research supported by va rehab. r&d riverside … 18 wambaugh handout.pdf · riverside...
TRANSCRIPT

1
Research supported by VA Rehab. R&D
Riverside Community Hospital
October 18, 2014
DISCLOSURE STATEMENT: Dr. Wambaugh is receiving financial
compensation for this presentation
◦ Review characteristics of AOS
◦ Discuss differential diagnosis
◦ Describe assessment for treatment planning
◦ Summarize the existing AOS Practice Guidelines
◦ Describe on-going guidelines work – update in progress
◦ Highlight important new developments in AOS treatment
◦ Discuss clinical application of existing treatments

2
Disruption of motor planning/programming ◦ sound selection and ordering assumed to be intact
◦ neuromuscular system for realizing articulatory command assumed to be intact
Problem with the translation of correctly selected sounds to previously learned articulatory-kinematic parameters ◦ what? when? where? how long? how fast? with how
much force?
Slowed rate of speech production ◦ Increased interval time between words and syllables
◦ Increased time to produce individual sound segments and to transition between sounds
Sound Errors ◦ distortions (predominant type), perceived
substitutions, omissions, additions (intrusive schwa)
◦ relatively consistent across repeated productions - location and type*
Prosodic Abnormalities ◦ Related to slow rate

3
Articulatory groping
Increasing errors with increasing word length or complexity
Perseverative errors
Speech initiation difficulties
Awareness of errors (e.g., self-corrections)
Automatic speech better than propositional speech
Islands of error free speech
Have been used in the past
May co-occur
More likely to be attributable to other disorders
◦ anticipatory errors (pillow lillow)
◦ transposition errors (spaghetti psghetti)

4
Mild-moderate AOS; samples from Duffy protocol (2005)
Moderate PURE AOS ◦ http://heart.utah.gov/hearthighway/time.html
Butterfly Octopus Volcano Animal

5
F, mild AOS, minimal aphasia ◦ Mono-multisyllabic words
M, mild-mod. AOS, mod.-severe aphasia ◦ Monosyllabic
◦ Mono-, multisyllabic
M, moderate AOS, mod. Aphasia ◦ ABA words of increasing length
◦ Naming
◦ 3X repetition
◦ Picture description
Prosody/Rate ◦ Slow rate in “on-target” and “off-target” phrases
and sentences
◦ Inability to increase rate while maintaining sound integrity
◦ Prolonged movement transitions
◦ Prolonged interword intervals
◦ Abnormally long vowels
◦ Increased movement durations

6
Sound Errors: ◦ sound distortions
◦ distorted substitutions, perseverations, anticipatory, exchange, and cluster errors (primarily prolonged phonemes and devoiced sounds)
◦ location of errors is relatively consistent from trial to trial
◦ types of errors are consistent (NOT VARIABLE) from trial to trial
◦ schwa insertions common
M, mod-severe PP, moderate Conduction aphasia ◦ Monosyllabic words
◦ Conversation
M, moderate PP, moderate Conduction aphasia ◦ Words
◦ conversation

7
Dronkers (Nature, 1996) – insula (superior, precentral gyrus of insula), double-dissociation ◦ 25 AOS, 19 non AOS
◦ Ogar et al., 2006 – additional S’s
◦ AOS subject selection problematic: catastrophe: “/patastrophe/, /t/, /katasrifrobee/, /k/, /kata/, /sh/….I don’t know”
◦ Hillis (2004) suggests insula is particularly vulnerable to MCA occlusion
Hillis (2004) – different approach: probability of insular lesion causing AOS - no assoc. between AOS & insula ◦ Pts. studied patients at stroke onset with Diffusion
Weighted MRI (DWI; to identify areas of infarct) and Perfusion Weighted MRI (PWI; to identify areas of reduced blood flow or hypoperfusion)
◦ 80 left MCA stroke – 40 with and 40 without insular damage
◦ ½ pts. with AOS had insular damage ◦ 2/3 pts. without AOS had insular damage ◦ 84% of pts with AOS had hypoperfusion to Broca’s area; 9%
w/o AOS had hypoperfusion to Broca’s area left, inf. frontal gyrus assoc. with AOS

8
McNeil et al. (1990) – 2/4 S’s with relatively pure AOS had insular damage
Robin and colleagues (2008) – post hoc ◦ 7 pts. with relatively pure AOS ◦ Structural MRI ◦ Only region of overlap was BA 6 in 6/7 pts. ◦ 1 subcortical only – basal ganglia & insula ◦ All had lesions beyond BA 6 (especially BA 44 &
BA45)
Left posterior inferior frontal gyrus (BA 44 &45)
Supplementary motor areas (BA 6)
Insula
Parietal lobe

9
ABA-2 (Dabul, 2000) ◦ DDK Rate
◦ Increasing Word Length
◦ Limb Apraxia and Oral Apraxia
◦ Latency Time and Utterance Time for Polysyllabic Words
◦ Repeated Trials
◦ Inventory of Articulation Characteristics of Apraxia
10
Exhibits phonemic anticipatory errors (e.g., gleen glass for green glass) ◦ Not an AOS symptom (level of phonology)
Exhibits phonemic perseverative errors (e.g., pep for pet) ◦ Not an AOS symptom (level of phonology)
Exhibits phonemic transposition errors (e.g., Arifca for Africa) ◦ Not an AOS symptom (level of phonology)
Exhibits phonemic voicing errors (ben for pen) ◦ Could be AOS or PP (phonologic or motoric)
Exibits phonemic vowel errors (moan for man) ◦ Could be AOS or PP (phonologic or motoric)
Exhibits visible/audible searching ◦ Could be AOS or PP

11
Exhibits numerous and varied off-target attempts at the word o Numerous attempts = consistent with AOS o Numerous, varied, off-target = PP
Errors are highly inconsistent o NOT AN AOS SYMPTOM
Errors increase as phonemic sequence increases o Consistent with AOS & PP
Exhibits fewer errors in automatic speech than in volitional speech ◦ Consistent with AOS & PP
Exhibits marked difficulty initiating speech ◦ Consistent with AOS & PP
Intrudes a schwa sound between syllables or in consonant clusters ◦ Consistent with AOS
12
Exhibits abnormal prosodic features ◦ Consistent with AOS
Exhibits awareness of errors and inability to correct them ◦ Consistent with AOS & PP
Exhibits a receptive-expressive gap ◦ Consistent with AOS & PP
Duffy, J.R. (2005). Motor speech disorders. Substrates, differential diagnosis, and management (2nd ed.). St. Louis, MO: Elsevier Mosby.
AOS screening tool

13
Sound repetition
Monosyllabic words – inventory of consonants in (i) and (f) positions: fife, pipe
Polysyllabic words
Increasing length
Repeated productions
Sentence repetition
AMRs & SMRs
Counting
Days of the week
Singing familiar tunes
Conversational & narrative speech
Reading aloud
Slowed rate of speech production ◦ Increased interval time between word and syllables
◦ Increased time to produce individual sound segments and to transition between sounds
Sound Errors ◦ distortions (predominant type), perceived
substitutions, omissions, additions (intrusive schwa)
◦ relatively consistent across repeated productions - location and type
Prosodic Abnormalities

14
Articulatory groping
Increasing errors with increasing word length or complexity
Perseverative errors
Speech initiation difficulties
Awareness of errors (e.g., self-corrections)
Automatic speech better than propositional speech
Islands of error free speech
Sound Errors
◦ Percentage of errors
◦ Level of breakdown
Intelligibility
Rate/ durational measures
◦ Segments
◦ Syllabic/word durations
◦ ISIs
Measures of prosody
Ratings of naturalness
Functional measures
Non discriminatory behaviors
Etc.

15
AOS
Sound error analysis Intelligibility assessment Durational analysis Quantification of accompanying behaviors OTHER
Aphasia Oral, nonverbal apraxia Dysarthria Cognition
Sounds in isolation * Single monosyllabic words/syllables (all word
positions) Multisyllabic words Words of increasing length Phrases Sentences Discourse

16
Repetition
Oral reading
Sentence completion
Self generation
Patterns
Generative analysis
% of errors
Level of breakdown - context & elicitation
17
May use assessments designed for dysarthria
Should not use primary clinician as “listener”
◦ Use another clinician
◦ Use a student
◦ Use a significant other Be consistent in use of listener
False starts Silent or audible groping Starters Fillers Overall communication efficiency
◦ (e.g., CIU’s/time) Perceived effort # of verbal initiations

18
Content measure in discourse
Narrative & procedural discourse elicited systematically
Measures ◦ Total # words
◦ Total # CIUs
◦ Efficiency measure
Normative data
4 single pictures (cookie thief, picnic scene, cat up tree, dog & birthday cake)
2 sequences of pictures
2 response to requests for personal information Do on Sundays?
Where live? Describe.
2 procedural descriptions Doing dishes
Write & send a letter

19
TREE: Ah how say that…cat cat da ah dog ahm
man bird girl ah bike bike ahm how say that two men ahm how say that hm ah gi gi truck truck trunk
Words: 22
CIUs: 9

20
Nicholas, L.E., & Brookshire, R.H. (1993). A system for quantifying the informativeness and efficiency of the connected speech of adults with aphasia. JSHR, 36, 338-350.
Most applicable if working on rate control or prosody
Syllables or words per second
Efficiency measure (e.g., CIUs per minute)
Segmental measures – acoustic analyses

21
Sound error analysis
Intelligibility assessment
Durational analysis
Accompanying behaviors quantification
Paucity of functional outcome measures
◦Majority of measures reflect WHO body function
◦WHO activity and participation levels have received limited attention
◦Wambaugh & Mauszycki (2010)

22
Functional Assessment of Communication Skills for Adults (ASHA FACS; Fratalli et al., 1995)
Communication Effectiveness Index (CETI; Lomas et al., 1989) & CETI-M (Ball et al., 2004)
Quality of Communication Life Scale (ASHA QCL; Paul et al., 2004)
Dysarthria Impact Profile (DIP; Walsh, Peach, & Miller, 2009).
Communicative Participation Item Bank (Baylor et al., 2010)
Walshe, M., Peach, R.K., & Miller, N. (2009). Dysarthria impact profile: development of a scale to measure psychosocial effects. Int. Journal of Language and Communication Disorders, 44(50), 893-715.

23
Effect of dysarthria (AOS – speech difficulty) on me as a person
Accepting my dysarthria (AOS)
How I feel others react to my speech
How dysarthria (AOS) affects my communication with others
10-14 questions per section
Negatively and positively worded
I am as confident now as I was before I had a speech problem.
I am not happy with my speech as it is now
I don’t care what people think of my speech
The difficulties I have with my speech restrict my social life

24
Sponsored by Academy of Neurologic Communication Disorders and Sciences (also supported by ASHA’s SIG 2)
J. Wambaugh, J. Duffy, M. McNeil, D. Robin, M. Rogers
www.ancds.org
Wambaugh, J.L., Duffy, J.R., McNeil, M.R., Robin, D.A., & Rogers, M.(2006). Treatment guidelines for acquired apraxia of speech: A synthesis and evaluation of the evidence. Journal of Medical Speech Language Pathology, 14(2), xv-xxxiii. Wambaugh, J.L., Duffy, J.R., McNeil, M.R., Robin, D.A., & Rogers, M.(2006). Treatment guidelines for acquired apraxia of speech: Treatment descriptions and recommendations. Journal of Medical Speech Language Pathology, 14(2), xxxv-ixvii. Wambaugh, J.L. (2006). Treatment guidelines for apraxia of speech: Lessons for future research. Journal of Medical Speech-Language Pathology, 14(4), 317-321.

25
English language reports published through 2003
59 published reports ◦ there was measurement of effects of treatment on the
impact of acquired apraxia of speech (AOS) at any or all levels of functioning
◦ authors must have indicated their intention 1) to treat AOS; 2) to measure the impact of a treatment on AOS; or 3) to impact the sequelae of AOS
◦ report must have provided some form of data pertinent to the effects of treatment with at least one person with AOS
“n” = 146
Etiology: 93% CVA, 5% TBI, 2% other
Gender: 78% male, 22% female
Age: mean = 54 yrs, min-max = 21-82
TPO: mean = 31 months; median = 14
months; min-max: 2 weeks – 192 months
26
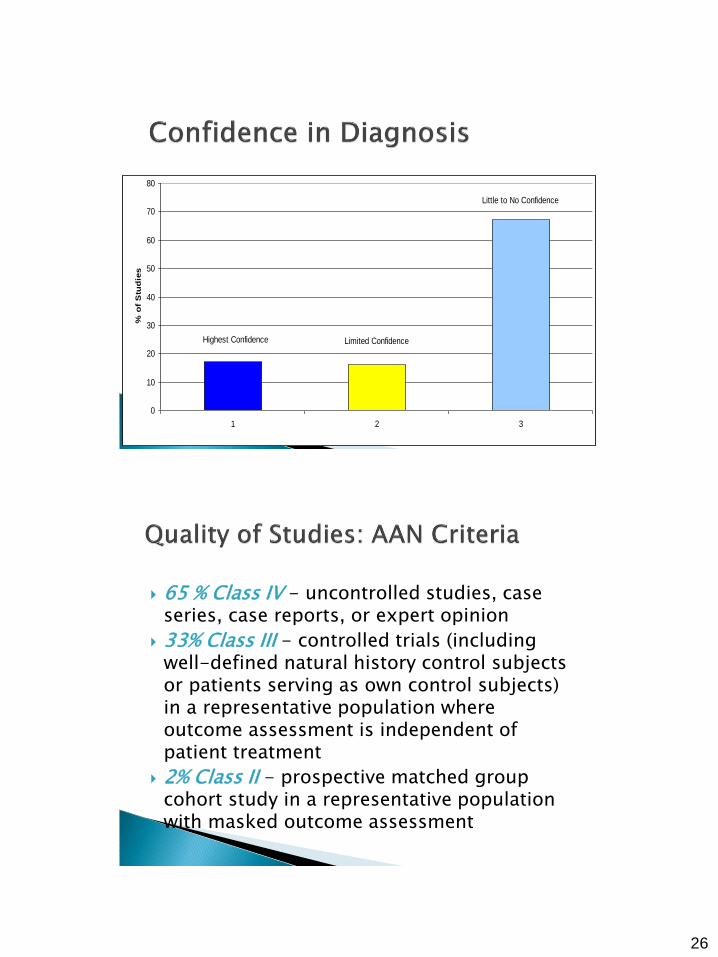
Highest Confidence Limited Confidence
Little to No Confidence
0
10
20
30
40
50
60
70
80
1 2 3
% o
f S
tud
ies
65 % Class IV - uncontrolled studies, case series, case reports, or expert opinion
33% Class III - controlled trials (including well-defined natural history control subjects or patients serving as own control subjects) in a representative population where outcome assessment is independent of patient treatment
2% Class II - prospective matched group cohort study in a representative population with masked outcome assessment
27
Relatively small “n” overall and in individual studies
Few attempts to replicate findings
Only a few systematic lines of research
Synthesis of findings of studies with generally similar foci (e.g., AAC, rate/rhythm control)
Consequently, treatment guidelines are more general than specific
General approaches summarized ◦ rationales
◦ treatment techniques
◦ treatment targets
◦ outcomes
◦ participants
◦ candidacy issues
◦ quality of the evidence

28
Articulatory-Kinematic – use of techniques to improve articulatory accuracy
Rate/Rhythm control – use of techniques to reduce rate, impose timing or rhythm
Intersystemic reorganization – use of relatively intact systems to facilitate speech production
AAC – use of alternative or augmentative means of communication
Other
Therapies that “concentrate on the disordered articulation…(and) emphasize the regaining of adequate points of articulation and the sequencing of articulatory gestures” (Rosenbek et al., p. 463).
29
Repeated practice
Modeling
Integral stimulation
Articulatory placement cues
Shaping
Minimal contrast practice – practice of contrasts
Visual biofeedback
Verbal feedback
PROMPT
Nonspeech movement practice (e.g., tongue tip movements)
Txs. that imposed control over rhythm/timing/rate
Rationale for use: ◦ Increased time to reach articulatory postures ◦ Improved functioning of central pattern generators ◦ Decreased degrees of freedom in speech production ◦ Increased allocation of resources ◦ Motoric “spillover” ◦ Increased afference

30
Metronomic pacing
Finger tapping – finger counting
Instructional feedback
Computerized pacing – oral reading
Pacing board
Indirect control (MIT, PROMPT)
Use of a relatively intact system to facilitate functioning of another system
Iconic Gestures – Amerind most frequently used to facilitate and/or supplement speech
Rhythmic Gestures – tapping, fingercounting
Vibrotactile Stimulation – externally applied rhythmic stimulation
Singing – choral singing, sentence completion, phrase production

31
Gestures – Amerind most frequently used
Communication boards/notebooks
Spoken computer output
Multiple communication systems – writing,
drawing, notebooks, gestures
Electrolarynx
Alternative strategies for unproductive
behaviors
Conversational practice
Training significant others (e.g., interviewing
skills)
Head movement training
Biofeedback for tension reduction
Silent rehearsal

32
Case/
Series
S-S
Design
Group
Non-
exp.
Group
Exp.
Internal
Validity
Artic-Kinem. 14 14 1 1 13
Rate/Rhythm 4 3 0 0 3
Intersyst. 4 4 0 0 3
AAC 7 1 0 0 1
Other 4 1 0 0 0
articulatory kinematic approaches - “probably
effective”
rate/rhythm control approaches - “possibly
effective”
intersystemic approaches - “possibly effective”
AAC approaches - could not be rated in terms
of likelihood of benefit

33
Designations which “communicates the guideline developers’ (and the sponsoring organizations’) assessment of the importance of adherence to a particular recommendation” (Marcuse et al., 2004)
“guidelines are never intended to overrule professional judgment; rather they may be viewed as a relative constraint on individual clinician discretion in a particular clinical circumstance”
Strong recommendation – none
Recommendation - articulatory kinematic approaches be utilized with individuals with moderate to severe AOS who demonstrate disrupted communication due to disturbances in the spatial and temporal aspects of speech production
Options – rate/rhythm, intersystemic, AAC
In 2006 there was no evidence concerning superiority of one technique over another

34
Treatment for AOS can be expected to result in improvements in speech production, particularly when treatment has an articulatory-kinematic focus
More than half of the evidence base is derived from A-K treatments
Across all studies, all participants had AOS plus aphasia
Evidence base is modest in terms of “n” and experimental control, but is improving
New Guidelines Committee ◦ Kirrie Ballard – chair
◦ Joe Duffy
◦ Mick McNeil
◦ Julie Wambaugh
◦ Edwin Maas
◦ Shannon Mauszycki
In process – initial report provided at ASHA 2013 convention, published update expected soon
35
~32 studies identified beyond the 2006 ANCDS guidelines report
◦ 23 - articulatory kinematic tx.
◦ 2 - rate/rhythm control tx.
◦ 1 - implicit phoneme manipulation tx.
◦ 1 - visual speech perception
◦ 2- script training (1 w/ A-K; 1 w/ sp. percep.)
◦ 2 – multimodality stimulation
◦ 1 – tDCS (+ modeling/repetition/slowed rate)
Feedback ◦ Frequency
◦ Timing
◦ Biofeedback
Repeated Practice
Stimuli
Instructional Method
Intensity of Treatment
Plus tDCS
Feedback

36
Frequency of Feedback : “n” = 4 ◦ High Frequency Feedback (HFF) = 100%
◦ Low Frequency Feedback (LFF) = 60%
◦ Performance enhanced with LFF for 2/4
Timing of Feedback: “n” = 2 ◦ Immediate Feedback = no delay
◦ Delayed Feedback =5 second delay
◦ Performance enhanced with DF for 1/2

37
Sensors placed on articulators of interest (lips, teeth, tongue)
Display provided to participant - target zone for the desired sound/word
Series of treatment investigations by Katz and McNeil et al. ◦ Improvements in articulation reported for
participants with chronic AOS
Cost may be prohibitive
Targeted control of voicing (“n” = 2)
Used spectrographic feedback + phonetic placement cues
Participants consistently produced voiced fricatives and stops as voiceless prior to treatment
Improvements seen for treated and untreated sounds (of same manner)

38

39
No new studies published recently
Mauszycki et al. – in progress with 3 AOS speakers
Biofeedback of tongue position relative to palate
Cost may not be prohibitive for clinical practice
May be desirable for persons with AOS who have issues with proprioceptive feedback

40
Feedback ◦ Frequency
◦ Timing
◦ Biofeedback
Repeated Practice
Stimuli
Instructional Method
Intensity of Treatment
Plus tDCS
Repeated Practice
10 participants
Chronic AOS + non fluent aphasia
Repeated practice tx. only until plateau
Metronomic pacing + hand-tapping added
after plateau

41
8/10 improved from repeated practice alone
Addition of metronome resulted in slight
improvement for a few participants
2/10 did not improve with any treatment
At least a few sound errors remained after tx.

42

43
Feedback ◦ Frequency
◦ Timing
◦ Biofeedback
Repeated Practice
Stimuli
Instructional Method
Intensity of Treatment
Plus tDCS
Stimuli

44
Scheider & Frens (2005) trained complex and less complex non words – “n” = 3 (e.g., Level 4: natigbo, Level 1: bobobobo) ◦ Complex generalized to less complex (1 of 4 tx.
opportunities)
◦ Less complex generalized to more complex (1 of 4 opportunities)
Equivocal findings
Differs from findings from Aichert & Ziegler (2008)
Aichert & Ziegler (2008) – “n” = 4 ◦ Production of words with complex syllables (e.g.,
CCVCC) improved following practice of less complex
◦ Less complex were derived from the more complex
◦ Phonetically similar syllables may share motor program units at subsyllabic levels
Schoor, Aichert, & Ziegler (2012) found generalization occurred only when practiced and unpracticed syllables overlapped in the POSITION of shared syllabic constituents (i.e., same initial consonant and vowel)

45
Feedback ◦ Frequency
◦ Timing
◦ Biofeedback
Repeated Practice
Stimuli
Instructional Method
Intensity of Treatment
Plus tDCS
Instructional Method
Treatment involved provision of information concerning manner & place of articulation ◦ Verbal
◦ Gestural (cued articulation)
◦ Combined verbal + gestural
No clinically relevant difference among delivery modes
Suggested that type of information provided (artic. Instruction contrasting target & error) more important than delivery method

46
Feedback ◦ Frequency
◦ Timing
◦ Biofeedback
Repeated Practice
Stimuli
Instructional Method
Intensity of Treatment
Plus tDCS
Intensity of Treatment
Principles of experience-dependent neural plasticity (Kleim & Jones, 2008): “intensity matters” - increased intensity is likely to be associated with improved outcomes
But…distributed practice vs. massed practice or treatment trials: distributed practice over a longer period of time may produce superior results (Janiszewki et al., 2003; Schmidt & Lee, 2005)
47
Blocked Practice: More rapid acquisition effects during treatment
Randomized Practice: Better maintenance effects
Schmidt & Lee, 2005
Multiple Baseline Design ◦ Across Participants
◦ Across Behaviors
4 replications of treatment
Intensive – Blocked
Intensive – Randomized
Traditional – Blocked
Traditional – Randomized
Wambaugh et al. (2013). AJSLP

48
Intense
4 hours per days / 4 days per week
32 hours of tx. over 2 weeks
Traditional
1 hour per day / 3 days per week
32 hours of tx. over 11 weeks
Blocked: all items for a given sound target practiced in a block, then all items for the other target practiced in a block
Randomized: items for each sound target were practiced in alternating manner

49
Positive changes in articulation occurred for all treatment variations for all participants
For the INTENSE application, performance was similar for Blocked and Random for all Participants
For the TRADITIONAL applications, P2 and P3 had poorer performance upon conclusion of the Random treatment, but differences were not apparent at follow-up
Feedback ◦ Frequency
◦ Timing
◦ Biofeedback
Repeated Practice
Stimuli
Instructional Method
Intensity of Treatment
Plus tDCS
Plus tDCS

50
Anodic tDCS – used to increase cortical
excitability.
Compared to a sham treatment
Both paired with A-K therapy with “n” = 3
Improvements found with both conditions
BUT…greater increases with tDCS condition for
all participants – maintained at 2 months post
tx.
3 new investigations (Brendel & Ziegler, 2008; Mauszycki & Wambaugh, 2008, Wambaugh et al., 2012)
Reinforces previous findings that practice in the context of rate/rhythm control results in improved articulation – without direct articulation instruction

51
pacing tones reflect the natural, relative
distances of syllables (taken from waveforms)
compared to non-pacing, control tx. – variety
of artic.-kinem. techniques
10 speakers with AOS
both txs. reduced # errors
MPT reduced dysfluencies
Mauszycki & Wambaugh (2008) ◦ Participant with mild AOS
◦ 4-5 syllable words & sentences
◦ Reduced rate, then increased rate
◦ Positive findings
Wambaugh et al. (2012) ◦ Modest improvements in sound production accuracy
with addition of R/R tx. for some, but not all participants

52
Use of AAC device as a means for improving speech production; as opposed to replacing and/or supplementing speech
Lasker et al. (2008; 2010) ◦ Speech generating device
◦ Motor Learning Guided Treatment
◦ Face-to-face plus home practice with AAC device
◦ Also…employed Skype (2010)
Interest in capitalizing on theorized actions of mirror neurons (automatic process that
links/matches observed actions with performance – shared motor representations for observation and execution – controversial)
◦ Fridricksson et al. (2012) – “speech entrainment” (integral stimulation)
Computerized therapy ◦ Whiteside et al. (2012)

53
Principles of Motor Learning ◦ Trend toward increased interest / use ◦ Maas et al., (2008) AJSLP
Combining AOS and aphasia therapy ◦ Youmans et al. (2011) – SCRIPT + artic. Instruction ◦ Wambaugh et al. (in prep) – Combined Aphasia and
Apraxia of Speech Treatment (CAAST)
Modified Response Elaboration Training (M-RET) plus Sound Production Treatment
Designed to improve… ◦ Production of content (Correct Information Units)
◦ Length of utterance
◦ Sound production

54

55
CIUs (Correct Information Units; Nicholas & Brookshire, 1993) ◦ With experimental stimuli (trained & untrained
pictures) ◦ With N & B stimuli
Percent Consonants Correct – sentence repetition ◦ With printed sentences ◦ Without printed sentences
Word Intelligibility
Participant 1
0 5 10 15 20 25 30
SE
T 1
: #
CIU
s
0
20
40
60
80
100
120
140
160
180Baselilne Treatment
0 5 10 15 20 25 30
SE
T 3
: # C
IUs
0
20
40
60
80
100
120
140
160
180
Probe Sessions
0 5 10 15 20 25 30
SE
T 2
: #
CIU
s
0
20
40
60
80
100
120
140
160
180
Follow Up2 & 6 weeks
adjusted trend line
adjusted mean line
d=8.89
d=6.9
d=4.12

56
Participant 2
0 5 10 15 20 25 30 35
SE
T 3
: #
CIU
s
0
10
20
30
40
50
60Baselilne Treatment
0 5 10 15 20 25 30 35
SE
T 1
: #
CIU
s
0
10
20
30
40
50
60
Probe Sessions
0 5 10 15 20 25 30 35
SE
T 2
: #
CIU
s
0
10
20
30
40
50
60
Maintenance Follow Up2 & 6 weeks
adjusted trend line
adjusted mean line
d=5.41
d=6.11
d=3.8
Participant 3
0 5 10 15 20 25 30 35 40
SE
T 1
: #
CIU
s
0
20
40
60
80
100
120
140
160
180
200
220
240Baselilne Treatment
0 5 10 15 20 25 30 35 40
SE
T 3
: # C
IUs
0
20
40
60
80
100
120
140
160
180
200
220
240
Probe Sessions
0 5 10 15 20 25 30 35 40
SE
T 2
: #
CIU
s
0
20
40
60
80
100
120
140
160
180
200
220
240
Maintenance Follow Up 2 & 6 weeks
adjusted trend line
adjusted mean line
d=15.52
21.63
d=5.72

57
Participant 4
0 5 10 15 20 25 30 35
SE
T 2
: #
CIU
s0
10
20
30
40
50
60Baselilne Treatment
0 5 10 15 20 25 30 35
SE
T 3
: #
CIU
s
0
10
20
30
40
50
60
Probe Sessions
0 5 10 15 20 25 30 35
SE
T 1
: #
CIU
s
0
10
20
30
40
50
60
Maintenance Follow Up 2 & 6 weeks
adjusted trend line
adjusted mean line
d=13.64
d=16.01
d=5.79
All participants CIU production with experimental stimuli ◦ Trained pictures
◦ Untrained pictures
2/4 participants CIU productions in Nicholas & Brookshire task
2/4 participants PCC in sentence repetition – larger increases with written stimuli
1/4 participants intelligibility

58
AOS Guidelines update indicates a trend toward use of PML ◦ Treatments based specifically on PML
e.g., Motor Learning Guided (MLG) Lasker et al. (2008)
◦ Many treatments have incorporated some PML – including SPT
Few direct tests of PML applied to AoS tx.
Systematic review by Bislick et al. (2012) ◦ Limited evidence with some promising findings
◦ More research needed
Blocked practice – all trials for a given behavior are grouped together in a practice session
Random practice – across the practice session different behaviors are practiced in non predictable order
Robust effects in motor learning literature ◦ More rapid improvements during practice with
Blocked practice
◦ Better retention and generalization with Random practice

59
Knock, Ballard, Robin, & Schmidt (2000) ◦ 1 of 2 participants had advantage for random
practice (probe performance)
Wambaugh, Nessler, Cameron, & Mauszycki (2013) ◦ Pilot investigation with 4 participants
◦ Treatment intensity & practice schedule
◦ No differences observed for random and blocked practice schedules
Maas & Farinella (2012)
Dynamic Temporal and Tactile Cueing treatment (Strand et al., 2006)
Findings ◦ 2 participants - advantage for Blocked
◦ 1 participant – advantage for Random
◦ 1 participant – no response with either

60
To examine the effects of Sound ProductionTreatment (SPT) administered with BLOCKED stimulus presentation and with RANDOM stimulus presentation on accuracy of production of target sounds
NOT designed as a pure test of blocked vs. random practice
◦ Maintain the basic SPT protocol ◦ Focus on optimizing clinical application
61
n: 6
Gender: 5 men, 1 woman
Etiology: stroke
◦ L hemisphere, ischemic, MCA
MPO: 28 to 87 months
Age: 46 - 71 yrs
Yrs. Ed: 11-20
Handedness: right
Hemiparesis: RUE & RLE
Consistently slow rate
Sound errors ◦ often perceived as distortions
◦ relatively predictable – location and type of error
◦ some sounds consistently in error
Disrupted prosody
after McNeil et al., 2009
62
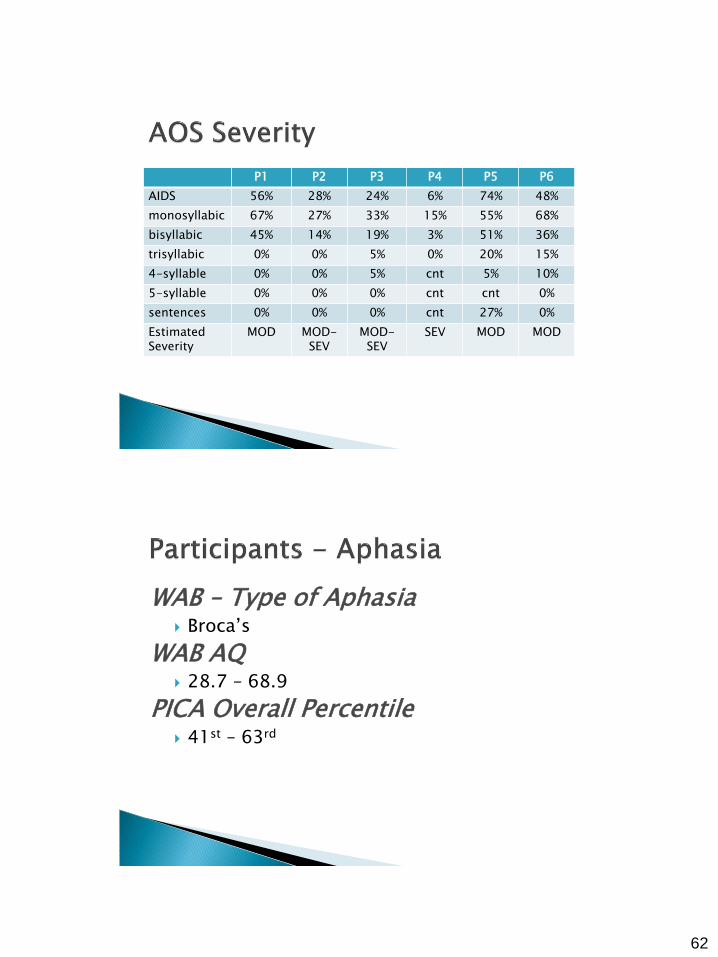
P1 P2 P3 P4 P5 P6
AIDS 56% 28% 24% 6% 74% 48%
monosyllabic 67% 27% 33% 15% 55% 68%
bisyllabic 45% 14% 19% 3% 51% 36%
trisyllabic 0% 0% 5% 0% 20% 15%
4-syllable 0% 0% 5% cnt 5% 10%
5-syllable 0% 0% 0% cnt cnt 0%
sentences 0% 0% 0% cnt 27% 0%
Estimated Severity
MOD MOD-SEV
MOD-SEV
SEV MOD MOD
WAB – Type of Aphasia Broca’s
WAB AQ 28.7 – 68.9
PICA Overall Percentile 41st – 63rd

63
Single subject multiple baseline design across behaviors & subjects ◦ Minimum of 5 baseline probes
Treatment applied sequentially to 2 sets of words
2 week no-treatment interval after 1st treatment phase ◦ Maintenance probe with 1st treated set at 2 weeks
◦ Extended pre treatment probing with 2nd set
Follow-up probes at 2, 6, and 10 weeks following end of all treatment
2 sets of 30 items each ◦ 20 treatment & 10 generalization items
◦ 15 exemplars for each of 2 sound targets
10 tx & 5 generalization items for each target
Individualized for each participant ◦ Monosyllabic words – 3 syllable words w/ carrier
phrase

64
P2: Set 1 – T1 stab, start
T2 rose, news
Set 2 – T1 glass,globe
T2 knife, leaf
P6: Set 1 – T1 threading, throughout
T2 glossary glamorous
Set 2 – T1 snapdragon, snowmobile
T2 quietly, quotation
Step 1: Modeling-repetition ◦ minimal contrast practice on error (monosyllabic)
Step 2: Orthographic cue + modeling/rep
Step 3: Integral stimulation
Step 4: Articulatory production instruction
Next Item
Blocked & Random Phases counterbalanced

65
20 sessions per phase
3X per week
Treatment time = 50-60 minutes
# trials determined by session length ◦ Fewer trials in initial sessions
Probes conducted prior to treatment ◦ Excluded from session length determination
ASHA certified SLPs
Accurate production of sound target in words produced in probes
30 words for each set presented one at a time by examiner and repetition requested
Scored online with audio recordings used for verification
Target required to be produced… ◦ Without distortion
◦ In correct location of word
◦ Number of correct syllables required
66
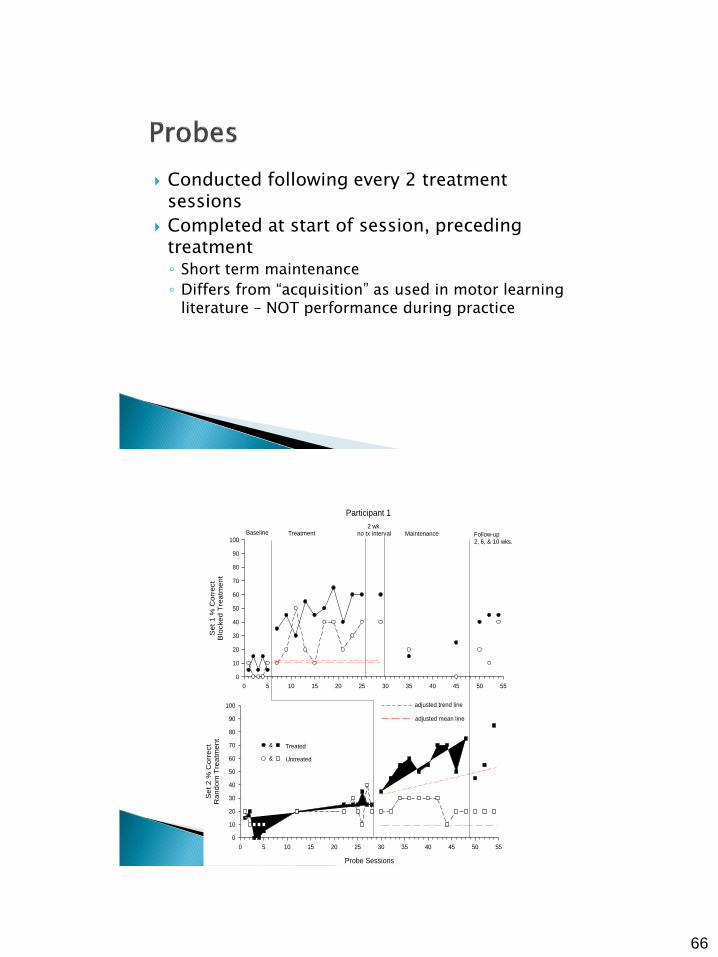
Conducted following every 2 treatment sessions
Completed at start of session, preceding treatment ◦ Short term maintenance
◦ Differs from “acquisition” as used in motor learning literature – NOT performance during practice
Participant 1
0 5 10 15 20 25 30 35 40 45 50 55
Set
1 %
Corr
ect
Blo
cked T
reatm
ent
0
10
20
30
40
50
60
70
80
90
100
Probe Sessions
0 5 10 15 20 25 30 35 40 45 50 55
Set
2 %
Corr
ect
Random
Tre
atm
ent
0
10
20
30
40
50
60
70
80
90
100
Baseline Treatment Maintenance Follow-up2, 6, & 10 wks.
2 wk.no tx interval
Treated
Untreated
&
&
adjusted trend line
adjusted mean line

67
Participant 2
0 5 10 15 20 25 30 35 40 45 50 55 60 65
Set
1 %
co
rrect
Rando
m T
rea
tmen
t
0
10
20
30
40
50
60
70
80
90
100
Probe Sessions
0 5 10 15 20 25 30 35 40 45 50 55 60 65
Set
2 %
Corr
ect
Blo
cked T
rea
tmen
t
0
10
20
30
40
50
60
70
80
90
100
Baseline Treatment Maintenance2 wk.
no tx interval
Follow-up2,6,&10 wks.
Treated
Untreated
&
&
adjusted trend line
adjusted mean line
Participant 3
0 5 10 15 20 25 30 35 40 45 50 55 60
Se
t 1
% C
orr
ect
Ra
nd
om
Tre
atm
en
t
0
10
20
30
40
50
60
70
80
90
100
Probe Sessions
0 5 10 15 20 25 30 35 40 45 50 55 60
Se
t 2
% C
orr
ect
Blo
cke
d T
rea
tme
nt
0
10
20
30
40
50
60
70
80
90
100
Baseline Treatment 2 wk.no tx interval
MaintenanceFollow-up
2, 6, & 10 wks.
Treated
Untreated
&
&
adjusted trend line
adjusted mean line

68
Participant 4
0 5 10 15 20 25 30 35 40 45 50 55 60
Set
1 %
Corr
ect
Blo
cked T
reatm
ent
0
10
20
30
40
50
60
70
80
90
100
Probe Sessions
0 5 10 15 20 25 30 35 40 45 50 55 60
Set
2 %
Corr
ect
Random
Tre
atm
ent
0
10
20
30
40
50
60
70
80
90
100
Baseline Treatment2 wk.
no tx interval Maintenance Follow-up2,6, & 10 wks.
Treated
Untreated
&
&
adjusted trend line
adjusted mean line
Participant 5
0 5 10 15 20 25 30 35 40 45 50 55 60
Set
1 %
Corr
ect
Blo
cked T
rea
tmen
t
0
10
20
30
40
50
60
70
80
90
100
110
Probe Sessions
0 5 10 15 20 25 30 35 40 45 50 55 60
Set
2 %
Corr
ect
Rando
m T
rea
tmen
t
0
10
20
30
40
50
60
70
80
90
100
Baseline Treatment
2 wk. no tx interval Maintenance Follow-up
2, 6, & 10 wks.
Treated
Untreated
&
&
adjusted trend line
adjusted mean line

69
Participant 6
0 5 10 15 20 25 30 35 40 45 50 55 60
Set
1 %
Corr
ect
Blo
cked T
reatm
ent
0
10
20
30
40
50
60
70
80
90
100
Probe Sessions
0 5 10 15 20 25 30 35 40 45 50 55 60
Set
2 %
Corr
ect
Random
Tre
atm
ent
0
10
20
30
40
50
60
70
80
90
100
Baseline Treatment Maintenance Follow-up2, 6, & 10 wks.
2 wk. no tx interval
Treated
Untreated&
&
adjusted trend line
adjusted mean line

70
See Wambaugh (2010) in Perspectives for Summary
Articulatory - kinematic approach ◦ “is a nonlinguistic sensorimotor disorder of
articulation.....Therefore, therapy should concentrate on the disordered articulation...(and) emphasize the regaining of adequate points of articulation and the sequencing of articulatory gestures” (Rosenbek et al., 1973)
Derived from Rosenbek et al.’s (1983) “8-step continuum”
Techniques ◦ Verbal and visual modeling ◦ Repeated practice ◦ Integral stimulation ◦ Minimal contrast practice
target sound paired with typical replacing sound provides articulatory contrast
71
Identify problematic sounds
Determine appropriate level/complexity of production
Prioritize sounds to be treated
Group sounds to be treated
Elicit production of all sounds in desired word positions
Productions should include several exemplars of each sound with varied phonetic context
Randomized presentation likely to be more difficult than blocked
72
Suggest selecting 1-3 sounds to be treated
at one time 8-10 items needed for each sound (if only
one word position) ◦ “items” = monosyllabic words, multisyllabic words,
words in phrases/sentences ◦ Real words preferred
matching minimal contrast words for each ◦ may need to approximate error
vary phonetic contexts!!! (variety of vowels) ◦ vary syllable shape if appropriate
/r/ = 30% accuracy ◦ ray → way
◦ rip → wip
/sh/ = 0% accuracy ◦ shy → sigh
◦ she → see
/k/ = 10% accuracy ◦ key → dee
◦ car → dar

73
Level of success
Impact on intelligibility ◦ % in error
◦ homonymy
◦ frequency of occurrence in language
Trial therapy - stimulability
ray…way (CV…eɪ) rip…whip (CVC…ɪ) rock…wok (CVC…ɑ) rue…woo (CV…u) right…white (CVC…aɪ) reed…weed (CVC…i) row…woe (CV…o) rut…what (CVC…ʌ)
74
shave…save (CVC…e) ship…sip (CVC…ɪ) shock…sock (CVC…ɑ) shoe…Sue (CV…u) shy…sigh (CV…aɪ) she…see (CV…i) show…sew (CV…o) shun…sun (CVC…ʌ)
Kay…day (CV…e) kill…dill (CVC…ɪ) cot…dot (CVC…ɑ) coo…do (CV…u) cab…dab (CVC…æ) keep…deep (CVC…i) comb…dome (CVC…o)
Ken…den (CVC…ɛ)

75
Distortions errors
More than one replacing sound
Cluster errors
Perseveration
pie….die (CV…aɪ) pot….dot (CVC…ɑ)
ping….ding (CVC…ɪ)
pea….thee (CV... i ) pay…they (CV…eɪ) pope…dope (CVC…o) pen…then (CVC…ɛ)
pert…dirt (CVC)…ɝ)

76
lie…thy (CV…aɪ) low…though (CV…o) lip…dip (CVC…ɪ) late…date (CVC…eɪ) lamb…dam (CVC…æ) lark…dark (CVCC…ɑr) luck…duck (CVC…ʌ) loose…deuce (CVC…u)
star…tar stop…top sty…tie stew…two store…tore stack…tack Stan…tan stow…toe
77
Step 1 – Modeling/Imitation
Step 2 – Modeling + Written letter cue/Imitation
Step 3 – Integral Stimulation
Step 4 – Modeling with silent juncture
Step 5 – Artic. Placement instructions & production of sound in isolation
All steps ◦ 5 additional repetitions attempted upon correct
response Step 1
◦ target only attempted initially ◦ Minimal pair introduced only upon incorrect
response Step 3
◦ Integral stimulation attempted up to 3X Step 4
◦ eliminated Step 5
◦ Integral stimulation integrated with articulatory placement cues
Blocked and random practice incorporated into trials
78
1. Say word and request repetition ◦ if correct, request additional repetitions (5 times*)
and go to next item. ◦ if incorrect, give feedback and say: “Now, let’s try
a different word” and present minimal pair word.
if correct, give feedback and say: “Now, let’s go back to the other word” & go to step 2 with the target word
if incorrect, give feedback, attempt with integral stimulation up to 3 times and go to 2 with target word
2. Show letter representing the target sound, say word, and request repetition
◦ if correct, request additional repetitions (5 times*) and go to the next item
◦ if incorrect, go to 3
79
3. Integral stimulation – “watch me, listen to me, and say it with me” up to 3 times ◦ If correct, request additional repetitions (5
times*) and go to next item ◦ If incorrect, go to 4
4. give Articulatory Placement Cues, attempt word again after cueing using integral stimulation ◦ if correct, request additional repetitions (5
times*) ◦ if incorrect, go to next item
5. go to the next item
Moderate AOS
Severe AOS /s/
/l/
/b/

80
hierarchy applied to each target word ◦ response contingent
◦ not reversed
8-10 words presented in random order = 1 trial
attempt to complete at least 6- 7 trials per session
session – 45 min to 1 hour
research application – 3X/week
1st trial: blocked presentation ◦ if target sounds are correct in <6/8 words (for any of
the sounds), next trial is blocked ◦ if target sounds are correct in 6/8+ words for all 3
sounds, next trial is randomized
if 6/8 criteria is met (on 1st or any subsequent trials), alternate between blocked and randomized for the rest of the session
but, continue with blocked until criteria is met

81
Blocked
pie, pot, ping, pea, pay, pope, pen, pert
say, sis, seal, sigh, sue, sock, sank, soap
loose, luck, lamb, lark, lie, low, lip, late
Randomized
sis, pope, ping, low, late, sigh, pert, loose, soap, say, pen, luck, pot, sock, lamb….etc.
Probe vs. treatment data
Acquisition measure: is the person learning what he/she has been working on in therapy?
Can the target behaviors be produced when not in the context of therapy? (under similar conditions, but without treatment occurring)

82
Response Generalization Measure – to untrained exemplars of trained behaviors
Production of items that are very similar to the trained items ◦ same target sound
◦ same syllable structure
◦ same elicitation procedure
Response Generalization Measure – to untrained behaviors
production of behaviors that are related to, but not the same as, the trained behaviors ◦ different, but related sound ◦ voiced cognate ◦ similar in manner or place ◦ behavior that MIGHT respond to the treatment of the
trained behavior
83
Stimulus Generalization Measures – to untrained contexts
production of the behavior in contexts that vary from the training context ◦ complexity ◦ phonetic environment ◦ method of elicitation
how where who
Acquisition: 24 trained items produced in response to examiner model prior to treatment session; no feedback; no treatment
Response Generalization (untrained exemplars): 4-5 untrained items of trained sounds ◦ pack, pole, pop, paw
◦ seed, sign, saw, soup
◦ leak, limb, load, lay

84
Response Generalization – untrained, related sounds ◦ /p/ by, bee, bed, bit, bay ◦ /s/ zoo, zip, Zane, zeal, zing ◦ /l/ ??
Stimulus Generalization ◦ different word position ◦ phrases ◦ bisyllabic words ◦ different elicitation mode (e.g., story completion) ◦ etc.
Pt: 55 yr old male, 24 mpo, severe AOS with verbal perseveration, mod-severe Broca’s aphasia
results of sound testing: all sounds except /w/ and /n/ produced incorrectly
perseveration: “water” or variant (i.e., replacing sound = /w/)

85
Develop 8 treatment items and 5 response generalization items (untrained exemplars of trained) for /b/, /s/, /l/ ◦ use CV and CVC syllable shapes
Develop 8 treatment items and 5 response generalization items for /m/ , /f/, /d/ ◦ CV and CVC
Develop response generalization stimuli for sounds of interest ◦ untrained exemplars of untrained, related sounds
◦ suggest 5 exemplars for each
86
Develop at least 2 stimulus generalization tasks to assess treatment effects
3 participants ◦ Moderate to severe, chronic AOS
◦ Significant Broca’s aphasia
SPT applied to one sound at a time
Multiple baseline design across sounds and participants
87
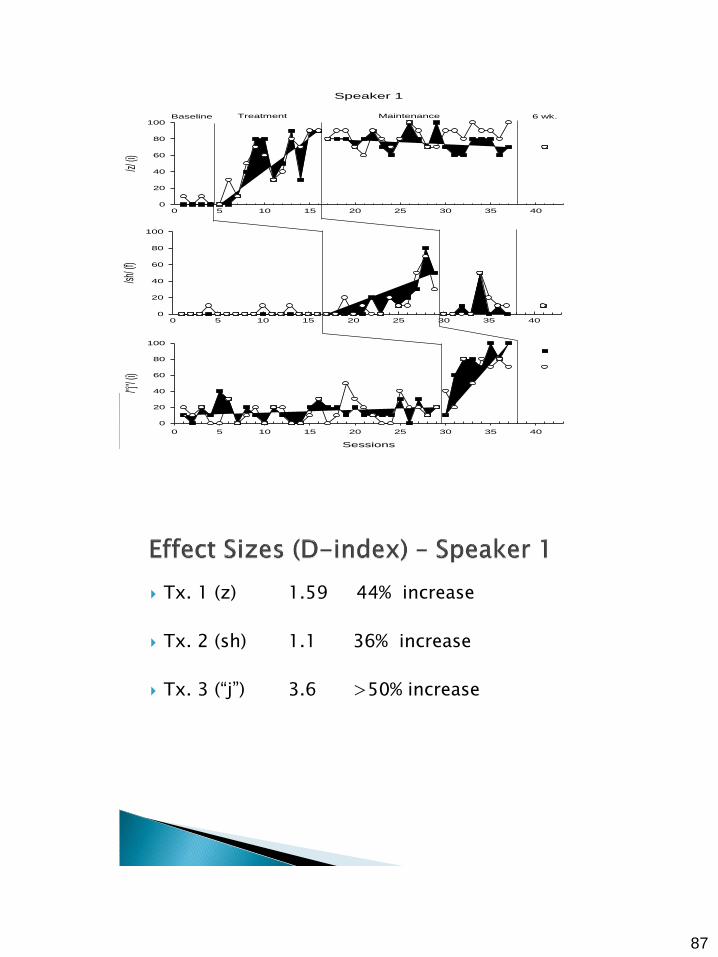
Speaker 1
0 5 10 15 20 25 30 35 40
/z/ (i)
0
20
40
60
80
100
0 5 10 15 20 25 30 35 40
/sh/ (
f)
0
20
40
60
80
100
Sessions
0 5 10 15 20 25 30 35 40
/"j"/
(i)
0
20
40
60
80
100
Baseline Treatment Maintenance 6 wk.
Tx. 1 (z) 1.59 44% increase
Tx. 2 (sh) 1.1 36% increase
Tx. 3 (“j”) 3.6 >50% increase

88
Speaker 2
0 5 10 15 20 25
/sh/ (i
)
0
20
40
60
80
100
0 5 10 15 20 25
/r/ (i)
0
20
40
60
80
100
Sessions
0 5 10 15 20 25
/sw/ (i
)
0
20
40
60
80
100
Baseline Treatment Maintenance 6-wk
Measured to target words embedded in phrases
Speaker 1 – slight change (40% increase) for 1 sound
Speaker 2 – increase to 80% accuracy for all 3 sounds
Speaker 3 – no sustained changes for any sound

89
Wambaugh & Martinez, 2000
Mauszycki & Wambaugh, 2008
Schematic and tapping review
↓ ___ ___ Metronome set at reduced rate (increase
word durations about 50%) ◦ CM – one production ◦ Patient taps along while clinician models (4-5X) ◦ Unison production and tapping (3X) ◦ Patient production (1X)
Feedback = about tapping accuracy, # syllables, production to the beat (not about sound production)
Target items presented in random order (n=20; ?X)

90
Benefit
↓ ___ ___ Spaghetti
___ ↓ ___
Represent
___ ___ ↓
Schematic & tapping review Reduced metronome setting ◦ Clinician model (1X) ◦ PPT (3X)
If errors (tapping to beat or # syllables) then CM (1X) + unison production and tapping
If correct – next word
Feedback – same Scoring: +/- for 1st production of PPT

91
Schematic & tapping review
Metronome set to reduced rate ◦ Clinician produces word with normal rate &
prosody (not to the beat and with no tapping)
◦ PPT (3X) If errors (tapping to beat or # syllables) then CM (1X) +
PPT (3X)
If errors remain, then CM (1X) + UPT (3X)
If correct – next word
Feedback – same
Scoring: +/- for 1st production of PPT
Schematic & tapping review
Metronome setting increased from previous levels ◦ Clinician produces word with normal rate &
prosody (not to the beat and with no tapping)
◦ PPT (3X) If errors (tapping to beat or # syllables) then CM (1X) +
PPT (3X)
If errors remain, then CM (1X) + UPT (3X)
If correct – next word
Feedback – same
Scoring: +/- for 1st production of PPT
92
Clinician explains concept of syncopation ◦ Target word produced in 2 beats
◦ 1st syllable on first beat
◦ 2nd syllable & 3rd syllable on second beat
Schematic, tapping review
Metronome set at Level 4 rate
Apply syncopation to Levels 1-4
ignorant management crocodile therapy cranium dangerous rosary industry replica generate camisole moccasin
treasury dignity badminton restaurant habitat Winchester celibate satisfy wonderful saxophone fabulous

93
Dangerous Regular Moccasin* Chivalry* Casual* Cranium* Restaurant Calcium* Generate Recipe Beautiful* Fabulous Management* Casserole * = UNTRAINED,
GENERALIZATION ITEMS
Rosary* Wonderful Hospital* Antelope Sensitive* Therapy Badminton Benefit Winchester* Celibate Replica* Dignity* Treasury* Galaxy
Target Pre-Post
% words
Pre-Post
%Cs
Group 1 – Tx. (1st syllable) 9 - 72 64 – 94
Group 1 – Untx. 5 - 60 75 – 85
Group 3 – Tx. (3rd syllable) 20 - 90 67 – 91
Group 2 – Untx. (2nd syllable) 29 - 48 79 – 95
Group 4 – Untx. (4 syllables) 16 - 35 70 – 86
Group 5 – Untx. (blends) 28 - 60 81 - 90

94
Few significant durational changes in probes
Increased duration of 1st syllable
Increased ratio of 1st syllable to total word
Consider combining with a-k
Select rate for practice
Select tx. items
Select generalization items

95
Hand-tapping – hand/location
Amount of therapist instruction/modeling – fading of participation
Type of metronome control – Visible? Audible?
Criteria for changing timing
Type/amount/timing of feedback
Outcome measures