short-bowel-syndromemucosalimmunology.ch/images/content/ppt-presentations_free_access/... · bc...
TRANSCRIPT
BC 2019 R.Wiest 1
Klinik für Viszerale Chirurgie und Medizin
Short-Bowel-Syndrome
Reiner Wiest M.D.
Michele Leuenberger, M.D.
BC 2019 R.Wiest 2
Klinik für Viszerale Chirurgie und Medizin
Content – Outline – Topics - Highlights
Definition
Epidemiology
Etiology, Physiology
Classification-systems
Clinical, diagnostic Issues
Therapy
…………..
BC 2019 R.Wiest 3
Klinik für Viszerale Chirurgie und Medizin
Small intestine: normal length ?
Definition of short bowel syndrome – SBS
Small intestine: 275 cm – 850 cm normal range
shorter in women and hence SBS more frequent in women (67%)
< 200 cm remaining functional short bowel
usually results in short bowel syndrome:
Bryant 1924 ESPEN Clinical Nutrition 2015
SBS is a malabsorptive condition characterized by the inability
to maintain protein-energy, fluid, electrolyte or micronutrient balances
when on a conventionally accepted, normal diet.
SBS is the main mechanism (accounting for 75%) of chronic intestinal failure (IF)
BC 2019 R.Wiest 4
Klinik für Viszerale Chirurgie und Medizin
Definition of intestinal failure ?
reduction in gastrointestinal function
below the minimum necessary for the absorption of
macornutrients a/o water and electrolytes such that
intravenous supplementation is required
to maintain health/growth
BC 2019 R.Wiest 5
Klinik für Viszerale Chirurgie und Medizin
Epidemiology, incidence, prevalence of SBS
True incidence is not known (in europe, switzerland)
Neonatal incidence overall 24.5 per 100.000 live birth
Adults: 9/1.ooo.ooo/year 1
:
Prevalence HPE: 5-80/1Mio; Incidence 7.7-15 /1Mio/year
50-70% can be weaned off from HPE long-term, but
Case fatality rate up to 30% as well1Lal: Aliment Pharmocol Therapeut 20062Clin Nutr 2018;37:1798-1809.
DiBaise JK et al. Am J Gastroenterol 2004;99:1386-95

BC 2019 R.Wiest 6
Klinik für Viszerale Chirurgie und Medizin
Most common causes of short bowel syndrome
pathophysiological groups –
Short-bowel:
Parenchymal disease
Fistula
Motility disorder
Mechanical Obstruction
Malabsorption due to
=reduced absorptive
/functional mucosal surface
Feed related exacerbation of symptoms
=restriction of oral/enteral nutrition

BC 2019 R.Wiest 7
Klinik für Viszerale Chirurgie und Medizin
Most common causes of short bowel syndrome
examples for parenchymal/ SBS
Short-bowel: 75% in adults Parenchymal disease (5%):
Extensive surgical resection for:
Mesenteric infarction/thrombosis
Crohn's disease
Surgical complications
Intestinal volvulus, Intussusception
Familial polyposis
Abdominal trauma
…….
Radiation enteritis
Coeliac disease
Immunodeficiency
Crohn's disease
Lymphangectasia
Radiation enteritis
Tufting enteropathy
Autoimmune enteropathy
Microvillus atrophy
Others
BC 2019 R.Wiest 8
Klinik für Viszerale Chirurgie und Medizin
Most common causes of short bowel syndrome
examples for motility/obstruction-group
Motility disorder (20%): Mechanical obstruction:
Acute: critical illness due to post-operative,
systemic inflammatory, neurological reactions…..
acute colonic non-mechanical obstruction
Chronic Intestinal Pseudo-Obstruction
Primary/idiopathic (with no underlying disorder)
Neuropathic: inflammatory or degenerative
Myopathic: damage of the smooth muscle
familial visceral myopathy mostly type 3
Endocrine: diabetes, HPT, ….
Medications…
«frozen» abdomen
«bowel rest» due to
Obturation
Tumors, intussusception,
Gallstones, foreign bodies, …
Intrinsic bowel lesions
stenosis or strictures:
- neoplastic,
- inflammatory bowel disease
- chemical,
- anastomotic
BC 2019 R.Wiest 9
Klinik für Viszerale Chirurgie und Medizin
High-output fistula is defined as ?
> 500ml /day in fasted condition via fistula
Fistula (2-5%):
Exogenous aetiology: (75-85%)
Post-surgically
Endogenous etiology (15-25%)
crohn^s disease, irradiation, malignancy……
Fistula – groups and examples ?
BC 2019 R.Wiest 10
Klinik für Viszerale Chirurgie und Medizin
Pediatric/children special causes, e.g. congenital….
Congenital defects of glycosylation, primary bile acid malabsorption,
Glucose-galactose malabsorption,
Gastroschisis
Nectrotizing enteritis
Midgut volvolus
Intestinal atresia
Microvillous inclusion disease and intestinal
Epithelial dysplasia
………………………………………
BC 2019 R.Wiest 11
Klinik für Viszerale Chirurgie und Medizin
FKl 11
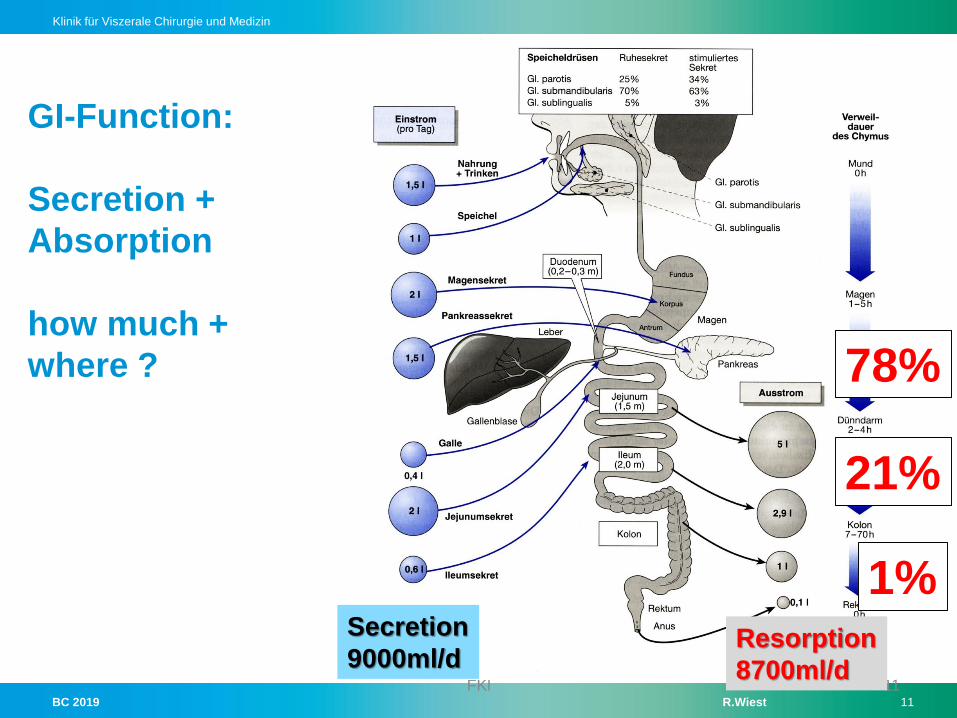
GI-Function:
Secretion +
Absorption
how much +
where ? 78%
21%
1%Secretion
9000ml/dResorption
8700ml/d
BC 2019 R.Wiest 12
Klinik für Viszerale Chirurgie und Medizin
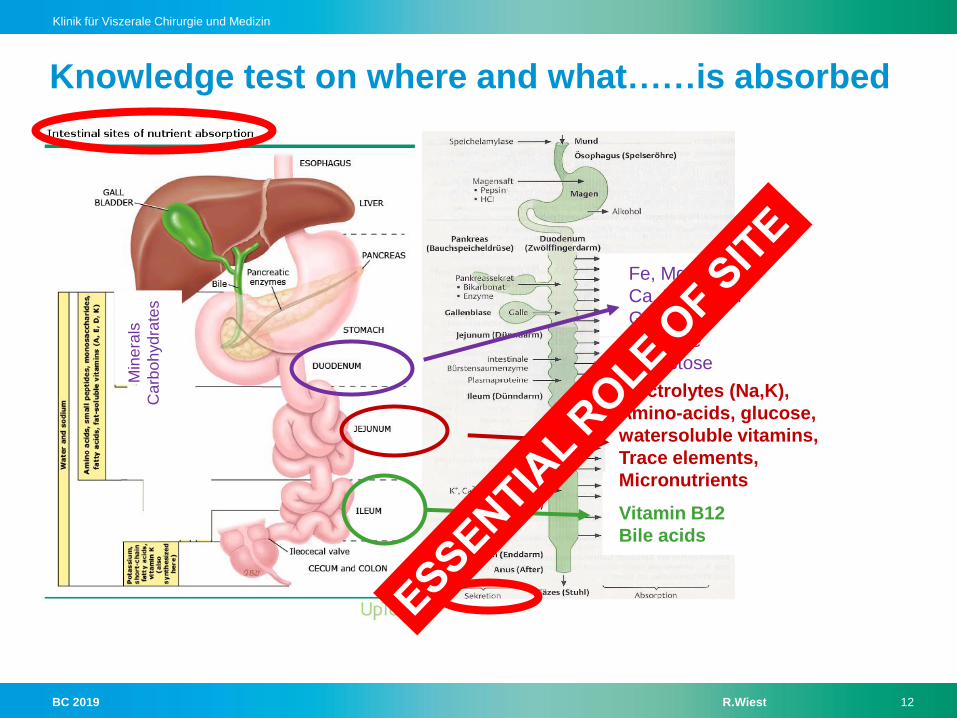
Knowledge test on where and what……is absorbed
Fe, Mg, Zn, P
Ca, Folic acid
Glucose
Fructose
Galactose
Min
era
ls
Carb
oh
yd
rate
s
Electrolytes (Na,K),
Amino-acids, glucose,
watersoluble vitamins,
Trace elements,
Micronutrients
Vitamin B12
Bile acids
BC 2019 R.Wiest 13
Klinik für Viszerale Chirurgie und Medizin
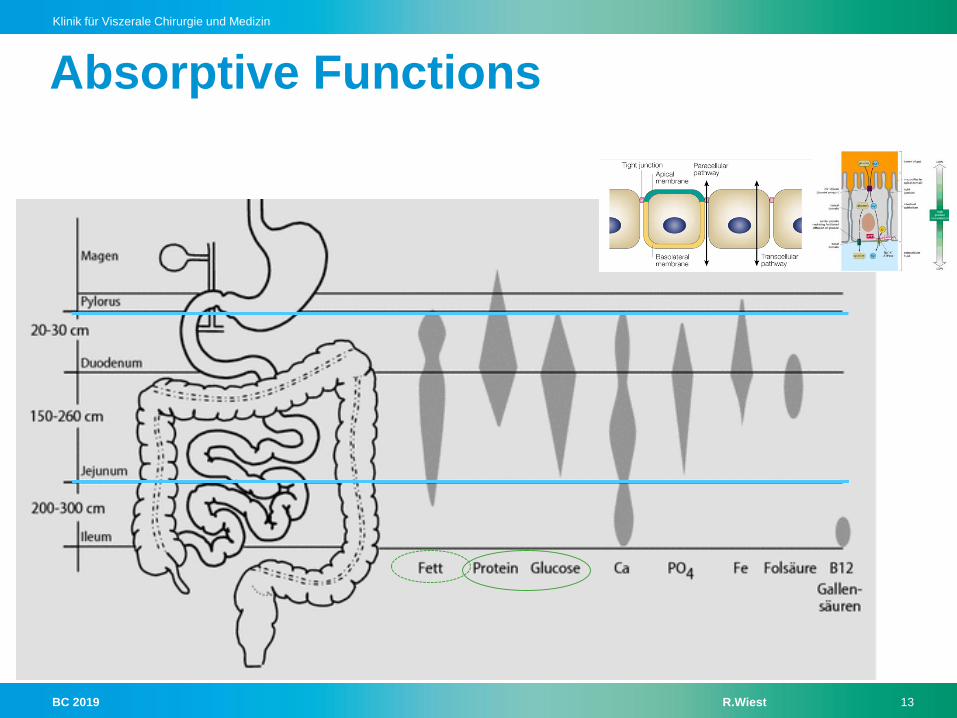
Absorptive Functions
BC 2019 R.Wiest 14
Klinik für Viszerale Chirurgie und Medizin
Ileum: different from Jejunum also as for ………. ?
Inter-cellular junctions:
Water + sodium flux:
Fluid reabsorption:
Capacity for adaptation:
Tighter than in upper GI-tract
less para-cellular permeability
Less flux than in upper GI-tract
Substantially higher – concentrating content
also due to active NaCl-transport
Greater than in upper GI-tract
BC 2019 R.Wiest 15
Klinik für Viszerale Chirurgie und Medizin
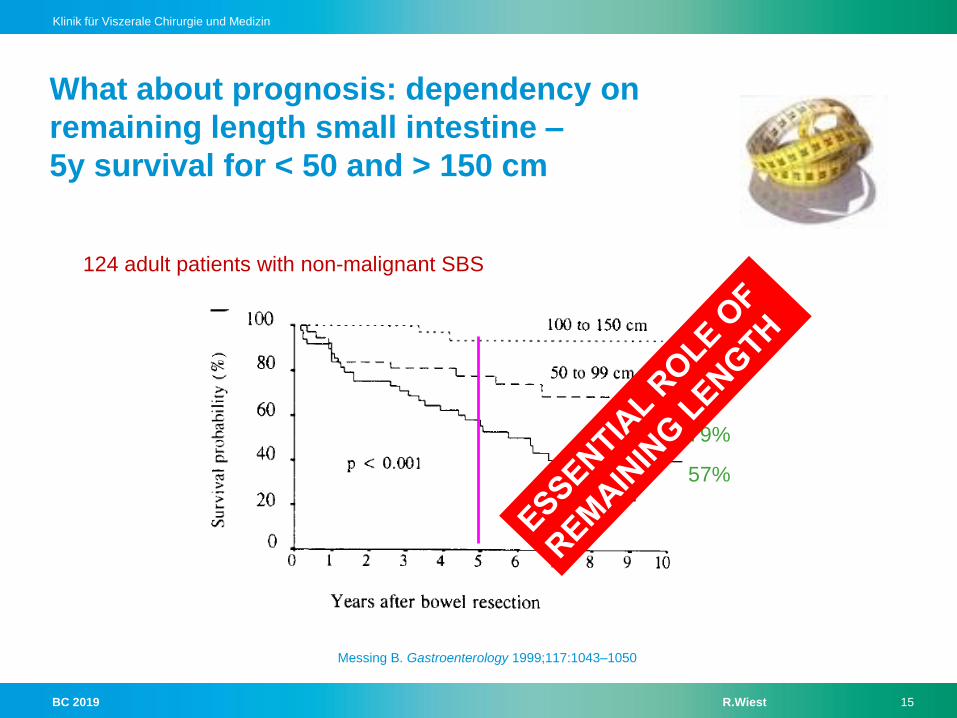
What about prognosis: dependency on
remaining length small intestine –
5y survival for < 50 and > 150 cm
124 adult patients with non-malignant SBS
93%
79%
57%
Messing B. Gastroenterology 1999;117:1043–1050
BC 2019 R.Wiest 16
Klinik für Viszerale Chirurgie und Medizin
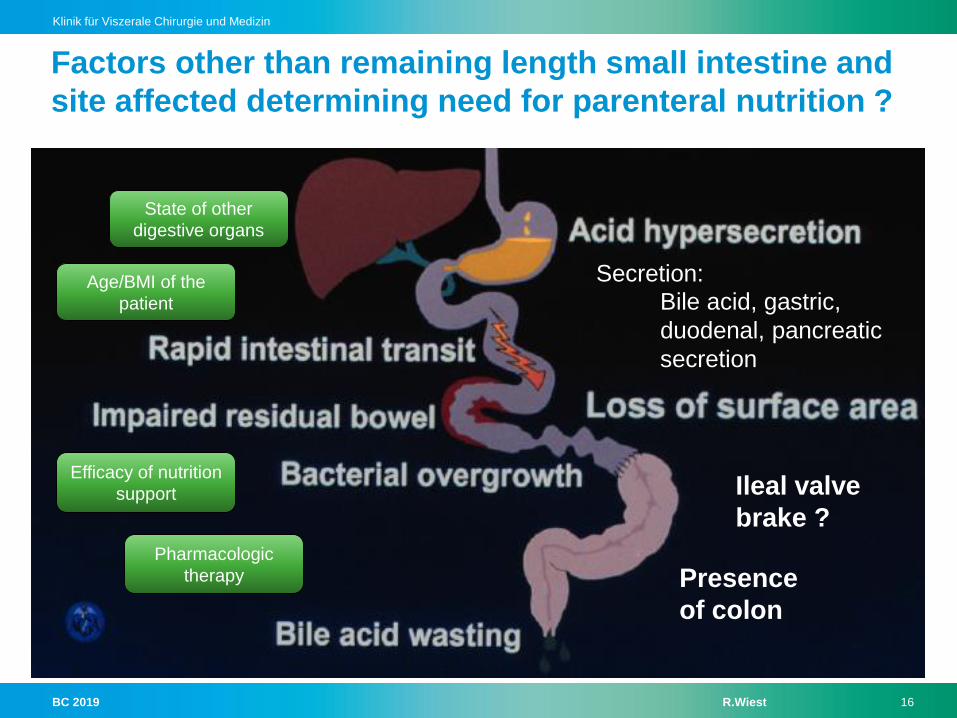
Factors other than remaining length small intestine and
site affected determining need for parenteral nutrition ?
Secretion:
Bile acid, gastric,
duodenal, pancreatic
secretion
Presence
of colon
Ileal valve
brake ?
State of other
digestive organs
Age/BMI of the
patient
Efficacy of nutrition
support
Pharmacologic
therapy

BC 2019 R.Wiest 17
Klinik für Viszerale Chirurgie und Medizin
What is the «ileal brake» and
how does it work ?
Peptide YY (and Enteroglukagon, Neurotensin)
released from L-cells in distal ileum
do slow gastric emptying and tansit-time
Loss of distal ileum
= loss of those hormones
= loss of feedback inhibition
-> transit-time faster, loss of fluids and nutrients bigger
-> colonic bacteria can colonize small intestine,
worsening diarrhoe and nutrient loss
Intact valve:
Chyme more time in
Small intestine =
Contact with
aborptive mucosa
BC 2019 R.Wiest 18
Klinik für Viszerale Chirurgie und Medizin
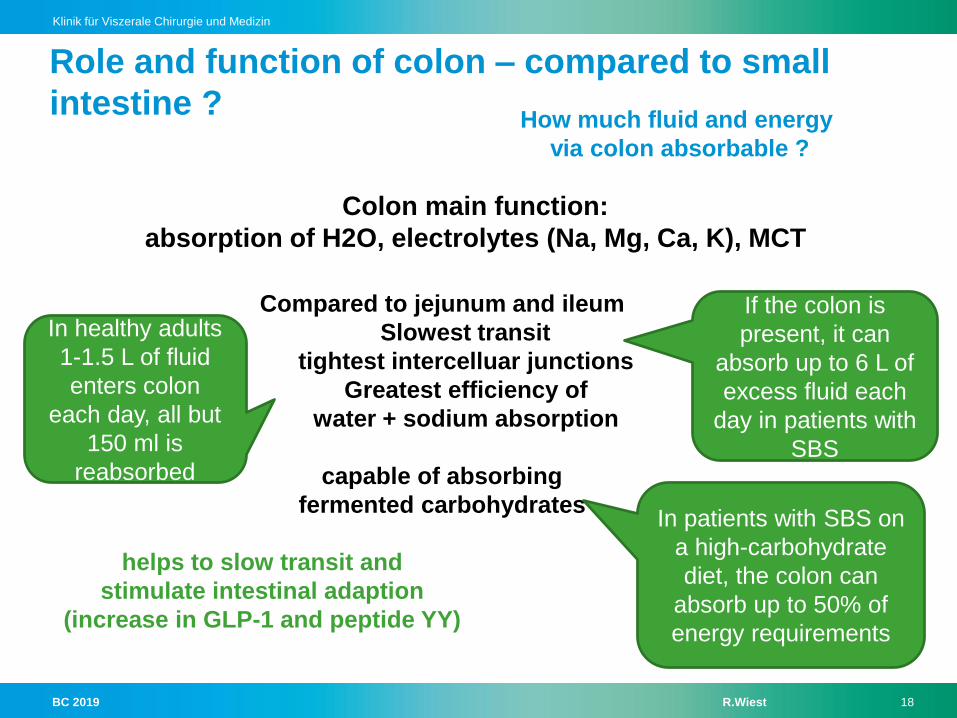
Role and function of colon – compared to small
intestine ?
Colon main function:
absorption of H2O, electrolytes (Na, Mg, Ca, K), MCT
Compared to jejunum and ileum
Slowest transit
tightest intercelluar junctions
Greatest efficiency of
water + sodium absorption
capable of absorbing
fermented carbohydrates
In healthy adults
1-1.5 L of fluid
enters colon
each day, all but
150 ml is
reabsorbed
helps to slow transit and
stimulate intestinal adaption
(increase in GLP-1 and peptide YY)
How much fluid and energy
via colon absorbable ?
If the colon is
present, it can
absorb up to 6 L of
excess fluid each
day in patients with
SBS
In patients with SBS on
a high-carbohydrate
diet, the colon can
absorb up to 50% of
energy requirements

BC 2019 R.Wiest 19
Klinik für Viszerale Chirurgie und Medizin
Increasing colonic water
absorption as much as 5-
times ist normal capacity
Resident bacteria capacity
to metabolize undigested
CHO into SCFA- which are
preferred fuel source for
coloncytes & body
Increasing incidence of
urinary calcium oxalate stone
formation
Small intestinal
bacterial overgrowth
Po
sit
ive
Ne
ga
tive
Positive/negative effects if colon is preserved ?
BC 2019 R.Wiest 20
Klinik für Viszerale Chirurgie und Medizin
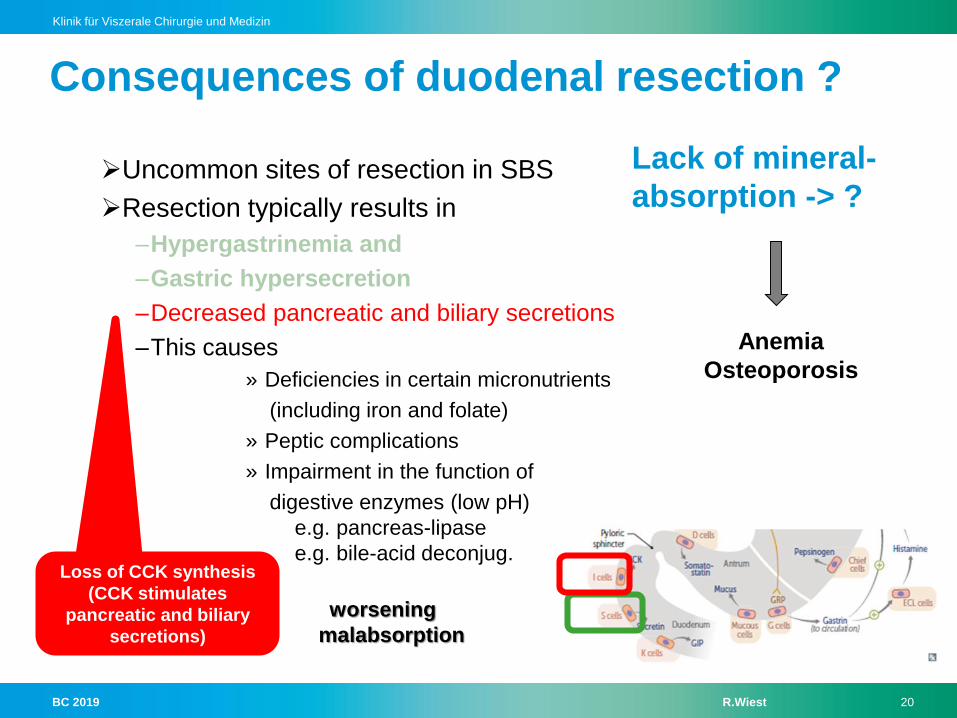
Uncommon sites of resection in SBS
Resection typically results in
–Hypergastrinemia and
–Gastric hypersecretion
–Decreased pancreatic and biliary secretions
–This causes
» Deficiencies in certain micronutrients
(including iron and folate)
» Peptic complications
» Impairment in the function of
digestive enzymes (low pH)
e.g. pancreas-lipase
e.g. bile-acid deconjug.
worsening
malabsorption
Negative feedback for
inhibiting gastrin secretion
and reducing gastric acid
production is removed
Loss of CCK synthesis
(CCK stimulates
pancreatic and biliary
secretions)
Consequences of duodenal resection ?
Lack of mineral-
absorption -> ?
Anemia
Osteoporosis
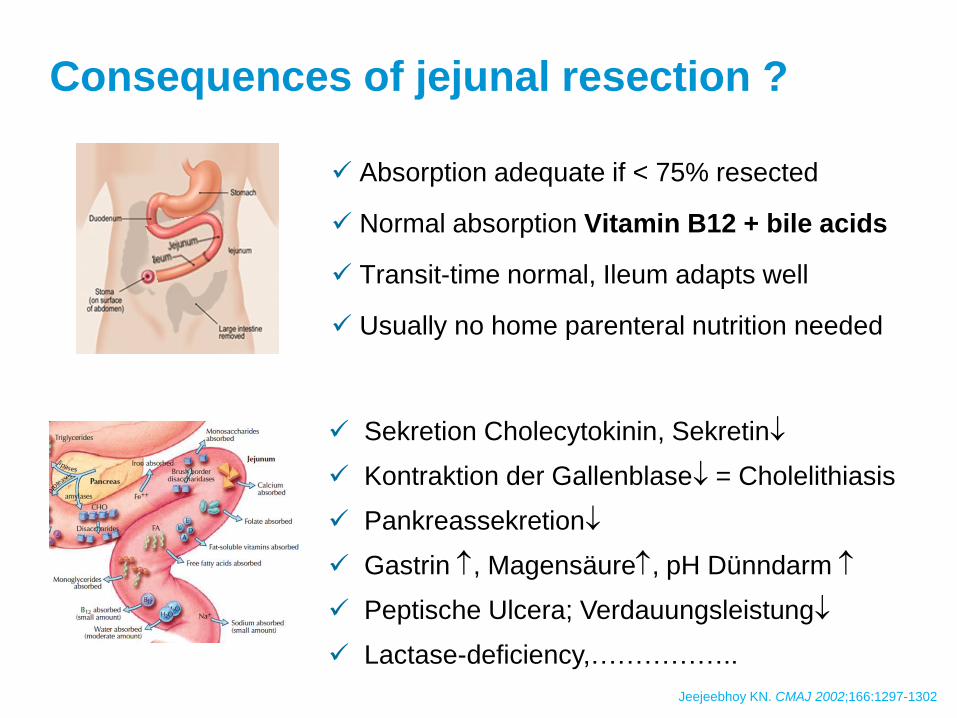
Absorption adequate if < 75% resected
Normal absorption Vitamin B12 + bile acids
Transit-time normal, Ileum adapts well
Usually no home parenteral nutrition needed
Jeejeebhoy KN. CMAJ 2002;166:1297-1302
Consequences of jejunal resection ?
Sekretion Cholecytokinin, Sekretin
Kontraktion der Gallenblase = Cholelithiasis
Pankreassekretion
Gastrin , Magensäure, pH Dünndarm
Peptische Ulcera; Verdauungsleistung
Lactase-deficiency,……………..

Jejunum less capacity to adapt
Resection > 25cm: chologenic diarrhoe
Resection > 50 cm Vitamin B12-Malabsorption with
inadequate energy- and fluid-absorption
> 100cm: Steatorrhoe (Vitamines A,D,E,K!)
Bacterial overgrowth
Messing B. Gastroenterol. 1999; 117:1043-1059
Consequences of
ileum resection ?

BC 2019 R.Wiest 23
Klinik für Viszerale Chirurgie und Medizin
Kruis W. Dt Ärzteblatt 1982
Compensated vs. Decompensated BA-loss-syndrome
3-10-times increased
Hepatic BA-synthesis
Speeds motility
Hyperpermeability
Mucus/Na-Cl-secretion…
BA-loss cannot be compensated
By the liver, luminal BA-conc
Degrades ->
Fat-malabsorption-> steatorrhoe
BC 2019 R.Wiest 24
Klinik für Viszerale Chirurgie und Medizin
How do bile acides cause diarrhoe ?
Colonic microbiome deconjugates BA to secondary BA e.g. DCA, LCA
Particularly dihydroxylated BA chenodeoxycholate and deoxycholate
stimulate electrolyte and water secretion
Cholestyramine: when to use and/or not ?
Good response in compensated BA-loss-syndrome
Contraindicated in decompensated syndrome and
No effect/do-not-do it if no colon is preserved
BC 2019 R.Wiest 25
Klinik für Viszerale Chirurgie und Medizin
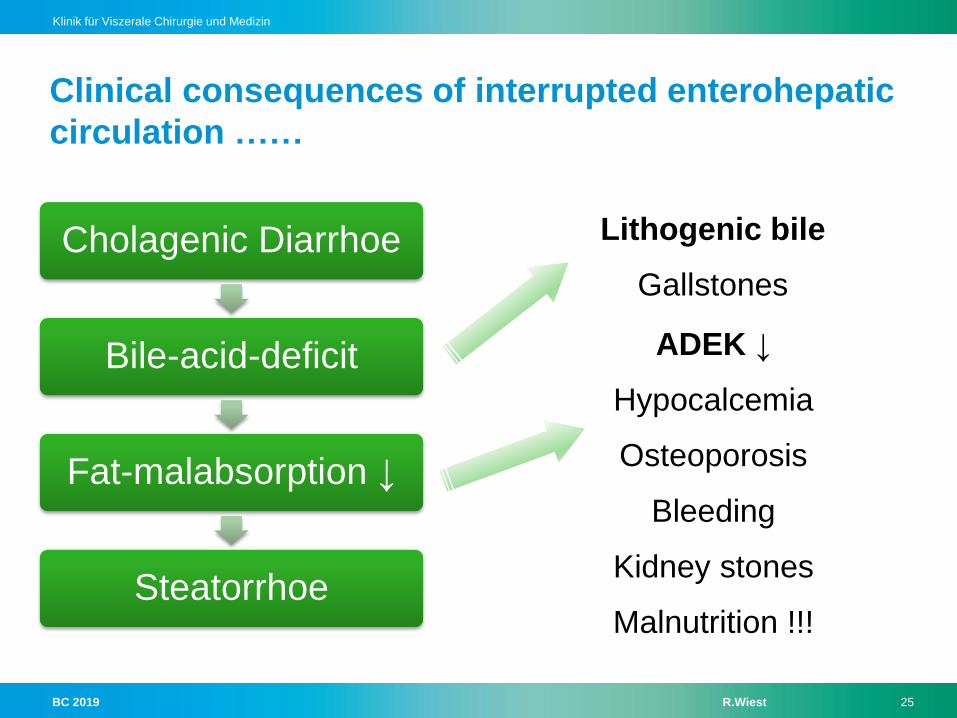
Clinical consequences of interrupted enterohepatic
circulation ……
Cholagenic Diarrhoe
Bile-acid-deficit
Fat-malabsorption ↓
Steatorrhoe
Lithogenic bile
Gallstones
ADEK ↓
Hypocalcemia
Osteoporosis
Bleeding
Kidney stones
Malnutrition !!!

BC 2019 R.Wiest 26
Klinik für Viszerale Chirurgie und Medizin
What is «functional classification» of intestinal
failure ?
On basis of onset, metabolic and expected outcome criteria
Type I acute, short-term and usually self limiting condition
Type II prolonged acute condition, often in metabolically unstable
patients, requiring complex multi-disciplinary care and
intravenous supplementation over periods of weeks or months
Type III chronic condition, in metabolically stable patients,
requiring intravenous supplementation over months or years.
It may be reversible or irreversible
BC 2019 R.Wiest 27
Klinik für Viszerale Chirurgie und Medizin
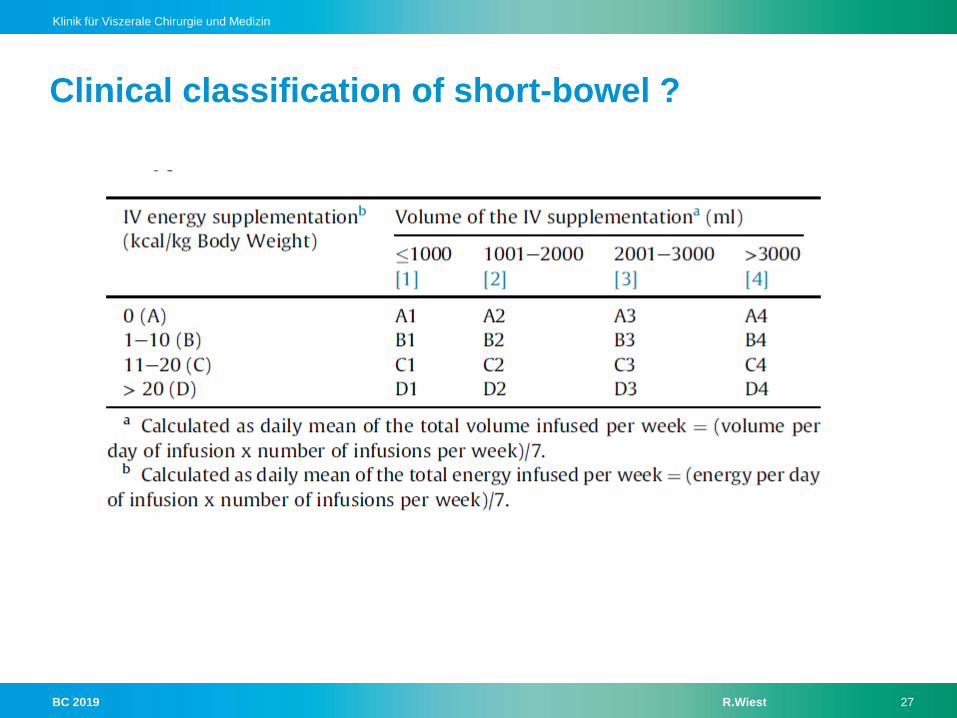
Clinical classification of short-bowel ?
BC 2019 R.Wiest 28
Klinik für Viszerale Chirurgie und Medizin
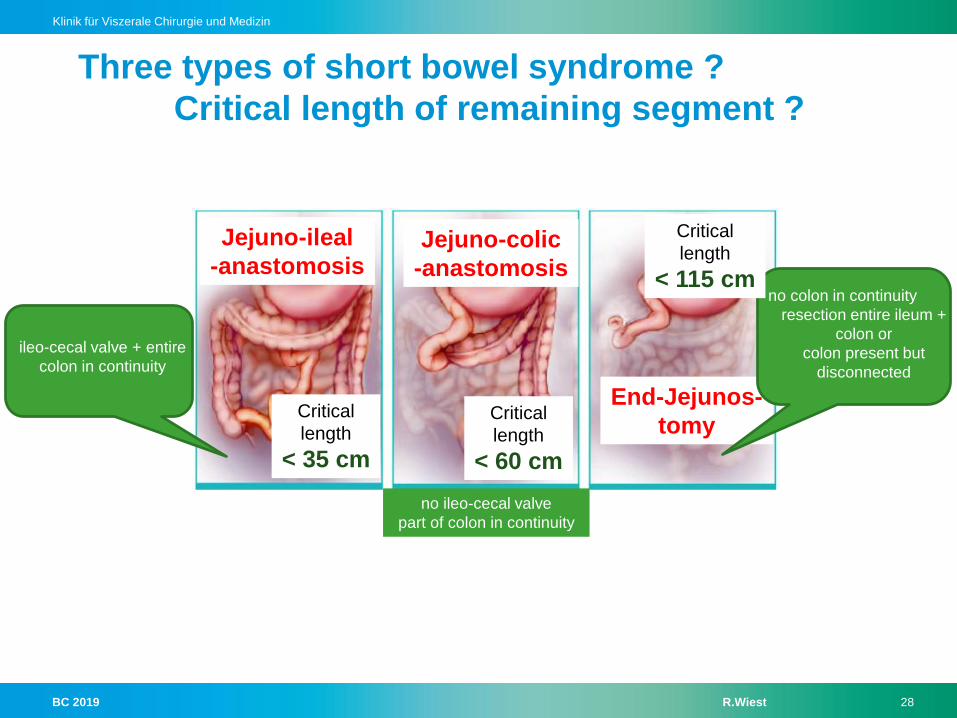
Three types of short bowel syndrome ?
Critical length of remaining segment ?
Jejuno-ileal
-anastomosisJejuno-colic
-anastomosis
End-Jejunos-
tomy
no colon in continuity
resection entire ileum +
colon or
colon present but
disconnected
ileo-cecal valve + entire
colon in continuity
no ileo-cecal valve
part of colon in continuity
Critical
length
< 35 cm
Critical
length
< 60 cm
Critical
length
< 115 cm
BC 2019 R.Wiest 29
Klinik für Viszerale Chirurgie und Medizin
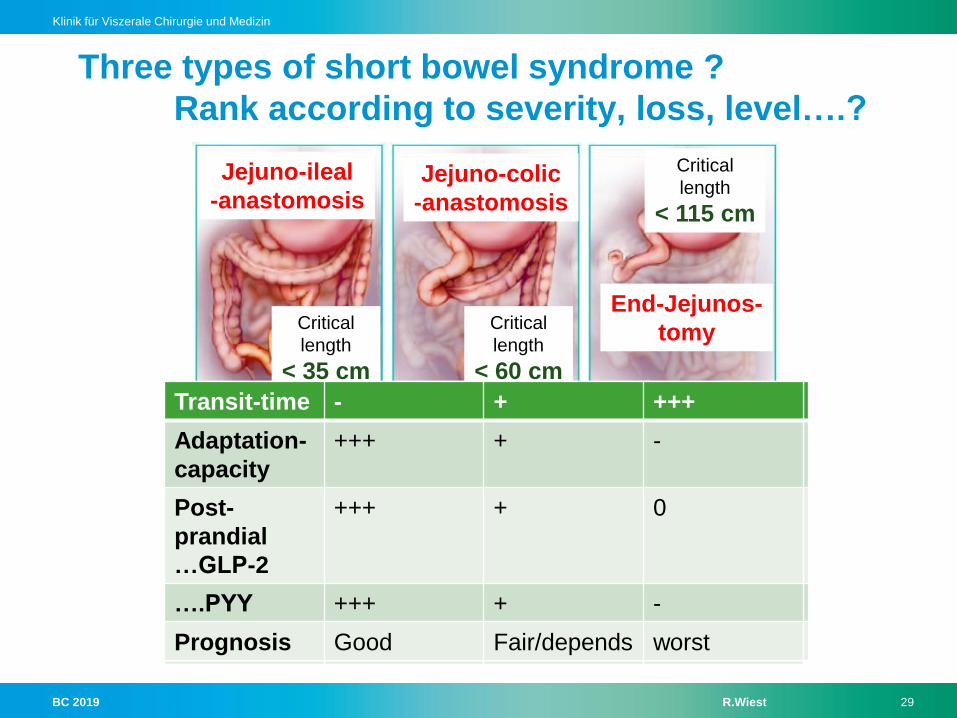
Three types of short bowel syndrome ?
Rank according to severity, loss, level….?
Jejuno-ileal
-anastomosisJejuno-colic
-anastomosis
End-Jejunos-
tomyCritical
length
< 35 cm
Critical
length
< 60 cm
Critical
length
< 115 cm
Transit-time
Adaptation-
capacity
Post-
prandial
…GLP-2
….PYY
Prognosis
Transit-time - + +++
Adaptation-
capacity
Post-
prandial
…GLP-2
….PYY
Prognosis
Transit-time - + +++
Adaptation-
capacity
+++ + -
Post-
prandial
…GLP-2
….PYY
Prognosis
Transit-time - + +++
Adaptation-
capacity
+++ + -
Post-
prandial
…GLP-2
+++ + 0
….PYY
Prognosis
Transit-time - + +++
Adaptation-
capacity
+++ + -
Post-
prandial
…GLP-2
+++ + 0
….PYY +++ + -
Prognosis Good Fair/depends worst
BC 2019 R.Wiest 30
Klinik für Viszerale Chirurgie und Medizin
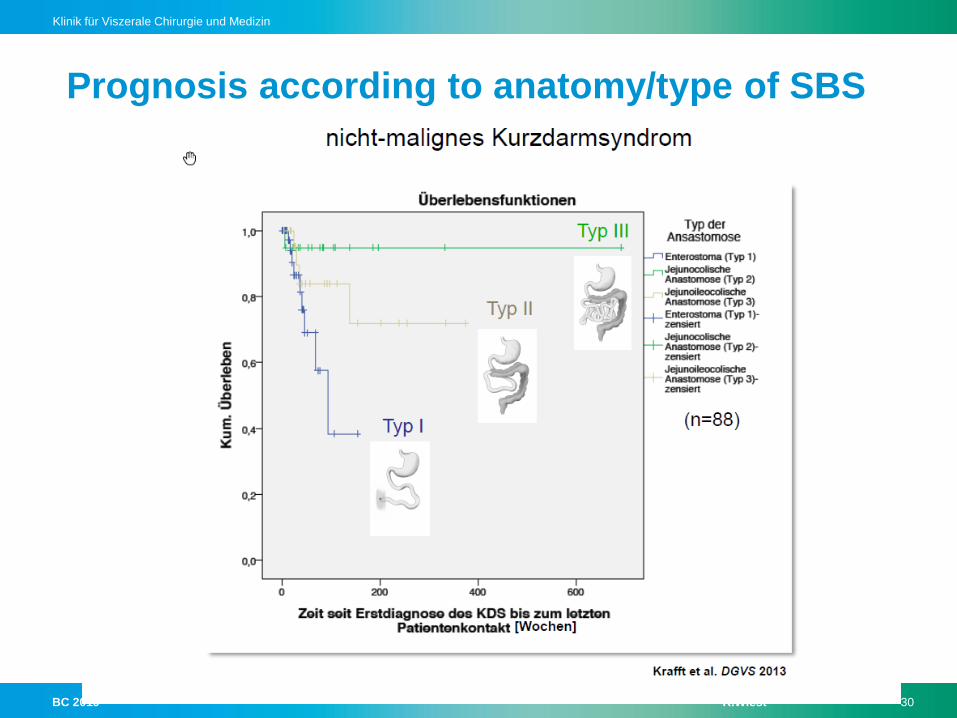
Prognosis according to anatomy/type of SBS
BC 2019 R.Wiest 31
Klinik für Viszerale Chirurgie und Medizin
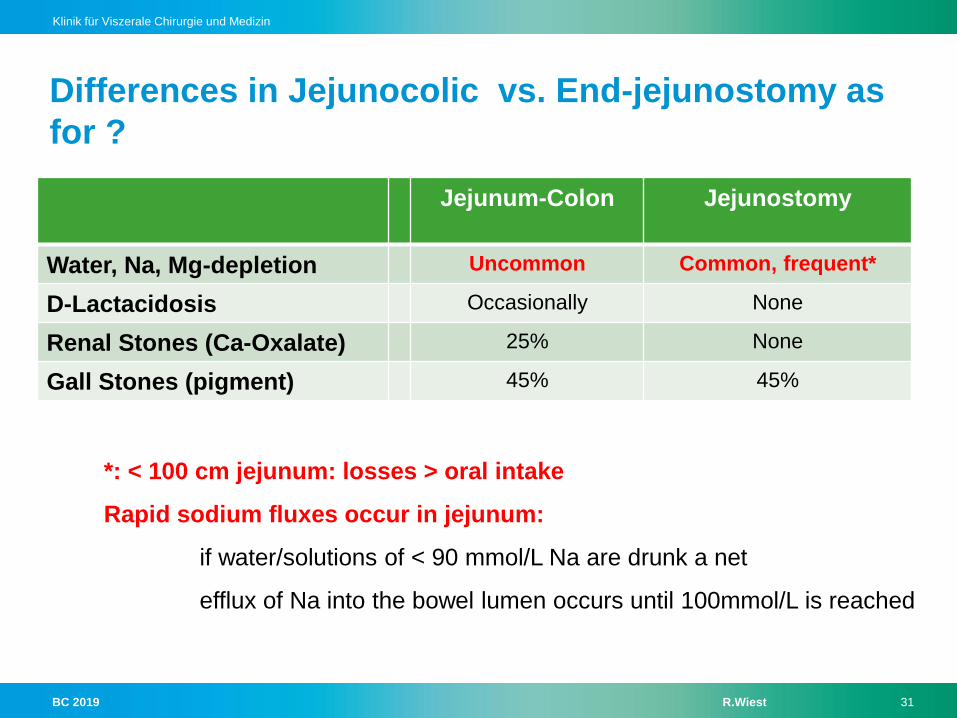
Differences in Jejunocolic vs. End-jejunostomy as
for ?
Jejunum-Colon Jejunostomy
Water, Na, Mg-depletion Uncommon Common, frequent*
D-Lactacidosis Occasionally None
Renal Stones (Ca-Oxalate) 25% None
Gall Stones (pigment) 45% 45%
*: < 100 cm jejunum: losses > oral intake
Rapid sodium fluxes occur in jejunum:
if water/solutions of < 90 mmol/L Na are drunk a net
efflux of Na into the bowel lumen occurs until 100mmol/L is reached
BC 2019 R.Wiest 32
Klinik für Viszerale Chirurgie und Medizin
D-Lactat-acidosis: when ? why ? Clinical features ?
Present colon: overflow of non-absorbable, undigested carbohydrates
from the small intestine (lack of digestion) into the colon: ->
anaerobic microbial fermentation-> lowering pH->
overgrowth of acid resistant bacteria such as Lactobacill acidophilus...
D-lactate not metabolizable (vs. L-lactat->LDH/liver: pyruvat) and accumulates
Diagnostic: serum level > 3 mmol/L; high anion gap, normal L-lactate
Effects of D-lactat:
aggravation of osmotic diarrhoe, metabolic acidosis
neurologic symptoms: encephalopathy, confusion, ataxia, visual defect
BC 2019 R.Wiest 33
Klinik für Viszerale Chirurgie und Medizin
BC 2019 R.Wiest 34
Klinik für Viszerale Chirurgie und Medizin
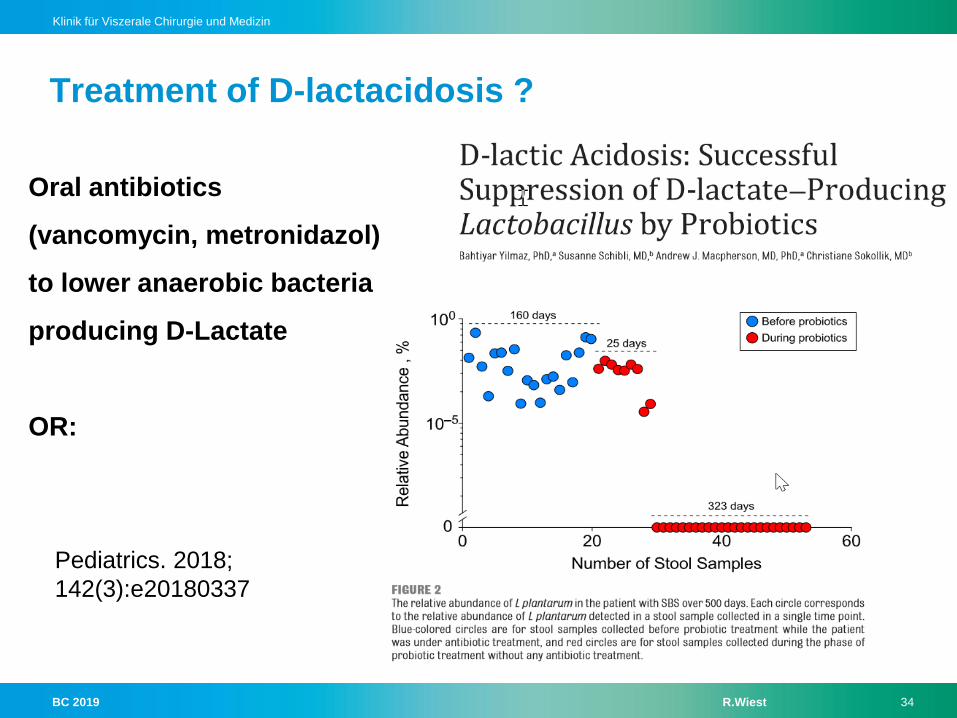
Treatment of D-lactacidosis ?
Pediatrics. 2018;
142(3):e20180337
Oral antibiotics
(vancomycin, metronidazol)
to lower anaerobic bacteria
producing D-Lactate
OR:
BC 2019 R.Wiest 35
Klinik für Viszerale Chirurgie und Medizin
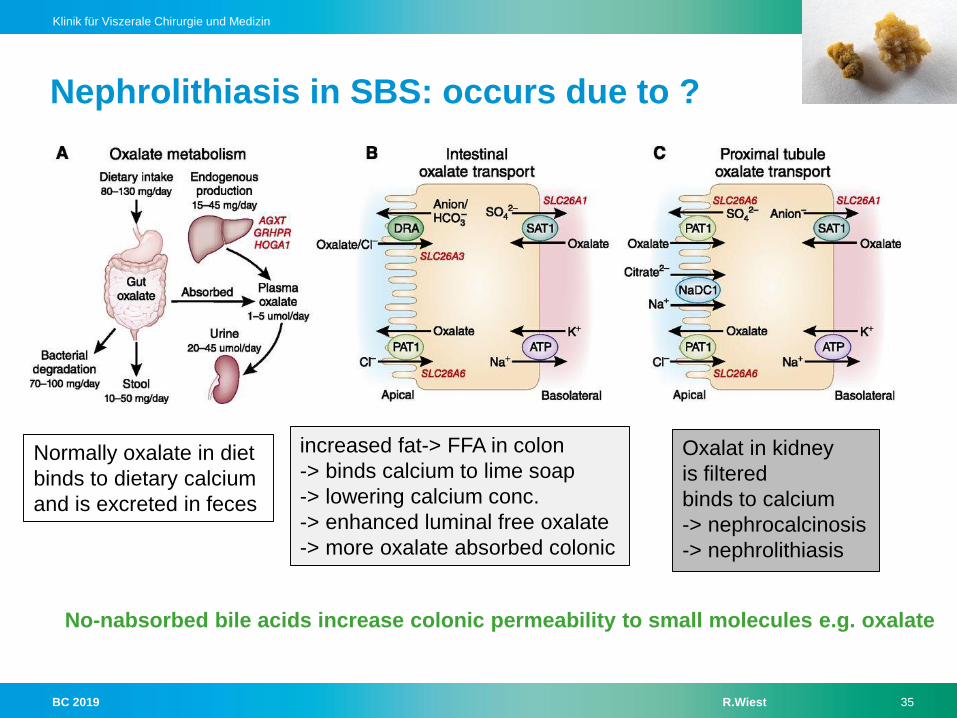
Nephrolithiasis in SBS: occurs due to ?
No-nabsorbed bile acids increase colonic permeability to small molecules e.g. oxalate
Normally oxalate in diet
binds to dietary calcium
and is excreted in feces
increased fat-> FFA in colon
-> binds calcium to lime soap
-> lowering calcium conc.
-> enhanced luminal free oxalate
-> more oxalate absorbed colonic
Oxalat in kidney
is filtered
binds to calcium
-> nephrocalcinosis
-> nephrolithiasis
BC 2019 R.Wiest 36
Klinik für Viszerale Chirurgie und Medizin
Bones in short-bowel-syndrome ?
High risk of osteomalacy and osteoporosis
due to
- Immobilisation
- Acidosis
- Malabsorption (Ca,Mg)
- Vit-D-Deficit
Bone-densitometry
every 2 years
BC 2019 R.Wiest 37
Klinik für Viszerale Chirurgie und Medizin
Below which Mg-level symptomatic ? Clinical picture ?
Mostly when high-output stoma/fistula (End-Jejunostomy), but also
Chelation of Mg with unabsorbed fatty acids reduces absorption
Increased renal excretion*, e.g. secondary hyperaldosteronism
Low Mg reduces 1,25 Vit-D-synthesis-> less Mg-absorption....
PPIs are often associated with hypomagnesaemia
*: low Mg per se reduces secretion/function of PTH, -> impact on kidney
Mechanisms – Role of – Magnesium-Deficiency
< 0.6 mmol/L serum-concentration->
Depression, muscle weakness, arrythmia, convulsions…..
Treatment: hydration, low-fat-diet (when colon is preserved); Mg
supplementation (oral difficult-> i.v.), evtl. Vit-D3, -B6
BC 2019 R.Wiest 38
Klinik für Viszerale Chirurgie und Medizin
Post-resection adaptations are …..?
Structural adaptations:
macroscopic
-elongation and dilatation
microscopic
-villus: increase height, diameter
-crypt elongation
-epithelial proliferation increased
-decreased apoptosis
Functional adaptations:
slowing gastrointestinal transit
Upregulation sodium-glucose transporter
Induced / influenced by ?
GI-regulatory peptides
luminal content, nutrients,
-pancreatico-biliary secretions
Systemic factors
- growth factors, hormones,
- Cytokines
Tissue factors
- immune system, mesenchymal factors
- Mesenteric blood flow, neural influences
BC 2019 R.Wiest 39
Klinik für Viszerale Chirurgie und Medizin
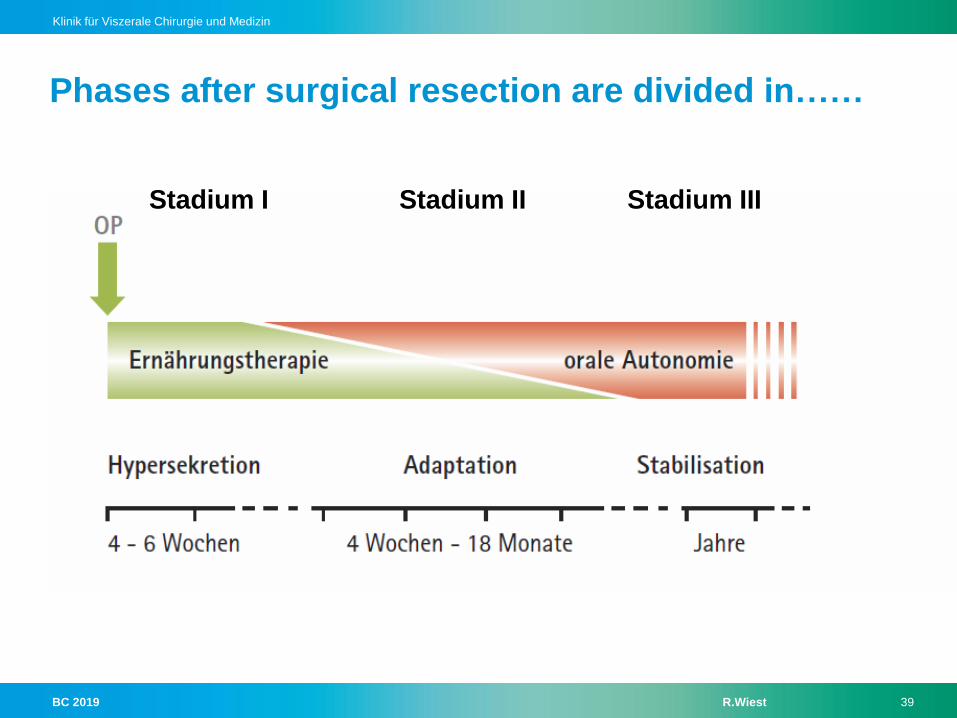
Phases after surgical resection are divided in……
Stadium I Stadium II Stadium III
BC 2019 R.Wiest 40
Klinik für Viszerale Chirurgie und Medizin
THERAPY