selective mutism (sm) (312.23) presentation by benson munyan
TRANSCRIPT
Selective Mutism (SM) (312.23)
Presentation by Benson Munyan

SM Primer
DSM5 Diagnostic Review• When encountering social interactions outside of the
home of the child or adult, those with SM will not initiate speech or reciprocate responses.
• This may lead to academic or educational impairment, as well as social communication.
• Children may participate is social activities when speech is not required.
APA, 2013

DSM5 Criteria• A: Consistent failure to speak in specific situations in which there is an expectation
for speaking despite speaking in other situations.
• B: The disturbance interferes with educational or occupational achievement or with social communication.
• C: The duration of the disturbance is at least 1 month.
• D: The failure to speak is not attributable to a lack of knowledge of, or comfort with, the spoken language required in the social situation.
• E: The disturbance is not better explained by a communication disorder and does not occur exclusively during the course of autism spectrum disorder, schizophrenia, or another psychotic disorder.
APA, 2013

Associated Features Supporting Dx• Excessive shyness• Fear of social embarrassment• Social isolation and withdrawal• Clinging• Compulsive traits• Negatism• Temper tantrums• Mild Oppositional behavior
APA, 2013

Prevalence• Selective Mutism is relatively rare.– Has not been included in epidemiological studies of
prevalence.
Prevalence is thought to be between .03% and 1%
Does not vary by gender/ethnicity.
APA, 2013
Development & CourseOnset is generally prior to age 5, but may not be noticed until entry into school
Persistence of Disorder is variable.
May be outgrown, but longitudinal course is unknown.
APA, 2013

Risk and PrognosisTemperamental risk factors are not well identified. Neuroticism or behavioral inhibition may play a role.
Environmental: Parental social inhibition may play a role.
Genetics: Due to overlap with social anxiety disorder, there may be shared genetic factors.
APA, 2013
Cultural Diagnostic IssuesIn people who have immigrated from a country that utilizes a different language, refusal to speak the new language due to lack of knowledge of the language may present itself.
If comprehension of the new language is adequate but refusal persists, diagnosis may be warranted.
APA, 2013

Functional ConsequencesSM may result in social impairment, and later, social isolation.
In academic settings, children may suffer academic impairment due to failure to communicate with teachers regarding academic or personal needs.
SM may serve as a compensatory strategy to decrease anxious arousal in social encounters.
APA, 2013

Differential DiagnosisCommunication Disorders: SM should be distinguished from Language disorder, Speech Sound disorder, child-onset fluency disorder, and pragmatic communication disorder. (These are not restricted to specific situations.)
Neurodevelopmental Disorders:Autism Spectrum disorder, Schizophrenia, other psychotic disorders and severe intellectual disorders may have problems with social communication, which may impair social interaction. To contrast, SM should be diagnosed when there is an established capacity to speak in some situations (e.g., home).
APA, 2013

ComorbidityMost Common:
Other anxiety disordersSocial anxiety disorderSeparation anxietySpecific Phobia
Communication Delays may also appear in some children with SM.
APA, 2013

DSM5 Model
APA, 2013

Literature Review

Parental Social PhobiaChavira et al. (2007)
Generalized social phobia was present in 37.0% of SM parents compared to 14.1% of control parents.(x2 = 10.98; p < .001; odds ratio 3.6, 95% confidence interval 1.6-7.9).
Avoidant personality disorder was present in 17.5% of the SM parents compared to 4.7% of control parents (x2 = 6.18; p < .05; odds ratio 4.3, 95% confidence interval 1.3-14.9)
SM parents had higher neuroticism and lower openness scores on the NEO Personality Inventory than control parents.
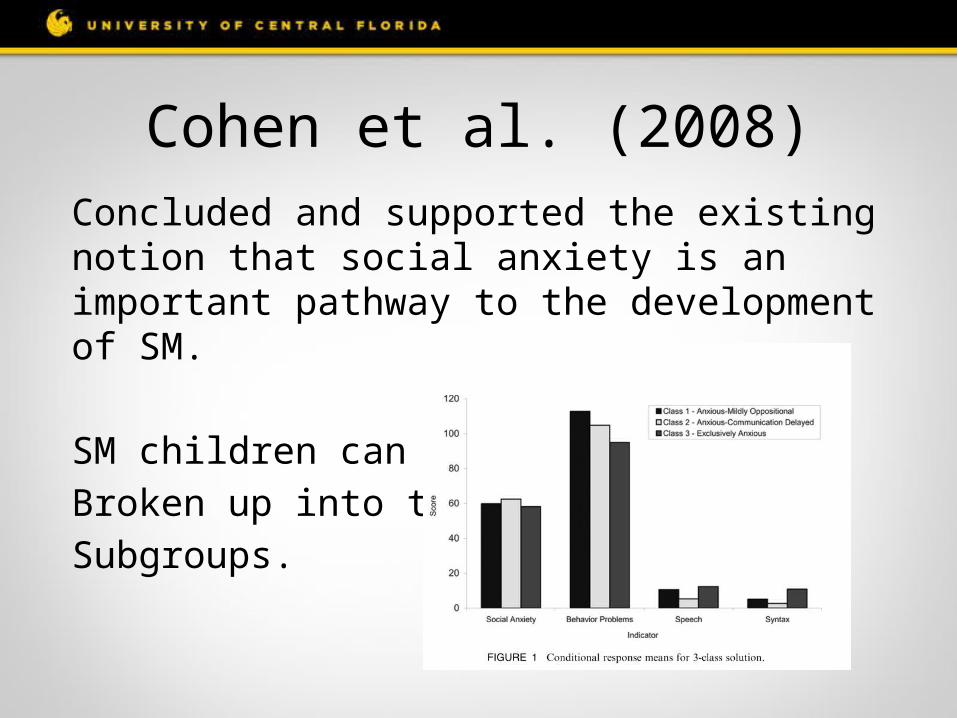
Cohen et al. (2008)Concluded and supported the existing notion that social anxiety is an important pathway to the development of SM.
SM children can beBroken up into threeSubgroups.

Communication Delays
Multiple studies found evidence of articulation problems, delayed speech, or other communication disorders.
Krohn et al. (1992)Steinhausen & Juzi (1996)Wilkins (1985)

CNTNAP2• Stein et al (2011) found a common genetic
variant associated with ASD and more specifically, the developmental language delayed component of autism.
• Mechanisms are still not understood.

Heritability?Cohan et al (2006) found in a sample (n=30) of children, 15% of parents and 19% of siblings had a history of SM.
44% of parents had a history of social phobia or avoidant disorder.
21% of siblings had similar histories.

Comorbidity• Social Phobia• Communication Disorders• Elimination Disorders
(Encopresis and Enuresis)• Developmental Disorders• Oppositional defiant disorder

Outstanding Theoretical Questions• Is SM a disorder, or a learned contingency?– Negative and Positive Reinforcement• (Mowrer, 1947)
• Is SM founded in anxiety, or oppositional behavior?
• Are parents modeling social anxiety?• Are parents “rescuing” children with SM?
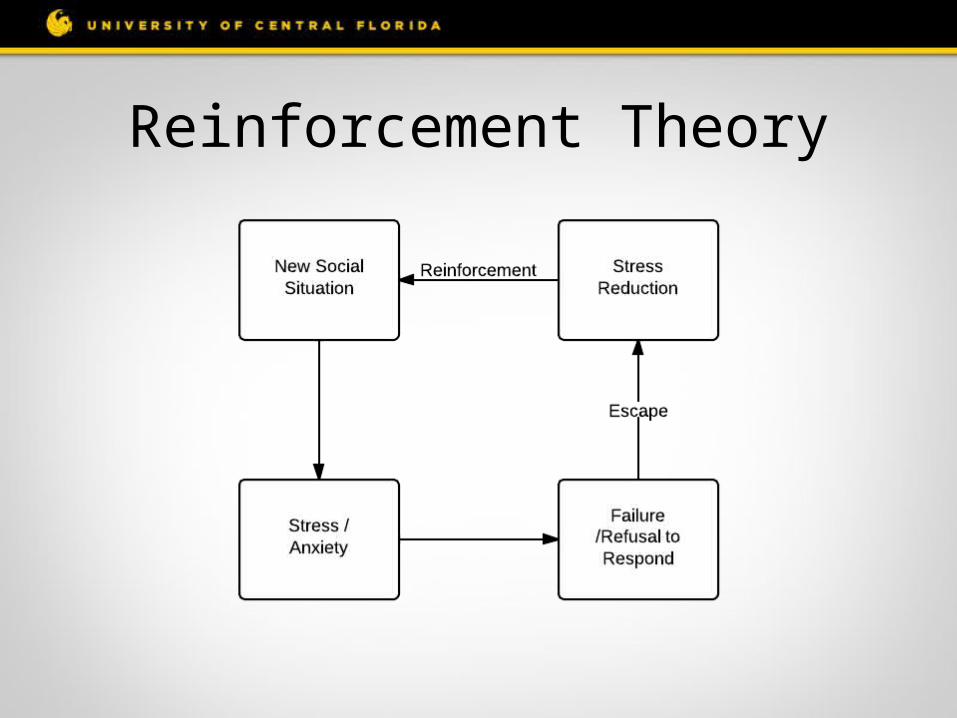
Reinforcement Theory
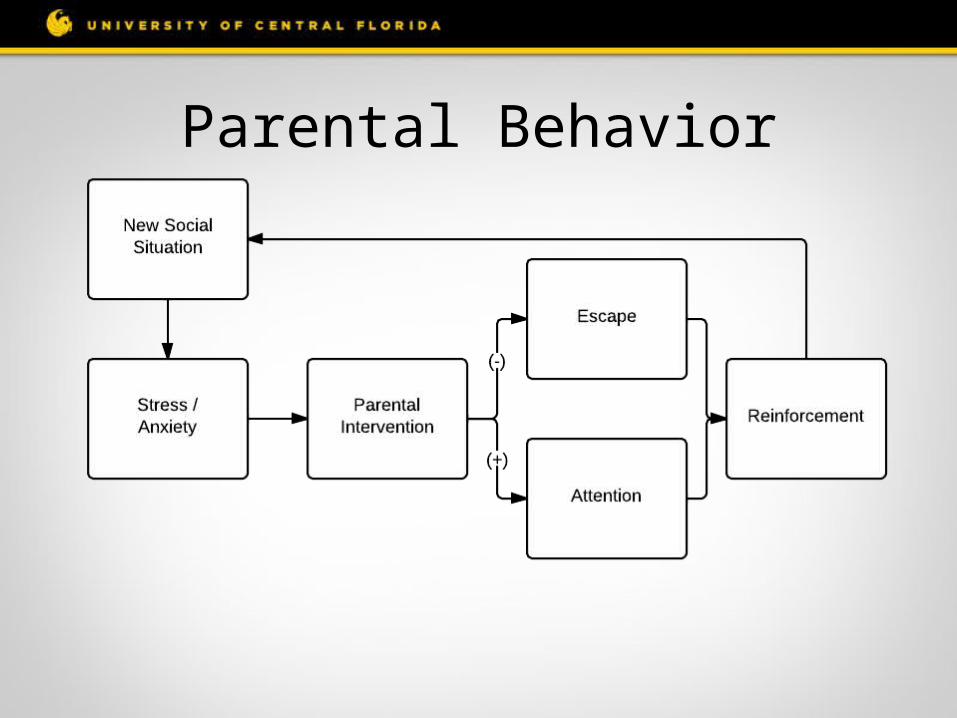
Parental Behavior

Black & Uhde Potential Model

Theoretical Model
References• American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
http://dx.doi.org/10.1176/appi.books.9780890425596.910646• Black, B., & Uhde, T. (1995). Psychiatric characteristics of children with selective mutism: a pilot study. … American Academy of Child & Adolescent
Psychiatry, 34(7), 847–856. Retrieved from http://www.sciencedirect.com/science/article/pii/S0890856709635942• Bunnell, B. E., & Beidel, D. C. (2013). Incorporating Technology Into the Treatment of a 17-Year-Old Female With Selective Mutism. Clinical Case
Studies, 12(4), 291–306. doi:10.1177/1534650113483357• Chavira, D. a, Shipon-Blum, E., Hitchcock, C., Cohan, S., & Stein, M. B. (2007). Selective mutism and social anxiety disorder: all in the family? Journal of
the American Academy of Child and Adolescent Psychiatry, 46(11), 1464–72. doi:10.1097/chi.0b013e318149366a• Dummit ES, Klein RG, Tancer NK, et al. Systematic assessment of 50 children with selective mutism. Journal of American Academy of Child Adolescent
Psychiatry. 1997; 36:653-660• Krohn, D. D., Weckstein, S. M., & Wright, H. L. (1992). A study of the effectiveness of a specific treatment for elective mutism. Journal of the American
Academy of Child & Adolescent Psychiatry, 31, 711–718.• Mowrer, O. H. (1947). On the dual nature of learning: A reinterpretation of “conditioning” and “problem- solving.” Harvard Education Review, 17, 102-
148.• Steinhausen, H., & Juzi, C. (1996). Elective mutism: An analysis of 100 cases. Journal of the American Academy of Child & Adolescent Psychiatry, 35,
606–614.• Wilkins, R. (1985). A comparison of elective mutism and emotional disorders in children. The British Journal of Psychiatry, 146, 198–203.• Stein, M. B., Yang, B.-Z., Chavira, D. a, Hitchcock, C. a, Sung, S. C., Shipon-Blum, E., & Gelernter, J. (2011). A common genetic variant in the neurexin
superfamily member CNTNAP2 is associated with increased risk for selective mutism and social anxiety-related traits. Biological psychiatry, 69(9), 825–31. doi:10.1016/j.biopsych.2010.11.008