tb vaccines: what is on the horizon? tom evans, md chief scientific officer, aeras iac, washington,...
TRANSCRIPT

TB vaccines: what is on the horizon?
Tom Evans, MDChief Scientific Officer, Aeras
IAC, Washington, D.C., July 27, 2012
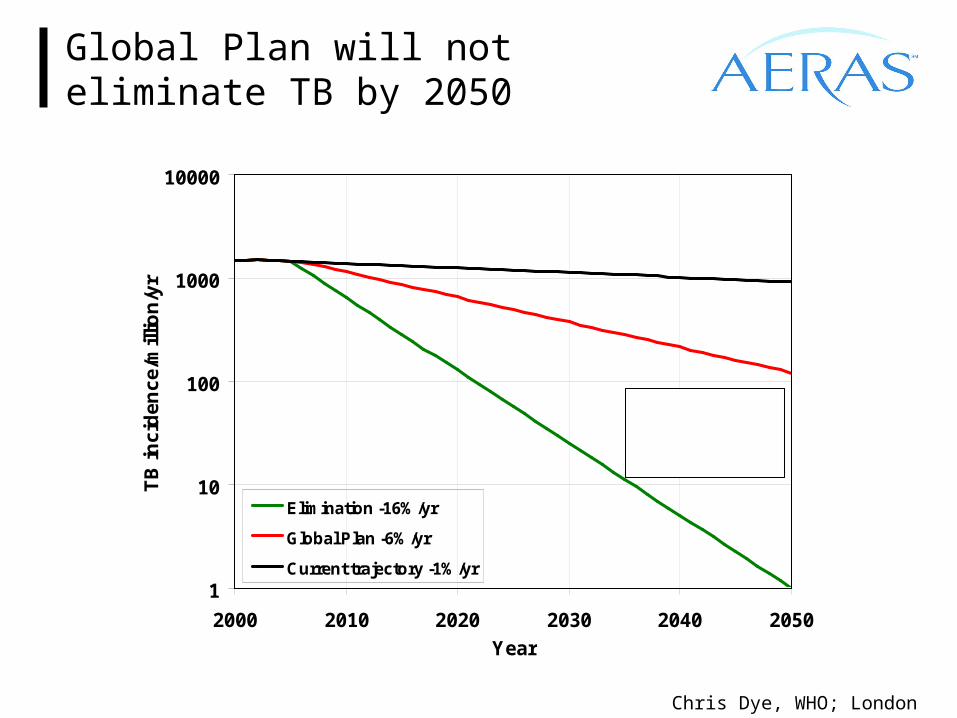
Global Plan will not eliminate TB by 2050
1
10
100
1000
10000
2000 2010 2020 2030 2040 2050
Year
TB
inc
ide
nc
e/m
illio
n/y
r
Elimination -16%/yr
Global Plan -6%/yr
Current trajectory -1%/yr
Projected incidence in 2050 >100x elimination
threshold
Chris Dye, WHO; London 2009
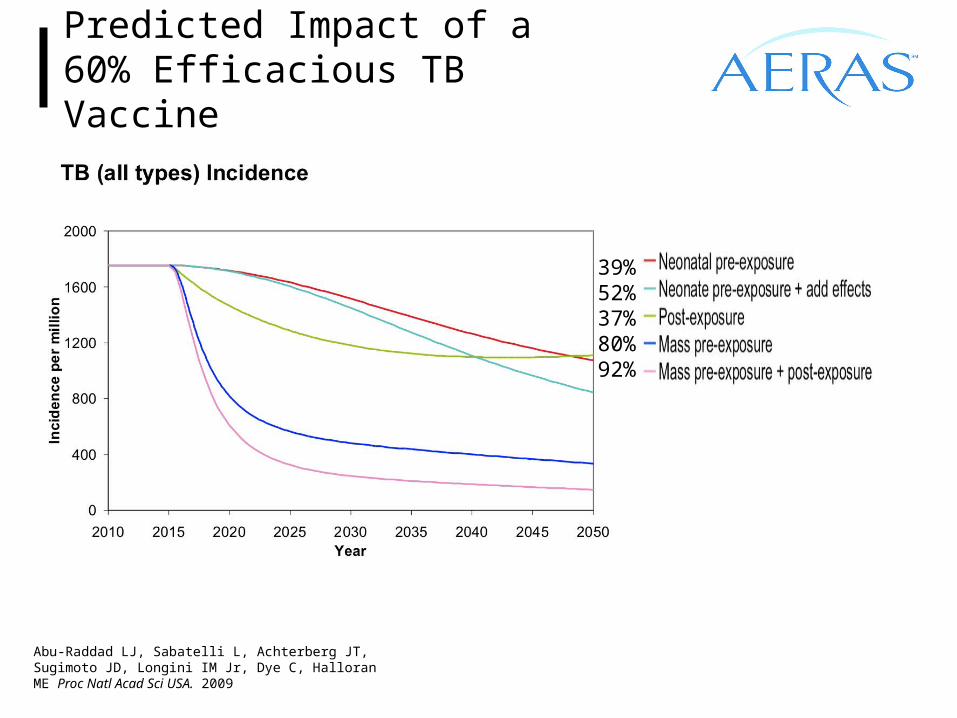
Predicted Impact of a 60% Efficacious TB Vaccine
Abu-Raddad LJ, Sabatelli L, Achterberg JT, Sugimoto JD, Longini IM Jr, Dye C, Halloran ME Proc Natl Acad Sci USA. 2009
39%52%37%80%92%
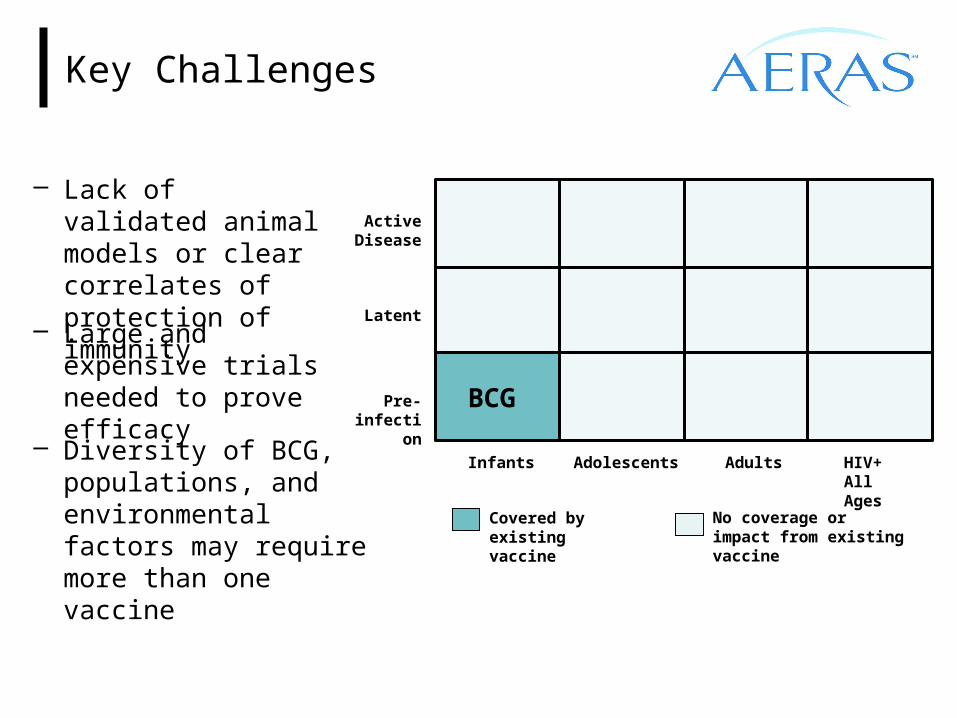
Key Challenges
– Lack of validated animal models or clear correlates of protection of immunity
Covered by existing vaccine
No coverage or impact from existing vaccine
Active Disease
Latent
Pre-infection
Infants Adolescents Adults HIV+ All Ages
BCG
– Large and expensive trials needed to prove efficacy
– Diversity of BCG, populations, and environmental factors may require more than one vaccine
Better TB Vaccines: Reasons to be Optimistic
‒ Most people (80-90%) do not get disease when infected‒ Evidence of BCG vaccine efficacy in children‒ New TB vaccine candidates protect in animal models‒ There are clinical clues to guide immunologic hypotheses
• Low CD4+ T cells are more susceptible to M.tb infection• Anti-TNF treatment is associated with reactivation
‒ New TB vaccines boost cellular immune responses in multiple clinical studies

Strategies for TB Vaccine Development
‒ Pre-infection: to prevent infection• Improved priming vaccines• Novel booster vaccines Block Initial
Infection
Prevent Early Disease
Prevent LatentInfection
Prevent Reactivation
Disease
‒ Post-infection: to prevent disease • Develop novel booster vaccines to
extend and enhance immune protection
‒ Immunotherapeutic: treatment • Shorten the course of chemotherapy
for active TB• Improve efficacy of MDR/XDR/TDR-
TB treatment

Why conduct TB vaccine studies in HIV+ patients?
PROS‒ 1/3 of all deaths from HIV in Africa‒ Incidence ~ 2% annually despite ART and INH preventative Rx‒ Population with high mortality‒ Able to access through the medical system ‒ Easier “downstream” population to vaccinate
CONS‒ Immune response may be modified, with possible negative results‒ Use of preventative INH as recommended by WHO is not uniformly
followed‒ May be a greater rate of re-infection as opposed to reactivation‒ Continually changing treatment and prevention landscape for trials lasting
3-4 years‒ Possible issues of safety, especially with live vaccines
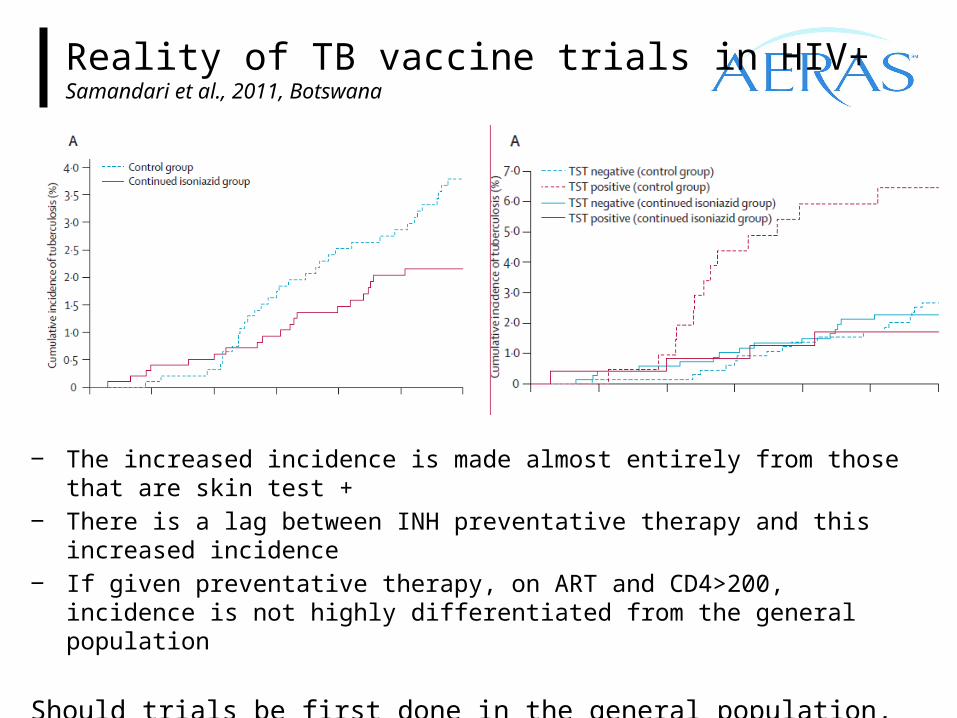
Reality of TB vaccine trials in HIV+Samandari et al., 2011, Botswana
‒ The increased incidence is made almost entirely from those that are skin test +‒ There is a lag between INH preventative therapy and this increased incidence‒ If given preventative therapy, on ART and CD4>200, incidence is not highly
differentiated from the general population
Should trials be first done in the general population, and only then bridged back to the HIV+ population?
M. Vaccae
Phase II Phase IIIPhase IIbP h a s e I
Global Clinical TB Vaccine Pipeline – 2000
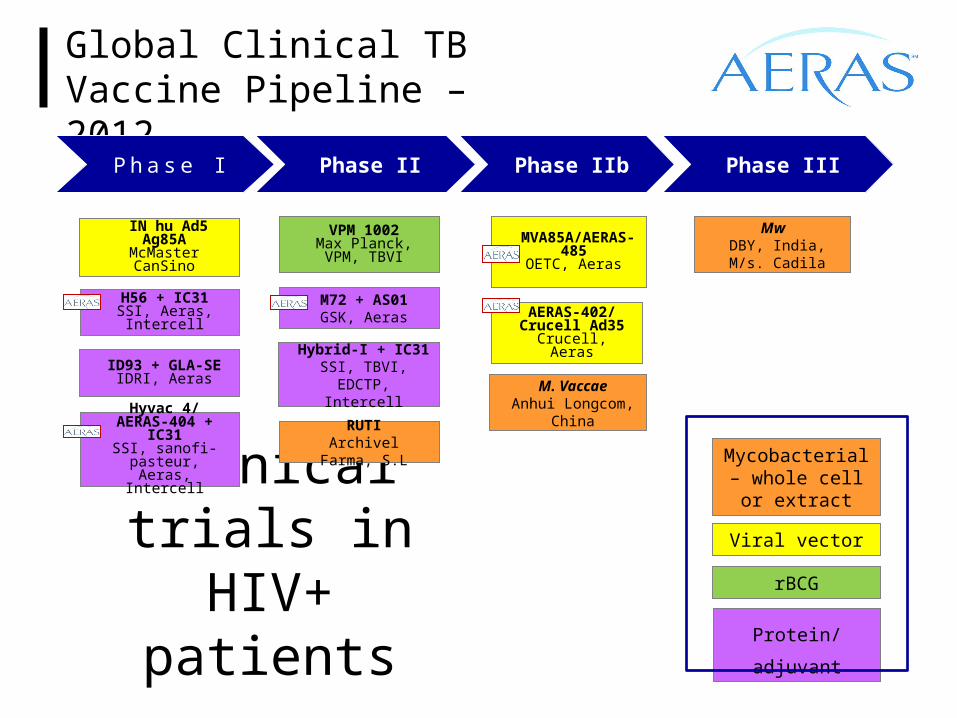
Clinical trials in HIV+ patients
Global Clinical TB Vaccine Pipeline – 2012
ID93 + GLA-SE IDRI, Aeras
IN hu Ad5 Ag85AMcMaster CanSino
VPM 1002Max Planck, VPM,
TBVI
Hybrid-I + IC31SSI, TBVI, EDCTP,
Intercell
RUTIArchivel Farma, S.L
Mw DBY, India, M/s.
Cadila
Phase II Phase IIIPhase IIbP h a s e I
Mycobacterial – whole cell or
extract
rBCG
Viral vector
Protein/adjuvant
Hyvac 4/ AERAS-404 + IC31
SSI, sanofi-pasteur, Aeras, Intercell
H56 + IC31SSI, Aeras, Intercell
M72 + AS01GSK, Aeras
MVA85A/AERAS-485
OETC, Aeras
AERAS-402/Crucell Ad35Crucell, Aeras
M. VaccaeAnhui Longcom,
China
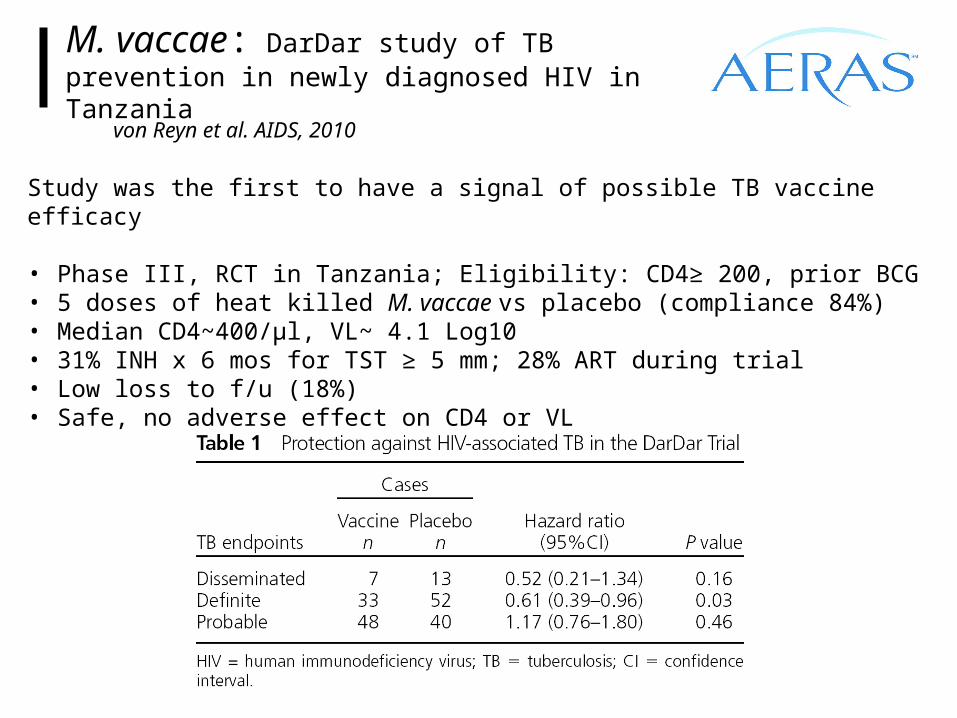
M. vaccae: DarDar study of TB prevention in newly diagnosed HIV in Tanzania
von Reyn et al. AIDS, 2010
Study was the first to have a signal of possible TB vaccine efficacy
• Phase III, RCT in Tanzania; Eligibility: CD4≥ 200, prior BCG• 5 doses of heat killed M. vaccae vs placebo (compliance 84%)• Median CD4~400/µl, VL~ 4.1 Log10• 31% INH x 6 mos for TST ≥ 5 mm; 28% ART during trial• Low loss to f/u (18%)• Safe, no adverse effect on CD4 or VL
MVA85A
‒ Oxford Emergent TB Consortium (OETC)/Wellcome Trust/Aeras
‒ Modified Vaccinia Ankara (MVA) expressing M.tb antigen 85A
• Attenuated poxvirus, replication deficient in mammalian cells• Administered to 120,000 vaccinees (smallpox eradication)
‒ Protects animals in multiple models from M.tb challenge after BCG prime-MVA85A boost administered intradermally
‒ 14 clinical trials completed or ongoing involving >2000 participants
‒ Acceptable safety profile in all populations studied• Site of injection reactions in most subjects
‒ Preferentially induces CD4+ (vs. CD8+) T cell responses• Appears more immunogenic in adults, two doses needed in
HIV+• No effect of vaccination on CD4 count or viral load (Scriba et
al. 2012)
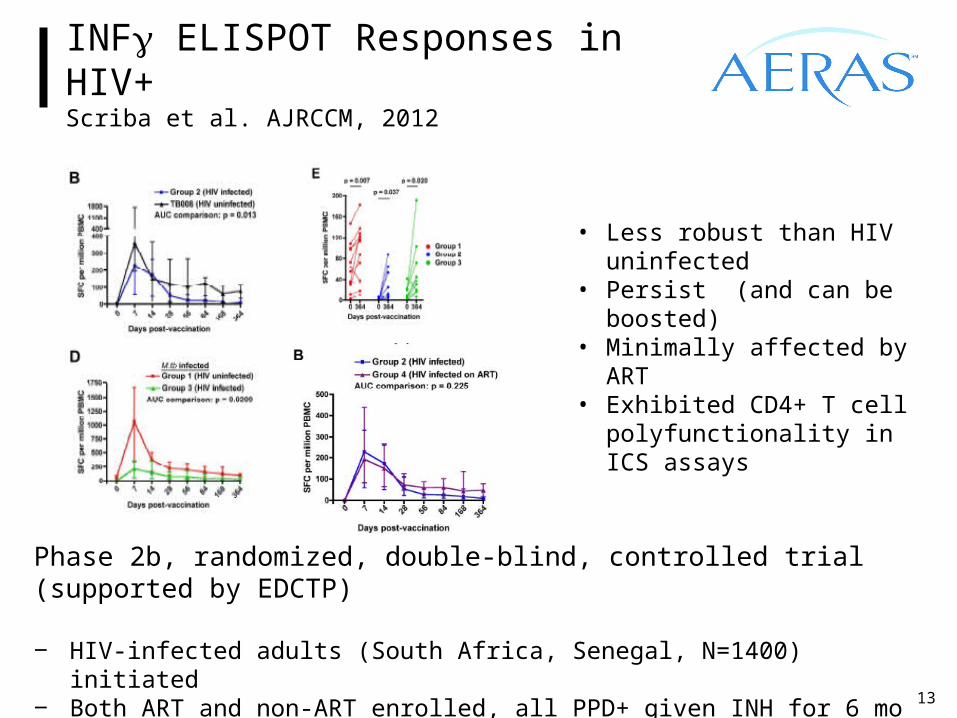
INFg ELISPOT Responses in HIV+Scriba et al. AJRCCM, 2012
13
• Less robust than HIV uninfected
• Persist (and can be boosted)
• Minimally affected by ART• Exhibited CD4+ T cell
polyfunctionality in ICS assays
Phase 2b, randomized, double-blind, controlled trial (supported by EDCTP)
‒ HIV-infected adults (South Africa, Senegal, N=1400) initiated ‒ Both ART and non-ART enrolled, all PPD+ given INH for 6 mo prior to enrollment‒ Over 400 subjects enrolled
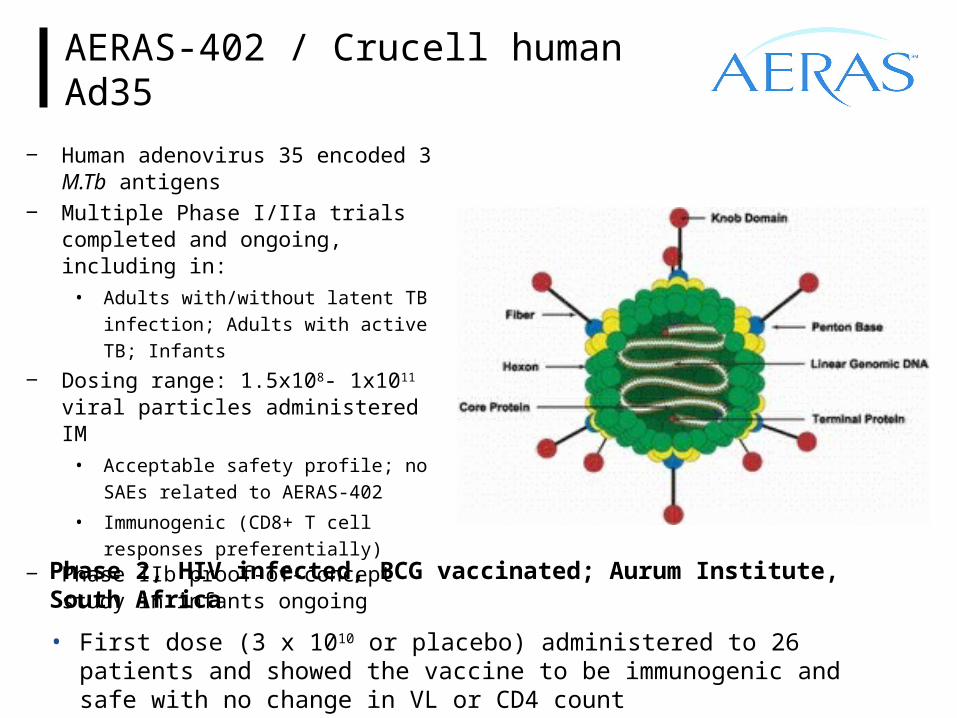
AERAS-402 / Crucell human Ad35
‒ Human adenovirus 35 encoded 3 M.Tb antigens
‒ Multiple Phase I/IIa trials completed and ongoing, including in:
• Adults with/without latent TB infection;
Adults with active TB; Infants
‒ Dosing range: 1.5x108- 1x1011 viral particles administered IM
• Acceptable safety profile; no SAEs
related to AERAS-402
• Immunogenic (CD8+ T cell responses
preferentially) ‒ Phase IIb proof-of-concept study in
infants ongoing
Phase 2, HIV infected, BCG vaccinated; Aurum Institute, South Africa
• First dose (3 x 1010 or placebo) administered to 26 patients and showed the vaccine to be immunogenic and safe with no change in VL or CD4 count
15
VPM1002 in HIV-exposed infants
BCG is not recommended by WHO for HIV-infected infants, although this recommendation is not followed in practice.
‒ rBCG that expresses listeriolysin to induce endosomal perforation, apoptosis induction, and cross presentation to increase CD8+ responses
‒ Safer than BCG in the SCID mouse model‒ Showed superior protection to BCG in some animal studies‒ Studied in healthy adults, TB infected adults, and infants
Presently in a trial in HIV uninfected infants in South Africa in preparation for a Proof of Concept trial in HIV exposed newborns
16
Decade of progress
‒ $600 million invested since 2005
‒ Rich pipeline of 15 new vaccine candidates entered clinical trials
‒ Promising activities for development of new biomarkers emerged
‒ Capacity for vaccine production and carrying out large-scale clinical trials established
‒ Better understanding of safety and immunogenicity
‒ Robust pipeline of discovery and preclinical candidates
17
Decade to come
‒ First efficacy data from proof-of-concept trials that are underway
‒ Better understanding of correlates of immunity, accelerating the testing of future vaccines
‒ Start of multiple phase III studies
‒ Possibility of TB vaccine licensure

Aeras gratefully acknowledges the volunteers in our clinical trials, hard work of many partners, and support of the following major donors:
Netherlands Ministry of Foreign Affairs
US Food and Drug Administration
Global TB vaccine development collaboration

Thank You!
For more information:www.aeras.org
An ounce of prevention is worth a pound of cure.