slide 1 fosamax ™ once weekly actonel ™ once a week comparison trial fosamax™ (alendronate) is...
Post on 18-Dec-2015
218 views
TRANSCRIPT

Slide 1
FOSAMAX™ Once Weekly
ACTONEL™ Once A Week Comparison
Trial
FOSAMAX™ (alendronate) is a trademark of Merck & Co., Inc, Whitehouse Station, NJ, USA.
ACTONEL™ (risedronate) is a trademark of Procter & Gamble Pharmaceuticals.

Slide 2
IntroductionIntroduction• Both alendronate and risedronate are commonly used
bisphosphonates for the treatment of postmenopausal osteoporosis
• Head-to-head clinical trial data are needed to help clinicians make decisions regarding these treatment options for postmenopausal women with osteoporosis
Adapted from National Osteoporosis Foundation. Physician's Guide to Prevention and Treatment of Osteoporosis. Washington, DC: National Osteoporosis Foundation; 2003; Cummings SR et al JAMA 1998;280(24):2077–2082; Black DM et al J Clin Endocrinol Metabol 2000;85(11):4118–4124; Reginster J et al Osteoporos Int 2000;11(1):83–91; Harris ST et al JAMA 1999;282(14):1344–1352; McAlister FA et al JAMA 1999;282(14):1371–1377.

Slide 3
How Bisphosphonates Work How Bisphosphonates Work in Osteoporosisin Osteoporosis
Adapted from Rodan GA, Fleisch HA J Clin Invest 1996;97:2692–2696; Chesnut CH III et al Am J Med 1995;99:144–152; Garnero P et al J Clin Endocrinol Metab 1994;79(6):1693–1700; Wasnich RD, Miller PD J Clin Endocrinol Metab 2000;85(1):231–236; Chavassieux PM et al J Clin Invest 1997;100(6):1475–1480; Adami S Bone 1995;17(4):383–390.
Altered microarchitecture and mineralization
Bone Turnover
Bone MineralDensity
FractureRiskBone
Strength

Slide 4
FOSAMAXFOSAMAX™™ ACTONEL ACTONEL™™ Comparison Comparison Trial (FACT) Study DesignTrial (FACT) Study Design
• FOSAMAX Once Weekly vs. ACTONEL Once A Week • Randomized, double-blind, double-dummy,
active-comparator study
• 1053 postmenopausal women from 78 US sitesrandomized (1:1) to– alendronate 70 mg (n = 520) and risedronate placebo
or– risedronate 35 mg (n = 533) and alendronate placebo
• Calcium ≥1000 mg and vitamin D 400 IU daily
• Central Lab and Quality Assurance centers used for all lab and DXA evaluations (DXA at 0, 6, and12 months)DXA=dual-energy x-ray absorptiometry
FOSAMAX™ (alendronate) is a trademark of Merck & Co., Inc, Whitehouse Station, NJ, USA.ACTONEL® (risedronate) is a registered trademark of Procter & Gamble Pharmaceuticals.

Slide 5
Entry CriteriaEntry Criteria
• Community-dwelling, ambulatory women
40 years of age (25 years if surgically menopausal) and 6 months postmenopausal
• Osteoporosis (BMD T-score –2.0) at either the trochanter, femoral neck, total hip, or lumbar spine
• No bisphosphonates within previous year or for more than two years within past five years
• No estrogen or estrogen analogues (SERMs) within the previous six months, or PTH within the previous year
• No abnormality of the esophagus that would delay emptying (i.e., stricture, achalasia)
SERMs=selective estrogen receptor modulators; PTH=parathyroid hormone

Slide 6
Study EndpointsStudy Endpoints
• Primary– Hip trochanter BMD at 12 months
• Secondary– Total hip, femoral neck, and lumbar spine BMD at 12
months – Biochemical markers of bone turnover (serum BSAP,
P1NP, CTx, and urinary NTx) at 3, 6, and 12 months – Percentage of patients with BMD gains 0% and 3%– Change in BMD at all sites at 6 months– Tolerability and safety profile, including percentage of
patients with any upper-GI adverse events at 12 months
BMD=bone mineral density; BSAP=serum bone-specific alkaline phosphatase; P1NP=N-terminal Propeptide of type 1 Procollagen; CTx=serum C-telopeptide; NTx=N-telopeptide corrected for creatinine; GI=gastrointestinal
Slide 7
Statistical MethodsStatistical Methods
• Primary analysis for BMD – Modified intention-to-treat (mITT)
• Primary analysis for biochemical markers– Per protocol (PP)
• 90% power to detect a 1.2% difference between alendronate and risedronate at a statistically significant alpha level of 0.05

Slide 8
454 completed (85.2%)438 completed (84.2%)
Patient AccountingPatient Accounting
1759 patients screened
706 excluded
Alendronate 520 randomized
515 treated
Risedronate 533 randomized
527 treated
82 discontinued (15.8%)Clinical adverse event=33 (6.3%)Lost to follow-up=14Moved=4Withdrew consent=29Deviation from protocol=2Lab adverse event=0
79 discontinued (14.8%)Clinical adverse event=33 (6.2%)Lost to follow-up=9Moved=3Withdrew consent=28Deviation from protocol=5Lab adverse event=1
1053 patients randomized

Slide 9
Baseline DemographicsBaseline Demographics
Alendronate70 mg OW
(n=520)
Risedronate 35 mg OW
(n=533)Total
(n=1053)
Age (years) 64.2 64.8 64.5
Years since menopause 18.3 18.7 18.5
Race (% Caucasian) 94.4 96.1 95.3
Upper-GI disorder (%)
Fracture* after age 45 (%)
125 (24)
60 (11.5)
139 (26.1)
66 (12.4)
264 (25.1)
126 (12.0)
*Hip, spine or wrist
OW=once weekly

Slide 10
Baseline BMD T-scoresBaseline BMD T-scores**
SiteAlendronate
(n=520)Risedronate
(n=533)Total
(n=1053)
Trochanter –1.58 –1.58 –1.58
Total hip –1.76 –1.78 –1.77
Femoral neck –2.12 –2.16 –2.14
Lumbar spine –2.26 –2.23 –2.24
*mean scores
Slide 11
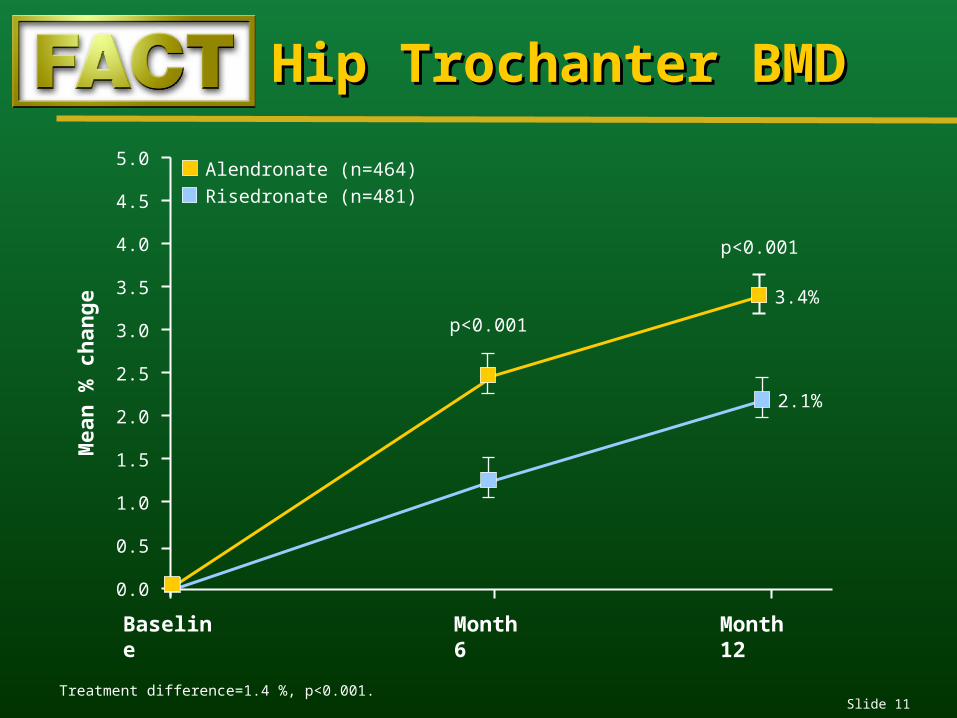
Hip Trochanter BMDHip Trochanter BMD
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Baseline Month 6 Month 12
p<0.001
3.4%
2.1%
Mea
n %
ch
ang
e
p<0.001
Treatment difference=1.4 %, p<0.001.
Alendronate (n=464)
Risedronate (n=481)
Slide 12
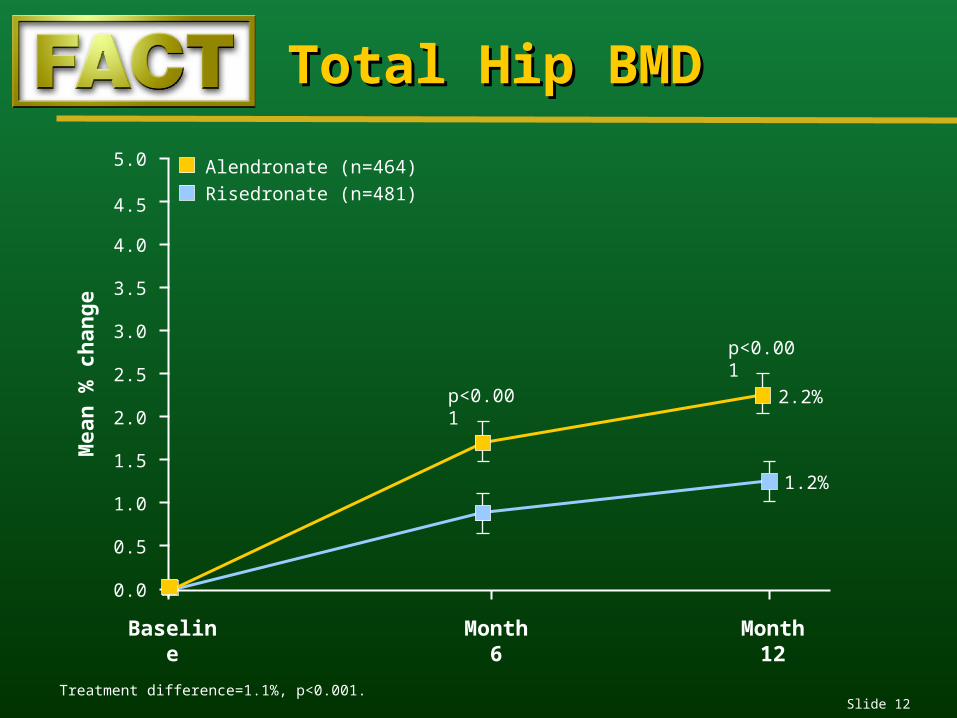
Total Hip BMDTotal Hip BMD
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Baseline Month 6 Month 12
p<0.001 2.2%
1.2%
Mea
n %
ch
ang
e
p<0.001
Treatment difference=1.1%, p<0.001.
Alendronate (n=464)
Risedronate (n=481)

Slide 13
Femoral Neck BMDFemoral Neck BMD
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Baseline Month 6 Month 12
p=0.0351.6%
0.9%
Mea
n %
ch
ang
e
p=0.005
Treatment difference=0.7%, p=0.005.
Alendronate (n=464)
Risedronate (n=481)

Slide 14
Lumbar Spine BMDLumbar Spine BMD
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
Baseline Month 6 Month 12
p=0.002
3.7%
2.6%
Mea
n %
ch
ang
e
p<0.001
Treatment difference=1.2 %, p<0.001.
Alendronate (n=464)
Risedronate (n=481)

Slide 15
BMD Response at Lumbar BMD Response at Lumbar SpineSpine
0
100
20
40
60
80
% Change in BMD
% P
atie
nts
–3%
4%1%
p=0.008
0%
87%
76%
p<0.001
3%
60%
41%
p<0.001
5%
35%
23%
p<0.001
Alendronate (n=464)
Risedronate (n=481)

Slide 16
% P
atie
nts
% Change in BMD
0
100
20
40
60
80
85%
68%
51%
41%
31%
20%
5%
11%
p=0.002
p<0.001
p<0.001
p<0.001
–3% 0% 3% 5%
BMD Response at Hip BMD Response at Hip TrochanterTrochanter
Alendronate (n=464)
Risedronate (n=481)

Slide 17
Bone Resorption MarkersBone Resorption Markers
–100
–80
–60
–40
–20
0
Baseline Month 6 Month 12
Mea
n %
ch
ang
e
Urine NTx Serum CTx
p<0.001
p<0.001 –40%
–53% –55%
–74%
p<0.001
p<0.001
Month 3
p<0.001
Treatment difference 13%
p<0.001
Treatment difference 19%
Alendronate n = 442 429 414 365 449 443 423 382Risedronate n = 457 449 426 375 459 455 433 387
Alendronate 70 mg OW Risedronate 35 mg OW
–100
–80
–60
–40
–20
0
Baseline Month 6 Month 12Month 3

Slide 18
Bone Formation MarkersBone Formation Markers
Serum BSAP Serum P1NP
p<0.001
p<0.001
–28%
–41%–48%
–64 %p<0.001
p<0.001
Treatment difference 13%
p<0.001
p<0.001
Treatment difference 16%
Alendronate n = 449 441 422 382 447 440 419 378Risedronate n = 458 454 430 387 459 455 432 387
–100
–80
–60
–40
–20
0
Baseline Month 6 Month 12
Mea
n %
ch
ang
e
Month 3
–100
–80
–60
–40
–20
0
Baseline Month 6 Month 12Month 3
Alendronate 70 mg OW Risedronate 35 mg OW

Slide 19
Adverse ExperiencesAdverse Experiences
Number (%) of patients
Alendronate 70 mg OW
(n=515)
Risedronate 35 mg OW
(n=527)
1 clinical adverse experience 394 (76.5) 399 (76.1)
Serious adverse experience 45 (8.7) 41 (7.8)
Discontinued due to adverse experience 33 (6.4) 33 (6.3)
No significant differences between treatment groups

Slide 20
UGI Adverse ExperiencesUGI Adverse Experiences
No significant differences between treatment groups
Number (%) of patients
Alendronate 70 mg OW
(n=515)
Risedronate 35 mg OW
(n=527)
1 Upper-GI adverse experience 116 (22.5) 106 (20.1)
Discontinued due to upper-GI
adverse experience 13 (2.5) 16 (3.0)

Slide 21
SummarySummary• At 6 and 12 months, alendronate produced significantly
greater BMD increases at hip trochanter,* total hip,* femoral neck,** and lumbar spine*** than did risedronate
• Greater decreases in indices of bone turnover (BSAP, P1NP, CTx, and urinary NTx) were seen with alendronate as compared to risedronate at 3, 6, and 12 months
• Significantly more patients experienced gains in BMD≥3% at the hip trochanter (p=0.002) and lumbar spine (p<0.001) with alendronate than with risedronate
• Overall (including upper-GI) safety profile and tolerability of alendronate and risedronate were similar
*p<0.001 at months 6 and 12; **p=0.035 at month 6 and p=0.005 at month 12; ***p=0.002 at month 6 and p<0.001 at month 12

Slide 22
ConclusionsConclusions
• In this head-to-head study, alendronate 70 mg OW produced larger increases in BMD and greater reductions in markers of bone turnover than did risedronate 35 mg OW.
• The superior antiresorptive effect of alendronate was seen as early as three months.
• These results are consistent with results of previous clinical trials and are important for physicians to consider when evaluating treatment options for postmenopausal women with osteoporosis.
Adapted from McAlister FA et al JAMA 1999;282(14):1371–1377; Hosking D et al Curr Med Res Opin 2003;19:383–394; Cranney A et al Endocr Rev 2002;23(4):570–578.

Slide 23
ReferencesReferences1. National Osteoporosis Foundation. Osteoporosis: Physician's Guide to Prevention and Treatment of Osteoporosis. Washington, DC:
National Osteoporosis Foundation; 2003.
2. Cummings SR, Black DM, Thompson DE et al, for the Fracture Intervention Trial Research Group. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: Results from the Fracture Intervention Trial. JAMA 1998;280(24):2077–2082.
3. Black DM, Thompson DE, Bauer DC et al, for the FIT Research Group. Fracture risk reduction with alendronate in women with osteoporosis: The Fracture Intervention Trial. J Clin Endocrinol Metab 2000;85(11):4118–4124.
4. Reginster J, Minne HW, Sorensen OH et al. Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos Int 2000;11(1):83–91.
5. Harris ST, Watts NB, Genant HK et al. Effects of risedronate treatment on vertebral and nonvertebral fractures in women with postmenopausal osteoporosis: A randomized controlled trial. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. JAMA 1999;282(14):1344–1352.
6. Schnitzer T, Bone, H, Crepaldi G et al. Therapeutic equivalence of alendronate 70 mg once weekly and alendronate 10 mg daily in the treatment of osteoporosis. Aging (Milano) 2000;12(1):1–12.
7. Brown JP, Kendler DL, McClung MR et al. The efficacy and tolerability of risedronate once a week for the treatment of postmenopausal osteoporosis. Calcif Tissue Int 2002;71(2):103–111.
8. McAlister FA, Laupacis A, Wells GA et al. Users' Guides to the Medical Literature: XIX. Applying clinical trial results B. Guidelines for determining whether a drug is exerting (more than) a class effect. JAMA 1999;282(14):1371–1377.
9. Hosking D, Adami S, Felsenberg D et al. Comparison of change in bone resorption and bone mineral density with once-weekly alendronate and daily risedronate. Curr Med Res Opin 2003;19:383–394.
10. Rosen, CJ, Hochberg M, Bonnick S et al. Treatment with once-weekly alendronate 70 mg compared to once-weekly risedronate 35 mg in women with postmenopausal osteoporosis: A randomized, double-blind study. J Bone Min Res Web First September 29, 2004; 1–51.
11. Data on file, MSD ____________.

Slide 24
References (cont’d)References (cont’d)12. Rodan GA, Fleisch HA. Bisphosphonates: Mechanisms of action. J Clin Invest 1996;97:2692–2696.
13. Chesnut CH III, McClung MR, Ensrud KE et al. Alendronate treatment of the postmenopausal osteoporotic woman: Effect of multiple dosages on bone mass and bone remodeling. Am J Med 1995;99:144–152.
14. Garnero P, Shih WJ, Gineyts E et al. Comparison of new biochemical markers of bone turnover in late postmenopausal osteoporotic women in response to alendronate treatment. J Clin Endocrinol Metab 1994;79(6):1693–1700.
15. Wasnich RD, Miller PD. Antifracture efficacy of antiresorptive agents are related to changes in bone density. J Clin Endocrinol Metab 2000;85(1):231–236.
16. Chavassieux PM, Arlot ME, Reda C et al. Histomorphometric assessment of the long-term effects of alendronate on bone quality and remodeling in patients with osteoporosis. J Clin Invest 1997;100(6):1475–1480.
17. Adami S, Passeri M, Ortolani S et al. Effects of oral alendronate and intranasal salmon calcitonin on bone mass
and biochemical markers of bone turnover in postmenopausal women with osteoporosis. Bone 1995;17(4):383–390.
18. Cranney A, Guyatt G, Griffith L et al. Meta-analyses of therapies for postmenopausal osteoporosis. IX: Summary of meta-analyses of therapies for postmenopausal osteoporosis. Endocr Rev 2002;23(4):570–578.

FACT FACT ((FFOSAMAX™ OSAMAX™ AACTONELCTONEL®®
CComparison omparison TTrial)rial)Year-1 ResultsYear-1 Results
Before prescribing, please consult the manufacturers’
prescribing information.
Merck does not recommend the use of any product
in any different manner than as described
in the prescribing information.
Copyright © 2004 Merck & Co., Inc., Whitehouse Station, NJ, USA.All rights reserved. 10-05 FSM 2004-W-7082-SS
VISIT US ON THE WORLD WIDE WEB AT http://www.merck.com