scaling up public-private partnerships to achieve family planning equity goals in india
DESCRIPTION
Scaling up public private partnerships to achieve family planning a researchTRANSCRIPT

Scaling Up Public-Private Partnerships to Achieve Family Planning Equity Goals in India
Suneeta Sharma, PhD MHA, Managing Director, Futures Group India Tanya Liberham, MA, Knowledge Management Officer, Futures Group India

Taking PPP models to scale under Innovations in FP Technical Assistance Project (ITAP): success factors
Four examples
• The Sambhav (“Possible”) Voucher system
• The Accredited Social Health Activist (ASHA) Plus program
• The Mobile Health Van Initiative
• The MerryGold Social Franchise Model
Way forward
Outline

Government (national and state) leadership and ownership
Think scale up from the beginning
Strengthen and build on existing structures and systems
Consultative and transparent process of setting goals and building partnerships
Clearly defined and agreed upon monitoring indicators and performance levels
Follow an active problem solving approach
Sustainable financing
Linkage between proven models and policies
Scale Up: Success Factors

Framework for Strengthening Private Sector Role to Achieve Health Equity Goals
4
Advocacy and Dialogue Action
Public Private
Demand
Policy
Supply
Create an enabling environment
Balance Public Private Sector roles Build Public Private
Partnerships
Analysis
5D Approach
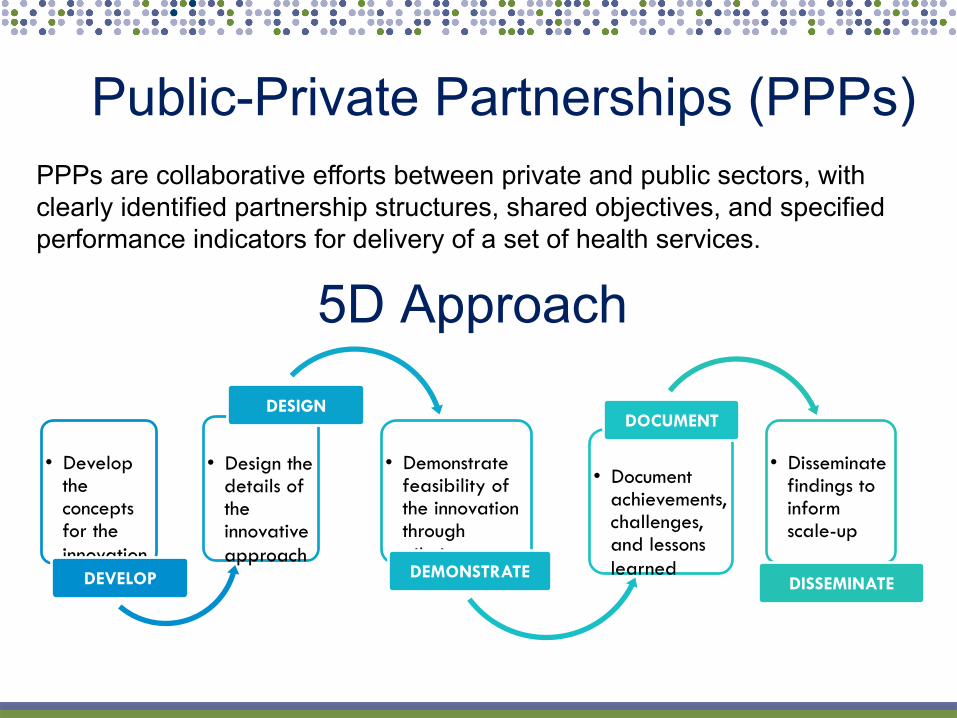
Public-Private Partnerships (PPPs)
PPPs are collaborative efforts between private and public sectors, with clearly identified partnership structures, shared objectives, and specified performance indicators for delivery of a set of health services.
• Develop the concepts for the innovation
DEVELOP
• Design the details of the innovative approach
DESIGN
• Demonstrate feasibility of the innovation through piloting DEMONSTRATE
• Document achievements, challenges, and lessons learned
DOCUMENT
• Disseminate findings to inform scale-up
DISSEMINATE

Sambhav Voucher System To reduce inequities in reproductive health care by enabling access to services, while empowering the below poverty line population to choose their own provider
6
Voucher Management
Agency
Voucher Redemption
Private Nursing Homes
Voucher Redemption
BPL Families Voucher Distribution
ANM/ASHA
Voucher Distribution
Payment for Services

Voucher System Implementation IMPLEMENTATION
SYSTEMS
• Design and conduct baseline survey
• Design, print and distribute vouchers
• Orient ASHAs and community members
• Develop guidelines for identification of BPL families
• Establish and build capacity of VMU
• Develop and implement MIS • Create PNH network • Develop contractual
agreements between Society and VMU, and VMU and PNH
• Develop system for reimbursement for PNH
• Establish referral systems • Design and conduct endline
survey
DEMAND CREATION
• Conduct formative research • Identify communication
needs • Design communication
strategy • Develop BCC/ IEC
materials for PNH and clients
QUALITY ASSURANCE SYSTEMS
• Prepare quality standard guidelines for PNH
• Develop accreditation guidelines
• Assess and accredit PNH • Design client verification
system • Conduct Medical Audit of
PNHs • Conduct Client Satisfaction
Survey • Provide Continuous
Medical Education for PNH

Voucher System Achievements Sambhav voucher system pilots
• 12,500 institutional deliveries
• 44,000 ANC Visits/10,300 PNC visits
• 9,500 FP methods
Uttarakhand: BPL population coverage increased
• from 0.15million in two blocks (Pilot)
• to 2.58 million poor across the state
UP scaled up the urban slum voucher system from one city to eleven cities
Jharkhand: injectables accounted for 43% of modern method use
8 Source: : IFPS Technical Assistance Project (ITAP). 2012. Sambhav: Vouchers Make High-Quality Reproductive Health Services Possible for India’s Poor. Gurgaon, Haryana: Futures Group, ITAP.
26.7
34.8 30.8
53.3
38.5 36
43
54
0
10
20
30
40
50
60
Use of modern contraceptive
use
Institutional delivery
Perc
enta
ge
Improving FP/RH Uptake: Urban and Rural Poor
Agra (rural) Baseline, 2006 Agra (rural) Endline, 2009 Kanpur Nagar (slum) Baseline, 2006 Kanpur Nagar (slum) Endline, 2011

ASHA Plus Program
9
ASHAs unable to sustain themselves covering a smaller number of people than intended
ASHAs introduced under NRHM to promote healthy behaviors
In Uttarakhand, ASHAs faced challenges in providing uniform services due to
• Hilly terrain,
• Small scattered settlements covering large geographical area
• Poor connectivity
• Limited public transport
ASHA Plus program a viable and evidence based Operations Research model
• Piloted in six blocks of three bordering districts
• Flexible population coverage
• Performance based remuneration
• Enhanced training package

Partnerships in ASHA Plus
• Creating awareness & disseminating information
on health programs • Community mobilization
• Organizing community level meetings
• Strengthening linkages
• Recruiting and training of ASHAs
• Supportive supervision • Taking feedback from the
community • Piloting all training materials and tools
• Conceptualize and design program
• Selection of project intervention areas
• Selection of NGOs • Monitoring and review of
the program
• Ensuring financial flows • Training and capacity
building • Coordinating with other
departments • Cooperating with ASHA
Plus worker State
Government ITAP
ASHA plus Workers NGOs

Achievements of ASHA Plus
Scale up:
• 6 blocks to 6 districts
• Population coverage increased from .26million to 3.13million
47 Block Coordinators and 550 ASHA Facilitators support 11,086 ASHA at block and sub block levels
Learning's of ASHA Plus were incorporated in ASHA Support System
Rural Development Institute and 10 NGOs are implementing ARCs across the state

Reaching the Underserved: Mobile Health Vans
A fixed day, fixed time, and fixed place approach to provide primary healthcare services in remote rural areas

Facilitating Implementation Pilot phase Evaluation of early MHV models Van specifications Route design and operations Service provision Personnel Capacity building Community engagement and demand
generation Management and oversight Links to public health system Private sector engagement Cost recovery Financial allocation and expenditures
13
Scale Up • Expansion of MHV operations
in the state • Evaluation of MHVs and design
of a synchronization plan • MHV synchronization strategy • Refinement of monitoring
activities • Financial scale up

Scale up Mobile Health Vans
• Scale up
• From 1 van to 30 vans throughout UK
• Population coverage from 0.5 million to 10 million
• Performance (2010 – 2011)
• Organized 5000 camps
• Reached 300,000 people
IFPS Technical Assistance Project (ITAP). 2012. Reaching Underserved Communities through Mobile Health Vans in Uttarakhand, India. Gurgaon, Haryana: Futures Group, ITAP.

15
MerryGold Social Franchising An innovative, sustainable, for-profit PPP model to deliver maternal
health and family planning services at below market prices
• Business format approach for SUSTAINABILITY THROUGH INNOVATIONS
• Market research fundamental to future growth of the network • Three-tiered approach with a mix of full and fractional franchising • Building brand value: ‘beyond just the logos’ • Linkages with existing government schemes • Franchisor’s role in:
– Building capacities and training – Development of vendors and procurement at competitive prices – Regulating quality assurance systems – Marketing of the network

Partnerships in Social Franchising • Support formation and operation of
network • Overall management • Monitor the project • Benchmark formulation and report
to USAID
• As the franchisor, recruit qualified franchisees
• Build and market the brand; Define guidelines and protocols
• Manage the network • Build capacities of franchisees • Quality assurance • Reporting to SIFPSA
• Design and develop the network • Process documentation and
dissemination • Conduct periodic studies and
assessments
• Adherence to network guidelines • Provide quality services to
‘clients’ at pre-determined prices • Conduct outreach activities • Quality management at facility

Social Franchising Achievements
17
Performance during Oct 2007 – February 2012
• 756,100 antenatal checkups
• 133,900 deliveries
• 10,600 sterilizations
• 38,200 IUCD insertions
• >1 million CYPs generated so far
Under consolidation phase, included in the Program Implementation Plan (PIP) 2013
Replicating the same model in Rajasthan
Source: IFPS Technical Assistance Project (ITAP). 2012. Social Franchising as a Public Private Partnership Model - Lessons Learned from the MerryGold Health Network of Uttar Pradesh, India. Gurgaon, Haryana: Futures Group, ITAP.
L1
L2
L2
L2
L2
L3 L3
L3
L3
L3 L3
L3
L3
L0
Hub and Spoke model of MGHN
Extending Best Practices DFID RH Framework – Family Planning
(Bihar and Orissa)
• Social franchising, social marketing and innovative PPP models
USAID PIPPSE Project – HIV/AIDS (UP, Uttarakhand, Rajasthan)
• Employer led models
• PPP structures and roadmap
• PPP course
Global Fund – Malaria (7 north eastern states)
• Private sector mapping, capacity building, and engagement
18

Thank You!