routine chest radiographs in the surgical intensive … · routine chest radiographs in the...
TRANSCRIPT
Daily routine chest radiographs (CR) are com-monly performed in surgical ICU. UnnecessaryCR increase costs and expose the staff and thepatients to radiation risk. The goal of our stu-dywas to estimate the value of daily routine CR inthe ICU and to determine the correlation between CR and physical findings in surgical ICU pati-
ents. Prospective observational study was conductedduring period of two months at the ICU department atthe Clinic for Digestive Surgery, Clinical Center of Se-rbia, Belgrade. It included 97 consecutive patients whounderwent digestive surgery and stayed at the ICU forat least two days. During their ICU stay, CRs were ob-tained as a clinical routine or to monitor lung pathol-ogy. Patients were followed daily, and CRs (as the pro-portion of positive findings) were compared with phy-sical examination and clinical presentation. A total of717 CRs were obtained, median number per patientwas 4.0 (2.0-7.0). Proportion of positive findings wassignificantly higher comparing to auscultation untilthe sixth day of ICU stay. There was no difference inCR findings from day to day after the sixth day. The-rapeutic efficacy of CRs was low as only 56 (7.8%) re-sulted in a change of patient management. We conclu-de that daily routine CRs are justified in the first sixdays of ICU stay, and after that time they show no ad-vantages over clinical examination.
Key words: radiography, thoracic - intensive care unit -therapeutic efficacy - postoperative period
INTRODUCTION
Chest radiographs (CRs) are commonly performed insurgical intensive care units (ICUs). Some of them
are obtained as dictated by protocols, after interven-tions such as thoracotomy, central venous catheter pla-
cement or intubation, and others for monitoring ofpulmonary pathology (pneumonia, atelectasis, pleuraleffusions, pneumothorax, etc).1
CRs are frequently made on a daily basis, as a part of asurgical ICU daily routine, irrespective of a patient’s cli-nical status and the clinical judgement of the intensivist.2
The main purpose of any CR is to reveal an abnormalitythat otherwise wouldn’t be detected and help in diagnosticand therapeutic decision making. According to until re-cently valid recommendations of American College ofRadiology (ACR), routine daily CRs were indicated forpatients with acute cardiopulmonary problems and thosetreated with mechanical ventilation. Following of theserecommendations would include almost all ICU patients.However, this practice has become a subject of numerousdebates over the efficacy of CRs in ICU patients and thusthe value of routine daily monitoring. They resulted inchange of ACR guidelines which restrict the use of routi-ne daily CRs in patients with acute cardiopulmonary prob-lems and suggest follow-up CRs only when clinically in-dicated.3 CRs have high accuracy in detecting malpositionof medical devices used in critically ill patients such asendotracheal tubes, central venous lines and thoracicdrains.4 There are studies with findings that support dailyCRs in surgical ICU, in subpopulation of mechanicallyventilated patients and those with pulmonary artery cathe-ters.5,6 Many others advocate different strategy of obtain-ing on-demand CRs, when indicated and specifically re-quested by the intensivist. This approach is based on re-sults that showed low diagnostic and therapeutic efficacyof routine daily CRs, demonstrating that abandoning thispractice doesn’t adversely affect clinical outcome of ICUpatients.7,8,9 Multiple studies have shown that daily CRsdon’t reveal new information, at the same time increasingcosts and exposing patients and the staff to radiation ri-sk.7,10
The practice of routine CRs in surgical ICU patients iswidespread in Serbia, and there were no studies to questi-on and confirm its value, specially in a limited resourcessetting.The aim of our study was to estimate the value ofdaily routine CRs in the surgical ICU and to determine theco-rrelation between CRs, clinical presentation andphysical findings.
. ........................................
Routine chest radiographs in the surgical intensivecare unit: Can we change clinical habits with noproven benefit?
Jelena V. Veli~kovi}1, Sanela A. Hajdarevi}1, Ivan G. Palibrk1,2,Nataša R. Jani}1, Marija Djukanovi}1, Bojana Miljkovi}1, DejanM.Veli~kovi}1,2, Vesna Bumbaširevi}1,2 1Center for Anesthesiology and Reanimatology, Clinical Center ofSerbia, Belgrade2University of Belgrade, Faculty of Medicine, Belgrade
/STRU^NI RADUDK 617.3:616.24-073-7
DOI:10.2298/ACI1303039V
rezi
me

MATERIAL AND METHODS
We conducted a prospective observational study evalua-ting the clinical value of daily routine CRs during periodof two months. The study was performed at the ICU de-partment of the Clinic for Digestive Surgery, ClinicalCenter of Serbia, Belgrade which is a university-affiliatedteaching hospital, from November 2012 till January 2013.Its ICU is a 14-bed "open format" department with surgi-cal patients only and permanent physician staff consistingof one surgeon, one anesthesiologist and two residents.
The study included all patients expected to stay at theICU more than two days (after surgery or admission forother reasons) in whom CRs were performed according toICU protocol day after day. The ICU policy is to orderCR in all admitted patients soon after admission.
According to the study protocol, ICU physicians duringtheir morning round recorded patients’ clinical presentati-on and did the physical examination (inspection, ausculta-tion, thoracic percussion, etc). Afterwards, daily routineCRs were obtained in all mechanically ventilated patients,all patients with pulmonary pathology or thoracic surgeryand patients in whom chest recording was dictated by theprotocol of their surgical ward. Only routine CRs wereevaluated. Additional on-demand CRs, made later duringthe day, because of clinical deterioration or placement of anew device (ET tube, chest drain, central venous line, fee-ding tube) were not analyzed.
To evaluate the CRs, a formatted questionnaire was de-signed, including patient’s demographic data, diagnosis,surgery, indication for ICU admission and stay, as well asdata about comorbidities and preadmission CRs. Radio-logic section of the form contained radiologic findings,which were labeled for the sake of simplicity just as "posi-tive" or "negative". Radiologic positive findings were pre-defined as shown in Table 1. Physical examination resultswere also categorized as "positive" or "negative" on dis-cretion of the attending physician. It was also noticed ifCR finding influenced the change in patient managementplan and the physician’s judgement about whether the CRwas clinically indicated. Therapeutic efficacy of CR wasexpressed as the ratio of CRs resulting in change oftherapy and the total number of CRs.
Data were prospectively collected and entered into adatabase (Microsoft Excel 2007). They are expressed asmean (+SD) or median (+IQR). CR findings (expressed asthe proportion of positive results) were compared withclinical presentation and physical findings. Data wereanalyzed with Cochran’s Q test and differences werecompared with X2 test using statistical software (SPSSversion 19). P value < 0.05 was considered statisticallysignificant.
RESULTS
During the two month study period, 97 patients wereevaluated through 108 ICU admissions (97 postoperativ-elly and 11 as ICU readmission). Since majority of read-missions were due to respiratory failure, for the sake ofcomparability, only postoperative admissions to ICU werefinally analyzed. A total of 717 daily routine CRs wereobtained (620 of them as routine daily control). The me-dian number of CRs per patient was 4.0 (IQR,2.0-7.0).Mean number of CRs taken prior to admission to ICU was
1.7(+ 1.1). The average length of ICU stay was 6.0 days(3.0-11.0) and the longest stay was 28 days. Mechanicalventilation was performed in 43 patients for at least oneday. Demographic and clinical patient characteristics arepresented in table 2.
The first evaluated routine daily CRs were done on thesecond day of patient’s ICU stay (first routine control). Of97 CRs obtained during that day, only 25(25.8%) revealeda predefined positive radiologic finding, while only15(15.5%) patients had a positive finding on auscultationand 14(14.4%) of them exhibited a clinical presentationindicating pulmonary abnormality (p=0.01). Proportion ofpositive findings on CRs was significantly higher com-paring to auscultation and clinical feature until the sixth
TABLE 1
PREDEFINED CR FINDINGS
Radiologic positive finding Comment
Pulmonary infiltrates Any type or size
Atelectasis Segmental or lobar
Pulmonary congrestion
Pneumothorax/Pneumomediastinum Any air collection
Pleural effusion
Mediastinal abnormalityMediastinal wideningor distension ofesophageal substituent
Device malposition
Central venous catheter Tip of the cahteter notin the superior vena cava
Tracheal tube <2 cm from carina
Chest tube Outside thorax, toodeep or twisted
TABLE 2
DEMOGRAPHIC AND CLINICAL DATA
Variable Value
Patients 97
Male gender 49/50.5/
Age, years 61.8+18.2
Respiratory comorbidity 11/11.3/
Smoker 33/34.0/
Reason for ICU admission
Abdominal surgery 72/74.8/
Thoracic surgery 25/25.8/
Mechanical ventilation 43/44.3/
ICU lenght of stay, days (median/IQR/)
6/3-11/
Data are expressed as number (%) and mean standard deviationunless stated otherwise; IQR-interquartile range
40 J. Velickovic et al. ACI Vol.LX

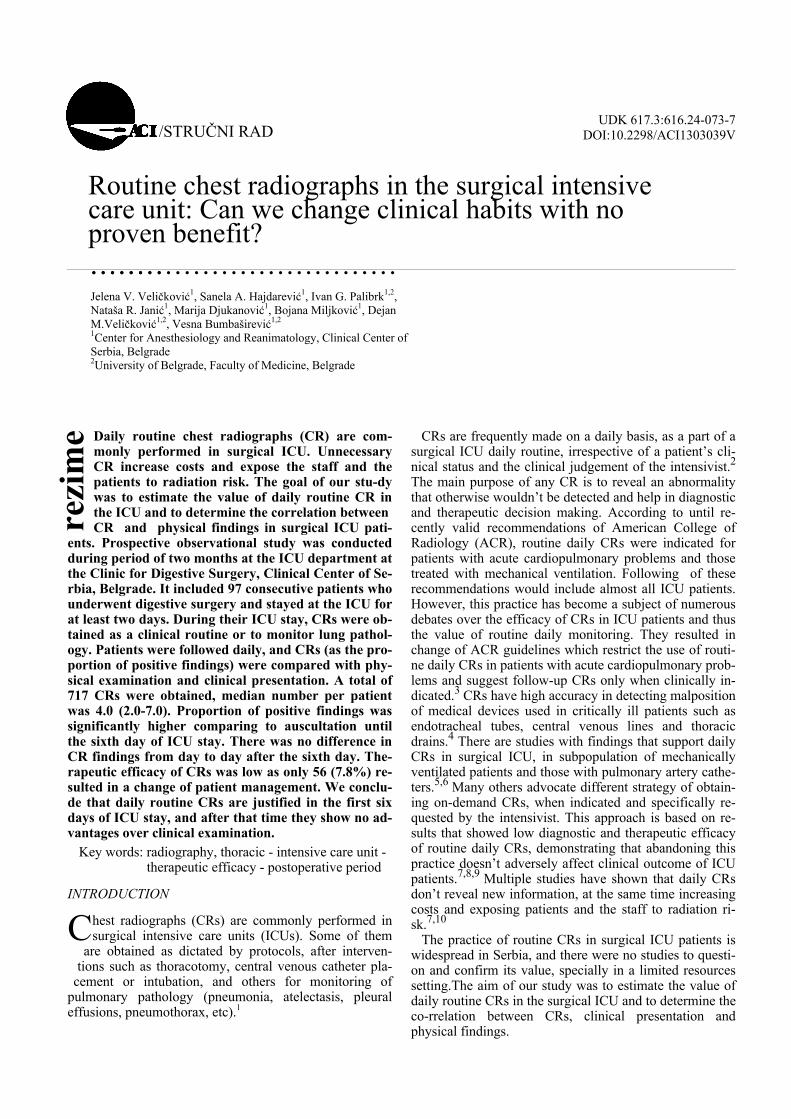
day of ICU stay, and after that there were no differencesuntil discharge from ICU, suggesting that a chest abnor-mality could have been detected similarly with CR andphysical examination (Table 3; Figure 1). There was nosignificant difference in CR findings from day to day afterthe sixth day (p>0.05).
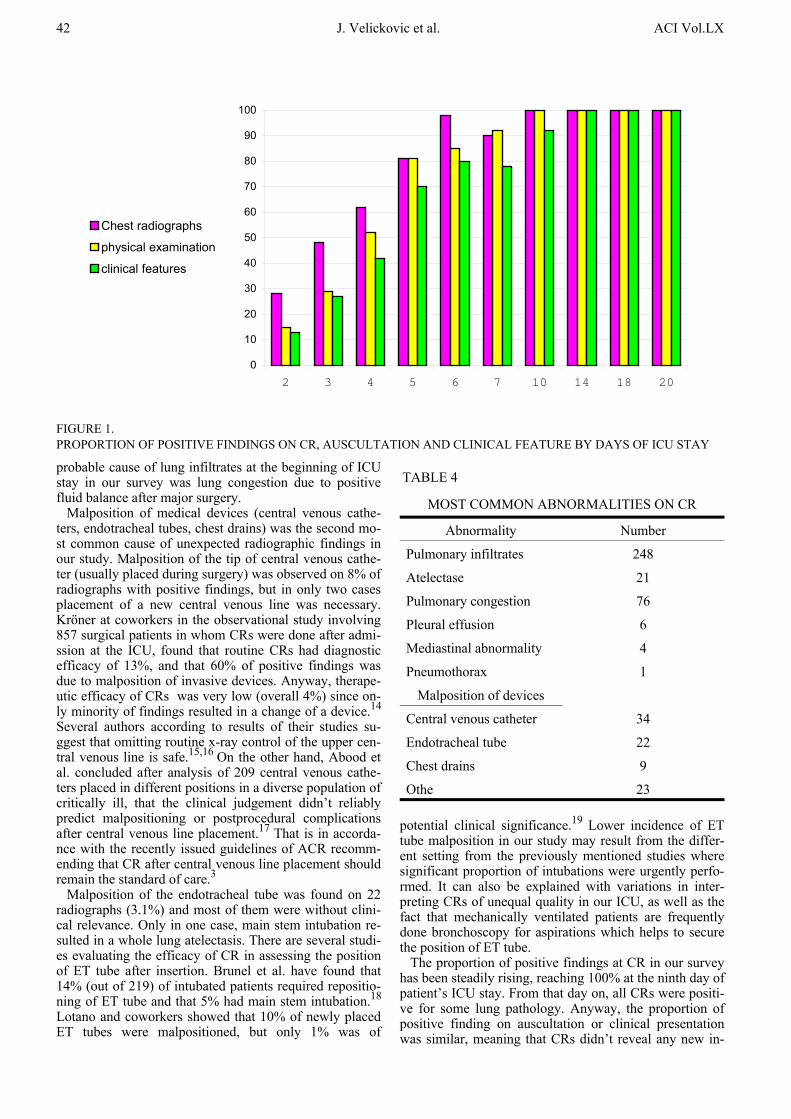
Total number of control CRs with positive findings was424 (out of 620; 68.4%) The most common CR abnorma-lities were pulmonary infiltrates, atelectases, severe pul-monary congestion, pleural effusion, malposition of endo-tracheal tube, malposition of chest drains, distension ofgastroplasty or coloplasty and pneumothorax. (Table 4)However, the therapeutic efficacy of CRs was very low asin only 56(7.8%) CRs positive finding resulted in a chan-ge of patient management (most commonly bronchosco-py, thoracocenthesis, thoracic drainage, administration ofantibiotics and diuretics).
Attending physicians considered that 401 out of 717CRs (55.9%) were unnecessary (not clinically indicated)and in just 6 cases those CRs resulted in a change of pati-ent therapy.
DISCUSSION
The present study was undertaken to investigate the va-lue of routine daily CRs in a surgical ICU and to compareit to physical examination and clinical presentation.
The main findings of our survey can be summarized asfollows: 1) The ability of daily routine CR to reveal moreinformation than physical findings and clinical feature istime dependent and is higher at the beginning of ICU stayand 2) Daily routine CRs have low therapeutic efficacy inpostsurgery ICU patients.
Although physical examination, lung auscultation andchest radiography are the most commonly used methodsof bedside clinical evaluation of lung pathology, to date,only a few studies have compared their diagnostic perfor-mance in ICU patients. Lichtenstein et al. prospectivelystudied 32 patients with ARDS in order to compare diag-nostic efficacy of auscultation, CR and lung ultrasoundwith computed tomography, when diagnosing three enti-ties of lung pathology: pleural effusion, alveolar consoli-dation and alveolar-interstitial syndrome.11 They foundthat the diagnostic accuracy of auscultation was 61% for
pleural effusion, 36% for alveolar consolidation and 55%for alveolar-interstitial syndrome, while for bedside CR itwas 47%, 75% and 72% respectively. Lung ultrasoundappeared to be the most sensitive and specific methodwith accuracy over 90%, and was the only one that couldquantify the extent of lung injury. Graat and coworkersshowed an extremely low sensitivity (2.1%) of ICU clini-cians in predicting abnormalities on daily routine CRs intheir prospective observational study conducted in a 28-bed mixed medical/surgical ICU.(8) It is very much incontrast with results of Bhangwanjee and Muckart whofound that sensitivity of examiners in predicting signifi-cant changes on CRs was 93% and 97%.12 The authorsconcluded that clinical examination can effectively predictthe need for CR in ventilated ICU patients. The differencein findings of previous studies might be the result of diffe-rences in study populations and ICU setting as well as stu-dy design, since in study of Bhangwanjee and Muckart thethorough auscultation was performed in search for abnor-malities, while in survey of Graat et al. the prediction ofCR changes was based rather on general impression of theattending physician.
Our results showed that CR abnormality couldn’t havebeen accurately predicted with auscultation or clinical fea-ture during the first six days of ICU stay. Abnormalitiesthat couldn’t have been detected with clinical examinationduring that time in majority of cases were new or progre-ssive pulmonary infiltrates, atelectases (less than 2 lobes)and malposition of medical devices. In one case, pneumo-thorax that required chest drainage was missed. Pulmo-nary infiltrates have been shown to be the most frequentlyunrecognized lung abnormality on physical examinationin majority of studies, although their nature and clinicalrelevance haven’t been specified.7,8 Diverse etiologies areresponsible for pulmonary infiltrates in surgical ICU pa-tients. In only 30% they are due to pneumonia, anotherthird origin from lung edema, while acute lung injury andatelectases account for the remaining.13 In our study, anypulmonary infiltrate (even minor) was treated as positiveradiologic finding which possibly overestimated their in-cidence and since the majority of patients were admittedto the ICU after major elective surgery (with normal CR),it may explain why clinicians didn’t suspect pneumonia oracute lung injury during the first six days. The most
TABLE 3
POSITIVE FINDINGS ON CHEST RADIOGRAPH, AUSCULTATION AND CLINICAL PRESENTATION
Day Number of patients Chest radiograph Auscultation Clinical presentation P value
2 97 25 (0.26) 15 (0.16) 14 (0.15) 0.01
3 74 28 (0.38) 22 ( 0.30) 19 (0.26) 0.02
4 58 36 (0.62) 31 (0.53) 25 (0.43) 0.002
5 42 35 (0.83) 35 (0.83) 30 (0.71) 0.062
6 36 34 (0.94) 30 (0.85) 28 (0.78) 0.042
7 34 30 (0.88) 29 (0.85 ) 28 (0.82) 0.3
8 22 21 (0.95) 21 (0.95) 19 (0.86) 1.35
9 17 17 (1.00) 16 (0.94) 14 (0.82) 0.97
Data are expressed as number (proportion) of patients with positive findings
Br. 3 Routine chest radiographs in the surgical intensive care: 41can we change clinical habit with no proven benefit?
probable cause of lung infiltrates at the beginning of ICUstay in our survey was lung congestion due to positivefluid balance after major surgery.
Malposition of medical devices (central venous cathe-ters, endotracheal tubes, chest drains) was the second mo-st common cause of unexpected radiographic findings inour study. Malposition of the tip of central venous cathe-ter (usually placed during surgery) was observed on 8% ofradiographs with positive findings, but in only two casesplacement of a new central venous line was necessary.Kröner at coworkers in the observational study involving857 surgical patients in whom CRs were done after admi-ssion at the ICU, found that routine CRs had diagnosticefficacy of 13%, and that 60% of positive findings wasdue to malposition of invasive devices. Anyway, therape-utic efficacy of CRs was very low (overall 4%) since on-ly minority of findings resulted in a change of a device.14
Several authors according to results of their studies su-ggest that omitting routine x-ray control of the upper cen-tral venous line is safe.15,16 On the other hand, Abood etal. concluded after analysis of 209 central venous cathe-ters placed in different positions in a diverse population ofcritically ill, that the clinical judgement didn’t reliablypredict malpositioning or postprocedural complicationsafter central venous line placement.17 That is in accorda-nce with the recently issued guidelines of ACR recomm-ending that CR after central venous line placement shouldremain the standard of care.3
Malposition of the endotracheal tube was found on 22radiographs (3.1%) and most of them were without clini-cal relevance. Only in one case, main stem intubation re-sulted in a whole lung atelectasis. There are several studi-es evaluating the efficacy of CR in assessing the positionof ET tube after insertion. Brunel et al. have found that14% (out of 219) of intubated patients required repositio-ning of ET tube and that 5% had main stem intubation.18
Lotano and coworkers showed that 10% of newly placedET tubes were malpositioned, but only 1% was of
potential clinical significance.19 Lower incidence of ETtube malposition in our study may result from the differ-ent setting from the previously mentioned studies wheresignificant proportion of intubations were urgently perfo-rmed. It can also be explained with variations in inter-preting CRs of unequal quality in our ICU, as well as thefact that mechanically ventilated patients are frequentlydone bronchoscopy for aspirations which helps to securethe position of ET tube.
The proportion of positive findings at CR in our surveyhas been steadily rising, reaching 100% at the ninth day ofpatient’s ICU stay. From that day on, all CRs were positi-ve for some lung pathology. Anyway, the proportion ofpositive finding on auscultation or clinical presentationwas similar, meaning that CRs didn’t reveal any new in-
0
10
20
30
40
50
60
70
80
90
100
2 3 4 5 6 7 10 14 18 20
Chest radiographs
physical examination
clinical features
FIGURE 1. PROPORTION OF POSITIVE FINDINGS ON CR, AUSCULTATION AND CLINICAL FEATURE BY DAYS OF ICU STAY
TABLE 4
MOST COMMON ABNORMALITIES ON CR
Abnormality Number
Pulmonary infiltrates 248
Atelectase 21
Pulmonary congestion 76
Pleural effusion 6
Mediastinal abnormality 4
Pneumothorax 1
Malposition of devices
Central venous catheter 34
Endotracheal tube 22
Chest drains 9
Othe 23
42 J. Velickovic et al. ACI Vol.LX

formation. In studies performed on adult surgical or me-dical ICU patients the incidence rate of abnormal findingsvaries widely. If they screened both for malposition ofmedical devices and cardiopulmonary pathology, the inci-dence of positive findings varied from as low as 3% to91%.20,21 Some of these studies classified positive CR fin-dings as new or old, expected or unexpected, major or mi-nor, unlike our study where a "positive CR finding" wascounted as present no matter of kind or extent of abnor-mality. Only 7.8% of all performed CRs in our study in-fluenced a patient care by change of patient managementplan, showing that only a small proportion of positive CRswas of substantional clinical relevance. In the study bySilverstein et al., although a total incidence rate of posi-tive CR findings was 91%, only 1.3% of CR required achange of malpositioned device, and only 12% of CRsshowed a new cardiopulmonary finding with only 3 ofthem (3.7%) with potential clinical impact.21 A prospec-tive study of Tolsma and coworkers in a population of po-stcardiosurgery patients showed that 33.5% of postopera-tive CRs revealed some abnormality, while only 2.4% ledto an intervention.22 Several other studies demonstratedsimilar results.8,23
It is interesting to notice that in our study intensivistsjudged a high number (401/717) of CRs to be unnecessa-ry. The results of a French survey conducted among 82 in-tensivists from 32 ICUs revealed that there was no conse-nsus about the necessity of CR in various clinical situa-tions. Anyway, 75% of ICU specialists that completed thequestionnaire didn’t deem that routine daily CRs were in-dicated in intubated patients.24 Randomized, controlledstudy comparing routine vs restrictive prescription strate-gy of CRs demonstrated that 885 CRs were obtained inthe routine group, while only 94 CRs were done in the re-strictive (clinically indicated) group during the same pe-riod.10 The rate of new findings was 7,2% and 66% res-pectively, suggesting significantly higher value of clini-cally indicated CRs.
There are several limitations of our study that need to bementioned. First, radiographic findings were not classifiedas minor or major. Also, it wasn’t obvious from the ques-tionnaire whether the positive findings were old or new,and if old, whether they have been in progression or re-gression. It would add a valuable information and allowfurther and more detailed analysis of appropriateness ofdaily routine CRs. Second, CRs were interpreted by ICUphysicians and not radiologists, but it represents a stan-dard practice in our ICU and it is very unlikely that theimportant findings were missed. Third, there was a smallnumber of patients who spent a long time at the ICU. Ma-ybe the results would have been different if the surveil-lance period had been longer.
We conclude that, according to our findings, the dailyroutine CRs in surgical ICU patients are justified in the fi-rst six days of ICU stay. After that time, routine CRsshow no advantage over clinical examination. Low rate ofCR induced therapy changes indicates that it would bemore rational to implement the strategy of clinically indi-cated (on demand) CRs or to replace CRs with alternativesafe and reliable technique such as the lung ultrasound.25 Further studies are needed to confirm that abandoningdaily routine CRs in open format surgical ICU is safe andcost saving.
SA@ETAK
Rutinske radiografije grudnog koša (RGK) se ~estoizvode u hirurškim jedinicama intenzivnog le~enja (JIL).Nepotrebne RGK pove}avaju troškove le~enja i izla‘uosoblje i bolesnike riziku od x-zra~enja. Cilj našeg is-tra‘ivanja je bio da proceni opravdanost svakodnevnih,rutinskih RGK u JIL i ispita korelaciju izmedju RGK ifizikalnog nalaza kod hirurških bolesnika u JILu.Prospektivna opservaciona studija u trajanju od dvameseca izvedena je na odeljenju intenzivnog le~enja priKlinici za digestivnu hirurgiju Klini~kog centra Srbije uBeogradu. Ona je obuhvatila 97 uzastopnih bolesnikapodvrgnutih operacijama na digestivnom sistemu, koji suu JIL proveli najmanje dva dana. Tokom njihovogboravka u JIL, RGK su sprovodjene rutinski ili u ciljupra}enja plu}ne patologije. Bolesnici su pra}enisvakodnevno, a RGK (izra‘ene kao proporcija pozitivnihnalaza) poredjene su sa fizikalnim pregledom i klini~komslikom. Na~injeno je ukupno 717 RGK (medijana popacijentu 4.0 (2.0-7.0)). Proporcija pozitivnih nalaza naRGK je bila zna~ajno viša u odnosu na auskultaciju došestog dana boravka u JILu. Nije bilo zna~ajne razlike unalazu RGK od dana do dana nakon šestog dana boravkau JIL. Terapijska efikasnost RGK bila je niska jer je samo56 (7.8%) dovelo do promene u terapijskom planu.
Zaklju~ak: Svakodnevne rutinske RGK su opravdanetokom prvih šest dana boravka u JIL, a nakon toga onenemaju prednost u odnosu na klini~ki pregled.
Klju~ne re~i: Radiografija grudnog koša - Jedinicaintenzivog le~enja - Terapijska efikasnost- Postoperativni period
REFERENCES
1.Trotman-Dickenson B. Radiology in the intensive careunit (Part I). J Intensive Care Med 2003; 18:198-210
2. Graat ME, Hendrikse KA, Spronk PE, et al. Chestradiography practice in critically ill patients: a postalsurvey in the Netherlands. BMC Med Imaging 2006; 6-8
3. American College of Radiology. Routine chest radi-ographs in ICU patients. Available at: http://www.acr.org/departments/appropriateness_criteria.AccessedJuly 2013
4. Henschke CI, Yankelevitz DF, Wand A, Davis SD,Shiau M. Accuracy and efficacy of chest radiography inthe intensive care unit. Radiol Clin North Am 1996;34:21-31
5. Horst HM, Fagan B, Beute GH. Chest radiographs insurgical intensive care patients: a valuable "routine". He-nry Ford Hosp Med J 1986;34(2):84-6
6. Hall JB, White SR, Karrison T. Efficacy of dailyroutine chest radiographs in intubated, mechanically ven-tilated patients. Crit Care Med 1991;19(5):689-93
7. Hendrikse KA, Gratama JWC, Hove W, Rommes JH,Schultz MJ, Spronk PE. Low value of routine chest radio-graphs in a mixed medical-surgical ICU. Chest 2007;132(3):823-8
8. Graat ME, Choi G, Wolthuis EK, et al. The clinicalvalue of daily routine chest radiographs in a mixes medi-cal-surgical intensive care unit is low. Crit Care 2006;10(1):R11
Br. 3 Routine chest radiographs in the surgical intensive care: 43can we change clinical habit with no proven benefit?

9. Oba Y, Zaza T. Abandoning daily routine chestradiography in the intensive care unit: meta-analysis.Radiology 2010;255(2):386-95
10. Clec’h C, Simon P, Hamdi A, et al. Are dailyroutine chest radiographs useful in critically ill,mechanically ventilated patients? A randomized study.Intensive Care Med 2008;34(2):264-70
11. Lichtenstein D, Goldstein I, Mourgeon E, Cluzel P,Grenier P, Rouby JJ. Comparative diagnostic performan-ces of auscultation, chest radiography, and lung ultrasono-graphy in acute respiratory distress syndrome. Anesthesi-ology 2004;100:9-15
12. Bhagwanjee S, Muckart DJ. Routine daily chestradiography is not indicated for ventilated patients in asurgical ICU. Intensive Care Med 1996;22:1335-8
13. Singh N, Falestiny M, Rogers P, et al. Pulmonaryinfiltrates in the surgical ICU. Prospective assessment ofpredictors of etiology and mortality. Chest 1998; 114:1129-36
14. Kröner A, Iperen E, Horn J, et al. The low thera-peutic efficacy of postoperative chest radiographs for sur-gical intensive care unit patients. Minerva Anesthesiol2011;77:147-53
15. Lessnau KD. Is chest radiography necessary afteruncomplicated insertion of a triple-lumen catheter in theright internal jugular vein, using the anterior approach?Chest 2005;127(1):220-3 6
16. Molgaard O, Nielsen MS, Handberg BB, Jansen JM,Kiaegaard J, Juul N. Routine x-ray control of upper cen-tral venous lines: Is it necessary? Acta Anesthesiol Scand2004;48(6):685-9
17. Abood GJ,Davis KA, Esposito TJ, Luchete FA,Gamelli RL. Comparison of routine chest radiograph ver-sus clinician judgment to determine adequate central lineplacement in critically ill patients. J Trauma 2007:63(1):50-6
18. Brunel W, Coleman D, Schwarty DE, Peper E,Cohen NH. Assessment of routine chest roentgenogramsand the physical examination to confirm endotracheal tu-be position. Chest 1989;96:1043-5
19. Lotano R, Gerber D, Aseron C, Santarelli R, PratterM. Utility of postintubation chest radiographs in the inten-sive care unit. Crit Care 2000;4(1):50-3
20. Hall JB, White SR, Karrison T. Efficacy of daily ro-utine chest radiographs in intubated, mechanically venti-lated patients. Crit Care Med 1991;19(5):689-93
21. Silverstein DS, Livingston DH, Elcavage J, KovarL, Kelly KM. The utility of routine daily chest radiogra-phy in the surgical intensive care unit. J Trauma 1993;35:643-6
22. Tolsma M, Kröner A, Hombergh CLM, et al. Theclinical value of routine chest radiographs in the first 24hours after cardiac surgery. Anesth Analg 2011;112:139-42
23. Ruza GC, Moritz RD, Machado FO. Re chest radio-graphy in intensive care: impact on decision-making. RevBras Ter Intensiva 2012;24(3):252-7
24. Hejblum G, Ioos V, Vibert JF, et al. A web-basedDelphi study on the indications of chest radiographs forpatients in ICUs. Chest 2008;133(5):1107-12
25. Ioos V, Galbois A, Chalumeau-Lemoine L, GuidetB, Maury E, Hejblum G. An integrated approach for pres-cribing fewer chest x-rays in the ICU. Ann Intensive Care2011; 1(1):4
Note: Results of this paper were presented in part as a posterpresentation at the Second Congress of Intensive Care Medicine, heldin Belgrade, 22-24 of May 2013. The poster was awarded as the bestpresentation by international jury.
44 J. Velickovic et al. ACI Vol.LX