study of diabetes mellitus among patients with hepatitis c
TRANSCRIPT

Study of diabetes mellitus among patients with hepatitis C virusMona Abdel Raoufa, Zeinab A. Yousrya, Olfat M. Hindyb, Somayh S. Eissaa
and Dalia S. Solimanc
aDepartment of Internal Medicine, Faculty of Medicinefor Girls, AL-Azhar University, bDepartment of ClinicalPathology, National Liver Institute, El-MenoufyaUniversity and cDepartment of Internal Medicine,Police Authority Hospital
Correspondence to Somayh S. Eissa, 131 SakerQuriesh, New Maadi, Cairo, EgyptTel: + 01 113 754 668;e-mail: [email protected]
Received 1 February 2012Accepted 15 April 2012
The Egyptian Journal of Internal Medicine
2012, 24:17–23
Introduction
Hepatitis C virus (HCV) infection and type 2 diabetes are two common disorders with
high impact on health worldwide. There is growing evidence to support the concept
that HCV is associated with type 2 diabetes.
Purpose
This work aimed to study the clinical phenotype of type 2 diabetes in HCV patients.
Patients and methods
Our study was conducted upon 100 nonobese, noncirrhotic hepatitis C positive
patients who were classified into two groups according to homeostatic model
assessment (HOMA) test for insulin resistance (HOMA IR). This study also included
15 nonobese type 2 diabetic patients negative for HCV and hepatitis B virus infection
classified as control groups. We excluded alcoholics and drug addicts and patients
with conditions that affect blood glucose such as endocrine diseases associated with
disordered glucose metabolism and use of drugs. All participants were subjected to
full history taking and complete clinical examination including BMI and the following
investigations: complete blood count, fasting blood sugar, 2 h postprandial blood
sugar, glycosylated hemoglobin, fasting insulin level, cholesterol level, HDL, LDL,
triglyceride, serum urea, creatinine, complete urine analysis, liver function tests:
total bilirubin, alkaline phosphatase, albumin, prothrombin time, INR, SGOT,
SGPT, quantitative PCR for determination of HCV-RNA, surface antigen (HbsAg),
abdominal ultrasonography, liver biopsy when needed and possible for HCV
patients, and ECG.
Results
In this study, we found that the prevalence of type 2 diabetes in group I is 24%. HCV
can independently contribute to IR with viral genotypes 1 or 4. We noticed significant
positive correlation between fasting insulin and HOMA IR in hepatitis C +ve patients.
IR in HCV-infected patients is high irrespective of the degree of liver injury even
before a minimal fibrosis is present. Both IR and diabetes can adversely affect the
course of chronic hepatitis C, leading to enhanced steatosis and liver fibrosis, and
even increase the risk of hepatocellular carcinoma. A significant correlation between
HOMA IR and steatosis, a significant positive correlation between fasting insulin and
steatosis and a negative correlation between steatosis and BMI in HCV patients was
found. No correlation was found between HOMA IR and the viral load (quantitative
HCV RNA).
Conclusion
We can concluded that diabetic HCV patients had intermediate clinical phenotype
lower BMI and LDL than control and development of type 2 diabetes mellitus in HCV
patients was significantly higher in nontreated patients than treated patients. Antiviral
therapy and clearance of HCV improves IR, b-cell function, the blood glucose
abnormalities.
Keywords:
hepatitis C virus, insulin resistance, type 2 diabetes mellitus
Egypt J Intern Med 24:17–23& 2012 The Egyptian Society of Internal Medicine1110-7782
Introduction
Hepatitis C virus (HCV) infection and type 2 diabetes
are two common disorders that adversely affect health
worldwide. A high prevalence of type 2 diabetes among
HCV-infected patients with chronic hepatitis has been
reported, and there is growing evidence indicating that
HCV is associated with type 2 diabetes (Albert et al.,2006) [1]. An increased prevalence of type 2 diabetes has
been found in liver cirrhosis irrespective of the etiology.
It is less clear whether HCV is associated with type 2
diabetes in the absence of cirrhosis [2]. HCV may directly
damage B cells or disturb their function, leading to dia-
betes [1]. HCV can induce insulin resistance, disturbing
Original article 17
1110-7782 & 2012 The Egyptian Society of Internal Medicine DOI: 10.7123/01.EJIM.0000415588.62804.fc
Copyright © The Egyptian Society of Internal Medicine. Unauthorized reproduction of this article is prohibited.

the insulin signal pathway because of the effect of the
HCV core protein. Moreover, a significant association
between diabetes and stage of fibrosis in HCV patients,
independent of obesity and steatosis, has been found on
liver biopsy (Marcin et al., 2006) [3]. Insulin resistance
mediated by proinflammatory cytokines, rather than
defects in insulin secretion, could be the primary
pathogenic mechanism involved in the development of
diabetes associated with HCV infection [1]. There is a
strong link between diabetes and hepatic steatosis or non
alcoholic steatohepatitis. Hyperglycemia and hyperinsuli-
nemia have been suggested to be important factors for the
progression of fibrosis [4]. Advanced fibrosis was observed
more frequently in patients with diabetes than in patients
without diabetes [5].
This work aimed to study the insulin resistance and
clinical phenotype of type 2 diabetes in HCV patients.
Patients and methodsThis work was carried out on 100 patients with chronic
HCV infection, diagnosed by anti-HCV antibodies, PCR
for HCV-RNA, ranging in age from 42 to 60 years, with
mean ± SD (46.2 ± 3.69) years, and mass index (BMI)
ranging from 22.2 to 25.6 kg/m2, with mean ± SD
(23.8 ± 0.8). Twenty-four of these patients were women;
69 of them received combined therapy interferon and
ribavirin, 12 of them received interferon monotherapy, and
19 did not receive treatment for HCV. Fifteen patients with
type 2 diabetes diagnosed on the basis of a fasting plasma
glucose level of at least 126 mg/dl, negative for both HCV
and hepatits B virus, ranging in age from 42 to 60 years, with
mean ± SD (48.7 ± 5.69) years, and BMI ranging from 24.5
to 25.7 kg/m2, with mean ± SD (25.2 ± 0.36), were included
in the control group. Five of them were women; 12 received
oral hypoglycemic drugs and three received insulin for
diabetes. We excluded obese, cirrhotic patients, alcoholics,
drug addicts and individuals with any condition that affects
blood glucose such as endocrine diseases and those using
drugs associated with glucose metabolism disorder. The
patients and control groups were selected from the
outpatient clinic of Al Zahra University Hospital, National
Liver Institute El-Menoufya University, and Police Author-
ity Hospitals. Consent was obtained from all patients
included in the study.
All the patients studied were subjected to (a) full medical
history and a complete clinical examination including
assessment of BMI [weight in kg divided by the square
of height in meters [6]; (b) laboratory investigations
including: complete blood count using an automated
hemology analyzer (Baker system 8210); fasting blood
sugar (FBS), 2 h postprandial blood sugar; lipid profile
including cholesterol, HDL, LDL, and triglyceride;
serum urea, creatinine, and liver functions including
SGPT, SGOT, alkaline phosphatase, total bilirubin,
albumin, prothrombin concentration and time, INR,
using an autoanalyzer (Hitachi-911, USA). Glycosylated
hemoglobin (HAc1) was determined using the fast,
optimized ion-exchange resin procedure-separation direct
in the tube [7]. Fasting insulin levels for homeostatic
model assessment (HOMA IR) indices are used as
markers of insulin resistance and calculated as follows [8]:
Fasting insulin IU/mlð Þ�fasting serum glucose mmol/lð Þ22:5
:
It is considered to be elevated at HOMA ratio of at least
3 [9]. Quantitative PCR for the determination of HCV-
RNA was carried out using a Roboscreen Taqman reagent
mix Germany for HCV and an ABI PRISM 7000 Sequence
Detection System (Applied Biosystems Germany); surface
antigen for hepatitis B virus; and complete urine analysis.
(c) Abdominal ultrasonography was carried out using a
real-time scanner (Hitachi, EUD 200). (d) Liver biopsy
was performed when needed and only for patients. The
biopsy was performed using a gun and a modified 18-gauge
or 16-gauge Trucut needle and was guided by ultrasono-
graphy using a complete sterile technique and local
anesthesia [10]. (e) ECG was also performed for all
patients.
Data were analyzed using Microsoft Office 2003 (excel)
and the Statistical Package for Social Science version 10.
Parametric data were expressed as mean ± SD and
nonparametric data were expressed as number and
percentage of the total. Comparison of the mean ± SD
of two groups was carried out using Student’s t-test. The
mutual correspondence between two values was deter-
mined using the Spearman correlation coefficient.
ResultsTwenty-four patients with chronic HCV infection devel-
oped type 2 diabetes after HCV infection (24%), and they
had high FBS (160.25 ± 48.75), high post prandial (PP)
(220.33 ± 80.12), and HBA1c (7.90 ± 2.56) (Fig. 1). All 24
patients had HOMA IR above 3 (5.85 ± 3.33); 18 of these
patients did not receive treatment for HCV and six patients
who received combined therapy interferon and ribavirin
developed type 2 diabetes after HCV infection.
Table 1 showed histological scoring system [11].
Table 2 showed that: the mean BMI, FBS, PP, HA1C,
HOMA IR, cholesterol, and triglyceride are significantly
lower in HCV patients than in the control individuals and
platelets were nonsignificantly lower in HCV patients.
Table 1 Histological scoring systems [11]
Stage Metavir system Ishak system
0 No fibrosis No fibrosis1 Periportal fibrosis
expansionFibrous expansion of some portal areas
with or without short fibrous septa2 P–P septae
(41 septum)Fibrous expansion of most portal areas,
with or without short fibrous septae3 P–C septae Fibrous expansion of most portal areas,
with occasional P–P bridging4 Cirrhosis Fibrous expansion of portal areas, with
marked bridging (P–P or P–C)5 – Marked bridging (P–P or P–C) with
occasional nodules (incompletecirrhosis)
6 – Cirrhosis
18 The Egyptian Journal of Internal Medicine
Copyright © The Egyptian Society of Internal Medicine. Unauthorized reproduction of this article is prohibited.

Table 3 shows that the mean BMI, FBS, and PP are
significantly lower in HCV patients positive for diabetes
than the control individuals and platelets were nonsigni-
ficantly lower in HCV patients positive for diabetes than
the control individuals.
Table 4 shows that the mean age, BMI, FBS, PP, HA1C,
insulin, HOMA IR, cholesterol, and triglyceride are
significantly higher in HCV patients positive for diabetes
(HOMA IRZ3) than HCV patients negative for diabetes
(HOMA IRo3); platelets were significantly lower in
HCV patients positive for diabetes (HOMA IRZ3) than
HCV patients negative for diabetes (HOMA IRo3).
Our results showed a significant positive correlation
between fasting insulin, HOMA IR, and steatosis among
HCV patients, whereas the correlations between fasting
insulin, HOMA IR, and stage of fibrosis among HCV
patients were nonsignificantly positive. Moreover, the
correlation between steatosis and BMI in HCV patients
was negative (Fig. 2–6). High fasting insulin, HOMA IR,
and diabetes were detected even before minimal fibrosis
and steatosis in chronic HCV infection (Fig. 8), which
indicates that insulin resistance is an independent factor
in predicting fibrosis in HCV-infected patients. Surpris-
ingly, no correlation was found between HOMA IR and
the viral load (quantitative HCV-RNA) (Fig. 7).
DiscussionAn increased prevalence of type 2 diabetes has been
found in liver cirrhosis irrespective of the etiology [12].
No association was found between type 1 diabetes and
HCV infection [13]. Type 2 diabetes mellitus is
associated with a chronic infection of HCV [14]. HCV
causes extrahepatic manifestations including insulin
resistance and type 2 diabetes mellitus [15]. HCV
infection increases the risk of development of diabetes
as a consequence of HCV-induced liver damage. Ad-
vanced cirrhosis induces dysregulation of glycemic con-
trol, which may result in overt diabetes [16]. Our study
showed that the prevalence of type 2 diabetes in HCV
patients was 24%, and fasting insulin level was signifi-
cantly higher in noncirrhotic HCV + DM + patients
(HOMA IRZ3) than in noncirrhotic HCV + DM –
patients (HOMA IRo3); this result is in agreement
with that of [17]. Insulin resistance is a common
condition in chronic hepatitis; it occurs at an early stage
during the course of HCV infection [2]. b-cell dysfunc-
tion as indicated by C-peptide levels and a limited insulin
response [18] as well as insulin resistance was found in
patients with chronic hepatitis C infection [19]; Albert
and his colleagues (2006) reported that a high fasting
insulin level has been observed in HCV-infected patients
with a moderate or a severe degree of hepatic fibrosis [1].
Virus-induced insulin resistance may be a mechanism for
fibrogenesis in HCV. Activation of the tumor necrosis
factor system in chronic HCV infection correlates with
the disease activity [20]. The presence of visible
hepatocyte triglyceride droplets is a consequence of
insulin resistance, hyperinsulinemia, and the resulting
excessive flux of free fatty acids through the liver.
Triglyceride droplets may be inert with respect to
promoting injury and altered cellular homeostasis [21].
HCV infection promotes insulin resistance mainly
through increased production of tumor necrosis factor-aand cytokine suppressor (SOCS-3). Both events inhibit
the insulin receptor and insulin receptor substrate-1 [22].
An increase in insulin resistance even before a minimal
degree of hepatic fibrosis was observed in our study, that
is, insulin resistance may be an independent factor
in predicting fibrosis in HCV-infected patients and may
not attributable to advanced liver disease, which is in
agreement with Nagao et al. [15] and Negro et al. [23],
who reported that HCV infection may induce insulin
resistance irrespective of the severity of liver disease,
and its effect seems to be genotype specific. Also,
Tsochatzis et al. [16] reported that insulin resistance is an
Table 2 Comparison between hepatitis C virus patients and the control group
HCV patients Age BMI FBG (mg/dl) PP (mg/dl) HBA1c Insulin HOMA IR Cholesterol HDL LDL TG Platelets
Mean 46.2 23.8 102 134.2 5.69 8.78 2.25 187.73 47.4 117.2 147.1 187.4SD 3.69 0.8 41.16 64.19 2.04 5.29 1.92 33.57 13.5 34.39 76.23 42.62Control group
Mean 48.7 25.2 213.7 298.9 8.4 11.56 5.85 240.07 43.74 147.8 205.3 187.53SD 5.69 0.36 43.93 77.03 1.47 7.24 3.33 47.35 11.24 36.14 59.29 34.85P value 0.110 0.000 0.000 0.000 0.000 0.171 0.001 0.001 0.261 0.006 0.003 0.990
FBG, fasting blood glucose; HCV, hepatitis C virus; HOMA IR, homeostatic model assessment test for insulin resistance; TG, triglyceride.
Table 3 Comparison between hepatitis C virus patients positive for diabetes (HOMA IRZ3) and the control group
HCV patients positive fordiabetes (HOMA IRZ3) Age BMI
FBGmg/dl PP mg/dl HBA1c Insulin
HOMAIR Cholesterol HDL LDL TG Platelets
Mean 48.08 24.43 160.25 220.33 7.90 14.47 5.08 212.42 44.21 136.29 201.79 163.04SD 3.57 0.54 48.75 80.12 2.56 6.60 2.06 43.17 10.86 43.16 77.68 52.07Control group
Mean 48.73 25.17 213.73 298.93 8.40 11.56 5.85 240.07 43.74 147.79 205.33 187.53SD 5.69 0.36 43.93 77.03 1.47 7.24 3.33 47.35 11.24 36.14 59.29 34.85P value 0.696 0.001 0.001 0.005 0.448 0.218 0.434 0.077 0.899 0.376 0.873 0.087
FBG, fasting blood glucose; HCV, hepatitis C virus; HOMA IR, homeostatic model assessment test for insulin resistance; TG, triglyceride.
Study of diabetes mellitus Raouf et al. 19
Copyright © The Egyptian Society of Internal Medicine. Unauthorized reproduction of this article is prohibited.
early event in chronic HCV infection, occurring in 20% of
nonobese patients with minimal fibrosis. Metabolic
abnormalities further exacerbate insulin resistance and
contribute toward progression of fibrosis. In contrast,
there was no association between HOMA IR values and
the presence of advanced fibrosis or a faster progression of
fibrosis [24]. Our study showed that the clinical
phenotype associated with type 2 diabetes is character-
ized by higher blood pressure, older age, higher BMI,
serum triglycerides, and lower HDL cholesterol levels
than HCV-positive patients; similar results were obtained
by Antonelli et al. [2]. We found that patients with type 2Ta
ble
4C
om
pa
riso
nb
etw
ee
nH
OM
AIR
43
(HC
V+
DM
+)
an
dH
OM
AIR
o3
(HC
V+
DM
–)
HO
MA
IR4
3(H
CV
+)
Ag
eB
MI
FB
G(m
g/d
l)P
P(m
g/d
l)H
BA
1c
Insu
linH
OM
AIR
Cho
lest
ero
lH
DL
LDL
TGP
late
lets
Sta
ge
HA
I/1
8S
teat
osi
s
Mea
n4
8.0
82
4.4
31
60
.25
22
0.3
37
.90
14
.47
5.0
82
12
.42
44
.21
13
6.2
92
01
.79
16
3.0
42
.54
9.4
27
.22
SD
3.5
70
.54
48
.75
80
.12
2.5
66
.60
2.0
64
3.1
71
0.8
64
3.1
67
7.6
85
2.0
71
.64
2.7
52
.56
HO
MA
IRo
3(H
CV
+)
Mea
n4
5.5
72
3.5
88
3.6
21
09
.24
4.8
76
.99
1.3
91
79
.93
48
.46
11
1.1
41
29
.79
19
5.2
00
.47
5.2
55
.63
SD
3.5
40
.76
8.8
81
2.7
00
.54
3.1
50
.59
25
.69
14
.11
28
.92
67
.53
36
.18
0.8
12
.97
1.7
7P
valu
e0
.00
50
.00
00
.00
00
.00
00
.00
00
.00
00
.00
00
.00
20
.12
80
.01
20
.00
00
.00
80
.00
00
.00
00
.08
1
FB
G,
fast
ing
blo
od
glu
cose
;H
CV,
hep
atiti
sC
viru
s;H
OM
AIR
,ho
meo
stat
icm
od
elas
sess
men
tte
stfo
rin
sulin
resi
stan
ce;
TG,
trig
lyce
ride;
HA
I,hi
sto
log
yac
tivity
ind
ex.
P4
0.0
5is
cons
ider
edno
nsig
nific
ant.
Po
0.0
5is
cons
ider
edsi
gni
fican
t.Po
0.0
1is
cons
ider
edhi
ghl
ysi
gni
fican
t.
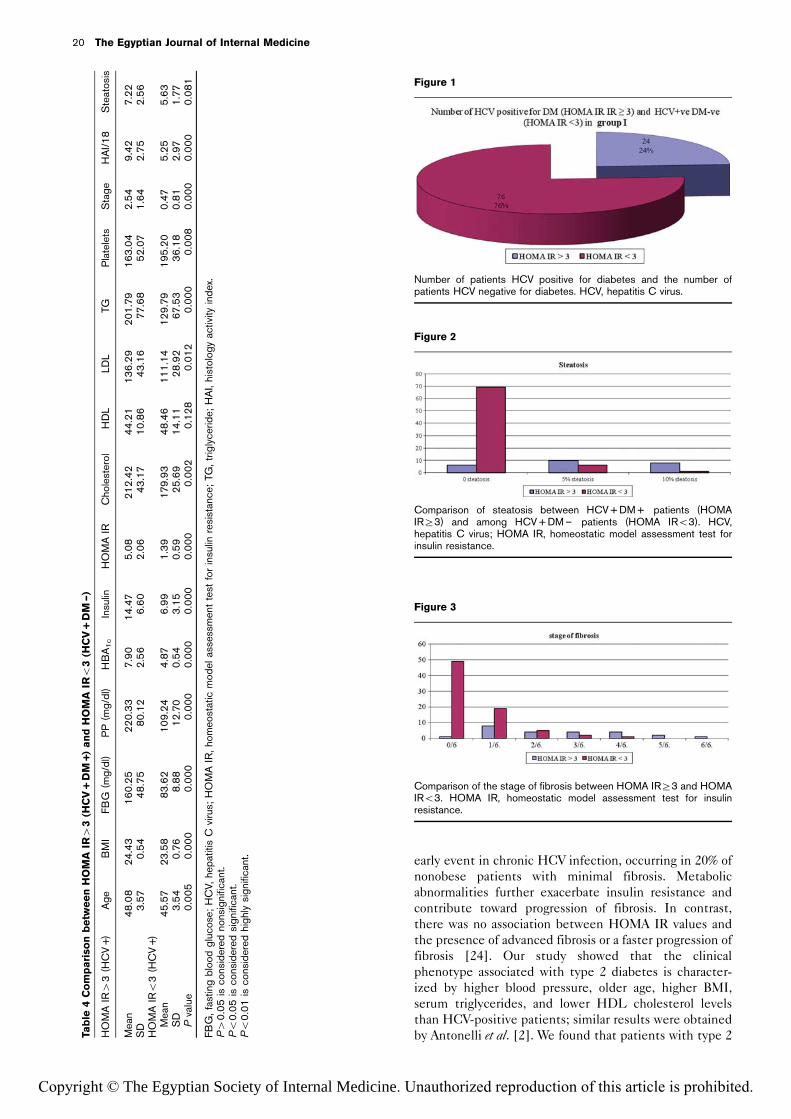
Figure 1
Number of patients HCV positive for diabetes and the number ofpatients HCV negative for diabetes. HCV, hepatitis C virus.
Figure 2
Comparison of steatosis between HCV + DM + patients (HOMAIRZ3) and among HCV + DM – patients (HOMA IRo3). HCV,hepatitis C virus; HOMA IR, homeostatic model assessment test forinsulin resistance.
Figure 3
Comparison of the stage of fibrosis between HOMA IRZ3 and HOMAIRo3. HOMA IR, homeostatic model assessment test for insulinresistance.
20 The Egyptian Journal of Internal Medicine
Copyright © The Egyptian Society of Internal Medicine. Unauthorized reproduction of this article is prohibited.

diabetes, noncirrhotic HCV positive (NC-HCV +), had
lower BMI than the type 2 diabetic control group; the
same result was obtained by Antonelli et al. [25]. In this
study, a highly significant positive correlation was found
between HOMA IR and BMI among HCV patients.
Negro et al. [23] reported that BMI is an independent
predictor of insulin resistance in HCV infection. Also, we
found a negative correlation between steatosis and BMI
in hepatitis C-positive patients, which is in agreement
with the findings of Lecube et al. [26]. Similar findings
were obtained by Castera et al. [27], who concluded that
mild steatosis may be associated with high BMI and
moderate to severe steatosis is more likely to be caused
directly by the virus, favoring liver fibrosis. We found a
significant positive correlation between HOMA IR and
steatosis and a nonsignificant positive correlation be-
tween HOMA IR and stage of fibrosis among HCV
patients, which is in agreement with the previous study
carried out by Albert et al. [1]. Also, we observed that
steatosis was higher in HCV + DM + patients (HOMA
IRZ3) than in HCV + DM – patients (HOMA IRo3).
A similar result was obtained by Machado and Cortez
Pinto [22]. Insulin resistance and diabetes can adversely
affect the course of chronic hepatitis C and lead to
enhanced steatosis, steatohepatitis, and liver fibrosis [1].
Both increased adipocity and the presence of steatosis
have been associated with a decreased rate of response to
antiviral treatment [19]. Clearance of HCV improves
insulin resistance [28]. Eradication of HCV infection
reduces the incidence of glucose abnormalities in chronic
HCV patients [29]. Insulin resistance and type 2 diabetes
not only accelerate the histological and clinical progres-
sion of chronic hepatitis C but also reduce the early and
sustained virological response to interferon-a (IFN-a)-
based therapy [23]. In contrast, IFN-a has been observed
Figure 4
Highly significant positive correlation between fasting insulin andHOMA IR HCV patients. HCV, hepatitis C virus; HOMA IR,homeostatic model assessment test for insulin resistance.
Figure 5
Significant positive correlation between fasting insulin and stage offibrosis in HCV patients. HCV, hepatitis C virus.
Figure 6
Negative correlation between steatosis and BMI in HCV patients.HCV, hepatitis C virus.
Figure 7
Correlation between HOMA IR and HCV RNA (PCR) among patients.
Figure 8
Section from liver tissue case no. 27 showing a preserved architecture(stage of fibrosis 0/6, negative steatosis) and a mild portal lymphocyticinfiltrate (Masson trichrome staining).
Study of diabetes mellitus Raouf et al. 21
Copyright © The Egyptian Society of Internal Medicine. Unauthorized reproduction of this article is prohibited.

to be associated with the development of diabetes [30].
The acute administration of IFN-a may induce some
degree of insulin resistance in both healthy individuals
and in patients with chronic hepatitis C [31].
ConclusionHCV itself can contribute toward insulin resistance, as
evidenced by high HOMA IR among HCV patients.
Insulin resistance is a predictor of the stage of fibrosis and
the rate of fibrosis progression. Insulin resistance and
diabetes increase the risk of advanced liver disease,
including steatosis, fibrosis, cirrhosis, and hepatocellular
carcinoma. Diabetic HCV-positive patients had an inter-
mediate clinical phenotype (lower BMI and LDL)
compared with the control group (HCV–DM +). A
sustained response to IFN-a-based therapy may result
in improvements in blood glucose abnormalities, insulin
resistance, and diabetes. Early antiviral therapy decreases
the risk of type 2 diabetes and progression of fibrosis in
patients with chronic hepatitis C and insulin resistance.
AcknowledgementsConflicts of interestAll members of Internal Medicine Departments of Al-Zahraa UniversityHospital, National Liver Institute and Police Authority Hospital.
References1 Albert L, Cristina H, Joan G, et al. Glucose abnormalities with hepatitis C
virus infection. Diabetes Care 2006; 29:1140.
2 Antonelli A, Ferri C, Fallahi P, Pampana A, Ferrari SM, Goglia F, et al.Hepatitis C virus infection: evidence for an association with type 2 diabetes.Diabetes Care 2005; 28:2548–2550.
3 Marcin S, Zozuliska D, Juszyk J, et al. Hepatitis C Virus infection: evidence foran association with type2 diabetes. Diabetes care 2006; 29:750.
4 Clark JM, Brancati FL, Diehl AM. Nonalcoholic fatty liver disease. Gastro-enterology 2002; 122:1649–1657.
5 Papatheodoridis GV, Chrysanthos N, Savvas S, Sevastianos V, Kafiri G,Petraki K, et al. Diabetes mellitus in chronic hepatitis B and C: prevalenceand potential association with the extent of liver fibrosis. J. Viral Hepatitis2006; 13:303–310.
6 Miyao M, Shoji M, Shinji A. Decresed plasma adiponectin concentration inwamen with dyslipidemia. J Clin Endoc and Met 2002; 87:2764–2769.
7 Abraham EG, Blisse E, Gonen E. Glycosylated hemoglobin. Chromatog1985; 81.
8 Matthews DR, Hosker JP, Rudenski AS. Homeostasis model assessment:insulin resistance and b-cell function from fasting plasma glucose and insulinconcentrations in man. Diabetologia 1985; 28:412–419.
9 Matsubara M, Chiba H, Maruoka S, Katayose S. Elevated serum leptinconcentrations in women with components of multiple risk factor clusteringsyndrome. J Atherosc Thromb 2000; 7:231–237.
10 Garcıa Pagan JC, Calleja JL, Banares R. Liver diseases [Enfermedadeshepaticas]. Gastroenterol Hepatol 2006; 29 (Suppl 3): 99–111.
11 Desmet GL, Soni A, Quinn PG. Clinical features of hepatitis C infectedpatients with persistently normal alanine transferase levels in United States.Heoatology 2000; 30:1307.
12 Thuluvath PJ, John PR. Association between hepatitis C, diabetes mellitusand race: a case-control study. Am J Gastroenterol 2003; 98:438–441.
13 Wang CS, Wang ST, Yao WJ, Chang TT, Chou P. Community-based study ofhepatitis C virus infection and type 2 diabetes: an association affected byage and hepatitis severity status. Am J Epidemiol 2003; 158:1154–1160.
14 Moriishi K, Mori Y, Matsuura Y. Processing and pathogenicity of HCV coreprotein. Uirusu J Virol 2008; 58:183–190.
15 Nagao Y, Kawasaki K, Sata M. Insulin resistance and LP in patients withhepatitis C virus infection liver diseases. J Gastroentrol Hepatol 2008;23:580–585.
16 Tsochatzis E, Manolakopoulos S, Papatheodoridis GV, Hadziyannis E,Triantos C, Zisimopoulos K, et al. Serum HCV RNA levels and HCV geno-type do not affect insulin resistance in nondiabetic patients with chronichepatitis C: a multicentre study. Alimen Pharmacol Therap 2009; 30:947–954.
17 Sougleri M, Labropoulou Karatza C, Paraskevopoulou P, Fragopanagou H,Alexandrides T. Chronic hepatitis C virus infection without cirrhosis inducesinsulin resistance in patients with b-thalassaemia major. Eur J GastroenterolHepatol 2001; 13:1195–1199.
18 Skowroski M, Zozuli D, Juszczyk D, et al. Hepatitis C virus infection: evi-dence for an association with Type 2 diabetes. Diabetes Care 2006; 29:750.
19 Bjornsson E, Angulo P. Hepatitis C and steatosis. Arch Med Res 2007;38:621–627.
20 Jason M. Insulin is associated with chronic hepatitis C virus infection fibrosisprogression. Gastoentrol 2003; 2:125.
21 Moucari R, Asselah T, Cazals Hatem D, Voitot H, Boyer N, Ripault M, et al. Insulinresistance in chronic hepatitis C: association with genotypes 1 and 4, serumHCV RNA level and liver fibrosis. Gastroenterology 2008; 134:416–423.
22 Machado MV, Cortez Pinto H. Insulin resistance and steatosis in chronichepatitis C. Ann Hepatol 2009; 8 (Suppl. 1): S67–S75.
23 Negro F, Alaei M. Hepatitis C virus and type 2 diabetes. World J Gastro-enterol 2009; 15:1537–1547.
24 Merchante N, Macıas J, Ramayo E, Vergara S, Garcıa Garcıa JA, Mira JA, et al.Insulin resistance is not associated with liver fibrosis progression in HIV/hepatitis C virus-coinfected patients. J Viral Hepatitis 2006; 13:449–456.
25 Antonelli A, Ferri C, Fallahi P, Sebastiani M, Nesti C, Barani L, et al. Type 2diabetes in hepatitis C-related mixed cryoglobulinaemia patients. Rheuma-tology 2004; 43:238–240.
26 Lecube A, Hernandez C, Genesca J, Simo R. Proinflammatory cytokines,insulin resistance and insulin secretion in chronic hepatitis C patients: acase-control study. Diabetes Care 2006; 29:1096–1101.
27 Castera L, Chouteau P, Hezode C, Zafrani ES, Dhumeaux D, Pawlotsky JM.Hepatitis C virus-induced hepatocellular steatosis. Am J Gastroenterol2005; 100:711–715.
28 Kawaguchi T, Ide T, Taniguchi E, Hirano E, Itou M, Sumie S, et al. Clearanceof HCV improves insulin resistance, beta-cell function and hepatic expres-sion of insulin receptor substrate 1 and 2. Am J Gastroenterol 2007;102:570–576.
29 Simo R, Lecube A, Genesca J, Esteban JI, Hernandez C. Sustained vir-ological response correlates with reduction in the incidence of glucose ab-normalities in patients with chronic hepatitis C virus infection. Diabetes Care2006; 29:2462–2466.
30 Azocar J. Adult onset diabetes mellitus in hepatitis C virus infection. 2003;Available at: http://www.hcvadvocate.org/hcsp/articles/Azocar-1.html.
31 Shaw RJ, Lamia KA, Vasquez D, Koo SH, Bardeesy N, DePinho RA, et al.Medicine: the kinase LKB1 mediates glucose homeostasis in liver andtherapeutic effects of metformin. Science 2005; 310:1642–1646.
22 The Egyptian Journal of Internal Medicine
Copyright © The Egyptian Society of Internal Medicine. Unauthorized reproduction of this article is prohibited.

Study of diabetes mellitus Raouf et al. 23
Copyright © The Egyptian Society of Internal Medicine. Unauthorized reproduction of this article is prohibited.