b) regular review of whether those processes and systems have been implemented and of their effectiveness.
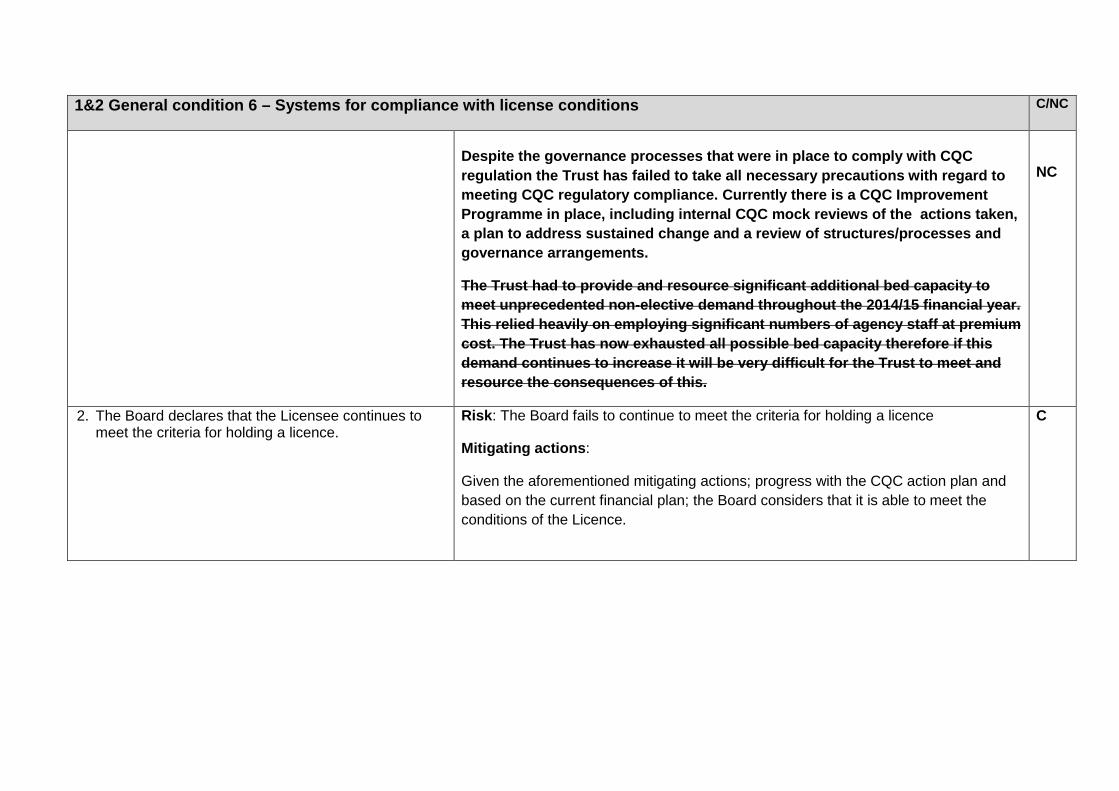
1&2 General condition 6 – Systems for compliance with license conditions C/NC
Despite the governance processes that were in place to comply with CQC regulation the Trust has failed to take all necessary precautions with regard to meeting CQC regulatory compliance. Currently there is a CQC Improvement Programme in place, including internal CQC mock reviews of the actions taken, a plan to address sustained change and a review of structures/processes and governance arrangements.
The Trust had to provide and resource significant additional bed capacity to meet unprecedented non-elective demand throughout the 2014/15 financial year. This relied heavily on employing significant numbers of agency staff at premium cost. The Trust has now exhausted all possible bed capacity therefore if this demand continues to increase it will be very difficult for the Trust to meet and resource the consequences of this.
NC
2. The Board declares that the Licensee continues to meet the criteria for holding a licence.
Risk: The Board fails to continue to meet the criteria for holding a licence
Mitigating actions:
Given the aforementioned mitigating actions; progress with the CQC action plan and based on the current financial plan; the Board considers that it is able to meet the conditions of the Licence.
C
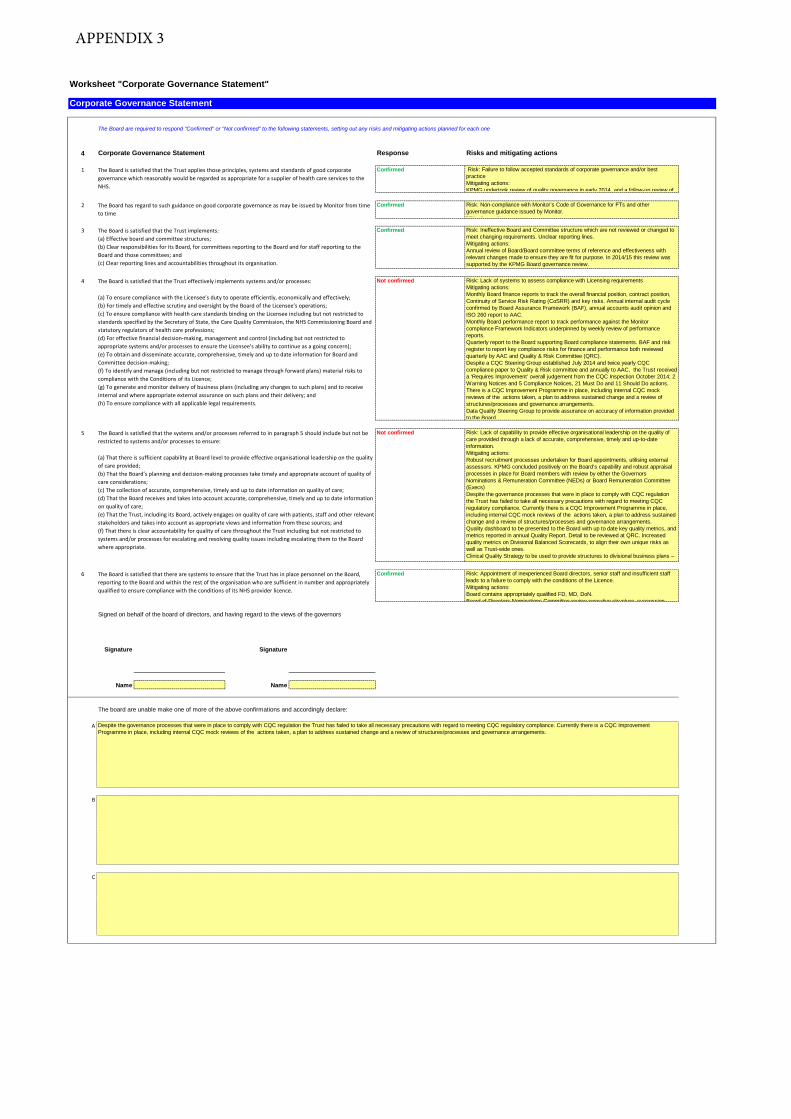
Worksheet "Corporate Governance Statement"
Corporate Governance Statement
The Board are required to respond "Confirmed" or "Not confirmed" to the following statements, setting out any risks and mitigating actions planned for each one
4 Corporate Governance Statement Response Risks and mitigating actions
1 Confirmed Risk: Failure to follow accepted standards of corporate governance and/or best practiceMitigating actions:KPMG undertook review of quality governance in early 2014, and a follow-up review of
2 Confirmed Risk: Non-compliance with Monitor’s Code of Governance for FTs and other governance guidance issued by Monitor.Mitigating actions:
3 Confirmed Risk: Ineffective Board and Committee structure which are not reviewed or changed to meet changing requirements. Unclear reporting lines.Mitigating actions: Annual review of Board/Board committee terms of reference and effectiveness with relevant changes made to ensure they are fit for purpose. In 2014/15 this review was supported by the KPMG Board governance review.
4 Not confirmed Risk: Lack of systems to assess compliance with Licensing requirements Mitigating actions: Monthly Board finance reports to track the overall financial position, contract position, Continuity of Service Risk Rating (CoSRR) and key risks. Annual internal audit cycle confirmed by Board Assurance Framework (BAF), annual accounts audit opinion and ISO 260 report to AAC.Monthly Board performance report to track performance against the Monitor compliance Framework Indicators underpinned by weekly review of performance reports.Quarterly report to the Board supporting Board compliance statements. BAF and risk register to report key compliance risks for finance and performance both reviewed quarterly by AAC and Quality & Risk Committee (QRC).Despite a CQC Steering Group established July 2014 and twice yearly CQC compliance paper to Quality & Risk committee and annually to AAC, the Trust received a ‘Requires Improvement’ overall judgement from the CQC Inspection October 2014; 2 Warning Notices and 5 Compliance Notices, 21 Must Do and 11 Should Do actions. There is a CQC Improvement Programme in place, including internal CQC mock reviews of the actions taken, a plan to address sustained change and a review of structures/processes and governance arrangements.Data Quality Steering Group to provide assurance on accuracy of information provided to the Board.
5 Not confirmed Risk: Lack of capability to provide effective organisational leadership on the quality of care provided through a lack of accurate, comprehensive, timely and up-to-date information.Mitigating actions:Robust recruitment processes undertaken for Board appointments, utilising external assessors. KPMG concluded positively on the Board’s capability and robust appraisal processes in place for Board members with review by either the Governors Nominations & Remuneration Committee (NEDs) or Board Remuneration Committee (Execs) Despite the governance processes that were in place to comply with CQC regulation the Trust has failed to take all necessary precautions with regard to meeting CQC regulatory compliance. Currently there is a CQC Improvement Programme in place, including internal CQC mock reviews of the actions taken, a plan to address sustained change and a review of structures/processes and governance arrangements.Quality dashboard to be presented to the Board with up to date key quality metrics, and metrics reported in annual Quality Report. Detail to be reviewed at QRC. Increased quality metrics on Divisional Balanced Scorecards, to align their own unique risks as well as Trust-wide ones.Clinical Quality Strategy to be used to provide structures to divisional business plans –
6 Confirmed Risk: Appointment of inexperienced Board directors, senior staff and insufficient staff leads to a failure to comply with the conditions of the Licence.Mitigating actions:Board contains appropriately qualified FD, MD, DoN.Board of Directors Nominations Committee review executive structure succession
Signed on behalf of the board of directors, and having regard to the views of the governors
Signature Signature
Name Name
A
B
C
The Board is satisfied that the Trust applies those principles, systems and standards of good corporate governance which reasonably would be regarded as appropriate for a supplier of health care services to the NHS.
The Board has regard to such guidance on good corporate governance as may be issued by Monitor from time to time
The Board is satisfied that the Trust implements: (a) Effective board and committee structures;(b) Clear responsibilities for its Board, for committees reporting to the Board and for staff reporting to the Board and those committees; and(c) Clear reporting lines and accountabilities throughout its organisation.
The Board is satisfied that the Trust effectively implements systems and/or processes:
(a) To ensure compliance with the Licensee’s duty to operate efficiently, economically and effectively;(b) For timely and effective scrutiny and oversight by the Board of the Licensee’s operations; (c) To ensure compliance with health care standards binding on the Licensee including but not restricted to standards specified by the Secretary of State, the Care Quality Commission, the NHS Commissioning Board and statutory regulators of health care professions;(d) For effective financial decision-making, management and control (including but not restricted to appropriate systems and/or processes to ensure the Licensee’s ability to continue as a going concern); (e) To obtain and disseminate accurate, comprehensive, timely and up to date information for Board and Committee decision-making;(f) To identify and manage (including but not restricted to manage through forward plans) material risks to compliance with the Conditions of its Licence;(g) To generate and monitor delivery of business plans (including any changes to such plans) and to receive internal and where appropriate external assurance on such plans and their delivery; and(h) To ensure compliance with all applicable legal requirements.
The Board is satisfied that the systems and/or processes referred to in paragraph 5 should include but not be restricted to systems and/or processes to ensure:
(a) That there is sufficient capability at Board level to provide effective organisational leadership on the quality of care provided; (b) That the Board’s planning and decision-making processes take timely and appropriate account of quality of care considerations;(c) The collection of accurate, comprehensive, timely and up to date information on quality of care;(d) That the Board receives and takes into account accurate, comprehensive, timely and up to date information on quality of care;(e) That the Trust, including its Board, actively engages on quality of care with patients, staff and other relevant stakeholders and takes into account as appropriate views and information from these sources; and(f) That there is clear accountability for quality of care throughout the Trust including but not restricted to systems and/or processes for escalating and resolving quality issues including escalating them to the Board where appropriate.
Despite the governance processes that were in place to comply with CQC regulation the Trust has failed to take all necessary precautions with regard to meeting CQC regulatory compliance. Currently there is a CQC Improvement Programme in place, including internal CQC mock reviews of the actions taken, a plan to address sustained change and a review of structures/processes and governance arrangements.
The board are unable make one of more of the above confirmations and accordingly declare:
The Board is satisfied that there are systems to ensure that the Trust has in place personnel on the Board, reporting to the Board and within the rest of the organisation who are sufficient in number and appropriately qualified to ensure compliance with the conditions of its NHS provider licence.
APPENDIX 3
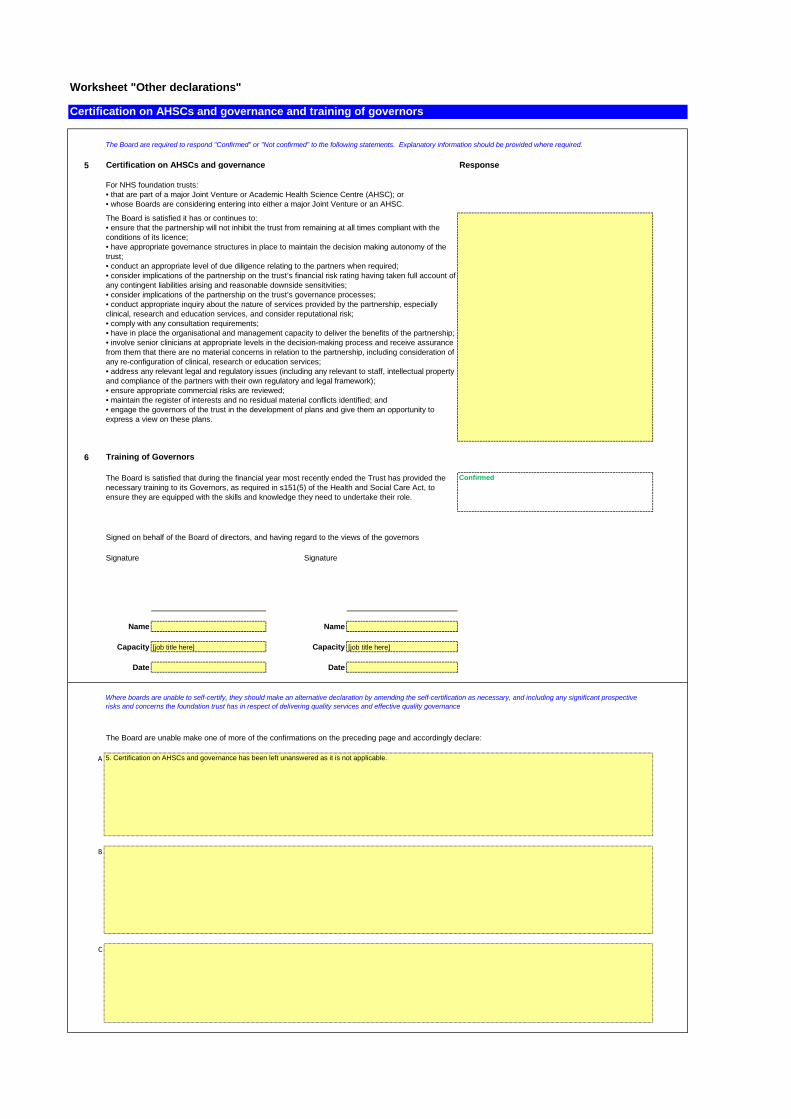
Worksheet "Other declarations"
Certification on AHSCs and governance and training of governors
5 Certification on AHSCs and governance Response
6 Training of Governors
Confirmed
Signed on behalf of the Board of directors, and having regard to the views of the governors
Signature Signature
Name Name
Capacity [job title here] Capacity [job title here]
Date Date
A
B
C
The Board is satisfied it has or continues to:• ensure that the partnership will not inhibit the trust from remaining at all times compliant with the conditions of its licence;• have appropriate governance structures in place to maintain the decision making autonomy of the trust;• conduct an appropriate level of due diligence relating to the partners when required;• consider implications of the partnership on the trust’s financial risk rating having taken full account ofany contingent liabilities arising and reasonable downside sensitivities;• consider implications of the partnership on the trust’s governance processes;• conduct appropriate inquiry about the nature of services provided by the partnership, especially clinical, research and education services, and consider reputational risk;• comply with any consultation requirements;• have in place the organisational and management capacity to deliver the benefits of the partnership;• involve senior clinicians at appropriate levels in the decision-making process and receive assurance from them that there are no material concerns in relation to the partnership, including consideration of any re-configuration of clinical, research or education services;• address any relevant legal and regulatory issues (including any relevant to staff, intellectual property and compliance of the partners with their own regulatory and legal framework);• ensure appropriate commercial risks are reviewed;• maintain the register of interests and no residual material conflicts identified; and• engage the governors of the trust in the development of plans and give them an opportunity to express a view on these plans.
The Board is satisfied that during the financial year most recently ended the Trust has provided the necessary training to its Governors, as required in s151(5) of the Health and Social Care Act, to ensure they are equipped with the skills and knowledge they need to undertake their role.
The Board are required to respond "Confirmed" or "Not confirmed" to the following statements. Explanatory information should be provided where required.
For NHS foundation trusts:• that are part of a major Joint Venture or Academic Health Science Centre (AHSC); or• whose Boards are considering entering into either a major Joint Venture or an AHSC.
Where boards are unable to self-certify, they should make an alternative declaration by amending the self-certification as necessary, and including any significant prospective risks and concerns the foundation trust has in respect of delivering quality services and effective quality governance
The Board are unable make one of more of the confirmations on the preceding page and accordingly declare:
5. Certification on AHSCs and governance has been left unanswered as it is not applicable.

Worksheet "Certification G6"
1 & 2 General condition 6 - Systems for compliance with license conditions
1 Not confirmed
2 Confirmed
Signed on behalf of the board of directors, and having regard to the views of the governors
Signature Signature
Name Name
Capacity [job title here] Capacity [job title here]
Date Date
A
B
Declarations required by General condition 6 of the NHS provider licence
Further explanatory information should be provided below where the Board has been unable to confirm declarations 1 or 2 above.
The board are required to respond "Confirmed" or "Not confirmed" to the following statements (please select 'not confirmed' if confirming another option). Explanatory information should be provided where required.
Despite the governance processes that were in place to comply with CQC regulation the Trust has failed to take all necessary precautions with regard to meeting CQC regulatory compliance. Currently there is a CQC Improvement Programme in place, including internal CQC mock reviews of the actions taken, a plan to address sustained change and a review of structures/processes and governance arrangements.
Following a review for the purpose of paragraph 2(b) of licence condition G6, the Directors of the Licensee are satisfied, as the case may be that, in the Financial Year most recently ended, the Licensee took all such precautions as were necessary in order to comply with the conditions of the licence, any requirements imposed on it under the NHS Acts and have had regard to the NHS Constitution.
ANDThe board declares that the Licensee continues to meet the criteria for holding a licence.
APPENDIX 4
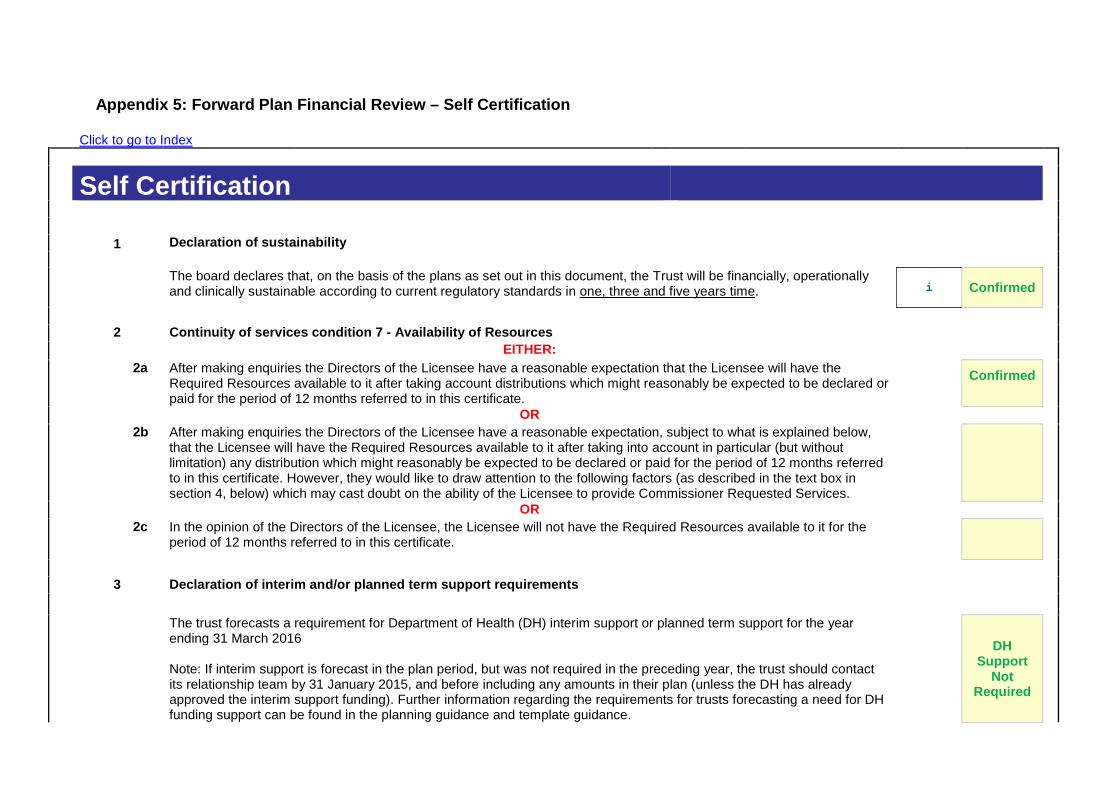
Appendix 5: Forward Plan Financial Review – Self Certification
Click to go to Index
Self Certification 1 Declaration of sustainability
The board declares that, on the basis of the plans as set out in this document, the Trust will be financially, operationally and clinically sustainable according to current regulatory standards in one, three and five years time. i Confirmed
2 Continuity of services condition 7 - Availability of Resources EITHER:
2a After making enquiries the Directors of the Licensee have a reasonable expectation that the Licensee will have the Required Resources available to it after taking account distributions which might reasonably be expected to be declared or paid for the period of 12 months referred to in this certificate.
Confirmed
OR
2b After making enquiries the Directors of the Licensee have a reasonable expectation, subject to what is explained below, that the Licensee will have the Required Resources available to it after taking into account in particular (but without limitation) any distribution which might reasonably be expected to be declared or paid for the period of 12 months referred to in this certificate. However, they would like to draw attention to the following factors (as described in the text box in section 4, below) which may cast doubt on the ability of the Licensee to provide Commissioner Requested Services.
OR
2c In the opinion of the Directors of the Licensee, the Licensee will not have the Required Resources available to it for the period of 12 months referred to in this certificate.
3 Declaration of interim and/or planned term support requirements
The trust forecasts a requirement for Department of Health (DH) interim support or planned term support for the year ending 31 March 2016 Note: If interim support is forecast in the plan period, but was not required in the preceding year, the trust should contact its relationship team by 31 January 2015, and before including any amounts in their plan (unless the DH has already approved the interim support funding). Further information regarding the requirements for trusts forecasting a need for DH funding support can be found in the planning guidance and template guidance.
DH Support
Not Required
Meeting of the Board of Directors – public session
Wednesday 29th May 2015 Agenda item 23
Report on Actions in Response to Kate Lampard’s Report into Themes and Lessons Learnt from NHS Investigations into Matters relating to Jimmy Savile
Reason for item: Following the death of Jimmy Savile a number of allegations were made about his conduct in NHS establishments which led to Kate Lampard QC being asked to produce a ‘lessons learned’ report. The report included a number of recommendations, of which 10 apply to acute Trusts. The purpose of this paper is to update the Trust Board on progress of actions in response to Kate Lampard’s report into Themes and lessons learnt from NHS investigations into matters relating to Jimmy Saville. Monitor require Trusts to provide an overview of their response to the recommendations using the attached template by 15th June 2015. Summary: The Trust has responded to the recommendations in the Lampard Report, there are several outstanding actions included in the progress report that should be completed by the end of July 2015. These include: • Integrating the protocol for managing formal guest visits into a more robust policy. • Ensuring that all volunteers receive safeguarding adults and children leaflets and
develop a programme to ensure refresher training is implemented. • Review of restricted Internet sites by Information Governance Steering Group (IGSG) in
July 2015 and publicising to staff, patients and visitors key information about the relevant policies.
Completion of these actions will be monitored by the Trust Safeguarding Committee Board Action required: The Board is asked to: 1. Review the response overview and the actions in place. Report from: Bev Hall, Deputy Director of Nursing and Patient Experience Report sponsor: Theresa Murphy, Director of the Patient Experience and Nursing Links to Trust strategic priorities: • To create a patient centred organisation to deliver improvements in patient experience
and the quality of care we provide. Previous consideration at Board or Committees: None.

Equality and diversity considerations: None Financial implications: Business cases will be written to support the creation of a Child Safeguarding Advisor role and to extend the Safeguarding Administrator position beyond the current six months non recurrent funding.
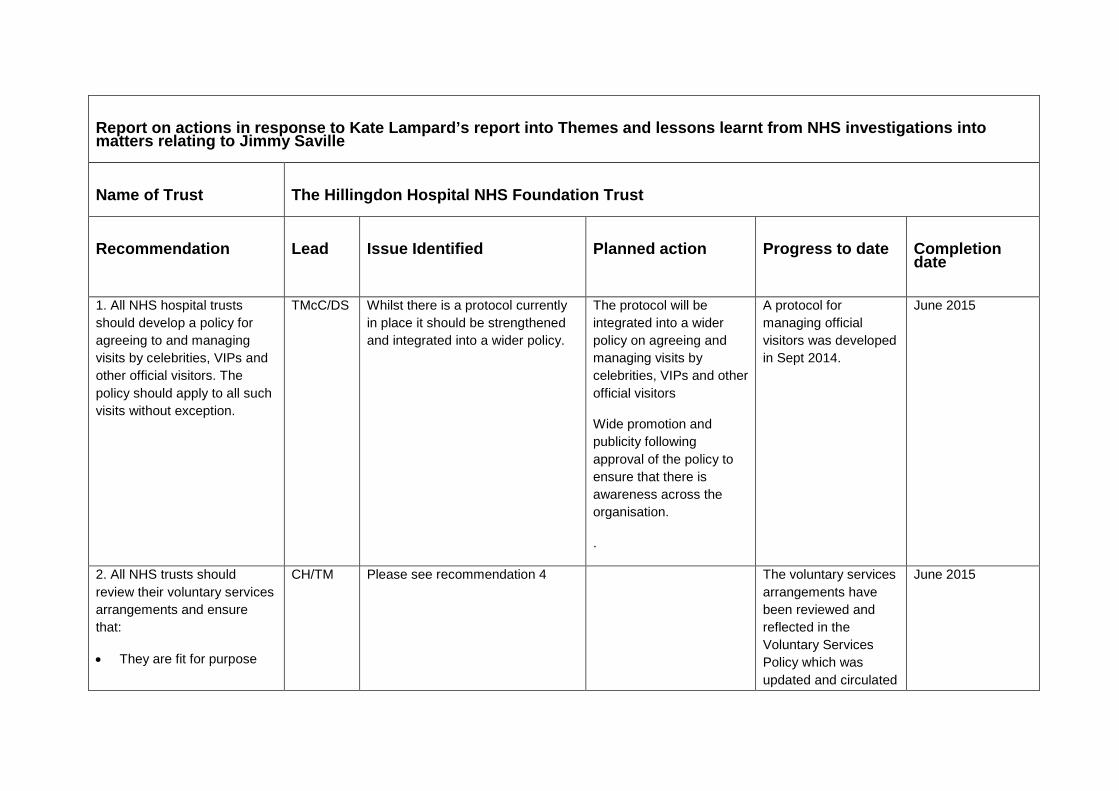
Report on actions in response to Kate Lampard’s report into Themes and lessons learnt from NHS investigations into matters relating to Jimmy Saville Name of Trust
The Hillingdon Hospital NHS Foundation Trust
Recommendation
Lead
Issue Identified
Planned action
Progress to date
Completion date
1. All NHS hospital trusts should develop a policy for agreeing to and managing visits by celebrities, VIPs and other official visitors. The policy should apply to all such visits without exception.
TMcC/DS
Whilst there is a protocol currently in place it should be strengthened and integrated into a wider policy.
The protocol will be integrated into a wider policy on agreeing and managing visits by celebrities, VIPs and other official visitors
Wide promotion and publicity following approval of the policy to ensure that there is awareness across the organisation.
.
A protocol for managing official visitors was developed in Sept 2014.
June 2015
2. All NHS trusts should review their voluntary services arrangements and ensure that:
• They are fit for purpose
CH/TM Please see recommendation 4
The voluntary services arrangements have been reviewed and reflected in the Voluntary Services Policy which was updated and circulated
June 2015
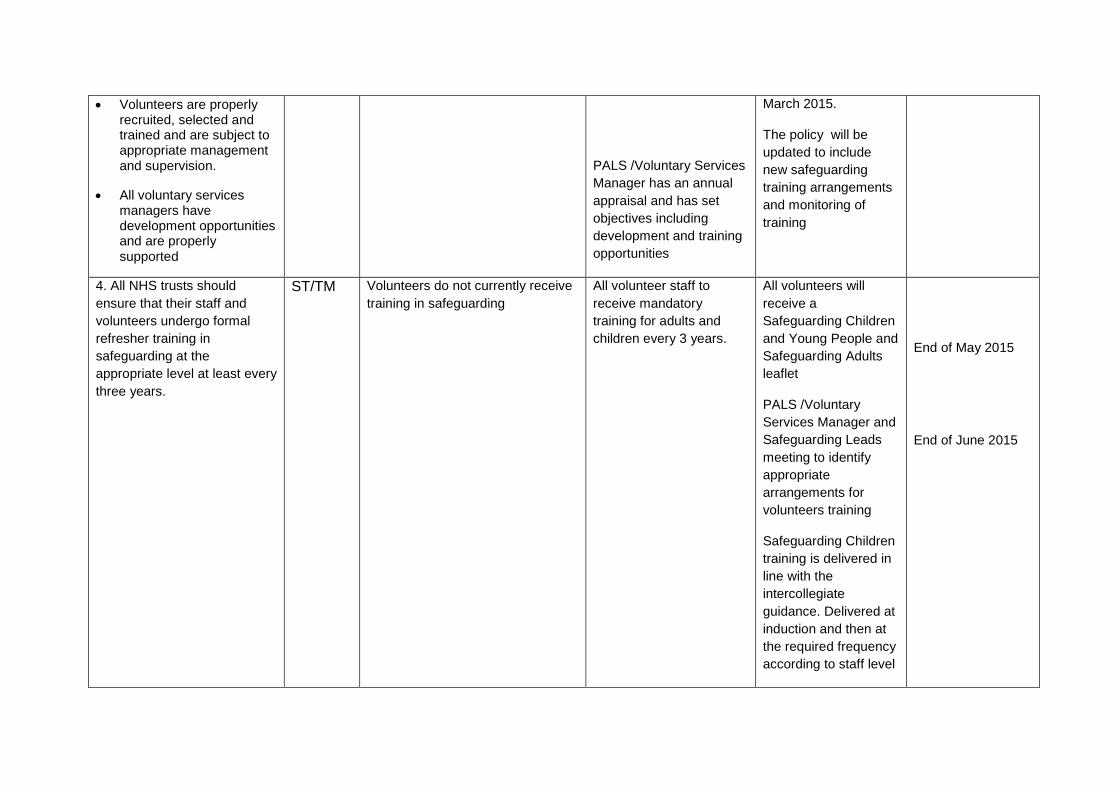
• Volunteers are properly recruited, selected and trained and are subject to appropriate management and supervision.
• All voluntary services managers have development opportunities and are properly supported
PALS /Voluntary Services Manager has an annual appraisal and has set objectives including development and training opportunities
March 2015.
The policy will be updated to include new safeguarding training arrangements and monitoring of training
4. All NHS trusts should ensure that their staff and volunteers undergo formal refresher training in safeguarding at the appropriate level at least every three years.
ST/TM
Volunteers do not currently receive training in safeguarding
All volunteer staff to receive mandatory training for adults and children every 3 years.
All volunteers will receive a Safeguarding Children and Young People and Safeguarding Adults leaflet
PALS /Voluntary Services Manager and Safeguarding Leads meeting to identify appropriate arrangements for volunteers training
Safeguarding Children training is delivered in line with the intercollegiate guidance. Delivered at induction and then at the required frequency according to staff level
End of May 2015
End of June 2015
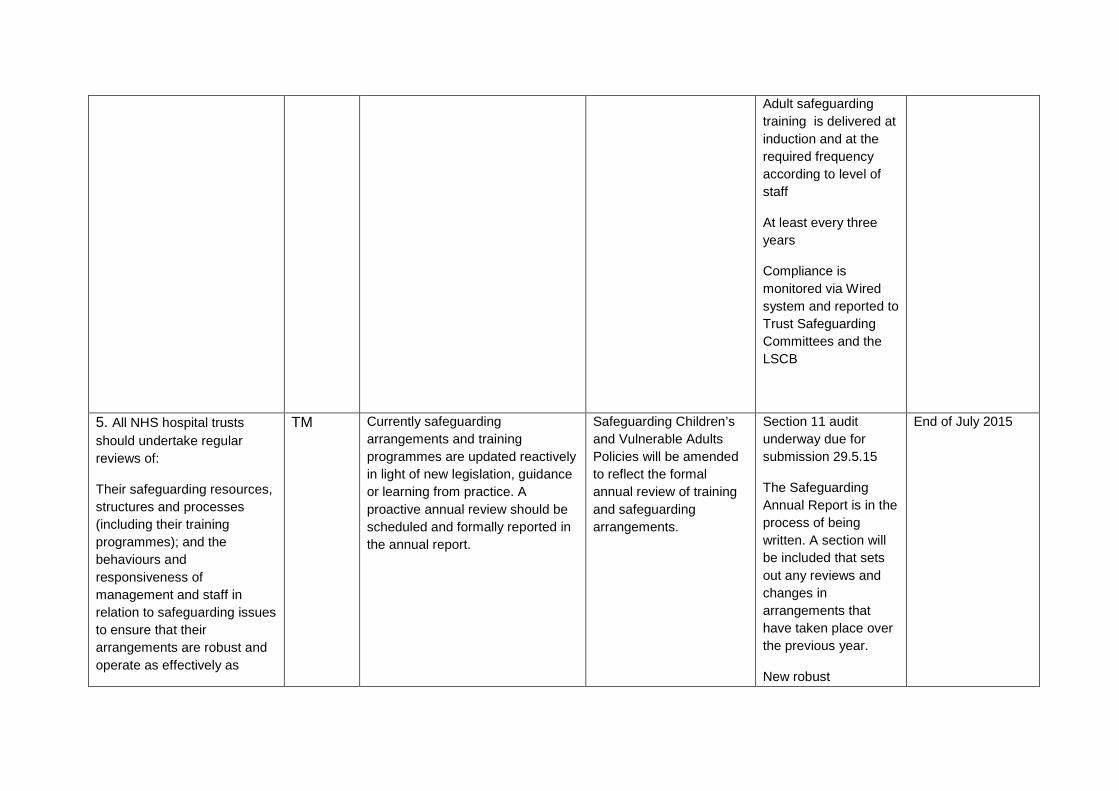
Adult safeguarding training is delivered at induction and at the required frequency according to level of staff
At least every three years
Compliance is monitored via Wired system and reported to Trust Safeguarding Committees and the LSCB
5. All NHS hospital trusts should undertake regular reviews of:
Their safeguarding resources, structures and processes (including their training programmes); and the behaviours and responsiveness of management and staff in relation to safeguarding issues to ensure that their arrangements are robust and operate as effectively as
TM Currently safeguarding arrangements and training programmes are updated reactively in light of new legislation, guidance or learning from practice. A proactive annual review should be scheduled and formally reported in the annual report.
Safeguarding Children’s and Vulnerable Adults Policies will be amended to reflect the formal annual review of training and safeguarding arrangements.
Section 11 audit underway due for submission 29.5.15
The Safeguarding Annual Report is in the process of being written. A section will be included that sets out any reviews and changes in arrangements that have taken place over the previous year.
New robust
End of July 2015
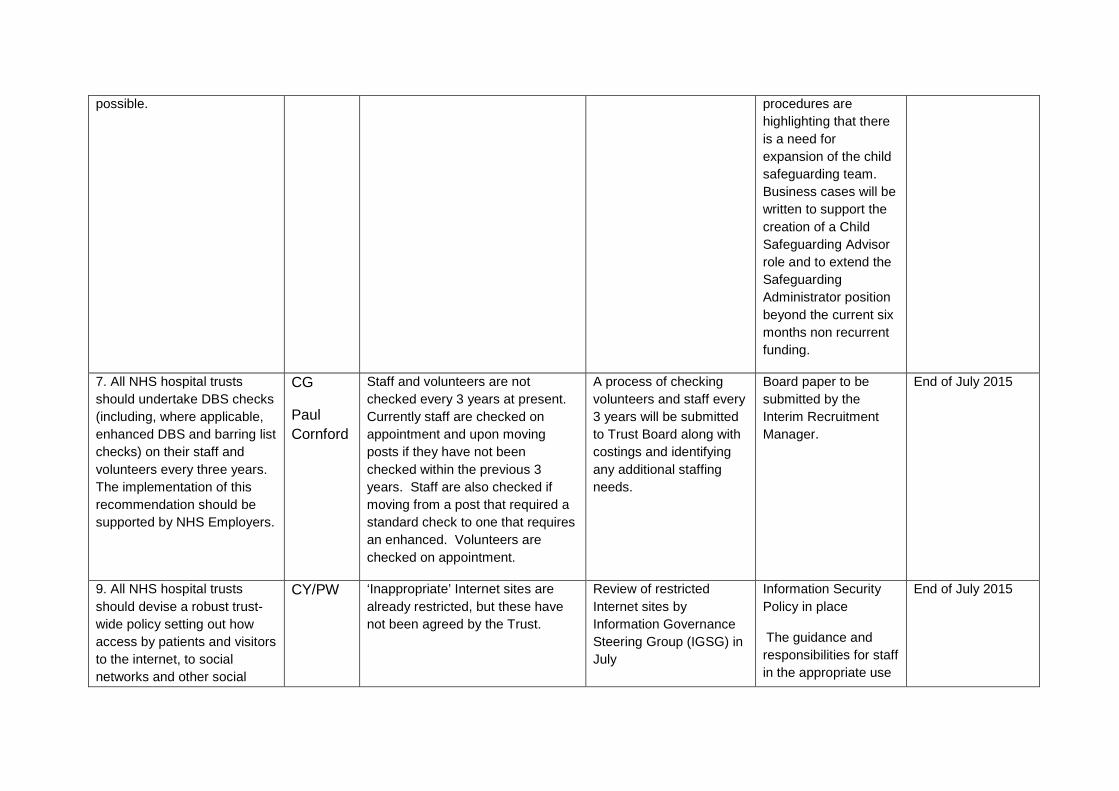
possible.
procedures are highlighting that there is a need for expansion of the child safeguarding team. Business cases will be written to support the creation of a Child Safeguarding Advisor role and to extend the Safeguarding Administrator position beyond the current six months non recurrent funding.
7. All NHS hospital trusts should undertake DBS checks (including, where applicable, enhanced DBS and barring list checks) on their staff and volunteers every three years. The implementation of this recommendation should be supported by NHS Employers.
CG
Paul Cornford
Staff and volunteers are not checked every 3 years at present. Currently staff are checked on appointment and upon moving posts if they have not been checked within the previous 3 years. Staff are also checked if moving from a post that required a standard check to one that requires an enhanced. Volunteers are checked on appointment.
A process of checking volunteers and staff every 3 years will be submitted to Trust Board along with costings and identifying any additional staffing needs.
Board paper to be submitted by the Interim Recruitment Manager.
End of July 2015
9. All NHS hospital trusts should devise a robust trust-wide policy setting out how access by patients and visitors to the internet, to social networks and other social
CY/PW
‘Inappropriate’ Internet sites are already restricted, but these have not been agreed by the Trust.
Review of restricted Internet sites by Information Governance Steering Group (IGSG) in July
Information Security Policy in place
The guidance and responsibilities for staff in the appropriate use
End of July 2015
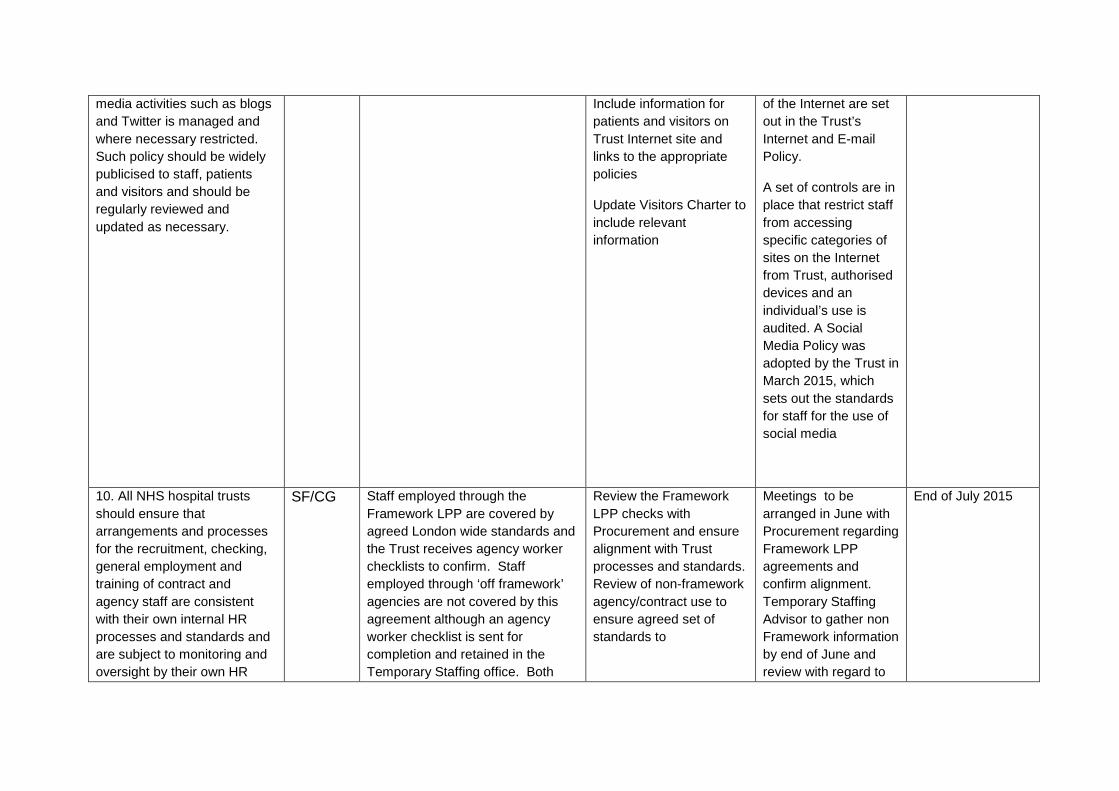
media activities such as blogs and Twitter is managed and where necessary restricted. Such policy should be widely publicised to staff, patients and visitors and should be regularly reviewed and updated as necessary.
Include information for patients and visitors on Trust Internet site and links to the appropriate policies
Update Visitors Charter to include relevant information
of the Internet are set out in the Trust’s Internet and E-mail Policy.
A set of controls are in place that restrict staff from accessing specific categories of sites on the Internet from Trust, authorised devices and an individual’s use is audited. A Social Media Policy was adopted by the Trust in March 2015, which sets out the standards for staff for the use of social media
10. All NHS hospital trusts should ensure that arrangements and processes for the recruitment, checking, general employment and training of contract and agency staff are consistent with their own internal HR processes and standards and are subject to monitoring and oversight by their own HR
SF/CG
Staff employed through the Framework LPP are covered by agreed London wide standards and the Trust receives agency worker checklists to confirm. Staff employed through ‘off framework’ agencies are not covered by this agreement although an agency worker checklist is sent for completion and retained in the Temporary Staffing office. Both
Review the Framework LPP checks with Procurement and ensure alignment with Trust processes and standards. Review of non-framework agency/contract use to ensure agreed set of standards to
Meetings to be arranged in June with Procurement regarding Framework LPP agreements and confirm alignment. Temporary Staffing Advisor to gather non Framework information by end of June and review with regard to
End of July 2015
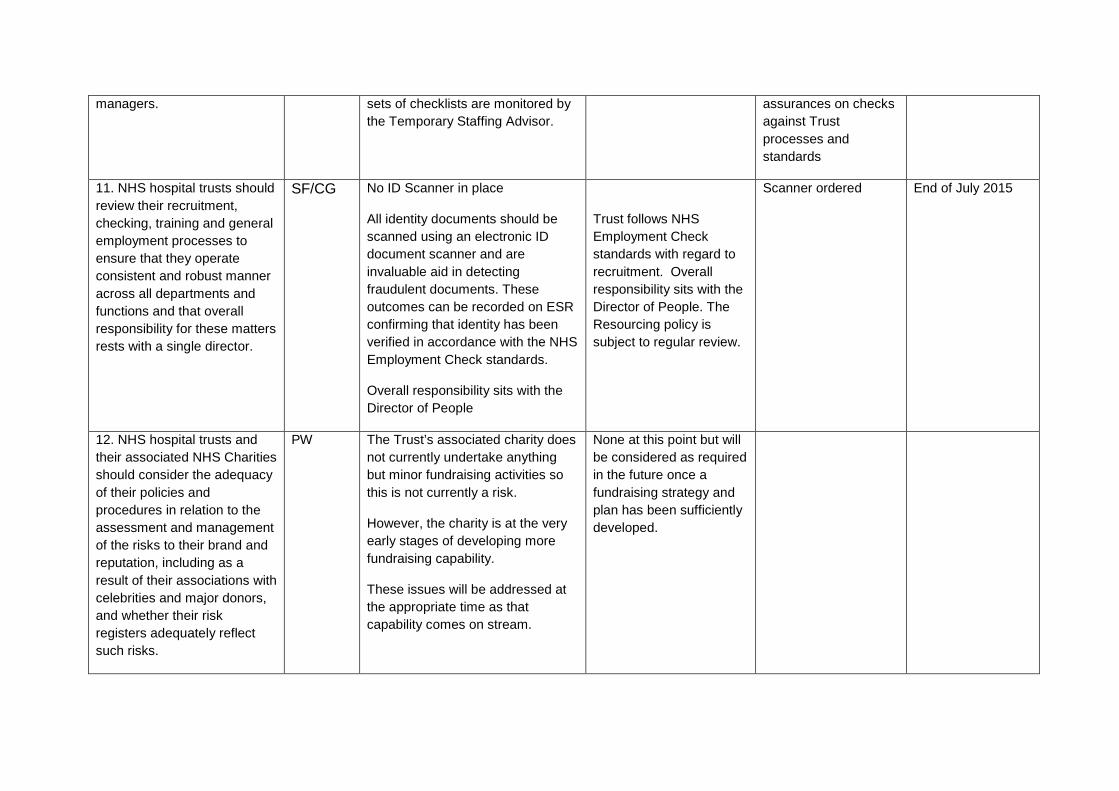
managers. sets of checklists are monitored by the Temporary Staffing Advisor.
assurances on checks against Trust processes and standards
11. NHS hospital trusts should review their recruitment, checking, training and general employment processes to ensure that they operate consistent and robust manner across all departments and functions and that overall responsibility for these matters rests with a single director.
SF/CG No ID Scanner in place
All identity documents should be scanned using an electronic ID document scanner and are invaluable aid in detecting fraudulent documents. These outcomes can be recorded on ESR confirming that identity has been verified in accordance with the NHS Employment Check standards.
Overall responsibility sits with the Director of People
Trust follows NHS Employment Check standards with regard to recruitment. Overall responsibility sits with the Director of People. The Resourcing policy is subject to regular review.
Scanner ordered End of July 2015
12. NHS hospital trusts and their associated NHS Charities should consider the adequacy of their policies and procedures in relation to the assessment and management of the risks to their brand and reputation, including as a result of their associations with celebrities and major donors, and whether their risk registers adequately reflect such risks.
PW The Trust’s associated charity does not currently undertake anything but minor fundraising activities so this is not currently a risk.
However, the charity is at the very early stages of developing more fundraising capability.
These issues will be addressed at the appropriate time as that capability comes on stream.
None at this point but will be considered as required in the future once a fundraising strategy and plan has been sufficiently developed.
Monitor, the Trust Development Authority, the Care Quality Commission and NHS England should exercise their powers to ensure that NHS hospital trusts,(and where applicable, independent hospital and care organisations), comply with recommendations 1, 2, 4, 5, 7, 9, 10 and 11.
Meeting of the Board of Directors – public session
Wednesday 27th May 2015
Agenda item 24 Emergency Preparedness Resilience and Response (EPRR) Reason for item: This report seeks to provide assurance that the Trust is aligned with the Civil Contingencies Act and is compliant with the necessary requirements placed upon the Trust as a Category 1 responder. Summary: The NHS must be able to plan for and respond to a wide range of emergencies and business continuity incidents that could affect health or patient safety. These could be anything from severe weather to an infectious disease outbreak or a major transport accident. Under the Civil Contingencies Act (2004) (CCA 2004), the Trust must demonstrate that we can effectively respond to emergencies and business continuity incidents while maintaining services to patients. This work is referred to as Emergency Preparedness, Resilience and Response (EPRR). Under the definition of the CCA 2004, all Acute Trusts are classed as Category 1 Responders by being organisations at the core of health emergency response. To be compliant with the Act the Trust has to meet a set of core standards that are assessed annually by the EPRR Department of NHS England (London Region) who in turn report to the Department of Health. Board Action required: The Board is asked to: 1. Review the report. 2. Note the assurance in relation to the Trust’s emergency preparedness compliance with
the Civil Contingencies Act 2004. Report from: Jayne Austin Emergency Planning Liaison Officer; Vikas Sharma Governance and Business Continuity Manager; Melissa Mellett, Acting Director of Operational Performance Report sponsor: Joe Smyth Chief Operating Officer Links to Trust strategic priorities: The report relates to the delivery of all of the strategic priorities. Equality and diversity considerations: There is no positive or negative impact from this report. Financial implications: none directly arising from the report.
1
Emergency Preparedness Resilience and Response (EPRR)
1. Introduction The NHS must be able to plan for and respond to a wide range of emergencies and business continuity incidents that could affect health or patient safety. These could be anything from severe weather to an infectious disease outbreak or a major transport accident. Under the Civil Contingencies Act (2004) (CCA 2004), the Trust must demonstrate that we can effectively respond to emergencies and business continuity incidents while maintaining services to patients. This work is referred to as Emergency Preparedness, Resilience and Response (EPRR). Under the definition of the CCA 2004, all Acute Trusts are classed as Category 1 Responders by being organisations at the core of health emergency response. To be compliant with the Act the Trust has to meet a set of core standards that are assessed annually by the EPRR Department of NHS England (London Region) who in turn report to the Department of Health. The Trust is a member of the North West London Network for EPRR. 2. Key Statutory Obligations of the CCA 2004 for the Trust. • Have a nominated Director level Accountable Emergency Officer who will be
responsible for EPRR, a designated Emergency Planning Liaison Officer and a Business Continuity Manager.
• Contribute to area planning for EPRR through local health resilience partnerships (LHRPs) and other relevant groups.
• Have suitable, proportionate and up to date plans to cover the Trust response to Major and Internal Incidents.
• Have business continuity plans as identified in national and community risk registers.
• Training and exercising must include: i. a communications exercise every six months
ii. a desktop exercise once a year
iii. a major live exercise every three years.
• Have appropriately trained competent staff and suitable facilities available round the clock to effectively manage an emergency and business continuity incident.
• Share resources as required to respond to an emergency or business continuity incident.
• Have arrangements in place to inform, warn and advise the public during an incident.
3. Trust Compliance • The Chief Operating Officer holds the post of the Accountable Emergency
Officer. The Executive Director of Patient Experience and Nursing has 2
responsibility for the management and delivery of business continuity. A part time dedicated Emergency Planning Liaison Officer (EPLO) is in post and a Governance and Business Continuity manager (at approx. 0.1 wte allocated resource) to deal with the Trust’s EPRR.
• The Trust has an overarching EPRR policy which outlines key responsibilities and the Trust process for dealing with EPRR.
• The Trust has in place an EPRR Committee chaired by the Director of Operations, with senior staff from all key areas in attendance thus ensuring cohesive and inclusive planning and to oversee and operationally manage the EPRR agenda.
• The Trust has developed a number of plans to ensure its resilience in line with the CCA 2004 including Major and Internal Incidents, Heatwave, VIP Plans, Flu Pandemic, Major Incident Communication Plan, and Business continuity plans (overarching, service level, threat specific and IT).
• The Trust is assessed annually by NHS England (NHSE) against the NHSE core standards for EPRR in line with the requirements of the CCA 2004 and achieved a rating of substantial assurance against the Core Standards review for 2014/15. In addition the Trust has participated in a number of regional desktop emergency planning exercises.
• The Trust has recently relocated the major incident room into the Private Patient Suite meeting room. This provides a better facility to co-ordinate the Trust’s response to a major incident.
• The major incident room provides a facility for silver command to allocate resources as required. The major incident plan makes provision for Gold Command that can co-ordinate with external bodies and share resource as deemed appropriate.
• The major incident plan contains instructions on establishing a press office and references the Trust’s communication policy.
4 Risks • Resources for comprehensive training. The EPRR team plan to investigate e-
learning packages and cascade training to mitigate this risk.
• Training records not held centrally in ESR/Wired. The Acting Director of Operations will take this forward with Learning and Development with a view to incorporate EPRR training records into the Trust central system.
• Inconsistent post-exercise/event reports. The EPRR team plan to implement a consistent post exercise template format including timescales for completion.
3
Meeting of the Board of Directors – public session
Wednesday 27th May 2015 Agenda item 25
Appointment of the Senior Independent Director Reason for item: To enable the Board to appoint the Trust’s Senior Independent Director. Summary: The NHS Code of Governance published by Monitor states that the Board of Directors of a Foundation Trust should appoint one of the Non-Executive Directors to be a Senior Independent Director (SID) in consultation with the Governors.
The role of the SID is to provide a sounding board for the Chair and to serve as an intermediary for the other Directors where necessary. The SID should be available to Governors if they have concerns which contact through the normal channels of Chairman, Chief Executive, Finance Director, or Trust Secretary has failed to resolve or for which such contact is inappropriate. Monitor state that the SID could be the Deputy Chair. The SID is also responsible for leading the performance evaluation of the Chairman, taking into account the views of Directors and Governors. The role description of the SID is contained in appendix 1.
In April 2014 the Board appointed Pradip Patel as the acting Senior Independent Director (SID) given that the existing SID James Reid was taking on the Interim Chair role. Having consulted the Governors present at a Governor ‘drop-in’ session, in November 2014 the Board agreed that Pradip would continue to hold the SID position in addition to being Deputy Chair. The Chair committed to discuss the appointment moving forward with the Governors at a future Council of Governors meeting.
The Council of Governors discussed this issue at its meeting on 5th May 2015 and unanimously supported Pradip continuing in this role given his tenure on the Board, success in the role, and that he continues to hold the support of colleagues. The Board is therefore asked to reconfirm Pradip’s reappointment as SID.
The Board is also asked to agree that as part of this role, Pradip continues as the Non-Executive Director member of the Council of Governors Nominations & Remuneration Committee when it is considering matters relating to the Trust Chair. Board Action required: The Board is asked to: 1. Continue Pradip Patel’s appointment as the Senior Independent Director (SID) until the
end of Pradip’s term of office or otherwise decided by the Board. 2. Agree that as part of this role, Pradip will continue as the Non-Executive Director
member of the Council of Governors Nominations & Remuneration Committee when it is considering matters relating to the Trust Chair.
Report from: Richard Sumray, Trust Chair
1

Links to Trust strategic priorities: • N/A Previous consideration at Board or Committees: this was last considered by the Board in November 2014 Equality and diversity considerations: none. Financial implications: none.
2
APPENDIX 1
ROLE OF THE SENIOR INDEPENDENT DIRECTOR (SID)
The Board of Directors will appoint one of the Non-Executive Directors as the Senior Independent Director (SID). In addition to their existing responsibilities as a Non-Executive Director, the SID will:
1. Provide a sounding board for the Chair.
2. Be available to Board members if they have concerns about the performance of the Board or the welfare of the Trust, which contact through the normal channels of Chairman, Chief Executive, Finance Director, or Trust Secretary has failed to resolve or for which such contact is inappropriate;
3. Facilitate the appraisal of the Chairman, including at least annually hold a meeting with the other independent Non-Executive Directors to evaluate the performance of the Chairman;
4. Be available to Governors and Members if they have concerns about the performance of the Board of Directors, the Trust’s compliance with its Licence or the welfare of the Trust, which contact through the normal channels of Chairman, Chief Executive, Finance Director or Trust Secretary has failed to resolve or for which such contact is inappropriate;
5. Help resolve any disagreements that may arise between the Council of Governors and Board of Directors, in accordance with any procedures agreed by the Trust;
6. Maintain a sufficient dialogue with Governors (including attending meetings as appropriate) in order to develop a balanced understanding of the issues and concerns of Governors. The Board of Directors will consult the Council of Governors when appointing the Senior Independent Director. The Board should state its reasons for determining a director is ‘independent’, if the director:
• Has been an employee of the NHS Foundation Trust within the last five years;
• Has, or has had within the last three years, a material business relationship with the NHS Foundation Trust either directly, or as a partner, shareholder, director or senior employee of a body that has such a relationship with the NHS Foundation Trust;
• Has received or receives additional remuneration from the NHS Foundation Trust apart from a director’s fee, participates in the NHS Foundation Trust’s performance-related pay scheme, or is a member of the NHS Foundation Trust’s pension scheme;
• Has close family ties with any of the NHS Foundation Trust’s advisers, directors or senior employees;
• Holds cross-directorships or has significant links with other directors through involvement in other companies or bodies; or
• Has served on the Board for more than six years from the date of their first appointment.
Approved by the Board 30th April 2014.
3
ITEM 27 Board Meeting in Public
27th May 2015
USE OF THE TRUST SEAL
The Board is asked to note the following use of the Trust Seal:
1) Ref No 188: Section 106 Agreement for Car Park between The Hillingdon Hospitals NHS Foundation Trust and London Borough of Hillingdon
Date seal applied: 24th April 2015 Seal applied by: The Hillingdon Hospitals NHS Foundation Trust Signatories: Shane DeGaris and Richard Sumray Location of sealed document: Capsticks Solicitors Signed under delegated authority to the Chief Executive.
Shane DeGaris Chief Executive