leeds teaching hospitals nhs trust operational plan … · leeds teaching hospitals nhs trust...
TRANSCRIPT
1
Leeds Teaching Hospitals NHS Trust Operational Plan 2016/17
Public Document 18th April 2016

2
Contents
1. Strategic Overview ............................................................................................... 3 2. Activity Planning .................................................................................................. 5 3. Quality ................................................................................................................. 8 4. Workforce Planning ........................................................................................... 13 5. Financial Planning ............................................................................................. 16 6. Capital Planning ................................................................................................. 23 7. Link to the emerging Sustainability and Transformation Plans .......................... 24
3
1. Strategic Overview
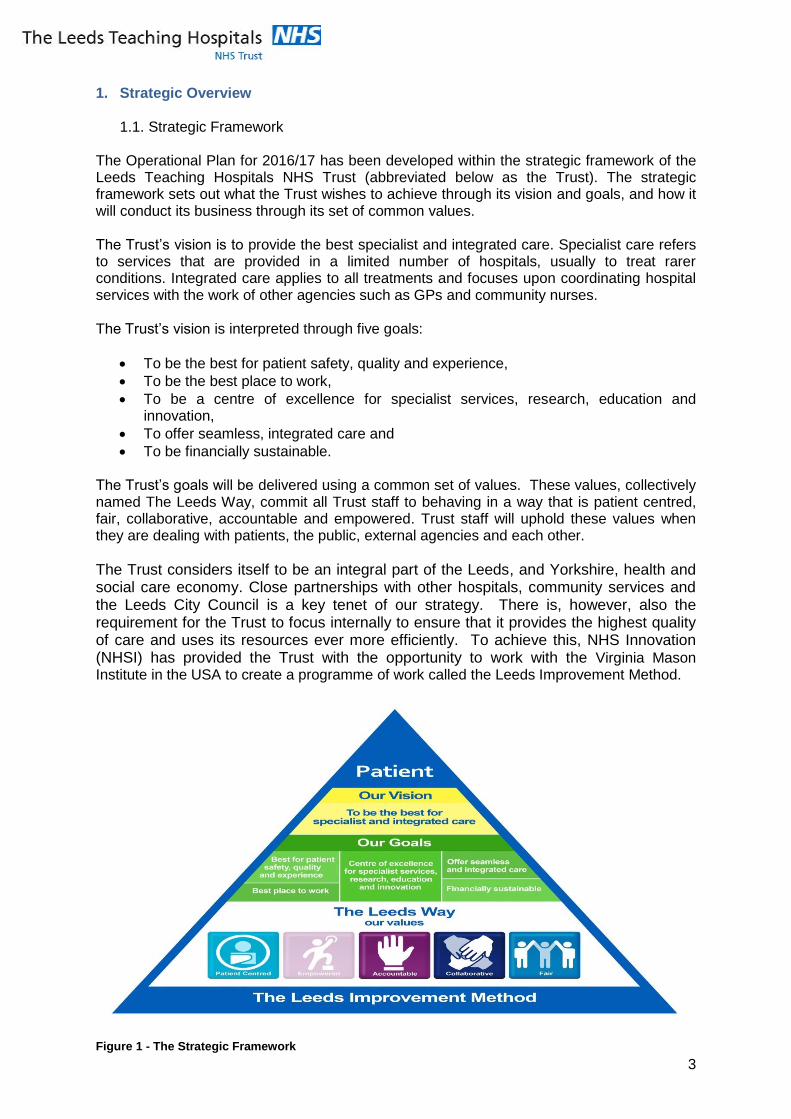
1.1. Strategic Framework The Operational Plan for 2016/17 has been developed within the strategic framework of the Leeds Teaching Hospitals NHS Trust (abbreviated below as the Trust). The strategic framework sets out what the Trust wishes to achieve through its vision and goals, and how it will conduct its business through its set of common values. The Trust’s vision is to provide the best specialist and integrated care. Specialist care refers to services that are provided in a limited number of hospitals, usually to treat rarer conditions. Integrated care applies to all treatments and focuses upon coordinating hospital services with the work of other agencies such as GPs and community nurses. The Trust’s vision is interpreted through five goals:
To be the best for patient safety, quality and experience,
To be the best place to work,
To be a centre of excellence for specialist services, research, education and innovation,
To offer seamless, integrated care and
To be financially sustainable. The Trust’s goals will be delivered using a common set of values. These values, collectively named The Leeds Way, commit all Trust staff to behaving in a way that is patient centred, fair, collaborative, accountable and empowered. Trust staff will uphold these values when they are dealing with patients, the public, external agencies and each other.
The Trust considers itself to be an integral part of the Leeds, and Yorkshire, health and social care economy. Close partnerships with other hospitals, community services and the Leeds City Council is a key tenet of our strategy. There is, however, also the requirement for the Trust to focus internally to ensure that it provides the highest quality of care and uses its resources ever more efficiently. To achieve this, NHS Innovation (NHSI) has provided the Trust with the opportunity to work with the Virginia Mason Institute in the USA to create a programme of work called the Leeds Improvement Method.
Figure 1 - The Strategic Framework
4
1.2. Strategy Development In developing the Trust’s strategy, the Board produced a number of tangible strategic statements which have been used in framing the Trust’s plans:
The Trust will continue to provide a range of local and specialist clinical services. It will also educate clinical and non-clinical staff in conjunction with the city’s universities. The Trust will develop its research activities to become a centre of excellence.
The Trust will monitor the various government initiatives on devolving regional health budgets and continue to work closely with colleagues in other organisations , in particular the Leeds Health and Social Care Transformation Board,.
Recognising the financial situation in the national and local health economies, the Trust will work with the Clinical Commissioning Groups (CCGs) and NHS England, who commission hospital services, to agree savings programmes. The Trust will expect to be fairly paid for the work it is asked to do.
The Trust will be a reliable partner to other organisations and seek to support other hospitals in their provision of local services in the West Yorkshire conurbation where it is financially and clinically viable for the Trust to do so. This will include working with the West Yorkshire Alliance of Acute Trusts.
The Trust will liaise with its commissioners to take account of the predicted population growth in Leeds and Yorkshire. This is currently an increase of 0.7% per year in Leeds, including a 2.4% increase in the population who are over 80 years old.
The Operational plan has benefitted from improved internal planning arrangements at the Trust. Corporate services have strengthened their financial and activity planning functions, and links with clinical areas have been improved. There has also been an increased emphasis on the estate, particularly the size and suitability of the Trust’s buildings at the Leeds General Infirmary (LGI) where the Trust is working with its partners in the Leeds health economy to replace the old Victorian buildings with new, smaller and more effective facilities. The bulk of the Trust plans are driven by its eighteen Clinical Service Units (CSUs) which are made up of related groups of clinical specialties led by a Clinical Director and a local management team, neurosciences is one example. Each CSU has created its own five year strategy which were discussed and signed off by the Trust’s Board. The purpose of these Clinical Business Strategies was to:
Create tangible plans within each clinical specialty that contribute to the Trust’s strategic framework,
Extend the Trust’s clinical and business planning horizons to five years,
Involve the Trust’s staff and other agencies in the planning process,
Drive the content of the Trust’s plans from its clinical services. In order to implement the Clinical Business Strategies, each CSU has developed its own one year operational plan for 2016/17. At the time of writing, these plans are work in progress with each plan having had an initial review at Trust level. The focus of these reviews is to ensure that each CSU fully contributes to Trust goals and that corporate departments support the CSUs in addressing their pressures and priorities.
1.3. Strategic Direction in 2016/17 The Trust welcomed the publication of the Department of Health’s Five Year Forward View. The Trust will work with its health and social care partners to develop the new, multi-agency Sustainability and Transformation Plans (STPs) by local geographic area, which was a main recommendation of the report. As part of this work, the Trust will seek to ensure that patients are given high quality treatment in the most appropriate setting and do not spend longer in hospital than they need to. Internally the Trust will continue to improve its financial
5
sustainability and strengthen its quality of care through the Leeds Improvement Method. These processes will be led by the Trust’s Board and Clinical Directors working within the values of the Leeds Way. 2. Activity Planning
2.1. Approach to activity planning Each year the Trust sets a contract with its local CCGs to commission the type and number of patients it will treat during the year. There is a similar contract with NHS England for the rarer, more specialist, work. It is important that both the Trust and its commissioners plan their activity accurately to ensure that there is bed and operating theatre capacity available, and to prevent either organisation suffering financially during the year.
The Trust has established a number of forums with its commissioners, under a Contract Management Board, through which capacity, demand and associated performance issues are discussed throughout the year. Commissioners have open access to the Trust’s elective (routine) referral demand monitoring system as well as a real time understanding of non-elective (urgent) demand through the System Resilience Group.
On an annual basis, the Trust uses demand and capacity modelling software, which has been endorsed by commissioners, to confirm the required level of activity for the coming year. The model is validated at speciality level through review and discussion with individual clinical teams. Each clinical team has also completed a horizon scan of anticipated changes to local and regional demand for its services including advances in medical technology and the availability of staff. This is used to inform discussions with commissioners about the likely demand for clinical services and the levels of activity that the Trust can deliver.
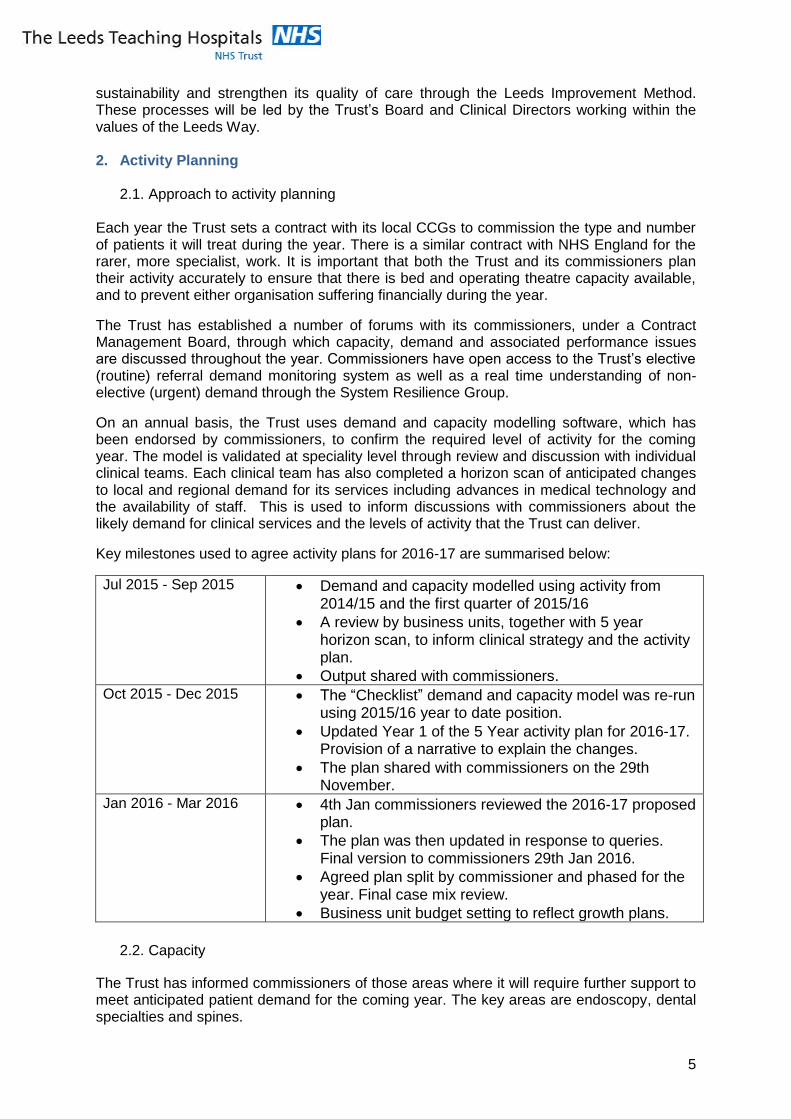
Key milestones used to agree activity plans for 2016-17 are summarised below:
Jul 2015 - Sep 2015 Demand and capacity modelled using activity from 2014/15 and the first quarter of 2015/16
A review by business units, together with 5 year horizon scan, to inform clinical strategy and the activity plan.
Output shared with commissioners. Oct 2015 - Dec 2015 The “Checklist” demand and capacity model was re-run
using 2015/16 year to date position.
Updated Year 1 of the 5 Year activity plan for 2016-17. Provision of a narrative to explain the changes.
The plan shared with commissioners on the 29th November.
Jan 2016 - Mar 2016 4th Jan commissioners reviewed the 2016-17 proposed plan.
The plan was then updated in response to queries. Final version to commissioners 29th Jan 2016.
Agreed plan split by commissioner and phased for the year. Final case mix review.
Business unit budget setting to reflect growth plans.
2.2. Capacity
The Trust has informed commissioners of those areas where it will require further support to meet anticipated patient demand for the coming year. The key areas are endoscopy, dental specialties and spines.

6
Commissioners have been told of the Trust’s intention to use the independent health sector to deliver a relatively small part of its activity plan where there are difficulties with capacity. In such cases the patients will still be NHS patients but they will be treated at a private hospital. This is predominantly a factor in endoscopy, spines and cardiac surgery.
The Trust has considered in its activity assumptions the effects of increased urgent admissions during the winter, improving length of stay, the number of delayed discharges in hospital beds, staff shortages in key areas and efficiency factors such as expected levels of theatre and clinic utilisation.
Unplanned changes in demand are monitored on an on-going basis against agreed contract levels with commissioners. Unpredicted events are tracked through weekly monitoring of activity at specialty level with additional capacity available through out of hours sessions and through the independent sector if required.
Discussions continue with the West Yorkshire Association of Acute Trusts to identify services which are in danger of becoming unsustainable and causing a significant shift in referral patterns which may result in a performance and financial impact to the Trust.
2.3. Performance Trajectories Given that many of the service change discussions have yet to be concluded, the effects have not been calculated in the current capacity and performance trajectories. Other important assumptions in the trajectories include:
Referral demand is maintained at current levels,
Maintenance of the number of Trust elective beds with no increase in delayed transfers of care,
Maintenance of bed availability through the winter of 2016/17 with no exceptional impacts from winter pressures,
Maintenance of workforce numbers at planned levels, with no exceptional variation to staff availability,
No specific capacity constraints in individual specialties preventing the delivery of additional activity,
Referring organisations achieving their agreed trajectories for referral of patients to the Trust by day 38 to prevent risk to the 62 day cancer waiting time standard.
2.4. Mandatory Standards and the NHS Constitution
Referral to Treatment Times
The Trust has consistently achieved the referral to treatment time (RTT) for the incomplete performance standard during 2015/16 (i.e. patients who are still awaiting their treatment). The Trust has put plans in place to maintain this standard during 2016/17. To sustain performance, beds and operating theatre capacity for routine activity need to be maintained throughout the year. The longest waiting patients, with the same clinical urgency, are always prioritised for treatment. The Trust has had no patients waiting over 52 weeks in 2015/16. As part of the 2016/17 planning process, all CSUs have established target patient activity levels, with any specialties who are failing to achieve their RTT standards, identifying backlog clearance levels and phasing plans to deliver sustainable performance in year. Shortfalls in capacity have been identified and notified to commissioners in relation to Endoscopy, Spines, Oral Surgery, Paediatric and Restorative Dentistry. Specialties with significant RTT risks continue to be prioritised for additional capacity where possible.
7
It is the Trusts intention to continue to achieve sustainable performance against the RTT standard in 2016/17.
Cancer Waiting Times Standards
In 2015/16, the Trust has continued to achieve all of the 31 day cancer waiting time (CWT) standards (31 days from decision to treat to first treatment). The Trust has consistently achieved the two week wait Urgent Referral to First Seen and the two week wait breast symptoms standard from quarter three and is expected to continue for quarter four. The 62 day Urgent Referral to Treatment standard has been consistently achieved from October in quarter three of 2015. Plans to sustain performance in relation to the standard are in place.
The Trust continues to work closely with all referring Trusts and commissioners to ensure referrals from other centres are timely, monitoring agreed improvement trajectories for the relevant referring organisations.
Diagnostic Standard
The Trust has achieved the Diagnostic 6 Week Wait standard since August 2015, including the delivery of three months performance in Endoscopy to support full Joint Advisory Group accreditation on gastrointestinal endoscopy. However pressures from increased demand continue in many diagnostic services particularly MRI and Endoscopy and the Trust have committed to achieve the standard if commissioner support for additional capacity can be identified.
Emergency Care Standard The standard has not been met across the Trust since October 2015 due to acute winter pressures, delayed transfers of care and increased volumes of patients attending, and being admitted, through A+E. A programme of actions with partners in the local health community has been identified during this year’s winter months. The Trust anticipates difficulties in 2016/17 due to reduced funded capacity within the community sector.
Mixed Sex accommodation breaches
There have been no mixed sex ward accommodation breaches in 2015/16 and this is expected to continue in 2016/17. This has been delivered through the robust processes already in place.
Cancelled Operations which were not rebooked within 28 Days
This standard was not achieved in 2015/16, although performance was much improved against that reported in 2014/15 despite winter pressures in quarter four. An increased focus on sustaining routine capacity through the winter period has improved performance against this standard.
No Urgent Operation Cancelled for a Second Time
No urgent operations cancelled for a second time were reported in 2015/16. The Trust expects to continue to report no breaches of this standard in 2016/17.
Supporting delivery
The Trust manages the various standards and targets mentioned above through its Integrated Accountability process. This involves the comprehensive monitoring and circulation of information with weekly performance trigger meetings. Persistent problems will

8
involve the intervention of the Trust’s Executive Directors. There is weekly Executive oversight of all non performing areas through a detailed performance scorecard. As well as the weekly meetings, every CSU will discuss performance with the Executive team when they formally meet on a twice yearly basis. For key areas of performance (Diagnostics, Cancer 62 day and RTT/ 18 weeks), detailed recovery plans are scrutinised at Trust Board level with regular Board updates presented throughout the year. This practice will continue during 2016/17. The Trust is in discussions with commissioners and the CSUs about the key performance targets for 2016/17. These are principally linked to Cancer, RTT, cancelled operations, the Emergency Care Standard and CQUINs (The Commissioning for Quality and Innovation (CQUINs) payments encouraging hospitals to adopt and share best practice). 3. Quality
3.1. Approach to quality improvement The Trust has developed a Quality Improvement Strategy, which was endorsed by the Trust Board in September 2014. This sets out a comprehensive programme of work over the next 2-3 years.
The aim of the Strategy is for the Trust to;
Be one of the safest hospitals in the UK,
Be one of the best hospitals for quality of care in the UK,
Develop integrated health and social care services with its partners in other agencies.
The Strategy was created to help the Trust realise the potential of its existing quality programmes and develop its ambition to work consistently to the highest level of quality and safety.
The Strategy set out programmes of improvement work focussing on four main areas:
Harm Free Care: Developing a world-class culture of ‘first do no harm’ to deliver the safest healthcare in the UK. This will focus on harm free care in Trust wards, for example the reduction in hospital acquired infections;
Patient Experience: Improving the experience for patients and carers whilst in the care of the Trust, evidenced by the NHS “Friends and Family” survey;
Avoidable Mortality: Reducing deaths that could be judged avoidable and improving the national mortality rate to be one of the best performers in the UK,
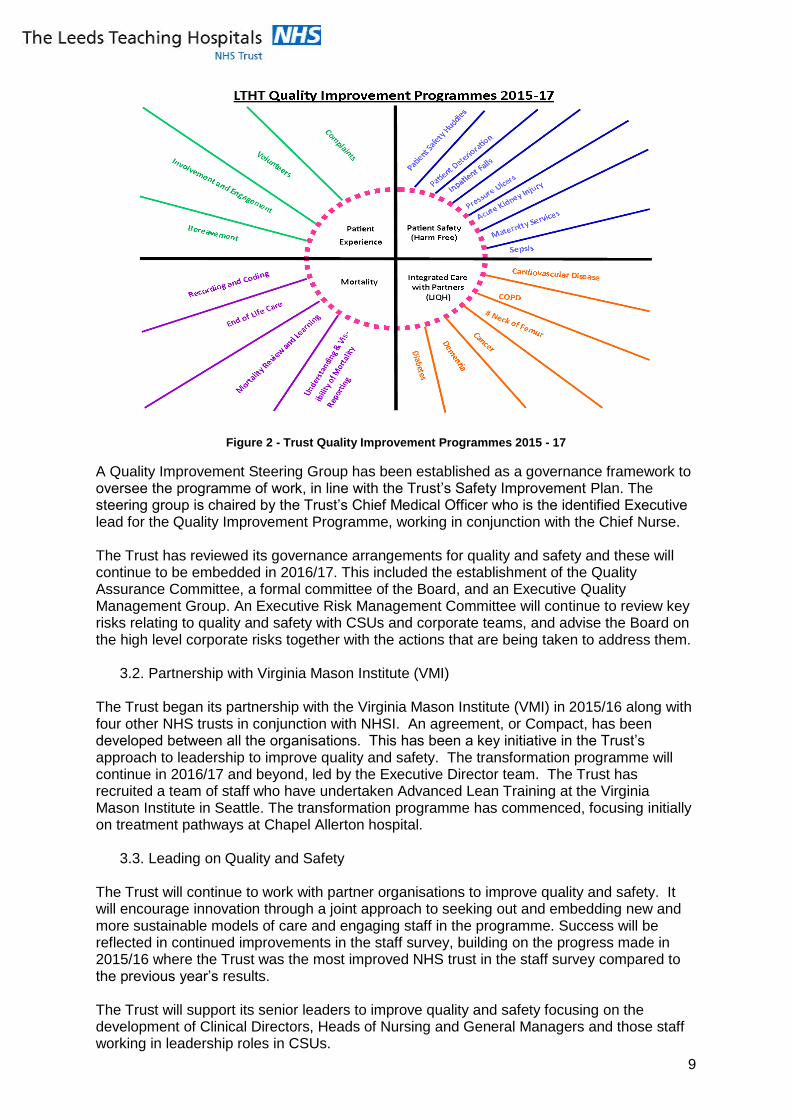
Integrated Care with Partners: Working with the Leeds Institute for Quality Healthcare to develop improvements in care for the whole of the patient pathway of care (from GP referral to post hospital care) particularly for patients with specific conditions (see figure 2).
The programme implementation is supported by a “Faculty” of doctors and nurses, focusing initially on the reduction of falls and the care of the deteriorating patient. The Strategy will be refreshed in spring 2016 and informed by a second Quality Ambitions Workshop which is currently being planned. The existing programmes of work are illustrated in the chart below.
9
Figure 2 - Trust Quality Improvement Programmes 2015 - 17
A Quality Improvement Steering Group has been established as a governance framework to oversee the programme of work, in line with the Trust’s Safety Improvement Plan. The steering group is chaired by the Trust’s Chief Medical Officer who is the identified Executive lead for the Quality Improvement Programme, working in conjunction with the Chief Nurse. The Trust has reviewed its governance arrangements for quality and safety and these will continue to be embedded in 2016/17. This included the establishment of the Quality Assurance Committee, a formal committee of the Board, and an Executive Quality Management Group. An Executive Risk Management Committee will continue to review key risks relating to quality and safety with CSUs and corporate teams, and advise the Board on the high level corporate risks together with the actions that are being taken to address them.
3.2. Partnership with Virginia Mason Institute (VMI)
The Trust began its partnership with the Virginia Mason Institute (VMI) in 2015/16 along with four other NHS trusts in conjunction with NHSI. An agreement, or Compact, has been developed between all the organisations. This has been a key initiative in the Trust’s approach to leadership to improve quality and safety. The transformation programme will continue in 2016/17 and beyond, led by the Executive Director team. The Trust has recruited a team of staff who have undertaken Advanced Lean Training at the Virginia Mason Institute in Seattle. The transformation programme has commenced, focusing initially on treatment pathways at Chapel Allerton hospital.
3.3. Leading on Quality and Safety The Trust will continue to work with partner organisations to improve quality and safety. It will encourage innovation through a joint approach to seeking out and embedding new and more sustainable models of care and engaging staff in the programme. Success will be reflected in continued improvements in the staff survey, building on the progress made in 2015/16 where the Trust was the most improved NHS trust in the staff survey compared to the previous year’s results. The Trust will support its senior leaders to improve quality and safety focusing on the development of Clinical Directors, Heads of Nursing and General Managers and those staff working in leadership roles in CSUs.
10
The Trust’s Quality Improvement Strategy will be reviewed and priorities re-defined following a Quality Improvement workshop held with senior leaders in April 2016. The Executive Directors and Non-Executive Director members of the Board will continue to undertake weekly leadership visits to clinical areas The Trust joined the Sign up to Safety Campaign in August 2014, developing its Safety Improvement Plan based on the quality priorities identified in section 3.1. This will continue to be implemented in 2016/17. The Trust was awarded £750k following submission of the Safety Improvement Plan to improve maternity care. This plan will continue to be implemented, including staff training, investment in equipment and IT infrastructure. In 2016/17 the specific priorities will be to focus on rolling out the Quality Improvement programme, embedding the approach to being open, including the Duty of Candour, and sharing learning led by the Learning Lessons group that has been established.
3.4. Care Quality Commission The Care Quality Commission (CQC) is the branch of the Department of Health whose role it
is to regulate and inspect health and social care services in England. The CQC will undertake an inspection of the Trust in May 2016, following a comprehensive inspection in March 2014. The inspection will focus on the areas that were judged to require improvement from their last visit. It will involve their five key lines of inquiry (safe, caring, effective, responsive and well-led) and their eight core service classifications (medicine, surgery, critical care, urgent care, children’s, maternity, outpatients/diagnostics and end of life care). A programme has been established to prepare for the inspection led by the Executive Director team working in conjunction with the CSUs and corporate teams. The Trust will engage with staff groups, its members and partner organisations, including the CCG and Healthwatch Leeds. Particular focus will be on safe care, responsiveness and leadership and those core services that were judged to require improvement in March 2014 (medicine, surgery, critical care and children’s services) to ensure that the CQCs Fundamental Standards are being met.
3.5. Seven Day Services The Trust is a significant provider of urgent and emergency hospital care for Leeds and Yorkshire. Following an invitation from NHS England, the Trust has agreed to become an early implementer of the Department of Health’s seven day services standards. The aim is to deliver acute hospital services that are compliant with the four priority clinical standards (Standards 2, 5, 6 and 8) by March 2017. The Trust has a Seven Day Services Committee that includes membership from the CCG. The Trust has appointed a Lead Clinician for seven day services who is supported by a Clinical Leadership Fellow and the Associate Medical Director for Workforce. Initial audit work has been carried out against the four priority standards and the Trust will evaluate the financial implications of moving to a seven day service in compliance with these areas in the next few months. CSUs have been asked to consider seven day service provision in their Clinical Governance Forums and submit Quality Improvement Plans. The approach is to use the expertise of the Trust’s clinical teams to ensure that adopting the standards will result in improved patient care.
3.6. Quality Impact Assessments
It is a key financial duty of all NHS organisations to produce on-going financial savings. Whilst organisations have delivered the required savings over recent years, it can be a difficult process and care must be taken not to harm the quality of patient care. There is therefore a process in place which matches relevant Cost Improvement Programmes (CIPs) against Quality Impact Assessments (QIAs).

11
The guidelines for undertaking QIAs were produced to reflect the national guidance. They also make explicit the roles of accountable officers on behalf of the Board, including the Chief Medical Officer and Chief Nurse/Deputy Chief Executive. The final responsibility for the assessment of CIPs rests with the Trust Board who must be assured that QIAs are undertaken to the required level of diligence. The responsibility for initiating a QIA rests with the Clinical Director, Head of Nursing and General Manager for each CSU. The responsible CSU agrees the measures they will use to judge how quality is affected by the change, based on the 3 domains of quality. Examples of these measures include:
Patient safety feedback from patients, including complaints, incident reports, including serious incidents, healthcare associated infection, information on deteriorating patients,
Patient experience feedback from patients on quality of care through local and national
surveys including friends and family test, waiting times, cancelled operations or procedures on the day of admission, breaches in same-sex accommodation, breaches in the four hour emergency care standard,
Clinical outcomes and effectiveness rate of 30 day readmissions, length of stay, mortality rates, including alerts issued.
Subsequent QIAs are reviewed and signed off by the Chief Medical Officer and Chief Nurse/Deputy Chief Executive. The QIA is monitored and reviewed by the clinical team to ensure that the risks identified relating to the CIP, or service changes, are successfully mitigated. Assurance is provided through the Trust’s governance structure regarding specific CIPs and service plans where the associated risks are considered to be significant. Oversight of the CIP programme is provided by the Trust’s Finance and Sustainability Board, chaired by the Chief Executive. The Medical and Nursing Directors from the three Leeds CCGs meet with health providers prior to commencement of the contractual year to receive outline details and assurance of providers’ cost improvement plan proposals. The purpose of the meeting is to understand the nature and content of the CIPs and be assured that they have been appropriately assessed for impact upon quality.
3.7. Risks to Quality and Safety The Trust will continue to review its principal risks relating to quality and safety. These are set out in the Corporate Risk Register and reviewed at the Executive Risk Management Committee before being reported to Trust Board. Emerging risks, including potential serious incidents and serious complaints, are also reviewed by the Chief Medical Officer and Chief Nurse at a weekly meeting. The Trust faces challenges that affect services across its hospitals consistent with partners both locally and nationally. These include pressures from emergency attendances and discharging patients to a suitable environment, where reviews across the city are being undertaken by commissioners. This programme of work will continue in 2016/17. Mitigating the risk of harm to patients has been supported by the work with NHSI, and partner

12
organisations, resulting in changing assessment and referral processes in the Trust and new ways of working with partners. A robust escalation process is in place to maintain patient safety and regular reports are provided to the Trust Board, NHSI and the System Resilience Group. The Trust has continued to face challenges relating to healthcare associated infections and, although it has met the commissioners’ threshold for clostridium difficile infection, incidences of methicillin-resistant staphylococcus aureus (MRSA) have exceeded the Trust’s plan. Root cause analysis and face to face reviews take place for all reported incidents together with ribotyping to determine incidence of transmission. Support has also been provided by NHSI with lessons learned shared through Trust-wide quality and safety briefings. In line with the national picture, there remain staffing challenges in hard to recruit areas notably Theatres, Critical Care and Acute Medicine specialities. Medical staffing pressures are also being experienced in Urgent Care and Paediatrics. This is further challenged by the national agency cap. The impact of workforce pressures has been mitigated by the Trust’s robust escalation processes involving director engagement and identifying changes to the workforce to reflect the differing needs of patients who are waiting discharge. Internally defined staffing levels are reviewed every six months for planning purposes and daily for day to day care delivery requirements. A professional support team is in place for any clinical area that demonstrates signs of deterioration. Workforce reports are provided to the Trust board at each meeting. The Trust Board agreed a significant investment plan, with a net increase of over 500 registered nurses and this will continue to be delivered in 2016/17. The Trust has experienced an increased incidence of patients with challenging behaviour, including those with mental health needs and whose behaviour may be influenced by other medical conditions. This has resulted in serious incidents which have provided opportunities for significant learning. Closer working with partner organisations, including the Leeds Partnership Foundation Trust, has taken place across key areas including referral, transfer and training. Internal changes to patient risk assessment have also taken place and have been shared as an example of good practice nationally. The Trust has been involved in a national pilot for 'specialing' for this patient group and has been successful in the recruitment of a bespoke workforce to support patient requirements. Where required, external support has been commissioned for incidents requiring investigation. All of the above areas are documented in the Trust corporate risk register.
3.6 Triangulation of indicators A summary of indicators relating to quality, workforce and finance is included in the Trust Board Quality and Performance Report (QPR). This is also reviewed at the Trust’s Finance and Performance Committee and at the monthly quality review meeting with commissioners at NHS West Leeds CCG. A combined report on incidents, complaints, claims and coroner’s inquests is reviewed at the Trust’s Quality Assurance Committee together with a summary of the agreed actions where improvements are required. The Ward Healthcheck consists of a number of indicators that have been developed to help assess quality and safety on individual wards. This provides a “Red Amber Green” rating based on a percentage compliance with 13 standards which influence patient outcomes and experience. Against this is mapped information from the Ward Workforce Healthcheck, drawing information on staffing levels, attendance, recruitment, turnover, and temporary staff utilisation, for each clinical area. In Midwifery the ratio of midwives to deliveries is measured against the national standard. The information is used to promote and target recruitment into high need areas.

13
Twice yearly a Trust wide review of the level of patient acuity (the intensity of nursing care required) and patient dependency is undertaken. This package of information then informs biannual reviews of nursing and midwifery staffing establishments.
4. Workforce Planning The Trust’s approach to workforce planning has developed in line with its approach to service planning in general, with the CSU’s leading the process. The CSU’s are asked to submit their workforce plans as an integral part of the business planning process. The overall approach to workforce planning is set out in The Trust’s People Strategy 2015-2020. The particularly pertinent chapters are highlighted below: • The Workforce Plan - operational & strategic plan, • The Best Place to Work - staff engagement plan, • The Best Place to Volunteer - volunteering plan, • Leading Excellence in Leeds - talent & leadership plan, • The Best Place to Work & Train - education, learning & development plan. The Trust Board approved The People Strategy in 2015. The workforce planning elements will be updated based on the feedback from staff within the Trust and the comments from regulators, commissioners and health economy partners on the Trust’s Operational plan. A central principle of The People Strategy is the positive impact of staff engagement. The Trust has worked hard to engage with its staff and continues to do so. The approach is called The Leeds Way and the feedback to date has been positive. However, work continues to build sustainable engagement across all staff groups especially those who are traditionally hard to reach, such as doctors in training, facilities staff and support workers. The results of the 2015 Staff Survey, where the whole workforce had the opportunity to comment, are being analysed at Trust, CSU and Departmental level. This will ensure that appropriate actions plans are developed and implemented. CSU’s submitted a workforce commentary in August 2015, highlighting their key issues and proposals. Local commissioning strategies and priorities were also taken into account through the close working between Trust and commissioning colleagues. The final plans were assessed against the Trust’s activity and financial plans and culminated in the Trust workforce plan of September 2015. By using this process the overall workforce plan was sense checked against clinical priorities, the current labour market and the overall financial position of the Trust, including the need to ensure CIPs were taken into account. Workforce priorities are managed through a Workforce Productivity Programme Board which reports to the Trust’s Financial Sustainability Board and is chaired by the Chief Executive. Through the planning process workforce risks are identified and mitigated against. A senior team of Human Resource managers review specific Trust wide workforce risks on a regular basis to identify appropriate actions. The Trust’s approach to performance management with the CSU’s also ensures workforce risks are discussed and local actions identified. There are risks around the implementation of the new contract for Doctors in Training due to the uplift in basic pay and arrangements for protection. Work is underway to model the impact of the new contract on our Doctors in Training following the publication of the contract. This work has not been completed so the risks to service delivery and the financial implications have not been completed. There is also a potential negative impact on performance targets due to the risk of continuing industrial action by our Doctors in Training. Workforce CIP’s are required to have a Quality Impact Assessment. These are assessed by an independent group within the Trust. To ensure that the assessment is comprehensive, it

14
considers the impact on the quality of services and the impact on the relevant staff. Where the staff are likely to experience a significant change, Trust managers will use the agreed change process, and engage with the staff and their representatives, to ensure effective consultation takes place. The change process is built in to the CIP timescales. Work continues to ensure that changes in workforce are well managed and do not impact on patient safety and the quality of care. All workforce developments will be linked to specific funding streams and aligned with the Five Year Forward View. The Trust aims to work with partner organisations to ensure collaborative working, whether that is within Vanguards, local clinical networks or the developing local STPs. As part of this work the Trust is working with education partners to embed new roles across its services; including Advanced Practitioners and Physician Associates. In addition the Trust is continuing to employ large numbers of apprentices across different disciplines including a joint health and social care apprenticeship. This work has been underway for some time but will help the Trust respond to the forthcoming Apprenticeship levy. The Trust provides an annual plan to the Local Education and Training Board of Health Education England. The plans set out a five year plan by staff group. The number based plans are supplemented by narratives from a wide range of senior staff within the Trust, including the Chief Executive, Chief Nurse, Chief Medical Officer and Director of Human Resources. This will be submitted in June 2016. With regard to balancing agency rules with appropriate staffing levels, a process has been put in place. The Trust’s priority will always be patient safety and, to this end, the local clinical leads have the final influence in the staffing level decisions. To monitor the use of agency staff, and to reduce the Trust’s reliance upon them, an agency working group has been established. The work to date has seen a significant reduction in the use of administrative agency staff. Work continues to reduce reliance in other key staff groups and to ensure effective control of agency deployment. It is recognised that the further agency payment reductions, in line with government policy, will be a challenge to the Trust but it will work collaboratively with agencies and other trusts to maintain the recommended rates. The Trust is developing its own bank through engaging with Doctors in Training, Nurses and Midwives and other staff groups. This work includes promotion of bank options and monitoring pay rates. The Trust has a successful medical deployment service which works with CSU’s and a neutral vendor to ensure bookings are appropriate and represents the best value available to the Trust. For nursing and midwifery, bookings are made to NHS Professionals in the first instance and then on to agencies if the shifts cannot be filled. The responsibility for the service lies with the Trust’s matrons, supported by the Corporate Nursing team. Efficient staff rostering is important and is achieved through the e-Rostering system and the team that supports it. The Trust has an audit function that reviews the roster templates, and how they are used, in order to improve staff deployment. Rostering is used across medical staff, pathology, Allied Health Professions, administration and Nursing and Midwifery staff groups. The use of e-Rostering has provided the Trust with a number of efficiency gains in recent years. Implementing these improvements takes place in conjunction with the Nursing and Midwifery Rostering sub group which includes a staff representative. 2016 will be used to consolidate the use of the system to ensure that all efficiencies are identified and achieved before further roll out. The Trust is working closely with the Lord Carter team to review its operational productivity. This will take place across the various aspects of the Trust’s activities but specifically within the deployment of its workforce. The Trust is also looking at a number of opportunities to

15
increase the use of technology to improve efficiency. This includes both corporate areas, such as in recruitment services, and operational management activities, such as the Electronic Staff Record Self Service. The Trust’s risk management process allows risks to be identified and managed, including workforce risks. The management of risks takes place at a local level within CSU’s but themes and cross cutting risks are managed at Trust level. The Trust’s workforce approach is underpinned by leadership development within the organisation, particularly clinical leadership. The education, training and development of staff is seen as an essential element in the Trust’s pursuit of financial sustainability. To support this approach, the Trust is working with the Virginal Mason Institute to develop The Leeds Improvement Method which engages clinical staff in developing improvement opportunities and implementing them in line with The Leeds Way. The Trust is an employer fully committed to developing and supporting staff, and its Apprenticeship Programmes are a working example of its commitment to this objective. The programmes currently include: Apprentices in Clinical Support Workers, Business Administration, Clinical Skills and Simulation Technicians, Medical Physics, Medical Engineering and Medical & Electrical Engineering. To prepare for the introduction of the government’s apprenticeship levy on organisations, the Trust is reviewing its existing contractual arrangements with apprenticeship providers and building flexibility into its workforce plans for apprenticeship posts to ensure maximum return on the levy payment. Work is also taking place with health and social care partners to explore opportunities for collaborative working to reap the maximum return on the levy, identifying potential for the expansion of apprenticeship activity and ensuring further information is utilised as soon as it becomes available. The Trust is fully engaged in the pan Leeds Workforce Enabling Group which reports to the Workforce Transformation Programme. The Trust’s Director of Human Resources and Organisational Development is a member of the group and three of the project leads are from the Trust and therefore regularly attend the monthly group. In addition, the workforce leads within the Trust are active participants in a specific workforce planners sub group which, in 2015, produced a first version of a city wide workforce plan. This work will influence the plans submitted to NHS Improvement and to the Local Education and Training Board in coming years. The Trust is therefore taking a lead in producing pan Leeds workforce information which cuts across the city’s three NHS Trusts, the three CCG’s and the Local Authority. The work is now looking to extend the scope of the information to include the private, voluntary and independent sectors and to provide additional information to local change projects. This includes specific projects looking at general recruitment, nursing and midwifery specifically and health and social care apprenticeships. As a major trauma centre, and with two emergency departments, the Trust is also fully engaged with the West Yorkshire Urgent Emergency Care vanguard. As part of the Leeds Academic Health Partnership, the Trust’s Director of Human Resources and Organisational Development chairs a working group which is developing a vision and scope for a Health and Social Care Academy. The Academy aims to integrate research, education and workforce development to enhance innovation and quality across the city’s health and social care providers.

16
5. Financial Planning
5.1 Introduction In 2015/16 the Trust improved its financial performance compared with the previous year despite a number of challenges and financial pressures. The Trust will now build on its changes in systems and processes resulting in improved performance and develop further to ensure in 2016/17 the Trust will move towards a surplus position.
5.2 Performance 2015/16
The Trust is forecasting the delivery of a deficit of £30.2 million in line with the revised plan submitted in September 2015 which included a £3 million stretch target for the year. 2015/16 has been challenging financially at the Trust in line with many other NHS acute providers. The forecast income and expenditure position at the end of the financial year is shown below and also includes an adjustment for a transfer of £1million capital to revenue:
Table 1: Forecast Income and Expenditure in 2015/16.
2015/16 Income and Expenditure Forecast £m
Patient Care Income 943.8
Other Operating Income 168.7
Sub Total - Income 1,112.5
Pay Costs (651.0)
Non Pay Costs (441.3)
Sub Total - Expenditure (1,092.3)
EBITDA 20.1
Non-operating Expenditure (47.5)
Retained Deficit (27.4)
Technical adjustments (2.8)
Adjusted Deficit (30.2)
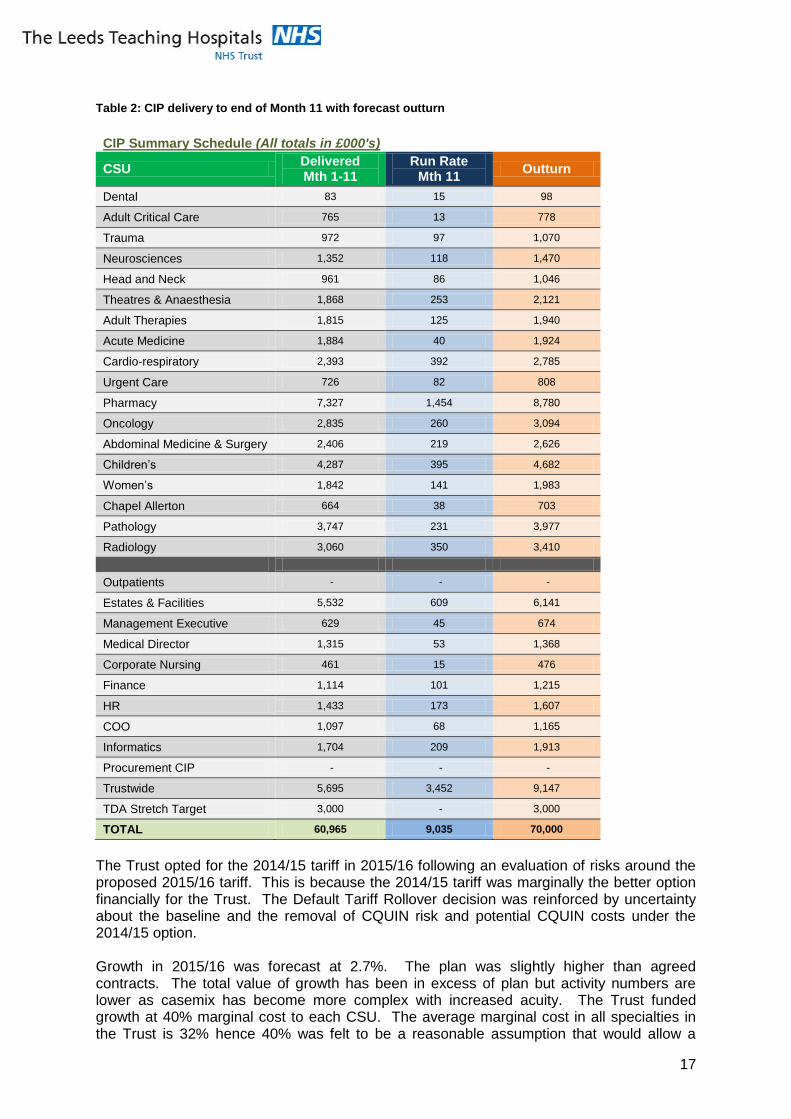
During the year the Trust has further developed its clinical strategies and plans but has faced a number of challenges. The plan assumed delivery of a £67million Cost Improvement Programme to reduce the deficit position of 2014/15 and to ensure the Trust had sufficient resources to cover cost pressures and its required safety and quality investments. The Trust reviewed nurse staffing levels and agreed a three year investment plan with 2015/16 being the second year. This meant an increase in nursing costs of £6.3 million during the year to ensure safe staffing levels. An increase of 53% in the Clinical Negligence Scheme for Trusts (CNST) premium added to cost pressures for the year. The CIP target was further increased to £70million to deliver the stretch target. The current position of CIP delivery is shown in the table below:-
17
Table 2: CIP delivery to end of Month 11 with forecast outturn
CIP Summary Schedule (All totals in £000's)
CSU Delivered Mth 1-11
Run Rate Mth 11
Outturn
Dental 83 15 98
Adult Critical Care 765 13 778
Trauma 972 97 1,070
Neurosciences 1,352 118 1,470
Head and Neck 961 86 1,046
Theatres & Anaesthesia 1,868 253 2,121
Adult Therapies 1,815 125 1,940
Acute Medicine 1,884 40 1,924
Cardio-respiratory 2,393 392 2,785
Urgent Care 726 82 808
Pharmacy 7,327 1,454 8,780
Oncology 2,835 260 3,094
Abdominal Medicine & Surgery 2,406 219 2,626
Children’s 4,287 395 4,682
Women’s 1,842 141 1,983
Chapel Allerton 664 38 703
Pathology 3,747 231 3,977
Radiology 3,060 350 3,410
Outpatients - - -
Estates & Facilities 5,532 609 6,141
Management Executive 629 45 674
Medical Director 1,315 53 1,368
Corporate Nursing 461 15 476
Finance 1,114 101 1,215
HR 1,433 173 1,607
COO 1,097 68 1,165
Informatics 1,704 209 1,913
Procurement CIP - - -
Trustwide 5,695 3,452 9,147
TDA Stretch Target 3,000 - 3,000
TOTAL 60,965 9,035 70,000
The Trust opted for the 2014/15 tariff in 2015/16 following an evaluation of risks around the proposed 2015/16 tariff. This is because the 2014/15 tariff was marginally the better option financially for the Trust. The Default Tariff Rollover decision was reinforced by uncertainty about the baseline and the removal of CQUIN risk and potential CQUIN costs under the 2014/15 option. Growth in 2015/16 was forecast at 2.7%. The plan was slightly higher than agreed contracts. The total value of growth has been in excess of plan but activity numbers are lower as casemix has become more complex with increased acuity. The Trust funded growth at 40% marginal cost to each CSU. The average marginal cost in all specialties in the Trust is 32% hence 40% was felt to be a reasonable assumption that would allow a

18
further reduction in the deficit. The Trust does have some capacity shortages in specific specialties due to estate and staff shortages which have resulted in the continued use of the independent sector to ensure access targets and high quality services can be delivered at the Trust. Shortage of capital resources resulted in the Trust being unable to make investments earlier in the year to improve patient flow and provide additional capacity. The number of delayed transfers of care at the Trust equated to 2,500 bed days per month during 2015/16 with a peak of 3,049 bed days lost in October 2015, representing 309 potential patients. The Trust has therefore over performed against plan on non-elective (emergency) patients but continued to underperform on elective (routine activity). This has been due to an increased length of stay and severity of patients’ conditions. The Trust has also had a much higher number of patients above the non-elective cap than in previous years. With funding only at 30% for these patients, many have resulted in costs being above the income received by the Trust. With the support of NHSI, a number of healthcare summits have taken place to improve integration of care services and ensure delayed transfers of care will be reduced and care provide in an appropriate setting in the future.
5.3 Plan 2016/17
The Trust has reviewed its clinical strategies and developed activity plans in conjunction with Commissioners as outlined in Section 2. Budgets have been developed following a zero based budgeting approach and in line with activity plans. Financial pressures have been reviewed by the Executive Team to ensure realism and the evaluation of risk in line with Trust strategy and objectives. The Trust is forecasting a small surplus of £1.2million in 2016/17 but this assumes the CIP is fully delivered. Commissioner agreements are in line with forecast, and cost pressures contained within contingencies held by the Trust. The forecast Income and Expenditure, Balance Sheet, Cashflow and capital plan are shown below. Table 3: Forecast Income and Expenditure in 2016/17.
2016/17 Income and Expenditure Plan £m
Patient Care Income 995.3
Other Operating Income 158.6
Sustainability and Transformation fund 22.8
Sub Total - Income 1,176.7
Pay Costs (661.5)
Non Pay Costs (461.1)
Sub Total - Expenditure (1,122.7)
EBITDA 54.0
Non-operating Expenditure (49.8)
Retained Deficit 4.2
Technical adjustments (3.0)
Adjusted Deficit 1.2
Key assumptions within the Income and Expenditure forecast for 2016/17
Pay award funded as per recent announcement of 1%.
Incremental increases have been funded in addition to the 1% pay award.
Increases in employers’ National Insurance contributions due to changes in rules around contracted out pensions, calculated at £10.7m as per Monitor Economic Assumptions document.
19
Other non-pay inflation based on combination of RPI and specific areas already notified to the Trust.
Agency will be contained within the Trust’s notified ceiling of £26.035m
Increase in CNST contributions of £2.8m.
New safety pressures funded at £14.7m plus £0.5m brought forward from 2015/16.
CIP at 4% of expenditure in 2016/17 plus non-recurrently delivered CIP from 2015/16, resulting in total CIP to £65.6m.
Marginal cost of activity growth funded at 40% of income.
£7m support funding in 2015/16 is non-recurrent.
The Trust will receive £22.8 m from the Transformation and Sustainability Fund and will deliver all requirements for the Fund payments.
Capital includes £1.5m of £5m GSC business case in 15/16, with remainder in 16/17.
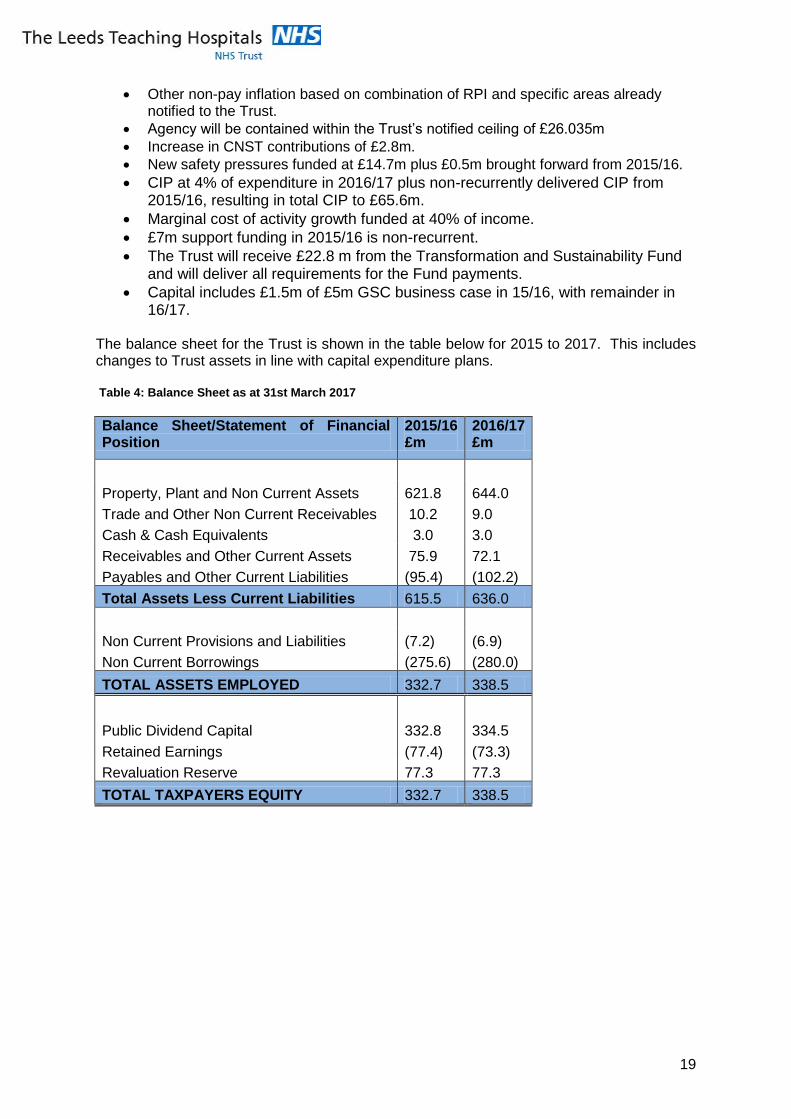
The balance sheet for the Trust is shown in the table below for 2015 to 2017. This includes changes to Trust assets in line with capital expenditure plans. Table 4: Balance Sheet as at 31st March 2017
Balance Sheet/Statement of Financial Position
2015/16 £m
2016/17 £m
Property, Plant and Non Current Assets 621.8 644.0
Trade and Other Non Current Receivables 10.2 9.0
Cash & Cash Equivalents 3.0 3.0
Receivables and Other Current Assets 75.9 72.1
Payables and Other Current Liabilities (95.4) (102.2)
Total Assets Less Current Liabilities 615.5 636.0
Non Current Provisions and Liabilities (7.2) (6.9)
Non Current Borrowings (275.6) (280.0)
TOTAL ASSETS EMPLOYED 332.7 338.5
Public Dividend Capital 332.8 334.5
Retained Earnings (77.4) (73.3)
Revaluation Reserve 77.3 77.3
TOTAL TAXPAYERS EQUITY 332.7 338.5

20
Table 5: Cashflow Statement as at 31
st March 2017
2015/16 £m
2016/17 £m
Opening Balance 3.2 3.0
Capital Expenditure (inc PFI contribution) (28.4) (49.9)
Operating surplus/(deficit) (4.5) 26.5
Depreciation 24.7 27.6
PDC Dividends. (10.3) (9.8)
Loans Received 42.7 17.1
Loans Repaid (inc interest) (22.4) (22.3)
PDC Received 0.0 1.6
Disposal Proceeds/Capital Receipts 0.1 0.0
Changes in Working Capital (2.1) 9.2
Closing Balance 3.0 3.0
Table 6: Capital plan 2016/17
Capital Expenditure Plan 2016/17 £m
Building and Engineering 29.2
Medical Equipment 14.6
Informatics 6.0
Total Expenditure 49.8
Capital Funding Plan
Depreciation 20.0
PFI 6.7
Donations 4.4
PDC 1.0
Genome 0.6
Loans - approved by TDA 8.9
Loans subject to TDA approval:
GSC Phase 2 6.0
LGI Development 1.5
Salix Energy Efficiency 0.7
Total Funding 49.8
5.4 Budget Setting

21
The 2016/17 budgets have been set in line with a number of consistent principles and use the roll forward budget as a starting point. Pay budgets have been set using payroll data of individuals in post in October 2015, and have been calculated using details of shift patterns/rotas and include enhanced pay rates as appropriate. Vacancies have been calculated at the bottom of the scale unless local intelligence suggests that recruitment takes place higher up the pay scale. Ward nursing budgets under the scope of the ‘Nursing Investment’ project have been calculated separately in collaboration with Corporate Nursing and CSU Heads of Nursing to reflect approved safe staffing levels and expected recruitment patterns. The roll forward budgets align with the 2015/16 activity plans and therefore the 2016/17 budgets have been adjusted to reflect planned changes in activity in 2016/17. Non-pay budgets have been set to reflect realistic 2016/17 expenditure levels based on planned activity, CIP plans and known price changes. More specifically, budgets for pass through blood, drugs and devices have been set to match expected pass through income.
Quality pressures have been identified but budgets will not be included until formal approval has been given. A quality review process has already assessed the validity of all quality bids and the group included the Chief Medical Officer and Chief Nurse. The recommendations have now been submitted to the Trust Board for approval.
5.5 Efficiency CIP’s have been set at realistic levels and in line with likely delivery for the year. A number of transformation programmes will be fully implemented in 2016/17 which will ensure delivery of further savings.
Table 7: 2016/17 CIP
CIP (£m) Pay Non-Pay Income TOTAL %
Identified 6.9 4.0 2.5 13.4 20%
Plans in progress 6.3 5.6 1.2 13.1 20%
Opportunity 5.5 1.1 1.3 7.9 12%
Unidentified 23.0 8.2 0.0 31.2 48%
TOTAL 41.8 18.8 4.9 65.6
100%
TOTAL % 64% 29% 8% 100%
5.6 Procurement Practices
The Trust has recently implemented Oracle R12 Financials & Procurement, as part of this role out in order to give a greater visibility and control the i-proc electronic requisition module has been implemented, this linked to greater and strict catalogue management will ensure adherence to approved products. In addition to the procurement of non-stock, the Trust continues to roll out inventory management for high value implants. As part of this implementation the Trust has recently been awarded the GS1 demonstrator site project by the Department of Health, this will allow greater visibility of use, clinical preference and costs.

22
The Trust continues to submit all its purchase data to the Business Services Authority via Scorpio and is participating in the top 100 basket of goods. In addition work has been on-going within the Carter cohort of 32 to identify best practice procurement activities and share experience and benchmarking data. 5.7 Financial Risks The key risks to achievement of a surplus in 2016/17 are shown in the table below with mitigating actions and performance monitoring arrangements.
Financial Risk Mitigations
Achievement of efficiency savings in line with target and no change in quality of service.
Quality Impact Assessment process evaluates any impact on quality of service for all significant CIP schemes. Senior Finance business partners continue to support CSUs to identify further areas for efficiency improvement by analysis of costing data, benchmarking and further data analysis through continued updates to knowing the business exercise.
Delivery of elective activity plan and ensuring the Trust is able to manage demand for non-elective activity within capacity.
The Trust has completed detail capacity plans to ensure demand and capacity are in place and operating as effectively as possible. The Leeds Improvement method will ensure efficient use of resources. The Trust has identified additional resource requirements in the private sector. A detail business case planning process is now in place for any further service developments that ensures all resource implications are identified for service developments.
Lack of investment in previous years in IT, building and engineering and medical equipment infrastructure may result in lack of resilience in current services and limited ability to transform, modernise and change care pathways.
The Trust has commenced a procurement process to appoint an IT strategic partner. This may include investment in IT infrastructure and clinical systems. The Trust has commenced the completion of a SOC for the re-development of the LGI and St James site. This will explore options and alternative funding methods. A review of medical equipment has been undertaken.
Assumptions in income assume a contract settlement with Commissioners which is currently £23 million above current contract offers.
The Trust has submitted an application for formal mediation to NHS Improvement.
The Trust is currently experiencing increase in demand in some specialties due to service reductions or changes in other Trusts and it is assumed there are no further changes in local service profile.
This is being regularly reviewed by the Assistant Director of Operations with a view to monitoring demand and taking appropriate action.
5.8 Conclusion.

23
The Trust Board recognises the Trust can deliver a surplus in 2016/17 if CIP’s are fully delivered in line with plans, and commissioner contracts are also in line with plan. Further reviews are taking place with the Executive team and CSU’s to ensure processes are in place to identify and implement CIP’s in line with agreed targets. The Trust has received the Carter Report which indicates scope for cost reduction but its overall conclusion suggests that the Trust’s costs are below national averages. Utilising the Leeds improvement method (based on work with the VMI), we will be working to reduce “unnecessary waste”. The Trust is involved in a number of benchmarking exercises which will identify further areas in which cost reductions can be achieved during this year. Patient level information is being developed and recently action plans on the top ten loss making specialties was reviewed by the Trust Board with actions to review. Working in the Leeds system to improve flow has to be the cornerstone of a successful transformation. The Trust will require the support from the Transformation and Sustainability Fund to deliver a surplus of £1.2 million and will make progress in delivering access targets during the year.
6. Capital Planning The Trust will always provide safe accommodation for its patients and use medical equipment that is fit for purpose. How this is achieved will evolve over time, reflecting the changes to the Trust’s models of care and its discussions with patients and partners in other agencies. This will be influenced by the development of better integrated care within Leeds, the provision of specialist care to the wider population in Yorkshire and support to clinical research programmes with the city’s universities and commercial partners. Currently the Trust has a large capital spend backlog of £87m in building and engineering, to bring the existing buildings and plant up to date, and £90m in medical and surgical equipment. There is also a significant backlog in informatics. Capital will therefore have to be allocated very carefully in 2016/17 to ensure that the very limited resource is directed at protecting patient safety, modernising capacity where possible, and increasing the productivity of Trust systems and processes. There are estate, equipment and infrastructure strategies in place to deliver the Trust’s longer term ambitions and recognise the backlog difficulties. Each of the Trust’s capital programmes has an agreed process for deciding spend which starts with the CSUs and ends with the Trust Board, based on a system of prioritisation against agreed criteria. The Estates Strategy highlights the age and suitability of some of the Trust’s building stock. Site development plans have been completed for all hospital sites and a plan is in place to dispose of 70,000sqm of the Trust’s 526,000sqm estate with some of this land available for housing. A group is looking again at all Trust property to identify any areas that can be better used and the feasibility of any further areas that could be disposed of. A major strategic initiative, which will be focussed on in 2016/17, will be working with partners on the development of the LGI site which still has many Victorian buildings. In terms of infrastructure, the Trust’s immediate focus is on maintaining the estate and modernising it where funding is available. Current priorities include upgrading the LGI generating complex to provide sufficient electrical infrastructure for the site, undertaking further work on the electrical infrastructure at the St James’s site and replacing air handling units and uninterrupted power supplies at both of the main sites. More visible schemes include the reopening of a redundant theatre and the development of an ambulatory unit for gynaecology. There is also a focus on quality environmental improvements such as facilities for adults with complex disabilities and refurbishments of areas of wards which are not up to modern acceptable standards. The Pathology managed equipment service is now in place at the LGI site and this will be expanded to the St James’s site in 2016/17.

24
Developing day case and same day admission facilities is a priority on all sites and better theatre and ICU facilities are required as the acuity of patients increase. The Trust is also bidding in the next round for Clinical Research Facility (CRF) designation with a focus on Oncology. There is a proposal to create a CRF facility within the Bexley Wing and the centralisation of the Trust’s Research & Innovation HQ using a vacant grade 2 listed building in the middle of the St James’s site.
7. Link to the emerging Sustainability and Transformation Plans The timeline for agreeing STPs has been significantly extended beyond the Operational Plan submission date. This section therefore uses the information that is currently available and details the process, high level agreements and areas of focus which have been suggested so far. Further detail will be available in the final STP submission in June. The Trust supports the introduction of STPs across the NHS. As highlighted in the strategic framework, the Trust sees partnership working as key to its success. It is increasingly apparent to all health economy members that many major issues affecting patients within the NHS cannot be solved by one organisation alone. Prior to the release of the 16/17 planning guidance the Leeds health economy had already been addressing a number of these issues. The Leeds Transformation Board overlooks a number of executive groups where discussion and development on joint work takes place. It is felt that the addition of STPs will further support these processes and provide a vehicle to implement some of the major changes that these groups have been discussing. There are however issues surrounding healthcare in Leeds which can only be resolved by regional action, therefore it has been decided that the Trust will complete a STP with other members of the West Yorkshire health economy. Within this plan there will also be a significant section devoted to addressing any concerns contained within the Leeds footprint. It is felt that this geography will provide the greatest opportunity for transformational change. Rob Webster, CEO for South West Yorkshire Partnership NHS Foundation Trust has been named as the single responsible officer for the West Yorkshire STP. In addition, to ensure that the system achieves the desired change, a sub group of the Leeds Executive Committee has been set up to lead on progressing the work on the Leeds section of the STP. This is made up of the following individuals:
Tom Riordan - Chief Executive, Leeds City Council
Phil Corrigan - Chief Executive, Leeds West CCG
Julian Hartley - Chief Executive, Leeds Teaching Hospitals NHS Trust Beneath this group Leeds South and East CCG have agreed to coordinate this work. Their Chief Operating Officer will lead this process and Chair a larger group made up of representatives from each organisation who will be tasked with representing their organisation’s views. This structure has allowed Leeds to develop an initial work plan which will focus on the following:
The project lead is to meet with strategy leads across the locale to develop key actions to understand what work needs to take place,
The production of high level governance and a timeline,
Development of a list of questions to return to the Executive Team which require broad strategic agreement, such as:
What are the key transformations which we want to take place? How do the finances work both in terms of process and also the overall
financial framework?
25
At present the group has only set out initial ideas for transformation and these will be further agreed and developed via the programme described above. This work will be closely linked with the Five Fear Forward View priorities of improving access to out of hours care, reducing excess deaths and improving access to primary care at weekends and evenings whilst also providing solutions to local priorities which affect the Leeds healthcare system. The present proposed areas of focus are listed below although these may change as work progresses.
Providing appropriate preventative services for specific high-risk groups within the Leeds population regarding: smoking, cardio vascular disease, diabetes, serious mental health conditions and learning difficulties,
Meeting the urgent and emergency care standard, including improving internal processes, ambulance response times, decision support capability and reducing delayed transfers of care,
Targeted screening for cancer,
Developing Health Coaching, self care and an “asset based” community care model,
Making appropriate assessments at the right time and in the right place (at acute front-of-house and at discharge, and reducing admission rates,
Optimising the use of technology e.g. telehealth,
Developing the Leeds Academic Health Partnership (LAHP) to support training, change management and workforce planning.
The Trust will support the development of STPs, including the emphasis on health education and whole system solutions as set out in the Five Year Forward View. The Trust will actively engage in plans to provide sustainable specialist care for Yorkshire and in the development of new models of care for the people of Leeds, ensuring that patients do not spend time in hospital if they can be better treated elsewhere. The Trust will also wish to discuss the use of its workforce and facilities to ensure that there is a whole system approach to care being provided sustainably, seven days a week, in an environment that is fit for purpose. In line with the Five Year Forward View, the Trust will work to develop STPs to enhance healthcare quality and strengthen financial sustainability within the region.