surgical neonatal - suny downstate neonatal jaundice usu accumulation ... treatment used to do a...
TRANSCRIPT

SURGICAL NEONATAL JAUNDICE
Long Island College Hospital g g pJoelle PierreJanuary 2009
www.downstatesurgery.org

Case Presentation
BG G Born by CS on 9/11/2008 full term – 38 4/7 weeksApgar scores were 8,9Birth weight 3335 gmsCongenital endocushion heart defect diagnosed in uteroMother was 26 yrs old this was her 2nd pregnancy –the first was uneventful
www.downstatesurgery.org

Physical examPhysical examPink, acyanotic, RA sat O2 was 87%, 96% on 0.1 l/minSystolic II/IV murmur at the left sternal borderSystolic II/IV murmur at the left sternal borderno dysmorphic featuresNo palpable abdominal massesp pNo acholic stoolsFeeding well g
www.downstatesurgery.org
Initial Workupp
Echocardiogram – 2 chamber heartgDextrocardiaSingle atriumLarge RV, very small LVAorta originating from the RV,
d lTransposed great vesselsPulmonic stenosis
Abdominal USAbdominal USCholedochal cyst
Total bili 5 8 Direct bili 2 3 LFTs wnlTotal bili 5.8 Direct bili 2.3 LFTs wnl
www.downstatesurgery.org

Dextrocardia
Heart
Right LeftRight
www.downstatesurgery.org

MRCP
High T2 signal structure just inferior to the intrahepatic High T2 signal structure just inferior to the intrahepatic ductal confluence with communication to the gallbladder – suspicious for choledochal cystg p y
www.downstatesurgery.org

HIDA –Tc99mHIDA Tc99m
No clearance of radiotracer at 24 hours in the hours in the hepatic or common bile ducts
ti f suggestive of biliary atresia
www.downstatesurgery.org

Operative Interventionp
DOL #15Exploratory laparotomy, intraoperative cholangiogram, liver biopsy, broviac catheter g g , p y,placement Findings: g
Preduodenal portal veinCholedochal cystPolyspleniaMalrotation : ileo cecal junction on the left and the colon going to the right
www.downstatesurgery.org

Portal vein
www.downstatesurgery.org

Portal vein
duodenum
www.downstatesurgery.org

Choledochal cyst
www.downstatesurgery.org

www.downstatesurgery.org

right left
Appendix
www.downstatesurgery.org

polysplenia
www.downstatesurgery.org

Intraoperative cholangiogram p g g
•Bilobed choledochal cyst •Flow into the small bowel•Arborization of the hepatic ductsCholedochal
cysty
www.downstatesurgery.org

Pathology gy
Liver biopsy: Liver biopsy: Intrahepatic duct paucity compatible with intrahepatic biliary atresia
www.downstatesurgery.org

UGI
•Contrast sweeps Contrast sweeps into the small bowel in the right upper
d quadrant. •Compatible with mid gut malrotation•No obstruction
www.downstatesurgery.org

www.downstatesurgery.org

MR of the abdomen
Preduodenal portospenic confluence, portal veinp p , pCholedochal cyst Multiple small soft tissue masses in the gastrosplenicp g pligament consistent with polyspleniaAorta is anterior and to the right of the midline at the level of the diaphragmSma is to the right of the smvNo intrahepatic IVCDuplicated IVC
www.downstatesurgery.org

Heterotaxy syndrome/ Situs Ambigous
Abnormal arrangement of body organs or complete g y g psitus inversusMajor cardiac anomaliesGI anomalies
Midline liverMalposition of stomach Malposition of stomach Anomalies of intestinal rotation and fixation
Including malrotation, preduodenal portal vein Intraperitoneal pancreas
Asplenia or polysplenia
www.downstatesurgery.org

OR Take 2
DOL #30By now: T.B 6.5 Ast/alt 30/20GGT 371
Operative Procedure : Exploratory laparotomyLysis of adhesionsCholecystectomyResection of choledochal cyst and atretic common hepatic duct up to the porta hepatisH t t t t ith R Y t iHepatoportoenterostomy with a Roux en-Y anastomosisModified Ladd’s procedure – appendectomyDid not have to bypass the retro portal vein duodenum
www.downstatesurgery.org

Pre duodenal l iportal vein
www.downstatesurgery.org

Gall bladder
Choledochal cyst
www.downstatesurgery.org

www.downstatesurgery.org

Pathologygy
Choledochal cyst – type IICholedochal cyst type IIHepatic duct ; dense fibroconnective tissue containing a minute atretic ductcontaining a minute atretic duct
www.downstatesurgery.org

Post-operative coursep
POD #2 extubated, bilious drainage from the JP POD #2 extubated, bilious drainage from the JP drainPOD #5 greenish stools! T.Bili 2POD #5 greenish stools! T.Bili 2POD#6 tolerates PO diet POD #25 with green/yellow stools tolerating diet POD #25 with green/yellow stools, tolerating diet and starting to gain weight – discharge planning in progress progress
www.downstatesurgery.org

Questions?www.downstatesurgery.org

Surgical causes of neonatal jaundiceSurgical causes of neonatal jaundice
www.downstatesurgery.org

Neonatal jaundice
Usu accumulation of unconjugated bilirubinConjugated through glucuronyl transferaseConjugated water soluble then excreted into the biliary system Gi tract. biliary system Gi tract. Newborns
high Hgb, Rh, ABO and rare blood group abnormalities leading to hemolysisto hemolysisimmature conjugating systeminfections
S h t i t l ti f bili bi i th ti So can have transient accumulation of bilirubin in the tissues – physiologic jaundice of the neonatal periodEvident day 5-7 Usually goes away by week 2
www.downstatesurgery.org

Persistent neonatal jaundicej
Biliary atresia (60%)Biliary atresia (60%)Neonatal Hepatitis (35%)
hepatic inflammation that can be secondary to several p ydifferent causes
cmv, syphilis, herpes, toxoM b li d f Al h 1 i i d fi i l iMetabolic defects : Alpha 1-antitrypsin deficiency, galactosemia
Choledochal cyst (5%)Al ill d t i h ti d l i Alagille syndrome – arteriohepatic dysplasia –congenital syndrome associated with abnormal facies.
Paucity and hypoplasia of interlobar bile ducts Paucity and hypoplasia of interlobar bile ducts
www.downstatesurgery.org

continued
Spontaneous perforation of extrahepatic bile ductsp p pAscites, mild jaundice, failure to thriveUsu occurs at the junction between the cystic and common bile ducts
Inspissated bile syndrome – bile plug syndromeE h i b i f h bil d b biliExtrrahepatic obstruction of the bile ducts by biliarysludgeAssociated with massive hemolysis, hemorrhage, TPN, y , g , N,cystic fibrosis and other intestinal diseases such as Hirchsprungs
www.downstatesurgery.org

Choledochal cysty
Congenital biliary tract disorderCongenital biliary tract disorder1: 2 million – 1: 13,000Idiopathic dilation of the common bile ductIdiopathic dilation of the common bile duct
www.downstatesurgery.org

Etiology:
Can be associated with an anomalous jcn of the jpancreatic and common bile ductsPossibly an abnormal pancreatic and biliary duct j i i h h f i f h l b junction with the formation of a common channel by which the pancreatic enzymes are secreted. Reflux of pancreatic enzymes into the bile duct Reflux of pancreatic enzymes into the bile duct
This weakens the bile duct wall by enzymatic wall destruction dilation inflammation cyst formation Infectious agentsBiliary autonomic dysfunction
www.downstatesurgery.org

Presentation
More common in females than males 4:1More common in asians – japaneseCan present in the neonatal periodUsually present in toddlersClassically: Abdominal pain, mass, jaundiceMore commonly: episodic abdominal pain, minimal jaundicePt d l h l iti i f t d t t l Pts can develop cholangitis, infected cysts, portal hypertension and cirrhosisRarely: present with bile peritonitis from a ruptured cystRarely: present with bile peritonitis from a ruptured cyst
www.downstatesurgery.org

Diagnosis g
Frequently diagnosed in the fetus during a Frequently diagnosed in the fetus during a screening prenatal USPostnatally – a cystic structure seen on US Postnatally a cystic structure seen on US originating from the biliary treeCT and MRCP can be used in order to elucidate the CT and MRCP can be used in order to elucidate the cyst’s relationship with the bilary tree, porta hepatis and delineate its anatomy
www.downstatesurgery.org
Classes
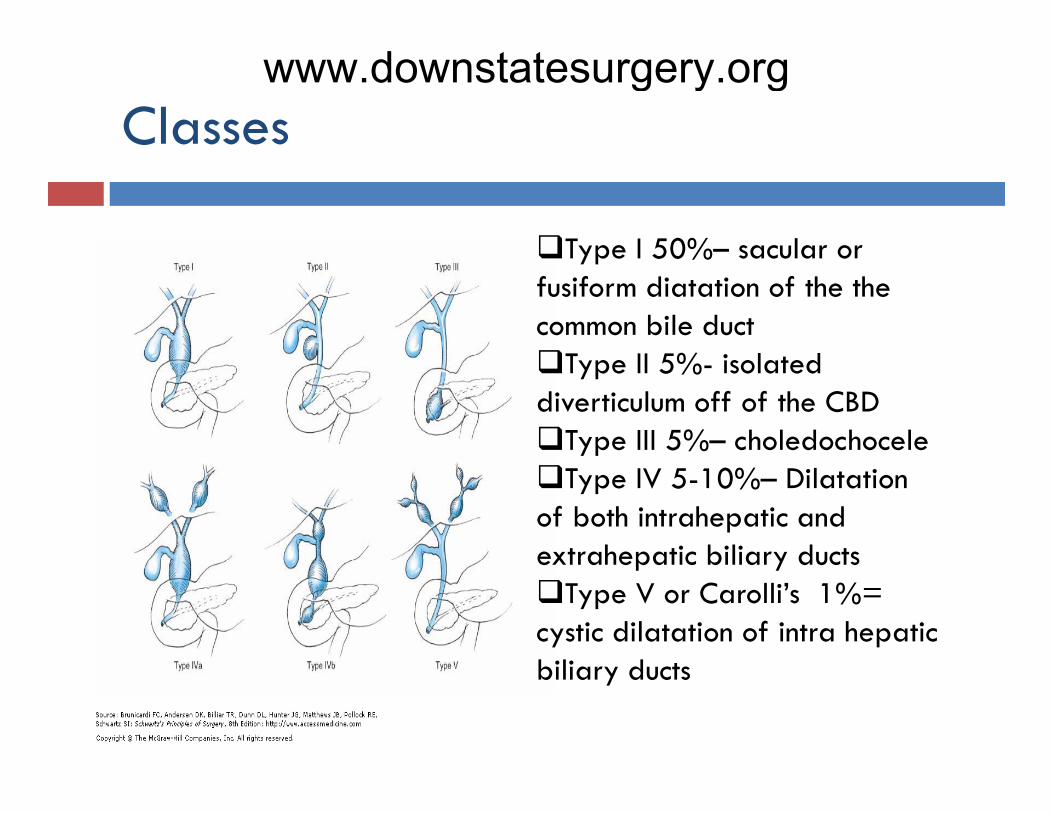
Type I 50%– sacular or Type I 50% sacular or fusiform diatation of the the common bile duct
T II 5% i l d Type II 5%- isolated diverticulum off of the CBD
Type III 5%– choledochoceleType IV 5-10%– Dilatation
of both intrahepatic and extrahepatic biliary ducts extrahepatic biliary ducts
Type V or Carolli’s 1%= cystic dilatation of intra hepatic bili d tbiliary ducts
www.downstatesurgery.org

Untreated can cause cholangitis and Untreated can cause cholangitis and cholangiocarcinomaRisk of ca in the 1st decade – 0.7%Risk of ca in the 1 decade 0.7%Increases in the 2nd decade to 14%In types I II IV : excision of the extrahepatic biliary In types I, II, IV : excision of the extrahepatic biliary tree, cholecystectomy and with a Roux-en-Y hepaticojejunostomyhepaticojejunostomyIV may require additional segmental resection Type III sphincterotomyType III - sphincterotomy
www.downstatesurgery.org

Treatment
Used to do a cyst-enterostomy however many of Used to do a cyst enterostomy however many of these pts went on to develop cholangiocarcinoma
cholecystectomyy yCyst excisionBiliary enteric reconstructiony
www.downstatesurgery.org

Prognosis g
Generally excellent Generally excellent Complications:
Anastomotic strictureAnastomotic strictureCholangitisIntrahepatic stonesIntrahepatic stones
www.downstatesurgery.org

Biliary Atresiay
Incidence 1/20,000Incidence 1/20,000Obliterative process of the extrahepatic bile ductsAssociated with hepatic fibrosis Associated with hepatic fibrosis Ladd and Gross : arrest of development during the solid stage of bile duct formation solid stage of bile duct formation. Etiology unclearA i d i i i l i f i Acquired – immune vs systemic viral infections Congenital – association with polysplenia
www.downstatesurgery.org

Atretic ducts – solid fibrous cords that may contain yoccasional islands of biliary epitheliumThree patterns
Proximal extrahepatic bile ducts are patent and ducts distal to the cystic duct are obliteratedThe gallbladder, cystic duct and CBD are patent and g , y pproximal ducts occludedEntire extrahepatic system is occluded
O i h f il bil l i Over time the failure to excrete bile results in progressive periportal fibrosis and obstruction of the intrahepatic portal veins hepatic cirrhosis p p p
www.downstatesurgery.org

Presentation Presentation Grey or acholic stools – secondary to obstructed bile flowbile flowFailure to thrive Liver failure and portal hypertensionLiver failure and portal hypertensionBilirubin > 3 mg/dl Alk h 500 1000Alk phos 500-1000GGT > 300
www.downstatesurgery.org

Diagnosisg
Technetiun-99m iminodiacetate (HIDA) after pre-Technetiun 99m iminodiacetate (HIDA) after pretreatment with phenobarbital ( promotes tracer uptake) p )If radionucleotide appears in the intestine then the biliary tree in presumed to be patenty p pUltrasound can exclude choledochal cyst10% of pts - gallbladder is visualized and the 10% of pts gallbladder is visualized and the distal ducts are patent.Percutaneous liver biopsy can r/o neonatal hepatitisPercutaneous liver biopsy can r/o neonatal hepatitis
www.downstatesurgery.org
Intraoperative cholangiogram Intraoperative cholangiogram Can use the gallbladder as a conduitDefines the extrahepatic biliary anatomy Defines the extrahepatic biliary anatomy
www.downstatesurgery.org

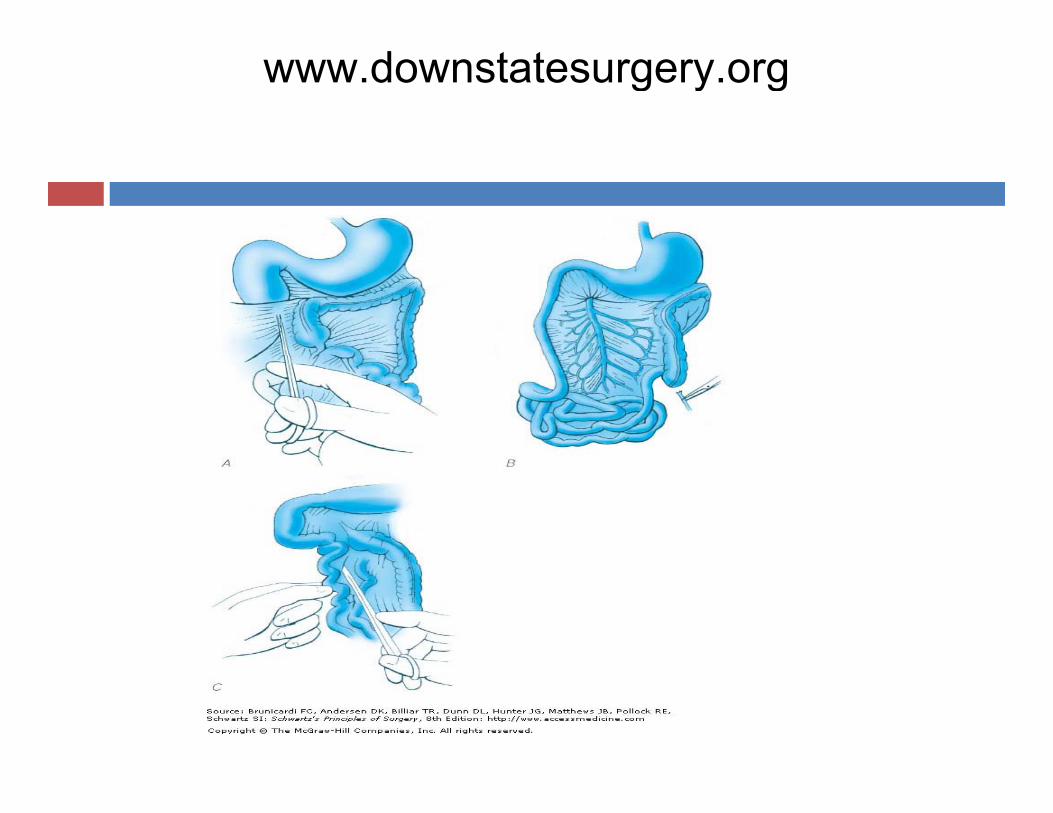
treatment
KasaiExcise scarred bile ducts and gall bladderPortoenterostomy
Bile flow into the intestinesRoux en y limb of the jejunumLiver biopsy to evaluate the degree of fibrosisSurgical success is increased if its done before 8 weeks
Intussucepted antireflux valve using appendix and jejunal limb –minimize postoperative cholangitis
Supposed to minimize postoperative cholangitisD t t it t ll d t i t t th h f ll t f Data suggests it actually does not impact outcome thus has fallen out of favor
Complicationcholangitischolangitis
www.downstatesurgery.org

www.downstatesurgery.org

Outcome
Usu successful if done before 2 months Two thirds of the require liver transplant secondary to progressive liver failure
1/3 of pts remain asymptomatic 1/3 never have bile flow and require early transplant/1/3 initially have good bile flow but subsequently
develop cirrhosis Independent risk factors for failure Independent risk factors for failure
Bridging liver fibrosisPost op cholangitic episodesp g p
www.downstatesurgery.org

Without surgery or liver transplant life span – 19 Without surgery or liver transplant life span 19 monthsDeath Death
Progressive liver failure Bleeding from esophageal varicesBleeding from esophageal varicesSepsis
Liver TransplantLiver Transplant
www.downstatesurgery.org

Questions
A 54 yr male is found to have a type I choledochal A 54 yr male is found to have a type I choledochal cyst incidentally while being worked up for appendicitis. Treatment?pp
Observe and do serial CTs Q 6 monthsObserve and do nothing unless symptomaticCholecystectomyCholecystectomy, choledochal cyst excision, hepatoenterostomy
www.downstatesurgery.org

A 54 yr male is found to have a type I choledochal A 54 yr male is found to have a type I choledochal cyst incidentally while being worked up for appendicitis. Treatment?pp
Observe and do serial CTs Q 6 monthsObserve and do nothing unless symptomaticCholecystectomyCholecystectomy, choledochal cyst excision, hepatoenterostomy
www.downstatesurgery.org

A 3 week old infant is brought to the ER with glethargy and vomiting. The infant had been doing well at home until today, when she became lethargic
d i i i h i l Whi h f h and was vomiting greenish material. Which of the following would be most accurate in making the diagnosis?diagnosis?
Abdominal USUGICTXRBarium enema
www.downstatesurgery.org

A 3 week old infant is brought to the ER with lethargy A 3 week old infant is brought to the ER with lethargy and vomiting. The infant had been doing well at home until today, when she became lethargic and was vomiting greenish material. Which of the following would be most accurate in making the diagnosis?
Abd i l USAbdominal USUGI
CTCTXRBarium enema
www.downstatesurgery.org

Which of the following is included in the LADD’s Which of the following is included in the LADD s procedure?
Cholecystectomyy yAppendectomyBoth neither
www.downstatesurgery.org

Which of the following is included in the LADD’s Which of the following is included in the LADD s procedure?
Cholecystectomyy yAppendectomyBoth neither
www.downstatesurgery.org

The most common type of Choledochal cyst isThe most common type of Choledochal cyst isIIIIIIIIIVV
www.downstatesurgery.org
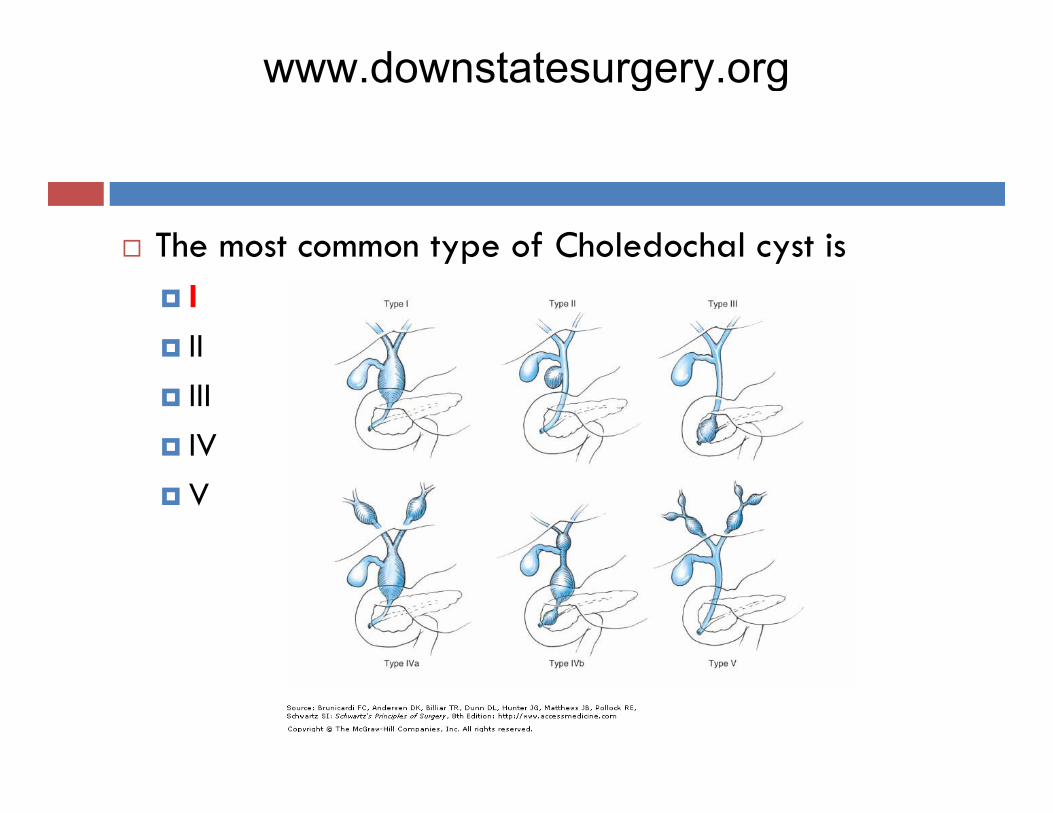
The most common type of Choledochal cyst isThe most common type of Choledochal cyst isIIIIIIIIIVV
www.downstatesurgery.org

TRUE OR FALSETRUE OR FALSEApproximately 60% of pts with biliary atresia who undergo a Kasai procedure will eventually need a undergo a Kasai procedure will eventually need a liver transplant
www.downstatesurgery.org

TRUE OR FALSETRUE OR FALSEApproximately 60% of pts with biliary atresia who undergo a Kasai procedure will eventually need a undergo a Kasai procedure will eventually need a liver transplant
www.downstatesurgery.org

References
Grosfeld: Pediatric Surgery 6th ed. Grosfeld: Pediatric Surgery 6 ed. Chang J. Brueckner M. Touloukian RJ: Intestinal rotation and fixation abnormalities in heterotaxia: rotation and fixation abnormalities in heterotaxia: early detection and management J Pediatr Surg 1993; 28:1281.Maingot’s Abdominal Operations Siegel, M., Jaundice in Infants and Children, Siegel, M., Jaundice in Infants and Children, Ultrasound clin, 2006;1,431-446Schwartz’s Principles of SurgerySchwartz s Principles of Surgery
www.downstatesurgery.org
www.downstatesurgery.org