retina and retinal vascular diseases dr mahmood fauzi assist prof ophthalmology al maarefa college
TRANSCRIPT

Retina and retinal vascular diseases
Dr Mahmood FauziASSIST PROF OPHTHALMOLOGY
AL MAAREFA COLLEGE

Objectives
Explain the clinical anatomy of retina and retinal microcirculation
Enumerate retinal diagnostic procedures -Retinal examination
Describe patho-physiology and clinical presentation and management of retinal vascular disorders ie- (a) Periphlebitis (b) Central retinal artery/ vein occlusion (c)Retinopathy-diabetic and hypertensive
• Other retinal conditions(Macular Degeneration, Retinitis Pigmentosa, Retinal Detachment, Retinal Dystrophy,Retinoblastoma)


Clinical anatomy of retina
Retina converts light rays into electrical impulses and sends towards brain through optic nerve.
Contain photoreceptors-rods and cones. Blood supply The central retinal artery(branch of
opthalmic artery) enters the globe from the center of the optic nerve, immediately adjacent and parallel to the exiting central retinal vein.
Inner layer→ central retinal vascular system
Outer layer→ choroid(ciliary vascular system)
Macula lutea→ choriocapillaries Inner barrier(blood–retina
barrier) Dense connection of retinal capillary endothelium
Outer barrier(choroid-retina barrier)
zonula occludens between the RPE RPE- Bruch’s membrane +choriocapillaries complex
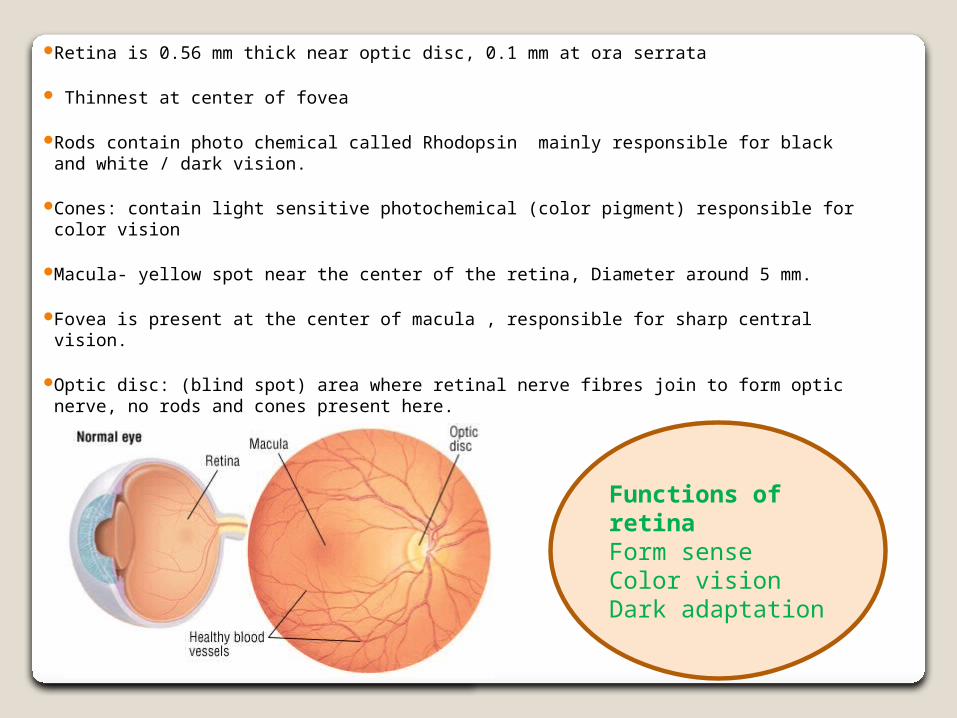
Retina is 0.56 mm thick near optic disc, 0.1 mm at ora serrata
Thinnest at center of fovea
Rods contain photo chemical called Rhodopsin mainly responsible for black and white / dark vision.
Cones: contain light sensitive photochemical (color pigment) responsible for color vision
Macula- yellow spot near the center of the retina, Diameter around 5 mm.
Fovea is present at the center of macula , responsible for sharp central vision.
Optic disc: (blind spot) area where retinal nerve fibres join to form optic nerve, no rods and cones present here.
Functions of retinaForm senseColor visionDark adaptation


Diagnostic Procedures Of Retina
Fundus examination by Ophthalmoscopy (A) Direct Ophthalmoscopy (B) In-Direct OphthalmoscopySlit lamp examination with 70-9O D
Digital Fundus Photography
Fluorescein angiography
Ultrasonography b-scan
Optical coherence tomography(OCT)

Retinal examinationIn-Direct OphthalmoscopyDirect Ophthalmoscopy


Indirect slit-lamp biomicroscopy

Fluorescein Angiography

Optical coherence tomography(OCT)

Ocular ultrasound

Retinal vascular disorders


Periphlebitis retinae Inflammation of the wall of the retinal veins commonly due to
1. tuberculosis (Mycobacterium tuberculosis).2. Sarcoidosis, 3. multiple sclerosis,4. Eales Disease (“periphlebitis retinae).
Cause hemorrhages in retina and vitrus Commonly effect adult(20-30 year) Cause sudden loss of vision due to vitrus hemorrhage Treatment Control the basic eitiology Corticosteroid help to control inflammation Photocoagulation (laser) of leakage area

Central retinal artery occlusion-CRAO
It is obstruction of the circulation of the retina due to embolus and thrombosis.
Caused by hypertension and arteriosclerosis .
Commonly results in complete or permanent blindness.
FFA in CRAO- complete absence in filling central retinal artery

Symptoms
Signs
Sudden painless vision lose of one eye
Direct light reflex disappear, indirect light reflex normal
Retinal edema、 cherry-red spotRetina artery narrowing, retinal hemorrhages
Treatment Vasodilator (acetylencholine p.s effect) dilate the spasm artery acetylsalicylic acid(aspirin) to prevent clot formation

Central retinal vein occlusion - CRVO Obstruction due to veins circulation thrombosis and embolus Caused by hypertension , Arteriosclerosis Predisposing factor advancing age Causes sudden impairment of vision not sudden loss of vision
Ischemic type CRVO Non-Ischemic type CRVO

TYPES : Nonischemic CRVO is milder form of disease. May
present with good vision, few retinal hemorrhages and cotton-wool spots, no relative afferent pupillary defect, and good perfusion to the retina. May resolve fully with good visual outcome or may progress to the ischemic type.
Ischemic CRVO is severe form of the disease.May present initially as the ischemic type, or it may progress from nonischemic. Usually, presents with severe visual loss, extensive retinal hemorrhages and cotton-wool spots, presence of relative afferent pupillary defect, poor perfusion to retina, and presence of severe electroretinographic changes. In addition, patients may end up with neovascular glaucoma and a painful blind eye.

Non-Ischemic CRVO Ischemic CRVO
NON ISCHEMIC CRVO –Diffuse flame shaped retinal hemorrage Tortuosity and engorgenent of retinal veins
ISCHEMIC CRVO: diffuse capillary non perfusion—rubiosis iridis—neovascular glaucoma(NVG)

Causes Central retinal vein obstruction has been associated with various systemic
pathological conditions, although the exact cause and effect relationship has not been proven.
Some of the conditions in which CRVO has been associated include the following:
Systemic vascular disease - Hypertension, diabetes mellitus, cardiovascular disease
Blood dyscrasias - Polycythemia vera, lymphoma, leukemia Clotting disorders - Activated protein C resistance, lupus anticoagulant,
anticardiolipin antibodies, protein C, protein S, antithrombin III Paraproteinemia and dysproteinemias - Multiple myeloma,
cryoglobulinemia Vasculitis - Syphilis, sarcoidosis Autoimmune disease - Systemic lupus erythematosus Oral contraceptive use in women Obstructive sleep apnea - This affects more patients with retinal vein
obstruction than other disorders; treatment of the sleep apnea may help prevent central vein obstruction.[11]
Other rare associations - Closed-head trauma, optic disc drusen, arteriovenous malformations of retina

Treatment exact pathogenesis of the CRVO is not known Identifying and treating any systemic medical problems
to reduce further complications is important Advocated treatments are as follows: Aspirin Anti-inflammatory agents Isovolemic hemodilution Plasmapheresis Systemic anticoagulation with warfarin, heparin, and
alteplase Fibrinolytic agents Systemic corticosteroids intravitreal injection of anti-angiogenic drugs like ranibizumab , aflibercept , triamcinolone , bevacizumab Dexamethasone intra vitreal implants

Hypertensive retinopathy Fundus changes occurring in
patient suffering from systemic hypertensive due to vaso-construction and arteriosclerosis etc.
High blood pressure can cause damage to blood vessels in the eyes.
Cause headaches and visual disturbance.
Treatment • A major aim of treatment is to prevent target organ damage by
high blood pressure • Control of high blood pressure (hypertension) is the only
treatment for hypertensive retinopathy• Regular eye examinations are important.

Vaso-constrictive and early sclerotic changes in hypertensive retinopathy, including diffuse arteriolar narrowing, sinusoidal tortuosity, copper wire appearance, arteriovenous crossing changes, tapering of veins and increased arteriolar branching angles.
The changes seen in the fundus secondary to hypertension are representative of changes taking place in the arterioles throughout the body.Grading of hypertensive retinopathy : grade I, generalized arteriolar narrowing; grade II, generalized narrowing and focal constrictions; grade III, more narrowing, focal constriction, hemorrhage, and exudation; grade IV, marked narrowing and focal constrictions with hemorrhages, exudates, and papilloedema of the disc.



Diabetic retinopathy




Incidence of d. retinopathy related to the duration of diabetes 15% after 5 year50% after 10 year60% after 15 year70% after 20 year 90% after 30 year

Retinopathy effects the circulatory system of the retina
Causing damage of blood vessels of eye
Leakage of blood (hemorrhage)
fluid leakage (oedema)
Commonly cause blindness or loss of vision
Cause darkening in image

1.Background retinopathy
small red dots will appear on retina due to tiny
swellings in the blood vessel walls
3.Proliferative retinopathyIt is third stage of retinopathyextensive neovascularization, usually causing a sudden loss of vision
2.Pre-proliferative retinopathyretina swells and leaks blood reading small print may become particularly difficult.


TREATMENTBackground retinopathy Requires no treatment, but should have Regular
eye Examinations by Ophthalmologist
Pre-proliferative retinopathy also does not require treatment, Laser treatment can be an option if leakage
begins Laser treatment cannot restore any lost vision,
but can be used to prevent further growth
Proliferative retinopathy Laser treatment is used to 'burn' the abnormal
blood vessels to prevent further growth of new blood vessel


Diabetic maculopathy
Involvement of fovea occur at any stage of retinopathy due to
Macular edema Macular hemorrhages Macular detachment

Other retinal disorders

Macular degeneration Also called age related macular
degenerationIt is a non heredity most common cause
permanent irreversible central loss of vision


Age related macular degeneration-AMRD


Type Nonexudative(atrophic or dry) 90% most
common type of MD
Exudative(wet):10% cause of ARMD presence of fluid and hemorrhages it is more dangerous
TreatmentAntivascular endothelial growth factor-
AVEGF(avastin)Photodynamic therapy(PDT)

Retinal detachment Separation of sensory retina from
pigmented epithelium is called retinal detachment
Types Primary or simple: separation of
retina in the form of hole or tear. This hole allows the vitreous to raise retina from its normal position
Secondary: due to pathology and the accumulation of fluid to push retina from its normal position
Treatment-Laser treatment Retinopexy use to reattach the detached retina.

Rhegmatogenous retinal detachment formation
retinal degeneration Basis liquefied vitreous retinal hole→RD aging
Predisposing high myopia ocular trauma

Pigmented retinal dystrophy It is a heredity disease caused degeneration of
rods and cones in childhood caused night blindness as well as complete blindness

Retinoblastoma Rapidly developing carcinoma which develops
in the cells of the retinaIt is common congenital tumor of retina
occurring in childhood(2-4) year. Approximately 1in 20,000 birth
Children of the same family usually effected due to Rb oncogene involved.
Many children have unilateral retinoblastoma which has an excellent prognosis. The prognosis for bilateral involvement depends on the size and location of the tumor.



Treatment
Laser therapy: A laser is used to vaporize the tumor
Thermotherapy: This process uses heat to destroy the cancer cells may be combined with chemotherapy or radiotherapy
Chemotherapy: Chemotherapy is the use of anti-cancer (cytotoxic) drugs to destroy cancer cells

Night blindness
Due to deficiency of vitamin- AV-A is present in cytoplasm of rods and
pigmented layer of retinaWithout the V-A the amount of retinal and
rhodopsin may severally depressed this condition is known as night blindness
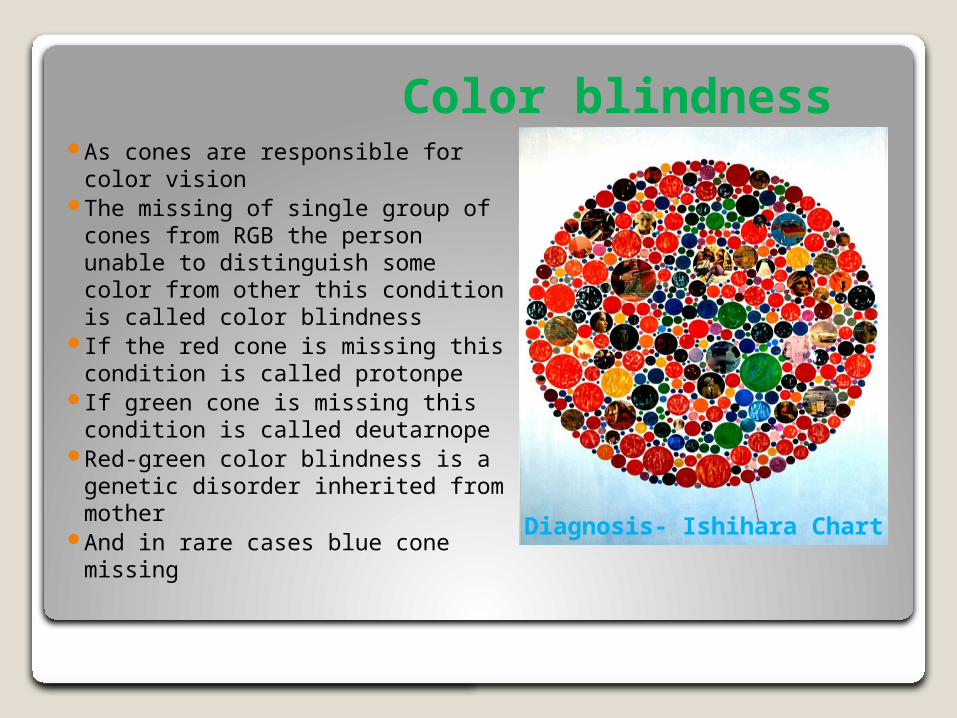
Color blindness As cones are responsible for color
vision The missing of single group of
cones from RGB the person unable to distinguish some color from other this condition is called color blindness
If the red cone is missing this condition is called protonpe
If green cone is missing this condition is called deutarnope
Red-green color blindness is a genetic disorder inherited from mother
And in rare cases blue cone missing
Diagnosis- Ishihara Chart

Resources http://
www.mayoclinic.org/diseases-conditions/retinal-diseases/basics/definition/con-20036725
http://www.sciencedirect.com/science/journal/13509462
http://www.snec.com.sg/eye-conditions-and-treatments/common-eye-conditions-and-procedures/Pages/retinal-vascular-disorders.aspx
http://www.academy.org.uk/lectures/barnard5.htm
