10 year review of paediatric tracheostomies the leeds teaching hospitals nhs trust
TRANSCRIPT
10 Year Review of Paediatric Tracheostomies
The Leeds Teaching HospitalsNHS Trust
Changing times
• Changing indications for tracheostomy
• Fewer short-term tracheostomies
• Most for chronic problems leading to tracheostomy use for months or years

Parental competency in tracheostomy management
• 2 carers trained• Gain competencies in:– Suctioning tube– Changing tapes– Changing tubes– Coping with emergencies• Tube obstruction• Tube dislodgement
– Basic paediatric life support
Study Objectives
• To review indications and length of hospital stay in children undergoing tracheostomy
• To highlight reasons for prolonged hospitalisation once medically fit
• Identify impediments to timely discharge

Methods
• 10 year retrospective study 2000 – 2010
• All children undergoing tracheostomy in LTH– Mr Knight, Mr Crabbe
• Identified using theatre database
• Case notes reviewed

Data collected
• Demographics• Indication for tracheostomy• Length of hospital stay• Reasons for extended stay • Destination on discharge• Mortality
Results
• 109 children identified
• 101 notes reviewed – Age range 0-15 years
• ENT - Mr Knight – 47
• Paed Surgery - Mr Crabbe – 45
• Other - 9
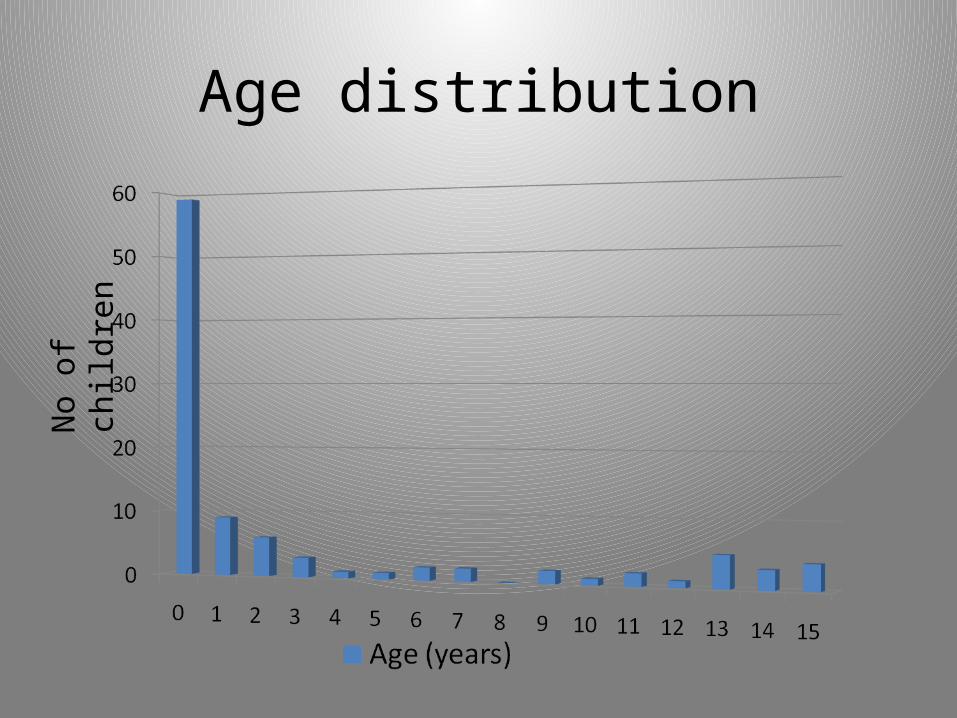
Age distributionN
o o
f ch
ildre
n
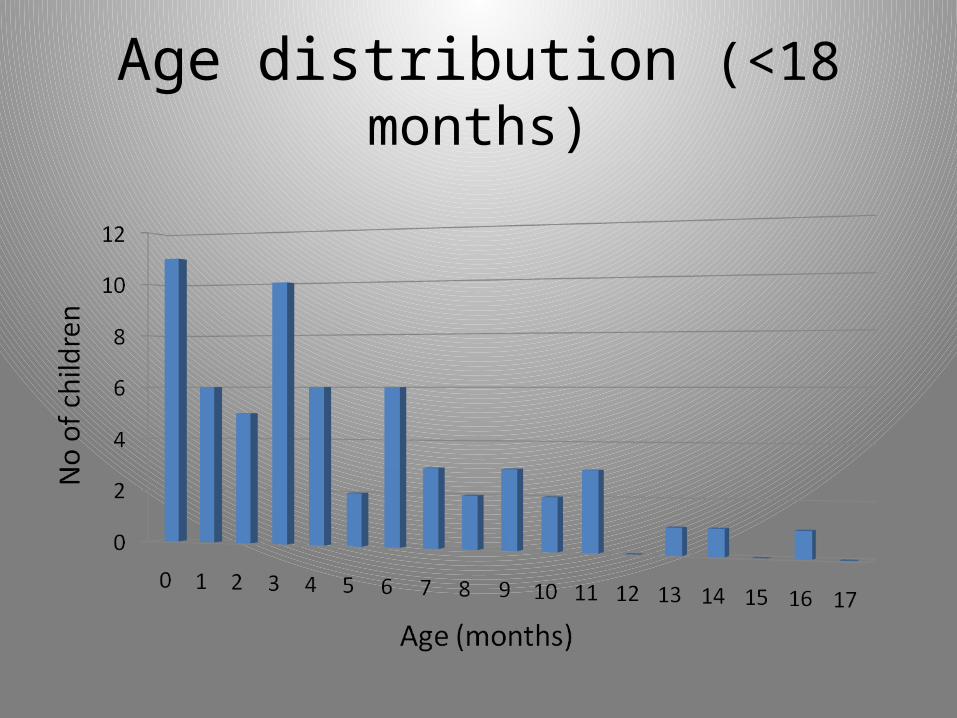
Age distribution (<18 months)
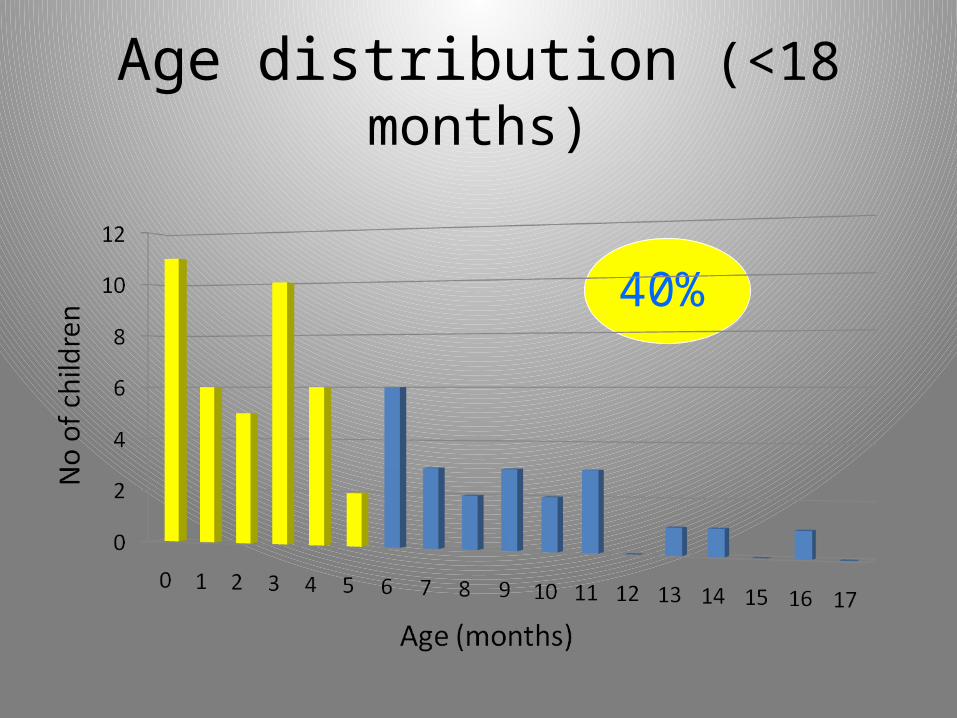
Age distribution (<18 months)
40%

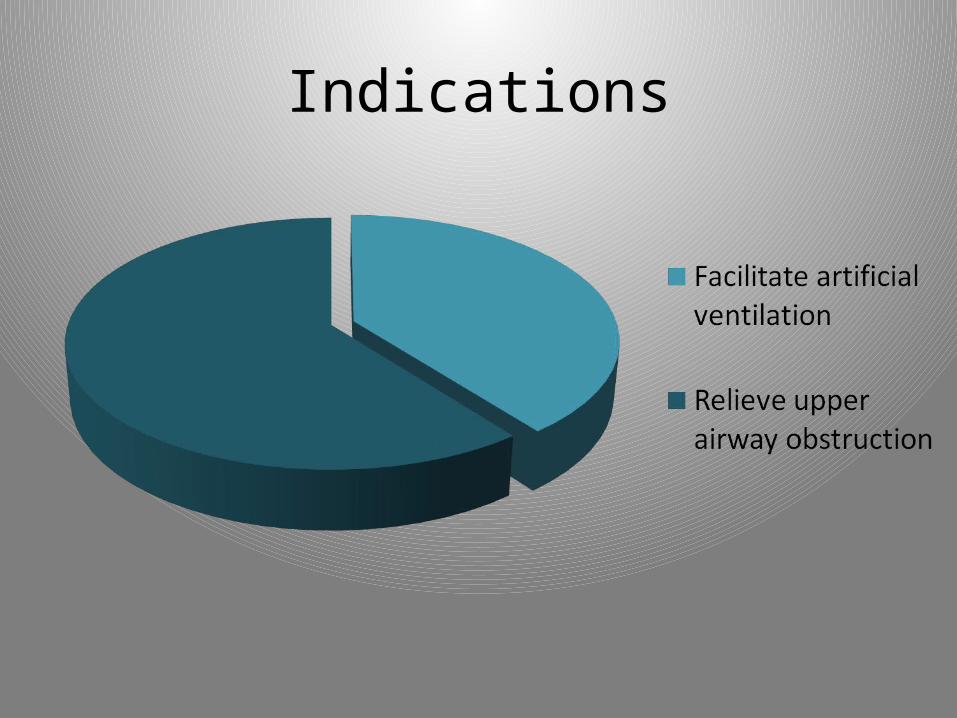
Indications
To facilitate artificial ventilation
To relieve upper airway obstruction
Indications
To facilitate artificial ventilation
• Weaning from ventilator• Needs prolonged ventilation• Needs regular pulmonary
toilet
To relieve upper airway obstruction
• Bypass blockage or narrowing in upper airway
Indications
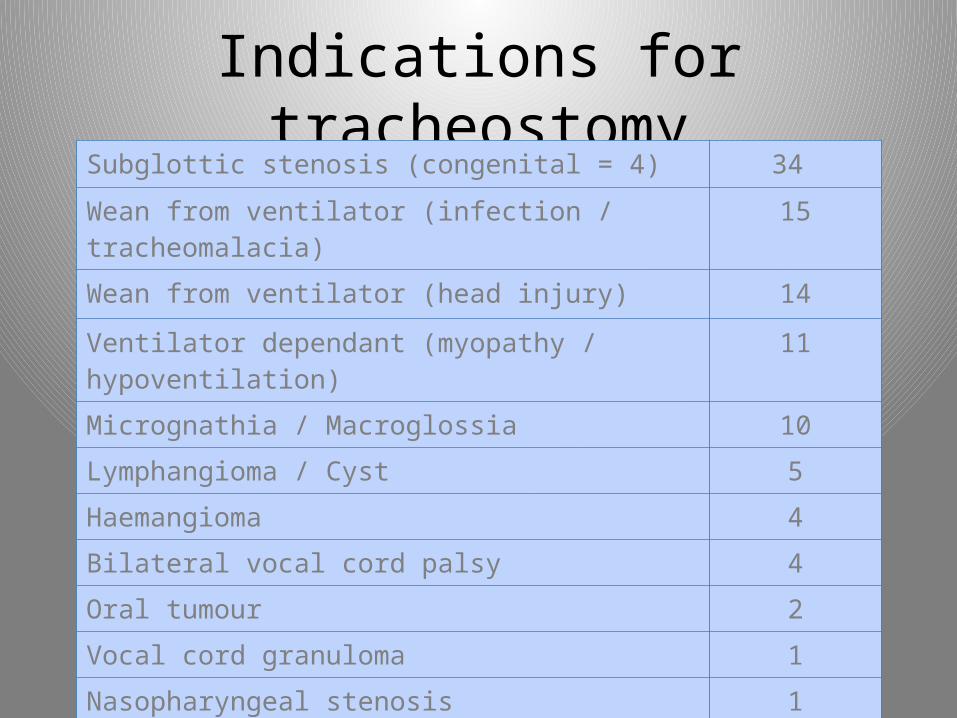
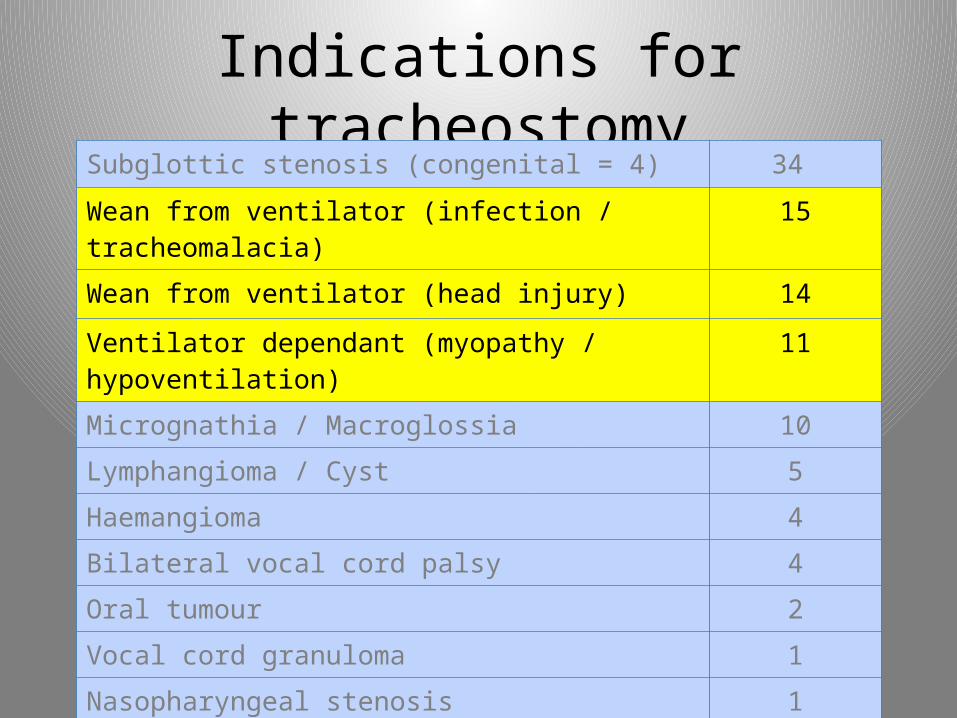
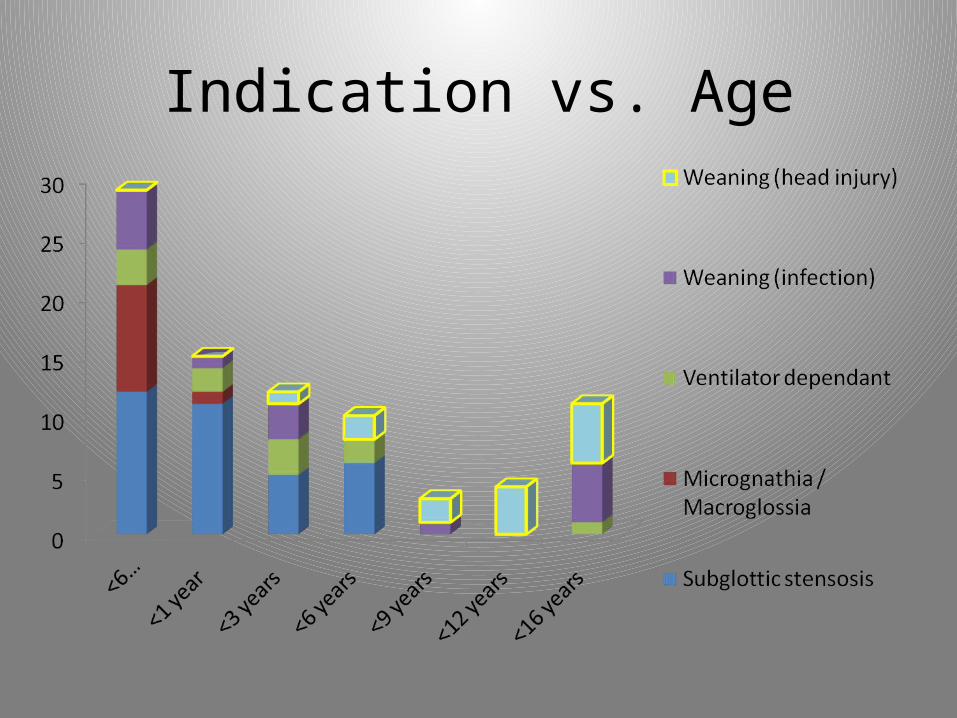
Indications for tracheostomySubglottic stenosis (congenital = 4) 34
Wean from ventilator (infection / tracheomalacia) 15
Wean from ventilator (head injury) 14
Ventilator dependant (myopathy / hypoventilation) 11
Micrognathia / Macroglossia 10
Lymphangioma / Cyst 5
Haemangioma 4
Bilateral vocal cord palsy 4
Oral tumour 2
Vocal cord granuloma 1
Nasopharyngeal stenosis 1
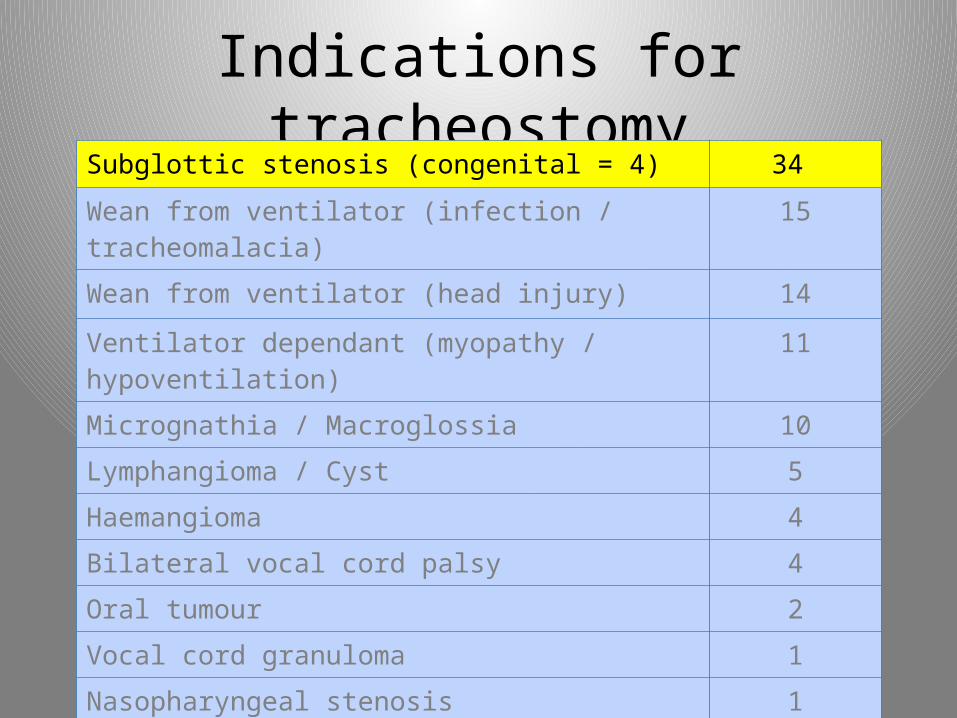
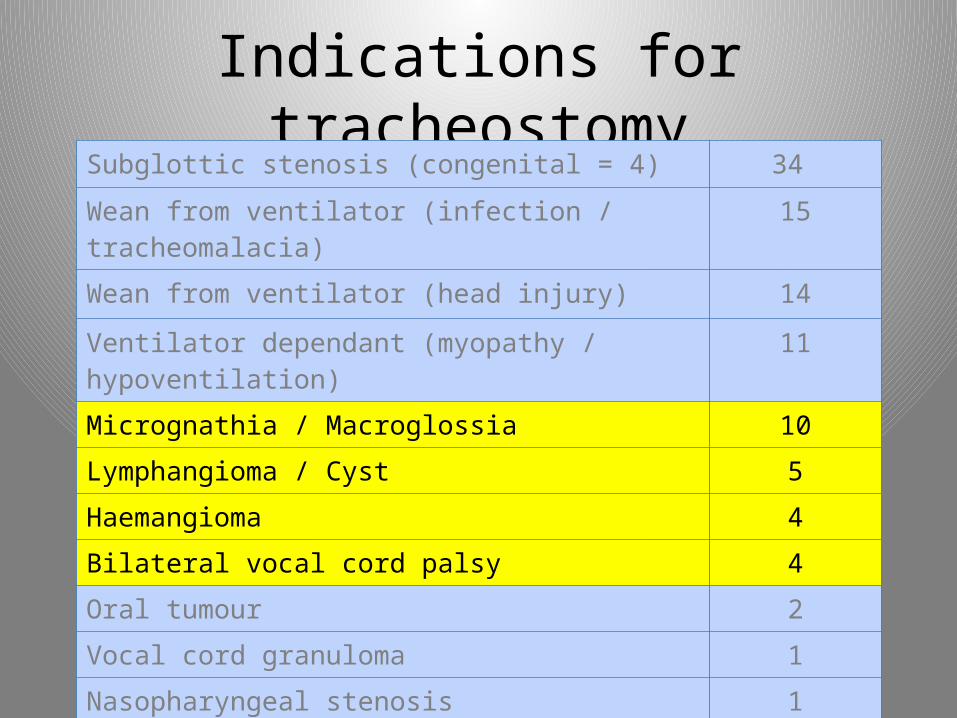
Indications for tracheostomySubglottic stenosis (congenital = 4) 34
Wean from ventilator (infection / tracheomalacia) 15
Wean from ventilator (head injury) 14
Ventilator dependant (myopathy / hypoventilation) 11
Micrognathia / Macroglossia 10
Lymphangioma / Cyst 5
Haemangioma 4
Bilateral vocal cord palsy 4
Oral tumour 2
Vocal cord granuloma 1
Nasopharyngeal stenosis 1
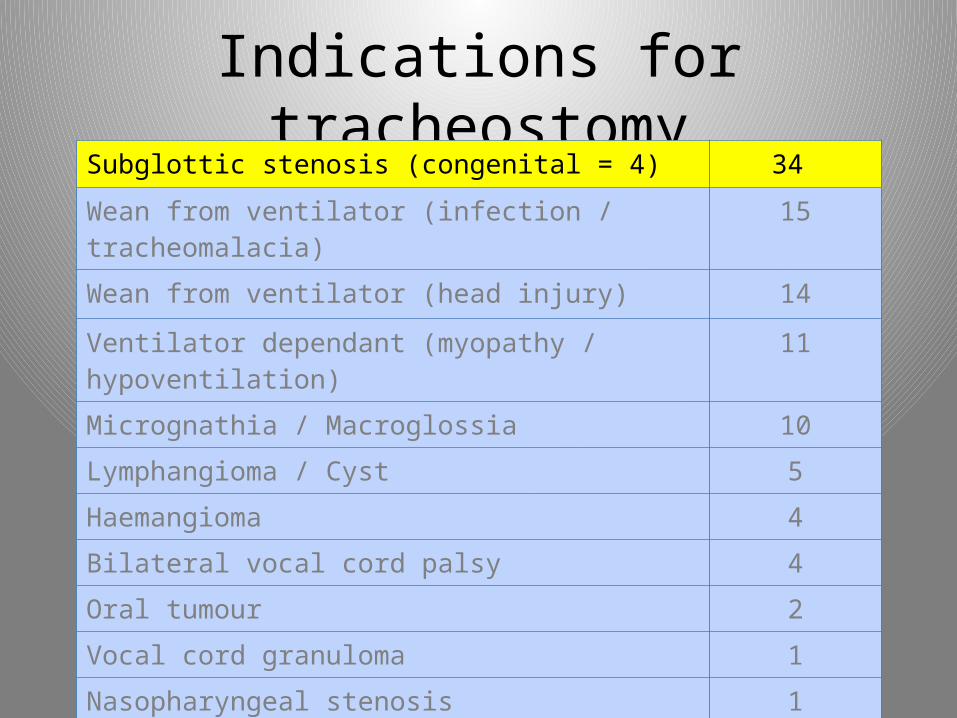
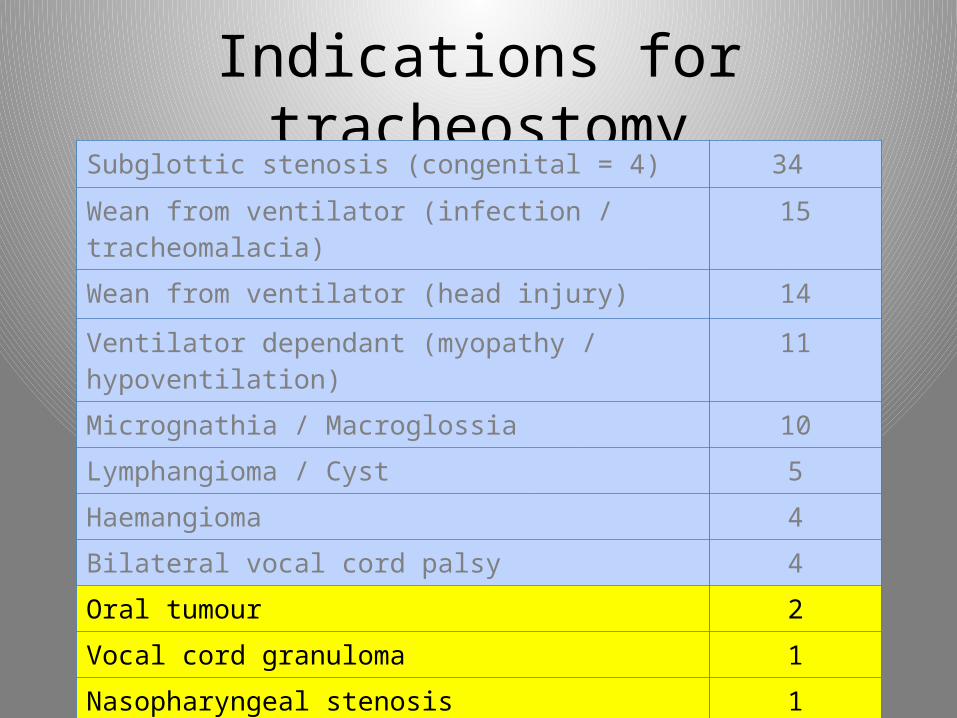
Indications for tracheostomySubglottic stenosis (congenital = 4) 34
Wean from ventilator (infection / tracheomalacia) 15
Wean from ventilator (head injury) 14
Ventilator dependant (myopathy / hypoventilation) 11
Micrognathia / Macroglossia 10
Lymphangioma / Cyst 5
Haemangioma 4
Bilateral vocal cord palsy 4
Oral tumour 2
Vocal cord granuloma 1
Nasopharyngeal stenosis 1
Indications for tracheostomySubglottic stenosis (congenital = 4) 34
Wean from ventilator (infection / tracheomalacia) 15
Wean from ventilator (head injury) 14
Ventilator dependant (myopathy / hypoventilation) 11
Micrognathia / Macroglossia 10
Lymphangioma / Cyst 5
Haemangioma 4
Bilateral vocal cord palsy 4
Oral tumour 2
Vocal cord granuloma 1
Nasopharyngeal stenosis 1
Indications for tracheostomySubglottic stenosis (congenital = 4) 34
Wean from ventilator (infection / tracheomalacia) 15
Wean from ventilator (head injury) 14
Ventilator dependant (myopathy / hypoventilation) 11
Micrognathia / Macroglossia 10
Lymphangioma / Cyst 5
Haemangioma 4
Bilateral vocal cord palsy 4
Oral tumour 2
Vocal cord granuloma 1
Nasopharyngeal stenosis 1

Indications for tracheostomySubglottic stenosis (congenital = 4) 34
Wean from ventilator (infection / tracheomalacia) 15
Wean from ventilator (head injury) 14
Ventilator dependant (myopathy / hypoventilation) 11
Micrognathia / Macroglossia 10
Lymphangioma / Cyst 5
Haemangioma 4
Bilateral vocal cord palsy 4
Oral tumour 2
Vocal cord granuloma 1
Nasopharyngeal stenosis 1
Indications for tracheostomySubglottic stenosis (congenital = 4) 34
Wean from ventilator (infection / tracheomalacia) 15
Wean from ventilator (head injury) 14
Ventilator dependant (myopathy / hypoventilation) 11
Micrognathia / Macroglossia 10
Lymphangioma / Cyst 5
Haemangioma 4
Bilateral vocal cord palsy 4
Oral tumour 2
Vocal cord granuloma 1
Nasopharyngeal stenosis 1
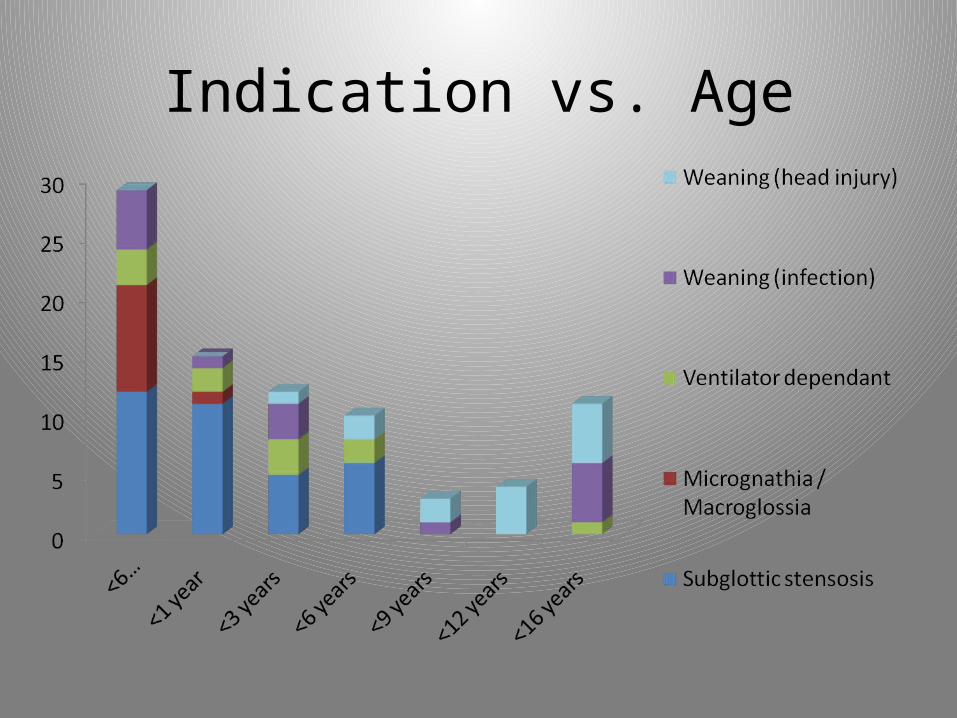
Indication vs. Age

Indication vs. Age
Indication vs. Age
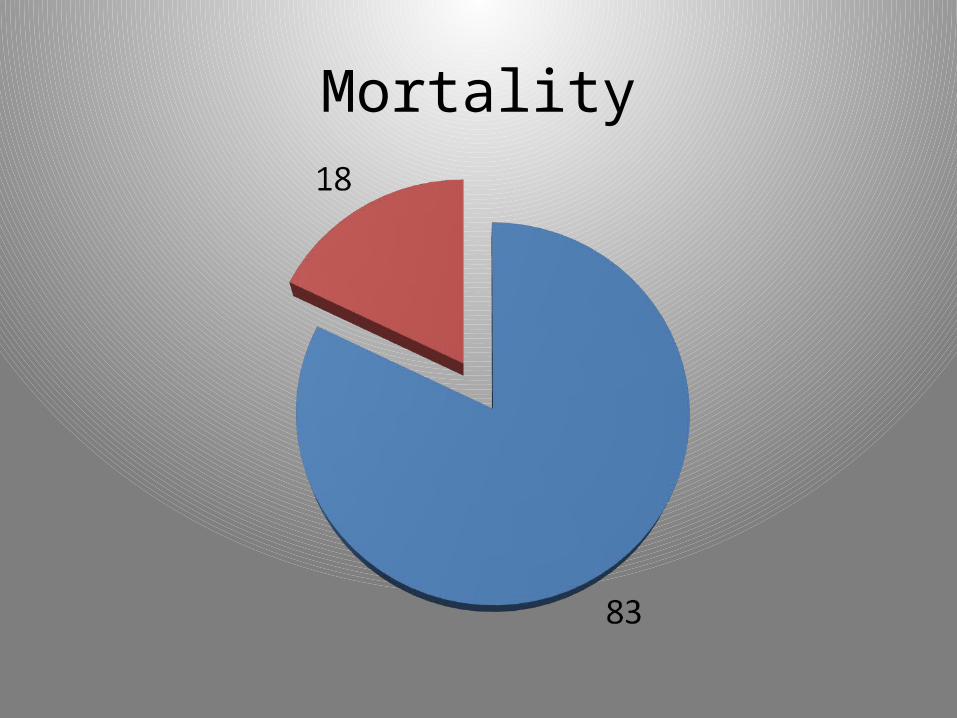
Mortality
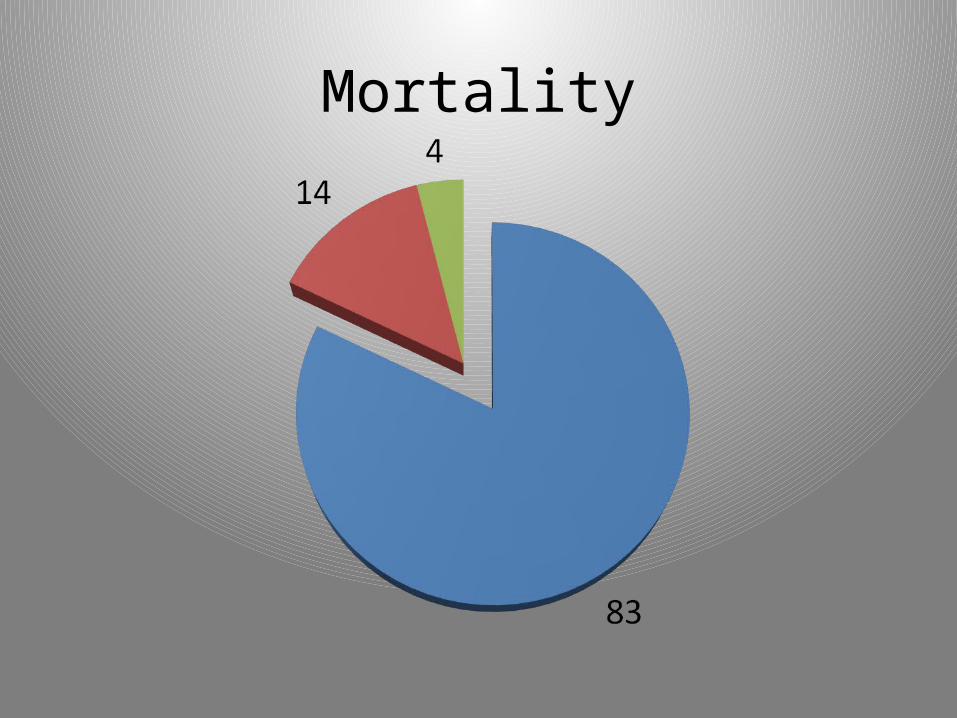
Mortality
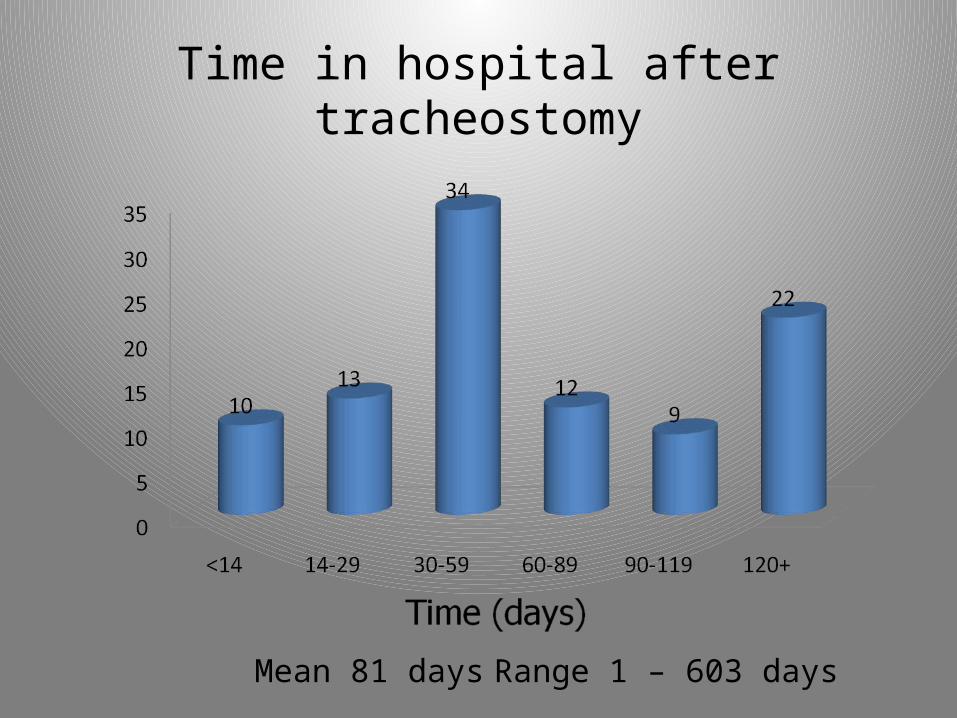
Time in hospital after tracheostomy
Mean 81 days Range 1 – 603 days
Time in hospital after “medically fit”
• Mean: 19 days
• Range: 0 – 265 days
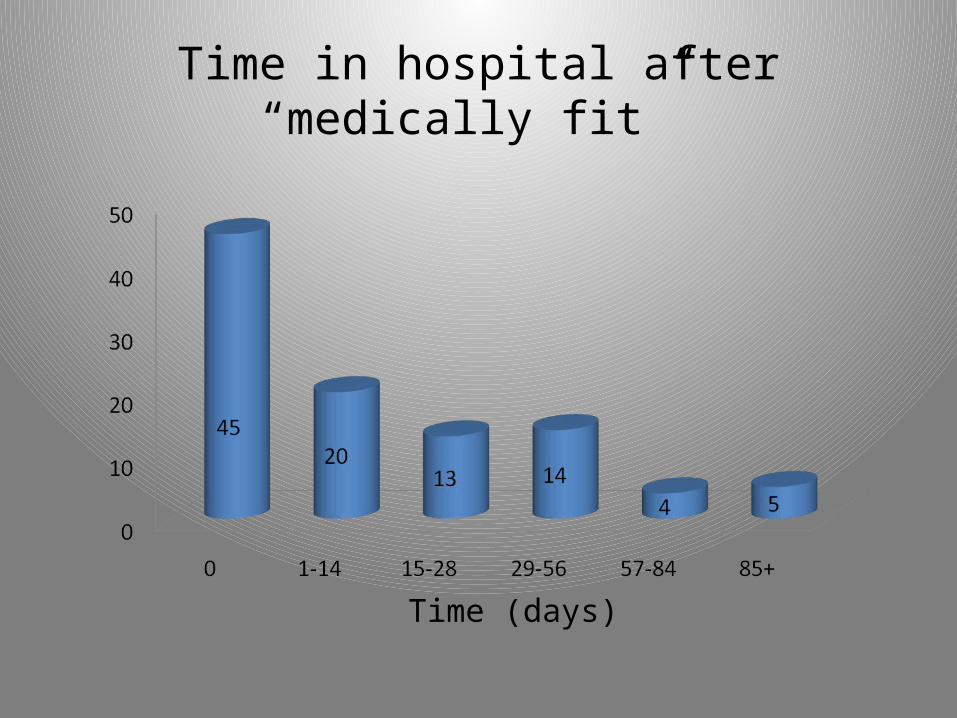
Time in hospital after “medically fit”
Time (days)
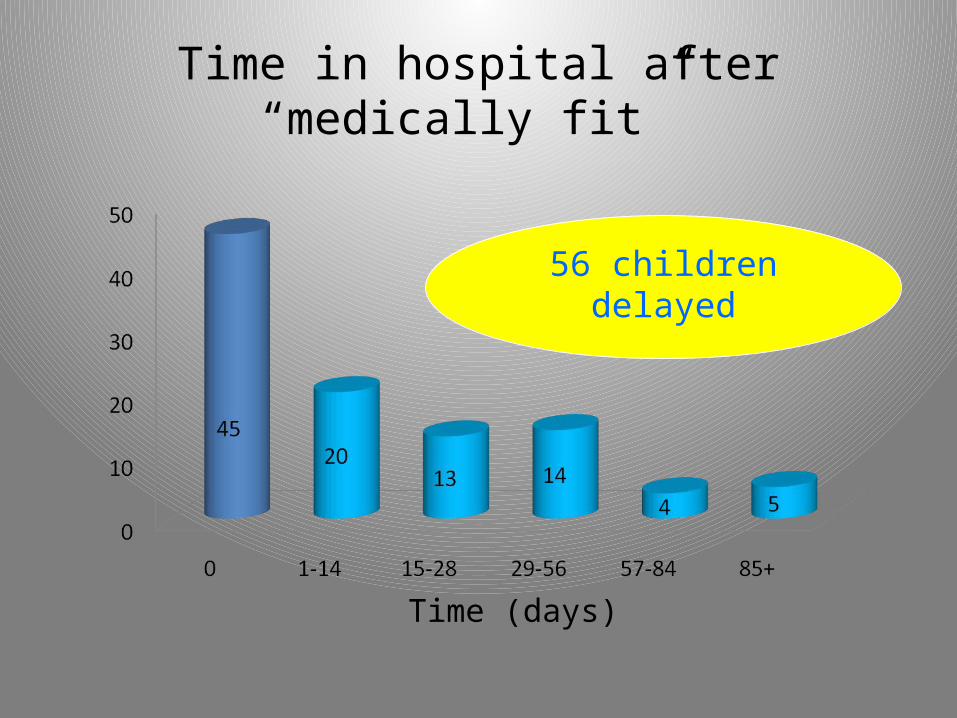
Time in hospital after “medically fit”
Time (days)
56 children delayed

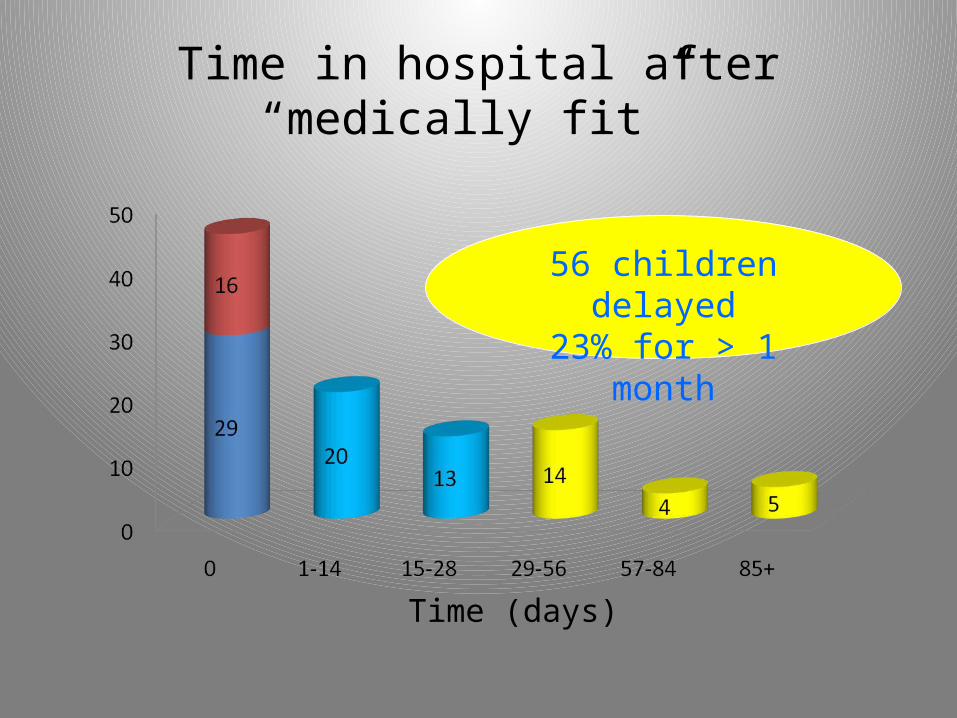
Time in hospital after “medically fit”
Time (days)
56 children delayed23% for > 1 month
Time in hospital after “medically fit”
Time (days)
56 children delayed23% for > 1 month
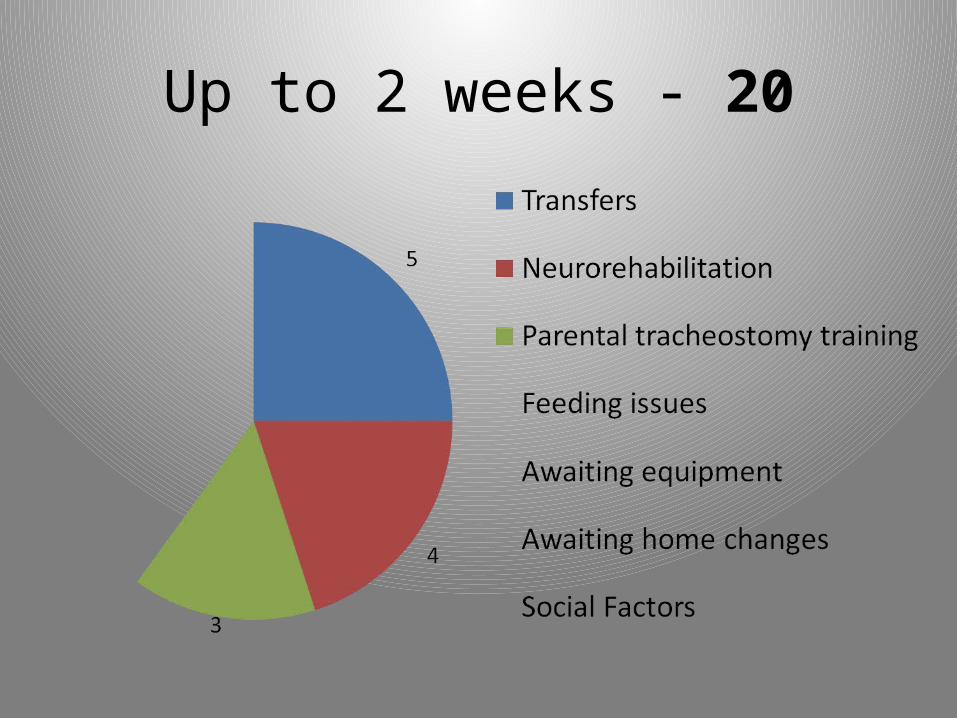
• Less than 2 weeks• 2 to 4 weeks• 4 to 8 weeks• 8 to 12 weeks• More than 12 weeks
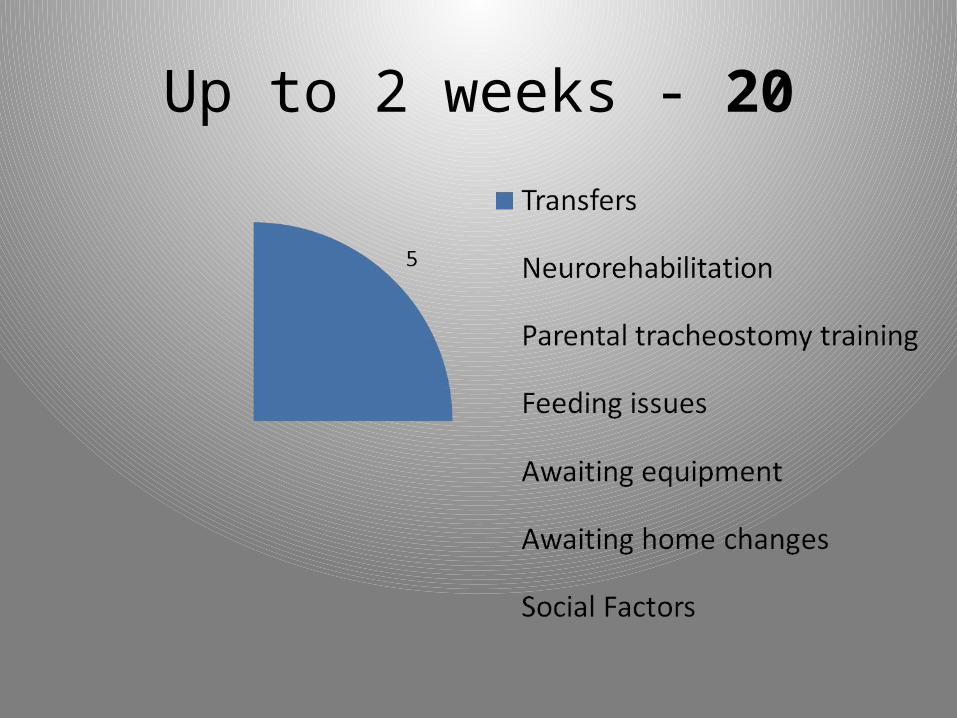
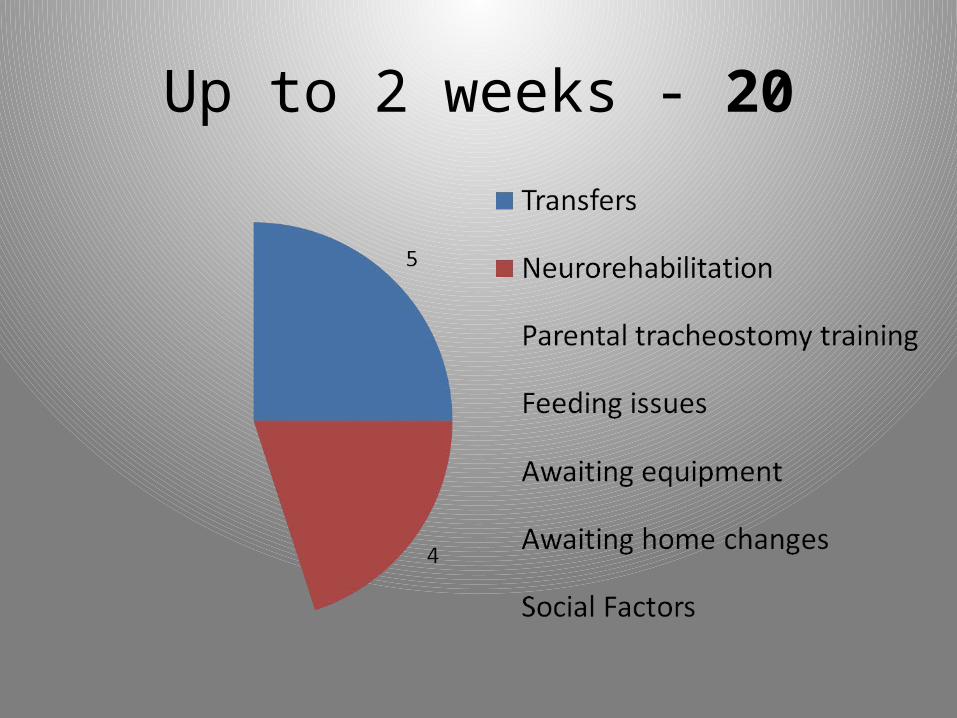
Up to 2 weeks - 20
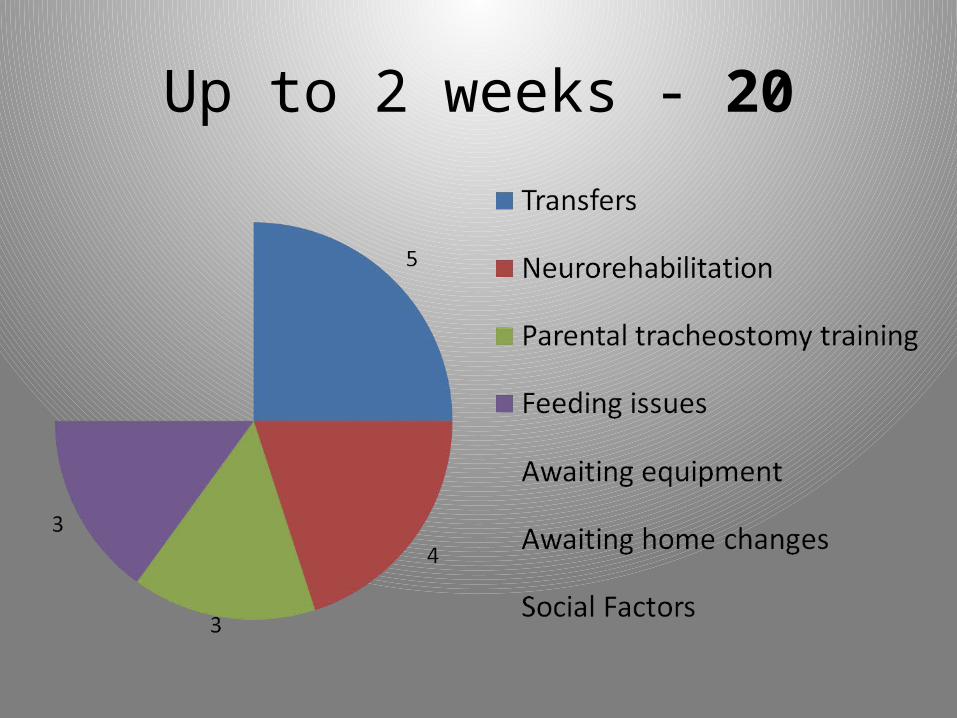
Up to 2 weeks - 20
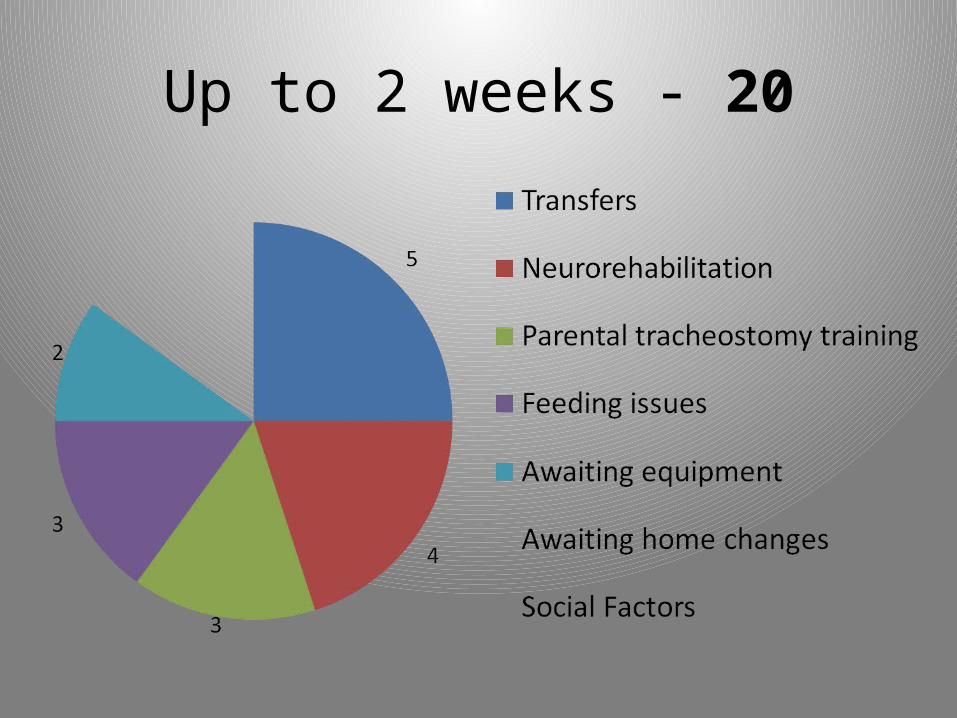
Up to 2 weeks - 20
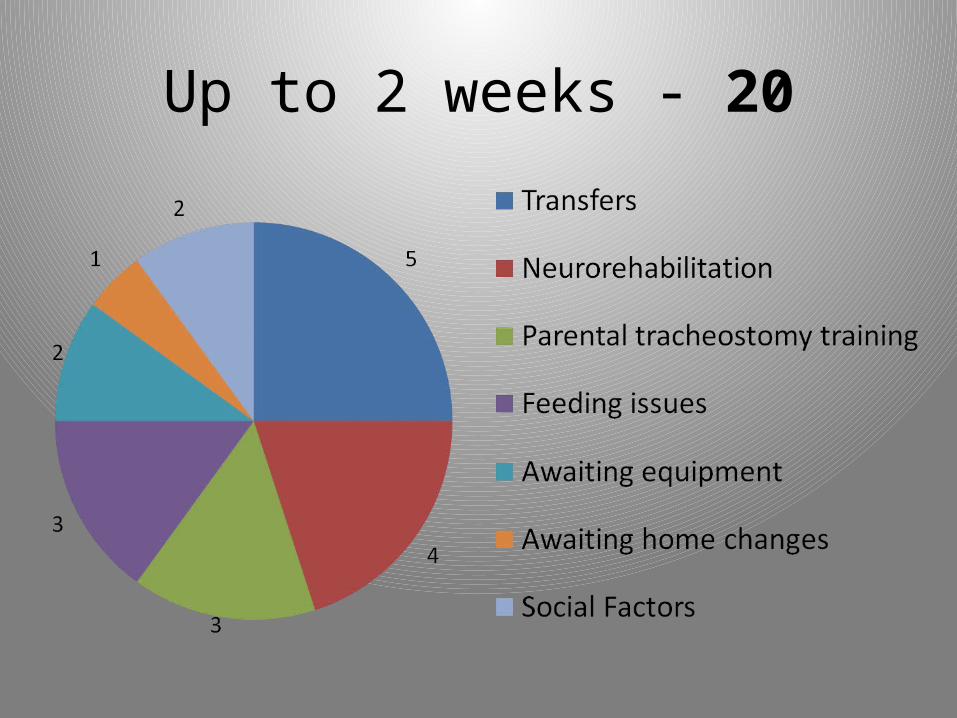
Up to 2 weeks - 20
Up to 2 weeks - 20
Up to 2 weeks - 20

Up to 2 weeks - 20
Up to 2 weeks - 20
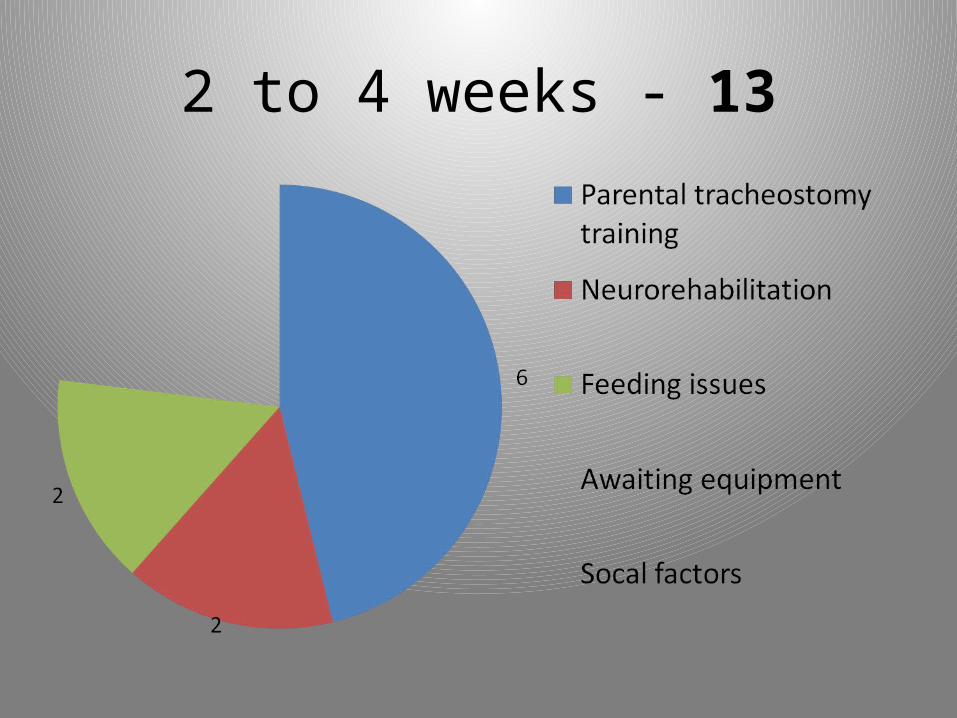
2 to 4 weeks - 13

2 to 4 weeks - 13

2 to 4 weeks - 13
2 to 4 weeks - 13

2 to 4 weeks - 13

2 to 4 weeks - 13
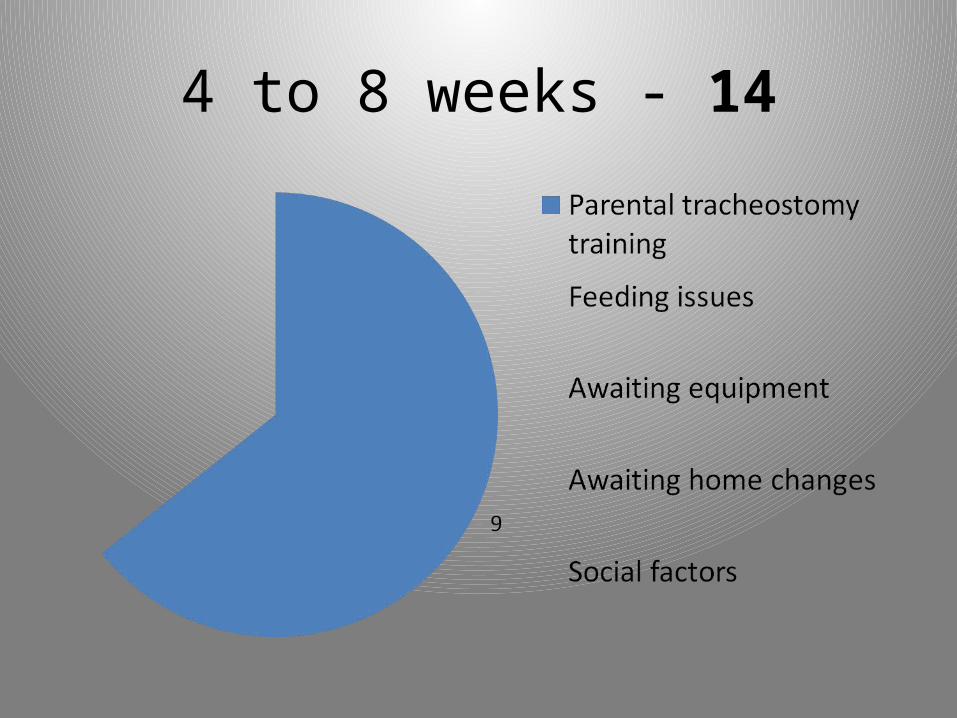
4 to 8 weeks - 14
4 to 8 weeks - 14
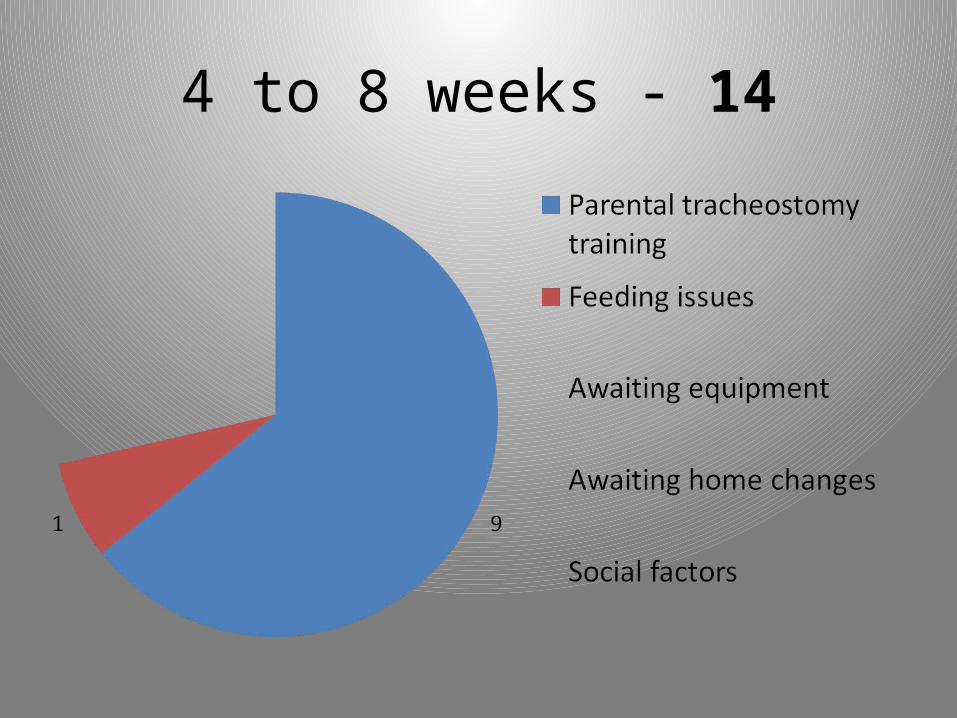
4 to 8 weeks - 14

4 to 8 weeks - 14
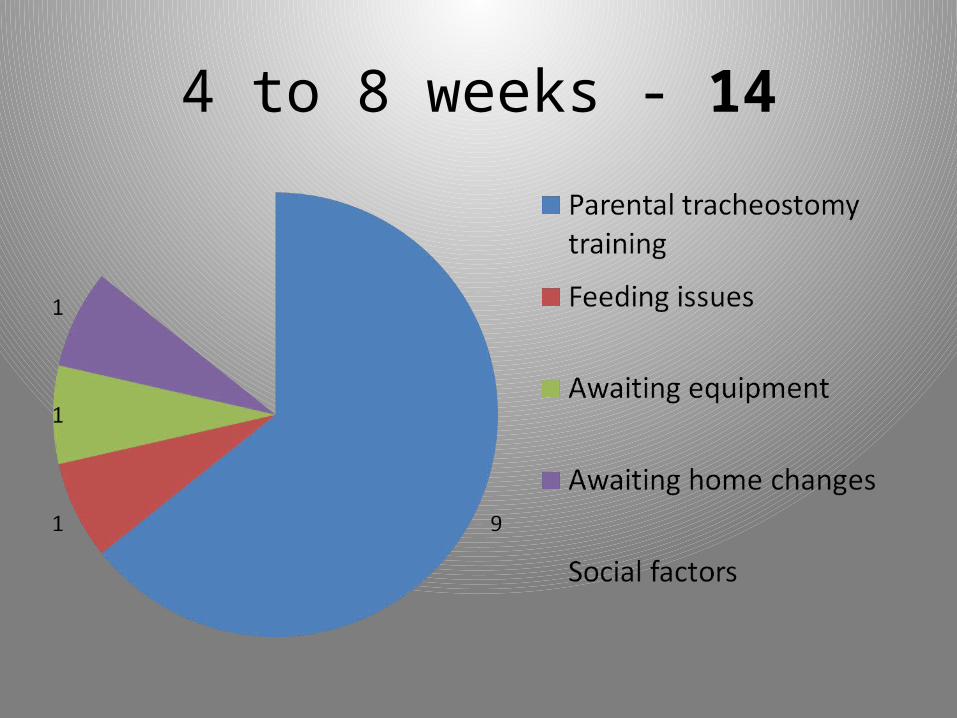
4 to 8 weeks - 14
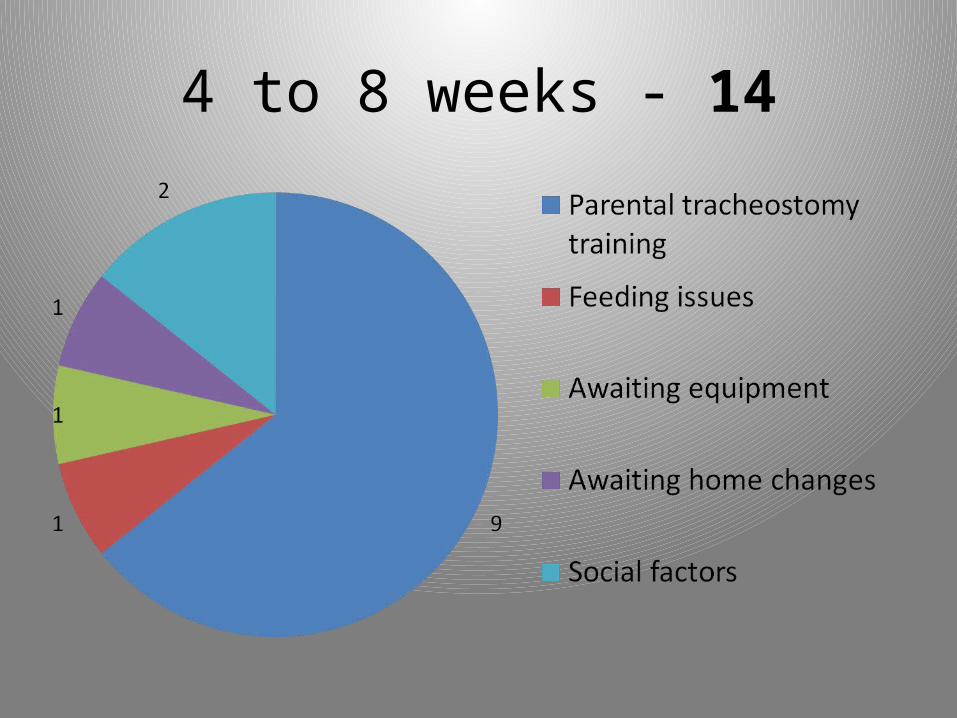
4 to 8 weeks - 14
8 to 12 weeks - 4
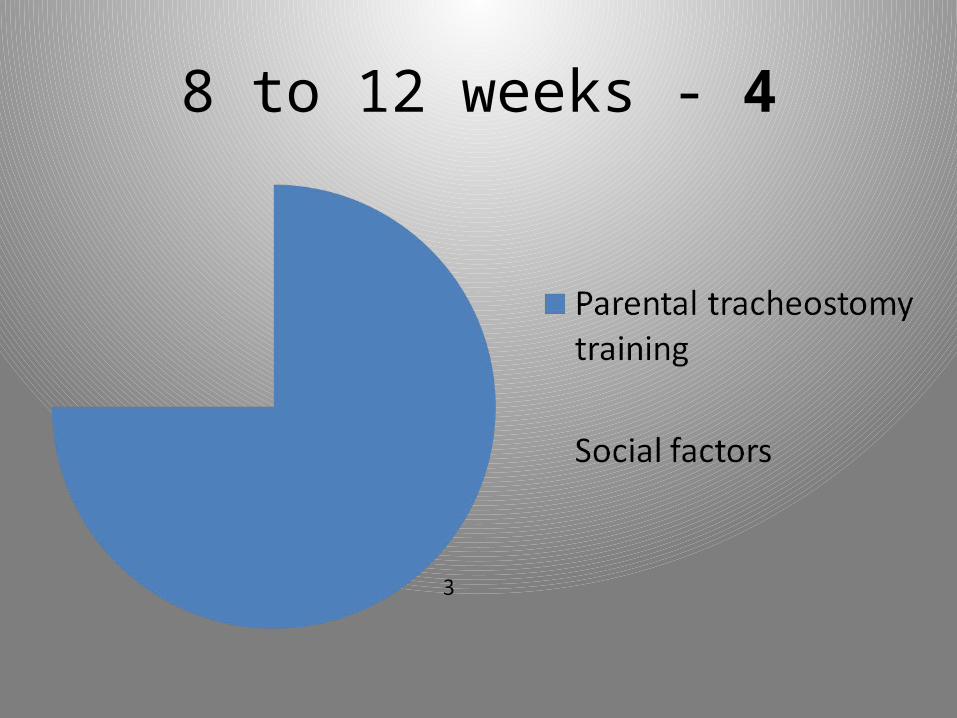
8 to 12 weeks - 4
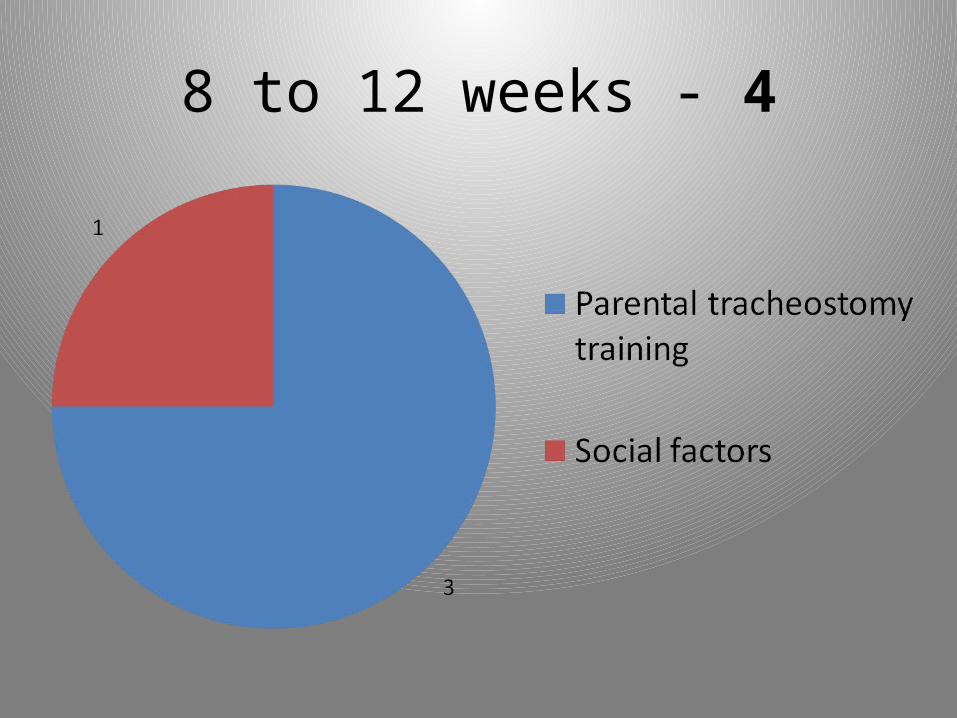
8 to 12 weeks - 4
More than 12 weeks
• 5 children
• Multiple factors– awaiting changes to housing – 3 – social problems – 3 – tracheostomy training – 1
Delays due to….
• Equipment provision• Changes to home environment• Parental tracheostomy training – 22 children
• Social factors
Social & external factors
• Concerns about parenting ability
• Parental drug and alcohol abuse
• Family on “at risk register”
• Children placed in foster care– 5 children

Social & external factors
• Parental separation / divorce
• Single parents
• Effects on employment

Social & external factors
• English not as 1st language
–18 families
– Interpreters required
What can we do?
• Can’t prevent external factors
• Early enrolment of parents on structured training programme
• Early involvement of social care organisations• Good integration of medical, social and
outreach services
What can we do?
• Dedicated paediatric tracheostomy nurse specialist to coordinate the discharge of infants and children with tracheostomies
Summary
Paediatric tracheostomy may result in:
• significant impact on both child and family
• direct and indirect financial burden to both family and health service
• prolonged hospitalisation
• delayed discharge due to social factors