sharmin banu anam, md pgy-3 feb 27, 2014. common dermatological conditions in primary care 2
TRANSCRIPT

SHARMIN BANU ANAM, MDPGY-3
Feb 27, 2014

• Common Dermatological Conditions in Primary Care
2

3

4

Macules: Macules are nonpalpable lesions that vary in pigmentation from the surrounding skin. Macules are not raised or atrophic
Papules: Papules are palpable, discrete lesions measuring ≤5 mm diameter
Nodules: Nodules are palpable, discrete lesions measuring ≥6 mm diameter
Plaques: Plaques are large (>5 mm) superficial flat lesions, often formed by a confluence of papules
Pustules: Pustules are small, circumscribed skin papules containing purulent material
Vesicles:Vesicles are small (<5 mm diameter), circumscribed skin papules containing serous material
Whales: Irregularly elevated edematous skin, erythematous Scales: Superficial epidermal cells that are dead and cast off from
the skin Crusts: Dried exudate
5

6

7

8

9
Skin dryness, erythema, oozing and crusting, and lichenification - Itching is hallmark Treatment:Avoid trigger factors - heat, perspiration, low humidityTreat skin infections - staphylococcus aureus, herpesAntihistamines – sedation, control of itchingTreat stress and anxietyImmunomodulator (protopic)UVA, UVB, nbUVB,PUVA

10
Causes: InfectionsAllergic reactions to medications, foods, or insect stings and bitesMast cell activation- narcotics NSAIDsTreatment: Antihistamine( 1st and 2nd generation)H2 blocker( ranitidine)Short course of steroid ( prednisone/ prednisolone)

11
– Poison ivy– Poison oak– Poison sumac– Cashew– Mango– Ginkgo– Japanese lacquer tree
• Linear lesions• Vesicles– Fluid does not contain resin and won’t spread rash• Erythema• May occur within 8 hrs or up to a weekafter exposure

12
Treatment:
Decontamination within 10 min after exposure– Not helpful after 1 hr Wet compresses Topical corticosteroids Systemic corticosteroids – Prednisone 20 mg BID x 1 week – Prednisone 40-60 mg single dose IM steroids– Triamcinalone acetonide (Kenalog) 40 mg IM

13
Autoimmune blistering diseases in adultsIgG antibodies against bullous pemphigoid antigen
Treatment: Clobetasol, immunomodulators, antibiotics, immunosuppressant

14

15
Herpes Zoster (Shingles)• Varicella-zoster virus• Reactivation of latent infection• 10-20% lifetime incidence• Generally involves skin of a single dermatome• Pre-eruptive pain, itching, burning (4-5 days)• Fever, headache, malaise

16
Herpes Zoster (Shingles)• Vesicles, of varying size, on erythematous base• Successive crops over 7 days• Crust lasts 2-3 weeks• Postherpetic neuralgia– Increases with age of patient– Increases with pain during eruptive phase– Incidence = 20% at 1 month
Herpes Zoster – Treatment• Analgesics• Wet compresses (Burrow’s Solution)• Antiviral therapy– Acyclovir (Zovirax) 800 mg QID x 7 days– Famciclovir (Famvir) 500 mg q 8 hrs x 7 days– Valacyclovir (Valtrex) 1 g TID x 7 days

17
Herpes Zoster – Treatment• Oral corticosteroids (Prednisone)– May decrease pain initially during acute phase– Does not reduce subsequent postherpetic neuralgia• Sympathetic nerve blocks– Bupivacaine– Must be given within 2 months of onset to be effective
Postherpetic Neuralgia – Treatment• Narcotic analgesics• Anticonvulsants– Pregabalin (Lyrica)– Gabapentin (Neurontin)• Tricyclics• Capsaicin

18
Herpes Zoster Vaccine (Zostavax)• Contains the same live attenuated varicella virus as Varivax but at a much higher titer of vaccine virus• Approved by FDA for persons 50 years of age and older• Recommended by CDC for > 60 y/o• Regardless of past hx of zoster• Do not use if immunosuppressed,immunodeficient, pregnant, TB, or allergic to neomycin/gelatin• Administered by the subcutaneous route

19
Psoriasis• Oval, erythematous, plaque-like lesions• Can develop at sites of trauma• Often involves extensor surfaces– Elbows, knees & scalp• Pitting fingernails• Associated with asymmetric polyarthritis

20
Types• Chronic plaque psoriasis• Guttate psoriasis• Pustular psoriasis• Erythrodermic psoriasis
Treatment• < 20% of body involved– Topical corticosteroids– Calcipotriene (Dovonex)• Vitamin D3 analog– Tazarotene (Tazorac)– Anthralin (Anthra-derm)– Tar– UVB– Intralesional steroids
Treatment Contd• > 20% of body involved (phototherapy)– UVB• Broad band, narrow band• +/- topical, systemic, biologic agents( protopic)– PUVA• Ultraviolet + psoralen• +/- topical, systemic, UVB– Excimer laser

21
Treatment Contd• Severe recalcitrant disabling (FDA approved)– Methotrexate (Rheumatrex)• Gold standard– Acitretin (Soriatane) • Plaque type– Cyclosporine (Sandimmune)• Anti-TNF agents– Infliximab, Etanercept, Adalimumab

22
Squamous cell ca in situ:Head and neck (55 %)Dorsum of the hands and forearms (18 %)Legs (13%)Arms (3%)Shoulder or back (4%)Chest or abdomen (4%)
Diagnosis: Shave, punch, or excision biopsiesTreatment: Mohs surgery

23
Keratinization or disorders of cornification Inherited/acquired( malignancy, autoimmune or infectious disease, and nutritional deficiency)Treatment: topical steroid moderate to high potency- Triamcinolone Betamethasone Intralesional steroid-Tacrolimus-Antimalarial

24
? virus/ herpes 50 to 90 percent -"herald" or "mother" patch, ( single round or oval, sharply delimited, pink or salmon-colored lesion on the chest, neck, or back)Spreads centrifugally KOH to r/u dermatophytosis Treatment:If pruritus- medium potency topical steroid/ oral antihistamine-Erythromycin/ acyclovir -UVB

25
Scabies• Hypersensitivity reaction to Sarcoptes scabiei– Eggs, fecal pellets (scybala)• Nocturnal pruritis– Scratching spreads mites to other areas• Curved or linear burrows• Vesicles or small papules• Pustules indicate secondary infection
• Location of lesions– Finger webs– Wrists– Elbows– Knees– Buttocks– Axilla– Waist– Breasts– Genitals

26
Scabies – Diagnosis• Locate burrow with felt tip pen ink• Scrape with #15 curved scalpel blade• View under mineral oil or KOH• Look for mites, eggs, feces (scybala)
Norwegian (Crusted) Scabies• Overwhelming infestation• Crusted lesions• Not particularly pruritic• Seen mostly in immunocompromised patients

27
Treatment Launder all bedding and clothes worn within 48 hrs in hot water or dry clean Treat patient, intimate contacts, and family members in same household• 5% Permethrin cream (Elimite)– Drug of choice– Apply below the neck, may repeat in 1 week• Lindane (Kwell)– More toxic, especially in children/pregnancy• Ivermectin (Stromectol)– Effective for Norwegian scabies• Crotamiton (Eurax)• Benzyl benzoate 25% lotion• 6% precipitated sulfur in petrolatum

28
Acne Vulgaris• Androgen mediated disorder of pilosebaceous units• Androgens stimulate sebum production and proliferation of keratinocytes• Keratin plug obstructs follicle os• Proprionibacterium acnes proliferates in plugged follicle• P. acnes growth produces inflammation

29
Acne Vulgaris – Treatment• Comedonal acne– Keratinolytic agent• Mild inflammatory acne– Keratinolytic agent +/ topical antibiotic• Moderate inflammatory acne– Topical antibiotic +/- systemic antibiotic• Severe (nodulocystic) acne– Isotretinoin
• Topical keratinolytics– Tretinoin (Retin-A)• start with lowest concentration of cream and advance as tolerated• apply qhs after washing• may cause an initial flare of lesions• side effects include erythema, dryness, scaling– Adapalene (Differin)• apply hrs after washing• better tolerated than tretinoin and equally effective

30
Treatment:Topical keratinolytic: Tretinoin( retin A), Adapalene, Tezarotine, Azeleic acid
Topical antibacterial: Benzoyl peroxide with or without antibiotic
Topical antibiotic: erythromycin,clindamycin,tetracycline,metronidazole,dapsone
Systemic antibiotic: Tetra / mino/ doxycycline, erythro/ azithromycin, Bactrim
OCP
Spironolactone
Isotretinoin, Acutane(2 form of birthcontrol)
need to register to iPLEDGE program
31
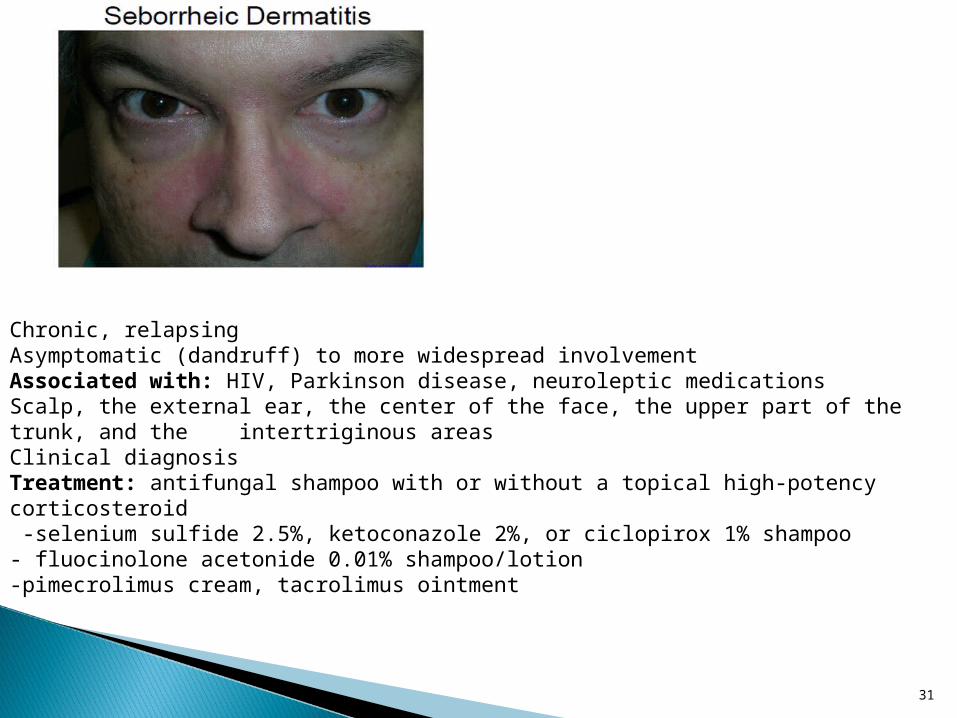
Chronic, relapsingAsymptomatic (dandruff) to more widespread involvementAssociated with: HIV, Parkinson disease, neuroleptic medicationsScalp, the external ear, the center of the face, the upper part of the trunk, and the intertriginous areasClinical diagnosisTreatment: antifungal shampoo with or without a topical high-potency corticosteroid -selenium sulfide 2.5%, ketoconazole 2%, or ciclopirox 1% shampoo- fluocinolone acetonide 0.01% shampoo/lotion-pimecrolimus cream, tacrolimus ointment

32
Rosacea• Prevalence = 15 million in US• Most common in Celtic ethnicity• Most common after age 30• More common in women• Unknown etiology• Chronic, intermittent• Involves forehead, cheeks, nose, ocular area

33
Primary features– Erythema• Transient symmetric flushing– Accentuated by hot liquids and alcohol• Non-transient– Papules and pustules– Telangiectasia
Secondary features– Burning or stinging– Plaque– Dry appearance– Edema– Nasal hypertrophy/scarring (rhinophyma)– Ocular manifestations
Triggers for flushing• Extremes of temperature• Sunlight• Spicy foods• Alcohol• Exercise• Acute psychological stressors• Medications• Menopausal hot flashes

34
Rosacea – Treatment• Topical antibiotics• 0.75% Metronidazole (Metrogel) – BID• 1% Metronidazole (Noritate) – daily• Azelaic acid 15% (Azelex) – BID• Benzoyl peroxide 5% - BID• +/- erythromycin or clindamycin• Clindamycin cream – less effective• Other topical agents• Pimecrolimus (Elidel) 1% cream• Adapalene 0.1% gel, Tretinoin 0.025% cream• Permethrin

35
Rosacea – Treatment
• Oral antibiotics• Doxycycline (Vibramycin) 100-200 mg/day• Tetracycline 1 gram/day• Erythromycin 1 gram/day• Minocycline (Minocin) 100-200 mg/day• Metronidazole (Flagyl) 250 mg BID• Azithromycin (Zithromax) 500 mg, then 250 mg x 4 days• Retinoids• Isotretinoin (Accutane) 0.5 mg/kg/day x 20 weeks for severe resistant cases

36
Rosacea – Treatment• Vascular laser– Useful for resistant telangectasia & persistent erythema• Rhinophyma Rx– Mechanical dermabrasion– CO2 laser peel– Surgical excision– Electrocautery

37
Face, neck, upper trunk, and proximal extremitiesUsually asymptomatic Cause: Atopy, sun exposure, bathingTreatment: protect from sun exposureTopical steroid/ calcinurin inhibitorMay take months to year to get better

38
1% populationAntibody to melanocyteAssociated with: Other autoimmune disorders, thyroid disease, pernicious anemia, SLE, Addison disease Treatment:Corticosteroids( 10% of body) – medium potency >6 mo Calcineurin inhibitors( elidel, protopic) UVA/ UVB Surgery

39
Tinea Versicolor• Caused by Malassezia (Pityrosporum)species• Lesions result from conversion from budding to mycelial form• Occurs with heat, humidity, pregnancy, steroids, immunosupression• More common at ages associated with high sebaceous activity

40
Tinea Versicolor – Treatment• Topical – for limited disease– Ketoconizole 2% shampoo (Nizoral) x 3 days– Selenium sulfide 2.5% x 7 days or q week x 4– Terbinafine 1% solution (Lamisil) BID x 1 week
Oral – for extensive disease or nonresponders– Itraconazole (Sporanox) 200 mg daily x 5-7 days– Fluconazole (Diflucan) 300 mg single dose,repeat in 1 week– Avoid oral ketoconizole-Concern about hepatotoxicity
Prophylaxis– Ketoconizole 2% shampoo (Nizoral) q week– Itraconazole (Sporanox) 200 mg PO BID q month x 6 months

41
Pruritic, circular or oval, erythematous, scaling patch or plaque that spreads centrifugally. Central clearingOutbreaks among athletes who have skin-to-skin contact, wrestlers (tinea corporis gladiatorum)Diagnosis: KOH preparation, segmented hyphae and arthrosporesTreatment: Topical antifungals (nystatin is ineffective) Oral terbinafine, fluconazole, and itraconazole

42
Mostly in small childrenThree forms, "gray patch," "black dot" and favusDiagnosis: KOH examination of manually epilated hairTreatment: Grieseofulvin Terbinafine

43
Tinea corporis has been altered by the use of topical corticosteroids

44
HPV type 1 -plantar warts 6 and 11 -anogenitalSpread by:Skin-to-skin contact,sites of trauma (Koebner phenomenonSpontenious remission in 2/3 patients Cellular immunity impaired Diagnosis: clinical, may see thrombosed vein on scraping by 15 scalpelTreatment: Trichloroacetic acid, imiquimod, canthraridinCryotherapy, snip or shave excisionPlanter wart – consult dermatologist ( painful)

45
Genital Wart – Treatment Patient administered– Podofilox -0.5% BID x 3 days, off 4 days, repeat cycle x 4– Imiquimod -5% cream (Aldara) HS, 3x/week, x 16 wks– Sinecatechins 15% ointment (Veregen) TID for maximum of 16 wks Provider administered– Cryotherapy– TCA– Podophylin resin 10-25%– Surgical or laser removal– Interferon alfa-2B (Intron-A)

46
Genital Herpes – Treatment• Acyclovir (Zovirax)– Primary = 400 mg TID x 7 days, 200 mg 5x/day x 7 days– Recurrent = 400 mg TID x 5 days, 800 mg TID x 2 days– Suppression = 400 mg BID• Famciclovir (Famvir)– Primary = 250 mg TID x 7 days– Recurrent = 125 mg BID x 5 days, 1 g BID x 1 day– Suppression = 250 mg BID• Valacyclovir (Valtrex)– Primary = 1 g BID x 7 days– Recurrent = 1 g daily x 5 days, 500 mg BID x 3 days– Suppression = 500 mg or 1 g daily

47
Molluscum Contagiosum• Caused by double-stranded DNA Poxvirus• Spread by skin to skin contact and autoinoculation• Umbilicated, firm, flesh-colored, domeshaped papules• Children -Lesions anywhere except palms & soles• Adults – Lesions mostly in genital area

48
Molluscum Contagiosum –Treatment• Curettage– May cause scarring• Cryosurgery• Imiquimod 5% cream (Aldara)– TID x 5 days/wk x 1 month• Cantharidin• Cimetidine (Tagamet) 40 mg/kg/day x 2 months(children)• Laser• TCA peel q 2 weeks• KOH 5%

49
Basal Cell Carcinoma• Most common skin cancer• Male > female• Mostly in age > 40• 85% occur in head/neck• Clinical course is unpredictable– Can remain small for years or develop in growth spurts
Subtypes• Nodular-Most common,less aggressive• Superficial– Plaque like• Sclerosing– Rare• Pigmented

50
• Diagnosis by biopsy Excisional biopsy– Often adequate for small lesions• Electrodesiccation/curettage, cryotherapy– Nodular & superficial < 6 mm in size, < 3 mm in depth

51
Moh’s micrographic surgery – Sclerosing, poorly defined margins – High-recurrence areas - Nose, eyelid – Large (> 2 cm) primary or recurrent BCCs – Lesions where conservation of tissue is importantRadiationChemotherapyImiquimod 5% cream(Aldera)5FU 5% ( Efudex)

52
Hypertrophy of sebaceous glandsDiagnosis is clinicalNo treatment necessaryMay do electrosurgery or shave biopsy

53
• Dome-shaped nodule,keratin-filled crater• Resemble cutaneous squamous cell carcinoma• Hair-bearing, sun-exposed skin• Middle-aged, elderly adults, fair complexions • Diagnosis: clinical, Excisional Biopsy• Spontanious resolution

54
De Morgan spotsCapillary proliferation in middle ageConfused with amelanotic melanomasTreatment:Small – electrocauterization Large - shave excision - laser

55
Benign acquired melanocytic neoplasm-Asymmetric, irregular borders, multiple colors, and diameter >5 mm-Increases risk of melanomaDiagnosis: Clinical Management: Total body skin exam Life long follow up

56
ABCDE’s of Melanoma• A – Asymmetry• B – Border irregularity• C – Color variegation• D – Diameter greater than 6 mm• E – Evolving (changing)
Malignant Melanoma• Thickness determines prognosis– Breslow microstage (mm)• Measured depth of tumor invasion• Most accurate– Clark level• Histologic layer of dermis involvement

57
Malignant Melanoma• Mostly found in non-Hispanic Caucasians• Median age = 53• Men 1.5x > women• Metastasize widely
Risk Factors• Large number of atypical nevi• Other skin cancers• Congenital giant nevus• Family history of melanoma• Immunosuppression• UV radiation exposure
Subtypes• Superficial spreading– Most common– Upper back & legs in 40-50 y/o• Nodular– Mostly men in 50-60 y/o• Lentigo maligna– Facial location in 60-70 y/o• Acral lentiginous– Digits & mucous membranes

58

59
• Stuck on appearance • Benign
Treatment: Not necessary • Curettage +/- electrodesiccation• Cryosurgery

60
Squamous cell carcinoma: papules, plaques, or nodules, and smooth, hyperkeratotic, or ulcerative lesionsdevelop in sites of chronic wounds, chronic inflammation, or scarringBiopsy is necessary for diagnosis: Shave, punch, or excisional biopsiesTreatment: Mohs surgery
Actinic keratosisSquamous cell carcinoma

61
Photo Quiz

62

63

64

65

66

67

68

69

70
References: AAFP Family Medicine Board Review Express, 2014 Phillips, Charles M. MD, Dept. of Medicine, Brody School of Medicine Usatine, Richard P MD, Dept. of Family Medicine, UTHSCSA Habif, Thomas Clinical Dermatology 5th Edition, 2009 Centers for Disease Control & Prevention,Sexually Transmitted Diseases DivisionDaniel BS, Borradori L, Hall RP 3rd, Murrell DF. Evidence-based management of bullous pemphigoid. Dermatol Clin 2011; 29:613.Joly P, Roujeau JC, Benichou J, et al. A comparison of oral and topical corticosteroids in patients with bullous pemphigoid. N Engl J Med 2002; 346:321.Joly P, Roujeau JC, Benichou J, et al. A comparison of two regimens of topical corticosteroids in the treatment of patients with bullous pemphigoid: a multicenter randomized study. J Invest Dermatol 2009; 129:1681.Murrell DF, Daniel BS, Joly P, et al. Definitions and outcome measures for bullous pemphigoid: recommendations by an international panel of experts. J Am Acad Dermatol 2012; 66:479.English DR, Armstrong BK, Kricker A, et al. Demographic characteristics, pigmentary and cutaneous risk factors for squamous cell carcinoma of the skin: a case-control study. Int J Cancer 1998; 76:628.Gloster HM Jr, Neal K. Skin cancer in skin of color. J Am Acad Dermatol 2006; 55:741.Asuquo ME, Ngim O, Ugare G, et al. Major dermatologic malignancies encountered in a teaching hospital surgical department in South Nigeria. Am J Clin Dermatol 2008; 9:383.Mora RG, Perniciaro C. Cancer of the skin in blacks. I. A review of 163 black patients with cutaneous squamous cell carcinoma. J Am Acad Dermatol 1981; 5:535.Fleischer AB Jr, Feldman SR, McConnell RC. The most common dermatologic problems identified by family physicians, 1990-1994. Fam Med 1997; 29:648.García-Hidalgo L, Orozco-Topete R, Gonzalez-Barranco J, et al. Dermatoses in 156 obese adults. Obes Res 1999; 7:299.Romano G, Moretti G, Di Benedetto A, et al. Skin lesions in diabetes mellitus: prevalence and clinical correlations. Diabetes Res Clin Pract 1998; 39:101.Nahass GT, Meyer AJ, Campbell SF, Heaney RM. Prevalence of cutaneous findings in hospitalized medical patients. J Am Acad Dermatol 1995; 33:207.Krowchuk DP, Bradham DD, Fleischer AB Jr. Dermatologic services provided to children and adolescents by primary care and other physicians in the United States. Pediatr Dermatol 1994; 11:199.Ernst E. The usage of complementary therapies by dermatological patients: a systematic review. Br J Dermatol 2000; 142:857.Gerbert B, Maurer T, Berger T, et al. Primary care physicians as gatekeepers in managed care. Primary care physicians' and dermatologists' skills at secondary prevention of skin cancer. Arch Dermatol 1996; 132:1030.Federman DG, Reid M, Feldman SR, et al. The primary care provider and the care of skin disease: the patient's perspective. Arch Dermatol 2001; 137:25.Gropper CA. An approach to clinical dermatologic diagnosis based on morphologic reaction patterns. Clin Cornerstone 2001; 4:1.Federman DG, Kirsner RS. The patient with skin disease: an approach for nondermatologists. Ostomy Wound Manage 2002; 48:22.