mutism selective - juliagloraso.files.wordpress.com · journal of school psychology, 36(3),...
TRANSCRIPT
Selective Mutism
Mia, Julia, Esther, Ali, Keenan & Savanna
1. What is selective mutism?
2. Identifying and teaching students
3. Treatment and intervention
4. Top 10 myths
5. What can recovered adults tell us?
Tonight’s Agenda...
➔ https://www.youtube.com/watch?v=FcSk44QfJ8g
➔ https://www.youtube.com/watch?v=hZ0ZYIOQ7gY
➔
1.What is selective
mutism?
Selective Mutism is...
➔ A pediatric psychiatric disorder.
➔ When a child consistently fails to speak when he/she is expected to, (at school or in social situations).
➔ These children do, however, manage to speak appropriately in other settings.
➔ Most often diagnosed when the child starts school or preschool.
Characteristics of Selective Mutism
➔ It can have an impact on a child’s socialization and academic development.
➔ Sufferers can speak and comprehend language.
➔ It is very rare, about 0.1% of children suffer from it.
➔ It is treatable.
Why?
➔ The condition is most frequently accompanied by anxiety and shyness.
➔ Causes of the condition remain unclear.
➔ It is treated most often with therapy.
➔ In severe cases or in cases where the child may be suffering from other illnesses, the patient may be treated with medication as well.
A PEDIATRIC PSYCHIATRIC DISORDER WHERE A CHILD FAILS
TO SPEAK WHEN S/HE IS EXPECTED TO
WHAT IS SELECTIVE MUTISM?
TREATABLE; VERY RARE; CHILD’S SOCIALIZATION AND
ACADEMIC DEVELOPMENT CAN BE IMPACTED
WHAT ARE CHARACTERISTICS OF SELECTIVE MUTISM?

2.Identifying &
Teaching Students
Identifying Selective Mutism
➔ Can be diagnosed after 1-6 months of mutism (not counting the first month of school!)
➔ Sudden loss of speech is referred to as hysterical mutism, and is often short.
➔ Age of onset: between 3 and 8 years old.
➔ Diagnosis cannot be made if the child’s difficulties can be better explained by a lack of knowledge of the language (think ESL classroom or Classe d’Accueil).
Factors Contributing to or Maintaining Selective Mutism
Predisposing:
➔ Presence of speech and language impairment
➔ Anxiety, wariness and hypersensitivity
➔ Family history of shyness or selective mutism
➔ Family history of other psychiatric illness, especially anxiety
Precipitating:
➔ Separation, loss or trauma
➔ Frequent moves or migration
➔ School or nursery admission
➔ Self-awareness of speech impairment
➔ Teasing and other negative reactions
Perpetuating/Exacerbating
➔ Reinforcement of the mutism by increased attention and affection
➔ Lack of appropriate intervention or management
➔ Over-acceptance of the mutism
➔ Ability to convey messages successfully non-verbally
➔ Geographical or social isolation
➔ Family belonging to an ethnic or linguistic minority
What can I do as a teacher?
In the classroom:
➔ Do not force student to speak;
➔ Consider implementing an IEP;
➔ Minimize anxiety-producing situations;
➔ Classmates need to understand the situation and be encouraged to interact positively with the student;
➔ Make sure the student understands that help/support is available from teachers, other adults, and classmates;
➔ Encourage intrinsic motivation.
BETWEEN AGES 3 AND 8 YEARS OLD
WHAT IS THE AGE OF ONSET OF SELECTIVE MUTISM?
CONSIDER IMPLEMENTING AN IEP; MINIMIZE ANXIETY-PRODUCING
SITUATIONS; SHOW SUPPORT
WHAT CAN I DO AS A TEACHER?

3.Treatment & Intervention

From the Get-go
➔ Treatment in regards to selective mutism is quite critical; treatment/intervention at an early age is very important
➔ Seeking treatment can prevent ongoing mutism and prevents worsening the condition
➔ Ensure an accommodating, supportive environment
3 Types of Treatment
➔ Behavioural strategies ◆ Gradual exposure to social activities/situations
➔ Cognitive-behavioural strategies ◆ Coping thoughts and easing ‘worry thoughts’
➔ Medication ◆ for children who do not respond to behavioural strategies
➔ As teachers, we want to focus on behavioural techniques we can use in the classroom
Classroom/School Interventions➔ Specific intervention techniques used widely:
◆ Sliding-in
◆ Fading
◆ Successive approximation
➔ Encourage the student to participate in structured social activities like team sports
➔ Good morning/goodbye rituals (“See you again!”)
➔ Educating other students and staff
➔ Parental involvement:
◆ Ensuring the child has a proper doctor
◆ Working with the doctor/teacher/parent/child so they can all work together to progress the communication of the student
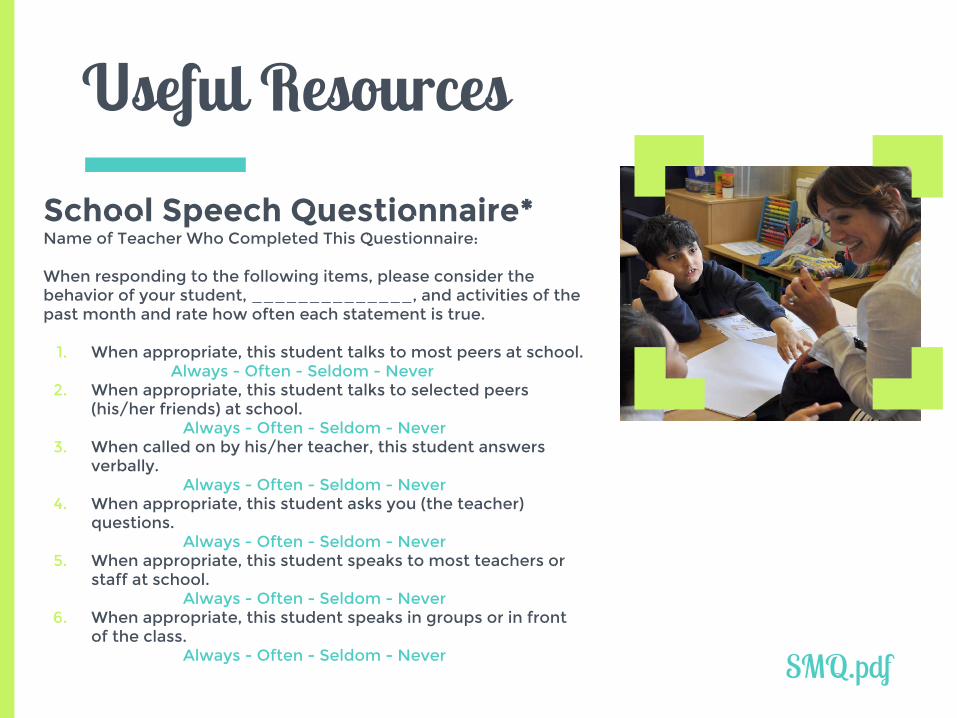
Useful Resources
School Speech Questionnaire*Name of Teacher Who Completed This Questionnaire:
When responding to the following items, please consider the behavior of your student, ______________, and activities of the past month and rate how often each statement is true.
1. When appropriate, this student talks to most peers at school. Always - Often - Seldom - Never
2. When appropriate, this student talks to selected peers (his/her friends) at school.
Always - Often - Seldom - Never3. When called on by his/her teacher, this student answers
verbally.Always - Often - Seldom - Never
4. When appropriate, this student asks you (the teacher) questions.
Always - Often - Seldom - Never5. When appropriate, this student speaks to most teachers or
staff at school.Always - Often - Seldom - Never
6. When appropriate, this student speaks in groups or in front of the class.
Always - Often - Seldom - Never
SMQ.pdf
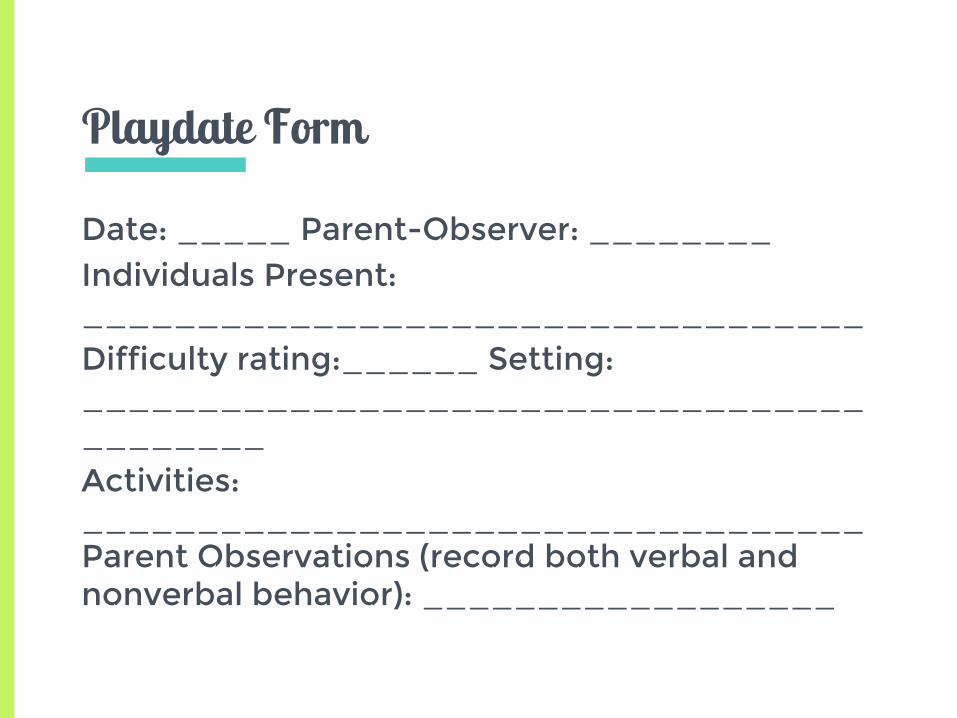
Playdate Form
Date: _____ Parent-Observer: ________Individuals Present: __________________________________Difficulty rating:______ Setting:__________________________________________Activities: __________________________________Parent Observations (record both verbal and nonverbal behavior): __________________
-GRADUAL EXPOSURE TO SOCIAL ACTIVITIES/ SITUATIONS
- COPING THOUGHTS AND EASING “WORRY THOUGHTS”
- MEDICATION

WHAT ARE TREATMENTS FOR SELECTIVE MUTISM?
SLIDING-IN
FADING
SUCCESSIVE APPROXIMATION
WHAT ARE INTERVENTION TECHNIQUES FOR SELECTIVE
MUTISM?

4.Top 10 Myths
Let’s start with the first set of slides
MYTH # 1Selective mutism is extremely rare.
7.1 in every 1,000 (Bergman, 2002)➔ 0.8 per 1,000 (Fundudis, 1979)
➔ Lack of knowledge: inadequate recognition of symptoms
◆ “just shy”
◆ Diagnosed autistic
MYTH # 2Selectively mute children are typically severely emotionally disturbed, usually because they have suffered abuse, neglect or trauma.
➔ Assumed in older case reports, but no evidence is offered
➔ Anxiety causes certain people to be overly sensitive
◆ Normal life events trigger anxious responses (such as selective mutism)
MYTH # 3Families of children with selective mutism are typically dysfunctional.
➔ High incidence of anxiety in close relatives of selectively mute children, but there is no evidence that family pathology causes SM symptoms
➔ Older literature discusses overly- or under-attached mothers to children with SM
◆ Bonding difficulties might be a result rather than a cause

MYTH # 4Selectively mute children use their silence as a form of passive aggression, manipulation, or defiance.
➔ Implies that a children makes a conscious decision to be silent

MYTH # 5Selective mutism is extremely difficult to treat.
➔ Now that we understand it, most children make great progress
➔ What increases the odds of success?
◆ Early diagnosis
◆ Multimodal treatment
MYTH # 6Selective mutism is really just severe shyness; most children will grow out of it.
➔ Shyness is not paralyzing as is selective mutism
➔ Physicians and educators should recommend evaluation of any child meeting the criteria for selective mutism. Otherwise, the window of opportunity for optimal treatment results will be missed.
MYTH # 7Adults who work with selectively mute children should let the children know that there is a firm expectation for speech.
➔ Expectation of speech causes anxiety
➔ SM children need:
◆ Intervention to reduce anxiety
◆ Instruction on recognizing & coping
◆ Support & encouragement
MYTH # 8Selective mutism is a form of autism or is on the autism spectrum.
➔ Behaviour of SM children varies with situation, environment, or audience.
◆ Selective mutism is SELECTIVE… unlike autism
➔ Clinicians are unfamiliar with this disorder
◆ DSM-IV does not recognize all behaviours that come with SM (blank expression, lack of eye contact)
◆ The diagnostic criteria [of DSM-V]are largely unchanged from DSM-IV
MYTH # 9Selectively mute children tend to be below average in intelligence.
➔ Difficult to evaluate by traditional verbal methods
➔ Clinicians that work with large pop. of SM believe that they are above average in intelligence, and that many are gifted
◆ Not proven/more research is needed

MYTH # 10Children with selective mutism usually don’t function well in the mainstream classroom and often shouldn’t be promoted to the next grade level because they aren’t speaking.
➔ Many do well, especially if not pressured to speak
➔ Alternative methods to complete assignments
➔ Children with disabilities have accommodations to place them on a level playing field

5.What can recovered
adults tell us?

5 MAIN THEMES1. Origins of selective mutism
2. Maintenance of selective mutism and the importance of social role
3. Determination, social anxiety and loneliness
4. The recovery process
5. Current psychological adjustment

1. Origins of Selective Mutism
Many recovering adults realized that their selective mutism stemmed from a traumatic experience in their childhood.
2. Maintenance of Selective Mutism and the Importance of Social Role
“ I think they just got used to or thought that, OK, that’s how they are, and there’s not much to do about it. They just accepted it, they gave up. “
3. Determination, Social Anxiety & Loneliness
“We were terribly worried, especially about new situations, unfamiliar situations, different
situations; we were scared to death, new people, especially men and dominating people, authoritarian people, formal situations.”
(Identical Twins)
4. The Recovery Process “I didn’t actually know who I was. I thought it
was normal, that things are like this. It’s only the huge inner anxiety that gave me a clue that this
is not normal and I have to do something.”
5. Current Psychosocial Adjustment
“But I have no limits, I can do it. No one can disconcert me as long as I’m in control.”
SELECTIVE MUTISM IS:-EXTREMELY DIFFICULT TO
TREAT-REALLY JUST SEVERE SHYNESS
-A FORM OF AUTISM
WHAT ARE MYTHS OF SELECTIVE MUTISM?
SUDDEN LOSS OF SPEECH(SHORT TERM)
WHAT IS HYSTERICAL MUTISM?
Thanks!Any questions?
Johnson, M., & Wintgens, A. (2001). The Selective Mutism Resource Manual. Retrieved from http://specialchildren-magazine.com/feature/how-identify-and-support-children-selective-mutism
Kaakeh, Y. & Stumpf, J.L. (2008). Treatment of selective mutism: Focus on selective serotonin reuptake inhibitors. Pharmacotherapy, 28(2), 214-224. Retrieved from Ebsco.
Kehle, T., & Bray, M. (2004). Selective mutism: A primer for parents and educators. The National Association of School Psychologists, 167-169. Retrieved from http://www.nasponline.org/educators/selectivemu
Kehle, T. J., Madaus, M. M. R., Baratta, V. S., & Bray, M. A. (1998). Augmented self-modeling as a treatment for children with selective mutism. Journal of School Psychology, 36(3), 377–399.
Omdal, H. (2007) Can adults who have recovered from selective mutism in childhood and adolescence tell us anything about the nature of the condition and/or recovery from it?, European Journal of Special Needs Education, 22:3, 237-253. Retrieved from Ebsco
Stanley, C. Selective Mutism Group~ Childhood Anxiety Network Speaking Out for Our Children Speaking Out for Our Children.
Stein, M.T., Rapin, I., & Yapko, D. (2001). Challenging case: Developmental delays and regressions. American Academy of Pediatrics, 107, 926-929. Retrieved from Ebsco
UCLA School Mental Health Project. (n.d.). A Personal Look at a Student’s Selective Mutism. Retrieved from http://smhp.psych.ucla.edu/pdfdocs/selectmut.pdf
Bibliography
5 Questions Submitted to prof. Conrod
1. When a child consistently fails to speak when he/she is expected to, (at school or in social situations) this is a symptom of:
a. Intrapersonal Objection Disorderb. Selective Mutismc. Communicative Hesitance Disorderd. Hysterical Mutism
2. Which of the following are treatments for Selective Mutism?a. Gradual exposure to social activities/situationsb. Forceful encouragement to interactc. Coping thoughts and easing worry thoughtsd. A & Be. A & C
3. Selectively mute children are typically severely emotionally disturbed, usually because they have suffered abuse, neglect or trauma
a. Trueb. False
4. Families of children with selective mutism are typically dysfunctional
a. Trueb. False
5. _________________ can be used for children who do not respond to behavioural strategies.